AJR:194, April 2010 993 The nodularity associated with cirrhosis is typically relatively fine and diffuse rather than coarse and lobulated [2]. However, non- cirrhotic causes of fine, diffuse nodularity are occasionally encountered and include pseudo- cirrhosis of treated breast cancer metastases to the liver, fulminant hepatic failure, miliary metastases, and sarcoidosis [3–6]. Pseudocirrhosis of Treated Breast Cancer Metastas es to the Liver A variety of hepatic contour changes can oc- cur in breast cancer patients with metastases to the liver after chemotherapy including fine, dif- fuse nodularity that resembles cirrhosis (Fig. 1), which is commonly referred to as “pseudo- cirrhosis” [3]. Multifocal retraction of the liv- er capsule and enlargement of the caudate lobe also can be seen in this setting. The his- topathologic or pathophysiologic basis of these changes is not well understood, and the prefix “pseudo-” may be a misnomer because these patients can develop features of portal hyper- tension such as portosystemic venous collater- als and bland ascites (Figs. 1 and 2). Why this phenomenon seems almost specific for breast cancer (Fig. 3) remains unclear, with only spo- radic reports of these changes in other primary malignancies with liver metastases [7]. Fulminant Hepatic Failure Fulminant hepatic failure constitutes acute severe impairment of hepatic function in the ab- sence of preexisting liver disease and receives higher priority for hepatic transplantation than Radiologic Mimics of Cirrhosis Priyanka Jha 1 Liina Poder Zhen J. Wang Antonio C. Westphalen Benjamin M. Yeh Fergus V. Coakley Jha P , Poder L, Wang ZJ, Westphalen AC, Yeh BM, Coakley FV 1 All authors: Department of Radiology, University of California, San Francisco, 505 Parnassus Ave., Box 062 8, M-372, San Francisco, CA 94143-0628 . Address correspondence to F. V. Coakley (Fergus.Coakley@ radiology.ucsf.edu). CME This article is available for CME credit. See www.arrs.org for more information. Gastrointestinal Imaging • Pictorial Essay AJR 2010; 1 94:993–9 99 0361–803X/10/1944–993 © American Roentgen Ray Society C T of patients with established cir- rhosis show s diff use surface nod- ularity of the liver and also may show decreased liver volume with relative hypertrophy of the left and caudate lobes or signs of portal hypertension. When seen at imaging, diffuse hepatic surface nodu- larity or signs of portal hypertension (i.e., splenomegaly, ascites, or portosystemic va- rices) are usually due to cirrhosis, but other conditions can also cause these findings. Knowledge of radiologic mimics of cirrhosis is increasingly important because some have been described only recently and because an erroneous diagnosis of cirrhosis in some set- tings could adversely impact contemporary treatment options. For example, underlying cirrhosis lowers the transplantation status of patients with acute hepatic failure. This article aims to provide a practical and current review of the condition s other than cir rhosis that can result in diffuse hepatic surface nodularity or signs of portal hypertension . Noncirrhotic Causes of Diffuse Hepatic Surface Nodularity General Comments Diffuse irregularity of the hepatic contour may be fine or coarse (Appendix 1). Causes of coarse lobulation include chronic Budd- Chiari syndrome, chronic portal vein throm- bosis, and pseudomyxoma peritonei [1]. The hepatic contour changes due to these condi- tions usually are easily distinguishable from cirrhosis because of characteristic features. Keywords: cirrhosis, liver, liver disease, pseudocirrhosis DOI:10.2214/AJR.09.3409 Received July 30, 200 9; accepted after revision September 1 5, 2009 . Z. J. Wang was supported by an NIBIB training grant (1 T32 EB001631). OBJECTIVE. The objective of this article is to provide a practical review of the condi- tions other than cirrhosis that can result in diffuse surface nodularity of the liver or portal hypertension. CONCLUSION. Conditions that can mimic cirrhosis on imaging include pseudocirrho- sis of treated breast cancer metastases to the liver, fulminant hepatic failure, miliary metasta- ses, sarcoidosis, schistosomiasis, congenital hepatic fibrosis, idiopathic portal hypertension, early primary biliary cirrhosis, chronic Budd-Chiari syndrome, chronic portal vein thrombo- sis, and nodular regenerative hyperplasia. Jha et al. Radiologic Mimics of Cirrhosis Gastrointestinal Imaging Pictorial Essay D o w n l o a d e d f r o m w w w . a j r o n l i n e . o r g b y 3 6 . 8 0 . 1 1 4 . 7 o n 0 7 / 0 5 / 1 5 f r o m I P a d d r e s s 3 6 . 8 0 . 1 1 4 . 7 . C o p y r i g h t A R R S . F o r p e r s o n a l u s e o n l y ; a l l r i g h t s r e s e r v e d

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
7/18/2019 AJR JURNAL RADIOLOGI
http://slidepdf.com/reader/full/ajr-jurnal-radiologi 1/7
AJR:194, April 2010 993
The nodularity associated with cirrhosis is
typically relatively fine and diffuse rather
than coarse and lobulated [2]. However, non-
cirrhotic causes of fine, diffuse nodularity are
occasionally encountered and include pseudo-
cirrhosis of treated breast cancer metastases
to the liver, fulminant hepatic failure, miliary
metastases, and sarcoidosis [3–6].
Pseudocirrhosis of Treated Breast Cancer
Metastases to the Liver
A variety of hepatic contour changes can oc-
cur in breast cancer patients with metastases to
the liver after chemotherapy including fine, dif-
fuse nodularity that resembles cirrhosis (Fig.
1), which is commonly referred to as “pseudo-
cirrhosis” [3]. Multifocal retraction of the liv-
er capsule and enlargement of the caudate
lobe also can be seen in this setting. The his-
topathologic or pathophysiologic basis of these
changes is not well understood, and the prefix
“pseudo-” may be a misnomer because these
patients can develop features of portal hyper-
tension such as portosystemic venous collater-
als and bland ascites (Figs. 1 and 2). Why thisphenomenon seems almost specific for breast
cancer (Fig. 3) remains unclear, with only spo-
radic reports of these changes in other primary
malignancies with liver metastases [7].
Fulminant Hepatic Failure
Fulminant hepatic failure constitutes acute
severe impairment of hepatic function in the ab-
sence of preexisting liver disease and receives
higher priority for hepatic transplantation than
Radiologic Mimics of Cirrhosis
Priyanka Jha1
Liina Poder
Zhen J. Wang
Antonio C. Westphalen
Benjamin M. Yeh
Fergus V. Coakley
Jha P, Poder L, Wang ZJ, Westphalen AC, Yeh BM,Coakley FV
1All authors: Department of Radiology, University of
California, San Francisco, 505 Parnassus Ave., Box 062 8,
M-372, San Francisco, CA 94143-0628 . Addresscorrespondence to F. V. Coakley (Fergus.Coakley@
radiology.ucsf.edu).
CME
This article is available for CME credit.
See www.arrs.org for more information.
Gastrointest inal Imaging • Pictorial Essay
AJR 2010; 194:993–9 99
0361–803X/10/1944–993
© American Roentgen Ray Society
CT of patients with established cir-
rhosis shows diffuse surface nod-
ularity of the liver and also may
show decreased liver volume with
relative hypertrophy of the left and caudate
lobes or signs of portal hypertension. When
seen at imaging, diffuse hepatic surface nodu-
larity or signs of portal hypertension (i.e.,
splenomegaly, ascites, or portosystemic va-
rices) are usually due to cirrhosis, but other
conditions can also cause these findings.
Knowledge of radiologic mimics of cirrhosis
is increasingly important because some have
been described only recently and because an
erroneous diagnosis of cirrhosis in some set-
tings could adversely impact contemporary
treatment options. For example, underlying
cirrhosis lowers the transplantation status of
patients with acute hepatic failure. This article
aims to provide a practical and current review
of the conditions other than cirrhosis that can
result in diffuse hepatic surface nodularity or
signs of portal hypertension.
Noncirrhotic Causes of DiffuseHepatic Surface Nodularity
General Comments
Diffuse irregularity of the hepatic contour
may be fine or coarse (Appendix 1). Causes
of coarse lobulation include chronic Budd-
Chiari syndrome, chronic portal vein throm-
bosis, and pseudomyxoma peritonei [1]. The
hepatic contour changes due to these condi-
tions usually are easily distinguishable from
cirrhosis because of characteristic features.
Keywords: cirrhosis, liver, liver disease, pseudocirrhosis
DOI:10.2214/AJR.09.3409
Received July 30, 200 9; accepted after revision
September 15, 2009 .
Z. J. Wang was supported by an NIBIB training grant
(1 T32 EB001631).
OBJECTIVE. The objective of this article is to provide a practical review of the condi-
tions other than cirrhosis that can result in diffuse surface nodularity of the liver or portal
hypertension.
CONCLUSION. Conditions that can mimic cirrhosis on imaging include pseudocirrho-
sis of treated breast cancer metastases to the liver, fulminant hepatic failure, miliary metasta-
ses, sarcoidosis, schistosomiasis, congenital hepatic fibrosis, idiopathic portal hypertension,
early primary biliary cirrhosis, chronic Budd-Chiari syndrome, chronic portal vein thrombo-sis, and nodular regenerative hyperplasia.
Jha et al.Radiologic Mimics of Cirrhosis
Gastrointestinal ImagingPictorial Essay

7/18/2019 AJR JURNAL RADIOLOGI
http://slidepdf.com/reader/full/ajr-jurnal-radiologi 2/7
994 AJR:194, April 2010
Jha et al.
hepatic failure developing in the setting of cir-
rhosis. The distinction of acute from acute-on-
chronic hepatic failure may be clinically diffi-
cult and hepatic surface nodularity might be
considered indicative of underlying cirrhosis,
adversely impacting transplantation status. Re-
cently, fulminant hepatic failure alone was
shown to result in diffuse surface nodularity be-cause of a combination of alternating foci of
confluent regenerative nodules and necrosis
rather than cirrhosis [8] (Figs. 4 and 5).
Miliary Metastases
Diffuse surface nodularity due to miliary
metastases is rare (Figs. 6 and 7) and is un-
likely to mimic cirrhosis. In a large ultra-
sound study [4] of hepatic metastases (n =
225), surface irregularity was observed in 16
patients (7%); in only two patients, one with
squamous cell carcinoma of the tonsil and one
with ovarian carcinoma, was surface nodular-
ity the only sign of metastatic disease [4].
Sarcoidosis
Sarcoidosis of the liver is common patho-
logically but is rarely visible at imaging be-
cause the noncaseating granulomas are usu-
ally microscopic. Occasionally, hepatic
sarcoidosis can be visible as diffuse granular
heterogeneity with or without fine nodularity
of the hepatic surface [5] (Figs. 8 and 9).
Noncirrhotic Causes of Portal
Hypertension
General CommentsNoncirrhotic causes of portal hyperten-
sion (Appendix 2) include chronic Budd-
Chiari syndrome, chronic portal vein throm-
bosis, sarcoidosis, schistosomiasis, nodular
regenerative hyperplasia, congenital hepatic
fibrosis, idiopathic portal hypertension, and
early primary biliary cirrhosis [9].
Nodular Regenerative Hyperplasia
Nodular regenerative hyperplasia is a rare
but increasingly recognized condition char-
acterized by widespread transformation of
normal liver parenchyma into hyperplastic
regenerative nodules that vary in size frommicroscopic to large and masslike [10]; the
absence of fibrosis distinguishes nodular re-
generative hyperplasia from cirrhosis. From
a radiologic perspective, there appear to be
two forms of the condition: a diffuse form in
which the nodules are small and a widespread
and a focal form in which the nodules are few
in number, are scattered throughout the liver,
and measure up to a few centimeters.
The pathogenesis of diffuse nodular regen-
erative hyperplasia is unknown, but there are
well-recognized associations (Appendix 3)
with systemic cardiovascular, myeloprolifer-
ative, and autoimmune diseases, particularly
systemic lupus erythematosus; the administra-
tion of certain drugs including chemotherapy;
solid organ and bone marrow transplantation;and HIV infection [10]. Focal nodular regener-
ative hyperplasia has been primarily reported
in long-standing Budd-Chiari syndrome, al-
though similar masses have also been report-
ed in autoimmune hepatitis [11, 12]. Diffuse
nodular regenerative hyperplasia frequent-
ly results in noncirrhotic portal hypertension
[10], and affected patients may present with
variceal bleeding or hypersplenism.
Imaging findings in patients with nodular
hyperplasia can be subtle across all techniques,
although parenchymal findings may be more
obvious on ultrasound than on CT or MRI [13].
At ultrasound, widespread nodularity sugges-
tive of cirrhosis or multiple masses may be
seen (Fig. 10). At CT, the nodules may be hy-
podense with little enhancement. At MRI, dif-
fuse nodular regenerative hyperplasia is usual-
ly of similar signal intensity to the liver on T1,
T2, and gadolinium-enhanced sequences. Sur-
face nodularity and features of portal hyper-
tension may be seen across all techniques (Fig.
11). In focal nodular regenerative hyperplasia,
CT or MRI typically shows multiple hypervas-
cular masses in a patient with long-standing
Budd-Chiari syndrome or autoimmune hepa-
titis. These masses may suggest metastases orhepatocellular carcinoma, although stability on
follow-up studies or biopsy should help in mak-
ing the correct diagnosis.
Early Primary Biliary Cirrhosis
Investigators recently found that portal
hypertension can develop early in prima-
ry biliary cirrhosis—even before the onset
of cirrhosis [14]—possibly resulting from
compression of the portal venous branch-
es by granulomatous inflammation causing
presinusoidal fibrosis and portal hyperten-
sion [14]. This condition has been described
as the portal hypertensive variant of primarybiliary cirrhosis and appears to carry a high-
er risk of hepatocellular carcinoma than the
other variants of primary biliary cirrhosis.
Congenital Hepatic Fibrosis
Hepatic involvement in this multisys-
tem autosomal recessive disorder consists
of widespread periportal fibrosis leading to
portal hypertension [15]. Portal vein throm-
bosis is common, and segmental biliary dila-
tation may also be observed (Fig. 12).
Idiopathic Portal Hypertension
Idiopathic portal hypertension is character-
ized by long-standing presinusoidal portal hy-
pertension of unknown cause in adults and may
reflect damage to the intrahepatic small portalveins or portal tracts by an immunologic dis-
turbance, thromboembolism, or an infection.
Imaging findings (Fig. 13) include subcapsular
parenchymal atrophy, portal and parenchymal
fibrosis, and portal venous thrombosis. Inter-
estingly, cirrhosis does not develop even in the
advanced stages of the disease [16].
Conclusion
Diffuse surface nodularity of the liver or
signs of portal hypertension usually reflect un-
derlying cirrhosis, but noncirrhotic causes of
these imaging findings include pseudocirrhosis
of treated breast cancer metastases to the liver,
fulminant hepatic failure, miliary metastases,
sarcoidosis, schistosomiasis, congenital hepat-
ic fibrosis, idiopathic portal hypertension, early
primary biliary cirrhosis, chronic Budd-Chiari
syndrome, chronic portal vein thrombosis, and
nodular regenerative hyperplasia.
Pseudocirrhosis of treated breast cancer me-
tastases can be easily identified by reviewing
the patient’s medical history and prior imaging
examinations. Pseudocirrhosis of fulminant
hepatic failure should be considered in previ-
ously healthy patients with acute liver decom-
pensation. Miliary metastases should be con-sidered when fine hepatic surface nodularity is
seen in a patient with a known primary malig-
nancy and no signs of portal hypertension. A
raised serum angiotensin-converting enzyme
level or mediastinal adenopathy suggests sar-
coidosis. Congenital hepatic fibrosis should be
considered in children with findings of portal
hypertension, particularly if there are cysts in
the kidneys. A smooth liver of normal size with
features of portal hypertension should raise sus-
picion for idiopathic portal hypertension, but
biopsy may be required because this diagno-
sis is one of exclusion. Diffuse nodular regen-
erative hyperplasia should be considered whenmultiple small masses are seen in the liver of a
patient with known risk factors, particularly if
the clinical picture does not favor malignancy
and if the lesions are more prominent at ultra-
sound than on other techniques. Focal nodular
regenerative hyperplasia should be considered
when multiple hypervascular hepatic masses
are seen in a patient with long-standing Budd-
Chiari syndrome or autoimmune hepatitis.

7/18/2019 AJR JURNAL RADIOLOGI
http://slidepdf.com/reader/full/ajr-jurnal-radiologi 3/7
AJR:194, April 2010 995
Radiologic Mimics of Cirrhosis
Although these distinguishing features may
be helpful, histologic correlation will be required
to diagnose some cases. Careful radiologic anal-
ysis and clinical correlation may be required to
prevent an erroneous diagnosis that could po-
tentially adversely impact management.
References 1. Lipson JA, Qayyum A, Avrin DE, Westphalen A,
Yeh BM, Coakley FV. CT and MRI of hepatic
contour abnormalities. AJR 2005; 184:75–81 [Er-
ratum in AJR 2005; 184:1028]
2. Keedy A, Westphalen AC, Qayyum A, et al. Diag-
nosis of cirrhosis by spiral computed tomography:
a case-control study with feature analysis and as-
sessment of interobserver agreement. J Comput
Assist Tomogr 2008; 32:198–203
3. Qayyum A, Lee GK, Yeh BM, Allen JN, Venook
AP, Coakley FV. Frequency of hepatic contour
abnormalities and signs of portal hypertension at
CT in patients receiving chemotherapy for breast
cancer metastatic to the liver. Clin Imaging 2007;
31:6–10
4. Di Lelio A, Cestari C, Lomazzi A, Beretta L. Cir-
rhosis: diagnosis with sonographic study of the
liver surface. Radiology 1989; 172:389–392
5. Scott GC, Berman JM, Higgins JL Jr. CT patterns
of nodular hepatic and splenic sarcoidosis: a re-
view of the literature. J Comput Assist Tomogr
1997; 21:369–372
6. Brancatelli G, Federle MP, Ambrosini R, et al.
Cirrhosis: CT and MR imaging evaluation. Eur J
Radiol 2007; 61:57–69
7. Kang SP, Taddei T, McLennan B, Lacy J. Pseudocir-
rhosis in a pancreatic cancer pat ient with liver metas-
tases: a case report of complete resolution of pseudo-
cirrhosis with an early recognition and management.
World J Gastroenterol 2008; 14:1622–1624
8. Poff JA, Coakley FV, Qayyum A, et al. Frequency
and histopathologic basis of hepatic surface nodu-
larity in patients with fulminant hepatic failure.
Radiology 2008; 249:518–523
9. Kumar V, Abbas AK, Fausto N, Robbins SL,
Cotran RS, eds. Robbins and Cotran pathologic
basis of disease, 7th ed. Philadelphia, PA: Elsevi-
er Saunders, 2005
10. Dachman AH, Ros PR, Goodman ZD, Olmsted
WW, Ishak KG. Nodular regenerative hyperplasia
of the liver: clinical and radiologic observations.
AJR 1987; 148:717–722
11. Qayyum A, Graser A, Westphalen A, et al. CT of
benign hypervascular liver nodules in autoim-
mune hepatitis. AJR 2004; 183:1573–1576
12. Rha SE, Lee MG, Lee YS, et al. Nodular regen-
erative hyperplasia of the liver in Budd-Chiari
syndrome: CT and MR features. Abdom Imaging
2000; 25:255–258
13. Casillas C, Mar ti-Bonmati L, Galant J. Pseudotu-
moral presentation of nodular regenerative hyper-
plasia of the liver: imaging in five patients includ-
ing MR imaging. Eur Radiol 1997; 7:654–658
14. Murata Y, Abe M, Furukawa S, et al. Clinical fea-
tures of symptomatic primary biliary cirrhosis
initially complicated with esophageal varices. J
Gastroenterol 2006; 41:1220–1226
15. Akhan O, Karaosmanoglu AD, Ergen B. Imaging
findings in congenital hepatic fibrosis. Eur J Ra-
diol 2007; 61:18–24
16. Nakanuma Y, Tsuneyama K, Ohbu M, Katayanagi
K. Pathology and pathogenesis of idiopathic por-
tal hypertension with an emphasis on the liver.
Pathol Res Pract 2001; 197:65–76
APPENDIX 1: Noncirrhotic Causes of Diffuse Hepatic Contour Irregularity
Coarse lobulation
Chronic Budd-Chiari syndrome
Chronic portal vein thrombosis
Pseudomyxoma peritonei
Fine nodularity
Pseudocirrhosis of treated breast cancer metastases to the liver
Fulminant hepatic failure
Miliary metastases
Sarcoidosis
APPENDIX 2: Noncirrhotic Causes of Portal Hypertension
1. Chronic Budd-Chiari syndrome
2. Chronic portal vein thrombosis
3. Sarcoidosis
4. Schistosomiasis
5. Nodular regenerative hyperplasia
6. Congenital hepatic fibrosis
7. Idiopathic portal hypertension
8. Early primary biliary cirrhosis
APPENDIX 3: Associations of Diffuse and Focal Forms of Nodular Regenerative Hyperplasia
Diffuse formCardiovascular diseases
Myeloproliferative diseases
Autoimmune diseases, particularly systemic lupus erythematosus
Certain drugs including chemotherapy
Solid organ and bone marrow transplantation
HIV infection
Focal form
Chronic Budd-Chiari syndrome
Autoimmune hepatitis
7/18/2019 AJR JURNAL RADIOLOGI
http://slidepdf.com/reader/full/ajr-jurnal-radiologi 4/7
996 AJR:194, April 2010
Jha et al.
A
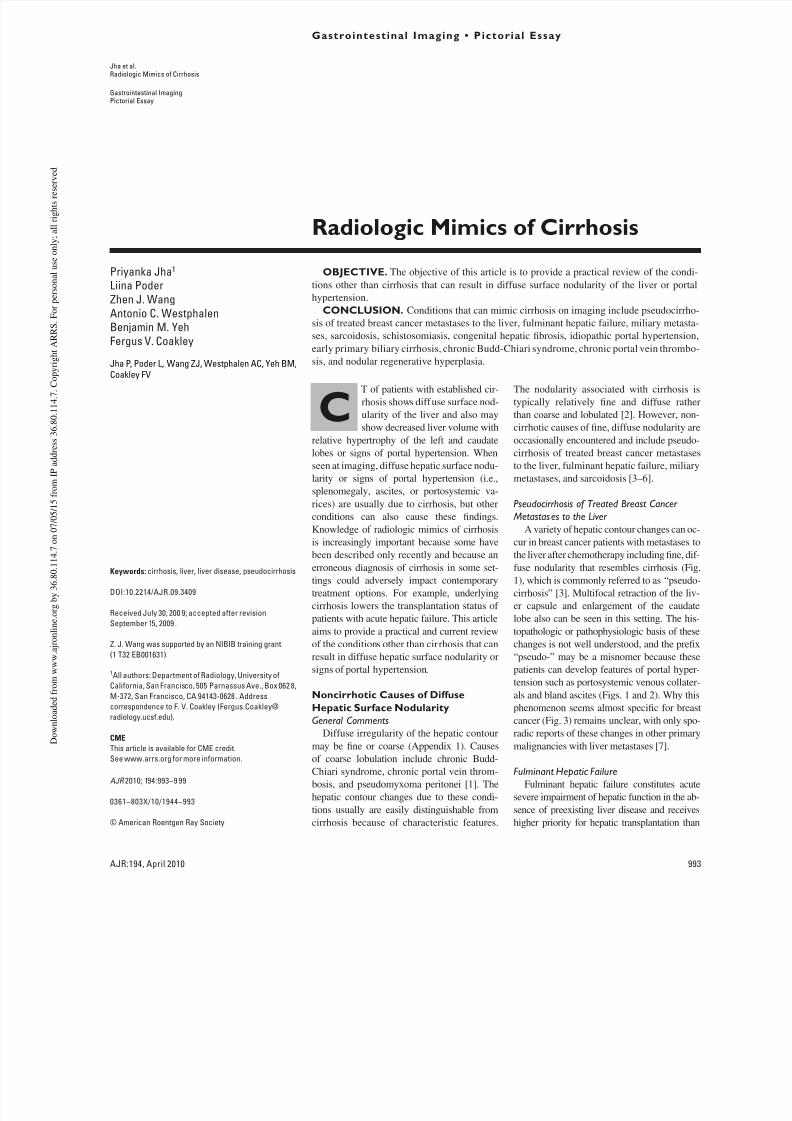
Fig. 1—62-year-old woman with breast cancer treated with chemotherapy.A, Axial contrast-enhanced CT image obtained after patient had received chemotherapy treatment shows diffuse surface nodularity in liver and recanalized umbilicalvein (arrow ); these findings are suggestive of cirrhosis.B, Axial contrast-enhanced CT image obtained 6 months before A, which was before patient started chemotherapy, shows multiple hepatic metastases. Liver isotherwise normal. Setting of breast cancer metastases treated with chemotherapy indicates rapid development of diffuse changes seen in A likely representspseudocirrhosis of treated breast cancer.
B
A
Fig. 2—59-year-old woman with multiple hypodense biopsy-proven hepatic metastases from invasive ductal carcinoma of breast.A, Axial contrast-enhanced CT image obtained before patient started chemotherapy.B, Axial contrast-enhanced CT image obtained 6 months after A—that is, after patient had started chemotherapy—shows diffuse hepatic nodularity, bland ascites(asterisk ), esophageal varices (arrow ), and partial regression of hepatic metastases. Findings are of pseudocirrhosis of treated breast cancer metastases; however,without prior studies and clinical history, these findings could suggest diagnosis of cirrhosis.
B
7/18/2019 AJR JURNAL RADIOLOGI
http://slidepdf.com/reader/full/ajr-jurnal-radiologi 5/7
AJR:194, April 2010 997
Radiologic Mimics of Cirrhosis
A
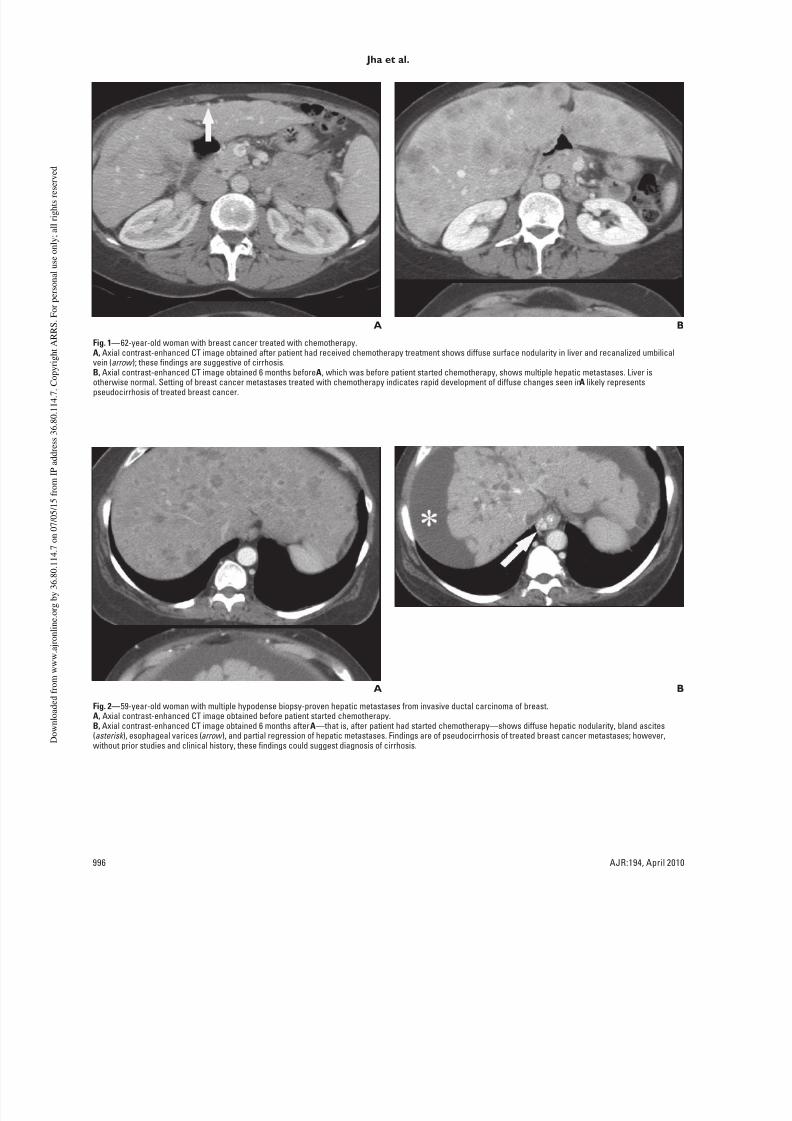
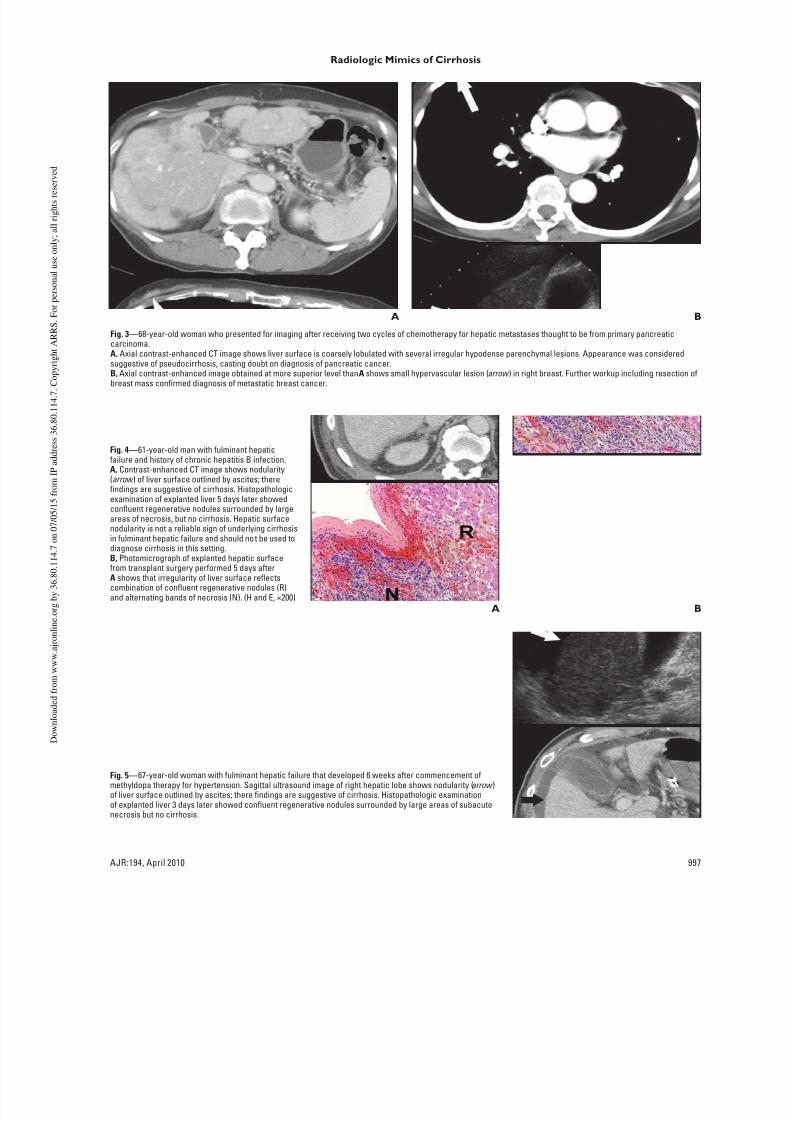
Fig. 3—68-year-old woman who presented for imaging after receiving two cycles of chemotherapy for hepatic metastases thought to be from primary pancreaticcarcinoma.A, Axial contrast-enhanced CT image shows liver surface is coarsely lobulated with several irregular hypodense parenchymal lesions. Appearance was consideredsuggestive of pseudocirrhosis, casting doubt on diagnosis of pancreatic cancer.B, Axial contrast-enhanced image obtained at more superior level than A shows small hypervascular lesion (arrow ) in right breast. Further workup including resection ofbreast mass confirmed diagnosis of metastatic breast cancer.
B
A
Fig. 4—61-year-old man with fulminant hepaticfailure and history of chronic hepatitis B infection.A, Contrast-enhanced CT image shows nodularity(arrow ) of liver surface outlined by ascites; therefindings are suggestive of cirrhosis. Histopathologicexamination of explanted liver 5 days later showedconfluent regenerative nodules surrounded by largeareas of necrosis, but no cirrhosis. Hepatic surfacenodularity is not a reliable sign of underlying cirrhosisin fulminant hepatic failure and should not be used todiagnose cirrhosis in this setting.B, Photomicrograph of explanted hepatic surfacefrom transplant surgery performed 5 days afterA shows that irregularity of liver surface reflectscombination of confluent regenerative nodules (R)and alternating bands of necrosis (N). (H and E, ×200)
B
Fig. 5—67-year-old woman with fulminant hepatic failure that developed 6 weeks after commencement ofmethyldopa therapy for hypertension. Sagittal ultrasound image of right hepatic lobe shows nodularity (arrow )of liver surface outlined by ascites; there findings are suggestive of cirrhosis. Histopathologic examinationof explanted liver 3 days later showed confluent regenerative nodules surrounded by large areas of subacutenecrosis but no cirrhosis.

7/18/2019 AJR JURNAL RADIOLOGI
http://slidepdf.com/reader/full/ajr-jurnal-radiologi 6/7
998 AJR:194, April 2010
Jha et al.
Fig. 6—64-year-old woman with metastatic lobular breast cancer. Axial contrast-enhanced CT image shows fine nodularity of hepatic surface. Liver biopsyrevealed metastatic breast cancer without cirrhosis.
Fig. 7—58-year-old woman with bilateral lobular breast cancer. Axial contrast-enhanced CT image shows widespread diffuse parenchymal and surface hepaticnodularity. Biopsy revealed metastatic disease without cirrhosis.
Fig. 8—32-year-old man with sarcoidosis. Axial contrast-enhanced CT imageshows widespread diffuse parenchymal and surface hepatic nodularity (arrow ).Appearance of liver on CT alone could be interpreted as cirrhosis, but notemultiple hypodense nodules in spleen. Retroperitoneal adenopathy (not shown)
was also present. Nodal biopsy confirmed diagnosis of sarcoidosis.
Fig. 9—44-year-old man with sarcoidosis. Axial unenhanced CT image showssplenomegaly (asterisk ) and recanalized umbilical vein (arrow ) arising fromsomewhat shrunken and irregular liver. Liver biopsy revealed sarcoidosis withoutcirrhosis. Sarcoidosis is one cause of noncirrhotic portal hypertension.

7/18/2019 AJR JURNAL RADIOLOGI
http://slidepdf.com/reader/full/ajr-jurnal-radiologi 7/7
AJR:194, April 2010 999
Radiologic Mimics of Cirrhosis
F O R Y O U R I N F O R M A T I O N
This artic le is avai lable for CME c redit. See w ww.a rrs.org for more inform ati on.
Fig. 11—60-year-old man with portal hypertension leading to gastrointestinalbleeding, ascites, and thrombocytopenia due to biopsy-proven nodularregenerative hyperplasia in liver transplant; transplantation was performed 18years earlier for primary sclerosing cholangitis. Axial contrast-enhanced CTimage shows liver surface (arrow ) is irregular and shows relative hypertrophy ofleft hepatic lobe (asterisk ). These findings mimic those of cirrhosis.
Fig. 12—11-year-old girl with renal failure due to autosomal recessive polycystickidney disease. Coronal T2-weighted MR image shows kidneys (K) are replacedby innumerable relatively small cysts. Focal segmental biliary dilatation (arrow )in liver reflects coexistent congenital hepatic fibrosis, which can occur inassociation with autosomal recessive polycystic kidney disease and is cause ofnoncirrhotic portal hypertension. Note spleen (asterisk ) is enlarged.
A
Fig. 10—58-year-old man with history ofrenal transplantation for HIV nephropathywho presented with sepsis 1 day after righthemicolectomy for colonic volvulus.A, Sagittal ultrasound image of righthepatic lobe shows subtle echogenicnodularity of liver that could be consideredsuggestive of cirrhosis. Representativenodule (arrow ) is visible anteriorly.
B, Axial contrast-enhanced CT imageshows subtle parenchymal heterogeneityconsisting of small hypodense nodules.Representative nodule (arrow ) isvisible posteriorly. Subsequent liverbiopsy confirmed diagnosis of nodularregenerative hyperplasia.
B
Fig. 13—68-year-old man with idiopathic portal hypertension. Axial contrast-enhancedCT image shows splenomegaly (S), gastroesophageal varices (white arrow ), and ascites(black arrow ), but liver appears normal in size and contour. Liver biopsy confirmedabsence of cirrhosis; final diagnosis was idiopathic portal hypertension.
Related Documents











