8/9/2019 Amino Acid Analyzers http://slidepdf.com/reader/full/amino-acid-analyzers 1/17 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA Tel +1 (610) 825-6000 Fax +1 (610) 834-1275 Web www.ecri.org E-mail [email protected] UMDNS Information This Product Comparison covers the following device term and product code as listed in ECRI Institute’s Universal Medical Device Nomenclature System™ (UMDNS™): Analyzers, Laboratory, Body Fluid, Amino Acid [15-090] Amino Acid Analyzers Scope of this Product Comparison This Product Comparison covers automated amino acid analyzers that can be used in the clinical laboratory. The major components are listed in the chart; however, several manufacturers make other configurations available. The two most commonly used high-performance liquid chromatography (HPLC) techniques for amino acid analysis, ion-exchange and reversed-phase liquid chromatography (LC), are discussed. (See the Product Comparison titled Chromatography Systems, Liquid, High-Performance for more information on the principles of HPLC.) Purpose Amino acid analyzers detect and quantify primary and secondary amino acids in physiologic fluids such as plasma and urine to confirm diagnoses and monitor treatment of inborn metabolism errors and of other disorders. These disorders are usually genetically produced errors in protein metabolism and can have serious complications if not detected and treated early. The most common of disorder is phenylketonuria (PKU), in which an enzyme deficiency results in increased concentrations of phenylalanine. PKU occurs an average of once in every 10,000 births and is associated with mental retardation, seizures, and eczema. Other aminoacidurias include tyrosinemia, alkaptonuria, homocystinuria, and branched-chain ketoaciduria (maple syrup urine disease), in which an enzyme defect in the decarboxylation of branched-chain α-keto acids increases concentrations of leucine, isoleucine, valine, and alloisoleucine. Changes in amino acid levels can also be caused by starvation, injury, sepsis, liver or renal failure, and cancer. Amino acid analyzers can also detect neurochemically active amino acids (aspartate, glutamate, and α- aminobutyric acid) in cerebrospinal fluid and can be used to assess the nutritional status of patients before surgery as well as to follow the progress of their treatment. Principles of operation Amino acids are organic compounds containing an amino group (NH2) and a carboxyl group (COOH), which are linked by peptide bonds to form proteins. Many are synthesized by the body, while others are supplied in the diet. The important feature in separating amino acids is their basic structure: they are highly polar substances Comprehensive of Biomedical Engineering Site (www.dezmed.com W W W . D E Z M E D . C O M

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 1/17
5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA Tel +1 (610) 825-6000 Fax +1 (610) 834-1275 Web www.ecri.org E-mail [email protected]
UMDNS Information
This Product Comparison covers the followingdevice term and product code as listed in ECRIInstitute’s Universal Medical Device NomenclatureSystem™ (UMDNS™):
Analyzers, Laboratory, Body Fluid, Amino Acid [15-090]
Amino Acid Analyzers
Scope of this Product Comparison
This Product Comparison covers automated amino acid analyzers that can be used in the clinical laboratory.
The major components are listed in the chart; however, several manufacturers make other configurations
available. The two most commonly used high-performance liquid chromatography (HPLC) techniques for amino
acid analysis, ion-exchange and reversed-phase liquid chromatography (LC), are discussed.
(See the Product Comparison titled Chromatography Systems, Liquid, High-Performance for more informationon the principles of HPLC.)
Purpose
Amino acid analyzers detect and quantify primary
and secondary amino acids in physiologic fluids such as
plasma and urine to confirm diagnoses and monitor
treatment of inborn metabolism errors and of other
disorders. These disorders are usually genetically
produced errors in protein metabolism and can have
serious complications if not detected and treated early.
The most common of disorder is phenylketonuria(PKU), in which an enzyme deficiency results in
increased concentrations of phenylalanine. PKU occurs
an average of once in every 10,000 births and is
associated with mental retardation, seizures, and eczema. Other aminoacidurias include tyrosinemia,
alkaptonuria, homocystinuria, and branched-chain ketoaciduria (maple syrup urine disease), in which an enzyme
defect in the decarboxylation of branched-chain α-keto acids increases concentrations of leucine, isoleucine,
valine, and alloisoleucine. Changes in amino acid levels can also be caused by starvation, injury, sepsis, liver or
renal failure, and cancer.
Amino acid analyzers can also detect neurochemically active amino acids (aspartate, glutamate, and α-
aminobutyric acid) in cerebrospinal fluid and can be used to assess the nutritional status of patients before
surgery as well as to follow the progress of their treatment.
Principles of operation
Amino acids are organic compounds containing an amino group
(NH2) and a carboxyl group (COOH), which are linked by peptide
bonds to form proteins. Many are synthesized by the body, while
others are supplied in the diet. The important feature in separating
amino acids is their basic structure: they are highly polar substances
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 2/17
Amino Acid Analyzers
2 ©2007 ECRI Institute. All Rights Reserved.
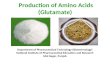
Figure 2. Difference between α - and β- amino acids
and exist in aqueous solutions as dipolar ions called
zwitterions, which have both negatively and
positively charged groups. The amino acids’
functional group (R), as shown in Figure 1, is used to
distinguish one amino acid from another; the figure
illustrates amino acid separation. Primary, orα , aminoacids have the amine group attached to the α , or first,
carbon atom adjacent to the carboxyl group;
secondary, or ß, amino acids have the amine group
attached to the ß, or second, carbon atom (see Figure
2). Some analyzers separate only primary amino acids,
while others separate both primary and secondary
amino acids.
Before chromatographic analysis, the peptide bonds
are dissolved in a solvent, and the sample is typically
reacted with phenyl isothiocyanate in a buffer to form a phenylthiocarbamyl (PTC) derivative. The PTC amino
acids are converted to phenylthiohydantoin amino acid derivatives that are then separated by chromatography
and react with a reagent, such as ninhydrin, forming a colored compound.
Chromatography separates sample components based on differences in their relative affinities for different
media, which are divided into two phases: stationary and mobile. Automated amino acid analysis requires HPLC,
which uses a liquid mobile phase forced through a column by a high-pressure pump. Sample injection can be
automatic or manual. The column contains the stationary phase, which in HPLC is composed of a liquid bound to
a solid or a liquid through which the mobile phase percolates.
There are five basic HPLC techniques: adsorption, partition or bonded phase, reversed phase, ion exchange,
and size exclusion. Adsorption chromatography separates components by differences in solubility and binding
strength to the adsorbent. In partition-phase chromatography, the stationary and mobile phases are immiscible
liquids, and the components are separated according to their solubility ratios in the two phases. Reversed-phase
chromatography is similar to the partition technique, except that the polarities of the two liquids are reversed.
Ion-exchange chromatography uses ion-exchange resins for the stationary phase and a buffer solution as the
mobile phase. Size-exclusion chromatography uses a porous packing material that retains larger molecules while
allowing smaller ones to pass through, thereby separating components by molecular size.
The basic components of an HPLC system are a solvent reservoir, high-pressure pump, sample injector,
analytical column, detector, data recorder, and microprocessor. The solvent reservoir contains the mobile phase.
The pump, either single- or dual-piston reciprocating, contains a cam or gears that drive a piston into and out of
the pump. In the fill mode, the piston is withdrawn from the chamber, and liquid is drawn from the solvent
reservoir into the pumping chamber. In the pumping mode, the inlet check valve closes, and the outlet valve
opens as the piston drives the liquid into the column. A disadvantage of this type of pump is the pulsing nature
of the solvent flow; however, most systems
incorporate a damping mechanism that controls
this effect. The pumps in amino acid analyzersmost frequently use pressures from 1,000 to 3,000
pounds per square inch (psi).
The sample injector introduces the sample into
the column. The fixed-loop injector, the most
widely used type, is filled using a noncalibrated
syringe; the sample volume is dictated by the size
and internal diameter of the sample loop.
Figure 1. Basic structure of an amino acid
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 3/17
Amino Acid Analyzers
©2007 ECRI Institute. All Rights Reserved 3
Variable-volume injectors use a calibrated syringe to inject a precise volume into the loop.
The analytical column contains the stationary phase and is the most important part of the separation system.Usually composed of stainless steel that can withstand pressures up to 10,000 psi, the column ranges from 10 to
150 cm in length and from 2 to 5 mm in internal diameter. Column packing material should have minimum dead
volume (i.e., be tightly packed) and ensure maximum efficiency (i.e., narrow peaks on the chromatogram). Two
types of columns—the precolumn and the guard column—protect the analytical column. The precolumn is
located between the pump and the injection valve; in amino acid analysis, it separates derivatized amino acids.
The guard column, located between the injector and the analytical column, prolongs the life of the analytical
column by collecting any particulate matter or debris that would otherwise accumulate there. HPLC columns are
highly efficient when used with small (3, 5, or 10 μm), porous particles. Particle size must be as uniform as
possible for efficient columns and optimal operating pressures. Spherical and irregularly shaped particles are
available; columns packed with these seem to be more durable and can operate at lower pressures.
In ion-exchange LC, the stationary phase is an ion-exchange resin that separates compounds by the sign andmagnitude of their ionic charges. An aqueous solution is used as the mobile phase. The resins are highly
polymerized supports consisting of hydrocarbons with ionized functional groups. Available in the form of beads
or granular particles, they have an exchangeable counterion, which carries a charge opposite from that of the
functional group (i.e., cation exchangers contain acidic groups, and anion exchangers contain basic groups). The
sample cation (X+) of the cation exchange resin (often used for amino acids) competes with the mobile-phase ions
(Y+) for ionic sites on the support. Figure 3 shows how the counterions are replaced by sample cations and bind to
the functional groups. The neutral molecules and anions flow through the column and separate from the attached
sample cations. Another ion of higher affinity or large amounts of the same counterion can be used to elute the
Figure 3. The principle of ion-exchange resins
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 4/17
Amino Acid Analyzers
4 ©2007 ECRI Institute. All Rights Reserved.
sample cations, releasing the weakly bound cations first. This method also incorporates a postcolumn reaction of
ninhydrin with free amino acids, so the results can be detected in the visible range. Elution can also be adjusted
by controlling the pH of the mobile phase, depending on the stationary phase and sample ion that are being used
in the column.
In reversed-phase LC, a derivatizing reagent is usually added to the sample before it enters the column. The
mobile phase is polar and the stationary phase is nonpolar, thereby allowing the amino acids to separate by theirpolar functional groups (amines), which in normal phase would adsorb too strongly to the silica. The nonpolar
packings are hydrocarbons chemically bound to a silica base, allowing the more polar compounds to separate
first. One type of packing is octadecyl (C18 hydrocarbon bonded to silica particles), referred to as ODS (octadecyl
silica). The polar mobile phase can consist of acetonitrile, aliphatic alcohols, water, tetrahydrofuran, or mixtures
of these solvents.
The detector quantifies compounds as they elute from the column by relying on changes in the bulk property
of the mobile phase and the sample constituents, such as the refractive index (color change), or on some
characteristic property of the sample constituent, such as fluorescence or ultraviolet absorption. The most widely
used detector is the fixed- or variable-wavelength ultraviolet-visible photometer, which can detect nanogram
quantities. Another detector, the fluorometer, has a high sensitivity for fluorescent compounds and can determine
picogram quantities.
Reported problems
Problems can occur when buffers are contaminated with microorganisms, mainly Pseudomonas species, that
exhibit dihydrolase activity for arginine and decarboxylase activity for ornithine and lysine. This contamination
can lead to a loss of arginine and can also affect other amino acid recoveries.
The storage of specimens for even 24 hours can alter the plasma amino acid levels; therefore, specimens should
be analyzed as soon as possible. Because some derivatizing reagents are unstable, derivatized amino acids must
be assayed rapidly, and repeat testing may not yield reproducible results. Inaccurate results can also be caused by
contamination from a previous sample when using fixed-loop valves. The valve must be flushed with 5 to 10 loop
volumes before loading.
The various standardization procedures have some limitations. External standardization is subject to variablesample losses— both during the preparative steps and before chromatography analysis—as well as sample
injection variability. Under normal conditions, the internal standard should not be present in the sample: the
difficulty involved in accurately measuring two peaks could limit precision.
The use of uncoated glassware in automated analyzers may pose a safety hazard to laboratory personnel
because of the risk of breakage from solvent or buffer bottles. One reported case involved a borosilicate glass
bottle in an amino acid analyzer that exploded. The agency that reported the incident, the Scottish Home and
Health Department, a branch of the U.K. Department of Health, also recommends that laboratories considering
the use of plastic-coated glassware check with the supplier to determine whether the glassware is suitable for its
intended applications, since different plastic coatings resist chemicals differently, have assorted properties at
varied temperatures and pressures, and have distinct aging properties.
Purchase considerations
ECRI Institute recommendations
The accompanying comparison chart includes ECRI Institute’s recommendations for minimum performance
requirements for amino acid analyzers. The specifications have been rated using three categories: Required,
Preferred, and Optional. A rating of Required indicates that this specification is the minimum necessary for the
analyzer to perform its indicated function. The Preferred rating is used for specifications that enhance either test
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 5/17
Amino Acid Analyzers
©2007 ECRI Institute. All Rights Reserved 5
operations or ease of use and, therefore, effectiveness. The Optional rating indicates a specification that does not
affect the analyzer performing its inherent function, but the presence of these options will provide wider
applications of use by offering greater testing options or minimizing user interaction, allowing the analyzer to be
effectively operated under a wide variety of circumstances.
Facilities purchasing amino acid analyzers should take into consideration the automated features of the
instrument. Certain automatic features are desirable to facilitate sample analysis. For example, automatic sampleinjection is preferred to manual injection. Automatic sample injection eliminates the possibility of operator error
and ensures that all samples are treated in the same manner. Automated flushing after sample analysis ensures
that the analyzer is properly prepared for each subsequent sample and that no crossover contamination will
interfere with readings. It is recommended that clinical laboratory analyzers be able to interface with a laboratory
information system (LIS) in order to more easily collect and report diagnostic test results. The analyzer should
also be capable of displaying results and other information both on a monitor and as a printout.
The sample column should be made with a rustproof material to ensure longevity of the column. The column
should generally have a length of 10 to 150 cm and a width of 2 to 5 mm. The particle size should be as uniform as
possible to ensure adequate separation of the sample. Dual-piston, single-piston, and syringe eluent pumps are all
generally acceptable. The pump should have a pressure limit of at least 2,000 psi.
Other considerations
Ideally, before making a purchase, facilities should evaluate the amino acid analyzers they are considering in
their own clinical environment for a few weeks. On-site evaluation enables laboratories to verify the
characteristics of the instrument reported by the manufacturer (e.g., pump flow accuracy, detector sensitivity and
stability) with the workload and sample types that the laboratory normally handles.
Because of the risk of infection involved with handling any body-fluid specimen, purchasers should consider
devices that minimize operator contact with specimens.
Final regulations of the Clinical Laboratory Improvement Amendments of 1988 (CLIA) were published by the
U.S. Department of Health and Human Services in February 1992. Under the CLIA regulations, all clinical
laboratories are required to obtain federally issued certificates. To acquire a certificate, a lab must meet all
relevant standards, which are determined by the complexity of the tests being performed. The standards set forth by CLIA apply to areas such as patient test management, quality control (QC), proficiency testing, personnel
qualifications, and quality assurance (QA) programs. Certification fees vary according to complexity level and
test volume. There are different levels of complexity outlined in the CLIA regulations with corresponding
calibration and quality control requirements. These requirements have changed as of January 2003. More
information can be found at the following Web site: http://www.cms.gov/clia.
Before purchasing new equipment or upgrading existing equipment, laboratories should thoroughly
investigate the CLIA regulations that apply to their facility and to the devices being considered. In certain
situations, purchasing or upgrading a device may change the complexity category of the procedures. This could
require additional staff training and certification, as well as changes in QC, proficiency testing, QA programs, and
other laboratory procedures.
An important consideration is the system’s computer interface capabilities. The effectiveness of the interfacewith the existing LIS or the hospital’s central computer system is crucial for inputting test data, verifying testing
accuracy, and maintaining QC, calibration, proficiency testing, and patient files according to CLIA guidelines.
Although CLIA does not mandate computerized reporting systems in hospital laboratories, it does require
laboratories to have a system in place to ensure compliance with CLIA performance standards for QC and QA of
patient testing instruments and procedures. An effective LIS interface is a fast and efficient way to manage the
large volume of test data that a laboratory generates each day as well as a convenient method of organizing and
storing data needed to comply with CLIA and other inspection agencies’ requirements. (See the Product
Comparison titled Information Systems, Laboratory for more information.)
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 6/17
Amino Acid Analyzers
6 ©2007 ECRI Institute. All Rights Reserved.
Cost containment
The following performance features can be used to assess an analyzer’s overall usefulness as well as its long -
term operating costs:
Column resolution. The ability of an LC column to separate a sample into its component amino
acids, as determined by a given control. Poor column resolution leads to costly duplicate and
corroborative testing on other instruments or, if the broad error range is not recognized, may
cause incorrect patient diagnoses.
Sample retention. The time it takes to process a sample in the chromatography column. Long
retention times lead to lengthy sample turnaround times, which can reduce long-term laboratory
productivity and revenue.
Analytical range. The concentration range over which the detector can measure a particular amino
acid compound. Purchasers should check these values carefully under conditions in their own
laboratories because actual ranges may vary significantly from those stated by the manufacturer.
Response/noise ratio. The ability of the instrument to distinguish between the signal of the amino
acid being analyzed and extraneous signals from other sources (e.g., column residue, interfering
compounds). Analyzers with low response/noise ratios produce inconclusive test results,
frequently requiring duplicate testing. Specificity. The ability of the detector to measure only the compound selected. If an analyzer
cannot discriminate between a selected amino acid and another substance with similar
properties, it includes them both in the analyte measurement. Instruments that measure a
substance nonspecifically can provide results that may lead to a false diagnosis, requiring costly
verification on other instruments.
Precision. A high degree of precision, which is a measure of how closely a test result can be
reproduced, not only provides a more sensitive determination of changes in the patient’s
condition but also reduces the need for much duplicate testing to verify the accuracy of initial test
results. Precision is expressed numerically in terms of the coefficient of variation (CV), with a
small CV indicating a highly precise instrument.
Stability. Analyzers that give readings with a high degree of precision for extended periods of usehave very stable calibration curves. These units may be less costly to operate than analyzers with
more labile curves because they do not require recalibration as often; the unit thus uses fewer
calibration controls and runs fewer nonpatient analytical tests.
Onboard reagent stability is an important consideration because some reagents lose their efficacy a short time
after they are inserted into the analyzer. Reagents that must be discarded because they have lost their effective
strength or have been contaminated will increase testing costs.
Carryover. The residue left over from a previous sample in a sample injector loop. This results
from incomplete flushing of the loop with a wash solution. Carryover can cause erroneously high
or low readings in samples and can result in duplicate testing or even unit shutdown if the
problem cannot be corrected by adjusting the washing cycle. Downtime. The time during which the analyzer is undergoing routine maintenance or is shut
down for troubleshooting and repairs. A unit that requires frequent maintenance or has a poor
reliability record cannot consistently handle a normal workload and will cost the laboratory
money to service (even with a good service contract), as well as lose testing revenue. Under these
circumstances, a reliable backup analyzer is a necessity.
Buyers should try to obtain a written guarantee from the device supplier specifying the length of time the
device is likely to operate at normal usage before it will require servicing. The guarantee should contain financial
penalties against the supplier if the device fails beforehand or if it fails again prematurely after servicing.
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 7/17
Amino Acid Analyzers
©2007 ECRI Institute. All Rights Reserved 7
Current analyzer users are valuable sources of information on the quality, reliability, and overall efficiency of
the instruments. Buyers should ask manufacturers to supply an unedited list of their customers when considering
an instrument.
Upgrading/interfacing. Potential purchasers should consider whether the analyzer can accept
future hardware upgrades and if the unit can interface with other laboratory instruments (e.g.,
chemistry analyzers) that can provide additional parameters. Included in an estimate of recurringexpenses should be the cost of upgrading the software annually.
Flexibility. Some amino acid analyzers can be used for other applications, such as therapeutic
drug monitoring and assaying for vitamins, certain hormones, and physiologic indicators (e.g.,
creatinine). Instruments with this kind of flexibility have an increased value to the laboratory
because of their wide range of uses as backup units to more dedicated instruments and as
alternative testing devices for running corroborative tests. They also help reduce the number of
workstations in the laboratory.
Hospitals should negotiate the best price for consumables (e.g., reagents, calibration gases, controls), training
programs, and service contracts at the time of purchase. They should also retain the option to accept or reject the
service contract at the end of the warranty period.
Stage of development
Technological advancements in HPLC have led to improved techniques in amino acid analysis and to a greater
variety of HPLC equipment, which, in turn, has enhanced market interest. Reversed-phase LC has become widely
accepted because it can reduce turnaround time without loss of sensitivity. In addition, some of the newer HPLC
derivatizing reagents can develop stable derivatives with amino acids. Online derivatization systems enhance
sensitivity and reduce manual input.
Advanced microprocessors have allowed the development of completely automated amino acid analysis
systems and have helped reduce turnaround time. Computer workstations allow automatic generation of
calibration curves from standards, automation of the chromatography system, rapid data input and test result
storage, and data communication with other computer systems in the laboratory and hospital. Analyzer
technology has become sufficiently versatile to adapt to batch analysis and is therefore useful in diagnosticapplications and for research.
Bibliography
Burtis CA, Ashwood ER, eds. Tietz fundamentals of clinical chemistry. 5th ed. Philadelphia: WB Saunders; 2001.
Centers for Disease Control and Prevention, Centers for Medicare & Medicaid Services. Medicare, Medicaid, and
CLIA programs; laboratory requirements relating to quality systems and certain personnel qualifications [final
rule]. Fed Regist 2003 Jan 24;68(16):3639-714.
Henry JB. Clinical diagnosis and management by laboratory methods. 20th ed. Philadelphia: WB Saunders; 2001.
Hersh LS, ed. New developments in clinical instrumentation. Boca Raton (FL): CRC Press; 1981.
Medicare, Medicaid and CLIA programs; regulations implementing the Clinical Laboratory Improvement
Amendments of 1988 (CLIA)—HCFA [final rule with comment period]. Fed Regist 1992 Feb 28;57(40):7002-186.
Narayanan S. Principles and applications of laboratory instrumentation. Chicago: ASCP Press; 1989.
Schoeff LE, Williams RH, eds. Principles of laboratory instruments. St. Louis: Mosby-Year Book; 1993.
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 8/17
Amino Acid Analyzers
8 ©2007 ECRI Institute. All Rights Reserved.
Supplier information
BIOCHROM
Biochrom Ltd [391206]
22 Cambridge Science Park Milton Road
Cambridge CB4 4FJ
EnglandPhone: 44 (1223) 423723 Fax: 44 (1223) 420164
Internet: http://www.biochrom.co.uk
E-mail: [email protected]
GBC SCIENTIFIC
GBC Scientific Equipment Inc [108495]
151 N State St Suite A PO Box 339
Hampshire, IL 60140
Phone: (847) 683-9870, (866) 442-2724 Fax: (847) 683-9871
Internet: http://www.gbcsci.com
E-mail: [email protected]
GBC Scientific Equipment Pty Ltd [139347]
12 Monterey Road
Dandenong 3175
Australia
Phone: 61 (3) 92133666 Fax: 61 (3) 92133677
Internet: http://www.gbcsci.com
E-mail: [email protected]
HITACHI
Hitachi High-Technologies America Inc [409074]
10 N Martingale Suite 500
Schaumburg, IL 60173
Phone: (847) 273-4141 Fax: (847) 273-4407Internet: http://www.hitachi-hhta.com
E-mail: [email protected]
Hitachi High-Technologies Europe (UK) [409777]
Craven House 40 Uxbridge Road Ealing
London W5 2BS
England
Phone: 44 (20) 73066727 Fax: 44 (20) 85665435
Internet: http://www.hht-eu.com
E-mail: [email protected]
Hitachi High-Technologies Europe GmbH [409776]
Berliner Strasse 91
Ratingen D-40880
Germany
Phone: 49 (2102) 453156 Fax: 49 (2102) 436858
Internet: http://www.hht-eu.com
E-mail: [email protected]
Hitachi High-Technologies Corp [409075]
1-24-14 Nishi-Shimbashi Minato-ku
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 9/17
Amino Acid Analyzers
©2007 ECRI Institute. All Rights Reserved 9
Tokyo 105-8717
Japan
Phone: 81 (3) 35047111 Fax: 81 (3) 35047123
Internet: http://www.hitachi-hitec.com
E-mail: [email protected]
JASCO
JASCO Corp [137956]
2967-5 Ishikawa-cho Hachioji
Tokyo 192-8537
Japan
Phone: 81 (426) 464111 Fax: 81 (4) 26464120
Internet: http://www.jasco.co.jp
E-mail: [email protected]
JASCO Eastern Europe Inf [418523]
Karolina utca 29-31
Budapest H-1113
Hungary
Phone: 36 (1) 4669579 Fax: 36 (1) 2093538Internet: http://www.jasco.co.jp
E-mail: [email protected]
JASCO Europe srl [152763]
via Confalonieri 25
Cremella (LC) I-23894
Italy
Phone: 39 (039) 956439 Fax: 39 (039) 958642
Internet: http://www.jasco-europe.com
E-mail: [email protected]
JASCO Inc [102714]8649 Commerce Dr
Easton, MD 21601-9903
Phone: (410) 822-1220, (800) 333-5272 Fax: (410) 822-7526
Internet: http://www.jascoinc.com
E-mail: [email protected]
JEOL
JEOL (Australasia) Pty Ltd [333604]
Unit 9 750-752 Pittwater Road
Brookvale 2100
Australia
Phone: 61 (2) 99058255 Fax: 61 (2) 99058286
Internet: http://www.jeol.com.au E-mail: [email protected]
JEOL (Europe) SA Poland [418633]
Oddziat w Warszawie ulica Szpitalna 1 pok 13
Warszawa PL-00-020
Poland
Phone: 48 (22) 8261252 Fax: 48 (22) 8261252
Internet: http://www.jeol.com
E-mail: [email protected]
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 10/17
Amino Acid Analyzers
10 ©2007 ECRI Institute. All Rights Reserved.
JEOL Ltd [140223]
Shin-Suzuharu Building 3/Fl 2-8-3 Akelbono-cho Tachikawa
Tokyo 190-0012
Japan
Phone: 81 (4) 25283363 Fax: 81 (4) 25283386
Internet: http://www.jeol.com E-mail: [email protected]
JEOL USA Inc [105627]
11 Dearborn Rd
Peabody, MA 01960
Phone: (978) 535-5900 Fax: (978) 536-2205
Internet: http://www.jeol.com
E-mail: [email protected]
KNAUER
Wissenschaftliche Geraetebau Dr Ing Herbert Knauer GmbH [179828]
Hegauer Weg 38
Berlin D-14163Germany
Phone: 49 (30) 8097270 Fax: 49 (30) 8015010
Internet: http://www.knauer.net
E-mail: [email protected]
WATERS
Waters Corp [186647]
34 Maple St
Milford, MA 01757
Phone: (508) 478-2000, (800) 252-4752 Fax: (508) 872-1990
Internet: http://www.waters.com
E-mail: [email protected]
Note: The data in the charts derive from suppliers’ specifications and have not been verified through
independent testing by ECRI Institute or any other agency. Because test methods vary, different products’
specifications are not always comparable. Moreover, products and specifications are subject to frequent changes.
ECRI Institute is not responsible for the quality or validity of the information presented or for any adverse
consequences of acting on such information.
When reading the charts, keep in mind that, unless otherwise noted, the list price does not reflect supplier
discounts. And although we try to indicate which features and characteristics are standard and which are not,
some may be optional, at additional cost.
For those models whose prices were supplied to us in currencies other than U.S. dollars, we have also listed the
conversion to U.S. dollars to facilitate comparison among models. However, keep in mind that exchange rates changeoften.
Need to know more
For further information about the contents of this Product Comparison, contact the HPCS Hotline at +1 (610) 825-6000, ext.
5265; +1 (610) 834-1275 (fax); or [email protected] (e-mail).
Last updated October 2007
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 11/17
Amino Acid Analyzers
©2007 ECRI Institute. All Rights Reserved 11
Policy Statement
The Healthcare Product Comparison System (HPCS) is published by ECRI Institute, a nonprofit organization.
HPCS provides comprehensive information to help healthcare professionals select and purchase diagnostic and
therapeutic capital equipment more effectively in support of improved patient care.
The information in Product Comparisons comes from a number of sources: medical and biomedical
engineering literature, correspondence and discussion with manufacturers and distributors, specifications from
product literature, and ECRI Institute’s Problem Reporting System. While these data are reviewed by qualified
health professionals, they have not been tested by ECRI Institute’s clinical and engineering personnel and are
largely unconfirmed. The Healthcare Product Comparison System and ECRI Institute are not responsible for the
quality or validity of information derived from outside sources or for any adverse consequences of acting on such
information.
The appearance or listing of any item, or the use of a photograph thereof, in the Healthcare Product Comparison
System does not constitute the endorsement or approval of the product’s quality, performance, or value, or of
claims made for it by the manufacturer. The information and photographs published in Product Comparisons
appear at no charge to manufacturers.
Many of the words or model descriptions appearing in the Healthcare Product Comparison System are
proprietary names (e.g., trademarks), even though no reference to this fact may be made. The appearance of any
name without designation as proprietary should not be regarded as a representation that is not the subject of
proprietary rights.
ECRI Institute respects and is impartial to all ethical medical device companies and practices. The Healthcare
Product Comparison System accepts no advertising and has no obligations to any commercial interests. ECRI
Institute and its employees accept no royalties, gifts, finder’s fees, or commissions from the medical device
industry, nor do they own stock in medical device companies. Employees engage in no private consulting work
for the medical device industry.
About ECRI Institute
ECRI Institute, a nonprofit organization, dedicates itself to bringing the discipline of applied scientific research
in healthcare to uncover the best approaches to improving patient care. As pioneers in this science for nearly 40
years, ECRI Institute marries experience and independence with the objectivity of evidence-based research.
More than 5,000 healthcare organizations worldwide rely on ECRI Institute’s expertise in patient safety
improvement, risk and quality management, healthcare processes, devices, procedures, and drug technology.
ECRI Institute is one of only a handful of organizations designated as both a Collaborating Center of the World
Health Organization and an Evidence-based Practice Center by the U.S. Agency for Healthcare Research and
Quality. For more information, visit http://www.ecri.org.
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 12/17
Amino Acid Analyzers
12 ©2007 ECRI Institute. All Rights Reserved.
Product Comparison Chart
MODEL ECRI INSTITUTE'SRECOMMENDEDSPECIFICATIONS1
BIOCHROM GBC SCIENTIFIC HITACHI
Amino Acid Analyzers Biochrom 30 Aminomate L-8800 A
WHERE MARKETED Worldwide Worldwide WorldwideFDA CLEARANCE Yes Yes NoCE MARK (MDD) Yes Yes YesPERFORMANCE
Type of reaction Postcolumn ninhydrin Precolumn FMOC Postcolumn NINAmino acids detected Primary, secondary Primary, secondary, imino Primary, secondary Depends on analysis, amino
sugars with special columnNo. of components Not specified 35+ Depends on analysisAnalysis time, min Sample dependent 30 20-150, varies
SAMPLE INJECTORModel Midas LC 1650 Built-inType (fixed or variableloop)
Variable Variable Variable
Manual or automatic Automatic, preferred Automatic Automatic AutomaticSample type Plasma, urine (preferred) Protein hydrolysate,
physiologic fluidsProtein, peptide,hydrolysates, feedhydrolysates, serum,plasma, IV fluids, beers,wines, juices
Protein hydrolysates,physiologic fluids
Sample volume, µL 1-5,000 1-200 0.1-100Sample capacity 84 160 200 1.5mL vialsVial size 100 µL, 200 µL; 2 mL 2 mL, 4 mL 1.5 mLAutoflushing Preferred User definable Optional Yes
DERIVATIZING REAGENT Ninhydrin FMOC NinhydrinOnline/manual Online (preferred) Online Online Online
COLUMNModel or variations Biochrom ODS-hypersoil Protein hydrolysate,
physiologic fluidsConstruction Rust-free material Polyetheretherketone
(PEEK), aluminumStainless steel Stainless steel
Length, cm/internaldiameter, mm
10-150/2-5 200/4.6, 100/4.6 15/4.6 Multiple available
Particle size, µm Uniform Not specified 5 3
Sorbent type Not specified Not specified Ion exchangeELUENT PUMP
Model Biochrom LC 1150 Built-inPump type Dual or single piston,
syringeDual piston Dual piston Dual piston
No. of pumps At least 1 2 1 2Flow range, mL/min 0.08-2.16 0-9.99 0.001-9.999Increment of flowsetting, mL/min
0.016 0.01 0.001
Flow precision, % 0.1 0.1 .075Flow accuracy, % 0.5 0.1 2Pressure limit, psi ≥2,000 2,160 6,000 5600Gradient (continuous ormultistep)
Multistep Continuous Selectable
No. of eluents 6 4 4
This is the first of two pagescovering the abovemodel(s). Thesespecifications continue ontothe next page.
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 13/17
Amino Acid Analyzers
©2007 ECRI Institute. All Rights Reserved 13
Product Comparison Chart
MODEL ECRI INSTITUTE'SRECOMMENDEDSPECIFICATIONS1
BIOCHROM GBC SCIENTIFIC HITACHI
Amino Acid Analyzers Biochrom 30 Aminomate L-8800 ADATA REDUCTION
Model LIS computer interface(optional)
Biosys EZChrom Elite EZChrom Elite
No. of channels 2 Multiple 2Display Monitor, printer Color monitor Color monitor Color monitorChromatograms, no.stored
Hard drive/networkdependent
80 GB hard drive, 4bytes/data point
Infinite with read, CD-RW
DETECTORModel Biochrom LC 1255s Built-inType Vis Fluorescence UV/Vis, optional
fluorescenceFilter/grating Filter Grating GratingReference wavelength,nm
NA Not specified 656.1
Available wavelengths,
nm
440-570 200-600, optional 900 440, 570 fixed
Light source Tungsten DC arc xenon DeuteriumDrift, AU/hr <0.001 Not specified <0.001Noise, AUFS <0.001 Not specified <0.001Cell volume, µL 8 12, optional 2 3.2Cell pathlength, mm 15 Not specified Not specifiedAvailable absorbancerange, AUFS
Not specified Not specified 0.001-2.2
Autozero Yes Yes YesOthers available Fluorescence UV/Vis, electrochemical,
conductivity, RI, PDAFluorescence
POWER REQUIREMENTS 115/220 V, 50/60 Hz 240, 220, 115 V, 50/60 Hz 115 V, 50/60 HzLIST PRICE $100,000 Not specified $76,000
YEAR FIRST SOLD 1969 1995 2005NUMBER OF UNITS SOLD >1,000 >400 Not specifiedFISCAL YEAR Not specified July to June April to March
OTHER SPECIFICATIONS None specified. IBM compatible; titaniumcorrosion-resistant path. Linear or step gradientsavailable; built-in automaticwash function; 3 pmoldetection using ninhydrin;postcolumn reaction columnminimizes peak diffusion;Windows 2000/XP operatingsystem.
LAST UPDATED October 2007 September 2006 September 2006Supplier Footnotes 1These recommendations
are the opinions of ECRIInstitute's technologyexperts. ECRI Instituteassumes no liability fordecisions made based onthis data.
Model Footnotes
Data Footnotes
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 14/17
Amino Acid Analyzers
14 ©2007 ECRI Institute. All Rights Reserved.
Product Comparison Chart
MODEL JASCO JEOL KNAUER WATERSOPA Amino Acid AnalysisSystem
AminoTac JLC-500/V Smartline Amino Acid Analyzer A0426 : A0515
MassTrak Amino Acid Analysis Solution
WHERE MARKETED Not specified Asia, Europe Worldwide WorldwideFDA CLEARANCE Not specified No Not specified Not specifiedCE MARK (MDD) Yes Yes Yes YesPERFORMANCE
Type of reaction Pre-/postcolumnderivatization
Ninhydrin Precolumn OPA or FMOC Precolumn AQC
Amino acids detected Primary and secondary Primary and secondary Primary (and secondarywith FMOC)
Primary and secondary
No. of components Not specified ≤46 ≤20 42Analysis time, min Not specified 30 (protein hydrolyzed) or
120 (physiologic fluid)30 32
SAMPLE INJECTORModel AS-2059 Built-in (JEOL) Spark Triathlon autosampler ACQUITY SMType (fixed or variableloop)
Selectable Variable Variable Variable
Manual or automatic Automatic Automatic Automatic Automatic
Sample type Protein hydrolysates,physiologic fluids
Protein hydrolysates, freeamino acids (plasma, urine)
Protein hydrolysates,feedstuffs, physiologicfluids, others
Urine and plasma
Sample volume, µL Variable mode standard 0.1-200 µL, optional 1-2,000 µL
1-200 35-10,000 0.5-1
Sample capacity 120, optional 224 96 96 96Vial size 2 mL, optional 0.6 and 0.3
mL180 µL, 1.6 mL 1.8, 4, 10 mL 0.9 mL
Autoflushing Yes Yes Yes YesDERIVATIZING REAGENT OPA/ninhydrin Ninhydrin OPA or FMOC Not specified
Online/manual Online Online Online ManualCOLUMN
Model or variations AA pack Na+ Cation exchanger Knauer column forprecolumn OPA or FMOC
Mass Trak AAA
Construction Stainless steel Stainless steel Stainless steel Stainless steelLength, cm/internaldiameter, mm
6/10 4/4, 3- or 4-segment 300/4 : 250/4.6 15/2.1
Particle size, µm 5 4 5 : 4 1.7Sorbent type Cation-exchanged resin Polymeric ion exchange ODS2 C18 : ODS2 C8 C-18
ELUENT PUMPModel PU-2089 Built-in (JEOL) Knauer Smartline 1000 ACQUITY BSMPump type Double-plunger/SSQD
methodFlow-sensor feedback,single piston
Dual piston, stainless steel 2 independently driven,software-controlled pistons
No. of pumps 1 2 1 2Flow range, mL/min 0.001-10 0.001-1 0.001-9.999 0.01-2Increment of flowsetting, mL/min
0.001 0.001 0.001 0.001
Flow precision, % ≤1 <1 0.1 0.15Flow accuracy, % 1% or 2 µL/min <1 0.5 1Pressure limit, psi 7,250 0.1 MPa/min 5,000 5,800 15,000Gradient (continuous ormultistep)
Continuous Multistep Continuous Continuous
No. of eluents 4 Up to 5 Up to 4 4
This is the first of two pagescovering the abovemodel(s). Thesespecifications continue ontothe next page.
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 15/17
Amino Acid Analyzers
©2007 ECRI Institute. All Rights Reserved 15
Product Comparison Chart
MODEL JASCO JEOL KNAUER WATERSOPA Amino Acid AnalysisSystem
AminoTac JLC-500/V Smartline Amino Acid Analyzer A0426 : A0515
MassTrak Amino Acid Analysis Solution
DATA REDUCTIONModel JASCO Borwin/HSS2000
workstationWindows 95 ChromGate or ClarityChrom
softwareEmpower 2
No. of channels 2 2 4 Not specifiedDisplay CRT Color monitor TFT monitor Color monitorChromatograms, no.stored
Not specified Depends on disk size Depends on disk size Not specified
DETECTORModel FP-2020 Built-in (JEOL) Shimadzu RF-10AXL ACQUITY TUVType Fluorescence Visible Fluorescence UV/visibleFilter/grating Grating Grating Not specified GratingReference wavelength,nm
Zero order, 220-900 690 330 Not specified
Available wavelengths,nm
Zero order, 220-700 440, 570 200-650 190-700
Light source 150 W xenon lamp Halogen Xenon Deuterium arc lamp
Drift, AU/hr Not specified Not specified Not specified <5.0 x 10-4Noise, AUFS SNR >350 for Raman peak
of waterNot specified Not specified 6 x 10-6 AU
Cell volume, µL 16 2 12 0.5Cell pathlength, mm Not specified 3 Not specified 10Available absorbancerange, AUFS
Not specified 0.0001-2 Not specified 0.00001-4
Autozero Yes Yes Yes YesOthers available None specified Fluorescence detector Knauer Smartline PDA
Detector 2800None specified
POWER REQUIREMENTS 100-240 V 100-230 V, 50/60 Hz 90-260 V, 50/60 Hz Not specifiedLIST PRICE Not specified Not specified $55,000 : $60,000 $95,000
YEAR FIRST SOLD Not specified 1985 1987 2008NUMBER OF UNITS SOLD Not specified 195 Not specified Not specifiedFISCAL YEAR September to August April to March Not specified January to DecemberOTHER SPECIFICATIONS None specified. Fully automated walkaway
system; 10 customer-madeanalysis methods; safetyaids; measure of amino acidresidue. Meetsrequirements of GLP.
For precolumn
derivatization; automatedreagent preparation withTriathlon autosampler.Meets requirements of GLPand TUV.
Includes standards,
reagents, vials, column, andmobile phases with pre-defined analysis andreporting methods;documentation installation,training and support arealso provided.
LAST UPDATED October 2007 October 2007 October 2007 October 2007Supplier Footnotes
Model Footnotes
Data Footnotes
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 16/17
Amino Acid Analyzers
16 ©2007 ECRI Institute. All Rights Reserved.
Product Comparison Chart
MODEL WATERSUPLC Amino Acid AnalysisSolution
WHERE MARKETED WorldwideFDA CLEARANCE Not specifiedCE MARK (MDD) YesPERFORMANCE
Type of reaction Precolumn AQCAmino acids detected Primary and secondaryNo. of components 32Analysis time, min 8.5
SAMPLE INJECTORModel ACQUITY SMType (fixed or variableloop)
Variable
Manual or automatic AutomaticSample type Protein hydrolysates, culture
media, fermentation broth,feed/food hydrolysates
Sample volume, µL 0.5-1Sample capacity 96Vial size 0.9 mLAutoflushing Yes
DERIVATIZING REAGENT AccQ-FluorOnline/manual Manual
COLUMNModel or variations AccQ-Tag UltraConstruction Stainless steelLength, cm/internaldiameter, mm
10/2.1
Particle size, µm 1.7Sorbent type C-18
ELUENT PUMPModel ACQUITY BSMPump type 2 independently driven,
software-controlled pistonsNo. of pumps 2Flow range, mL/min 0.01-2Increment of flowsetting, mL/min
0.001
Flow precision, % 0.15Flow accuracy, % 1Pressure limit, psi 15,000Gradient (continuous ormultistep)
Continuous
No. of eluents 4
This is the first of two pagescovering the abovemodel(s). These
specifications continue ontothe next page.
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M

8/9/2019 Amino Acid Analyzers
http://slidepdf.com/reader/full/amino-acid-analyzers 17/17
Amino Acid Analyzers
©2007 ECRI Institute All Rights Reserved 17
Product Comparison Chart
MODEL WATERSUPLC Amino Acid AnalysisSolution
DATA REDUCTIONModel Empower 2No. of channels Not specifiedDisplay Color monitorChromatograms, no.stored
Not specified
DETECTORModel ACQUITY TUVType UV/visibleFilter/grating GratingReference wavelength,nm
Not specified
Available wavelengths,nm
190-700
Light source Deuterium arc lampDrift, AU/hr <5.0 x 10-4
Noise, AUFS 6 x 10-6 AUCell volume, µL 0.5Cell pathlength, mm 10Available absorbancerange, AUFS
0.00001-4
Autozero YesOthers available Photodiode and
fluorescencePOWER REQUIREMENTS Not specifiedLIST PRICE $79,500
YEAR FIRST SOLD 2006NUMBER OF UNITS SOLD Not specifiedFISCAL YEAR January to DecemberOTHER SPECIFICATIONS Includes comprehensive
chemistry package, methoddocumentation, installation
and training. Specificallytested for AAA analysis.Validation, compliance, andquality programs available.
LAST UPDATED October 2007Supplier Footnotes
Model Footnotes
Data Footnotes
Comprehensive of Biomedical Engineering Site (www.dezmed.com
W
W W . D
E Z M E D
. C O M
Related Documents