
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
OVERVIEWOVERVIEW
Heat Related Illnesses
High Altitude Illnesses
Lightening Injuries
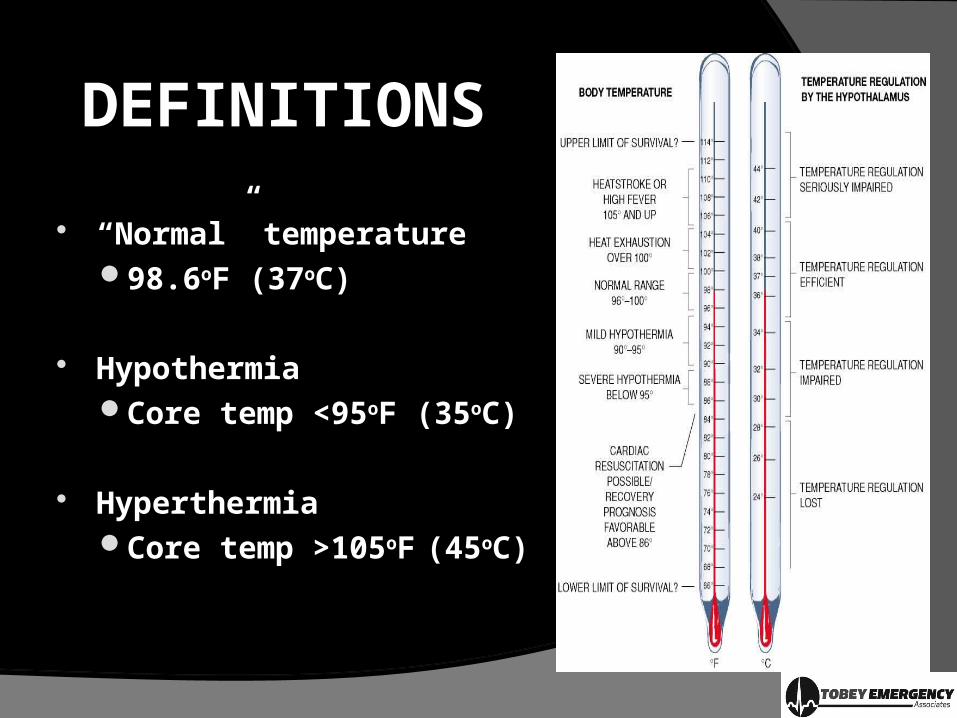
DEFINITIONSDEFINITIONS
“Normal” temperature98.6oF (37oC)
HypothermiaCore temp <95oF (35oC)
HyperthermiaCore temp >105oF (45oC)

HOMEOSTASIS: HOMEOSTASIS: THERMOREGULATIOTHERMOREGULATIO
NN Body’s desire to maintain a steady
internal environment
Maintain enzyme / cell activities & organ functions
Body temp maintained by multiple interconnected mechanismsPrimarily set by hypothalamus acting as a thermostatPeripheral & central thermoreceptors shunt blood to
core to maintain homeostasis
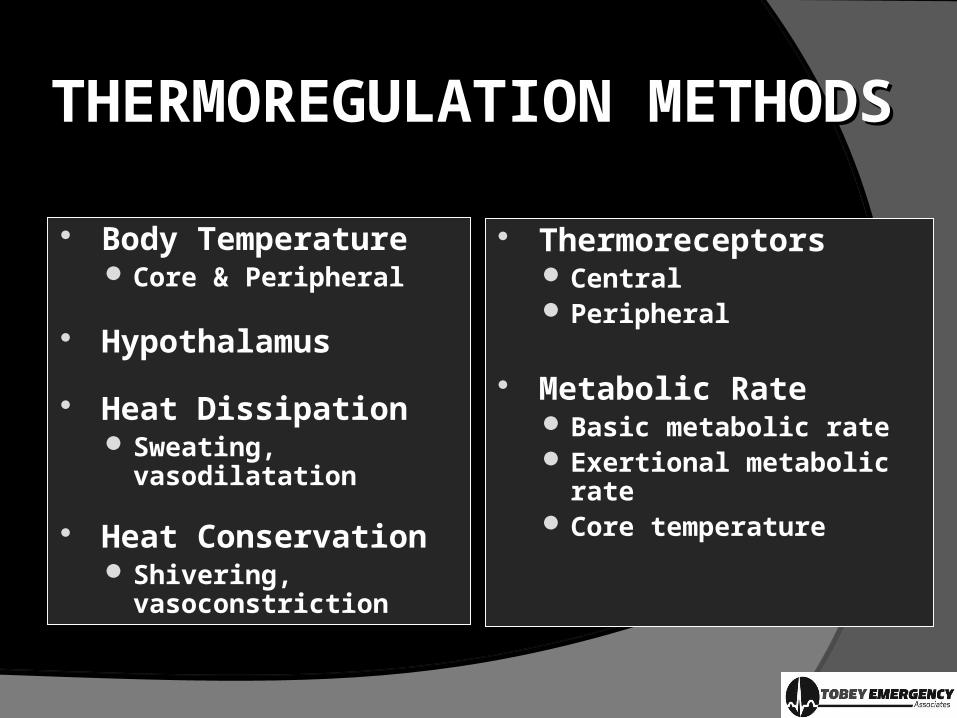
THERMOREGULATION THERMOREGULATION METHODSMETHODS
Body Temperature Core & Peripheral
Hypothalamus
Heat Dissipation Sweating, vasodilatation
Heat Conservation Shivering,
vasoconstriction
Thermoreceptors Central Peripheral
Metabolic Rate Basic metabolic rate Exertional metabolic rate Core temperature

HOMEOSTASIS: HOMEOSTASIS: THERMOLYSISTHERMOLYSIS
Conduction Direct loss of heat from one object to another
Convection Direct heat loss to air currents
Radiation Heat loss to nearby objects without direct contact
Evaporation Heat loss secondary to water evaporation from skin
Respiration Convection, radiation & evaporation
HOMEOSTASIS: HOMEOSTASIS: THERMOREGULATIONTHERMOREGULATION
Body generates cellullar level heat via mitochondrial metabolism
○ Basal metabolic rate○ Exertion metabolic rate
Shivering is an autonomic / automatic heat forming mechanism via muscle contraction

THERMAL REGULATIONTHERMAL REGULATION
Heat flows from area of high to low temperature
A body in warm environment gains heat, a body in a cool environment gives off heat
Other factors: Wind Relative humidity
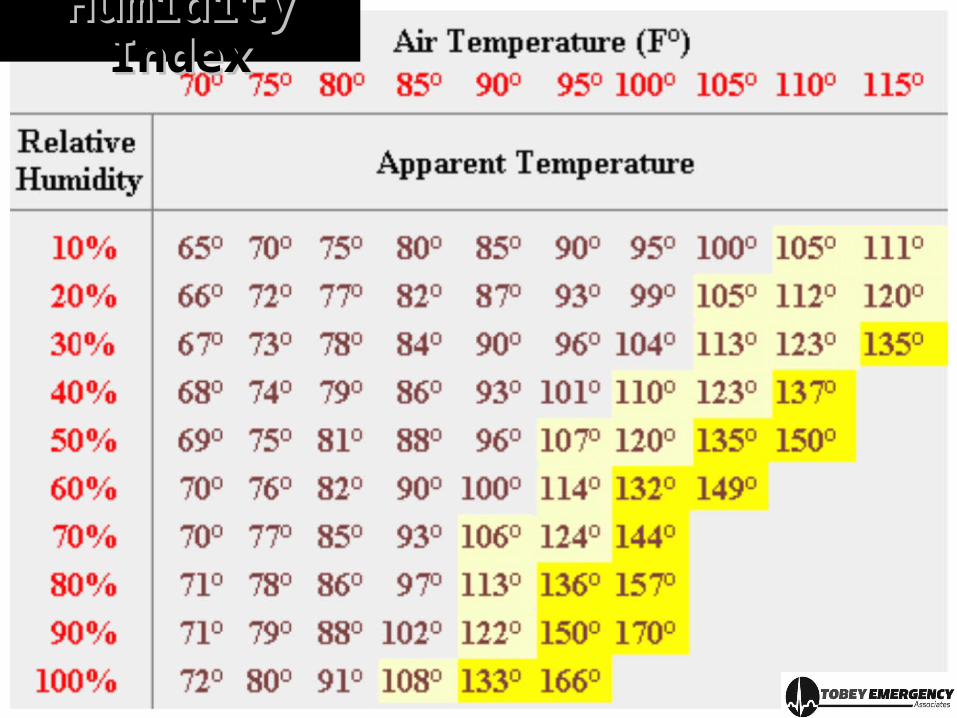
Humidity Humidity IndexIndex

RISK FACTORSRISK FACTORS Age
Age extremes less able to tolerate temp shifts
Poor Health & Predisposing PMH IDDM: autonomic dysfunction reduces ability to vasodilate &
sweat Cardiac: fluid shifts not tolerated well
Medications Beta blockers, Diuretics, Antipsychotics
Environmental Factors Acclimitization, exposure time, ambient temperature, Humidity,
Wind
PREVENTATIVE PREVENTATIVE MEASURESMEASURES
Adequate fluid intake Dehydration prevents thermolysis
Recognizing SSX Early: N / V / abd pain, vision disturbances, decreased urine
output, poor skin turgor, hypovolemic shock
Treatment Hydration Gradual acclimatization Limited exposure to hostile environments

HEAT EMERGENCIES HEAT EMERGENCIES SPECTRUMSPECTRUM
Heat Cramps: Muscle cramps relieved by salt & hydration
Heat Edema: Swollen ankles relieved by leg elevation
Heat Syncope: LOC from vasodilation; must r/o serious etiologies
Heat Exhaustion: Volume depletion with vague, non-specific SSX
Heat Stroke: CNS dysfunction is hallmark

HYPERTHERMIAHYPERTHERMIA
Abnormal elevation of core temperature typically caused by elevated external temperatures
Must differentiate from fever (“pyrexia”) Fever: normal response to infection caused by pyrogens
which reset hypothalamic thermostat & increase BMR
Fever makes body environment less hospitable to infectious organisms
Fever treatable with anti-pyretics, hyperthermia is not
HEAT CRAMPSHEAT CRAMPS
Painful “non-emergency” that must be differentiated from other disorders
Hyperthermia causes sweating Sweat consists of water & salt Sodium loss causes muscle cramping
Symptoms: Extremity muscle cramping A & O, though weak, faint or dizzy Skin is warm & moist Temp normal to mildly elevated Vitals “reasonably” normal, often with tachycardia

HEAT EXHAUSTIONHEAT EXHAUSTION Most common heat illness seen by EMS
Etiology: Sweat & sodium loss creates loss of blood volume Vasodilation worsens problem ultimately causing a drop in cardiac
output /BP with a rise in heart rate to compensate
SSX: Body temp >100F (37.8) Cool & clammy skin Tachypnea, tachycardia, hypotension Muscle cramping & generalized weakness CNS: Headache, Anxiety, Impaired judgment
Progresses to Heat Stroke if not treated
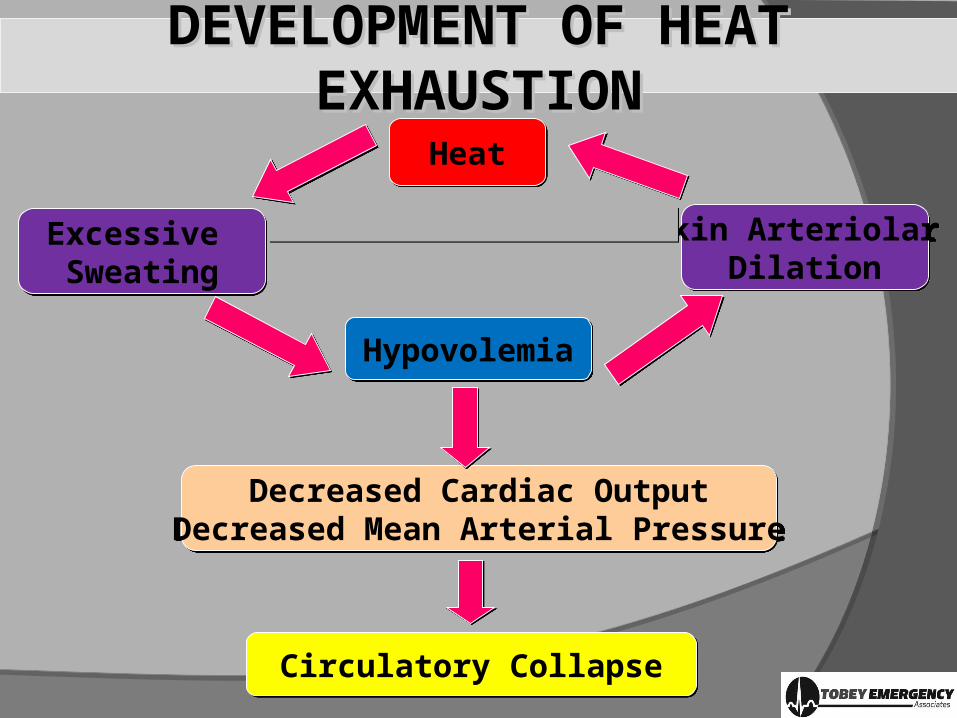
DEVELOPMENT OF HEAT DEVELOPMENT OF HEAT EXHAUSTIONEXHAUSTION
HeatHeat
Excessive Sweating
Excessive Sweating
HypovolemiaHypovolemia
Skin Arteriolar Dilation
Skin Arteriolar Dilation
Decreased Cardiac OutputDecreased Mean Arterial Pressure
Decreased Cardiac OutputDecreased Mean Arterial Pressure
Circulatory CollapseCirculatory Collapse

HEAT EXHAUSTION HEAT EXHAUSTION TREATMENTTREATMENT
Remove from environment
Remove clothing, active & passive cooling
Oral electrolytes or IV crystalloids
Resolves with hydration, rest & supine
If symptoms do not resolve consider other causes
HEAT STROKEHEAT STROKE
Environmental emergency with 80% mortality if late or inadequate treatment
Hallmark: hot dry skin without sweat plus AMS
Lack of hypothalamic thermoregulation causes uncontrolled hyperthermia
Core temp often >105 F Cellular death, protein denaturation Damage to brain, kidney & liver causes multi-system failure Rectal temperature is necessary to provide accurate reading
HEAT STROKE HEAT STROKE CATEGORIESCATEGORIES
“Classic” Secondary to altered thermoregulationElderly, chronically ill, patients with AMS
“Exertional”Healthy individuals with significant heat stressSkin initially moist due to exertional sweating
HEAT STROKE HEAT STROKE SSXSSX
Core temp >105F (40.5C)
Mental status changes / anxiety / Confusion
Hypotension
Tachypnea
Renal failure
DIC
Hypotension with bounding or thready tachycardia
Possible seizures

DEVELOPMENT OF HEAT DEVELOPMENT OF HEAT STROKESTROKE
Strenuous ExerciseHot, Humid Environment
Strenuous ExerciseHot, Humid Environment
Inadequate Temperature RegulationInadequate Temperature Regulation
Core Temperature ElevatesCore Temperature Elevates Impaired CNS FunctionImpaired CNS Function
Organ & Tissue DamageOrgan & Tissue Damage
Coma & DeathComa & Death

HEATSTROKHEATSTROKE E
TREATMENTTREATMENT
Transfer to cool environment
Remove clothing, start rapid active cooling Cover with moist sheets Mist with cool water
Target temperature 102F Overcooling may cause
reflex hypothermia
Administer O2 prn
IV rehydration
Cardiac monitor
AVOID vasopressors or anticholinergic drugs
Reassess vitals frequently
OEMS 2.3 HYPERTHERMIA /OEMS 2.3 HYPERTHERMIA /HEAT EMERGENCIESHEAT EMERGENCIES
Priorities: Rapid Recognition & Cooling! Scene safety, BSI Airway management, O2 as needed Continually assess & record LOC, ABCs, vitals SAMPLE history Loosen / remove clothing, move to cool environment If A&Ox3, give water or oral rehydration solution Rapid transport w/wo ALS in position of comfort Do not allow patient to exert themselves
OEMS 2.3 OEMS 2.3 MANAGEMENTMANAGEMENT
Rapid but not “over” cooling; If shivering occurs, discontinue active cooling
Cool packs to armpits, neck, groin and evaporation techniques (fans, windows)
Keep skin wet with towels or sponges Elevate legs if supine ALS intercept if necessary & available; Rapid transport w/wo ALS Notify receiving hospital
INTERMEDIATE AND PARAMEDIC Advanced airway management if necessary IV, O2, Monitor If SBP <100 give 250 bolus NS, titrate to hemodynamic status Medical Control for additional IVF boluses

HEAT HEAT EMERGENCIES EMERGENCIES
NOTESNOTES
No minimum temp for heat related illnesses Temperature severity does not
necessarily correlate with severity of heat illness Can be normothermic with heat cramps & exhaustion
Shivering begins when skin temperature drops, but core temp remains high Versed given to stop shivering and prevent core temperature
from rising despite cooling efforts

HEAT EMERGENCIES HEAT EMERGENCIES SUMMARYSUMMARY
Condition Muscle Cramps
Mental Status
Resp Pulse BP Core Temp Other
Heat Cramps
Yes Alert Normal Normal Normal Normal Weakness
Dizziness
‘Feel Faint’
Heat
Exhaustion
Possible Anxious, ALOC
Rapid, Shallow
Rapid, Weak
Normal Mildly Elevated
Headache
“Pins & Needles”
Diarrhea
Heat
Stroke
No ALOC, Delirium,
Coma
Deep & Rapid with
late Shallow Slowing
Rapid, Full with late slowing
Low Very High Seizures

LIGHTENING LIGHTENING INJURIESINJURIES
2nd largest US storm killer; mortality 45-50 persons/yr
Injuries 10x more commonly than fatalities
10% lightening injuries are in persons who are indoors
Use of cell phones & portable electronic devices does not increase the risk of injury except via distracting
US LIGHTENING FACTS
1/3 lightening injuries work-related
Most common days: Sat, Sun & Weds
Most common times: 1200–1800, 1800–midnight
Irrational fear of lightning: “astraphobia”
Study of lightning: “fulminology” by a “fulminlogist”

WHAT IS LIGHTNING?WHAT IS LIGHTNING? Atmospheric electrostatic
discharge of a “leader” bolt travelling at >220,000 km/h (140,000 mph) reaches temps of 30,000 °C (54,000 °F)
Hot enough to fuse sand into glass (fulgurites)
Causes air ionisation leading to formation of NO & nitric acid which act as fertilizer to green plant life
Lightning has (+) and (-) bolt polarity (-) current 30,000 amperes, 500 megajoules of energy (+) current 300 kA , 10X greater than (-) bolts Average single bolt peak power output one trillion watts
(terawatt), lasting for 30 millionthsof a second
Voltage proportional to length bolt
Bolt heats vicinity air to 20,000 °C (36,000 °F), 3X temp of sun’s surface which causes a supersonic acoustic shock wave (thunder)
Return stroke follows a charge channel 1cm wide

• Upper cloud carries (+) charge, lower part carries (-) charge
• “Step leader" originates from cloud for 50ms then zig-zags gaining (-) charge
• High speed electrons ionize air, providing conducting path for bolt
• As step leader nears ground, strong electric field drives (+) ground charge to neutralize (-) charge in the "return stoke“
• Upper cloud carries (+) charge, lower part carries (-) charge
• “Step leader" originates from cloud for 50ms then zig-zags gaining (-) charge
• High speed electrons ionize air, providing conducting path for bolt
• As step leader nears ground, strong electric field drives (+) ground charge to neutralize (-) charge in the "return stoke“

LIGHTENING LIGHTENING INJURIESINJURIES
Not pure direct or alternating current
Most important difference between lightning & high-voltage electrical injuries is duration of current exposure
While energy briefly flows through person. vast majority of lightning energy flashes around body surface
Most energy mediated by other factors including surrounding objects that when are hit then transmits energy to person <1/3 of affected persons have burns When burns occur, they are usually superficial
Lightning strikes primarily neurologic injuries
LIGHTENING STRIKESLIGHTENING STRIKES
Direct 3-5% of injuries
Side splash 30% of injuries
Contact voltage from touching object that is struck 1-2% of injuries
Current effect as energy spreads across ground 40-50% of injuries
Upward leader does not connect w/downward leader 20-25% of injuries

CARDIAC CARDIAC INJURIESINJURIES
Massive defibrillation into VF (most common) or asystole, from which heart often spontaneously recovers
Respiratory arrest lasts longer than cardiac arrest
A secondary cardiac event arrest from hypoxia or CNS injury may occur
Most commonly ECG change is QT prolongation

NEUROLOGICAL NEUROLOGICAL INJURIESINJURIES
Neurocognitive deficits similar to TBIs: difficulty processing new information or multitasking
Chronic pain syndromes
Sympathetic nervous system injury: vascular spasm, paralysis, transient HTN, extremity mottling (keraunoparalysis), vertigo &/ or tinnitus
If found unconscious, suspect CNS & spinal injury
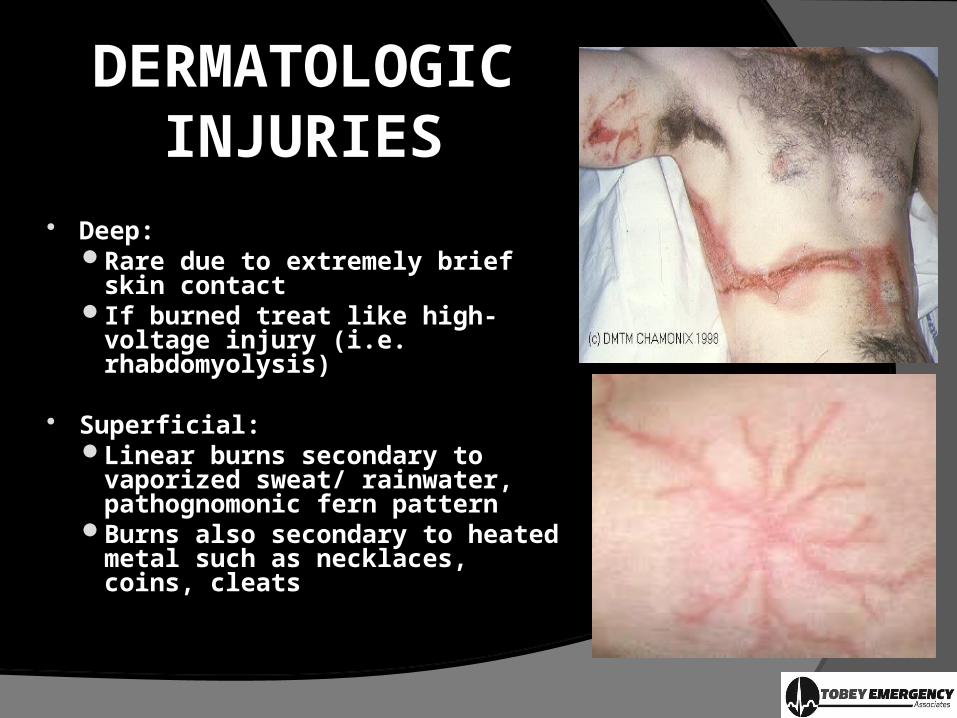
DERMATOLOGIC DERMATOLOGIC INJURIESINJURIES
Deep:Rare due to extremely brief skin
contact If burned treat like high-voltage
injury (i.e. rhabdomyolysis)
Superficial:Linear burns secondary to
vaporized sweat/ rainwater, pathognomonic fern pattern
Burns also secondary to heated metal such as necklaces, coins, cleats
BLUNT BLUNT TRAUMATRAUMA
Fractures more common in high-voltage injuries than directly related to lightning, but are common if patient fell or was thrown by the strike
Organ / cardiac / pulmonary contusions rare
Ear is sensory organ most commonly injured by lightningTM rupture from concussive or explosive force, direct
current entry, basilar skull fractureHearing loss, tinnitus, & CN 8 nerve symptoms
Eye injuries common: cataracts, macular holes, retinal separation, iritis

MANAGEMENTMANAGEMENT
Scene safety!
Resuscitation in the field if safe, otherwise evacuate
Spinal precautions if any LOC
ACLS protocols for specific arrythmia AEDs effectively used in a number of cases
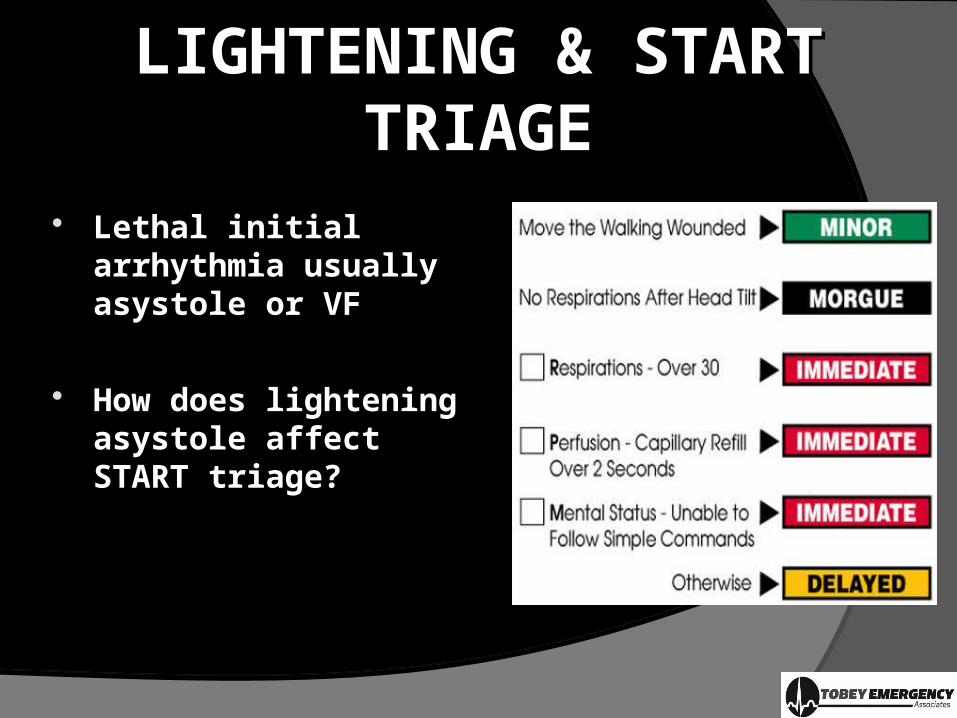
LIGHTENING & START LIGHTENING & START TRIAGETRIAGE
Lethal initial arrhythmia usually asystole or VF
How does lightening asystole affect START triage?

ALTITUDE ALTITUDE RELATED ILLNESSRELATED ILLNESS
Elevations > 5000 ft produce physiologic consequences from low oxygen levels
Hypoxia results in spectrum of mild to critical illnesses
History: recent gain in altitude with complaints of headache PLUS one of: GI upset Fatigue Dizziness Insomnia

SPECTRUMSPECTRUM
Mild Nonspecific SSX similar to viral illness
High Altitude Pulmonary Edema (HAPE): Dyspnea, fatigue, dry cough
High Altitude Cerebral Edema (HACE): ALOC with neurological findings
High Altitude Retinal Hemorrhage (HARH)
General Treatment Guidelines: Immediately descend Acetazolamide (also preventative)
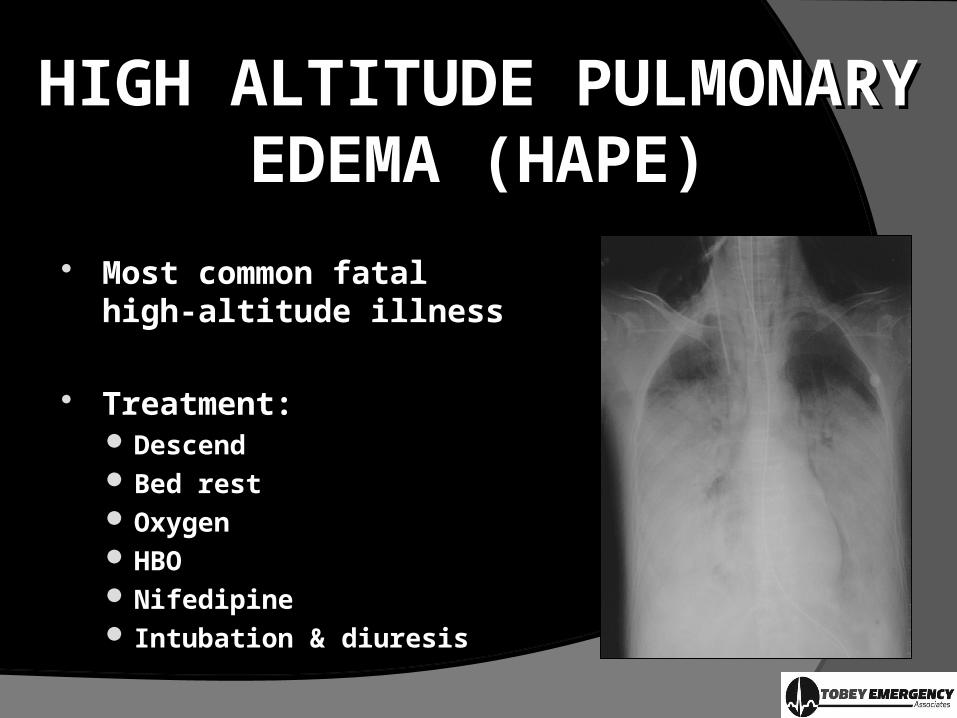
HIGH ALTITUDE PULMONARY HIGH ALTITUDE PULMONARY EDEMA (HAPE)EDEMA (HAPE)
Most common fatal high-altitude illness
Treatment: Descend Bed rest Oxygen HBO Nifedipine Intubation & diuresis

HIGH ALTITUDE CEREBRALHIGH ALTITUDE CEREBRALEDEMA (HACE)EDEMA (HACE)
Least common, most severe
Symptoms: Ataxia / Seizures Slurred speech Focal neurological deficits AMS
Treatment: Rapidly descend 100% Oxygen HBO

SUMMARYSUMMARY
Review of common environmental emergencies“Heat” “Height”“Holy Sh-t”

Related Documents











