Alzheimer’s, the caregiving experience, and helping the caregiver

Alzheimer’s, the caregiving experience, and helping the caregiver.
Dec 28, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Alzheimer’s, the caregiving experience, and helping the caregiver
Myth #1:Alzheimer’s is normal aging.
Dementia — "a loss of intellectual abilities of sufficient severity to interfere with functioning….The loss involves memory, judgment, abstract thought, and a variety of other higher cortical functions". (DSM IV, 1994).
Alzheimer's disease — Most prevalent form of dementia. Alois Alzheimer, a German neurologist, discovered in 1907 neurofibrillary tangles and neuritic plagues in the autopsied brain of a 51 year old patient who demonstrated demented behavior.
Because of the patient's age Alzheimer's disease was thought of as presenile dementia. Until 35 years ago it was considered rare.

Alzheimers was referred to as Primary Dementia in the DSM.
Different from delirium — literally means "off the track" (de=“off”; lira=“the ridge between furrows”).Not due to arteriosclerosis -- "hardening of the arteries" — not cause of most dementias.Not multi-infarct dementia (MID) caused by circulatory problems and clots lodging in the brain.Not Lewy-body or Parkinsonian dementia

Not Creutzfeld-Jakob disease – “Kuru”, a strange affliction of the Fore of New Guinea.
Not “dementia pugilistica”
All of these afflictions and forms of dementia are, like SDAT, not normal aging!!!!
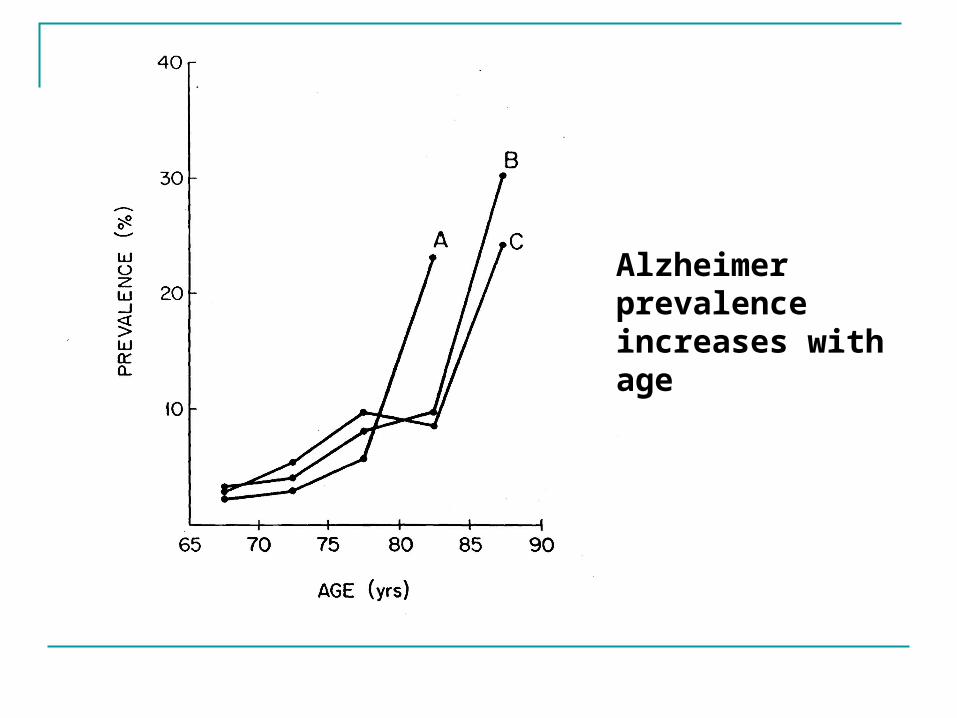
Alzheimer prevalence increases with age

Assessment of Dementia
1. Differential diagnosis
2. Functional assessment and care needs
3. Evaluation of the caregiver
Differential diagnosis of SDAT
lnclusionarv evidence
Exclusionary evidence
Why do we need both inclusionary and exclusionary evidence in disorders like SDAT?

What is types of evaluations or tests are included in the differential diagnosis process?

Conditions considered in the Differential Diagnosis of SDAT:
1. Diffuse diseases of the CNS, e.g., other dementias (Lewy-body, Parkinson's, etc.), Huntington's chorea, epilepsies.
2. Metabolic disorders, e.g., liver and kidney failure, hypo- and
hyperglycemia.
3. Vascular disorders, e.g., MID, hypoxia, anoxia.
3. Brain tumors.

5. Trauma and hematomas.
6. Infections, e.g., meningitis, encephalitis, CJD, neurosyphilis.
7. Dificiency disorders, e.g., Korsakoff's, B12 dificiency, folate dificiency.
8. Intoxications, e.g., alcohol, lead, mercury.
9. Other mental illness, e.g., MS.
Exclusionary evidence – “Rule outs” (see previous slide)
Inclusionary evidence:
1. History of cognitive deterioration
2. Presently unable to function
3. Memory impairment
4. At least one of the following:
a.Impaired abstract thinkingb.Impaired judgementc.Personality change

Myth #2:Alzheimer’s is hard to diagnose accurately.
Dementia is diagnosable with 90% accuracy. That is substantially better than many medical diagnoses for which there are no sensitive and specific, e.g., most viruses, depression, etc.
Autopsy provides sensitive and, for the most part, specific markers for SDAT. What are they?
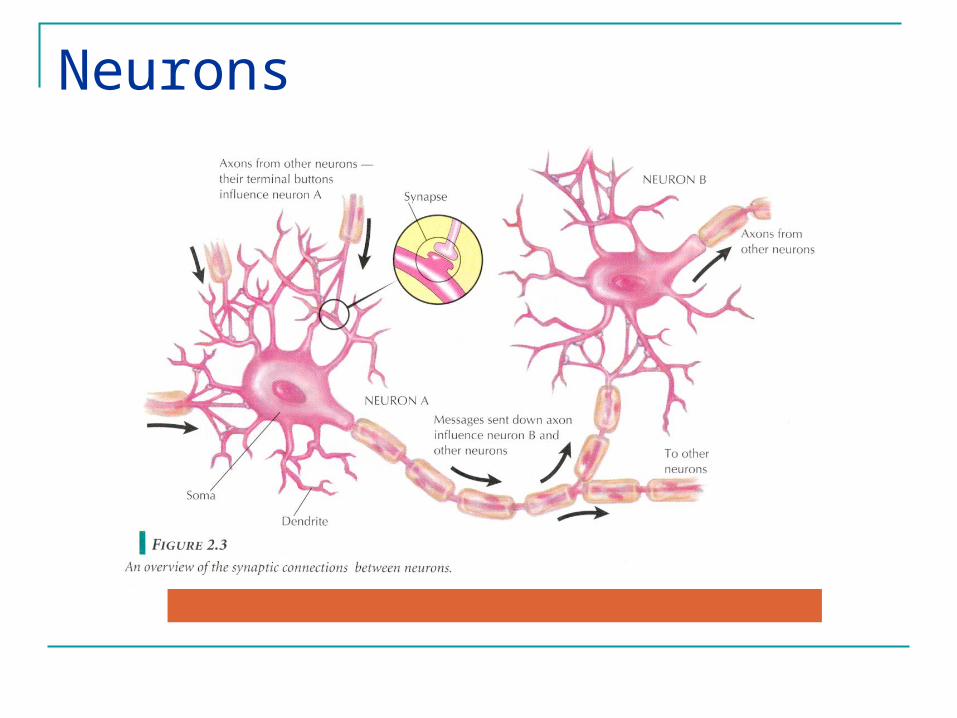
Neurons

Plaques and Tangles

Formation of Plaques

Neuritic plaques

Formation of Tangles
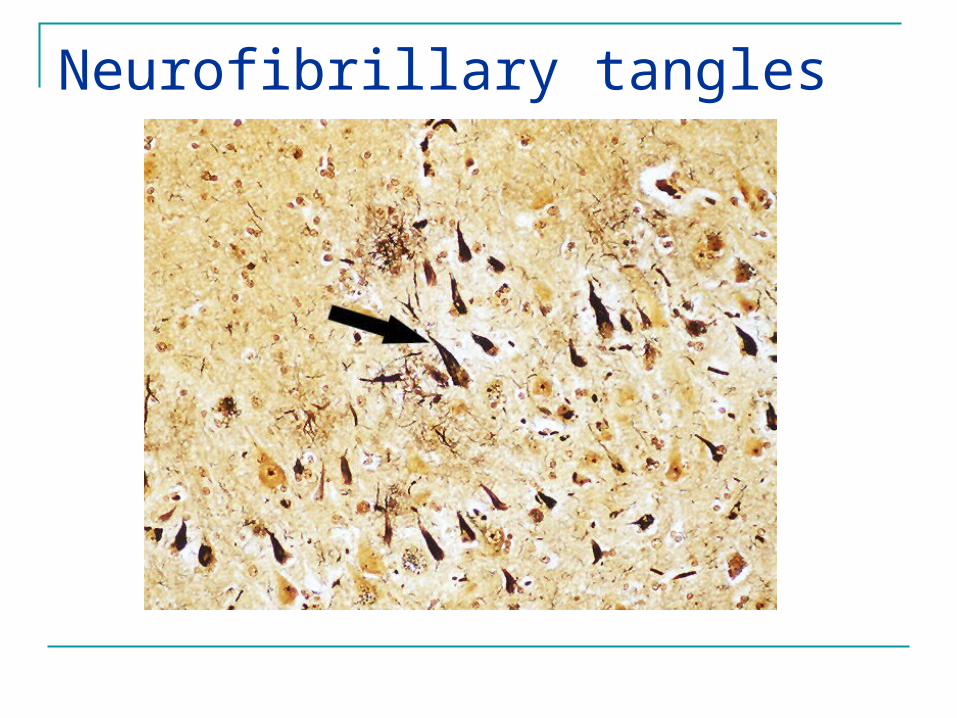
Neurofibrillary tangles
Myth #3:
Dementia is not treatable.
Basic notions of treatment:
"Excess disabilities” and the “Rule of Halves”
Effects of SDAT extend beyond the patient. Treatment targets functioning and extends beyond the patient.

Questions we will address today
1. In what ways do we change with SDAT?
2. Are these abnormal SDAT changes associated with functional changes?
3. Can we prevent or diminish these functional changes in the face of predictable abnormal SDATchanges?

Basic theme:1. Diminished capacity associated with
progression of SDAT
2. Loss of functioning at any point not be a necessary consequence of diminished capacity associated with SDAT.
3. Selection, optimization, and compensation (SOC) can transform activity and maintain functioning.
4. There are limits to maintenance of function in SDAT.









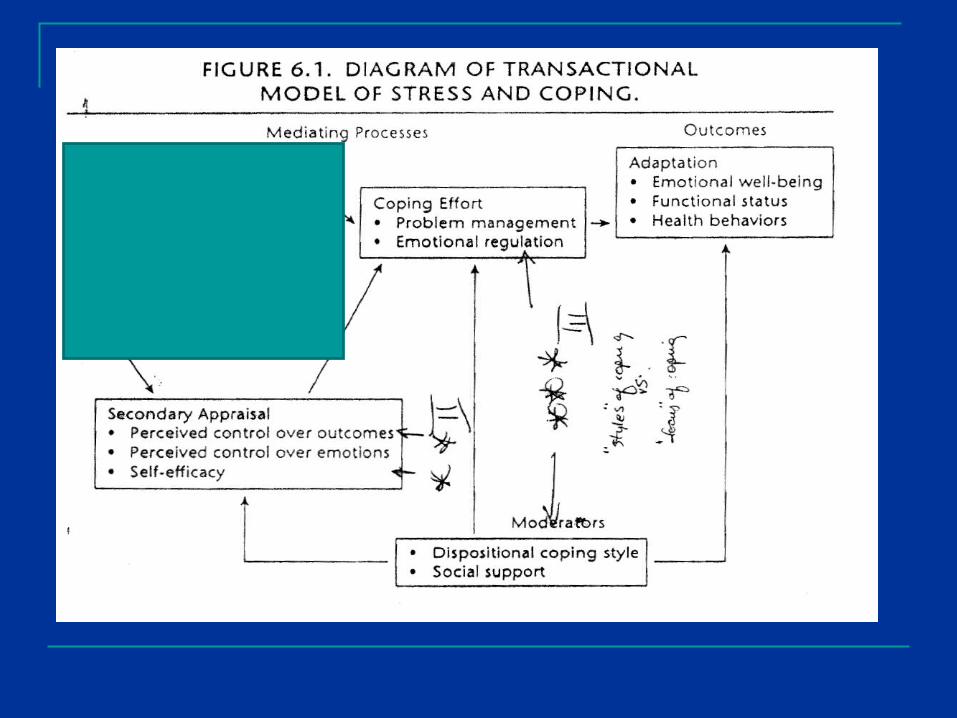
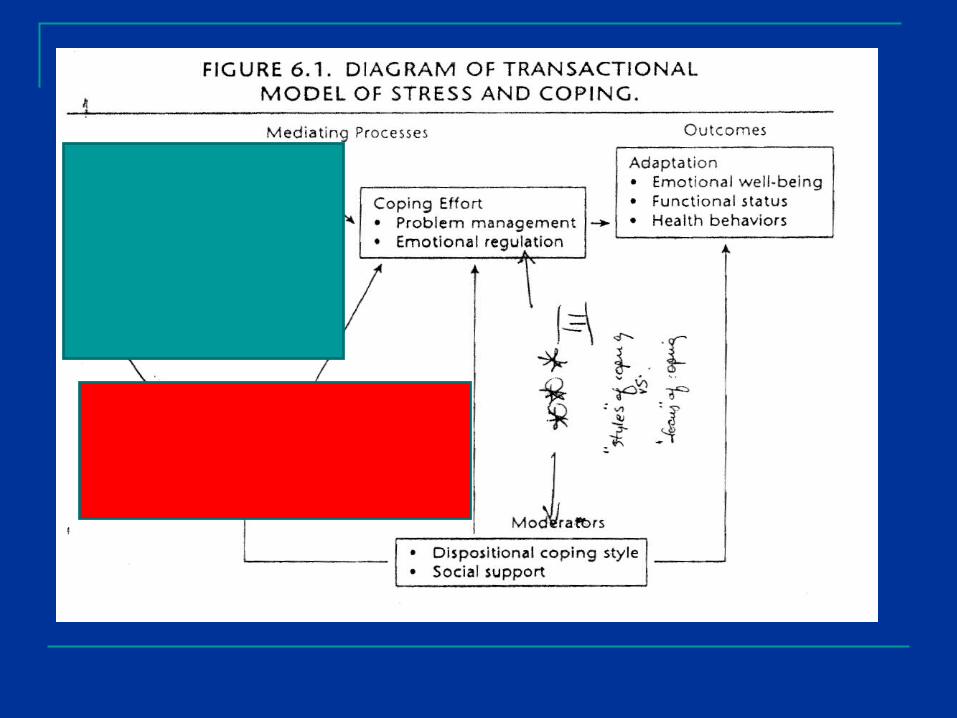
Caregiving for SDAT from the “Stress and Coping” Perspective

Stress and Copingas “hardwired” experience



Holmes & Rahe (1967)Social Readjustment Rating Scale (SRRS)

Lazarus and Folkman (1981)Hassles and Uplifts (HSUP)



Coping style vs.Coping success


What kinds of coping styles might be effective in coping with caring for and SDAT patient????
Q: How did Glenn Kirkland cope?
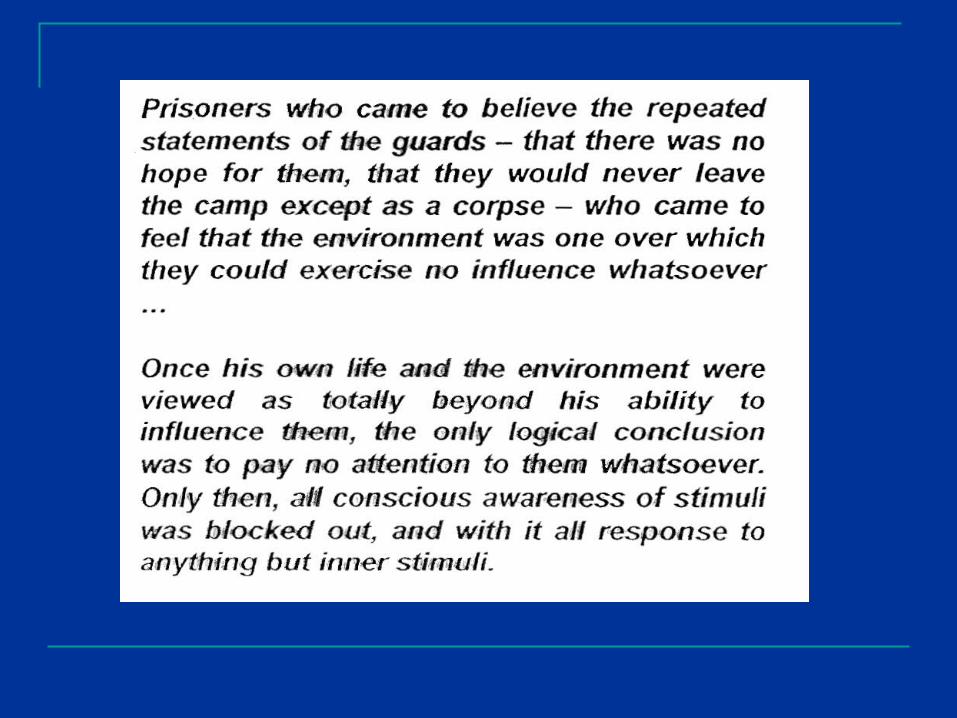
The importance of feeling “in control”
Langer and Rodin (1976)
Depression literature
Learned helplessness – Seligman’s rats, Harlow’s monkeys
Cognitive therapy for depression – Beck’s “negative triad”
Relocation effects
Lots of death following relocation.

Hypothesis
Elders moving to a nursing home given enhanced personal responsibility would demonstrate more physical and mental alertness, activity, well-being, and sociability than elders given less responsibilty.

Design and Procedure
Quasi-experimentor
Non-equivalent control group design
“Responsibility induced”vs
“Comparison”

Participants
•Drawn from two floors of a nursing home
•Subjects on the floors were of similar functional status and SES
•Whole floors in one condition or another
•91 ambulatory adults 65-90 yrs
47 in Responsibility-induced 44 in Comparison


Conclusions
Importance of free action and enhanced sense of control
What is the nature of this sense of control?
Mindfulness vs. mindlessness?
Do we have to be aware of the control we have?
Conclusions (cont’d)
18 month follow-up
Twice the mortality rate in the Comparison condition vs. Responsibility-induced condition (>30% vs. 14%)
Related Documents











