Trauma Airway Management: Myths & Pearls P tP t dFt Past Present and Future G Kovacs MD MHPE FRCPC G Kovacs MD MHPE FRCPC Professor, Department of Emergency Medicine & Anesthesiology & Anesthesiology Dalhousie University Halifax NS Halifax, NS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Trauma Airway Management:Myths & Pearls
P t P t d F tPast Present and FutureG Kovacs MD MHPE FRCPCG Kovacs MD MHPE FRCPC
Professor, Department of Emergency Medicine& Anesthesiology& Anesthesiology
Dalhousie UniversityHalifax NSHalifax, NS

Speaker Disclosure
I do not have an affiliation (financial or otherwise) with I do not have an affiliation (financial or otherwise) with any commercial organization that may have a direct or indirect connection to the content of my presentation.


Nuts and Bolts
Expect the unexpectedExpect the unexpectedExpect the unexpected…Expect the unexpected…
V 2

Expect the unexpectedExpect the unexpectedExpect the unexpected…Expect the unexpected…

Plan
• ATLS and the airway• Decisions• C spine• C-spine• Drugs• Devices
Trauma AirwayTrauma Airwaypast, present and future…past, present and future…

Who’s Job is it ?Who s Job is it ?
Who owns the airway..Anesthesiology? The TTL does: - EM, GP, CC, Surgeon, - Others: EMS, RT
Knowledge and SkillExperienceA il blitAvailablity


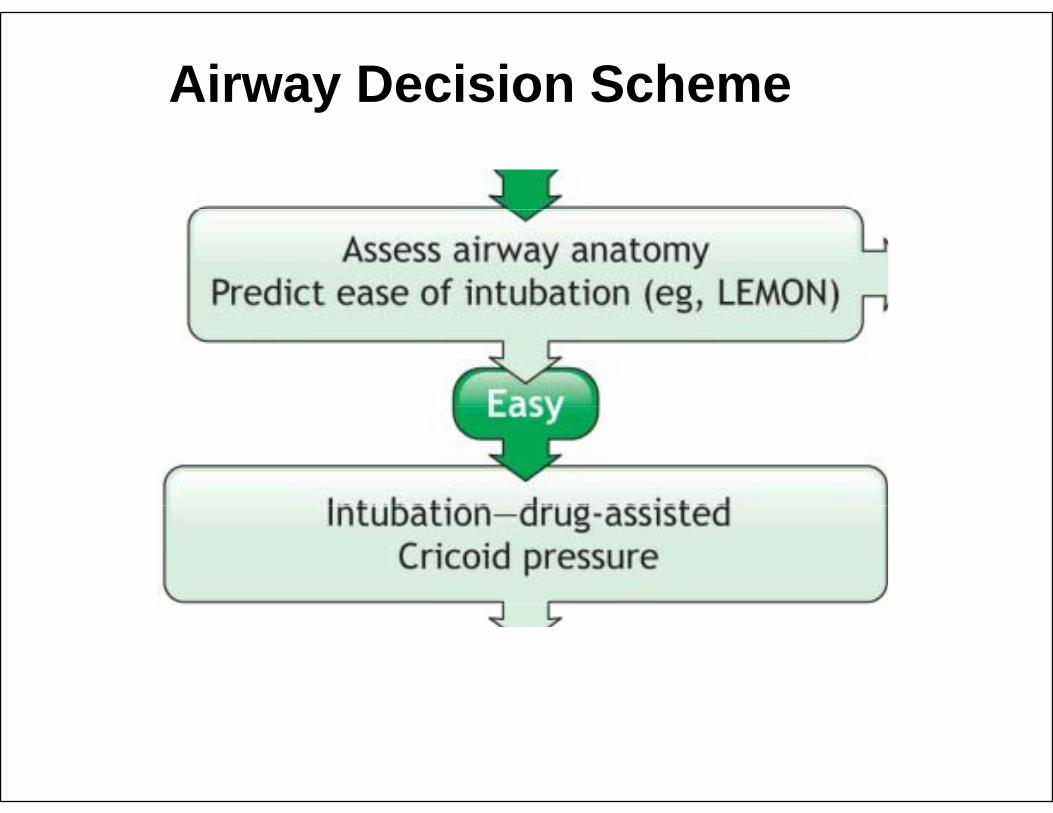
Airway Decision Schemey

The Decision:The Decision:Prioritization of Resuscitation?Prioritization of Resuscitation?

Reprioritization of Resuscitation

Decisions
Intubation acuity…Intubation acuity…

Duncan R, Thakore S. J Emerg Med. 2009


Ca tion
Protect the cervical spine during airway management!
Caution
y g

All hands on neck…

Airway and C-spine
Is it much a do about nothing?

Deficit after injurye c t a te ju y
• Prehospital phaseE t i ti– Extrication
– Immobilization• In ED
Assessment– Assessment– Airway management


Deterioration after tube
• Case reports• Related to
difficulty/# of yattemptsUnrestricted spine• Unrestricted spine movement
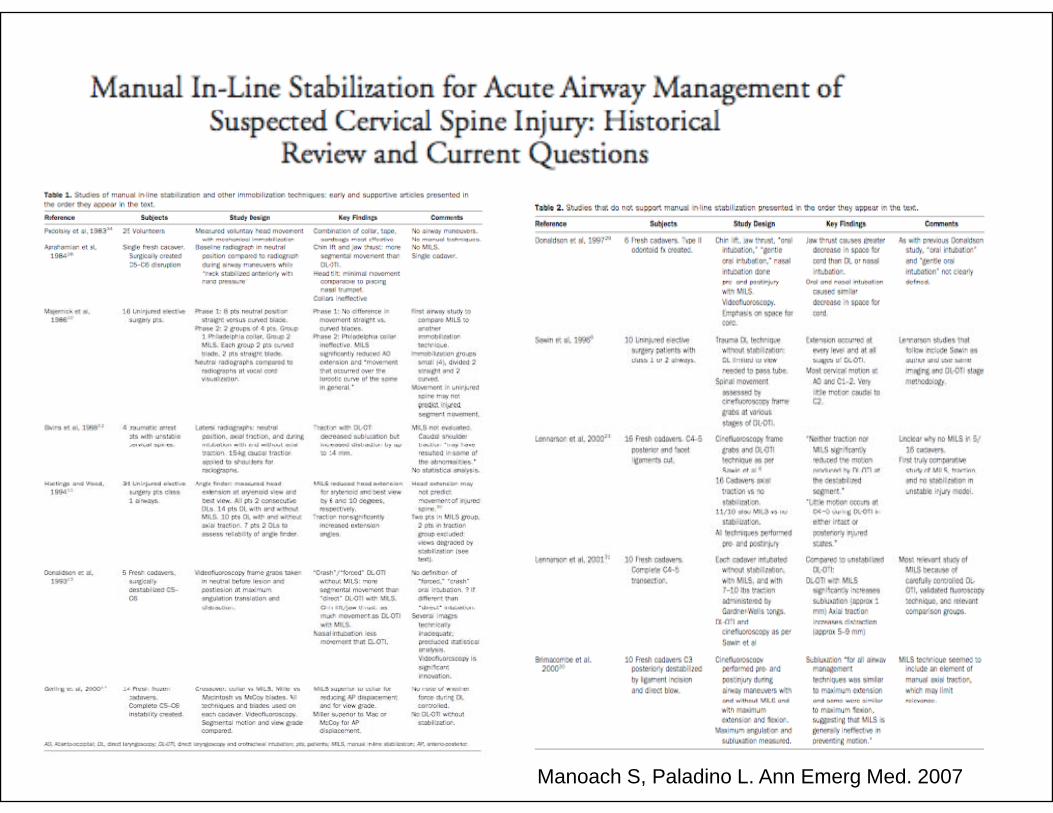
Manoach S, Paladino L. Ann Emerg Med. 2007
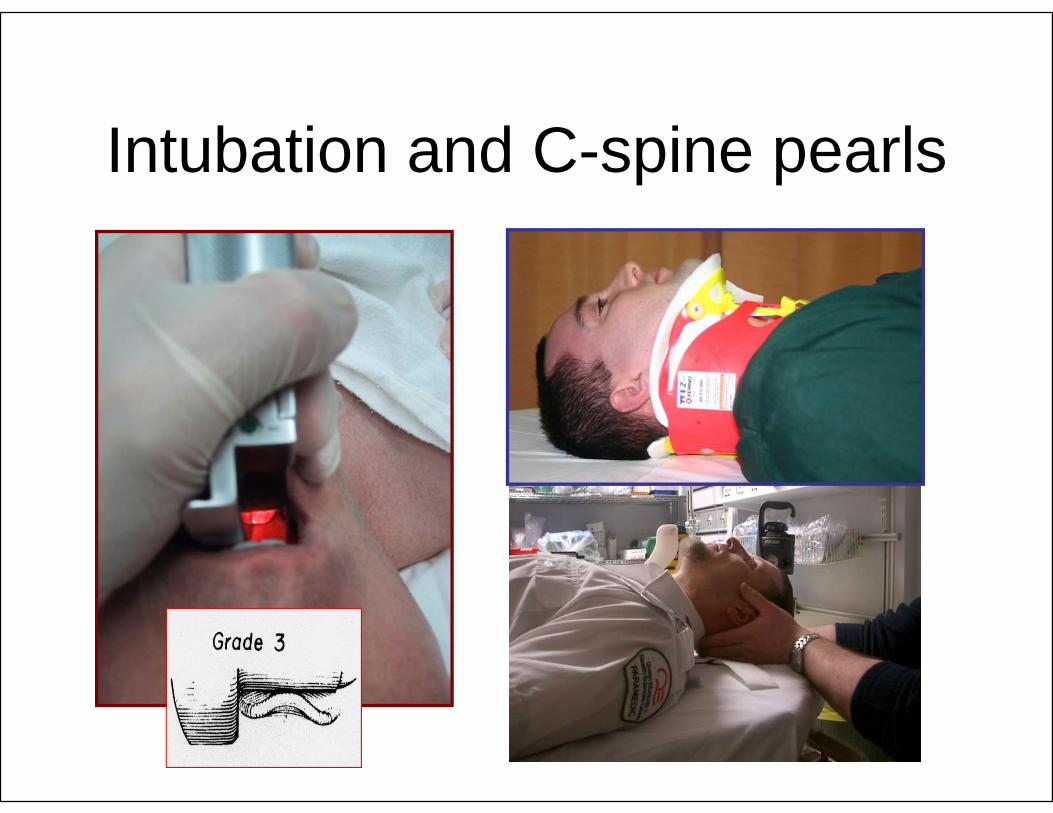
Intubation and C-spine pearls

Airway Decision Schemey

Airway Decision Scheme

What is our goal?
Is this a failed airway?

Redefining success
• Sample case of RSISample case of RSI with successful placement of ETTplacement of ETT
• In head injured patient
Davis et al A Follow up Analysis of Factors
patient
Davis et al, A Follow up Analysis of Factors Associated with Head Injury Mortality After Paramedic Rapid Sequence Intubation. J Trauma. 2005;59:484-488
Is this a successful airway ?
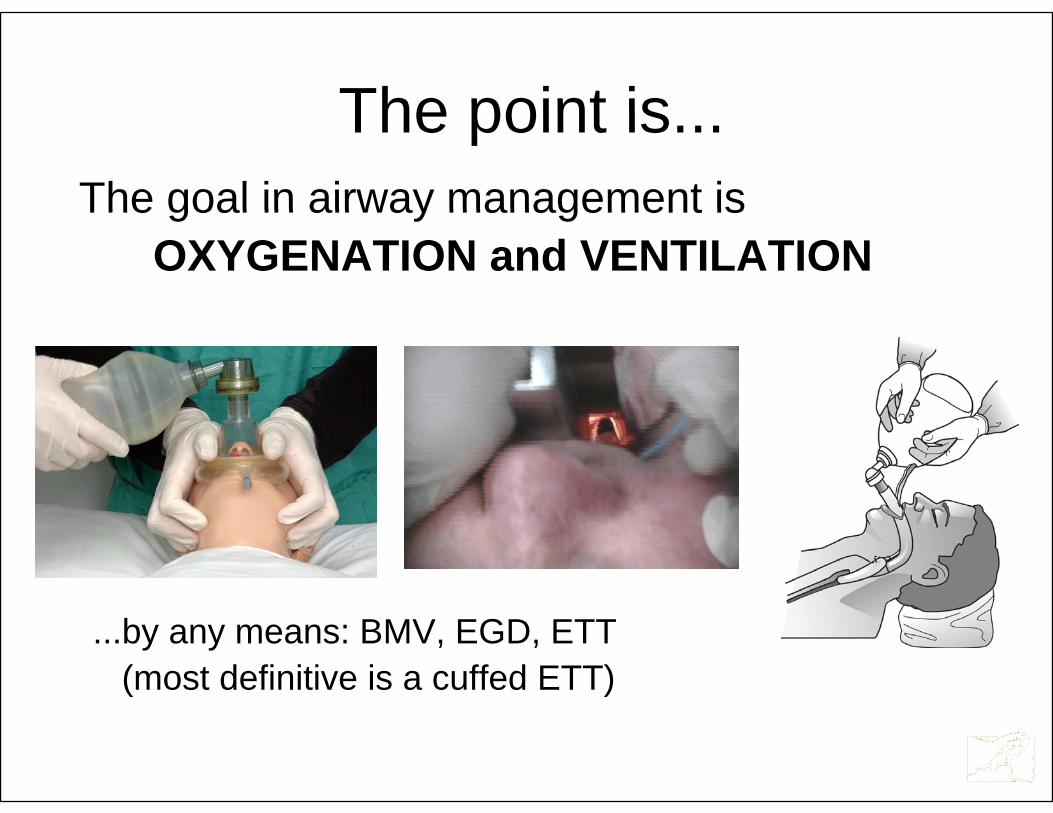
The point isThe point is...The goal in airway management isThe goal in airway management is
OXYGENATION and VENTILATION
...by any means: BMV, EGD, ETT(most definitive is a cuffed ETT)

Airway Decision Schemey
Airway Decision Schemey

Definitions and Drugs
• Rapid Sequence Induction (OR)– Intubated to provide anesthesia
• Rapid Sequence Intubation (ED)– Anesthetized/paralyzed to facilitate
intubation

Definitions and Drugs
To Sux or Not to Sux…To Sux or Not to Sux…90100
• Propofol alone vs Propofol with Sux 60
7080
Propofol with Sux• Optimal conditions: 30
4050 P
P+Sp30% vs 98%
0102030
0P P+S
Naguib M. Anesthesiology 2003Naguib M. Anesthesiology 2003
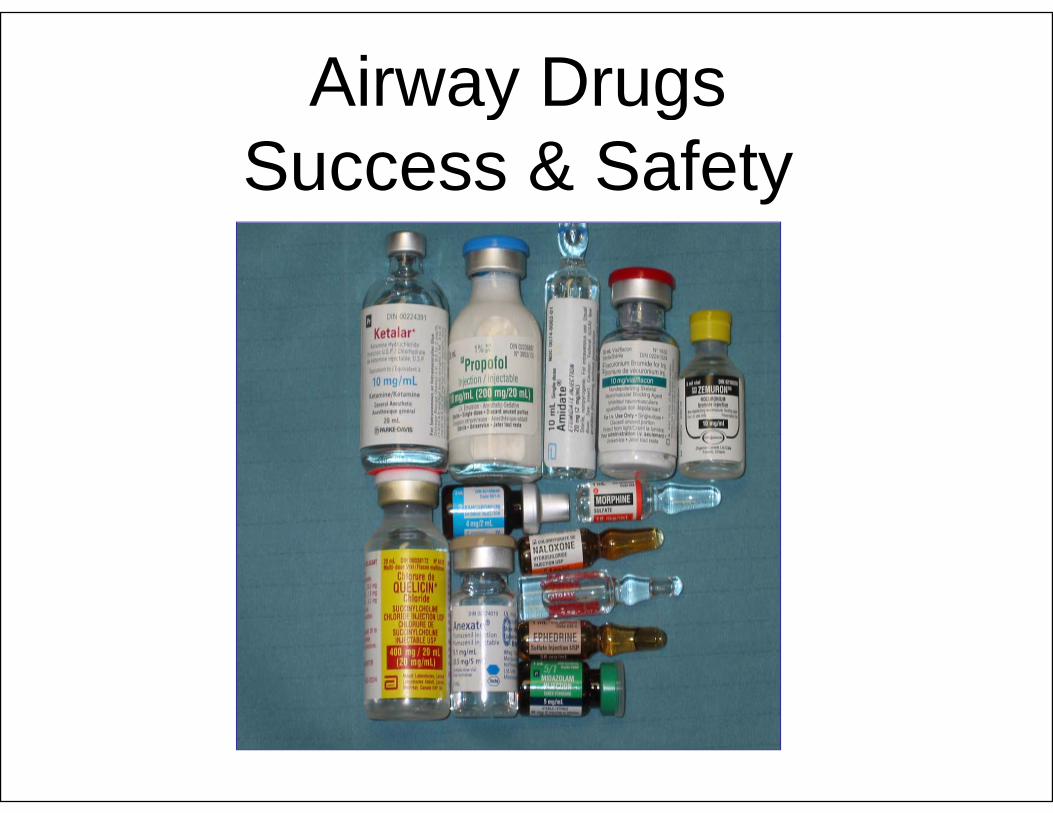
Airway Drugsy gSuccess & Safety

What’s new what’s old ?
W K t l J T 2009Warner K et al. J Trauma. 2009
Filannysky Y, Miller P. CJEM. 2010

Case: single shot .22
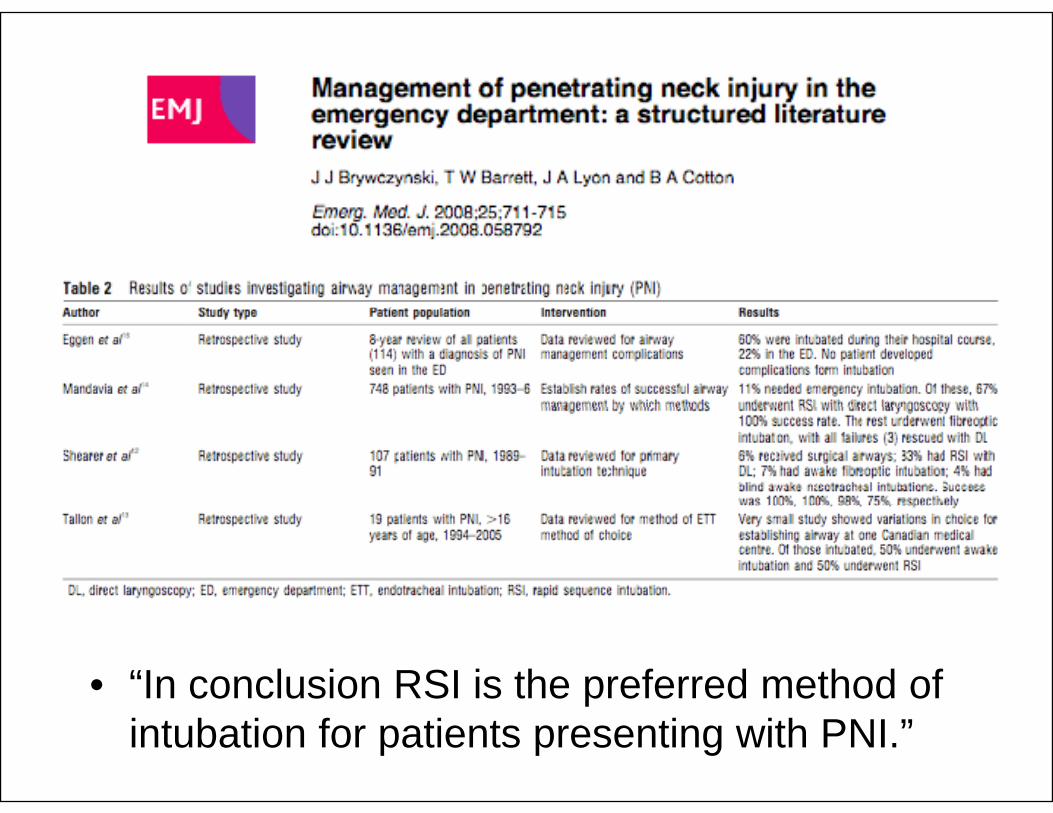
• “In conclusion RSI is the preferred method of pintubation for patients presenting with PNI.”
Is it ?
• Penetrating neck injury is only a ‘marker’ for airway injuryairway injury
• Is RSI safe with a penetrating neck injury ?I RSI f ith t ti i i j ?• Is RSI safe with a penetrating airway injury ?
• IF using an RSI:– Don’t mask vent – No blind device use
G t it 1 t tt t– Get it on 1st attempt

Airway Decision Schemey

Airway Decision SchemeAirway Decision Scheme

Where do you press?Where do you press?
Pushing on the thyroid cartilage usually helpsthe view…With ELM/BURP most patients improved one fulllaryngoscopic grade.
Benumof JL et.al. J. Clinical Anesthesia 1996
P hi th i id tilPushing on the cricoid cartilage may worsen the view …With Cricoid pressure (not ELM/BURP)worsens DL view in 30% of cases
Levitan R et al. Ann Emerg Med. 2006

Airway Decision SchemeAirway Decision Scheme
D i f iDevice confusion
“… turned out to be a diffi lt i t b tidifficult intubation. After desaturation
d b d diand bradycardia we switched to a li ht d hi hlightwand which was successful.”
… Fixation error
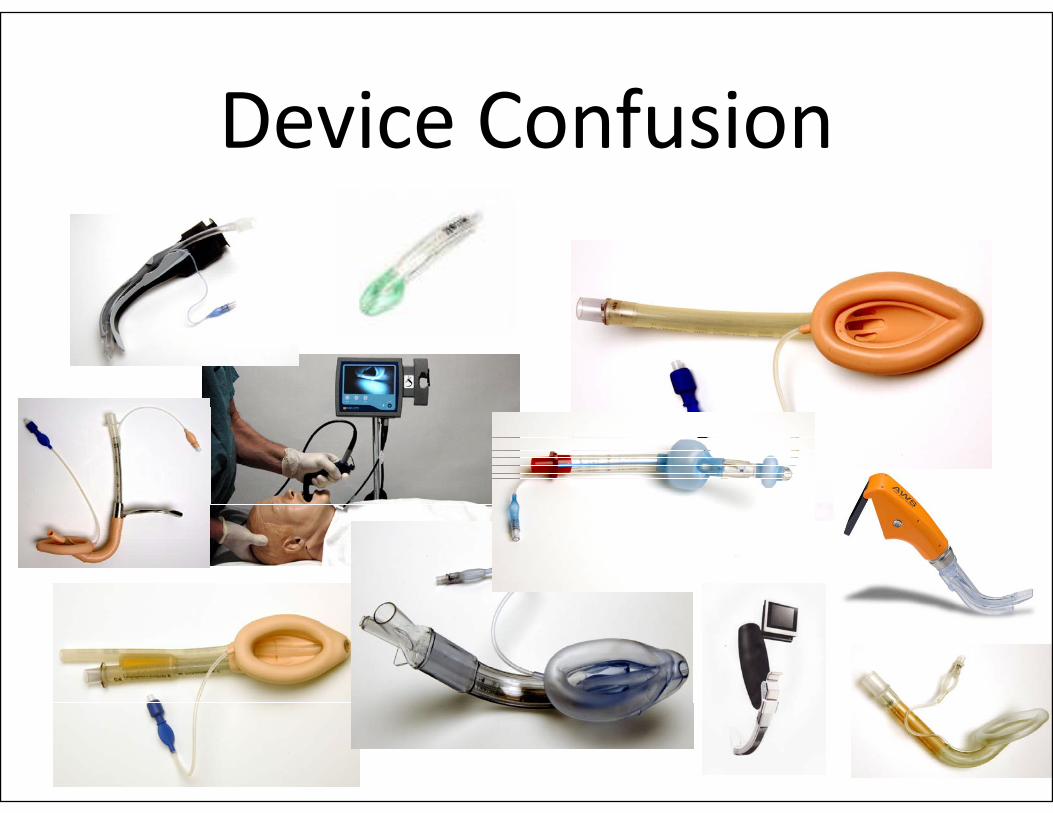
Device ConfusionDevice Confusion

I can’t get the tube…• You see this…
• “89, 88, 86, 84”


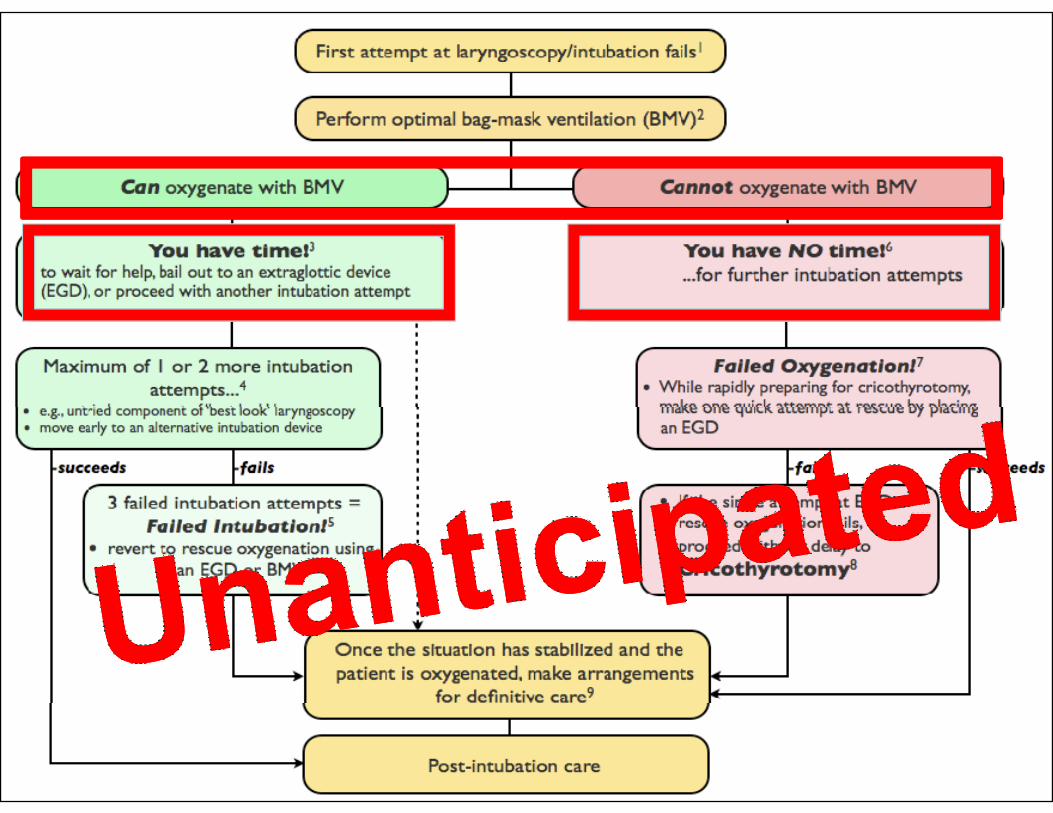
Can I Bag’em ?
•
YES NOYES NO

Can I Bag’em ?
•
YES NOYou have time… You have NO time…
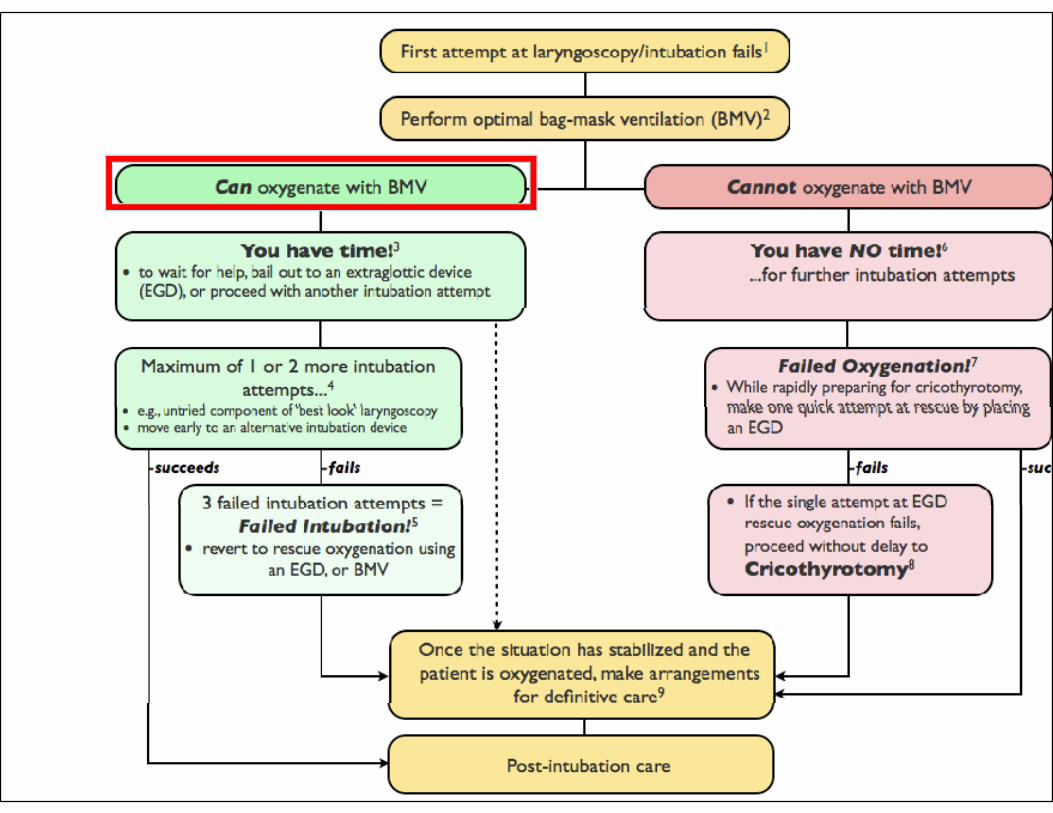

Have time devices
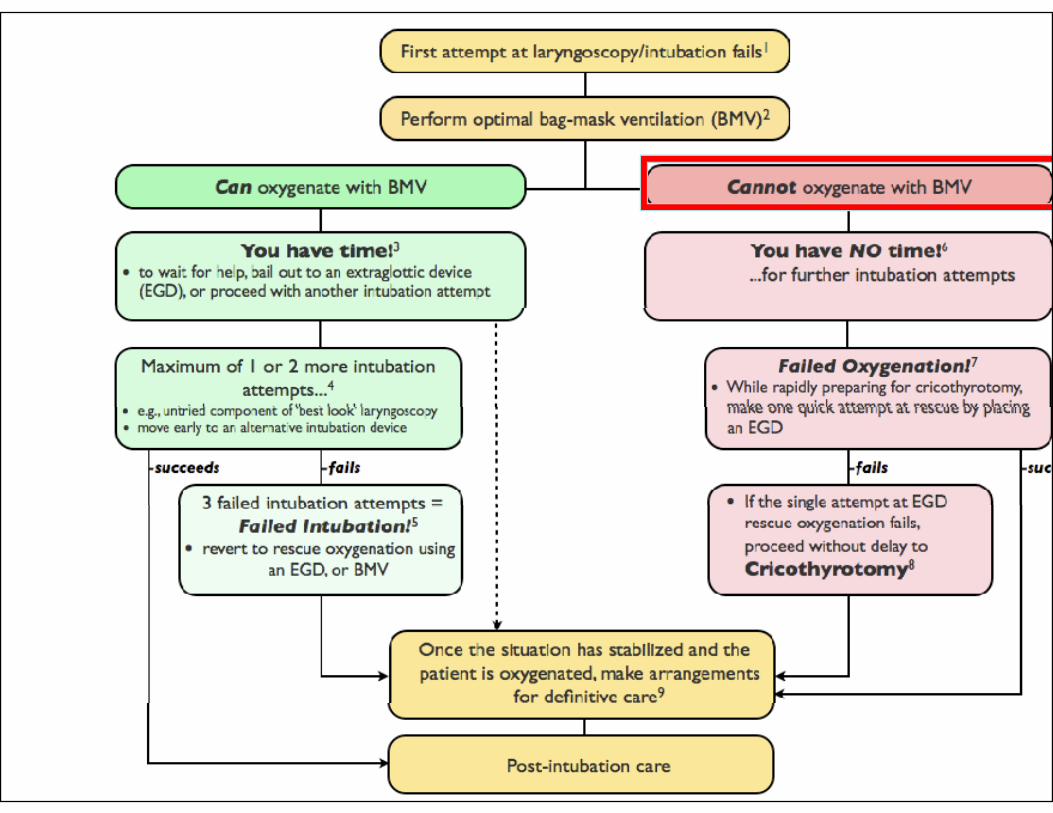

No time devices
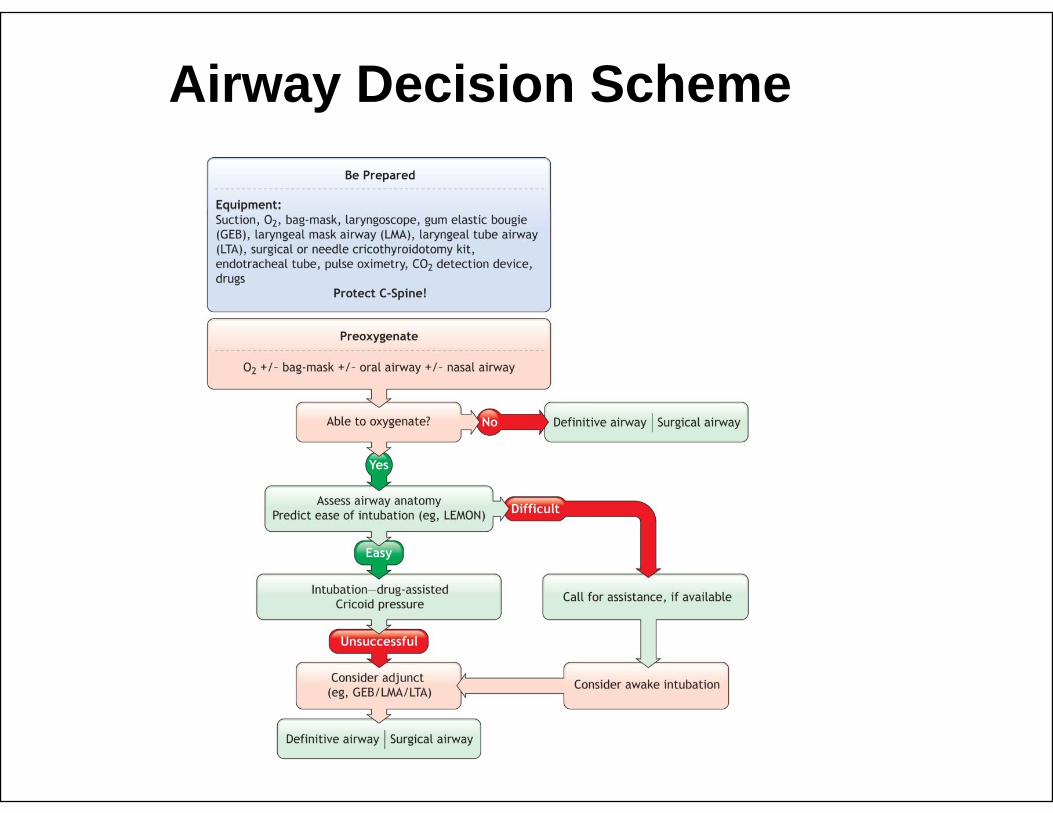
Airway Decision Schemey

Airway Decision SchemeAirway Decision Scheme

Surgical airwaySurgical airway when, why, what & wherewhen, why, what & where
• Cricothyroidotomy• Cricothyroidotomy vs TracheostomyOpen 4 step Qick• Open, 4-step, Qick-trach, Minitrach
• Melker, etc…
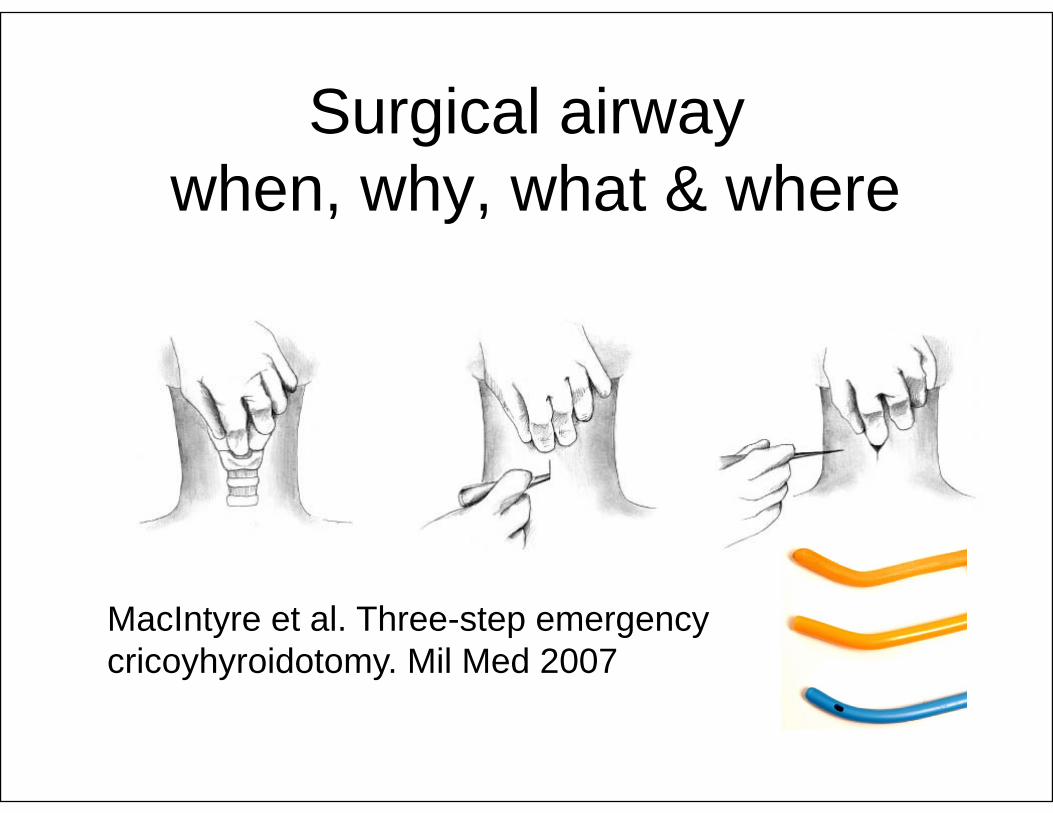
Surgical airwaySurgical airway when, why, what & wherewhen, why, what & where
MacIntyre et al. Three-step emergency cricoyhyroidotomy. Mil Med 2007

Surgical airway…

The future…
“Good judgment may come from experience but experience comes from bad judgment.”j g
...Mark Twain

Expect the Unexpected
Related Documents











