AFFECTIVE DISORDERS DR. Rabie A. Hawari Consultant Psychiatrist Clinical Assistant Professor

AFFECTIVE DISORDERS DR. Rabie A. Hawari Consultant Psychiatrist Clinical Assistant Professor.
Jan 01, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
AFFECTIVE DISORDERS
DR. Rabie A. HawariConsultant Psychiatrist
Clinical Assistant Professor
AFFECTIVE DISORDERS
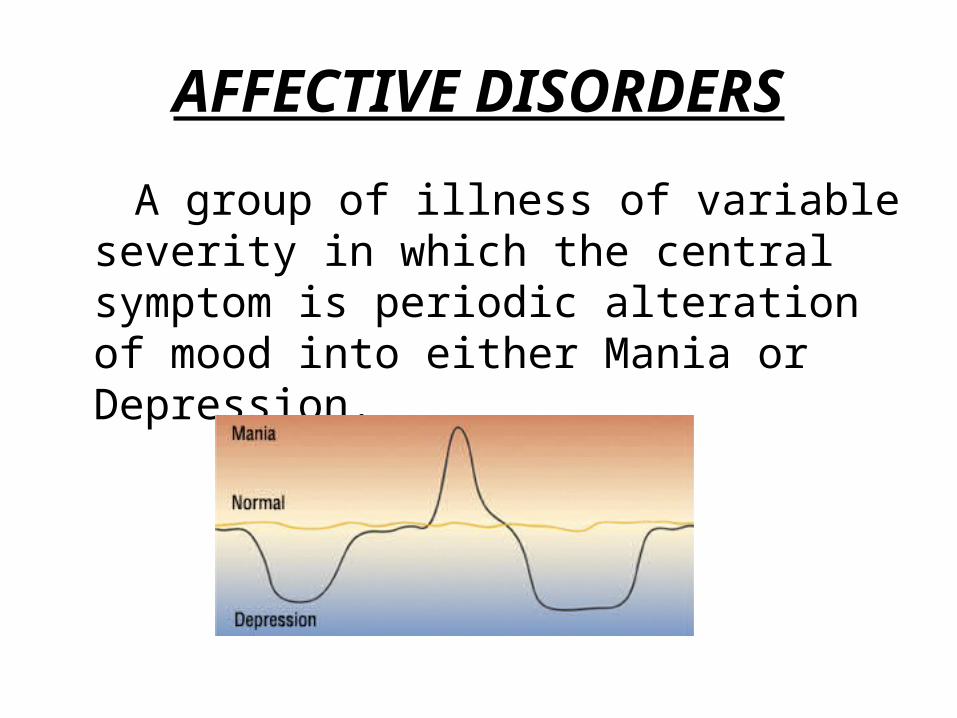
A group of illness of variable severity in which the central symptom is periodic alteration of mood into either Mania or Depression.
Epidemiology
• female: male = 2:1 (dep.)
• = 1:1 ( mania)
• age = dep. – 20-50. mean 40yr.
= mania – earlier mean 30yr
Etiology various theories • Genetics :- evidence is stronger for BAD, - 50% of pts.---> one parent have M.D, - BAD. pt. ----> 27% any child have M.D, - Both parents ----> 50-75% any child, - MZ twins ----> 75% concordance.• Biochemical :- - Norepinephrine & Serotonin reduced at receptor sites in the brain ---- > dep. - NE & 5HT increased at receptor sites ---> mania.. Psychological Factors :-
- Life Events. – P.M.P. – Psychoanalytic. - Cognitive. – learned helplessness.

DEPRESSION
Signs & Symptoms
• A. Mental:- • Mood:- Depressed, Diurnal Variation, Pessimism, Suicidal ideas, Loss of Interest, Anhedonia.• Thinking:- Poverty of thoughts, poor concentration, Poor cognition, poor judgment & insight, Delusions (paranoid, guilt, nihilistic, hypochondriases)• Perception: - Auditory Hallucination,(2nd. Person).
Signs & Symptoms(cont)
• B. Physical:- . Insomnia or Hypersomnia,
Loss of Appetite, Loss of Wt. or Gain, Psychomotor Retardation or Agitation, Loss of Libido, Loss Energy, Tiredness, stupor. Somatic c/o:-
headache, constipation,drymouth,abnormal menses, etc.
Types of depression
1. Major Depression: - unipolar – s/s. 2/52, 40ys.2. Dysthymia: - Neurotic depression. Chronic. 20 s.3. Seasonal Affective disorder (SAD): - - Major dep., in winter & fall (short daylight) - s/s: hypersomnia, hyperphagia & psychomotor
slowing - due to abn.Melatonin metabolism, - Rx. Exposure to light 3-6 hr. /day.4. Post Partum Depression: - after birth. 30 days. s/s .insomnia, fatigue, suicide, homicide & delusions.
Types of depression(cont.)
5. Myxedema Madness: -HypothyroidismS/s.fatigability, Dep. suicidal impulse, delusions, hallucination & Paranoia.
6. Organic Mood Disorder-- Depression type: - secondary to organic cause e.g. Cushing’s Synd., Propranlol med.,
• Infections (flu, Aids,).
7. Pseudo Dementia: - Dementia Synd. Of depression in the elderly. Dep. Is primary than the cognitive dysfunction
8. Adjustment Diso. with Depressed Mood: - response to a clear identifiable stress.
Types of depression(cont.)
9. Grief: - sadness secondary to major loss.—not Dep., remits with time, no suicide or helplessness.10. Depression in children: - not uncommon, same s/s. Masked dep. = running away from home, school Phobia, substance abuse & suicide.11. Double Dep.: - Major dep. On top of dysthymia.12. Atypical Dep.: - s/s. do not meet criteria of depression - intermittent dysthymic episodes, - Wt. gain & hypersomnia.

Treatment of Depression
• Pharmacological:- a. TCA: - Imipramine, Amitriptyline,Clomipramine, (3/52 to start to act). b. MAOI: - Phenelzine, Parnate (Tyramine dietary restrictions). c. SSRIs: - Fluvoxamine, fluoxetine, “Rx. For 6/12. if recurrent lithium as an adjunct
appears to be affective “
* Physical :- ElecrtoConvulsiveTherapy (ECT).
Treatment of Depression(cont)
• Psychological:- a). Cognitive: corrections of chronic distortions in thinking which led to depression. b). Behaviour: aimed at specific behaviour. c). Interpersonal: emphasis on ongoing current issues. d). Psychoanalytic: to understand the unconscious conflicts & motivations that might sustain depression. e). Group Rx. f). Family Rx. g). Supportive Rx.

MANIA
Signs & Symptoms A. Mental:-
- Mood:- Elevated (Elated) mood over days or weeks. - may be interrupted by episode of depression, - Irritability with Angry outbursts. - Impulsiveness. -Thinking:- - Low concentration, Distractibility, - Over talkative, Laud, Rapid, - Pressure of thoughts, - Flight of Ideas, - Memory & Orientation = intact, - Judgment & Insight = impaired, - Delusions = Grandiose, Paranoid, - Inflated self-esteem.- Perception: - Hallucination may be present.
Signs & Symptoms(cont)
B. Physical:
- Insomnia,
- Increase activities & energy,
- Increase Libido, Disinhibtion,
- Psychomotor agitation,
- Wt. loss due exhaustion.

TYPES OF MANIA •Organic Mood Disorder: - Manic Type .• Secondary to organic disorder e.g. – Tertiary • Syphilis, Influenza, Corticosteroids, TLE ,• Amphetamine, Hyperthyroidism, Head Trauma,
Vit. Def. (B12, Folate, Thiamine), MS
Cyclothymia: - 2yrs. Symptoms, recurrent mood swings
• •Rapid Cycling Bipolar Disorder: - Mania/Depression Episodes
with intervals 48-72 hrs.•Bipolar Disorder not otherwise specified (NOS) -:
1 Depression episode & 1 manic episode.
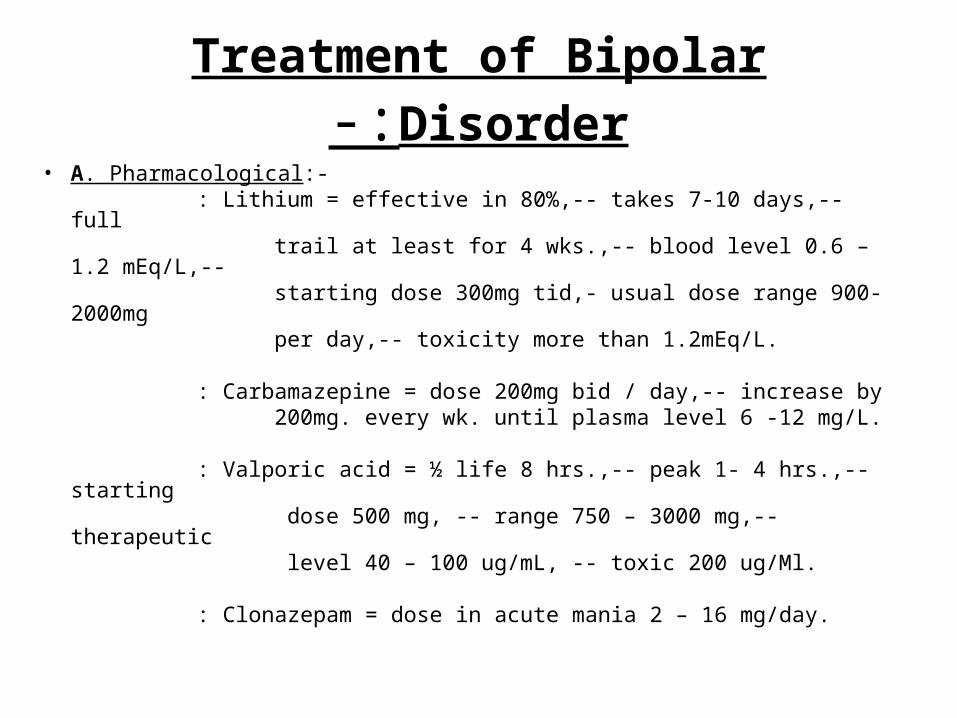
Treatment of Bipolar Disorder-:• A. Pharmacological:- : Lithium = effective in 80%,-- takes 7-10 days,-- full trail at least for 4 wks.,-- blood level 0.6 – 1.2 mEq/L,-- starting dose 300mg tid,- usual dose range 900-2000mg per day,-- toxicity more than 1.2mEq/L. : Carbamazepine = dose 200mg bid / day,-- increase by 200mg. every wk. until plasma level 6 -12 mg/L.
: Valporic acid = ½ life 8 hrs.,-- peak 1- 4 hrs.,-- starting dose 500 mg, -- range 750 – 3000 mg,-- therapeutic level 40 – 100 ug/mL, -- toxic 200 ug/Ml.
: Clonazepam = dose in acute mania 2 – 16 mg/day.
Treatment of Bipolar Disorders(con)
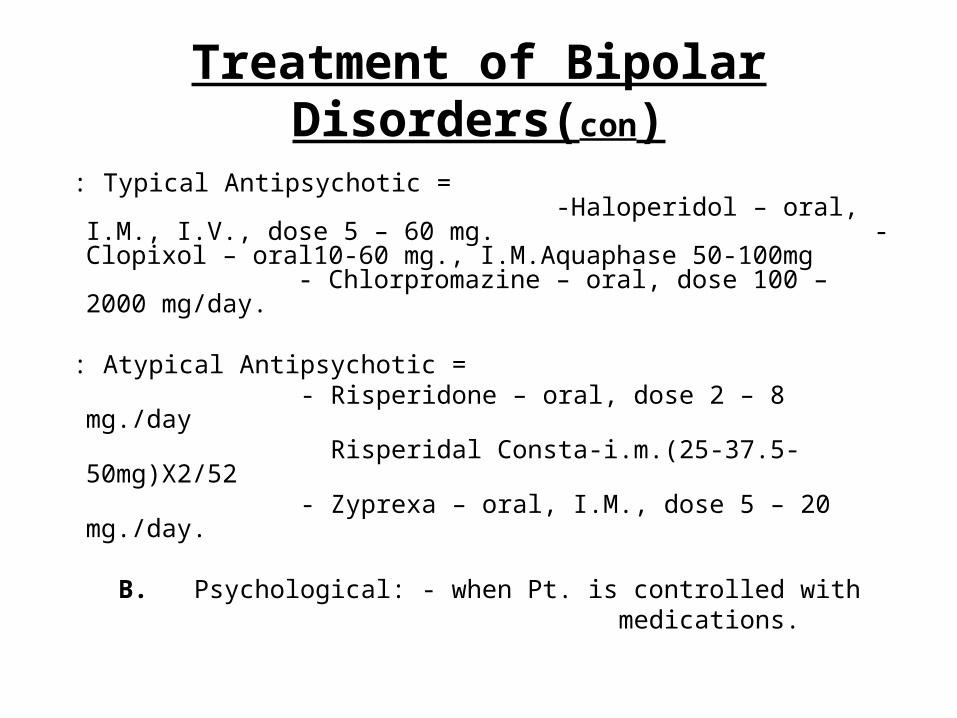
: Typical Antipsychotic = -Haloperidol – oral, I.M., I.V., dose 5 – 60 mg. - Clopixol – oral10-60 mg., I.M.Aquaphase 50-100mg - Chlorpromazine – oral, dose 100 – 2000 mg/day.
: Atypical Antipsychotic = - Risperidone – oral, dose 2 – 8 mg./day Risperidal Consta-i.m.(25-37.5-50mg)X2/52 - Zyprexa – oral, I.M., dose 5 – 20 mg./day.
B. Psychological: - when Pt. is controlled with medications.

COURSE & PROGNOSIS
• Depression: - - 15% commit suicide. - Untreated – episode last for 10 months. - 75% have secondary episode after 6/12 - Average No. of episodes in lifetime = 5.
PROGNOSIS: -– 50% recover. – 30% partially recover.– 20% have chronic course.– 20-30% of Dysthymic or cyclothymic
develop major Dep., or mania.
COURSE & PROGNOSIS(cont)
• Mania; - - 45 % recur. - Untreated – episode last 3-6 months.
High rate of recurrence average 10.
-80-90 % experience a full Dep., episode.• PROGNOSIS: -
– fair.– 15 % recover. – 50 – 60 % partially recover– 1/3 have some evidence of chronic symptoms
& social deterioration.
Related Documents











