FACULTY OF MEDICINE AND HEALTH SCIENCES Academic Year 2011 - 2012 AKI-6 Epidemiology of Acute Kidney Injury Anne NOBELS Promotor: Prof. Dr. E. Hoste Co-promotor: Prof. Dr. J. Kellum (Pittsburg) Dissertation presented in the 2 nd Master year in the program of Master in Medicine

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
FACULTY OF MEDICINE AND
HEALTH SCIENCES
Academic Year 2011 - 2012
AKI-6 Epidemiology of Acute Kidney Injury
Anne NOBELS
Promotor: Prof. Dr. E. Hoste
Co-promotor: Prof. Dr. J. Kellum (Pittsburg)
Dissertation presented in the 2nd
Master year
in the program of
Master in Medicine

FACULTY OF MEDICINE AND HEALTH SCIENCES
Academic Year 2011 - 2012
AKI-6 Epidemiology of Acute Kidney Injury
Anne NOBELS
Promotor: Prof. Dr. E. Hoste
Co-promotor: Prof. Dr. J. Kellum (Pittsburg)
Dissertation presented in the 2nd
Master year
in the program of
Master in Medicine

“The author and the promotor give the permission to use this thesis for consultation and to
copy parts of it for personal use. Every other use is subject to the copyright laws, more
specifically the source must be extensively specified when using results from this thesis.”
Date
Anne Nobels (student) Prof. Dr. E. Hoste (promotor)
Foreword
This master thesis is the result of two years hard work. I want to thank sincerely all those people who
helped me during this period.
First of all I want to thank my promotor, Prof. Dr. Eric Hoste, for his endless patience, for his critical
view, for his feedback, for all the time he spend on my master thesis, and for the opportunity to work
further on a scientific paper after this master thesis.
I want to thank Prof. Dr. John Kellum and Dr. Nattachai Sisrawat to help me understand the AKI-6
database and the different AKI classifications.
Chris Danneels and Bram Gadeyne, I want to thank for their ICT help and their patience with an
ICTstarter like me. Special thanks to Chris Danneels for writing a program to calculate the duration of
the AKI episodes.
Jonathan De Rudder, I want to thank for his mathematical insight and his recalculation of the CKD-
EPI equitation.
My parents, family and friends I want to thank for their support during this master thesis and my
studies in general.
Table of Contents
1. Abstract ........................................................................................................................................... 1
1.1. Introduction ............................................................................................................................. 1
1.2. Materials and Methods ............................................................................................................ 1
1.3. Results ..................................................................................................................................... 1
1.4. Conclusion ............................................................................................................................... 2
2. Introduction ..................................................................................................................................... 3
3. Materials and methods ..................................................................................................................... 4
3.1. Literature ................................................................................................................................. 4
3.2. Study Design ........................................................................................................................... 4
3.3. Acute Kidney Injury (AKI) ..................................................................................................... 5
3.3.1. RIFLE classification for AKI .......................................................................................... 5
3.3.2. Acute Kidney Injury Network (AKIN) diagnostic and classification system for AKI ... 6
3.3.3. The Kidney Disease Improving Global Outcomes (KDIGO) definition and staging
system for AKI ................................................................................................................................ 6
3.3.4. Baseline serum creatinine concentration ......................................................................... 7
3.3.5. Classification of patients into AKI categories ................................................................. 8
3.4. Transient Acute Kidney Injury ................................................................................................ 8
3.5. Statistical analysis ................................................................................................................... 8
3.6. Presentation of the results ........................................................................................................ 9
4. Results ........................................................................................................................................... 10
4.1. Basic Characteristics of the study population ....................................................................... 10
4.2. Acute Kidney Injury .............................................................................................................. 12
4.3. Outcomes ............................................................................................................................... 14
4.3.1. ICU Mortality ................................................................................................................ 14
4.3.2. Hospital Mortality ......................................................................................................... 16
4.3.3. ICU Length of stay ........................................................................................................ 17
4.3.4. Hospital Length of Stay ................................................................................................. 19
4.4. Transient AKI ........................................................................................................................ 22
4.4.1. Transient AKI defined as ≤3 days of AKI (AKIt3) ....................................................... 22
4.4.2. Transient AKI defined as ≤ 2 days of AKI (AKIt2) ...................................................... 24
4.4.3. Transient AKI defined as ≤1 day of AKI (AKIt1) ........................................................ 26
4.4.4. Comparison of mortality between AKIt1, AKIt2 and AKIt3 ........................................ 28
5. Discussion ..................................................................................................................................... 31
5.1. Prevalence of AKI ................................................................................................................. 31
5.2. Outcomes ............................................................................................................................... 32
5.3. Classifications of AKI ........................................................................................................... 33
5.3.1. AKI and transient AKI prevalence ................................................................................ 34
5.3.2. AKI and transient AKI outcomes .................................................................................. 34
5.4. Strengths and limitations ....................................................................................................... 35
6. Conclusion ..................................................................................................................................... 36
7. Nederlandse samenvatting ............................................................................................................. 37
7.1. Inleiding................................................................................................................................. 37
7.2. Methodologie ......................................................................................................................... 37
7.3. Resultaten .............................................................................................................................. 39
7.4. Besluit .................................................................................................................................... 41
8. References ..................................................................................................................................... 42
1 AKI-6 Epidemiology of Transient Acute Kidney Injury
1. Abstract
1.1. Introduction
Acute Kidney Injury (AKI) is associated with increased mortality, even after correction for covariates
(1). In 2004 the Acute Dialysis Quality Initiative (ADQI) group developed a consensus definition for
AKI, the RIFLE classification (2). Up to two-thirds of all ICU patients will develop AKI defined by
the RIFLE classification (1). In the meantime two modifications of the RIFLE classification were
developed, the AKIN classification (3), and recently the KDIGO classification (4).
Recently, transient AKI or transient azotemia (TA) was defined as AKI lasting for < 72 h (5). Patients
with TA had a significantly higher odds ratio for hospital mortality, and long-term mortality (5).
1.2. Materials and Methods
The AKI-6 TRansient AKI Study (TRAK Study) is a retrospective multicenter international cohort
study. Data were collected by the Acute Kidney Injury 6 study group (AKI-6). AKI-6 is a multicenter,
transatlantic study group of intensivists of 6 centers, 2 centers in the USA, 2 European centers and 2
Australian centers. A total of 11,309 patients admitted on the Intensive Care Unit in the period 2005-
2007 were analyzed. When baseline creatinine was not available, this was calculated by the 4-variable
MDRD (6) or CKD-EPI equation (7). Therefore, AKI patients were classified according to 5 AKI
classifications: RIFLE MDRD, RIFLE CKD-EPI, AKIN, KDIGO MDRD and KDIGO CKD-EPI. We
analyzed 4 clinical outcomes: ICU mortality, hospital mortality, ICU length of stay, and hospital
length of stay. AKI patients and patients without AKI were compared, as well as patients with
transient AKI and patients with a longer AKI episode. We defined transient AKI in three different
ways:
1. Transient AKI with duration of ≤ 3 days of AKI (AKIt3)
2. Transient AKI with duration of ≤ 2 days of AKI (AKIt2)
3. Transient AKI with duration of ≤ 1 days of AKI (AKIt1)
1.3. Results
Acute Kidney Injury occurred in 17.8% to 31.0% of the ICU patients according to the AKI
classification used and was associated with worse clinical outcomes. Patients with AKI had a higher
2 AKI-6 Epidemiology of Transient Acute Kidney Injury
ICU mortality (17.6%-24.0%) compared to the patients without AKI (4.5%-5.5%). There was also
higher hospital mortality in AKI patients (25.5%-32.9%) compared to patients without AKI (7.9%-
9.4%). Patients with AKI had a longer ICU and hospital length of stay compared to patients without
AKI.
Transient AKI occurred frequently. The period prevalence of AKIt3 varied according to the
classification used between 13.9% and 22.7% of ICU patients, the period prevalence of AKIt2 varied
between 8.0% and 19.7%, and the period prevalence of AKIt1 varied between 6.4% and 13.1%. AKIt3
occurred in 65.7% to 78% of AKI patients, AKIt2 in 34.0% to 67.1% and AKIt1 in 28.2% to 42.1%.
Transient AKI (AKIt1, AKIt2 and AKIt3) was associated with a higher ICU and hospital mortality
compared to patients without AKI. There was no difference in mortality between the different transient
AKI definitions, and also not with all AKI.
The duration of an AKI episode was associated with a longer ICU and hospital length of stay. We
couldn’t find an association with ICU mortality. Hospital mortality of patients with AKIt2 and 3 was
lower compared to patients with longer duration of AKI. Patients with AKIt1 had a similar hospital
mortality compared to patients with a longer AKI episode (>1 day).
Comparing the five classification used in this analysis: RIFLE MDRD, RIFLE CKD-EPI, AKIN,
KDIGO MDRD and KDIGO CKD-EPI, differences can be seen in AKI prevalence, duration of the
first AKI episode, clinical outcomes, transient AKI prevalence and transient AKI outcomes.
1.4. Conclusion
In this large multicenter international cohort of ICU patients, AKI was common and related to an
increase of ICU and hospital mortality, and a longer ICU and hospital length of stay. Transient AKI
occurred in up to 2 third of all AKI cases. ICU and hospital mortality was higher in transient AKI
patients compared to patients without AKI, but similar between Transient AKI variants and all AKI.
Compared to AKI with longer duration, most Transient AKI had similar ICU mortality, but lower
hospital mortality. A longer AKI episode was associated with a longer length of stay.
Although the AKI definitions are very similar, there was important variation in prevalence of AKI and
transient AKI, and outcomes among the different AKI definitions.
Duration of AKI should be incorporated in new AKI consensus definitions and used in clinical studies.

3 AKI-6 Epidemiology of Transient Acute Kidney Injury
2. Introduction
Acute Kidney Injury (AKI) is a common condition in critical ill patients with a significant higher risk
of death. For years there was no consensus definition for AKI, but in the last decade three consensus
definitions were developed using a combination of creatinine and urine output criteria. In 2004 the
Acute Dialysis Quality Initiative (ADQI) group developed the RIFLE classification (2). Up to two-
thirds of all intensive care unit patients will develop AKI defined by the RIFLE classification (1). In
2007 The Acute Kidney Injury Network (AKIN) developed an adaptation of the RIFLE classification
(3). The last definition was developed only a few months ago by the KDIGO group (4). The RIFLE
and KDIGO classification work with a baseline creatinine value. If there is no baseline value available,
the baseline is calculated out of the glomerular filtration rate (GFR) value by the 4-variable
Modification of Diet in Renal Disease (MDRD) equitation (6). In 2009 Levey et al. (7) proposed a
new and more accurate equitation to calculate the GFR, the Chronic Kidney Disease Epidemiology
Collaboration (CKD-EPI) equitation.
Most AKI epidemiology studies examined the relation between morbidity and mortality based on the
maximum RIFLE class. Uchino et al. (5) demonstrated that patients with transient AKI (<72h) had a
significantly higher odds ratio for hospital mortality. Coca et al.(8) demonstrated that the duration of
an postoperative AKI episode is associated with an increased risk of long-term mortality in diabetic
US veterans.
The aim of the TRAK study (AKI-6 Transient AKI Study) was to determine the influence of AKI
duration on outcomes (mortality, length of stay) in an Intensive Care Unit (ICU) population. We
compared different AKI classifications and different ways of calculating baseline creatinine value.

4 AKI-6 Epidemiology of Transient Acute Kidney Injury
3. Materials and methods
3.1. Literature
Before starting the analyses there was performed a literature study. Articles were found using Pubmed
and following keywords: Acute kidney injury, RIFLE, AKIN, KDIGO, MDRD, CKD-EPI….
References of found articles were also used. These articles were used in the in the introduction and
discussion section of this thesis. An overview of the articles can be found under references. The
references were compiled using “Endnote X5”.
3.2. Study Design
The TRAK study is a retrospective multicenter international cohort study. Data were collected by the
Acute Kidney Injury 6 study group (AKI-6). AKI-6 is a multicenter, transatlantic study group of
intensivists of 6 centers, Dr. J.A. Kellum, University of Pittsburgh Medical Center, (Pittsburgh, PA,
USA), Dr. G. Ognjen, the Mayo Clinic (Rochester, Minnesota, USA), Dr. S Webb, Royal Perth
Hospital (Perth, Australia), Dr. R. Bellomo, Austin Health Center (Melbourne, Australia), Dr. E. Hoste,
Ghent University Hospital (Ghent, Belgium), Dr. C. Ronco and Dr. D. Cruz, Ospedale San Bortolo di
Vicenza (Vicenza, Italy). In the rest of this master thesis the participating centers will be referred as
the cities were they are situated.
In Pittsburg, Rochester, Perth and Ghent every patient admitted on the Intensive Care Unit (ICU) was
registered from 2005 till 2007. In Melbourne and Vicenza patients were registered during a shorter
time period within the same study period. This is the main reason for the unequal patient distribution
in the database.
During the whole ICU stay the following data were recorded: worst serum creatinine concentration,
urine output, treatment with mechanical ventilation, and treatment with renal replacement therapy.
ICU mortality, hospital mortality, ICU length of stay and hospital length of stay, were registered as
outcomes.
5 AKI-6 Epidemiology of Transient Acute Kidney Injury
To compare serum creatinine values in the different centers, the values had to be recalibrated to
Isotope Dilution Mass Spectrometry reference measurement procedure (IDMS standards). Ghent,
Mayo, Perth and Vicenza were already using the IDMS standards in their lab, so recalibration was not
necessary. For Pittsburg and Melbourne we used the same recalibration formulas as Zavada et al. (9).
Pittsburg:
Austin:
(SCr: Serum creatinine concentration)
3.3. Acute Kidney Injury (AKI)
Acute kidney Injury (AKI) was defined according to the different consensus staging systems for AKI
that have recently been published: the RIFLE criteria (2), AKIN criteria (3) and KDIGO criteria (4).
AKIN and KDIGO are modifications of the RIFLE criteria, therefore the differences between the 3
staging systems are limited on first sight. In all three staging systems, AKI can be staged based on an
increase of serum creatinine concentration or a period of oliguria. As urine output criteria were not
available in the majority of patients, we used only the creatinine criteria for staging and classification
of AKI.
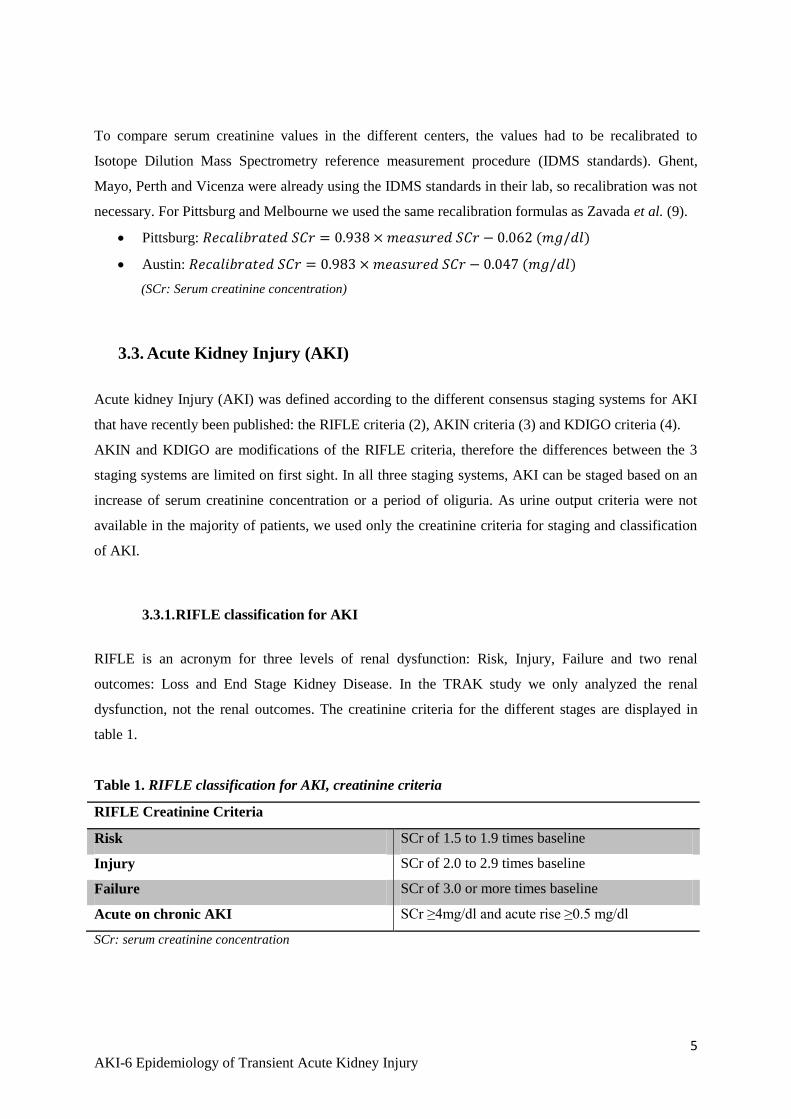
3.3.1. RIFLE classification for AKI
RIFLE is an acronym for three levels of renal dysfunction: Risk, Injury, Failure and two renal
outcomes: Loss and End Stage Kidney Disease. In the TRAK study we only analyzed the renal
dysfunction, not the renal outcomes. The creatinine criteria for the different stages are displayed in
table 1.
Table 1. RIFLE classification for AKI, creatinine criteria
RIFLE Creatinine Criteria
Risk SCr of 1.5 to 1.9 times baseline
Injury SCr of 2.0 to 2.9 times baseline
Failure SCr of 3.0 or more times baseline
Acute on chronic AKI SCr ≥4mg/dl and acute rise ≥0.5 mg/dl
SCr: serum creatinine concentration
6 AKI-6 Epidemiology of Transient Acute Kidney Injury
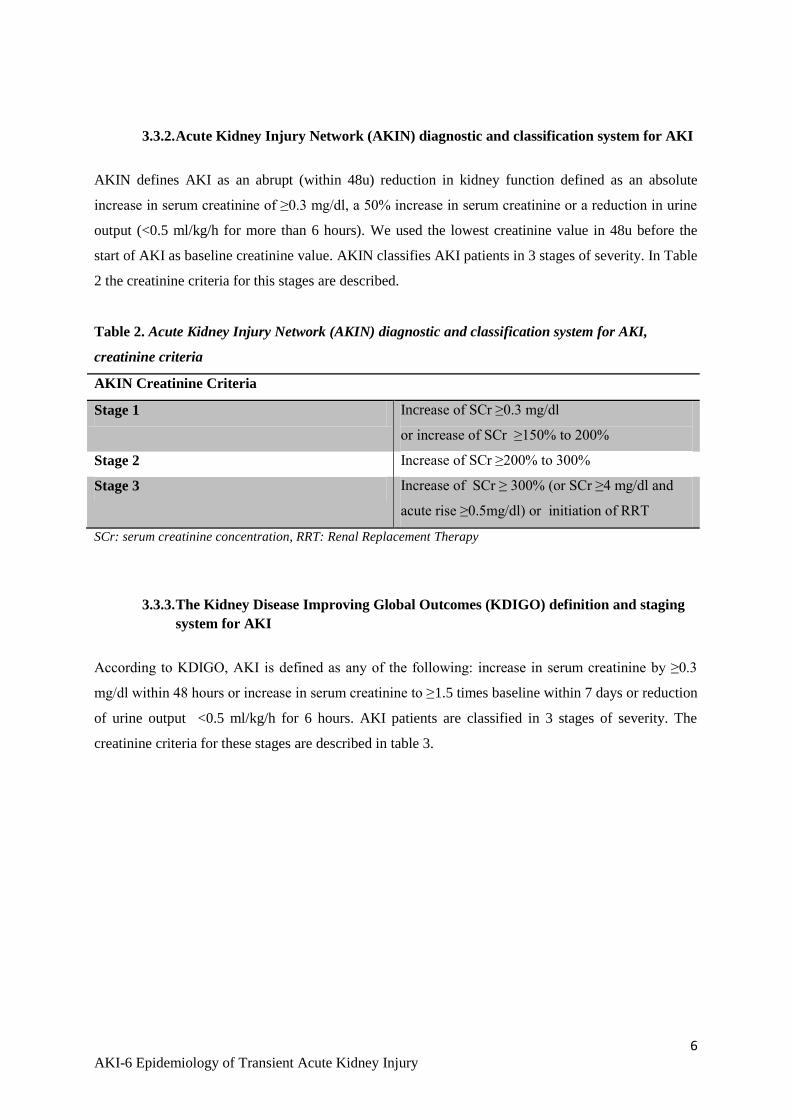
3.3.2. Acute Kidney Injury Network (AKIN) diagnostic and classification system for AKI
AKIN defines AKI as an abrupt (within 48u) reduction in kidney function defined as an absolute
increase in serum creatinine of ≥0.3 mg/dl, a 50% increase in serum creatinine or a reduction in urine
output (<0.5 ml/kg/h for more than 6 hours). We used the lowest creatinine value in 48u before the
start of AKI as baseline creatinine value. AKIN classifies AKI patients in 3 stages of severity. In Table
2 the creatinine criteria for this stages are described.
Table 2. Acute Kidney Injury Network (AKIN) diagnostic and classification system for AKI,
creatinine criteria
AKIN Creatinine Criteria
Stage 1 Increase of SCr ≥0.3 mg/dl
or increase of SCr ≥150% to 200%
Stage 2 Increase of SCr ≥200% to 300%
Stage 3 Increase of SCr ≥ 300% (or SCr ≥4 mg/dl and
acute rise ≥0.5mg/dl) or initiation of RRT
SCr: serum creatinine concentration, RRT: Renal Replacement Therapy
3.3.3. The Kidney Disease Improving Global Outcomes (KDIGO) definition and staging
system for AKI
According to KDIGO, AKI is defined as any of the following: increase in serum creatinine by ≥0.3
mg/dl within 48 hours or increase in serum creatinine to ≥1.5 times baseline within 7 days or reduction
of urine output <0.5 ml/kg/h for 6 hours. AKI patients are classified in 3 stages of severity. The
creatinine criteria for these stages are described in table 3.
7 AKI-6 Epidemiology of Transient Acute Kidney Injury
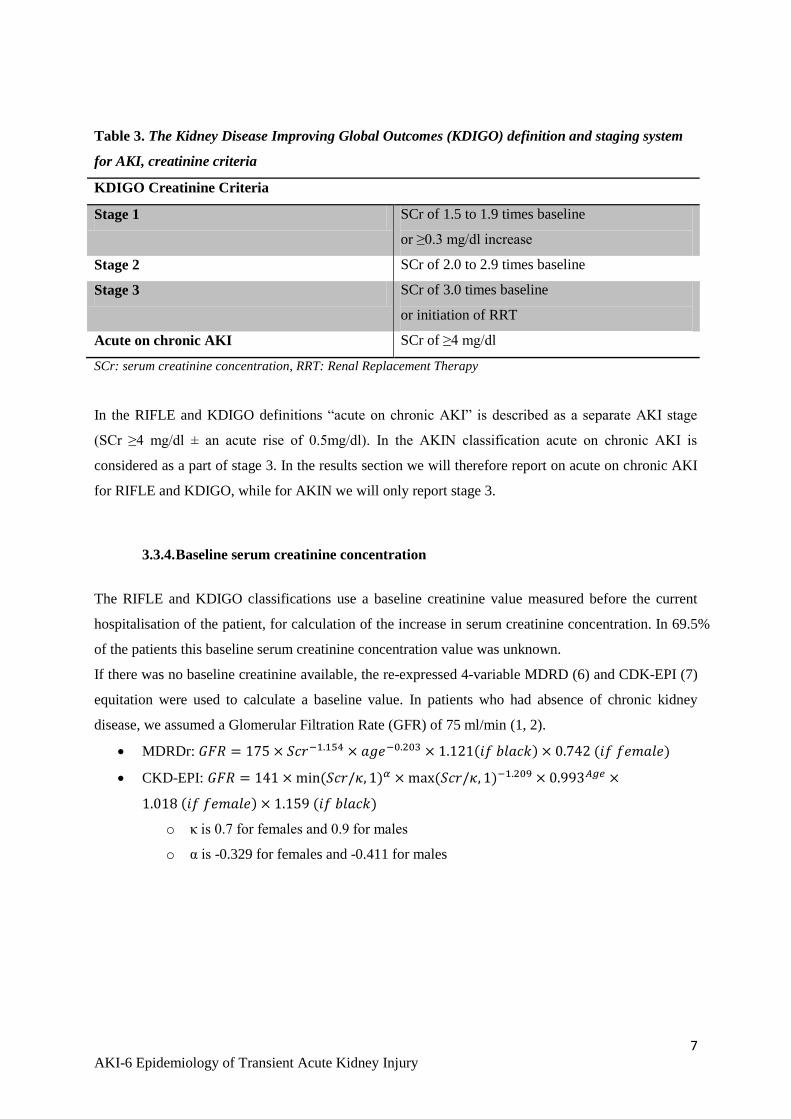
Table 3. The Kidney Disease Improving Global Outcomes (KDIGO) definition and staging system
for AKI, creatinine criteria
KDIGO Creatinine Criteria
Stage 1 SCr of 1.5 to 1.9 times baseline
or ≥0.3 mg/dl increase
Stage 2 SCr of 2.0 to 2.9 times baseline
Stage 3 SCr of 3.0 times baseline
or initiation of RRT
Acute on chronic AKI SCr of ≥4 mg/dl
SCr: serum creatinine concentration, RRT: Renal Replacement Therapy
In the RIFLE and KDIGO definitions “acute on chronic AKI” is described as a separate AKI stage
(SCr ≥4 mg/dl ± an acute rise of 0.5mg/dl). In the AKIN classification acute on chronic AKI is
considered as a part of stage 3. In the results section we will therefore report on acute on chronic AKI
for RIFLE and KDIGO, while for AKIN we will only report stage 3.
3.3.4. Baseline serum creatinine concentration
The RIFLE and KDIGO classifications use a baseline creatinine value measured before the current
hospitalisation of the patient, for calculation of the increase in serum creatinine concentration. In 69.5%
of the patients this baseline serum creatinine concentration value was unknown.
If there was no baseline creatinine available, the re-expressed 4-variable MDRD (6) and CDK-EPI (7)
equitation were used to calculate a baseline value. In patients who had absence of chronic kidney
disease, we assumed a Glomerular Filtration Rate (GFR) of 75 ml/min (1, 2).
MDRDr:
CKD-EPI:
o κ is 0.7 for females and 0.9 for males
o α is -0.329 for females and -0.411 for males
8 AKI-6 Epidemiology of Transient Acute Kidney Injury
3.3.5. Classification of patients into AKI categories
As we used for this analysis 3 different classifications for AKI, and 2 estimates for missing baseline
serum creatinine concentrations, we classified patients according to 5 different classifications.
1) RIFLE MDRD: AKI was classified using the RIFLE classification. If there was no baseline
creatinine available the re-expressed 4-variable MDRD was used to calculate a baseline value.
2) RIFLE CKD-EPI: AKI was classified using the RIFLE classification. If there was no baseline
creatinine available the CKD-EPI equitation was used to calculate a baseline value.
3) AKIN: AKI was classified using the AKIN classification. We used the lowest creatinine value
in 48u before the start of AKI as baseline creatinine value.
4) KDIGO MDRD: AKI was classified using the KDIGO classification. If there was no baseline
creatinine available the re-expressed 4-variable MDRD was used to calculate a baseline value.
5) KDIGO CKD-EPI: AKI was classified using the KDIGO classification. If there was no
baseline creatinie available the CKD-EPI equitation was used to calculate a baseline value.
Only the first AKI episode was included in our analysis.
3.4. Transient Acute Kidney Injury
Transient Acute Kidney Injury was defined in three different ways:
1. Transient AKI with duration of ≤ 3 days of AKI (AKIt3)
2. Transient AKI with duration of ≤ 2 days of AKI (AKIt2)
3. Transient AKI with duration of ≤ 1 days of AKI (AKIt1)
3.5. Statistical analysis
To describe the characteristics of the study population MS Access 2010 was used. The number of AKI
episodes per patient and duration of these episodes were calculated using MS Access 2010. Specific
cases were selected and exported to SPSS for further statistical analysis
9 AKI-6 Epidemiology of Transient Acute Kidney Injury
SPSS Statistics version 19 was used to perform the statistical analysis. Categorical variables are
displayed as number (percentage). To analyze categorical variables we used the Chi-square test.
Continuous variables are displayed as median and 25th and 75
th percentiles. We tested continuous
variables for normality by distribution plots, and compared means using Student’s T-test when
normally distributed, and Kruskall-Wallis test and Mann-Whitney-U test when not. A double sided p-
value <0.05 was considered significant.
3.6. Presentation of the results
Tables were made by MS Word 2010. The bar charts were made by MS Excel 2010.
10 AKI-6 Epidemiology of Transient Acute Kidney Injury
4. Results
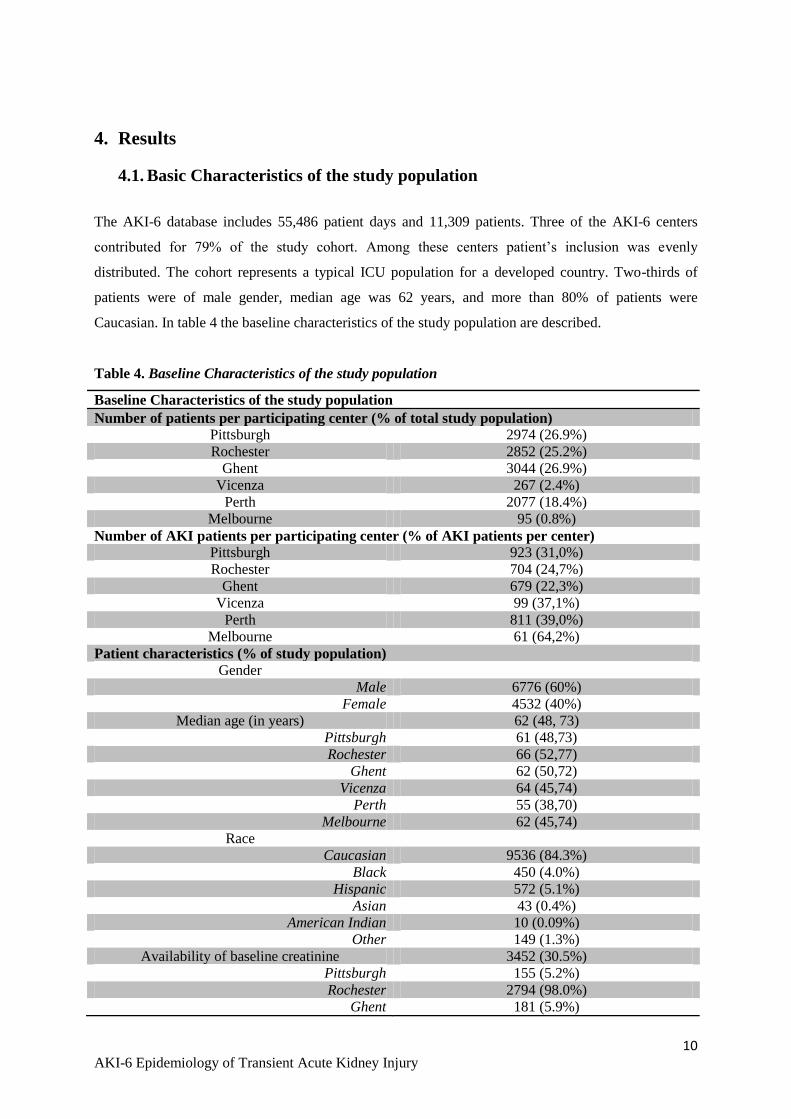
4.1. Basic Characteristics of the study population
The AKI-6 database includes 55,486 patient days and 11,309 patients. Three of the AKI-6 centers
contributed for 79% of the study cohort. Among these centers patient’s inclusion was evenly
distributed. The cohort represents a typical ICU population for a developed country. Two-thirds of
patients were of male gender, median age was 62 years, and more than 80% of patients were
Caucasian. In table 4 the baseline characteristics of the study population are described.
Table 4. Baseline Characteristics of the study population
Baseline Characteristics of the study population
Number of patients per participating center (% of total study population)
Pittsburgh 2974 (26.9%)
Rochester 2852 (25.2%)
Ghent 3044 (26.9%)
Vicenza 267 (2.4%)
Perth 2077 (18.4%)
Melbourne 95 (0.8%)
Number of AKI patients per participating center (% of AKI patients per center) Pittsburgh 923 (31,0%)
Rochester 704 (24,7%)
Ghent 679 (22,3%)
Vicenza 99 (37,1%)
Perth 811 (39,0%)
Melbourne 61 (64,2%)
Patient characteristics (% of study population) Gender
Male 6776 (60%)
Female 4532 (40%)
Median age (in years) 62 (48, 73)
Pittsburgh 61 (48,73)
Rochester 66 (52,77)
Ghent 62 (50,72)
Vicenza 64 (45,74)
Perth 55 (38,70)
Melbourne 62 (45,74)
Race
Caucasian 9536 (84.3%)
Black 450 (4.0%)
Hispanic 572 (5.1%)
Asian 43 (0.4%)
American Indian 10 (0.09%)
Other 149 (1.3%)
Availability of baseline creatinine 3452 (30.5%)
Pittsburgh 155 (5.2%)
Rochester 2794 (98.0%)
Ghent 181 (5.9%)
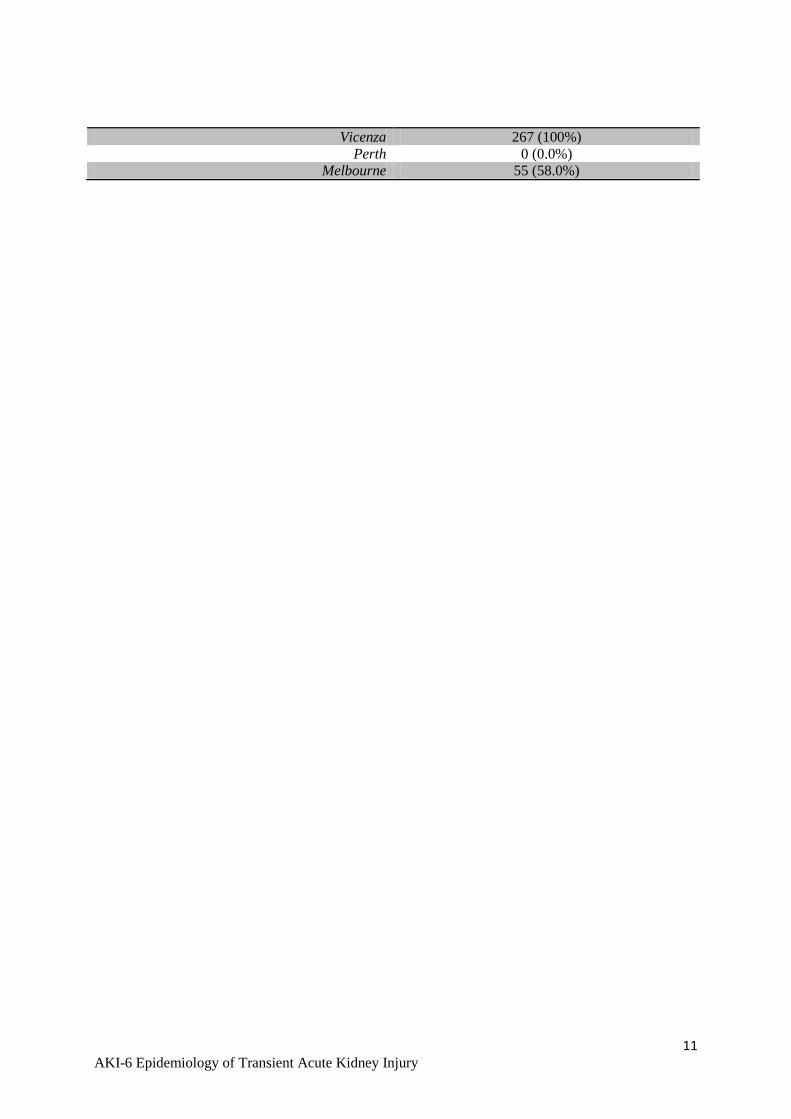
11 AKI-6 Epidemiology of Transient Acute Kidney Injury
Vicenza 267 (100%)
Perth 0 (0.0%)
Melbourne 55 (58.0%)
12 AKI-6 Epidemiology of Transient Acute Kidney Injury
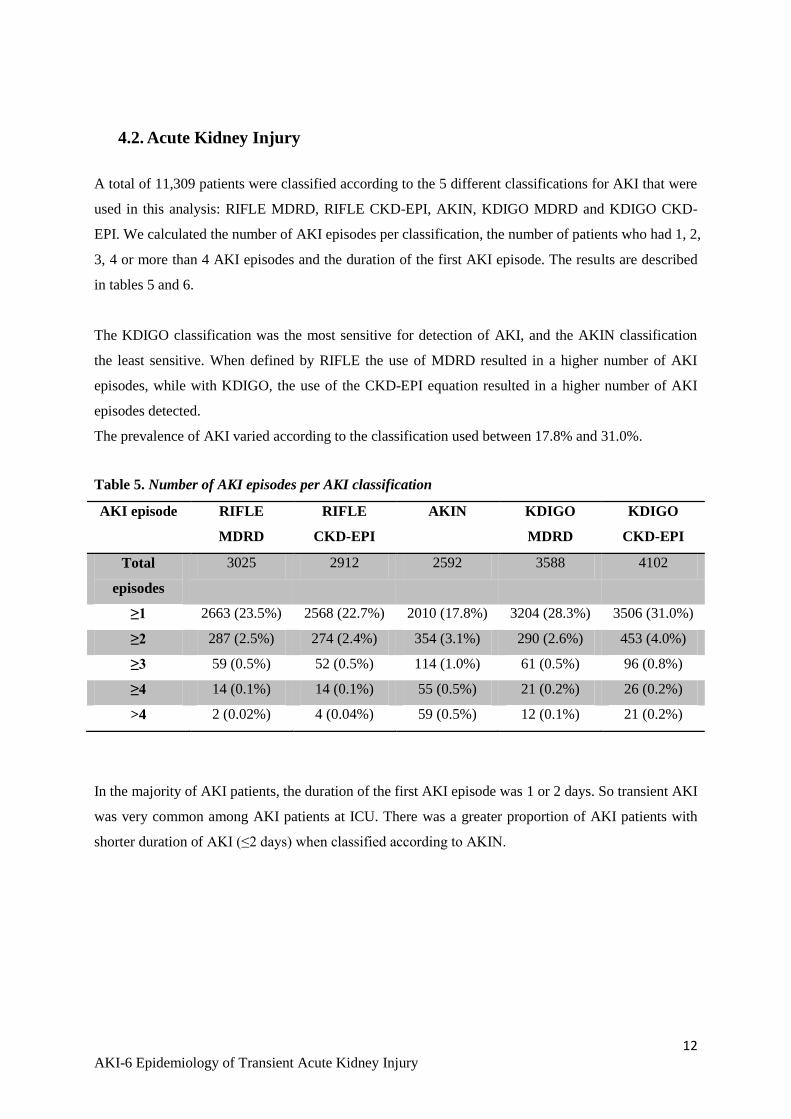
4.2. Acute Kidney Injury
A total of 11,309 patients were classified according to the 5 different classifications for AKI that were
used in this analysis: RIFLE MDRD, RIFLE CKD-EPI, AKIN, KDIGO MDRD and KDIGO CKD-
EPI. We calculated the number of AKI episodes per classification, the number of patients who had 1, 2,
3, 4 or more than 4 AKI episodes and the duration of the first AKI episode. The results are described
in tables 5 and 6.
The KDIGO classification was the most sensitive for detection of AKI, and the AKIN classification
the least sensitive. When defined by RIFLE the use of MDRD resulted in a higher number of AKI
episodes, while with KDIGO, the use of the CKD-EPI equation resulted in a higher number of AKI
episodes detected.
The prevalence of AKI varied according to the classification used between 17.8% and 31.0%.
Table 5. Number of AKI episodes per AKI classification
AKI episode
RIFLE
MDRD
RIFLE
CKD-EPI
AKIN
KDIGO
MDRD
KDIGO
CKD-EPI
Total
episodes
3025 2912 2592 3588 4102
≥1 2663 (23.5%) 2568 (22.7%) 2010 (17.8%) 3204 (28.3%) 3506 (31.0%)
≥2 287 (2.5%) 274 (2.4%) 354 (3.1%) 290 (2.6%) 453 (4.0%)
≥3 59 (0.5%) 52 (0.5%) 114 (1.0%) 61 (0.5%) 96 (0.8%)
≥4 14 (0.1%) 14 (0.1%) 55 (0.5%) 21 (0.2%) 26 (0.2%)
>4 2 (0.02%) 4 (0.04%) 59 (0.5%) 12 (0.1%) 21 (0.2%)
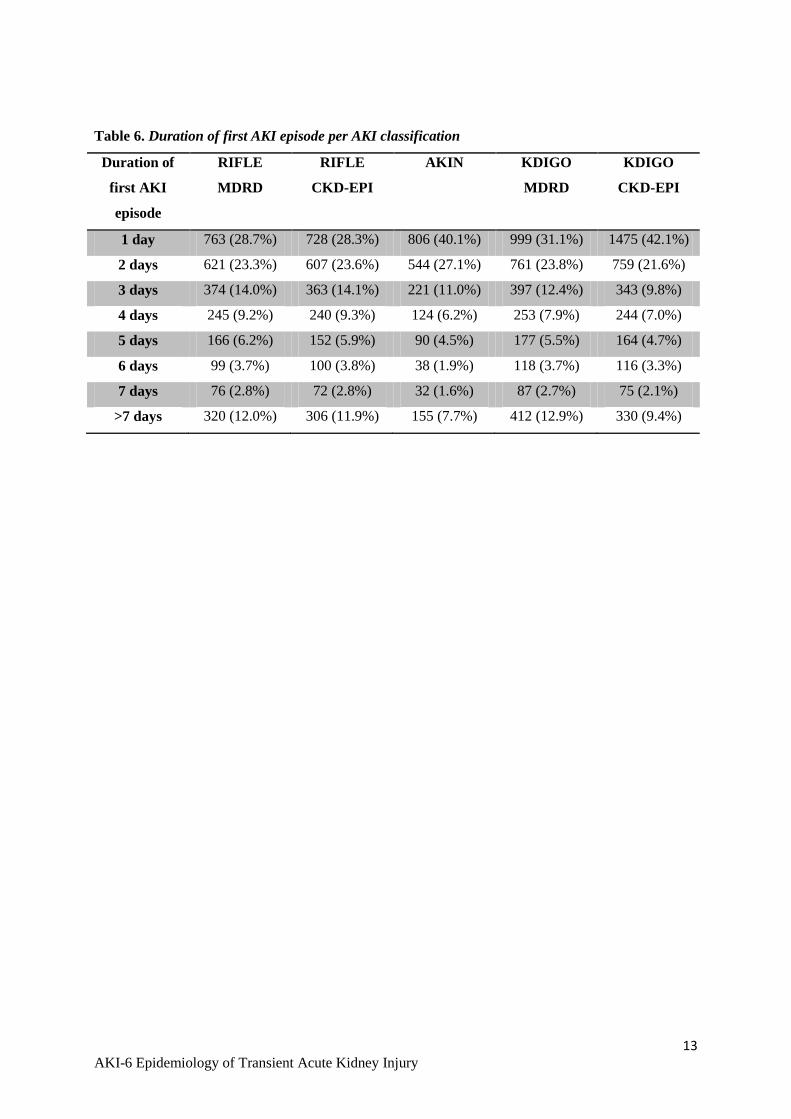
In the majority of AKI patients, the duration of the first AKI episode was 1 or 2 days. So transient AKI
was very common among AKI patients at ICU. There was a greater proportion of AKI patients with
shorter duration of AKI (≤2 days) when classified according to AKIN.
13 AKI-6 Epidemiology of Transient Acute Kidney Injury
Table 6. Duration of first AKI episode per AKI classification
Duration of
first AKI
episode
RIFLE
MDRD
RIFLE
CKD-EPI
AKIN KDIGO
MDRD
KDIGO
CKD-EPI
1 day 763 (28.7%) 728 (28.3%) 806 (40.1%) 999 (31.1%) 1475 (42.1%)
2 days 621 (23.3%) 607 (23.6%) 544 (27.1%) 761 (23.8%) 759 (21.6%)
3 days 374 (14.0%) 363 (14.1%) 221 (11.0%) 397 (12.4%) 343 (9.8%)
4 days 245 (9.2%) 240 (9.3%) 124 (6.2%) 253 (7.9%) 244 (7.0%)
5 days 166 (6.2%) 152 (5.9%) 90 (4.5%) 177 (5.5%) 164 (4.7%)
6 days 99 (3.7%) 100 (3.8%) 38 (1.9%) 118 (3.7%) 116 (3.3%)
7 days 76 (2.8%) 72 (2.8%) 32 (1.6%) 87 (2.7%) 75 (2.1%)
>7 days 320 (12.0%) 306 (11.9%) 155 (7.7%) 412 (12.9%) 330 (9.4%)
14 AKI-6 Epidemiology of Transient Acute Kidney Injury
4.3. Outcomes
The outcomes we analyzed were Intensive Care Unit Mortality (ICU Mortality), Hospital Mortality,
Intensive Care Unit Length of Stay (ICU Length of Stay) and Hospital Mortality. We compared
patients with and without AKI. AKI patients were classified according to the 5 different AKI
classifications: RIFLE MDRD, RIFLE CKD-EPI, AKIN, KDIGO MDRD and KDIGO CKD-EPI. We
also compared the outcomes of the different AKI stages. Only the first AKI episode was included in
our analyses.
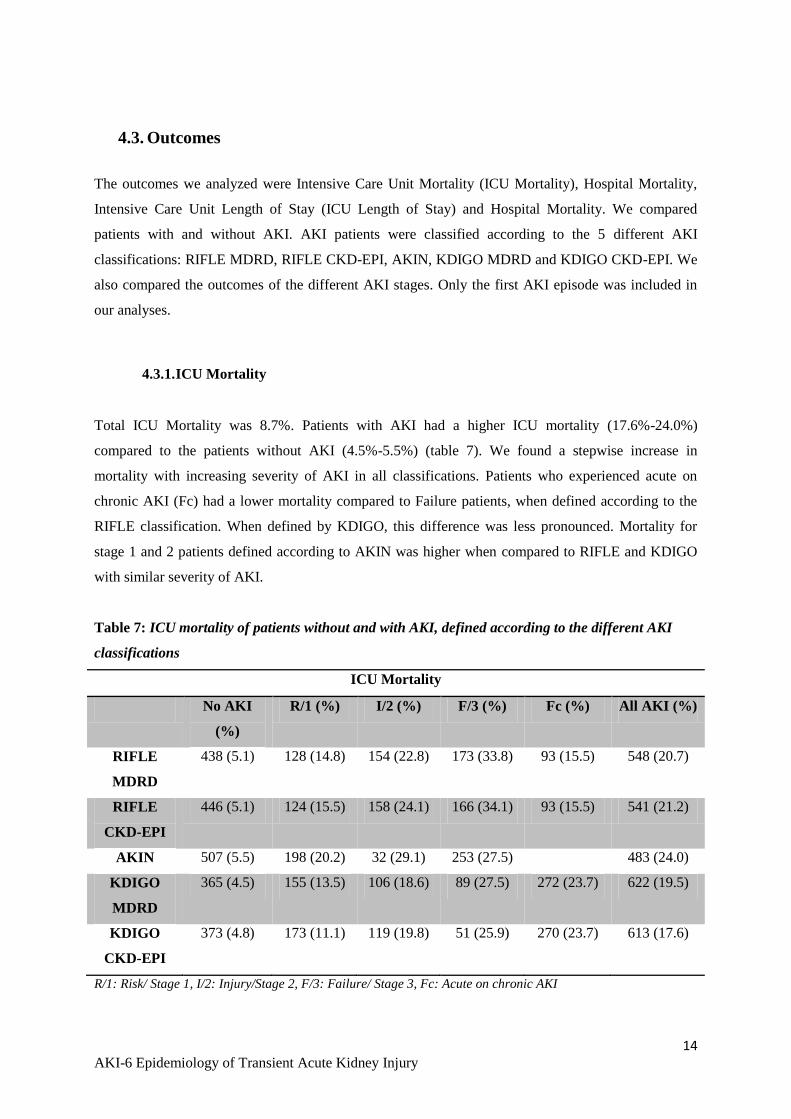
4.3.1. ICU Mortality
Total ICU Mortality was 8.7%. Patients with AKI had a higher ICU mortality (17.6%-24.0%)
compared to the patients without AKI (4.5%-5.5%) (table 7). We found a stepwise increase in
mortality with increasing severity of AKI in all classifications. Patients who experienced acute on
chronic AKI (Fc) had a lower mortality compared to Failure patients, when defined according to the
RIFLE classification. When defined by KDIGO, this difference was less pronounced. Mortality for
stage 1 and 2 patients defined according to AKIN was higher when compared to RIFLE and KDIGO
with similar severity of AKI.
Table 7: ICU mortality of patients without and with AKI, defined according to the different AKI
classifications
ICU Mortality
No AKI
(%)
R/1 (%) I/2 (%) F/3 (%) Fc (%) All AKI (%)
RIFLE
MDRD
438 (5.1) 128 (14.8) 154 (22.8) 173 (33.8) 93 (15.5) 548 (20.7)
RIFLE
CKD-EPI
446 (5.1) 124 (15.5) 158 (24.1) 166 (34.1) 93 (15.5) 541 (21.2)
AKIN 507 (5.5) 198 (20.2) 32 (29.1) 253 (27.5) 483 (24.0)
KDIGO
MDRD
365 (4.5) 155 (13.5) 106 (18.6) 89 (27.5) 272 (23.7) 622 (19.5)
KDIGO
CKD-EPI
373 (4.8) 173 (11.1) 119 (19.8) 51 (25.9) 270 (23.7) 613 (17.6)
R/1: Risk/ Stage 1, I/2: Injury/Stage 2, F/3: Failure/ Stage 3, Fc: Acute on chronic AKI
15 AKI-6 Epidemiology of Transient Acute Kidney Injury
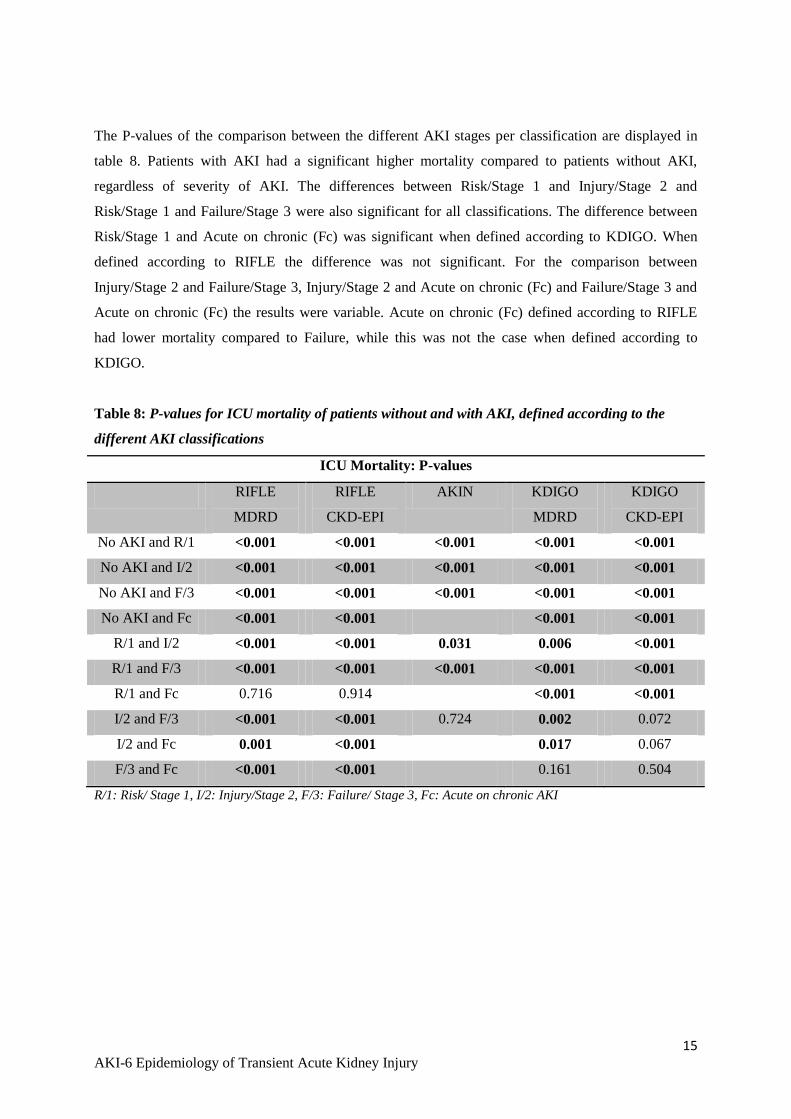
The P-values of the comparison between the different AKI stages per classification are displayed in
table 8. Patients with AKI had a significant higher mortality compared to patients without AKI,
regardless of severity of AKI. The differences between Risk/Stage 1 and Injury/Stage 2 and
Risk/Stage 1 and Failure/Stage 3 were also significant for all classifications. The difference between
Risk/Stage 1 and Acute on chronic (Fc) was significant when defined according to KDIGO. When
defined according to RIFLE the difference was not significant. For the comparison between
Injury/Stage 2 and Failure/Stage 3, Injury/Stage 2 and Acute on chronic (Fc) and Failure/Stage 3 and
Acute on chronic (Fc) the results were variable. Acute on chronic (Fc) defined according to RIFLE
had lower mortality compared to Failure, while this was not the case when defined according to
KDIGO.
Table 8: P-values for ICU mortality of patients without and with AKI, defined according to the
different AKI classifications
ICU Mortality: P-values
RIFLE
MDRD
RIFLE
CKD-EPI
AKIN KDIGO
MDRD
KDIGO
CKD-EPI
No AKI and R/1 <0.001 <0.001 <0.001 <0.001 <0.001
No AKI and I/2 <0.001 <0.001 <0.001 <0.001 <0.001
No AKI and F/3 <0.001 <0.001 <0.001 <0.001 <0.001
No AKI and Fc <0.001 <0.001 <0.001 <0.001
R/1 and I/2 <0.001 <0.001 0.031 0.006 <0.001
R/1 and F/3 <0.001 <0.001 <0.001 <0.001 <0.001
R/1 and Fc 0.716 0.914 <0.001 <0.001
I/2 and F/3 <0.001 <0.001 0.724 0.002 0.072
I/2 and Fc 0.001 <0.001 0.017 0.067
F/3 and Fc <0.001 <0.001 0.161 0.504
R/1: Risk/ Stage 1, I/2: Injury/Stage 2, F/3: Failure/ Stage 3, Fc: Acute on chronic AKI
16 AKI-6 Epidemiology of Transient Acute Kidney Injury
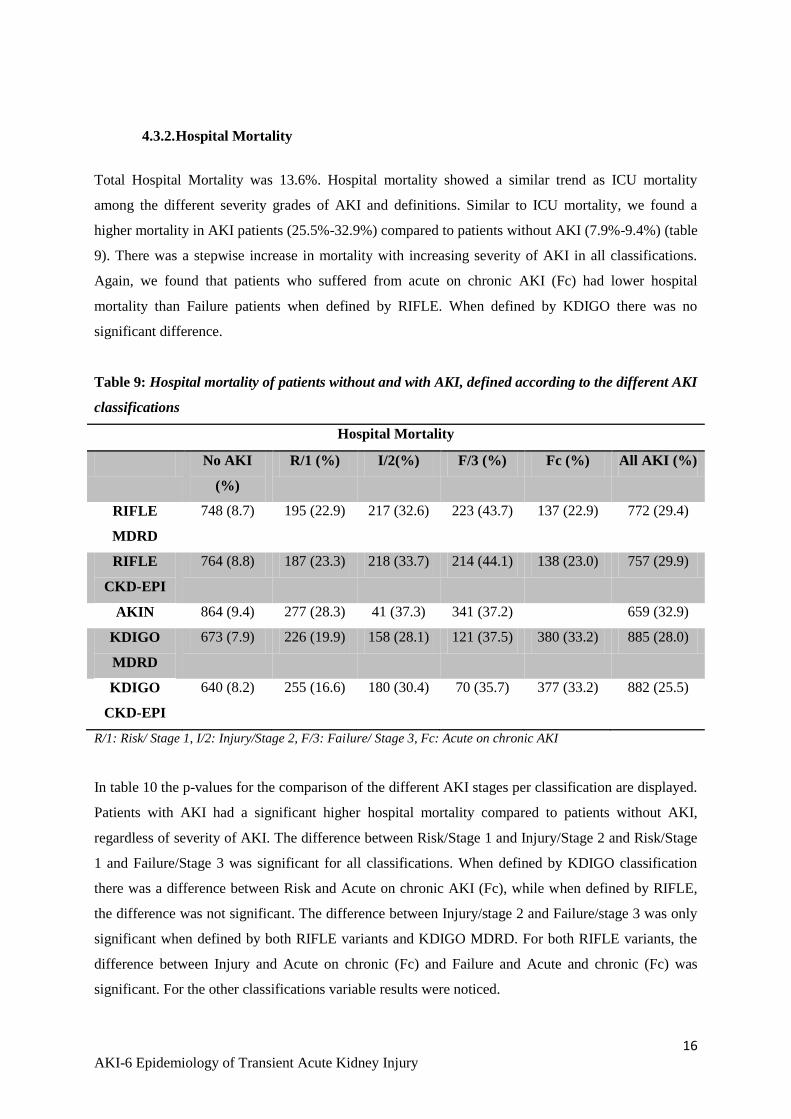
4.3.2. Hospital Mortality
Total Hospital Mortality was 13.6%. Hospital mortality showed a similar trend as ICU mortality
among the different severity grades of AKI and definitions. Similar to ICU mortality, we found a
higher mortality in AKI patients (25.5%-32.9%) compared to patients without AKI (7.9%-9.4%) (table
9). There was a stepwise increase in mortality with increasing severity of AKI in all classifications.
Again, we found that patients who suffered from acute on chronic AKI (Fc) had lower hospital
mortality than Failure patients when defined by RIFLE. When defined by KDIGO there was no
significant difference.
Table 9: Hospital mortality of patients without and with AKI, defined according to the different AKI
classifications
Hospital Mortality
No AKI
(%)
R/1 (%) I/2(%) F/3 (%) Fc (%) All AKI (%)
RIFLE
MDRD
748 (8.7) 195 (22.9) 217 (32.6) 223 (43.7) 137 (22.9) 772 (29.4)
RIFLE
CKD-EPI
764 (8.8) 187 (23.3) 218 (33.7) 214 (44.1) 138 (23.0) 757 (29.9)
AKIN 864 (9.4) 277 (28.3) 41 (37.3) 341 (37.2) 659 (32.9)
KDIGO
MDRD
673 (7.9) 226 (19.9) 158 (28.1) 121 (37.5) 380 (33.2) 885 (28.0)
KDIGO
CKD-EPI
640 (8.2) 255 (16.6) 180 (30.4) 70 (35.7) 377 (33.2) 882 (25.5)
R/1: Risk/ Stage 1, I/2: Injury/Stage 2, F/3: Failure/ Stage 3, Fc: Acute on chronic AKI
In table 10 the p-values for the comparison of the different AKI stages per classification are displayed.
Patients with AKI had a significant higher hospital mortality compared to patients without AKI,
regardless of severity of AKI. The difference between Risk/Stage 1 and Injury/Stage 2 and Risk/Stage
1 and Failure/Stage 3 was significant for all classifications. When defined by KDIGO classification
there was a difference between Risk and Acute on chronic AKI (Fc), while when defined by RIFLE,
the difference was not significant. The difference between Injury/stage 2 and Failure/stage 3 was only
significant when defined by both RIFLE variants and KDIGO MDRD. For both RIFLE variants, the
difference between Injury and Acute on chronic (Fc) and Failure and Acute and chronic (Fc) was
significant. For the other classifications variable results were noticed.
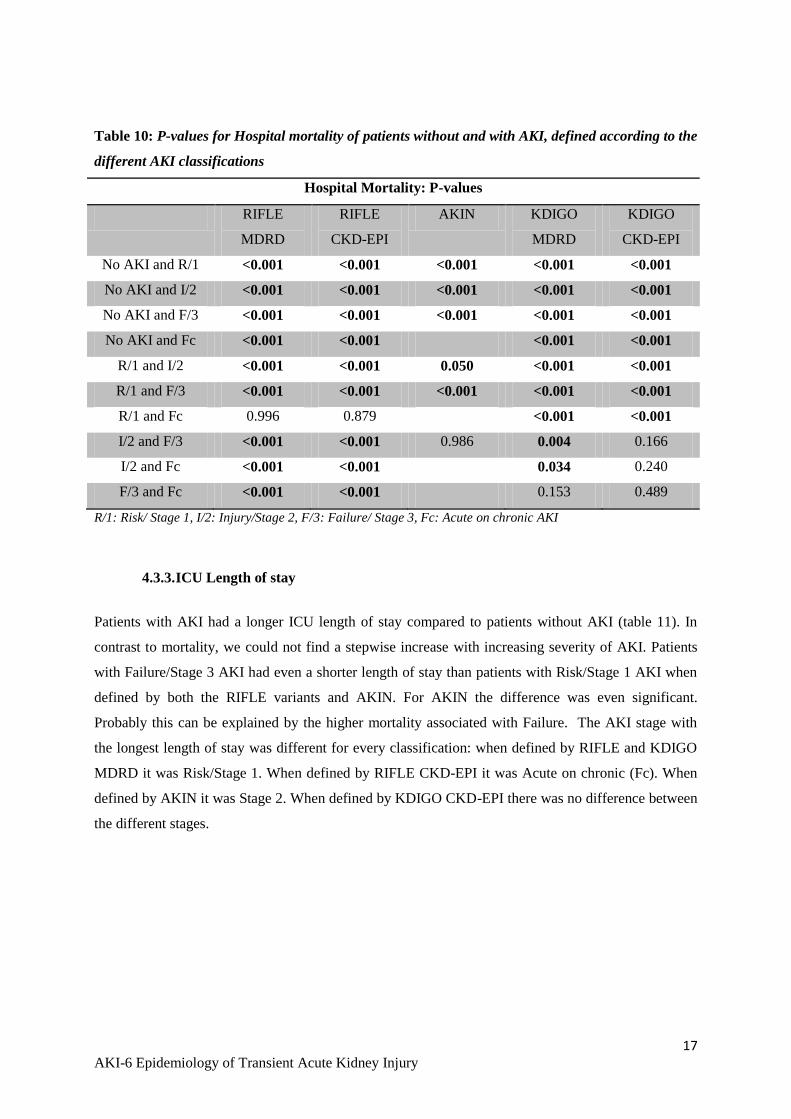
17 AKI-6 Epidemiology of Transient Acute Kidney Injury
Table 10: P-values for Hospital mortality of patients without and with AKI, defined according to the
different AKI classifications
Hospital Mortality: P-values
RIFLE
MDRD
RIFLE
CKD-EPI
AKIN KDIGO
MDRD
KDIGO
CKD-EPI
No AKI and R/1 <0.001 <0.001 <0.001 <0.001 <0.001
No AKI and I/2 <0.001 <0.001 <0.001 <0.001 <0.001
No AKI and F/3 <0.001 <0.001 <0.001 <0.001 <0.001
No AKI and Fc <0.001 <0.001 <0.001 <0.001
R/1 and I/2 <0.001 <0.001 0.050 <0.001 <0.001
R/1 and F/3 <0.001 <0.001 <0.001 <0.001 <0.001
R/1 and Fc 0.996 0.879 <0.001 <0.001
I/2 and F/3 <0.001 <0.001 0.986 0.004 0.166
I/2 and Fc <0.001 <0.001 0.034 0.240
F/3 and Fc <0.001 <0.001 0.153 0.489
R/1: Risk/ Stage 1, I/2: Injury/Stage 2, F/3: Failure/ Stage 3, Fc: Acute on chronic AKI
4.3.3. ICU Length of stay
Patients with AKI had a longer ICU length of stay compared to patients without AKI (table 11). In
contrast to mortality, we could not find a stepwise increase with increasing severity of AKI. Patients
with Failure/Stage 3 AKI had even a shorter length of stay than patients with Risk/Stage 1 AKI when
defined by both the RIFLE variants and AKIN. For AKIN the difference was even significant.
Probably this can be explained by the higher mortality associated with Failure. The AKI stage with
the longest length of stay was different for every classification: when defined by RIFLE and KDIGO
MDRD it was Risk/Stage 1. When defined by RIFLE CKD-EPI it was Acute on chronic (Fc). When
defined by AKIN it was Stage 2. When defined by KDIGO CKD-EPI there was no difference between
the different stages.
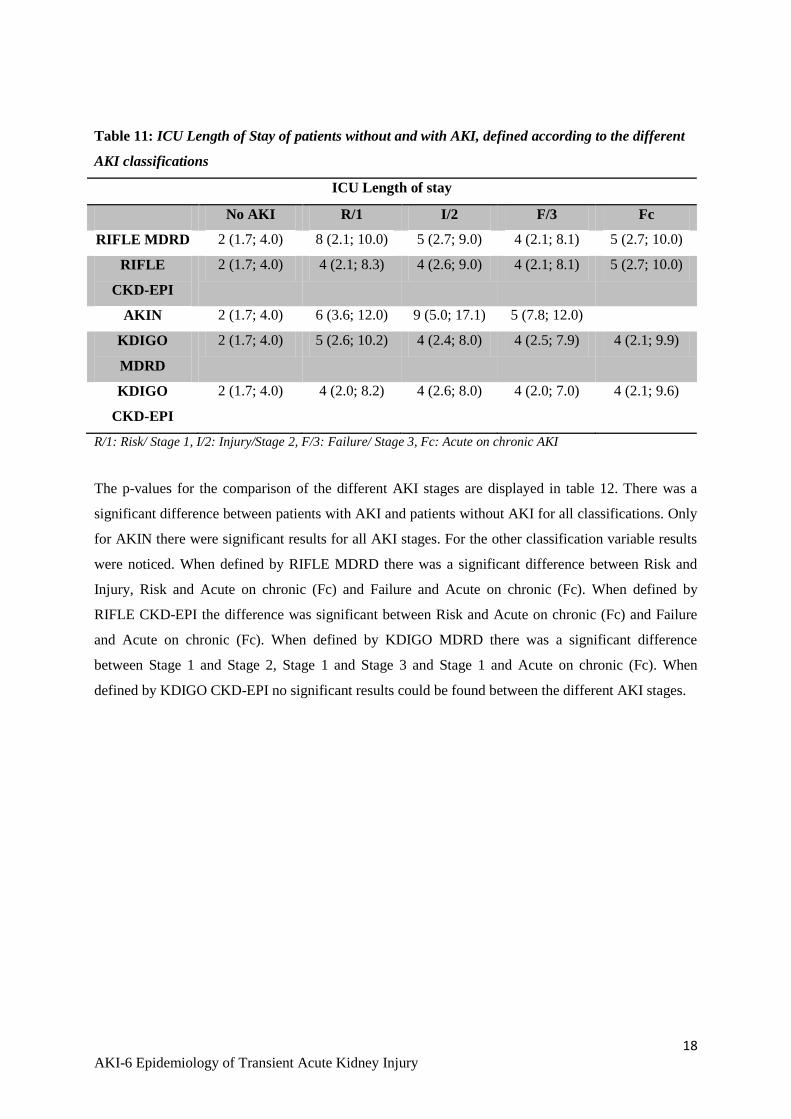
18 AKI-6 Epidemiology of Transient Acute Kidney Injury
Table 11: ICU Length of Stay of patients without and with AKI, defined according to the different
AKI classifications
ICU Length of stay
No AKI R/1 I/2 F/3 Fc
RIFLE MDRD 2 (1.7; 4.0) 8 (2.1; 10.0) 5 (2.7; 9.0) 4 (2.1; 8.1) 5 (2.7; 10.0)
RIFLE
CKD-EPI
2 (1.7; 4.0) 4 (2.1; 8.3) 4 (2.6; 9.0) 4 (2.1; 8.1) 5 (2.7; 10.0)
AKIN 2 (1.7; 4.0) 6 (3.6; 12.0) 9 (5.0; 17.1) 5 (7.8; 12.0)
KDIGO
MDRD
2 (1.7; 4.0) 5 (2.6; 10.2) 4 (2.4; 8.0) 4 (2.5; 7.9) 4 (2.1; 9.9)
KDIGO
CKD-EPI
2 (1.7; 4.0) 4 (2.0; 8.2) 4 (2.6; 8.0) 4 (2.0; 7.0) 4 (2.1; 9.6)
R/1: Risk/ Stage 1, I/2: Injury/Stage 2, F/3: Failure/ Stage 3, Fc: Acute on chronic AKI
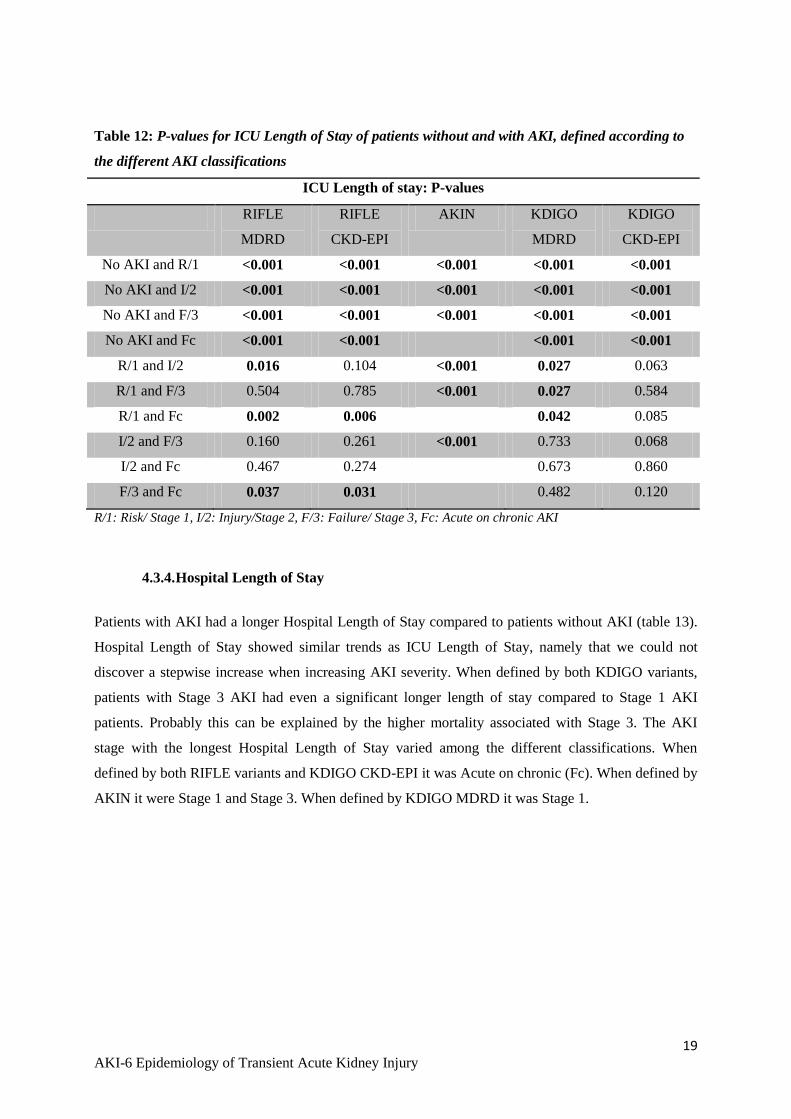
The p-values for the comparison of the different AKI stages are displayed in table 12. There was a
significant difference between patients with AKI and patients without AKI for all classifications. Only
for AKIN there were significant results for all AKI stages. For the other classification variable results
were noticed. When defined by RIFLE MDRD there was a significant difference between Risk and
Injury, Risk and Acute on chronic (Fc) and Failure and Acute on chronic (Fc). When defined by
RIFLE CKD-EPI the difference was significant between Risk and Acute on chronic (Fc) and Failure
and Acute on chronic (Fc). When defined by KDIGO MDRD there was a significant difference
between Stage 1 and Stage 2, Stage 1 and Stage 3 and Stage 1 and Acute on chronic (Fc). When
defined by KDIGO CKD-EPI no significant results could be found between the different AKI stages.
19 AKI-6 Epidemiology of Transient Acute Kidney Injury
Table 12: P-values for ICU Length of Stay of patients without and with AKI, defined according to
the different AKI classifications
ICU Length of stay: P-values
RIFLE
MDRD
RIFLE
CKD-EPI
AKIN KDIGO
MDRD
KDIGO
CKD-EPI
No AKI and R/1 <0.001 <0.001 <0.001 <0.001 <0.001
No AKI and I/2 <0.001 <0.001 <0.001 <0.001 <0.001
No AKI and F/3 <0.001 <0.001 <0.001 <0.001 <0.001
No AKI and Fc <0.001 <0.001 <0.001 <0.001
R/1 and I/2 0.016 0.104 <0.001 0.027 0.063
R/1 and F/3 0.504 0.785 <0.001 0.027 0.584
R/1 and Fc 0.002 0.006 0.042 0.085
I/2 and F/3 0.160 0.261 <0.001 0.733 0.068
I/2 and Fc 0.467 0.274 0.673 0.860
F/3 and Fc 0.037 0.031 0.482 0.120
R/1: Risk/ Stage 1, I/2: Injury/Stage 2, F/3: Failure/ Stage 3, Fc: Acute on chronic AKI
4.3.4. Hospital Length of Stay
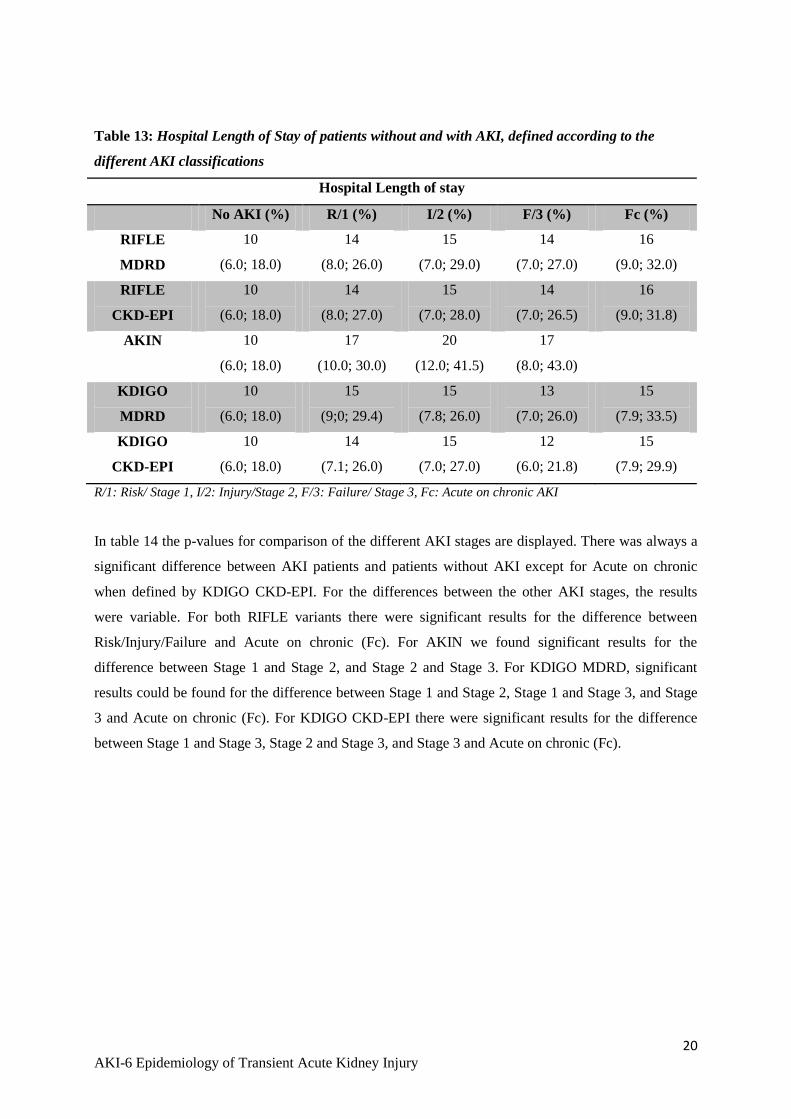
Patients with AKI had a longer Hospital Length of Stay compared to patients without AKI (table 13).
Hospital Length of Stay showed similar trends as ICU Length of Stay, namely that we could not
discover a stepwise increase when increasing AKI severity. When defined by both KDIGO variants,
patients with Stage 3 AKI had even a significant longer length of stay compared to Stage 1 AKI
patients. Probably this can be explained by the higher mortality associated with Stage 3. The AKI
stage with the longest Hospital Length of Stay varied among the different classifications. When
defined by both RIFLE variants and KDIGO CKD-EPI it was Acute on chronic (Fc). When defined by
AKIN it were Stage 1 and Stage 3. When defined by KDIGO MDRD it was Stage 1.
20 AKI-6 Epidemiology of Transient Acute Kidney Injury
Table 13: Hospital Length of Stay of patients without and with AKI, defined according to the
different AKI classifications
Hospital Length of stay
No AKI (%) R/1 (%) I/2 (%) F/3 (%) Fc (%)
RIFLE
MDRD
10
(6.0; 18.0)
14
(8.0; 26.0)
15
(7.0; 29.0)
14
(7.0; 27.0)
16
(9.0; 32.0)
RIFLE
CKD-EPI
10
(6.0; 18.0)
14
(8.0; 27.0)
15
(7.0; 28.0)
14
(7.0; 26.5)
16
(9.0; 31.8)
AKIN 10
(6.0; 18.0)
17
(10.0; 30.0)
20
(12.0; 41.5)
17
(8.0; 43.0)
KDIGO
MDRD
10
(6.0; 18.0)
15
(9;0; 29.4)
15
(7.8; 26.0)
13
(7.0; 26.0)
15
(7.9; 33.5)
KDIGO
CKD-EPI
10
(6.0; 18.0)
14
(7.1; 26.0)
15
(7.0; 27.0)
12
(6.0; 21.8)
15
(7.9; 29.9)
R/1: Risk/ Stage 1, I/2: Injury/Stage 2, F/3: Failure/ Stage 3, Fc: Acute on chronic AKI
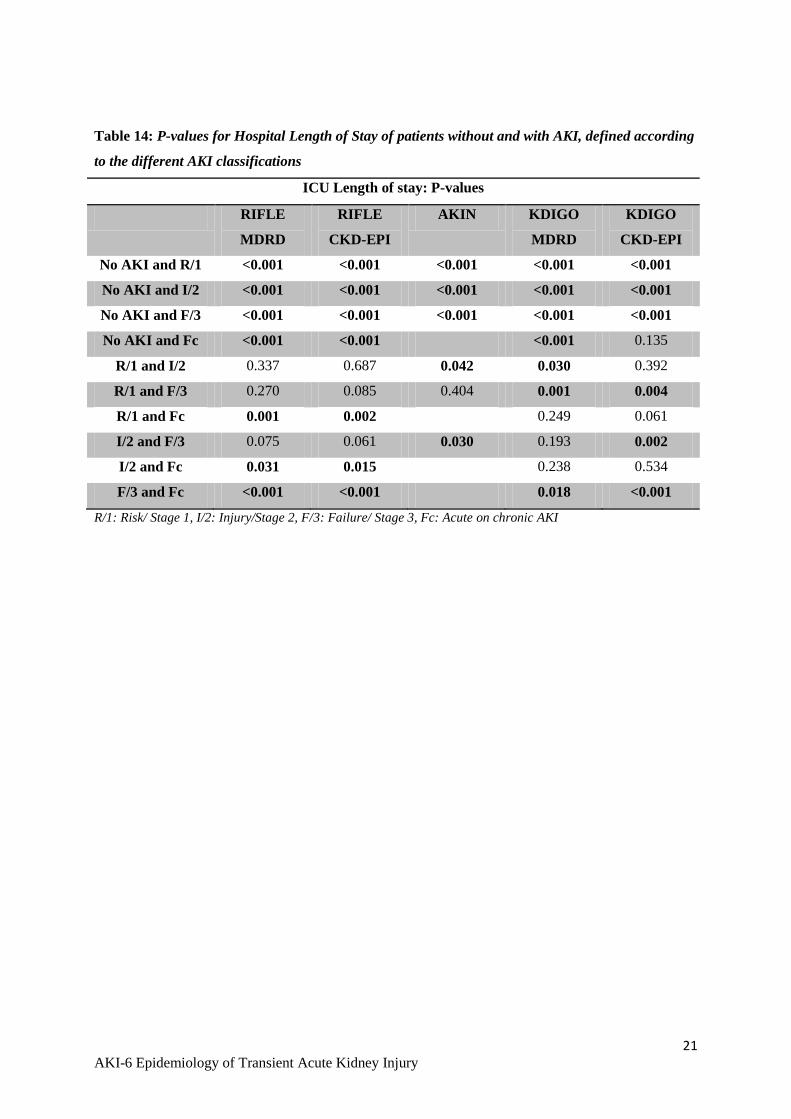
In table 14 the p-values for comparison of the different AKI stages are displayed. There was always a
significant difference between AKI patients and patients without AKI except for Acute on chronic
when defined by KDIGO CKD-EPI. For the differences between the other AKI stages, the results
were variable. For both RIFLE variants there were significant results for the difference between
Risk/Injury/Failure and Acute on chronic (Fc). For AKIN we found significant results for the
difference between Stage 1 and Stage 2, and Stage 2 and Stage 3. For KDIGO MDRD, significant
results could be found for the difference between Stage 1 and Stage 2, Stage 1 and Stage 3, and Stage
3 and Acute on chronic (Fc). For KDIGO CKD-EPI there were significant results for the difference
between Stage 1 and Stage 3, Stage 2 and Stage 3, and Stage 3 and Acute on chronic (Fc).
21 AKI-6 Epidemiology of Transient Acute Kidney Injury
Table 14: P-values for Hospital Length of Stay of patients without and with AKI, defined according
to the different AKI classifications
ICU Length of stay: P-values
RIFLE
MDRD
RIFLE
CKD-EPI
AKIN KDIGO
MDRD
KDIGO
CKD-EPI
No AKI and R/1 <0.001 <0.001 <0.001 <0.001 <0.001
No AKI and I/2 <0.001 <0.001 <0.001 <0.001 <0.001
No AKI and F/3 <0.001 <0.001 <0.001 <0.001 <0.001
No AKI and Fc <0.001 <0.001 <0.001 0.135
R/1 and I/2 0.337 0.687 0.042 0.030 0.392
R/1 and F/3 0.270 0.085 0.404 0.001 0.004
R/1 and Fc 0.001 0.002 0.249 0.061
I/2 and F/3 0.075 0.061 0.030 0.193 0.002
I/2 and Fc 0.031 0.015 0.238 0.534
F/3 and Fc <0.001 <0.001 0.018 <0.001
R/1: Risk/ Stage 1, I/2: Injury/Stage 2, F/3: Failure/ Stage 3, Fc: Acute on chronic AKI
22 AKI-6 Epidemiology of Transient Acute Kidney Injury
4.4. Transient AKI
One of the important aims of the TRAK study was to investigate the influence of AKI duration on
outcomes in ICU patients. To explore this influence we compared patients with transient AKI and
patients with a longer AKI episode. We defined transient AKI in three different ways:
1. Transient AKI with duration of ≤ 3 days of AKI (AKIt3)
2. Transient AKI with duration of ≤ 2 days of AKI (AKIt2)
3. Transient AKI with duration of ≤ 1 days of AKI (AKIt1)
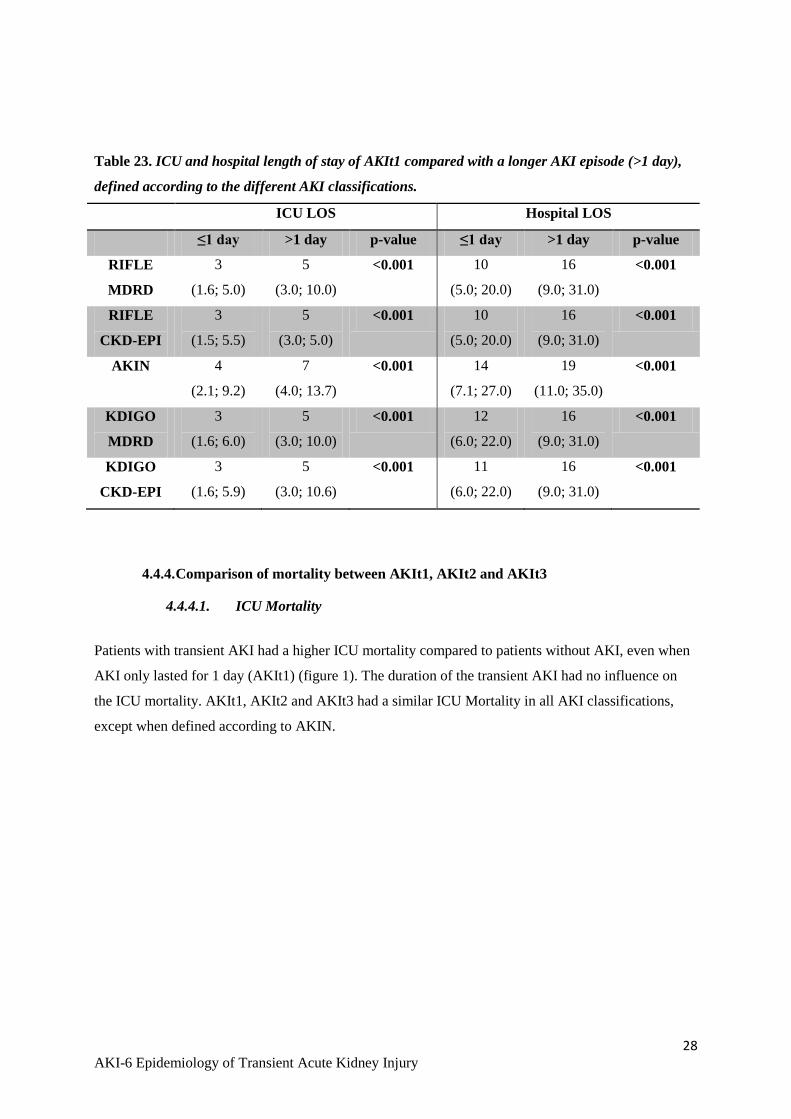
In table 15 to 23, the period prevalence of transient AKI and the influence of AKI duration on
outcomes are described for the 5 different AKI classifications used in this analysis: RIFLE MDRD,
RIFLE CKD-EPI, AKIN, KDIGO MDRD, KDIGO CKD-EPI.
We also compared the ICU and hospital mortality of the different transient AKI definitions (figure 1, 2
and table 24 and 25).
4.4.1. Transient AKI defined as ≤3 days of AKI (AKIt3)
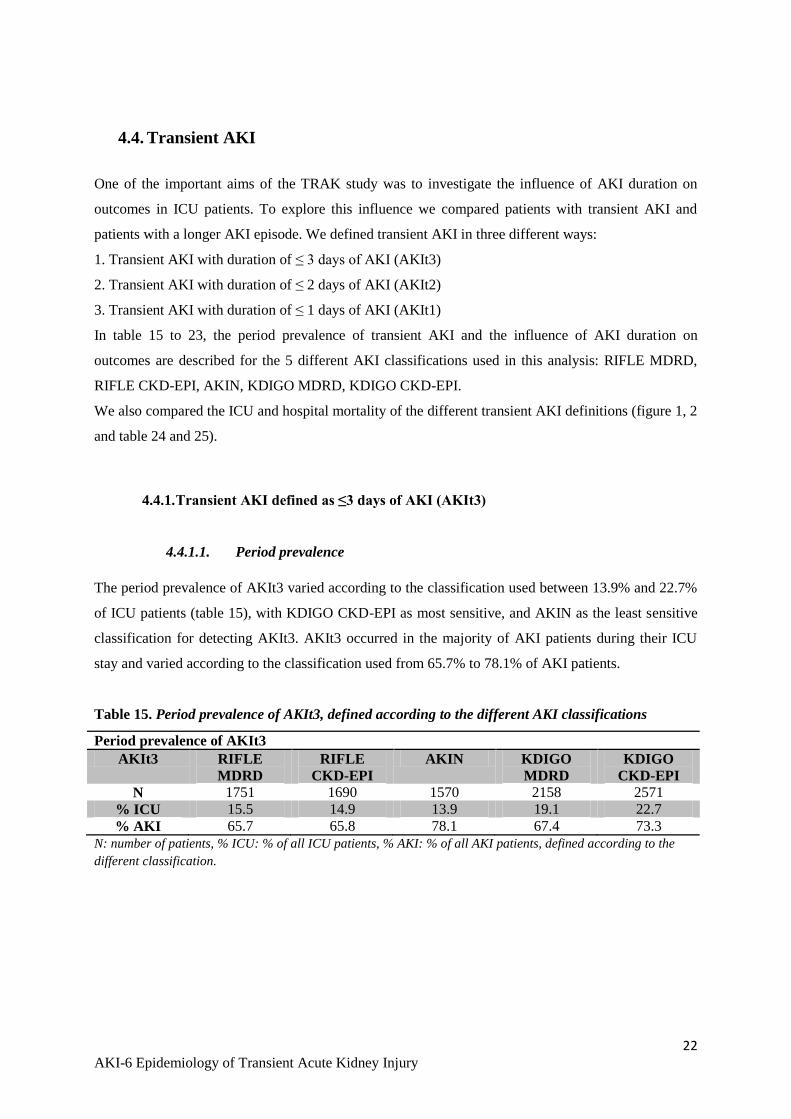
4.4.1.1. Period prevalence
The period prevalence of AKIt3 varied according to the classification used between 13.9% and 22.7%
of ICU patients (table 15), with KDIGO CKD-EPI as most sensitive, and AKIN as the least sensitive
classification for detecting AKIt3. AKIt3 occurred in the majority of AKI patients during their ICU
stay and varied according to the classification used from 65.7% to 78.1% of AKI patients.
Table 15. Period prevalence of AKIt3, defined according to the different AKI classifications
Period prevalence of AKIt3
AKIt3 RIFLE
MDRD
RIFLE
CKD-EPI
AKIN KDIGO
MDRD
KDIGO
CKD-EPI
N 1751 1690 1570 2158 2571
% ICU 15.5 14.9 13.9 19.1 22.7
% AKI 65.7 65.8 78.1 67.4 73.3
N: number of patients, % ICU: % of all ICU patients, % AKI: % of all AKI patients, defined according to the
different classification.
23 AKI-6 Epidemiology of Transient Acute Kidney Injury
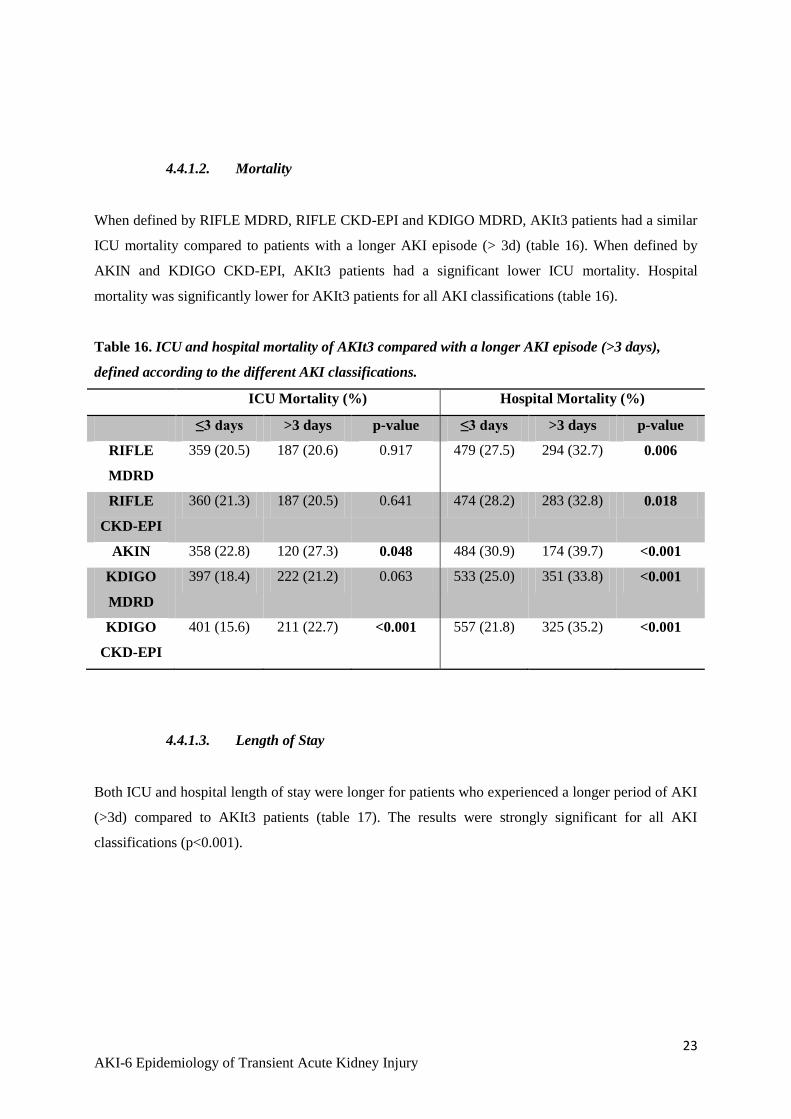
4.4.1.2. Mortality
When defined by RIFLE MDRD, RIFLE CKD-EPI and KDIGO MDRD, AKIt3 patients had a similar
ICU mortality compared to patients with a longer AKI episode (> 3d) (table 16). When defined by
AKIN and KDIGO CKD-EPI, AKIt3 patients had a significant lower ICU mortality. Hospital
mortality was significantly lower for AKIt3 patients for all AKI classifications (table 16).
Table 16. ICU and hospital mortality of AKIt3 compared with a longer AKI episode (>3 days),
defined according to the different AKI classifications.
ICU Mortality (%) Hospital Mortality (%)
≤3 days >3 days p-value ≤3 days >3 days p-value
RIFLE
MDRD
359 (20.5) 187 (20.6) 0.917 479 (27.5) 294 (32.7) 0.006
RIFLE
CKD-EPI
360 (21.3) 187 (20.5) 0.641 474 (28.2) 283 (32.8) 0.018
AKIN 358 (22.8) 120 (27.3) 0.048 484 (30.9) 174 (39.7) <0.001
KDIGO
MDRD
397 (18.4) 222 (21.2) 0.063 533 (25.0) 351 (33.8) <0.001
KDIGO
CKD-EPI
401 (15.6) 211 (22.7) <0.001 557 (21.8) 325 (35.2) <0.001
4.4.1.3. Length of Stay
Both ICU and hospital length of stay were longer for patients who experienced a longer period of AKI
(>3d) compared to AKIt3 patients (table 17). The results were strongly significant for all AKI
classifications (p<0.001).
24 AKI-6 Epidemiology of Transient Acute Kidney Injury
Table 17. ICU and hospital length of stay of AKIt3 compared with a longer AKI episode (>3 days),
defined according to the different AKI classifications.
ICU LOS Hospital LOS
≤3 days >3 days p-value ≤3 days >3 days p-value
RIFLE
MDRD
3
(2.0;5.3)
8
(5.0;18;0)
<0.001 12
(6.0; 22.0)
22
(14.0; 39.0)
<0.001
RIFLE
CKD-EPI
5
(2.0; 5.5)
8
(5.0; 14.7)
<0.001 12
(6.0; 22;0)
22
(14.0; 40.0)
<0.001
AKIN 5
(2.8; 10.0)
10
(6.4; 19.0)
<0.001 15
(8.0; 29.0)
26
(15.0; 44.0)
<0.001
KDIGO
MDRD
3
(2.0; 6.0)
8
(5.0; 15.0)
<0.001 12
(7.0; 23.0)
21
(13.0; 39.0)
<0.001
KDIGO
CKD-EPI
3
(1.8; 5.8)
7
(4.0; 13.0)
<0.001 12
(6.0; 22.0)
19
(11.0; 36.0)
<0.001
4.4.2. Transient AKI defined as ≤ 2 days of AKI (AKIt2)
4.4.2.1. Period prevalence
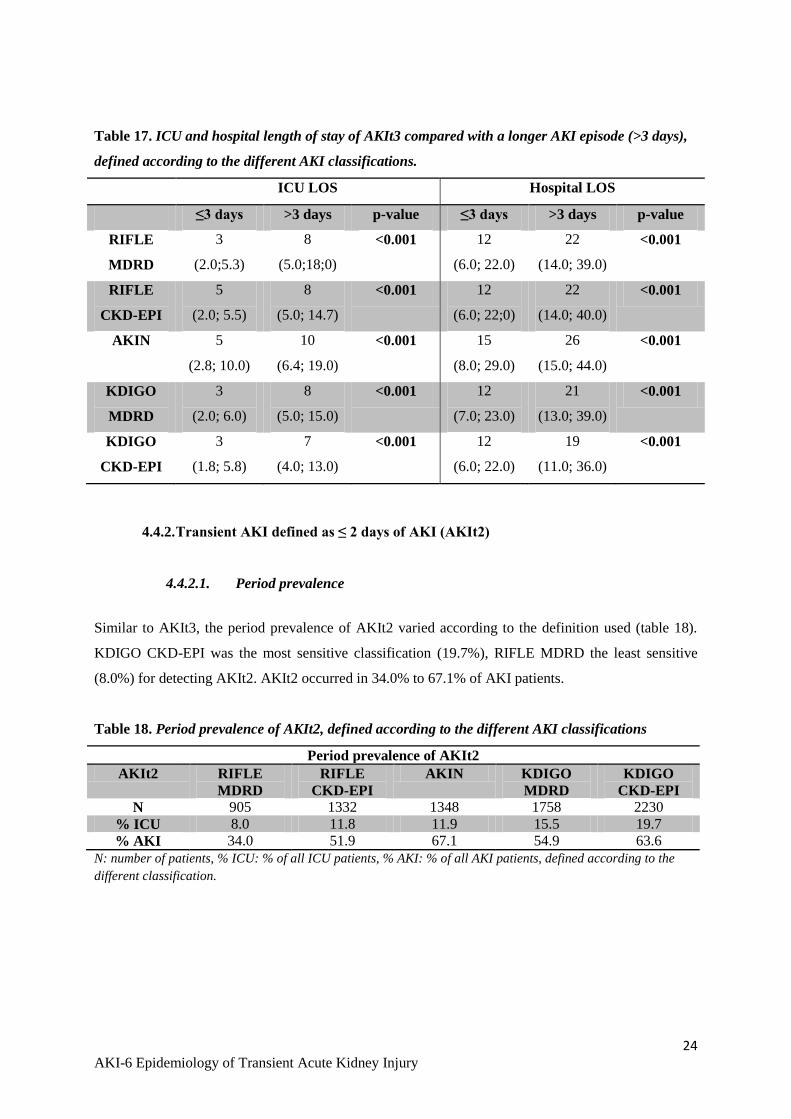
Similar to AKIt3, the period prevalence of AKIt2 varied according to the definition used (table 18).
KDIGO CKD-EPI was the most sensitive classification (19.7%), RIFLE MDRD the least sensitive
(8.0%) for detecting AKIt2. AKIt2 occurred in 34.0% to 67.1% of AKI patients.
Table 18. Period prevalence of AKIt2, defined according to the different AKI classifications
Period prevalence of AKIt2
AKIt2 RIFLE
MDRD
RIFLE
CKD-EPI
AKIN KDIGO
MDRD
KDIGO
CKD-EPI
N 905 1332 1348 1758 2230
% ICU 8.0 11.8 11.9 15.5 19.7
% AKI 34.0 51.9 67.1 54.9 63.6
N: number of patients, % ICU: % of all ICU patients, % AKI: % of all AKI patients, defined according to the
different classification.
25 AKI-6 Epidemiology of Transient Acute Kidney Injury
4.4.2.2. Mortality
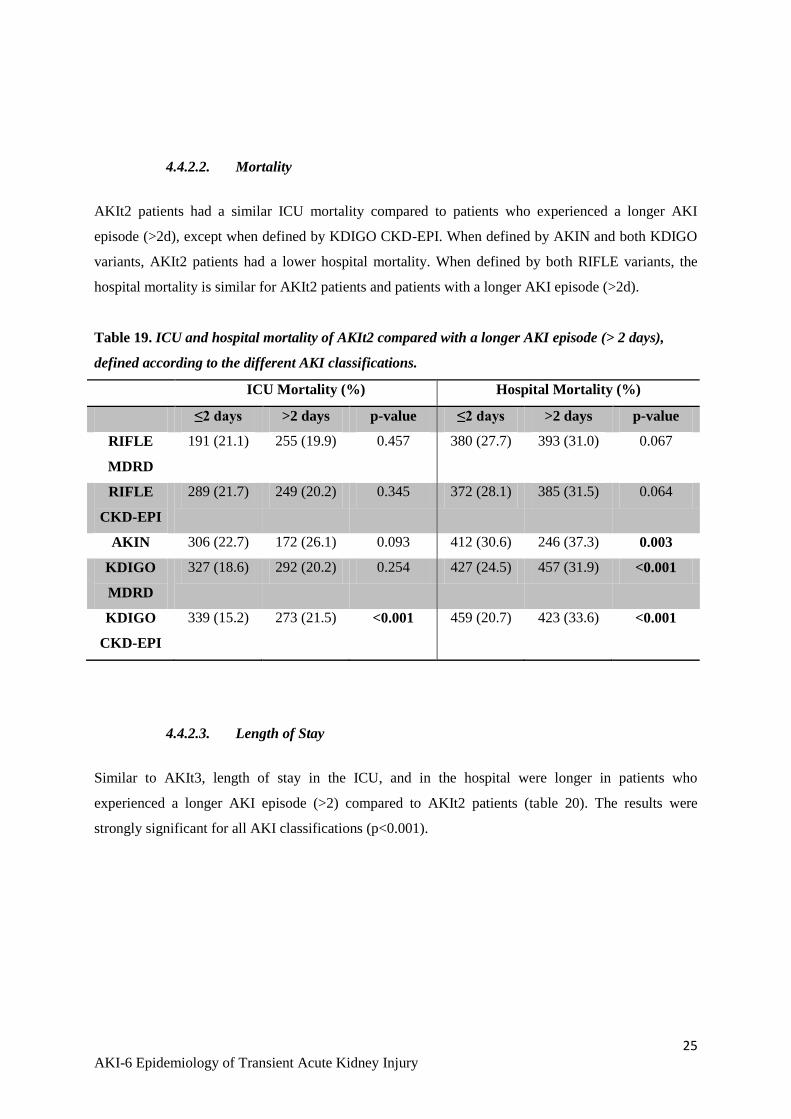
AKIt2 patients had a similar ICU mortality compared to patients who experienced a longer AKI
episode (>2d), except when defined by KDIGO CKD-EPI. When defined by AKIN and both KDIGO
variants, AKIt2 patients had a lower hospital mortality. When defined by both RIFLE variants, the
hospital mortality is similar for AKIt2 patients and patients with a longer AKI episode (>2d).
Table 19. ICU and hospital mortality of AKIt2 compared with a longer AKI episode (> 2 days),
defined according to the different AKI classifications.
ICU Mortality (%) Hospital Mortality (%)
≤2 days >2 days p-value ≤2 days >2 days p-value
RIFLE
MDRD
191 (21.1) 255 (19.9) 0.457 380 (27.7) 393 (31.0) 0.067
RIFLE
CKD-EPI
289 (21.7) 249 (20.2) 0.345 372 (28.1) 385 (31.5) 0.064
AKIN 306 (22.7) 172 (26.1) 0.093 412 (30.6) 246 (37.3) 0.003
KDIGO
MDRD
327 (18.6) 292 (20.2) 0.254 427 (24.5) 457 (31.9) <0.001
KDIGO
CKD-EPI
339 (15.2) 273 (21.5) <0.001 459 (20.7) 423 (33.6) <0.001
4.4.2.3. Length of Stay
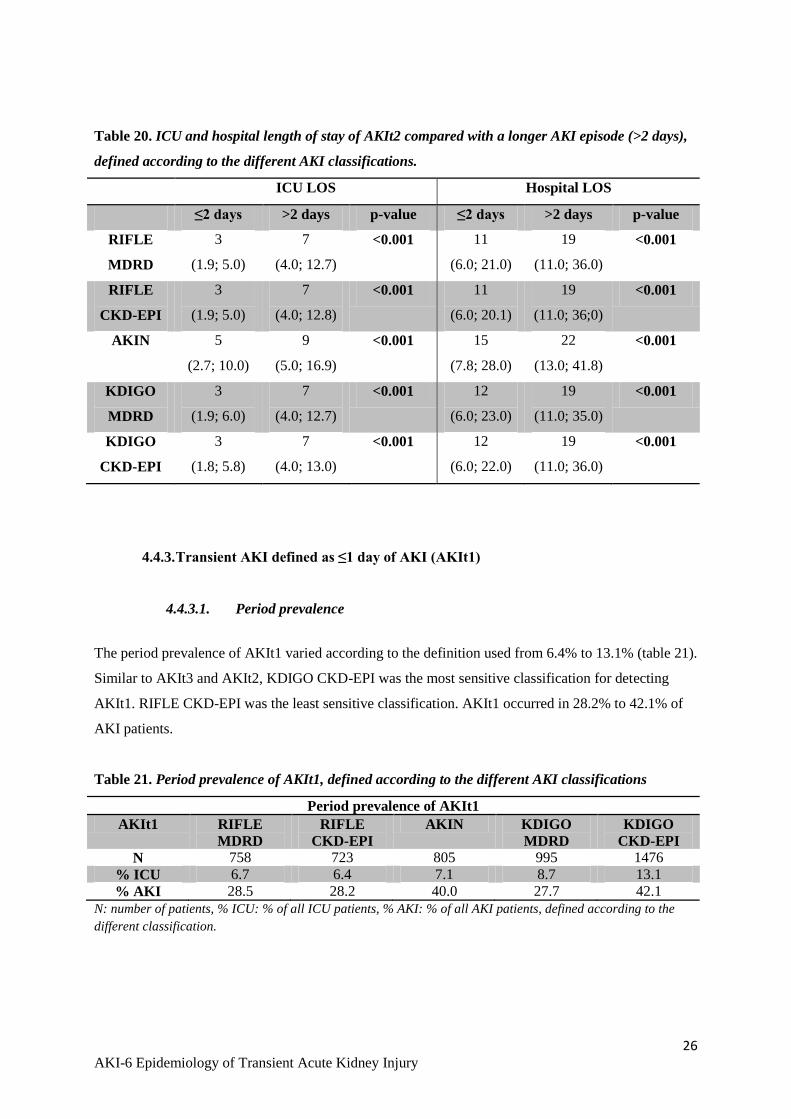
Similar to AKIt3, length of stay in the ICU, and in the hospital were longer in patients who
experienced a longer AKI episode (>2) compared to AKIt2 patients (table 20). The results were
strongly significant for all AKI classifications (p<0.001).
26 AKI-6 Epidemiology of Transient Acute Kidney Injury
Table 20. ICU and hospital length of stay of AKIt2 compared with a longer AKI episode (>2 days),
defined according to the different AKI classifications.
ICU LOS Hospital LOS
≤2 days >2 days p-value ≤2 days >2 days p-value
RIFLE
MDRD
3
(1.9; 5.0)
7
(4.0; 12.7)
<0.001 11
(6.0; 21.0)
19
(11.0; 36.0)
<0.001
RIFLE
CKD-EPI
3
(1.9; 5.0)
7
(4.0; 12.8)
<0.001 11
(6.0; 20.1)
19
(11.0; 36;0)
<0.001
AKIN 5
(2.7; 10.0)
9
(5.0; 16.9)
<0.001 15
(7.8; 28.0)
22
(13.0; 41.8)
<0.001
KDIGO
MDRD
3
(1.9; 6.0)
7
(4.0; 12.7)
<0.001 12
(6.0; 23.0)
19
(11.0; 35.0)
<0.001
KDIGO
CKD-EPI
3
(1.8; 5.8)
7
(4.0; 13.0)
<0.001 12
(6.0; 22.0)
19
(11.0; 36.0)
<0.001
4.4.3. Transient AKI defined as ≤1 day of AKI (AKIt1)
4.4.3.1. Period prevalence
The period prevalence of AKIt1 varied according to the definition used from 6.4% to 13.1% (table 21).
Similar to AKIt3 and AKIt2, KDIGO CKD-EPI was the most sensitive classification for detecting
AKIt1. RIFLE CKD-EPI was the least sensitive classification. AKIt1 occurred in 28.2% to 42.1% of
AKI patients.
Table 21. Period prevalence of AKIt1, defined according to the different AKI classifications
Period prevalence of AKIt1
AKIt1 RIFLE
MDRD
RIFLE
CKD-EPI
AKIN KDIGO
MDRD
KDIGO
CKD-EPI
N 758 723 805 995 1476
% ICU 6.7 6.4 7.1 8.7 13.1
% AKI 28.5 28.2 40.0 27.7 42.1
N: number of patients, % ICU: % of all ICU patients, % AKI: % of all AKI patients, defined according to the
different classification.
27 AKI-6 Epidemiology of Transient Acute Kidney Injury
4.4.3.2. Mortality
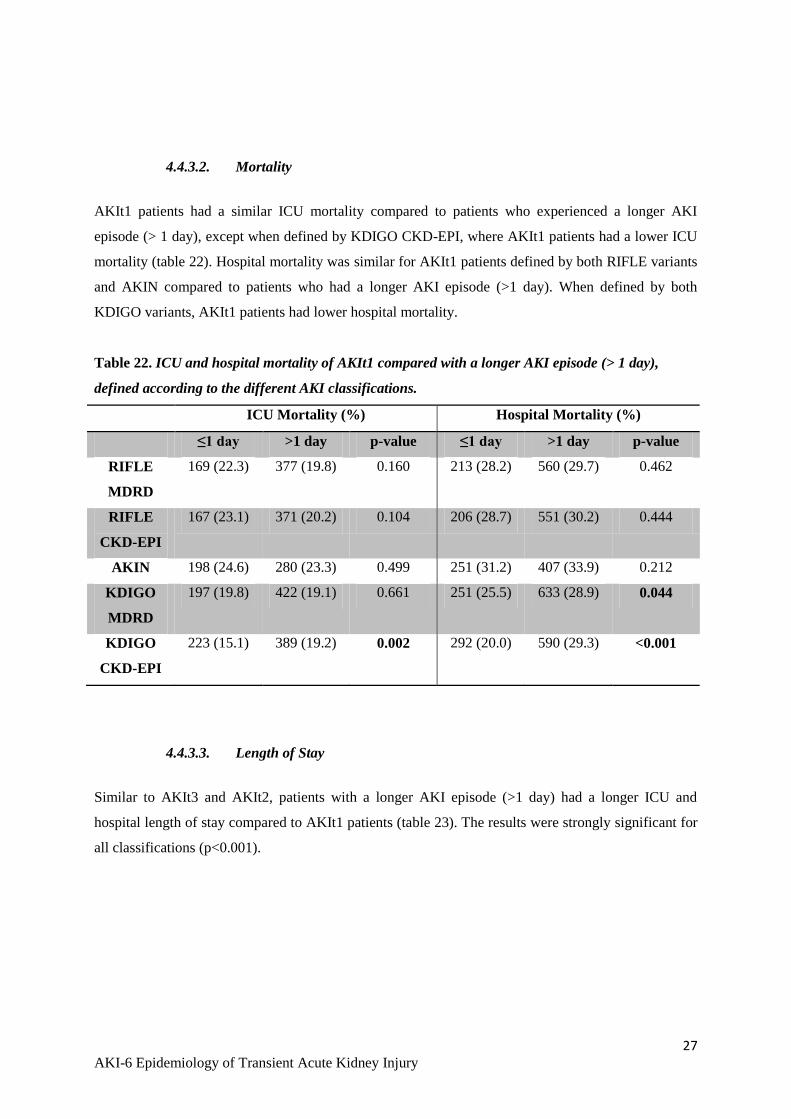
AKIt1 patients had a similar ICU mortality compared to patients who experienced a longer AKI
episode (> 1 day), except when defined by KDIGO CKD-EPI, where AKIt1 patients had a lower ICU
mortality (table 22). Hospital mortality was similar for AKIt1 patients defined by both RIFLE variants
and AKIN compared to patients who had a longer AKI episode (>1 day). When defined by both
KDIGO variants, AKIt1 patients had lower hospital mortality.
Table 22. ICU and hospital mortality of AKIt1 compared with a longer AKI episode (> 1 day),
defined according to the different AKI classifications.
ICU Mortality (%) Hospital Mortality (%)
≤1 day >1 day p-value ≤1 day >1 day p-value
RIFLE
MDRD
169 (22.3) 377 (19.8) 0.160 213 (28.2) 560 (29.7) 0.462
RIFLE
CKD-EPI
167 (23.1) 371 (20.2) 0.104 206 (28.7) 551 (30.2) 0.444
AKIN 198 (24.6) 280 (23.3) 0.499 251 (31.2) 407 (33.9) 0.212
KDIGO
MDRD
197 (19.8) 422 (19.1) 0.661 251 (25.5) 633 (28.9) 0.044
KDIGO
CKD-EPI
223 (15.1) 389 (19.2) 0.002 292 (20.0) 590 (29.3) <0.001
4.4.3.3. Length of Stay
Similar to AKIt3 and AKIt2, patients with a longer AKI episode (>1 day) had a longer ICU and
hospital length of stay compared to AKIt1 patients (table 23). The results were strongly significant for
all classifications (p<0.001).
28 AKI-6 Epidemiology of Transient Acute Kidney Injury
Table 23. ICU and hospital length of stay of AKIt1 compared with a longer AKI episode (>1 day),
defined according to the different AKI classifications.
ICU LOS Hospital LOS
≤1 day >1 day p-value ≤1 day >1 day p-value
RIFLE
MDRD
3
(1.6; 5.0)
5
(3.0; 10.0)
<0.001 10
(5.0; 20.0)
16
(9.0; 31.0)
<0.001
RIFLE
CKD-EPI
3
(1.5; 5.5)
5
(3.0; 5.0)
<0.001 10
(5.0; 20.0)
16
(9.0; 31.0)
<0.001
AKIN 4
(2.1; 9.2)
7
(4.0; 13.7)
<0.001 14
(7.1; 27.0)
19
(11.0; 35.0)
<0.001
KDIGO
MDRD
3
(1.6; 6.0)
5
(3.0; 10.0)
<0.001 12
(6.0; 22.0)
16
(9.0; 31.0)
<0.001
KDIGO
CKD-EPI
3
(1.6; 5.9)
5
(3.0; 10.6)
<0.001 11
(6.0; 22.0)
16
(9.0; 31.0)
<0.001
4.4.4. Comparison of mortality between AKIt1, AKIt2 and AKIt3
4.4.4.1. ICU Mortality
Patients with transient AKI had a higher ICU mortality compared to patients without AKI, even when
AKI only lasted for 1 day (AKIt1) (figure 1). The duration of the transient AKI had no influence on
the ICU mortality. AKIt1, AKIt2 and AKIt3 had a similar ICU Mortality in all AKI classifications,
except when defined according to AKIN.
29 AKI-6 Epidemiology of Transient Acute Kidney Injury
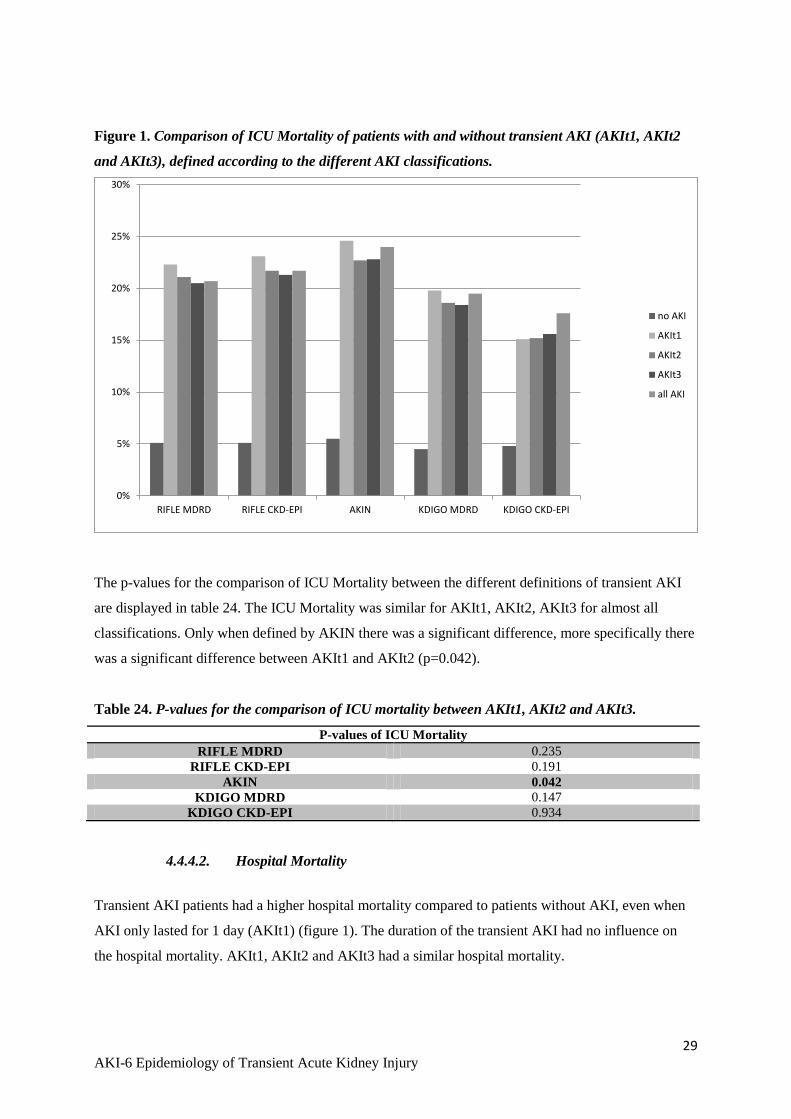
Figure 1. Comparison of ICU Mortality of patients with and without transient AKI (AKIt1, AKIt2
and AKIt3), defined according to the different AKI classifications.
The p-values for the comparison of ICU Mortality between the different definitions of transient AKI
are displayed in table 24. The ICU Mortality was similar for AKIt1, AKIt2, AKIt3 for almost all
classifications. Only when defined by AKIN there was a significant difference, more specifically there
was a significant difference between AKIt1 and AKIt2 (p=0.042).
Table 24. P-values for the comparison of ICU mortality between AKIt1, AKIt2 and AKIt3.
P-values of ICU Mortality
RIFLE MDRD 0.235
RIFLE CKD-EPI 0.191
AKIN 0.042
KDIGO MDRD 0.147
KDIGO CKD-EPI 0.934
4.4.4.2. Hospital Mortality
Transient AKI patients had a higher hospital mortality compared to patients without AKI, even when
AKI only lasted for 1 day (AKIt1) (figure 1). The duration of the transient AKI had no influence on
the hospital mortality. AKIt1, AKIt2 and AKIt3 had a similar hospital mortality.
0%
5%
10%
15%
20%
25%
30%
RIFLE MDRD RIFLE CKD-EPI AKIN KDIGO MDRD KDIGO CKD-EPI
no AKI
AKIt1
AKIt2
AKIt3
all AKI
30 AKI-6 Epidemiology of Transient Acute Kidney Injury
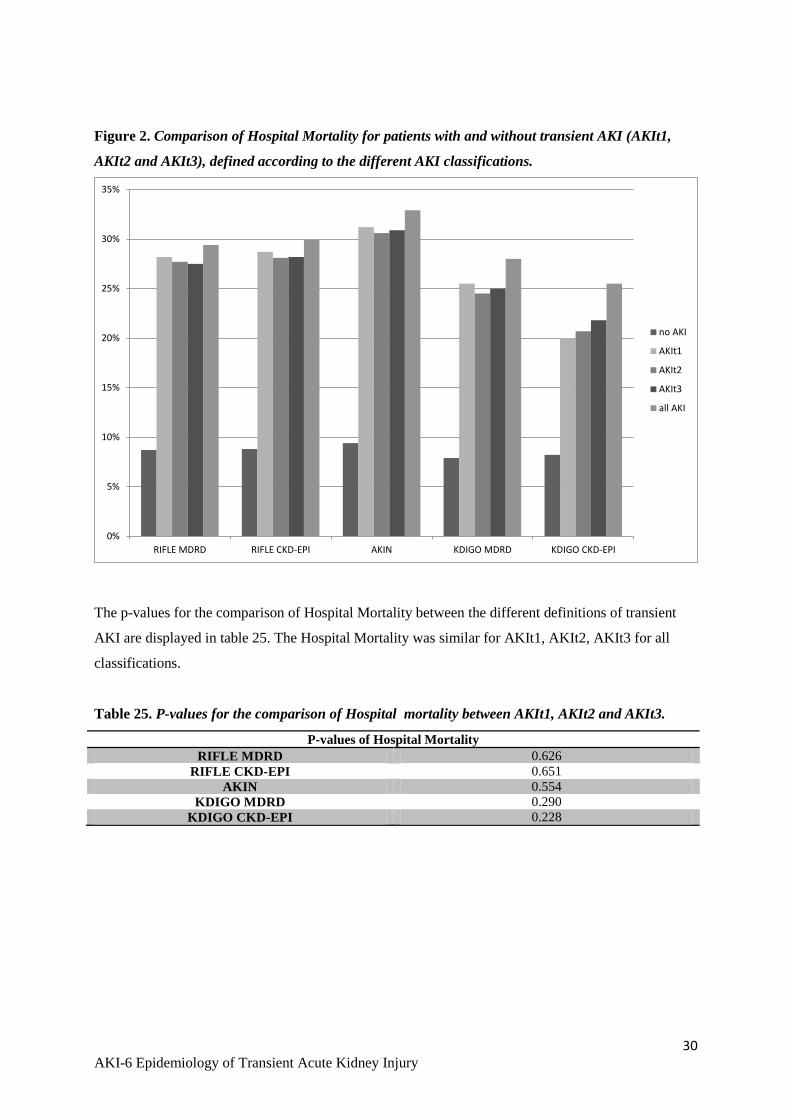
Figure 2. Comparison of Hospital Mortality for patients with and without transient AKI (AKIt1,
AKIt2 and AKIt3), defined according to the different AKI classifications.
The p-values for the comparison of Hospital Mortality between the different definitions of transient
AKI are displayed in table 25. The Hospital Mortality was similar for AKIt1, AKIt2, AKIt3 for all
classifications.
Table 25. P-values for the comparison of Hospital mortality between AKIt1, AKIt2 and AKIt3.
P-values of Hospital Mortality
RIFLE MDRD 0.626
RIFLE CKD-EPI 0.651
AKIN 0.554
KDIGO MDRD 0.290
KDIGO CKD-EPI 0.228
0%
5%
10%
15%
20%
25%
30%
35%
RIFLE MDRD RIFLE CKD-EPI AKIN KDIGO MDRD KDIGO CKD-EPI
no AKI
AKIt1
AKIt2
AKIt3
all AKI
31 AKI-6 Epidemiology of Transient Acute Kidney Injury
5. Discussion
Acute Kidney Injury (AKI) was a common finding in this large cohort of ICU patients, and the period
prevalence varied largely depending the AKI classification used. During ICU stay, 17.8 to 31.0% of
the patients had an episode of AKI. This was associated with worse clinical outcomes such as
increased length of stay and mortality.
Transient AKI was prevalent amongst ICU and AKI patients, and was also associated with a higher
mortality. ICU and hospital mortality of Transient AKI variants (1 to 3 days AKI) were comparable to
that of all AKI. Finally, a longer duration of an AKI episode was associated with a higher mortality
and a longer length of stay compared to transient AKI.
5.1. Prevalence of AKI
In our TRAK study we found an overall AKI prevalence of 17.8-31.0% depending on which
classification was used. The AKI prevalence per classification was: 23.5% for RIFLE MDRD, 22.7%
for RIFLE CKD-EPI, 17.8% for AKIN, 28.3% for KDIGO MDRD and 31.0% for KDIGO CKD-EPI.
The prevalence and incidence of AKI varied among ICU studies, depending on the study population (1,
10). In the NEiHROS-AKI study, the first prospective multicenter study of AKI, 10.8% of the 2164
ICU patients suffered from AKI (11). Thakar et al. (12) found in the Veteran Affairs Hospital ICUs
across the US an overall incidence of AKI of 22% when AKI was defiend by creatinine criteria only.
In the study by Ostermann and Chang (13) AKI occurred in 35.8% of the ICU patients. Bashaw et al.
(14) analyzed AKI by RIFLE using only creatinine values. The incidence of AKI in their ICU
population was 36.1%. Recently Mandelbnaum found an incidence of 57% when AKI was defined by
AKIN criteria (15). Finally, in a study by Hoste et al. (16) in 5,383 ICU patients of University of
Pittsburg Medical Center, AKI occurred in 67% of the patients.
Differences between these cohorts can be explained by differences in the cohort observed (different
patient characteristics or observation period) and differences in the definition for AKI used (creatinine
criteria only, or combination of creatinine and urine output criteria, variant of urine output criteria, …).
A remarkable result was that the AKI prevalence of the Pittsburg cohort in the TRAK study was only
31.0%, which was very low compared to the 67% found by Hoste et al. (16). Several reasons could be
found to explain this difference. Firstly this was a different patient cohort. The Pittsburg cohort from
the Hoste study was from 2000 to 2001, the Pittsburg cohort from the TRAK study was from 2005 to
2007. Secondly the urine output criteria were not included in the TRAK study in contrast to the Hoste
study. Thirdly there was a different method of estimating baseline creatinine. In the study by Hoste et
al. (16) the lowest creatinine value among the hospital admission creatinine, the ICU admission
32 AKI-6 Epidemiology of Transient Acute Kidney Injury
creatinine or the MDRD creatinine value was used as the baseline value. This could result in an
overestimating of the prevalence of AKI. In the TRAK study the baseline creatinine value was used
when available. When there was no baseline available, the re-expressed 4-variable MDRD or CKD-
EPI equitation were used to calculate a baseline value. This was also suggested by Zavada et al. (9).
They stated that the use of the 4-variable MDRD equitation to calculate baseline creatinine may over-
or underestimate some mild AKI cases, but does not misclassify patients in Injury and Failure.
Whenever possible, recorded creatinine values should be used as a reference of baseline. In a big
cross-sectional analysis, the CKD-EPI creatinine equitation proved to be better than the MDRD
equation, especially at higher GFR, and could replace it for routine clinical use (7). In the TRAK study
small differences were seen between the use of the re-expressed 4 variable MDRD and the CKD-EPI
equitation for calculating a baseline creatinine value. Further analyses will be needed to explore these
differences in more detail.
5.2. Outcomes
Patients with AKI had a higher ICU mortality (17.6%-24.0%) compared to the patients without AKI
(4.5%-5.5%). Similar to ICU mortality we found higher hospital mortality in AKI patients (25.5%-
32.9%) compared to patients without AKI (7.9%-9.4%). AKI patients also had a longer ICU and
hospital length of stay.
Patients in the Risk stage of RIFLE or Stage 1 of AKIN and KDIGO had a significant higher ICU and
hospital mortality and significant longer ICU and hospital length of stay compared to patients without
AKI. This again emphasizes the importance of early AKI detection, AKI treatment and AKI
prevention at ICU.
Transient AKI patients had also a higher ICU and hospital mortality compared to patients without AKI,
even when the AKI episode only lasted for 1 day. Also this result emphasizes the importance of early
AKI detection, AKI treatment and AKI prevention at ICU. There was no difference in mortality
between the different definitions of transient AKI and also not between Transient AKI and all AKI.
The reason for this remained unclear. Further research will be needed to clarify this result.
The longer the duration of AKI, the more impact we found on outcomes. Patients with AKIt3 had
similar ICU mortality, but lower hospital mortality compared to patients with a longer AKI episode
(>3 days). AKIt2 patients had similar ICU mortality compared to patients with a longer AKI episode (>
2 days). But, according to the classification used, AKIt2 patients had similar or lower hospital
mortality compared to patients who experienced a longer AKI episode (>2 days). Finally, patients with

33 AKI-6 Epidemiology of Transient Acute Kidney Injury
AKIt1 had a similar ICU and hospital mortality compared to patients with a longer AKI episode (>1
day). Transient AKI defined according to the 3 time periods (AKIt3, AKIt2 and AKIt1) was associated
with a significant shorter ICU and hospital length of stay compared to longer AKI episodes.
It was remarkable that transient AKI patients (AKIt3 and AKIt2) had similar ICU mortality, but lower
hospital mortality than patients with longer AKI episodes. A possible explanation for this may be, that
a longer period of AKI could also be associated with greater severity of AKI (more stage 2 or 3
patients), and is therefore a more important modifier of outcome. Also, longer duration of AKI may be
lead to more comorbidity and so impact on outcome. Further analyses will be needed to clarify the
cause of this remarkable result.
In almost all AKI studies the relation between morbidity and mortality was examined based on the
maximum AKI stage. Uchino et al. (5) and Coca et al.(8) demonstrated that the duration of AKI has
also an impact on hospital mortality. Uchino classified patients with an AKI episode of <72h as
transient azotemia (TA). Patients with TA had a significantly higher odds ratio for hospital mortality,
even when lasting only for 24 hours (5).
Coca prospectively studied 35,302 US diabetic veterans undergoing their first noncardiac surgery.
AKI was classified according to the AKIN classification and by duration (short (less than 2 days),
medium (3-6 days) or long (7 days or more)). 17.8% of the patient population suffered from AKI.
Both a higher stage and duration were independently associated with increased risk of long-term
mortality. Within each stage, longer duration of AKI was significantly associated with a graded higher
rate of mortality (8).
The strength of these studies is their large study population. Their major limitation is their limited
external validity. The Uchino study is a single-center study in hospitalized patients and the Coca study
only included US diabetic veterans undergoing their first noncardiac surgery, which can result in a
higher incidence of AKI in the study population.
5.3. Classifications of AKI
Comparing the five classification used in this analysis: RIFLE MDRD, RIFLE CKD-EPI, AKIN,
KDIGO MDRD and KDIGO CKD-EPI, differences could be seen in AKI prevalence, duration of the
first AKI episode, clinical outcomes, transient AKI prevalence and transient AKI outcomes.
34 AKI-6 Epidemiology of Transient Acute Kidney Injury
5.3.1. AKI and transient AKI prevalence
The KDIGO classification was the most sensitive for identifying AKI, the AKIN classification the
least sensitive. The use of CKD-EPI as a marker for baseline serum creatinine concentration in
patients where this was not available gave various results. When defined by RIFLE, AKI prevalence
decreased when using CKD-EPI, when defined by KDIGO, AKI prevalence increased. The duration of
the first AKI episode also varied according to the classification used. There was a greater proportion of
AKI patients with shorter duration of AKI (≤2 days) when classified according to AKIN.
The prevalence of transient AKI also varied among the different classifications. For the three different
definitions of transient AKI, the prevalence was the highest for KDIGO CKD-EPI. For AKIt3, the
prevalence was the lowest for AKIN. For AKIt2, the prevalence was the lowest for RIFLE MDRD.
For AKIt1, the prevalence was the lowest for RIFLE CKD-EPI.
Using CKD-EPI increased the incidence of transient AKI for the KDIGO classification and gave
various results for the RIFLE classification compared with using MDRD.
The prevalence of transient AKI within AKI patients also differed among the different classifications.
Of all AKI cases, the period prevalence of AKIt3 was 65.7 to 78.1%, of AKIt2 34.0 to 67.1% and of
AKIt12 27.7 to 42.1% according to the classifications used. So transient AKI had a very high
prevalence among AKI patients. Transient AKI also had a high prevalence in ICU patients. AKIt3
occurred in 13.9 to 22.7% of ICU patients according to the AKI classification used. AKIt2 and AKIt1
were still relatively prevalent in this large ICU cohort (AKIt2: 8.0 to 19.7%, and AKIt1: 6.4 to 13.1%
of ICU patients).
5.3.2. AKI and transient AKI outcomes
Although the AKIN and KDIGO classification are modifications of the RIFLE classification and they
only differ in minor details, large differences can be seen in clinical outcomes between the different
classifications. ICU mortality varied from 17.6% to 24.0% among the different classifications, hospital
mortality varied from 25.5% to 32.9% and also ICU and hospital length of stay differed among the
different classifications. The differences between the different AKI stages varied also according to the
classification used.
Also for transient AKI, outcomes varied among the different classifications, except for the ICU and
hospital length of stay, which was significantly shorter in transient AKI patients for all classifications.
For ICU and hospital mortality we found various results for the different classifications.

35 AKI-6 Epidemiology of Transient Acute Kidney Injury
These findings illustrate the importance of the classification used for AKI when comparing studies.
Similar to findings by Joannidis et al. (17) we found that the AKIN classification was found less
sensitive in this cohort. Also, the use of the more precise CKD-EPI equation for assessment of
baseline creatinine yielded different results compared to the recent golden standard, the MDRD
equation. Further analyses will be needed to explore the cause of this difference in AKI prevalence and
outcomes between the different AKI classifications.
5.4. Strengths and limitations
Our TRAK study had both strengths and limitations. AKI-6 was a multicenter, transatlantic database
containing 11,309 ICU patients from Belgium, Italy, US (2 centers) and Australia (2 centers). It was
also the first study that explored in such great detail duration of AKI and transient AKI. On the other
hand, the TRAK study was a retrospective study with an unequal patient distribution (Ghent, Pittsburg
and Rochester together included more than 75% of the study population). Secondly we did not
incorporate urine output data, which may result in an underestimating of the AKI prevalence. Thirdly
there was no baseline value available for 69.5% of the patients, which may result in a misclassification
and over- or underestimating of AKI prevalence. Fourthly we did not analyze the severity of transient
AKI. Further analyses will be needed to explore this is more detail.

36 AKI-6 Epidemiology of Transient Acute Kidney Injury
6. Conclusion
In this large multicentric, international cohort of ICU patients, we found that AKI occurred in one fifth
to one-third of ICU patients. Further, transient AKI accounted for two-thirds of AKI cases, and
occurred in 10 to 20% of ICU patients. AKI and transient AKI were related to an increase of ICU and
hospital mortality and a longer ICU and hospital length of stay. ICU mortality was comparable
between AKIt2 and AKIt3 patients, and patients with longer duration of AKI. Hospital mortality was
however lower. AKIt1 had similar ICU and hospital mortality compared to patients with longer AKI
duration. A longer AKI duration was associated with a longer ICU and hospital length of stay.
Different AKI classifications, i.e. the three AKI classifications, RIFLE, AKIN, KDIGO, and the use of
the re-expressed 4-variable MDRD and CKD-EPI equation, resulted in large variations. Further
research will be needed to explore these differences in more detail.
In the future, duration of AKI should be incorporated in new AKI consensus definitions and used in
clinical studies.
37 AKI-6 Epidemiology of Transient Acute Kidney Injury
7. Nederlandse samenvatting
7.1. Inleiding
Acute nierinsufficiëntie (AKI) is een veel voorkomende problematiek op Intensieve Zorgen (IZ) en is
geassocieerd met een hoger risico op sterfte. Gedurende vele jaren was er geen consensus definitie
voor acute nierinsufficiëntie, maar in de laatste 10 jaar zijn er verschillende ontwikkeld. In 2004
ontwikkelde de Acute Dialysis Quality Initiative (ADQI) groep de RIFLE classificatie (2). Studies
toonden aan dat tot twee derde van de IZ patiënten acute nierinsufficiëntie, gedefinieerd volgens de
RIFLE classificatie, ontwikkelden (1). Ondertussen werden er al twee aanpassingen van de RIFLE
classificatie gepubliceerd. In 2007 ontwikkelde het Acute Kidney Injury Network de AKIN
classificatie (3) en enkele maanden geleden werd de KDIGO classificatie ontwikkeld (4).
Recent werd transiënte acute nierinsufficiëntie door Uchino et. al (5) gedefinieerd als acute
nierinsufficiëntie die minder dan 72 uur duurde. Patiënten met transiënte acute nierinsufficiëntie
hadden een grotere odds ratio voor mortaliteit. Een andere studie van Coca et al. (8) toonde aan dat de
duur van een postoperatieve episode van acute nierinsufficiëntie geassocieerd was met een hogere
mortaliteit bij Amerikaanse veteranen met diabetes mellitus.
Het doel van deze AKI-6 Transiënte nierinsufficiëntie Studie (TRAK Studie) was om de invloed van
de duur van een episode van acute nierinsufficiëntie op mortaliteit en opnameduur te onderzoeken in
een IZ populatie. We hebben de verschillende classificaties voor acute nierinsufficiëntie en de
verschillende manieren om de basis creatinine waarde te berekenen, vergeleken.
7.2. Methodologie
De TRAK Studie is een retrospectieve, multicentrische, internationale cohort studie. De data werden
verzameld met behulp van de AKI-6 studie groep. AKI-6 is een multicentrische, trans-Atlantische
studiegroep met intensivisten van 6 verschillende centra, 2 centra in de Verenigde Staten, 2 Europese
centra en 2 Australische centra. De databank bestond uit 11,309 patiënten die opgenomen waren op IZ
in de periode 2005 tot 2007.
Tijdens het IZ verblijf werden verschillende gegevens geregistreerd: laagste serum creatinine waarde,
urine output, behandeling met mechanische ventilatie en behandeling met niervervangende therapie
(dialyse). Er werden ook verschillende outcomes geregistreerd, namelijk mortaliteit tijdens de opname
op IZ, mortaliteit tijdens de ziekenhuisopname, opnameduur op IZ en opnameduur in het ziekenhuis.
38 AKI-6 Epidemiology of Transient Acute Kidney Injury
Om de creatinine waarden van de verschillende centra te kunnen vergelijken, werden de waarden
omgezet naar de IDMS standaarden. Vier van de zes centra gebruikten de IDMS methode al in hun lab,
dus daar was geen herberekening nodig. Voor de andere twee centra gebruikten we de formules van
Zavada et al. (9).
Patiënten met acute nierinsufficiëntie werden geclassificeerd volgens de RIFLE, AKIN en KDIGO
classificaties. Door het groot aantal ontbrekende waarden voor de urine output, werden enkel de
creatinine waarden gebruikt. De creatinine waarden voor de verschillende classificaties zijn
weergegeven in tabel 1-3. De RIFLE en KDIGO classificaties gebruikten als basis creatinine waarde
een waarde die bij de patiënt gemeten werd voor de huidige IZ opname. Indien deze waarde niet
gekend was, werd de basis creatinine waarde berekend a.d.h.v. de Glomerulaire Filtratie Snelheid
(GFR). De MDRD met 4 variabelen (gecorrigeerd voor IDMS) (6) en de CKD-EPI formule (7)
werden gebruikt om de basis creatinine waarde te berekenen. Bij patiënten zonder chronische
nierinsufficiëntie zijn we uitgegaan van een GFR van 75 ml/min (1, 2).
De AKIN definitie maakte geen gebruik van een vooraf gemeten basis creatinine. Hier werd de laagste
creatinine waarde in 48u voor het optreden van de acute nierinsufficiëntie gebruikt.
Op deze manier komen we dus tot 5 definities voor acute nierinsufficiëntie die gebruikt werden in
deze studie: RIFLE MDRD, RIFLE CKD-EPI, AKIN, KDIGO MDRD en KDIGO CKD-EPI.
Transiënte acute nierinsufficiëntie werd gedefinieerd op 3 verschillende manieren:
1. Episode van acute nierinsufficiëntie van ≤ 3 dagen (AKIt3)
2. Episode van acute nierinsufficiëntie van ≤ 2 dagen (AKIt2)
3. Episode van acute nierinsufficiëntie van ≤ 1 dag (AKIt1)
Om de karakteristieken van de studie populatie te beschrijven werd er gebruik gemaakt van MS
Access 2010 en SPSS Statistics versie 19. Categorische variabelen werden weergegeven als aantallen
(percentage) en werden geanalyseerd m.b.v. de Chi-kwadraat test. Continue variabelen werden
weergegeven als de mediaan en het 25ste
en 75ste
percentiel. Continue variabelen werden getest op
normale verdeling m.b.v. distributie plots en geanalyseerd m.b.v. de Students’ T-test indien ze
normaal verdeeld waren en m.b.v. de Kruskal-Wallis test en de Mann-Whitney U test indien niet. Een
2-zijdige p-waarde van ≤0.05 werd als significant beschouwd.
39 AKI-6 Epidemiology of Transient Acute Kidney Injury
7.3. Resultaten
Van alle IZ patiënten hadden 17.8% tot 31.0% acute nierinsufficiëntie (AKI) (tabel 5). De KDIGO
classificatie was de gevoeligste classificatie om AKI te detecteren, de AKIN classificatie de minst
gevoelige. Indien we AKI definieerden volgens RIFLE gaf het gebruik van de MDRD formule de
meeste AKI episodes. Indien we AKI definieerden volgens KDIGO gaf de CKD-EPI formule de
meeste AKI episodes (tabel 5).
In de meerderheid van de AKI patiënten duurde de eerste AKI episode maar 1 of 2 dagen. Dit betekent
dat transiënte acute nierinsufficiëntie zeer veel voorkwam bij patiënten met AKI. Er was een grotere
proportie patiënten met een kortere AKI episode (≤2 dagen) indien AKI gedefinieerd werd volgens de
AKIN criteria (tabel 6).
Patiënten met acute nierinsufficiëntie hadden een hogere IZ mortaliteit (17.6%-24.0%) in vergelijking
met patiënten zonder acute nierinsufficiëntie (4.5%-5.5%). Er was een stapsgewijze toename van de
mortaliteit bij een toename van de ernst van de acute nierinsufficiëntie. De patiënten die acute
bovenop chronische nierinsufficiëntie (Fc) hadden, hadden iets andere kenmerken dan de andere
patiënten (tabel 7). De verschillen tussen de verschillende AKI stadia varieerden naargelang de
classificatie die gebruikt werd (tabel 8).
De ziekenhuismortaliteit toonde dezelfde trends als de IZ mortaliteit, met ook hier een stapsgewijze
toename van de mortaliteit bij ernstigere AKI stadia. Patiënten met acute nierinsufficiëntie hadden een
hogere ziekenhuismortaliteit (25.5%-32.9%) in vergelijking met patiënten zonder acute
nierinsufficiëntie (7.9%-9.4%) (tabel 9). De verschillen tussen de verschillende AKI stadia varieerden
ook hier naargelang de classificatie die gebruikt werd (tabel 10).
Patiënten met acute nierinsufficiëntie hadden een langer verblijf op IZ dan patiënten zonder acute
nierinsufficiëntie. Maar in tegenstelling tot bij de mortaliteit konden we hier geen stapsgewijze trend
waarnemen (tabel 11). Ook hier waren er verschillen tussen de verschillende classificaties (tabel 12).
Ook het verblijf in het ziekenhuis was langer bij patiënten met acute nierinsufficiëntie in vergelijking
met patiënten zonder acute nierinsufficiëntie en ook hier was er geen stapsgewijze trend waar te
nemen (tabel 13). De verschillen tussen de verschillende classificaties worden weergegeven in tabel 14.
Een transiënte episode van acute nierinsufficiëntie van ≤3 dagen (AKIt3) kwam voor in 13.9% tot 22.7%
van de IZ patiënten. De KDIGO CKD-EPI was de meest gevoelige classificatie voor het detecteren

40 AKI-6 Epidemiology of Transient Acute Kidney Injury
van AKIt3, AKIN de minst gevoelige classificatie. AKIt3 kwam voor bij 65.7% tot 78.1% van de
patiënten met acute nierinsufficiëntie (tabel 15).
AKIt3 patiënten hadden een gelijkaardige IZ mortaliteit in vergelijking met patiënten met een langere
AKI episode (>3 dagen) indien AKI gedefinieerd werd volgens RIFLE MDRD, RIFLE CKD-EPI en
KDIGO MDRD. Indien AKI gedefinieerd werd volgens AKIN en KDIGO CKD-EPI, hadden de
AKIt3 patiënten een significant lagere IZ mortaliteit (tabel 16). Een AKI episode van >3 dagen was
wel geassocieerd met een hogere ziekenhuismortaliteit (tabel 16) en een langer verblijf op IZ en in het
ziekenhuis (tabel 17), en dit voor alle classificaties van AKI.
Een transiënte episode van acute nierinsufficiëntie van ≤2 dagen (AKIt2) kwam voor in 8.0% tot 19.7%
van de IZ patiënten. De KDIGO CKD-EPI was de meest gevoelige classificatie voor het detecteren
van AKIt2, RIFLE MDRD de minst gevoelige classificatie. AKIt2 kwam voor bij 34.0% tot 67.1%
van de patiënten met acute nierinsufficiëntie (tabel 18).
AKIt2 patiënten hadden een gelijkaardige IZ mortaliteit in vergelijking met patiënten met langere AKI
episode (>2 dagen), behalve wanneer AKI gedefinieerd werd volgens KDIGO CKD-EPI (tabel 19).
Indien AKI gedefinieerd werd volgens AKIN en beide KDIGO varianten hadden AKIt2 patiënten een
lagere ziekenhuismortaliteit. Indien AKI gedefinieerd werd volgens beide RIFLE varianten was de
ziekenhuismortaliteit gelijkaardig bij AKIt2 patiënten met en patiënten met een langere AKI episode
(tabel 19). Een AKI episode >2 dagen was geassocieerd met een langer verblijf op IZ en in het
ziekenhuis (tabel 20).
Een transiënte episode van acute nierinsufficiëntie van ≤1 dag (AKIt1) kwam voor in 6.4% tot 13.1%
van de IZ patiënten. Net zoals bij AKIt2 en AKIt3, was KDIGO CKD-EPI de meest gevoelige
classificatie voor het detecteren van AKIt1, RIFLE CKD-EPI was de minst gevoelige classificatie.
AKIt1 kwam voor in 28.2% tot 42.1% van de AKI patiënten (tabel 21).
AKIt1 patiënten hadden een gelijkaardige IZ mortaliteit in vergelijking met patiënten met een langere
AKI episode (>1 dag), behalve wanneer AKI gedefinieerd werd volgens KDIGO CKD-EPI. Indien
AKI gedefinieerd werd volgens de beide KDIGO varianten, hadden AKIt1 patiënten een lagere
ziekenhuissterfte. Indien AKI gedefinieerd werd volgens de beide RIFLE varianten en de AKIN
classificatie, hadden AKIt1 patiënten een gelijkaardige ziekenhuissterfte in vergelijking met patiënten
met een langere AKI episode (>1 dag) (tabel 22). Een AKI episode van >1 dag was geassocieerd met
een langer verblijf op IZ en in het ziekenhuis (tabel 23).

41 AKI-6 Epidemiology of Transient Acute Kidney Injury
Patiënten met transiënte AKI hadden een hogere IZ en ziekenhuismortaliteit dan patiënten zonder
acute nierinsufficiëntie (figuur 1, 2). Er is geen verschil in mortaliteit tussen de verschillende definities
voor transiënte AKI (tabel 24, 25) en tussen transiënte AKI en de totale AKI mortaliteit (figuur 1,2).
7.4. Besluit
In deze grote multicentrische, internationale cohort studie van IZ patiënten, kwam AKI voor in één
vijfde tot één derde van de IZ patiënten. Transiënte AKI kwam voor in twee derde van de AKI
patiënten en in 10 à 20% van de IZ patiënten. AKI en transiënte AKI waren geassocieerd met een
stijging van de IZ en ziekenhuissterfte en een langere opnameduur op IZ en in het ziekenhuis. De IZ
sterfte was vergelijkbaar tussen AKIt2 en AKIt3 patiënten en patiënten met een langere duur van AKI,
maar ziekenhuissterfte was lager voor AKIt2 en AKIt3 patiënten. AKIt1 patiënten hadden een
gelijkaardige IZ en ziekenhuissterfte vergeleken met patiënten met een langere AKI episode. Een
langere AKI duur was geassocieerd met een langere opnameduur op IZ en in het ziekenhuis.
Er waren verschillen te zien tussen de drie AKI classificaties RIFLE, AKIN en KDIGO en het gebruik
van de 4-variable MDRD en CKD-EPI formule. Verder onderzoek is nodig om deze verschillende
verder uit te klaren.
In de toekomst zou de duur van AKI geïncorporeerd moeten worden in AKI definities en gebruikt
worden in klinische studies.
42 AKI-6 Epidemiology of Transient Acute Kidney Injury
8. References
1. Hoste EAJ, Schurgers M. Epidemiology of acute kidney injury: how big is the problem?
Critical care medicine. 2008;36(4 Suppl):S146-S51.
2. Bellomo R, Ronco C, Kellum J, Mehta R, Palevsky P. Acute renal failure - definition,
outcome measures, animal models, fluid therapy and information technology needs: the Second
International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Critical
care. 2004;8(4):R204-R12.
3. Mehta R, Kellum J, Shah S, Molitoris B, Ronco C, Warnock D, et al. Acute Kidney Injury
Network: report of an initiative to improve outcomes in acute kidney injury. Critical care.
2007;11(2):R31-R.
4. Kellum JA, Lameire N, Aspelin P, Barsoum RS, Burdmann EA, Goldstein SL, et al. KDIGO
Practical guideline for acute kidney injury. Kidney International Supplements. 2012;2(1):1-138.
5. Uchino S, Bellomo R, Bagshaw S, Goldsmith D. Transient azotaemia is associated with a high
risk of death in hospitalized patients. Nephrology, Dialysis, Transplantation. 2010;25(6):1833-9.
6. Levey A, Coresh J, Greene T, Marsh J, Stevens L, Kusek J, et al. Expressing the Modification
of Diet in Renal Disease Study equation for estimating glomerular filtration rate with standardized
serum creatinine values. Clinical Chemistry. 2007;53(4):766-72.
7. Levey A, Stevens L, Schmid C, Zhang Y, Castro A, Feldman H, et al. A new equation to
estimate glomerular filtration rate. Annals of Internal Medicine. 2009;150(9):604-12.
8. Coca S, King J, Rosenthal R, Perkal M, Parikh C. The duration of postoperative acute kidney
injury is an additional parameter predicting long-term survival in diabetic veterans. Kidney
international. 2010;78(9):926-33.
9. Zvada J, Hoste E, Cartin Ceba R, Calzavacca P, Gajic O, Clermont G, et al. A comparison of
three methods to estimate baseline creatinine for RIFLE classification. Nephrology, Dialysis,
Transplantation. 2010;25(12):3911-8.
10. Srisawat N, Kellum JA. Acute kidney injury: definition, epidemiology, and outcome. Current
Opinion in Critical Care. 2011;17:548-55.
11. Cruz D, Bolgan I, Perazella MA, Bonello M, de Cal M, Corradi V, et al. North East Italian
Prospective Hospital Renal Outcome Survey on Acute Kidney Injury (NEiPHROS-AKI): Targeting
the Problem with the RIFLE Criteria. Clinical journal of the American Society of Nephrology
2007;2(3):418-25.
12. Thakar CV, Christianson A, Freyberg R, Almenoff P, Render ML. Incidence and outcomes of
acute kidney injury in intensive care units: A Veterans Administration study. Critical care medicine
2009;37(9):2552 -8
43 AKI-6 Epidemiology of Transient Acute Kidney Injury
13. Ostermann M, Chang RWS. Acute kidney injury in the intensive care unit according to RIFLE.
Critical Care Medicine. 2007;35(8):1837-43.
14. Bagshaw SM, George C, Bellomo R. A comparison of the RIFLE and AKIN criteria for acute
kidney injury in critically ill patients. Nephrology, Dialysis, Transplantation. 2008;23(5):1569-74.
15. Mandelbaum T, Scott DJ, Lee J, Mark RG, Malhotra A, Waikar SS, et al. Outcome of
critically ill patients with acute kidney injury using the Acute Kidney Injury Network criteria. Critical
Care Medicine. 2011;39(12):000-.
16. Hoste EA, Clermont G, Kersten A, Venkataraman R, Angus DC, De Bacquer D, et al. RIFLE
criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort
analysis. Critical Care. 2006;10(3):R73-R.
17. Joannidis M, Metnitz B, Bauer P, Schusterschitz N, Moreno R, Druml W, et al. Acute kidney
injury in critically ill patients classified by AKIN versus RIFLE using the SAPS 3 database. Intensive
care medicine. 2009;35(10):1692-702.
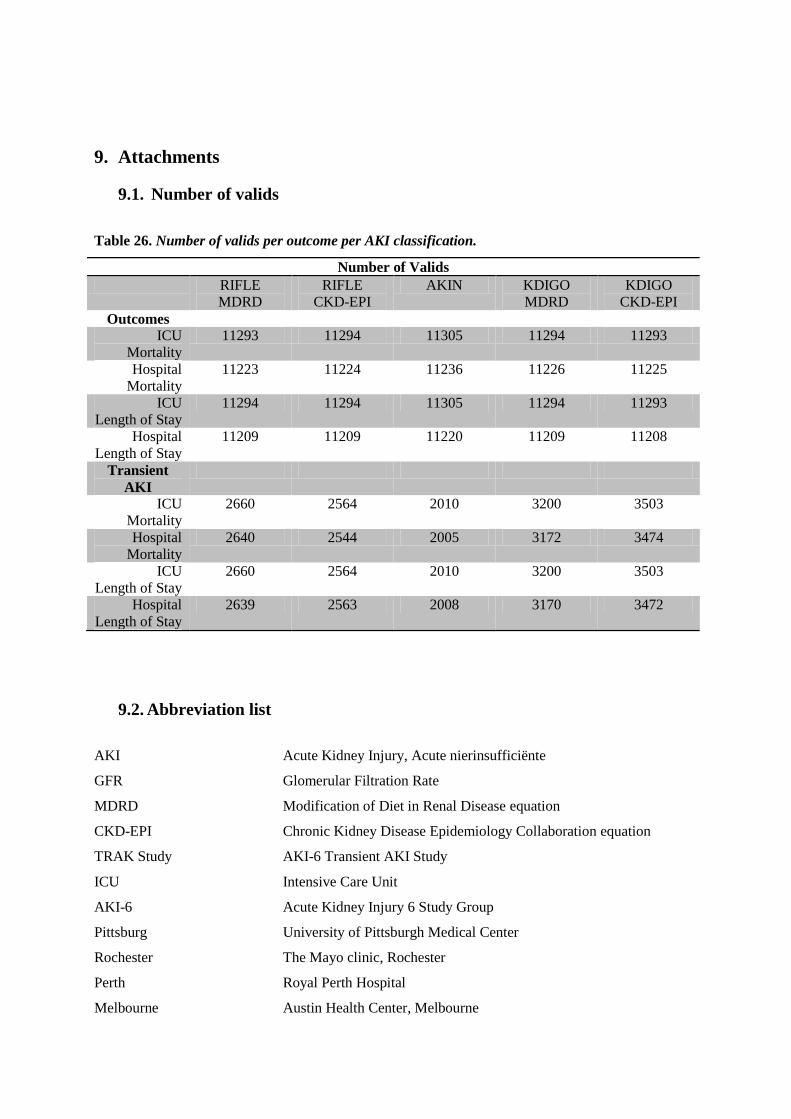
9. Attachments
9.1. Number of valids
Table 26. Number of valids per outcome per AKI classification.
Number of Valids
RIFLE
MDRD
RIFLE
CKD-EPI
AKIN KDIGO
MDRD
KDIGO
CKD-EPI
Outcomes
ICU
Mortality
11293 11294 11305 11294 11293
Hospital
Mortality
11223 11224 11236 11226 11225
ICU
Length of Stay
11294 11294 11305 11294 11293
Hospital
Length of Stay
11209 11209 11220 11209 11208
Transient
AKI
ICU
Mortality
2660 2564 2010 3200 3503
Hospital
Mortality
2640 2544 2005 3172 3474
ICU
Length of Stay
2660 2564 2010 3200 3503
Hospital
Length of Stay
2639 2563 2008 3170 3472
9.2. Abbreviation list
AKI Acute Kidney Injury, Acute nierinsufficiënte
GFR Glomerular Filtration Rate
MDRD Modification of Diet in Renal Disease equation
CKD-EPI Chronic Kidney Disease Epidemiology Collaboration equation
TRAK Study AKI-6 Transient AKI Study
ICU Intensive Care Unit
AKI-6 Acute Kidney Injury 6 Study Group
Pittsburg University of Pittsburgh Medical Center
Rochester The Mayo clinic, Rochester
Perth Royal Perth Hospital
Melbourne Austin Health Center, Melbourne
Ghent Ghent University Hospital
Vicenza Ospedale San Bortolo di Vicenza
IDMS Isotope Dilution Mass Spectrometry reference measurement procedure
SCr Serum creatinine concentration
RIFLE RIFLE classifcation for AKI
AKIN Acute Kidney Injury Network diagnostic and classification system for
AKI
KDIGO The Kidney Disease Improving Global Outcomes definition and
staging system for AKI
AKIt3 AKI episode of ≤ 3 days
AKIt2 AKI episode of ≤ 2 days
AKIt1 AKI episode of ≤ 1 days
ICU Mortality Intensive Care Unit Mortality
ICU Length of Stay Intensive Care Unit Length of Stay
R/1 Risk in RIFLE classification / Stage 1in AKIN and KDIGO
classification
I/2 Injury in RIFLE classification /Stage 2 in AKIN and KDIGO
classification
F/3 Failure in RIFLE classification / Stage 3 in AKIN and KDIGO
classification
Fc Acute on chronic AKI

Related Documents