-
8/3/2019 Affective Disorders DepressionII Oct 2011
1/33
Affective Disorders
and their treatment.
Dr Trevor Bushell
X2856
-
8/3/2019 Affective Disorders DepressionII Oct 2011
2/33
Objectives
know the major forms of affective disorders
be able to discuss the biogenic amine hypothesis ofaffective disorders
know the mechanism of action of anti-depressant drugs
be familiar with the side effects and drug interaction of
antidepressants
-
8/3/2019 Affective Disorders DepressionII Oct 2011
3/33
Classification of affective disorders
Affective disorders are all characterised by a disturbance of mood.
Severely depressed subjects, symptoms include:
profound sadness, guilt and unworthiness, lack of motivation,suicidal thoughts
Mania, symptoms include:
hyperactivity and elation
Affective disorders are not solely extremes in mood, they are also
disproportionate and unresponsive to outside influence.
-
8/3/2019 Affective Disorders DepressionII Oct 2011
4/33
Biogenic amine hypothesis of
depression Low levels of NA and/or 5-HT depression
Raised levels of NA and/or 5-HT mania
Hence, if return the levels of NA and/or 5-HT
to normal, reverse depression or mania.
Actual answer is not that simple!!
-
8/3/2019 Affective Disorders DepressionII Oct 2011
5/33
Evidence supporting the hypothesis
Reserpine depletes stores of noradrenaline,
dopamine and 5-HT, this leads to depression-
like states in animal models. This can be reversed
by 5-HT precursor
Metabolite levels: Decreased metabolite levels
for NA and 5-HT in some clinically depressedpatients.
-
8/3/2019 Affective Disorders DepressionII Oct 2011
6/33
Problems with the hypothesis
Drug action is relatively fast (hours) but relief of symptoms
takes longer (days)
Antidepressants have differing mode of action (i.e. 5-HT v NA)
but work similarly on symptoms.
Receptor adaptations following long term treatment do not
fit with the simple hypothesis:
Down regulation ofb-adrenoceptors usually transmission
Down regulation of presynaptic a2-adrenoceptors - transmission
Down regulation of 5-HT2 receptorsusually transmission
-
8/3/2019 Affective Disorders DepressionII Oct 2011
7/33
Antidepressants:
mechanism of action and side effects
Electroconvulsve Shock Treatment (ECT)
Monoamine Oxidase Inhibitors (MAOIs)
Tricyclic antidepressants (TCAs)
Atypical antidepressants and SSRIs
-
8/3/2019 Affective Disorders DepressionII Oct 2011
8/33
Electroconvulsve Shock Treatment (ECT)
Therapeutic potential discovered by Ugo
Cerletti in Rome in 1937.
Even most severe bouts of depression are
usually responsive to ECT.
Still used today in cases of very severe
depression with a high risk of suicide,
where there has been no response to drugtreatments.
2272 people were treated with ECT in the
last survey conducted (JanMar 2002). Film based on real-life experiences of
Ken Casey in an Oregon mental hospital
-
8/3/2019 Affective Disorders DepressionII Oct 2011
9/33
The use of ECT is controversial, do
you think it is a viable treatment for
depression?
-
8/3/2019 Affective Disorders DepressionII Oct 2011
10/33
Overview of synaptic transmission.
-
8/3/2019 Affective Disorders DepressionII Oct 2011
11/33
Monoamine Oxidase Inhibitors (MAOIs)
First drugs found to have some efficacy in treating depression.
First found by accident when an antituberculosis drug was found
to improve the mood of the treated patients.
Compound was later discovered to be an inhibitor of
monoamine oxidase (MAO).
MAOs are one of two enzymes involved in the degradation ofcatecholamines (i.e. NA) along with catechol-O-methyl transferase
(COMT).
-
8/3/2019 Affective Disorders DepressionII Oct 2011
12/33
MAOs exist in two forms:
MAO-A preferred substrate 5-HT but also NA
MAO-B preferred substrate benzylamine & phenylethylamine
Early MAOIs were irreversible, thus enzyme activity will return
only following the synthesis of new enzyme.
Theory: Inhibition of the degradation pathway leads to increased
levels of NA and 5-HT.
HENCE, FOLLOWING THE AMINE HYPOTHESIS
levels of 5-HT & NA depression
NB in non-depressed patients, MAOIs anxiety & agitation
-
8/3/2019 Affective Disorders DepressionII Oct 2011
13/33
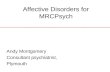
MAOIs and the noradrenergic neurone
(applies to 5-HT as well)
MAOIs
Block
DegradationOf
NA & 5-HT
-
8/3/2019 Affective Disorders DepressionII Oct 2011
14/33
Clinically used MAOIs
Largely superceded by TCAs, as greater efficacy and less side
effects.
Advent of MAOIs selective for MAO-A have renewed the interest
in them.
Irreversible MAOIs include: phenelzine
tranylcypromine
iproniazid
pargylline
Reversible inhibitors for MAO-A: clorgilline
moclobemide
Reversible inhibitor for MAO-B, selegilline, is used in Parkinsons.
-
8/3/2019 Affective Disorders DepressionII Oct 2011
15/33
Side effects associated with MAOIs
Hypotension (pargylline once used as an antihypertensive)
Weight gain (can lead to discontinued use of drug)
Some atropine-like side effects (dry mouth, blurred vision etc)
Less than with TCAs.
Extreme cases can lead to hepatotoxicity (phenelzine, iproniazid).
Overdose can leads to convulsions.
-
8/3/2019 Affective Disorders DepressionII Oct 2011
16/33
Drug interactions(one of main reasons for their decline in use).
The cheese reaction.
Food containing high levels of tyramine acute hypertension
Tyramine enters nerve terminals and displaces
NA from vesicles
Large release of NA
vasoconstriction
Ususally degraded by
MAO in gut & liver
Can lead to severe headaches
& even intracranial haemorrhage
-
8/3/2019 Affective Disorders DepressionII Oct 2011
17/33
Drug interactions (contd)
Interaction with indirectly acting sympathomimetics (amphetamines)also leads to severe hypertension.
Co-administration of MAOIs and TCAs has also been reported to
lead to severe hypertension.
-
8/3/2019 Affective Disorders DepressionII Oct 2011
18/33
How does the action of MAOs fit
with the monoamine hypothesis?
-
8/3/2019 Affective Disorders DepressionII Oct 2011
19/33
Tricyclic antidepressants (TCAs)
Closely related to phenothiazine compounds used to treat psychoticbehaviour.
Initially produced as antipsychotic compunds. No use in
schizophrenia but elevated mood of depressed patients.
First drug introduced was IMIPRAMINE in the 1950s.
Other drugs such as CLOMIPRAMINE were developed from
this initial compound.
Development of other antipsychotic drugs lead to discovery of
AMITRIPTYLINE (tertiary amine) and its demethylated metabolites,
DESIPRAMINE & NORTRYPTILINE (secondary amines).
-
8/3/2019 Affective Disorders DepressionII Oct 2011
20/33
Structure of TCAs
-
8/3/2019 Affective Disorders DepressionII Oct 2011
21/33
Mechanism of action of TCAs
Primary effect is to block uptake of amines by competition at the
reuptake transporter protein (little effect on DA reuptake).
reuptake of amines
Some TCAs also increase synaptic levels of amines by desensitisingpresynaptic a2 receptors i.e. inhibit autoinhibition of release
Levels of
NA & 5-HTdepression
Note: secondary TCAs i.e. desipramine, are more selective forNA uptake than are tertiary amines i.e amitriptyline, which
inhibit both NA & 5-HT uptake.
-
8/3/2019 Affective Disorders DepressionII Oct 2011
22/33
How will TCAs affect NA or
5-HT at the synaptic level?
-
8/3/2019 Affective Disorders DepressionII Oct 2011
23/33
TCAs and the noradrenergic neurone
TCAs
Block
Reuptake
of
amines
TCAs
inhibitpresynaptic
2 receptorsa
-
8/3/2019 Affective Disorders DepressionII Oct 2011
24/33
Side effects associated with TCAs
In non-depressed patients, some TCAs cause sedation and confusion.Similar effects seen in depressed patients for first few days but wear
off as antidepressant effects develop. Can be useful in agitated patients!!
Atropine-like side effects: blurred vision, dry mouth,
constipation, urinary retention
Ventricular dysrhythmias via K channels block (particularly in
overdose; caution in patients with cardiovascular problems).
Overdose can lead to in seizure threshold.
Ventricular dysrhythmias and in seizure threshold, main reasons
for death when TCAs used for suicide attempts.
-
8/3/2019 Affective Disorders DepressionII Oct 2011
25/33
Drug interactions
TCAs bind strongly to plasma proteins, hence effects enhancedwhen given with competing drugs i.e. aspirin
Metabolised by liver enzymes, these are inhibited by potential
co-administered compounds such as steroids and some antipsychotics
Strongly potentiated by alcohol
l i 5 i k i hibi
-
8/3/2019 Affective Disorders DepressionII Oct 2011
26/33
Selective 5-HT (serotonin) reuptake inhibitors
(SSRIs)
More recently developed drugs used to treat depression.
Not only used in depression, but also useful in treating anxiety,
panic attacks and obsessive-compulsive disorders.
As name suggests, mechanism of action is the selective blockadeof 5-HT reuptake.
reuptake of 5-HT
Drugs include fluoxetine (prozac)
fluvoxamine
paroxetine
setraline
citalopram
synaptic levels
of 5-HTdepression
-
8/3/2019 Affective Disorders DepressionII Oct 2011
27/33
Blockade of 5-HT reuptake.
-
8/3/2019 Affective Disorders DepressionII Oct 2011
28/33
Side effects
In general, less side effects than TCAs and MAOIs.
Compared to TCAs, less anticholinergic side effects and
less dangerous in overdose.
No cheese reaction as observed with MAOIs
Despite this, they do produce some nausea, anorexia, insomnia,
sexual dysfunction.
IN SPITE OF REDUCED SIDE EFFECTS, STUDIES
REVEALED NO PREFERENCE FOR SSRIs OVER TCAs
IN STUDIES OF PATIENT ACCEPTABILITY.
-
8/3/2019 Affective Disorders DepressionII Oct 2011
29/33
Atypical antidepressants
Several atypical antidepressants are used clinically.
Appears to be no common mechanism of action.
No higher efficacy at treating depression but generally
have fewer side effects.
Show efficacy in patients not responding to other treatments.
-
8/3/2019 Affective Disorders DepressionII Oct 2011
30/33
Atypical antidepressants
Drug Mech of action Side effectsMaprotilline selective NA reuptake atropine-like effects
blocker sedation
Mianserin H1, 5-HT2 & a2 agranulocytosis
Trazodone Weak 5-HT uptake hypotension,
blocker, H1 & 5-HT2 antag sedation,
Venlafaxine Non-selective 5-HT as with SSRIs
& NA uptake blocker
receptor antag.
-
8/3/2019 Affective Disorders DepressionII Oct 2011
31/33
Use of lithium as a mood stabiliser
Lithium used to calm manic patients and prophylacticallyas a mood stabiliser.
Results observed quicker and are considered safer
(no overdose potential).
Mechansim of action is not well understood. Suggested
mechanisms are:
inhibition of inositol triphosphate formationinterference of cAMP formationaccumulation of Li+ in cell, leading to sustained depolarisation
Side effects: long half-life leads to commn side effects such asnausea, thirst, tremor, mental confusion
-
8/3/2019 Affective Disorders DepressionII Oct 2011
32/33
Clinical application of drugs to treat affective disorders.
Anti-depressants:1st line - SSRIs primarily fluoxetine and citalopram
2nd linevenlafaxine but several options may need to be tried
in order to find a suitable treatment if the depression
is somewhat drug resistant.
Bipolar disorder: BZD ( i.e. lorazepam) may be useful in
intial stages but cannot be used over extended periods.
Lithium and sodium valproate are used as a mood stabiliser
over an extended period. These may be given with or withoutan SSRI to treat depressive episodes.
-
8/3/2019 Affective Disorders DepressionII Oct 2011
33/33
Research is still ongoing!!!