Agilent Dissolution Seminar Series 1 © - 2013 All Rights Reserved DISSOLUTION TECHNIQUE The Dissolution Test The analyst is responsible for verification of the physical parameters. Verify that the equipment is clean. The Dissolution Test Prepare dissolution media and properly deaerate. USP Method: Heat media to 41°C, vacuum filter through 0.45μm filter, continue to pull vacuum for 5 additional minutes. The Dissolution Test Care must be taken in measuring the dissolution media to maintain the volumetric accuracy at ±1%. Volumetric accuracy is based on dissolution media measured at room temperature. The Dissolution Test Alternatively, dissolution media may be weighed.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Agilent Dissolution Seminar Series
1© - 2013 All Rights Reserved
DISSOLUTION TECHNIQUE
The Dissolution Test
The analyst is responsible for verification of the physical parameters.
Verify that the equipment is clean.
The Dissolution Test
Prepare dissolution media and properly deaerate.
USP Method: Heat media to 41°C, vacuum filter through 0.45µm filter, continue to pull vacuum for 5 additional minutes.
The Dissolution Test
Care must be taken in measuring the dissolution media to maintain the volumetric accuracy at ±1%.
Volumetric accuracy is based on dissolution media measured at room temperature.
The Dissolution Test
Alternatively, dissolution media may be weighed.

Agilent Dissolution Seminar Series
2© - 2013 All Rights Reserved
The Dissolution Test
Measure and carefully introduce dissolution media to the vessel.
Have materials ready for the test including all sampling equipment.
The Dissolution Test
Allow media in each vessel to reach 37 °C ± 0.5 °C and use immediately.
The Dissolution Test
Always handle dosage units with gloves (not cotton), forceps or tweezers which will not scratch or damage the surface of the dosage unit.
Examine the six dosage units. Do not use chipped, cracked or capped tablets
The Dissolution Test
Option: Record the dosage unit weights? Weight is for information and investigation purposes only.
Dosage units are to be chosen at random and may not be selected or discarded based on weight.
The Dissolution Test
Have analyst notebook or dissolution worksheets for recording information. All information must be recorded directly into analyst notebooks or official batch record worksheets.
The Dissolution Test
Prepare to drop tablets. Lower paddles to proper height, or suspend baskets until ready to begin the test.
Note: Apparatus 1 baskets should be tested immediately after placing the tablet inside and clipping to the shaft. Exposure to humidity can alter test results.

Agilent Dissolution Seminar Series
3© - 2013 All Rights Reserved
The Dissolution Test
Prepare calibrated timer.
Record times as tablets are dropped.
The Dissolution Test
For the paddle apparatus, drop the dosage units into non-rotating medium. They must settle to the bottom of the vessel before rotation of the shaft
begins. Then start rotation.
Visually inspect the dosage forms for air bubbles immediately after dropping.
For the basket apparatus, lower the baskets into non-rotating medium.
When at the correct height, immediately start rotation.
Record any unusual observations.
The Dissolution Test
Most immediate release tablets disintegrate very rapidly and will reaggregate in the form of a cone on the bottom of the vessel.
As the active drug goes into solution during the dissolution process, some excipient material may be visible on the bottom of the vessel at the end of the test.
The Dissolution Test
Withdraw sample at the proper time ± 2% (a 30 minute sample must be pulled within ± 36 seconds) and filter immediately.
Temperature must be taken a second time at least, generally after the last sample is pulled and before the shaft has stopped
The samples are withdrawn at a depth halfway between the top of the paddle (or basket) and the top of the medium and not less than 1cm from the wall of the vessel.
The Dissolution Test The Dissolution Test
Filtration stops the dissolution process and defines the end of the first phase of the test which is basically a sample preparation period executed under strictly controlled physical parameters.

Agilent Dissolution Seminar Series
4© - 2013 All Rights Reserved
The Dissolution Test
Once the sample has been filtered the second phase of the testing begins to determine the analytical concentration of the sample.
Analytical concentration is generally determined through UV-Vis spectroscopy or HPLC analysis. HPLC is primarily used for drug products
containing multiple active components or for stability testing.
The responses from the analytical finish will be used to calculate the amount
of sample released from the dosage form within the specific time interval.
Calculation
The sample concentration will be calculated against a reference standard of known concentration. The result in % label claim will be compared to
acceptable ranges stated in the dissolution method or monograph.
The following calculation provides results in % label claim (%LC)
100(mg) Claim Label
(mL) Vol. Sample
(mL) Vol. Standard
(mg) Wt.Standard
Abs. Standard
Abs. Sample×××
What is Q?
Q, as it relates to dissolution is commonly used in the USP for immediate release and delayed release dosage forms.
The quantity of Q is the amount of dissolved active ingredient specified in the individual monograph expressed as a percentage of the labeled content.
Immediate Release Forms – Acceptance Table USP <711>
Stage Number Tested Acceptance Criteria
S1 6 Each unit is ≥ Q + 5%.
S2 6 Average of 12 units (S1 + S2) is ≥ Q and no unit is < Q – 15%.
S3 12 Average of 24 units (S1 + S2 + S3) is ≥ Q, not more than 2 units are < Q – 15% and no
single unit is less than Q – 25%.
If a sample fails either Stage S1 or S2, proceed to the next stage and test
the number of units indicated.
Delayed Release Forms – Acid Stage USP <711>
•USP Delayed Release Dosage Forms – Method A:
•Media is 750 mL of 0.1N HCl
•Samples are removed for analysis after 2 hours ± 2%.
Delayed Release Forms – Acid Stage Acceptance Table USP <711>
Stage Number Tested
Acceptance Criteria
A1 6 No individual value exceeds 10% dissolved.
A2 6 Average of 12 units (A1 + A2) is no more than 10% dissolved and no single
unit is greater than 25% dissolved.
A3 12 Average of 24 units (A1 + A2 + A3) is not more than 10% dissolved and no single
unit is more than 25% dissolved.
If a sample fails either Stage A1 or A2, proceed to the next stage
and test the number of units indicated.
Agilent Dissolution Seminar Series
5© - 2013 All Rights Reserved
Delayed Release Forms - Buffer Stage
•Within 5 minutes of withdrawing the acid stage sample aliquots, add 250 mL of 0.20-M tribasic sodium phosphate, adjusting to pH + 0.05 at 37 °C while stirring at the specified rate.
•Dissolution continues for 0.75 h (or per monograph) or less.
•Sample aliquots are then analyzed with Q being the total % dissolved for both acid and buffer stages.
Delayed Release Forms - Buffer Stage Acceptance Table USP <711>
Stage Number Tested
Acceptance Criteria
B1 6 Each unit is ≥ Q + 5%.
B2 6 Average of 12 units (B1 + B2) is ≥ Q and no unit is < Q – 15%.
B3 12 Average of 24 units (B1 + B2 + B3) is ≥Q, not more than 2 units are < Q –
15% and no single unit is less than Q –
25%.
If a sample fails either Stage B1 or B2, proceed to the next stage
and test the number of units indicated.
Delayed Release Forms – Acid StageUSP <711>
•USP Delayed Release Dosage Forms – Method B:
•Media is 1000 mL of 0.1N HCl
•Samples are removed for analysis after 2 hours ± 2%.
Delayed Release Forms – Buffer StageUSP <711>
•USP Delayed Release Dosage Forms – Method B:
•Drain the acid from the original vessel and replace with
1000mL pH6.8 phosphate buffer pre equilibrated at 37°C
•or switch the dosage form to a second vessel containing the
phosphate buffer
USP APPARATUS 3 AND 4FLOW-THROUGH APPARATUS
USP Apparatus 3 & 4
USP Apparatus 3 & 4 are now found in USP General Chapter <711> Dissolution
USP Apparatus 3 is called the Reciprocating Cylinder Apparatus
USP Apparatus 4 is called the Flow-Through Cell
Agilent Dissolution Seminar Series
6© - 2013 All Rights Reserved
USP APPARATUS 3THE RECIPROCATING CYLINDER
USP Apparatus 3
General Apparatus 3 Description
Reciprocating cylinder
Vessels
Current physical parameters
USP calibration requirements
Typical products tested
Non-Compendial variations
USP Apparatus 3
General Apparatus 3 Description
A presentation at the 1980 Federation Internationale Pharmaceutique (FIP)
drew attention to acute problems associated with USP Apparatus 1 and 2 dissolution results. The conference inspired the concept for the USP
Apparatus 3.
USP Apparatus 3
General Apparatus 3 Description
The USP Apparatus 3 (Bio-Dis) is an excellent apparatus for developing
controlled release products because it can quickly and easily expose products to mechanical and physiochemical conditions which may influence
the release of the products in the GI tract.
USP Apparatus 3
General Apparatus 3 Description
The Bio-Dis Extended Release Tester was designed to test the dissolution
rates of extended release products or any dosage form requiring release profiling at multiple pH levels.
The ability to transfer the product from one pH to another makes it an
excellent candidate for delayed release products.
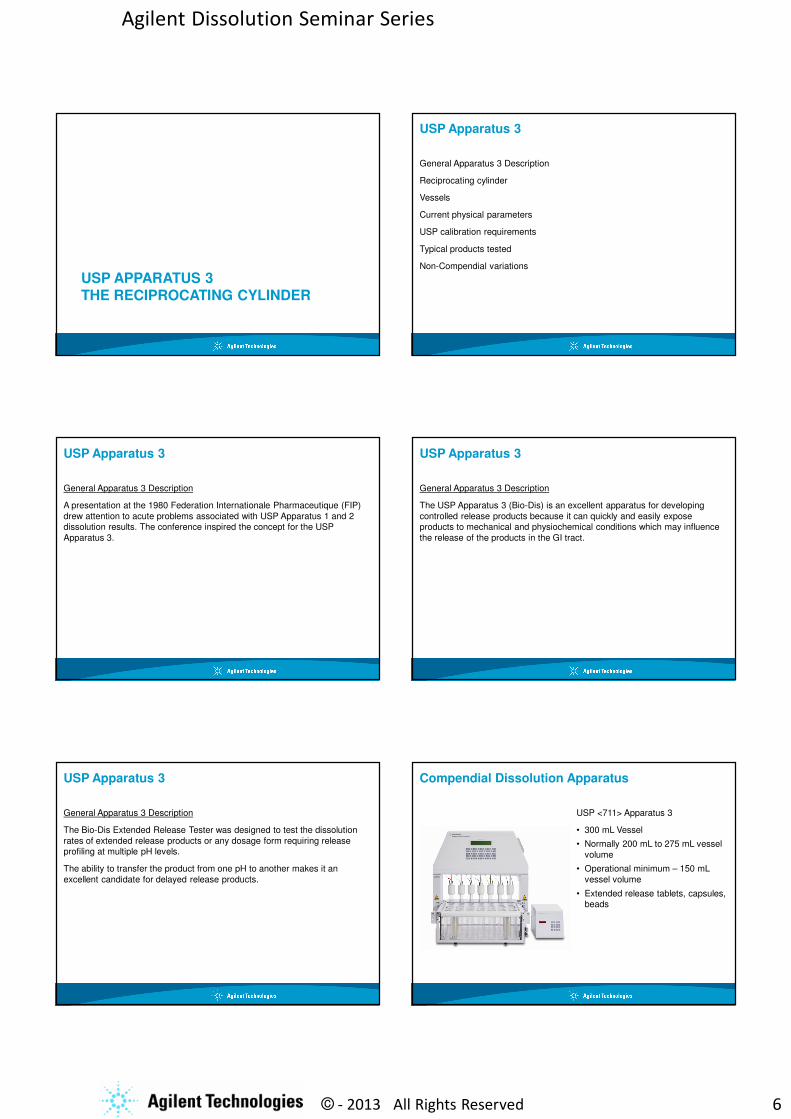
Compendial Dissolution Apparatus
USP <711> Apparatus 3
• 300 mL Vessel
• Normally 200 mL to 275 mL vessel
volume
• Operational minimum – 150 mL
vessel volume
• Extended release tablets, capsules, beads

Agilent Dissolution Seminar Series
7© - 2013 All Rights Reserved
USP Apparatus 3
General Apparatus 3 Description
The reciprocating cylinder apparatus consists of sets of cylindrical, flat
bottom glass vessels with corresponding sets of reciprocating cylinders.
USP Apparatus 3
General Apparatus 3 Description
A motor and drive assembly reciprocate the cylinders vertically inside the vessels.
The cylinders are allowed to move from row to row to expose the undissolved drug product to various pH levels.
USP Apparatus 3
Reciprocating Cylinders
The reciprocating cylinders are glass tubes fitted with top and bottom caps containing screens designed to contain the product under evaluation.
USP Apparatus 3
Reciprocating Cylinders
As the cylinder reciprocated vertically the drug product is constantly exposed to media contained in the vessel.
USP Apparatus 3
Vessels
This picture shows the Apparatus 3 with automatic sampling.
The last position on each row contains a blank and standard tube to be sampled for automated analysis.

Agilent Dissolution Seminar Series
8© - 2013 All Rights Reserved
USP Apparatus 3
Current Physical Parameters and Tolerances
Temperature 37 ± 0.5 °C
Dip rate (DPM) ± 5% of set speed
Stroke Distance 10.0 ± 0.1 cm
Bottom screen Per method
Top screen Per method (optional)
Timepoints ± 2% of specified time
USP PVT Chlorpheniramine Maleate – No longer required per USP 2012. USP working to replace the PVT since it is no longer available.
USP Apparatus 3
USP Calibration Requirements
Originally, Apparatus Suitability was demonstrated with USP
Chlorpheniramine Maleate tablets
This test was withdrawn from 1st February 2012
USP APPARATUS 4THE FLOW-THROUGH CELL
USP Apparatus 4
General apparatus description
Flow-through cell
Current physical parameters
Typical products tested
USP Apparatus 4
General Apparatus Description
The flow-through cell was developed for lipophilic solid dosage forms such as
suppositories and soft capsules. It is made up of three transparent parts which fit into each other.
The lower part consists of two adjacent chambers connected to an overflow
device.
USP Apparatus 4
General Apparatus Description
The dissolution media passes into the lower part of the chamber then flows
upward to an exit in the upper chamber which leads to a filter assembly.
The middle part of the cell has a cavity and holder designed to contain the dosage unit.

Agilent Dissolution Seminar Series
9© - 2013 All Rights Reserved
USP Apparatus 4
General Apparatus Description
Initially designed for poorly soluble extended release compounds
Typical flow rates from 4 mL per minute up to 16 mL per minute
A closed system with a small media reservoir could reduce volume to 100 mL
Extended release tablets, beads, suppositories and implants
USP Apparatus 4
General Apparatus Description
With a flow through system the specimen is placed in a small column which is continuously flushed with a stream of fluid, simultaneously providing the medium and the mechanical agitation for dissolution of the drug substance.
USP Apparatus 4 can be run as an open or closed system. The open system provides a large volume of multiple solvents as needed.
USP Apparatus 4
Current Physical Parameters and Tolerances
Temperature 37 ± 0.5 °C
Pump rate 240 - 960 mL/hour
Std flow rates 4,8,16 mL/minute
Flow rate accuracy ± 5%
Pulsation 120 ± 10 pulses/min
Cell Diameters 12 and 22.6mm
USP APPARATUS 5, 6, AND 7PADDLE OVER DISK, ROTATING CYLINDER, RECIPROCATING HOLDER
USP Apparatus 5, 6 and 7
These apparatus are primarily used for the analysis of transdermal systems and are decscribed in the USP general chapter <724> Drug Release.
The transdermal systems are typically run at 32 °C, similar to the temperature of the skin.
Transdermal Delivery
Prior to the 1980s, the skin was seldom regarded as a suitable route for administration of drugs to systemic circulation.
However, the transdermal route offered several potential advantages for the systemic delivery of drugs.

Agilent Dissolution Seminar Series
10© - 2013 All Rights Reserved
Transdermal Delivery
Drugs with narrow therapeutic indices can be good candidates for transdermal route because of the absence of the peak and valley feature
common to conventional oral dosage forms.
Transdermal systems provide controlled blood levels of potent drugs.
Transdermal Delivery
Lastly, because of its noninvasive delivery, transdermal patches may be removed easily if toxicity or side effects begin to appear, an advantage over
both the oral and the parenteral routes.
Transdermal Advantages
The employment of the skin as a portal of drug entry into the systemic circulation provides a convenient route for the sustained administration of
a premeasured amount of drug.
Because of the long-acting feature, the patient is always protected,
especially during sleep.
Transdermal Advantages
Because the drug reaches the blood circulation directly, it does not have to travel through the gastrointestinal tract, where it can degrade, suffer from
poor absorption or cause distress.
Drugs avoid the first pass effect, common to the oral route, where some
drugs are metabolized partially by the liver before reaching systemic
circulation.
USP APPARATUS 5PADDLE OVER DISK
USP Apparatus 5
The apparatus is used as described under <711> Dissolution apparatus 2 paddle with the exception of a stainless steel disk holder placed in the bottom
of the vessel.
The transdermal patch is attached to a disk, composed of a stainless steel
support screen, metal ring and Teflon ring.
This system ensures that the release surface of the system is as flat as
possible.

Agilent Dissolution Seminar Series
11© - 2013 All Rights Reserved
USP Apparatus 5 USP Apparatus 5
Current Physical Parameters and Tolerances
Dimensions per USP
Paddle Height 25mm ± 2 mm from disk
Centering ± 2 mm center line
Speed ± 4% of set speed
Vessel Temp. 32 ± 0.5°C
Timepoints ± 2% or ± 15 minutes of specified time (lesser)
USP APPARATUS 6ROTATING CYLINDER
USP Apparatus 6
Use the vessel assembly from Apparatus 1 and 2 as described under <711> Dissolution, except to replace the shaft with a stainless steel cylinder stirring
element and to maintain the temperature at 32 ± 0.5°C.
USP Apparatus 6
The dosage unit is placed on the cylinder at the beginning of each test.
The distance between the inside bottom of the vessel and the cylinder is maintained at 25 ± 2 mm during the test.
USP Apparatus 6

Agilent Dissolution Seminar Series
12© - 2013 All Rights Reserved
USP Apparatus 6
Current Physical Parameters and Tolerances
Dimensions per USP
Height 25 mm ± 2 mm
Centering ± 2 mm center line
Speed ± 4% of set speed
Vessel Temp. 32 ± 0.5°C
Timepoints ± 2% or ± 15 minutes of specified time (lesser)
USP Apparatus 6
Typical Test System Preparation
Remove the system from the package.
Remove the protective liner from the system.
Place the adhesive side on a piece of Cuprophan that is not less than 1 cm
larger on all sides of the system perimeter.
USP Apparatus 6
USP Apparatus 6
Place the system on a clean surface with the Cuprophan side down.
Apply a suitable adhesive to the exposed Cuprophan borders, and back if
necessary (Dow Corning , 355 medical adhesive 18.5% in Freon 113, or equivalent).
USP Apparatus 6
Carefully apply the adhesive-coated side of the system to the
exterior of the cylinder with the
long axis of the system fitting around the circumference of the
cylinder.

Agilent Dissolution Seminar Series
13© - 2013 All Rights Reserved
USP Apparatus 6
Press the Cuprophan covering to remove trapped air bubbles.
Place the cylinder in the dissolution apparatus, lower into
the media and immediately rotate
at the specified speed.
USP APPARATUS 7RECIPROCATING CYLINDER
USP Apparatus 7
Also known as the “Alza apparatus” USP apparatus 7 has evolved to handle not only transdermal apparatus but other sustained release products.
The apparatus utilizes sets of volumetrically or gravimetrically calibrated tubes and a mechanical device capable of reciprocating the specific holders
vertically in the tubes containing dissolution medium.
Compendial Dissolution Apparatus
USP <724> Apparatus 7
• Typical 40 mL – 50 mL
• Operational minimum around 25 mL
• Modifications have been made to accommodate 300 mL vessels
• Extended release tablets, capsules,
beads, implants, transdermals, osmotic pumps, and other novel
dosage forms
USP Apparatus 7
Current Physical Parameters and Tolerances
Temperature 32±0.5°C
Dip rate 30 DPM
Stroke Distance 2 cm
Holder Per USP
Timepoints ± 2% of specified time

Agilent Dissolution Seminar Series
14© - 2013 All Rights Reserved
MODIFICATION OF USP APPARATUS 7 FOR DRUG ELUTING STENTS
What is a Stent
A stent is a wire metal mesh tube used to prop open an artery during angioplasty.
The stent is collapsed to a small diameter on a balloon catheter. It is then moved into the area of blockage, When the balloon is inflated, the stent expands, locks in place as a scaffold. This holds the artery open.
The stent stays in the artery permanently, holds it open, improves the blood flow and relieves the symptoms
Angioplasty
A tiny balloon that presses the plaque blockage against the artery so that
blood may flow more freely through
the vessel
Stenting
A stent is inserted into an artery after angioplasty to help ensure that blood continues to flow freely through the vessel and to reduce the chance that plaque will block the artery again.
Development of Coated and Drug-Eluting Stents
Physicians and companies began testing a variety of drugs that were
known to interrupt the biological
processes that caused restenosis. Stents were coated with these drugs,
sometimes imbedded in a thin
polymer for time-release, and clinical trials were begun.
Case StudyDrug Eluting Stents
• Initially, most drug eluting stent manufacturers utilized a rocking “incubator,” shaker tables or USP Apparatus 4 or 7 as their instruments of choice.
• Modifications to App 7 allowed smaller volumes and automated sampling.
• Custom holders had been designed for various stents and other medical devices.

Agilent Dissolution Seminar Series
15© - 2013 All Rights Reserved
Challenges with Traditional Apparatus 7
• Instrument was not originally designed for extremely low volumes.
• Evaporation control was difficult due to reciprocating rod (which held the
dosage form/device). Many methods allowed for media addition (“top up”)
prior to analysis.
• Initial design was difficult to automate The smaller volume tubes had
smaller diameter openings; as a result, clearance was tight for sample and return lines.
• The requirement for testing 12 stents at a time lead to the development of a 12 place collector.
Early DevelopmentProof of Concept Unit
The intent was to develop a prototype inexpensively in order to test:
1) theory of operation
2) conformance with USP specifications and
3) eliminate problems associated with past units.
Utilized existing hardware with modified firmware.
The unit was built for manual testing, sampling and media changes where done by hand
Proof of ConceptApparatus 7 with Magnetic Drive
How did it work?
• Each rack was designed for a specific size stent/tube
• The rack reciprocated the USP specified 2 cm distance
• Each rack had a magnetic plate which drove the stent holder within each tube
Design Advantages
• Matched USP specifications for Apparatus 7
• Able to handle small volumes (5 -
50mls)
• Inert materials used in design
allowed solvents to be used
• Able to change DPM to more
closely match in-vivo release
• Provided a tool for IVIVC work as
well as accelerated QC release testing
• High throughput in a single tester (customize the number of available
rows)
• Excellent temperature control, allows elevated temperatures
• Sealed system; essentially no evaporation
• Disposable tubes (no dead volume or cleaning issues to contend with)
Small Volume Drug Release Apparatus Prototype to Commercial Product
Agilent 400-DS
• Parent module has the ability to test 13 samples and incorporates the ability to access up to four types of media.
• Sample collection is built into each module.
• Additional modules, each capable of testing 13 samples, can be added to the parent module to extend testing capacity to 52 samples.
• Each unit is individually operated and controlled via the software provided.

Agilent Dissolution Seminar Series
16© - 2013 All Rights Reserved
400-DS: Dissolution Cell Design
Dissolution Cell
Heater
Jacket
Temperature
Probe
Media / Sample
Port
• A glass tube (dissolution cell), open at both ends, is placed atop a base seal
• A heating jacket fits around each tube (no water bath is used)
• The sample holder is inserted and the tube is capped
• All media fill and sampling is done via the bottom of the tube via the media/sample port
• Media temperature is recorded and controlled through the built-in temperature probe
• Dissolution cells are disposable and can be readily replaced when necessary
400-DS Temperature Control
• External jacket designed to provide uniform heating of the test media
• Temperature feedback provided by internal temperature probe in the base of each chamber
• No water bath!
Dissolution cells -5 mL and 10 mL
Heater jackets surround the dissolution cells
Temperature probe and sampling port at bottom of the dissolution cells
Reciprocating holder for drug-eluting stents of various lengths
400-DS – Improved Test Performance
The 400-DS successfully addresses the many challenges associated with the testing of combination products:
• Small Volume
• Low Evaporative Loss
• Use of organic solvent media
• Automated Sampling and Media Replacement
• Bathless
• Regulatory Compliance
• Small footprint
400-DS Reciprocating Holder Options
400-DS Contact Lens Holder
Related Documents











