Age, outcomes, and treatment effects of fibrinolytic and antithrombotic combinations: Findings from Assessment of the Safety and Efficacy of a New Thrombolytic (ASSENT)-3 and ASSENT-3 PLUS Peter R. Sinnaeve, MD, PhD, a Yao Huang, PhD, b Kris Bogaerts, PhD, a Alec Vahanian, MD, PhD, c Jennifer Adgey, MD, PhD, d Paul W. Armstrong, MD, e Lars Wallentin, MD, f Frans J. Van de Werf, MD, PhD, a Christopher B. Granger, MD, b on behalf of the ASSENT-3 and ASSENT-3 PLUS investigators Leuven, Belgium; Durham, NC; Paris, France; Belfast, Northern Ireland; Alberta, Edmonton, Canada; and Uppsala, Sweden Background Elderly patients with acute myocardial infarction are at particularly high risk for death and bleeding complications. The efficacy and safety of antithrombotic strategies in these patients remain unclear. Methods To provide more insight into the risk and benefit of antithrombotic strategies in the elderly, we examined patients from the ASSENT-3 and ASSENT-3 PLUS trials with STEMI who were treated with tenecteplase (TNK) and unfractionated heparin (UFH) or enoxaparin, or half-dose TNK with abciximab and reduced-dose UFH. Results Older patients had a higher risk profile, and lower use of concomitant therapies and revascularization procedures. We found an interaction between age and treatment effect for the efficacy end point ( P = .0007) and the efficacy plus safety end point ( P b .0001). Younger patients (b65 years) had a lower risk of the composite efficacy plus safety end point with enoxaparin (relative risk [RR] 0.84, 95% CI 0.74-0.94) or abciximab (RR 0.79, 95% CI 0.69-0.90) compared with UFH. In patients N65 years of age, the benefit of enoxaparin appeared to be offset by an increased risk of bleeding complications. The risk of the efficacy plus safety end point tended to be higher in elderly patients receiving abciximab and half-dose TNK (RR 1.18, 95% CI 0.91-1.51 for 76-85 years of age and RR 1.48, 95% CI 0.88-2.49 for N85 years of age). Conclusions Although TNK with either enoxaparin or abciximab appeared to be more effective than with standard UHF in younger patients, these combinations tended to be less effective and even may be unsafe in the elderly. Development of new combination strategies and dosing schemes of fibrinolytics and antithrombotics with improved efficacy and safety in the elderly remains a high priority. (Am Heart J 2006;152:684.e12684.e9.) Patients N75 years of age constitute 6% of the US population, but they represent over half of all deaths after a myocardial infarction (MI). Increasing age is indeed the most important adverse prognostic factor after an MI. 1,2 Demographic risk factors such as female sex, low body weight, anterior wall infarction and previous MI, Killip class III to IV, and hypertension tend be more prevalent in the elderly population, which in part explains their poorer outcome. 3-8 Elderly patients are also more likely to have adverse events, especially intracranial hemorrhage (ICH) and other major bleeding complications. 8 Thus, the elderly present an important challenge to the clinician: they are both in greatest need of more effective antithrombotic therapy and at greatest risk of complications from the therapy. More aggressive antithrombotic therapies have been introduced in an effort to decrease the rate of recurrent ischemia and reinfarction after thrombolysis in patients with ST-elevation MI. Glycoprotein IIb/IIIa inhibitors have been combined with reduced-dose lytics to offset the increased risk of bleeding complications, especially in the elderly. 9-12 In the ASSENT-3 trial, conjunctive therapy with enoxaparin and full-dose TNK, or abcix- imab and half-dose TNK reduced the composite end point of death, reinfarction, and refractory angina compared with unfractionated heparin (UFH) in patients treated with TNK (relative risk 0.74, 95% CI 0.63-0.87 for enoxaparin and relative risk 0.72, 95% CI 0.61-84 for abciximab, respectively). 12 Based on dividing age by From the a Department of Cardiology, University Hospital Gasthuisberg, Leuven, Belgium, b Duke Clinical Research Center, Durham, NC, c Cardiology Department, Bichat Hospital, Paris, France, d Regional Medical Cardiology Centre, Royal Victoria Hospital, Belfast, Northern Ireland, e Department of Cardiology, University of Alberta, Edmonton, Canada, and f Department of Cardiology University Hospital, Uppsala, Sweden. Submitted October 5, 2005; accepted July 3, 2006. Reprint requests: Peter R. Sinnaeve, MD, PhD, Department of Cardiology, University Hospital Gasthuisberg, Herestraat 49, 3000 Leuven, Belgium. E-mail: [email protected] 0002-8703/$ - see front matter n 2006, Mosby, Inc. All rights reserved. doi:10.1016/j.ahj.2006.07.005

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Age, outcomes, and treatment effects of fibrinolyticand antithrombotic combinations: Findings fromAssessment of the Safety and Efficacy of a NewThrombolytic (ASSENT)-3 and ASSENT-3 PLUSPeter R. Sinnaeve, MD, PhD,a Yao Huang, PhD,b Kris Bogaerts, PhD,a Alec Vahanian, MD, PhD,c
Jennifer Adgey, MD, PhD,d Paul W. Armstrong, MD,e Lars Wallentin, MD,f Frans J. Van de Werf, MD, PhD,a
Christopher B. Granger, MD,b on behalf of the ASSENT-3 and ASSENT-3 PLUS investigators Leuven, Belgium;Durham, NC; Paris, France; Belfast, Northern Ireland; Alberta, Edmonton, Canada; and Uppsala, Sweden
Background Elderly patients with acute myocardial infarction are at particularly high risk for death and bleedingcomplications. The efficacy and safety of antithrombotic strategies in these patients remain unclear.
Methods To provide more insight into the risk and benefit of antithrombotic strategies in the elderly, we examinedpatients from the ASSENT-3 and ASSENT-3 PLUS trials with STEMI who were treated with tenecteplase (TNK) andunfractionated heparin (UFH) or enoxaparin, or half-dose TNK with abciximab and reduced-dose UFH.
Results Older patients had a higher risk profile, and lower use of concomitant therapies and revascularizationprocedures. We found an interaction between age and treatment effect for the efficacy end point ( P = .0007) and theefficacy plus safety end point ( P b .0001). Younger patients (b65 years) had a lower risk of the composite efficacy plus safetyend point with enoxaparin (relative risk [RR] 0.84, 95% CI 0.74-0.94) or abciximab (RR 0.79, 95% CI 0.69-0.90) comparedwith UFH. In patients N65 years of age, the benefit of enoxaparin appeared to be offset by an increased risk of bleedingcomplications. The risk of the efficacy plus safety end point tended to be higher in elderly patients receiving abciximab andhalf-dose TNK (RR 1.18, 95% CI 0.91-1.51 for 76-85 years of age and RR 1.48, 95% CI 0.88-2.49 for N85 years of age).
Conclusions Although TNK with either enoxaparin or abciximab appeared to be more effective than withstandard UHF in younger patients, these combinations tended to be less effective and even may be unsafe in the elderly.Development of new combination strategies and dosing schemes of fibrinolytics and antithrombotics with improvedefficacy and safety in the elderly remains a high priority. (Am Heart J 2006;152:684.e12684.e9.)
Patients N75 years of age constitute 6% of the US
population, but they represent over half of all deaths
after a myocardial infarction (MI). Increasing age is
indeed the most important adverse prognostic factor
after an MI.1,2 Demographic risk factors such as female
sex, low body weight, anterior wall infarction and
previous MI, Killip class III to IV, and hypertension tend
be more prevalent in the elderly population, which in
part explains their poorer outcome.3-8 Elderly patients
From the aDepartment of Cardiology, University Hospital Gasthuisberg, Leuven, Belgium,bDuke Clinical Research Center, Durham, NC, cCardiology Department, Bichat Hospital,
Paris, France, dRegional Medical Cardiology Centre, Royal Victoria Hospital, Belfast,
Northern Ireland, eDepartment of Cardiology, University of Alberta, Edmonton, Canada,
and fDepartment of Cardiology University Hospital, Uppsala, Sweden.
Submitted October 5, 2005; accepted July 3, 2006.
Reprint requests: Peter R. Sinnaeve, MD, PhD, Department of Cardiology, University
Hospital Gasthuisberg, Herestraat 49, 3000 Leuven, Belgium.
E-mail: [email protected]
0002-8703/$ - see front matter
n 2006, Mosby, Inc. All rights reserved.
doi:10.1016/j.ahj.2006.07.005
are also more likely to have adverse events,
especially intracranial hemorrhage (ICH) and other
major bleeding complications.8 Thus, the elderly present
an important challenge to the clinician: they are both in
greatest need of more effective antithrombotic therapy
and at greatest risk of complications from the therapy.
More aggressive antithrombotic therapies have been
introduced in an effort to decrease the rate of recurrent
ischemia and reinfarction after thrombolysis in patients
with ST-elevation MI. Glycoprotein IIb/IIIa inhibitors
have been combined with reduced-dose lytics to offset
the increased risk of bleeding complications, especially
in the elderly.9-12 In the ASSENT-3 trial, conjunctive
therapy with enoxaparin and full-dose TNK, or abcix-
imab and half-dose TNK reduced the composite end
point of death, reinfarction, and refractory angina
compared with unfractionated heparin (UFH) in patients
treated with TNK (relative risk 0.74, 95% CI 0.63-0.87 for
enoxaparin and relative risk 0.72, 95% CI 0.61-84 for
abciximab, respectively).12 Based on dividing age by
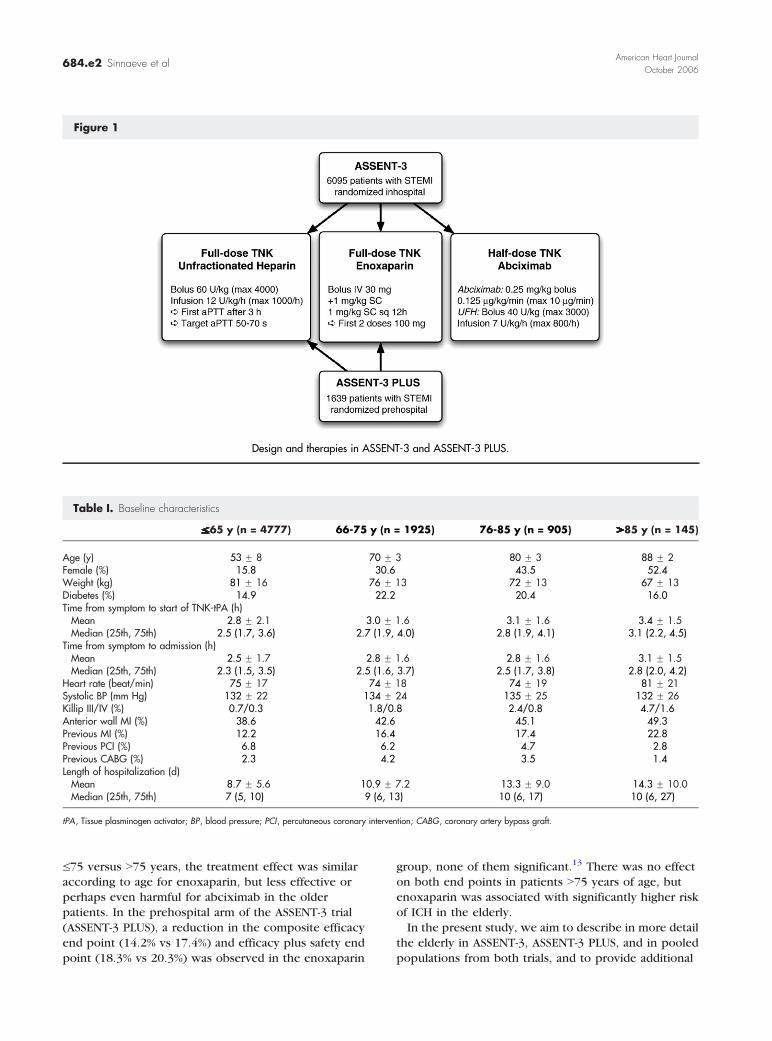
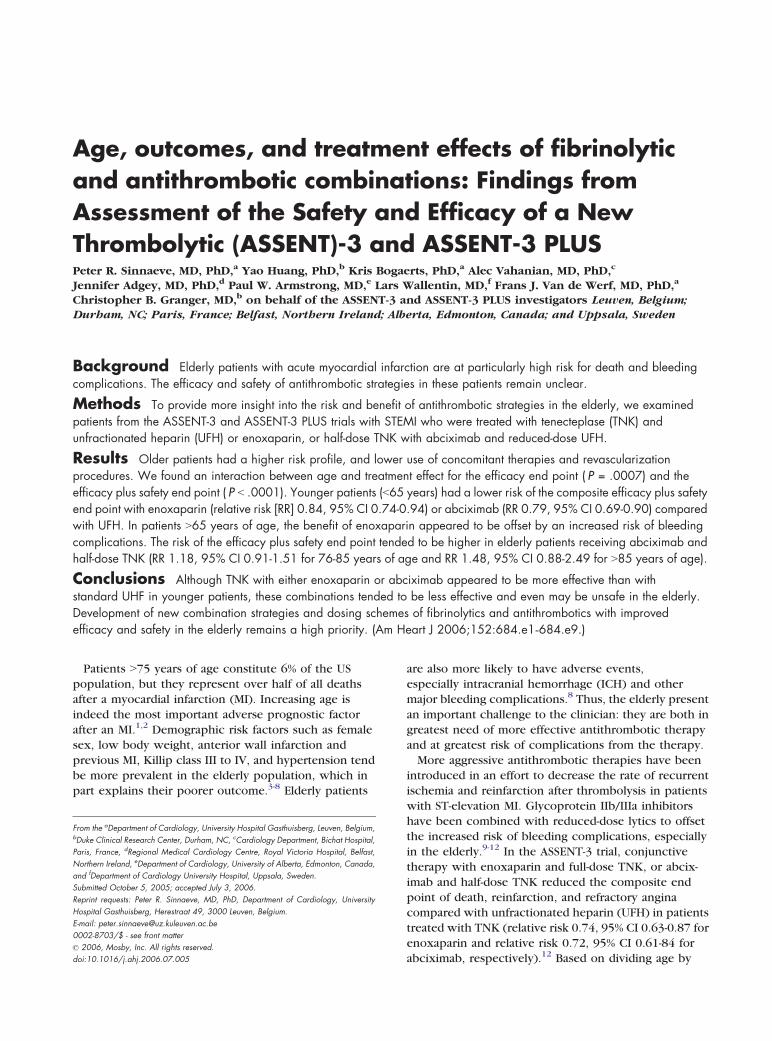
Figure 1
Design and therapies in ASSENT-3 and ASSENT-3 PLUS.
Table I. Baseline characteristics
VVVVVVVVVVVVVVVVVVVVVVVVVVVVV__65 y (n = 4777) 66-75 y (n = 1925) 76-85 y (n = 905) NNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNN85 y (n = 145)
Age (y) 53 F 8 70 F 3 80 F 3 88 F 2Female (%) 15.8 30.6 43.5 52.4Weight (kg) 81 F 16 76 F 13 72 F 13 67 F 13Diabetes (%) 14.9 22.2 20.4 16.0Time from symptom to start of TNK-tPA (h)
Mean 2.8 F 2.1 3.0 F 1.6 3.1 F 1.6 3.4 F 1.5Median (25th, 75th) 2.5 (1.7, 3.6) 2.7 (1.9, 4.0) 2.8 (1.9, 4.1) 3.1 (2.2, 4.5)
Time from symptom to admission (h)Mean 2.5 F 1.7 2.8 F 1.6 2.8 F 1.6 3.1 F 1.5Median (25th, 75th) 2.3 (1.5, 3.5) 2.5 (1.6, 3.7) 2.5 (1.7, 3.8) 2.8 (2.0, 4.2)
Heart rate (beat/min) 75 F 17 74 F 18 74 F 19 81 F 21Systolic BP (mm Hg) 132 F 22 134 F 24 135 F 25 132 F 26Killip III/IV (%) 0.7/0.3 1.8/0.8 2.4/0.8 4.7/1.6Anterior wall MI (%) 38.6 42.6 45.1 49.3Previous MI (%) 12.2 16.4 17.4 22.8Previous PCI (%) 6.8 6.2 4.7 2.8Previous CABG (%) 2.3 4.2 3.5 1.4Length of hospitalization (d)
Mean 8.7 F 5.6 10.9 F 7.2 13.3 F 9.0 14.3 F 10.0Median (25th, 75th) 7 (5, 10) 9 (6, 13) 10 (6, 17) 10 (6, 27)
tPA, Tissue plasminogen activator; BP, blood pressure; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft.
American Heart Journal
October 2006684.e2 Sinnaeve et al
V75 versus N75 years, the treatment effect was similar
according to age for enoxaparin, but less effective or
perhaps even harmful for abciximab in the older
patients. In the prehospital arm of the ASSENT-3 trial
(ASSENT-3 PLUS), a reduction in the composite efficacy
end point (14.2% vs 17.4%) and efficacy plus safety end
point (18.3% vs 20.3%) was observed in the enoxaparin
group, none of them significant.13 There was no effect
on both end points in patients N75 years of age, but
enoxaparin was associated with significantly higher risk
of ICH in the elderly.
In the present study, we aim to describe in more detail
the elderly in ASSENT-3, ASSENT-3 PLUS, and in pooled
populations from both trials, and to provide additional
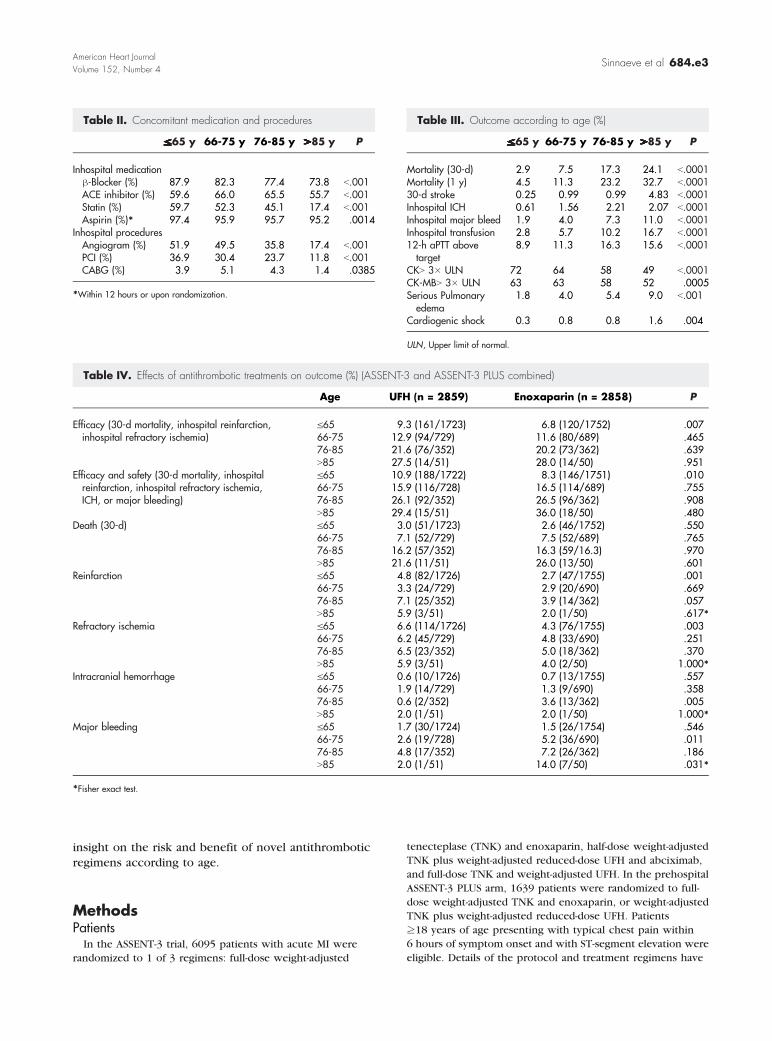
Table III. Outcome according to age (%)
VVVVVVVVVVVVVVVVVVVVVVVVVVVVV__65 y 66-75 y 76-85 y NNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNN85 y P
Mortality (30-d) 2.9 7.5 17.3 24.1 b.0001Mortality (1 y) 4.5 11.3 23.2 32.7 b.000130-d stroke 0.25 0.99 0.99 4.83 b.0001Inhospital ICH 0.61 1.56 2.21 2.07 b.0001Inhospital major bleed 1.9 4.0 7.3 11.0 b.0001Inhospital transfusion 2.8 5.7 10.2 16.7 b.000112-h aPTT above
target8.9 11.3 16.3 15.6 b.0001
CKN 3� ULN 72 64 58 49 b.0001CK-MBN 3� ULN 63 63 58 52 .0005Serious Pulmonary
edema1.8 4.0 5.4 9.0 b.001
Cardiogenic shock 0.3 0.8 0.8 1.6 .004
ULN, Upper limit of normal.
Table II. Concomitant medication and procedures
VVVVVVVVVVVVVVVVVVVVVVVVVVVVV__65 y 66-75 y 76-85 y NNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNN85 y P
Inhospital medicationh-Blocker (%) 87.9 82.3 77.4 73.8 b.001ACE inhibitor (%) 59.6 66.0 65.5 55.7 b.001Statin (%) 59.7 52.3 45.1 17.4 b.001Aspirin (%)* 97.4 95.9 95.7 95.2 .0014
Inhospital proceduresAngiogram (%) 51.9 49.5 35.8 17.4 b.001PCI (%) 36.9 30.4 23.7 11.8 b.001CABG (%) 3.9 5.1 4.3 1.4 .0385
*Within 12 hours or upon randomization.
Table IV. Effects of antithrombotic treatments on outcome (%) (ASSENT-3 and ASSENT-3 PLUS combined)
Age UFH (n = 2859) Enoxaparin (n = 2858) P
Efficacy (30-d mortality, inhospital reinfarction,inhospital refractory ischemia)
V65 9.3 (161/1723) 6.8 (120/1752) .00766-75 12.9 (94/729) 11.6 (80/689) .46576-85 21.6 (76/352) 20.2 (73/362) .639N85 27.5 (14/51) 28.0 (14/50) .951
Efficacy and safety (30-d mortality, inhospitalreinfarction, inhospital refractory ischemia,ICH, or major bleeding)
V65 10.9 (188/1722) 8.3 (146/1751) .01066-75 15.9 (116/728) 16.5 (114/689) .75576-85 26.1 (92/352) 26.5 (96/362) .908N85 29.4 (15/51) 36.0 (18/50) .480
Death (30-d) V65 3.0 (51/1723) 2.6 (46/1752) .55066-75 7.1 (52/729) 7.5 (52/689) .76576-85 16.2 (57/352) 16.3 (59/16.3) .970N85 21.6 (11/51) 26.0 (13/50) .601
Reinfarction V65 4.8 (82/1726) 2.7 (47/1755) .00166-75 3.3 (24/729) 2.9 (20/690) .66976-85 7.1 (25/352) 3.9 (14/362) .057N85 5.9 (3/51) 2.0 (1/50) .617*
Refractory ischemia V65 6.6 (114/1726) 4.3 (76/1755) .00366-75 6.2 (45/729) 4.8 (33/690) .25176-85 6.5 (23/352) 5.0 (18/362) .370N85 5.9 (3/51) 4.0 (2/50) 1.000*
Intracranial hemorrhage V65 0.6 (10/1726) 0.7 (13/1755) .55766-75 1.9 (14/729) 1.3 (9/690) .35876-85 0.6 (2/352) 3.6 (13/362) .005N85 2.0 (1/51) 2.0 (1/50) 1.000*
Major bleeding V65 1.7 (30/1724) 1.5 (26/1754) .54666-75 2.6 (19/728) 5.2 (36/690) .01176-85 4.8 (17/352) 7.2 (26/362) .186N85 2.0 (1/51) 14.0 (7/50) .031*
*Fisher exact test.
American Heart Journal
Volume 152, Number 4Sinnaeve et al 684.e3
insight on the risk and benefit of novel antithrombotic
regimens according to age.
MethodsPatients
In the ASSENT-3 trial, 6095 patients with acute MI were
randomized to 1 of 3 regimens: full-dose weight-adjusted
tenecteplase (TNK) and enoxaparin, half-dose weight-adjusted
TNK plus weight-adjusted reduced-dose UFH and abciximab,
and full-dose TNK and weight-adjusted UFH. In the prehospital
ASSENT-3 PLUS arm, 1639 patients were randomized to full-
dose weight-adjusted TNK and enoxaparin, or weight-adjusted
TNK plus weight-adjusted reduced-dose UFH. Patients
z18 years of age presenting with typical chest pain within
6 hours of symptom onset and with ST-segment elevation were
eligible. Details of the protocol and treatment regimens have
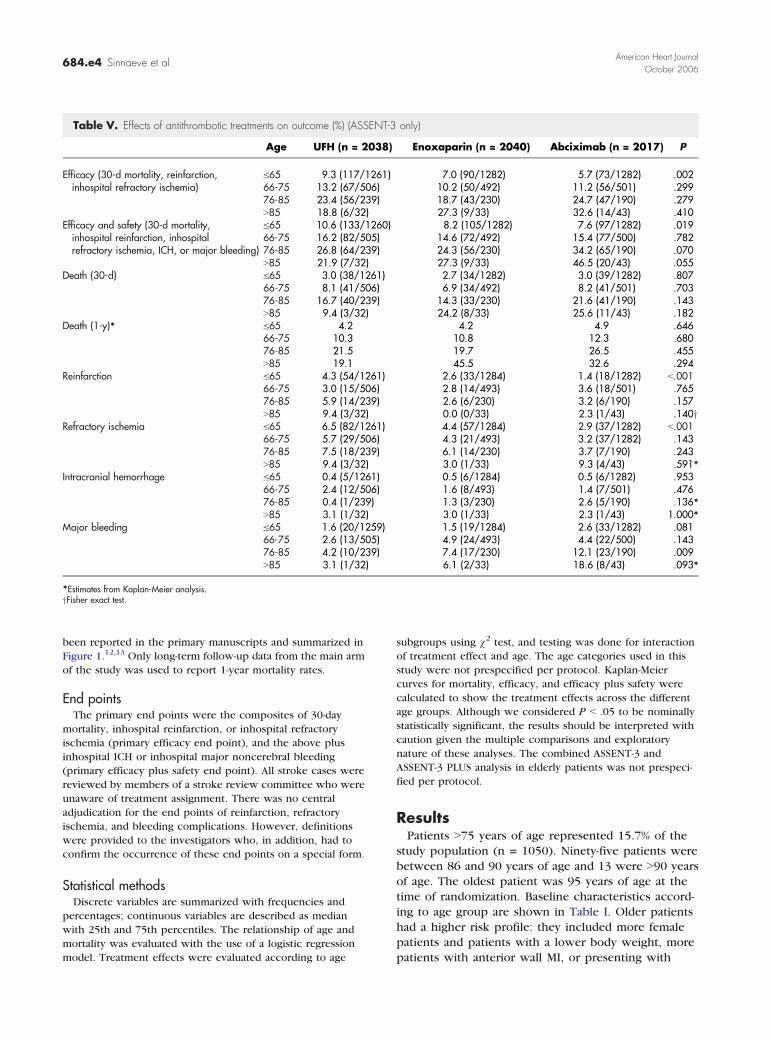
Table V. Effects of antithrombotic treatments on outcome (%) (ASSENT-3 only)
Age UFH (n = 2038) Enoxaparin (n = 2040) Abciximab (n = 2017) P
Efficacy (30-d mortality, reinfarction,inhospital refractory ischemia)
V65 9.3 (117/1261) 7.0 (90/1282) 5.7 (73/1282) .00266-75 13.2 (67/506) 10.2 (50/492) 11.2 (56/501) .29976-85 23.4 (56/239) 18.7 (43/230) 24.7 (47/190) .279N85 18.8 (6/32) 27.3 (9/33) 32.6 (14/43) .410
Efficacy and safety (30-d mortality,inhospital reinfarction, inhospitalrefractory ischemia, ICH, or major bleeding)
V65 10.6 (133/1260) 8.2 (105/1282) 7.6 (97/1282) .01966-75 16.2 (82/505) 14.6 (72/492) 15.4 (77/500) .78276-85 26.8 (64/239) 24.3 (56/230) 34.2 (65/190) .070N85 21.9 (7/32) 27.3 (9/33) 46.5 (20/43) .055
Death (30-d) V65 3.0 (38/1261) 2.7 (34/1282) 3.0 (39/1282) .80766-75 8.1 (41/506) 6.9 (34/492) 8.2 (41/501) .70376-85 16.7 (40/239) 14.3 (33/230) 21.6 (41/190) .143N85 9.4 (3/32) 24.2 (8/33) 25.6 (11/43) .182
Death (1-y)* V65 4.2 4.2 4.9 .64666-75 10.3 10.8 12.3 .68076-85 21.5 19.7 26.5 .455N85 19.1 45.5 32.6 .294
Reinfarction V65 4.3 (54/1261) 2.6 (33/1284) 1.4 (18/1282) b.00166-75 3.0 (15/506) 2.8 (14/493) 3.6 (18/501) .76576-85 5.9 (14/239) 2.6 (6/230) 3.2 (6/190) .157N85 9.4 (3/32) 0.0 (0/33) 2.3 (1/43) .140y
Refractory ischemia V65 6.5 (82/1261) 4.4 (57/1284) 2.9 (37/1282) b.00166-75 5.7 (29/506) 4.3 (21/493) 3.2 (37/1282) .14376-85 7.5 (18/239) 6.1 (14/230) 3.7 (7/190) .243N85 9.4 (3/32) 3.0 (1/33) 9.3 (4/43) .591*
Intracranial hemorrhage V65 0.4 (5/1261) 0.5 (6/1284) 0.5 (6/1282) .95366-75 2.4 (12/506) 1.6 (8/493) 1.4 (7/501) .47676-85 0.4 (1/239) 1.3 (3/230) 2.6 (5/190) .136*N85 3.1 (1/32) 3.0 (1/33) 2.3 (1/43) 1.000*
Major bleeding V65 1.6 (20/1259) 1.5 (19/1284) 2.6 (33/1282) .08166-75 2.6 (13/505) 4.9 (24/493) 4.4 (22/500) .14376-85 4.2 (10/239) 7.4 (17/230) 12.1 (23/190) .009N85 3.1 (1/32) 6.1 (2/33) 18.6 (8/43) .093*
*Estimates from Kaplan-Meier analysis.yFisher exact test.
American Heart Journal
October 2006684.e4 Sinnaeve et al
been reported in the primary manuscripts and summarized in
Figure 1.12,13 Only long-term follow-up data from the main arm
of the study was used to report 1-year mortality rates.
End pointsThe primary end points were the composites of 30-day
mortality, inhospital reinfarction, or inhospital refractory
ischemia (primary efficacy end point), and the above plus
inhospital ICH or inhospital major noncerebral bleeding
(primary efficacy plus safety end point). All stroke cases were
reviewed by members of a stroke review committee who were
unaware of treatment assignment. There was no central
adjudication for the end points of reinfarction, refractory
ischemia, and bleeding complications. However, definitions
were provided to the investigators who, in addition, had to
confirm the occurrence of these end points on a special form.
Statistical methodsDiscrete variables are summarized with frequencies and
percentages; continuous variables are described as median
with 25th and 75th percentiles. The relationship of age and
mortality was evaluated with the use of a logistic regression
model. Treatment effects were evaluated according to age
subgroups using v2 test, and testing was done for interaction
of treatment effect and age. The age categories used in this
study were not prespecified per protocol. Kaplan-Meier
curves for mortality, efficacy, and efficacy plus safety were
calculated to show the treatment effects across the different
age groups. Although we considered P b .05 to be nominally
statistically significant, the results should be interpreted with
caution given the multiple comparisons and exploratory
nature of these analyses. The combined ASSENT-3 and
ASSENT-3 PLUS analysis in elderly patients was not prespeci-
fied per protocol.
ResultsPatients N75 years of age represented 15.7% of the
study population (n = 1050). Ninety-five patients were
between 86 and 90 years of age and 13 were N90 years
of age. The oldest patient was 95 years of age at the
time of randomization. Baseline characteristics accord-
ing to age group are shown in Table I. Older patients
had a higher risk profile: they included more female
patients and patients with a lower body weight, more
patients with anterior wall MI, or presenting with
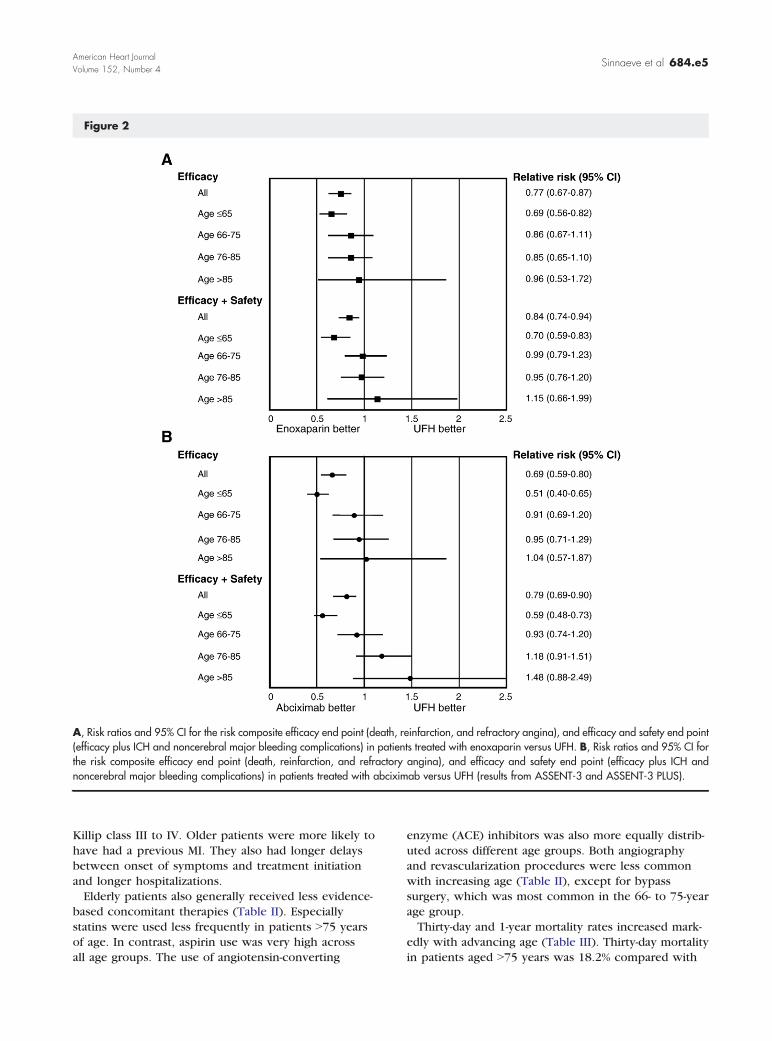
Figure 2
A, Risk ratios and 95% CI for the risk composite efficacy end point (death, reinfarction, and refractory angina), and efficacy and safety end point(efficacy plus ICH and noncerebral major bleeding complications) in patients treated with enoxaparin versus UFH. B, Risk ratios and 95% CI forthe risk composite efficacy end point (death, reinfarction, and refractory angina), and efficacy and safety end point (efficacy plus ICH andnoncerebral major bleeding complications) in patients treated with abciximab versus UFH (results from ASSENT-3 and ASSENT-3 PLUS).
American Heart Journal
Volume 152, Number 4Sinnaeve et al 684.e5
Killip class III to IV. Older patients were more likely to
have had a previous MI. They also had longer delays
between onset of symptoms and treatment initiation
and longer hospitalizations.
Elderly patients also generally received less evidence-
based concomitant therapies (Table II). Especially
statins were used less frequently in patients N75 years
of age. In contrast, aspirin use was very high across
all age groups. The use of angiotensin-converting
enzyme (ACE) inhibitors was also more equally distrib-
uted across different age groups. Both angiography
and revascularization procedures were less common
with increasing age (Table II), except for bypass
surgery, which was most common in the 66- to 75-year
age group.
Thirty-day and 1-year mortality rates increased mark-
edly with advancing age (Table III). Thirty-day mortality
in patients aged N75 years was 18.2% compared with
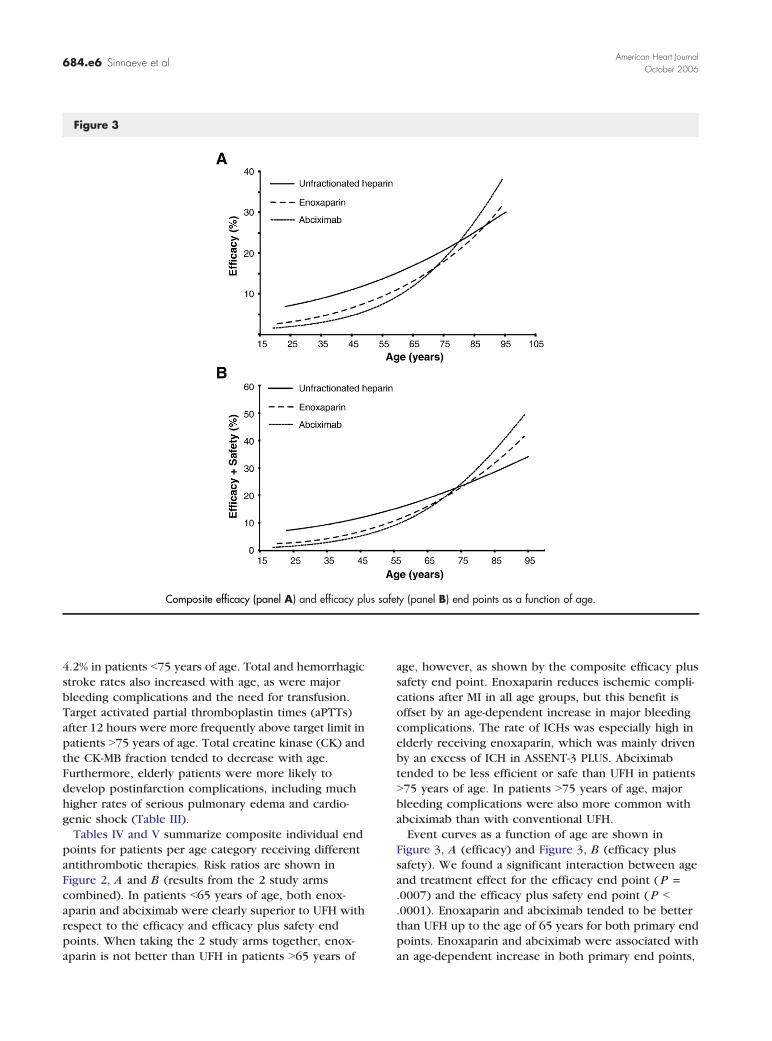
Figure 3
Composite efficacy (panel A) and efficacy plus safety (panel B) end points as a function of age.
American Heart Journal
October 2006684.e6 Sinnaeve et al
4.2% in patients b75 years of age. Total and hemorrhagic
stroke rates also increased with age, as were major
bleeding complications and the need for transfusion.
Target activated partial thromboplastin times (aPTTs)
after 12 hours were more frequently above target limit in
patients N75 years of age. Total creatine kinase (CK) and
the CK-MB fraction tended to decrease with age.
Furthermore, elderly patients were more likely to
develop postinfarction complications, including much
higher rates of serious pulmonary edema and cardio-
genic shock (Table III).
Tables IV and V summarize composite individual end
points for patients per age category receiving different
antithrombotic therapies. Risk ratios are shown in
Figure 2, A and B (results from the 2 study arms
combined). In patients b65 years of age, both enox-
aparin and abciximab were clearly superior to UFH with
respect to the efficacy and efficacy plus safety end
points. When taking the 2 study arms together, enox-
aparin is not better than UFH in patients N65 years of
age, however, as shown by the composite efficacy plus
safety end point. Enoxaparin reduces ischemic compli-
cations after MI in all age groups, but this benefit is
offset by an age-dependent increase in major bleeding
complications. The rate of ICHs was especially high in
elderly receiving enoxaparin, which was mainly driven
by an excess of ICH in ASSENT-3 PLUS. Abciximab
tended to be less efficient or safe than UFH in patients
N75 years of age. In patients N75 years of age, major
bleeding complications were also more common with
abciximab than with conventional UFH.
Event curves as a function of age are shown in
Figure 3, A (efficacy) and Figure 3, B (efficacy plus
safety). We found a significant interaction between age
and treatment effect for the efficacy end point ( P =
.0007) and the efficacy plus safety end point ( P b
.0001). Enoxaparin and abciximab tended to be better
than UFH up to the age of 65 years for both primary end
points. Enoxaparin and abciximab were associated with
an age-dependent increase in both primary end points,

American Heart Journal
Volume 152, Number 4Sinnaeve et al 684.e7
an effect that was less pronounced for UFH. This
resulted in a crossover point at 75 years of age, after
which UFH tends to be more effective and safe than
enoxaparin or abciximab.
DiscussionWe have evaluated the effects of different antithrom-
botic strategies in combination with TNK on the elderly
in ASSENT-3 and ASSENT-3 PLUS. The present study
confirms findings from previous studies that mortality
increases dramatically with age after fibrinolysis for
acute MI.4,8 Enoxaparin with full-dose TNK appears to
be equally effective as UFH, but this benefit is offset by
an age-dependent increase in major bleeding complica-
tions and especially ICHs. Abciximab in combination
with half-dose TNK also appears to be less effective than
UFH in elderly patients. Moreover, ICH and major
bleeding rates are higher with abciximab in patients
N75 years of age.
When given with full-dose TNK, enoxaparin compared
favorably to UFH over all age categories except for the
very old as indicated by the efficacy end point. This
benefit seems to be offset largely by an increase in major
bleeding complications. The combination of abciximab
with half-dose TNK was significantly less effective and
safe than UFH in patients aged N75 years, in contrast
with the promising low efficacy plus safety end point
rate compared with UFH in younger patients. Similar
results have been observed in GUSTO-V with half-dose
reteplase and abciximab.11 Abciximab plus half-dose
reteplase also reduced nonfatal ischemic events post-
infarction in GUSTO-V in the overall population, but not
in patients N75 years of age.11 In contrast, abciximab
was also shown to be superior to placebo in elderly
patients (N65 years) with acute MI treated with primary
stenting.14 The reason why combination therapy is less
safe even when combining with half-dose lytics in
ASSENT-3 and GUSTO-V remains unclear.
Major noncerebral bleeding complications in the
elderly were modestly higher with enoxaparin and
markedly higher with abciximab compared with UFH.
Although a stricter and more conservative heparin
dosing scheme was used compared with that in GUSTO-
I, aPTT levels also tended to be more frequently above
target limits in patients N75 years of age, which might in
part be responsible for some of the bleedings. The
reason for over-anticoagulation in the elderly remains
unclear, but might reflect changes in pharmacokinetics
with age. It also demonstrates that anticoagulation
monitoring needs to be improved in these patients.
Finally, it remains difficult to determine the real impact
of abciximab on outcome in the elderly.15 An increased
risk of bleeding complications in the elderly might be
associated with a higher incidence of anemia, which
might precipitate reinfarction.
In elderly patients, inappropriately high levels of
enoxaparin may cause an increased risk of bleeding
complications when combined with fibrinolysis. Never-
theless, when using a weight-adjusted dose of enoxa-
parin, only severely decreased renal function, but not
age, appears to affect anti-Xa levels independently.16 In
ASSENT-3 and ASSENT-3 PLUS, patients with impaired
renal function (creatinine N2.5 mg/dL for men or
N2.0 mg/dL for women) were excluded. Still, impaired
renal function tends to occur more frequently in the
elderly, which might indirectly lead to inappropriately
high levels of enoxaparin causing an increased risk of
bleeding complications. On the other hand, decreased
renal function was not found to be associated with a
higher incidence of bleeding complications with enox-
aparin in patients treated with fibrinolysis in the
CLARITY study, although no patients N75 years of age
were included.17 In the ExTRACT study, which com-
pared enoxaparin with UFH in patients with STEMI
receiving fibrinolysis, patients N75 years of age received
no bolus and a reduced maintenance dose of enoxaparin
(0.75 mg/kg BID). Although the exact impact of this
dose on bleeding complications in the elderly has not
yet been reported by the authors, no significant
interaction between treatment and age was observed for
the primary efficacy end point.18 Interestingly, when
dose reduction of enoxaparin (65%) was left to the
discretion of the physician in a study of unselected
patients with acute coronary syndrome, elderly subjects
had more frequently suboptimal anti-Xa levels, which
was associated with worse outcome.19
Elderly patients had a higher risk of ICH. Comparable
to rates in GUSTO-I and GUSTO-V.8,11 Intracranial
hemorrhage rate is N3 times as frequent in patients
N75 years of age compared with those b65 years of age.
Intracranial hemorrhage is more frequent in elderly
patients receiving enoxaparin or abciximab. Neverthe-
less, the ASSENT-3 study was underpowered to demon-
strate any difference in ICH between treatments.
Because of the very small number of events, there is also
considerable variation in ICH rate in different treatment
and age groups.
As in previous trials, elderly patients tended to receive
less evidence-based co-therapy. Aspirin, h-blockers and
statins were less frequently given to older patients. The
lower percentage of patients N75 years of age receiving
aspirin in ASSENT-3 and ASSENT-3 PLUS might reflect
the hesitance of some investigators to add aspirin to
more aggressive antithrombotic treatment, especially in
the elderly. In this respect, a similar rationale has led the
investigators in another trial comparing enoxaparin with
UFH in ST-elevation MI to withhold aspirin until after the
study period.20 In contrast, ACE inhibitors were pre-
scribed more frequently in patients between 65 and
85 years of age, perhaps reflecting the higher incidence
of heart failure in the elderly. We did not record

American Heart Journal
October 2006684.e8 Sinnaeve et al
contraindications against evidence-based therapies,
which might in part explain less frequent use in
elderly. Nevertheless, previous studies have reported a
similar underuse of proven drugs despite adjustments
for contraindications.21
Angiography and revascularization procedures were
markedly less common in patients N75 years of age. In
the second NRMI-2 registry, 63% of patients N70 years of
age had a cardiac catheterization compared with 85% of
those b49 years of age.22 In contrast, only 20% of
patients N75 years of age underwent a cardiac catheter-
ization during their hospital stay in a population of
192311 Medicare patients.23 Because mortality after an
acute MI in the elderly is markedly higher than in
younger patients, the reason for withholding angiogra-
phy or revascularization in older patients remains
unclear, but is probably multifactorial. Elderly patients
are more likely to have more extensive coronary
lesions.8,24 Investigators might also be apprehensive in
performing angiography or percutaneous coronary in-
tervention in elderly patients receiving low-molecular-
weight heparin or glycoprotein IIb/IIIa antagonists.
This study has some potential limitations. The overall
sample size is too small to comment on mortality
differences between treatment groups. In addition, some
of the subgroups might also be too small to draw
conclusions, especially in the very old. Furthermore,
clinical trials generally enroll lower-risk patients when
compared with those treated in daily practice. There-
fore, the elderly in ASSENT-3 and ASSENT-3 PLUS may
have relatively lower rates of complications than the
general elderly population.
In conclusion, the present analysis confirms that
elderly patients represent a high-risk population and are
at increased risk of death and major bleeding complica-
tions. Although the combination of half-dose fibrinolytic
agent plus abciximab is a safe and effective therapeutic
option in patients b65 years of age with an acute MI,
data from ASSENT-3 and ASSENT-3 PLUS suggest that
half-dose fibrinolytic and abciximab might be unsafe and
even less effective in the elderly. Enoxaparin as
adjunctive therapy to TNK appears to be at least as
effective as UFH except in the very elderly, but the risk
of major bleeding complications in full dosing is
unacceptably high in patients N75 years of age. Devel-
opment of new dosing schemes or treatment combina-
tions with improved efficacy and safety in the elderly
remains a high priority.
PR Sinnaeve is a Clinical Investigator of the Fund for
Scientific Research—Flanders (Belgium).
References1. Lee KL, Woodlief LH, Topol EJ, et al. Predictors of 30-day mortality
in the era of reperfusion for acute myocardial infarction. Results
from an international trial of 41,021 patients. GUSTO-I Investiga-tors. Circulation 1995;91:1659.
2. Stevenson R, Ranjadayalan K, Wilkinson P, et al. Short and longterm prognosis of acute myocardial infarction since introductionof thrombolysis. BMJ 1993;307:349.
3. Goldberg RJ, McCormick D, Gurwitz JH, et al. Age-related trends inshort-and long-term survival after acute myocardial infarction:a 20-year population-based perspective (1975-1995). Am JCardiol 1998;82:1311.
4. Maggioni AP, Maseri A, Fresco C, et al. Age-related increase inmortality among patients with first myocardial infarctions treatedwith thrombolysis. The investigators of the gruppo italiano per lostudio della sopravvivenza nell’infarto miocardico (GISSI-2). N EnglJ Med 1993;329:1442.
5. Paul SD, O’Gara PT, Mahjoub ZA, et al. Geriatric patients withacute myocardial infarction: cardiac risk factor profiles, presenta-tion, thrombolysis, coronary interventions, and prognosis. Am HeartJ 1996;131:710.
6. Thiemann DR, Coresh J, Schulman SP, et al. Lack of benefit forintravenous thrombolysis in patients with myocardial infarction whoare older than 75 years. Circulation 2000;101:2239.
7. Weaver WD, Litwin PE, Martin JS, et al. Effect of age on use ofthrombolytic therapy and mortality in acute myocardial infarction.The MITI Project Group. J Am Coll Cardiol 1991;18:657.
8. White HD, Barbash GI, Califf RM, et al. Age and outcome withcontemporary thrombolytic therapy. Results from the GUSTO-I trial.Global utilization of streptokinase and TPA for occluded coronaryarteries trial. Circulation 1996;94:1826.
9. Antman EM, Gibson CM, de Lemos JA, et al. Combinationreperfusion therapy with abciximab and reduced dose reteplase:results from TIMI 14. The thrombolysis in myocardial infarction(TIMI) 14 Investigators. Eur Heart J 2000;21:1944.
10. Giugliano RP, Roe M, Harrington R, et al. Combination reperfusiontherapy with eptifibatide and reduced dose tenecteplase forST-elevation myocardial infarction: results of the Integrilin andtenecteplase in acute myocardial infarction trial (INTEGRITI) phase IIangiographic trial. J Am Coll Cardiol 2003;14:1251 -60.
11. Topol EJ. Reperfusion therapy for acute myocardial infarction withfibrinolytic therapy or combination reduced fibrinolytic therapy andplatelet glycoprotein IIb/IIIa inhibition: the GUSTO V randomisedtrial. Lancet 2001;357:1905.
12. Efficacy and safety of tenecteplase in combination with enoxaparin,abciximab, or unfractionated heparin: the ASSENT-3 randomisedtrial in acute myocardial infarction. Lancet 2001;358:605.
13. Wallentin L, Goldstein P, Armstrong PW, et al. Efficacy and safety oftenecteplase in combination with the low-molecular-weight heparinenoxaparin or unfractionated heparin in the prehospital setting:the assessment of the safety and efficacy of a new thrombolyticregimen (ASSENT)-3 PLUS randomized trial in acute myocardialinfarction. Circulation 2003;108:135.
14. Montalescot G, Barragan P, Wittenberg O, et al. Platelet glyco-protein IIb/IIIa inhibition with coronary stenting for acute myocar-dial infarction. N Engl J Med 2001;344:1895.
15. Casterella PJ, Kereiakes DJ, Steinhubl SR, et al. The platelet functiondose-response to abciximab during percutaneous coronary revas-cularization is variable. Catheter Cardiovasc Interv 2001;54:497.
16. Becker RC, Spencer FA, Gibson M, et al. Influence of patientcharacteristics and renal function on factor Xa inhibition pharma-cokinetics and pharmacodynamics after enoxaparin administrationin non–ST-segment elevation acute coronary syndromes. Am Heart J2002;143:753.

American Heart Journal
Volume 152, Number 4Sinnaeve et al 684.e9
17. Sabatine MS, Morrow DA, Montalescot G, et al. Angiographicand clinical outcomes in patients receiving low-molecular-weightheparin versus unfractionated heparin in ST-elevation myocardialinfarction treated with fibrinolytics in the CLARITY-TIMI 28 Trial.Circulation 2005;112:3846 -54.
18. Antman EM, Morrow DA, McCabe CH, et al. Enoxaparin versusunfractionated heparin with fibrinolysis for ST-elevation myocardialinfarction. N Engl J Med 2006;354:1477 -88.
19. Montalescot G, Collet JP, Tanguy ML, et al. Anti-Xa activityrelates to survival and efficacy in unselected acute coronarysyndrome patients treated with enoxaparin. Circulation 2004;110:392 -8.
20. Baird SH, Menown IB, McBride SJ, et al. Randomized comparison ofenoxaparin with unfractionated heparin following fibrinolytic ther-apy for acute myocardial infarction. Eur Heart J 2002;23:627.
21. Tran CT, Laupacis A, Mamdani MM, et al. Effect of age on the use ofevidence-based therapies for acute myocardial infarction. Am HeartJ 2004;148:834 -41.
22. Spencer FA, Goldberg RJ, Frederick PD, et al. Age and theutilization of cardiac catheterization following uncomplicated firstacute myocardial infarction treated with thrombolytic therapy(The Second National Registry of Myocardial Infarction [NRMI-2]).Am J Cardiol 2001;88:107.
23. Alexander KP, Galanos AN, Jollis JG, et al. Post-myocardialinfarction risk stratification in elderly patients. Am Heart J2001;142:37.
24. Aguirre FV, McMahon RP, Mueller H, et al. Impact of age on clinicaloutcome and postlytic management strategies in patients treatedwith intravenous thrombolytic therapy. Results from the TIMI II Study.TIMI II Investigators. Circulation 1994;90:78.
Related Documents











