Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Amidst the Opioid Crisis:
Best Practices for
SMVF Resilience, Treatment, and Recovery
Donna Aligata, R.N.C. | SAMHSA’s Service Members, Veterans, and their Families
Technical Assistance Center, Policy Research Associates, Inc.
Kimberly A. Johnson, Ph.D. |Center for Substance Abuse Treatment, SAMHSA
Karen Drexler, M.D. | U.S. Department of Veterans Affairs
Michael Flaherty, Ph.D. | Clinical Psychologist
February 22, 2017
Disclaimer: The views, opinions, and content expressed in this
presentation do not necessarily reflect the views, opinions, or policies
of the Center for Mental Health Services (CMHS), the Substance
Abuse and Mental Health Services Administration (SAMHSA), or the
U.S. Department of Health and Human Services (HHS).
3

Welcome
Donna Aligata, R.N.C.
Project Director
Substance Abuse and Mental Health Services Administration (SAMHSA)
Service Members, Veterans, and their Families (SMVF)
Technical Assistance Center
Policy Research Associates, Inc.
4
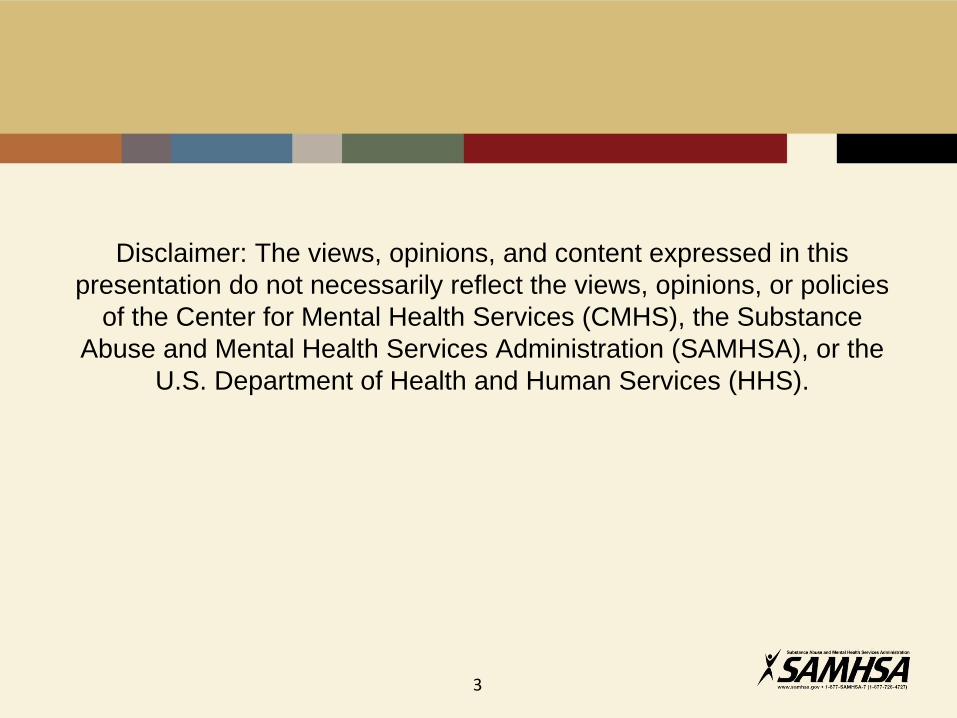
SMVF TA Center – Policy Academy States49 States, 4 territories, and the District of Columbia
5

SAMHSA’s SMVF TA Center
• Facilitates military and civilian interagency strategic planning
• Strengthens the coordination of military and civilian behavioral
health systems serving SMVF
• Implements SMVF best practices
• Builds workforce capacity
6
Webinar Objectives
• Explain the characteristics and risk factors among SMVF for opioid
misuse and addiction, including chronic pain, post-traumatic stress
disorder, and other co-occurring conditions
• Describe SAMHSA’s new and emerging national initiatives designed
to help states and communities better address the opioid crisis
among SMVF
• Identify the steps the VA has taken to address the opioid crisis
• Discover solutions for integrating military culture and recovery-
oriented approaches with medication-assisted treatment and
recovery
• Implement prevention strategies to reduce opioid-related SMVF
deaths
7

Kimberly A. Johnson, Ph.D.
Director
Center for Substance Abuse Treatment (CSAT)
SAMHSA
8
SMVF and Opioids:
Public Health Solutions
SMVF and SUDs:
The Surgeon General’s Report
https://addiction.surgeongeneral.gov/
9

Snapshot of Opioid Use/
Opioid Use Disorders in the U.S.
10
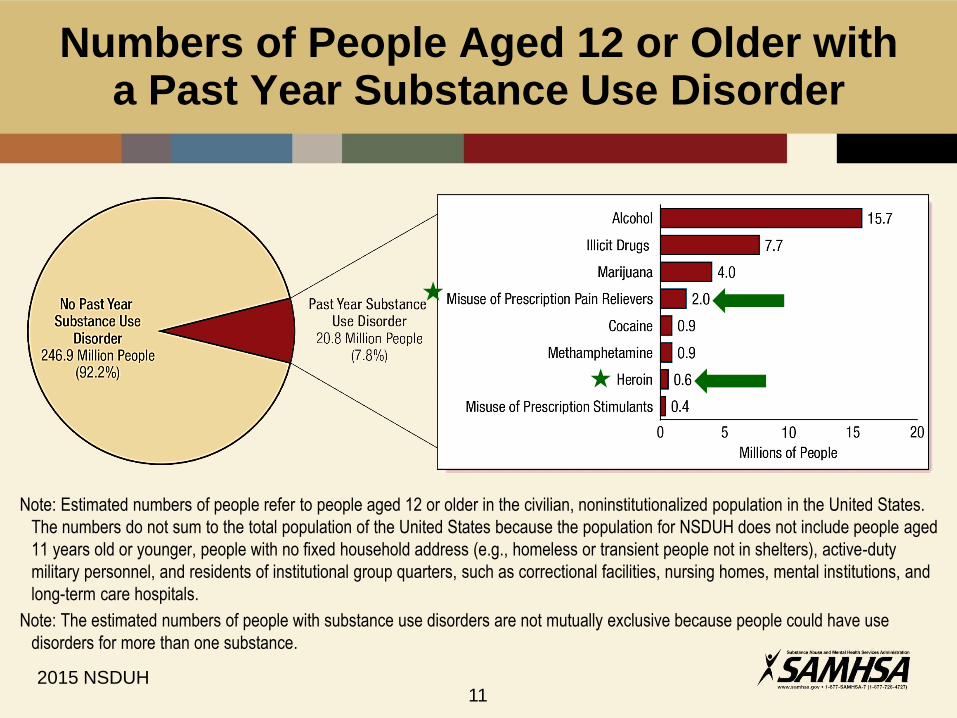
Numbers of People Aged 12 or Older with a Past Year Substance Use Disorder
Note: Estimated numbers of people refer to people aged 12 or older in the civilian, noninstitutionalized population in the United States.
The numbers do not sum to the total population of the United States because the population for NSDUH does not include people aged
11 years old or younger, people with no fixed household address (e.g., homeless or transient people not in shelters), active-duty
military personnel, and residents of institutional group quarters, such as correctional facilities, nursing homes, mental institutions, and
long-term care hospitals.
Note: The estimated numbers of people with substance use disorders are not mutually exclusive because people could have use
disorders for more than one substance.
2015 NSDUH11

Trends in Pain Reliever Use and Disorders in
People Aged 12 and Older
PAIN RELIEVER USE DISORDER
IN THE PAST YEAR PAST MONTH NONMEDICAL USE
OF PAIN RELIEVERS
(+): Difference between this estimate and the 2014 estimate is statistically significant at the .05
level.
NSDUH 2014 data 12
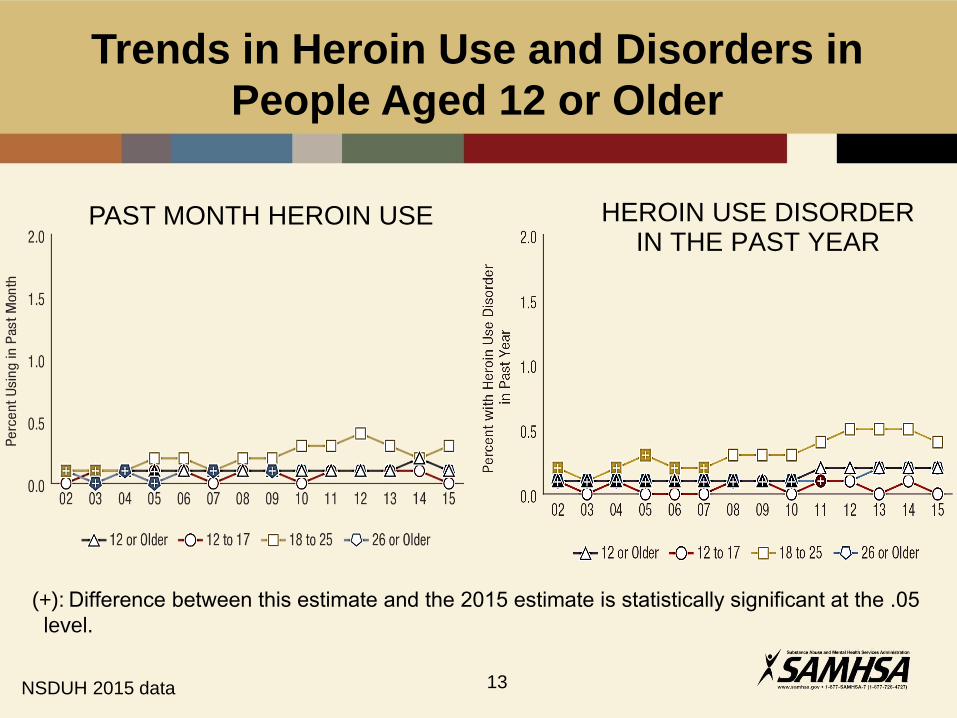
HEROIN USE DISORDER IN THE PAST YEAR
(+): Difference between this estimate and the 2015 estimate is statistically significant at the .05
level.
Trends in Heroin Use and Disorders in
People Aged 12 or Older
PAST MONTH HEROIN USE
NSDUH 2015 data 13
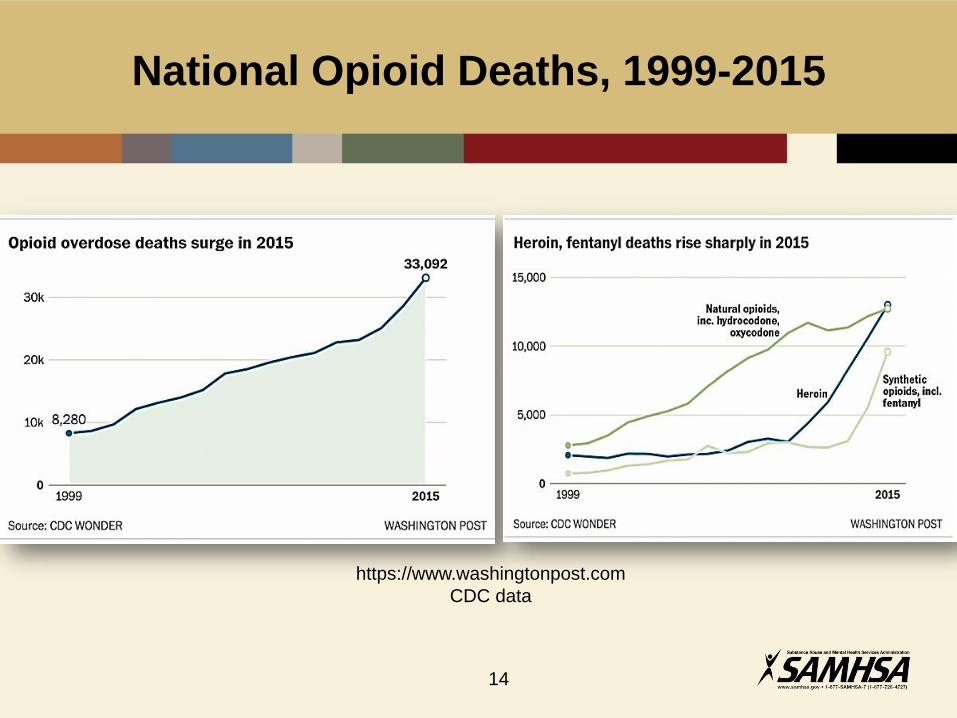
National Opioid Deaths, 1999-2015
https://www.washingtonpost.com
CDC data
14
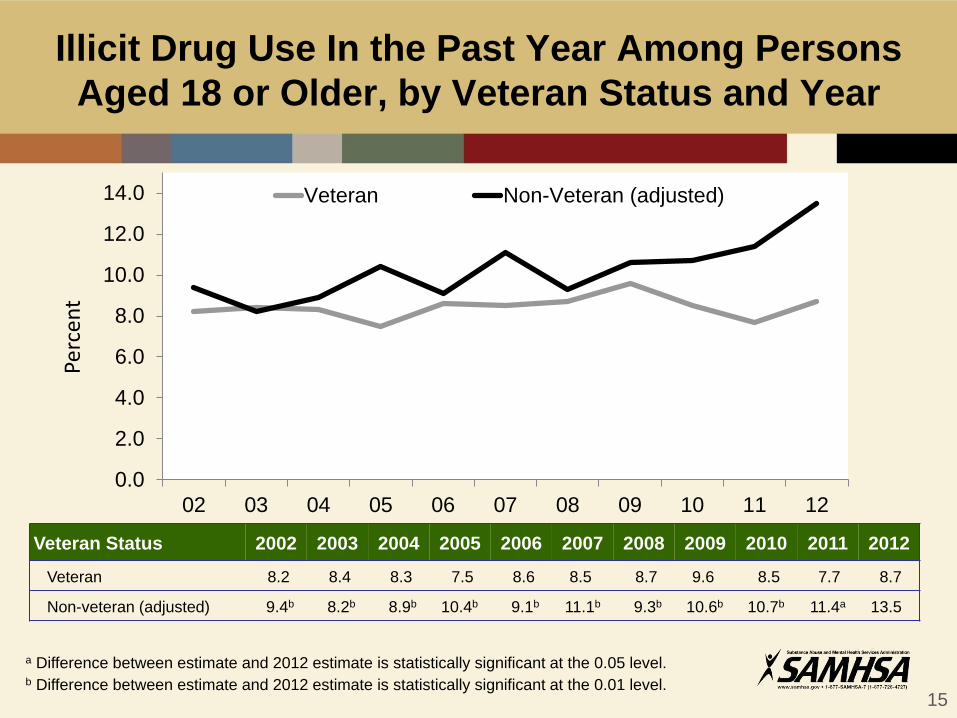
Illicit Drug Use In the Past Year Among Persons
Aged 18 or Older, by Veteran Status and Year
Veteran Status 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Veteran 8.2 8.4 8.3 7.5 8.6 8.5 8.7 9.6 8.5 7.7 8.7
Non-veteran (adjusted) 9.4b 8.2b 8.9b 10.4b 9.1b 11.1b 9.3b 10.6b 10.7b 11.4a 13.5
a Difference between estimate and 2012 estimate is statistically significant at the 0.05 level.b Difference between estimate and 2012 estimate is statistically significant at the 0.01 level.
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
02 03 04 05 06 07 08 09 10 11 12
Veteran Non-Veteran (adjusted)
Perc
ent
15
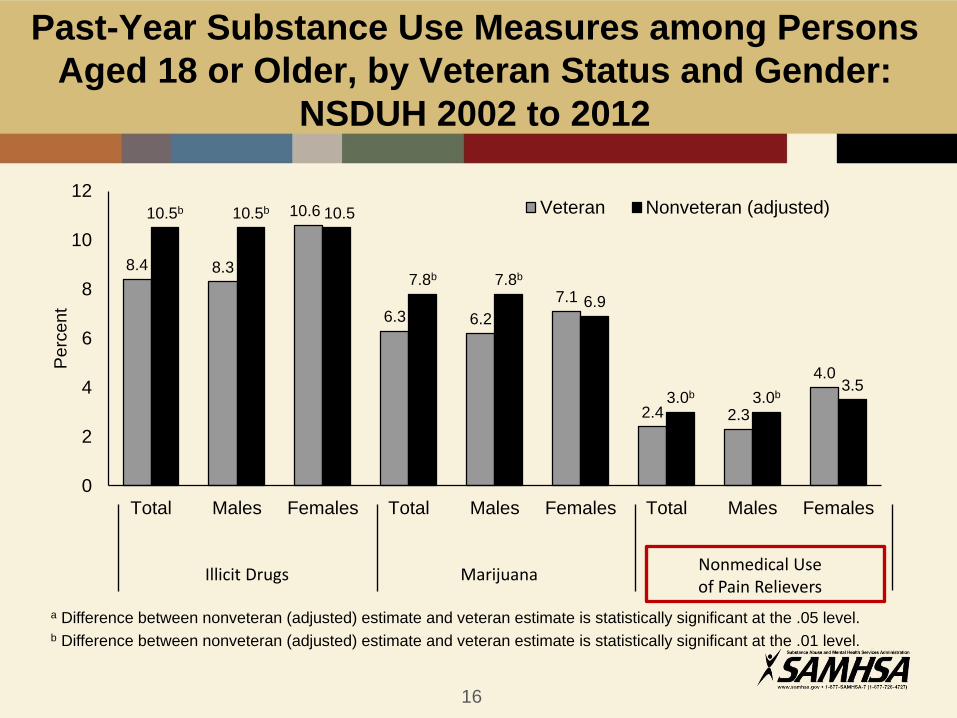
Past-Year Substance Use Measures among Persons
Aged 18 or Older, by Veteran Status and Gender:
NSDUH 2002 to 2012
16
a Difference between nonveteran (adjusted) estimate and veteran estimate is statistically significant at the .05 level.b Difference between nonveteran (adjusted) estimate and veteran estimate is statistically significant at the .01 level.
8.4 8.3
10.6
6.3 6.2
7.1
2.4 2.3
4.0
10.5b 10.5b 10.5
7.8b 7.8b
6.9
3.0b 3.0b3.5
0
2
4
6
8
10
12
Total Males Females Total Males Females Total Males Females
Perc
ent
Veteran Nonveteran (adjusted)
Illicit Drugs Marijuana Nonmedical Use of Pain Relievers
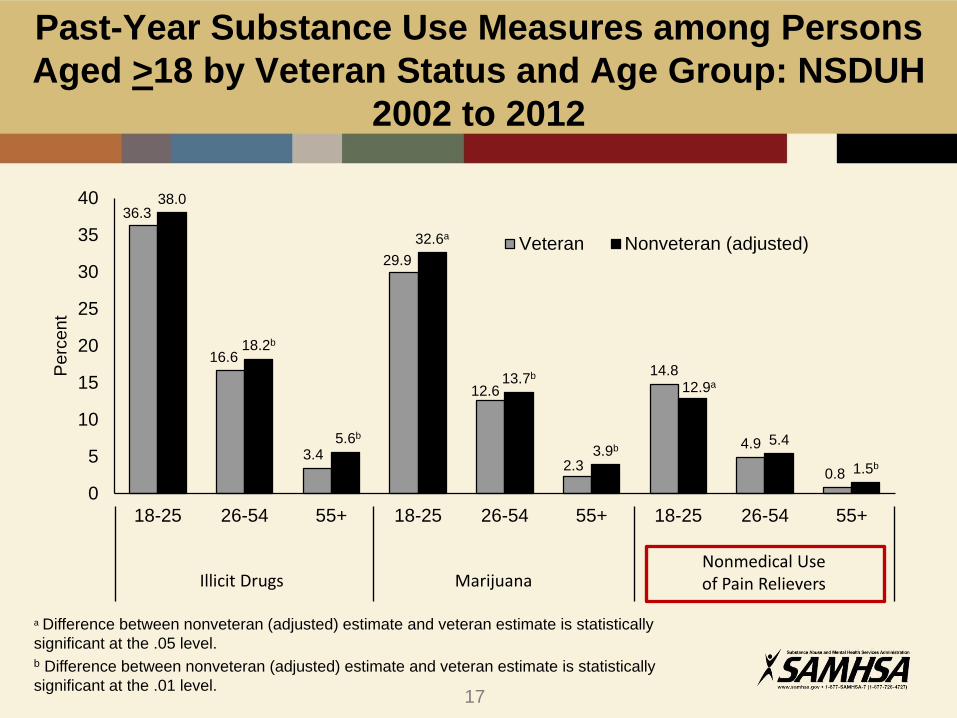
Past-Year Substance Use Measures among Persons
Aged >18 by Veteran Status and Age Group: NSDUH
2002 to 2012
36.3
16.6
3.4
29.9
12.6
2.3
14.8
4.9
0.8
38.0
18.2b
5.6b
32.6a
13.7b
3.9b
12.9a
5.4
1.5b
0
5
10
15
20
25
30
35
40
18-25 26-54 55+ 18-25 26-54 55+ 18-25 26-54 55+
Perc
ent
Veteran Nonveteran (adjusted)
a Difference between nonveteran (adjusted) estimate and veteran estimate is statistically
significant at the .05 level.b Difference between nonveteran (adjusted) estimate and veteran estimate is statistically
significant at the .01 level.
Illicit Drugs Marijuana Nonmedical Use of Pain Relievers
17
• 32 percent of individuals with chronic
pain (CP) estimated to have SUDs
• 29-60 percent of people with OUD report
CP
• CP and addiction are dynamic conditions
that can fluctuate in intensity over time
• Both require multimodal interventions,
and treatment for one may impede or
conflict with treatment for the other
• Both have serious consequences if left
untreated
Chronic Pain and SUDs
18
SMVF and Opioids
• Trauma, pain, depression, and other risk factors associated
with opioid use disorders (OUDs) are often experienced at
elevated levels by SMVF
• Data indicate that over 50 percent of VA patients seen in
primary care settings report chronic pain
• Prescription drug misuse among service members and
veterans has more than doubled since 2002
• In veterans aged 18–25 the risk for prescription drug misuse
is at an all time high
• Opioid use in the military is twice that of use in the general
population
19
SMVF, Opioids, and Overdose Risk
• Veterans are twice as likely to die from accidental overdose
compared to the non-veteran population
• Assessment of risk factors is important in our veteran
population especially in returning combat veterans
• Often they present to primary care seeking relief from both
physical and psychological pain
• Psychological distress may lead to inappropriate use of opioid
medications in patients with mental health disorders. Caution
should be used in this high risk population
https://www.va.gov/PAINMANAGEMENT/docs/OSI_1_Toolkit_Pain_Educational_Guide.pdf
20
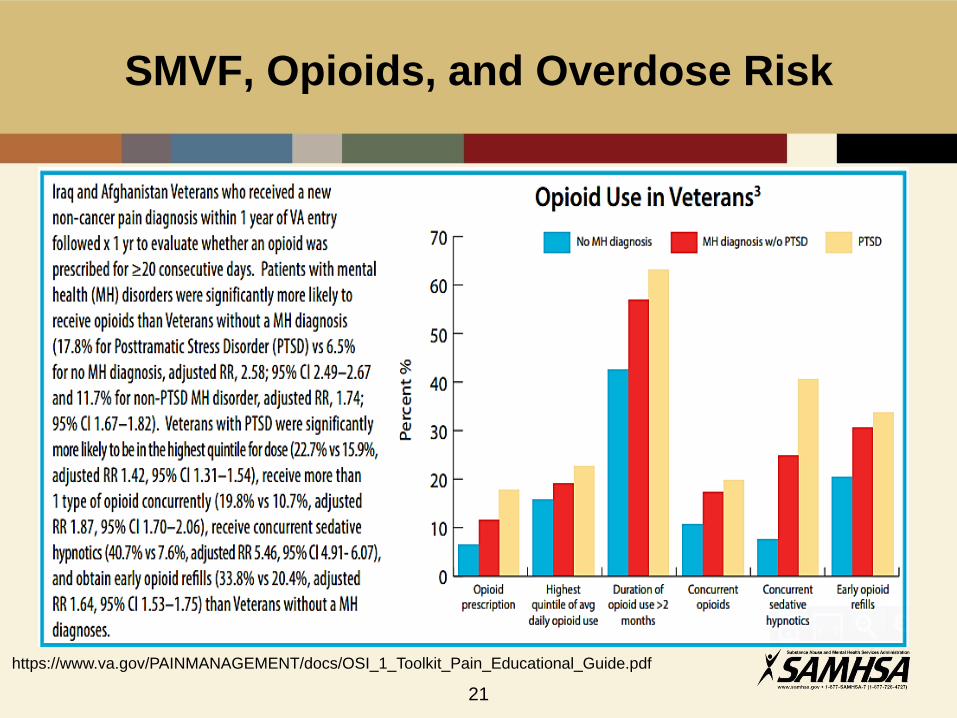
SMVF, Opioids, and Overdose Risk
https://www.va.gov/PAINMANAGEMENT/docs/OSI_1_Toolkit_Pain_Educational_Guide.pdf
21

• Approximately 20 veterans per day die of suicide
• Alcohol and drug misuse are often contributing
factors
• Highest risk age group is 30-64 years of age
• Higher prevalence in men than women
• Higher rate of women veterans than women in
general population
Addiction and Suicide
22

Past Year Illicit Drug Use among Wives of Military Personnel and All Married Women (18-49):
Percentages, 2015 NSDUH
23
+Difference between this estimate and the estimate for All Married Women Aged 18
to 49 is statistically significant at the .05 level.
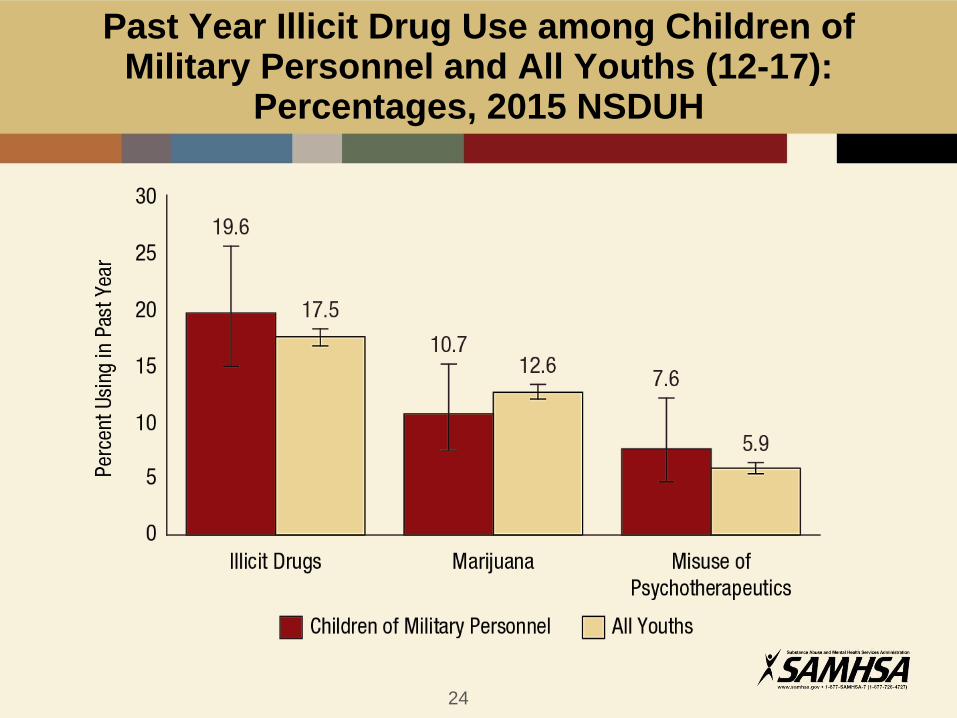
Past Year Illicit Drug Use among Children of Military Personnel and All Youths (12-17):
Percentages, 2015 NSDUH
24
SMVF and Opioids: SAMHSA’S Public Health Approach
25
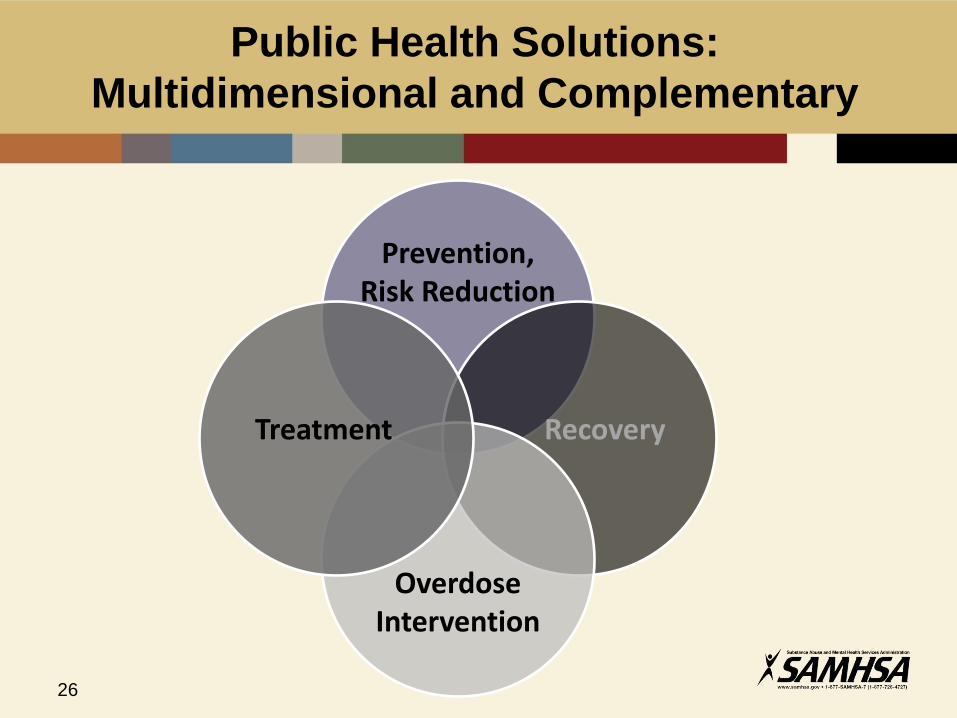
Public Health Solutions:
Multidimensional and Complementary
Prevention, Risk Reduction
Treatment Recovery
Overdose Intervention
26

Select SAMHSA Initiatives that Serve
SMVF and their Communities
• Block Grants
• Discretionary Grants
• Technology Transfer &
Technical Assistance
• Workforce Development
• Health Information
Technology
27

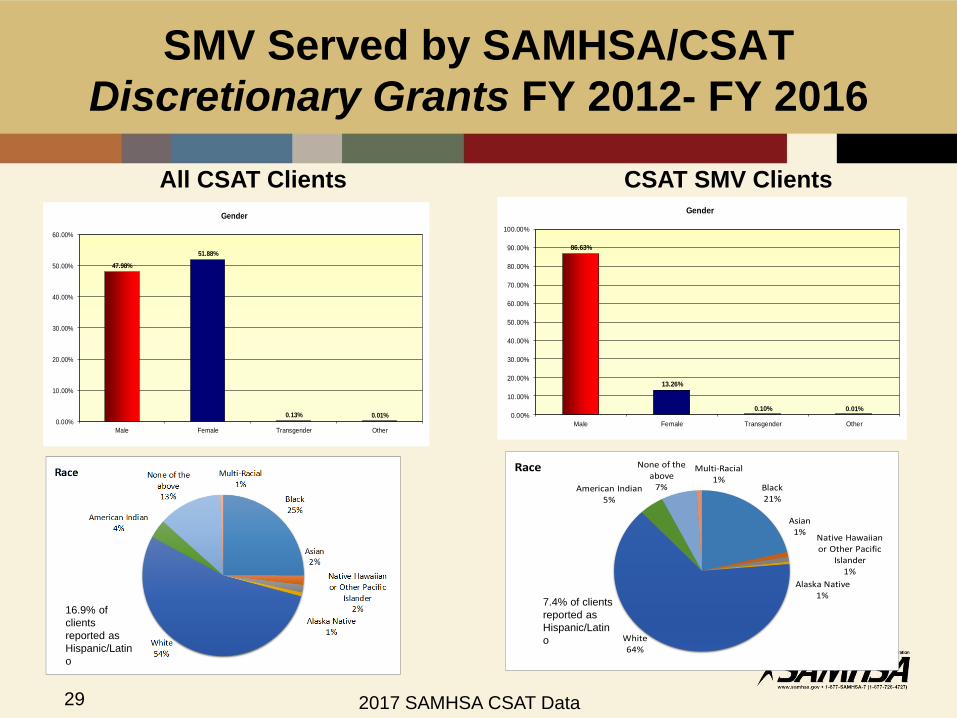
SMV Served by SAMHSA/CSAT
Discretionary Grants FY 2012- FY 2016
All CSAT SAIS Grantees
Number Military
Number Currently on Active Duty
Number Ever
Deployed to Combat
Zone
Number ofClients Served
1,678,044 62,023 17,127 21,008
2017 SAMHSA CSAT Data
28
SMV Served by SAMHSA/CSAT
Discretionary Grants FY 2012- FY 2016
47.98%
51.88%
0.13% 0.01%0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
Male Female Transgender Other
Gender
All CSAT Clients CSAT SMV Clients
Black21%
Asian1%
Native Hawaiian or Other Pacific
Islander1%
Alaska Native1%
White64%
American Indian5%
None of the above
7%
Multi-Racial1%
Race
16.9% of
clients
reported as
Hispanic/Latin
o
7.4% of clients
reported as
Hispanic/Latin
o
86.63%
13.26%
0.10% 0.01%0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Male Female Transgender Other
Gender
2017 SAMHSA CSAT Data29
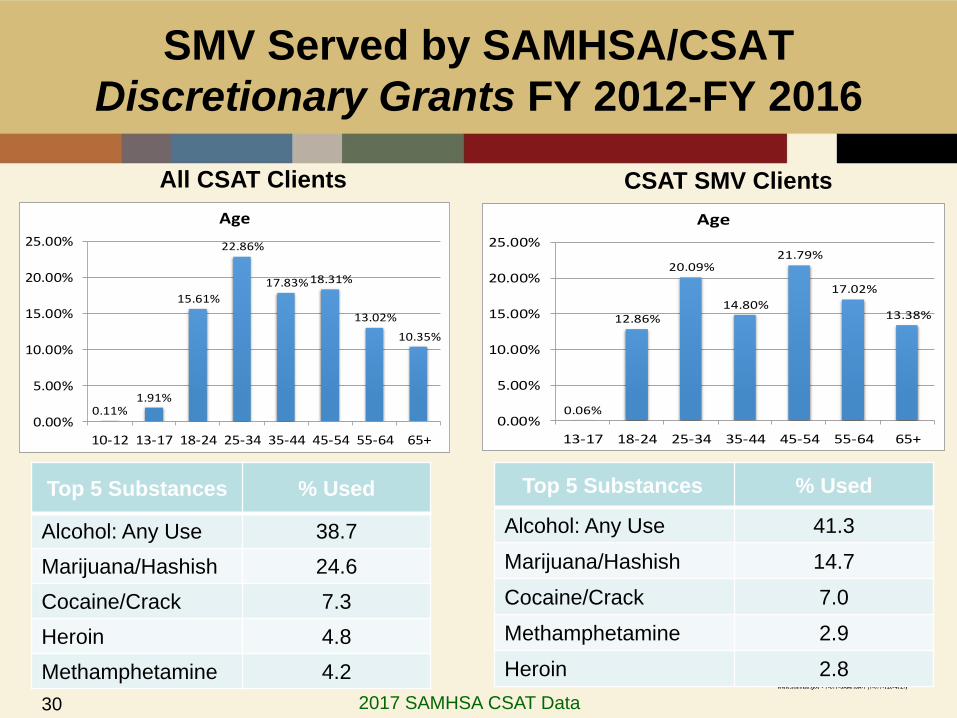
SMV Served by SAMHSA/CSAT
Discretionary Grants FY 2012-FY 2016
All CSAT Clients CSAT SMV Clients
Top 5 Substances % Used
Alcohol: Any Use 38.7
Marijuana/Hashish 24.6
Cocaine/Crack 7.3
Heroin 4.8
Methamphetamine 4.2
0.11%1.91%
15.61%
22.86%
17.83%18.31%
13.02%
10.35%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
10-12 13-17 18-24 25-34 35-44 45-54 55-64 65+
Age
0.06%
12.86%
20.09%
14.80%
21.79%
17.02%
13.38%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
13-17 18-24 25-34 35-44 45-54 55-64 65+
Age
Top 5 Substances % Used
Alcohol: Any Use 41.3
Marijuana/Hashish 14.7
Cocaine/Crack 7.0
Methamphetamine 2.9
Heroin 2.8
2017 SAMHSA CSAT Data30
SAMHSA Serves SMVF:
Veterans Helping Veterans
The primary goal of the Jobs2Vets program is to help
homeless veterans with substance use disorders and
co-occurring disorders achieve and maintain
employment, while preventing relapse and promoting
improvement in overall mental health functioning.
Jobs2Vets is a collaborative effort between MTI IBD,
SAMHSA, VANJ, and the Rutgers-Bloustein Center
for Survey Research.
The Jobs2Vets peer mentorship and recovery
support model is increasing employment
opportunities, promoting workforce development, and
helping Veterans break the cycle of mental illness,
substance misuse and chronic homelessness.
31
SAMHSA Serves SMVF:
Veterans Helping Veterans
32

SAMHSA Serves SMVF VIA Technology Transfer
and Technical Assistance
33

SAMHSA Serves SMVF Through Workforce
Development
34
SAMHSA Serves SMVF Through Workforce
Development
35
SAMHSA Serves SMVF Through HIT
36
SAMHSA Serves SMVF Through HIT
37
SAMHSA’S Commitment
Serving America’s SMVF and
their communities through
leadership, partnership, &
funding to ensure that high
quality, trauma-informed,
culturally appropriate health
care and related services are
readily accessible, affordable,
and effective.
https://www.samhsa.gov/veterans-military-families38
Karen Drexler, M.D.
National Mental Health Program Director, Substance Use Disorders
U.S. Department of Veterans Affairs
40
VA Response to the Opioid Crisis
Karen Drexler, M.D.
National Program Director- Substance Use Disorders
Department of Veterans Affairs
February 22, 201741
VA’s Mission
42
“To care for him who shall have borne the battle and for his widow, and his orphan.”
- Abraham Lincoln, 1865
The Pain Challenge in VHA
43
In Veterans, chronic pain is common.
– Veterans: more than 50% of older Veterans experience chronic pain
• 60% of Veterans from Middle East conflicts
• Up to 75% of female Veterans have chronic pain
– More than 2 Mil Veterans with ≥ one pain diagnosis in VA (2012, 1/3 on opioids)
– National Health Interview Survey (NHIS) (2016)
66% of Veterans vs. 56% of non-veterans with pain in prior 3 month
joint pain (43.6%), back pain (32.8% - axial 20.5%, sciatica 12.2%), neck pain (15.9%), migraine (10.0%) and jaw pain (3.6%)
In Veterans, chronic pain is often severe and complex
– Posttraumatic Stress Disorder (PTSD) and Opioid Use Disorder (OUD)
NHIS: interview of 67,696 US adults in 2010-14. Nahin RL, J. Pain 2016
Substance Use Disorder (SUD): Prevalence
• Veterans receiving VA health care in FY 2015
• 560,922, or 9.7%, were diagnosed with a SUD*
* Compares to 8.4% of U.S. adults
44
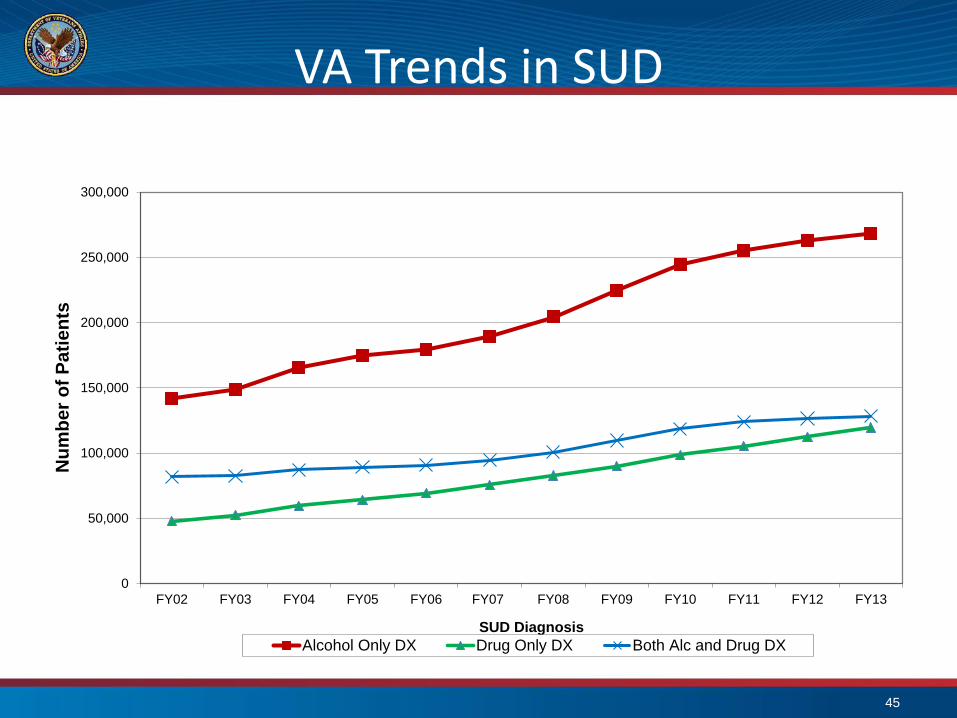
VA Trends in SUD
45
0
50,000
100,000
150,000
200,000
250,000
300,000
FY02 FY03 FY04 FY05 FY06 FY07 FY08 FY09 FY10 FY11 FY12 FY13
Nu
mb
er
of
Pati
en
ts
SUD Diagnosis
Alcohol Only DX Drug Only DX Both Alc and Drug DX
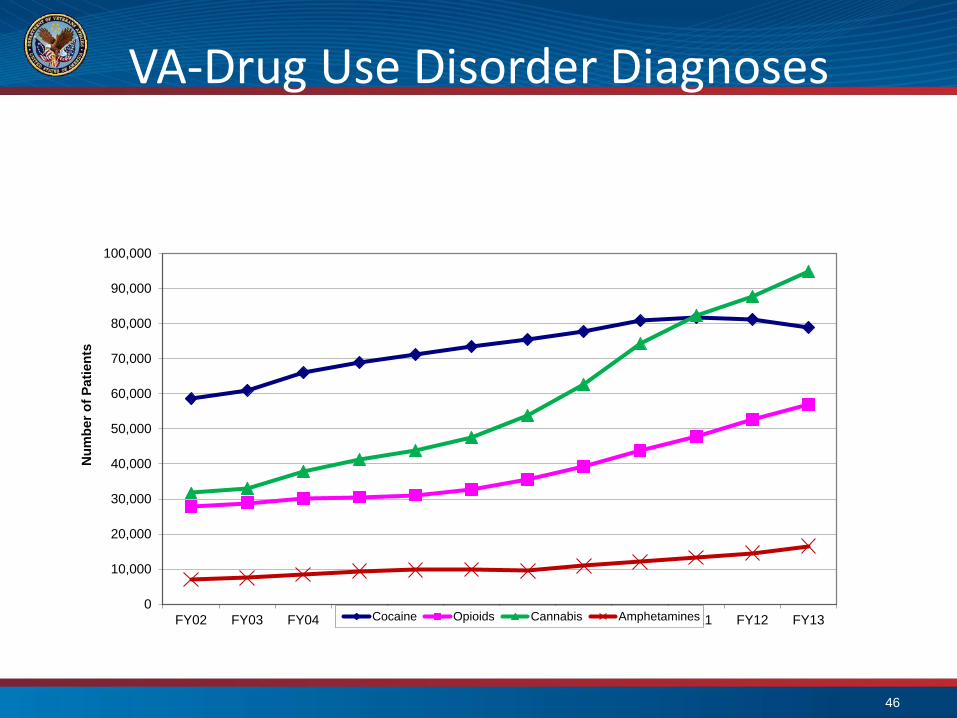
VA-Drug Use Disorder Diagnoses
46
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
80,000
90,000
100,000
FY02 FY03 FY04 FY05 FY06 FY07 FY08 FY09 FY10 FY11 FY12 FY13
Nu
mb
er
of
Pa
tie
nts
Cocaine Opioids Cannabis Amphetamines
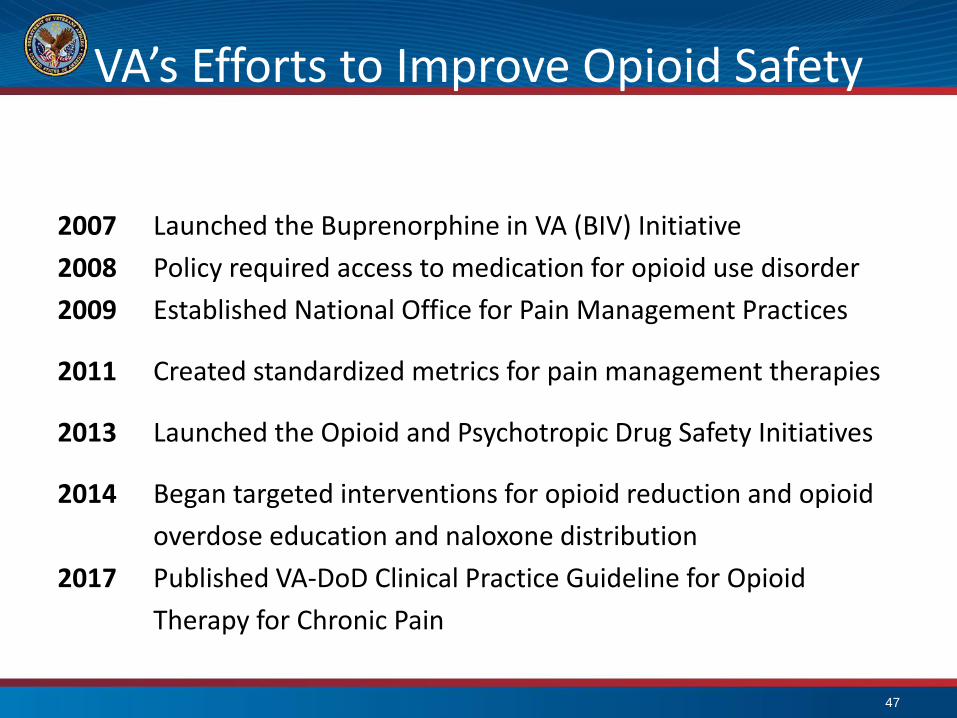
VA’s Efforts to Improve Opioid Safety
2007 Launched the Buprenorphine in VA (BIV) Initiative
2008 Policy required access to medication for opioid use disorder
2009 Established National Office for Pain Management Practices
2011 Created standardized metrics for pain management therapies
2013 Launched the Opioid and Psychotropic Drug Safety Initiatives
2014 Began targeted interventions for opioid reduction and opioid
overdose education and naloxone distribution
2017 Published VA-DoD Clinical Practice Guideline for Opioid
Therapy for Chronic Pain
47
Impact of Efforts: 2012-2016
• 170,000 fewer Veterans were prescribed opioids (25% reduction)
• 51,000 fewer (42% reduction) concomitant use of opioids and benzodiazepines
• 19,000 less (32% reduction) in dosage of those on chronic opioids
48
Approaches to Opioid Use and SUD
49
• Guidelines and best practice implementation
• Stepped pain care
• VA/DoD guidelines
• Informatics tools: leveraging big data
• Stratification Tool for Opioid Risk Mitigation (predictive analytics for opioid misuse)
• Opioid Safety Initiative dashboard
• Psychotropic Drug Safety Initiative
• Pain management, complementary care, and National Formulary
• Pharmacologic and non-pharmacologic therapies
• National Formulary includes all recommended medications
• Provider and patient education
• National community of practice (i.e., consultation, webinars, e-mail groups)
• Buprenorphine in VA initiative
• Mini-residencies in pain management
• Academic Detailing using 285pharmacists
• Medication Take Back Program
• Informed consent process for patients
50
Evidence Hierarchy
51
Meta-analyses of RCTs
Randomized Controlled Trials
Observational Studies
Non-Analytical Studies
Expert Opinion

VA-DoD SUD Guideline Key Recommendations
52
• Screening and brief alcohol intervention
• Treatment (pharmacotherapy and psychosocial interventions)
• Alcohol use disorder
• Opioid use disorder
• Cannabis use disorder
• Stimulant use disorder
• Promoting group mutual help (e.g. AA, NA, Smart Recovery)
• Address co-occurring mental health conditions and psychosocial problems
• Continuing care guided by ongoing assessment
• Stabilization and withdrawal
SUD Medications Psychosocial Intervention
Alcohol AcamprosateDisulfiramNaltrexoneTopiramateGabapentin*
Behavioral Couples TherapyCognitive Behavioral therapy (CBT)Community Reinforcement Approach (CRA)Motivation Enhancement Therapy (MET)Twelve Step Facilitation
Opioid BuprenorphineMethadoneER-InjectableNaltrexone*
Medical Management**Contingency Management (CM)/Individual Drug Counseling (IDC)**
Cannabis CBT/MET
Stimulant CBT/CRA/IDC +/- CM
http://www.healthquality.va.gov/guidelines/MH/sud/
*suggested **recommended only with medication
Patient-Centered Care and Shared Decision Making
53
• Patient is the expert on his/her life and experience
• Elicit preferences and goals
• Clinicians are experts on risks-benefits of the full menu of treatment options
• Provide easily understandable information for patient to make an informed decision
• Collaborate to develop treatment goals/objectives/interventions
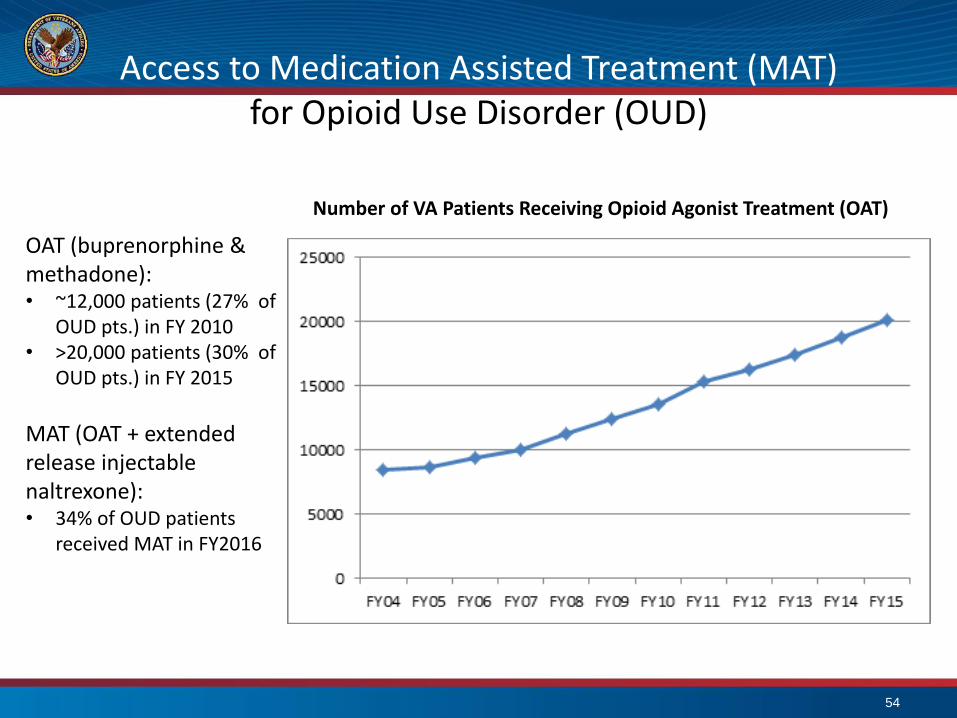
Access to Medication Assisted Treatment (MAT)for Opioid Use Disorder (OUD)
54
OAT (buprenorphine & methadone):• ~12,000 patients (27% of
OUD pts.) in FY 2010 • >20,000 patients (30% of
OUD pts.) in FY 2015
MAT (OAT + extended release injectable naltrexone):• 34% of OUD patients
received MAT in FY2016
Number of VA Patients Receiving Opioid Agonist Treatment (OAT)
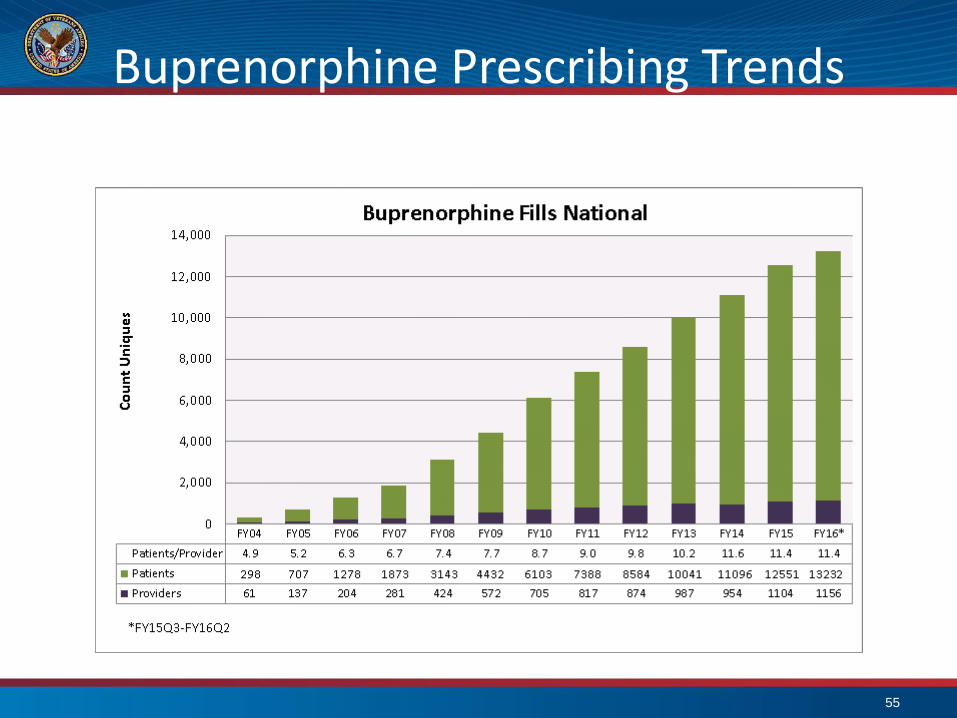
Buprenorphine Prescribing Trends
55
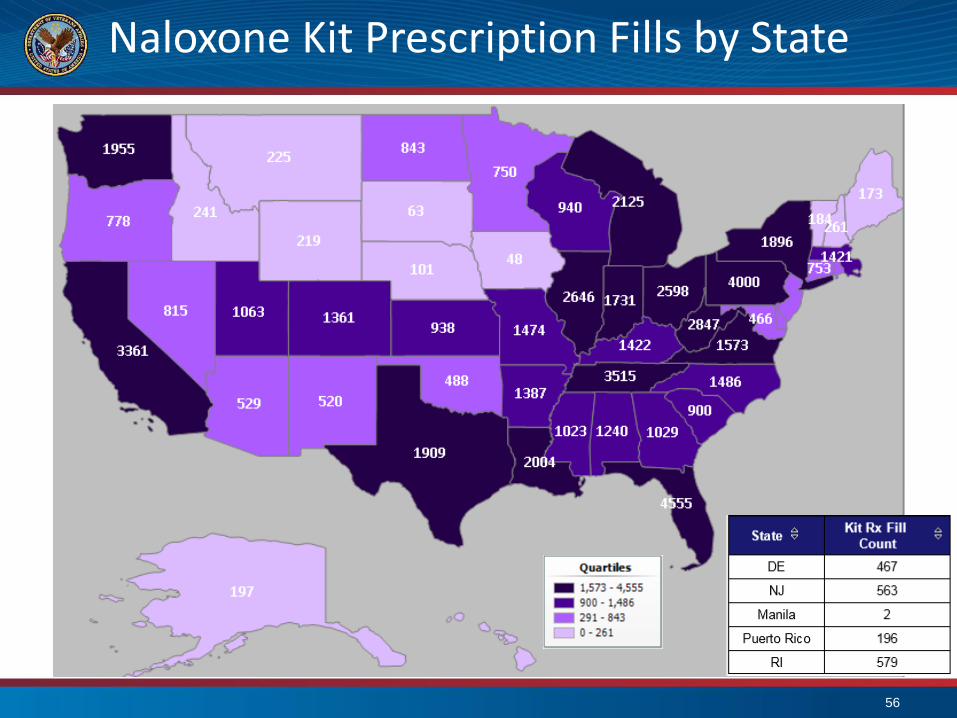
Naloxone Kit Prescription Fills by State
56
Veterans Health Administration
• The nation’s largest integrated healthcare system
– Serving over 8.76 million Veterans
– Over 1700 sites of care
• Basic Medical Benefits Package includes:
– Preventive Care
– Hospital (Inpatient) Services
– Ancillary Services
– Mental Health
– Home Health Care
– Geriatrics and Extended Care
– Medical Equipment
57
https://www.va.gov/healthbenefits
/
Mental Health Services
• Outpatient care including counseling, medication and care coordination:
• Brief counseling & medication in Primary Care
• General Mental Health Clinics (including telehealth)
• Specialty Mental Health Clinics (e.g. PTSD, Substance Use Disorder-SUD)
• Intensive outpatient care (e.g. Intensive Outpatient SUD care);
• Residential Treatment Programs- Domiciliaries
• Short-term inpatient (hospital) care
• Supported work settings.
58
http://www.mentalhealth.va.gov/VAMentalHealthGroup.asp

Apply for Health BenefitsOnline or by phone at 855-574-7286
59
https://www.vets.gov/
60
AboutFace
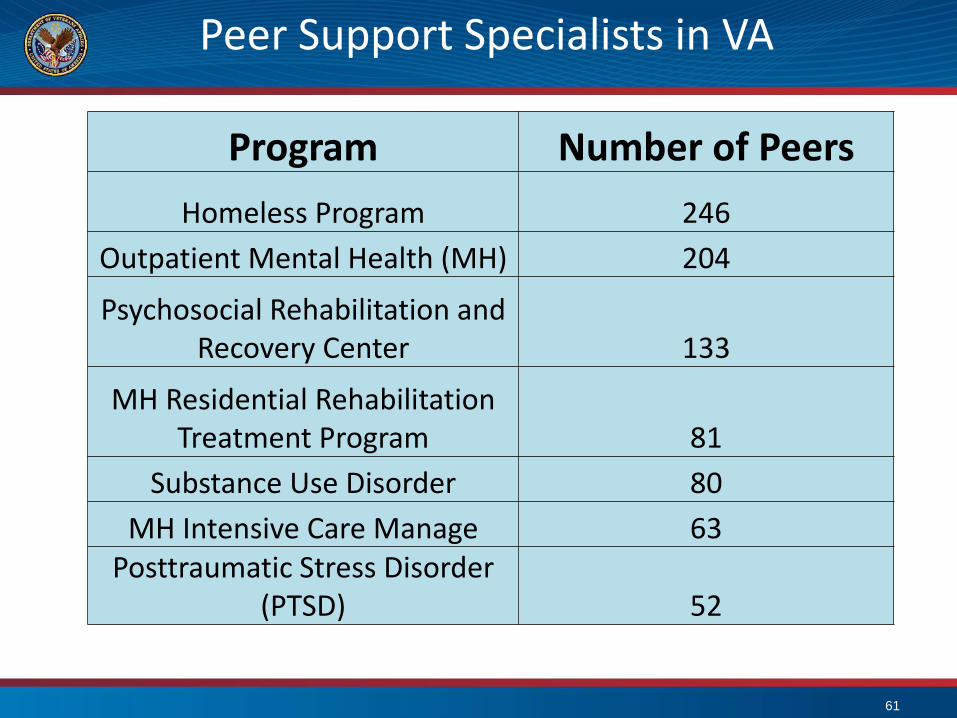
Peer Support Specialists in VA
Program Number of Peers
Homeless Program 246
Outpatient Mental Health (MH) 204
Psychosocial Rehabilitation and Recovery Center 133
MH Residential Rehabilitation Treatment Program 81
Substance Use Disorder 80
MH Intensive Care Manage 63Posttraumatic Stress Disorder
(PTSD) 52
61
About the Consultants
Experienced senior psychologists, psychiatrists, social workers, pharmacists, and other
health professionals who treat Veterans with PTSD
Available to consult on everything from your toughest cases to general PTSD questions
Ask about:
Evidence-based treatment
Medications
Clinical management
Resources
Assessment
Referrals
Collaborating with VA on Veterans’ care
Developing a PTSD treatment program
Available Resources - www.ptsd.va.gov/consult
Free continuing education
Videos, educational
handouts, and manuals
PTSD-related publications
PTSD and trauma assessment and screening tools
Mobile apps, and more
WWW.PTSD.VA.GOV
62

http://www.mentalhealth.va.gov/communityproviders/ 63
Providing Key Information and
Tools for Providers Serving
Veterans:
• Military service screening
• Military culture
• Behavioral health treatment
services and resources
ListenMore than 600 videos of real stories from Veterans experiencing mental health challenges and how they found support
LearnInformation about life events, signs and symptoms, and conditions
LocateFind VA, SAMHSA and National Resource Directory resources near you
64
Video GalleryFilter customizes video
results in real time,
providing user with stories of
Veterans with similar
experiences.
Choose from several filter
identifiers including a list of
signs and symptoms and
conditions
Expansive library of more
than 600 videos
65
Facebook Community
One of the largest and most engaged Facebook communities in the U.S. Government.
Robust dialogue from Veterans encouraging each other, sharing their experiences.
Posts designed to engage Veterans and family members with stories and videos from the website.
66
Conclusions
• Pain can be managed safely and more effectively with comprehensive strategies.
• SUD and PTSD are brain diseases that respond to recommended treatment
• VA performance-improvement efforts are increasing access to evidence-based treatments for PTSD & SUD
• Veterans and their families and those who care for them are encouraged to access VA services and to partner to with VA (e.g. Choice Program)
67

Michael T. Flaherty, Ph.D.Clinical/Consulting Psychologist
Founder – Institute for Research, Education and Training in the Addictions (IRETA)
Captain, USNR (Ret)
68
Amidst an Opioid Crisis: Best Practices for
SMVF Resilience, Treatment, and Recovery
Serving Service Members, Veterans, their and Families (SMVF)
69

System Challenges
SMVF navigate 4 systems:
• Active duty care or hospital
• Veterans Center
• Veterans clinic or hospital
• Civilian care or hospital
70
Mission
To serve those who have served
by implementing and integrating substance use
disorder (SUD) best practices across systems for
SMVF
71
Today’s SMVF
“Members of the armed forces are not immune to the
substance use problems that affect the rest of society.
Although illicit drug use is lower among U.S. military
personnel than among civilians (3.9 percent versus 17.2
percent) heavy alcohol and tobacco use, and especially
prescription drug misuse, are much more prevalent and are
on the rise.” –National Institute on Drug Abuse
72
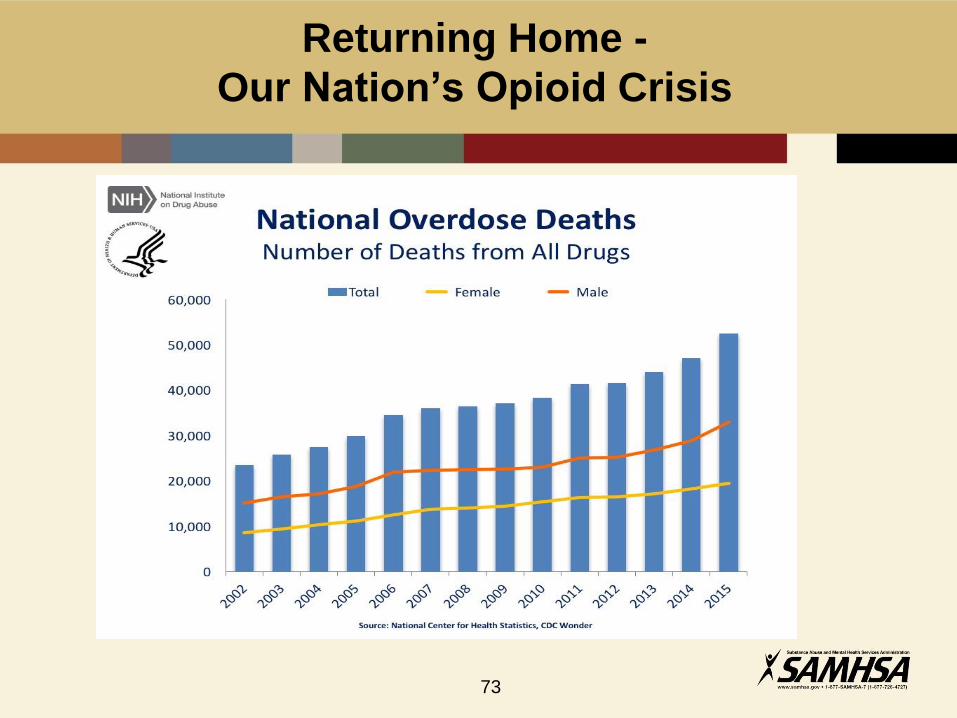
Returning Home -
Our Nation’s Opioid Crisis
73
The Facts
• Today 1 in 8 active duty military personnel are current users of
illicit drugs 1.
• Nearly half of active duty service members reported binge
drinking 2.
• 60 percent of the 140,000 veterans in federal and state prisons
struggle with substance use disorders 3.
• Over 50 percent of male and female VA patients seen in
primary care settings report chronic pain 4.
74
The Facts (cont’d)
• In younger veterans, ages 18–25, risk for prescription drug
misuse is at an all time high 5.
• Today 11 percent of service members report misusing
prescription drugs with opioid pain medication being most
frequently misused
• Pain reliever prescriptions written by military physicians
quadrupled between 2001 and 2009 to almost 3.8 million*
(NIDA)
75
What we need to know
Unique risk factors for SMVF:
• Stress of deployment – in wartime or peace; often multiple
deployments
• Zero-tolerance policies1
• Stigma
• Confidentiality
• Pre-existing conditions, e.g., chronic pain, PTSD, or other
psychological or physical wounds2
([email protected] /866-948-7880)
• Suicide*
76
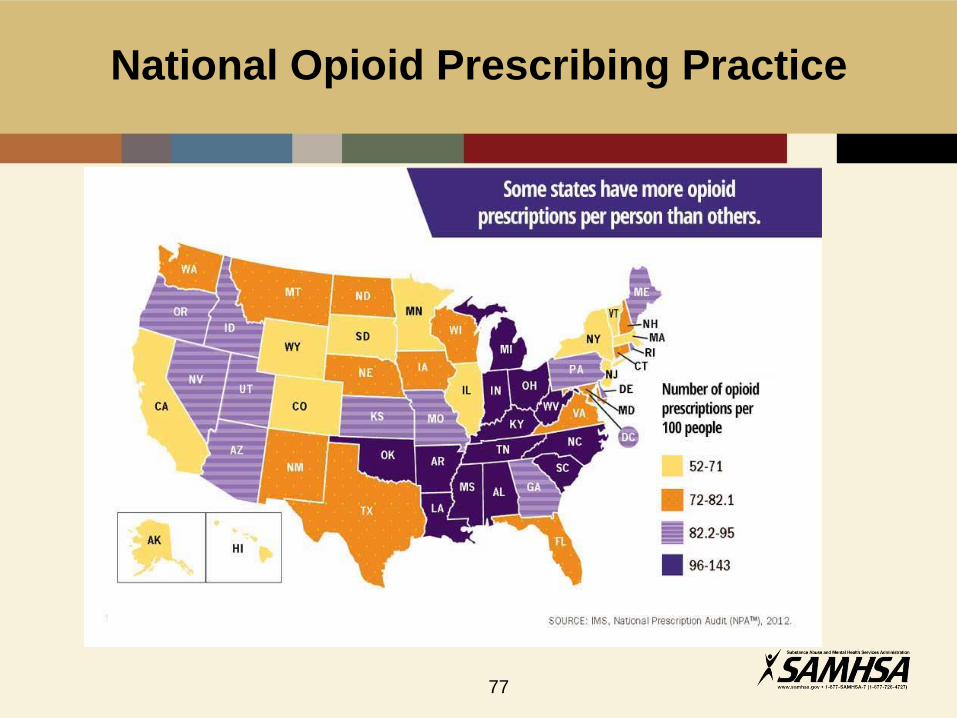
National Opioid Prescribing Practice
77
What We Can Do: Our “Op-Plan”
Understand the world from the perception and need of the service member and his or her family and align services.
Practice emergency, urgent, and general medicine over a continuum of care with a focus on long-term health, wellness, and recovery.
78
What We Can Do
Understand the belief system of the service member
• Army: This We’ll Defend
• Navy: Semper Fortis – Always Courageous
• Marine Corps: Semper Fidelis – Always Faithful
• Air Force: Above All
• Coast Guard: Semper Paratus – Always Ready
79
Know: The Military’s Guiding Rule
“Substance abuse by military personnel is inconsistent with the Department of Defense’s Values, the Warrior Ethos, and
the standards of performance, discipline, and readiness necessary to accomplish the DoD’s mission.” (1)
80
Know
Military Culture … and Civilian Realities
• Emphasizes discipline, hierarchy, and readiness
• Prioritizes the group over an individual
• Expects core values: loyalty, duty, respect, selfless
service, honor, integrity and personal courage
Many service members and their families are
experiencing multiple deployments
81
Know Combat to Home Defenses
Combat-Zone
Cohesion with buddies
Accountability and control
Targeted aggression
Tactical awareness
Lethally armed
Emotional control
Non-defensive driving
Discipline & obeying orders
Home-Zone
Withdrawal from others
Lack of control
Inappropriate aggression
Hypervigilance
Locked & loaded at home
Detached and uncaring
Aggressive driving
Giving orders…conflict
82
([email protected] /866-948-7880)
Know the Warrior’s Perception
By seeking treatment:
• 65 percent fear the perception of being seen as “weak”
• 63 percent fear leadership might treat them differently
• 59 percent fear others would have less confidence in
them
83
Substance Misuse Affects Military Families:
Resilience, Reintegration and Recovery
84
In Sum: What We Can Do
Understand this is a valued and unique population
surrounded by:
• Military culture and warrior mind
• Zero tolerance policies
• High stress, drinking, denial
• Co-occurring mental health/substance use issues
• Family needs
• High rates of PTSD, suicide, homelessness
• A fragmented system
85
What We Can Do to Address Opiate
Dependence
Increase Access to Treatment
• Service members struggling with addiction are being
discharged to local communities and VA Centers where a
capacity for treatment exists for only 20 percent of the existing
total population
• System or treatment access is the greatest barrier to care
• Nearly 2.7 million veterans have enrolled in the VA health
care since 2009
• 54,000 of these veterans will likely need substance use
screening and treatment
86
Build Prevention and Early Intervention
• Increase population resilience with community prevention
and involvement of all services, systems, and communities*
Educate, educate.
• Create a systemic approach to identify drug use earlier so as
to reduce harm and costs, e.g., Screening, Brief Intervention,
Referral to Treatment (SBIRT); Prescription Drug Abuse
Monitoring Program (PDMP); Pain Management Medical
Substance Use Monitoring
87
Build Prevention and Early Intervention
(cont’d)
• Expand addiction treatment services for SMVF in
community health centers; expand access to Medication
Assisted Treatment (MAT)
• Expand access to care
88
Know What is Working
• Naloxone/NARCAN - high risk populations
• Increased access to MAT, with an understanding for military
status and benefits and family
• Offer treatment on demand – 30 percent reduction (CDC)
• 24/7 Crisis Stabilization with MAT and treatment
• Boston Medical Center – Opioid Urgent Care Center
• Zuckerberg San Francisco General Hospital
89
Know What is Working (cont’d)
• Implement an operational PDMP across systems
• Crisis hotline: 1-888-796-8226; Crisis Text Line: text 4HOPE
to 741741 (24/7)
• Build peer supports – warm handoffs; recovery center
• Monitor all overdoses for root cause system improvement,
educate the community and empower it and parents to step
up … and have hope
Build military community resilience and recovery capital!
90
Join With Other Successful Initiatives
• Use veterans or community or family drug courts
• SBIRT in all medical settings; Community Reinforcement
and Family Training (CRAFT) for families
• Peer support – “Battle Buddies” – “No one left behind”
• Sober housing, homeless, and jail outreach
• Education and awareness – e.g., National Guard Beyond
the Yellow Ribbon
91
What We Can Do
• Design cross system care to build person-centered and
person-driven care for a continuity of care for SMVF
• Integrate care* – medically and behaviorally at all levels of
service for each person in the community
92

What We Can Do (cont’d)
• Make identified cross system “barriers” challenges for
refinement*
• Accept a shared responsibility to make seamless care
available; use peers for retention and to strengthen the
opportunity for recovery in all care across a continuum,
whatever the system providing it, i.e., Recovery Oriented
Systems of Care (ROSC)
93
We Know What to do
94
Resources
• SAMHSA: www.samhsa.gov
• U.S. Department of Veterans Affairs: https://www.va.gov/
• The Surgeon General’s Report on Alcohol, Drugs, and Health:
https://addiction.surgeongeneral.gov/
• National Survey on Drug and Health 2014:
https://www.samhsa.gov/data/sites/default/files/NSDUH-FRR1-
2014/NSDUH-FRR1-2014.pdf
• Pain Management Opioid Safety Educational Guide:
https://www.va.gov/PAINMANAGEMENT/docs/OSI_1_Toolkit_Pain_Ed
ucational_Guide.pdf
• VA/DoD Clinical Practice Guidelines: http://www.healthquality.va.gov/
95
Resources (cont’d)
• U.S. Department of Veterans Affairs Health Benefits:
https://www.va.gov/healthbenefits/
• U.S. Department of Veterans Affairs Mental Health:
http://www.mentalhealth.va.gov/VAMentalHealthGroup.asp
• U.S. Department of Veterans Affairs About Face Program:
http://www.ptsd.va.gov/apps/AboutFace/
• U.S. Department of Veterans Affairs - The PTSD Consultation Program:
www.ptsd.va.gov/consult
• U.S. Department of Veterans Affairs Community Provider Toolkit:
http://www.mentalhealth.va.gov/communityproviders/
• National Institute on Drug Abuse – Substance Abuse in the Military,
https://www.drugabuse.gov/publications/drugfacts/substance-abuse-in-
military
96
Resources (cont’d)
• Center for Disease Control and Prevention IMS National Prescription Audit
2012: https://www.cdc.gov/vitalsigns/opioid-prescribing/infographic.html
• National Institute on Drug Abuse: https://www.drugabuse.gov/related-
topics/trends-statistics/overdose-death-rates
• The Prescription Opioid and Heroin Crisis: A Public Health Approach to an
Epidemic of Addiction: https://www.ncbi.nlm.nih.gov/pubmed/25581144
• Equipping Behavioral Health Systems and Authorities to Promote Peer
Specialists/Peer Recovery Coaching Services:
http://www.naadac.org/assets/1959/samsha_2012_expert_panel_meeting_r
eport_-_equipping_behavioral_health.pdf
• DOJ/ONDCP National Heroin Task Force 2015:
www.justice.gov/file/822231/download
97
For Technical Assistance Questions,
Please Contact
345 Delaware Avenue
Delmar, NY 12054
Phone: 518-439-7415, ext. 5270
Email: [email protected]
98
Related Documents