REVISED 04/12/18 ___________________________________ Child’s Name Please complete the attached paperwork for Pre-K Counts and return to the address below. In addition, please include the child’s birth certificate, immunizations record and proof of income. If any questions, please call. 3590 O’Neil Blvd. McKeesport, PA 15132 Attn: Allison Wynn Phone: 412-664-3612 Fax: 412-664-3638 Please indicate which Pre-K Counts class in which you want to enroll your child. _____Half day AM – 8:00 am to 10:45 am – located at Founders’ Hall. Best option for 3 year olds _____Half day PM – 12:15 pm to 3:00 pm – located at Founders’ Hall. Best option for 3 year olds _____FULL DAY – 8:00 am to 2:00 pm – located at Founders’ Hall. Best option for 4 year olds Please keep in mind that parents must provide transportation to and from school. MASD Pre-K counts utilizes a prioritization strategy based on several additional risk factors beyond income and age.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
REVISED 04/12/18
___________________________________ Child’s Name
Please complete the attached paperwork for Pre-K Counts and return to the
address below. In addition, please include the child’s birth certificate, immunizations record and proof of income. If any questions, please call.
3590 O’Neil Blvd.
McKeesport, PA 15132 Attn: Allison Wynn
Phone: 412-664-3612 Fax: 412-664-3638
Please indicate which Pre-K Counts class in which you want to enroll your child.
_____Half day AM – 8:00 am to 10:45 am – located at Founders’ Hall. Best option for 3 year olds
_____Half day PM – 12:15 pm to 3:00 pm – located at Founders’ Hall. Best option for 3 year olds
_____FULL DAY – 8:00 am to 2:00 pm – located at Founders’ Hall. Best option for 4 year olds
Please keep in mind that parents must provide transportation to and from school.
MASD Pre-K counts utilizes a prioritization strategy based on several additional risk factors beyond income and age.
ENROLLMENT INFORMATION
_______________________ STUDENT’S LAST NAME
_______________________ STUDENT’S FIRST NAME
_______________________ MIDDLE NAME
_______________________ STUDENT’S BIRTHDATE
_______________________ TODAY’S DATE
___________________________________________________ STREET ADDRESS
___________ APT. #
___________ RACE HISPANIC NON-HISPANIC
_______________________ HOME PHONE #
___________________________________________________ CITY
PA STATE
___________ ZIP CODE
___________ GENDER
N/A ENROLLMENT DATE
_______________________ CELL PHONE #
N/A PPID#
MASD Pre-K Counts SCHOOL OF ENROLLMENT
N/A GRADE
__________________________________________________ EMAIL ADDRESS
N/A HOMEROOM
N/A COUNSELOR
PERSONAL INFORMATION ______________________________ PERSON’S NAME WITH WHOM STUDENT RESIDES
___________________ RELATIONSHIP DO OTHER CHILDREN WHO LIVE IN THE HOME ATTEND MASD SCHOOLS? YES NO
__________________________ BIOLOGICAL MOTHER’S LAST NAME ___________________
FIRST NAME DECEASED IS THERE ANY CUSTODY INFORMATION THAT WE SHOULD BE AWARE OF? YES NO
__________________________ BIOLOGICAL FATHER’S LAST NAME ___________________
FIRST NAME DECEASED IF YES, PLEASE EXPLAIN? _______________________________________________
__________________________ GUARDIAN’S LAST NAME ___________________
FIRST NAME DOES YOUR CHILD CURRENTLY HAVE AN IEP? YES NO
DOES YOUR CHILD CURRENTLY RECEIVE DART SERVICES? YES NO
IN WHAT COUNTRY WAS YOUR CHILD BORN? _______________ DOES YOUR CHILD CURRENTLY HAVE A GIEP? YES NO
WHEN DID HE/SHE BEGIN LIVING IN THE UNITED STATES? _______________ DOES YOUR CHILD CURRENTLY RECEIVE SPEECH SERVICES? YES NO
IN WHAT STATE WAS YOUR CHILD BORN? _______________ WHAT IS THE PRIMARY SPOKEN LANGUAGE IN THE HOME? ______________________
WHEN DID HE/SHE BEGIN LIVING IN PENNSYLVANIA? _______________
PLEASE LIST SIBLINGS BELOW: PLEASE PROVIDE YOUR CHILD’S SCHOOL HISTORY BELOW:
NAME DATE OF BIRTH GENDER MONTH AND YEAR ATTENDED GRADES DISTRICT AND BUILDING NAME REASON FOR LEAVING
____________________________ ____________ __________ ___________________ _________ ________________ ________________
____________________________ ____________ __________ ___________________ _________ ________________ ________________
____________________________ ____________ __________ ___________________ _________ ________________ ________________
____________________________ ____________ __________ ___________________ _________ ________________ ________________
PARENT/GUARDIAN INFORMATION
__________________________________ PARENT/GUARDIAN NAME RESIDES IN HOME WITH CHILD? YES NO
MOTHER FATHER GRANDPARENT GUARDIAN OTHER
BIOLOGICAL FOSTER ADOPTIVE STEP-PARENT OTHER
_________________________________ PARENT/GUARDIAN NAME RESIDES IN HOME WITH CHILD? YES NO
MOTHER FATHER GRANDPARENT GUARDIAN OTHER
BIOLOGICAL FOSTER ADOPTIVE STEP-PARENT OTHER
Education Status of Guardian 1:
Up to 8th Grade Vocational or Technical Program after High School 9th to 11th Grade Associates Degree High School Diploma Bachelor’s Degree GED Graduate/Professional School Some College Unknown
Education Status of Guardian 2:
Up to 8th Grade Vocational or Technical Program after High School 9th to 11th Grade Associates Degree High School Diploma Bachelor’s Degree GED Graduate/Professional School Some College Unknown
Employment Status of Guardian 1:
Employed Full-Time (30 hours/week and over) Seasonal Employed Part-Time (Fewer than 30 hours/week) Student or Job Trainee Multiple Part-Time Unemployed
Employment Status of Guardian 2:
Employed Full-Time (30 hours/week and over) Seasonal Employed Part-Time (Fewer than 30 hours/week) Student or Job Trainee Multiple Part-Time Unemployed
CHECK ANY COMMUNITY-BASED SERVICES THE FAMILY HAS PARTICIPATED IN:
Emergency/Crisis Intervention Housing Assistance Transportation Assistance Mental Health Services English as a Second Language (ESL) Training Adult Education Substance Abuse Prevention or Treatment Job Training Child Abuse and Neglect Services Domestic Violence Services Child Support Assistance Health Education Children and Youth Services Parenting Education Assistance to Families of Incarcerated Individuals Marriage Education Services Assistance in Obtaining Health Insurance None Assistance in Identifying Health Care/Medical Providers Unknown
HOUSEHOLD INCOME INFORMATION
FAMILY TYPE:
ONE PARENT TWO PARENT FOSTER CHILD CHILD LIVING WITH RELATIVE
INCLUDING YOUR CHILD, HOW MANY PEOPLE LIVE IN THE HOME?________________________
BASED ON THE MEMBERS OF YOUR HOUSEHOLD, HOW MANY PEOPLE (EXCLUDING COLLEGE STUDENTS), CONTRIBUTE TO THE HOUSEHOLD INCOME? _______________ PLEASE PROVIDE THEIR NAMES: ______________________________________________________________ NOTE: ALL MEMBER NAMES ABOVE WILL NEED TO PROVIDE PROOF OF INCOME.
HOUSEHOLD INCOME (REQUIRED) LESS THAN $5,000 $5,001 - $10,000 $10,001 - $15,000 $15,001 - $20,000 $20,001 - $25,000 $25,001 - $30,000 $30,001 - $35,000 $35,001 - $40,000 $40,001 - $45,000 $45,001 - $50,000 $50,001 - $60,000 $60,001 - $70,000 $70,001 - $100,000 More than $100,000
ARE YOUR CHILD’S IMMUNIZATIONS UP-TO-DATE? YES NO
HAS YOUR CHILD UNDERGONE A LEAD TEST? YES NO
IS THE BIOLOGICAL MOTHER OR FATHER INCARCERATED? YES NO
WAS THE CHILD BORN TO THE BIOLOGICAL PARENTS WHILE AT LEAST ONE PARENT WAS 19 OR YOUNGER? YES NO
FOR OFFICE USE ONLY: ACTUAL ANNUAL VERIFIED GROSS HOUSEHOLD (FAMILY) INCOME: _________________________________
Family income is at or below 300% of federal poverty level (Required risk factor). Consider all sources of income. See end of document for income chart relative to family size. (Must be verified prior to enrollment.)
ABOUT YOUR CHILD PERSONAL HABITS: Does your child usually eat breakfast? ______________ Mid morning snack? ______________ Is your child allergic to any foods, medications, pets, etc. ______________________________ Is there anything unusual about your child’s eating habits that you believe we should know? ______________________________________________________________________________ What is your child’s usual bedtime? ___________ Wake-up time? ___________________ Does your child take a morning nap? __________ Afternoon nap? __________________ At what age did your child walk? ______________ Talk? ___________________________ At what age was your child toilet trained? _______ How does your child state his/her need to go to the bathroom? __________________________ Does your child have periodic accidents? ________ Are there any other areas that you are concerned about? _______________________________ PLAY AND SOCIABILITY: Does your child prefer to play alone: ____ Always ____ Often ____ Seldom ____ Never Does your child want the involvement of _____ adults? _____children? Are your child’s playmates _____ girls? _____ boys? _____ younger? _____ older? What play materials does your child use most? _______________________________________ Does your child have the opportunity to play outdoors? ________________________________ What experience does your child have with music at home? _____________________________ What opportunities for hearing stories are offered? ___________________________________ How often do family members read to your child?
At least once a day At least once a week At least once a month Less than once a month How many children’s books are in your home? 0-5 5-10 11-20 More than 20 PERSONALITY AND EMOTIONAL DEVELOPMENT: Do you regard your child as affectionate? _____________ To Whom? __________ Does your child accept new people easily? ___________________________________________ Does your child have any fears? _____________________ Of what? ______________________ When you find it necessary to exert authority with your child, what do you do? Mother: _______________________________________________________________________ Father: ________________________________________________________________________ OTHER: List below any further information about your child or your family which you believe will be helpful to us in understanding your child’s behavior and needs: ___________________________________________________ __________________________________________________________________________________________ Are there any financial, religious or cultural factors that we need to consider here at school? ____________________________________________________________________________________________________________________________________________________________________________________
ZERO INCOME DECLARATION LETTER
Name of Parent ____________________________________________________________
Name of Child ____________________________________________________________
Program Name ____________________________________ Program Year ___________
Date ______________________
I am signing this letter to declare that I currently do not have any income from any source. My financial
support comes from (please describe):
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
I agree to notify the above program about changes in my income within 30 days of the change.
I certify that the information submitted is accurate and true to the best of my knowledge. I
understand that by completing, signing, and dating this form, I declare I have no household income
and that the information I am providing is correct. I understand that providing false information may
result in denial of services.
Parent Name ___________________________________________________
Parent Signature ___________________________________________________
Reviewer Name ___________________________________________________
Reviewer Signature ___________________________________________________
Date ___________________
McKeesport Area School District
Home Language Survey*
The Office of Civil Rights (OCR) requires that school districts/charter schools/full day AVTS identify limited
English proficient (LEP) students in order to provide appropriate language instructional programs for them.
Pennsylvania has selected HOME Language Survey as the method for the identification.
School District: McKEESPORT AREA SCHOOL DISTRICT
Name of Child: _________________________________________ Date: __________________
Address: ______________________________________________ Grade: ________________
School: _______________________________________________
Name of School State Dates Attended
_____________________________ _____________ ______________________________
_____________________________ _____________ ______________________________
_____________________________ _____________ ______________________________
Person completing this form (If other than parent/guardian):__________________________________
Parent/Guardian Signature: ____________________________________________________________
*The school district/charter school/full day AVTS has the responsibility under the federal law to serve students who are
limited English proficient and need English instructional services. Given this responsibility, the school district/charter
school/full day ABTS has the right to ask for the information it needs to identify English language Learners (ELLs). As
part of the responsibility to locate and identify ELLs, the school district/charter school/full day AVTS may conduct
screenings or ask for related information about students who are already enrolled in the school as well as from students
who enroll in the school district/charter school/full day AVTS in the future
NCLB-B1 – Home Language Survey-(09/05)
1. What is/was the student’s first language? ____________________
2. Does the student speak a language(s) other than English?
(Do not include languages learned in school.)
If yes, specify the language(s):
Yes No
____________________
3. What Language(s) is/are spoken in your home? ____________________
4. Has the student attended any United States school in any 3
years during his/her lifetime?
Yes No
If yes, complete the following:
EMERGENCY CONTACT / PARENTAL CONSENT FORM
CHILD’S NAME
BIRTHDATE
ADDRESS
MOTHER’S NAME/LEGAL GUARDIAN HOME OR CELL PHONE NUMBER(S)
ADDRESS WORK TELEPHONE NUMBER(S)
FATHER’S NAME/LEGAL GUARDIAN HOME OR CELL PHONE NUMBER(S)
ADDRESS WORK PHONE NUMBERS(S)
EMERGENCY CONTACT PERSON(S) NAME TELEPHONE NUMBER(S) 1.
2.
3.
PERSON(S) TO WHOM CHILD MAY BE RELEASED NAME TELEPHONE NUMBER(S)
1.
2. 3.
NAME OF CHILD’S PHYSICIAN/MEDICAL CARE PROVIDER TELEPHONE NUMBER
ADDRESS
SPECIAL DISABILITIES (IF ANY) ALLERGIES (INCLUDING MEDICATION REACTION)
MEDICAL OR DIETARY INFORMATION NECESSARY IN AN EMERGENCY SITUATION MEDICATION, SPECIAL CONDITIONS
ADDITIONAL INFORMATION ON SPECIAL NEEDS OF CHILD
HEALTH INSURANCE COVERAGE FOR CHILD OR MEDICAL ASSISTANCE BENEFITS POLICY NUMBER (REQUIRED)
PARENT’S SIGNATURE IS REQUIRED FOR EACH ITEM BELOW TO INDICATE PARENTAL CONSENT
OBTAINING EMERGENCY MEDICAL CARE ADMINISTERING MINOR FIRST-AID PROCEDURES
WALKS AND TRIPS SWIMMING
TRANSPORTATION BY THE FACILITY
_____________________________________________________________ ________________________________________ SIGNATURE OF PARENT OR GUARDIAN DATE
_____________________________________________________________ ________________________________________ SIGNATURE OF PARENT OR GUARDIAN DATE
POLICY SIGNATURE PAGE AND PHOTO RELEASE
I have received and read the following McKeesport Area School District Regulations & Policies. Please place a check mark next to the ones below you have received & read (see attached
policies):
Acceptable Use of Technology/Internet
Bus Riding Rules and Regulations
Weapon Policy
Unlawful Harassment Policy
.
Your child’s photo may be taken for inclusion in the district publication or in local newspapers or magazine articles or letters relating to school activities.
Yes, I give permission
No, I do not give permission
Signature of Student Signature of Parent
Date of Signature
Dress and Grooming
Pre-K Counts Attendance
No, I do not give permission
Yes, I give permission
Pre-K Counts Parent Involvement
McKeesport Area School District Pre-K Counts is required to obtain parent permission for administering hand sanitizer.
Student Name:_____________________________________
Birthdate:_________________________________________
Please check the appropriate answer:
____ I wish for school personnel to do a vision screening.
____ I wish for my family optometrist to do the vision screening.
____ I wish for school personnel to do a dental screening.
____ I wish for my family dentist to do the dental screening.
____ I wish for school personnel to do a hearing screening.
____ I wish for my family audiologist to do the hearing screening.
If you choose to have your family doctors provide the screenings, you must provide the
results to the MASD Pre-K Counts Program. If we do not have your child’s documentation by the date of the school screenings, your child will be given a screening.
Parent/Guardian Signature:__________________________
Date:____________________________________________
McKeesport Area School District
McKeesport, PA 15132 School:_____________________________________________ Today’s Date: _________________________
Student Name: ______________________________________ Student No.: __________________________
Grade: _____________________________________________ Room No. : ___________________________
HEALTH INFORMATION The following information is considered confidential and is for use of teachers, principal, school nurse/health staff, or other staff
who will be in contact with and responsible for your child during the school day. If you prefer talking personally to the school nurse/health staff regarding any of the following statements, please mark here _____ and she will contact you.
Home: ________________________ Work/Cell: ________________________ Signature: _____________________________
CHECK ANY OF THESE CONDITIONS WHICH YOUR CHILD HAS:
_____ Cancer _____Kidney/Bladder Disease _____Vision Problems _____ADD
_____ Diabetes _____Convulsions/Seizures _____Hearing Problems _____ADHD
_____Heart Disease _____Orthopedic/Bone _____Social/Emotional/Behavioral Concerns
_____Autism _____Bowel Concerns _____In Counseling
_____ Allergy To:___________________________________________________________ Severe: ___Yes ____No
_____Asthma – Provoked by: _________________________________________________ Severe: ___Yes ____No
Has above condition been diagnosed by a medical doctor? _____ Yes _____ No
If yes, what is the doctor’s name? ___________________________________________
May we obtain this information? ___ Yes ___ No Signature for release of information: ___________________________
What does the child do to manage their own condition? ____________________________________________________________________________________________________________________________________________________________________________________________________
How can the teacher help with this at School? ____________________________________________________________________________________________________________________________________________________________________________________________________
What symptoms should we report to you? _______________________________________________________________
Takes Medication Daily at _____ Home _____ School
Medication is: ______________________________________________________________________________________
Taken for: _________________________________________________________________________________________
IF YOUR CHILD MUST RECEIVE MEDICATION WHILE AT SCHOOL AN “AUTHORIZATION FOR MEDICATION” FORM MUST BE COMPLETED AND SIGNED BY THE ATTENDING PHYSICIAN AND PARENT(S) OR LEGAL GUARDIAN(S) OF THE CHILD (CHAPTER 195-182). YOU CAN OBTAIN THESE FROM THE
SCHOOL SECRETARY
Provide any information not included above which you think we should know about your child’s physical, mental, or emotional health which might affect school performance or require special consideration (i.e. limitations in activities, etc.).
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
OFFICE USE ONLY
ALERT FLAG 78 Health Code 1 125 Health Code 1 125 Health Code 125
Rev. 04/03 TransACT 2006
By signing below, I certify that all the information in this application is true and correct to the best of my knowledge.
Parent/Guardian Signature: _______________________ Date:_______
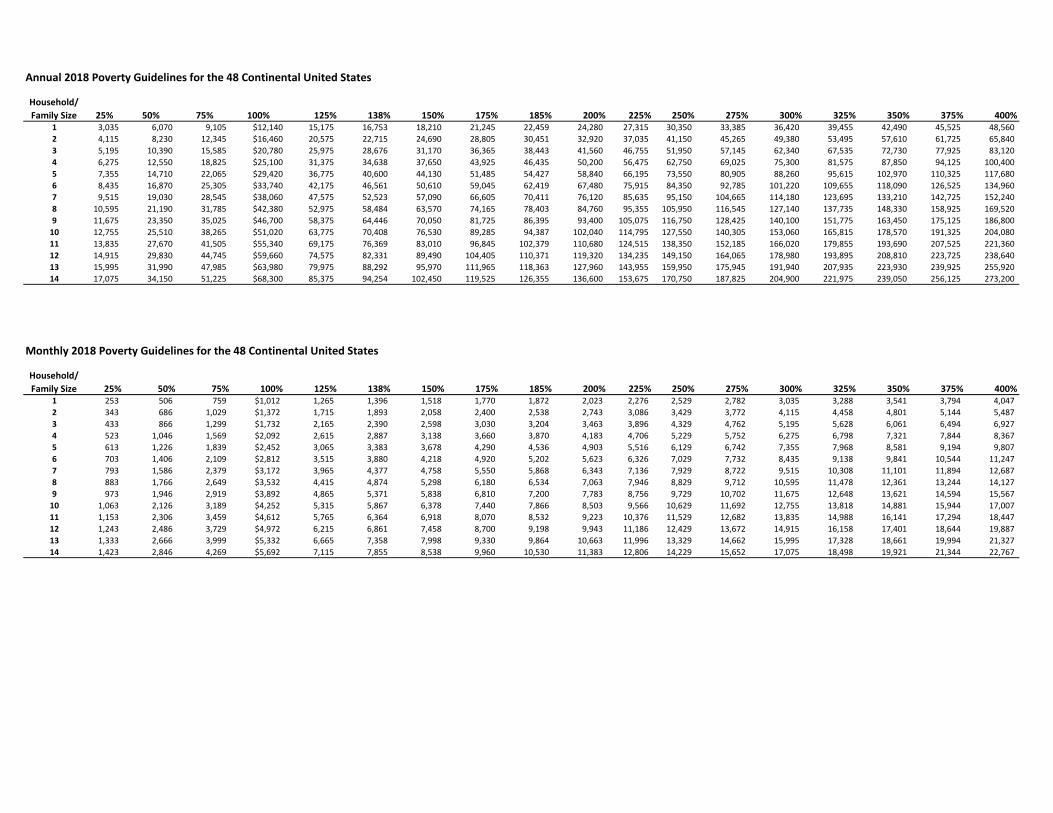
Annual 2018 Poverty Guidelines for the 48 Continental United States
Household/Family Size 25% 50% 75% 100% 125% 138% 150% 175% 185% 200% 225% 250% 275% 300% 325% 350% 375% 400%
1 3,035 6,070 9,105 $12,140 15,175 16,753 18,210 21,245 22,459 24,280 27,315 30,350 33,385 36,420 39,455 42,490 45,525 48,560 2 4,115 8,230 12,345 $16,460 20,575 22,715 24,690 28,805 30,451 32,920 37,035 41,150 45,265 49,380 53,495 57,610 61,725 65,840 3 5,195 10,390 15,585 $20,780 25,975 28,676 31,170 36,365 38,443 41,560 46,755 51,950 57,145 62,340 67,535 72,730 77,925 83,120 4 6,275 12,550 18,825 $25,100 31,375 34,638 37,650 43,925 46,435 50,200 56,475 62,750 69,025 75,300 81,575 87,850 94,125 100,400 5 7,355 14,710 22,065 $29,420 36,775 40,600 44,130 51,485 54,427 58,840 66,195 73,550 80,905 88,260 95,615 102,970 110,325 117,680 6 8,435 16,870 25,305 $33,740 42,175 46,561 50,610 59,045 62,419 67,480 75,915 84,350 92,785 101,220 109,655 118,090 126,525 134,960 7 9,515 19,030 28,545 $38,060 47,575 52,523 57,090 66,605 70,411 76,120 85,635 95,150 104,665 114,180 123,695 133,210 142,725 152,240 8 10,595 21,190 31,785 $42,380 52,975 58,484 63,570 74,165 78,403 84,760 95,355 105,950 116,545 127,140 137,735 148,330 158,925 169,520 9 11,675 23,350 35,025 $46,700 58,375 64,446 70,050 81,725 86,395 93,400 105,075 116,750 128,425 140,100 151,775 163,450 175,125 186,800
10 12,755 25,510 38,265 $51,020 63,775 70,408 76,530 89,285 94,387 102,040 114,795 127,550 140,305 153,060 165,815 178,570 191,325 204,080 11 13,835 27,670 41,505 $55,340 69,175 76,369 83,010 96,845 102,379 110,680 124,515 138,350 152,185 166,020 179,855 193,690 207,525 221,360 12 14,915 29,830 44,745 $59,660 74,575 82,331 89,490 104,405 110,371 119,320 134,235 149,150 164,065 178,980 193,895 208,810 223,725 238,640 13 15,995 31,990 47,985 $63,980 79,975 88,292 95,970 111,965 118,363 127,960 143,955 159,950 175,945 191,940 207,935 223,930 239,925 255,920 14 17,075 34,150 51,225 $68,300 85,375 94,254 102,450 119,525 126,355 136,600 153,675 170,750 187,825 204,900 221,975 239,050 256,125 273,200
Monthly 2018 Poverty Guidelines for the 48 Continental United States
Household/Family Size 25% 50% 75% 100% 125% 138% 150% 175% 185% 200% 225% 250% 275% 300% 325% 350% 375% 400%
1 253 506 759 $1,012 1,265 1,396 1,518 1,770 1,872 2,023 2,276 2,529 2,782 3,035 3,288 3,541 3,794 4,047 2 343 686 1,029 $1,372 1,715 1,893 2,058 2,400 2,538 2,743 3,086 3,429 3,772 4,115 4,458 4,801 5,144 5,487 3 433 866 1,299 $1,732 2,165 2,390 2,598 3,030 3,204 3,463 3,896 4,329 4,762 5,195 5,628 6,061 6,494 6,927 4 523 1,046 1,569 $2,092 2,615 2,887 3,138 3,660 3,870 4,183 4,706 5,229 5,752 6,275 6,798 7,321 7,844 8,367 5 613 1,226 1,839 $2,452 3,065 3,383 3,678 4,290 4,536 4,903 5,516 6,129 6,742 7,355 7,968 8,581 9,194 9,807 6 703 1,406 2,109 $2,812 3,515 3,880 4,218 4,920 5,202 5,623 6,326 7,029 7,732 8,435 9,138 9,841 10,544 11,247 7 793 1,586 2,379 $3,172 3,965 4,377 4,758 5,550 5,868 6,343 7,136 7,929 8,722 9,515 10,308 11,101 11,894 12,687 8 883 1,766 2,649 $3,532 4,415 4,874 5,298 6,180 6,534 7,063 7,946 8,829 9,712 10,595 11,478 12,361 13,244 14,127 9 973 1,946 2,919 $3,892 4,865 5,371 5,838 6,810 7,200 7,783 8,756 9,729 10,702 11,675 12,648 13,621 14,594 15,567
10 1,063 2,126 3,189 $4,252 5,315 5,867 6,378 7,440 7,866 8,503 9,566 10,629 11,692 12,755 13,818 14,881 15,944 17,007 11 1,153 2,306 3,459 $4,612 5,765 6,364 6,918 8,070 8,532 9,223 10,376 11,529 12,682 13,835 14,988 16,141 17,294 18,447 12 1,243 2,486 3,729 $4,972 6,215 6,861 7,458 8,700 9,198 9,943 11,186 12,429 13,672 14,915 16,158 17,401 18,644 19,887 13 1,333 2,666 3,999 $5,332 6,665 7,358 7,998 9,330 9,864 10,663 11,996 13,329 14,662 15,995 17,328 18,661 19,994 21,327 14 1,423 2,846 4,269 $5,692 7,115 7,855 8,538 9,960 10,530 11,383 12,806 14,229 15,652 17,075 18,498 19,921 21,344 22,767
Revised February 2011
Administrative Procedures Appendix #6a Income and Family Size Verification Guidance
Income Verification Guidance: The following are included in verifying income:
• Earned income from all sources including gross wages from work, cash, and in‐kind payments received by an individual in exchange for services and net income from self employment
• Unearned income including cash and contributions received by an individual for which the individual does not perform a service such as alimony, child support, military family allotments or other regular support from an absent family member, pensions, public assistance (including Temporary Assistance for Needy Families, Supplemental Security Insurance, Emergency Assistance money payments and non‐Federally Funded General Assistance or General Relief money payments), and dividends, interest, net income, net royalties and periodic receipts from estates or trusts.
• Unearned benefits received periodically by an individual, such as unemployment compensation, workman’s compensation, gambling or lottery winnings, or retirement benefits.
Income Deductions: The following are deducted when determining family income:
• Voluntary or court‐ordered child support or child support paid by the parent or caretaker or family member to a present or former spouse not residing in the same household.
• A medical expense not reimbursed through medical insurance that exceeds 10% of the family gross monthly income.
Income Exclusions: The following are excluded when determining family income:
• Employment earnings of an individual who is an emancipated minor
• Tax refunds, including earned income tax credits
• Withdrawals of bank, credit union or brokerage deposits or money borrowed
• Loans or grants, such as scholarships or income from federal student aid or participation in work‐study program
• Payments to Volunteers in Service to America, such as AmeriCorps or Foster Grandparent programs
• Any foster care payments by a foster care placement agency, including payments to permanent legal custodians or adoption assistance payments by county children and youth agency
• Food Stamps Whose Income is Counted?:
• The parent or caretaker of the child
• The parent or caretaker’s spouse or the other biological parent if living together
• Children’s, excluding a child’s earned income
Revised February 2011
• “Caretaker” means the father or mother of a child, an adult who has legal custody of a child, an adult who is the guardian of a child, or an adult who stands in loco parentis, as defined in this rule, with respect to a child and whose presence in the home is needed as the caretaker of the child.
• “Spouse” means married to the parent of the eligible child. If not married but residing with the parent of the eligible child, person’s income does not count.
Time Period: The period of time for income verification is the twelve months immediately preceding the month in which the application or reapplication for enrollment of a child is made, or for the calendar year immediately preceding the calendar year in which the application or reapplication is made. Verification of Income:
• Acceptable verification of earned income from employment includes pay stubs reflecting earnings, W‐2 forms, the IRS form used for reporting tips, a written employer statement of anticipated earnings or other document that establishes the parent’s or caretaker’s anticipated earnings from employment.
• Acceptable verification from self employment includes tax returns, business records or other documents establishing profit from self employment.
• Acceptable verification of unearned income includes a copy of a current benefit check, an award letter that designates the amount of a grant or benefit, such as a letter from the Social Security Administration stating the amount of the social security benefit, a bank statement, a court order, or other document or data base report that establishes the amount of unearned income.
• If a family receives or pays child support, the eligibility agency shall verify the amount of support received or paid by the family by documents from the Department of Public Welfare.
Acceptable forms of documentation maintained on file include, but are not limited to:
• Paystubs‐ a minimum of one if the year to date salary is included, if no year to date, 3 paystubs should be maintained
o Income is determined by calculating the weekly or monthly income and multiplying it by the appropriate multiplier, 52 for weekly, 26 for bi‐weekly, 12 for monthly
o If the paystub income varies, calculate the average rate and multiply by # of stubs used/# the multiplier (see above). EXAMPLE: 3 stubs equaling $900.00, 1200.00 and 950.00 if the average rate is $1016/week * 52 weeks the annual salary is $ 52,832.00 Assuming this is a family of 3 or more, the child is eligible
• W‐2’s‐ a copy of all family members W‐2 should be maintained. Income is typically counted from box #1 on the W‐2s
o Family is identified as the parent/guardian responsible for the child o If the parents are living with grandparents, the grandparent’s income would not be
taken into consideration unless they are the guardian • Tax forms‐ a copy of the current or prior year’s form • Employer Verification‐ A letter provided by the employer, including employer contact
information, verifying wages and number of hours worked
Revised February 2011
• TANF‐ Cash assistance TANF award documentation • CCIS Eligibility Detail Page • Food Stamps Case number • Family Letter indicating No Income • Disability documentation • Unemployment documentation
Note: COMPASS may be used to verify eligibility if the system indicates the family receives TANF or Food Stamps. No other information provided on COMPASS is acceptable for income verification. Pre‐K Counts Providers are still required to collect the family size and income for data entry in PELICAN.. Family Size The number of people in the house to be counted for the purposes of reporting “family size” include the child or children for whom PA Pre‐K Counts is being requested and the following individuals who live with that child or children in the same household:
• Parent of the child. The parent is the biological or adoptive mother or father, stepmother or father, caretaker and spouse who exercise care and control over the child requesting PA Pre‐K Counts.
• A biological, adoptive, unrelated or foster child or stepchild of the parent or caretaker who is under 18 years of age and not emancipated.
• A child who is 18 years of age or older but under 22 years of age who is enrolled in high school, a general educational development program, or a post‐secondary program leading to a degree, diploma or certificate and who is wholly or partially dependent on the income of the parent or caretaker or spouse of the parent or caretaker.
• Foster children should be entered as a family size of 1.
Related Documents











