JOURNAL OF CLINICAL ONCOLOGY A S C O S P E C I A L A R T I C L E Interventions to Address Sexual Problems in People With Cancer: American Society of Clinical Oncology Clinical Practice Guideline Adaptation of Cancer Care Ontario Guideline Jeanne Carter, Christina Lacchetti, Barbara L. Andersen, Debra L. Barton, Sage Bolte, Shari Damast, Michael A. Diefenbach, Katherine DuHamel, Judith Florendo, Patricia A. Ganz, Shari Goldfarb, Sigrun Hallmeyer, David M. Kushner, and Julia H. Rowland A B S T R A C T Purpose The adaptation of the Cancer Care Ontario (CCO) guideline Interventions to Address Sexual Problems in People With Cancer provides recommendations to manage sexual function adverse effects that occur as a result of cancer diagnosis and/or treatment. Methods ASCO staff reviewed the guideline for developmental rigor and updated the literature search. An ASCO Expert Panel (Table A1) was assembled to review the guideline content and recommendations. Results The ASCO Expert Panel determined that the recommendations from the 2016 CCO guideline are clear, thorough, and based upon the most relevant scientific evidence. ASCO statements and modifications were added to adapt the CCO guideline for a broader audience. Recommendations It is recommended that there be a discussion with the patient, initiated by a member of the health care team, regarding sexual health and dysfunction resulting from cancer or its treatment. Psy- chosocial and/or psychosexual counseling should be offered to all patients with cancer, aiming to improve sexual response, body image, intimacy and relationship issues, and overall sexual func- tioning and satisfaction. Medical and treatable contributing factors should be identified and addressed first. In women with symptoms of vaginal and/or vulvar atrophy, lubricants in addition to vaginal moisturizers may be tried as a first option. Low-dose vaginal estrogen, lidocaine, and dehydroepiandrosterone may also be considered in some cases. In men, medication such as phosphodiesterase type 5 inhibitors may be beneficial, and surgery remains an option for those with symptoms or treatment complications refractory to medical management. Both women and men experiencing vasomotor symptoms should be offered interventions for symptomatic improvement, including behavioral options such as cognitive behavioral therapy, slow breathing and hypnosis, and medications such as venlafaxine and gabapentin.Additional information is available at: www.asco. org/survivorship-guidelines and www.asco.org/guidelineswiki. J Clin Oncol 36:492-511. © 2017 by American Society of Clinical Oncology INTRODUCTION Extraordinary advances in cancer diagnosis and treatment have led to more than 16.5 million people living with and beyond cancer in the United States. 1 Modern multimodality treatment, including surgery, radiotherapy, systemic che- motherapy, and targeted therapy, can result in short-term and long-term adverse physical and/or psychosocial effects. Although prevalence rates of sexual difficulties associated with cancer and its treatment vary depending on primary diagnosis, treatment modality, methods of assessment, and type of sexual difficulty, 2 estimates are reported to range from 40% to 100%. 3,4 This includes dis- orders of sexual desire and sexual response influenced by the biologic, physiologic, and psy- chological challenges that cancer and its treat- ments present. Author affiliations and support information (if applicable) appear at the end of this article. Published at jco.org on December 11, 2017. J.C. and J.H.R. were Expert Panel co-chairs. Clinical Practice Guideline Committee approved: August 24, 2017. Editor’s note: This American Society of Clinical Oncology Clinical Practice Guideline provides recommendations, with comprehensive review and analyses of the relevant literature for each recommendation. Additional information, including a Data Supplement with additional evidence tables, a Methodology Supplement, slide sets, clinical tools and resources, and links to patient information at www.cancer.net, is available at www. asco.org/survivorship-guidelines and www.asco.org/guidelineswiki. Reprint requests: American Society of Clinical Oncology, 2318 Mill Rd, Suite 800, Alexandria, VA 22314; guidelines@ asco.org. Corresponding author: American Society of Clinical Oncology, 2318 Mill Rd, Suite 800, Alexandria, VA 22314; e-mail: [email protected]. © 2017 by American Society of Clinical Oncology 0732-183X/18/3605w-492w/$20.00 ASSOCIATED CONTENT Appendix DOI: https://doi.org/10.1200/JCO. 2017.75.8995 Data Supplement DOI: https://doi.org/10.1200/JCO. 2017.75.8995 DOI: https://doi.org/10.1200/JCO.2017. 75.8995 492 © 2017 by American Society of Clinical Oncology VOLUME 36 • NUMBER 5 • FEBRUARY 10, 2018 Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121 Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

JOURNAL OF CLINICAL ONCOLOGY A S C O S P E C I A L A R T I C L E
Interventions to Address Sexual Problems in People WithCancer: American Society of Clinical Oncology ClinicalPractice Guideline Adaptation of Cancer CareOntario GuidelineJeanne Carter, Christina Lacchetti, Barbara L. Andersen, Debra L. Barton, Sage Bolte, Shari Damast, Michael A.Diefenbach, Katherine DuHamel, Judith Florendo, Patricia A. Ganz, Shari Goldfarb, Sigrun Hallmeyer, David M.Kushner, and Julia H. Rowland
A B S T R A C T
PurposeThe adaptation of the Cancer Care Ontario (CCO) guideline Interventions to Address SexualProblems in People With Cancer provides recommendations to manage sexual function adverseeffects that occur as a result of cancer diagnosis and/or treatment.
MethodsASCO staff reviewed the guideline for developmental rigor and updated the literature search. AnASCOExpert Panel (Table A1) was assembled to review the guideline content and recommendations.
ResultsThe ASCO Expert Panel determined that the recommendations from the 2016 CCO guideline areclear, thorough, and based upon the most relevant scientific evidence. ASCO statements andmodifications were added to adapt the CCO guideline for a broader audience.
RecommendationsIt is recommended that there be a discussion with the patient, initiated by a member of the healthcare team, regarding sexual health and dysfunction resulting from cancer or its treatment. Psy-chosocial and/or psychosexual counseling should be offered to all patients with cancer, aiming toimprove sexual response, body image, intimacy and relationship issues, and overall sexual func-tioning and satisfaction. Medical and treatable contributing factors should be identified andaddressed first. In women with symptoms of vaginal and/or vulvar atrophy, lubricants in addition tovaginal moisturizers may be tried as a first option. Low-dose vaginal estrogen, lidocaine, anddehydroepiandrosterone may also be considered in some cases. In men, medication such asphosphodiesterase type 5 inhibitors may be beneficial, and surgery remains an option for those withsymptoms or treatment complications refractory to medical management. Both women and menexperiencing vasomotor symptoms should be offered interventions for symptomatic improvement,including behavioral options such as cognitive behavioral therapy, slow breathing and hypnosis, andmedications such as venlafaxine and gabapentin.Additional information is available at: www.asco.org/survivorship-guidelines and www.asco.org/guidelineswiki.
J Clin Oncol 36:492-511. © 2017 by American Society of Clinical Oncology
INTRODUCTION
Extraordinary advances in cancer diagnosis andtreatment have led to more than 16.5 millionpeople living with and beyond cancer in theUnited States.1 Modern multimodality treatment,including surgery, radiotherapy, systemic che-motherapy, and targeted therapy, can result inshort-term and long-term adverse physical and/or
psychosocial effects. Although prevalence rates ofsexual difficulties associated with cancer and itstreatment vary depending on primary diagnosis,treatment modality, methods of assessment, andtype of sexual difficulty,2 estimates are reportedto range from 40% to 100%.3,4 This includes dis-orders of sexual desire and sexual responseinfluenced by the biologic, physiologic, and psy-chological challenges that cancer and its treat-ments present.
Author affiliations and support information
(if applicable) appear at the end of this
article.
Published at jco.org on December 11,
2017.
J.C. and J.H.R. were Expert Panel
co-chairs.
Clinical Practice Guideline Committee
approved: August 24, 2017.
Editor’s note: This American Society of
Clinical Oncology Clinical Practice
Guideline provides recommendations,
with comprehensive review and analyses
of the relevant literature for each
recommendation. Additional information,
including a Data Supplement with
additional evidence tables, aMethodology
Supplement, slide sets, clinical tools and
resources, and links to patient information
at www.cancer.net, is available at www.
asco.org/survivorship-guidelines and
www.asco.org/guidelineswiki.
Reprint requests: American Society of
Clinical Oncology, 2318Mill Rd, Suite 800,
Alexandria, VA 22314; guidelines@
asco.org.
Corresponding author: American Society
of Clinical Oncology, 2318 Mill Rd, Suite
800, Alexandria, VA 22314; e-mail:
© 2017 by American Society of Clinical
Oncology
0732-183X/18/3605w-492w/$20.00
ASSOCIATED CONTENT
Appendix
DOI: https://doi.org/10.1200/JCO.
2017.75.8995
Data Supplement
DOI: https://doi.org/10.1200/JCO.
2017.75.8995
DOI: https://doi.org/10.1200/JCO.2017.
75.8995
492 © 2017 by American Society of Clinical Oncology
VOLUME 36 • NUMBER 5 • FEBRUARY 10, 2018
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

THE BOTTOM LINE
Interventions to Address Sexual Problems in People With Cancer: American Society of Clinical Oncology ClinicalPractice Guideline Adaptation of Cancer Care Ontario Guideline
Guideline QuestionWhat is the effectiveness of pharmacological interventions, psychosocial counseling, or devices to manage sexual problems after cancertreatment? More specifically, issues in men and in women were examined separately.
Target PopulationThis guideline is applicable to adult ($ 18 years of age) men and women (and their partners) of all sexual orientations living withcancer of any type. For the purposes of this guideline, men and women who were previously treated for a childhood cancer were notincluded.
Target AudienceHealth care practitioners, such as oncologists, urologists, gynecologists, primary care providers, surgeons, nurses, physiotherapists,social workers, counselors, psychologists, psychiatrists, and sex therapists/counselors, and advanced practice providers, such asphysician assistants and nurse practitioners.
ASCO Recommendations for Interventions to Address Sexual Problems in People With CancerThe ASCO Expert Panel’s modifications to Cancer Care Ontario’s (CCO’s) recommendations and qualifying statements appear in bolditalics. ASCO’s own qualifying statements appear in italics. A list of the original CCO recommendations can be found in Table 1.
For All People With Cancer
Recommendation 1. It is recommended that there be a discussion with the patient, initiated by a member of the health care team,regarding sexual health and dysfunction resulting from the cancer or its treatment. The conversation could include the patient’spartner, only if the patient so wishes. This issue should be raised with the individual at the time of diagnosis and continue to bereassessed periodically throughout follow-up. The Expert Panel believes that this is a vital recommendation. The recommendationsthat follow cannot be used unless someone has taken the initiative to ask.
It is recommended that there be access to resources or referral information for the patient (and partner).
ASCOQualifying Statement. The Expert Panel believes that introduction of the topic of sexual function should be held with the patient alone,with the option of later partner inclusion if desired by the patient. Discussions should be congruent with the patient’s literacy level, cultural/religious beliefs, and sexual orientation. This discussion should be offered at varied points of treatment and survivorship to assess or addressany changes.
For Women With Cancer
CONDITION: SEXUAL RESPONSERecommendation 1. The Expert Panel believes that psychosocial and/or psychosexual counseling should be offered to women withcancer, aiming to improve elements of sexual response such as desire, arousal, or orgasm. Current evidence does not support one typeof psychosocial or psychosexual counseling to be superior to another.
Clinicians may offer flibanserin to premenopausal women who are experiencing hypoactive sexual desire disorder.14,15
CCO Qualifying Statement. It is the opinion of the Expert Panel that any kind of regular stimulation (including masturbation) wouldlikely be of benefit for improving sexual response, regardless of the stimulation used.
ASCO Qualifying Statement. It should be noted that flibanserin has not been evaluated in women with a history of cancer or those onendocrine therapy. In addition, the risk/benefit ratio for this medication is uncertain.
CONDITION: BODY IMAGERecommendation 2. It is recommended that psychosocial counseling be offered to women with cancer and body image issues.
If a woman is partnered, evidence indicates that couples-based interventions are effective when compared with usual care.(continued on following page)
jco.org © 2017 by American Society of Clinical Oncology 493
Sexual Problems in People With Cancer Guideline Adaptation
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

THE BOTTOM LINE (CONTINUED)
No recommendation can be made for or against group therapy (with or without exercise) for women with body image issues.
ASCOQualifying Statement. Clinicians should assess for body image issues early and often in the cancer care continuum and should take intoaccount cultural and/or religious variations. Patients with preexisting depression and/or body image issues may be at a higher risk ofsusceptibility.
CONDITION: INTIMACY/RELATIONSHIPSRecommendation 3. It is recommended that psychosocial counseling be offered to women with cancer aiming to improve intimacy andrelationship issues. If a woman is partnered, evidence indicates that couples-based interventions are effective when compared withusual care.
ASCO Qualifying Statement. The Expert Panel views partner involvement in all cases to be the choice of the patient.
CONDITION: OVERALL SEXUAL FUNCTIONING AND SATISFACTIONRecommendation 4. The Expert Panel believes that psychosocial counseling directed at the individual or couple or delivered in a groupbe offered to women with cancer who have problems with overall sexual functioning. Physical exercise or pelvic floor physiotherapy, inaddition to psychosocial counseling, may also be of benefit.
Current evidence does not support a specific psychosocial counseling intervention to improve sexual functioning and satisfaction.
Health care providers should screen patientswith cancer for overall sexual functioning and satisfaction, and a diagnosisshould be established when there are physical issues playing a contributing role.
All patients should be offered education and symptom management based on the patient’s diagnosis. For patientshaving persistent concerns, such as physical issues, a gynecologic examination would be ideal. For those continuing tohave relationship issues and/or distress, mental health counseling should be an option.
ASCO Qualifying Statement. The ASCO Expert Panel believes patients can still benefit if counseling is provided by licensed counselorsavailable at the medical center even if specialized therapists (eg, sex therapists) are not available.
CONDITION: VASOMOTOR SYMPTOMSRecommendation 5. For women with vasomotor symptoms, hormone therapy is the most effective intervention. For women unwillingor unable to use hormonal therapy, alternatives exist: for example, paroxetine, venlafaxine, gabapentin, or clonidine.
Having a hormone-sensitive breast cancer is a contraindication to using systemic hormone therapy.
Psychosocial counseling (cognitive behavioral therapy) and/or clinical hypnosis may provide a benefit and reduce vasomotorsymptoms and should be offered.16-19
CCO Qualifying Statement. The Expert Panel emphasizes that women with non–hormone-sensitive cancers who develop vasomotorsymptoms from their cancer treatment should be counseled to consider hormone therapy until the average age of menopause,approximately 51 years, at which point they should be re-evaluated. Risks typically cited for hormone therapy are derived from studiesof postmenopausal women. Beyond the age of 51 years, hormone therapy is an individual therapy with few risks for symptomaticpatients in their 50s. It should be intermittently evaluated for long-term use.
When not contraindicated, estrogen therapy alone (oral, transdermal, or vaginal) is recommended for women who have hada hysterectomy, as it has a more beneficial risk/benefit profile.
Paroxetine and fluoxetine should not be offered to women with breast cancer taking tamoxifen. Adverse events of clonidine includehypotension, light-headedness, headache, dry mouth, dizziness, sedation, and constipation. Sudden cessation can lead to significantelevations in blood pressure.
ASCOQualifying Statement. The use of systemic hormone therapy is not necessarily contraindicated in patients with other hormone-sensitivecancers like endometrial and ovarian cancer. Clinicians should discuss all options, including integrative approaches, with their patient,outlining the benefits and risks of each.
CONDITION: GENITAL SYMPTOMSRecommendation 6. The Expert Panel believes that for women with symptoms of vaginal and/or vulvar atrophy, such as dryness,the following stepwise approach should be followed:
(continued on following page)
494 © 2017 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Carter et al
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.
THE BOTTOM LINE (CONTINUED)
Lubricants for all sexual activity or touch, in addition to vaginal moisturizers to improve vulvovaginal tissue quality, maybe tried first. It should be noted that moisturizers may need to be applied at a higher frequency (three to five times perweek) in the vagina, at the vaginal opening, and on the external folds of the vulva for symptom relief in female patientswith cancer and survivors.151
For those who do not respond or whose symptoms are more severe at presentation, low-dose vaginal estrogen can be used. For womenwith hormone-positive breast cancer who are symptomatic and not responding to conservative measures, low-dose vaginal estrogencan be considered after a thorough discussion of risks and benefits.
Lidocaine can also be offered for persistent introital pain and dyspareunia.152
For women with current or a history of breast cancer who are on aromatase inhibitors and have not responded toprevious treatment, clinicians may offer vaginal dehydroepiandosterone.20-23
Finally, clinicians may offer the selective estrogen receptor modulator ospemifene to postmenopausal women withoutcurrent or a history of breast cancer who are experiencing dyspareunia, vaginal atrophy, or other vaginal pain.24-26
Clinicians should offer pain relievers to women on aromatase inhibitors who are experiencing arthralgia that interfereswith intimacy.
Clinicians may suggest the use of skin protectants/sealants applied to the external folds of the vulva in women usingpads for leakage and/or discharge.
Vaginal dilators may be of benefit in the management of vaginismus and/or vaginal stenosis and can be offered to anyone having painwith examinations and/or sexual activity. This is particularly important for women treated with pelvic (or vaginal) radiationtherapy. Ideally, benefit is greatest when started early and should not be recommended based on sexual activity or sexual orientationbut, rather, to all women at risk for vaginal changes to be proactive in their sexual and vulvovaginal health.
Cognitive behavioral therapy and pelvic floor (Kegel) exercisesmay be useful to decrease anxiety and discomfort and can lower urinarytract symptoms.
The Expert Panel believes that pelvic floor physiotherapy may be beneficial for patients experiencing symptoms of a potential pelvicfloor dysfunction, including persistent pain and urinary and/or fecal leakage. Clinicians may refer patients to a urologist orurogynecologist for further evaluation and treatment of urinary incontinence or to a colorectal surgeon for fecal incontinence.
ASCOQualifying Statement. There is limited supportive data on the use of vaginal dehydroepiandosterone in women with a history of canceror on endocrine therapy, so the risk/benefit for this population is not fully known. Ospemifene has not been evaluated in women with a historyof cancer or on endocrine therapy, and therefore, the risk/benefit is not known for this population. A thorough discussion outlining theuncertainty should be had with the patient.
For Men With Cancer
CONDITION: SEXUAL RESPONSERecommendation 1. It is recommended that phosphodiesterase type 5 inhibitor (PDE5i) medications be used to help men with erectiledysfunction.
Men who do not respond to PDE5i medications should consider alternate interventions, such as a vacuum erectile device (VED),medicated urethral system for erection, or intracavernosal injection.
There may be some benefit to initiating the use of any of the above interventions earlier after cancer treatment rather than later.Introduction prior to treatment initiation may be of benefit to some men.
(continued on following page)
jco.org © 2017 by American Society of Clinical Oncology 495
Sexual Problems in People With Cancer Guideline Adaptation
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

THE BOTTOM LINE (CONTINUED)
Surgical interventions, including penile prosthesis implantation for erectile dysfunction, can be offered to patients whoare not responding to conventional medical therapy or reporting adverse effects with such therapy.
Clinicians may refer patients to a urologist for evaluation and treatment of stress urinary incontinence.
CCO Qualifying Statement. The Expert Panel believes that men are best served by being offered a combination of psychosocialcounseling with the aim of greater adaptation toward long-term use and PDE5i medication adherence together with PDE5i treatment.For men who are partnered, psychosocial counseling should be directed at the couple.
Men should be aware that it might take a long time for medications to work and that PDE5i medications might not work for all men,especially in those with preexisting comorbidities. Clinicians should discuss with patients the appropriate duration of use andalternative options (eg, surgery) if the medications fail to work satisfactorily.
It is the opinion of the Expert Panel that any kind of regular stimulation (including masturbation) would likely be of benefit forimproving sexual response, regardless of the stimulation used.
Contraindications include the use of nitrates in any form. Common acute adverse effects of PDE5i medications include headaches,flushing, dizziness, upset stomach, nasal congestion, and dyspepsia.
CONDITION: GENITAL CHANGESRecommendation 2. It is recommended that a VED be used daily to prevent penis length loss. There may be some benefit to initiatingthe use of VEDs earlier after cancer treatment rather than later. Early treatment with PDE5i medications may also be beneficial for thisoutcome.
CONDITION: INTIMACY/RELATIONSHIPSRecommendation 3. The Expert Panel believes that individual or couples counseling should be offered for those wishing toimprove relationship or intimacy issues. Current evidence does not support a particular intervention to improve intimacy orrelationships.
ASCO Qualifying Statement. The opportunity for partners to be involved should be offered rather than viewed as a necessarycondition.
CONDITION: OVERALL SEXUAL FUNCTIONING AND SATISFACTIONRecommendation 4: It is recommended that psychosocial counseling be offered to men with cancer (and partners) to potentiallyimprove sexual functioning and satisfaction. It is also recommended that the use of pro-erectile agents and devices be considered,recognizing that most of the benefit is specifically for erectile dysfunction. With men who have sex with men, additional educationmay need to be provided on the changes in erection and alternative ways to maintain sexual intimacy.
Body image, including such issues as weight changes, disfigurement, scarring, and hair loss, should be discussed andnormalized in men.
Clinicians should check testosterone levels, even if the patient has a cancer that is not typically associated withhormone changes. Options should be discussed when testosterone levels are within normal range but the patient orclinician feels supplementation can have a clinical benefit and is not contraindicated.
CCO Qualifying Statement. Psychosocial counseling could be used to help couples integrate interventions into their usual sexualactivities.
CONDITION: VASOMOTOR SYMPTOMSRecommendation 5. Men with vasomotor symptoms should be offered medication for symptomatic improvements. Options wouldinclude venlafaxine, medroxyprogesterone acetate, cyproterone acetate, and gabapentin. Acupuncture may be a suitable alternative, asmay be other integrative medicine options, such as slow-breathing techniques and hypnosis, as evidence demonstrates clinical benefitin women.
(continued on following page)
496 © 2017 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Carter et al
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

Sexual health is an integral component of quality of life acrossthe lifespan. Cancer survivors who experience sexual morbidity areat an increased risk of distress and poor quality of life. Impairedemotional well-being and quality of life in turn contribute tohigher rates of morbidity and mortality among affected cancersurvivors.5,6 Sexual problems commonly include decreased desire,arousal disorders, pain (largely in women), and erectile dysfunc-tion (in men). In addition to cultural and religious influences,sexual function is affected in a multifactorial way by one’s overallhealth (the patient’s and that of his/her partner), partner re-lationships, previous sexual history, medications, fatigue and stress,mood, view of sexual self, body image, incontinence, and hor-monal changes. Cancer can independently affect sexual function bythe nature of the disease and its treatment and/or result in changesto health, body image, or view of sexual self, and altered re-lationships secondary to illness.
There remains an overall reluctance from both clinicians andpatients to talk about cancer- and treatment-related sexualdifficulties.2,7,8 Barriers from the clinician’s perspective can includefeeling inadequately trained or insufficiently skilled, limitedawareness of effective interventions, lack of time, lack of privacy,and concerns about making patients feel uncomfortable.9 Beyondthese reasons, studies also suggest that clinicians may make as-sumptions based on factors such as age and presumed interest,overall prognosis, and whether the patient has a current partner.10
For patients, barriers similarly may include concerns about makingthe doctor feel uncomfortable, embarrassment around the topic,belief that it is the clinician’s responsibility to raise the issue, andthat their sexual health concerns are not valid or are an expectedand untreatable complication of their disease and itstreatment.9,11-13
In 2016, Cancer Care Ontario (CCO) released guideline rec-ommendations regarding interventions to improve sexual functionin individuals with cancer. ASCO has established a process forendorsing and/or adapting other organizations’ clinical practiceguidelines. This article summarizes the results of that process andpresents the adapted practice recommendations.
The original CCO recommendations appear in Table 1 and onlineat https://www.cancercareontario.ca/en/content/interventions-address-sexual-problems-people-cancer.
OVERVIEW OF THE ASCO GUIDELINE ADAPTATION PROCESS
ASCO has policies and procedures for endorsing and/or adaptingpractice guidelines that have been developed by other professionalorganizations, with the goal of increasing the number of high-quality, ASCO-vetted guidelines available to the ASCO member-ship. The ASCO endorsement process involves an assessment byASCO staff of candidate guidelines for methodological qualityusing the Rigor of Development subscale of the Appraisal ofGuidelines for Research and Evaluation II (AGREE II) instrument.(See Methodology Supplement for more details.) The CCOguideline for Interventions to Address Sexual Problems in PeopleWith Cancer rated highly on the AGREE II instrument and wasidentified as a potential candidate for endorsement by ASCO.During the endorsement process, modifications and qualifyingstatements were made by the ASCO Expert Panel (Appendix TableA1, online only) to improve the guideline’s applicability to the broaderASCO guideline audience. Due to the number and significance ofthese changes, the ASCO Clinical Practice Guidelines Committeeleadership agreed that this product should be considered a guidelineadaptation, and it was labeled as such going forward. All funding forthe administration of the project was provided by ASCO.
DisclaimerThe clinical practice guidelines and other guidance published
herein are provided by the American Society of Clinical Oncology,Inc. (“ASCO”) to assist providers in clinical decision-making. Theinformation therein should not be relied upon as being complete oraccurate, nor should it be considered as inclusive of all propertreatments or methods of care or as a statement of the standard ofcare. With the rapid development of scientific knowledge, new
THE BOTTOM LINE (CONTINUED)
Psychosocial counseling (cognitive behavioral therapy) may provide a benefit and reduce vasomotor symptoms andshould be offered.
ASCO Qualifying Statement. Evidence supporting the clinical effectiveness of various integrative medicine techniques exists for womenexperiencing vasomotor symptoms.16-19 The ASCO Expert Panel feels extrapolation to male patients is reasonable and an option for mensuffering from vasomotor symptoms.
Additional ResourcesMore information, including a Data Supplement, a Methodology Supplement, slide sets, and clinical tools and resources, is available atwww.asco.org/survivorship-guidelines and www.asco.org/guidelineswiki. Patient information is available at www.cancer.net.
A link to the guideline, Interventions to Address Sexual Problems in People With Cancer, can be found at https://www.cancercareontario.ca/en/content/interventions-address-sexual-problems-people-cancer
ASCO believes that cancer clinical trials are vital to informmedical decisions and improve cancer care, and that all patients shouldhave the opportunity to participate.
jco.org © 2017 by American Society of Clinical Oncology 497
Sexual Problems in People With Cancer Guideline Adaptation
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

Table1.
Orig
inal
CCO
andASCO
Ada
pted
Rec
ommen
datio
nsan
dQua
lifying
Statemen
ts
CCO
Rec
ommen
datio
nCCO
Qua
lifying
Statemen
tASCO
Ada
pted
Rec
ommen
datio
nASCO
Qua
lifying
Statemen
t
Forallp
eoplewith
canc
erRec
ommen
datio
n1.
Itis
reco
mmen
dedthat
therebe
adiscus
sion
with
thepa
tient,initiated
byamem
berof
thehe
alth
care
team
,reg
arding
sexu
alhe
alth
anddy
sfun
ctionresu
lting
from
the
canc
eror
itstrea
tmen
t.Idea
lly,the
conv
ersatio
nwou
ldinclud
ethepa
tient’s
partne
r,ifpa
rtne
red.
This
issu
esh
ould
beraised
atthetim
eof
diag
nosisan
dco
ntinue
tobe
reas
sess
edpe
riodica
llythroug
hout
follow-up.
TheExp
ertPan
elbe
lieve
sthat
this
isavital
reco
mmen
datio
n.Th
ereco
mmen
datio
nsthat
follow
cann
otbe
used
unless
someo
neha
stake
ntheinitiativeto
ask.
Itis
reco
mmen
dedthat
therebe
acce
ssto
reso
urce
sor
referral
inform
ationforthepa
tient
(and
partne
r).
Non
eRec
ommen
datio
n1.
Itis
reco
mmen
dedthat
therebe
adiscus
sion
with
thepa
tient,initia
tedby
amem
berof
thehe
alth
care
team
,rega
rdingse
xual
health
and
dysfun
ctionresu
lting
from
theca
ncer
orits
trea
tmen
t.Th
eco
nversa
tionco
uldinclud
ethepa
tient’s
partne
r,on
lyifthepa
tient
sowishe
s.Th
isissu
esh
ould
beraised
with
theindividu
alat
thetim
eof
diag
nosisan
dco
ntinue
tobe
reas
sess
edpe
riodica
llythroug
hout
follow-up.
TheExp
ertPan
elbe
lieve
sthat
this
isavital
reco
mmen
datio
n.Th
ereco
mmen
datio
nsthat
follow
cann
otbe
used
unless
someo
neha
stake
ntheinitiative
toask.
Itisreco
mmen
dedthat
therebe
acce
ssto
reso
urce
sor
referral
inform
ationforthepa
tient
(and
partne
r).
ASCO
Qua
lifying
Statemen
t.The
Expe
rtPa
nel
belie
vesthat
introd
uctio
nof
thetopicof
sexu
alfunc
tionsh
ould
behe
ldwith
thepa
tient
alon
e,with
theop
tionof
laterp
artner
inclus
ionifde
sired
bythepa
tient.Discu
ssions
shou
ldbe
cong
ruen
twith
thepa
tient’s
literac
yleve
l,cu
ltural/religious
belie
fs,an
dse
xual
orientation.
Thisdisc
ussion
shou
ldbe
offeredat
varie
dpo
ints
oftrea
tmen
tan
dsu
rvivorsh
ipto
asse
ssor
addres
san
ych
ange
s.
Forwom
enwith
canc
erSex
ualR
espo
nse
Rec
ommen
datio
n1.
TheExp
ertPan
elbe
lieve
sthat
psyc
hoso
cial
coun
selingsh
ould
beofferedto
wom
enwith
canc
er,aimingto
improv
eelem
ents
ofse
xualresp
onse
such
asde
sire,arou
sal,or
orga
sm.Current
eviden
cedo
esno
tsu
pporton
etype
ofps
ycho
social
psyc
hose
xual
educ
ationan
dco
unse
lingto
besu
perio
rto
anothe
r.Noreco
mmen
datio
nca
nbe
mad
efor
pharmac
olog
ical
interven
tions
.
Itistheop
inionof
theExp
ertP
anel
that
anykind
ofregu
larstim
ulation(in
clud
ingmasturbation)
wou
ldlikelybe
ofbe
nefitforim
prov
ingse
xual
resp
onse
,rega
rdless
ofthestim
ulation.
Rec
ommen
datio
n1.
TheExp
ertPan
elbe
lieve
sthat
psycho
social
and/or
psyc
hose
xual
coun
selingsh
ould
beofferedto
wom
enwith
canc
er,aimingto
improv
eelem
ents
ofse
xualresp
onse
such
asde
sire,arous
al,o
rorga
sm.C
urrent
eviden
cedo
esno
tsup
porton
etype
ofps
ycho
social
orps
ycho
sexu
aled
ucationan
dco
unse
lingto
besu
perio
rto
anothe
r.Clin
icians
may
offerfliba
nserin
toprem
enop
ausa
lwom
enwho
areex
perie
ncinghy
poac
tivese
xual
desire
diso
rder.1
4,15
Itistheop
inionof
theExp
ertP
anel
that
anykind
ofregu
larstim
ulation(in
clud
ingmasturbation)
wou
ldlikelybe
ofbe
nefitforim
prov
ingse
xual
resp
onse
,rega
rdless
ofthestim
ulation.
ASCO
Qua
lifying
Statemen
t.Itsh
ould
beno
ted
that
fliba
nserin
hasno
tbee
nev
alua
tedin
wom
enwith
ahistoryof
canc
eror
thos
eon
endo
crine
therap
y.In
additio
n,theris
k/be
nefit
ratio
forthis
med
icationis
unce
rtain.
Bod
yim
age
Rec
ommen
datio
n2.
Itis
reco
mmen
dedthat
psyc
hoso
cialco
unse
lingbe
offeredto
wom
enwith
canc
eran
dbo
dyim
ageissu
es.
Ifawom
anis
partne
red,
eviden
ceindica
tes
that
coup
les-ba
sedinterven
tions
areeffective
whe
nco
mpa
redwith
usua
lcare.
Noreco
mmen
datio
nca
nbe
mad
eforor
agains
tgrou
ptherap
y(w
ithor
with
out
exercise
)for
wom
enwith
body
imag
eissu
es.
Non
eRec
ommen
datio
n2.
Itis
reco
mmen
dedthat
psycho
social
coun
selingbe
offeredto
wom
enwith
canc
eran
dbo
dyim
ageissu
es.
Ifawom
anis
partne
red,
eviden
ceindicatesthat
coup
les-ba
sedinterven
tions
areeffectivewhe
nco
mpa
redwith
usua
lcare.
Noreco
mmen
datio
nca
nbe
mad
eforor
agains
tgrou
ptherap
y(w
ithor
with
oute
xercise)
forw
omen
with
body
imag
eissu
es.
ASCO
Qua
lifying
Statemen
t.Clin
icians
shou
ldas
sess
forbo
dyim
ageissu
esea
rlyan
doftenin
theca
ncer
care
continuu
man
dsh
ould
take
into
acco
untcu
lturala
nd/orrelig
ious
varia
tions
.Pa
tientswith
pree
xistingde
pres
sion
and/or
body
imag
eissu
esmay
beat
ahigh
erris
kof
susc
eptib
ility.
Intim
acy/relatio
nships
Rec
ommen
datio
n3.
Itis
reco
mmen
dedthat
psyc
hoso
cialco
unse
lingbe
offeredto
wom
enwith
canc
eraimingto
improv
eintim
acyan
drelatio
nshipissu
es.
Ifawom
anis
partne
red,
eviden
ceindica
tes
that
coup
les-ba
sedinterven
tions
areeffective
whe
nco
mpa
redwith
usua
lcare.
Non
eRec
ommen
datio
n3.
Itis
reco
mmen
dedthat
psycho
social
coun
selingbe
offeredto
wom
enwith
canc
eraimingto
improv
eintim
acyan
drelatio
nship
issu
es.
Ifawom
anis
partne
red,
eviden
ceindicatesthat
coup
les-ba
sedinterven
tions
areeffectivewhe
nco
mpa
redwith
usua
lcare.
ASCO
Qua
lifying
Statemen
t.The
Expe
rtPa
nel
view
spa
rtne
rinvo
lvem
entin
allc
ases
tobe
the
choice
ofthepa
tient.
(con
tinue
don
followingpa
ge)
498 © 2017 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Carter et al
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

Table1.
Orig
inal
CCO
andASCO
Ada
pted
Rec
ommen
datio
nsan
dQua
lifying
Statemen
ts(con
tinue
d)
CCO
Rec
ommen
datio
nCCO
Qua
lifying
Statemen
tASCO
Ada
pted
Rec
ommen
datio
nASCO
Qua
lifying
Statemen
t
Ove
rallse
xual
func
tioning
andsatis
faction
Rec
ommen
datio
n4.
TheExp
ertPan
elbe
lieve
sthat
psyc
hoso
cial
coun
seling
directed
attheindividu
alor
coup
leor
delivered
inagrou
pbe
offeredto
wom
enwith
canc
erwho
have
prob
lemswith
overalls
exua
lfunc
tioning
.Phy
sica
lexe
rciseor
pelvic
floo
rph
ysiotherap
y,in
additio
nto
psycho
social
coun
seling,
may
also
beof
bene
fit.
Current
eviden
cedo
esno
tsu
pportasp
ecific
psyc
hoso
cial
coun
selinginterven
tionto
improv
ese
xual
func
tioning
andsatis
faction.
Non
eRec
ommen
datio
n4.
TheExp
ertPan
elbe
lieve
sthat
psycho
social
coun
selingdirected
attheindividu
alor
coup
leor
delivered
inagrou
pbe
offeredto
wom
enwith
canc
erwho
have
prob
lemswith
overalls
exua
lfunc
tioning
.Phy
sicale
xerciseor
pelvic
floo
rph
ysiotherap
y,in
additio
nto
psycho
social
coun
seling,
may
also
beof
bene
fit.
Current
eviden
cedo
esno
tsu
pportasp
ecific
psyc
hoso
cialco
unse
linginterven
tionto
improv
ese
xual
func
tioning
andsa
tisfaction.
Hea
lthca
reprov
iderssh
ould
screen
patie
ntswith
canc
erforo
verallse
xual
func
tioning
andsa
tisfaction,
andadiag
nosissh
ould
bees
tablishe
dwhe
nthereare
phys
ical
issu
esplay
ingaco
ntrib
utingrole.
Allpa
tientssh
ould
beoffereded
ucationan
dsy
mptom
man
agem
entba
sedon
thepa
tient’s
diag
nosis.
For
patie
ntsha
ving
persistent
conc
erns
,suc
has
phys
ical
issu
es,a
gyne
cologicex
aminationwou
ldbe
idea
l.Fo
rthos
eco
ntinuing
toha
verelatio
nshipissu
esan
d/or
distress,men
talh
ealth
coun
selin
gsh
ould
bean
optio
n.
ASCO
Qua
lifying
Statemen
t.The
ASCO
Expe
rtPa
nelb
elieve
spa
tientsca
nstill
bene
fitif
coun
selin
gis
prov
ided
bylic
ense
dco
unse
lors
availableat
themed
ical
center
even
ifsp
ecialized
therap
ists
(eg,
sextherap
ists)areno
tav
ailable.
Vas
omotor
symptom
sRec
ommen
datio
n5.
Forwom
enwith
vaso
motor
symptom
s,ho
rmon
etherap
yisthe
mos
teffectiveinterven
tion.
Forwom
enun
willingor
unab
leto
useho
rmon
altherap
y,alternatives
exist;forex
ample,
paroxe
tine,
venlafax
ine,
gaba
pentin,or
clon
idine.
Havingaho
rmon
e-se
nsitive
brea
stcanc
eris
aco
ntraindica
tionto
usingsy
stem
icho
rmon
etherap
y.Psy
chos
ocialc
ouns
eling(cog
nitiv
ebe
havioral
therap
y)may
prov
ideabe
nefitan
dredu
ceva
somotor
symptom
san
dsh
ould
beoffered.
TheExp
ertPan
elem
phas
izes
that
wom
enwith
non–
horm
one-se
nsitive
canc
erswho
deve
lop
vaso
motor
symptom
sfrom
theirc
ance
rtreatmen
tsh
ould
beco
unse
ledto
cons
ider
horm
onetherap
yun
tiltheav
erag
eag
eof
men
opau
se,app
roximately
51ye
ars,
atwhich
pointthey
shou
ldbe
re-
evalua
ted.
Risks
typically
citedforho
rmon
etherap
yarede
rived
from
stud
iesof
postmen
opau
salw
omen
.Bey
ondtheag
eof
51ye
ars,
horm
onetherap
yis
anindividu
altherap
ywith
few
risks
forsymptom
atic
patie
ntsin
their
50s.
Itsh
ould
beinterm
itten
tlyev
alua
tedforlong
-term
use.
Whe
nno
tcon
traind
icated
,estroge
ntherap
yalon
e(oral,tran
sdermal,o
rvagina
l)is
reco
mmen
dedfor
wom
enwho
have
hadahy
sterec
tomy,
asitha
samorebe
neficial
risk/be
nefitprofi
le.
Parox
etinean
dfluo
xetin
esh
ould
notb
eofferedto
wom
enwith
brea
stcanc
ertaking
tamox
ifen.
Adv
erse
even
tsof
clon
idineinclud
ehy
potens
ion,
light-hea
dedn
ess,
head
ache
,dry
mou
th,d
izzine
ss,
seda
tion,
andco
nstip
ation.
Sud
dence
ssationcan
lead
tosign
ificant
elev
ations
inbloo
dpres
sure.
Rec
ommen
datio
n5.
Forwom
enwith
vaso
motor
symptom
s,ho
rmon
etherap
yis
themos
teffective
interven
tion.
Forwom
enun
willingor
unab
leto
use
horm
onal
therap
y,alternatives
exist:forex
ample,
paroxe
tine,
venlafax
ine,
gaba
pentin,or
clon
idine.
Hav
ingaho
rmon
e-se
nsitive
brea
stca
ncer
isaco
ntraindica
tionto
usingsy
stem
icho
rmon
etherap
y.Psy
chos
ocialc
ouns
eling(cog
nitiv
ebe
havioral
therap
y)an
d/or
clinical
hypn
osis
may
prov
ideabe
nefitan
dredu
ceva
somotor
symptom
san
dsh
ould
beoffered.
16-19
ASCO
Qua
lifying
Statemen
t.Th
eExp
ertPan
elem
phas
izes
that
wom
enwith
non–
horm
one-
sens
itive
canc
erswho
deve
lopvaso
motor
symptom
sfrom
theirca
ncer
trea
tmen
tsh
ould
beco
unse
ledto
cons
ider
horm
onetherap
yun
tilthe
averag
eag
eof
men
opau
se,ap
prox
imately51
years,
atwhich
pointthey
shou
ldbe
re-eva
luated
.Risks
typically
citedforho
rmon
etherap
yare
deriv
edfrom
stud
iesof
postmen
opau
salw
omen
.Bey
ondtheag
eof
51ye
ars,ho
rmon
etherap
yisan
individu
altherap
ywith
few
risks
forsy
mptom
atic
patie
ntsin
their50
s.Itsh
ould
beinterm
itten
tlyev
alua
tedforlong
-term
use.
The
useof
system
icho
rmon
etherap
yis
not
nece
ssarily
contraindica
tedin
patie
ntswith
othe
rho
rmon
e-se
nsitive
canc
erslik
een
dometria
land
ovarianca
ncer.Clin
icians
shou
lddisc
ussion
all
optio
ns,includ
ingintegrativeap
proa
ches
,with
theirpa
tient,ou
tlining
thebe
nefitsan
dris
ksof
each
.Whe
nno
tcon
traind
icated
,estroge
ntherap
yalon
e(oral,tran
sdermal,o
rva
gina
l)is
reco
mmen
dedfor
wom
enwho
have
hadahy
sterec
tomy,
asitha
samorebe
neficial
risk/be
nefitprofi
le.
Parox
etinean
dfluo
xetin
esh
ould
notb
eofferedto
wom
enwith
brea
stca
ncer
taking
tamox
ifen.
Adv
erse
even
tsof
clon
idineinclud
ehy
potens
ion,
light-hea
dedn
ess,
head
ache
,dry
mou
th,d
izzine
ss,
seda
tion,
andco
nstip
ation.
Sud
dence
ssationca
nlead
tosign
ifica
ntelev
ations
inbloo
dpres
sure.
(con
tinue
don
followingpa
ge)
jco.org © 2017 by American Society of Clinical Oncology 499
Sexual Problems in People With Cancer Guideline Adaptation
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.
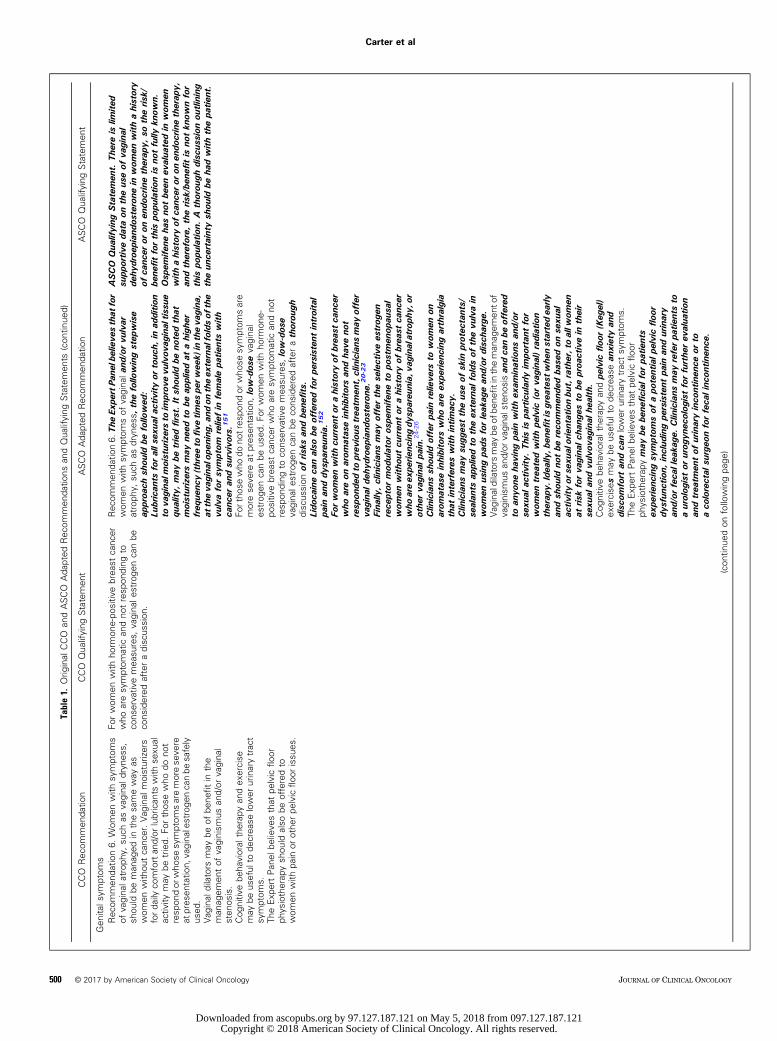
Table1.
Orig
inal
CCO
andASCO
Ada
pted
Rec
ommen
datio
nsan
dQua
lifying
Statemen
ts(con
tinue
d)
CCO
Rec
ommen
datio
nCCO
Qua
lifying
Statemen
tASCO
Ada
pted
Rec
ommen
datio
nASCO
Qua
lifying
Statemen
t
Gen
itals
ymptom
sRec
ommen
datio
n6.
Wom
enwith
symptom
sof
vagina
latrop
hy,su
chas
vagina
ldryne
ss,
shou
ldbe
man
aged
inthesa
meway
aswom
enwith
outca
ncer.Vag
inal
moisturizers
ford
ailyco
mfortan
d/or
lubrican
tswith
sexu
alac
tivity
may
betried.
Forthos
ewho
dono
tresp
ondor
who
sesy
mptom
saremorese
vere
atpres
entatio
n,va
gina
lestroge
nca
nbe
safely
used
.Vag
inal
dilators
may
beof
bene
fitin
the
man
agem
entof
vaginism
usan
d/or
vagina
lsten
osis.
Cog
nitiv
ebe
havioral
therap
yan
dex
ercise
may
beus
eful
tode
crea
selower
urinarytrac
tsy
mptom
s.Th
eExp
ertPan
elbe
lieve
sthat
pelvic
floo
rph
ysiotherap
ysh
ould
also
beofferedto
wom
enwith
pain
orothe
rpe
lvic
floo
rissu
es.
Forwom
enwith
horm
one-po
sitiv
ebrea
stcanc
erwho
aresy
mptom
atic
andno
tresp
onding
toco
nservativ
emea
sures,
vagina
lestroge
ncanbe
cons
idered
afteradiscus
sion
.
Rec
ommen
datio
n6.
The
Expe
rtPa
nelb
elieve
sthat
for
wom
enwith
symptom
sof
vagina
land
/orvu
lvar
atroph
y,su
chas
dryn
ess,
thefollo
wingstep
wise
approa
chsh
ould
befollo
wed
:Lu
brican
tsforalls
exua
lactivity
ortouc
h,in
additio
nto
vagina
lmoisturizersto
improv
evu
lvov
aginal
tissu
equ
ality
,may
betriedfirst.Itsh
ould
beno
tedthat
moisturizersmay
need
tobe
appliedat
ahigh
erfreq
uenc
y(three
tofiv
etim
espe
rwee
k)in
theva
gina
,at
theva
gina
lope
ning
,and
ontheex
ternalfoldsof
the
vulvaforsy
mptom
relie
fin
femalepa
tientswith
canc
eran
dsu
rvivors.
151
Fortho
sewho
dono
tres
pond
orwho
sesy
mptom
sare
morese
vere
atpres
entatio
n,low-dos
eva
gina
les
trog
enca
nbe
used
.Fo
rwom
enwith
horm
one-
positiv
ebrea
stca
ncer
who
aresy
mptom
atic
andno
tresp
onding
toco
nserva
tivemea
sures,
low-dos
evagina
lestroge
ncanbe
cons
idered
afterathorou
ghdiscus
sion
ofris
ksan
dbe
nefits.
Lido
caineca
nalso
beofferedforpe
rsistent
introital
pain
anddy
spareu
nia.
152
Forwom
enwith
curren
tor
ahistoryof
brea
stca
ncer
who
areon
arom
atas
einhibitors
andha
veno
tresp
onde
dto
prev
ious
trea
tmen
t,clinicians
may
offer
vagina
ldeh
ydroep
iand
osterone
.20-23
Fina
lly,clinicians
may
offerthese
lectivees
trog
enrece
ptor
mod
ulator
ospe
mife
neto
postmen
opau
sal
wom
enwith
outcu
rren
tor
ahistoryof
brea
stca
ncer
who
areex
perie
ncingdy
spareu
nia,
vagina
latrop
hy,o
rothe
rva
gina
lpain.
24-26
Clin
icians
shou
ldofferpa
inrelie
vers
towom
enon
arom
atas
einhibitors
who
areex
perie
ncingarthralgia
that
interferes
with
intim
acy.
Clin
icians
may
sugg
esttheus
eof
skin
protec
tants/
sealan
tsap
pliedto
theex
ternal
foldsof
thevu
lvain
wom
enus
ingpa
dsforleak
agean
d/or
disc
harge.
Vag
inaldilators
may
beof
bene
fitintheman
agem
ento
fvaginism
usan
d/or
vagina
lsteno
sisan
dca
nbe
offered
toan
yone
having
pain
with
exam
inations
and/or
sexu
alac
tivity
.Thisis
particularly
impo
rtan
tfor
wom
entrea
tedwith
pelvic
(orva
gina
l)radiation
therap
y.Idea
lly,b
enefitisgrea
test
whe
nstartedea
rlyan
dsh
ould
notbe
reco
mmen
dedba
sedon
sexu
alac
tivity
orse
xual
orientationbu
t,rather,toallw
omen
atris
kforva
gina
lcha
nges
tobe
proa
ctivein
their
sexu
alan
dvu
lvov
aginal
health.
Cog
nitiv
ebe
havioral
therap
yan
dpe
lvic
floor
(Keg
el)
exercise
smay
beus
eful
tode
crea
sean
xietyan
ddisc
omfort
andca
nlower
urinarytrac
tsy
mptom
s.Th
eExp
ertPan
elbe
lieve
sthat
pelvic
floo
rph
ysiotherap
ymay
bebe
nefic
ialfor
patie
nts
expe
rienc
ingsy
mptom
sof
apo
tentialp
elvicflo
ordy
sfun
ction,
includ
ingpe
rsistent
pain
andurinary
and/or
feca
llea
kage
.Clin
icians
may
referpa
tientsto
aurolog
istor
urog
ynec
olog
istforfurthe
rev
alua
tion
andtrea
tmen
tof
urinaryinco
ntinen
ceor
toaco
lorectal
surgeo
nforfeca
linc
ontin
ence
.
ASCO
Qua
lifying
Statemen
t.The
reis
limite
dsu
pportiv
eda
taon
theus
eof
vagina
lde
hydroe
pian
dosteron
ein
wom
enwith
ahistory
ofca
ncer
oron
endo
crinetherap
y,so
theris
k/be
nefit
forthis
popu
latio
nis
notfully
know
n.Osp
emife
neha
sno
tbe
enev
alua
tedin
wom
enwith
ahistoryof
canc
eror
onen
docrinetherap
y,an
dtherefore,
theris
k/be
nefit
isno
tkn
ownfor
this
popu
latio
n.A
thorou
ghdisc
ussion
outlining
theun
certaintysh
ould
beha
dwith
thepa
tient.
(con
tinue
don
followingpa
ge)
500 © 2017 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Carter et al
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.
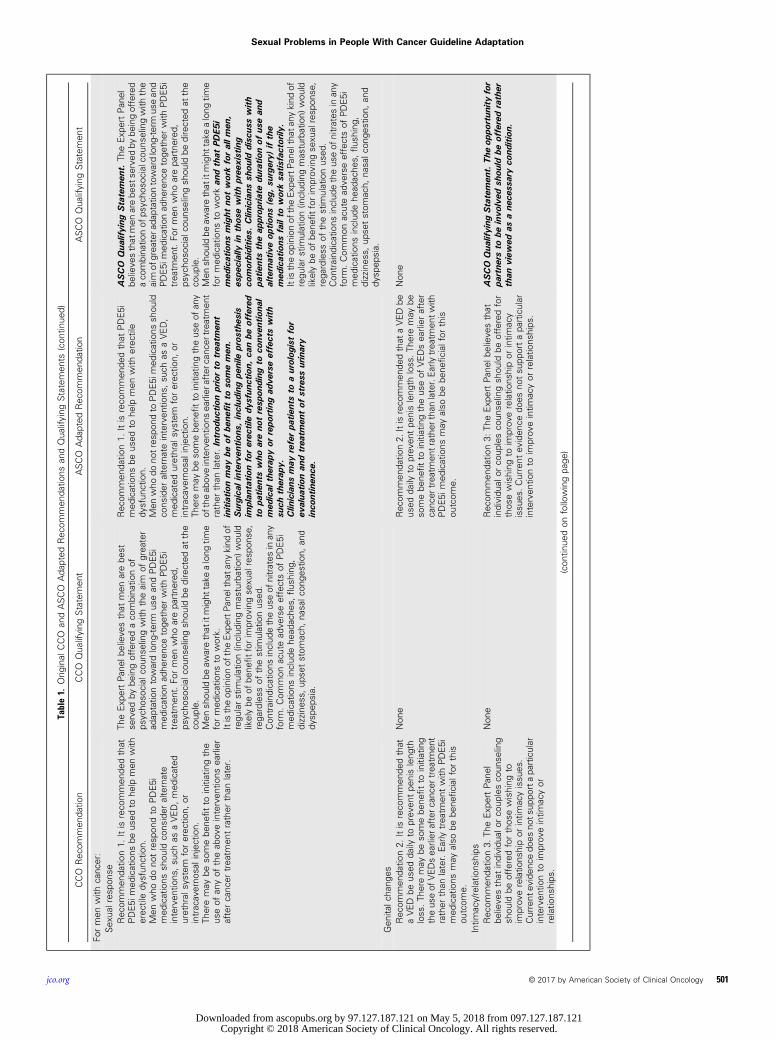
Table1.
Orig
inal
CCO
andASCO
Ada
pted
Rec
ommen
datio
nsan
dQua
lifying
Statemen
ts(con
tinue
d)
CCO
Rec
ommen
datio
nCCO
Qua
lifying
Statemen
tASCO
Ada
pted
Rec
ommen
datio
nASCO
Qua
lifying
Statemen
t
Formen
with
canc
er:
Sex
ualres
pons
eRec
ommen
datio
n1.
Itis
reco
mmen
dedthat
PDE5i
med
ications
beus
edto
help
men
with
erec
tiledy
sfun
ction.
Men
who
dono
tresp
ondto
PDE5i
med
ications
shou
ldco
nsider
alternate
interven
tions
,su
chas
aVED,med
icated
urethral
system
forerec
tion,
orintracaverno
salinjec
tion.
Theremay
beso
mebe
nefitto
initiatingthe
useof
anyof
theab
oveinterven
tions
earlier
aftercanc
ertrea
tmen
trather
than
later.
TheExp
ertPan
elbe
lieve
sthat
men
arebe
stse
rved
bybe
ingofferedaco
mbina
tionof
psycho
social
coun
selingwith
theaim
ofgrea
ter
adap
tatio
ntowardlong
-term
usean
dPDE5i
med
icationad
herenc
etoge
ther
with
PDE5i
trea
tmen
t.Fo
rmen
who
arepa
rtne
red,
psycho
social
coun
selingsh
ould
bedirected
atthe
coup
le.
Men
shou
ldbe
awarethat
itmight
take
along
time
formed
ications
towork.
Itistheop
inionof
theExp
ertP
anel
that
anykind
ofregu
larstim
ulation(in
clud
ingmasturbation)
wou
ldlikelybe
ofbe
nefitforim
prov
ingse
xual
resp
onse
,rega
rdless
ofthestim
ulationus
ed.
Con
traind
ications
includ
etheus
eof
nitrates
inan
yform
.Com
mon
acutead
verseeffectsof
PDE5i
med
ications
includ
ehe
adac
hes,
flus
hing
,dizzines
s,up
setstom
ach,
nasalc
onge
stion,
and
dysp
epsia.
Rec
ommen
datio
n1.
Itis
reco
mmen
dedthat
PDE5i
med
ications
beus
edto
help
men
with
erec
tile
dysfun
ction.
Men
who
dono
tres
pond
toPDE5i
med
ications
shou
ldco
nsider
alternateinterven
tions
,su
chas
aVED,
med
icated
urethral
system
forerec
tion,
orintracaverno
salinjec
tion.
Theremay
beso
mebe
nefitto
initiatingtheus
eof
any
oftheab
oveinterven
tions
earlier
afterc
ance
rtreatmen
trather
than
later.Introd
uctio
npriorto
trea
tmen
tinitiationmay
beof
bene
fitto
somemen
.Surgica
linterve
ntions
,includ
ingpe
nile
pros
thes
isim
plan
tatio
nforerec
tiledy
sfun
ction,
canbe
offered
topa
tientswho
areno
tresp
onding
toco
nven
tiona
lmed
ical
therap
yor
repo
rtingad
verseeffectswith
such
therap
y.Clin
icians
may
referpa
tientsto
aurolog
istfor
evalua
tionan
dtrea
tmen
tof
stress
urinary
inco
ntinen
ce.
ASCO
Qua
lifying
Statemen
t.Th
eExp
ertPan
elbe
lieve
sthat
men
arebe
stse
rved
bybe
ingoffered
aco
mbina
tionof
psyc
hoso
cialco
unse
lingwith
the
aim
ofgrea
tera
daptationtowardlong
-term
usean
dPDE5i
med
icationad
herenc
etoge
ther
with
PDE5i
trea
tmen
t.Fo
rmen
who
arepa
rtne
red,
psyc
hoso
cial
coun
selingsh
ould
bedirected
atthe
coup
le.
Men
shou
ldbe
awarethat
itmight
take
along
time
formed
ications
toworkan
dthat
PDE5
imed
ications
might
notworkforallm
en,
espe
cially
inthos
ewith
pree
xisting
comorbiditie
s.Clin
icians
shou
lddisc
usswith
patie
ntstheap
prop
riate
duratio
nof
usean
dalternativeop
tions
(eg,
surgery)
ifthe
med
ications
failto
worksa
tisfactorily
.Itistheop
inionof
theExp
ertP
anel
that
anykind
ofregu
larstim
ulation(in
clud
ingmasturbation)
wou
ldlikelybe
ofbe
nefitforim
prov
ingse
xual
resp
onse
,rega
rdless
ofthestim
ulationus
ed.
Con
traind
ications
includ
etheus
eof
nitrates
inan
yform
.Com
mon
acutead
verseeffectsof
PDE5i
med
ications
includ
ehe
adac
hes,
flus
hing
,dizzines
s,up
setstom
ach,
nasalc
onge
stion,
and
dysp
epsia.
Gen
italc
hang
esRec
ommen
datio
n2.
Itis
reco
mmen
dedthat
aVED
beus
edda
ilyto
prev
entpe
nisleng
thloss
.Th
eremay
beso
mebe
nefitto
initiating
theus
eof
VEDsea
rlier
afterc
ance
rtreatmen
trather
than
later.Early
trea
tmen
twith
PDE5i
med
ications
may
also
bebe
neficial
forthis
outcom
e.
Non
eRec
ommen
datio
n2.
Itisreco
mmen
dedthat
aVED
beus
edda
ilyto
prev
entpe
nisleng
thloss
.The
remay
beso
mebe
nefitto
initiatingtheus
eof
VEDsea
rlier
after
canc
ertrea
tmen
trathe
rtha
nlater.Earlytrea
tmen
twith
PDE5i
med
ications
may
also
bebe
neficial
forthis
outcom
e.
Non
e
Intim
acy/relatio
nships
Rec
ommen
datio
n3.
TheExp
ertPan
elbe
lieve
sthat
individu
alor
coup
lesco
unse
ling
shou
ldbe
offeredforthos
ewishing
toim
prov
erelatio
nshipor
intim
acyissu
es.
Current
eviden
cedo
esno
tsup
portapa
rticular
interven
tionto
improv
eintim
acyor
relatio
nships
.
Non
eRec
ommen
datio
n3:
TheExp
ertPan
elbe
lieve
sthat
individu
alor
coup
lesco
unse
lingsh
ould
beofferedfor
thos
ewishing
toim
prov
erelatio
nshipor
intim
acy
issu
es.C
urrent
eviden
cedo
esno
tsu
pportapa
rticular
interven
tionto
improv
eintim
acyor
relatio
nships
.
ASCO
Qua
lifying
Statemen
t.The
oppo
rtun
ityfor
partne
rsto
beinvo
lved
shou
ldbe
offeredrather
than
view
edas
ane
cessaryco
ndition
.
(con
tinue
don
followingpa
ge)
jco.org © 2017 by American Society of Clinical Oncology 501
Sexual Problems in People With Cancer Guideline Adaptation
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

Table1.
Orig
inal
CCO
andASCO
Ada
pted
Rec
ommen
datio
nsan
dQua
lifying
Statemen
ts(con
tinue
d)
CCO
Rec
ommen
datio
nCCO
Qua
lifying
Statemen
tASCO
Ada
pted
Rec
ommen
datio
nASCO
Qua
lifying
Statemen
t
Ove
rallse
xual
func
tioning
andsatis
faction
Rec
ommen
datio
n4.
Itis
reco
mmen
dedthat
psyc
hoso
cial
coun
selingbe
offeredto
men
with
canc
er(and
partne
rs)to
potentially
improv
ese
xualfunc
tioning
andsatis
faction.
Itis
also
reco
mmen
dedthat
theus
eof
pro-
erec
tileag
ents
andde
vice
sbe
cons
idered
,reco
gnizingthat
mos
tof
thebe
nefitis
spec
ifically
forerec
tiledy
sfun
ction.
Psy
chos
ocialc
ouns
elingco
uldbe
used
tohe
lpco
uplesintegrateinterven
tions
into
theirus
ual
sexu
alactiv
ities
.
Rec
ommen
datio
n4.
Itis
reco
mmen
dedthat
psycho
socialco
unse
lingbe
offeredto
men
with
canc
er(and
partne
rs)topo
tentially
improv
ese
xualfunc
tioning
andsatis
faction.
Itisalso
reco
mmen
dedthat
theus
eof
pro-erec
tileag
ents
andde
vice
sbe
cons
idered
,reco
gnizingthat
mos
tof
thebe
nefitis
spec
ifically
for
erec
tiledy
sfun
ction.
With
men
who
have
sexwith
men
,add
ition
aled
ucationmay
need
tobe
prov
ided
onthech
ange
sin
erec
tionan
dalternativeway
sto
maintainse
xual
intim
acy.
Bod
yim
age,
includ
ingsu
chissu
esas
weigh
tcha
nges
,disfigurem
ent,
scarrin
g,an
dha
irloss,sh
ould
bedisc
usse
dan
dno
rmalized
inmen
.Clin
icians
shou
ldch
ecktestos
terone
leve
ls,ev
enif
thepa
tient
hasaca
ncer
that
isno
ttypica
llyas
sociated
with
horm
onech
ange
s.Options
shou
ldbe
disc
usse
dwhe
ntestos
terone
leve
lsarewith
inno
rmal
rang
ebu
tthepa
tient
orclinicianfeels
supp
lemen
tatio
nca
nha
veaclinical
bene
fitan
disno
tco
ntraindica
ted.
Psy
chos
ocialc
ouns
elingco
uldbe
used
tohe
lpco
uplesintegrateinterven
tions
into
theirus
ual
sexu
alactiv
ities
.
Vas
omotor
symptom
sRec
ommen
datio
n5.
Men
with
vaso
motor
symptom
ssh
ould
beofferedmed
icationfor
symptom
atic
improv
emen
ts.Options
wou
ldinclud
eve
nlafax
ine,
med
roxy
prog
esterone
acetate,
cyproteron
eac
etate,
andga
bape
ntin.
Acu
punc
ture
may
beasu
itablealternative.
Non
eRec
ommen
datio
n5.
Men
with
vaso
motor
symptom
ssh
ould
beofferedmed
icationforsy
mptom
atic
improv
emen
ts.Options
wou
ldinclud
eve
nlafaxine,
med
roxy
prog
esterone
acetate,
cyproteron
eac
etate,
andga
bape
ntin.Acu
punc
ture
may
beasu
itable
alternative,
asmay
beothe
rintegrativemed
icine
optio
ns,su
chas
slow
-breathing
tech
niqu
esan
dhy
pnos
is,a
sev
iden
cede
mon
stratesclinicalbe
nefit
inwom
en.
Psyc
hoso
cial
coun
selin
g(cog
nitiv
ebe
havioral
therap
y)may
prov
ideabe
nefit
andredu
ceva
somotor
symptom
san
dsh
ould
beoffered.
ASCO
Qua
lifying
Statemen
t.Ev
iden
cesu
pportin
gtheclinical
effectiven
essof
vario
usintegrativemed
icinetech
niqu
esex
ists
for
wom
enex
perie
ncingva
somotor
symptom
s.16-19
The
ASCO
Expe
rtPa
nelfee
lsex
trap
olationto
malepa
tientsisreas
onab
lean
dan
optio
nform
ensu
fferingfrom
vaso
motor
symptom
s.
NOTE
.Add
ition
alASCOExp
ertP
anelstatem
ents
anded
itsto
originalCCOstatem
ents
appe
arinbo
ldita
lics.Abb
reviations
:CCO,C
ance
rCareOntario;P
DE5i,p
hosp
hodies
terase
type
5inhibitor;VED,vac
uum
erec
tile
device
.
502 © 2017 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Carter et al
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

evidence may emerge between the time information is developedand when it is published or read. The information is not con-tinually updated and may not reflect the most recent evidence. Theinformation addresses only the topics specifically identified thereinand is not applicable to other interventions, diseases, or stages ofdiseases. This information does not mandate any particular courseof medical care. Further, the information is not intended to sub-stitute for the independent professional judgment of the treatingprovider, as the information does not account for individual vari-ation among patients. Recommendations reflect high, moderate, orlow confidence that the recommendation reflects the net effect ofa given course of action. The use of words like “must,” “must not,”“should,” and “should not” indicate that a course of action is rec-ommended or not recommended for either most or many patients,but there is latitude for the treating physician to select other coursesof action in individual cases. In all cases, the selected course of actionshould be considered by the treating provider in the context oftreating the individual patient. Use of the information is voluntary.ASCO provides this information on an “as is” basis, and makes nowarranty, express or implied, regarding the information. ASCOspecifically disclaims any warranties of merchantability or fitness fora particular use or purpose. ASCO assumes no responsibility for anyinjury or damage to persons or property arising out of or related toany use of this information or for any errors or omissions.
Guideline and Conflicts of InterestThe Expert Panel was assembled in accordance with ASCO’s
Conflict of Interest Policy Implementation for Clinical PracticeGuidelines (“Policy,” found at http://www.asco.org/rwc). Allmembers of the Expert Panel completed ASCO’s disclosure form,which requires disclosure of financial and other interests, includingrelationships with commercial entities that are reasonably likely toexperience direct regulatory or commercial impact as a result ofpromulgation of the guideline. Categories for disclosure includeemployment; leadership; stock or other ownership; honoraria,consulting or advisory role; speaker’s bureau; research funding;patents, royalties, other intellectual property; expert testimony; travel,accommodations, expenses; and other relationships. In accordancewith the Policy, the majority of the members of the Expert Panel didnot disclose any relationships constituting a conflict under the Policy.
CLINICAL QUESTION AND TARGET POPULATION
The guideline, Interventions to Address Sexual Problems in PeopleWith Cancer, addressed the effectiveness of pharmacological in-terventions, psychosocial counseling, or devices to manage sexualproblems after cancer treatment in both men and women. Thecomplete set of recommendations are provided in Table 1.
The target population for the guideline, Interventions toAddress Sexual Problems in People With Cancer, is adult ($ 18years) men and women (and their partners) of all sexual orien-tations living with or surviving from cancer of any type. For thepurposes of this guideline, men and women who were previouslytreated for a childhood cancer were not included. Although out ofthe scope of this guideline, the Expert Panel believes that adolescents(younger than 18) with cancer also require a tailored discussion
regarding sexual health and fertility, even if they are not yet sexuallyactive. Further discussion of special issues affecting the adolescentand young adult population with cancer are found elsewhere.27,28
SUMMARY OF THE CCO GUIDELINEDEVELOPMENT METHODOLOGY
The CCO guideline was developed by an author Expert Panel anda Scientific Advisory Panel that included experts in gynecology,urology, medical oncology, radiation oncology, psychology, psy-chiatry, behavioral sciences, supportive care, and sexual health. Theliterature search of OvidMEDLINE, EMBASE, CINAHL, PsycINFO,and Cochrane Database was conducted on March 6, 2013. Owing tothe lack of intervention studies identified, including patients withhematologic cancer, separate searches were also run onMay 1, 2014,in the same databases. Details of the search strategies and the studyinclusion criteria and outcomes of interest are available at https://www.cancercareontario.ca/en/content/interventions-address-sexual-problems-people-cancer.
The searches identified 103 studies for inclusion in the guideline’squalitative synthesis of the literature. The CCO panel reviewed datafrom systematic reviews and primary studies covering sexual response,body image, intimacy and relationships, vasomotor symptoms, genitalsymptoms, and overall sexual function and satisfaction.
RESULTS OF THE ASCO METHODOLOGY REVIEW
The methodology review of the guideline, Interventions to AddressSexual Problems in People With Cancer, was completed in-dependently by two ASCO guideline staff members using the Rigorof Development subscale from the AGREE II instrument. TheRigor subscale consists of seven items that assess the quality of theprocesses used to gather and synthesize the relevant data and themethods used to formulate the guideline recommendations. Itemssuch as the use of systematic methods in the search of the evidence,explicit links between the recommendations and the evidence, andconsideration of benefits and risks were assessed. Each subscale itemis rated on a seven-point scale from 1 (strongly disagree) to 7(strongly agree). Detailed results of the scoring for this guideline areavailable upon request to [email protected]. Overall, the guideline,Interventions to Address Sexual Problems in People With Cancer,itself scored 80%. There were someminor deficiencies with reportingon the methods for formulating the recommendations and on thestrengths and limitations of the evidence considered (see Method-ology Supplement at www.asco.org/survivorship-guidelines).
The preliminary ASCO content reviewers of the Interventionsto Address Sexual Problems in People With Cancer as well as theASCO Expert Panel found the recommendations to be clear andthorough in the original guideline. Each section, including theguideline recommendations, the evidentiary base, and the devel-opment methods and external review process, was clear and wellreferenced from the systematic review.
This is the most recent information as of the publication date.For updates, the most recent information, and to submit newevidence, please visit www.asco.org/survivorship-guidelines andthe ASCO Guidelines Wiki (www.asco.org/guidelineswiki).
jco.org © 2017 by American Society of Clinical Oncology 503
Sexual Problems in People With Cancer Guideline Adaptation
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

RESULTS OF THE ASCO CONTENT REVIEW
The ASCO Expert Panel reviewed the guideline, Interventions toAddress Sexual Problems in People With Cancer, and concurs thatthe recommendations are clear, thorough, and based on the mostrelevant scientific evidence in this content area and present optionsthat will be acceptable to patients. For the most part, the ASCOExpert Panel agrees with the recommendations as stated in theguideline, but modifications and further qualifications are made.
METHODS AND RESULTS OF THE ASCO UPDATEDLITERATURE REVIEW
This systematic review-based guideline product was developed byan Expert Panel with multidisciplinary, including patient, repre-sentation and by ASCO guidelines staff with health research
methodology experience. ASCO guidelines staff updated the In-terventions to Address Sexual Problems in People With Cancerliterature search. PubMed was searched up to April 3, 2017. Thesearch was restricted to articles published in English. The updatedsearch was guided by the “signals”29 approach that is designed toidentify only new, potentially practice-changing data—signals—thatmight translate into revised practice recommendations. The approachrelies on targeted routine literature searching and the expertise ofASCO Expert Panel members to help identify potential signals. TheMethodology Supplement (available at www.asco.org/survivorship-guidelines) provides additional information about the signalsapproach.
The updated search yielded 159 records. A review of theseresults plus studies identified by searching reference lists andknown seminal papers resulted in 19 new, recommendation-changing studies being included.14-18,20,22-26,30-36,152 Table 2summarizes the number and types of studies included per sex-ual dysfunction condition.
Table 2. Symptoms and Interventions for Sexual Dysfunction (adapted from CCO guideline)
Symptom Possible Intervention Evidence
For women with cancerDifficulty with sexual response,such as desire, arousal, ororgasm
Psychosocial counseling, psychosexual counselingRegular stimulation (including masturbation)Flibanerin for premenopausal women
Two systematic reviews14,15
Two RCTs56,57
Three other58-60
Body image Psychosocial counseling, couples-based interventions Two systematic reviews61,62
Six RCTs56,57,63-66
One other67
Intimacy/relationships Psychosocial counseling, couples-based interventions Zero systematic reviewsFive RCTs56,57,63,64,68
Three other59,60,67
Overall sexual functioning andsatisfaction
Psychosocial counseling, education and symptommanagement, mental healthcounselingPhysical exercise or pelvic floor physiotherapy
Four systematic reviews61,69-71
Eleven RCTs57,63-66,68,72-76
Five other59,60,67,77,78
Vasomotor symptoms Psychosocial counseling (cognitive behavioral therapy)Paroxetine, fluoxetine (should not be offered to women with breast cancertaking tamoxifen), venlafaxine, gabapentin, or clonidineIntegrative approaches, such as clinical hypnosisEstrogen therapy alone (oral, transdermal, or vaginal) when not contraindicated;hormone therapy (for women with non–hormone-sensitive cancers)
Three guidelines19,79,80
One position statement19
Zero systematic reviewsSeven RCTs16-18,65,66,75,76
Genital symptoms, includingdyspareunia, vaginal atrophy,or other vaginal pain
Cognitive behavioral therapyExercise, pelvic floor physiotherapyVaginal moisturizers, lubricants, vaginal estrogen, liquid sealants, vaginaldilatorsSelective estrogen receptor modulator ospemifene (for postmenopausalwomen without a current or history of breast cancer)Lidocaine dehydroepiandosteronePain relievers (for women on aromatase inhibitors)
Two guidelines79,81
Three systematic reviews26,70,71
Eleven RCTs20,22-25,65,66,72,75,82,152
Four other78,83,84,151
For men with cancerSexual response, includingerectile dysfunction
PDE5i medications, VED, medicated urethral system, intracavernosal injectionSurgical intervention, including penile and testicular prosthesesPsychosocial counselingRegular stimulation (including masturbation)
Two systematic reviews85,86
Twenty RCTs87-116
Twenty-sixother30-36,77,111-113,117-131
Genital changes, body image VEDPDE5i medications
Zero systematic reviewsTwo RCTs98,104
One other114
Intimacy/relationships Individual or couples counseling One systematic review102,132
Five RCTs102,103,110,133,134
Three other116,135,136
Overall sexual functioning andsatisfaction
Psychosocial counselingPro-erectile agents and devices
Two systematic reviews132,137
Six RCTs89,98,105,110,138,139
Three other77,116,140
Vasomotor symptoms Venlafaxine, medroxyprogesterone acetate, cyproterone acetate, andgabapentinAcupuncture, hypnosisPsychosocial counseling (cognitive behavioral therapy)
Seven RCTs16-18,115,141-143
Seven other144-150
Abbreviations: CCO, Cancer Care Ontario; PDE5i, phosphodiesterase type 5 inhibitor; RCT, randomized controlled trial; VED, vacuum erectile device.
504 © 2017 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Carter et al
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

Characteristics and Quality Assessment of IncludedStudies
Three systematic reviews,14,15,26 nine randomized controlledtrials (RCTs),16-18,20,22-25,152 and seven observational studies30-36
were identified and met the inclusion criteria for the updatedliterature review.
Two systematic reviews14,15 collected RCT evidence andconducted meta-analyses to assess the efficacy and safety of fli-banserin in the treatment of hypoactive sexual desire disorder inwomen. Three RCTs16-18 investigated clinical hypnosis as a non-hormonal treatment of hot flashes in women. One systematicreview with meta-analysis26 and two RCTs24,25 assessed the efficacyand safety of ospemifene in treating dyspareunia associated withpostmenopausal vulvar and vaginal atrophy. Three RCTs in-vestigated intravaginal dehydroepiandrosterone on moderate tosevere dyspareunia and vaginal dryness, symptoms of vulvovaginalatrophy, and the genitourinary syndrome of menopause,20-22 andone RCT considered lidocaine in breast cancer survivors withsevere penetrative dyspareunia.152 Finally, seven observationalsurgical studies investigated penile prosthesis for erectile dys-function and testicular prosthesis for patients who have undergoneorchiectomy for cancer of the testis.30-36 While none of the studieswere found to have serious methodological flaws that would raiseconcerns about the findings, the inherent limitations of surgicalobservational studies should be taken into consideration. Surgicalstudies tended to include a relatively small number of patients, andsome studies only reported short follow-up times.30,31,33,36
Outcomes of Included StudiesIn 2015, the US Food and Drug Administration approved
flibanerin as a treatment of hypoactive sexual desire disorder inpremenopausal women.14 Two systematic reviews with meta-analyses examined the effectiveness of flibanserin on primaryoutcomes, such as satisfying sexual events, sexual desire score, andfemale sexual function index.14,15 Both found statistically signif-icant effects in women randomized to flibanserin compared withthose randomized to placebo. However, there also appeared to bea statistically significant increase in the risk of adverse effects suchas dizziness, somnolence, nausea, and fatigue.
Three RCTs examined the effect of hypnosis16-18 on reductionof vasomotor symptoms in postmenopausal women with orwithout a history of breast cancer. Each study found that hypnosisresulted in significant reductions in self-reported and physiolog-ically measured hot flashes and hot flash scores in women. Ad-ditional benefits such as reduced anxiety and depression andimproved sleep were also observed.17
One systematic review,26 one pooled analysis of two RCTs,24 andone additional RCT25 investigated ospemifene, a selective estrogenreceptor modulator, for the treatment of vulvovaginal atrophy anddyspareunia in postmenopausal women. All studies found a statisti-cally significant improvement in primary outcomes that includedfemale sexual dysfunction, vaginal dryness, dyspareunia, and vaginaland/or vulvar irritation/itching compared with placebo.
Three RCTs investigating intravaginal dehydroepiandrosterone(prasterone) in postmenopausal women all showed improvements inthe signs and symptoms of vaginal atrophy, including pain at sexualactivity, vaginal dryness, vaginal pH, and arousal/sensation.20-23
Serum steroid levels appear to remain within normal post-menopausal values.20-23
In another RCT of 46 estrogen-deficient breast cancer sur-vivors with severe penetrative dyspareunia, less pain during in-tercourse was reported with 4% aqueous lidocaine use comparedwith saline.152 There was a statistically significant decrease in sexualdistress (median score, 14; interquartile range, 3 to 20; P , .001),and sexual function improved in all but one domain with lidocaineuse. Of prior abstainers from intercourse who completed the study,85% had resumed comfortable penetrative intimacy.152
Seven observational studies investigated penile prosthesis forerectile dysfunction and testicular prosthesis for patients who haveundergone orchiectomy for cancer of the testis. Studies evaluatingthe efficacy, safety, and satisfaction with penile prosthesis im-plantation in men with various etiologies of erectile dysfunction,including consequence of radical prostatectomy and other pelvicsurgery, vascular and metabolic syndrome, and spinal trauma,found the implants to be safe and efficacious with high patient andpartner satisfaction.30-34 While the surgical techniques and types ofimplants used differed in these studies, overall results appear to beconsistent. Statistically and/or clinically significant improvementswere found in the mean International Index of Erectile Function-5(IIEF-5) scores,30,32,33 Erectile Dysfunction Inventory of TreatmentSatisfaction (EDITS) scores,30,31 Erection Harness Score,34 andGlobal Assessment Questionnaire (GAQ) scores.34
High overall satisfaction with testicular implants is reportedand ranges from 73% to 97%.35 However, dissatisfaction withseveral particular attributes of the implants have been reported,namely the shape, consistency, size, and high intrascrotal posi-tion.35 Acceptance rate appears to vary with age, such that thelikelihood of accepting a prosthesis decreases with increasing age.35
Psychological assessments measuring anxiety during sexual activityand desires and attempts to selectively avoid exposing one’s body(or parts of one’s body) to sexual partners (Body Exposure duringSexual Activities Questionnaire) showed statistically significantimprovements with testicular implants (P, .001).36 Similarly, theBody-Esteem Scale, whichmeasures self-confidence of each patienttoward sexuality, also showed statistically significant improvementswith the implants (P , .001).36 Interference with sexual activity,erectile functioning, or ejaculation was not observed.36
DISCUSSION
The CCO recommendations were adapted by a multidisciplinarygroup of experts using evidence from the supplementary literaturesearch and clinical experience as a guide. The majority of therecommendation text is listed verbatim from the guideline;however, there are some instances where the ASCO Expert Panelmade modifications or additions to the recommendations for thebroader ASCO audience and to reflect local context and updatedempirical evidence. These changes are identified by bold italics inthe Bottom Line Box and Table 1 and discussed further below.
Initiate at Each VisitThe Expert Panel strongly recommends designation of
a specific treatment team member to query and discuss with each
jco.org © 2017 by American Society of Clinical Oncology 505
Sexual Problems in People With Cancer Guideline Adaptation
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

patient any impact of cancer or cancer treatment on his/hersexuality. All patients should be provided with disease- andtreatment-specific education and symptom management. Clini-cians should initiate a discussion with the patient at the time ofdiagnosis and inquire about function periodically across treatmentand into follow-up. For patients reporting problems in function,a diagnosis should be established when there are physical issuesplaying a contributing role. For women having persistent physicalconcerns, a gynecologic exam would be important. For women ormen who disclose relationship difficulties and/or distress, referralfor marital therapy should be available.
This guideline and its recommendations are patient focused,and inclusion of others, such as a partner, is the prerogative of thepatient. It was acknowledged that psychosexual education is dif-ferent from psychosocial education as sexual health and intimacy isoften omitted in the latter conversations. Furthermore, clarifica-tion should be made about the difference between sex counselingand sex therapy. However, absence of a specialized sex therapistshould not be a reason for lack of discussion. Patients can stillbenefit by counseling provided by available generic counselors whocan help normalize the experience and increase support andguidance when a specialized sex therapist is not available. Ideally,education about the potential effect of cancer treatments on sexualfunction should be part of the informed consent process as well asany dialogue around plans for symptom management wheretherapies used themselves may affect sexual function (eg, painmedications, steroid use, antidepressants, etc). Discussions shouldbe congruent with the patient’s literacy level, cultural/religiousbeliefs, and sexual orientation.
ResourcesA key barrier to the delivery of optimal sexual care of patients
with cancer and survivors is lack of awareness of whom or whatmay be available to address sexual problems or concerns whenraised. Clinicians are encouraged to conduct a landscape review ofkey personnel and local resources to address sexual health withinand proximate to their practice as a first step. Because these maychange over time, an annual update of this list may be needed. TheExpert Panel felt it equally important for clinicians to be madeaware of high-quality national resources available for both patients(and their partners) and clinicians to help with education, as-sessment, andmanagement of this distinct problem. The AmericanCancer Society (www.cancer.org) and the National Cancer In-stitute (www.cancer.gov) both have comprehensive patient in-formational booklets about sex after cancer. Internationalresources are also available and include the MacMillan CancerSupport Community in the United Kingdom (www.macmillan.org.uk), the Cancer Council of Australia (www.cancercouncil.com.au), and the Scientific Network on Female Sexual Health andCancer (www.cancersexnetwork.org).9
Finding ways to ask about and assess sexual function is im-portant. General screening tools include those from the NationalComprehensive Cancer Network9 and Patient-Reported OutcomesMeasurement Information System (PROMIS-1) item screener.37
Gender-specific tools include the Brief Sexual Symptom Check-list38 (note: this scale has been adapted for use specifically in femalepatients with cancer9), Arizona Sexual Experience Scale (ASEX),39
and Female Sexual Function Index (FSFI) for women.40 For men,the Sexual Health Inventory for Men (SHIM),41 Sexual Quality ofLife Male (SQoL-M),42 and PROMIS are options. (Of note, FSFIand ASEX have been validated/used in cancer survivors; othershave not.) Use of standardized, validated measures are recom-mended for screening and assessment. Consideration should begiven to routine use of a simple screening measure in the clinicalsetting. This may help ensure that issues related to sexual health areidentified and addressed; it can also help send a message to patientsthat addressing sexual problems is an important part of theircancer care.
Professional organizations also exist to help clinicians identifyand facilitate connections with specialists in various areas of ex-pertise. Sexual health counselors and therapists with expertise intreating cancer survivors can be located through the AmericanAssociation of Sexuality Educators, Counselors, and Therapists orthe Society for Sex Therapy and Research. Additional resources formen can be found at Sexual Medicine Society of North America(www.sexhealthmatters.org). Resources specific for women in-clude the International Society for the Study of Women’s SexualHealth (www.isswsh.org); The North American Menopause So-ciety (www.menopause.org); the American Association of Sexu-ality Educators, Counselors and Therapists (www.aasect.org); andthe Society for Sex Therapy and Research (www.starnet.org).
Different Diagnoses Need Different ManagementThe ASCO Expert Panel noted the importance of broadly
recognizing that different sexual problems will have differentmanagement strategies. It is important to consider both thephysical as well as the psychosocial care appropriate for each ofthese. Furthermore, attention needs to be given to the fact thatsexual satisfaction is not dependent on (and should not be nar-rowly defined as) the ability to engage in intercourse. Consider-ation should be given to the multiple ways of achieving sexualsatisfaction for oneself, with or without a partner.
Across care, it is important to recognize that when adverseeffects of treatment contribute to sexual dysfunction (eg, painsyndromes secondary to use of an aromatase inhibitor for womenor erectile dysfunction secondary to hormonal therapy amongmen), this can lead to nonadherence or even discontinuation ofcancer therapy. Providing information about and, as needed, relieffrom these (eg, pain medication for use with aromatase inhibitors)can improve sexual function. In general, improved symptommanagement leads to improved sexual response.43
Patients at high risk of cancer who choose to undergo cancerrisk–reducing surgeries, such as bilateral mastectomy and/or oo-phorectomy, may also experience an effect on sexual functioning.Clinicians should be aware that while the target population of thisguideline is people with cancer, the management strategies andsupport for patients undergoing prophylactic surgery should re-main the same as outlined in this guideline.
Overall Sexual Functioning and Satisfaction for WomenRecommendation
The Expert Panel noted that current recommendations didnot address the important role of symptom management and itseffect on the sexual response. Improved symptom management
506 © 2017 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Carter et al
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

can be associated with improvement in the domains of the sexualresponse.44 To this end, any underlying physical issue contributingto sexual dysfunction should be identified and managed.
Sexual Response for Men RecommendationsBody image is important to men’s sexual health. Issues such as
weight change, increase in breast size, disfigurement, scarring, andhair loss should also be discussed and normalized in men. Nor-malizing these issues may help men reach a new comfort level withbody image and functioning following their cancer.
In considering potential physical contributions to men’ssexual function, clinicians should check testosterone levels, even ifthe patient has a cancer that is not typically associated withhormone changes. Options for potential supplementation shouldbe discussed as indicated, including when testosterone levels arewithin normal range but the patient or clinician feels supple-mentation could have a clinical benefit and is not contraindicated.
Additional management options not covered in the CCOguideline warrant further discussion, including surgical inter-ventions for erectile dysfunction. For patients refractory to medicaltherapy with oral phosphodiesterase type 5 inhibitors and intra-cavernosal vasoactive agents, penile prosthesis implant remainsa relevant and desired option.45 Indeed, penile implants haveprovided a predictable and reliable way for restoring erections inthose patients for whommore-conservativemeasures have failed.46
Available modern models have improved durability and operabilityand are less prone to wear.46 As such, any patient with cancer inwhom more conservative measures for erectile dysfunction havefailed should be offered a discussion of the risks and benefits ofprosthesis implantation surgery. Guidelines from the AmericanUrological Association recommend that any patient consideringprosthesis implantation should be informed of the types ofprostheses available and made aware of possible adverse events,including infection, erosion, mechanical failure, and penileshortening.47 Referral to urology is appropriate for these patients.
HEALTH DISPARITIES
ASCO clinical practice guidelines represent expert recommenda-tions on the best practices in disease management to provide thehighest level of cancer care. However, many have limited access tohealth care. Racial and ethnic disparities in health care contributesignificantly to this problem in the United States. Racial/ethnicminorities suffer disproportionately from comorbidities, experi-ence more substantial obstacles to receiving care, are more likely tobe uninsured, and are at greater risk of receiving care of poorquality than other Americans.48-51 Many other patients lack accessto care because of their geographic location and distance fromappropriate treatment facilities. Awareness of these disparities inaccess to care should be considered in the context of this clini-cal practice guideline, and health care providers should strive todeliver the highest level of cancer care to these vulnerablepopulations.
Medically underserved populations may also suffer from lowgeneral literacy, low health literacy, and language and cultural
differences that can make assessment of sexual health a challenge.52
In the general population, low socioeconomic status is associatedwith a higher prevalence of sexual problems, and evidence suggeststhat cancer survivors in medically underserved populations havehigh rates of sexual inactivity and sexual dysfunction.52
Sexual and gender minority populations are another diversegroup at risk for receiving disparate care and suboptimal expe-riences with their health care journey.53 While not well studied,some evidence suggests that predictors of sexual function aftercancer do not differ by sexual orientation.10 Regardless, sexual andgender minorities should have access to culturally sensitive andcompetent support services (www.lgbtcancer.org).
Ultimately, health care providers should strive to offer dis-cussions and materials congruent with the survivor’s literacy level,cultural or religious beliefs, and sexual orientation. It is paramountfor ensuring optimum care for such vulnerable populations.
ADDITIONAL RESOURCES
More information, including a Data Supplement with a reprint ofall Interventions to Address Sexual Problems in People WithCancer guideline recommendations, a Methodology Supplement,slide sets, and clinical tools and resources, is available at www.asco.org/survivorship-guidelines and www.asco.org/guidelineswiki.Patient information is available at www.cancer.net. Visit www.asco.org/guidelineswiki to provide comments on the guideline or tosubmit new evidence.
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTSOF INTEREST
Disclosures provided by the authors are available with this article atjco.org.
AUTHOR CONTRIBUTIONS
Manuscript writing: All authorsFinal approval of manuscript: All authors
Related ASCO Guidelines
• Fertility Guideline54 (http://ascopubs.org/doi/10.1200/jco.2013.49.2678)
• Integration of Palliative Care Into Standard OncologyPractice55 (http://ascopubs.org/doi/10.1200/JCO.2016.70.1474)
• Screening, Assessment, and Care of Anxiety andDepressive Symptoms5 (http://ascopubs.org/doi/10.1200/jco.2013.52.4611)
jco.org © 2017 by American Society of Clinical Oncology 507
Sexual Problems in People With Cancer Guideline Adaptation
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

REFERENCES
1. Jemal A, Ward EM, Johnson CJ, et al: Annualreport to the nation on the status of cancer, 1975-2014, featuring survival. J Natl Cancer Inst 109:109,2017
2. White ID: Sexual difficulties after pelvic ra-diotherapy: Improving clinical management. ClinOncol (R Coll Radiol) 27:647-655, 2015
3. Zhou ES, Nekhlyudov L, Bober SL: The primaryhealth care physician and the cancer patient: Tips andstrategies for managing sexual health. Transl AndrolUrol 4:218-231, 2015
4. Hendren SK, O’Connor BI, Liu M, et al:Prevalence of male and female sexual dysfunction ishigh following surgery for rectal cancer. Ann Surg242:212-223, 2005
5. Andersen BL, DeRubeis RJ, Berman BS, et al:Screening, assessment, and care of anxiety anddepressive symptoms in adults with cancer: AnAmerican Society of Clinical Oncology guideline ad-aptation. J Clin Oncol 32:1605-1619, 2014
6. Weaver KE, Forsythe LP, Reeve BB, et al:Mental and physical health-related quality of lifeamong U.S. cancer survivors: Population estimatesfrom the 2010 National Health Interview Survey.Cancer Epidemiol Biomarkers Prev 21:2108-2117,2012
7. Flynn KE, Reese JB, Jeffery DD, et al: Patientexperiences with communication about sex duringand after treatment for cancer. Psychooncology 21:594-601, 2012
8. White ID, Faithfull S, Allan H: The re-construction of women’s sexual lives after pelvicradiotherapy: A critique of social constructionist andbiomedical perspectives on the study of femalesexuality after cancer treatment. Soc Sci Med 76:188-196, 2013
9. Bober SL, Reese JB, Barbera L, et al: How toask and what to do: A guide for clinical inquiry andintervention regarding female sexual health aftercancer. Curr Opin Support Palliat Care 10:44-54, 2016
10. Dizon DS, Suzin D, McIlvenna S: Sexual healthas a survivorship issue for female cancer survivors.Oncologist 19:202-210, 2014
11. SteadML, Brown JM, Fallowfield L, et al: Lackof communication between healthcare professionalsand women with ovarian cancer about sexual issues.Br J Cancer 88:666-671, 2003
12. Hordern AJ, Street AF: Communicating aboutpatient sexuality and intimacy after cancer: Mis-matched expectations and unmet needs. Med J Aust186:224-227, 2007
13. Forbat L, White I, Marshall-Lucette S, et al:Discussing the sexual consequences of treatment inradiotherapy and urology consultations with couplesaffected by prostate cancer. BJU Int 109:98-103,2012
14. Jaspers L, Feys F, Bramer WM, et al: Efficacyand safety of flibanserin for the treatment of hypo-active sexual desire disorder in women: A systematicreview and meta-analysis. JAMA Intern Med 176:453-462, 2016
15. Gao Z, Yang D, Yu L, et al: Efficacy and safetyof flibanserin in women with hypoactive sexual de-sire disorder: A systematic review andmeta-analysis.J Sex Med 12:2095-2104, 2015
16. Barton DL, Schroeder KCF, Banerjee T, et al:Efficacy of a biobehavioral intervention for hotflashes: A randomized controlled pilot study. Men-opause 24:774-782, 2017
17. Elkins G, Marcus J, Stearns V, et al: Ran-domized trial of a hypnosis intervention for treatmentof hot flashes among breast cancer survivors. J ClinOncol 26:5022-5026, 2008
18. Elkins GR, Fisher WI, Johnson AK, et al:Clinical hypnosis in the treatment of postmenopausalhot flashes: A randomized controlled trial. Meno-pause 20:291-298, 2013
19. The North American Menopause Society:Nonhormonal management of menopause-associated vasomotor symptoms: 2015 positionstatement of The North American Menopause So-ciety. Menopause 22:1155-1172 2015
20. Labrie F, Archer DF, KoltunW, et al: Efficacy ofintravaginal dehydroepiandrosterone (DHEA) onmoderate to severe dyspareunia and vaginal dryness,symptoms of vulvovaginal atrophy, and of the geni-tourinary syndrome of menopause. Menopause 23:243-256, 2016
21. Labrie F, Archer D, Bouchard C, et al: Serumsteroid levels during 12-week intravaginal dehy-droepiandrosterone administration. Menopause 16:897-906, 2009
22. Labrie F, Archer D, Bouchard C, et al: Intra-vaginal dehydroepiandrosterone (prasterone),a physiological and highly efficient treatment ofvaginal atrophy. Menopause 16:907-922, 2009
23. Labrie F, Archer D, Bouchard C, et al: Effect ofintravaginal dehydroepiandrosterone (prasterone) onlibido and sexual dysfunction in postmenopausalwomen. Menopause 16:923-931, 2009
24. Bruyniks N, Nappi RE, Castelo-Branco C, et al:Effect of ospemifene on moderate or severesymptoms of vulvar and vaginal atrophy. Climacteric19:60-65, 2016
25. Constantine G, Graham S, Portman DJ, et al:Female sexual function improved with ospemifene inpostmenopausal women with vulvar and vaginal at-rophy: Results of a randomized, placebo-controlledtrial. Climacteric 18:226-232, 2015
26. Cui Y, Zong H, Yan H, et al: The efficacy andsafety of ospemifene in treating dyspareunia asso-ciated with postmenopausal vulvar and vaginal at-rophy: A systematic review and meta-analysis. J SexMed 11:487-497, 2014
27. Morgan S, Davies S, Palmer S, et al: Sex,drugs, and rock ‘n’ roll: Caring for adolescents andyoung adults with cancer. J Clin Oncol 28:4825-4830,2010
28. Levine J, Canada A, Stern CJ: Fertility pres-ervation in adolescents and young adultswith cancer.J Clin Oncol 28:4831-4841, 2010
29. Shojania KG, Sampson M, Ansari MT, et al:How quickly do systematic reviews go out of date? Asurvival analysis. Ann Intern Med 147:224-233, 2007
30. Antonini G, Busetto GM, De Berardinis E, et al:Minimally invasive infrapubic inflatable penile pros-thesis implant for erectile dysfunction: Evaluation ofefficacy, satisfaction profile and complications. Int JImpot Res 28:4-8, 2016
31. Gentile G, Franceschelli A, Massenio P, et al:Patient’s satisfaction after 2-piece inflatable penileprosthesis implantation: An Italian multicentric study.Arch Ital Urol Androl 88:1-3, 2016
32. Egydio PH, Kuehhas FE: Penile lengtheningand widening without grafting according to a modi-fied ‘sliding’ technique. BJU Int 116:965-972, 2015
33. Martınez-Salamanca JI, Espinos EL, MoncadaI, et al: Management of end-stage erectile dysfunc-tion and stress urinary incontinence after radicalprostatectomy by simultaneous dual implantationusing a single trans-scrotal incision: Surgical
technique and outcomes. Asian J Androl 17:792-796,2015
34. Yiou R, Binhas M: Combined implantation ofa penile prosthesis and adjustable continence ther-apy ProACT in patients with erectile dysfunction andurinary incontinence after radical prostatectomy:Results of a prospective pilot study. J Sex Med 12:2481-2484, 2015
35. Dieckmann KP, Anheuser P, Schmidt S, et al:Testicular prostheses in patients with testicularcancer —acceptance rate and patient satisfaction.BMC Urol 15:16, 2015
36. Catanzariti F, Polito B, Polito M: Testicularprosthesis: Patient satisfaction and sexual dysfunc-tions in testis cancer survivors. Arch Ital Urol Androl88:186-188, 2016
37. Flynn KE, Lindau ST, Lin L, et al: Developmentand validation of a single-item screener for self-reporting sexual problems in U.S. adults. J Gen In-tern Med 30:1468-1475, 2015
38. Hatzichristou D, Rosen RC, Derogatis LR, et al:Recommendations for the clinical evaluation of menand women with sexual dysfunction. J Sex Med 7:337-348, 2010
39. McGahuey CA, Gelenberg AJ, Laukes CA,et al: The Arizona Sexual Experience Scale (ASEX):Reliability and validity. J Sex Marital Ther 26:25-40,2000
40. Rosen R, Brown C, Heiman J, et al: The Fe-male Sexual Function Index (FSFI): A multidimen-sional self-report instrument for the assessment offemale sexual function. J Sex Marital Ther 26:191-208, 2000
41. Cappelleri JC, Rosen RC: The Sexual HealthInventory for Men (SHIM): A 5-year review of re-search and clinical experience. Int J Impot Res 17:307-319, 2005
42. Abraham L, Symonds T, Morris MF: Psycho-metric validation of a sexual quality of life question-naire for use in men with premature ejaculation orerectile dysfunction. J Sex Med 5:595-601, 2008
43. DuHamel K, Schuler T, Nelson C, et al: Thesexual health of female rectal and anal cancer sur-vivors: Results of a pilot randomized psycho-educational intervention trial. J Cancer Surviv 10:553-563, 2016
44. Ganz PA, Greendale GA, Petersen L, et al:Managing menopausal symptoms in breast cancersurvivors: Results of a randomized controlled trial.J Natl Cancer Inst 92:1054-1064, 2000
45. Chung E: Penile prosthesis implant: Scientificadvances and technological innovations over the lastfour decades. Transl Androl Urol 6:37-45, 2017
46. Mulcahy JJ: The development of modernpenile implants. Sex Med Rev 4:177-189, 2016
47. Montague DK, Jarow JP, Broderick GA, et al:Chapter 1: The management of erectile dysfunction:An AUA update. J Urol 174:230-239, 2005
48. Howlader N, Noone AM, Krapcho M, et al:SEER cancer statistics review, 1975-2013, 2016.http://seer.cancer.gov/csr/1975_2013
49. Mead H, Cartwright-Smith L, Jones K, et al:Racial and Ethnic Disparities in U.S. Health Care: AChartbook. New York, NY, The CommonwealthFund, 2008
50. American Cancer Society: Cancer facts andfigures for African Americans 2016-2018, 2016. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/cancer-facts-and-figures-for-african-americans/cancer-facts-and-figures-for-african-americans-2016-2018.pdf
51. US Cancer Statistics Working Group: UnitedStates Cancer Statistics: 1999-2014 Cancer
508 © 2017 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Carter et al
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

Incidence and Mortality Data, 2017. https://www.cdc.gov/uscs
52. Bradford A, Fellman B, Urbauer D, et al: As-sessment of sexual activity and dysfunction inmedically underserved women with gynecologiccancers. Gynecol Oncol 139:134-140, 2015
53. Griggs J, Maingi S, Blinder V, et al: AmericanSociety of Clinical Oncology position statement:Strategies for reducing cancer health disparitiesamong sexual and genderminority populations. J ClinOncol 35:2203-2208, 2017
54. Loren AW, Mangu PB, Beck LN, et al: Fertilitypreservation for patients with cancer: American So-ciety of Clinical Oncology clinical practice guidelineupdate. J Clin Oncol 31:2500-2510, 2013
55. Ferrell BR, Temel JS, Temin S, et al: In-tegration of palliative care into standard oncologycare: American Society of Clinical Oncology clinicalpractice guideline update. J Clin Oncol 35:96-112,2017
56. Kalaitzi C, Papadopoulos VP, Michas K, et al:Combined brief psychosexual intervention aftermastectomy: Effects on sexuality, body image, andpsychological well-being. J Surg Oncol 96:235-240,2007
57. Jun EY, Kim S, Chang SB, et al: The effect ofa sexual life reframing program on marital intimacy,body image, and sexual function among breastcancer survivors. Cancer Nurs 34:142-149, 2011
58. Mathias C, Cardeal Mendes CM, Ponde deSena E, et al: An open-label, fixed-dose study ofbupropion effect on sexual function scores in womentreated for breast cancer. Ann Oncol 17:1792-1796,2006
59. Brotto LA, Erskine Y, Carey M, et al: A briefmindfulness-based cognitive behavioral interventionimproves sexual functioning versus wait-list controlin women treated for gynecologic cancer. GynecolOncol 125:320-325, 2012
60. Schroder M, Mell LK, Hurteau JA, et al: Clitoraltherapy device for treatment of sexual dysfunction inirradiated cervical cancer patients. Int J Radiat OncolBiol Phys 61:1078-1086, 2005
61. Hersch J, Juraskova I, Price M, et al: Psy-chosocial interventions and quality of life in gynae-cological cancer patients: A systematic review.Psychooncology 18:795-810, 2009
62. Scott JL, Kayser K: A review of couple-basedinterventions for enhancing women’s sexual ad-justment and body image after cancer. Cancer J 15:48-56, 2009
63. Baucom DH, Porter LS, Kirby JS, et al: Acouple-based intervention for female breast cancer.Psychooncology 18:276-283, 2009
64. Sharif F, Abshorshori N, Tahmasebi S, et al:The effect of peer-led education on the life quality ofmastectomy patients referred to breast cancer-clinics in Shiraz, Iran 2009. Health Qual Life Out-comes 8:74, 2010
65. Duijts SF, van BeurdenM,Oldenburg HS, et al:Efficacy of cognitive behavioral therapy and physicalexercise in alleviating treatment-induced meno-pausal symptoms in patients with breast cancer:Results of a randomized, controlled, multicenter trial.J Clin Oncol 30:4124-4133, 2012
66. Yang EJ, Lim JY, Rah UW, et al: Effect ofa pelvic floor muscle training program on gynecologiccancer survivors with pelvic floor dysfunction: Arandomized controlled trial. Gynecol Oncol 125:705-711, 2012
67. Decker CL, Pais S, Miller KD, et al: A briefintervention to minimize psychosexual morbidity in
dyads coping with breast cancer. Oncol Nurs Forum39:176-185, 2012
68. Classen CC, Chivers ML, Urowitz S, et al:Psychosexual distress in women with gynecologiccancer: A feasibility study of an online support group.Psychooncology 22:930-935, 2013
69. Taylor S, Harley C, Ziegler L, et al: In-terventions for sexual problems following treatmentfor breast cancer: A systematic review. BreastCancer Res Treat 130:711-724, 2011
70. Miles T, Johnson N: Vaginal dilator therapy forwomen receiving pelvic radiotherapy. Cochrane Da-tabase Syst Rev (9):CD007291, 2010
71. Johnson N, Miles TP, Cornes P: Dilating thevagina to prevent damage from radiotherapy: Sys-tematic review of the literature. BJOG 117:522-531,2010
72. Rowland JH,Meyerowitz BE, Crespi CM, et al:Addressing intimacy and partner communication af-ter breast cancer: A randomized controlled groupintervention. Breast Cancer Res Treat 118:99-111,2009
73. Marcus AC, Garrett KM, Cella D, et al: Cantelephone counseling post-treatment improve psy-chosocial outcomes among early stage breast cancersurvivors? Psychooncology 19:923-932, 2010
74. Schover LR, Yuan Y, Fellman BM, et al: Effi-cacy trial of an Internet-based intervention for cancer-related female sexual dysfunction. J Natl ComprCanc Netw 11:1389-1397, 2013
75. Sismondi P, Kimmig R, Kubista E, et al: Effectsof tibolone on climacteric symptoms and quality oflife in breast cancer patients—data from LIBERATEtrial. Maturitas 70:365-372, 2011
76. Schover LR, Rhodes MM, Baum G, et al:Sisters Peer Counseling in Reproductive Issues AfterTreatment (SPIRIT): A peer counseling program toimprove reproductive health among African Ameri-can breast cancer survivors. Cancer 117:4983-4992,2011
77. Ayaz S, Kubilay G: Effectiveness of thePLISSIT model for solving the sexual problems ofpatients with stoma. J Clin Nurs 18:89-98, 2009
78. Juraskova I, Jarvis S, Mok K, et al: The ac-ceptability, feasibility, and efficacy (phase I/II study)of the OVERcome (Olive Oil, Vaginal Exercise, andMoisturizeR) intervention to improve dyspareuniaand alleviate sexual problems in women with breastcancer. J Sex Med 10:2549-2558, 2013
79. Reid R, Abramson BL, Blake J, et al: Managingmenopause. J Obstet Gynaecol Can 36:830-833,2014
80. North American Menopause Society: The2012 hormone therapy position statement of: TheNorth American Menopause Society. Menopause19:257-271, 2012
81. The North American Menopause Society:Management of symptomatic vulvovaginal atrophy:2013 position statement of The North AmericanMenopause Society. Menopause 20:888-902, 2013
82. Lee YK, Chung HH, Kim JW, et al: Vaginal pH-balanced gel for the control of atrophic vaginitisamong breast cancer survivors: A randomized con-trolled trial. Obstet Gynecol 117:922-927, 2011
83. Law E, Kelvin JF, Thom B, et al: Prospectivestudy of vaginal dilator use adherence and efficacyfollowing radiotherapy. Radiother Oncol 116:149-155, 2015
84. Witherby S, Johnson J, Demers L, et al:Topical testosterone for breast cancer patients withvaginal atrophy related to aromatase inhibitors: Aphase I/II study. Oncologist 16:424-431, 2011
85. Candy B, Jones L, Vickerstaff V, et al: In-terventions for sexual dysfunction following treat-ments for cancer in women. Cochrane Database SystRev 2:CD005540, 2016
86. Montorsi F, McCullough A: Efficacy of silde-nafil citrate inmenwith erectile dysfunction followingradical prostatectomy: A systematic review of clinicaldata. J Sex Med 2:658-667, 2005
87. Park SY, Choi GS, Park JS, et al: Efficacy andsafety of udenafil for the treatment of erectile dys-function after total mesorectal excision of rectalcancer: A randomized, double-blind, placebo-controlled trial. Surgery 157:64-71, 2015
88. Ilic D, Hindson B, Duchesne G, et al: A rand-omised, double-blind, placebo-controlled trial ofnightly sildenafil citrate to preserve erectile functionafter radiation treatment for prostate cancer. J MedImaging Radiat Oncol 57:81-88, 2013
89. Watkins Bruner D, James JL, Bryan CJ, et al:Randomized, double-blinded, placebo-controlledcrossover trial of treating erectile dysfunction withsildenafil after radiotherapy and short-term androgendeprivation therapy: Results of RTOG 0215. J SexMed 8:1228-1238, 2011
90. Incrocci L, Hop WC, Slob AK: Efficacy of sil-denafil in an open-label study as a continuation ofa double-blind study in the treatment of erectiledysfunction after radiotherapy for prostate cancer.Urology 62:116-120, 2003
91. Incrocci L, Slagter C, Slob AK, et al: A ran-domized, double-blind, placebo-controlled, cross-over study to assess the efficacy of tadalafil (Cialis)in the treatment of erectile dysfunction followingthree-dimensional conformal external-beam radio-therapy for prostatic carcinoma. Int J Radiat OncolBiol Phys 66:439-444, 2006
92. Incrocci L, Slob AK, Hop WC: Tadalafil (Cialis)and erectile dysfunction after radiotherapy for pros-tate cancer: An open-label extension of a blinded trial.Urology 70:1190-1193, 2007
93. Harrington C, Campbell G, Wynne C, et al:Randomised, placebo-controlled, crossover trial ofsildenafil citrate in the treatment of erectile dys-function following external beam radiation treatmentof prostate cancer. J Med Imaging Radiat Oncol 54:224-228, 2010
94. Pace G, Del Rosso A, Vicentini C: Penile re-habilitation therapy following radical prostatectomy.Disabil Rehabil 32:1204-1208, 2010
95. Bannowsky A, Schulze H, van der Horst C,et al: Recovery of erectile function after nerve-sparingradical prostatectomy: Improvement with nightlylow-dose sildenafil. BJU Int 101:1279-1283, 2008
96. Mosbah A, El Bahnasawy M, Osman Y, et al:Early versus late rehabilitation of erectile functionafter nerve-sparing radical cystoprostatectomy: Aprospective randomized study. J Sex Med 8:2106-2111, 2011
97. McCullough AR, Levine LA, Padma-Nathan H:Return of nocturnal erections and erectile functionafter bilateral nerve-sparing radical prostatectomy inmen treated nightly with sildenafil citrate: Sub-analysis of a longitudinal randomized double-blindplacebo-controlled trial. J Sex Med 5:476-484, 2008
98. Montorsi F, Brock G, Stolzenburg JU, et al:Effects of tadalafil treatment on erectile functionrecovery following bilateral nerve-sparing radicalprostatectomy: A randomised placebo-controlledstudy (REACTT). Eur Urol 65:587-596, 2014
99. Ricardi U, Gontero P, Ciammella P, et al: Ef-ficacy and safety of tadalafil 20 mg on demand vs.tadalafil 5 mg once-a-day in the treatment of post-radiotherapy erectile dysfunction in prostate cancer
jco.org © 2017 by American Society of Clinical Oncology 509
Sexual Problems in People With Cancer Guideline Adaptation
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

men: A randomized phase II trial. J Sex Med 7:2851-2859, 2010100. Pavlovich CP, Levinson AW, Su LM, et al:
Nightly vs on-demand sildenafil for penile re-habilitation after minimally invasive nerve-sparingradical prostatectomy: Results of a randomizeddouble-blind trial with placebo. BJU Int 112:844-851,2013101. Montorsi F, Brock G, Lee J, et al: Effect of
nightly versus on-demand vardenafil on recovery oferectile function in men following bilateral nerve-sparing radical prostatectomy. Eur Urol 54:924-931,2008102. Canada AL, Neese LE, Sui D, et al: Pilot in-
tervention to enhance sexual rehabilitation for cou-ples after treatment for localized prostate carcinoma.Cancer 104:2689-2700, 2005103. Schover LR, Canada AL, Yuan Y, et al: A
randomized trial of internet-based versus traditionalsexual counseling for couples after localized prostatecancer treatment. Cancer 118:500-509, 2012104. Kohler TS, Pedro R, Hendlin K, et al: A pilot
study on the early use of the vacuum erection deviceafter radical retropubic prostatectomy. BJU Int 100:858-862, 2007105. Zelefsky MJ, Shasha D, Branco RD, et al:
Prophylactic sildenafil citrate improves select as-pects of sexual function in men treated with radio-therapy for prostate cancer. J Urol 192:868-874, 2014106. Engel JD: Effect on sexual function of a vac-
uum erection device post-prostatectomy. Can J Urol18:5721-5725, 2011107. Lin YH, Yu TJ, Lin VC, et al: Effects of early
pelvic-floor muscle exercise for sexual dysfunction inradical prostatectomy recipients. Cancer Nurs 35:106-114, 2012108. Titta M, Tavolini IM, Dal Moro F, et al: Sexual
counseling improved erectile rehabilitation after non-nerve-sparing radical retropubic prostatectomy orcystectomy—results of a randomized prospectivestudy. J Sex Med 3:267-273, 2006109. Cormie P, Newton RU, Taaffe DR, et al: Ex-
ercise maintains sexual activity in men undergoingandrogen suppression for prostate cancer: A ran-domized controlled trial. Prostate Cancer ProstaticDis 16:170-175, 2013110. Hanisch LJ, Bryan CJ, James JL, et al: Impact
of sildenafil on marital and sexual adjustment in pa-tients and their wives after radiotherapy and short-term androgen suppression for prostate cancer:Analysis of RTOG 0215. Support Care Cancer 20:2845-2850, 2012111. Nishizawa Y, Ito M, Saito N, et al: Male sexual
dysfunction after rectal cancer surgery. Int J Co-lorectal Dis 26:1541-1548, 2011112. Salonia A, Gallina A, Zanni G, et al: Acceptance
of and discontinuation rate from erectile dysfunctionoral treatment in patients following bilateral nerve-sparing radical prostatectomy. Eur Urol 53:564-570,2008113. Reese JB, Porter LS, Somers TJ, et al: Pilot
feasibility study of a telephone-based couples in-tervention for physical intimacy and sexual concernsin colorectal cancer. J Sex Marital Ther 38:402-417,2012114. Dalkin BL, Christopher BA: Preservation of
penile length after radical prostatectomy: Early in-tervention with a vacuum erection device. Int J ImpotRes 19:501-504, 2007115. Irani J, Salomon L, Oba R, et al: Efficacy of
venlafaxine, medroxyprogesterone acetate, and cy-proterone acetate for the treatment of vasomotor hotflushes in men taking gonadotropin-releasing
hormone analogues for prostate cancer: A double-blind, randomised trial. Lancet Oncol 11:147-154,2010116. Ramsawh HJ, Morgentaler A, Covino N, et al:
Quality of life following simultaneous placement ofpenile prosthesis with radical prostatectomy. J Urol174:1395-1398, 2005117. Pahlajani G, Raina R, Jones JS, et al: Early
intervention with phosphodiesterase-5 inhibitors af-ter prostate brachytherapy improves subsequenterectile function. BJU Int 106:1524-1527, 2010118. Pugh TJ, Mahmood U, Swanson DA, et al:
Sexual potency preservation and quality of life afterprostate brachytherapy and low-dose tadalafil. Bra-chytherapy 14:160-165, 2015119. Fujioka H, Ishimura T, Sakai Y, et al: Erectile
function after brachytherapy with external beam ra-diation for prostate cancer. Arch Androl 50:295-301,2004120. Ogura K, Ichioka K, Terada N, et al: Role of
sildenafil citrate in treatment of erectile dysfunctionafter radical retropubic prostatectomy. Int J Urol 11:159-163, 2004121. Schiff JD, Bar-Chama N, Cesaretti J, et al:
Early use of a phosphodiesterase inhibitor afterbrachytherapy restores and preserves erectile func-tion. BJU Int 98:1255-1258, 2006122. Mulhall JP, Parker M, Waters BW, et al: The
timing of penile rehabilitation after bilateral nerve-sparing radical prostatectomy affects the recoveryof erectile function. BJU Int 105:37-41, 2010123. Megas G, Papadopoulos G, Stathouros G,
et al: Comparison of efficacy and satisfaction profile,between penile prosthesis implantation and oralPDE5 inhibitor tadalafil therapy, in men with nerve-sparing radical prostatectomy erectile dysfunction.BJU Int 112:E169-E176, 2013124. Menard J, Tremeaux JC, Faix A, et al: Erectile
function and sexual satisfaction before and afterpenile prosthesis implantation in radical prostatec-tomy patients: A comparison with patients withvasculogenic erectile dysfunction. J Sex Med 8:3479-3486, 2011125. Mydlo JH, Viterbo R, Crispen P: Use of com-
bined intracorporal injection and a phosphodiesterase-5inhibitor therapy for men with a suboptimal responseto sildenafil and/or vardenafil monotherapy after rad-ical retropubic prostatectomy. BJU Int 95:843-846,2005126. Natali A, Masieri L, Lanciotti M, et al: A
comparison of different oral therapies versus notreatment for erectile dysfunction in 196 radicalnerve-sparing radical prostatectomy patients. Int JImpot Res 27:1-5, 2015127. Ohebshalom M, Parker M, Guhring P, et al:
The efficacy of sildenafil citrate following radiationtherapy for prostate cancer: Temporal consider-ations. J Urol 174:258-262, 2005128. Raina R, Agarwal A, Allamaneni SS, et al:
Sildenafil citrate and vacuum constriction devicecombination enhances sexual satisfaction in erectiledysfunction after radical prostatectomy. Urology 65:360-364, 2005129. Raina R, Agarwal A, Goyal KK, et al: Long-term
potency after iodine-125 radiotherapy for prostatecancer and role of sildenafil citrate. Urology 62:1103-1108, 2003130. Raina R, Pahlajani G, Agarwal A, et al: The early
use of transurethral alprostadil after radical prosta-tectomy potentially facilitates an earlier return oferectile function and successful sexual activity. BJUInt 100:1317-1321, 2007
131. Balbontin FG, Moreno SA, Bley E, et al: Long-acting testosterone injections for treatment of tes-tosterone deficiency after brachytherapy for prostatecancer. BJU Int 114:125-130, 2014132. Chisholm KE, McCabe MP, Wootten AC, et al:
Review: Psychosocial interventions addressing sex-ual or relationship functioning in men with prostatecancer. J Sex Med 9:1246-1260, 2012133. Porter LS, Keefe FJ, Baucom DH, et al:
Partner-assisted emotional disclosure for patientswith gastrointestinal cancer: Results from a ran-domized controlled trial. Cancer 115: 4326-4338,2009 (suppl 18)134. Porter LS, Keefe FJ, Baucom DH, et al:
Partner-assisted emotional disclosure for patientswith GI cancer: 8-week follow-up and processesassociated with change. Support Care Cancer 20:1755-1762, 2012135. Chambers SK, Schover L, Halford K, et al:
ProsCan for Couples: A feasibility study for evaluatingpeer support within a controlled research design.Psychooncology 22:475-479, 2013136. Collins AL, Love AW, Bloch S, et al: Cognitive
existential couple therapy for newlydiagnosedprostatecancer patients and their partners: A descriptive pilotstudy. Psychooncology 22:465-469, 2013137. Lassen B, Gattinger H, Saxer S: A systematic
review of physical impairments following radicalprostatectomy: Effect of psychoeducational in-terventions. J Adv Nurs 69:2602-2612, 2013138. Molton IR, Siegel SD, Penedo FJ, et al: Pro-
moting recovery of sexual functioning after radicalprostatectomy with group-based stress manage-ment: The role of interpersonal sensitivity.J Psychosom Res 64:527-536, 2008139. Siddons HM, Wootten AC, Costello AJ: A
randomised, wait-list controlled trial: Evaluation ofa cognitive-behavioural group intervention on psycho-sexual adjustment for men with localised prostatecancer. Psychooncology 22:2186-2192, 2013140. Lee IH, Sadetsky N, Carroll PR, et al: The
impact of treatment choice for localized prostatecancer on response to phosphodiesterase inhibitors.J Urol 179:1072-1076, 2008; discussion 1076141. Vitolins MZ, Griffin L, Tomlinson WV, et al:
Randomized trial to assess the impact of venlafaxineand soy protein on hot flashes and quality of life inmen with prostate cancer. J Clin Oncol 31:4092-4098, 2013142. Loprinzi CL, Dueck AC, Khoyratty BS, et al: A
phase III randomized, double-blind, placebo-controlledtrial of gabapentin in the management of hot flashes inmen (N00CB). Ann Oncol 20:542-549, 2009143. Frisk J, Spetz AC, Hjertberg H, et al: Two
modes of acupuncture as a treatment for hot flushesin men with prostate cancer—a prospective multi-center study with long-term follow-up. Eur Urol 55:156-163, 2009144. Moraska AR, Atherton PJ, Szydlo DW, et al:
Gabapentin for the management of hot flashes inprostate cancer survivors: A longitudinal continuationStudy-NCCTG Trial N00CB. J Support Oncol 8:128-132, 2010145. Ashamalla H, Jiang ML, Guirguis A, et al:
Acupuncture for the alleviation of hot flashes in mentreated with androgen ablation therapy. Int J RadiatOncol Biol Phys 79:1358-1363, 2011146. Beer TM, Benavides M, Emmons SL, et al:
Acupuncture for hot flashes in patients with prostatecancer. Urology 76:1182-1188, 2010147. Harding C, Harris A, Chadwick D: Auricular
acupuncture: A novel treatment for vasomotorsymptoms associated with luteinizing-hormone
510 © 2017 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Carter et al
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

releasing hormone agonist treatment for prostatecancer. BJU Int 103:186-190, 2009148. Loprinzi CL, Barton DL, Carpenter LA, et al:
Pilot evaluation of paroxetine for treating hot flashesin men. Mayo Clin Proc 79:1247-1251, 2004149. Naoe M, Ogawa Y, Shichijo T, et al: Pilot
evaluation of selective serotonin reuptake inhibi-tor antidepressants in hot flash patients under
androgen-deprivation therapy for prostate can-cer. Prostate Cancer Prostatic Dis 9:275-278,2006150. Vandecasteele K, Ost P, Oosterlinck W, et al:
Evaluation of the efficacy and safety of Salvia offi-cinalis in controlling hot flashes in prostate cancerpatients treated with androgen deprivation. Phyt-other Res 26:208-213, 2012
151. Carter J, Stabile C, Seidel B, et al: Vaginal andsexual health treatment strategies within a femalesexual medicine program for cancer patients andsurvivors. J Cancer Surviv 11:274-283, 2017152. Goetsch MF, Lim JY, Caughey AB: A practical
solution for dyspareunia in breast cancer survivors: Arandomized controlled trial. J Clin Oncol 33:3394-3400, 2015
AffiliationsJeanne Carter, Katherine DuHamel, and Shari Goldfarb, Memorial Sloan Kettering Cancer Center, New York; Michael A.
Diefenbach, Northwell Health, Manhasset, NY; Christina Lacchetti, American Society of Clinical Oncology, Alexandria; Sage Bolte,Inova, Fairfax, VA; Barbara L. Andersen, Ohio State University, Columbus, OH;Debra L. Barton, University ofMichigan, Ann Arbor, MI;Shari Damast, Yale School of Medicine, New Haven, CT; Judith Florendo, Florendo Physical Therapy, Chicago; Sigrun Hallmeyer,Oncology Specialists SC, Park Ridge, IL; Patricia A. Ganz, University of California, Los Angeles, CA; David M. Kushner, University ofWisconsin, Madison, WI; and Julia H. Rowland, National Cancer Institute, Bethesda, MD.
n n n
jco.org © 2017 by American Society of Clinical Oncology 511
Sexual Problems in People With Cancer Guideline Adaptation
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Interventions to Address Sexual Problems in People With Cancer: American Society of Clinical Oncology Clinical Practice Guideline Adaptation ofCancer Care Ontario Guideline
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated. Relationships areself-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For moreinformation about ASCO’s conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Jeanne CarterNo relationship to disclose
Christina LacchettiNo relationship to disclose
Barbara L. AndersenNo relationship to disclose
Debra L. BartonResearch Funding: Merck Foundation
Sage BolteNo relationship to disclose
Shari DamastNo relationship to disclose
Michael A. DiefenbachNo relationship to disclose
Katherine DuHamelNo relationship to disclose
Judith FlorendoNo relationship to disclose
Patricia A. GanzLeadership: Intrinsic LifeSciences (I)Stock or Other Ownership: Xenon Pharmaceuticals (I), IntrinsicLifeSciences (I), Silarus Therapeutics (I), Merganser Biotech (I), TEVAPharmaceuticals Industries, Novartis, Merck, Johnson & Johnson, Pfizer,GlaxoSmithKline, Abbott LaboratoriesHonoraria: Biogen (I)Consulting or Advisory Role: Keryx Biopharmaceuticals (I), MerganserBiotech (I), Silarus Therapeutics (I), InformedDNA, Vifor Pharma (I), EliLillySpeakers’ Bureau: La Jolla Pharmaceutical Company (I)Research Funding: Keryx Biopharmaceuticals (I)Patents, Royalties, Other Intellectual Property: Related to ironmetabolism and the anemia of chronic disease (I), Up-to-Date royalties forsection editor on survivorshipTravel, Accommodations, Expenses: Intrinsic LifeSciences (I), KeryxBiopharmaceuticals (I)
Shari GoldfarbConsulting or Advisory Role: Sermonix Pharmaceuticals, AMAGPharmaceuticals, Procter & Gamble, Adgero BiopharmaceuticalsResearch Funding: Paxman, Valeant Pharmaceuticals International
Sigrun HallmeyerEmployment: Oncology Specialists SC, Advocate Medical GroupLeadership: Oncology Specialists SC, Advocate Lutheran General HospitalHonoraria: Bristol-Myers Squibb, PfizerConsulting or Advisory Role:Cardinal Health, Bristol-Myers Squibb, KBLBiologicsSpeakers’ Bureau: Bristol-Myers Squibb, PfizerResearch Funding: Russell Research Institute (Inst)Travel, Accommodations, Expenses: Bristol-Myers Squibb, CardinalHealth
David M. KushnerNo relationship to disclose
Julia H. RowlandNo relationship to disclose
© 2017 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Carter et al
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.

Acknowledgment
The Expert Panel thanks Tara Henderson and Eric Singer and the Clinical Practice Guidelines Committee for their thoughtful reviewsand insightful comments on this guideline adaptation.
Appendix
Table A1. Interventions to Address Sexual Problems in PeopleWith Cancer: ASCO Clinical Practice Guideline Adaptation of Cancer Care Ontario Guideline Expert PanelMembership
Name Affiliation
Julia H. Rowland, PhD, co-chair National Cancer InstituteDevelopmental Psychology
Jeanne Carter, PhD, co-chair Memorial Sloan Kettering Cancer CenterClinical Psychology
Barbara L. Andersen, PhD Ohio State UniversityClinical Psychology
Debra L. Barton, PhD University of MichiganNursing
Shari Damast, MD Yale School of MedicineRadiation Oncology
Michael A. Diefenbach, PhD Northwell HealthBehavioral Science
Katherine DuHamel, PhD Memorial Sloan Kettering Cancer CenterClinical Psychology
Judith Florendo, DPT Florendo Physical TherapyPhysical Therapy
Patricia A. Ganz, MD University of CaliforniaBreast Medical Oncology
Shari Goldfarb, MD Memorial Sloan Kettering Cancer CenterBreast Medical Oncology
David M. Kushner, MD University of WisconsinGynecologic Oncology
Sigrun Hallmeyer, MD Oncology Specialists SCMedical Oncology, Practice Guidelines Implementation NetworkRepresentative
Sage Bolte, PhD InovaPatient Representative
Christina Lacchetti American Society of Clinical OncologyStaff/Health Research Methodologist
jco.org © 2017 by American Society of Clinical Oncology
Sexual Problems in People With Cancer Guideline Adaptation
Downloaded from ascopubs.org by 97.127.187.121 on May 5, 2018 from 097.127.187.121Copyright © 2018 American Society of Clinical Oncology. All rights reserved.
Related Documents











