ORIGINAL ARTICLE Affective response to the menstrual cycle as a predictor of self-reported affective response to alcohol and alcohol use Jeff Kiesner Received: 5 January 2012 / Accepted: 7 August 2012 / Published online: 23 August 2012 # Springer-Verlag 2012 Abstract Past research suggests that women with premen- strual syndrome (PMS) have higher levels of alcohol use/ abuse. The present study was conducted to test the hypothesis that women with diverse patterns of affective response to the menstrual cycle (PMS pattern, mid-cycle pattern, and noncy- clical pattern) would show mean-level differences on meas- ures of self-reported affective response to alcohol, alcohol use, and sleep changes following alcohol use. All participants from an initial study of n 0 213 college-aged women who had prospectively completed daily questionnaires for two full menstrual cycles were asked to complete a one-time retro- spective questionnaire regarding their alcohol use and typical affective response when consuming alcohol. From that original study, n 0 161 also participated in the present study. Results showed significant differences, in the expected direction, on three out of five measures (hard alcohol use, negative affective response to alcohol, and change in sleep following alcohol use). Women in the PMS pattern group reported (retrospectively) higher levels of hard alcohol use, a less negative affective response associated with alcohol use, and lower levels of sleep changes in relation to alcohol use, as compared to the mid-cycle group. The discussion considers potential mechanisms that may be responsible for these associations (i.e., GABA A modulation). Keywords PMS . PMDD . Menstrual cycle . Alcohol . Affect Research has shown a relation between alcohol consump- tion and symptoms of premenstrual syndrome/premenstrual dysphoric disorder (PMS/PMDD). However, recent research indicates that, whereas some women show no cyclical change in negative affect (e.g., anxiety and depression) associated with the menstrual cycle and other women show a classic PMS type of trajectory (symptoms high premen- strually and low around ovulation), other women show high levels of negative affect around ovulation and low levels premenstrually—the mirror opposite of a PMS pattern (Kiesner 2011; mid-cycle group). It was proposed by Kiesner (2011) that identifying this group would provide a novel comparison group for future research, thus allowing more specific hypothesis testing for a variety of problems potentially associated with individual response to the men- strual cycle. The present study takes this approach by com- paring alcohol-use variables across groups of women who (a) experience a classic PMS pattern of affective change, (b) experience the mid-cycle pattern of affective change, and (c) show no cyclic change in affect. PMS and alcohol consumption Several survey studies have used large nonclinical samples with retrospective reports to examine the relations between premenstrual symptoms and alcohol consumption. In one such study, using computerized telephone interviews with a sample of women between 18 and 44 years old (n 0 874), the 8.3 % who were identified as experiencing PMS symptoms demonstrated higher levels of alcohol consumption as com- pared to those not experiencing PMS symptoms (Deuster et al. 1999). In another study, using computer-assisted inter- views (n 0 11,648; 18–55 years old), alcohol consumption among “PMS cases” (19 % of sample) was significantly higher than use among noncases (Strine et al. 2005). A third study, using a large-sample mail survey of active-duty fe- male military personnel (n 0 6,026), also found higher alco- hol use among women experiencing PMS symptoms J. Kiesner (*) Dipartimento di Psicologia DPSS, Università degli Studi di Padova, via Venezia 8, 35131 Padua, Italy e-mail: [email protected] Arch Womens Ment Health (2012) 15:423–432 DOI 10.1007/s00737-012-0303-1 Author's personal copy

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ORIGINAL ARTICLE
Affective response to the menstrual cycle as a predictorof self-reported affective response to alcohol and alcohol use
Jeff Kiesner
Received: 5 January 2012 /Accepted: 7 August 2012 /Published online: 23 August 2012# Springer-Verlag 2012
Abstract Past research suggests that women with premen-strual syndrome (PMS) have higher levels of alcohol use/abuse. The present study was conducted to test the hypothesisthat women with diverse patterns of affective response to themenstrual cycle (PMS pattern, mid-cycle pattern, and noncy-clical pattern) would show mean-level differences on meas-ures of self-reported affective response to alcohol, alcohol use,and sleep changes following alcohol use. All participants froman initial study of n0213 college-aged women who hadprospectively completed daily questionnaires for two fullmenstrual cycles were asked to complete a one-time retro-spective questionnaire regarding their alcohol use and typicalaffective response when consuming alcohol. From that originalstudy, n0161 also participated in the present study. Resultsshowed significant differences, in the expected direction, onthree out of five measures (hard alcohol use, negative affectiveresponse to alcohol, and change in sleep following alcohol use).Women in the PMS pattern group reported (retrospectively)higher levels of hard alcohol use, a less negative affectiveresponse associated with alcohol use, and lower levels of sleepchanges in relation to alcohol use, as compared to the mid-cyclegroup. The discussion considers potential mechanisms that maybe responsible for these associations (i.e., GABAAmodulation).
Keywords PMS . PMDD .Menstrual cycle . Alcohol .
Affect
Research has shown a relation between alcohol consump-tion and symptoms of premenstrual syndrome/premenstrualdysphoric disorder (PMS/PMDD). However, recent research
indicates that, whereas some women show no cyclicalchange in negative affect (e.g., anxiety and depression)associated with the menstrual cycle and other women showa classic PMS type of trajectory (symptoms high premen-strually and low around ovulation), other women show highlevels of negative affect around ovulation and low levelspremenstrually—the mirror opposite of a PMS pattern(Kiesner 2011; mid-cycle group). It was proposed byKiesner (2011) that identifying this group would provide anovel comparison group for future research, thus allowingmore specific hypothesis testing for a variety of problemspotentially associated with individual response to the men-strual cycle. The present study takes this approach by com-paring alcohol-use variables across groups of women who(a) experience a classic PMS pattern of affective change, (b)experience the mid-cycle pattern of affective change, and (c)show no cyclic change in affect.
PMS and alcohol consumption
Several survey studies have used large nonclinical sampleswith retrospective reports to examine the relations betweenpremenstrual symptoms and alcohol consumption. In onesuch study, using computerized telephone interviews with asample of women between 18 and 44 years old (n0874), the8.3 % who were identified as experiencing PMS symptomsdemonstrated higher levels of alcohol consumption as com-pared to those not experiencing PMS symptoms (Deuster etal. 1999). In another study, using computer-assisted inter-views (n011,648; 18–55 years old), alcohol consumptionamong “PMS cases” (19 % of sample) was significantlyhigher than use among noncases (Strine et al. 2005). A thirdstudy, using a large-sample mail survey of active-duty fe-male military personnel (n06,026), also found higher alco-hol use among women experiencing PMS symptoms
J. Kiesner (*)Dipartimento di Psicologia DPSS,Università degli Studi di Padova,via Venezia 8,35131 Padua, Italye-mail: [email protected]
Arch Womens Ment Health (2012) 15:423–432DOI 10.1007/s00737-012-0303-1
Author's personal copy

(Hourani et al. 2004). Finally, using a much smaller sampleof female university students (n0194), a significant positiveassociation was found between severity of PMS symptomsand weekday alcohol consumption, but not weekend alcoholconsumption (Perry et al. 2004). This difference acrossweekday and weekend drinking suggests that, for college-aged women, the association between PMS symptoms andalcohol consumption is moderated by the social context ofdrinking (e.g., weekend parties and binge drinking).
Not all survey studies, however, have found support forthis association. For example, in a study of military womenliving on naval ships (n02,912), results showed no consis-tent relations between alcohol consumption and seven dif-ferent menstrual symptoms (Kritz-Silverstein et al. 1999).However, because of contextual characteristics specific tolife on a naval ship and because the measurement of men-strual symptoms included only physical characteristics ofmenstruation (no affective variables, such as depression,were assessed), conclusions are limited. In another study,using a sample of premenopausal and early perimenopausalwomen between 42 and 52 years old (n02,758), an inverserelation between alcohol use and premenstrual anxiety/mood was found (Gold et al. 2007). However, because thesample included both premenopausal and perimenopausalwomen and because 71 % of the sample was positive forpremenstrual anxiety, there are serious concerns about inter-pretation. Finally, two published reports based on the samedata of university students (n075) who were identified associal drinkers found no association between menstrual andpremenstrual symptoms and alcohol consumption (Charetteet al. 1990; Tate and Charette 1991). Although these studiesprospectively measured both menstrual/premenstrual symp-toms and alcohol consumption, selection criteria may haveresulted in range restriction on the measures of alcohol use(heavy drinkers were excluded) and premenstrual symptoms(no change in negative affect was observed across the men-strual cycle). Moreover, as noted above, alcohol consump-tion among university students may be more stronglydetermined by social context than by other factors, at leaston the weekend (e.g., Perry et al. 2004).
Research considering PMS/PMDD as a diagnosis, on theother hand, has provided stronger and more consistent evi-dence in support of an association between premenstrualdifficulties and alcohol consumption. For example, onestudy compared women with prospectively confirmedPMS (n021, M038 years) and normal controls (n016,M032 years) on daily ratings of affective symptoms andalcohol consumption across two full menstrual cycles.Results showed that women with PMS consumed signifi-cantly more alcohol than controls, but that alcohol consump-tion was not associated with menstrual phase (Tobin et al.1994). Moreover, there was no association between moodsymptom severity and alcohol use, suggesting that drinking
does not fluctuate in response to affective symptoms of themenstrual cycle.
Similarly, several studies using larger clinical samples ofPMS patients and controls have also found evidence for thisassociation. For example, Caan et al. (1993) comparedwomen with PMS (n0102, mean age of participants wasnot presented) and matched controls (n0102, matched byage and race; the only information on age, for either group,was that they were matched) on alcohol consumption during3 days of the premenstrual phase and 3 days of the post-menstrual phase. Results showed that women with PMSconsumed more alcohol during the postmenstrual phase,but not during the premenstrual phase. Because the differ-ence was found postmenstrually, the authors concluded thatthe observed difference in alcohol consumption was proba-bly not a result of self-medication to tolerate PMS symp-toms. Also, based on a large sample of women with PMS(n0190, M034 years) and women without PMS (n0182,M033 years), those with PMS showed higher levels of drugand alcohol use (not measured specific to the phase ofmenstrual cycle) than those without PMS (Chuong andBurgos 1995). Finally, Halliday et al. (1986) comparedPMS patients (n095, M034 years) and control patientsvisiting a general gynecological clinic for routine checkups(n0147, M030 years) and found that 21 % of the PMSpatients met the criteria for alcohol abuse and dependence,but only 12 % of the controls met this criteria—a statistical-ly significant difference.
Together, the evidence presented above provides substan-tial support for an association between PMS symptoms andalcohol use. However, recent findings on individual differ-ences in response to the menstrual cycle suggest that onepattern of affective change associated with the menstrualcycle has been overlooked. Research considering this addi-tional response pattern may provide important insights forunderstanding the association between PMS and alcoholuse.
Individual differences in response to the menstrual cycleand alcohol
Recent research regarding affective changes to the menstru-al cycle has underlined the importance of considering indi-vidual differences in these changes. For example, researchhas shown that, although physical and psychological symp-toms of the menstrual cycle are correlated (Kiesner 2009),there is a wide range of variability in these associations, withsome women demonstrating negative psychological changesand others positive psychological changes, in relation to thesame physical symptoms of the menstrual cycle (Kiesnerand Pastore 2010). Moreover, using a sample of 213 femaleuniversity students who completed daily symptom
424 J. Kiesner
Author's personal copy

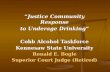
questionnaires for two menstrual cycles (i.e., daily reports ofsymptoms and menstruation for approximately 2 months),Kiesner (2011) showed that, in addition to women whodemonstrate the classic PMS pattern of symptom changes(61 %) and individuals demonstrating no cyclical change insymptoms (26 %), some women demonstrated a mid-cyclepattern of symptom changes (13 %)—with negative affectbeing highest around ovulation and lowest perimenstrually(see Fig. 1, which presents the average group trajectories onsymptoms of depression and anxiety across two menstrualcycles, separately for these four groups). These results, andothers (Bancroft et al. 1987; Schmidt et al. 1998), suggestthat some women respond positively, some respond nega-tively, and some show no changes to the same hormonalchanges.
Comparing women who demonstrate these very diversepatterns of response to the menstrual cycle may provideinsight for why women with PMS symptoms show higherlevels of alcohol use and abuse. Specifically, it could behypothesized that individual differences in response to themenstrual cycle will be correlated with individual differ-ences in response to alcohol. This is based on evidence thatthe effects of progesterone metabolites and alcohol sharecommon neurological substrates and that positive/negativeeffects associated with these progesterone metabolites maybe associated with similar positive/negative effects of alco-hol. Specifically, it has been shown that GABAA modula-tors, including allopregnanolone (a progesterone metabolitethat is associated with PMS/PMDD), benzodiazepine, andalcohol, demonstrate both beneficial effects on mood, suchas relaxation and anxiolysis, as well as negative effects onmood including anxiety and irritability (Andréen et al.2009). This paradoxical effect of GABAA modulators
appears to depend both on a dose–response curve as well asindividual differences across women (Andréen et al. 2009). Inthe context of the present study, because women who show aPMS pattern and those who show a mid-cycle pattern appearto have a mirror opposite response to the menstrual cycle andpresumably to the fluctuations in the associated steroids, theymay also show different responses to alcohol, and as a conse-quence, different alcohol-use patterns.
Based on research demonstrating individual differencesin response to the menstrual cycle and the possible role ofGABAA modulators, comparing the PMS pattern and themid-cycle pattern groups could be especially important andinformative. Specifically, because these groups appear todemonstrate opposite responses to the hormonal changesof the menstrual cycle, their response to alcohol may alsodiffer in a similar way. At a theoretical level, for understand-ing the causal mechanisms of the associations between PMSsymptoms and alcohol use, this comparison is potentiallymore informative and powerful than the comparison be-tween PMS and “normal controls.” Moreover, at a practicallevel, now that the mid-cycle pattern has been identified, itmust be considered in the same way that normal controlsmust be considered: Research should consider as much ofthe variability in individual response as can be measured.
Therefore, in the present study, we test whether womenwith a classic PMS pattern of mood changes, women withthe mid-cycle pattern of changes, and women with no cy-clical changes in mood across the menstrual cycle differfrom each other on their self-reported affective response toalcohol and their alcohol use. Alcohol use is consideredbecause, as discussed above, past research has shown thatwomen with PMS have higher levels of alcohol use andabuse. Affective response to alcohol is considered because itprovides a theoretically driven explanatory mechanism thatcould help explain why women who experience a PMSpattern of affective symptoms across the menstrual cyclemay use more alcohol: They may have a more positive/lessnegative affective response to alcohol, creating a more rein-forcing context for alcohol use.
Our first and primary hypothesis was that women with aPMS pattern would show either a more positive affectiveresponse to alcohol or a less negative affective response toalcohol, or both. These differences would be consistent withheavier drinking among women with PMS: More positiveexperiences and/or less negative experiences would be as-sociated with more alcohol use. Thus, our second hypothesiswas that women with a PMS pattern would show higherlevels of self-reported alcohol consumption. Together, thesehypotheses are consistent with past research showing thatheavy drinkers, as compared to light drinkers, show aheightened sensitivity to the stimulant/positive effects ofalcohol and weaker sedative/aversive effects (Holdstock etal. 2000; King et al. 2002).
Dep
ress
ion/
Anx
iety
1
1.2
1.4
1.6
1.8
2
2.2
2.4
2.6
0.0 0.5 1.0 1.5 2.0
Menstrual Cycle
Mid-Cycle Pattern (n=27)
PMS Pattern 1 (n=51)
PMS Pattern 2 (n=79)
Non-Cyclic (n=56)
Fig. 1 Trajectory of depression/anxiety scores across two menstrualcycles plotted separately for the four trajectory groups (lines are basedon fourth-order polynomial regressions). Used with permission fromKiesner (2011)
Response to the menstrual cycle and alcohol consumption 425
Author's personal copy

Based on these hypotheses, it should also be expectedthat, if women with a PMS pattern of response to themenstrual cycle consume more alcohol and report morefavorable affective response to alcohol, these two sets ofvariables should also be correlated: alcohol use should beassociated with affective response to alcohol.
Finally, although sleep changes are not an affective re-sponse to alcohol, we measured sleep changes because theyare commonly correlated with affective disturbances includ-ing major depression and PMS/PMDD (DSM-IV; AmericanPsychiatric Association 1994) and may also be affected byalcohol consumption (Brown et al. 1987). For example,correlational research suggests that, among college students,alcohol consumption leads to disruptions in sleep schedule,which lead to daytime sleepiness, which in turn leads tolower grade point average (Singleton and Wolfson 2009).Moreover, laboratory studies have shown that alcohol ad-ministration suppresses the phasic aspects of rapid eyemovement sleep (Feige et al. 2006) and inhibits parasympa-thetic nerve activity, thus interfering with the restorativefunction of sleep (Sagawa et al. 2011). These effects ofalcohol may vary across individuals and may be associatedwith menstrual cycle response pattern. Thus, consistent withthe above hypothesis that the PMS pattern group wouldreport a less negative affective response to alcohol, it wasalso hypothesized that the PMS pattern group would reportlower levels of sleep change associated with alcoholconsumption.
Method
Participants
Participants were 161 female university students with amean age of M022 years (SD02.67), who had participatedin an earlier study on individual difference in affectiveresponse to the menstrual cycle (Kiesner 2011) and whoagreed to participate in this follow-up study. Participantswere compensated for their participation in this follow-upstudy with a gift certificate for a book/music store. TheEthics Committee of Psychological Research of theUniversity of Padua approved this study, and all participantssigned an informed consent.
In the initial study, all first year female psychology stu-dents were asked to participate, and efforts were made toinclude women both with and without menstrual difficulties.Individuals could not participate in the initial study if theywere using hormonal contraceptives (HC) or therapy, butthis criterion was not applied to the follow-up. Thus, if theybegan using hormonal contraception between the initialstudy and the current study (a 1- to 2-year time interval),they were allowed to participate. Further details of subject
recruitment can be found in Kiesner (2011). Of the original213 participants from the initial study, n0178 agreed toparticipate in this follow-up study and provided data.However, 17 of those participants reported never havingtried alcohol and were, therefore, excluded from the presentanalyses, resulting in a final sample size of n0161.
Measures
Individual response to the menstrual cycle
In the initial study, 213 participants provided prospectivedaily reports, for two full menstrual cycles, of psychologicaland physical symptoms that are commonly associated withthe menstrual cycle. The average length of the two consec-utive menstrual cycles was M060.05 days, and the averagenumber of questionnaires for each participant was M055.09. Thus, on average, participants missed only 5 of thedaily questionnaires across the two menstrual cycles, and atotal of 11,735 questionnaires were included in those anal-yses. Although a variety of symptoms were measured, thedata analysis in the initial study examined affective symp-toms of depression and anxiety.
Based on these prospective daily reports of depressionand anxiety, the 213 participants were classified into fourgroups. The trajectory of change in depression/anxietyacross two menstrual cycles for each of these four groupsis presented in Fig. 1 (taken from Kiesner 2011). Thesegroups, based on data collected 1–2 years prior to thepresent study, are the groups that are used for the presentdata analyses.
Response to alcohol
A 17-item retrospective questionnaire was used to measureindividual response to alcohol consumption. For 16 items,participants were asked the question “When you drink alco-hol, do you feel/have…,” followed by a list of 16 affectivestates/emotions, with a yes/no response format. The emo-tional states were anxious, tense, depressed, down, cryingspells, sad, mood swings, irritable, happy, serene, relaxed,social, active, tired, nervous, and aggressive. Ayes responsewas coded as “1” and a no response was coded “0.”
Two subscales were created and used for the followinganalyses. One subscale was created for negative affectiveresponse to alcohol, and one subscale was created for pos-itive affective response to alcohol. Nine items were used forthe negative affective response scale. Specifically, theseitems were anxious, tense, depressed, down, sad, moodswings, irritable, nervous, and aggressive. The internal re-liability of this subscale was good (!00.68). The positiveaffective response scale included the following five items:
426 J. Kiesner
Author's personal copy

happy, serene, relaxed, social, and active. This scale alsoshowed good internal reliability (!00.60).
These measures were used because they would allow themeasurement of affective experiences that are also experi-enced in relation to the menstrual cycle and because they aresimilar to response expectations previously measured inresearch on alcohol use, such as the Alcohol ExpectancyQuestionnaire (AEQ; Brown et al. 1987). However, thismeasure was used rather than, for example, the AEQ, fortwo reasons. First, it allowed us to focus specifically onaffective symptoms, thus excluding general evaluative state-ments about alcohol or statements regarding other people’sresponse to alcohol, such as “After a few alcoholic drinks,people are less aware of what is going on around them,”“Having a few drinks is a nice way to celebrate specialoccasions,” and “Alcohol seems like magic,” that are foundin the AEQ. Second, it allowed us to keep the questionnaireshort (the AEQ has 90 questions).
In addition to these affective responses to alcohol, par-ticipants were also asked “If you drink alcohol at night,does your sleep change?” Participants could select one ofthree responses: “sleep more,” “sleep less,” and “nochange.” The “sleep more” and “sleep less” responseswere combined into one level, termed “change in sleep.”This was done for two reasons. First, combining theseresponses is consistent with research on depression andPMS, in which changes in sleep are considered as ageneral symptom, without distinguishing between in-creased sleep or decreased sleep. Second, because of lowbase rates, combining these two responses provided morestatistical power in the analyses. Thus, this variable hastwo levels: “change in sleep” and “no change in sleep,” inresponse to alcohol use.
Alcohol use
Alcohol use was measured with six questions asking aboutthe frequency and quantity of alcohol consumption duringthe last month. Specifically, the following two questionswere asked separately for wine/spritzer, beer, and hard alco-hol: “How often in the last month have you drank wine/spritzer?” and “Usually, when you do drink wine/spritzer,how many glasses do you drink?” The response for the firstquestion (frequency) was given on a Likert type of scaleranging from 00“never,” 10“1–3 times during the month,”20“1–3 times per week,” 30“4–6 times per week,”40“every day.” For the second question (quantity), partic-ipants were asked to write in a number. For each type ofalcohol (wine/spritzer, beer, and hard alcohol), the frequen-cy score was multiplied by the quantity score, resulting in asingle measure of alcohol consumption during the lastmonth of each type of alcohol. Based on the initial analysesof these scores, the wine/spritzer and beer scores were
combined together and the hard liquor score was treatedseparately. Therefore, there were two alcohol use measures.
Procedure
Appointments were made for a research assistant to meetwith each participant individually during one of the first3 days of their menstruation. This appointment was madeto provide a brief explanation of the study and to provideclarifications of questions when needed. The full question-naire regarding alcohol use was completed during this meet-ing. The general explanation did not focus on specifichypotheses, but rather explained that, whereas the initialstudy focused on how each individual may have a differentexperience related to the menstrual cycle, the present studyfocused on how each individual may have a different expe-rience related to alcohol use.
Results
The following analyses focused on three of the four men-strual cycle response groups (see Fig. 1): PMS pattern 1 (n038); mid-cycle group (n023); and the noncyclic group (n042). The PMS pattern 2 group was not included because,although they did demonstrate a cyclical change in affect, itwas a much weaker change than the PMS pattern 1 group.Therefore, only the three groups that showed the clearest/strongest pattern were included. However, it should be notedthat all of the following analyses were also conducted in-cluding the PMS pattern 2 group (n058) combined with thePMS pattern 1 group (as a combined single group), and theresults, significance tests, and conclusions did not changeacross analyses.
Descriptive statistics and correlations
The 17 participants who had never tried alcohol could not beincluded in these analyses because they had never experi-enced the effects of alcohol. However, for descriptive pur-poses, 10 % of the PMS group, 11 % of the noncyclic group,and 4 % of the mid-cycle group had never tried alcohol (nostatistical association was found between group membershipand having ever tried alcohol; "201.13, p00.57).
Of the 103 participants included in these analyses, n015reported using HC at the time of this data collection. Therewere no differences between women using HC and those notusing HC on the measures of beer and wine consumption(t00.15, ns), hard alcohol consumption (t00.87, ns), nega-tive affective response to alcohol (t01.08, ns), or positiveaffective response to alcohol (t00.78, ns). There was also noassociation between using HC and menstrual cycle responsegroup ("204.27, p00.11).
Response to the menstrual cycle and alcohol consumption 427
Author's personal copy

Although no mean-level differences were found betweenthe HC users and the nonusers, the use of HC could affectthe relations among variables. Therefore, the main hypoth-eses were tested both including and excluding HC users. Aswill be shown below, there were no differences across theseanalyses.
Correlations were calculated for the two alcohol-use var-iables and the two affective response variables. The twomeasures of alcohol use were significantly correlated (r00.45, p<0.001). However, the correlation between positiveand negative affective response to alcohol was small andnonsignificant (r0!0.15, p00.14), and none of the correla-tions between affective response to alcohol or alcohol usewere significant (all |r|"0.12). Although the overall patternof correlations was similar across the three groups, onedifference is worth mentioning: The correlation betweenthe two measures of alcohol use differed across the threegroups: r00.60 (p<0.0001), for the PMS pattern group; r00.49 (p00.02), for the mid-cycle group; and r00.36 (p00.02), for the noncyclic group. Although these differenceswere not statistically significant, this appears to be the resultof low statistical power. For example, when the parallelcorrelations were compared in the analyses combining thePMS pattern 1 and 2 groups (n096), the correlation for thatcombined group was r00.75 (p<0.0001), and Fisher’s r-to-ztransformations showed a significant difference between thecombined PMS pattern group and the noncyclic group (z03.12, p<0.002, two-tailed) and a marginally significant dif-ference between the combined PMS pattern group and themid-cycle group (z01.77, p00.08, two-tailed). Therefore,group differences may exist in the correlation between hardalcohol consumption and beer/wine consumption.
Group differences
To test for differences across the three menstrual responsegroups on the measures of affective response to alcohol andalcohol consumption, four one-way analyses of variance(ANOVAs) were conducted using menstrual cycle responsegroup as the only between-subjects factor. Tests of homo-geneity of variance across groups indicated that the groupsdiffered significantly in their variance on the measures ofhard alcohol consumption, beer and wine consumption, andnegative affective response to alcohol. Although ANOVAsare generally robust to violations of homoscedasticity, thisrobustness breaks down when sample size differs acrossgroups, as was the case in the present study. Therefore, forhard alcohol consumption, beer and wine consumption, andnegative affective response to alcohol, robust WelchANOVAs were used, allowing for unequal variance.
A significant effect of group was found for hard alcoholconsumption (FWelch(2, 66.64)03.85, p00.02, when includ-ing HC users, and FWelch(2, 56.15)04.53, p00.02, when
excluding HC users). The means are presented in Fig. 2a(based on data including HC users) and show that the PMSpattern group showed higher levels of hard alcohol con-sumption and the mid-cycle group the lowest level.Because a primary hypothesis was that the PMS pattern 1group and the mid-cycle group would differ, we directlycontrasted these two groups with a t test allowing for un-equal variance, which was significant (t0!2.38, p00.02,two-tailed). No significant effect of group was found forbeer and wine consumption (FWelch(2, 66.09)00.34, p00.71, when including HC users, and FWelch(2, 56.95)00.52, p00.60, when excluding HC users).
A significant group effect was found for negative affec-tive response to alcohol (FWelch(2, 45.10)05.70, p00.006,when including HC users, and FWelch(2, 34.34)06.31, p00.005, when excluding HC users). The means are presentedin Fig. 2b (based on data including HC users) and show thatthe mid-cycle group reported the highest level of negativeaffect associated with alcohol use, whereas the PMS patterngroup demonstrated the lowest level. Again, we directlycontrasted the PMS pattern 1 and mid-cycle groups using
Fig. 2 Means for a hard alcohol consumption and b negative affectassociated with alcohol presented separately for menstrual cycle re-sponse group. Error bars indicate the standard error for each group
428 J. Kiesner
Author's personal copy

a t test allowing for unequal variance and found a significantdifference (t02.10, p00.05, two-tailed). No significant ef-fect for group was found for the positive affective responseto alcohol (F(2, 100)00.18, p00.84, when including HCusers, and F(2, 85)00.49, p00.61, when excluding HCusers).
To test for differences in sleep changes related to alcoholuse, a "2 test was used, crossing change in sleep (yes, no)with menstrual cycle response group. A significant associa-tion was found ("207.73, p00.02, when including HCusers, and "209.00, p00.01, when excluding HC users).Women in the PMS pattern group and the noncyclic groupshowed a similar proportion of women reporting change insleep following alcohol use (26 and 33 %, respectively),whereas for the mid-cycle group, approximately 61 %reported change in sleep following alcohol use (based ondata including HC users).
Discussion
The present study was conducted to test for mean-leveldifferences in alcohol use and affective response to alcohol,across groups of women who demonstrate different patternsof affective response to the menstrual cycle. It was expectedthat women with a PMS pattern would show higher levels ofalcohol use and either a more positive affective response toalcohol or a less negative affective response to alcohol, orboth. It was also expected that affective response to alcohol(positive, negative, or both) would be associated with alco-hol use and, thus, could explain possible group differencesin alcohol use. Changes in sleep following alcohol con-sumption were also expected.
Results confirmed most of these hypotheses. Asexpected, women with a PMS pattern of response to themenstrual cycle reported higher levels of hard alcohol con-sumption, but not beer and wine consumption. Second,women with the PMS pattern also reported lower levels ofnegative affective response to alcohol, although no differ-ences were found for positive affective response to alcohol.Moreover, group differences were found for self-reportedchanges in sleep following alcohol use. However, there wasno evidence that alcohol consumption was associated withpositive or negative affective response to alcohol in thissample.
As proposed in the introduction, group differences inalcohol consumption and affective response to alcohol couldbe the result of individual differences in response toGABAA modulators, such as allopregnanolone and alcohol.That is to say, women who demonstrate different responsepatterns to the menstrual cycle may have underlying differ-ences in their response to allopregnanolone, which may alsobe evident in their response to alcohol. This hypothesis is
based on work by Andréen et al. (2009) who argue thatGABAA modulators (including allopregnanolone and alco-hol) show paradoxical biphasic effects on mood and thatsignificant individual differences exist in these responses.Thus, the present hypothesis is based on the idea that there isan underlying variable of individual response to GABAA
modulators, and this difference predicts the response to bothmenstrual cycle-related fluctuations in GABAA steroids, aswell as to alcohol.
The present study provides indirect evidence for thishypothesis by showing that women with different menstrualcycle response profiles (i.e., PMS pattern group and mid-cycle group) report different affective responses to alcohol,as well as different levels of alcohol use. Future researchshould attempt to study these processes with more objectivemeasures of alcohol effects and the associations betweenalcohol effects and the menstrual cycle, such as performance(Mumenthaler et al. 2001) and alcohol metabolism (Haddadet al. 1998).
Interestingly, research has demonstrated a causal associ-ation between alcohol use and serum levels of allopregna-nolone. Independent of PMS status, a low-dose alcoholinfusion in a laboratory setting was found to decrease serumconcentrations of allopregnanolone during the late lutealphase, but not the follicular phase (Nyberg et al. 2005).On the other hand, Torres and Ortega (2003) found in-creased levels of allopregnanolone and progesterone amongadolescent girls treated in an emergency care center foracute alcohol intoxication, as compared to a control groupseen in the same facility for mild trauma (sprains and con-tusions). These differences were found both during thefollicular and luteal phases of the menstrual cycle.Although this difference was attributed to acute alcoholintoxication, all of the girls seen for intoxication alsoreported habitual–weekly intoxication, and therefore, thesedifferences may also have been attributable to chronicallyhigh levels of alcohol use. Although the results of these twostudies appear to contradict each other, there are importantdifferences in alcohol dose, context, and drinking history,which make these results impossible to compare directly.Nonetheless, it does seem that alcohol consumption modu-lates the availability of progesterone and allopregnanoloneand that these effects may differ in relation to alcoholdosage.
The importance of the association between alcohol con-sumption and altered levels of allopregnanolone is that itsuggests a second path for an association between affectiveresponse to the menstrual cycle and alcohol use. The firstpath, as described above, is that women with a PMS patternwould have a more positive/less negative experience withalcohol, which would result in higher levels of alcohol use.The second path is that alcohol use modulates the availabil-ity of allopregnanolone, which then has further modulatory
Response to the menstrual cycle and alcohol consumption 429
Author's personal copy

effects on GABAA systems, in addition to, in competitionwith, or interacting with alcohol’s effects on the sameGABAA system. Such effects will be difficult to study, butmay provide important understanding of how these substan-ces influence each other and affect the same GABAA
systems.Although the observed group differences are fairly clear
when comparing the PMS pattern group and the mid-cyclegroup, they are slightly less clear when considering thenoncyclic group. For example, on the measures of hardalcohol consumption and changes in sleep following alcoholuse, the noncyclic group was more similar to the PMSpattern group, whereas on the negative affective responseto alcohol, the noncyclic group was closer to the mid-cyclegroup. Any attempt to explain this pattern, based on thecurrent data or theory, would be purely speculative.
Initially, the lack of association between affective re-sponse to alcohol and alcohol use may seem surprising.However, as noted in the introduction, among college stu-dents, alcohol consumption is likely to depend heavily onsocial context. For example, previous research has found anassociation between PMS symptoms and weekday alcoholconsumption, but not weekend alcohol consumption (Perryet al. 2004), suggesting that drinking motivations changeacross the week (see also, Orcutt and Harvey 1991). Asimilar mechanism may have been present with the currentsample of college students and may have thus biased theresults. Detailed assessment of daily alcohol use, socialcontext of use, and affective state following alcohol use willlikely be helpful for better understanding these associations.
Related to this possible bias created by age and drinkingcontext, it could be hypothesized that the association be-tween affective response to alcohol and alcohol consump-tion will be evident only across a developmental period inwhich alcohol use is less dependent on social rituals. That isto say, in the social context of college, affective response toalcohol may be relatively unimportant, but may emerge asan important factor later in life. The role of affective re-sponse to alcohol may emerge through processes of cumu-lative consequences of repeated positive or negativeexperiences conditioning the individual’s expectations andconsumption; or contemporary consequences that simplybecome relatively more important to an adult, as comparedto a 20-year-old. Further research, possibly with older, non-university age groups, will be needed to clarify theseassociations.
Comment should be made about group differences in thecorrelational results. Group differences were observed in thecorrelations between hard alcohol consumption and beerand wine consumption, with the PMS pattern group show-ing the strongest correlation and the noncyclic group theweakest correlation. One interpretation of this correlation isthat women in the PMS pattern group are less selective
about what they drink and women in the noncyclic groupare more selective. This selectivity may depend on theaffective response that is anticipated by the individual, pre-sumably derived from past experiences with alcohol.Because this was not an a priori hypothesis, these resultsshould be interpreted with caution.
Also relevant to the present discussion is past researchexamining differential effects of alcohol across the menstru-al cycle of women with and without PMS/PMDD. Forexample, research has shown that women with PMDD (n012, M035 years) have a blunted saccadic eye velocity anddeceleration following alcohol infusion during the late lutealphase, as compared to the mid-follicular phase, whereascontrol subjects (n012, M030 years) did not demonstratethis effect (Nyberg et al. 2004). Interestingly, during the lateluteal phase, four of the PMDD patients (e.g., 30 %) wereunable to perform the eye saccade task because they becametoo sedated, whereas no women in the control group had thisproblem during this phase. These data suggest that womenin the PMDD group demonstrated an amplified response toalcohol that is limited to the luteal phase.
It should be noted that not all research has supported thehypothesis that the effects of alcohol change across the men-strual cycle. However, these studies have had significant meth-odological limitations, such as small sample sizes (Brick et al.1986; Holdstock and de Wit 2000; Mumenthaler et al. 2001),no women with PMS/PMDD (Brick et al. 1986; Holdstock andde Wit 2000; Mumenthaler et al. 2001) and mixed samples ofpill users and nonusers (Brick et al. 1986), for example.
Levels of alcohol use have also been found to vary acrossthe menstrual cycle (Mello et al. 1990; McLeod et al. 1994;Pastor and Evans 2003; Svikis et al. 2006). Therefore, futureresearch on the associations between menstrual cycle re-sponse and alcohol use should examine these associationsacross different phases of the menstrual cycle. However,there are multiple reasons why alcohol use may vary accord-ing to menstrual cycle phase, and these reasons may varyfrom individual to individual. For example, some womenmay use alcohol premenstrually to self-medicate negativeemotions, whereas others may not drink premenstruallybecause of physical symptoms such as headaches.Therefore, within-subjects designs will also be needed tosufficiently address these issues.
Finally, although PMS/PMDD has been shown to be stableacross three menstrual cycles (Bloch et al. 1997) and up to48 months (Wittchen et al. 2002), no research has tested thestability of the mid-cycle pattern. Because of the long timeinterval between classification into menstrual cycle responsepattern and the measurement of the alcohol use and responsevariables, the level of stability in the mid-cycle group couldsignificantly influence the results. For example, if the mid-cycle pattern is stable across time, the present results wouldprovide a good estimate of effect size. However, as stability
430 J. Kiesner
Author's personal copy

decreases, the magnitude of association would also decrease.Future research will be needed to understand the level ofstability of the mid-cycle group.
Two limitations of the present study should be noted.First, the measure of affective response to alcohol was basedon retrospective self-reports, which may be influenced bymemory distortion and bias. Affective responses and socialinteractions at varying doses of alcohol in a controlledlaboratory setting may provide a better measure of individ-ual response. Although laboratory settings may themselveshave significant effects on mood and may greatly constrainthese responses, past research using a semi-naturalistic barlaboratory setting has provided rich data regarding individ-ual response in realistic social interactions with peers (Bot etal. 2007; Larsen et al. 2010). Systematic observations alsoprovide the opportunity to study affective responses to al-cohol in both social and nonsocial (when they drink alone)contexts. A second approach would be to ask friends andromantic partners about the individual’s behavioral changes.This approach would provide several important advantagesincluding a focus on real-world natural environments andbehaviors by people who know the individual well. Finally,daily prospective self-reports would provide a further meth-odological improvement, eliminating memory distortion andbias. Such a measure could easily be added to prospectiveself-report questionnaires used to measure daily affectivesymptoms. Moreover, the combination of diverse measure-ment strategies (laboratory-based, other-report, and self-report) would provide the most complete approach, in whichthe weaknesses of each approach are counterbalanced by thestrengths of other approaches.
A second limitation, already mentioned above, is that thepresent study is based on university students, which mayhave very different alcohol-use patterns that likely dependmore heavily on social rituals and norms. Because theseaspects of drinking are likely to change over time, futureresearch should examine these relations with an older groupof participants.
An important strength of this study is that menstrualcycle response patterns were based on a unique data set ofn0213 women who completed daily questionnaires acrosstwo full menstrual cycles. This strategy resulted in theidentification of three distinct patterns of response to themenstrual cycle, one of which had not previously beenidentified (mid-cycle group). Thus, in the present study,we were able to make group comparisons that could nothave been previously made.
Finally, a remarkable aspect of these results is that thepresent data were collected 1 to 2 years after the initialstudy, when participants were categorized into one of threemenstrual cycle response groups. Research across manyareas of psychology has shown that concurrent associationsbetween variables are strongest and that the magnitude of
these associations are attenuated with longer time intervalsthat separate the measurement of the relevant variables.Thus, it is likely that the present effect sizes are attenuatedas compared to what would be found if all measures wereconcurrently measured.
In conclusion, the present study is the first to comparethese specific groups of affective response to the menstrualcycle on the measures of alcohol use, affective response toalcohol, and sleep changes in response to alcohol. Resultsshowed clear differences, in the expected direction, on threeout of five measures (i.e., hard alcohol use, negative affec-tive response to alcohol, and change in sleep followingalcohol use). These results provide an important and novelbasis for further understanding the potential risks of alcoholuse/abuse associated with different response patterns to themenstrual cycle.
Conflict of interest The author has no financial interest in thismanuscript.
References
American Psychiatric Association (1994) Diagnostic and statisticalmanual of mental disorders, 4th edn. American PsychiatricAssociation, Washington, DC
Andréen L, Nyberg S, Turkmen S, van Wingen G, Fernández G,Bäckström T (2009) Sex steroid induced negative mood may beexplained by the paradoxical effect mediated by GABAA modu-lators. Psychoneuroendocrinology 34:1121–1132
Bancroft J, Boyle H, Warner P, Fraser HM (1987) The use of an LHRHagonist, buserelin, in the long-term management premenstrualsyndrome. Clin Endocrinol 27:171–182
Bloch M, Schmidt PJ, Rubinow DR (1997) Premenstrual syndrome:evidence for symptom stability across cycles. Am J Psychiatry154:1741–1746
Bot SM, Engels RCME, Knibbe RA, Meeus WHJ (2007) Sociometricstatus and social drinking: observations of modeling and persua-sion in young adult peer groups. J Abnorm Child Psychol 35:929–941
Brick J, Nathan PE, Westrick E, Frankenstein W, Shapiro A (1986) Theeffect of menstrual cycle on blood alcohol levels and behavior. JStud Alcohol 47:472–477
Brown SA, Christiansen BA, Goldman MS (1987) The alcohol expec-tancy questionnaire: an instrument for the assessment of adoles-cent and adult alcohol expectancies. J Stud Alcohol 48:483–491
Caan B, Duncan D, Hiatt R, Lewis J, Chapman J, Armstrong MA(1993) Associations between alcoholic and caffeinated beveragesand premenstrual syndrome. J Reprod Med 38:630–636
Charette L, Tate DL, Wilson A (1990) Alcohol consumption andmenstrual distress in women at higher and lower risk for alcohol-ism. Alcohol Clin Exp Res 14:152–157
Chuong CJ, Burgos DM (1995) Medical history in women with pre-menstrual syndrome. J Psychosom Obstet Gynecol 16:21–27
Deuster PA, Adera T, South-Paul J (1999) Biological, social, andbehavioral factors associated with premenstrual syndrome. ArchFam Med 8:122–128
Response to the menstrual cycle and alcohol consumption 431
Author's personal copy

Feige B, Gann H, Brueck R, Hornyak M, Litsch S, Hohagen F, RiemannD (2006) Effects of alcohol on polysomnographically recordedsleep in healthy subjects. Alcohol Clin Exp Res 30:1527–1537
Gold EB, Bair Y, Block G, Greendale GA, Harlow SD, Johnson S,Kravitz HM, Rasor MO, Siddiqui A, Sternfeld B, Utts J, Zhang G(2007) Diet and lifestyle factors associated with premenstrualsymptoms in a racially diverse community sample: Study ofWomen’s Health Across the Nation (SWAN). J Womens Health16:641–656
Haddad L, Milke P, Zapata L, de la Fuente JR, Vargas-Vorackova F,Lorenzana-Jimenez M, Corte G, Tamayo J, Kaplan M, MarquezM, Kershenobich D (1998) Effects of the menstrual cycle inethanol pharmacokinetics. J Appl Toxicol 18:15–18
Halliday A, Bush B, Cleary P, Aronson M, Delbanco T (1986) Alcoholabuse in women seeking gynecologic care. Obstet Gynecol68:322–326
Holdstock L, de Wit H (2000) Effects of ethanol at four phases of themenstrual cycle. Psychopharmacology 150:374–382
Holdstock L, King AC, de Wit H (2000) Subjective and objectiveresponses to ethanol in moderate/heavy and light social drinkers.Alcohol Clin Exp Res 24:789–794
Hourani LL, Yuan H, Bray RM (2004) Psychosocial and lifestylecorrelates of premenstrual symptoms among military women. JWomens Health 13:812–821
Kiesner J (2009) Physical characteristics of the menstrual cycle andpremenstrual depressive symptoms. Psychol Sci 20:763–770
Kiesner J (2011) One woman’s low is another woman’s high: paradoxicaleffects of the menstrual cycle. Psychoneuroendocrinology 36:68–76
Kiesner J, Pastore M (2010) Day-to-day co-variations of psychologicaland physical symptoms of the menstrual cycle: insights to individualdifferences in steroid reactivity. Psychoneuroendocrinology 35:350–363
King AC, Houle T, de Wit H, Holdstock L, Schuster A (2002) Biphasicalcohol response differs in heavy versus light drinkers. AlcoholClin Exp Res 26:827–835
Kritz-Silverstein D, Wingard DL, Garland FC (1999) The associationof behavior and lifestyle factors with menstrual symptoms. JWomens Health & Gender-Based Medicine 8:1185–1193
Larsen H, van der Zwaluw CS, Overbeek G, Granic I, Franke B,Engels RCME (2010) A variable-number-of-tandem-repeats poly-morphism in the dopamine D4 receptor gene affects social adap-tation of alcohol use: investigation of a gene–environmentinteraction. Psychol Sci 21:1064–1068
McLeod DR, Foster GV, Hoehn-Saric R, Svikis DS, Hipsley PA (1994)Family history of alcoholism in women with generalized anxietydisorder who have premenstrual syndrome: patient reports ofpremenstrual alcohol consumption and symptoms of anxiety.Alcohol Clin Exp Res 18:664–670
Mello NK, Mendelson JH, Lex BW (1990) Alcohol use and premen-strual symptoms in social drinkers. Psychopharmacology101:448–455
Mumenthaler MS, O’Hara R, Taylor JL, Friedman L, Yesavage JA(2001) Influence of the menstrual cycle on flight simulator per-formance after alcohol ingestion. J Stud Alcohol 62:422–433
Nyberg S, Wahlström G, Bäckström T, Sundström-Poromaa I (2004)Altered sensitivity to alcohol in the late luteal phase among patientswith premenstrual dysphoric disorder. Psychoneuroendocrinology29:767–777
Nyberg S, Andersson A, Zingmark E, Wahlström G, Bäckström T,Sundström-Poromaa I (2005) The effects of a low dose of alcoholon allopregnanolone serum concentrations across the menstrualcycle in women with severe premenstrual syndrome and controls.Psychoneuroendocrinology 30:892–901
Orcutt JD, Harvey LK (1991) The temporal patterning of tensionreduction: stress and alcohol use on weekdays and weekends. JStud Alcohol 52:415–424
Pastor AD, Evans SM (2003) Alcohol outcome expectancies and riskfor alcohol use problems in women with and without a familyhistory of alcoholism. Drug Alcohol Depend 70:201–214
Perry BL, Miles D, Burruss K, Svikis DS (2004) Premenstrual symp-tomatology and alcohol consumption in college women. J StudAlcohol 65:464–468
Sagawa Y, Kondo H, Matsubuchi N, Takemura T, Kanayama H,Kaneko Y, Kanbayashi T, Hishikawa Y, Shimizu T (2011)Alcohol has a dose-related effect on parasympathetic nerve activ-ity during sleep. Alcohol Clin Exp Res 35:2093–2100
Schmidt PJ, Nieman LK, Danaceau MA, Adams LF, Rubinow DR(1998) Differential behavioral effects of gonadal steroids in wom-en with and in those without premenstrual syndrome. N Eng JMed 338:209–216
Singleton RA, Wolfson AR (2009) Alcohol consumption, sleep, andacademic performance among college students. J Stud AlcoholDrugs 70:355–363
Strine TW, Chapman DP, Ahluwalia IB (2005) Menstrual-related prob-lems and psychological distress among women in the UnitedStates. J Womens Health 14:316–323
Svikis DS, Miles DR, Haug NA, Perry B, Hoehn-Saric R, McLeod D(2006) Premenstrual symptomatology, alcohol consumption, andfamily history of alcoholism in women with premenstrual syn-drome. J Stud Alcohol 67:833–839
Tate DL, Charette L (1991) Personality, alcohol consumption, andmenstrual distress in young women. Alcohol Clin Exp Res15:647–652
Tobin MB, Schmidt PJ, Rubinow DR (1994) Reported alcohol use inwomen with premenstrual syndrome. Am J Psychiatry 151:1503–1504
Torres JM, Ortega E (2003) Alcohol intoxication increases allopregnano-lone levels in female adolescent humans. Neuropsychopharmacology28:1207–1209
Wittchen HU, Becker E, Lieb R, Krause P (2002) Prevalence, inci-dence and stability of premenstrual dysphoric disorder in thecommunity. Psychol Med 32:119–132
432 J. Kiesner
Author's personal copy
Related Documents