© The Author 2015. Published by Oxford University Press on behalf of the Journal of Public Administration Research and Theory, Inc. All rights reserved. For permissions, please e-mail: [email protected]. 309 Journal of Public Administration Research And Theory, 2016, 309–326 doi:10.1093/jopart/muv016 Article Advance Access publication June 25, 2015 Article Antecedents and Consequences of Corporatization: An Empirical Analysis of German Public Hospitals Ivonne Lindlbauer,* Vera Winter, † Jonas Schreyögg † *University Medical Center Hamburg-Eppendorf; † University of Hamburg Address correspondence to the author at [email protected]. The article is our original unpublished work, and there are no submissions or previous reports that might be regarded as redundant or duplicate publication of the same or very similar work. The article was never submitted before to any journal. Abstract The idea of privatizing or corporatizing public enterprises to improve organizational performance is a central tenet of the new public management movement.Yet while privatization represents a well-estab- lished subject of inquiry, corporatization remains a research field scarcely trodden, leaving the public debate bereft of sound empirical evidence. Building on the contingency theory, principal-agent theory, and corporatization literatures, the purpose of this study is to help bridge this research gap by empiri- cally assessing the postulated relationships on the antecedents and consequences of corporatization. Choosing public hospitals as research subjects, it builds on a comprehensive longitudinal dataset and proceeds in four steps: calculating efficiency scores using data envelopment analysis; investigating the antecedents of corporatization with logistic regression; constructing an appropriate control group consisting of noncorporatized public-law hospitals using genetic matching; and comparing changes in efficiency between corporatized and noncorporatized hospitals by means of a difference-in-difference approach. The results indicate that public-law hospitals were significantly more likely to be corpora- tized under certain circumstances, namely, in areas with a higher degree of spatial competition, dur- ing the years around a major change in the reimbursement system (2003–2005), and if they were legally dependent entities. In contrast, having lower baseline efficiency had no significant effect on the likelihood of corporatization. Furthermore, corporatization had a significantly positively effect on the efficiency of previously public-law hospitals. This effect was higher for hospitals that had been legally independent than for those that had been legally dependent. In sum, corporatization is likely an effec- tive alternative to privatization, a finding that leads to a range of implications for practice and research. Introduction The new public management (NPM) movement has had a profound impact on the public sector globally, leading to several decades of government reforms aimed at improving the performance of public enter- prises (Ferlie 1996; Hood 1991). The movement is based on the idea of reforming the management of these enterprises, which are bureaucratic, inefficient, lacking in service orientation, and strongly influ- enced by politics. In a time of tight public budgets and market changes following the global financial crisis of 2007/08, there is still a need to draw on concepts from NPM. Indeed, governments in a range of coun- tries have been under pressure to reduce the scope of This study was supported by a research grant from the German Federal Ministry of Education and Research (BMBF) in Germany (Grant number: 01FL10055). The sponsor had no role in the study design, collection, and analysis of data, the writing of the report or the submission of the article for publication. We thank three anonymous reviewers for their valuable comments and suggestions. Downloaded from https://academic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 March 2022

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
© The Author 2015. Published by Oxford University Press on behalf of the Journal of Public Administration Research and Theory, Inc. All rights reserved. For permissions, please e-mail: [email protected].
309
Journal of Public Administration Research And Theory, 2016, 309–326doi:10.1093/jopart/muv016
ArticleAdvance Access publication June 25, 2015
Article
Antecedents and Consequences of Corporatization: An Empirical Analysis of German Public HospitalsIvonne Lindlbauer,* Vera Winter,† Jonas Schreyögg†
*University Medical Center Hamburg-Eppendorf; †University of Hamburg
Address correspondence to the author at [email protected]. The article is our original unpublished work, and there are no submissions or previous reports that might be regarded as redundant or duplicate publication of the same or very similar work. The article was never submitted before to any journal.
Abstract
The idea of privatizing or corporatizing public enterprises to improve organizational performance is a central tenet of the new public management movement. Yet while privatization represents a well-estab-lished subject of inquiry, corporatization remains a research field scarcely trodden, leaving the public debate bereft of sound empirical evidence. Building on the contingency theory, principal-agent theory, and corporatization literatures, the purpose of this study is to help bridge this research gap by empiri-cally assessing the postulated relationships on the antecedents and consequences of corporatization. Choosing public hospitals as research subjects, it builds on a comprehensive longitudinal dataset and proceeds in four steps: calculating efficiency scores using data envelopment analysis; investigating the antecedents of corporatization with logistic regression; constructing an appropriate control group consisting of noncorporatized public-law hospitals using genetic matching; and comparing changes in efficiency between corporatized and noncorporatized hospitals by means of a difference-in-difference approach. The results indicate that public-law hospitals were significantly more likely to be corpora-tized under certain circumstances, namely, in areas with a higher degree of spatial competition, dur-ing the years around a major change in the reimbursement system (2003–2005), and if they were legally dependent entities. In contrast, having lower baseline efficiency had no significant effect on the likelihood of corporatization. Furthermore, corporatization had a significantly positively effect on the efficiency of previously public-law hospitals. This effect was higher for hospitals that had been legally independent than for those that had been legally dependent. In sum, corporatization is likely an effec-tive alternative to privatization, a finding that leads to a range of implications for practice and research.
Introduction
The new public management (NPM) movement has had a profound impact on the public sector globally, leading to several decades of government reforms
aimed at improving the performance of public enter-prises (Ferlie 1996; Hood 1991). The movement is based on the idea of reforming the management of these enterprises, which are bureaucratic, inefficient, lacking in service orientation, and strongly influ-enced by politics. In a time of tight public budgets and market changes following the global financial crisis of 2007/08, there is still a need to draw on concepts from NPM. Indeed, governments in a range of coun-tries have been under pressure to reduce the scope of
This study was supported by a research grant from the German Federal Ministry of Education and Research (BMBF) in Germany (Grant number: 01FL10055). The sponsor had no role in the study design, collection, and analysis of data, the writing of the report or the submission of the article for publication. We thank three anonymous reviewers for their valuable comments and suggestions.
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022

310 Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
traditional government bureaucracies or to find new ways of delivering services, aiming to reduce costs or respond more effectively to market pressures. For many public organizations, increasing efficiency has become a crucial prerequisite for organizational sus-tainability. From an organizational perspective, two options for doing so are privatization and corporati-zation. Privatization involves selling formerly public organizations to private owners, whereas corporatiza-tion represents a change in legal form that separates service delivery from traditional government agencies while keeping the organization in public hands. Even though the specifics of such a change and the labeling of the newly formed entities vary from country to coun-try, corporatization generally entails a shift toward a more business-like form, with the new entity having its own legal identity regulated by private law, as well as increased managerial autonomy. The expected benefits of corporatization include improvements in efficiency and overall performance, which can be generated by greater managerial latitude and reductions in agency problems, enabling an organization to adapt more flexibly to environmental conditions (Aidemark and Lindkvist 2004; Aivazian, Ge, and Qiu 2005; Bilodeau, Laurin, and Vining 2007). However, while privatiza-tion and its consequences have been treated extensively in the management literature (Cuervo and Villalonga 2000; Tiemann and Schreyögg 2012), corporatization has not, even though it is no less common (Bilodeau, Laurin, and Vining 2007). Several authors have there-fore called for further research (Bilodeau, Laurin, and Vining 2007; Boyne 2003; Braithwaite, Travaglia, and Corbett 2011; Dan 2014).
The purpose of the present study is to provide com-prehensive empirical evidence on the antecedents and consequences of corporatization, focusing in particu-lar on efficiency gains. To do so, it uses the hospital industry as a research setting and draws on panel data from the years 2002 through 2010, allowing corpora-tized public organizations to be contrasted quantita-tively with noncorporatized public organizations using a large dataset. A range of hypotheses are first derived and tested based on a sample of 121 corporatized and 104 noncorporatized hospitals in Germany. The results are subsequently discussed alongside implications for practice and research.
Prior Literature on Corporatization
Prior studies relevant in our research context analyze the effects of NPM reforms in general, agencifica-tion as a related phenomenon, and corporatization. Additionally, corporatized and noncorporatized public organizations strongly differ in their degrees of close-ness to the government and politics—a distinction that
has often been analyzed under the notion of public-ness, which represents a well-established research field (Andrews, Boyne, and Walker 2011). Pollitt and Dan (2011) conducted a meta-analysis on the impacts of NPM in Europe, stating that the majority of studies find performance improvements, but a lot of studies also do not find any substantial changes in performance. They do not differentiate between effects of corporatization as one NPM mechanism, which is treated in 7.6% of the included studies, and effects of other NPM tools and mechanisms. They emphasize the lack of empiri-cal studies that convincingly address efficiency change. Dan (2014) reviews studies analyzing agencifications in Europe and finds that these often yield improve-ments in processes, user orientation, transparency, and accountability. Yet he also raises concerns related to fragmentation, coordination, or organizational sta-bility as unintended consequences of agencification. Moreover, Dan (2014) stresses that there is limited evidence on technical efficiency; in particular, he notes that “there is insufficient evidence to show that output levels improved, remained unchanged, or decreased less than the level of inputs”.
Agencification may or may not be set equal to cor-poratization. While some studies treat both concepts as synonyms (e.g., Dan 2014; Yamamoto 2006), oth-ers define agencification as internal autonomization or delegation within the public administration without legal independence and contrast it to corporatization as external autonomization or delegation to bod-ies outside the public administration (e.g., Lægreid, Roness and Rolland 2013). Vining, Laurin, and Weimer (2014) posit that agencies are almost never as autonomous as state-owned enterprises (which might result from corporatization), but they are usually more autonomous than traditional line bureaus that perform similar tasks. However, when examining the empirical evidence on agencification and performance, they also refer to corporatization studies. Hence, the implicit assumption is that agencification and corporatization, while having different starting and ending points with regards to the degree of autonomy, are comparable in terms of autonomization changes and their effects on performance. In line with this view, and due to the blurring boundaries between the two concepts as well as the paucity of quantitative empirical research, we refer to both agencification and corporatization studies in the following.
Studies empirically analyzing agencification effects mostly assess performance over several years, yet are often characterized by small sample sizes. Based on principal-agent theory, Bilodeau, Laurin, and Vining (2007) postulated that corporatization may reduce information asymmetry, leading to improved per-formance in governmental agencies. To test their
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022

311Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
hypothesis, they compared different pre- and post-periods for 11 corporatizations undertaken in Canada by the federal and Québec governments. The authors used the performance indicators total output, total revenues, revenues-to-expenditure ratio, output-to-expenditure ratio, and employee productivity. In a finding consistent with their hypothesis, they detected positive performance effects, except for the output-to-expenditure ratio, for the 3 years following corpora-tization. Pérez-López, Príor, and Zafra-Gómez (2015) analyzed how a set of NPM delivery forms, including agencification, affects the efficiency of local govern-ments, disaggregated into 8 types of services. They calculated efficiency scores for 1,058 Spanish munici-palities for the period 2001–2010 using the nonpara-metric order-m partial frontier approach. In truncated regression models with bootstrapped efficiency as dependent variable, they found the impact of agencies on efficiency varied depending on the public service provided. For some services, the impact was further-more moderated by the current economic situation. Vining, Laurin, and Weimer (2014) assessed labor pro-ductivity, financial performance, and costs of 13 agen-cies in Québec over 10 years. To detect performance effects, they conducted before-after-comparisons and panel regressions. They found annual gains in produc-tivity which persisted over an extended period, while the magnitude of these annual gains decreases over time. Yamamoto (2006) used a retrospective survey method to detect agencification effects in Japanese independent administrative institutions. Based on the responses of 181 individuals from 57 institutions, he mostly relied on descriptive analyses of results, sup-plemented by regression analysis to explain (subjec-tively reported) changes in performance attributed to corporatization. He concluded that respondents gen-erally consider organizational effectiveness, efficiency, quality, and accountability to be improved. Changes in performance have been in particular caused by changes in operational autonomy.
Studies addressing performance effects of corpora-tization are also rather scarce and heterogeneous with respect to methodology and performance measures. Aivazian, Ge, and Qiu (2005) investigated the corpo-ratization of state-owned enterprises in China using a sample of 308 corporatized firms. They found that prior performance had no impact on the probability that a state-owned enterprise would be corporatized. In regression analyses using different performance indica-tors (i.e., return on assets, return on sales, real output per employee, and real sales per employee), the authors included indicator variables for six post-corporatiza-tion years. Their results suggest that corporatization had a positive effect that increased over time. Cambini et al. (2011) assessed cost effects of corporatization
based on a sample of 33 local bus companies with cost data between 1999 and 2002. Estimating a gen-eralized least squares random-effects model based on a Translog cost function, they found that (two differ-ent versions of) corporatization of Italian bus entities resulted in a reduction of production costs. Nelson and Nikolakis (2012) investigated the corporatization of six Australian state-level forest state-owned enter-prises over the period 1989 to 2007. From descrip-tive analyses and interviews with representatives from each enterprise, they concluded that corporatization led to improvements in productivity (i.e., output per employee) and profitability.
Some empirical studies have used the hospital industry as a research setting. Aidemark and Lindkvist (2004) analyzed the effects of corporatization in two Swedish hospitals. They drew on group meetings, board meetings, and interviews with politicians, board members, management, and operational hospital staff over a 9-month period during the second year after the hospitals had been reorganized as limited compa-nies. They identified changes in leadership structure and management systems, as well as an improvement in production and financial resources. Rego, Nunes, and Costa (2010) assessed the effect of corporatiza-tion on efficiency using a sample of 59 Portuguese hos-pitals from 2002 through 2004. They calculated two different efficiency measures using data envelopment analysis (DEA). By comparing mean efficiencies, they found that efficiency values rose in corporatized hos-pitals in both years after the reform, while noncorpo-ratized hospitals did not always show positive changes in efficiency. Ferreira and Marques (2014) analyzed efficiency effects of corporatization in a sample of 49 Portuguese hospitals from 2002 to 2009. They use a Malmquist index to measure group performance, differentiate three ownership forms (two of which represent forms of corporatization, namely, hospital enterprises and corporate public entities) and estimate five efficiency models. While corporate public entities are more efficient than hospital enterprises in most models, noncorporatized administrative public sector hospitals exhibit significantly higher mean efficiency than both groups of corporatized hospitals.
Although these studies have generated valuable ini-tial insights into the antecedents and consequences of corporatization, the generalizability of their findings remains limited. The majority of studies did not com-pare corporatized organizations with noncorporatized organizations, making it difficult to attribute all changes in their outcome measures to the change in organiza-tional form. Furthermore, none of the studies ensured that baseline characteristics were balanced across the corporatized and noncorporatized firms. Failing to ensure that control variables are similarly distributed,
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022

312 Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
however, may lead to the effect of an intervention being overestimated or underestimated limiting the scope for robust policy recommendations (Cochran and Rubin 1973; Diamond and Sekhon 2013). Additionally, prior evidence is inconsistent regarding the longevity of the impact of corporatization. While Aivazian, Ge, and Qiu (2005) found increasing effects, Vining, Laurin, and Weimer (2014) detected that the effect decreased over time. Finally, most previous studies have been based on small samples limiting external validity of the findings. Further research in this field is therefore war-ranted to confirm these preliminary findings.
Corporatization and Privatization in the German Hospital Context
Public hospitals in Germany compete with private non-profit and private for-profit hospitals. This competition has been aggravated by the introduction in 2004 of a prospective reimbursement system based on diagnosis-related groups (DRGs). Payment systems of this nature had already been implemented in many other countries by this time and were introduced in regulated hospi-tal markets to reduce length of stay and increase effi-ciency through yardstick competition (Shleifer 1985; Hafsteinsdottir, Gudrun and Siciliani 2010). Broadly speaking, a DRG payment reflects the average cost of patients in a given DRG during a preceding period, and hospitals are likely to be on the winning side by not producing above-average costs. As a result, public hospitals need to find efficient and effective ways to sustain a competitive position. Two possible avenues are hospital privatization and corporatization.
Like most public institutions in Germany, public hos-pitals can have either a public legal form or a private legal form. For the sake of brevity, those with a public legal form will henceforth be described as “public-law hospitals,” and those with a private legal form will hence-forth be described as “private-law hospitals.” Private-law hospitals should not be confused with private for-profit or private nonprofit hospitals, neither of which are con-sidered in the present study. An overview over the differ-ent ownership and legal forms is given in figure 1.
Public-law hospitals have a typical administrative and hierarchical public management structure due to the standards set forth in public law. Furthermore, they are bound to tariff agreements for public services, such as regulated company pension schemes, and are therefore inflexible in their remuneration system. Outsourcing is restricted by public procurement law. In sum, they have a fairly restricted degree of mana-gerial autonomy with respect to finances and human resources. Public-law hospitals can be either legally dependent or legally independent. Legal dependence implies the unlimited liability of the public owner, a
more restricted degree of managerial autonomy, and the strong influence of political authorities. In particu-lar, in legally dependent public-law hospitals, political representatives of the local government, for example, the governing mayor, the local health select commit-tee, and often a committee of several representatives in different functions, have the supreme decision-making power over the executive management of the hospi-tal. This often results in bureaucratic, hierarchical lines of supervision and decision-making power. In legally independent hospitals, the executive management of the hospital is not directly dependent on the local government. Yet it is controlled by the supervisory board which contains only political representatives. Therefore, structures are less bureaucratic, but still subject to quite large political influences.
In private-law hospitals, the state holds the major-ity, if not all, of the shares. These hospitals are usually organized as limited liability companies (“Gesellschaft mit beschränkter Haftung”) or, less frequently, as incorporated companies with limited liability (“Aktiengesellschaft”). The executive management board of the hospital is controlled by a supervisory board, which comprises political representatives and hospital employees. These hospitals are generally flex-ible in their human resource management because they are not bound to employee tariffs and often establish affiliated companies for personnel services or may out-source services. As a result, they have more managerial autonomy, a business-like governance structure and greater flexibility. Hence, they might be compared what is called to state-owned enterprises in other studies.
In the present study, corporatization is defined as the shift, in a public hospital, from a public legal form to a private legal form. Similar definitions have been used in other studies on corporatization. Moreover, differences in management autonomy between corpo-ratized and noncorporatized public hospitals in this context are similar to those reported in other stud-ies (Aidemark and Lindkvist 2004; Aivazian, Ge, and Qiu 2005; Bilodeau, Laurin, and Vining 2007; Rego, Nunes, and Costa 2010).
In 2002, there were 817 public hospitals in Germany, 72% of which were public-law hospitals. Among the public-law hospitals, a large majority (79%) were legally dependent. By 2010, there were 630 public hospitals, 42% of which were public-law hospitals. Among the public-law hospitals, 45% were legally dependent (Federal Statistical Office of Germany [Destatis] 2012a). This large shift in legal form frequencies reflects the impact of the NPM move-ment on the public provision of health care services and suggests the tight financial situation of local and state governments. The substantial decrease in the total number of public hospitals (from 817 to 630) is in part
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022

313Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
due to privatizations. As mentioned above, there exists relatively sound empirical evidence on the effects of privatizations, also in the hospital context. Drawing on the same dataset used in this study and applying a very similar methodology, Tiemann and Schreyögg (2012) detected significant net efficiency gains after hospital privatizations. Empirical evidence for net efficiency gains after corporatizations, however, is still pending.
Theoretical Background and Hypothesis Development
Contingency theory postulates that “the best way to organize depends on the nature of the task environ-ment to which the organization relates” (Scott and Davis 2007, 127). It has been widely used in both theo-retical and empirical studies on organizational strategy to analyze the relationship between the organizational environment and decision-making (Ginsberg and Venkatraman 1985; Hofer 1975; Jauch, Osborn, and Glueck 1980; Zajac, Kraatz, and Bresser 2000). The theory implies that environmental factors affect deci-sions about the most appropriate organizational form for a given organization, which in the case of public-law organizations might entail the decision for corpo-ratization. The environmental factors that affect such decisions, however, are largely unclear and context-specific (Beach and Mitchell 1978). Hypotheses on four antecedents of corporatization are derived below.
One environmental factor that may increase the likeli-hood of organizational change is the competitive situa-tion within an industry (Zajac, Kraatz, and Bresser 2000). This situation may vary spatially. If there are many hos-pitals in one area competing for the same patients, the degree of competition will be higher than in areas with fewer hospitals. In turn, higher competition may exert isomorphic pressures on hospitals to adapt their organi-zational form. Public-law hospitals in highly competitive areas may therefore be more likely to be corporatized than public-law hospitals in less competitive areas. Thus, the first hypothesis could be phrased as follows:
H1: A higher degree of spatial competition increases the likelihood that a public-law hospital will be corporatized.
Another environmental factor that may increase the likelihood of organizational change is a change in regulation. By altering market mechanisms, regula-tory change can affect the competitive environment. An example in Germany was the introduction in 2004 of the DRG system, which led to severe reductions in the revenue of many hospitals. This often represented an existential threat, spurring hospitals to find ways to increase their efficiency. Indeed, the DRG system introduced an unprecedented notion of competition to the German hospital industry, as existing overcapaci-ties became unaffordable and hospitals had to increase occupancy, often at the expense of less successful hos-pitals. Faced by these new competitive pressures imme-diately before and after the introduction of the DRG system, public-law hospitals may have been more likely to be corporatized as a strategy to obtain a better envi-ronment–organization fit. The second hypothesis can therefore be phrased as follows:
H2: Public-law hospitals are more likely to be corporatized in the years around the intro-duction of a DRG system than during other periods.
In addition to environmental factors, there may be internal, organizational characteristics that affect the organization-environment fit and therefore the likeli-hood of organizational change. For example, this fit may vary across public-law hospitals depending on whether they are legally dependent or legally inde-pendent. Those that are legally dependent have a very low degree of managerial autonomy, characterized as they are by hierarchical, bureaucratic structures that make it difficult to react to market challenges. Furthermore, the public owner of these hospitals has unlimited liability, which could be regarded as inappropriate in times of high public debt. In con-trast, hospitals that are legally independent represent a lower risk to their public owner and have greater managerial autonomy, allowing them to act more flexibly. Public-law hospitals that are legally depend-ent may therefore perceive a greater need to adapt their organizational form than public-law hospitals that are legally independent:
Public hospitals Private hospitals (in private law)
Public-law hospitals Private-law hospitals
Private for-profit hospitals
Private non-profit hospitals
legally dependent legally independent
• completely state owned
• unlimited liability
• completely state owned
• limited liability
• state holds at least minimum of shares
• limited liability
• For-profit ownerholds at least minimum of shares
• Non-profit ownerholds at least minimum of shares
Corporatization
Privatization
Figure 1. Overview of hospital ownership and legal forms.
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022

314 Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
H3: Public-law hospitals that are legally dependent are more likely to be corpora-tized than public-law hospitals that are legally independent.
Finally, the organization-environment fit might be reflected in a hospital’s performance, specifically in its efficiency. Hospitals that operate inefficiently experi-ence a stronger need for organizational change and perceive greater potential to improve their perfor-mance (Aivazian, Ge, and Qiu 2005). As the aim of corporatization is to identify and exploit an organiza-tion’s full potential in terms of performance, this kind of organizational change may be a likely response to poor baseline efficiency, leading to the next hypothesis:
H4: Lower baseline efficiency increases the like-lihood that a public-law hospital will be corporatized.
Whether corporatization is truly an effective way to improve efficiency is still unclear. From a theoreti-cal perspective, the expected positive effects of reor-ganizing public entities, be it through privatization or corporatization, are often grounded in principal-agent theory (Bilodeau, Laurin, and Vining 2007; Hood 1991; Wistrich 1992). In public-law hospi-tals, the public owner as the principal and the hos-pital management as the agent are fairly distant and often connected via hierarchical, bureaucratic lines of authority. The principal’s role is often divided between several public authorities and committees comprising elected politicians. This results in a series of princi-pal-agent relationships, increasing the potential for self-interest and multiple objectives while creating long decision-making processes and high information asymmetries. At the same time, the distance between the principal(s) and the agent can impede a trusting, sustainable relationship. A lack of trust may lead to high agency costs for supervision, while a diversity of objectives may hamper actions that could improve efficiency. For instance, political objectives such as popularity and winning elections, as well as politi-cal disputes between the actors, may occasionally shift the focus away from what might be the best for a given hospital (Aidemark and Lindkvist 2004; Brown, Waterhouse, and Flynn 2003). Streamlining the principal’s role into one body, such as the super-visory board in a private-law organization, can help to shorten the distance between the principal and the agent and therefore create more efficient decision-making processes. Additionally, corporatization is accompanied by financial reporting requirements, which may further reduce information asymmetries and increase the accountability of the agent. In sum, corporatization may be an effective way to reduce
principal-agent problems, streamline the interests of the different decision makers, and allow for more flexible decision-making—all of which could help hospitals realize efficiency gains.
Aside from decreasing political control, increasing managerial autonomy and reducing information asym-metry, corporatization can also have a symbolic effect. A more business-like organizational form might induce a change in mentality and motivation among employ-ees, leading to a change in their working behavior and thus to more efficiency (Boyne 2003; Bilodeau, Laurin, and Vining 2007). Moreover, private-law hospitals can be sold to a private investor more easily than public-law hospitals. This could represent a constant threat to employees, making them more conscious of the need to maintain or increase productivity. Additionally, in con-trast to the supervisory boards of private-law hospitals, the controlling bodies of public-law hospitals do not include employee representatives. As a result, employees in public-law hospitals may feel more involved in manage-rial design and decision-making processes after corpora-tization, reducing internal information asymmetries and leading to a common way of acting and thinking. This may have positive effects on employees’ motivation and their acceptance of economically necessary changes. All in all, corporatization likely results in efficiency gains for public-law hospitals, as expressed in the next hypothesis.
H5: The corporatization of public-law hospitals has a positive effect on efficiency.
Even though they are both governed by public law, legally dependent and legally independent public-law hospitals may benefit differently from corporatization. Legal dependence may not be the best way to organize a hospital, whereas the managerial patterns of legally independent hospitals may be closer to those of the private industry. Legally dependent hospitals operate under the strongest political influence, are the least able to respond quickly to market changes, and have the narrowest managerial latitude. It is therefore likely that they have greater potential to improve efficiency through organizational change than do their legally independent counterparts. This results in the assump-tion that the degree of legal autonomy has a moderat-ing effect on the relationship between corporatization and efficiency, as expressed in the following hypothesis:
H6: A public-law organization’s degree of legal autonomy moderates the effect of corpo-ratization on efficiency, and the effect of corporatization on efficiency is greater for organizations that are legally dependent.
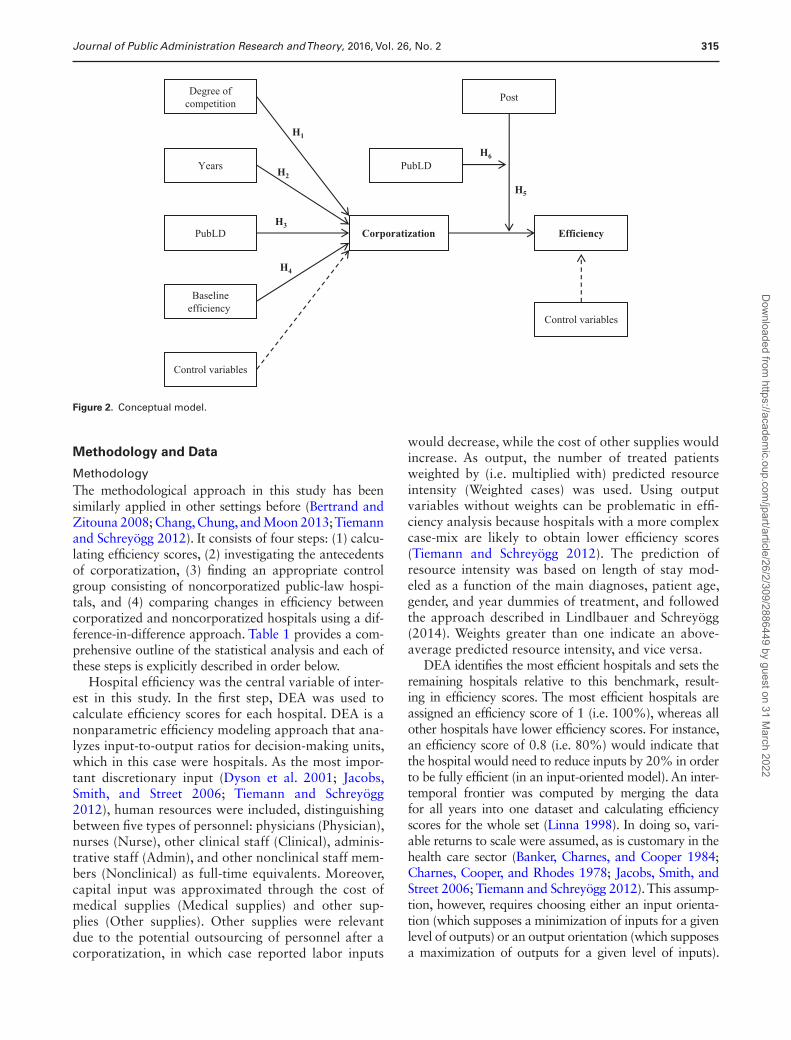
Figure 2 provides an overview of the conceptual model comprising these hypotheses on the antecedents and consequences of corporatization.
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022
315Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
Methodology and Data
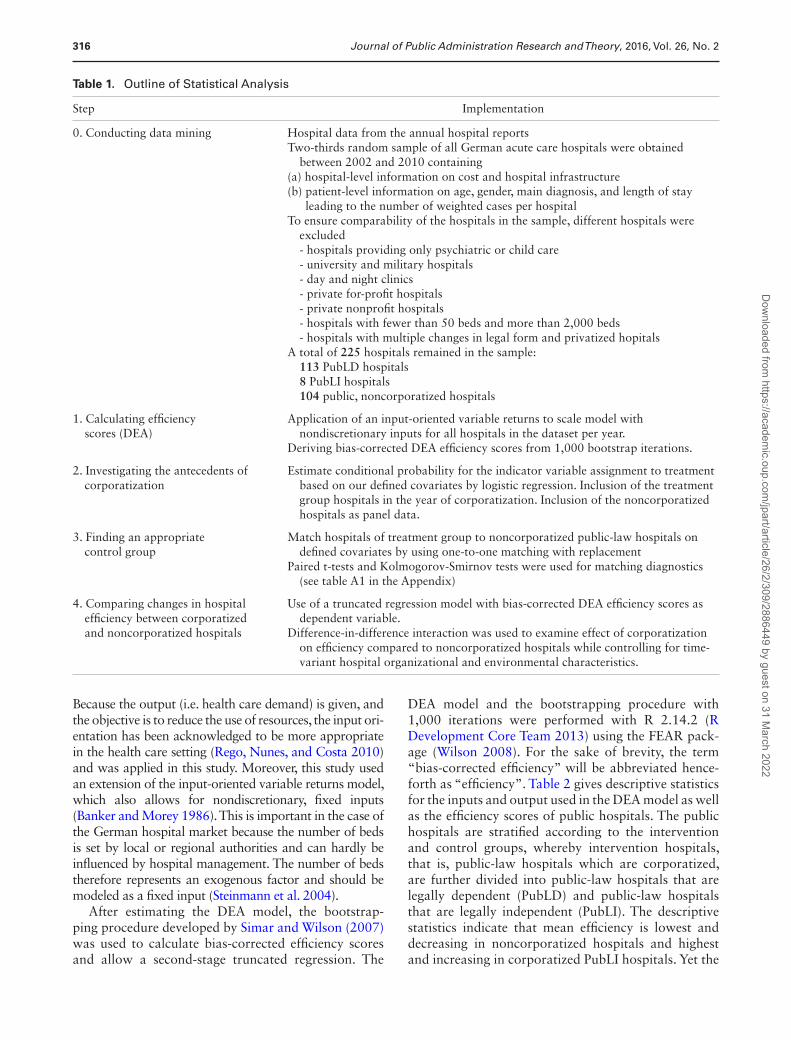
MethodologyThe methodological approach in this study has been similarly applied in other settings before (Bertrand and Zitouna 2008; Chang, Chung, and Moon 2013; Tiemann and Schreyögg 2012). It consists of four steps: (1) calcu-lating efficiency scores, (2) investigating the antecedents of corporatization, (3) finding an appropriate control group consisting of noncorporatized public-law hospi-tals, and (4) comparing changes in efficiency between corporatized and noncorporatized hospitals using a dif-ference-in-difference approach. Table 1 provides a com-prehensive outline of the statistical analysis and each of these steps is explicitly described in order below.
Hospital efficiency was the central variable of inter-est in this study. In the first step, DEA was used to calculate efficiency scores for each hospital. DEA is a nonparametric efficiency modeling approach that ana-lyzes input-to-output ratios for decision-making units, which in this case were hospitals. As the most impor-tant discretionary input (Dyson et al. 2001; Jacobs, Smith, and Street 2006; Tiemann and Schreyögg 2012), human resources were included, distinguishing between five types of personnel: physicians (Physician), nurses (Nurse), other clinical staff (Clinical), adminis-trative staff (Admin), and other nonclinical staff mem-bers (Nonclinical) as full-time equivalents. Moreover, capital input was approximated through the cost of medical supplies (Medical supplies) and other sup-plies (Other supplies). Other supplies were relevant due to the potential outsourcing of personnel after a corporatization, in which case reported labor inputs
would decrease, while the cost of other supplies would increase. As output, the number of treated patients weighted by (i.e. multiplied with) predicted resource intensity (Weighted cases) was used. Using output variables without weights can be problematic in effi-ciency analysis because hospitals with a more complex case-mix are likely to obtain lower efficiency scores (Tiemann and Schreyögg 2012). The prediction of resource intensity was based on length of stay mod-eled as a function of the main diagnoses, patient age, gender, and year dummies of treatment, and followed the approach described in Lindlbauer and Schreyögg (2014). Weights greater than one indicate an above-average predicted resource intensity, and vice versa.
DEA identifies the most efficient hospitals and sets the remaining hospitals relative to this benchmark, result-ing in efficiency scores. The most efficient hospitals are assigned an efficiency score of 1 (i.e. 100%), whereas all other hospitals have lower efficiency scores. For instance, an efficiency score of 0.8 (i.e. 80%) would indicate that the hospital would need to reduce inputs by 20% in order to be fully efficient (in an input-oriented model). An inter-temporal frontier was computed by merging the data for all years into one dataset and calculating efficiency scores for the whole set (Linna 1998). In doing so, vari-able returns to scale were assumed, as is customary in the health care sector (Banker, Charnes, and Cooper 1984; Charnes, Cooper, and Rhodes 1978; Jacobs, Smith, and Street 2006; Tiemann and Schreyögg 2012). This assump-tion, however, requires choosing either an input orienta-tion (which supposes a minimization of inputs for a given level of outputs) or an output orientation (which supposes a maximization of outputs for a given level of inputs).
Figure 2. Conceptual model.
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022
316 Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
Because the output (i.e. health care demand) is given, and the objective is to reduce the use of resources, the input ori-entation has been acknowledged to be more appropriate in the health care setting (Rego, Nunes, and Costa 2010) and was applied in this study. Moreover, this study used an extension of the input-oriented variable returns model, which also allows for nondiscretionary, fixed inputs (Banker and Morey 1986). This is important in the case of the German hospital market because the number of beds is set by local or regional authorities and can hardly be influenced by hospital management. The number of beds therefore represents an exogenous factor and should be modeled as a fixed input (Steinmann et al. 2004).
After estimating the DEA model, the bootstrap-ping procedure developed by Simar and Wilson (2007) was used to calculate bias-corrected efficiency scores and allow a second-stage truncated regression. The
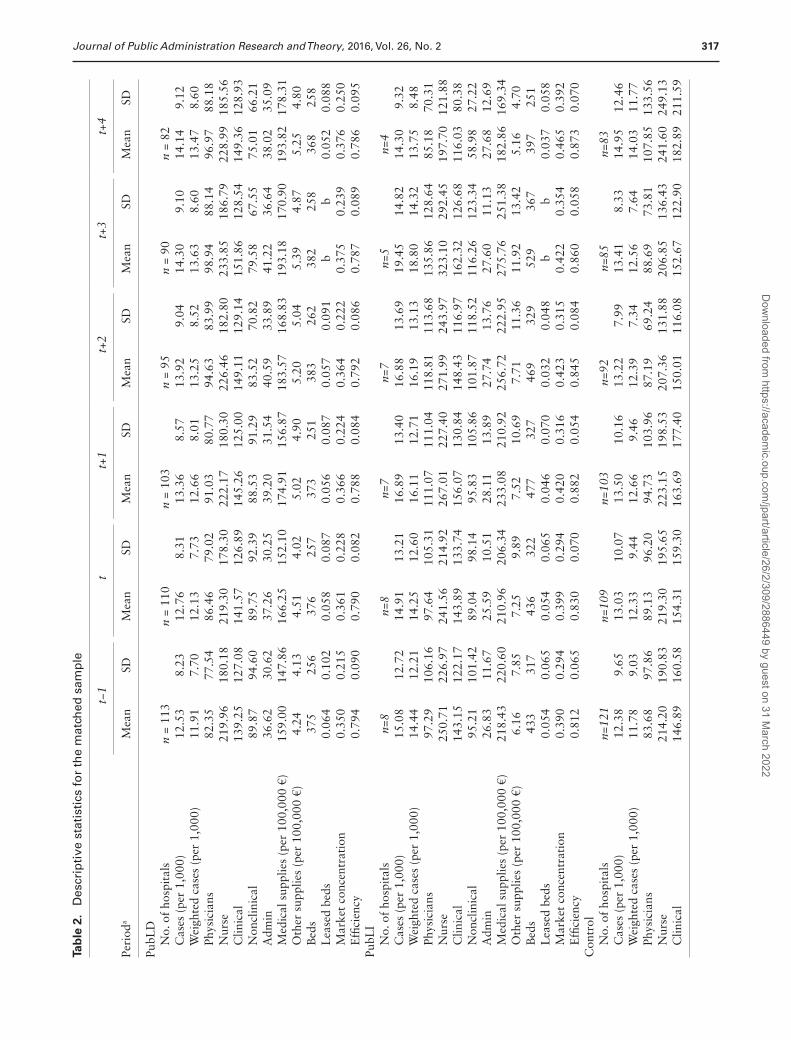
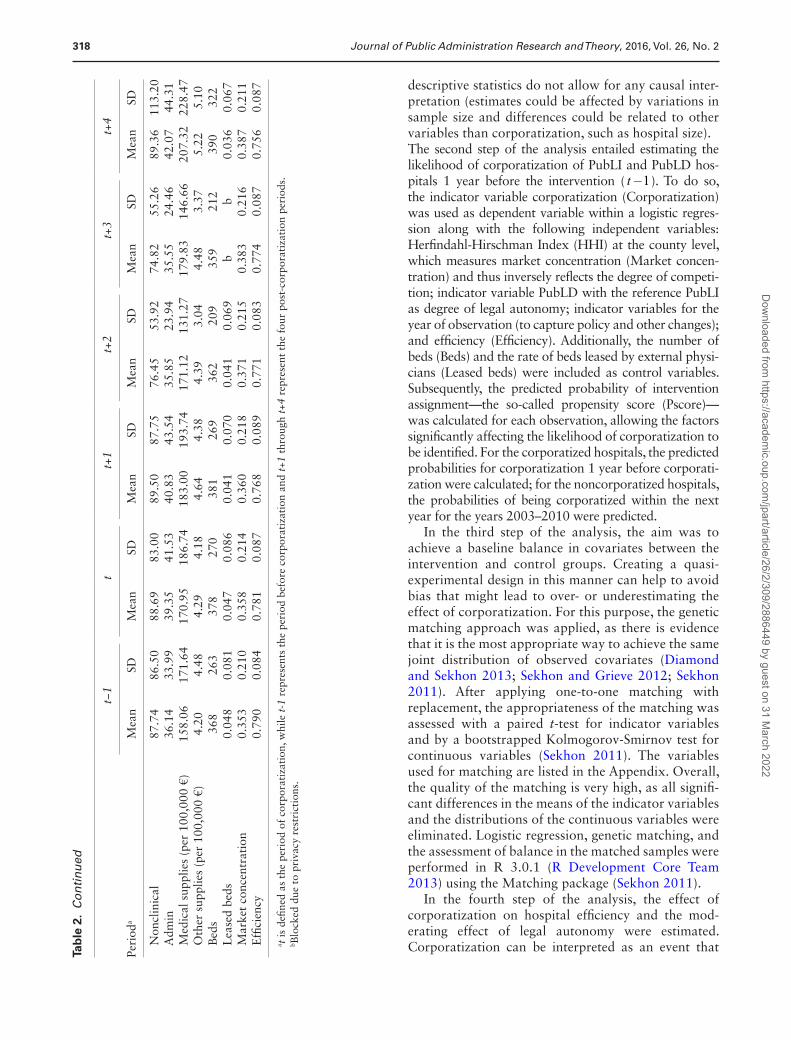
DEA model and the bootstrapping procedure with 1,000 iterations were performed with R 2.14.2 (R Development Core Team 2013) using the FEAR pack-age (Wilson 2008). For the sake of brevity, the term “bias-corrected efficiency” will be abbreviated hence-forth as “efficiency”. Table 2 gives descriptive statistics for the inputs and output used in the DEA model as well as the efficiency scores of public hospitals. The public hospitals are stratified according to the intervention and control groups, whereby intervention hospitals, that is, public-law hospitals which are corporatized, are further divided into public-law hospitals that are legally dependent (PubLD) and public-law hospitals that are legally independent (PubLI). The descriptive statistics indicate that mean efficiency is lowest and decreasing in noncorporatized hospitals and highest and increasing in corporatized PubLI hospitals. Yet the
Table 1. Outline of Statistical Analysis
Step Implementation
0. Conducting data mining Hospital data from the annual hospital reportsTwo-thirds random sample of all German acute care hospitals were obtained
between 2002 and 2010 containing(a) hospital-level information on cost and hospital infrastructure(b) patient-level information on age, gender, main diagnosis, and length of stay
leading to the number of weighted cases per hospitalTo ensure comparability of the hospitals in the sample, different hospitals were
excluded- hospitals providing only psychiatric or child care- university and military hospitals- day and night clinics- private for-profit hospitals- private nonprofit hospitals- hospitals with fewer than 50 beds and more than 2,000 beds- hospitals with multiple changes in legal form and privatized hopitals
A total of 225 hospitals remained in the sample:113 PubLD hospitals8 PubLI hospitals104 public, noncorporatized hospitals
1. Calculating efficiency scores (DEA)
Application of an input-oriented variable returns to scale model with nondiscretionary inputs for all hospitals in the dataset per year.
Deriving bias-corrected DEA efficiency scores from 1,000 bootstrap iterations.
2. Investigating the antecedents of corporatization
Estimate conditional probability for the indicator variable assignment to treatment based on our defined covariates by logistic regression. Inclusion of the treatment group hospitals in the year of corporatization. Inclusion of the noncorporatized hospitals as panel data.
3. Finding an appropriate control group
Match hospitals of treatment group to noncorporatized public-law hospitals on defined covariates by using one-to-one matching with replacement
Paired t-tests and Kolmogorov-Smirnov tests were used for matching diagnostics (see table A1 in the Appendix)
4. Comparing changes in hospital efficiency between corporatized and noncorporatized hospitals
Use of a truncated regression model with bias-corrected DEA efficiency scores as dependent variable.
Difference-in-difference interaction was used to examine effect of corporatization on efficiency compared to noncorporatized hospitals while controlling for time- variant hospital organizational and environmental characteristics.
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022
317Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
Tab
le 2
. D
escr
ipti
ve s
tati
stic
s fo
r th
e m
atch
ed s
amp
le
t−1
tt+
1t+
2t+
3t+
4
Peri
oda
Mea
nSD
Mea
nSD
Mea
nSD
Mea
nSD
Mea
nSD
Mea
nSD
PubL
D
No.
of
hosp
ital
sn
= 11
3n
= 11
0n
= 10
3n
= 95
n =
90n
= 82
C
ases
(pe
r 1,
000)
12.5
38.
2312
.76
8.31
13.3
68.
5713
.92
9.04
14.3
09.
1014
.14
9.12
W
eigh
ted
case
s (p
er 1
,000
)11
.91
7.70
12.1
37.
7312
.66
8.01
13.2
58.
5213
.63
8.60
13.4
78.
60
Phys
icia
ns82
.35
77.5
486
.46
79.0
291
.03
80.7
794
.63
83.9
998
.94
88.1
496
.97
88.1
8
Nur
se21
9.96
180.
1821
9.30
178.
3022
2.17
180.
3022
6.46
182.
8023
3.85
186.
7922
8.99
185.
56
Clin
ical
139.
2512
7.08
141.
5712
6.89
145.
2612
5.00
149.
1112
9.14
151.
8612
8.54
149.
3612
8.93
N
oncl
inic
al89
.87
94.6
089
.75
92.3
988
.53
91.2
983
.52
70.8
279
.58
67.5
575
.01
66.2
1
Adm
in36
.62
30.6
237
.26
30.2
539
.20
31.5
440
.59
33.8
941
.22
36.6
438
.02
35.0
9
Med
ical
sup
plie
s (p
er 1
00,0
00 €
)15
9.00
147.
8616
6.25
152.
1017
4.91
156.
8718
3.57
168.
8319
3.18
170.
9019
3.82
178.
31
Oth
er s
uppl
ies
(per
100
,000
€)
4.24
4.13
4.51
4.02
5.02
4.90
5.20
5.04
5.39
4.87
5.25
4.80
B
eds
375
256
376
257
373
251
383
262
382
258
368
258
L
ease
d be
ds0.
064
0.10
20.
058
0.08
70.
056
0.08
70.
057
0.09
1b
b0.
052
0.08
8
Mar
ket
conc
entr
atio
n0.
350
0.21
50.
361
0.22
80.
366
0.22
40.
364
0.22
20.
375
0.23
90.
376
0.25
0
Effi
cien
cy0.
794
0.09
00.
790
0.08
20.
788
0.08
40.
792
0.08
60.
787
0.08
90.
786
0.09
5Pu
bLI
N
o. o
f ho
spit
als
n=8
n=8
n=7
n=7
n=5
n=4
C
ases
(pe
r 1,
000)
15.0
812
.72
14.9
113
.21
16.8
913
.40
16.8
813
.69
19.4
514
.82
14.3
09.
32
Wei
ghte
d ca
ses
(per
1,0
00)
14.4
412
.21
14.2
512
.60
16.1
112
.71
16.1
913
.13
18.8
014
.32
13.7
58.
48
Phys
icia
ns97
.29
106.
1697
.64
105.
3111
1.07
111.
0411
8.81
113.
6813
5.86
128.
6485
.18
70.3
1
Nur
se25
0.71
226.
9724
1.56
214.
9226
7.01
227.
4027
1.99
243.
9732
3.10
292.
4519
7.70
121.
88
Clin
ical
143.
1512
2.17
143.
8913
3.74
156.
0713
0.84
148.
4311
6.97
162.
3212
6.68
116.
0380
.38
N
oncl
inic
al95
.21
101.
4289
.04
98.1
495
.83
105.
8610
1.87
118.
5211
6.26
123.
3458
.98
27.2
2
Adm
in26
.83
11.6
725
.59
10.5
128
.11
13.8
927
.74
13.7
627
.60
11.1
327
.68
12.6
9
Med
ical
sup
plie
s (p
er 1
00,0
00 €
)21
8.43
220.
6021
0.96
206.
3423
3.08
210.
9225
6.72
222.
9527
5.76
251.
3818
2.86
169.
34
Oth
er s
uppl
ies
(per
100
,000
€)
6.16
7.85
7.25
9.89
7.52
10.6
97.
7111
.36
11.9
213
.42
5.16
4.70
B
eds
433
317
436
322
477
327
469
329
529
367
397
251
L
ease
d be
ds0.
054
0.06
50.
054
0.06
50.
046
0.07
00.
032
0.04
8b
b0.
037
0.05
8
Mar
ket
conc
entr
atio
n0.
390
0.29
40.
399
0.29
40.
420
0.31
60.
423
0.31
50.
422
0.35
40.
465
0.39
2
Effi
cien
cy0.
812
0.06
50.
830
0.07
00.
882
0.05
40.
845
0.08
40.
860
0.05
80.
873
0.07
0C
ontr
ol
No.
of
hosp
ital
sn=
121
n=10
9n=
103
n=92
n=85
n=83
C
ases
(pe
r 1,
000)
12.3
89.
6513
.03
10.0
713
.50
10.1
613
.22
7.99
13.4
18.
3314
.95
12.4
6
Wei
ghte
d ca
ses
(per
1,0
00)
11.7
89.
0312
.33
9.44
12.6
69.
4612
.39
7.34
12.5
67.
6414
.03
11.7
7
Phys
icia
ns83
.68
97.8
689
.13
96.2
094
.73
103.
9687
.19
69.2
488
.69
73.8
110
7.85
133.
56
Nur
se21
4.20
190.
8321
9.30
195.
6522
3.15
198.
5320
7.36
131.
8820
6.85
136.
4324
1.60
249.
13
Clin
ical
146.
8916
0.58
154.
3115
9.30
163.
6917
7.40
150.
0111
6.08
152.
6712
2.90
182.
8921
1.59
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022
318 Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
descriptive statistics do not allow for any causal inter-pretation (estimates could be affected by variations in sample size and differences could be related to other variables than corporatization, such as hospital size).The second step of the analysis entailed estimating the likelihood of corporatization of PubLI and PubLD hos-pitals 1 year before the intervention ( t-1). To do so, the indicator variable corporatization (Corporatization) was used as dependent variable within a logistic regres-sion along with the following independent variables: Herfindahl-Hirschman Index (HHI) at the county level, which measures market concentration (Market concen-tration) and thus inversely reflects the degree of competi-tion; indicator variable PubLD with the reference PubLI as degree of legal autonomy; indicator variables for the year of observation (to capture policy and other changes); and efficiency (Efficiency). Additionally, the number of beds (Beds) and the rate of beds leased by external physi-cians (Leased beds) were included as control variables. Subsequently, the predicted probability of intervention assignment—the so-called propensity score (Pscore)—was calculated for each observation, allowing the factors significantly affecting the likelihood of corporatization to be identified. For the corporatized hospitals, the predicted probabilities for corporatization 1 year before corporati-zation were calculated; for the noncorporatized hospitals, the probabilities of being corporatized within the next year for the years 2003–2010 were predicted.
In the third step of the analysis, the aim was to achieve a baseline balance in covariates between the intervention and control groups. Creating a quasi-experimental design in this manner can help to avoid bias that might lead to over- or underestimating the effect of corporatization. For this purpose, the genetic matching approach was applied, as there is evidence that it is the most appropriate way to achieve the same joint distribution of observed covariates (Diamond and Sekhon 2013; Sekhon and Grieve 2012; Sekhon 2011). After applying one-to-one matching with replacement, the appropriateness of the matching was assessed with a paired t-test for indicator variables and by a bootstrapped Kolmogorov-Smirnov test for continuous variables (Sekhon 2011). The variables used for matching are listed in the Appendix. Overall, the quality of the matching is very high, as all signifi-cant differences in the means of the indicator variables and the distributions of the continuous variables were eliminated. Logistic regression, genetic matching, and the assessment of balance in the matched samples were performed in R 3.0.1 (R Development Core Team 2013) using the Matching package (Sekhon 2011).
In the fourth step of the analysis, the effect of corporatization on hospital efficiency and the mod-erating effect of legal autonomy were estimated. Corporatization can be interpreted as an event that
t−1
tt+
1t+
2t+
3t+
4
Peri
oda
Mea
nSD
Mea
nSD
Mea
nSD
Mea
nSD
Mea
nSD
Mea
nSD
N
oncl
inic
al87
.74
86.5
088
.69
83.0
089
.50
87.7
576
.45
53.9
274
.82
55.2
689
.36
113.
20
Adm
in36
.14
33.9
939
.35
41.5
340
.83
43.5
435
.85
23.9
435
.55
24.4
642
.07
44.3
1
Med
ical
sup
plie
s (p
er 1
00,0
00 €
)15
8.06
171.
6417
0.95
186.
7418
3.00
193.
7417
1.12
131.
2717
9.83
146.
6620
7.32
228.
47
Oth
er s
uppl
ies
(per
100
,000
€)
4.20
4.48
4.29
4.18
4.64
4.38
4.39
3.04
4.48
3.37
5.22
5.10
B
eds
368
263
378
270
381
269
362
209
359
212
390
322
L
ease
d be
ds0.
048
0.08
10.
047
0.08
60.
041
0.07
00.
041
0.06
9b
b0.
036
0.06
7
Mar
ket
conc
entr
atio
n0.
353
0.21
00.
358
0.21
40.
360
0.21
80.
371
0.21
50.
383
0.21
60.
387
0.21
1
Effi
cien
cy0.
790
0.08
40.
781
0.08
70.
768
0.08
90.
771
0.08
30.
774
0.08
70.
756
0.08
7
a t is
defi
ned
as t
he p
erio
d of
cor
pora
tiza
tion
, whi
le t
-1 r
epre
sent
s th
e pe
riod
bef
ore
corp
orat
izat
ion
and
t+1
thro
ugh
t+4
repr
esen
t th
e fo
ur p
ost-
corp
orat
izat
ion
peri
ods.
b Blo
cked
due
to
priv
acy
rest
rict
ions
.
Tab
le 2
. C
on
tin
ued
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022

319Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
alters the course of an organization and potentially its performance too. In order to analyze its effects, an approach that accounts for the periods before and after the event is recommended (Bilodeau, Laurin, and Vining 2007). In the present study, a difference-in-dif-ference approach was used, which allows identifying changes in efficiency of corporatized public hospitals relative to changes in efficiency of noncorporatized hos-pitals. Thus, it allows a before and after analysis of the intervention compared to the control group. To avoid the problem of serial correlation (Bertrand, Duflo, and Mullainathan 2004), five individual regression mod-els were applied to compare the pre-corporatization period, t-1 , with one of the five post-corporatization periods. Using t-1 as comparison period should rule out the underestimation of the corporatization effect due to any anticipatory effects. For each regression, a sample was drawn with observations from the pre-corporatization period and from the period of inter-est. A truncated regression was modeled to take into account that efficiency is truncated at 1, that is, cannot take larger values than 1. Each of the five regression models was estimated twice, that is, with and without the three-way interaction term “ β4Corp Post PubLDi T ” in order to assess hypotheses H5 and H6, as follows:
Efficiency Corp Post
Corp Post ZiT i T
i T iT
= + +
+ + +
β β ββ β0 1 2
3 5 uui iT+ε
where EfficiencyiT is the efficiency of the ith hos-pital at period T T T= 1 2, , with T t1 1= − as the pre-corporatization period used for matching and T t t t t t2 , 1, 2, 3, 4}∈{ + + + + depending on which comparison period, Post , was analyzed; Post is an indicator variable with value 0 in period T1 and with value 1 in period T2 ; Corp is an indicator variable with value 1 for hospitals in the intervention group and with value 0 for hospitals in the control group to control for time-invariant differences between intervention and control group; PubLD is an indicator variable (value 1) with reference PubLI (value 0) to indicate degree of legal autonomy; and ZiT are observable factors affect-ing the efficiency of hospital i at period T (i.e., the same time-variant hospital and environmental charac-teristics used for genetic matching except the Pscore). Finally, ui is the hospital’s fixed effect, and εiT is the random error. The effect of corporatization, coefficient β3 , identifies changes in efficiency relative to changes in efficiency in the control group, and coefficient β4 is the moderating effect of legal autonomy status. The difference-in-difference methodology assumes that all other temporal factors affecting hospital efficiency had the same impact on hospitals in the intervention group as they did on hospitals in the control group. Table 2 contains descriptive statistics for the Z-characteristics of the hospitals.
DataThe present study is based on data from the hospital reports submitted annually to the Research Data Centre of the Federal Statistical Office of Germany (Federal Statistical Office of Germany [Destatis] 2012b). This extensive dataset covers all hospitals in Germany and contains hospital-level information on cost and hospi-tal infrastructure, as well as patient-level information on age, gender, main diagnosis, and length of stay. In this study, a two-thirds1 random sample of data from the years 2002 through 2010 was used, filtering public acute care hospitals with and without changes in legal form. Acute care hospitals did not include university hospitals, military hospitals, day and night clinics, or hospitals with fewer than 50 or more than 2,000 beds. Hospitals with multiple changes in legal form and pri-vatized hospitals were also excluded from the study, as were hospitals without a pre-corporatization or at least one post-corporatization period. This resulted in a sample of 121 corporatized hospitals (113 PubLD and 8 PubLI hospitals) and 104 noncorporatized hospitals.
Results
Table 3 presents the results of the logistic regression on the binary variable corporatization. These indicate that the likelihood of hospital corporatization increased sig-nificantly as competition increased. This result is consist-ent with hypothesis 1. Regarding regulatory change and its effect on competitive pressures, the results indicate that the likelihood of corporatization was significantly higher in the years 2003 through 2005 than in 2002,
Table 3. Logistic Regression Estimates on Binary Variable Corporatization
Corporatization
Intercept −5.350*** (1.137)Beds (per 1,000) 1.062*** (0. 393)Leased beds −0.059 (0.761)Market concentration −1.116** (0.487)PubLI (Reference)PubLD 1.928*** (0.398)Efficiency 1.515 (1.197)Year 2002 (Reference)Year 2003 1.605*** (0.429)Year 2004 1.661*** (0.430)Year 2005 1.279*** (0.451)Year 2006 0.417 (0.535)Year 2007 0.222 (0.574)Year 2008 0.096 (0.577)
Note: **p < .05; ***p < .01; SE in parentheses.
1 The dataset provided in the research data center is limited by the Federal Statistical Office to two-thirds of the whole population due to privacy restrictions.
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022

320 Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
with the highest probability being in 2004. The estimates for the years 2006 through 2008 were not significant. These results support hypothesis 2. The estimate for the variable PubLD had a significantly positive value, indi-cating that politically dependent hospitals were more likely to be corporatized. This result is consistent with hypothesis 3. Lower baseline efficiency, however, did not significantly affect the likelihood of a hospital being corporatized. Hypothesis 4 is not supported.
Table 4 presents the results of the first set of differ-ence-in-difference regressions on efficiency, which did not differentiate between previously PubLD and PubLI hospitals. In each regression, the estimate of the inter-action term was positive and almost always significant. This supports hypothesis 5 that hospital corporatiza-tion has a positive effect on efficiency.
Table 5 provides the results of the second set of dif-ference-in-difference regressions on efficiency, which additionally considered the three-way interaction term Corp*Post*PubLD, thus allowing the corpora-tization effect to be differentiated between previously PubLD and PubLI hospitals. The estimates of the two-way interaction term, which represent the effects for previously PubLI hospitals, were positive and almost significant in each regression. The three-way interac-tion terms were significant and negative. This implies that the corporatization-based efficiency changes for previously PubLD hospitals were lower than the cor-poratization-based efficiency changes for previously PubLI hospitals. In short, the legal autonomy status
of a public-law hospital moderated the effect of hos-pital corporatization on efficiency changes, but not in the postulated direction. Hence, hypothesis 6 is not supported.
Additional to our hypothesis testing, results of all coefficients are reported in the Appendix (table A2 and figure A3). Table A2 shows the truncated regres-sion results for the difference-in-difference model (H6 specification) on efficiency comparing t and t+4 (coef-ficients and significance levels are similar for all other post-corporatization comparison periods). Figure A3 displays the estimated changes in efficiency over time in corporatized and noncorporatized hospitals. Efficiency is decreasing over time in noncorporatized hospitals (β2), but increasing in corporatized hospitals (β2 + β3 (+β4 for PubLD hospitals)). Additionally, some control variables have a significant effect. For instance, larger hospitals (measured in number of beds) are signifi-cantly more efficient than smaller hospitals.
One limitation of DEA is its sensitivity to model spec-ifications. In order to validate the results, two variants of the DEA model were used as sensitivity analyses. First, fixed beds were excluded as an input because includ-ing them makes a strong assumption about the under-lying production process. Second, a contemporaneous frontier was computed instead of an intertemporal one. A contemporaneous frontier involves computing the DEA efficiency score by taking each cross-section from 2002 through 2010 separately into the model (Linna 1998). After re-estimating the DEA, the same steps as
Table 4. Truncated Regression Results for Difference-in-Differences Models (H5 Specification) on Efficiency
Period Compared to t-1 Corp*Post Corp*Post*PubLD
N N β3 estimate (SE) β4 estimate (SE)
t 227 454 0.006 (0.005) — —t+1 213 426 0.021*** (0.006) — —t+2 194 388 0.020*** (0.007) — —t+3 180 360 0.013 (0.008) — —t+4 169 338 0.035*** (0.009) — —
Note: n = number of hospitals; N = number of observations.*p < .1; **p < .05; ***p < .01.
Table 5. Truncated Regression Results for Difference-in-Differences Models (H6 Specification) on Efficiency
Period Compared to t-1 Corp*Post Corp*Post*PubLD
n N β3 estimate (SE) β4 estimate (SE)
t 227 454 0.021* (0.012) −0.016 (0.012)t+1 213 426 0.072*** (0.018) −0.055*** (0.018)t+2 194 388 0.045** (0.018) −0.026 (0.018)t+3 180 360 0.056** (0.023) −0.046** (0.023)t+4 169 338 0.109*** (0.030) −0.077*** (0.030)
Note: n = number of hospitals; N = number of observations.
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022

321Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
before were performed using new efficiency scores. The direction of coefficients did not change in any of the sen-sitivity analyses, indicating that the results of the origi-nal regression models were robust.
Discussion and Implications
This study deals with the antecedents and consequences of hospital corporatization, focusing particularly on changes in hospital efficiency. The results of a logistic regression indicate that public-law hospitals were sig-nificantly more likely to be corporatized under certain circumstances, namely: in areas with a higher degree of competition, during the years around a major change in the reimbursement system (2003–2005), and if they were legally dependent entities. Having lower base-line efficiency, however, did not significantly affect the likelihood of corporatization. This last result is in line with the findings of Aivazian, Ge, and Qiu (2005), who detected that baseline performance did not affect the likelihood of corporatization. One possible explana-tion is that hospitals are unaware of their relative effi-ciency as calculated by DEA. Instead, they might base strategic decisions on their self-assessed or perceived efficiency, which can differ substantially from DEA scores. In sum, three of the four antecedents examined in this study appear to have had the postulated effects.
The results of the difference-in-difference regres-sions indicate that corporatization has a positive effect on efficiency. This study thus supports the findings of prior empirical analyses of the consequences of cor-poratization in the hospital context (Aidemark and Lindkvist 2004; Ferreira and Marques 2014; Rego, Nunes, and Costa 2010) as well as in other settings (Aivazian, Ge, and Qiu 2005; Cambini et al. 2011; Nelson and Nikolakis 2012). The impact of corpora-tization is stable over time, with a slight tendency to increases in magnitude in the 4 years following corpo-ratization, as can be seen by the mostly increasing DiD coefficients. This is in line with the findings of Aivazian, Ge, and Qiu (2005), who also found increasing effects, and stands in contrast to Vining, Laurin, and Weimer (2014), who detected that the effect decreased over time. Yet our results should be interpreted cautiously, because sample size varies depending on the time frame regarded and might affect the magnitude of the coefficients. Additionally, comparability with the two previous studies is limited, because we assess the net impact of corporatization (excluding time effects found in noncorporatized hospitals), while the other two studies do not empirically distinguish time effects. Furthermore, our results also indicate that the legal autonomy status of a hospital before corporatization is important, but that it affects the estimates differ-ently than expected: the positive effect for previously
PubLD hospitals was smaller than that for previously PubLI hospitals, rather than vice versa. Although this finding is counterintuitive at first glance, it is conceiv-able that PubLI hospitals are better prepared for an increase in managerial autonomy and to accept more business-like circumstances, as the changes imposed on their management are less extensive. PubLD hos-pitals, in turn, might experience paradigmatic changes in their managerial autonomy and principal-agent relationships. Indeed, in some cases, their manage-ment might be less able to respond effectively to the new requirements or might lack the necessary skills to use their increased managerial autonomy to generate gains in efficiency. Moreover, employees’ perceptions of their organization’s readiness for change might differ (Cinite, Duxbury, and Higgins 2009) between PubLD and PubLI hospitals, leading to differences in acceptance-resistance behavior. The “Resources as Facilitators” view (Kraatz and Zajac 2001) supports the above explanation by stating that resources, such as management’s experience and competence for deal-ing with change, serve as a positive moderator on the link between strategic change and performance. This view has already been espoused in previous research on improvements in public service provision (Boyne 2003). However, even though corporatization might lead to smaller efficiency gains for PubLD hospitals, the results of this study indicate that corporatiza-tion is still advantageous for both PubLD and PubLI hospitals. Thus, in line with the conclusion of other researchers (Aivazian, Ge, and Qiu 2005; Cambini et al. 2011), corporatization is likely an effective alternative to privatization. In comparison with the results of Tiemann and Schreyögg (2012), this study shows that corporatization enables hospitals to real-ize similar net efficiency gains as privatization does. Yet, caution is required in comparing the results of the two studies. Even though drawing on almost the same dataset, the samples of Tiemann and Schreyögg (2012) and this study diverge, because our sample includes hospitals in public ownership only (in particular, 121 corporatized and 104 noncorporatized public-law hospitals from 2002 to 2010), while the sample of Tiemann and Schreyögg (2012) comprises hospitals of all ownership forms (in particular, 132 privatized and 361 nonprivatized public hospitals from 1997 to 2007). Therefore, net changes in efficiency are not directly comparable, because the samples used for efficiency estimation differ. However, the two studies depict that net efficiency gains can be realized by both privatization and corporatization.
Another important aspect is the comparability and generalizability of our findings to other industries. While single industry studies can provide greater valid-ity by controlling for industry conditions, and similar
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022

322 Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
findings can be expected in hospitals embedded within similar health systems, it remains to be discussed whether our results can be extended more widely to other settings. Even though the outputs used in the efficiency estimation are clearly hospital specific, one could argue that the inputs, in particular in terms of human resources, are crucial in all other settings of public service provision, too. Prior studies predomi-nantly show that inputs or single input-output ratios decrease (e.g. Aivazian, Ge, and Qiu 2005; Cambini et al. 2011; Nelson and Nikolakis 2012; Vining, Laurin, and Weimer 2014), whereas our study addi-tionally depicts that this decrease is not accompanied by an equal reduction of outputs or an increase of com-plementary inputs. It seems probable that this finding also holds for other settings. However, the study of Pérez-Lopez, Príor, and Zafra-Gómez (2015) finds that the relation between agencification and efficiency dif-fers across services, which might indicate that causal effects of agencification might also be to some extent service specific. Furthermore, our study empirically showed that efficiency improvements can be attributed to corporatization and do not merely represent a time effect. On a more descriptive basis, Vining, Laurin, and Weimer (2014) provided evidence for the disentangle-ment of time and corporatization effects for agencies as well. Thus, our results support the prior evidence from the hospital industry and other research settings, which might at least indicate to some degree that cor-poratization works similarly in the hospital setting as in other areas. Empirical support for this conclusion, however, is pending.
This study has some important limitations. First, it is reasonable to assume that there are factors affecting the decision to corporatize other than those examined here. Examples include the political composition of local government or the financial situation of munici-palities. Data on these potentially relevant predictors of corporatization were, however, not readily available. Second, corporatization was defined in this study as a change from a public legal form to a private legal form. This kind of change can be accompanied by other stra-tegic decisions, such as those to build alliances or to sell a certain degree of hospital shares to private inves-tors. Partial privatizations like these, however, could not be detected in the data as long as the public owner kept the majority of shares. Further studies are there-fore needed to disentangle the effects of corporatiza-tion from the effects of other strategic changes. Third, although the study differentiated between hospitals that were legally dependent and those that were not when looking at the effects of subsequent corporati-zation on efficiency, the sample of legally independent hospitals was much smaller than the sample of legally dependent ones. Despite a small sample of legally
independent hospitals, however, the regression results were significant for the three-way interaction effect. Fourth, public hospitals with a private legal form can more easily outsource certain functions, leading to reductions in personnel. In this study, outsourced services were approximated by including the cost of supplies as an output, which can be regarded only as a rough control. The extent and impact of outsourc-ing after corporatization are open questions for future research. Finally, our study did not measure changes in quality of care. It may be possible efficiency gains are realized at the expense of quality of care, for instance if the number of nurses is reduced, which we cannot control for. Future studies could compare hospitals in terms of some of the commonly used quality measures such as fraction of patients with hospital acquired infections or readmitted, which were not available in our data.
Despite its limitations, the study also makes some valuable contributions. To start with, it adds to existing insights on the antecedents and effects of corporatiza-tion by drawing on a large and rich dataset, including data from approximately 500 public hospitals over a 9-year period and a broad range of inputs and outputs, as well as environmental and organizational character-istics. Moreover, the research setting, namely the hos-pital industry, is amenable to quantitative longitudinal analysis of spatial and temporal competition effects. The methodological approach is comprehensive and builds on recent developments in relevant methodol-ogy. Finally, the sensitivity analyses underscore the validity and robustness of the findings. Together, these represent an improvement over previous corporatiza-tion studies and an extension of the evidence base on hospital corporatization in particular.
As a result, the study provides some valuable insights for practice and future research. To start with, the number of PubLD hospitals has decreased continually and significantly over the past 10 years, and PubLD hospitals are more likely to be corporatized. As it may sometimes be preferable for a hospital to remain gov-erned under public law (e.g. to maintain more politi-cal control or to remain bound to employee tariffs or public procurement law), decision makers should consider opting for PubLI status instead of PubLD status, as the former would seem more appropriate to react to market pressures and engage in competition with other providers. However, if decision makers are under great pressure to improve efficiency, this study provides evidence that corporatization is likely an effective means to do so. Corporatization may there-fore also be an effective alternative to privatization, which entails a drastic loss of control for the public owner. This is a crucial argument for decision-makers who need to decide between the two approaches. The
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022

323Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
study also provides some evidence that there is a need to prepare for corporatization, especially in PubLD hospitals, where the degree of change in managerial and structural patterns might be too great to realize the full potential for efficiency gains. In terms of public policy, the results of this study emphasize that policy interventions that affect a hospital’s environment (such as changes to the reimbursement system) have con-sequences for structures in health care provision. As ownership diversity is protected by law in the German Social Code Book, the effect of policy interventions on health care provision structures must be carefully observed. Finally, the study’s results throw up the ques-tion as to how far perceptions of efficiency, which serve as the foundation for strategic management decisions, differ from efficiency assessments such as DEA. As the latter are supposedly more valid assessments of a hos-pital’s relative performance, it might be worthwhile to consider ways to improve transparency on this subject.
Regarding future research, this study suggests the need to consider factors that might moderate the cor-poratization-efficiency link. One fruitful avenue might be to investigate further the processes underlying the moderating effect of a hospital’s legal autonomy sta-tus. More generally, future research could also build on the insights of this study and attempt to identify other moderating variables of an environmental or organizational nature. Doing so could improve our understanding of the consequences of corporatization and provide sound evidence for making such decisions about organizational reform. Additionally, a simultane-ous study of corporatization and privatization effects seems interesting in order to directly compare both
NPM means. Doing this on a quantitative basis with the German hospital dataset seems difficult, because the sample would become too small to estimate sequential or interaction effects. These effects, however, are cru-cial for the validity of findings, because, for instance, it is mostly private-law hospitals which are privatized (while corporatized hospitals are per definition public-law hospitals before corporatization), and it would be necessary to disentangle the effects of legal form change and ownership change. Hence, larger datasets (or popu-lations) are needed, or comparative studies could first of all apply a more qualitative, in-depth approach to this question. A similar caveat of our data concerns the topic of partial privatization and mixed ownership forms. Our data provide information about the majority ownership only; yet it might be possible that a change in legal form is accompanied by a change from pure pub-lic ownership to a mixed public-private ownership with a public majority. The benefits from partial privatiza-tion have not always been confirmed by the empirical evidence, and mixed ownership forms have even been found to be negatively associated with efficiency (Oum, Yan, and Yu, 2008). Finally, this study draws on hospi-tals as research subjects. Due to the great economic and social relevance of the health care sector, analyzing the impact of corporatization in this context is clearly of high value. However, because the results depend in part on the underlying production process, it would also be useful to replicate this study in other research settings, such as in the water or energy sectors. Doing so would help in gaining a deeper understanding about how best to organize production and make empirically based sug-gestions about the state’s role in service provision.
Appendix
Table A1. Covariates Balance Before and After Genetic Matching
Hospitals Without Corporatization
Hospitals With Corporatization
t Test p Value
Kolmogorov-Smirnov Test p Value
No. of hospitals Before genetic matching 590 121 — — After genetic matching 121 121 — —Mean beds Before genetic matching 314 379 .013 < .001 After genetic matching 368 379 .103 .983Mean baseline efficiency Before genetic matching 0.800 0.795 .597 .641 After genetic matching 0.790 0.795 .034 .753Mean market concentration Before genetic matching 0.424 0.352 .002 .035 After genetic matching 0.353 0.352 .943 .221
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022
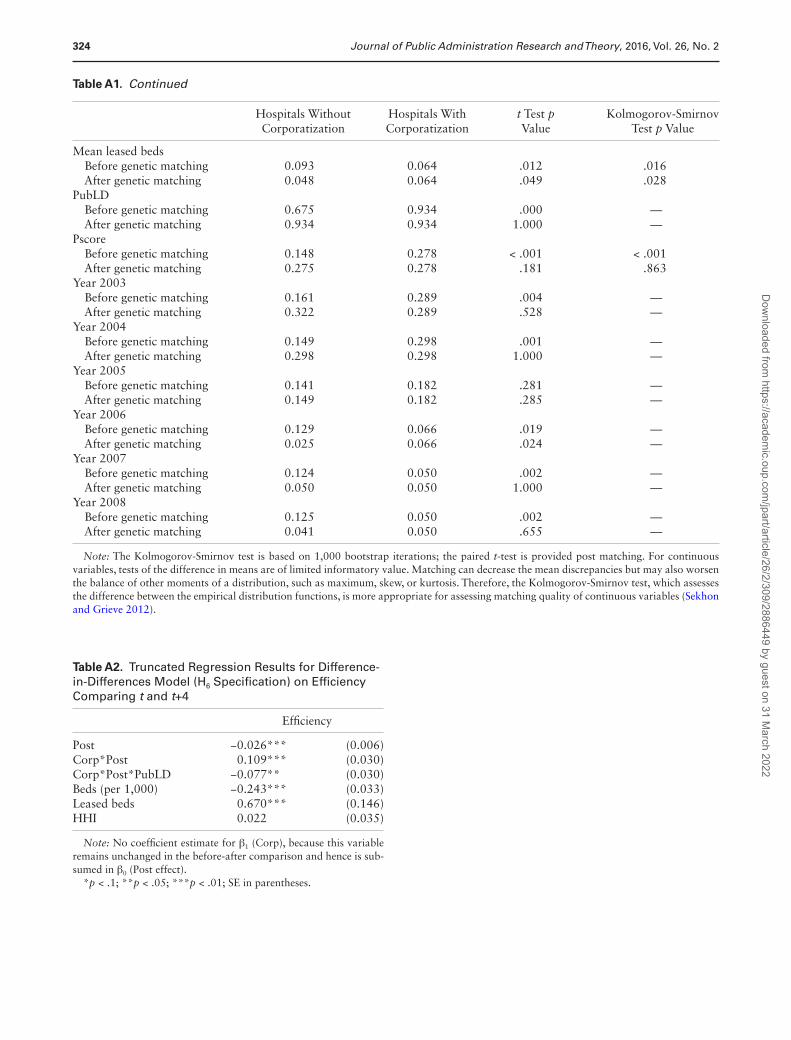
324 Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
Table A2. Truncated Regression Results for Difference-in-Differences Model (H6 Specification) on Efficiency Comparing t and t+4
Efficiency
Post −0.026*** (0.006)Corp*Post 0.109*** (0.030)Corp*Post*PubLD −0.077** (0.030)Beds (per 1,000) −0.243*** (0.033)Leased beds 0.670*** (0.146)HHI 0.022 (0.035)
Note: No coefficient estimate for β1 (Corp), because this variable remains unchanged in the before-after comparison and hence is sub-sumed in β0 (Post effect).
*p < .1; **p < .05; ***p < .01; SE in parentheses.
Hospitals Without Corporatization
Hospitals With Corporatization
t Test p Value
Kolmogorov-Smirnov Test p Value
Mean leased beds Before genetic matching 0.093 0.064 .012 .016 After genetic matching 0.048 0.064 .049 .028PubLD Before genetic matching 0.675 0.934 .000 — After genetic matching 0.934 0.934 1.000 —Pscore Before genetic matching 0.148 0.278 < .001 < .001 After genetic matching 0.275 0.278 .181 .863Year 2003 Before genetic matching 0.161 0.289 .004 — After genetic matching 0.322 0.289 .528 —Year 2004 Before genetic matching 0.149 0.298 .001 — After genetic matching 0.298 0.298 1.000 —Year 2005 Before genetic matching 0.141 0.182 .281 — After genetic matching 0.149 0.182 .285 —Year 2006 Before genetic matching 0.129 0.066 .019 — After genetic matching 0.025 0.066 .024 —Year 2007 Before genetic matching 0.124 0.050 .002 — After genetic matching 0.050 0.050 1.000 —Year 2008 Before genetic matching 0.125 0.050 .002 — After genetic matching 0.041 0.050 .655 —
Note: The Kolmogorov-Smirnov test is based on 1,000 bootstrap iterations; the paired t-test is provided post matching. For continuous variables, tests of the difference in means are of limited informatory value. Matching can decrease the mean discrepancies but may also worsen the balance of other moments of a distribution, such as maximum, skew, or kurtosis. Therefore, the Kolmogorov-Smirnov test, which assesses the difference between the empirical distribution functions, is more appropriate for assessing matching quality of continuous variables (Sekhon and Grieve 2012).
Table A1. Continued
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022
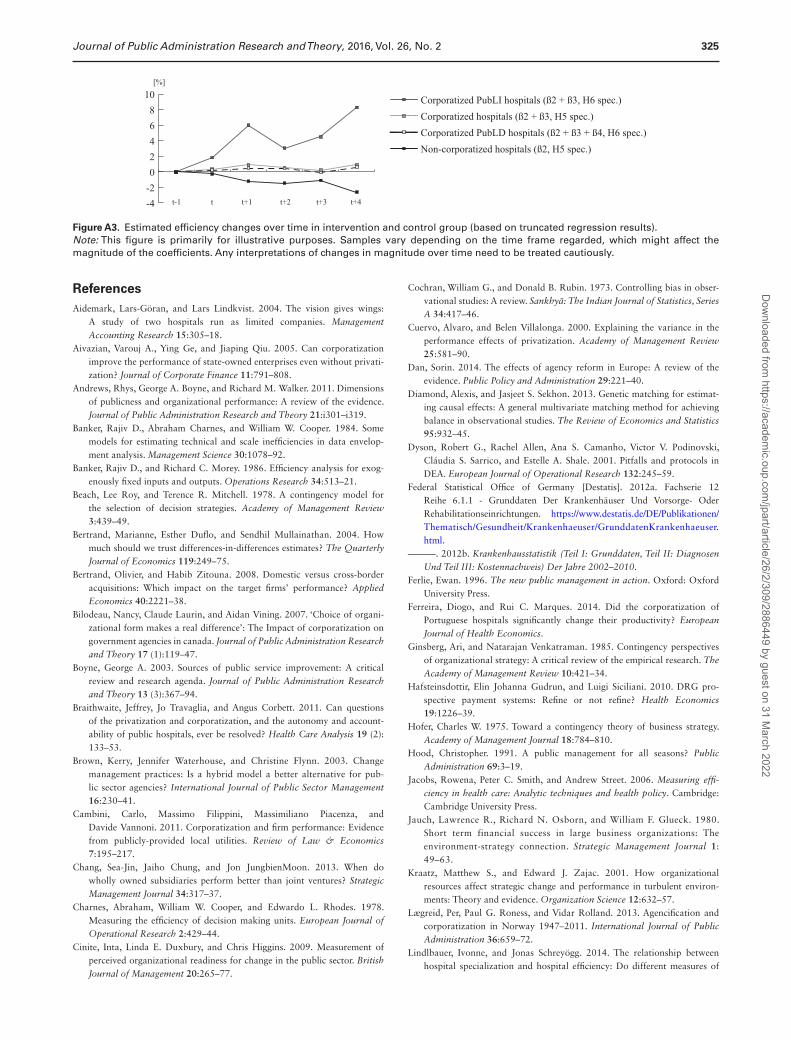
325Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
ReferencesAidemark, Lars-Göran, and Lars Lindkvist. 2004. The vision gives wings:
A study of two hospitals run as limited companies. Management Accounting Research 15:305–18.
Aivazian, Varouj A., Ying Ge, and Jiaping Qiu. 2005. Can corporatization improve the performance of state-owned enterprises even without privati-zation? Journal of Corporate Finance 11:791–808.
Andrews, Rhys, George A. Boyne, and Richard M. Walker. 2011. Dimensions of publicness and organizational performance: A review of the evidence. Journal of Public Administration Research and Theory 21:i301–i319.
Banker, Rajiv D., Abraham Charnes, and William W. Cooper. 1984. Some models for estimating technical and scale inefficiencies in data envelop-ment analysis. Management Science 30:1078–92.
Banker, Rajiv D., and Richard C. Morey. 1986. Efficiency analysis for exog-enously fixed inputs and outputs. Operations Research 34:513–21.
Beach, Lee Roy, and Terence R. Mitchell. 1978. A contingency model for the selection of decision strategies. Academy of Management Review 3:439–49.
Bertrand, Marianne, Esther Duflo, and Sendhil Mullainathan. 2004. How much should we trust differences-in-differences estimates? The Quarterly Journal of Economics 119:249–75.
Bertrand, Olivier, and Habib Zitouna. 2008. Domestic versus cross-border acquisitions: Which impact on the target firms’ performance? Applied Economics 40:2221–38.
Bilodeau, Nancy, Claude Laurin, and Aidan Vining. 2007. ‘Choice of organi-zational form makes a real difference’: The Impact of corporatization on government agencies in canada. Journal of Public Administration Research and Theory 17 (1):119–47.
Boyne, George A. 2003. Sources of public service improvement: A critical review and research agenda. Journal of Public Administration Research and Theory 13 (3):367–94.
Braithwaite, Jeffrey, Jo Travaglia, and Angus Corbett. 2011. Can questions of the privatization and corporatization, and the autonomy and account-ability of public hospitals, ever be resolved? Health Care Analysis 19 (2): 133–53.
Brown, Kerry, Jennifer Waterhouse, and Christine Flynn. 2003. Change management practices: Is a hybrid model a better alternative for pub-lic sector agencies? International Journal of Public Sector Management 16:230–41.
Cambini, Carlo, Massimo Filippini, Massimiliano Piacenza, and Davide Vannoni. 2011. Corporatization and firm performance: Evidence from publicly-provided local utilities. Review of Law & Economics 7:195–217.
Chang, Sea-Jin, Jaiho Chung, and Jon JungbienMoon. 2013. When do wholly owned subsidiaries perform better than joint ventures? Strategic Management Journal 34:317–37.
Charnes, Abraham, William W. Cooper, and Edwardo L. Rhodes. 1978. Measuring the efficiency of decision making units. European Journal of Operational Research 2:429–44.
Cinite, Inta, Linda E. Duxbury, and Chris Higgins. 2009. Measurement of perceived organizational readiness for change in the public sector. British Journal of Management 20:265–77.
Cochran, William G., and Donald B. Rubin. 1973. Controlling bias in obser-vational studies: A review. Sankhyā: The Indian Journal of Statistics, Series A 34:417–46.
Cuervo, Alvaro, and Belen Villalonga. 2000. Explaining the variance in the performance effects of privatization. Academy of Management Review 25:581–90.
Dan, Sorin. 2014. The effects of agency reform in Europe: A review of the evidence. Public Policy and Administration 29:221–40.
Diamond, Alexis, and Jasjeet S. Sekhon. 2013. Genetic matching for estimat-ing causal effects: A general multivariate matching method for achieving balance in observational studies. The Review of Economics and Statistics 95:932–45.
Dyson, Robert G., Rachel Allen, Ana S. Camanho, Victor V. Podinovski, Cláudia S. Sarrico, and Estelle A. Shale. 2001. Pitfalls and protocols in DEA. European Journal of Operational Research 132:245–59.
Federal Statistical Office of Germany [Destatis]. 2012a. Fachserie 12 Reihe 6.1.1 - Grunddaten Der Krankenhäuser Und Vorsorge- Oder Rehabilitationseinrichtungen. https://www.destatis.de/DE/Publikationen/Thematisch/Gesundheit/Krankenhaeuser/GrunddatenKrankenhaeuser.html.
———. 2012b. Krankenhausstatistik (Teil I: Grunddaten, Teil II: Diagnosen Und Teil III: Kostennachweis) Der Jahre 2002–2010.
Ferlie, Ewan. 1996. The new public management in action. Oxford: Oxford University Press.
Ferreira, Diogo, and Rui C. Marques. 2014. Did the corporatization of Portuguese hospitals significantly change their productivity? European Journal of Health Economics.
Ginsberg, Ari, and Natarajan Venkatraman. 1985. Contingency perspectives of organizational strategy: A critical review of the empirical research. The Academy of Management Review 10:421–34.
Hafsteinsdottir, Elin Johanna Gudrun, and Luigi Siciliani. 2010. DRG pro-spective payment systems: Refine or not refine? Health Economics 19:1226–39.
Hofer, Charles W. 1975. Toward a contingency theory of business strategy. Academy of Management Journal 18:784–810.
Hood, Christopher. 1991. A public management for all seasons? Public Administration 69:3–19.
Jacobs, Rowena, Peter C. Smith, and Andrew Street. 2006. Measuring effi-ciency in health care: Analytic techniques and health policy. Cambridge: Cambridge University Press.
Jauch, Lawrence R., Richard N. Osborn, and William F. Glueck. 1980. Short term financial success in large business organizations: The environment-strategy connection. Strategic Management Journal 1: 49–63.
Kraatz, Matthew S., and Edward J. Zajac. 2001. How organizational resources affect strategic change and performance in turbulent environ-ments: Theory and evidence. Organization Science 12:632–57.
Lægreid, Per, Paul G. Roness, and Vidar Rolland. 2013. Agencification and corporatization in Norway 1947–2011. International Journal of Public Administration 36:659–72.
Lindlbauer, Ivonne, and Jonas Schreyögg. 2014. The relationship between hospital specialization and hospital efficiency: Do different measures of
Figure A3. Estimated efficiency changes over time in intervention and control group (based on truncated regression results). Note: This figure is primarily for illustrative purposes. Samples vary depending on the time frame regarded, which might affect the magnitude of the coefficients. Any interpretations of changes in magnitude over time need to be treated cautiously.
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022

326 Journal of Public Administration Research and Theory, 2016, Vol. 26, No. 2
specialization lead to different results? Health Care Management Science 17:365–78.
Linna, Miika. 1998. Measuring hospital cost efficiency with panel data mod-els. Health Economics 7:415–27.
Nelson, Harry W., and William Nikolakis. 2012. How does corporatization improve the performance of government agencies? Lessons from the restructuring of state-owned forest agencies in Australia. International Public Management Journal 15:364–91.
Oum, Tae H., Jia Yan, and Chunyan Yu. 2008. Ownership forms matter for airport efficiency: A stochastic frontier investigation of worldwide air-ports. Journal of Urban Economics 64:422–35.
Pérez-López, Gemma, Diego Prior, and José L. Zafra-Gómez. 2015. Rethinking new public management delivery forms and efficiency: Long-term effects in Spanish local government. Journal of Public Administration Research and Theory 1–27. Online first.
Pollitt, Christopher, and Sorin Dan. 2011. The impact of the new pub-lic management in Europe: A meta-analysis.” COCOPS, European Commission. http://www.cocops.eu/wp-content/uploads/2012/03/WP1_Deliverable1_Meta-analysis_Final.pdf (accessed February 20, 2015).
R Development Core Team. 2013. R: A language and environment for sta-tistical computing (version 3.0.0). Vienna, Austria: R Foundation for Statistical Computing. www.r-project.org.
Rego, Guilhermina, Rui Nunes, and José Costa. 2010. The challenge of corpo-ratisation: The experience of Portuguese public hospitals. The European Journal of Health Economics 11:367–81.
Scott, William R., and Gerald F. Davis. 2007. Organizations and organizing: Rational, natural and open systems perspectives. Upper Saddle River, NJ: Pearson Prentice Hall.
Sekhon, Jasjeet S. 2011. Multivariate and propensity score matching soft-ware with automated balance optimization: The matching package for R. Journal of Statistical Software 42:1–52.
Sekhon, Jasjeet S., and Richard D. Grieve. 2012. A matching method for improving covariate balance in cost-effectiveness analyses. Health Economics 21:695–714.
Shleifer, Andrei. 1985. A theory of yardstick competition. The RAND Journal of Economics 16:319–27.
Simar, Léopold, and Paul W. Wilson. 2007. Estimation and inference in two-stage, semi-parametric models of production processes. Journal of Econometrics 136:31–64.
Steinmann, Lukas, Gunnar Dittrich, Alexander Karmann, and Peter Zweifel. 2004. Measuring and comparing the (in)efficiency of German and Swiss hospitals. The European Journal of Health Economics 5:216–26.
Tiemann, Oliver, and Jonas Schreyögg. 2012. Changes in hospital efficiency after privatization. Health Care Management Science 15:310–26.
Vining, Aidan R., Claude Laurin, and David Weimer. 2014. The longer-run performance effects of agencification: Theory and evidence from Québec agencies. Journal of Public Policy 1–30. Online first.
Wilson, Paul W. 2008. FEAR: A software package for frontier efficiency analy-sis with R. Socio-Economic Planning Sciences 42:247–54.
Wistrich, Enid. 1992. Restructuring government New Zealand style. Public Administration 70:119–35.
Yamamoto, Kiyoshi. 2006. Performance of semi-autonomous public bodies: Linkage between autonomy and performance in Japanese agencies. Public Administration and Development 26:35–44.
Zajac, Edward J., Matthew S. Kraatz, and Rudi K. F. Bresser. 2000. Modeling the dynamics of strategic fit: A normative approach to strategic change. Strategic Management Journal 21:429–53.
Dow
nloaded from https://academ
ic.oup.com/jpart/article/26/2/309/2886449 by guest on 31 M
arch 2022
Related Documents











