ALCAPA Eva Nunlist, D.O. Pediatric Cardiology Fellow, PGY-5 Miami Childrens Hospital 10/17/12

Alcapa.final
Oct 28, 2014
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ALCAPA
Eva Nunlist, D.O.Pediatric Cardiology Fellow, PGY-5
Miami Childrens Hospital10/17/12

Differential DiagnosesO In infants
O dilated cardiomyopathy and myocarditisO In children and adolescents
O MR due to myocarditis or cardiomyopathyO With continuous murmur
O PDA, coronary arteriovenous fistula, rupture of sinus of Valsalva aneurysm into right side chamber, arteriovenous fistula of internal mammary or intercostal vessels
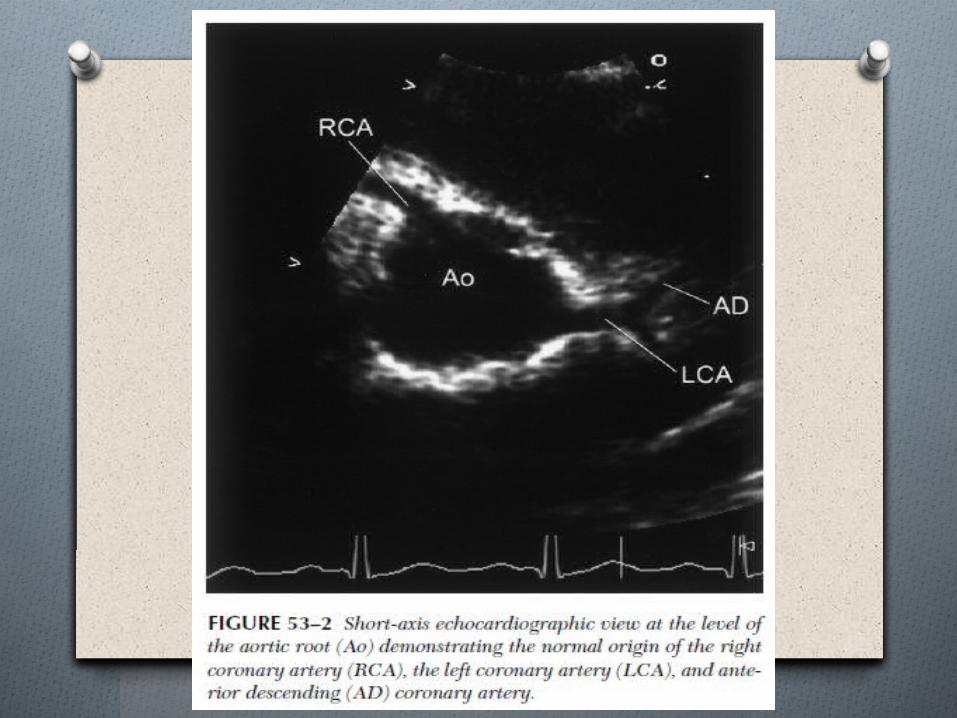
ECHOCARDIOGRAPHIC DIAGNOSIS OF
ALCAPA
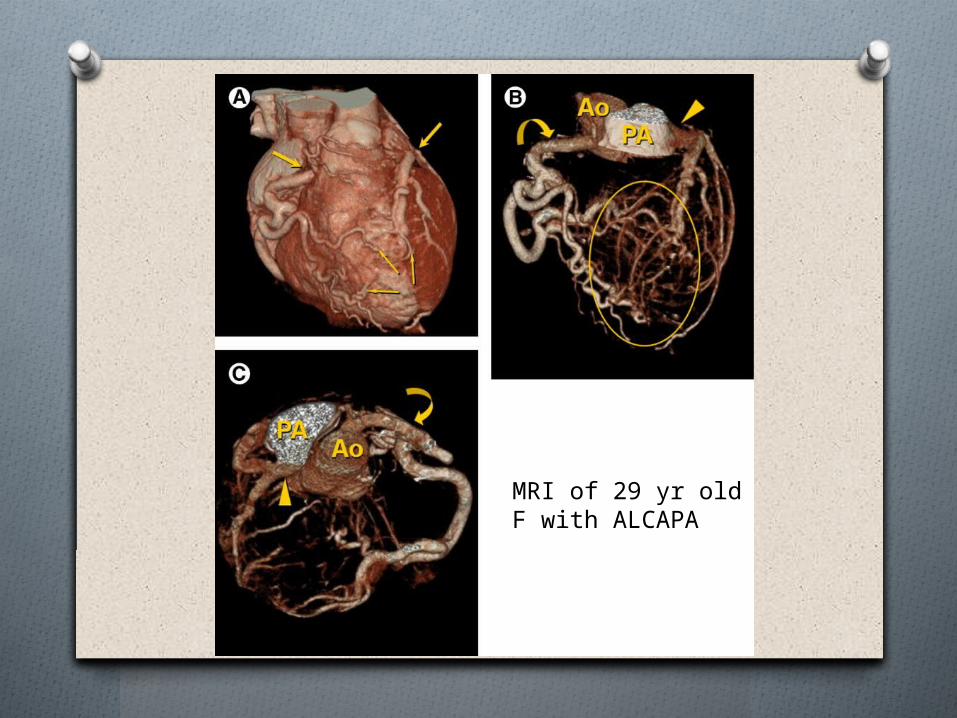
MRI of 29 yr old F with ALCAPA
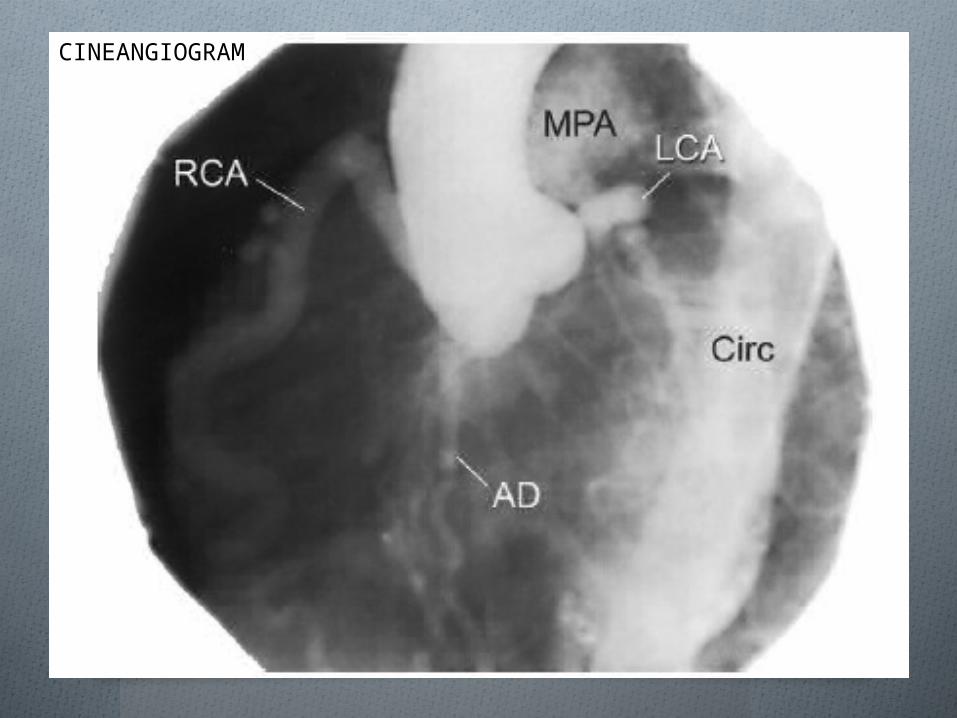
CINEANGIOGRAM
Preoperative Critical Care Mgmt
O Goal: stabilize patient while awaiting surgery
O Focus: optimize myocardial oxygen supply and minimize myocardial oxygen demand
Preoperative Critical Care Mgmt
O Infant with CHF and stable BP:O Diuretics – avoid hypovolemia
O To reduce pulmonary edema to lessen respiratory distress and improve oxygenation.
O To decrease myocardial wall tension to improve myocardial oxygen supply to demand ratio.
O Supplemental oxygenO To prevent hypoxia.
O Sedation and analgesiaO To reduce anginal pain, prevent tachycardia
Preoperative Critical Care Mgmt
O Antiarrhythmic drugs and a defibrillator should be readily available.
O Infants with severe CHF and unstable BP:O Intubation and controlled ventilation
O Avoid excessive mean airway pressure to avoid reduction in venous return to the heart.
O Vasoactive drugsO Dobutamine and milrinone may provide inotropic
support without significant tachycardia. O But milrinone may reduce afterload/blood pressure
and impair coronary perfusion.O Phenylephrine to raise diastolic pressure without
producing excessive afterload to heart.
Surgical Management
O 1953 – (Potts) aortopulmonary anastomosis to increase oxygen saturation in the main pulmonary artery
O 1953 – (Mustard) left carotid artery–to–anomalous left coronary artery procedure
O 1959 – (Sabiston) simple ligation of the proximal origin of the anomalous left coronary artery
O 1966 – (Cooley et al) saphenous vein grafting from the aorta to the anomalous left coronary artery
O 1968 – (Meyer et al) left subclavian artery–to–anomalous left coronary artery repair
O Internal mammary artery–to–anomalous left coronary artery from the pulmonary artery
O Pulmonary artery banding has been attempted to increase perfusion pressure in the anomalous left coronary artery from the pulmonary artery.
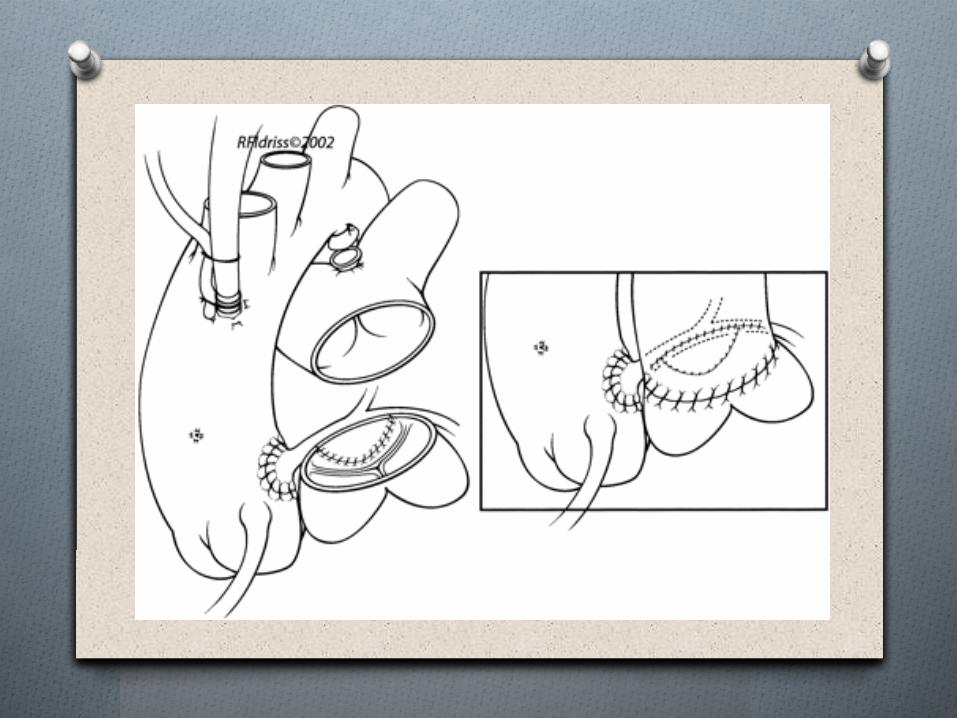
O Direct anastomosis of the anomalous left coronary artery from the pulmonary artery directly to the aorta was described in the 1970s and currently remains the procedure of choice.
O For patients in whom direct transfer of the coronary artery is not feasible, performing the novel repair of creating an intrapulmonary aortocoronary tunnel may be appropriate, as described by Takeuchi in 1979.
O Occasionally, cardiac transplantation has been required in patients with anomalous left coronary artery from the pulmonary artery with severe cardiac dysfunction.
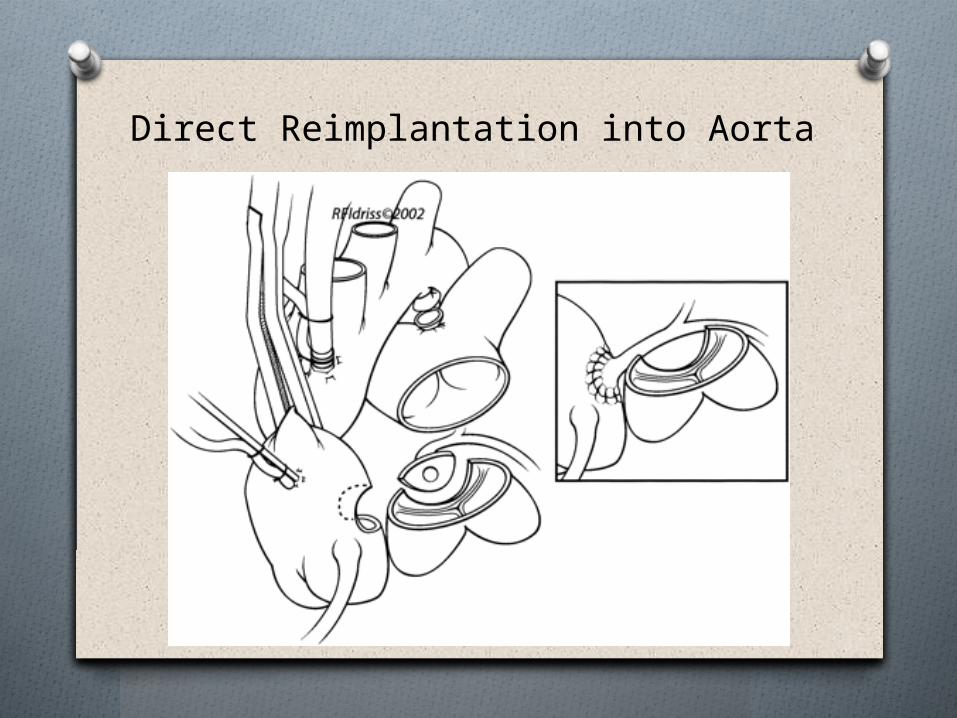
Direct Reimplantation into Aorta
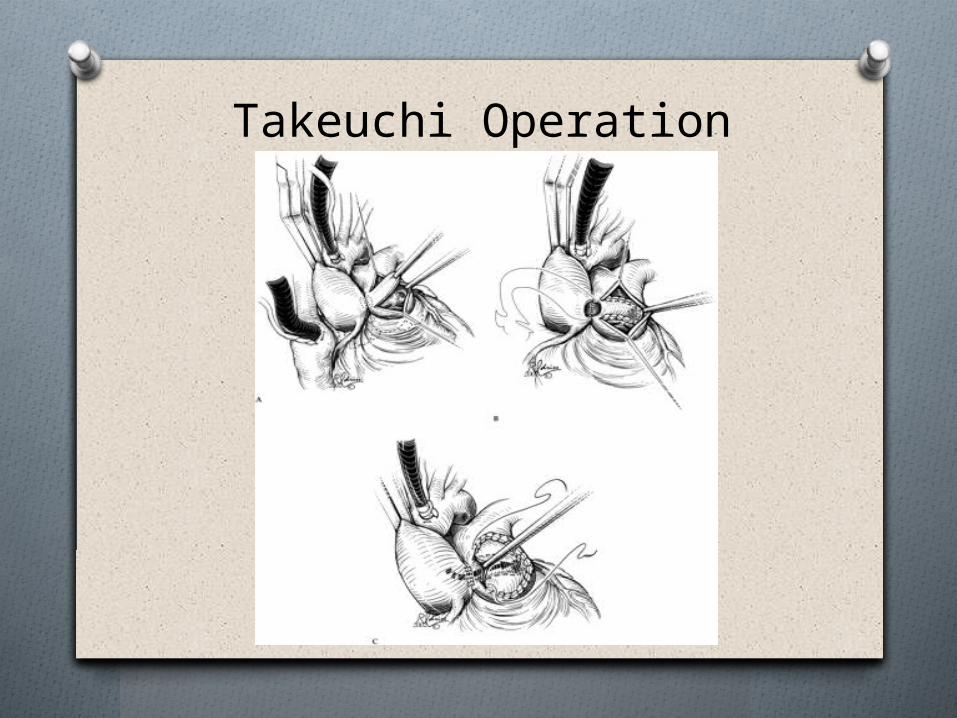
Takeuchi Operation
Post-operative Critical Care Mgmt
O Inotropic drugs to maintain adequate hemodynamics. Monitor LV fxn with serial ECGs and echos.
O If needed, mechanical support devices including CPS/ECMO or LV assist device via a centrifugal pump in infants.
O Intraaortic balloon counterpulsation may be attempted in older children and adults.
O Cardiac transplant if no improvement in ventricular fxn.
Excellent functional result in children after correction of anomalousorigin of left coronary artery from the pulmonary artery – a population-based complete follow-up studyTiina Ojalaa,*, Jukka Salminenb, Juha-Matti Happonena, Jaana Pihkalaa, Eero Jokinena, Heikki Sairanenb
ReferencesO Hillman N, Dodge-Khatami A, Mavroudis C. Anomalous
origin of the left coronary artery from the pulmonary artery: successful surgical strategy without assist devices. Semin Thorac Cardiac Surg Pediatr Cardiac Surg Annu 2000;3:165–72 [36].
O Cochrane, AD, et al. Excellent long-term functional outcome after an operation for anomalous left coronary artery from the pulmonary artery. J Thorac Cardiovasc Surg. 1999 Feb;117(2):332-42.
O Keane, JF, et al. Nadas’ Pediatric Cardiology. 2nd Ed. Philadelphia. 2006.
O Nichols, DG, et al. Critical Heart Disease in Infants and Children. 2nd Ed. Philadelphia. 2006.
O Satpathy, M. Clinical Diagnosis of Congenital Heart Disease. New Delhi. 2008.
THANK YOU!!!