AHRQ 2010 Annual Conference AHRQ Data Resources to Inform Health Policy Research: The Medical Expenditure Panel Survey (MEPS) Jeffrey Rhoades, Ph.D.

AHRQ 2010 Annual Conference AHRQ Data Resources to Inform Health Policy Research: The Medical Expenditure Panel Survey (MEPS) Jeffrey Rhoades, Ph.D.
Dec 28, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
AHRQ 2010 Annual Conference
AHRQ Data Resources to Inform Health Policy Research:
The Medical Expenditure Panel Survey (MEPS)
Jeffrey Rhoades, Ph.D.
Medical Expenditure Panel Survey
MEPS OVERVIEW
MEPS Overview
History & Purpose Survey Components & Design Sample Core Content Supplemental CAPI sections &
Questionnaires Public Use Files Dissemination of Data
MEPS History
1977 National Medical Care Expenditure Survey
1987 National Medical Expenditure Survey
1996 Medical Expenditure Panel Survey

MEPS-HC Purpose & Uses
Estimates and tracks annual health care use, expenditures and insurance coverage
Provides estimates of expenditures and sources of payment by selected demographic variables
Used for policy-related and behavioral research on the determinants of health care use, spending, and insurance coverage
Used in microsimulation models to analyze alternative health care delivery proposals
MEPS Survey Components
MEPS-HC -- Household Component
MEPS-MPC -- Medical Provider Component
MEPS-IC -- Insurance Component

MEPS-HC Survey Design
Sub-sample of respondents from the previous year’s National Health Interview Survey (NHIS)
Representative of the civilian non-institutionalized population of the US
Five in-person interviews over 2 ½ year period using Computer Assisted Personal Interview (CAPI)
Interviews average 90 minutes with a range of one to four hours
Oversampling in MEPS Panels 7-14 (2002-2009)
Carryover from NHIS– Blacks– Hispanics– Asians (panels 12-14 after 2006 NHIS redesign)
Additional MEPS Oversampling– Asians – Low income (panels 7-13)– Blacks (panels 9-11, 13-14)– Hispanics (panels 13-14)
9
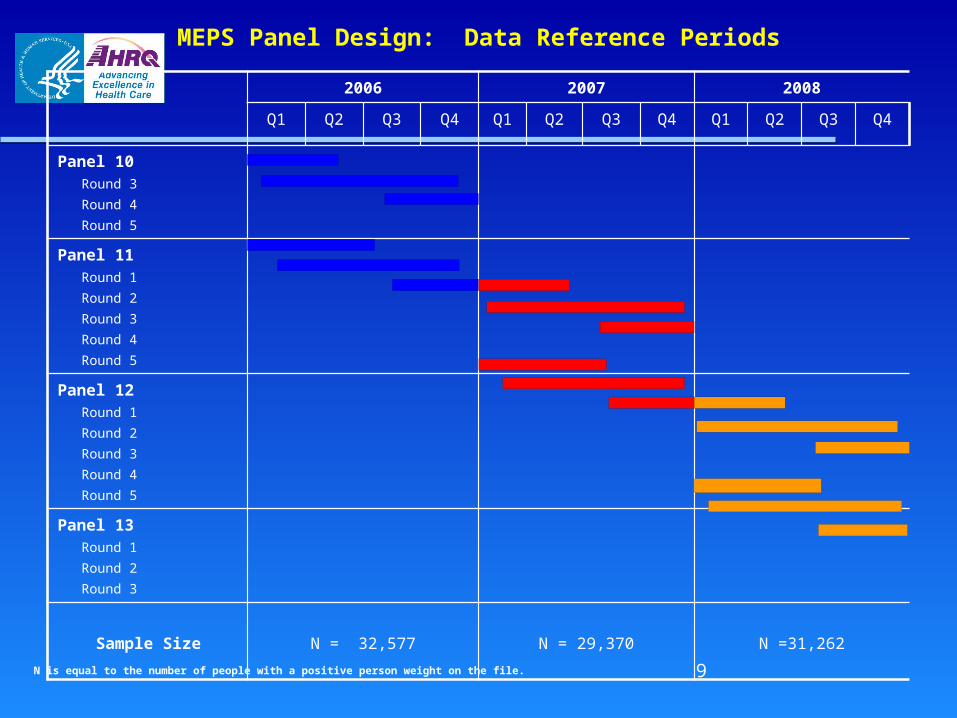
MEPS Panel Design: Data Reference Periods
2006 2007 2008
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Panel 10 Round 3 Round 4 Round 5
Panel 11 Round 1 Round 2 Round 3 Round 4 Round 5
Panel 12 Round 1 Round 2 Round 3 Round 4 Round 5
Panel 13 Round 1 Round 2 Round 3
Sample Size N = 32,577 N = 29,370 N =31,262
N is equal to the number of people with a positive person weight on the file.

MEPS-HC Sample Sizes
Year Families Persons
1996 8,655 21,5711997 13,087 32,6361998 9,023 22,9531999 9,345 23,5652000 9,515 23,8392001 12,852 32,1222002 14,828 37,4182003 12,860 32,6812004 13,018 32,7372005 12,810 32,3202006 12,811 32,5772007 11,615 29,3702008 12,957 31,262

MEPS-HC Core Interview Content
Demographics Charges and Payments Health Status Conditions Utilization Employment Health Insurance
MEPS- HC Supplemental CAPI Sections
Sections asked in rounds 2 and 4: Access to care Child preventive health Satisfaction with health plans &
providers
Sections asked in rounds 3 and 5: Assets (round 5 only) Income Preventive Care
MEPS-HC Supplemental Paper Questionnaires
Diabetes Care Survey (DCS)• Given once a year to each person identified as
having diabetes• Includes questions about diabetes related tests
and managing diabetes
Adult Self-Administered Questionnaire (SAQ)• Given once a year to each adult 18 years old and
older• Focuses on self-reported information such as
opinions about health care issues and quality of care measures, assessment of own health, and height /weight.
MEPS-HC Caveats and Limitations
Sample size limitations preclude some analyses
Typically, one respondent provides data for the entire household
Household respondents may not be able to report accurately certain types of information– type of health plan– detailed event information– diagnoses

MEPS Public Use Files

Levels of MEPS-HC Public Use Files
Person Level - detailed person information
Event Level - detailed event information
Condition Level - detailed condition information
Job Level - detailed job information
Types of MEPS-HC Files
Full-year Files – Contain expenditure and utilization data for the calendar year from several rounds of data collection.
– Full Year Consolidated Data File – Event File– Medical Conditions File – Jobs File – Person Round Plan Public Use File
Point-in-time Files - Data for the beginning of the year providing early glimpses of what full-year estimates will likely be.
MEPS/NHIS Link Files - Cross-walk files that allow merging of Household Component files and NHIS files.

Details on MEPS PUFs
Documentation Files– Contain general information about MEPS– Contain survey information specific to each file– Contain variable-source crosswalk to link back to
questionnaire items
File Codebooks– Contains names and location of all variables – List both weighted and unweighted estimates
Data files and related documentation are available for downloading on MEPS Web site: www.meps.ahrq.gov/mepsweb

Medical Expenditure Panel Survey
DISSEMINATION OF INFORMATION AND DATA
PRODUCTS
MEPS Web Site
Materials on the MEPS Web site: – Questionnaires
Core and Supplemental– Summary data tables
Expenditures by Health Care Service Expenditures by Medical Condition Health Insurance Quality of Care Prescription Drugs State-Level Medical Expenditures Access to Care
– Interactive MEPS query tool – MEPSnet– Publications
Statistical Briefs Methodology Reports Research Findings

Data User Workshops
Information will be posted on Workshops and Events section of web site
For inquiries please e-mail: [email protected]

MEPS Publications Statistical Briefs: Easy-to-read, concise graphical
summaries of MEPS data Research Findings and Highlights: Tables and
summaries of descriptive statistics Methodology Reports: Detailed information on MEPS
sample design and survey methods Chartbooks: Policy-sensitive topics in an accessible
question-and-answer format Working Papers: Preliminary analyses of methodological
and technical issues by AHRQ staff Research in Action: Analyses using research results from
AHRQ-sponsored studies, including MEPS data

AHRQ Data Center (ADC) Provides researchers access to non-
public use MEPS data (except directly identifiable information);
Location of data analysis – on secure LAN at AHRQ– Census Remote Data Center (RDC)
ADC Application And Procedures
Application procedures are on the MEPS web site
Submit proposal to Data Center coordinator
Review within 2 weeks for feasibility, and data availability
Institutional Review Board (IRB) review required
ADC Fees
User fee of $300 for approved projects to cover technical assistance, simple file construction, and/or up to 4 hours of programming support from data contractor
Additional programming support available from an AHRQ contractor at a cost of $105.00/hr
User fee waived for full-time students
No fee if you use a RDC

ADC Guidelines
Researcher may bring data in, but not out Researcher has access only to data needed for
approved project All tabular data will be reviewed for
confidentiality before release from Center Only approved tables can leave the Center Center will store data files, foreign merge files,
and all outputs needed for replication
Medical Expenditure Panel Survey
MEDICAL CONDITIONS DATA

MEPS Condition Roster
One roster per person Cumulates medical conditions reported across MEPS interviews Interviewer records verbatim responses to questions in the following 3 sections:
– Condition Enumeration– Medical Events – Disability
Condition Enumeration Question
We're interested in learning about health problems that may have bothered (PERSON) {since (START DATE)/between (START DATE) and (END DATE)}. – Health problems include physical conditions,
accidents, or injuries that affect any part of the body as well as mental or emotional health conditions, such as feeling sad, blue, or anxious about something.

Medical Events Condition Questions
What conditions were discovered or led (PERSON) to make this visit? PROBE: Any other condition? IF CONDITION IS ALREADY LISTED, ASK: Is this the same (NAME OF CONDITION) that we have already talked about before?– Types of visits
Inpatient Outpatient Emergency Room Office Based Home Health
Conditions associated with Prescribed Medicine purchases:– What health problem is (MEDICINE) prescribed for?
PROBE: Any other health problems?

Disability Days Condition Questions
Missed school or work– What are the health problems that caused
(PERSON) to miss work/school on those days? PROBE: Any other health problems?
Bed days– What are the health problems that caused
(PERSON) to spend half day or more in bed on those days? PROBE: Any other health problems?
Reporting and Recording Conditions
Respondents may report having the same condition more than once– Interviewer probes whether occurrence
of condition already reported– Each unique episode of a condition
recorded only once person may have multiple colds in year each cold has separate record
Accidents and Injury Questions
Following items asked if relevant to reported condition:– date of accident– place (work, home, school, etc.)– cause (gun, vehicle, fall, fire, etc.)– whether or not the person has recovered
from the injury
Medical Conditions File Structure
Each record represents unique condition or procedure for a person
Persons may be represented on file once, several times or not at all
Can be linked to person and event files for analysis
Condition Coding and Editing
Fully specified ICD-9 CM codes (up to 5 digits)
ICD-9 condition codes collapsed to 3 digits to maintain confidentiality
Approximately 10% of condition codes are collapsed further by combining 2 or more 3-digit codes

Procedure Coding and Editing
Only obtained from Medical Events Questions
Fully specified ICD-9 CM codes (up to 4 digits)– Collapsed to 2-digit codes– Approximately 3% collapsed further by
combining 2 or more 2-digit codes
Clinical Classification Codes (CCC)
ICD-9 codes aggregated into broad clinically meaningful categories
Edited to preserve confidentiality Crosswalk included in documentation Formerly Clinical Classification for
Health Policy Research (CCHPR)
Condition-Event Link Files
Used to link conditions to:– Persons on person files
all reported conditions or just those associated with events
– Events on event files most conditions associated with events
already included on event files
Separate link file for prescribed medicines

National Estimates of Conditions
Most appropriate to estimate “treated prevalence”– MEPS website summary data tables on
Expenditures by Medical Condition Condition more likely to be
underreported if:– respondent/person not aware– not salient or bothersome– no medical care received

Condition Data Limitations/Caveats
Household-reported – One respondent usually providing
information for all household members Many recorded text strings not easily
classifiable into ICD-9 codes Limited information on procedures Not suitable for prevalence estimates More salient conditions tend to be
better reported

Priority Conditions Section
Separate section of questionnaire
Series of questions asking if “ever” had condition– “yes/no” responses, no ICD9 coding– responses not directly linked to conditions
roster
Factors used in determining priority conditions– Prevalence– Expenditures– Policy relevance

Priority Conditions List (Panel 12 and beyond)
Heart disease Heart attack Angina High cholesterol Cancer Stroke High blood pressure Diabetes Asthma Arthritis/Joint pain Emphysema Chronic bronchitis Attention deficit disorder

Priority Condition Section Revisions
Revised section in Panel 12– Priority Conditions Enumeration (PE) section
replaced PC section in prior panels
Primary differences between PE and PC– Questions asked all rounds rather than 3/5 only– PE section substantially earlier in CAPI– Follow-up question on cancer remission added– Age of diagnosis collected for more conditions
Revisions may increase reporting of conditions and associated medical events
Medical Expenditure Panel Survey
Health Care Utilization And Expenditures Data

Health Care Utilization
MEPS household respondents asked to report all health care use for family members during reference period
Utilization is called an “event” in MEPS Event type categories:
– Office-Based Medical Provider Visits (OB)– Hospital Inpatient Stays (IP)– Outpatient Department Visits (OP)– Emergency Room Visits (ER)– Dental Visits (DN)– Prescription Medicine Purchases (RX)– Home Health Care (HH)– Other Medical Expenses (OM)
Health Care Expenditures Collected at the event level Represent payments to providers of
the health care Payments are reported by source
(e.g., out-of-pocket, private insurance, public program)
Total expenditure is sum of payments across all sources of payment
Source of Payment Categories in CAPI
Self or family Medicare Medicaid/SCHIP Private
insurance VA
TRICARE Other federal
gov’t State or local
gov’t Worker’s comp Other insurance

Sources of Expenditure Data
Expenditures derived from two survey components:– Medical Provider Component (MPC)– Household Component (HC)
MPC data used when available HC data used when no MPC data
available Events with no MPC or HC data on
expenditures are imputed– results in no missing values
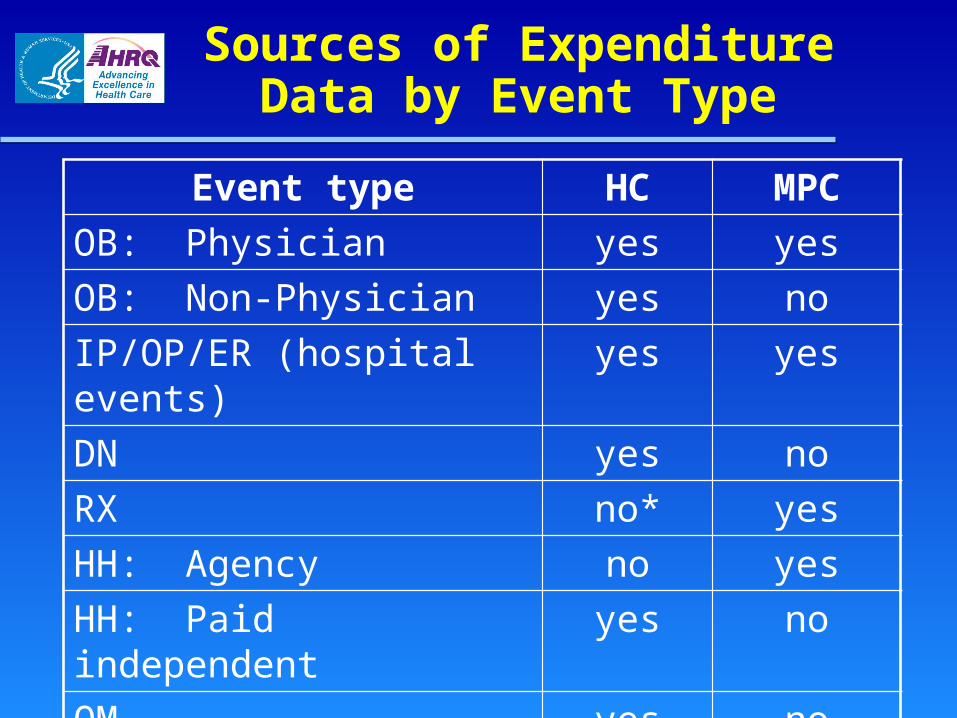
Sources of Expenditure Data by Event Type
Event type HC MPCOB: Physician yes yesOB: Non-Physician yes noIP/OP/ER (hospital events) yes yesDN yes noRX no* yesHH: Agency no yes
HH: Paid independent yes noOM yes no
*Except for self-filers

Annual Utilization and Expenditure Data
Annual data cumulated across approx 2 ½ rounds of data collection
Event level files– Separate by type of service– Unique record for each reported event
Some persons have no events Some persons have multiple events
Person-level file (full year consolidated) Variables derived from event level
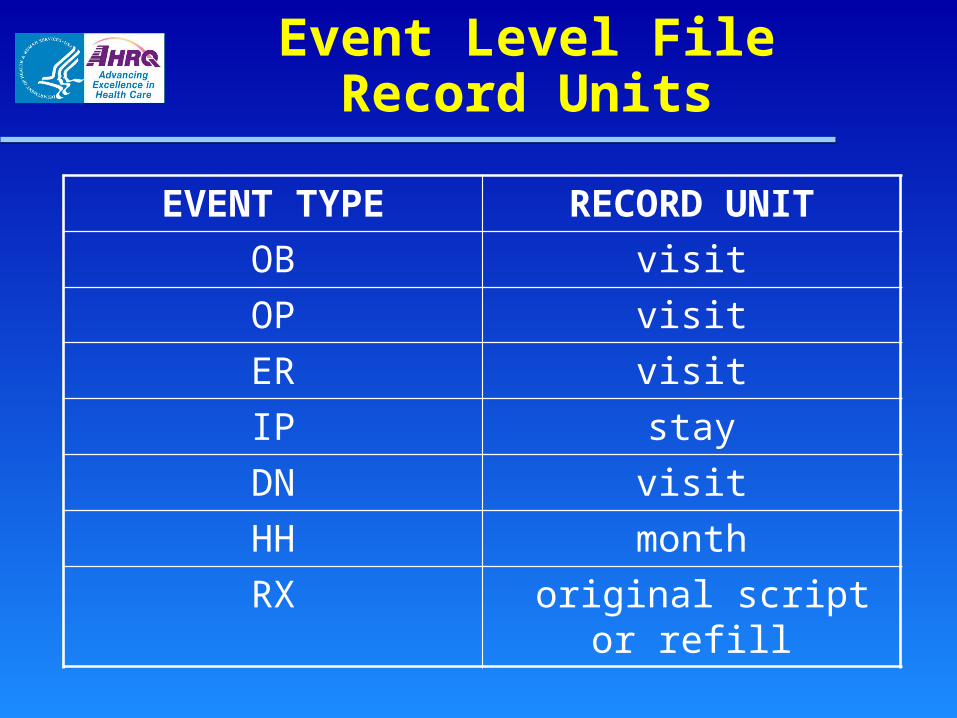
Event Level File Record Units
EVENT TYPE RECORD UNIT
OB visit
OP visit
ER visit
IP stay
DN visit
HH month
RX original script or refill
Event File Expenditure Variables:OB, DN and OM
12 expenditure by source of payment variables
A total expenditure variable – sum of 12 source of payment
variables
A total charge variable– provider’s charge before
adjustment or discount
Hospital Event Files Expenditure Variables: IP, OP, and ER
Facility Expenditure Variables – 12 expenditure by source of payment variables– A total facility expenditure variable– A total facility charge variable
Separately Billing Doctor Expenditure (SBD) Variables– 12 SBD expenditure by source of payment variables– A total SBD expenditure variable – A total SBD charge variable
Total Expenditures for the event– Sum of facility and SBD expenditures
Total charges for the event– Sum of facility and SBD charges
Common Variables in Event Files
Person/event ID Date(s) of care (not RX) Services/procedures Type of provider (not
RX,ER,IP) Expenditure variables Full year person weight Variance estimation variables Imputation flag

Event Files: Medical Conditions
IP – Up to 4 per event
OB, OP, ER & RX– Up to 3 per event
HH – Need to obtain from condition file
DN & OME – No medical conditions
IP variables
Have operation? Stay begin with ER visit? Number of nights in hospital Reason for stay (5 broad reasons) Stay related to specific condition (yes
or no); if yes, provide condition(s) VA facility?
Diagnostic Tests/Services Received During OB, OP, or ER Visit
Laboratory tests Sonogram/
Ultrasound X-ray Mammogram MRI/CAT SCAN
EKG/ECG EEG Vaccination Surgery Anesthesia Other tests or
exams
Main Medical ProviderOB and OP Visits
Specialty if a physician– 33 specialties plus “other”
Type of provider if not a physician– 17 types plus “other”

Category of Care Received During an OB or OP Visit
General checkup Diagnosis or
treatment Emergency Well child exam Follow-up or
post-op visit
Psychotherapy or mental health counseling
Maternity care Immunizations or
shots Laser eye
surgery
Treatments During an OB or OP Visit
Physical therapy Occupational
therapy Speech therapy Chemotherapy Radiation
therapy
Kidney dialysis IV therapy Treatment for
drug or alcohol Received allergy
shot Psychotherapy
or counseling

Prescribed Medicines (PMED) Event File
Each record represents an original RX script or refill – Includes diabetic supply/equipment and
insulin purchases– Contains drug characteristic and
expenditure variables

PMED File Expenditure Variables
Source – Nearly all MPC (pharmacy) data– Some source of payment information
collected from households filing their own insurance claims
Variables– 12 expenditure by source of payment– Total expenditure variable – No total charge variable

Variables in the PMED File
Household Component (HC) variables collected in each round– Medicine name– Number of times purchased– Used to treat a condition– Date first used – Pharmacy information– Names of free samples– Who files prescribed drug insurance claims

Drug characteristics
Drug characteristics included for each prescribed medicine event – Medication name– National drug code (NDC)– Quantity dispensed (e.g., 50)– Form (e.g., suspension)– Strength (e.g., 10)– Unit of measurement of form (e.g., cc) and strength
(e.g., mg)– Brand/generic designation (from Multum Lexicon)– Therapeutic class, sub-class, and sub sub-class (from
Multum Lexicon) – Pregnancy category (from Multum Lexicon)

Home Health (HH) Event File
Three broad categories – Agency care (including hospitals
and nursing homes)– Paid independent providers– Informal providers (e.g., family and
friends) Each record in file represents
monthly aggregate for specific type of care

HH File Expenditure Variables
Agency care– 12 expenditure by source of payment
variables – A total expenditure variable – A total charge variable
Paid independent providers– Same expenditure variables as Agency
care
Informal care – No expenditure variables
Home Health Variables
Type of worker(s) provided– Agency care only
Type of care
Amount of care– (frequency and length of visits)
Dental Event FileType of Provider Seen
General dentist
Dental Hygienist
Dental Technician
Dental Surgeon
Orthodontist
Endodontist
Periodontist
Other

Dental Services and Procedures
Diagnostic or preventative Restorative or endodontic Periodontic (gum treatment) Oral surgery Prosthetics Orthodontics Other procedures
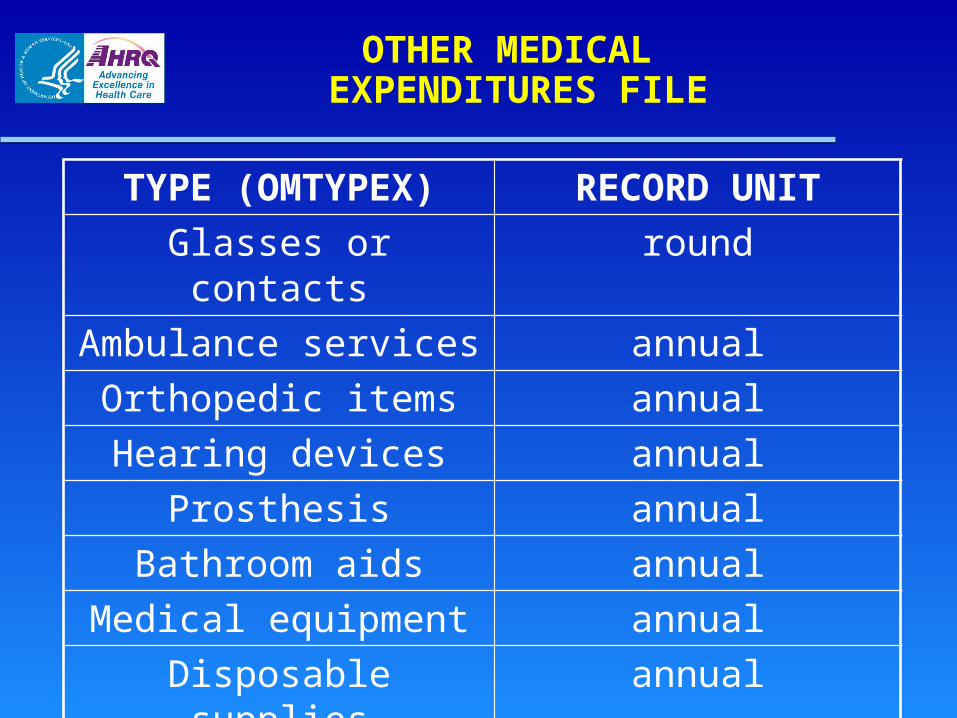
OTHER MEDICAL EXPENDITURES FILE
TYPE (OMTYPEX) RECORD UNITGlasses or contacts roundAmbulance services annual
Orthopedic items annualHearing devices annual
Prosthesis annualBathroom aids annual
Medical equipment annualDisposable supplies annual
Alterations/modifications annualOther annual
Flat Fees
What is a Flat Fee?– Fixed dollar amount paid for a group of
health care services– Common examples: orthodontic,
prenatal care Flat Fee ID: FFEEIDX Flat fee structure (FFevTYPE)
– Stem - Initial medical visit - expenditures– Leaf - subsequent medical visits - zero
expenditures

Zero Dollar Events
Reasons for $0 total expenditures– Flat fee leaf event from prior year– Follow-up visit without extra charge– Free care – Bad debt
Annual Person-Level File with Expenditure Data
Full Year Consolidated File– One record for each person in MEPS– Summary of all events and expenditures
Appendix 1 of documentation contains naming conventions for use and expenditure variables
– No detail on expenditures or characteristics of individual events
Medical Expenditure Panel Survey
HEALTH INSURANCE DATA
Health InsurancePublic Use Files, 2007-2008
MEPS HC-117 : 2009 P13R3/P14R1, Point-in-Time Population Characteristics
MEPS HC-115: 2008 Full Year Population Characteristics Data File
MEPS HC-111: 2007 Person Round Plan Public Use File

2009 Point-in-TimePublic Health Insurance Variables
TRINW31X COV BY TRICARE AT INTERVIEW – EDITED
MCARE31X COV BY MEDICARE – EDITED
MCAID31X COV BY MEDICAID – EDITED
OTPUBA31 COV BY/PAYS OTH GOV MCAID HMO
OTPUBB31 COV BY OTH PUBLIC NOT MCAID HMO
STPRG31 COV BY STATE SPECIFIC PROGRAM
PUB31X COV BY PUBLIC INS - EDITED
2009 Point-in-TimePrivate Health Insurance Variables
PRIEU31 COV BY PRIV EMPL/UNION PLAN
PRIDK31 COV BY PRIV DK PLAN PRING31 COV BY NONGROUP PLAN PRIOG31 COV BY OTH GROUP PLAN PRIS31 COV BY SELF-EMP-1 INS PRIOUT31 COV BY HOLDER OUTSIDE
RU PRIV31 COV BY PRIVATE INS INSRD31X INSURED - EDITED

2009 Point-in-TimePolicy Holder Insurance Variables
HPRIEU31 HOLDER OF PRIV EMPL/UNION PLAN
HPRIDK31 HOLDER OF PRIV DK PLAN HPRING31 HOLDER OF NONGROUP
PLAN HPRIOG31 HOLDER OF OTH GROUP
PLAN HPRIS31 HOLDER OF SELF-EMP-1
INS HPRIV31 HOLDER OF PRIV INS
PLAN
2008 Full Year Population Characteristics Data File
Public Insurance
Month by month indicators
TRIJA08X-TRIDE08X - TRICARE MCRJA08X-MCRDE08X - Medicare MCDJA08X-MCDDE08X - Medicaid/SCHIP OPAJA08-OPADE08 - managed care, other public
insurance OPBJA08-OPBDE08 - not managed care, other
public insurance STAJA08-STADE08 - state-specific program
participation PUBJA08X-PUBDE08X - indicates public insurance
in month
2008 Full Year Population Characteristics Data File
Private Insurance
Month by month indicators
PEGJA08-PEGDE08 - employer/union group insurance
PNGJA08-PNGDE08 - non-group private insurance POGJA08-POGDE08 - other group private insurance PDKJA08-PDKDE08 - don't know source of insurance POUJA08-POUDE08 - policy holder is outside the
household PRSJA08-PRSDE08 - self-employed with firm size of 1 PRIJA08-PRIDE08 - indicates private insurance in
month Policy Holders (repeat of Private) "H"

2008 Full Year Population Characteristics Data File
Summary Variables
Month by month indicators
PUBJA08X-PUBDE08X - indicates public insurance in month
PRIJA08-PRIDE08 - indicates private insurance in month
INSJA08X-INSDE08X - indicates any insurance in month
2008 Full Year Population Characteristics Data File
Summary Variables (continued)
UNINS08 – uninsured all of 08 INSCOV08 – health insurance
indicator 08– 1 = Any Private during 2008
– 2 = Public Only during 2008
– 3 = Uninsured all of 2008
2008 Full Year Population Characteristics Data File
Managed Care
Public insurance
Medicare Managed Care Plan
Medicaid or SCHIP HMO
Medicaid/SCHIP Gatekeeper Plans

2008 Full Year Population Characteristics Data File
Managed Care
Private insurance
Private HMOs Private HMO Plans that Pay for Visits to Non-Plan
Doctors Private Gatekeeper Plans Private Gatekeeper Plans that Pay for Visits to
Non-Plan Doctors Private Plan that has a Book or List of Doctors Private Plan that has a Book or List of Doctors
that Pays for Non-Plan Visits
2008 Full Year Population Characteristics Data File
Ever Covered During the Year
TRIEV08 - by TRICARE MCREV08 - by Medicare MCDEV08 - by Medicaid OPAEV08 - managed care, other public insurance OPBEV08 - not managed care, other public insurance PRVEV08 - by private health insurance

2008 Full Year Population Characteristics Data File
Medicare Part D
MCRPD31X– Medicare prescription drug benefit
(Part D), Rounds 3 and 1 MCRPD42X
– Medicare prescription drug benefit (Part D), Rounds 4 and 2
MCRPD08X– Medicare prescription drug benefit
(Part D), end of year

2008 Full Year Population Characteristics Data File
DENTIN31/42/53 – round specific variables– Covered by a private health insurance plan
that included at least some dental coverage
PMEDIN31/42/53 – round specific variables– Covered by a private health insurance plan
that included at least some prescribed medicine coverage
Person Round Plan Public Use File (PRPL)
Reflects complex and dynamic relationships between people and their private insurance.
Contains records for persons with – Hospital/physician coverage – Medigap – Dental, vision, or prescription medication
coverage
Contains variables pertaining to managed care and satisfaction with plan.
Out-of-pocket premiums (starting in 2001).

MEPS-IC Survey
Nationwide, annual survey of both private and public sector establishments
Funded by the Agency for Healthcare Research and Quality (AHRQ)
Conducted by the U.S. Census Bureau Survey data available for 1996 through
2008 (not 2007)

Types of Information Collected
Establishment-level (location) characteristics
Health insurance plan characteristics
Firm-level (company) characteristics
Establishment-level (Location) Characteristics
Number of active employees Whether or not establishment offers
health insurance Number of plans offered Number of employees eligible for
health insurance and number enrolled (full-time and part-time employees separately).
Workforce characteristics

Health Insurance Plan Characteristics
Premiums (single, employee-plus-one, family)
Contributions Plan types (by type of provider
arrangement) Self-Insured / Fully-Insured Enrollments (single, employee-plus-one,
family coverage) Deductibles / Copayments
Firm (Company) Characteristics
Size
Industry
Age of firm
Retiree offerings
Employee characteristics
MEPS-IC Sample Design
Private establishments from the Census Bureau’s Business Register– Approximately 42,000 establishments sampled
State and local governments from the Census of Governments– Approximately 2,500 governmental units
sampled

MEPS-IC Sample Design
Annual estimates– National– State– some Metro areas
Data Census Bureau Confidential - Public Use Files not available
Methodology Reports available on MEPS website
Related Documents











