Affective symptoms and cognitive functions in Parkinson's disease Michele Poletti, Anna De Rosa, Ubaldo Bonuccelli ⁎ Department of Neuroscience, University of Pisa, Pisa, Italy abstract article info Article history: Received 22 September 2011 Received in revised form 24 January 2012 Accepted 23 February 2012 Available online 13 April 2012 Keywords: Parkinson's disease Depression Apathy Anxiety Alexithymia Patients with Parkinson's disease (PD) typically present with motor symptoms, but several non-motor symp- toms, such as cognitive impairment, autonomic dysfunction and neuropsychiatric symptoms, are usually also present, when adequately looked for. The objective of this paper is to provide an up-to-date, comprehensive review of the influence of affective disorders, mainly depression and apathy, on cognitive functioning of PD patients. Reviewed empirical findings suggest that, although depression and apathy have differential neuro- biological bases in PD, both are associated to an increased risk of cognitive impairment, especially of execu- tive functions, in this clinical population. The potential influence of other affective disorders, as anxiety and alexithymia, on cognitive functioning of PD patients is actually almost unknown and needs further empirical investigation. The clinical implication of these findings is that the best assessment and management of PD patients should include both neuropsychological and neuropsychiatric evaluations and the presence of non-motor symptoms as cognitive disturbances and affective features should be investigated with patients and caregivers. © 2012 Elsevier B.V. All rights reserved. 1. Introduction Parkinson's disease (PD) is characterized by motor (bradykinesia, rigidity and resting tremors) and non-motor symptoms, as cognitive impairment, affective and behavioral disturbances [1]. Cognitive impairment is a common feature of PD [2,3], with deficits being most prominent in the domains of memory, executive and visuospa- tial functions; prospective studies showed that up to 75–80% of PD patients may eventually develop dementia during the course of the disease [4]. Affective disorders have a high prevalence in PD [5,6]; affective dis- orders, especially depression, have a detrimental effect on cognition in the general population [7,8] but their effect on cognition of PD patients has been less investigated. This paper aims at providing an update of current evidence on the influence of affective disorders on cognition in PD patients without dementia. This topic is of particular interest to distinguish the different effects on cognition of 1) affective disorders, 2) the PD-related neurodegeneration [9,10] and 3) dopaminergic ther- apies [11]. 2. Neuropathologic bases of cognitive dysfunction in PD PD is primarily caused by loss of dopaminergic neurons in the nigrostriatal pathway, producing reduction of dopamine levels in the striatum. This dopamine depletion impacts on the functioning of four frontostriatal networks involved in motor, cognitive, affective and motivational aspects of behavior [12]. Of particular interest with regard to cognitive dysfunction in PD patients are three of these circuits (Fig. 1): the “dorsolateral” circuit including the dorso- lateral prefrontal cortex (DLPFC), the striatum (dorsolateral caudate nucleus), the globus pallidus (dorsomedial) and the thalamus; the “orbital” circuit including the orbitofrontal cortex (OFC), the striatum (ventromedial caudate nucleus), the globus pallidus (dorsomedial) and the thalamus: the “anterior cingulate” circuit including the ante- rior cingulated cortex (ACC), the striatum (ventromedial caudate nucleus, ventral putamen) the nucleus accumbens, the olfactory tubercle, the globus pallidus (rostromedial) and the thalamus. Within each circuit, two loops connect the striatum with the prefrontal cor- tex (PFC): a direct excitatory loop and an indirect inhibitory loop [13,14]. Executive functions are a set of processes necessary for an appro- priate, contextual goal-directed behavior, allowing to formulate goals with regard to their consequences, to generate multiple response alternatives, to choose and to initiate appropriate actions, to self- monitor the adequacy and correctness of these actions, to correct and modify them when conditions change and finally to persist in the face of distractions [15]. The prefrontal impairment, usually de- fined as a dysexecutive syndrome (including impairment in complex attention and executive functions), that characterizes most of the PD patients from the early stages of the disease, is not due to a direct neuropathology of PFC, but to a reduced dopaminergic stimulation at striatal level, that disrupts the normal functioning of frontostriatal circuits. Anatomical and neuropathological evidence suggests that the evolving pattern of executive impairment in PD might be explained Journal of the Neurological Sciences 317 (2012) 97–102 ⁎ Corresponding author at: Department of Neuroscience, University of Pisa, Italy. Tel./fax: + 39 0584 6059539. E-mail address: [email protected] (U. Bonuccelli). 0022-510X/$ – see front matter © 2012 Elsevier B.V. All rights reserved. doi:10.1016/j.jns.2012.02.022 Contents lists available at SciVerse ScienceDirect Journal of the Neurological Sciences journal homepage: www.elsevier.com/locate/jns

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Journal of the Neurological Sciences 317 (2012) 97–102
Contents lists available at SciVerse ScienceDirect
Journal of the Neurological Sciences
j ourna l homepage: www.e lsev ie r .com/ locate / jns
Affective symptoms and cognitive functions in Parkinson's disease
Michele Poletti, Anna De Rosa, Ubaldo Bonuccelli ⁎Department of Neuroscience, University of Pisa, Pisa, Italy
⁎ Corresponding author at: Department of NeurosciTel./fax: +39 0584 6059539.
E-mail address: [email protected] (U. Bonuc
0022-510X/$ – see front matter © 2012 Elsevier B.V. Aldoi:10.1016/j.jns.2012.02.022
a b s t r a c t
a r t i c l e i n f oArticle history:Received 22 September 2011Received in revised form 24 January 2012Accepted 23 February 2012Available online 13 April 2012
Keywords:Parkinson's diseaseDepressionApathyAnxietyAlexithymia
Patients with Parkinson's disease (PD) typically present with motor symptoms, but several non-motor symp-toms, such as cognitive impairment, autonomic dysfunction and neuropsychiatric symptoms, are usually alsopresent, when adequately looked for. The objective of this paper is to provide an up-to-date, comprehensivereview of the influence of affective disorders, mainly depression and apathy, on cognitive functioning of PDpatients. Reviewed empirical findings suggest that, although depression and apathy have differential neuro-biological bases in PD, both are associated to an increased risk of cognitive impairment, especially of execu-tive functions, in this clinical population. The potential influence of other affective disorders, as anxiety andalexithymia, on cognitive functioning of PD patients is actually almost unknown and needs further empiricalinvestigation. The clinical implication of these findings is that the best assessment and management of PDpatients should include both neuropsychological and neuropsychiatric evaluations and the presence ofnon-motor symptoms as cognitive disturbances and affective features should be investigated with patientsand caregivers.
© 2012 Elsevier B.V. All rights reserved.
1. Introduction
Parkinson's disease (PD) is characterized by motor (bradykinesia,rigidity and resting tremors) and non-motor symptoms, as cognitiveimpairment, affective and behavioral disturbances [1]. Cognitiveimpairment is a common feature of PD [2,3], with deficits beingmost prominent in the domains of memory, executive and visuospa-tial functions; prospective studies showed that up to 75–80% of PDpatients may eventually develop dementia during the course of thedisease [4].
Affective disorders have a high prevalence in PD [5,6]; affective dis-orders, especially depression, have a detrimental effect on cognition inthe general population [7,8] but their effect on cognition of PD patientshas been less investigated. This paper aims at providing an update ofcurrent evidence on the influence of affective disorders on cognitionin PD patients without dementia. This topic is of particular interest todistinguish the different effects on cognition of 1) affective disorders,2) the PD-related neurodegeneration [9,10] and 3) dopaminergic ther-apies [11].
2. Neuropathologic bases of cognitive dysfunction in PD
PD is primarily caused by loss of dopaminergic neurons in thenigrostriatal pathway, producing reduction of dopamine levels inthe striatum. This dopamine depletion impacts on the functioning of
ence, University of Pisa, Italy.
celli).
l rights reserved.
four frontostriatal networks involved in motor, cognitive, affectiveand motivational aspects of behavior [12]. Of particular interestwith regard to cognitive dysfunction in PD patients are three ofthese circuits (Fig. 1): the “dorsolateral” circuit including the dorso-lateral prefrontal cortex (DLPFC), the striatum (dorsolateral caudatenucleus), the globus pallidus (dorsomedial) and the thalamus; the“orbital” circuit including the orbitofrontal cortex (OFC), the striatum(ventromedial caudate nucleus), the globus pallidus (dorsomedial)and the thalamus: the “anterior cingulate” circuit including the ante-rior cingulated cortex (ACC), the striatum (ventromedial caudatenucleus, ventral putamen) the nucleus accumbens, the olfactorytubercle, the globus pallidus (rostromedial) and the thalamus. Withineach circuit, two loops connect the striatum with the prefrontal cor-tex (PFC): a direct excitatory loop and an indirect inhibitory loop[13,14].
Executive functions are a set of processes necessary for an appro-priate, contextual goal-directed behavior, allowing to formulate goalswith regard to their consequences, to generate multiple responsealternatives, to choose and to initiate appropriate actions, to self-monitor the adequacy and correctness of these actions, to correctand modify them when conditions change and finally to persist inthe face of distractions [15]. The prefrontal impairment, usually de-fined as a dysexecutive syndrome (including impairment in complexattention and executive functions), that characterizes most of the PDpatients from the early stages of the disease, is not due to a directneuropathology of PFC, but to a reduced dopaminergic stimulationat striatal level, that disrupts the normal functioning of frontostriatalcircuits. Anatomical and neuropathological evidence suggests that theevolving pattern of executive impairment in PD might be explained
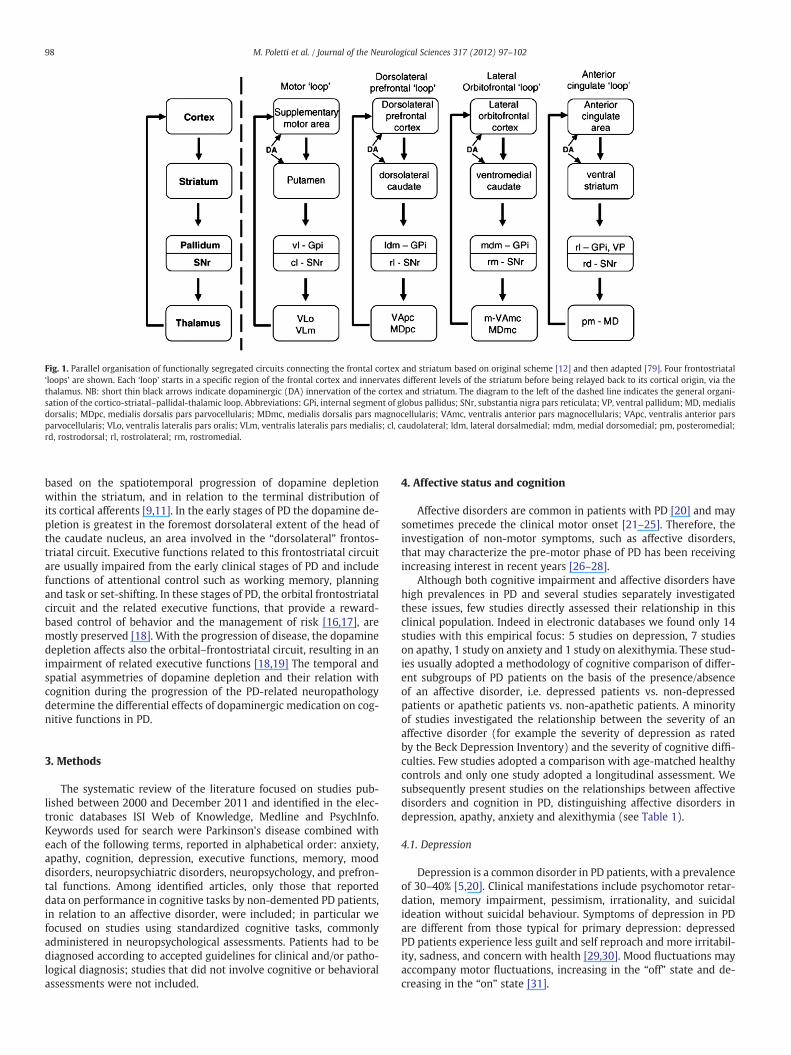
Fig. 1. Parallel organisation of functionally segregated circuits connecting the frontal cortex and striatum based on original scheme [12] and then adapted [79]. Four frontostriatal‘loops’ are shown. Each ‘loop’ starts in a specific region of the frontal cortex and innervates different levels of the striatum before being relayed back to its cortical origin, via thethalamus. NB: short thin black arrows indicate dopaminergic (DA) innervation of the cortex and striatum. The diagram to the left of the dashed line indicates the general organi-sation of the cortico-striatal–pallidal-thalamic loop. Abbreviations: GPi, internal segment of globus pallidus; SNr, substantia nigra pars reticulata; VP, ventral pallidum; MD, medialisdorsalis; MDpc, medialis dorsalis pars parvocellularis; MDmc, medialis dorsalis pars magnocellularis; VAmc, ventralis anterior pars magnocellularis; VApc, ventralis anterior parsparvocellularis; VLo, ventralis lateralis pars oralis; VLm, ventralis lateralis pars medialis; cl, caudolateral; ldm, lateral dorsalmedial; mdm, medial dorsomedial; pm, posteromedial;rd, rostrodorsal; rl, rostrolateral; rm, rostromedial.
98 M. Poletti et al. / Journal of the Neurological Sciences 317 (2012) 97–102
based on the spatiotemporal progression of dopamine depletionwithin the striatum, and in relation to the terminal distribution ofits cortical afferents [9,11]. In the early stages of PD the dopamine de-pletion is greatest in the foremost dorsolateral extent of the head ofthe caudate nucleus, an area involved in the “dorsolateral” frontos-triatal circuit. Executive functions related to this frontostriatal circuitare usually impaired from the early clinical stages of PD and includefunctions of attentional control such as working memory, planningand task or set-shifting. In these stages of PD, the orbital frontostriatalcircuit and the related executive functions, that provide a reward-based control of behavior and the management of risk [16,17], aremostly preserved [18]. With the progression of disease, the dopaminedepletion affects also the orbital–frontostriatal circuit, resulting in animpairment of related executive functions [18,19] The temporal andspatial asymmetries of dopamine depletion and their relation withcognition during the progression of the PD-related neuropathologydetermine the differential effects of dopaminergic medication on cog-nitive functions in PD.
3. Methods
The systematic review of the literature focused on studies pub-lished between 2000 and December 2011 and identified in the elec-tronic databases ISI Web of Knowledge, Medline and PsychInfo.Keywords used for search were Parkinson's disease combined witheach of the following terms, reported in alphabetical order: anxiety,apathy, cognition, depression, executive functions, memory, mooddisorders, neuropsychiatric disorders, neuropsychology, and prefron-tal functions. Among identified articles, only those that reporteddata on performance in cognitive tasks by non-demented PD patients,in relation to an affective disorder, were included; in particular wefocused on studies using standardized cognitive tasks, commonlyadministered in neuropsychological assessments. Patients had to bediagnosed according to accepted guidelines for clinical and/or patho-logical diagnosis; studies that did not involve cognitive or behavioralassessments were not included.
4. Affective status and cognition
Affective disorders are common in patients with PD [20] and maysometimes precede the clinical motor onset [21–25]. Therefore, theinvestigation of non-motor symptoms, such as affective disorders,that may characterize the pre-motor phase of PD has been receivingincreasing interest in recent years [26–28].
Although both cognitive impairment and affective disorders havehigh prevalences in PD and several studies separately investigatedthese issues, few studies directly assessed their relationship in thisclinical population. Indeed in electronic databases we found only 14studies with this empirical focus: 5 studies on depression, 7 studieson apathy, 1 study on anxiety and 1 study on alexithymia. These stud-ies usually adopted a methodology of cognitive comparison of differ-ent subgroups of PD patients on the basis of the presence/absenceof an affective disorder, i.e. depressed patients vs. non-depressedpatients or apathetic patients vs. non-apathetic patients. A minorityof studies investigated the relationship between the severity of anaffective disorder (for example the severity of depression as ratedby the Beck Depression Inventory) and the severity of cognitive diffi-culties. Few studies adopted a comparison with age-matched healthycontrols and only one study adopted a longitudinal assessment. Wesubsequently present studies on the relationships between affectivedisorders and cognition in PD, distinguishing affective disorders indepression, apathy, anxiety and alexithymia (see Table 1).
4.1. Depression
Depression is a common disorder in PD patients, with a prevalenceof 30–40% [5,20]. Clinical manifestations include psychomotor retar-dation, memory impairment, pessimism, irrationality, and suicidalideation without suicidal behaviour. Symptoms of depression in PDare different from those typical for primary depression: depressedPD patients experience less guilt and self reproach and more irritabil-ity, sadness, and concern with health [29,30]. Mood fluctuations mayaccompany motor fluctuations, increasing in the “off” state and de-creasing in the “on” state [31].
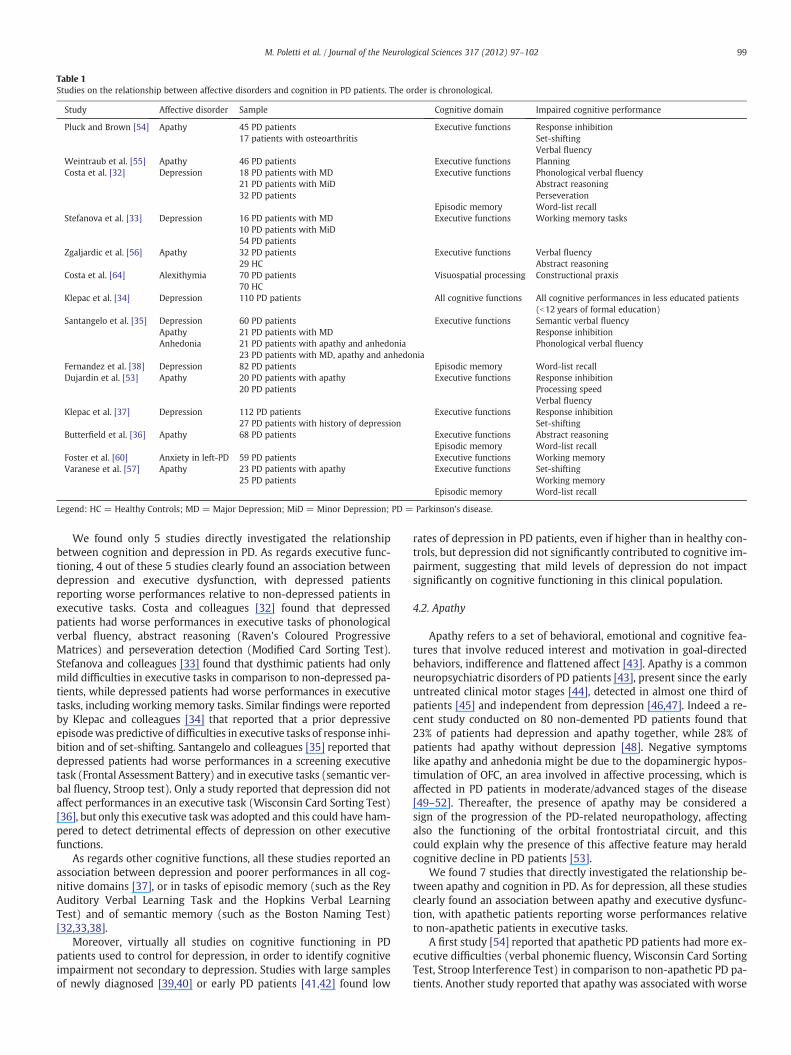
Table 1Studies on the relationship between affective disorders and cognition in PD patients. The order is chronological.
Study Affective disorder Sample Cognitive domain Impaired cognitive performance
Pluck and Brown [54] Apathy 45 PD patients17 patients with osteoarthritis
Executive functions Response inhibitionSet-shiftingVerbal fluency
Weintraub et al. [55] Apathy 46 PD patients Executive functions PlanningCosta et al. [32] Depression 18 PD patients with MD
21 PD patients with MiD32 PD patients
Executive functions Phonological verbal fluencyAbstract reasoningPerseveration
Episodic memory Word-list recallStefanova et al. [33] Depression 16 PD patients with MD
10 PD patients with MiD54 PD patients
Executive functions Working memory tasks
Zgaljardic et al. [56] Apathy 32 PD patients29 HC
Executive functions Verbal fluencyAbstract reasoning
Costa et al. [64] Alexithymia 70 PD patients70 HC
Visuospatial processing Constructional praxis
Klepac et al. [34] Depression 110 PD patients All cognitive functions All cognitive performances in less educated patients(b12 years of formal education)
Santangelo et al. [35] DepressionApathyAnhedonia
60 PD patients21 PD patients with MD21 PD patients with apathy and anhedonia23 PD patients with MD, apathy and anhedonia
Executive functions Semantic verbal fluencyResponse inhibitionPhonological verbal fluency
Fernandez et al. [38] Depression 82 PD patients Episodic memory Word-list recallDujardin et al. [53] Apathy 20 PD patients with apathy
20 PD patientsExecutive functions Response inhibition
Processing speedVerbal fluency
Klepac et al. [37] Depression 112 PD patients27 PD patients with history of depression
Executive functions Response inhibitionSet-shifting
Butterfield et al. [36] Apathy 68 PD patients Executive functions Abstract reasoningEpisodic memory Word-list recall
Foster et al. [60] Anxiety in left-PD 59 PD patients Executive functions Working memoryVaranese et al. [57] Apathy 23 PD patients with apathy
25 PD patientsExecutive functions Set-shifting
Working memoryEpisodic memory Word-list recall
Legend: HC = Healthy Controls; MD = Major Depression; MiD = Minor Depression; PD = Parkinson's disease.
99M. Poletti et al. / Journal of the Neurological Sciences 317 (2012) 97–102
We found only 5 studies directly investigated the relationshipbetween cognition and depression in PD. As regards executive func-tioning, 4 out of these 5 studies clearly found an association betweendepression and executive dysfunction, with depressed patientsreporting worse performances relative to non-depressed patients inexecutive tasks. Costa and colleagues [32] found that depressedpatients had worse performances in executive tasks of phonologicalverbal fluency, abstract reasoning (Raven's Coloured ProgressiveMatrices) and perseveration detection (Modified Card Sorting Test).Stefanova and colleagues [33] found that dysthimic patients had onlymild difficulties in executive tasks in comparison to non-depressed pa-tients, while depressed patients had worse performances in executivetasks, including working memory tasks. Similar findings were reportedby Klepac and colleagues [34] that reported that a prior depressiveepisodewas predictive of difficulties in executive tasks of response inhi-bition and of set-shifting. Santangelo and colleagues [35] reported thatdepressed patients had worse performances in a screening executivetask (Frontal Assessment Battery) and in executive tasks (semantic ver-bal fluency, Stroop test). Only a study reported that depression did notaffect performances in an executive task (Wisconsin Card Sorting Test)[36], but only this executive taskwas adopted and this could have ham-pered to detect detrimental effects of depression on other executivefunctions.
As regards other cognitive functions, all these studies reported anassociation between depression and poorer performances in all cog-nitive domains [37], or in tasks of episodic memory (such as the ReyAuditory Verbal Learning Task and the Hopkins Verbal LearningTest) and of semantic memory (such as the Boston Naming Test)[32,33,38].
Moreover, virtually all studies on cognitive functioning in PDpatients used to control for depression, in order to identify cognitiveimpairment not secondary to depression. Studies with large samplesof newly diagnosed [39,40] or early PD patients [41,42] found low
rates of depression in PD patients, even if higher than in healthy con-trols, but depression did not significantly contributed to cognitive im-pairment, suggesting that mild levels of depression do not impactsignificantly on cognitive functioning in this clinical population.
4.2. Apathy
Apathy refers to a set of behavioral, emotional and cognitive fea-tures that involve reduced interest and motivation in goal-directedbehaviors, indifference and flattened affect [43]. Apathy is a commonneuropsychiatric disorders of PD patients [43], present since the earlyuntreated clinical motor stages [44], detected in almost one third ofpatients [45] and independent from depression [46,47]. Indeed a re-cent study conducted on 80 non-demented PD patients found that23% of patients had depression and apathy together, while 28% ofpatients had apathy without depression [48]. Negative symptomslike apathy and anhedonia might be due to the dopaminergic hypos-timulation of OFC, an area involved in affective processing, which isaffected in PD patients in moderate/advanced stages of the disease[49–52]. Thereafter, the presence of apathy may be considered asign of the progression of the PD-related neuropathology, affectingalso the functioning of the orbital frontostriatal circuit, and thiscould explain why the presence of this affective feature may heraldcognitive decline in PD patients [53].
We found 7 studies that directly investigated the relationship be-tween apathy and cognition in PD. As for depression, all these studiesclearly found an association between apathy and executive dysfunc-tion, with apathetic patients reporting worse performances relativeto non-apathetic patients in executive tasks.
A first study [54] reported that apathetic PD patients had more ex-ecutive difficulties (verbal phonemic fluency, Wisconsin Card SortingTest, Stroop Interference Test) in comparison to non-apathetic PD pa-tients. Another study reported that apathy was associated with worse

100 M. Poletti et al. / Journal of the Neurological Sciences 317 (2012) 97–102
performances in a planning task (Tower of London) [55]. A studyreported that, in a group of non-demented PD patients, apathetic pa-tients were more impaired than non-apathetic patients on executivetasks of verbal fluency and conceptualization; moreover, the severityof apathy was mainly determined by the level of executive impair-ment (verbal fluency, working memory) and not associated withthe severity of motor symptoms [56]. Moreover, as reported before,apathy may herald cognitive decline: indeed, in the only reportedlongitudinal study [53] apathetic PD patients had more executive dif-ficulties than non-apathetic PD patients (Symbol Digit ModalitiesTest, Stroop Interference Test, verbal fluency) and, at the 18-monthfollow-up, apathetic PD patients had a higher prevalence of cognitivedecline and dementia in comparison to non-apathetic PD patients. Astudy reported that patients with apathy and anhedonia, relative topatients with depression, showed worse performances in executivetasks (Frontal Assessment Battery and phonological verbal fluency)[35]. A study reported that apathy was negatively associated to per-formances in an executive task (Wisconsin Card Sorting Test) and inepisodic memory task (Hopkins Verbal Learning Test) [36]. A recentstudy reported that apathetic PD patients had lower performancesrelative to non-apathetic PD patients in tasks of episodic memory(California Verbal Learning Test) and in executive tasks (BackwardDigit Span and Wisconsin Card Sorting Test) [57].
Globally considered, these findings suggest that, as for depression,apathy in non-demented PD patients could be strongly associatedwith executive dysfunction, although neurochemical substrates remainpoorly understood. Only two studies reported a relationship betweenapathy and poorer performances of episodic memory, therefore thisissue needs further empirical investigation.
4.3. Other affective disorders
Apart from apathy and depression, also other affective disordersmay characterize PD patients. Anxiety disorders have a current prev-alence of 25–43% [6,58] and a lifetime prevalence of 49% [6,58]. Dif-ferent anxiety disorders have been described in PD patients, such asgeneralized anxiety disorders, social anxiety disorder, panic attackdisorder and anxiety disorder not otherwise specified [58]. Anxietydisorders and depressive disorders may be comorbid in PD patients[58,59]. Only one study assessed the relationship between anxietyand cognitive functions in PD patients: authors reported that onlyanxious patients with a left-lateralized PD had working memory dif-ficulties, while anxious patients with a right-lateralized PD performedas well as healthy controls [60].
Also alexithymia may be detected in PD patients and its presence isstrongly associated to depression [61,62]. Alexithymia is an alteration inaffect regulation (including the inability to identify and describe feel-ings, difficulty distinguishing feelings from bodily sensations of emo-tional arousal, impaired symbolization and an externally orientedcognitive style, usually associated to depression [63]. Only one studyassessed the relationship between alexithymia and cognitive functionsin PD patients [64]: alexithymic PD patients had worse performancesrelative to non alexithymic PD patients in tasks requiring visuospatialprocessing, suggesting that the right hemisphere is involved in the de-velopment of alexithymic features.
5. Discussion
In this article recent studies on the relationship between affectivedisorders and cognitive functioning in non-demented PD patientshave been reviewed. PD patients without dementia present a neuro-cognitive profile characterized by deficits of executive functions,due to a neuropathology that primarily affects basal ganglia, progres-sively reducing their dopaminergic input to the prefrontal cortex.
With regard to the relationship between affective disorders andcognitive functioning, the majority of studies principally focused on
depression and apathy, two independent disorders that are often co-morbid in PD patients.
Depression and apathy in PD may be associated to different fac-tors: depression is probably related to the dysfunction of differentneurotransmitters, including dopamine, serotonin and norepineph-rine [65–71], to the effects of dopaminergic therapies on other neuro-transmitters [72] and to the amygdalar dysfunction [73–75] thataffects patients since the early stages of PD and is considered an hall-mark of depression [76]. Apathy is probably more related to thehypostimulation of OFC, an area involved in affective processing,which is affected in PD patients in moderate/advanced stages of thedisease [49–52].
Globally considered, reviewed studies provided evidence that, al-though not directly related to increased risk of dementia, in PD patientsthe presence of depression and apathymay indicate the presence of cog-nitive impairment. Indeed, depressed patients and apathetic patientshad worse performances in comparison to patients without these affec-tive disorders, especially for executive functions (both depression andapathy) and memory (almost depression). As regards the relationshipbetween executive dysfunction and depression, it must be underlinedthat findings implicating a dysfunction of frontostriatal pathways in ge-riatric depression led to the depression-executive dysfunction syndromehypothesis [77]. This hypothesis postulates that elderly patients with afrontostriatal dysfunction caused by a cerebrovascular disease or otheraging-related conditions, are predisposed for developing depression;therefore, different levels of executive deficits should be associatedwith different severity of depression, as well as to specific patterns ofdepression/executive dysfunction. Accordingly, patients with a frontal–subcortical disease like PD could be particularly vulnerable to depres-sion; indeed, in case executive dysfunction is a risk factor for depressionin the geriatric population, this association could be stronger in PD,which is characterized by a neurocognitive profile with executive dys-function as core deficit. Reviewed studies preliminary showed thatdepressed PD patients have more difficulties in executive tasks in com-parison to non-depressed patients, but further studies are needed totest the depression-executive dysfunction syndrome hypothesis in thispopulation. Further studies are needed to clarify if depression andexecutive deficits are both manifestations of the common frontostriataldysfunction or are manifestations related to different features of theneurodegenerative process (frontostriatal dysfunction for executive def-icits, serotonergic and amygdalar dysfunction for depression), even ifthese hypotheses appear as not mutually exclusive. Considering thatdepression relative to apathy had a clearer detrimental effect also onepisodic memory, a cognitive process based on temporal cortices andnot on frontostriatal circuits, depression has probably a multi-factorialetiology in PD andmay represent, however, a sign of the disease progres-sion and of a probable concomitant cognitive dysfunction (of executivefunctions and memory). Future studies should correlate scores ofdepressed and non-depressed PD patients in neuropsychological tasksand depression rating scales with measures from structural (to assessPFC atrophy) and functional (to assess frontostriatal activation duringexecutive tasks) neuroimaging [78] could clarify the neural basis of theassociation depression-executive dysfunction in PD.
As for depression, also apathy resulted independently associatedto executive dysfunction in PD, while less clear resulted the relation-ship between apathy and memory. The relationship between apathyand executive deficits suggests that both these manifestations, arerelated to the frontostriatal dysfunction of PD patients. In particularapathy may derive from a dysfunction of that orbital frontostriatalcircuit linking ventral striatum to the OFC, a circuit involved in re-ward processing. An impaired reward processing could result in aloss of motivation to action and in a blunted reactivity, as in apathy.Considering that the orbital circuit is preserved in the early clinicalmotor stages [18,19] and is affected in moderate/advanced stages ofPD [9] the appearance of apathy may be considered a sign of diseaseprogression and of an increased risk of cognitive impairment.

101M. Poletti et al. / Journal of the Neurological Sciences 317 (2012) 97–102
On the basis of these findings it could then be hypothesized that, ifdepression may appear early in the course of the disease, apathy mayappear in later stages of disease: thereafter the executive dysfunctionshould be more severe on patients with apathy than in patients withonly depression. This prediction has been confirmed by a recent studyreporting that patients with apathy and anhedonia, relative to pa-tients with depression, showed worse performances in some execu-tive tasks (Frontal Assessment Battery and verbal fluency) [35].However further studies are needed to establish if PD patients withapathy and PD patients with depression have distinct patterns of ex-ecutive deficits, in terms of severity and in terms of executive pro-cesses involved. For example, considering that apathy is probablymore dependent than depression to a dysfunction of the orbital fron-tostriatal circuit, it should be investigated how apathy and depressionare differently associated to performance in tasks that tap this circuit,as reversal learning and decision making under ambiguity.
Finally, the relationship between other affective disorders, as anx-iety and alexithymia, and cognitive functioning of PD patients is actu-ally almost unknown and needs further empirical investigation. Inconclusion, this review provided evidence that both depression andapathy are associated to an increased risk of cognitive impairmentin PD patients, especially of executive functions. The clinical implica-tion of these findings is that the best assessment and management ofPD patients should often include both neuropsychological and neuro-psychiatric evaluations and the presence of non-motor symptoms ascognitive disturbances and affective disorders especially depressionand apathy, should be investigated with patients and caregivers.
References
[1] Chaudhury KR, Healy DG, Schapira AHV. Non motor symptoms of Parkinson'sdisease: diagnosis and management. Lancet Neurol 2006;5:235–45.
[2] Aarsland D, Bronnick K, Larsen JP, Tysnes OB, Alves G, Norwegian ParkWest StudyGroup. Cognitive impairment in incident, untreated Parkinson's disease: theNorwegian ParkWest Study. Neurology 2009;72:1121–6.
[3] Muslimovic D, Post B, Speelman JD, Schmand B. Cognitive profile of patients withnewly diagnosed Parkinson disease. Neurology 2003;65:1239–45.
[4] Aarsland D, Anderson K, Larsen JP, Lolk A, Kragh-Sorensen P. Prevalence and char-acteristics of dementia in Parkinson disease. A 8-year prospective study. ArchNeurol 2003;60:387–92.
[5] Reijnders JS, Ehrt U, Weber WE, Aarsland D, Leentjens AF. A systematic review ofprevalence studies of depression in Parkinson's disease. Mov Disord 2008;23:183–9.
[6] Dissanayaka NN, Sellbach A, Matheson S, O'Sullivan JD, Silburn PA, Byrne GJ, et al.Anxiety disorders in Parkinson's disease: prevalence and risk factors. Mov Disord2010;25:838–45.
[7] Hermann LL, Goodwin GM, Ebmeier KP. The cognitive neuropsychology of depres-sion in the elderly. Psychol Med 2007;37:1693–702.
[8] McDermott LM, Ebmeir KP. A meta-analysis of depression severity and cognitivefunction. J Affect Disord 2009;119:1–8.
[9] Owen AM. Cognitive dysfunction in Parkinson's disease: the role of frontostriatalcircuitry. Neuroscientist 2004;10:525–37.
[10] Poletti M, Emre M, Bonuccelli U. Mild cognitive impairment and cognitive reservein Parkinson's disease. Parkinsonism Relat Disord 2011;17:579–86.
[11] Cools R. Dopaminergic modulation of cognitive function-implications for L-DOPAtreatment in Parkinson's disease. Neurosci Biobehav Rev 2006;30:1–23.
[12] Alexander GE, Delong MR, Strick PL. Parallel organisation of functionally segregat-ed circuits linking basal ganglia and cortex. Annu Rev Neurosci 1986;9:357–81.
[13] Frank MJ, Seeberger LC, O'Reilly RC. By carrot or by stick: cognitive reinforcementlearning in parkinsonism. Science 2004;306:1940–3.
[14] Sawamoto N, Piccini P, Hotton G, Pavese N, Thielemans K, Brooks DJ. Cognitivedeficits and striato-frontal dopamine release in Parkinson's disease. Brain 2008;131:1294–302.
[15] Miyake A, Friedman NP, EmersonMJ, Witzki AH, Howerter A, Wager TD. The unityand diversity of executive functions and their contributions to complex “frontallobe” tasks: a latent variable analysis. Cogn Psychol 2000;41:49–100.
[16] Rowe JB,Hughes L, GhoshBCP, EcksteinD,Williams-Gray CH, Fallon S, et al. Parkinson'sdisease and dopaminergic therapy: differential effects on movement, reward andcognition. Brain 2008;131:2094–105.
[17] Ardila A. On the evolutionary origins of executive functions. Brain Cogn 2008;68:92–9.
[18] Poletti M, Frosini D, Lucetti C, Del Dotto P, Ceravolo R, Bonuccelli U. Decisionmakingin de novo Parkinson's disease. Mov Disord 2010;25:1432–6.
[19] Poletti M, Cavedini P, Bonuccelli U. Iowa Gambling Task in Parkinson's disease.J Clin Exp Neuropsychol 2011;33:395–409.
[20] Aarsland D, Marsh L, Schrag A. Neuropsychiatric symptoms in Parkinson's disease.Mov Disord 2009;24:2175–86.
[21] Shiba M, Bower JH, Maragonore DM, McDonnell SK, Peterson BJ, Ahlskog JE, et al.Anxiety disorders and depressive disorders preceding Parkinson's disease: a case-control study. Mov Disord 2000;15:669–77.
[22] Weisskopf MG, Chen H, Schwarzschild MA, Kawachi I, Ascherio A. Prospective studyof phobic anxiety and risk of Parkinson's disease. Mov Disord 2003;18:646–51.
[23] Ishihara L, Brayne C. A systematic review of depression and mental illness preced-ing Parkinson's disease. Acta Neurol Scand 2006;113:211–20.
[24] Ishihara-Paul L, Wainwright NW, Khaw KT, Luben RN, Welch AA, Day N, et al.Prospective association between emotional health and clinical evidence of Parkinson'sdisease. Eur J Neurol 2008;15:1148–54.
[25] Jacob EL, Gatto NM, Thompson A, Bordelon Y, Ritz B. Occurrence of anxiety anddepression prior to Parkinson's disease. Parkinsonism Relat Disord 2010;16:576–81.
[26] Tolosa E, Gaig C, Santamaria J, Compta Y. Diagnosis and premotor phase of Parkinson'sdisease. Neurology 2009;72:S12–20.
[27] Winckler J, Ehret R, Buttner T, Dillmann U, Fogel W, Sbolek M, et al. Parkinson'sdisease risk score: moving to a premotor diagnosis. J Neurol 2011;258:S311–5.
[28] Poletti M, Bonuccelli U. Personality in patients with Parkinson's disease: assess-ment and clinical implications. J Neurol Nov 15 2011 (Epub ahead of print).
[29] Allain H, Schuck S, Mauduit N. Depression in Parkinson's disease. BMJ 2000;320:1287–8.
[30] Burn DJ. Beyond the iron mask: towards better recognition and treatment ofdepression associated with Parkinson's disease. Mov Disord 2002;17:445–54.
[31] Bayulkem K, Lopez G. Nonmotor fluctuations in Parkinson's disease: clinical spec-trum and classification. J Neurol Sci 2010;289:89–92.
[32] Costa A, Peppe A, Carlesimo GA, Pasqualetti P, Caltagirone C. Major and minor de-pression in Parkinson's disease: a neuropsychological investigation. Eur J Neurol2006;13:972–80.
[33] Stefanova E, Potrebic A, Ziropadja L, Maric J, Ribaric I, Kostic VS. Depression pre-dicts the pattern of cognitive impairment in Parkinson's disease. J Neurol Sci2006;248:131–7.
[34] Klepac N, Hajnesk S, Trkulja V. Cognitive performance in nondemented nonpsy-chotic Parkinson disease patients with or without a history of depression priorto the onset of motor symptoms. J Geriatr Psychiatry Neurol 2010;23:15–25.
[35] Santangelo G, Vitale C, Trojano L, Longo K, Cozzolino A, Grossi D, et al. Relation-ship between depression and cognitive dysfunctions in Parkinson's disease with-out dementia. J Neurol 2009;256:632–8.
[36] Butterfield LC, Cimino CR, Oelke LE, Hauser RA, Sanchez-Ramos J. The indepen-dent influence of apathy and depression on cognitive functioning in Parkinson'sdisease. Neuropsychology 2010;24:721–30.
[37] Klepac N, Trkulja V, Relja M. Nondemented Parkinson disease patients: is cogni-tive performance associated with depressive difficulties? Cogn Behav Neurol2008;21:87–91.
[38] Fernandez HH, See RH, Gary MF, Bowers D, Rodriguez RL, Jacobson C, et al.Depressive symptoms in Parkinson disease correlate with impaired global andspecific cognitive performance. J Geriatr Psychiatry Neurol 2009;22:223–7.
[39] Foltynie T, Brayne CEG, Robbins TW, Barker RA. The cognitive ability of an incidentcohort of Parkinson's patients in the UK. The CamPaIGN study. Brain 2004;127:550–60.
[40] Dujardin K, Defebvre L, Duhamel A, Lecouffe P, Rogelet P, Steinling M, et al. Cogni-tive and SPECT characteristics predict progression of Parkinson's disease in newlydiagnosed patients. J Neurol 2004;251:1383–92.
[41] Muslimovic D, Post B, Speelman JD. Cognitive profile of patients with newly diag-nosed Parkinson disease. Neurology 2005;65:1239–45.
[42] Aarsland D, Bronnick K, Williams-Gray C, Weintraub D, Marder K, Kulisevsky J,et al. Mild cognitive impairment in Parkinson's disease. A multicenter pooledanalysis. Neurology 2010;75:1052–69.
[43] Marin RS. Differential diagnosis of apathy and related disorders of diminishedmotivation. Psychiatr Ann 1997;27:30–3.
[44] Drijgers RL, Dujardin K, Reijnders JS, Defebvre L, Leentjens AF. Validation of diag-nostic criteria for apathy in Parkinson's disease. Parkinsonism Relat Disord 2010;16:656–60.
[45] Pedersen KF, Alves G, Bronnik K, Aarsland D, Tysnes OB, Larsen JP. Apathy in drug-naïve patients with incident Parkinson's disease: the Norwegian ParkWest study.J Neurol 2010;257:217–23.
[46] Dujardin K, Sockeel P, Devos D, Delliaux M, Krystkowiak P, Destèe A, et al. Charac-teristics of apathy in Parkinson's disease. Mov Disord 2007;22:778–84.
[47] OguruM, TachibanaH, Toda K,Okuda B, OkaN. Apathy and depression in Parkinson'sdisease. J Geriatr Psychiatry Neurol 2010;23:35–41.
[48] Kirsch-Darrow L, Fernandez HH, Marsiske M, Okun MS, Bowers D. Dissociatingapathy and depression in Parkinson's disease. Neurology 2006;67:33–8.
[49] Cramer CK, Friedman JH, Amick MM. Olfaction and apathy in Parkinson's disease.Parkinsonism Relat Disord 2010;16:124–6.
[50] Kunig G, Leenders KL, Martin-Solch C, Missimer J, Magyar S, Schultz W. Reduced re-ward processing in the brain of parkinsonian patients. Neuroreport 2000;11:3681–7.
[51] Martinez-Corral M, Pagonabarraga J, Llebaria G, Pascual-Sedano B, Garcia-SanchezC, Gironell A, et al. Facial emotion recognition impairment in patients withParkinson's disease and isolated apathy. Park Dis 2010:930627.
[52] Lawrence AD, Goerendt IK, Brooks DJ. Apathy blunts neural response to money inParkinson's disease. Soc Neurosci 2011;6:653–62.
[53] Dujardin K, Sockeel P, Delliaux M, Destée A, Defebvre L. Apathy may herald cogni-tive decline and dementia in Parkinson's disease. Mov Disord 2009;24:2391–7.
[54] Pluck GC, Brown RG. Apathy in Parkinson's disease. J Neurol Neurosurg Psychiatry2002;73:636–42.
[55] Weintraub D, Moberg PJ, Culbertson WC, Duda JE, Katz IR, Stern MB. Dimensionsof executive function in Parkinson's disease. Dement Geriatr Cogn Disord 2005;20:140–4.
102 M. Poletti et al. / Journal of the Neurological Sciences 317 (2012) 97–102
[56] Zgaljardic DJ, Borod JC, Foldi NS, Rocco M, Mattis PJ, Gordon MF, et al. Relationshipbetween self-reported apathy and executive dysfunction in nondemented patientswith Parkinson disease. Cogn Behav Neurol 2007;20:184–92.
[57] Varanese S, Perfetti B, Ghilardi MF, Di Rocco A. Apathy but not depression reflectsinefficient cognitive strategies in Parkinson's disease. PLoS One 2011;6:e17846.
[58] Pontone GM, Williams JR, Anderson KE, Chase G, Goldstein SA, Grill S, et al.Prevalence of anxiety disorders and anxiety subtypes in patients with Parkinson'sdisease. Mov Disord 2009;24:1333–8.
[59] Brown RG, Landau S, Hindle JV, Playfer J, Samuel M, Wilson CK, et al. Depressionand anxiety related subtypes in Parkinson's disease. J Neurol Neurosurg Psychiatry2011;82:803–9.
[60] Foster PS, Drago V, Yung RC, Skidmore FM, Skoblar B, Shenal BV, et al. Anxietyaffects working memory only in left hemibody onset Parkinson's disease patients.Cogn Behav Neurol 2010;23:14–8.
[61] Costa A, Peppe A, Carlesimo GA, Salalone G, Caltagirone C. Prevalence and charac-teristics of alexithymia in Parkinson's disease. Psychosomatics 2010;51:22–8.
[62] Poletti M, Frosini D, Pagni C, Lucetti C, Del Dotto P, Ceravolo R, et al. Alexithymia isassociated to depression in de novo Parkinson's disease. Psychother Psychosom2011;80:251–3.
[63] Taylor GJ, Bagby RM, Parker JDA. The alexithymia construct: a potential paradigmfor psychosomatic medicine. Psychosomatics 1991;32:153–64.
[64] Costa A, Peppe A, Carlesimo GA, Salamone G, Caltagirone C. Neuropsychologicalcorrelates of alexithymia in Parkinson's disease. J Int Neuropsychol Soc 2007;13:980–92.
[65] Leentjens AF, Scholtissenm B, Vreeling FW, Verhey FR. The serotonergic hypothe-sis for depression in Parkinson's disease: an experimental approach. Neuropsy-chopharmacology 2006;31:1009–15.
[66] Politis M, Wu K, Loane C, Turkheimer FE, Molloy S, Brooks DJ, et al. Depressivesymptoms in PD correlate with higher 5-HTT binding in raphe and limbic struc-tures. Neurology 2010;75:1920–7.
[67] Guttman M, Boileau I, Warsh J, Saint-Cyr JA, Ginovart N, McCluskey T, et al. Brainserotonin transporter binding in non-depressed patients with Parkinson's disease.Eur J Neurol 2007;14:523–8.
[68] Beucke JC, Uhl I, Plotkin M, Winter C, Assion HJ, Endrass T, et al. Serotonergic neu-rotransmission in early Parkinson's disease: a pilot study to assess implicationsfor depression in this disorder. World J Biol Psychiatry 2010;11:781–7.
[69] Tan SK, Hartung H, Sharp T, Temel Y. Serotonin dependent depression in Parkinson'sdisease: a role for the subthalamic nucleus? Neuropharmacology 2011;61:387–99.
[70] Remy Doder M, Lees A, Turjanski N, Brooks D. Depression in Parkinson's disease:loss of dopamine and noradrenaline innervation in the limbic system. Brain2005;128:1314–22.
[71] Brooks DJ, Piccini P. Imaging in Parkinson's disease: the role of monoamines inbehavior. Biol Psychiatry 2006;59:908–18.
[72] Eskow Jauranais KL, Angoa-Pereze M, Kuhn DM, Bishop C. Potential mechanismsunderlying anxiety and depression in Parkinson's disease: consequences of L-DOPAtreatment. Neurosci Biobehav Rev 2011;35:556–64.
[73] Ouchi Y, Yoshikawa E, Okada H, Futatsubashi M, Sekine Y, Iyo M, et al. Alterationsin binding site density of dopamine transporter in the striatum, orbitofrontal cortex,and amygdala in early Parkinson's disease: compartment analysis for -CFT bindingwith positron emission tomography. Ann Neurol 1999;45:601–10.
[74] Tessitore A, Hariri AR, Fera F, Smith WG, Chase TN, Hyde TM, et al. Dopaminemodulates the response of human amygdala: a study in Parkinson's disease.J Neurosci 2002;22:9099–103.
[75] Yoshimura N, Kawamura M, Masaoka Y, Homma I. The amygdala of patients withParkinson's disease is silent in response to fearful facial expressions. Neuroscience2005;131:523–34.
[76] Bellani M, Baiano M, Brambilla P. Brain anatomy of major depression. II Focus onamygdala. Epidemiol Psychiatr Sci 2011;20:33–6.
[77] Alexopoulos GS. Role of executive function in late-life depression. J Clin Psychiatry2003;64(S14):18–23.
[78] Koerts J, Leenders KL, Koning M, Portman AT, van Beilen M. Striatal dopaminergicactivity (FDOPA_PET) associated with cognitive items of a depression scale(MADRS) in Parkinson's disease. Eur J Neurosci 2007;25:3132–6.
[79] Chudasama Y, Robbinds TW. Functions of frontostriatal systems: comparativeneuropsychopharmacological studies in rats, monkeys and humans. Biol Psychol2006;73:19–38.
Related Documents











