Alterations in Cardiac Function Immediately Following Electrical Conversion of Atrial Fibrillation to Normal Sinus Rhythm By WILLIAM SHAPIRO, M.D., AND GARNER KLEIN, M.D. SUMMARY An assessment was made of cardiac function by means of right heart catheterization before and immediately after conversion of atrial fibrillation to sinus rhythm in 11 studies on 10 human subjects. Comparable data during exercise were available in five studies. Medical management of patients in this study was identical to that employed routinely for this procedure. After conversion to normal sinus rhythm cardiac output response was significantly increased only during exercise. The relationship of mean right atrial and mean pulmonary wedge pressures to right and left ventricular stroke work was uniformly improved both because of decreases in these pressures and in- creases in work. Indirect evidence of mitral valvular regurgitation was diminished to absent after conversion. "'A" waves and the pulse pressure of atrial contraction were very small in the right atrial tracings after conversion and these contours were usually inapparent on pulmonary wedge tracings. It is concluded that over-all cardiac per- formance was improved with re-establishment of sinus rhythm and that diminutions in atrial-venous pressure behind each ventricle may be important in explaining symp- tomatic improvement following electroconversion. Measures of both pressure and flow were required for complete description of the alterations induced by this intervention. Additional Indexing Words: Cardiac output Intracardiac pressu: Atrial function Right heart cathet Mitral stenosis (1 AREFULLY controlled investigations Xhave elucidated clearly the contribution made by a properly timed, effective atrial systole to cardiac performancel-3 and helped explain some of the deleterious effects of its absence in atrial fibrillation. Although con- From the Pauline and Adolph Weinberger Lab- oratory for Cardiovascular Research, Department of Internal Medicine, University of Texas South- western Medical School, Dallas, and the Dallas Vet- erans Administration Hospital, Dallas, Texas. Work was supported in part by Research Grant FR0001602 from the National Institutes of Health, U. S. Public Health Service and by a grant from the Dallas Heart Association. Presented in part at annual meeting of the Amer- ican College of Physicians, April 12, 1967, in San Francisco, California. 1074 res erization Pressure-flow relationships Ventricular function sideration of the manifest hazards of the presence of atrial fibrillation in patients favors conversion to sinus rhythm,4 alterations in human circulation that accompany such therapy are still under investigation and to some extent in dispute.5-8 The availability of a safe, effective means of conversion, in the form of direct current countershock,9 has stimulated studies designed to resolve some aspects of these issues. In general, investigations performed prior to the availability of electroshock therapy suffer from the fact that negative inotropic effects of quinidine were potentially present after, but not before, the administration of this drug. Recent studies, however, were performed without quinidine in order to Circulation, Volume XXXVIII, December 1968 by guest on May 19, 2018 http://circ.ahajournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Alterations in Cardiac FunctionImmediately Following Electrical Conversion
of Atrial Fibrillation to NormalSinus Rhythm
By WILLIAM SHAPIRO, M.D., AND GARNER KLEIN, M.D.
SUMMARYAn assessment was made of cardiac function by means of right heart catheterization
before and immediately after conversion of atrial fibrillation to sinus rhythm in 11studies on 10 human subjects. Comparable data during exercise were available in fivestudies. Medical management of patients in this study was identical to that employedroutinely for this procedure. After conversion to normal sinus rhythm cardiac outputresponse was significantly increased only during exercise. The relationship of meanright atrial and mean pulmonary wedge pressures to right and left ventricular strokework was uniformly improved both because of decreases in these pressures and in-creases in work. Indirect evidence of mitral valvular regurgitation was diminished toabsent after conversion. "'A" waves and the pulse pressure of atrial contraction werevery small in the right atrial tracings after conversion and these contours were usuallyinapparent on pulmonary wedge tracings. It is concluded that over-all cardiac per-formance was improved with re-establishment of sinus rhythm and that diminutionsin atrial-venous pressure behind each ventricle may be important in explaining symp-tomatic improvement following electroconversion. Measures of both pressure and flowwere required for complete description of the alterations induced by this intervention.
Additional Indexing Words:Cardiac output Intracardiac pressu:Atrial function Right heart cathetMitral stenosis
(1 AREFULLY controlled investigationsXhave elucidated clearly the contributionmade by a properly timed, effective atrialsystole to cardiac performancel-3 and helpedexplain some of the deleterious effects of itsabsence in atrial fibrillation. Although con-
From the Pauline and Adolph Weinberger Lab-oratory for Cardiovascular Research, Departmentof Internal Medicine, University of Texas South-western Medical School, Dallas, and the Dallas Vet-erans Administration Hospital, Dallas, Texas.Work was supported in part by Research Grant
FR0001602 from the National Institutes of Health,U. S. Public Health Service and by a grant from theDallas Heart Association.
Presented in part at annual meeting of the Amer-ican College of Physicians, April 12, 1967, in SanFrancisco, California.
1074
reserization
Pressure-flow relationshipsVentricular function
sideration of the manifest hazards of thepresence of atrial fibrillation in patientsfavors conversion to sinus rhythm,4 alterationsin human circulation that accompany suchtherapy are still under investigation and tosome extent in dispute.5-8 The availability ofa safe, effective means of conversion, in theform of direct current countershock,9 hasstimulated studies designed to resolve someaspects of these issues.In general, investigations performed prior
to the availability of electroshock therapysuffer from the fact that negative inotropiceffects of quinidine were potentially presentafter, but not before, the administration ofthis drug. Recent studies, however, wereperformed without quinidine in order to
Circulation, Volume XXXVIII, December 1968
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

ALTERATIONS IN CARDIAC FUNCTION
define the pure effects of the change fromatrial fibrillation to normal sinus rhythm.These studies used principally cardiac out-put determinations and showed that inmost,5 but not all,6' 7 patients a distinct in-crease in cardiac output occurred shortlyafter establishment of the sinus mechanism;additional evidence indicates that there isfurther progressive improvement in cardiacfunction with the passage of time.8' 10 Sinceordinary clinical use of direct current coun-tershock often includes the administration ofquinidine as well as barbiturate anesthesia,and because measurement of cardiac outputalone does not precisely describe alterationsin cardiac function, the present study wasdone in an attempt to assess the earliesteffects of changing atrial fibrillation to normalsinus rhythm under the usual clinical condi-tions in which this procedure has been car-ried out. Furthermore, to evaluate the in-duced changes, right heart catheterizationswere performed before and after these altera-tions in cardiac rhythm and, whenever pos-sible, additional observations were made dur-ing leg exercise in the supine position.
Methods
Eleven studies were carried out in 10 pa-tients. Seven studies were performed on the sixpatients in group A (table 1) whose mean agewas 62 years (range 46 to 74). Patients repre-senting group A studies 4, 5, and 6 had ischemicheart disease by virtue of previous myocardialinfarction. The etiology of congestive failure ingroup A studies 1 and 2 was considered mostlikely to be due to ischemic heart disease. Stud-ies 3 and 7 of group A were performed 9 monthsapart in a 46-year-old man who had diffuse myo-cardial disease of unknown etiology. The dura-tion of the arrhythmia in this group of patientsranged from 3 weeks to 5 years. All had had car-diomegaly and congestive heart failure on admis-sion to hospital. Group B consisted of four pa-tients who had undergone mitral commissurotomy2 to 7 months prior to study. Their mean agewas 42 years (range 32 to 51). Each had hadclassical clinical, hemodynamic, and operativefindings of significant mitral stenosis; patients 1, 2,and 3 had improvement demonstrated by postop-erative reduction in pulmonary arterial and wedgepressures. Patient 4 of this group, 3 months post-operative, had no improvement in symptoms or
Circulation, Volume XXXVIII, December 1968
hemodynamic findings. Patient 1 had complicat-ing angina pectoris and intermittent claudica-tion. All patients in group B had been known tohave had atrial fibrillation continuously for atleast 2 to 7 months.
Prior to study each patient had been treatedoptimally with digitalis and diuretics when indi-cated. In the 24 to 48 hours prior to study, digi-talis had been discontinued but quinidine sulfatewas given orally in doses of 0.2 g every 6 hours.During the period of this study four additionalprospective study patients were converted onthis regimen but were lost to follow-up. Medicalmanagement in this study was identical to thatutilized clinically in our hospital in patients be-ing prepared for elective conversion by externalcountershock.
Right heart catheterizations were carried outin the conventional manner during the postab-sorptive state, but premedication with sedativeor analgesic drugs was not given. Cardiac outputwas determined by the Fick principle. Followingresting determinations, leg exercise in the supineposition was carried out for 4 to 6 minutes ona bicycle-type ergometer. Control pulmonarywedge pressures at rest were measured with thelegs elevated in the exercising position; con-tinuous recordings were taken during exercise. Atthe end of the second minute of exercise, thecatheter was withdrawn into the pulmonary ar-tery and mean pulmonary artery pressure trac-ings were recorded. During the third to fifthminute, cardiac output was measured. Follow-ing completion of the measurements obtainedduring atrial fibrillation, the patient was anes-thetized with an ultra short-acting barbiturate(sodium pentothal or sodium methohexital) toa light plane of anesthesia. Synchronized elec-trical DC countershock was applied as describedby Lown and associates.1" Shocks of 150 to 300watt seconds were required for conversion. Fol-lowing establishment of normal sinus rhythm,the patients became responsive within 20 to 30minutes. At this point the determinations wererepeated.
Analysis of data was carried out on at least twoseparate occasions with care taken to average atleast 10 cardiac cycles to obtain heart rate andpressure levels, both during atrial fibrillationand sinus rhythm. Vascular resistance was ex-pressed in units.12 Stroke work was calculated ac-cording to the formula of Mitchell and co-work-ers.13 Calculations substituting pulmonary wedgemean pressure for left ventricular end-diastolicpressure may have underestimated actual leftventricular stroke work in those patients in groupB who had possible residual left atrial-left ven-tricular end-diastolic pressure gradients (mostlikely for group B, patient 4). Statistical analyses
1075
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

SHAPIRO, KLEIN
Table IComparison of Metabolic and Circulatory Data before and after Electrical Conversion of Atrial Fibrillation toNormal Sinus Rhythm
BMR Oxygen consumption Cardiac outputGroup l%) (mllmin) (L/min)and Before After Before Afterstudy Before After R E R E R E R E
-7+ 2+26+10+ 7-14+ 4.0
13.9NS
+12+12-1+11
8.56.4
25025028330023335026727639.5
28333323330028741.7
800800
700750
1100800650850850187
23328333333031730028329734.8NS
30031725033330035.9NS
5.8 280 825 29811.3 38.6 157 33.4
NS
900
900900
NS
1100900650850875185NS
883144NS
4.15.45.45.23.15.25.14.80.9
5.26.64.75.95.600.84
7.85.9
6.96.40.8
9.37.29.68.711.29
3.27.18.84.94.14.85.05.41.9NS
7.16.44.56.76.191.16NS
6.3
9.67.92.3NS
10.111.07.4
10.59.631.95NS
5.08 7.80 5.69 8.960.91 1.59 1.64 2.03
NS < 0.05
BMR = basal metabolic rate; A-V 02 arteriovenous 02 difference; R rest; E exercise.
including paired t-tests were carried out by stan-dard methods'4 with the aid of a digital computer.
ResultsData at RestThe individual and mean data as well as
the results of paired t-test analyses are pre-sented in tables 1 to 3, which indicate5 thatthe metabolic status of the entire series was
almost identical- during both periods of study.There were no material differences in mean
basal metabolic rate, oxygen consumption,heart rate, systemic vascular resistance, andpulmonary vascular resistance. In addition,resting cardiac output, stroke volume, arterio-venous oxygen difference, and right ventricu-lar stroke work were unchanged shortly afterestablishment of normal sinus rhythm. Con-versely, the mean pulmonary wedge pressurefor the entire series (group A + B, table 1)declined from 17.7 to 13.1 mm Hg (P < 0.01),
100
90
80
70
I 60 -
E 50-E 40
30
20
to
0
_ ATRIAL FIBRILLATION
n NORMAL SINUS RHYTHM
n =ll
PWm PAm RVED1<.01) (NS) (<.02) (<.01)
Figure 1
Comparison of mean pressures at rest before andafter establishment of sinus rhythm for entire series.
P values are below each pair of bars. PWm = pulmo-nary wedge mean; PAm = pulmonary artery mean;
RVEDP = right ventricular end-diastolic pressure;
RAm = right atrial mean; MABP = mean arterialblood pressure; NS = not significant.
Circulation, Volume XXXVIII, December 1968
Group A1234567
MeanSDp
Group B1234
MeanSDp
Group A+ BMeanSDP
-20-13+14-1+26-19- 2.1
18.8
7±19-8-1
4.311.6
- 0.415.9
NS
NS
1076
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

ALTERATIONS IN CARDIAC FUNCTION
Heart rate Stroke volume A-V 02(beats imin) (ml /beat) (vol%)
Before After Before After Before AfterR E R E R E R E R E R E
75 90 55 36 6.0 7.285 - 70 64 101 - 4.6 4.0 -65 96 92 82 95 5.3 3.880 102 90 65 76 54 5.8 10.3 6.870 84 86 102 44 70 47 62 7.5 14.4 7.8 14.3100 - 80 52 - 60 - 6.7 13.4 6.254 80 55 69 94 87 91 139 5.3 10.0 5.6 9.475.6 82 80.4 85.5 65.1 79 69.9 101 5.9 12.4 5.9 11.814.8 28 13.6 23 17.5 12 26.0 54 0.9 2.9 1.5 3.5
NS NS NS NS NS NS
54 130 75 98 97 95 103 5.4 - 4.2 10.9110 129 84 102 60 72 76 108 5.0 8.6 4.9 8.265 96 63 90 72 75 71 82 5.0 9.0 5.5 8.880 99 70 84 74 97 96 125 5.1 8.9 5.0 8.177.3 113.5 73 93.5 75.8 81.3 84.5 105 5.1 8.8 4.9 8.324.3 18.5 8.8 8.1 15.5 13.7 12.9 21.7 0.2 0.2 0.5 0.4
NS < 0.05 NS NS NS NS
76.2 103 77.7 90.8 69.0 80.2 74.4 103.2 5.61 10.2 5.55 9.817.5 21.7 12.2 12.8 16.9 11.5 22.7 31.3 0.84 2.4 1.33 2.6
NS NS NS NS NS <0.05
right ventricular end-diastolic pressure de-creased from 7.2 to 6.5 mm Hg (P <0.02),right atrial mean pressure decreased from 6.5to 3.3 mm Hg (P <0.01), whereas the aver-age pulmonary artery mean and radial arteri-al mean pressures did not change significant-ly (fig. 1).Mean data from group A alone revealed
significant decreases in right ventricular end-diastolic pressure from 8.8 to 7.0 mm Hg(P <0.05), and right atrial mean pressurefrom 8.1 to 6.0 mm Hg (P <0.05). Meanpulmonary wedge pressure declined 3 mmHg, and cardiac output increased 0.6 L/min,but these changes were not of statisticalsignAficance.
Significant mean changes in group B in-cluded an increase in left ventricular strokework from 62.3 to 76.7 g-m (P < 0.01), adecrease in mean pulmonary wedge pres-sure from 14.8 to 7.8 mm Hg (P < 0.01 ),and a decline in right atrial mean pressureCirculation, Volume XXXVIII, December 1968
from 3.5 to -1.5 mm Hg (P<0.02). Meancardiac output also increased 0.6 L/min ingroup B from 5.6 to 6.2 L/min and strokevolume increased from 76 to 85 ml/beat, butthese changes did not achieve significanceupon t-test analysis.
IEE.
0.D. P.O. MitralPulmonary Wedge Pressure - Mild Exercise
40 AF
NSR30
10 -II 1
Begin Exercise min 2 min
Figure 2
Mean pulmonary wedge pressure at rest and after 1and 2 minutes of exercise during atrial fibrillation(AF, solid line) and normal sinus rhythm (NSR, brokenline) in a group B patient.
1077
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

1078 SHAPIRO, KLEIN
Table 2Comparison of Systemic and Pulmonary Pressures and Resistances before and after Electrical Conversionof Atrial Fibrillation to Normal Sinus Rhythm
Mean arterialblood pressure(mm Hg)
Before AfterR E R E
8970889376988084.89.9
8865827576.310.6
1209281
9085.56.4
1088393809112.6
9275889578888085.17.5NS
965877617317.5NS
80
9085.07.1NS
10489935986.319.2NS
81.7 89.2 80.7 85.810.6 10.6 12.8 15.3
NS NS
Systemicvascularresistance(units)
Before After
19.9 25.912.3 10.313.8 9.115.6 17.523.5 19.217.5 17.513.8 13.916.6 16.23.9 5.7NS
16.2 13.99.6 9.5
16.5 17.611.2 8.813.4 12.53.5 4.1NS
Mean PA pressure(mm Hg)
Before AfterR E R E
38173738213128308.5
1824222121.32.5
625832
434615
49333832387.8
15.4 14.8 26.8 41.33.9 5.3 8.0 11.1
411934 4238 -
17 352836 4330 409.4 4NS NS
22 3915 3120 3816 3018.3 34.53.3 4.7NS NS
26.0 36.99.7 5.1NS NS
Pulmonary vascularresistance(units)
Before AfterR E R E
3.91.32.11.5
2.93.32.22.30.9
1.01.51.50.71.20.4
2.4
1.92.10.3
0.82.80.81.51.1
5.31.31.93.11.9
4.22.91.5NS
2.21.62.40.81.80.8NS
1.9 3.07 2.50.9 2.6 1.4
NS
2.7
1.72.20.7NS
1.91.02.80.81.51.1NS
1.80.9NS
R = rest; E = exercise.
Data during Exercise
Five complete studies during exercise were
obtained (group A 5, 7; group B 2, 3, 4).Of importance, the level of exercise was atthe same level before and after conversionas judged from the level of oxygen consump-tion. During exercise mean cardiac outputwas 1.16 L/min higher (P<0.05) after con-
version; A-V 02 difference was 0.4 vol % less(P<0.05), and pulmonary wedge mean was
2.6 mm Hg lower (P < 0.05) in these fivepatients. Compared with their respective rest-ing values before and after conversion, themean postconversion wedge pressure rose
2 mm Hg more during exercise (figure 2presents an example) while the mean pul-monary artery pressure rose 4 mm Hg lessthan during atrial fibrillation. Left ventricularstroke work was greater, rising from 66.8 to89.4 g-m. Although heart rate in the five
studies was slower during exercise after con-
version, 90.8 versus 103.0/min, this changewas not statistically significant. Analysis limit-ed to the three group B patients did revealthe preconversion and postconversion heartrates (113.5 versus 93.5) to be significantlyless (P<0.05).
W. T PO Mitral
A F NSR
20~ Right Atrial Pressure15
Figure 3Right atrial pressure contour in a group B patientat comparable heart rates during atrial fibrillation(AF, left panel) and after successful countershocktherapy (NSR, right panel).
Circulation, Volume XXXVIII, December 1968
Groupandstudy
Group A1234567
MeanSDp
Group B1234
MeanSDp
Group A + BMeanSDp
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from
ALTERATIONS IN CARDIAC FUNCTION
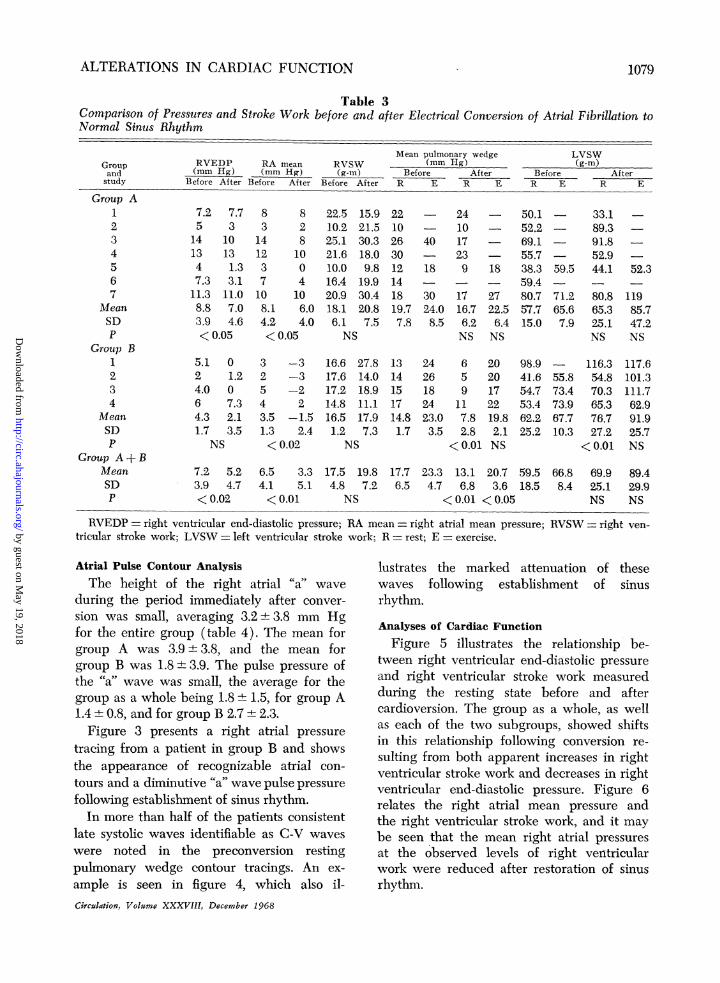
Table 3Comparison of Pressures and Stroke Work before and after Electrical Conversion of Atrial Fibrillation toNormal Sinus Rhythm
RVEDP RA mean RVSW(mm Hg) (mm Hg) (g-mn)
Before After Before After Before After
8 83 2
14 812 103 07 410 108.1 6.04.2 4.0<0.05
3 -32 -35 -24 23.5 -1.51.3 2.4<0.02
6.5 3.34.1 5.1<0.01
22.5 15.910.2 21.525.1 30.321.6 18.010.0 9.816.4 19.920.9 30.418.1 20.86.1 7.5NS
16.6 27.817.6 14.017.2 18.914.8 11.116.5 17.91.2 7.3NS
Mean pulmonary wedge(mm Hg)
Before AfterR E R E
2210263012141819.77.8
1314151714.81.7
17.5 19.8 17.74.8 7.2 6.5NS
40
18
3024.08.5
2426182423.03.5
241017239
1716.76.2NS
659
117.82.8
<0.01
18
2722.56.4NS
2020172219.82.1NS
LVSW(g-m)
Before AfterR E R E
50.152.269.155.738.359.480.757.715.0
98.941.654.753.462.225.2
59.5
71.265.67.9
55.873.473.967.710.3
23.3 13.1 20.7 59.5 66.84.7 6.8 3.6 18.5 8.4
<0.01 <0.05
33.189.391.8 -52.944.1 52.3
80.8 11965.3 85.725.1 47.2NS NS
116.3 117.654.8 101.370.3 111.765.3 62.976.7 91.927.2 25.7
<0.01 NS
69.}9 89.425.1 29.9NS NS
RVEDP = right ventricular end-diastolic pressure; RA mean = right atrial mean pressure;tricular stroke work; LVSW = left ventricular stroke work; R = rest; E = exercise.
Atrial Pulse Contour AnalysisThe height of the right atrial "a'" wave
during the period immediately after conver-
sion was small, averaging 3.2+± 3.8 mm Hgfor the entire group (table 4). The mean forgroup A was 3.9 3.8, and the mean forgroup B was 1.8 + 3.9. The pulse pressure ofthe "'a" wave was small, the average for thegroup as a whole being 1.8 1.5, for group A1.4+0.8, andforgroup B 2.7±2.3.Figure 3 presents a right atrial pressure
tracing from a patient in group B and showsthe appearance of recognizable atrial con-
tours and a diminutive "a" wave pulse pressure
following establishment of sinus rhythm.In more than half of the patients consistent
late systolic waves identifiable as C-V waves
were noted in the preconversion restingpulnonary wedge contour tracings. An ex-
ample is seen in figure 4, which also il-Circulatiorz, Volume XXXVIII, December 1968
RVSW = right ven-
lustrates the marked attenuation of thesewaves following establishment of sinusrhythm.
Analyses of Cardiac Function
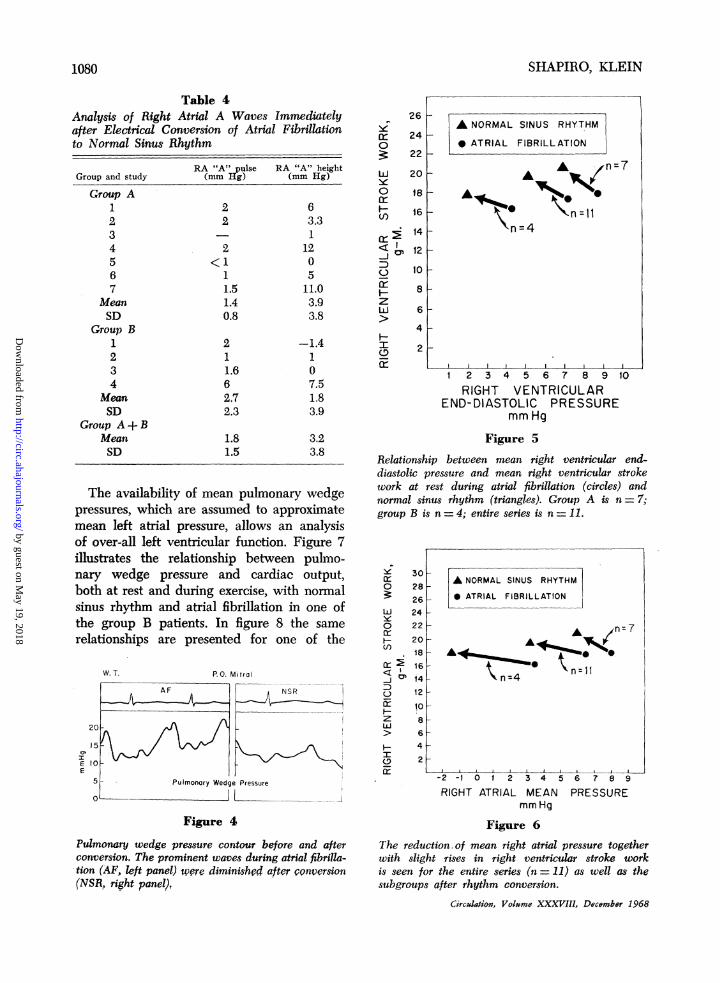
Figure 5 illustrates the relationship be-tween right ventricular end-diastolic pressureand right ventricular stroke work measuredduring the resting state before and aftercardioversion. The group as a whole, as wellas each of the two subgroups, showed shiftsin this relationship following conversion re-
sulting from both apparent increases in rightventricular stroke work and decreases in rightventricular end-diastolic pressure. Figure 6relates the right atrial mean pressure andthe right ventricular stroke work, and it maybe seen that the mean right atrial pressuresat the observed levels of right ventricularwork were reduced after restoration of sinusrhythm.
Groupandstudy
Group A1234567
MeanSDp
Group B1234
MeanSDp
Group A + BMeanSDp
7.2 7.75 3
14 1013 134 1.37.3 3.1
11.3 11.08.8 7.03.9 4.6< 0.05
5.1 02 1.24.0 06 7.34.3 2.11.7 3.5
NS
7.2 5.23.9 4.7<0.02
1079
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from
SHAPIRO, KLEIN
Table 4Analysis of Right Atrial A Waves Immediatelyafter Electrical Conversion of Atrial Fibrillationto Normal Sinus Rhythm
RA "A" pulse RA "A" heightGroup and study (mm Hg) (mm Hg)
Group A1 2 62 2 3.33 - 14 2 125 <1 06 1 57 1.5 11.0
Mean 1.4 3.9SD 0.8 3.8
Group B1 2 -1.42 1 13 1.6 04 6 7.5
Mean 2.7 1.8SD 2.3 3.9
Group A + BMean 1.8 3.2SD 1.5 3.8
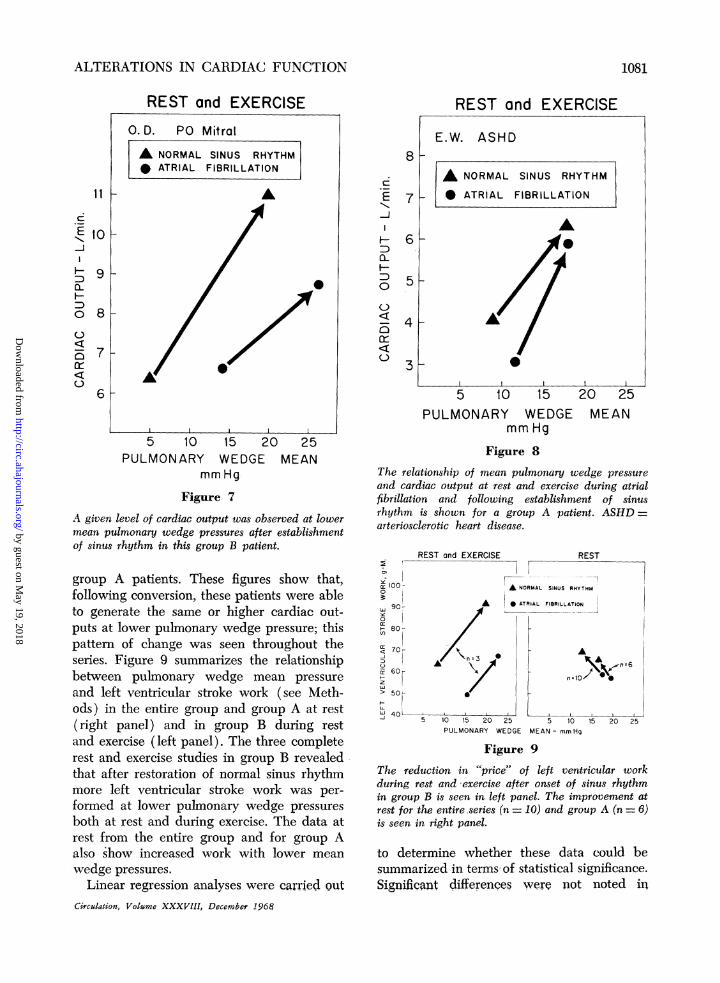
The availability of mean pulmonary wedgepressures, which are assumed to approximatemean left atrial pressure, allows an analysisof over-all left ventricular function. Figure 7illustrates the relationship between pulmo-nary wedge pressure and cardiac output,both at rest and during exercise, with normalsinus rhythm and atrial fibrillation in one ofthe group B patients. In figure 8 the same
relationships are presented for one of the
E
20
15
10
5
W.T. P.O. Mitral
AF NSR
Pulmonary Wedge Pressure
.. ... J~~~ _I
Figure 4
Pulmonary wedge pressure contour before and afterconversion. The prominent waves during atrial fibrilla-tion (AF, ileft panel) were diminished after conversion(NSR, right panel),
26y
240? 22
Lu 20y0 18
16
r-
LO
12-D 10Fr 8zLLJ 6
4
I 2
1 2 3 4 5 6 7 8 9 10
RIGHT VENTRICULAREND-DIASTOLIC PRESSURE
mm Hg
Figure 5
Relationship between mean right ventricular end-
diastolic pressure and mean right ventricular strokework at rest during atrial fibrillation (circles) andnormal sinus rhythm (triangles). Group A is n =7;group B is n = 4; entire series is n = 11.
0
3:LuJ0
.crE
C)J m~
z
I-
IL
Cr
30
28262422
2018
16
12
10
8
6
4
2
A NORMAL SINUS RHYTHM
* ATRIAL FIBRILLATION
A n7
\ x~~n=llan=4
-2 -1 0 1 2 3 4 5 6 7 8 9
RIGHT ATRIAL MEAN PRESSUREmm Hg
Figure 6
The reduction,of mean right atrial pressure togetherwith slight rises in right ventricular stroke workis seen for the entire series (n = 11) as well as thesubgroups after rhythm conversion.
Circdlation, Volume XXXVIII, December 1968
1080
A NORMAL SINUS RHYTHM
* ATRIAL FIBRILLATION
AA gzn=7
0 'Xn=llun=4
w
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from
ALTERATIONS IN CARDIAC FUNCTION
11
I-,H
:D0-
0
0
Sa:0
REST and EXERCISE0.D. PO Mitral
A NORMAL SINUS RHYTHM* ATRIAL FIBRILLATION
A
10 k
9 _
8k
7k
Al l
8k
N
1-J
D0L
D0
()
Sa:0
5 10 15 20 25PULMONARY WEDGE MEAN
mm Hg
Figure 7A given level of cardiac output was observed at lowermean pulmonary wedge pressures after establishmentof sinus rhythm in this group B patient.
group A patients. These figures show that,following conversion, these patients were ableto generate the same or higher cardiac out-puts at lower pulmonary wedge pressure; thispattern of change was seen throughout theseries. Figure 9 summarizes the relationshipbetween pulmonary wedge mean pressureand left ventricular stroke work (see Meth-ods) in the entire group and group A at rest(right panel) and in group B during restand exercise (left panel). The three completerest and exercise studies in group B revealedthat after restoration of normal sinus rhythmmore left ventricular stroke work was per-formed at lower pulmonary wedge pressuresboth at rest and during exercise. The data atrest from the entire group and for group Aalso show increased work with lower meanwedge pressures.
Linear regression analyses were carried outCirculation, Vohmme XXXVIII, December 196$
7
REST and EXERCISE
E.W. ASHD
A NORMAL SINUS RHYTHM
0 ATRIAL FIBRILLATION
Ar.5k
6
3
5 10 15PULMONARY WEDGE
mm Hg
20 25MEAN
Figure 8The relationship of mean pulmonary wedge pressureand cardiac output at rest and exercise during atrialfibrillation and following establishment of sinusrhythm is shown for a group A patient. ASHD =arteriosclerotic heart disease.
REST and EXERCISEE7 F~~~~~~iU o100- A NORMAL
LLJy0ir
V)
C-1
:DC)EF-zLLJ
L,ui
90- aA
80 7
701- \n-3 0
60
50[ F
40L -------5 10 15 20 25
PULMONARY WEDGE
STRIAL F
REST
SINUS RHYTHM
:IBRILLATION
A
5 10 15 20 25MEAN - mmHg
Figure 9
The reduction inr "price" of left ventricular workduring rest and -exercise after onset of sinus rhythmin group B is seen in left panel. The improvement atrest for the entire series (n = 10) and group A (n = 6)is seen in right panel.
to determine whether these data could besummarized in terms- of statistical significance.Significant differences were not noted in
1081
r
6
-7
---j
Ih Al*Ai
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

SHAPIRO, KLEIN
either the before and after slopes or y inter-cepts of the raw data. Since each pair of datarepresents a distinctly different subject, con-struction of before and after slopes showsgreat overlap, precluding the success of thistype of analysis in showing significant differ-ences. Table 3 shows that while right andleft ventricular stroke work only tended toincrease with sinus rhythm, the right ventricu-lar end-diastolic, mean right atrial, and meanpulmonary wedge pressures all declinedsignificantly when subjected to paired t-testanalyses.
DiscussionIt is clear that complete evaluation of cir-
culatory alterations after interventions suchas those here requires analysis of pressure-flowrelationships, since gross alterations in cardiacoutput may not always be observed follow-ing cardioversion,67 nor may changes in car-diac output necessarily completely describethe nature of what has occurred. The limitednumber of studies describing pressure-flowrelationships immediately before and afterelectrical conversion of atrial fibrillation tonormal sinus rhythm have yielded somewhatconflicting results with regard to the changesin cardiac output, left atrial pressure, and theimportance of a decrease in heart rate.7' 15Predictions of results based on atrial pressurecontours in the absence of simultaneous flowshave also been made.'6
In the present study mean cardiac outputdid increase in each group at rest and duringexercise, but these alterations were significantonly for the five exercise studies (P <0.05).
If one considers the mean right or leftatrial pressure associated with a given levelof ventricular work (that is, the "hemody-namic price" of ventricular work), it is clearthat these pressures were diminished in thepatients in the present study following es-tablishment of the sinus mechanism (figs. 6to 9). The pressures behind each ventricleat any given level of work appear to beimportant to an individual patient's sense ofwell being. The role of the rises in left atrial-
pulmonary venous pressure in the productionof dyspnea in patients with disease distal tothe pulmonary capillary bed seems clear'7and elevations of right atrial pressure lead toa variety of debilitating phenomena. Reduc-tions in pulmonary wedge pressure associatedwith re-establishment of sinus rhythm, espe-cially during exercise, may aid in preventionof pulmonary edema and dyspnea.17 Also, re-ductions in intracardiac pressures have re-portedly been associated with more favorableprognoses in patients with heart failure whencontrasted with those patients who maintainhigh pulmonary vascular pressures in thepresence of similar levels of cardiac output.'8The hemodynamic "stimulus" to ventricular
work, that is, ventricular end-diastolic pres-sure itself may be distinguished from the"<price" of that work.'9 The data in figure 5show reductions in right ventricular end-diastolic pressure and increases in rightventricular stroke work after conversion.These alterations may be interpreted as beingdue to positive inotropic effects associatedwith the establishment of the sinus mecha-nism. It is unclear from detailed analyses offactors regulating ventricular function19 whysuch left shifts should have occurred. Itwould rather have been expected that ven-tricular function should move upward on thesame curve with increases in stroke work. Apossible alternate explanation of these ap-parent inotropic effects may be inferred fromthe pressure tracing in figure 4. If it beaccepted that atrioventricular valvular re-gurgitation occurred during atrial fibrillation,as has been shown by Skinner and colleagues3(and which may be reflected in figure 4 andthe many similar tracings in other patients inthis series), then the analysis of present datawould have underestimated stroke work dur-ing the arrhythmia, and the shift to a differentfunction curve represents an artifact. Thetype of data obtained precludes quantitativeexpressions of the amount of such regurgita-tion. Other explanations of an actual orapparent shift to a new curve (improvedventricular function) include (1) increases
Circulatjv, VoQlme XXXVIII, December 1968
1082
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from
ALTERATIONS IN CARDIAC FUNCTION
in catecholamine levels; (2) change in pres-sure-volume relationships of the right ven-tricle; and (3) overestimation of rightventricular end-diastolic pressure duringfibrillation because of the varying nature ofthe pressures under these conditions.The failure to observe clear "a" waves in
pulmonary wedge pressure tracings followingconversion was not unexpected since atbest, pulmonary wedge contours representdamped, unpredictable, distorted images ofleft atrial pressure contours despite thealmost uniform similarity of wedge and leftatrial mean pressures. Analysis of right atrial"a" waves, however, revealed them to besmall and to have small pulse pressures.Follow-up studies would have been of inter-est to observe any associations between in-creases in these atrial pressure contours andover-all cardiac performance, but such stud-ies could not be carried out in the patientsunder discussion. Despite the small "a" waves,declines in mean atrial and right ventricularend-diastolic pressures occurred and wereassociated with what are interpreted asimprovements in over-all cardiac function. Itwould appear, therefore, that assessmentsbased on the small amplitude or unimpressiveform of this type of atrial contour alone maybe misleading in this situation.These observations reveal that, especially
under adverse circumstances, normal sinusrhythm is advantageous for cardiac perfor-mance. These data provide examples of fail-ure to find improvement in cardiac functionif evaluation had been made only on thebasis of increases in cardiac output. Theydo not agree with the explanation thatdiminution in heart rate is the major factorleading to improved ventricular function inpatients such as those in this series.7 Withthe likely exceptions of patients with ad-vanced mitral stenosis20 and patients withoutorganic heart disease, whose autonomic sys-tem can provide adequate compensation3' 6, 21(though perhaps not under maximal exercisestresses), it may be concluded that normalsinus rhythm permits a lowered hemodynamic"(price" to be paid for any given level ofCirculation, Volume XXXVIII, December 1968
ventricular work when contrasted with atrialfibrillation.
AcknowledgmentThe authors are grateful to Dr. N. S. Skinner for
his critical review of this work.
References1. MITCHELL, J. H., GILMORE, J. D., AND SARNOFF,
S. J.: Transport function of the atrium. AmerJ Cardiol 9: 237, 1962.
2. SKINNER, N. S., MITCHELL, J. H., WALLACE,A. G., AND SARNOFF, S. J.: Hemodynamiceffects of altering the timing of atrial systole.Amer J Physiol 205: 499, 1963.
3. SKINNER, N. S., MITCHELL, J. H., WALLACE,A. G., AND SARNOFF, S. J.: Hemodynamicconsequences of atrial fibrillation at constantventricular rates. Amer J Med 36: 342, 1964.
4. HURST, J. W., PAULK, E. A., PROCTOR, H. D.,AND SCHLANT, R. C.: Management of pa-tients with atrial fibrillation. Amer J Med 37:728, 1964.
5. MORRIS, J. J. J., ENTMAN, M. L., NORTH, W. C.,KONG, Y., AND MCINTOSH, H. D.: Changes incardiac output with reversion of atrial fibrilla-tion to sinus rhythm. Circulation 31: 670,1964.
6. KILLIP, T., AND BAER, R. A.: Hemodynamiceffects after reversion from atrial fibrillationto sinus rhythm by precordial shock. J ClinInvest 45: 658, 1966.
7. GRAETTINGER, J. S., CARLETON, R. A., ANDMUENSTER, J. J.: Circulatory consequences ofchanges in cardiac rhythm produced in pa-tients by transthoracic direct current shock.J Clin Invest 43: 2290, 1964.
8. RODMAN, T. B., POSTER, H., AND FIGUEROA, W.:Effect on cardiac output of conversion fromatrial fibrillation to normal sinus mechanism.Amer J Med 41: 249, 1966.
9. FRIEDBERG, C. K.: Diseases of the Heart. Phila-delphia, W. B. Saunders Co., 1966, p. 556.
10. ORAM, S., WEINGREN, L., DAVIES, J. P. M.,TAGGERT, P., AND KITCHEN, L. D.: Conver-sion of atrial fibrillation to sinus rhythm bydirect current shock. Lancet 2: 159, 1963.
1 1. LowN B., RAGHAVEN, A., AND NEWMAN, J.:New method for terminating cardiac arrhyth-mias. JAMA 182: 548, 1962.
12. WOOD, P.: Diseases of the Heart and Circula-tion, ed. 2. Philadelphia, J. B. LippincottCo., 1956, p. 177.
13. MITCHELL, J. H., WALLACE, A. G., AND SKIN-NER, N. S.: Relation between end-diastolicpressure and mean rate of ejection of left ven-tricle. J Appl Physiol 211: 83, 1966.
1083
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

SHAPIRO, KLEIN
14. STEEL, R. G. D., AND TORRIE, J. H.: Principlesand Procedures of Statistics. New York,McGraw-Hill Book Co., 1960, p. 78.
15. REALE, A.: Acute effects of countershock con-version of atrial fibrillation upon right andleft heart hemodynamics. Circulation 32: 214,1965.
16. BRAuNWALD, E.: Introduction to symposium oncardiac arrhythmias with comments on thehemodynamic significance of atrial systole.Amer J Med 37: 665, 1964.
17. MATJCK, H. P., JR., SHAPIRO, W., AND PATTER-SON, J. L., JR.: Pulmonary venous (wedge)pressure: Correlation with onset and disap-pearance of dyspnea in acute left ventricular
heart failure. Amer J Cardiol 13: 301, 1964.18. EICHNA, L. W.: Circulatory congestion and
heart failure. Circulation 22: 864, 1960.19. SARNOFF, S. J., AND MITCHELL, J. H.: Regula-
tion of the performance of the heart. AmerJ Med 30: 747, 1961.
20. CARLETON, R. H., AND GRAETTINGER, J. S.:Hemodynamic role of the atria with andwithout mitral stenosis. Amer J Med 42:532, 1967.
21. MARTIN, R. H., LIM, S. T., AND VAN CrrTERS,R. L.: Atrial fibrillation in the intact unanes-thetized dog: Hemodynamic effects duringrest, exercise and beta-adrenergic blockade.J Clin Invest 46: 205, 1967.
Early Transplantation Experiments (circa 1750)The success of this operation [transplanting teeth] is founded on a disposition in all
living substances, to unite when brought into contact with one another; although theyare of a different structure; and even although the circulation is only carried on in oneof them.
This disposition is not so considerable in the more perfect or complex animals, suchas quadrupeds, as it is in the more simple or imperfect; nor in old animals, as in young:for the living principle in young animals, and those of simple construction, is not somuch confined to, or derived from one part of the body; so that it continues longerin a part separated from their bodies, and even would appear to be generated in it forsome time; while a part, separated from an older, or more perfect animal, dies sooner,and would appear to have its life entirely dependent on the body from which it wastaken.
Taking off the young spur of a cock, and fixing it to his comb, is an old and wellknown experiment.
I have also frequently taken out the Testis of a cock and replaced it in his belly,where it has adhered, and has been nourished; nay, I have put the Testis of a cock intothe belly of a hen with the same effect.-JoHN HUNTER: The Natural HIistory of theHuman Teeth. London, Robert Hardwicke, 1865, p. 156.
Circulation, Volume XXXVIII, December 1968
1084
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from
WILLIAM SHAPIRO and GARNER KLEINAtrial Fibrillation to Normal Sinus Rhythm
Alterations in Cardiac Function Immediately Following Electrical Conversion of
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1968 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.38.6.1074
1968;38:1074-1084Circulation.
http://circ.ahajournals.org/content/38/6/1074located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from
Related Documents