-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
1/18
Workshop #8:"Health Insurance Exchang es: States in Charge!"ALEC S 381hAnnual M eetingThursday, August 4, 2011, 11:00 a.m. - 12:15p.m.La Galerie 2
Speaker BiosKevin Kuhlman is a M anager at the National Federation of Independent Businessfocusing his advocacy efforts on healthcare issues with M embers of Congress.NFIB is the nation's leading small business organization with over 350 ,000mem bers. For years, the rise in healthcare costs has been a top concern of NFIBmembers.Prior to his tenure at NFIB, K uhlman handled healthcare, labor, education andsmall business issues for Congressman Peter Roskam from the western suburbs ofChicago. He started his career on the Hill working as support and research stafffor the Com mittee on Ways and Means serving under C hairman Bill Thom as,Ranking M ember Jim McC rery, and then-Ranking M emberlnow-Chairman DaveCamp.Cheryl S. Smith is a Director at Leavitt Partners and helps guide the firm's healthinsurance exchange practice. Smith played a central role in developing andimplemen ting Utah's Health Insurance Exchange, one of only two functioningstate health insurance exchanges in the coun try.Prior to joining Leavitt Partners, Smith worked in the Utah Governor's Office ofEconom ic Developm ent as the Director of the Utah Health Exchange office. Herleadership and expertise drew national attention as U tah's health insuranceexchange was recognized in the Washington Post, The Boston G lobe, The WallStreet Jou rna l, Forbes.com, and BusinessW eek.com. Cheryl helped coordinateprojects and ensured adequate administrative and financial controls, quality, andprocedural efficiencies. She also managed the relationships between variousstakeholders, including the business comm unity, industry representatives, hospitalsand non-hospital providers, advocates and o ther interest groups.
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
2/18
In other work capac ities, Srni.thwas a Visiting Health Policy Fellow at TheHeritage Foundation in W ashington, D .C . While at Heritage she focused herresearch, analysis, and writing on the State Children's H ealth Insurance Program(SCHIP), Med icare drug pricing, and state health system reform.Smith has a B.A. in Political Science and a M aster of Public Policy (with anemphasis in health policy), both fiom Brigham Young University.Rep. Linda Upmeyer represen ts Iowa 's 12" District and currently serves asIow a's H ouse Majority Leader. She was first elected in 2002. Upm eyer is acardiology nurse practitioner.As a legislator, she serves on the Health and Human Services Task Force for theAm erican Legislative Exchange Council, and currently serves on their Board o fDirectors. She also serves on the Executive Committee of the Midwest Conferenceof State Governments.Upm eyer currently serves on the Administration and Rules Com mittee and hasformerly served on the Human Resources, Natural Resources, and EconomicGrowth comm ittees. Linda has also served on the Leadership Council andInternational Relations comm ittees.She is a former trustee for North Iowa Area C:ommunity College and a formerboard member of both .the National and Iowa Association of Community Co llegeTrustees.Upm eyer attended the University of Iowa, where she received her B .S. in Nursing.Sh e received her Master's in Nursing fiom Drake University.
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
3/18
Should Virginia Create a Health Insurance Exchange?Remarks byMichael F. CannonDirector of Health Policy Studies
Cato instituteiBefore theJoint Commission on Health CareRichmond, Virginia
June 14,2011Good morning, members of the Virginia Joint Coilmission on Health Care. I am verypleased to be with you today. My name is Michael F. Cannon. I am the director of health policystudies at the Cato Institute, a libertarian think tank in Washington, D.C.. The mission of the
Cato Institute is to promote the principles of individual liberty, limited government, free markets,and peace. I am also a 30-year resident of the Commonwealth of Virginia and a product ofVirginia public schools, from elementary through graduate school.Background
The most important health policy issue facing the Commonwealth is the fate of the healthcare law that President Barack Obama signed last year. That law is already increasing the cost ofhealth insurance by as much as 30 percent in some cases, and will cause even greater premiumincreases in the years to come.When that law takes full effect in 2014, it will set in motion several important changes.States are already struggling to pay for their current Medicaid programs. Starting in 2014, thislaw will add to those burdens with enormous unfunded mandates. The law's so-called"individual mandate" will compel nearly all Americans to purchase a nominally private butgovernment-designed health insurance policy. Those who fail to coinply will face penaltiesincluding fines andlor iinprisoml~ent.Finally, the law's health insurance "Exchanges" arescheduled to become operational in 2014. These new government bureaucracies would enforcethe law's regulations that will drive up health insurance premiums, and would distributehundreds of billions of taxpayer dollars to private health insurance companies, thereby driving upthe national debt.
-
The Health Care Law's Future Is in DoubtSupporters introduced the first draft of President Obama's health care law in Congress inJune 2009. A bipartisan majority or plurality of the American people have consistently opposedit ever since. A mere 38 percent of the public supports the law. Opposition is highest amonglikely voters. Officials representing 28 states and both political parties have filed suit to ovei-turnthe law. One of the two major political parties has committed itself to wholesale repeal.
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
4/18
A bipartisan majority of the General Assembly enacted legislation to block theellforcement of any such law in Virginia. The Conlm onwealth is suing the federal government(so far succ essfully) to have the ind ividual mand ate de:clared uncon stitutional, and has furtherasked the c ourts to strike down the entire act. In a sim.ilar case filed by 26 states and m anyprivate plaintiffs, a federal judge has struck down the entire law. These and othe r constitutionalchallenges ar e currently before federal appe llate court!;. Legal experts predict the U.S. Suprem eCou rt will ultimately rule on the law's constitutionalit:ysometime in the summ er of 2012.
Should Virginia Create a Health Insurance Exchange?Aga inst this backd rop, the most im med iate question facing state officials is whether tocreate a health insurance Exchange. In the remainder of ~ n yemarks, I will explain why,whether on e opposes or supports this law, the responsible course is not to create an Exchange.I am continually surprised by how many people around the country mistakenly believethe new law requires states to create an Exchange. To be clear: Virginia is under no o bligation
to create a health insurance Exchange. The authors of the health care law kn ew full well thatsuch a requirem ent wou ld be uncon stitutional. Instead, the law asks states to do the heavy liftingof creating these bureaucracies, offers thein considerable sums of money, and as a fallbackposition allows the federal government to create an Exchange if a state declines to do so.For state officials who ha ve taken the position that the federa l health ca re law isuncon stitutional, this should be an easy decision. Virginia officials, like state officialsnationw ide, take an oath to protect not just their ow11 state's Constitution, but also theCon stitution of the United States. They are therefore oath-bound to use all legal mean s to blocka law that they believe violates the U.S. Co nstitution. The sam e duty, then, that obliges them tosue to overturn the health care law also obliges them not to implement it. To implem ent this
health care law, such as by creating an Exchange, would be to violate their oath o f office.Regardless of whether one supports or opposes this law, however, the simplest and mostpowerful reason not to create an Exchang e is this: there is no money. Neither theCom monw ealth nor the federal government has money to waste on new government agenciesthat might be repealed or overturned tomorrow. Every dollar that Virginia spends on anExchange is a dollar it cannot spend on roads, education, or police. The Exchange planninggrant that Virginia has already received, and any federal additional funds the Com monw ealthmay receive, are adding to the nation's debt burden and bringing the United States closer to aGreek -style debt crisis. The fiscally responsible option, which many states have exercised, is tosend that money back to Washington and to refuse any additional funds.Exchange advo cates counter that Virginia must act now to ensure local control ofVirginia's health insurance market. This argument has even persuaded som e who oppose thelaw that they should create an Exchange as a way of hedging their bets in the event the lawremains on the boo ks. Yet this strategy rests on two faulty assumptions.The first is that creating an Exchange will give Virginia officials more control overVirginia's health insurance market. A recent Obam a administration missive explains that the
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
5/18
new law "authorizes [the federal governmeilt] to ensure that States with Exchanges aresubstantially enforcing the Federal standards.. .and to set up Exchanges in States that elect not todo so or are not substantia lly ei.zforcii7g rela tedyrovisions." (Eillphasis added.) In other words,the promise of local control is a mirage. The law allows the federal government to commandeerany Exchange that falls short of full compliance with federal dictates. Creating its ownExchange will not allow Virginia to control its o wl health insurance markets. In the end, there isno such thing as a state-run Exchange.
The second faulty assumption is that creating an Exchange will not affect whether the lawremains on the books. For several reasons, creating an Exchange would entrench the law andmake it less likely to be repealed or overturned.First, creating an Exchange lends the appearance of legitimacy to the law. The Obamaadministration heralds the creation of each new Exchange as proof that the law is gainingacceptance, and loudly interprets states accepting the federal grants available under thelaw in the same manner.Second, creating an Exchange undermines the credibility of state officials who areseeking to overturn the law. When these officials declare the law unconstitutional yetimplement it and accept the funding it offers, the media are correct to diagnose hypocrisy.Such duplicity is already undermining the lawsuits seeking to overturn the law. In hismost recent ruling, federal judge Roger Vinson wrote that the fact that some of theplaintiff states are implementing the law undercut their owl argument that he should haltall implementation.Third, to create an Exchange is to create a taxpayer-funded lobbyiilg group dedicated tofighting repeal. An Exchange's employees would owe their power and their paychecks tothis law. Naturally, they would join the fight to protect it.Fourth, Congress and the courts are less likely to eliminate actual governmentbureaucracies that have assembled dedicated constituencies than they are to eliiniilatetheoretical ones. The more disruptive repeal would be, the less likely it becomes.Fifth, if these bureaucracies begin handing out billions of taxpayer dollars in 2014, theprivate insurance companies who receive those subsidies will plow much of the nloneyback into fighting repeal.
The Obama administration is offering financial inducements to states to create Excl~angesbecause the administration knows that every new Exchange helps them shield the law fromCongress, the courts, and the American people. For opponents of the law, creating an Exchangeis less a hedging-your-bets strategy than a sabotaging-your bets strategy.
Some opponents of the law, most notably the conservative Heritage Foundation,recoinmend that states create "market-friendly" (i.e., non-compliant) Exchanges that offer an"alternative vision to ObamaCare." They will ultimately find this strategy self-defeating. AsThomas Jefferson explained more than 200 years ago: "The natural progress of things is for
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
6/18
liberty to yield, and g ov em ne nt to gain ground." Former Massachusetts Gov. Mitt Rornney (R)proposed a "m arket-friendly" health insurance Exchange in 2006. By the time it returned to hisdesk, it had becom e the very m arket-unfriendly plan on w hich Coilgress modeled PresidentObam a's health care law. The "market-friendly" Exchange that former Utah Gov. JimHuntsman (R) created in 2008 has also become increasingly less market-friendly. Wh en Utahpoliticians saw that health insurance was more expensive inside their Exchange than o n the op enmarket, they imposed a series of taxes on consulners outside of the Exchange to prop up thehealth plans in side it. In the process, Utah unwittingly put in place the infrastructure for afederal Exchange: if Utah's Exchange fails to com ply w ith the health care law in 2014, thefederal government w ill coinmandeer it or brush it aside.
There is simply no reason for Virginia to crea1:e any kind o f Exchange. A top U tahExchange official says, "Nearly every Exc l~an geunction a lready exists in the private sec tor."Heritage Foundatioil scholars want an E xc l~a ng e ecause they see it as a vehicle for enablingworkers to purchase their own health plan using tax-free dollars from their employers. AMinneapolis comp any called Bloom Health is already giving workers that freedom, without anynew government b ureaucracies or regulations.
Finally, I encourage the Co m niss ion to be m indful of conflicts of interest surroundingthe issue of health insuran ce Exchange s. The interests of those asking the legislature to create a nExchange m ay not line up with the interests of consume rs. For instance, private health insurancecompanies are lobbying state legislatures nationwide to create health insurance Exchanges. Thisactivism may be related to the fact that Exchanges are necessary for them to tap hundreds o fbillions of dollars of taxpayer subsidies. Sin ~ila rly,nsurance regulators and state health careofficials across the country have urged their g ovemol-s and legislatures to create an Exchange,which m ay stem from a fear that a federally administered Ex change would render them obsolete.Unfortunately, a state-run E xc l~a ng e annot save these state officials from obsolescence. Onlyrepealing o r overturning the health care law can do that.
ConclusionCreating an Exchange does not make the best of a bad situation. It makes the badsituation.The most responsible course for Virginia is to refuse to create an Exchange. Manygovernors, including Florida's Rick Scott (R) and Lo uisiana's B obby Jindal (R) have alreadydone so. Next, Virginia should send back to W ashington whatever funds it llas received underthis law, as Oklahom a, Wisconsin, Florida, and other states have don e. Virginia should send that
money back with a message that if Congress is looking to cut federal spending, it should startwith laws that federal courts have declared unconstitutional. At a minim um, Virginia shoulddefer the question o f creating a n Exchang e until the cou rts dispose of the constitutionalchallenges brought against this law. Legal scholars expect the U.S. Supreme Court to rule onthis law in the summ er of 2012. If the Cou rt upholds the law, Virginia would have time tosubmit an Exchange plan to W aslIington by the 2 0 13 deadline. If the Court voids the law,Virginia will be glad sh e waited.
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
7/18
In the meantime, there are other steps Virgiilia can take to make health insurance andmedical care more affordable to consumers.First, the General Assembly can permit Virgiilia employers and coilsuiners to purchasehealth insurance licensed by other states. Wyoming, Maine, and Georgia have already given
their residents this freedom. Enabling Virginians to purchase health insurance across state lineswould expand choice and competition, and would reduce premiums by letting consumers avoidunwanted regulatory costs. As important, granting Virginians this freedom would not requireany new government spending or the creation of any new govemnent bureaucracies. Suchlegislation has been introduced in the General Assembly in the past, though it has been opposedby domestic insurers who prefer what they call a "level playing field" - .e., where governmentblocks con~petition nd Virginians have fewer choices.Second, the General Assembly can make basic medical care inore affordable for the poorby broadening the scopes of practice of mid-level clinicians such as nurse practitioners andphysician assistants. One promising approach, similar to letting Virginians purchase health
insurance across state lines, is to let clinicians licensed by other states practice in Virginia underthe terms of their license but subject to Virginia's malpractice laws. Reforms such as thesewould spur the growth of retail clinics and other innovations that bring quality medical carewithin reach for more low-income Virginians.Third, the General Assembly can reduce unnecessary medical malpractice costs by givingpatients and doctors the freedoin to choose reforms such as caps on non-economic damages. Incontrast to mandatory caps on damages, this approach would make medical malpractice refoi-nlavailable to those who need it most, but still allow others to enjoy broader malpracticeprotections.Again, I am very pleased to be with you today, and I look forward to any questions youmay have.
' The Cato Institute is a nonpartisan, nonprofit, tax-exempt educational foundation organized under Section 501(c) 3of the Internal Revenue C ode. In order to maintain its independence, the Cato Institute accepts no go vem nen tfunding. Cato receives approximately 8 2 percent of its funding from individuals, 10 percent from foundations, 1percent from corporations, and the rem ainder the sale of publications. C ato's fiscal-year 2 009 revenues were over$20 million. Cato ha s approximately 105 full-tune employees, 75 adjunct scholars, and 23 fellows, plus interns.
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
8/18
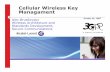
Sept 2010: Gov.Schwarzenegger signs Jan 2011: Exchange awsI exchange legislation l ~ ,o Into effectCalifornia < I >Jan 2010: Exchange 1 ~ Dec 2010: Apporntees to Apr 2011: First meetln g ofestablrshment egtslation Health B enefrt Exchange Exchange Board (flfth boardrntroduced (before PPACA) Board named member not yet named)
Early Mar 2011: Exchange Mid-M ar 2011: Gov. Deal June 2011: Gov. Deal signsestablishment legisla t~on shelves legislation due to Tea executive order creating anI introduced I Party opposition i exchange study panelGeorgia < >Feb 2011: Ins. Comm. I Early Mar 2011: I April 2011: Gov. Deal signs IHudgens announces plan Tea Party opposition Interstate Health Careto create an exchange Compact legislation
Idaho
Apr 2010: Act is approved Mar 2011:I by Gov. Barbour I Legislation failsMississippi < I >Mar 2010: Legislature I February 2011: Mul tiple May 2011: MS Comprehensive Healthpasses act to create exchange establishment bills Insurance Risk Pool Association Boardexchange study introduced in egislature votes to establish and operate the MScomm ittee Health Insurance Exchange
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
9/18
Health Care EquitableReimbursement actJane M. Orient, M.D.
Assn of American Physicians and Surgeons(AAPS) w ww.aapsonline.orgALEC 201 1, New Orleans
PricesFree-market: $6,500Chargemaster: $21,336.58=3.3~$6,500Insurance: f(c,n,x) = ? $5,500Marginal: 10 staff hrs, drugs, expendables,. $3,000
What is the purpose of thechargemaster rate?
PricesMedibid-agreed price: $6,500Hospital chargemaster: ??
Who pays chargemaster rate?Nobody?Rich, uninsuredGovernment (disproportionate share)3 "loss" 3 tax-exempt statusPerce ntage paid as "coinsurance," especia llyfor out-of-network patientsPatients with high-deductible insurance andno "re-pricing"
"Med ical care costs too much."Wall Street Journal ad
J Patrick Rooney
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
10/18
Insurance costs so much becausemedical care costs so much.Medical care costs so muchbecau se of "insurance" or third-party payment.
"If I had known that a C-section only costs$5,000, I wouldn't have spent so muchmoney on insurance!"--response to revelation about hospital's fixedprice arrang emen ts for obstetrical servicesto M exican nationals
Man aged care efficiency?Revenues: $6 51.8 millionSpent on "healthcare services": $554.3 milMLR: 85%Amount not spent on healthcare: $97.5 mil =1 0 , 0 0 0 ~10,00Osurgeries > 1,000 BMWs
Care lStHeath Plan, Arizona Health Care CostContainment System
Some free-market prices:ACL repair, $7,040Open rotator cuff repair, $6,160Bunion, $4,125Inguinal hernia, $2,860Lumbar laminectomy, $9,900Cochlear implant, $8,80 0
www.surgerycenterok.com
Medicaid spendingKaiser Family Foundation statehealthfacts.org
Purpose AZ/ .S.Managed care and health 83% 35%plansPhysicians, lab, xray 0.7%/ 6%In-patient hospital 4%/23%Pharmaceuticals 0.1%/7%
Characteristics of a free market?Discrimination on the basis of race, se x,age, ethnicity-or health planGovernment fundingProtection moneySecret agreementsHidden prices ("nontransparency")
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
11/18
Congress needs to provide statesMedicaid flexibilityby Congresswom an Cathy M cMorris R odgers and Jason MercierFebruary 15,2011
Whn President Obama s igned theunpopula r Patient Protection andAffordable Care Act last year, he m ad ema ny promises, including that the lawwould increase health c are access andlower costs. As states begin the processof devising their an nual budgets, it's m oreclear than ever that those promises aren'tbeing kept - especially in our h ome stateof Washington.Wa shington State officials last yeardebated opting-o ut of the federalMedicaid program so they could preserveflexibility in providing health careservices to needy families. Current lyWashington faces a projected $5 billionstate budget shortfall. The alternative toopting-out of Medicaid is the potentialelimination of all state-only health careprogram s such as the Basic Health Plan,prescription dr ug coverage, and theDisability Lifeline program.The new federal health care law imposesa Medicaid M aintena nce of Eligibilityrestriction o n the states that prohibitslocal elected officials from m akin greductions. This restriction, comb inedwith loom ing state budget deficits, meanslegislators an d governors a re faced withthe painful decision of funding state-only health care programs o r providingmatch ing fun ds for federal Medicaiddollars - hey can't do both. Alreadyhealth officials in Nevada an d Wyo minghave drafted white papers discussing thepossibility of opting-out of Medicaid t opreserve m ore bu dget flexibility. Similarconversations are occurring across thecoun try in blue states like Washingtonan d red sta tes like Texas. This problemtranscen ds which party controls a
state's budget an d d em ands bi-partisanCongressional suppo rt for Medicaidreform.Though a state actually opting-out ofMedicaid remains unlikely, the fact thatit is openly being discusse d signifies theneed for states to have mo re flexibilityin the Medicaid program. Otherw isestate health care spending will be limitedto adminis tering the federal Medicaidprogram at the expense of state-directedpriorities.While the new Republican majority inthe H ouse will not provide states anotherfederal bailout, working with the Senate,Congress can reform the Medicaidprogram to provide states the discretionto make local health care decisions. Weare working on a proposal to do just this.Unless states are provided mo re flexibilityover Medicaid sp end ing they will beforced to either opt-out of the program oreliminate state-only healthcare priorities.A better strategy would be for Congressto transform the cur rent categoricallyrestricted Medicaid program , whichis dictated by D.C. priorities, into anindexed block grant program tha twould allow each stat e to design acomprehensive state-based health caresystem that meets the unique ne eds andpriorities of their citizens while protectingthe m ost vulnerable.Many states are already asking th e federalgovernment for this type of Medicaidtlexibility, includin g legislators he rein Washington. Last mon th SenatorsLinda Evans Parlette, Joe Zarelli, RandiBecker and M inority Leader Mike
Hewitt introduced SB 5596 to require theDep artm ent of Social and Health Servicesto request an indexed Medicaid blockgrant waiver to "allow the state to opera teas a laboratory of innova tion for bendingthe cost c urve, preserving the safety net,and improving the mana geme nt of carefor low-income populations."To help dete rmi ne what indexed growthfactor should be used for a Medicaidblock grant program, governors and stateMedicaid Directors across the cou ntryshould work with Congress to design afiscal growth factor that would m eet stateneeds. This type of reform would alsohelp Congress with its deficit reductionefforts since Medicaid costs would bemore predictable.Congress should reform Medicaid toavoid radical disruptions to sta te healthcare networks. Failure to d o so willresult in states merely becom ing passiveadmin istrators of the federal Medicaidprogram while state-only health careprogram s are eliminated to balancebudgets. Reforming Medicaid into anindexed block grant that provides statespe ndin g flexibility will instead facilitatefifty laboratories of democracy workingto identify innovative health care reformsto provide a meaningful safety net for themost vulnerable in o ur society.Congresswoman Cathy McMorrisRodgers represents Washington's FifthCongressional District and serves as ViceChair of the House Republican Conference.Jason Mercier is Director of th e Cente rforGovernment Reform at the WashingtonPolicy Center based in Seattle.
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
12/18
THEWAlL STREETJOURNAL.OPINION I JUNE 7, 2011ObamaCare s Next Constitutional ChallengeThe Medicaidprovision ofthe health law spells the death knell forcompetition among the states.
By RICHARD A. EPSTEIN AND MARIO LOY OLAThe constitutional battle over ObamaCare has largely focused on the constitutionality of the individual mandate.Namely, does forcing individuals to buy h ealth insurance violate the com merce clause? But as the E leventh CircuitCourt of Appeals prepares to hear Florida v. United States, a seco nd issue is of e qual importance: Was District CourtJudge Rog er Vmson correct to rule that the federal government can fo rce states to expand their Medicaid programs as
a precondition for continuing to receive matching federal h n d s for the program?Under the Pa tient Protection and Affordable Care Act, states have a choice: Expand their Med icaid rolls or bear thefull cost of caring for their state's current M edicaid population, while continuing to subsidize the Medicaid program s ofother states. The co nstitutional danger of such a s cheme has long been recognized. In 1936, the Supreme Court warnedin US. v. Butler that if conditional federal grants were not restrained, the taxing and spending power "could becomethe instrum ent for the total subversion of the gov ernmental pow ers reserved to the individual states."And yet the govern ment is comparing this Medicaid requirem ent to a "voluntary" contract. Does anyone believe thata person is entitled "voluntarily" to continue his joumey so long as he pays for all poor people who use the roads? Thegovernm ent's action is plainly coercive because it necessarily conditions the exercise of one right upon the consciou ssurrender of a second.
Unfortunately, the Supreme Court's decision in SoutlzDakota v. Dole (1987) confused matters. Dole let Con-gress condition 5% of federal highway h n d s on the statesraising their drinking age to 21 . The C ourt argued that thismodest penalty was mere pe rs ua sio wn ot coercion-butcautioned that "in some circum stances, the financial in-ducemen t offered by Congres s might be so coerc ive as topass the point at which 'pressure tum s into compulsioi~."'The question, then, is where that point is. Judge Vin-soil denied that any such point exists because the federal
- 3 courts have routinely ignored the Court's warning in Do le- A y pproving virtually every cond itional federal grant pro-gram-no matter how intrusive.Laugh~ng tock/Corb~s
The reason why the analysis in Dole ha s failed to offer any protection for state autonomy is that it is fundamentallywrong to think of coercion as a matter of degree. The government always engages in coercion when it taxes awayinoney from the citizens of several states, only to return it to those states that abide by certain conditions.The M edicaid provision of ObamaC are spells the death knell to competition among the states. States cannot functionas "laboratories of democracyy'-as the 10th Ame ndment intended-if the federal governm ent can use its power to taxand spend to bludgeo n all states into conform ity.
continued on back
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
13/18
In New York v. United States (1992), the Supreme Court ruled that the federal government cannot require stategovernm ents to take ow nership of nuclear waste that citizens could not otherwise dispose of safely. And in Printz v.Unitedstates (1997), the Court held that the U.S. could not co ~n pe local law enforcement officers to conduct back-ground checks on prospective handgun ow ners without their consent, because such comm andeering of state publicofficials is contrary to the federal structure of our C onstitution.In neither New York nor Printz did the result turn on the "level" of co er ci o~ ~,or should it do so in the currentcase. The constant backdrop of the federal taxing power makes a mockery of the claim that state participation underObamaCare is voluntary. The only way to prevent this grave intrusion on state autonomy is to strike down theMedicaid provisions o f the health-reform law.Mr. Epstein is a professor of lmv at New York Univers ity and a senior fellow at the Hoover Institution. Mr. Loyolais director of the Center or Tenth Amendment Studies at the Exas Public Policy Foundation, whichfile d an amicusbrief in F lorida v. United States.
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
14/18
O b a m a c a r e C a n ' t Be Fixed, and Now Is the Time to D ismantle I tby Michael F. CannonMichael F. C annon is director of health policy studies at .the Cato Institute and co author of HealthyCom petition: What's Holding Bac k Health Care and How to Free It.Added to cato. org on March 9 , 20 11This article app eared in the March 21, 201 1 issue o National Review.A t th e 20 11 Conservative Political Action C onference, Indiana governor Mitch Daniels observed thato turn the United States into a European-style social dem ocracy, the L eft "n eed only play gooddefense. The fe deral spending coinrnitments now in place will bring about the leviathan state they havalways sought. The healthcare travesty now on the books will engulf private markets and produce asingle-payer system or its equivalent, and it won't take long to happen." We even know th e drop-deaddate: Jan. 1 ,2 014. That's when Obam acare takes full effect, and it's less than th ree years away.On that date, the fed s will compel you to purchase health coverage, dictate the conten t of that healthinsu rance , slap governm ent price controls on it, and begin handing out hundreds of billions of dollarsnew entitlement spending. The relatively m inor provisions of the law that have ta ken effec t to date a ralready killing jobs, increasing preiniuins and taxes, reducing take-home pay, causing private- insuranmark ets to collapse, and throwing Americans out of their health plans. Yet today's cost increases andother dislocations will look like the good old days comp ared with what Am ericans will suffer when-if- hey allow Obam acare to take full effect. The noilpartisan C ongressional Budget Office projectsfor exa inple, that Obam acare will permanently eliminate 800,000 jobs by 2021. That's not to mentionany tem porary job losses.Ev en m ore om inous: Obainacare is already creating constituencies dedicated to its preservation. Formoiiths, the O bama administration has been w riting checks to states, seniors, and em ployers, andtrum peting the implicit subsidies that flow from the law's price controls, all with the goal of protectingObam acare by making more and more people dependent on it.Such efforts have so far failed to make t he law popular. Polls still show that a m ajority or plurality ofthe public opposes the law, as has been the case since the fxs t draft of Obam acare was introduced inCongress in June 2009. The latest Rasmussen poll fmds that 84 percent of Repub licans and 59 percenof independents favor repeal. Not eve n the $250 checks that the legislation is sending seniors havewon thein ov er: The latest Kaiser Family Foundation poll shows that their opposition is now highertha n at an y point since enactment (59 percent).That will change if Obam acare is still on the books in 2014. Tens of millions of Am ericans will begin receive thousands of dollars each in government subsidies, whe ther tlu-ough an expande d M edicaidprogram or Obainacare's new health insurance "exchanges." Medicare's chief actuaiy predicts thatthese state-based exchan ges will slowly crowd out other private coverage (such as through employeruntil "essentially all" Americans get their health insurance through them. Just a s important, whateverpriva te insurance coinpallies are still stand ing in 2014 will begin enrolling tens of millions of custom e
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
15/18
on the ground and deep pockets, these two con stitue i~cie swilleffort to eliminate their new subsidies. Public opinion may ev en turn in favor of the law-se O bainaca re works, but becau se tens of millions of people will be depen dent o n it for theirhat this means is that oppo nents may never have inore power to chart Obainacare's course than theyght now. In particular, the decisions that federal and state officials make today could determine
e 2 012 elections produce a Congress and president who are willing to repeal the law. Inrds, the iron is hot.ional Republicans ap pear to g a s p the w eight of this moment. They are doing everything theyensure that Obamacare never sees the year 2014: forcing votes on repealing and de-funding theo-year campaign to expose its harmful effects. Unfortunately, their effortsundercut b y their fiiends back hom e.
er than b eat their plow shares into swords, Obam acare opponen ts in inost state capitols are layingbureaucratic foundations for the law's new entitlement spending and lending it legitimacy byting its debt-fm anced federal grants. Secretary of Health and Human S eivices Kathleen Sebeliusstates have already accepted a t least $1 rr~illioil ach froin the federal governm ent to
s not just D emocrats who have taken the mon ey. Wisc:onsin governor Scott Walker h as won plauditsing down governm ent-worker unions and returning a $637,000 Ob amacare grant. Yet Walker8 million Obamacare grant to help get Wisconsin's exchang e up and running. KansasBrow nback vo ted against Obainacare when he w as in the U.S. Senate. Yet he hasd a $32 m illion Obainaca re grant and is allowing his Republican insurance coinmissioner,Praeg er, to forge ahead with creating a Kansas exchange.and K ansas are two of the 26 plaintiff states in Florida v.HHS,he case in which a federalObainacare is unconstitutional and void. In response to tha t ruling, Walker's attorneyJ. B. V an Hollen, declared the law "d ead" in Wisconsin, a reality no less true in the otherf states. Yet B rownback and W alker acce pted their $30 inillion- lus Obamacare grants afterSoine governors, including Idaho Republican B utch O tter, have said that the fact that theyting Obam acare grants and holding exchange-planning meetings does not mean they haveate an exchange. B ut taking the m oney lends legitimacy to a law that Otter himself isto ov erturn as unco nstitutional. To date, only two g overnors- lorida's Rick Scott and Alaska'sParnell, both Repub licans- ave refused to accept any Obam acare inoney or create any
amacare takes a beating in Con gress, the federal courts, and the co urt of public opinion, whyoppo nents acting as its agents? Soine state officials say they are hedging their bets. "Someslators think the state version of the exchange is their only option, even if they d on't wan t it,"Twila Brase, president of the M innesota based Citizens' Council for Health Freedom. "T heyral exchange is an absolute certainty and tha t they'll have m ore power over it if it's at exchange." But th at rationale rests on the false premise tha t Obam acare can be fured, or itss imp lemented the right way.
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
16/18
Obaina care con fronts states with a veiled Hobson's choice. The law provides that in 2014, eac h statewill have its own health-insurance exchange where individuals who don't hav e job-based coverage inpurch ase a federally regulated and subsidized (but ''private") health plan. States that develop andobtain federal approval of an ex change blueprint by 20 13 inay adininister their own exchanges in201 4. In states that c hoose not to create a n exchange, HHS will step in to create and administer one.The veil is the assurance that states will be able to tailor their exchanges. Sebelius audaciously clahntha t O bam acare "is built on the belief that states understand their health-insurance markets better thaanyo ne else. As such, it puts the states in the driver's seat to lead the process." Other supporters havesought to frighten Republican governors into im plementing the law by holding out the nightinarescen ario of the fed eral government's administering the exchanges. W ho adm inisters the exchanges,how ever, is unimportant. W hat cou nts is who writes the rules tha t govern them. Those rules will bewritten entirely in Washington.Unfortun ately, many Republican governors have taken the bait. "W e cannot let the insuranceexch ang e default to federal control," says a spokesman for Ohio governor John Kasich, "so we aremoving forw ard with the planning that is required to make the exchang e work best for Ohio." Aspokesm an for Georgia governor Nathan Deal put it more forcefully: "The state canno t halt midstreabec ause that would be irresponsible. It would put us too far behind if our litigation is not successful ithe end." But federal control is not just the exchanges' default setting- t's the only setting.LII a Feb ruary 2 4 letter to th e nation's governors, Sebelius extolled th e four types o f flexibility thatOba macare allows states in shaping their exchanges: 1) States can restrict insurers from participating2) s tates can add e ven inore benefit man dates than Ob amaca re requires; 3) come 201 7, states can opout of Obam acare by creating a single-payer health-care sy stem; and 4) states can adopt their own"governance structure" and "operational philosophy." In sum, state s can im pose harsher regulationstha n O bam acare requires and can choose who sits on their exchange's board. That's it. The onlyadditional latitude the Obam a adininistration has offered came w hen President Obaina told theNationa l G overnors Association that he is open to letting them launch single-payer systems in 2 014rather than 201 7. (Vermont governor Pete r Shumlin is champing at the bit.) S tates already had all thepow ers, of course, and would continue to possess them if Obainacare w ere repealed tomorrow. Whastates need, and Oba macare d enies them, is the power to rem ove the law's harmful regulations, whicwill block market competition and cost-saving innovations.Runn ing their own exchanges won't empow er states to prevent both the most econom ical and the m ocomprehensive health plans from disappearing froin their markets. Affordable plans will disappearbecause Obam acare requires all purchasers to buy w hatever coverag e Sebelius man dates as"essential," a definition that will grow eve r broader, as sucll defmitions alw ays do. The law's pricecontrols will require insurers to charge everyone of a given age the same premium, regardless ofwheth er an actuarially fair premium might be $5,000 or $50,000. Ev en state-run e xchanges would secomprehensive health plans crumble under the weight of too many patients w ho cost $50,000 but pafar less. Nor can state-run exchange s prevent other dimensions of quality from eroding. Even in staterun exchanges, the sickest patients w ould struggle to get their c lahns paid by insurers who are tryingavoid, mistreat, and dum p them, because th at is what O bam acare's price controls reward.State s that run their own exchang es will likewise be powerless to prev ent HHS froin loading health-savings-account (HSA ) plans dow n with inandated benefits. They will have no power to save HSAs
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
17/18
o destroy health savings accounts.publican governors recently told Sebelius that she should prepare to administer theirunless HHS 1) provides them "coinplete flexibility" in running their exchanges; 2)
3) waives the provisions that threaten HSAs; and 4) gives"blanket discretion" to move non-disabled Medicaid eilrollees into the exchanges. There is zeroSebelius will accede, because she cannot. G:ranting he first three demands would meanst of Obainacare's central requirements: the price controls on health insurance, themandate, and the medical-loss-ratio requirements, for starters. That would require an act of
act of Congress would not fix Obamacare. The new entitlement spending, in Medicaidmandate on states. My colleague Jagadeesh Gokhale estimates that new York Statehardest, being forced to shell out an ad.ditional$66 billion over the first ten years.e "blanket discretion" these governors seek to inove Medicaid enrollees into the exchanges,
fairly shameless ploy to shift the cost of their Medicaid prograins to taxpayers inthe exchange subdies .
ius's official response to the governors was, effectively, "drop dead." Having received this21 governors should stick to their guns and join Scott and Parnell by refusing anynot create any Obamacare exchanges. Brase argues that such a move might doom the exchangesy cannot create that inany without the help of state officials. "The future is uncertainfederal exchange," she explains. "Why should we do the feds' work when they might never
exchange without our help?"the fantasy that they call create a better excl~ange, ne that does not comply withn audacious stratagem. But ask yourself: What insurance company will participate ine that flouts federal law? Before you answer, reinember that the federal gove iment iscompanies' largest customer.
every new bureaucracy is itself a constituency for more government.that states not create exchanges at all. "Anytime you can keep a government fromp any bureaucracy of any sort," writes Charlie .Arlinghausof New Hampshire's free-marketenter for Public Policy, "it is a victory."
even a less-bad way, for states or the feds to implement Obamacare'sther central elements. Permitted to stand, Obainacare will reduce Americans' incomes,and decrease their freedom. The only way to fix it is to demolish it. "Collaboration inp exchanges only encourages the corporate interests who will profit from them and sends athat 'repeal and replace' is not serious," writes the Pacific Research Institute's John R. Graham.h e , money, or energy creating constituencies for Obamacare, Graham mites,
-
8/4/2019 ALEC 8-4-11 Health Insurance Exchanges States in Charge
18/18
"w e have to discourage implementation, totally and immediately."In The Brid ge on the R iver Kw ai, the British PO W Coloilel Nicholson recognizes that his collaboratiwith his Japan ese cap tors was madness, and gives his life to undo it. State lawmake rs need to have asimilar epiphany about Obam acare, before things reach the point w here correcting their inistakes wilcost th em their p olitical lives. Unlike soldiers, politicians aren't into self-sacrifice.