Genitourin Med 1996;72:237-246 Adverse effects and drug interactions of medications commonly used in the treatment of adult HIV positive patients Rachel Heylen, Robert Miller Introduction Patients with advanced HIV disease com- monly take a large number of medications that are active against HIV, that treat or prevent opportunistic infections and that prevent the symptoms of HIV itself or those produced by the other medications. Many of these medica- tions have overlapping toxicities, and share the same methods of elimination from the body, leading to varied drug interactions. This article seeks to highlight those drugs that are used in HIV infected patients which are most commonly associated with drug interactions, the reasons for these interactions and to help physicians and pharmacists make decisions about which of the interactions are clinically significant. By examining available data on the toxicity, formulation and pharma- cokinetics of these different medications charts and explanatory notes have been compiled. Pharmacodynamic Interactions (tables 1-4) Additive toxicity One or a number of the main side effects of the two drugs overlap and can lead to increased toxicity. The classifica- tion of this toxicity is denoted by a letter: M-Myelotoxicity P-Pancreatitis N-Peripheral neuropathy K-Nephrotoxicity L-Hepatotoxicity The clinical significance of this interaction is as below. Increased Serum Levels This is usually due to inhibition of metabolism by the liver or excre- tion via the kidneys, and can lead to increased toxicity. The drug that has been affected is indicated by the direction of the arrow (table 1). The clinical significance of this interaction is described below. Decreased Serum Levels This is often caused by an increase in metabolism by the liver as a result of the use of drugs which induce liver enzymes such as rifampicin, or by a decrease in the absorption of the drug from the gas- trointestinal tract such as the bioavailability of ketoconazole is reduced by the administration of drugs which increase gastric pH. The clinical significance of this interaction is as below. Miscellaneous Interactions that have been reported but which do not fall under the above headings. Clinical Significance The interactions have been allocated to one of four categories as follows: ?-unknown clinical significance This category is used when there have been reports in the lit- erature of an interaction but these are only case reports or in vitro work or the conclusions of these reports are conflicting. It also includes drugs where an interaction may be expected (from those reported with other members of the same class of drugs etc) but no reports have been found, this may be important for drugs that have been recently released on to the market. !-take note This category is used when there is evidence of an interaction but it is of theo- retical interest rather than clinical importance or it involves the fine tuning of dosing eg reducing the dose of a relatively non toxic medication in renal failure. !!-use with caution This category is used when there is evidence of an interaction, and it is of clinical importance. Adjustments may have to be made in doses of toxic medications etc. skull and cross-contraindicated The combi- nation of drugs should be avoided where possi- ble. This includes well documented interactions that are clinically significant, com- binations that are precluded by the manufac- turer or combinations which share potentially very serious side effects, for example nephro- toxicity with co-administration of IV ampho- tericin and IV pentamidine. Antiretrovirals: Zidovudine (AZT), didanosine (ddI), zalcitabine (ddC), and stavudine (D4T) (Table 1) These four medications are nucleoside ana- logues which prevent viral replication by either causing chain termination and/or block- ing the reactive site of the enzyme reverse transcriptase thus inhibiting retroviral cDNA synthesis. They share some similarities in that all are metabolised in infected cells to the active triphosphate form. They are metabolised to differing extents by the liver, and both changed and unchanged drug is excreted in the urine. Pharmacokinetic interactions Approximately 70% of zidovudine is metab- olised in the liver by glucuronidation to 3- azido-3-deoxy-5-D-glucopyranosyl thymidine. Both changed and unchanged drug are excreted in the urine by renal tubular excretion.' After Pharmacy Department, University College London Hospitals (NHS) Trust, Middlesex Hospital Site, London, UK R Heylen Department of Sexually Transmitted Diseases, Division of Pathology and Infectious Diseases, University College London Medical School and Camden and Islington Community Health Services (NHS) Trust, London, UK R Miller Address correspondence to: Dr R F Miller, 4th Floor, Mortimer Market Centre, Mortimer Market, (off Capper Street), London WC1E 6AU, UK. Accepted for publication 26 June 1996 237 on January 15, 2020 by guest. Protected by copyright. http://sti.bmj.com/ Genitourin Med: first published as 10.1136/sti.72.4.237 on 1 August 1996. Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Genitourin Med 1996;72:237-246
Adverse effects and drug interactions ofmedications commonly used in the treatment ofadult HIV positive patients
Rachel Heylen, Robert Miller
IntroductionPatients with advanced HIV disease com-monly take a large number of medications thatare active against HIV, that treat or preventopportunistic infections and that prevent thesymptoms of HIV itself or those produced bythe other medications. Many of these medica-tions have overlapping toxicities, and share thesame methods of elimination from the body,leading to varied drug interactions.
This article seeks to highlight those drugsthat are used in HIV infected patients whichare most commonly associated with druginteractions, the reasons for these interactionsand to help physicians and pharmacists makedecisions about which of the interactions areclinically significant. By examining availabledata on the toxicity, formulation and pharma-cokinetics of these different medications chartsand explanatory notes have been compiled.
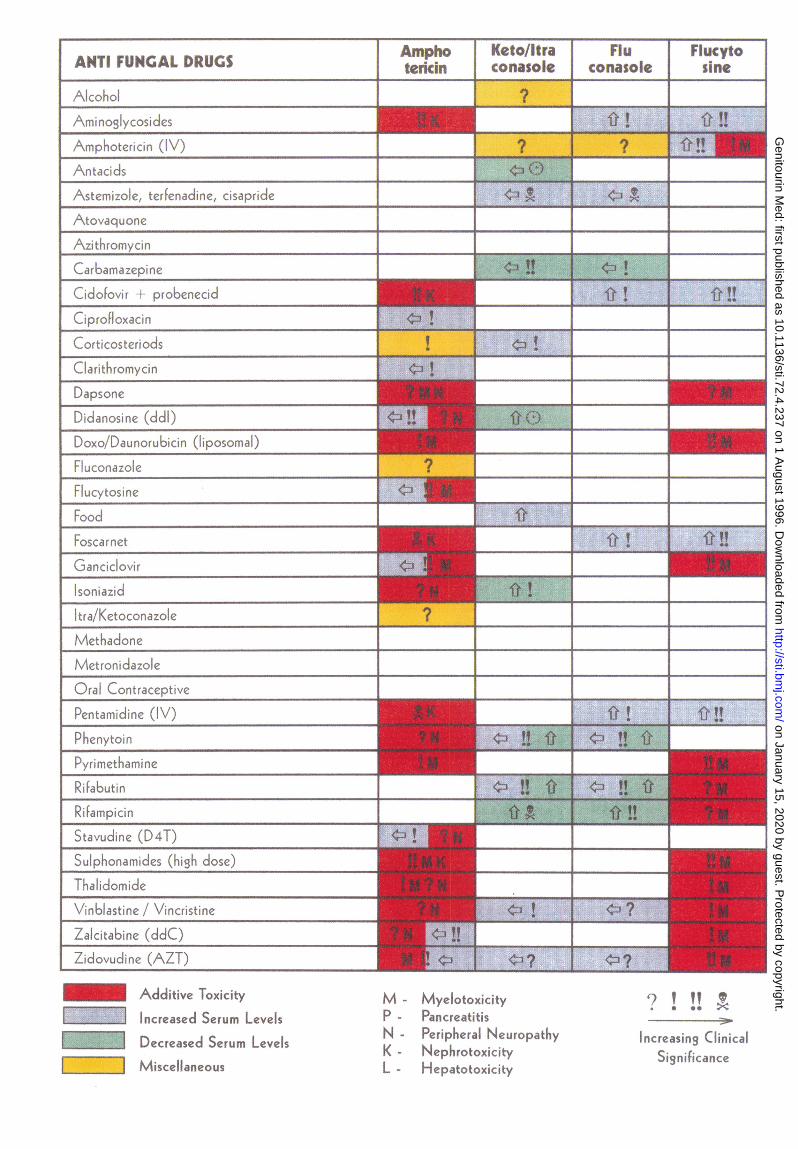
Pharmacodynamic Interactions (tables1-4)Additive toxicity One or a number of themain side effects of the two drugs overlap andcan lead to increased toxicity. The classifica-tion of this toxicity is denoted by a letter:
M-MyelotoxicityP-PancreatitisN-Peripheral neuropathyK-NephrotoxicityL-HepatotoxicityThe clinical significance of this interaction
is as below.Increased Serum Levels This is usually due toinhibition of metabolism by the liver or excre-tion via the kidneys, and can lead to increasedtoxicity. The drug that has been affected isindicated by the direction of the arrow (table1). The clinical significance of this interaction isdescribed below.
Decreased Serum Levels This is often causedby an increase in metabolism by the liver as aresult of the use of drugs which induce liverenzymes such as rifampicin, or by a decreasein the absorption of the drug from the gas-trointestinal tract such as the bioavailability ofketoconazole is reduced by the administrationof drugs which increase gastric pH. The clinicalsignificance of this interaction is as below.
MiscellaneousInteractions that have been reported but whichdo not fall under the above headings.
Clinical SignificanceThe interactions have been allocated to one offour categories as follows:?-unknown clinical significance This categoryis used when there have been reports in the lit-erature of an interaction but these are onlycase reports or in vitro work or the conclusionsof these reports are conflicting. It also includesdrugs where an interaction may be expected(from those reported with other members ofthe same class of drugs etc) but no reportshave been found, this may be important fordrugs that have been recently released on tothe market.!-take note This category is used when thereis evidence of an interaction but it is of theo-retical interest rather than clinical importanceor it involves the fine tuning of dosing egreducing the dose of a relatively non toxicmedication in renal failure.!!-use with caution This category is usedwhen there is evidence of an interaction, and itis of clinical importance. Adjustments mayhave to be made in doses of toxic medicationsetc.skull and cross-contraindicated The combi-nation of drugs should be avoided where possi-ble. This includes well documentedinteractions that are clinically significant, com-binations that are precluded by the manufac-turer or combinations which share potentiallyvery serious side effects, for example nephro-toxicity with co-administration of IV ampho-tericin and IV pentamidine.
Antiretrovirals: Zidovudine (AZT),didanosine (ddI), zalcitabine (ddC), andstavudine (D4T) (Table 1)These four medications are nucleoside ana-logues which prevent viral replication byeither causing chain termination and/or block-ing the reactive site of the enzyme reversetranscriptase thus inhibiting retroviral cDNAsynthesis. They share some similarities in thatall are metabolised in infected cells to theactive triphosphate form. They aremetabolised to differing extents by the liver,and both changed and unchanged drug isexcreted in the urine.
Pharmacokinetic interactionsApproximately 70% of zidovudine is metab-olised in the liver by glucuronidation to 3-azido-3-deoxy-5-D-glucopyranosyl thymidine.Both changed and unchanged drug are excretedin the urine by renal tubular excretion.' After
PharmacyDepartment,University CollegeLondon Hospitals(NHS) Trust,Middlesex HospitalSite, London, UKR HeylenDepartment ofSexually TransmittedDiseases, Division ofPathology andInfectious Diseases,University CollegeLondon MedicalSchool and Camdenand IslingtonCommunity HealthServices (NHS) Trust,London, UKR MillerAddress correspondence to:Dr R F Miller, 4th Floor,Mortimer Market Centre,Mortimer Market, (offCapper Street), LondonWC1E 6AU, UK.Accepted for publication26 June 1996
237
on January 15, 2020 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.72.4.237 on 1 A
ugust 1996. Dow
nloaded from

ANTIRETROVIRALS
i ..h
YT*.-Z V.:
ddC
1W ft!_...Ii f !! f\ !
41.-t!! |
D4T
,-o ..
j~ ~-.'U(91(Cd I- t f t f 1
K ~ on z...:.________ _~ a ed
rIln cIvC s. ---------------T
.')s(' _..__---r___it?(<-p)]UluiI!' \ipSora.?I (
I-i
FoscaF%th.__ __ . _ 'i! 1wi_v
al{' 11> j.
COFazl~f?___ --------_ __4.. ".A.lc>l )?C f!
6llull___s__ I___Ois_ _~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~___'
tQI'le.Ci' IJOl-iC j
; r3itra...c:cpti .4 ...P(-.l!alzlic,ric 1 \)g 9 *_ [ 0 ^ Ll j
_Ilf)1i*lo l-tzt7 ? 4i?)
~~~~~__ ____ --'.....-.4-.--. -||||I|
__._I__w ?-._ist.r'dinc (!) r T|uInoEnHIs l 1S ~id'r.rzti^iin!;! d:c.
M.c,_ A0
a C.cli! '.4' l .
-c - I-- .fJJ|C J[*f
,Additive Toxicity
w I 1 Increased Seruim Level s
Decreased Serum
Miscellanieous
[.d...
h .9
K. -
_ _ "U~~~~~.q
.. v Xw *4 7
---- .. - - --- 1- -- 1, 1 - .4nsU_r«n JU:Ts_a_Brs_wics tw OoEwX.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~__~~~._^w I rv . --1--------1 '~~~~~~~~~~~i b'- m 1ll-0.....
-2
.l'i1ddl A.
1A
.i ., .,'-; -1 Z.... L---'\. i ` i !"'! (_---) 1.7111
1 .1
,. .1,i ;, In ', C, ..-, -,
... ', ', '-
5
on January 15, 2020 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.72.4.237 on 1 A
ugust 1996. Dow
nloaded from

Adverse effects and drug interactions of medications commonly used in the treatment of adult HIVpositive patients
oral administration of didanosine, 50% isexcreted via the kidneys by active tubular secre-
tion and glomerular filtration. The metabolismof didanosine has not been evaluated in man.
Studies in dogs show that it undergoes exten-sive hepatic metabolism.2 Zalcitabine isexcreted largely unchanged in the urine.' Theexcretion of stavudine is divided between renaland non renal routes, undergoing net renaltubular secretion.4
Zidovudine has the greatest potential forinteractions with drugs that influence livermetabolism. Many drugs have been suspectedof inhibiting the metabolism of zidovudine.5 Inan early study the concurrent use of paraceta-mol (not in the table) with zidovudine was asso-
ciated with an increased incidence ofmyelotoxicity,6 and a case of severe hepatotoxic-ity has been reported.7 These were thought tobe caused by a pharmacokinetic interactionbetween zidovudine and paracetamol, howeverfurther research has not shown changes in thepharmacokinetic parameters of the two drugs.89
Clarithromycin has been reported both toreduce zidovudine concentrations and to haveno effect.'0 11 Similarly, serum levels of pheny-toin have been reported to be both increasedand decreased when zidovudine is started.5Methadone has been shown to increase the area
under the curve (AUC) of zidovudine in some
patients.'2 and In vitro and in vivo work whichhas examined the effect of the azoles on zidovu-dine metabolism, has shown a decrease inmetabolism of zidovudine to it's glucuronide.The clinical significance of this remains uncer-
tain."3 Concomitant administration ofprobenecid may inhibit the metabolism ofzidovudine to the glucuronide metabolite andmay also decrease the rate of excretion ofzidovudine and its metabolite."4 This may alsooccur with didanosine and stavudine.'5 4
Rifabutin used as prophylaxis ofMycobacterium avium-intracellulare (MAI) hasbeen shown to decrease zidovudine C.. andAUC, and increase zidovudine clearance.'6 It islikely that rifampicin would do likewise.Few drugs have been reported to alter the
pharmacokinetics of didanosine, zalcitabineand stavudine. Oral ganciclovir increasesplasma levels of didanosine by an unknownmechanism.'7 The combination of IV ganci-clovir and didanosine may increase the poten-tial for pancreatitis but the reason for this hasnot been elucidated.'8The renal excretion of zidovudine, didano-
sine, zalcitabine and stavudine may be inhibitedby drugs that cause renal toxicity such asaminoglycosides, IV amphotericin, foscarnet,cidofovir and IV pentamidine. Dosage reduc-tions are recommended by the manufacturersfor zidovudine, didanosine, and stavudine inpatients with renal impairment. The dose ofzalcitabine should also be reduced but neitherthe degree of reduction nor information aboutwhen this reduction should take place is avail-able.
Didanosine is unstable at the pH found inthe stomach. Therefore it is supplied as a
chewable/dispersible tablet with dihydroxyalu-minium sodium carbonate, magnesium
hydroxide and sodium citrate as buffer toincrease the pH of the stomach and thus itsbioavailability. The presence of the buffer mayinterfere with absorption of a number of drugsby two different mechanisms. By increasingthe pH it may reduce the solubility and thusabsorption of acid soluble drugs eg dapsone,ketoconazole, itraconazole, pyrimethamine,trimethoprim and rifampicin.'9 Alternatively,the aluminium and magnesium ions containedin the chewable/dispersible tablet formulationmay bind (chelate) the drug molecules egciprofloxacin, and tetracyclines (not in thetable) thus preventing their absorption.2 Toreduce the effect of didanosine on the absorp-tion of other drugs they should be adminis-tered at least 2 hours apart.
Pharmacodynamic interactionsThe most frequent adverse effects afterchronic use of zidovudine are related to bonemarrow toxicity and result in anaemia andneutropenia. Those of didanosine and zal-citabine are peripheral neuropathy and pan-creatitis. Zalcitabine has also been reported tocause thrombocytopenia in approximately 4%of patients. The major dose limiting toxicitiesof stavudine are peripheral neuropathy andincreased hepatic transaminases.4 The com-bined use of ganciclovir and zidovudine hasbeen reported to be poorly tolerated inpatients with HIV and serious cytomegalovirus(CMV) disease. In one study 82% of patientson this combination developed severe to lifethreatening haematological complications.20Zidovudine should be stopped whilst patientsare receiving high dose intravenous ganci-clovir. It may be reintroduced (generally at alower dose) when the dose of ganciclovir isreduced, or the patient is transferred to theoral formulation.The combination of foscarnet with zidovu-
dine is haematologically better tolerated thanthat of ganciclovir and zidovudine. However,one small study has reported increased trans-fusion.requirements in patients receiving bothzidovudine and foscarnet. This occurredmainly during the treatment period.2' Careshould be taken with other drugs reported tocause haematological toxicity (see table 1,opposite page).
Drugs that cause peripheral neuropathyshould be used with caution in combinationwith didanosine, zalcitabine, or stavudine anddrugs that cause pancreatitis in combinationwith didanosine and zalcitabine. If this is notpossible in an acute clinical situation, then theantiretroviral medication should be stoppedwhilst treatment is taking place and restartedafter a one-to-two week wash out period.22 Ifchronic treatment is required the patientshould be closely monitored for clinical andbiochemical signs of pancreatitis or peripheralneuropathy.
MiscellaneousZidovudine and Aciclovir There is a singlereport of a patient who whilst receiving intra-venous aciclovir for the treatment of herpessimplex infection experienced severe lethargy
239
on January 15, 2020 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.72.4.237 on 1 A
ugust 1996. Dow
nloaded from
Ampho IKeto/Itra T Flu FlucytoANTI FUNGALDRUGS ~~~~~~~ ~ ~~~~~~~~~~~~~~~~tericinconasole conasole sine
1-0~~~~~~~~~~~~~~~~~~.
cLcl IZ1C.9:flC
tp P a(Cifln
Qort1CoS c-,ri oc(.fsCjarih raonyci n
Dapsone
D-----ctOS/ unorbcn lpso l
r r
hoecetc.!o!
Kt/Kectoc rn1:1zoIc-i\~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~CtI0flIddZOIC~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~......
Cral Coi,tracice-ptive<Pentanmidinc ('!)o
P henytov].Pvrirneham nle.
___ _ _ ii~f~ ! 1ii!-0 lf1
RiFabUtin
Rifam-picirn I~"Stvuin (D4)
S uIoph ona fil51CS (hIligh doSec).T" ai5o d
\ .inUIlast.!ne / \icitn
Zalcitabine (ddcC)ZIdo0\' LldtneK,AZT)
9
A_.la.~!!
am~~~
I 1
Iz1IzIizI_____?Additive ToxicityIncreased Serum L-evelsDecreased Serum LevelsMiscellaneous
N -
K -
MyelotoxicityPan cre atitUsPeriphieral' Neur'opdthyNephrotoxicityH epatotoxic itty
4? ¶I* os zN
Increasing CilinicalSignificance
LIII'LIZ'LIII
mF. i
g
1 1
1. 4.l 11 a4* ch1
on January 15, 2020 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.72.4.237 on 1 A
ugust 1996. Dow
nloaded from

Adverse effects and drug interactions of medications commonly used in the treatment of adult HIVpositive patients
and fatigue on initiation of zidovudine. Thesesymptoms resolved when the aciclovir wasstopped.23 In practice zidovudine and aciclovirare frequently used together without this prob-lem being encountered.
Zidovudine and pyrimethamine andpyrimetha-minelsulphadiazine Zidovudine has beenfound to antagonise the toxoplasmocidal effectof a low concentration of pyrimethamine invitro, and in vitro synergism betweenpyrimethamine and sulphadiazine againstToxoplasma gondii is reversed by zidovudine.Zidovudine also antagonises the therapeuticeffect of pyrimethamine in mice acutelyinfected with Tgondii. The clinical significanceof this finding is unclear.24
Zidovudine and stavudine In cell cultureszidovudine inhibits the phosphorylation ofstavudine, while stavudine has no effect on thephosphorylation of zidovudine. This findingmay potentially influence the decision to usestavudine and zidovudine as combinationtherapy for HIV infection.25
Zidovudineldidanosine and ganciclovir Invitro work has suggested that ganciclovirantagonises the anti-HIV effect of zidovu-dine/didanosine.26
Didanosine and drugs with a low bioavailabil-ity such as atovaquone and oral ganciclovir Thebuffer in didanosine may induce diarrhoea insome patients. In patients taking drugs with alow bioavailability this may reduce absorptionand make the medication ineffective.27
Antifungal medication: amphotericin,ketoconazole, itraconazole, fluconazoleand flucytosine (Table 2 see oppositepage)Antifungal medications are widely used in thetreatment of the HIV positive patient. Severityof infection ranges from superficial oral can-dida to cryptococcal meningitis and pul-monary aspergillosis. The sensitivity of theorganism, site of infection, drug toxicity andinteractions will often dictate the choice oftherapy to be used. Amphotericin, althoughextremely nephrotoxic is the treatment ofchoice in severe infections.
Pharmacokinetic interactionsKetoconazole, and itraconazole share many ofthe same interactions. They require an acidenvironment for optimal absorption, are exten-sively metabolised in the liver and excretedalmost exclusively in the faeces and the urine.In contrast the absorption of fluconazole isunaffected by gastric pH and it is minimallymetabolised, with 80% being excretedunchanged in the urine. Fluconazole is the onlyazole for which dose reduction is necessary inrenal impairment and care needs to be takenwith nephrotoxic drugs.
All three azoles inhibit the cytochrome P450liver metabolising isoenzyme CYP3A4 leadingto increased serum levels of many drugs (seetable 2).28-31 Concurrent administration ofazoles with astemizole, terfenadine and cis-apride is contraindicated following reports ofprolongation ofthe QT interval and fatalities.2932
Phenytoin toxicity has been observed when flu-conazole was added to patients' treatment regi-mens.33The metabolism of ketoconazole, itracona-
zole, and fluconazole is accelerated by drugswhich induce liver enzymes such as rifampicin,rifabutin, phenytoin etc. Almost negligibleserum levels of itraconazole have been reportedin a patient taking concurrent rifampicin anditraconazole,3435 and poor treatment outcomesand clinical relapse have been reported inpatients taking fluconazole and rifampicin.3637Carbamazepine and phenobarbitone have alsobeen shown to induce itraconazole metabo-lism.38 Isoniazid decreases plasma levels ofketoconazole and so may possibly have thesame effect on itraconazole levels.39The absorption of ketoconazole and itra-
conazole is reduced as the pH of the stomachincreases. In a study comparing the absorptionof ketoconazole and fluconazole in patientsreceiving intravenous cimetidine, in order totitrate their stomach acid to pH 6.0 and above,there was a dramatic effect on the disposition ofketoconazole. Reductions of 90% in AUC andmaximum concentrations were seen.40 The dis-position of fluconazole was unaffected. Toincrease the solubility and thus absorption ofketoconazole and itraconazole patients areadvised to take them with an acidic carbonatedbeverage eg lemon and lime carbonated drinks,carbonated water or cola.4' Any drug whichincreases gastric pH including didanosine,should be taken at least two hours after keto-conazole or itraconazole, and where possiblethey should be taken with or after food (exceptfor itraconazole liquid which contains a bufferand is better absorbed in a fasted state).
Flucytosine is excreted mostly unchanged inthe urine. It is extremely myelotoxic and toxicityis related to serum levels. Serum levels must bemonitored closely especially when it is beingused in combination with a nephrotoxic agenteg amphotericin.
Pharmacodynamic interactionsThe main toxicities of amphotericin are feverand chills on administration, abnormal renalfunction, hypokalaemia and hypomagnesaemia.Acute liver failure, normochromic normocyticanaemia, thrombocytopenia, leucopenia andother haematological abnormalities have alsobeen reported. The use of amphotericin withother nephrotoxic drugs should be avoidedwherever possible or if this is not possible itshould be used with extreme caution (see table2). Acute, rapidly progressive, renal failure hasbeen documented with the simultaneous use ofIV amphotericin and IV pentamidine.42The main toxicities of the azoles are rash and
elevations of liver function tests. Unless abnor-mal liver function tests are present the use ofazoles with other potentially hepatotoxic drugsis not precluded. There is a possible interactionbetween alcohol and ketoconazole (see undermiscellaneous).As flucytosine is extremely myelotoxic, its
use with other myelotoxic drugs should beavoided. If this is not possible eg the use offlucytosine with cytotoxic drugs, or IV ampho-
241
on January 15, 2020 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.72.4.237 on 1 A
ugust 1996. Dow
nloaded from

MYCOBACTERIAL DRUGS Rifarnpicin~ Rifalbutin LiClarithro Az ithro
ILM~~~~~~~~~~~~~~~~~~~~~
-V3 0F'G 'Er fr! -
d 1-1 L!isaride1 4
rc)~~~~~~~~~~~~~~
Y'ICKC) clunci
Qihtomcn --c!K' '
_____________________________________________________________ fit!! ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~' !. .._....._
( Kapsone~~~~~ c
vtOrro1i
L,nv U clO, r_______
t o :a S___t________ _n________ _____
z.cVHd'C- (tC) .?L .
Zdovu inccL ) 4 ? -C____ ___F
......Additive To--xicity7 7 I.ncreased Serum Levels
Lu-- Decreased Serum Levels
LIZZIZZI M'scelianeous
N
1.
Myelotoxi-cityPanecreat it is
Peripheral Neuropathy
Nephro.toxicityHe patotoxicity
ia) ! ; C
S.iqnifi( a-Ince
on January 15, 2020 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.72.4.237 on 1 A
ugust 1996. Dow
nloaded from

Adverse effects and drug interactions of medications commonly used in the treatment of adult HIVpositive patients
tericin, close monitoring of the patient'shaematological parameters is necessary.
MiscellaneousAmphotericin and corticosteroids The combineduse of IV amphotericin and corticosteroidsmay exacerbate the renal potassium losscaused by amphotericin.43
Amphotericin and azoles There is a theoreti-cal interaction between amphotericin andazoles. Azoles inhibit ergosterol synthesis andthereby eliminate the target for the activityof amphotericin. The clinical significance ofthis interaction has not yet been clearlydefined.445
Ketoconazole and alcohol Exceptional casesof a disulfiram-like reaction to alcohol charac-terised by flushing, rash, peripheral oedema,nausea and headache have been reported. Allsymptoms resolved completely within a fewhours.39
Mycobacterial drugs: rifampicin,rifabutin, clarithromycin andazithromycin (Table 3 see opposite page)Combinations of these drugs are used to treatboth Mycobacterium tuberculosis (TB) and dis-seminated MAI infections.
Pharmacokinetic interactionsRifampicin and rifabutin are derivatives of therifamycin molecule. Both are hepaticallymetabolised. Metabolic products are princi-pally excreted in bile and to a lesser extent inurine. The dose of rifampicin does not have tobe reduced in patients with renal impairment,but the dose of rifabutin should be reduced ifthe creatinine clearance falls below 30ml/min.Both drugs induce liver enzymes resulting inthe accelerated metabolism of other hepaticallymetabolised drugs (see table 3), the effect ofrifampicin being greater than that of rifabutin.The effects of enzyme induction may be seenwithin a few days, but maximal induction takesmore than a week to occur.The effect of rifampicin on the metabolism
of azoles (see above), corticosteroids, clar-ithromycin, dapsone, methadone, the oral con-traceptive, phenytoin and warfarin (not intable) are clinically very important. For exam-ple; it is recommended that the dose of corti-costeroids be doubled in some instances.46 It isreported that prophylaxis of Pneumocystiscarinii pneumonia with dapsone failed becauseof the interaction with rifampicin47 and serumlevels of phenytoin, and the clinical effective-ness of warfarin and the oral contraceptive arereduced.4849 Rifampicin increases the rate ofmetabolism of many opiates includingmethadone and withdrawal symptoms may beinduced.50
In one prospective study, rifampicin, and to alesser extent rifabutin, were shown to signifi-cantly reduce the mean serum levels of clar-ithromycin.51 This has raised doubts as to theeffectiveness of this combination for the treat-ment of MAI and further studies are required.Clarithromycin in turn has been shown toinhibit the metabolism of rifabutin leading to
an increased incidence of uveitis and neutrope-nia. Fluconazole and potentially the otherazoles have also been shown to increase plasmalevels of rifabutin.52-57
Clarithromycin and azithromycin are bothmacrolide antibiotics. Clarithromycin is exten-sively hepatically metabolised to its activemetabolite 14-hydroxy clarithromycin. Thehalf life of clarithromycin and its metaboliteare increased in the presence of renal impair-ment, leading to the recommendation that thedose is reduced in this situation. The propor-tion of absorbed azithromycin that undergoeshepatic biotransformation is unknown. Severalmetabolites have been identified but these arenot thought to possess significant antimicrobialactivity. The primary route of azithromycinelimination may be via the bile and faeces,although transintestinal elimination has alsobeen proposed as a primary route of elimina-tion. Less than 6% of a dose of azithromycin isrecovered in the urine within one week ofadministration.58The mechanism of the inhibition of hepatic
cytochrome P450 enzymes by macrolideantibiotics has been well documented.59Clarithromycin shares many of the interactionsof erythromycin. It appears to inhibit themetabolism of carbamazepine leading toincreased serum concentrations,60 it inhibitsthe metabolism of the non-sedating antihista-mines and cisapride increasing the risk of car-diac arrhymias.6' The potential for otherinteractions seen with erythromycin needs tobe borne in mind eg increased levels of digoxinand theophylline, and enhanced clinical effectsof corticosteroids warfarin62 and vinblastine.63
In contrast to clarithromycin, azithromycinhas been shown to be relatively free of druginteractions. It does not exhibit the interactionwith the non-sedating antihistamines and cis-apride.61 However, the possibilities of interac-tions should be considered as an increase inneutropenia comparable to that which occurswith clarithromycin was reported whenazithromycin was used in conjunction withrifabutin.Y
Pharmacodynamic interactionsWith all these drugs most frequently encoun-tered side effects involve the gastrointestinaltract, for example nausea and vomiting.
Rifampicin and rifabutin will stain bodysecretions red/orange colour, rifabutin will alsostain the skin. Both have the potential toincrease liver enzymes, and to cause neutrope-nia. High serum concentrations of rifabutinincrease the incidence of uveitis and are alsoassociated with a syndrome of arthralgia/arthritis.52 57 In the treatment of TB abnormalliver function tests, that may be rifampicininduced, have been reported more commonlyin alcohol abusers, those aged > 35 years, themalnourished or those with known hepatic dis-ease. Care should be taken with the use ofrifampicin in these patients.65
MiscellaneousClarithromycin and zidovudine See underzidovudine
243
on January 15, 2020 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.72.4.237 on 1 A
ugust 1996. Dow
nloaded from

ANTIVIRALS Aciclovir IGancilclovir Foscarnet Cidofovir' &_______ ~~~~~probencid
L\mrhl tcri0 IVC!,(iI v) C f '----------
tticrf'n in, inpd
AthIIrolniycinCarLarnaC1zepine
Ctdoov probenc'd 1 i!
C".IprofioxacinC-orticosterilodsClar"IthromnycinDa psOflCr
Didanosinc (ddi)Doxor/Da,unorubicin (liposomlal) _____
t IUiconadzo01e
Flu cytos ine
(000i
Foscairn-et I! !
'snc iovi 1!_ _ _ _3__c!
son Iiaz ICtr/Ket-ocona-zol e
MethadoDne
fviet ron iciazoleOral C"-onitraceptive
PhenytonPvrimethairrune
PifamnpicinStfavu!jdinrie (D4T)Sulphonamid'es (highi dose)
-I-
Thai dorn ideV1:inblastine 71- \vincri stinieZa-clcltaUsne (dd-C) ______
Zi1dovudinc_(A\ZT) ______
I 7o!!
LfE
4nWL
i- hf1LI- ~~Additive Toxicity
EIIIIIII Increased Serum LevelsEIIIIIIIDecreased Serum Lev-els[171171 Miscerllaneours
N -
K -
MyelotoxicityPancreati tisPeripheral NeuropathyNephrotoxicityHepiatn:-tnvic ity1
9) I II0. * 00 ;
Increasing ClinicalSignificance
i i t iAtas
I
.1-
I
on January 15, 2020 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.72.4.237 on 1 A
ugust 1996. Dow
nloaded from

Adverse effects and drug interactions of medications commonly used in the treatment of adult HIVpositive patients
Antivirals: aciclovir, ganciclovir,foscarnet, cidofovir and probenecid(Table 4 see opposite page)In HIV positive patients aciclovir is used forthe treatment and maintenance of herpes sim-plex virus 1 and 2, and varicella zoster.Ganciclovir, foscarnet, and cidofovir are usedmainly for the treatment and maintenance ofcytomegalovirus, but also have activity againstthe herpesviruses.
Pharmacokinetic interactionsAciclovir is slowly and incompletely absorbed;its oral bioavailability is approximately15-30%.66 In infected cells it is converted byvirus-encoded thymidine kinase to its mono-phosphate derivative. Subsequent diphospho-rylation and triphosphorylation are catalysedby cellular enzymes. Aciclovir triphosphateinhibits viral DNA synthesis by acting as asubstrate for viral DNA polymerases and pre-venting further DNA chain elongation.Aciclovir is minimally metabolised, and about85% is excreted unchanged in the urinethrough glomerular filtration and renal tubularsecretion. Drugs such as probenecid thatinhibit renal tubular secretion or resorptionmay reduce clearance of aciclovir and thusincrease plasma concentrations. The dose ofaciclovir should be reduced in patients withimpaired renal function.
Ganciclovir shares the same enzymaticchanges and mode of action as aciclovir. It haspoor oral bioavailability with values of 3-4-6%being quoted.67 Bioavailability may beincreased if ganciclovir is taken with food.68Almost 100% of ganciclovir is excretedunchanged in the urine. As with aciclovirprobenecid may increase plasma levels and sothe dose of ganciclovir should be reduced inpatients with impaired renal function.
Foscamet has very poor oral absorption, theserum levels required for activity against CMVand other herpesviruses may only be achievedby intravenous administration. Renal clear-ance accounts for most of the plasma clear-ance, however, up to 20% of a cumulativedose may have been deposited in bone 7 daypost infusion.69 The dose of foscarnet must bereduced in patients with impaired renal func-tion. As foscamet may cause nephrotoxicitythe doses of renally cleared drugs being usedconcurrently with foscamet should be moni-tored closely (see table 4).
Cidofovir is an acyclic nucleotide analogue.Unlike aciclovir and ganciclovir it does notdepend on phosphorylation by viral nucleosidekinases to exert its antiviral effect. Instead, thedrug is phosphorylated to its active form bycellular enzymes. In vitro studies have sug-gested that the resulting active metabolites arecleared slowly from the intracellular space.Approximately 90% of the intravenous dosewas recovered unchanged in the urine in 24hours. It has been shown that active tubularsecretion played a significant role in the clear-ance of cidofovir. The dose limiting toxicity ofcidofovir is nephrotoxicity. The concurrentadministration of probenecid has been shownto ameliorate its effect on proximal tubularcells, perhaps by decreasing the initial concen-
tration of cidofovir in the cortex of the kid-ney.70 The dose of cidofovir must be reducedin patients with impaired renal functionalthough there are few data available on whichto base decisions about dose reductions inrelation to specific creatinine clearances. Ascidofovir may cause nephrotoxicity the dosesof concurrently used renally cleared drugsshould be monitored closely (see table 4). Ascidofovir is always administered withprobenecid, it is important to considerprobenecid drug interactions (see table 4).
Pharmacodynamic interactionsAciclovir is well tolerated. At high intravenousdoses aciclovir has been reported to crystalisein the kidneys. Therefore care should be takenwith the use of other potentially nephrotoxicdrugs and the dose of aciclovir should bereduced if nephrotoxicity occurs.The dose limiting toxicities of ganciclovir
are neutropenia and thrombocytopenia. Careshould be taken in using ganciclovir with othermyelotoxic drugs as an increased incidence ofmyelotoxicity has been reported with the con-current use of zidovudine and ganciclovir (seeabove).
Foscarnet and cidofovir are both nephro-toxic. As with amphotericin (see above) con-current use of other nephrotoxic drugs shouldbe avoided where possible.
MiscellaneousAciclovir and zidovudine See under zidovu-dine
Combined use of aciclovir with ganciclovirlfos-carnetlcidofovir This should not be requiredas ganciclovir/foscarnet/cidofovir all haveactivity against herpes viruses. Occasionally,patients experience a break through of herpeswhen on maintenance doses of these agents. Ifthis occurs aciclovir should be used in the nor-mal manner.
Ganciclovir and imipenem (not in table)Seizures have been reported with this combi-nation (data sheet).
Ganciclovir and zidovudineldidanosine Seeabove.
Foscarnet and ciprofloxacin Seizures havebeen reported with this combination.7'
Foscarnet and corticosteroids Amphotericinand foscamet cause potassium depletion,therefore from the interaction betweenamphotericin and corticosteroids it followsthat corticosteroids may increase the potas-sium depletion seen with foscamet.
Part 2 In the second part of this article thenewer anti retrovirals will be considered: indi-navir, saquinavir, ritonavir and lamivudine(3TC).We acknowledge the help of Ms Sally Hibbert, SeniorComputer Services Technician, Pharmacy Departmnent, UCLHospitals for her help in the design and compilation of theinteraction charts and Jane Rutherford for help with the typingof this manuscript.
1 Blum MR, Liao SH, Good SS, de Miranda P.Pharmacokinetics and bioavailability of zidovudine inhumans. AmJrMed 1988 85: (suppl 2A) 189-4.
2 ABPI Data Sheet Compendium 1995-96:326-8. Videx.3 ABPI Data Sheet Compendium 1995-96:1431-3. 1431-3.
Hivid.
245
on January 15, 2020 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.72.4.237 on 1 A
ugust 1996. Dow
nloaded from
Heylen, Miller
4 Dudley M, Graham K, Kaul S, et al. Pharmacokinetics ofstavudine in patients with AIDS or AIDS-related com-plex. JInfect Dis 1992;166:480-5.
5 ABPI Data Sheet Compendium 1995-96:1952-6. Retrovir.6 Fischl MA, Richman DD, Grieco MH, et al. The efficacy of
azidothymidine (zidovudine) in the treatment of patientswith AIDS and AIDS related complex. A double blindplacebo-controlled trial. N Engl Jf Med 1987;317:185-91.
7 Shriner K, Bidwell Goetz M. Severe hepatotoxicity in apatient receiving both acetaminophen and zidovudine.AmJMed 1992;93:94-6.
8 Steffe EM, King JH, Inciardi JF, et al. The effect of aceta-minophen on zidovudine metabolism in HIV-infectedpatients. JAcquir Immun DefSynd 1990;3:691-4.
9 Burger DM, Meenhorst PL, Koks CHW, Beijnen JH.Pharmacokinetics of zidovudine and acetaminophen in apatient on chronic acetaminophen therapy. AnnPharmacother 1994;28:327-30.
10 Craft MS, Craft JC. Drug interaction between clar-ithromycin and oral zidovudine in HIV-1 infectedpatients. Clin Pharmacol Ther 1994;53:163.1-114.
11 Vance E, Watson-Bitar M, Gustavson L, Kazanjian P.Pharmacokinetics of clarithromycin and zidovudine inpatients with AIDS. Antimicrob Agents Chemother 1995;39:1355-60.
12 Schwartz EL, Brechbuhl AB, Kahl P, Miller MA, SelwynPA, Friedland GH. Pharmacokinetic interactions ofzidovudine and methadone in intravenous drug-usingpatients with HIV infection. Jf Acquir Immun Def Synd1992;5:619-26.
13 Asgari M, Back DJ. Effect of azoles on the glucuronidation ofzidovudine by human liver UDP-glucuronosyltransferase. JfInfect Dis 1995;172:1634-6.
14 Hansten PD, Horn JR. Drug Interactions and Updates.Vancouver, Applied Therapeutics Inc. 1990.
15 Jones M, Bristol-Myers Squibb Pharmaceuticals Ltd:Personal communication, didanosine and probenecid.
16 Narang P, Nightingale S, Manzone C, et al. Does rifabutinaffect zidovudine disposition in HIV + ve patients ? VIIIInternational Conference on AIDS, HI STD WorldCongress July 1992; Abstract PoB 3888.
17 Gaines K, Wong R, Jung D, et al. Pharmacokinetic interac-tions with oral ganciclovir: zidovudine, didanosine,probenecid. 10th International Conference on AIDS:1994 Aug 7-12; Yokohama (japan) 1994 Abstract 004B.
18 Personal communication Syntex Pharmaceuticals Ltddidanosine and ganciclovir.
19 Metroka CE, McMechan MF, Andrada R, Laubenstein U,
Jacobus DP. Failure of prophylaxis with dapsone inpatients taking dideoxyinosine. N Engl Jf Med 1991;325:737.
20 Hochster H, Dieterich D, Bozette S, et al. Toxicity ofCombined ganciclovir and zidovudine for cytomegalo-virus disease associated with AIDS. Ann Int Med 1990;113:111-7.
21 Palestine AG, Polis MA, De Smet MD, et al. A randomised,controlled trial of foscarnet in the treatment ofcytomegalovirus retinitus in patients with AIDS. Ann IntMed 1991;ll5:665-73.
22 NIAID updates dideoxyinosine toxicity profile, suggestsways to reduce risk of pancreatitis. Clinical Pharmacy1990;9:832-8.
23 Bach MC. Possible drug interaction during therapy with azi-dothymidine and acyclovir for AIDS. N Engl Jf Med1987;316:547.
24 Israelski DM, Corrynne T, Remington JS. Zidovudineantagonises the action of pyrimethamine in experimentalinfection with Toxoplasma gondii. Antimicrob AgentsChemother 1989;33:30-4.
25 Sandstrom E, Oberg B. Antiviral therapy in humanimmunodeficiency virus infections. Current status (part1). Drugs 1993;45:488-508.
26 Medina DJ, Hsiung GD, Mellors JW. Ganciclovir antago-nises the anti-human immunodeficiency virus type activityof zidovudine and didanosine in vitro. Antimicrob AgentsChemother 1992;36:2217-30.
27 Hughes W, Leoung G, Kramer F, et al. Comparison of ato-vaquone (566C80) with trimethoprim-sulphamethoxa-zole to treat PCP in patients with AIDS. New EnglJ Med1993;328: 1521-7.
28 Seaton TL, Celum CL, Black DJ. Possible potentiation ofwarfarin by fluconazole. DICP. Ann Pharmacother 1990;24:1177-8.
29 Honig PK, Wortham DC, Hull R, Zamani K, Smith JE,Cantilena LR. Itraconzole affects single-dose terfenadinepharmacokinetics and cardiac repolarization pharmaco-dynamics. Clin Pharmacol 1993;33: 1201-6.
30 Bohme A, Ganser A, Hoelzer D. Aggravation of vincristine-induced neurotoxicity by itraconazole in the treatment ofadult ALL. Ann Haematol 1995;71:311-2.
31 Olkkola KT,et al. Midazolam should be avoided in patientsreceiving the systemic antimycotics ketoconazole or itra-conazole. Clin Pharmacol Ther 1994;55:481-5.
32 Committee on Safety of Medicines. Medicines Control
Agency. Curr Probl Pharmacovigil 1996;22: 1-2.
33 Cadle RM, Zenon GJ,Rodriguez-Barradas MC, Hamill
RJ. Fluconazole induced symptomatic phenytoin toxicity.Ann Pharmacother 1994;28:191-5.
34 Blomley M, Teare EL, de Belder A, Thway Y, Weston M.Itraconazole and anti-tuberculosis drugs. Lancet 1990;336:1255.
35 Drayton J, Dickinson G, Rinaldi MG. Coadministration of
rifampicin and itraconazole leads to undetectable levelsof serum itraconazole. Clin Infect Dis 1994;18:266.
36 Nicolau DP, Crowe HM, Nightingale CH, Quintiliani R.
Rifampicin-fluconazole interaction in critically ill
patients. Ann Pharmacother 1995;29:994-6.37 Coker RJ, Tomlinson DR, Parkin J, Harris JRW, Pinching
AJ. Interaction between fluconazole and rifampicin. BMJr
1990;301:818.38 Bonay M, Jonvile-Bera AP, Diot P, Lemarie E, Lavandier
M, Autret E. Possible interaction between phenobarbital,carbamazepine and itraconazole. Drug Safety 1993;9:309-11.
39 ABPI Data Sheet Compendium 1995-96:734-5. Nizoral.40 Blum RA, D'Andrea DT, Florentino BM, et al. Increased
gastric pH and the bioavailability of fluconazole andketoconazole. Ann Intern Med 1991;114:755-7.
41 Sugar EF, Sugar AM, Kreger BE. Effect of common bever-ages on the dissolution of ketoconazole tablets. AIDS1992;6:1221-2.
42 Antoniskis D, Larsen RA. Acute progressive renal failurewith the simultaneous use of amphotericin B and pen-tamidine. Antimicrob Agents Chemother 1990;34:470-2.
43 ABPI Data Sheet Compendium 1995-6:1774 Fungizoneintravenous.
44 Pahls S, Schaffner A. Aspergillus fumigatus pneumonia inneutropenic patients receiving fluconazole for infectiondue to Candida species: is amphotericin B combined withfluconazole the appropriate answer? Clin Infect Dis 1994;18:484-5.
45 Scheven M, Scheven ML. Interaction between azoles andamphotericin B in the treatment of candidiasis. Clin InfectDis 1995;20:1079.
46 Buffington GA, Dominguez JH, Piering WF, et al.Interaction of rifampicin and glucorticoids. JAMA 1976;236:1958-60.
47 Horowitz HW, Jorde UP, Wormser GP. Drug interactions inuse of dapsone for Pneumocystis carinii prophylaxis.Lancet 1992;339:747.
48 Wagner JC. Rifampicin-Phenytoin drug interaction. DrugIntell Clin Pharm 1984;18:497 [Abstract].
49 ABPI Data Sheet Compendium 1995-6:950-2. Rifadin.50 Jacobson M, Yajko D, Nothfelt D, et al. Randomised
placebo controlled trial of rifampicin, ethambutol, andciprofloxacin for AIDS patients with disseminated MACinfection. _J Infect Dis 1993;168:112-9.
51 Wallace RJ, Brown BA, Griffith DE, Girard W, Tanaka K.Reduced serum levels of clarithromycin in patientstreated with multidrug regimens including rifampicin orrifabutin for Mycobacterium avium-M. intraceUulare infec-tion. _l Infect Dis 1995;171:747-50.
52 Griffith DE, Brown BA, Girard WM, Wallace RJ. Adverseevents associated with high-dose rifabutin in macrolide-containing regimens for the treatment of Mycobacteriumavium complex lung disease. Clin Infect Dis 1995;21:594-8.
53 Siegal FP, Eilbott D, Burger H, et al. Dose-limiting toxicityof rifabutin in AIDS-related complex: syndrome ofarthralgia/arthritis. AIDS. 1990;4:433-41.
54 Rifabutin prophylaxis against Mycobacterium avium com-plex infection. New Engl Med 1994;330:436-39. Miscauthors. Comments on Nightingale SD, Cameron DW,Gordin FM, et al. Two controlled trials of rifabutin pro-phylaxis against Mycobacterium avium complex infectionin AIDS. NEngl_JMed 1993;329:828-33.
55 Frank MO, Graham MB, Wispelway B. Rifabutin anduveitis. NEnglJMed 1994;330:868.
56 Fuller JD, Stanfield LED, Craven DE. Rifabutin prophy-laxis and uveitis. NEng7Med 1994;330:1315-6.
57 Narang PK, Trapnell CB, Schoenfelder JR, Lavelle JP,Bianchine JR. Fluconazole and enhanced effect ofrifabutin prophylaxis. N EnglJ, Med 1994;330: 1316.
58 Ballow C, Amsden GW. Azithromycin: The first azalideantibiotic. Ann Pharmacother 1992;26:1253-61.
59 Pensayre D, Larrey D, Funck-Brentano C, Benhamen JP.Drug interaction and hepatitis produced by somemacrolide antibiotics. _J Antimicrob Chemother 1985;16:(Suppl A):181-94.
60 Albani F, Riva R, Barmzzi A, et al. Clarithromycin-carba-mazepine interaction: a case report. Epilepsia 1993;34:161-2.
61 Hansten P, Horn JR. Drug interactions with non-sedatingantihistamines. Drug Interactions Newsletter 1994:737-40.
62 ABPI Data Sheet Compendium 1995-6:15-6. Klaricid.63 Tobe SW, Sui LL, Jamal SA, et al. Vinblastine and ery-
thromycin: an unrecognised serious drug interaction.Cancer Chemother Pharmacol 1995;35: 188-90.
64 Yonren S. Phase 1 study to evaluate the pharmacokineticinteraction between rifabutin and the macrolidesazithromycin and clarithromycin in healthy subjects.(066-074) Personnal communication 26.9.95.
65 Caplin M, Thompson N, Hamilton M, McIntyre N,Burroughs A. Antituberculous therapy and acute liverfailure. Lancet 1995;345:1171.
66 de Miranda P, Blium MR. Pharmacokinetics of aciclovirafter intravenous and oral administration. 7 AntimicrobChemother 1983; (Suppl B):29-37.
67 Jacobson M, de Miranda P, Cederberg DM, et al. Humanpharmacokinetics and tolerance of oral ganciclovir.Antimicrob Agents Chemother 1987;31: 1251-4.
68 Byrne AK, Lavelle J, Follensbee S, et al. Multiple dosecross over pharmacokinetic study to evaluate the effect offood on the relative bioavailability of oral ganciclovir(abstract no. PuB 7077). Proceedings of the VIIIInternational Conference on AIDS and the III STDWorld Congress; 1992 Jul 19-24: Amsterdam.
69 Sjovall J, Bergdahl S, Movin G, Ogenstad S, Saarimaki M.Pharmacokinetics of foscarnet and distribution to cere-brospinal fluid after intravenous infusion in patients withHIV. Antimicrob Agents Chemother 1989;33: 1023-31.
70 Cundy K, Petty BG, Flaherty J, et al. Clinical pharmacoki-netics of cidofovir in human immunodeficiency virus-infected patients. Antimicrob Agents Chemother 1995;39:1247-52.
71 Fan-Harvard P, Sanchorawala V, Oh J, Moser EM, SmithSP. Concurrent use of foscarnet and ciprofloxacin mayincrease the propensitity for seizures. Ann Pharmacother1994;28:869-72.
246
on January 15, 2020 by guest. Protected by copyright.
http://sti.bmj.com
/G
enitourin Med: first published as 10.1136/sti.72.4.237 on 1 A
ugust 1996. Dow
nloaded from
Related Documents











