All Naive Patients Are Not Equal: When and How to Start ART Therapeutic Management Strategies (WELP03) XVI International AIDS Conference, Toronto, August 2006 Jens D. Lundgren, M.D. Professor – University of Copenhagen Director - Copenhagen HIV Programme (www.cphiv.dk )

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

All Naive Patients Are Not Equal: When and How to Start ART
Therapeutic Management Strategies (WELP03) XVI International AIDS Conference, Toronto, August 2006
Jens D. Lundgren, M.D.
Professor – University of CopenhagenDirector - Copenhagen HIV Programme (www.cphiv.dk)
Case 1
•38 year old HIV-infected male – born and raised in Denmark
•Followed in clinic for last 3 years•Past medical history: no chronic diseases,
herpes zoster 5 years previously•Current evaluation: no clinical evidence of
immunodeficiency•No medications•Understands treatment issues and wants to
begin therapy if you think it is appropriate
If his viral load is 30,000 c/ml, above what CD4 threshold would you recommend deferring therapy?1. 750 cells/µl2. 500 cells/µl3. 350 cells/µl4. 300 cells/µl5. 250 cells/µl6. < 200 cells/µl7. Would observe8. Would treat at any CD4 count

CD4-guided deferral of ART
• Precondition: asymptomatic patient • If eg. fatigue and seborrheic dermatitis then treat
• Two essential questions in case ART is deferred: • Is there a threshold or a gradient of risk
according of CD4 counts for contracting AIDS ?•Biological question
• When is the risk of AIDS acceptable low ?•Treatment programme question
–public health vs. individual patient

Risk of disease progression andcurrent CD4+ lymphocyte cell count
0
20
40
60
80
100
Current CD4+ cell count (cells/µL)
%p
rog
ress
ed
Death
AIDS
300 250 200 150 100 50 0
EuroSIDA

N OIs: 134 45 13 9 2 2 89 55 61 35 13 16 12 9 10 11 11 14
0,01
0,1
1
10
100
0,01
0,1
1
10
100
0,01
0,1
1
10
100
Incidence of opportunistic infections for Incidence of opportunistic infections for various CD4+ cell count strata: various CD4+ cell count strata:
Traditionally believed thresholds value indicated Traditionally believed thresholds value indicated
EuroSIDA: Podlekareva EuroSIDA: Podlekareva et alet al, JID 2006, JID 2006
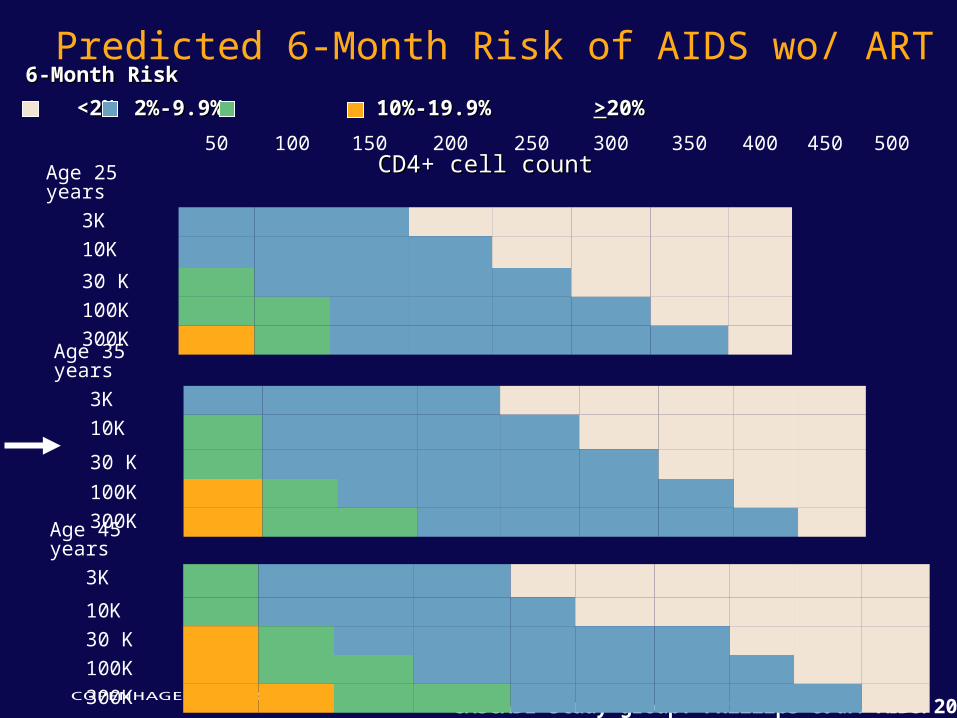
Predicted 6-Month Risk of AIDS wo/ ART
CASCADE study group: Phillips et al. AIDS. 2004
50 100 150 200 250 300 350 400 450 500
Age 25 years 3K
10K
30 K
100K
300KAge 35 years 3K
10K
30 K
100K
300KAge 45 years 3K
10K
30 K
100K
300K
6-Month Risk6-Month Risk
<2%<2% 2%-9.9% 2%-9.9% 10%-19.9% 10%-19.9% >>20%20%
CD4+ cell countCD4+ cell count
Case 1d
•38 year old HIV-infected male immigrated from Mali 3 years previously
•Followed in clinic for last 3 years•Past medical history: no chronic diseases, herpes zoster 5
years previously•Current evaluation: Miliary TB – just initiated 4 drug Tx•No medications•Laboratory:
– CD4: 25 cells/µL– HIV-RNA: 145.000 c/mL
•Understands treatment issues and wants to begin therapy if you think it is appropriate
You recommend to
1. Initiate ART – to enhance benefit of specific TB treatment
2. Initiate ART – to reduce risk of other opportunistic diseases
3. Defer ART for 2-3 months – to reduce risk of immune reconstitution disease
4. Defer ART – this episode of TB should not impact on decision to initiate ART

Incidence of AIDS-Defining EventsAfter Initiation of HAART
ART-CC: d’Arminio Monforte et al. Arch Intern Med. 2005
Period After Starting HAART (mo)Period After Starting HAART (mo)
Inci
den
ce
(pe
r 1
00
0 p
ers
on
ye
ars
)
Period After Starting HAART (mo)Period After Starting HAART (mo)
0
5
10
15
20
25
0-3 0-3 4-5 7-12 4-5 7-12 13-24 25-3613-24 25-36
Mycobacterium aviumMycobacterium avium Disease Disease
0
5
10
15
20
25
0-3 0-3 4-5 7-12 4-5 7-12 13-24 25-3613-24 25-36
Kaposi’s SarcomaKaposi’s Sarcoma
Inci
den
ce
(pe
r 1
00
0 p
ers
on
ye
ars
)
0
5
10
15
20
25
Period After Starting HAART (mo)Period After Starting HAART (mo) 0-3 0-3 4-5 7-12 4-5 7-12 13-24 25-3613-24 25-36
Pneumocystis jiroveci Pneumocystis jiroveci PneumoniaPneumonia
Inci
den
ce
(pe
r 1
00
0 p
ers
on
ye
ars
)
0
5
10
15
20
25
Period After Starting HAART (mo)Period After Starting HAART (mo) 0-3 0-3 4-5 7-12 4-5 7-12 13-24 25-3613-24 25-36
Cytomegalovirus DiseaseCytomegalovirus Disease
Inci
den
ce
(pe
r 1
00
0 p
ers
on
ye
ars
)

Prognosis from starting ART according to pre-therapy CD4 cell counts and HIV-
RNA levelsCD4 Cell Count (cells/CD4 Cell Count (cells/µL)µL)
ART CC. Egger et al, Lancet. 2002
Pro
bab
ility
of
AID
S o
r D
eath
(%
)P
rob
abili
ty o
f A
IDS
or
Dea
th (
%)
Years From Starting ARTYears From Starting ART
0 1 2 30 1 2 3
0-490-49
50-9950-99
>>350350
2525
2020
1515
1010
55
00
100-199100-199
200-349200-349

Immune restoration disease:Clinical deterioration after initiation of ART
• Definition• Worsening symptoms of inflammation• Temporally association with initiating ART• Atypical symptoms not explained by newly acquired infection• > 1 log10 HIV-RNA
• Case-control study matched for CD4 count:• # prior opportunistic infections (eg: TB, MAC, cryptococcus) • CD8+ counts • baseline levels of ALT• haemoglobin levels
• Remains undefined whether delay of ART reduce risk of IRD• Risk of fatal outcome presumably minimal is appropriately
managed (specific antiinfective and antiinflammatory medication)
Robertson Robertson et alet al CIDCID 2006; Shelburne 2006; Shelburne et alet al AIDSAIDS 2005 2005
Case 1e•38 year old native HIV-infected male•Followed in clinic for last 3 years•Past medical history: no chronic diseases, herpes zoster 5 years
previously, HBeAg+•Current evaluation: Asymptomatic•Liver biopsy: moderate fibrosis (F2)•Lab
– HBV-DNA = 28.000 IU/mL– ALT: x 2– CD4: 448 cells/µL
•No medications•Understands treatment issues and wants to begin therapy if you
think it is appropriate

You recommend
1. Initiate lamivudine monotherapy2. Initiate adefovir monotherapy3. Initiate entecavir or adefovir4. Initiate high-dose alpha-interferon5. Initiate ART – including TNF and
FTC/3TC6. Initiate ART – including 3TC7. Defer all treatment
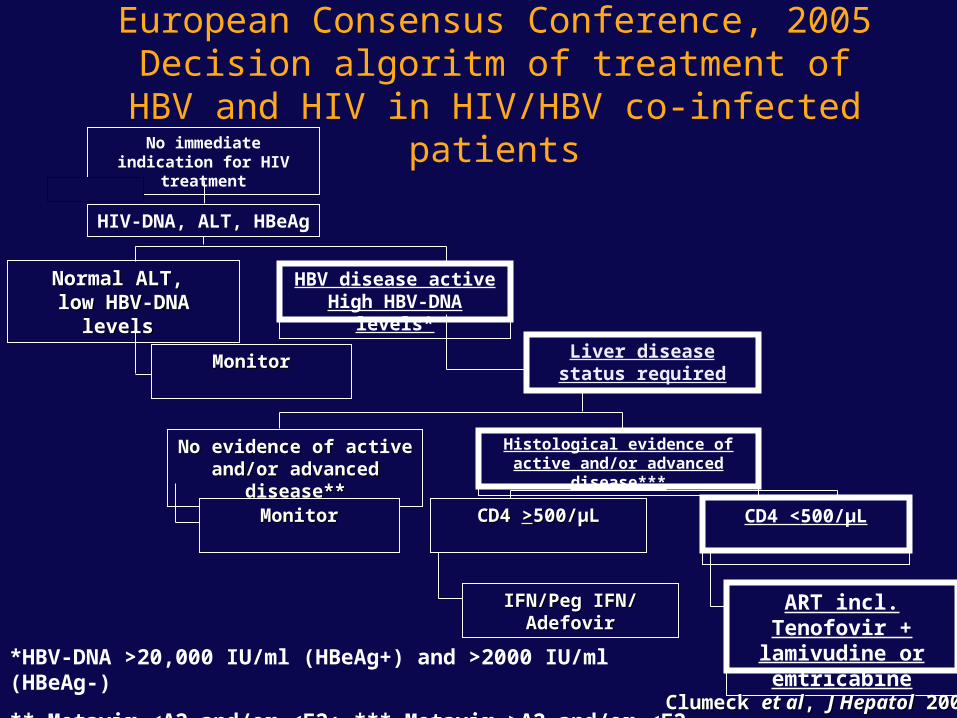
Normal ALT, Normal ALT, low HBV-DNA low HBV-DNA
levels levels
No immediate indication for HIV
treatment
HIV-DNA, ALT, HBeAg
HBV disease activeHigh HBV-DNA
levels*
MonitorMonitor Liver disease status required
No evidence of active No evidence of active and/or advanced and/or advanced
disease**disease**
Histological evidence of active and/or advanced
disease***
MonitorMonitor CD4 CD4 >>500/µL500/µL CD4 <500/µL
IFN/Peg IFN/ IFN/Peg IFN/ AdefovirAdefovir
ART incl. Tenofovir +
lamivudine or emtricabine
*HBV-DNA >20,000 IU/ml (HBeAg+) and >2000 IU/ml (HBeAg-)
** Metavir <A2 and/or <F2; *** Metavir >A2 and/or <F2
European Consensus Conference, 2005Decision algoritm of treatment of HBV and
HIV in HIV/HBV co-infected patients
Clumeck Clumeck et alet al, , J HepatolJ Hepatol 2005 2005

Deaths in D:A:DMultivariable relationships with death rate
latest CD4 count
1 10 100
Relative rate (95% CI)
>500
200-349
100-19950-99<50
350-499
>500
200-349
100-19950-99
<50
350-499
All-cause mortality
Liver-related mortality
Latest CD4 count
D:A:D study: Weber D:A:D study: Weber et alet al, , Arch Intern MedArch Intern Med 2006 2006

Case 1f
•38 year old native HIV-infected female•Followed in clinic for last 3 years•Past medical history: no chronic diseases, herpes zoster 5
years previously•Current evaluation: no clinical evidence of
immunodeficiency•No medications•Understands treatment issues and wants to begin therapy if
you think it is appropriate•Lab results:
–CD4: 240 cells/µL–HIV-RNA 48.500 c/mL

You recommend that she starts:
1. 2 nRTIs and an NNRTI2. 3 nRTIs and an NNRTI3. 2 nRTIs and a boosted PI4. 3 nRTIs 5. Boosted PI monotherapy6. Some other kind of regimen

Systematic Overview of 49 Clinical Trials: ART in Treatment-Naïve Patients
0
20
40
60
80
100
HIV RNA <50 copies/mLHIV RNA <50 copies/mL
Pat
ien
ts (
%)
Pat
ien
ts (
%)
64%*64%*
ART RegimensART Regimens
BoostedBoostedPIPI
NNRTINNRTI NRTINRTI PIPI
64%*64%*
51%51%††
44%44%
0
50
100
150
200
250
CD4 Cell Gain (cells/mmCD4 Cell Gain (cells/mm33))
Gai
n (
cells
/mm
Gai
n (
cells
/mm
33 ))
209209‡‡
ART RegimensART Regimens
BoostedBoostedPIPI
NNRTINNRTI NRTINRTI PIPI
174174
150150§§
178178
1994 to March 2004 (n=13,137 patients).1994 to March 2004 (n=13,137 patients).**PP<0.01 vs NRTI and PI; <0.01 vs NRTI and PI; ††PP<<0.05 vs PI; <<0.05 vs PI; ‡‡PP<<0.003 vs NNRTI, NRTI, PI; 0.003 vs NNRTI, NRTI, PI; §§PP<0.05 vs NNRTI and PI.<0.05 vs NNRTI and PI.
Bartlett JA et al. JAIDS 2006
Efavirenz and teratogenecity• Product information: Possible evidence of human fetal risk• Animal studies: signal of CNS defects• Birth defects among live-born pregnancies in humans
• while exposed to EFV during 1st trimester (two studies)• 5/228 with defects: 2.2% (95% CI: 0.7 – 5.1)• 0/19 with defects: 0.0% (0%-17.6%)
• General population• 3.1% (95% CI: 3.1%-3.2%)
• For women of child-bearing potential on efavirenz• Planning to become pregnant: switch to other ARV drug• Not planning to become pregnancy and proper
contraceptives are used: continue• If pregnancy has occurred: don’t panic (don’t stop ART;
don’t recommend uniformly abortion), switch to other drug
AIDS Res TherapyAIDS Res Therapy 2006;3:11; 2006;3:11; www.APRregistry.com; ; Birth defects researchBirth defects research 2003;67:617; 2003;67:617; JAIDS JAIDS 2005;40:116 2005;40:116

Drug resistent mutations (DRM’s) in HIV from ART-naive patients
• Prevalence: remains < 10-15% • Reflects drug consumption: type and coverage• In regions with reasonable coverage (>5-10% of
the infected population on ART) or in patients specifically suspected for harbouring resistant virus• Do a resistance test
• Let the decision on which drugs to use depend on results from resistance test• Current situation do not warrant revisions of
general treatment guidelines
J Clin VirolJ Clin Virol 2004;30:1; 2004;30:1; J Clin VirolJ Clin Virol 2003;26:153, 2003;26:153, JACJAC 2005:56:265 2005:56:265 AIDSAIDS 2004;18:1571 / 18:1683; 2004;18:1571 / 18:1683;
JIDJID 2005;192:958; 2005;192:958; AVTAVT 2004;9:375; 2004;9:375; Eur J Med ResEur J Med Res 2004:9:2732004:9:273

Comparison of coformulated dual NRTI Comparison of coformulated dual NRTI backbonesbackbones
AZT / 3TC ABV / 3TC TFV / FTC
convenience one pill bd one pill qd one pill qd
AZT/ABV/TFV:Acute
Long-term
nauseaheadacheanaemia
mitochondrial
lipodystrophy
hypersensitivity
Non identified
negligible
kidney/bone (?)
3TC/FTC tox: negligible negligible uncertain

Summary
• Most patients in the western world initiate ART to late – beyond the point of debate on when to start
• Patients – off or on ART - with CD4 between 200-350 cells/µL are at increased risk of AIDS compared with patients with higher CD4 counts• Argument in favour of initiating ART prior to this level of disease
progression
• Patients with HIV-related symptoms should initiate ART regardless of CD4 level
• Timing of initiation of ART for patients presenting with severe opportunistic disease is not defined• Arguments favours initiating ART as soon as possible in cases of
severe immunodeficiency
• Use dual active drugs for chronic Hepatitis B virus infection • ART should consist of 3 drugs from two classes
Case 1b
•38 year old native HIV-infected male•Followed in clinic for last 3 years•Past medical history: no chronic diseases,
herpes zoster 5 years previously•Current evaluation: fatique and seborrheic dermatitis
•No medications•Understands treatment issues and wants
to begin therapy if you think it is appropriate

If his viral load is 30,000 c/ml, above what CD4 threshold would you recommend deferring therapy?
1. 750 cells/µl2. 500 cells/µl3. 350 cells/µl4. 300 cells/µl5. 250 cells/µl6. < 200 cells/µl7. Would observe8. Would treat at any CD4 count

When To Start Treatment? – Summary of Current Guidelines
Guidelines symptoms or
CD4 <200
CD4 200-350
CD4 >350
IAS-USA:JAMA 2004<www.iasusa.Org>
treat consider Monitor closely; watch for rapid CD4 decline;
DHHS:<www.aidsinfo.nih.gov>
treat offer defer if VL <100K; treat or defer if VL >100K
EACS, 2005<www.eacs.ws>
treat consider Defer

Pre-therapy Median CD4 cell count in ART-naive patients initiating ART in
Europe and North America
0
50
100
150
200
250
300
1995-6 1997 1998 1999 2000 2001 2002-3
Year of initiating ARTYear of initiating ART# pts: 1232 4785 4583 3699 3203 # pts: 1232 4785 4583 3699 3203 2783 1932 2783 1932 ART Cohort Collaboration, Lancet, 2006ART Cohort Collaboration, Lancet, 2006

1
5
10
50
100
Rat
e %
of
AID
S (
per
yea
r) –
no
te l
og
sca
le
0 .5 1 1.5 2Years from start of ART
0-49
50-199
200-349
350-499
500+
CD4 count (95% CI)
ART-Cohort Collaboration 2004
Up to what CD4 count is the risk of AIDS reduced if ART is started ?

Case 1c• 38 year old HIV-infected male immigrated from Mali 3
years previously• Followed in clinic for last 3 years• Past medical history: no chronic diseases, herpes zoster 5
years previously• Current evaluation: Pulmonary TB – just initiated 4
drug Tx• No medications• Laboratory:
– CD4: 630 cells/µL– HIV-RNA: 125.000 c/mL
• Understands treatment issues and wants to begin therapy if you think it is appropriate

You recommend to
1. Initiate ART – to enhance benefit of specific TB treatment
2. Initiate ART – to reduce risk of other opportunistic diseases
3. Defer ART for 2-3 months – to reduce risk of immune reconstitution disease
4. Defer ART – this episode of TB should not impact on decision to initiate ART
Related Documents










![[DBND01] Naive Dreamer - Naive Muse (2010)](https://static.cupdf.com/doc/110x72/568bda301a28ab2034a9d5d9/dbnd01-naive-dreamer-naive-muse-2010.jpg)
