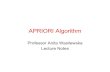
Congenital Heart Diseases Cyanotic Normal Flow RVH LVH Non Cyanotic Plethora CoA MR PS MS CoA Bayi LVH RVH VSD PDA ASD PAVSD PAPVD Oligemia Plethora TOF PS + Shunt Obstruktif + L→R PA Ebstein Anomaly Common Mixing Atrial • TAPVD • Uniatrial Common mixing AV • CAVSD Common Mixing Ventricle • Single ventricle • HLHS, TA, MA • DORV, DILV Truncus (A-P Window) TGA + VSD

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Congenital Heart Diseases
Cyanotic
Normal Flow
RVHLVH
Non Cyanotic
Plethora
CoAMR
PSMS
CoA Bayi
LVH RVH
VSDPDA
ASDPAVSDPAPVD
Oligemia Plethora
TOFPS + ShuntObstruktif + L→RPAEbstein Anomaly
Common Mixing Atrial• TAPVD• UniatrialCommon mixing AV• CAVSDCommon Mixing Ventricle• Single ventricle• HLHS, TA, MA• DORV, DILV Truncus (A-P Window)TGA + VSD

Common Mixing
• Pressure & saturation of O2 in Aorta & pulmonal is the same

PDA
Adolescent/Adult
HF (+) PH (-)HF (-) PH (+)
Premature Mature
Medical th/+
IndomethacinControlled Failed
Elective After >12 weeks
L→R L↔R
•Clinical•EKG•CXR•Echo
Medical th/
Closedspontaneously Ligation or Amplatzer Ductal Occluder Conservative
Controlled Failed
reactiveNon
reactiveElective After
>12 weeks
Cath
Neonate/Baby
HF :heart failurePH : Plumonary hipertensionIndomethacin 0,2 mg/kgbb 3x interval 12 hour
<10days

ASD
Big Shunt
Observe
PH (-)
HF (+)
PH (+)Evaluate5-8 yo Elective
> 1 yo
CathControlledFailed
Immediately
PVD (+)
•Clinical•EKG•CXR•Echo
Medical th/
Conservative Ligation or Amplatzer Septal Occluder Conservative
FR < 1.5 reactive Non reactive
Cath
Small Shunt
HF :heart failurePH : Plumonary hipertensionPVD : Pulmonary Vascular DiseasesASO tidak dapat dilakukan pada bayi < 8 Kg
FR > 1.5
Baby Adolescent Adult
HF (-)
> 1 yo
PVD (-)

VSD
HF (-)
ControlledFailed
PVD (+)
•Clinical•EKG•CXR•Echo
Medical th/
VSD Closure
Conservative
FR < 1.5reactive Non reactive
Cath
HF (+)
HF :heart failurePH : Plumonary hipertensionPVD : Pulmonary Vascular DiseasesReactive : PARI < 8 u/m2
FR > 1.5
Natural History
PVD (-)PABIf weight
< 3kg
Evaluate6 mo
ProlapsAo valve
StenosisInfundibulum
PulmonalHypertension Smaller
ClosedSpontaneously
CathCath 5 yo
CathPARI & FRRV : infundibularLV : VSD typeAo : prolaps

VSD + PH
Pulmonary Hypertension
Yes No or
High Flow
Follow upTill Pre School
Catheterization
PARI Flow ratio
Oxygen Test
< 8 u/m2 >8 u/m2
VSD Closure
< 8 u/m2 > 8 u/m2
< 1,5 > 1,5
High Flow

TOF
> 1 yo
Spell (+)
PROPANOLOL
Cath
ControlledFailed
•Clinical•EKG•CXR•Echo
TOTAL CORRECTION OPERATION
Cath
< 1 yo
BTS : Blalock Taussig ShuntPropanolol 0,5-1,5 mg/kg/dose 3-4x
CI : asthma
Spell (-)
BTS
PA/RV graphy
BTS
Cath
evaluate 6 mo
PA/RV graphy
Small PA Good size PA
Criteria for Operation– Good PA size– Good LV function
Cath– PA confluence/size– Anomaly coroner– MAPCA
Spell : – O2 100%– Knee Chest Position– MO 0,1 mg/kgbb– Diazepam 0,1 mg/kgbb– BicNat 3-5 meq/kgbb– Propanolol 0,02-0,1 mg/kg– Fenilefrine CI 2-5 mg/kgbb/mt IV 0,02 mg/kg IM 0,1 mg/kg
if not controlledVentilation BT Shunt,sat <30

BCPS CRITERIA
1. PAp < 18 mmHg
2. PARI < 4 Um2
3. PA Confluence
4. PA half size suitable (Kirklin)

CRITERIA FONTAN1. PAp < 15 mmHg2. PARI < 4 Um2
3. PA Confluence4. PA half size suitable (Kirklin)5. AV valve regurg. (-)6. LV dimension & function
adequate for Systemic Pump7. Arrhythmia (-)8. Age over 2-3 yo.

TGA
VSD (+)
LVOTO (-) LVOTO (+)< 1 mo > 1 mo
> 3 mo Dynamic LVOTOor
Can be resected
•Clinical•EKG•CXR•Echo
< 3 mo
ARTERIAL SWITCHARTERIAL SWITCH & PERFORATED VSD RASTELLI
LV > 2/3
PABCath
VSD (-)
LVOTO : left ventricular outflow tract obstruction
Cath
LV < 2/3
Cath
PARI< 8
PARI> 8
Can not be resected
BTS

SEQUENTIAL ANALYSIS
1. Established Atrial Situs
2. Ascertain Atrioventicular connexions
3. Decide Ventriculo-Arterial
4. Ascertain relationships– Right – Left & Anterior – Posterior
relationship

Morphology Right Atrium
• Atrial appendages “blunt ending”
• Receives Systemic Venous Return
• Coronary sinus enter to the smooth wall sinus venorum separated by from trabeculated right auricle by crista terminalis

Morphology Left Atrium
• Atrial Appendages “Finger Shaped”
• Receive blood from Pulmonary Vein
• Smooth walled is not separated from trabeculated wall by crista

Morphology Right Ventricle
• Coarse trabeculation of the wall• Shape “Rounded”• Contain infundibulum & tricuspid valve• Tricuspid valve separated from Pulmonary valve
by crista supraventricularis
trabecula septomarginalis• Insertion of papillary muscle of Tricuspid
– Single Anterior– Multiple Posterior– Medial

MORPHOLOGY LEFT VENTRICLE
• Fine Trabeculation
• Shape “ellipse”• Mitral valve & Ao Valve in fibrous continuity
• Bileaflet mitral valve• No medial papillary insertion, all to free wall

SITUSEstablished Atrial Situs• Situs Solitus
• Morphology right Atrium right side• Morphology left Atrium on the left side
• Situs Inversus• Morphology right Atrium left side• Morphology left Atrium on the right side
• Situs Ambigus• Not possible to separate right & left atria by
morphological

Situs Solitus
By Plain Ro• Right sided liverMeans / Inference Right Sided• Inferior vena cava & RA• Sinus Node• Tri-lobed, morphologically right Lung• Echo
– short axis Subxiphoid Thoracal XV A
Spine

Bronchial Branches
• Strong Xray
• Right side three lobed distance from bifurcatio shorter
• Left side two lobed distance from the bifurcatio shorter

• IVC always to RA
• In LA isomerism, there must be an interrupted IVC.
Azygos to SVC (Left)
Hemiazygos to SVC (right)
• SVC doesn’t always into RA, can be bilateral

SITUS AMBIGUS
By Plain Ro• Liver both side, stomach in the middleBilateral right lung type• RA isomerism• AspleniaBilateral left lung type• LA isomerism• Polysplenia

AV connection
• Discordant• Ambigus • Double inlet• Single inlet (univentricular)• Straddling,
– insertion of papillary muscle MV in RV or – insertion of papillary muscle TV in LV
• Overriding– Insertion papillary of overriding mitral in the LV
• Ventricle inversion can be determined by EKG– Normal V1 RSR, V6 qRS– Ventricle inversion V1 qRS, V6 RSR

VA c Ao onnection
• Physical examination– 2nd Heart sound single, not accentuated : PA– 2nd Heart sound single, loud : TGA
» Side by side» Anterior (Ao) posterior (P)
Normal
P
PP
Ao
AoAo

Hyperoxidation Test
• O2 100% 10-20 minutes
• Lung problem– Saturation O2 increased to 100%
• Cardiac problem – saturation O2 increased less than 30%

Posisi jantung dalam rongga toraks
5 Langkah Utama– Situs Atrial– Loop bulbo ventrikuler– Koneksi atrioventrikuler– Relasi kedua pembuluh darah utama– Koneksitas ventrikulo arterial
Anomali pada setiap segmen

SITUS ATRIALPANDANGAN SUBCOSTAL ( SAGITAL KORONAL )
Situs solitus : morfologi RA ada di kanan
morfologi LA ada di kiri
IVC ada di kanan kolum vertebrae ke RA
AoD ada di kiri kolum vertebrae
Situs Inversus : morfologi RA ada di kiri
moprfologi LA ada di Kanan
IVC ada di kiri kolum vertebrae ke RA
AoD ada di kanan kolum vertebrae

SITUS ATRIALSITUS ATRIALPANDANGAN SUBCOSTAL ( SAGITAL KORONALPANDANGAN SUBCOSTAL ( SAGITAL KORONAL ) )
Situs ambigus :RA isomerisme ( asplenia )
• Keduanya morfologi RA• IVS dan AOD satu sisi di kanan atau di kiri kolum
vertebrae.
LA isomerisme ( polisplenia )• Keduanya morfologi LA• IVS terputus melalui v. azygos / v.hemoazygos
masuk ke VCS dan RA

LOOP BULBO VENTRIKULER
D – loop : Morfologi RV di kanan
Morfologi LV di kiri
L – loop :Morfologi RV di kiri
Morfologi LV di kanan

Morfologi Ventrikel PANDANGAN PARASTERNAL DAN PANDANGAN APIKAL 4 RUANG
Ventrikel kanan • Katup trikuspid : lebih dekat ke apex
insersi khorda ke septum (+)• Moderator band• Trabekular kasar
Ventrikel kiri• Katup mitral ( bikuspid) : lebih jauh dari apex
Insersi khorda ke septum (-)• 2 muskulus papalaris besar ada di dinding ventrikel• Trabekel halus

Koneksi AtroventrikulerPANDANGAN APIKAL / SUBKOSTAL 4 RUANG
Konkordan :Morfologi RA berhubungan dengan morfologi RV
Morfologi LA berhubungan dengan morfologi LV
Diskordan : Morfologi RA berhubungan dengan morfologi
LV
Morfologi LA berhubungan dengan morfologi RV

Koneksi AtroventrikulerPANDANGAN APIKAL / SUBKOSTAL 4 RUANG
Ambigus :Apa bila morfologi ke 2 atrium : RA atau LA
(ambiogus)
Double inlet : Kedua atrium berhubingan dengan satu ventrikel
Satu katup AV absen Atresia katip trikuspid atau katup mitral

Relasi kedua pembuluh darah utamaPANDANGAN PARASTERNAL SUMBU PENDEK
A. Pulmonalis : bifucartio
bercabang dua
Relasi normal : Aorta di posterior kanan PA
Malposisi Aorta di : Anterior PA
Anterior kiri PA
Kiri dan kanan PA ( side by side )

Anomali tiap Segmen Jantung
Alir balik vena : sistemik Bilateral SVC pulmonal APVD
Rongga atrium : Septal atrium ASD
Cor triatriatum
Atrioventrikular junction : Katup AV : stenosis, atresia, cleft, regurgitasi, stradlling Septum : AVSD

Anomali tiap Segmen Jantung
Rongga ventrikel :Anomalous muscle band
VSD
Obstruksi alur keluar
Pembuluh darah Utama :Katup : stenosis, atresia, regirgitasi,
overriding
PDA , AP window
Arkus aorta : koartasio aorta, interuptus

KESIMPULAN
• Ekokardiografi 2 dimensi paling penting untuk diagnosis PJB
• Diagnosis lengkap dan akurat bila dilakukan secara sistimatis ( analisa squensial )
• Pemeriksa harus :1.Mengerti anatomi dan morfologi jantung
2.Mengetahui gambaran karakteristik dari echo 2 D
3.Trampil dan teliti

Hyperoxidation Test
• O2 100% 10-20 minutes
• Lung problem– Saturation O2 increased to 100%
• Cardiac problem – saturation O2 increased less than 30%

DORV
VSD non Committed
PS (-)PS (+) PS (+)PS (+) PS (-)
TOFalgorithm
PS Nonresectable
•Clinical•EKG•CXR•Echo
PAB
INTRAVENTRICULARTUNNELLING
CONSER
VATIVE
FONTANTCPC
Reactive NonReactive
Cath
VSD Subaortic
DORV : Double Outlet Right VemtriclePAB : Pulmonary Artery BandingBTS : Blalock-Taussig ShuntBCPS : Bi Cavo-Pulmonary ShuntPS : Plumonary StenosisTB : Taussig Bing
VSD SADC VSD SP (TB)
Cath Cath
PAB
< 1 yo
Cath
BTS
EXTRACARDIAC CONDUIT/ FONTAN
PS resectable
ARTERIAL / ATRIALSWITCH
CONSER
VATIVE
> 3 mo< 3 mo
reactive Nonreactive
PS (-)
CathCath
BTS < 6 mo < 6 moPAB
BCPSBCPS

Taussig Bing
• Echo– Great arteries side by side– Conus between
• MV & PV • PV & Ao poss. Stenosis post arterial switch.
– Often associated with Ao Arch Hypoplastic
IN TGA there uss. Without Conus.

APVD
Partial
Obstruction (+)
PH (-)
•Clinical•EKG•CXR•Echo
TAPVD CORRECTION
Cath
Total
APVD : Anomaly Pulmonary Vein DrainageSVD : Sinus Venosus DefectBAS : Ballon Atrial Septostomy
Obstruction (-)
BAS
Cath
Supra cardiacIntra cardiacInfra cardiac
PH (+)
PH (+) PH (-)
CONSERVATIVE INTRA ATRIAL BAFFLE
REACTIVE NON REACTIVE REACTIVE

PA + IVS
Tricuspid ValveScore 2 > - 4
< 6 mo
Tricuspid ValveScore 2 < - 4Sinusoid RV
Anomaly Coroner
BTS
> 6 mo
BCPS
Cath
Small PA Big PA
BTS
FONTAN /TCPC
PGE1 BAS
•Clinical•EKG•CXR•Echo
Cath
Valvotomy Pulmonal(closed)+ BTS
+ PDA ligation
ASD CLOSURE + PV REPAIR

PA + VSD
BABY & CHILDNEONATUS
Shunt
Cath
MAPCA (+) MAPCA (-)
Univocalisasi + BTS
RASTELLI OPERATION
PGE1
•Clinical•EKG•CXR•Echo
Cath
Selective Aortography

TRICUSPID ATRESIA
< 6 mo
•Clinical•EKG•CXR•Echo
FONTAN TCPC
Cath
PULMONARY FLOW
PGE1BAS/BH
Cath
< 6 mo > 6 mo
Pap > 15 mmhgPARI < 4 HRU
< 15 mmhg< 4 HRU
PULMONARY FLOW (N) PULMONARY FLOW
> 6 mo
BTS
BTS
Cath
PAB
Cath
> 15 mmhg< 4 HRU
PAB < 2 yo > 2 yo
BCPSBCPS
BCPS CONSERVATIVE

CONGENITAL AS
CHILD / ADULT
SeverePG > 4.75 cm2/m2
INFANT / BABY
BAV
Mild / ModeratePG > 4.75 cm2/m2
Cath
NORWOOD
•Clinical•EKG•CXR•Echo
FONTAN
ValvotomiAorta
Cath
Cath
PG > 60 mmhgPG < 60 mmhg• LV strain• Syncope• Chest Pain
Ao Valvotomy
BAV

COARCTATIO AORTA
CoA + VSD
Ao Arch Hypoplastic
SIMPLE CoA
Hypoplastic LV & MVHLH
•Clinical•EKG•CXR•Echo
CoArc RepairVSD Closure
REPAIR• E-E• Subclavian Flap• Patch
COMPLEX CoA
Ao Arch Normal
Single VSD Multiple/Big VSD
CoArc RepairPAB
Complete RepairIn CPB CoArc Repair
+Intra Cardiac
Repair
NORWOODHIGH RISK
FONTAN
Related Documents