Adverse Drug Reactions in Dentistry (ADRs): Burden of Disease and Special Considerations Michael J. Rieder Section of Paediatric Clinical Pharmacology Children’s Hospital of Western Ontario Division of Clinical Pharmacology Faculty of Medicine & Dentistry University of Western Ontario London, Ontario [email protected]

Adverse Drug Reactions in Dentistry (ADRs): Burden of Disease and Special Considerations Michael J. Rieder Section of Paediatric Clinical Pharmacology.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Adverse Drug Reactions in Dentistry (ADRs): Burden of
Disease and Special Considerations
Michael J. RiederSection of Paediatric Clinical Pharmacology
Children’s Hospital of Western OntarioDivision of Clinical PharmacologyFaculty of Medicine & DentistryUniversity of Western Ontario
London, [email protected]
Maria• 6 year old child who had a dental abscess
treated in the clinic• Penicillin started 1 week ago• Over the past two days, she has developed
fever, malaise and a rash
QuickTime™ and aPhoto - JPEG decompressor
are needed to see this picture.

Objectives
• Appreciate rate of ADRs• Understand patterns of ADRs to
drugs common to dental practice• Appreciate an approach to an ADR
associated with dental therapy

Perspective on Therapy
•God and His Majesty forbid, the fire of the enemy is not half so dangerous as a single drug–M. Platov, 1812
Selective Therapy
• Era of selective therapy began in two labs in Europe– Cambridge in 1928 - Sir Alexander Fleming -
discovery of penicillin– Germany in 1935 - Gerhard Domagk -
discovery of sulfanilamide• Demonstration of antimicrobial activity• Serenpedity at work - neither investigator was
trying to find an antibiotic

Changes in the Paradigm
• Demonstration of antimicrobial activity of major importance
• Illustration - therapy of Strep. meningitis consisted of rabbit serum, supportive therapy and prayer
• Infectious deaths common• Medical paradigm - care, not cure

Changes in Care - Consequences
• Sulfanilamide activity described in 1935• Widespread clinical use by 1937• Major change in clinical care paradigms
– In first 10 years of use, 10,000 lives saved in UK among children who would have died of Strep. Infections
– Care becomes Cure (Lewis Thomas, Reflections of a Biology Watcher)

Elixir of Sulfanilamide Tragedy
• Sulfanilamide dissolved in ethylene glycol to improve palatability
• Ethylene glycol - a potent nephrotoxin• No pre-marketiug toxicity studies done• Approximately 170 deaths from renal failure,
mostly among children• Responsible chemist committed suicide• Major issue in Congress - led to changes that
led to current drug regulatory system

Introduction
• Adverse Drug Reactions are a common and important clinical problem
• Seen in 5% of patients treated• Responsible for 5% of all hospital
admissions– JAMA 1998; 279: 1200-5
98,000 people in the USA die 98,000 people in the USA die each year as a result of medical errorseach year as a result of medical errors

ADRs in Dentistry
• Relatively little data with respect to ADRs in Dental practice compared to Medical practice
• What data is present suggests that overall rates may be similar
• No a priori reason to assume different rates

ADR Rates
• Overall, rate of ADRs in dental patients appears to be similar to adults
• Risk appears to relate to known risk factors– Int J Clin Pharmacol Ther 1988; 36:
530-3

Risk Factors for ADRs
• History of a previous ADR• Polypharmacy• Impairment of the organs of excretion
(hepatic or renal dysfunction)• Extremes of age• Female gender

History of ADRs
• Elixir of Sulfanilamide Tragedy, 1937• Chloramphenicol Grey Baby
Syndrome, 1950’s• Thallidomide Teratogenicity, 1960’s• Drug substitution errors 1980’s• Ten-fold errors 1990’s• Molecular Misadventures

ADR Classification
• ADRs often called “drug allergy”• Immune involvement is common,
but true drug allergy is relatively rare
• Mislabelling leads to therapeutic confusion
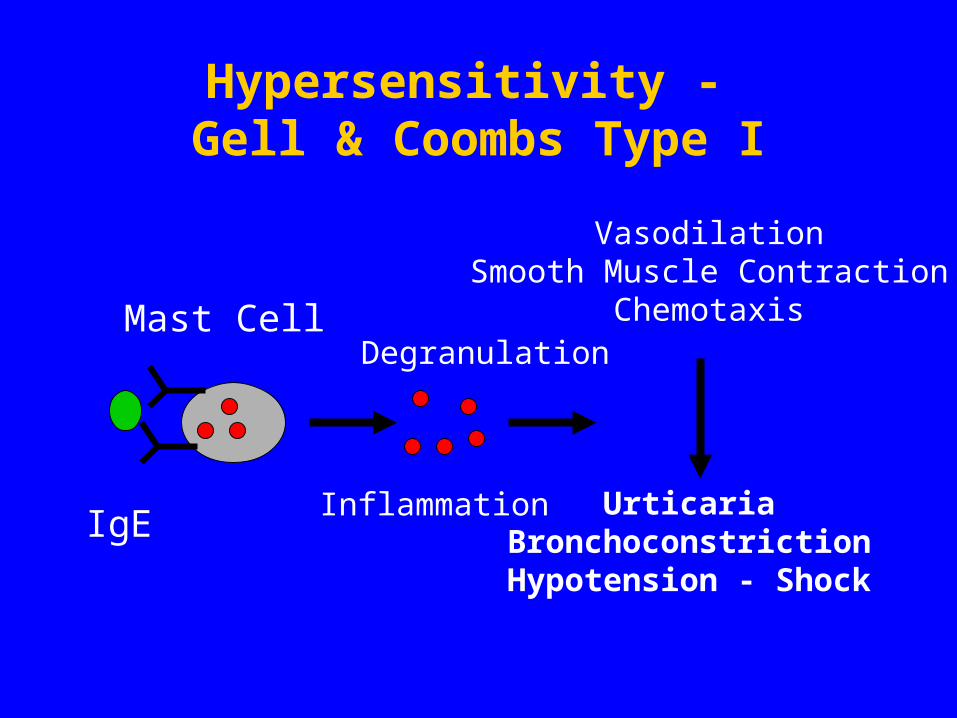
Hypersensitivity - Gell & Coombs Type I
Mast CellDegranulation
Inflammation
VasodilationSmooth Muscle Contraction
Chemotaxis
UrticariaBronchoconstrictionHypotension - Shock
IgE

Hypersensitivity - Gell & Coombs Type II
NK Cell
Phagocyte
IgG
Complement
Cell lysisPhagocytosis
Removed byReticuloendothelial
System

Hypersensitivity - Gell & Coombs Type III
Phagocyte
IgGComplement
ImmuneComplexes
ReactiveOxygenSpecies
Inflammation
BloodVessel
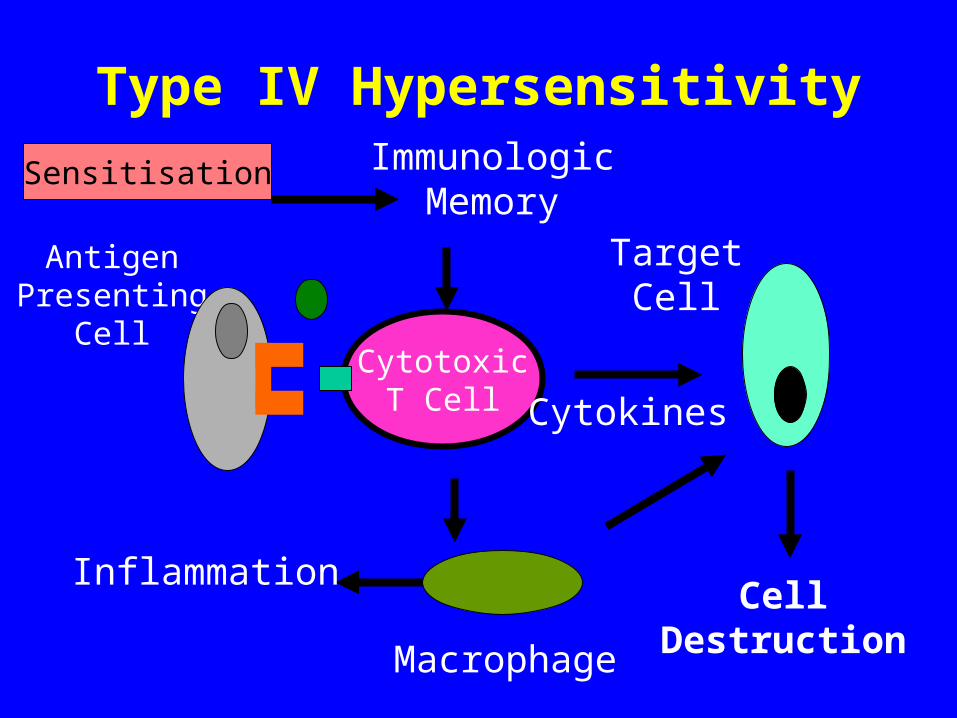
Type IV Hypersensitivity
CytotoxicT Cell
AntigenPresenting
Cell
Macrophage
TargetCell
CellDestruction
Cytokines
Inflammation
ImmunologicMemory
Sensitisation

Gell and Coombs
• Elegant, erudite classification system
• Mechanistic • Sadly, does not address the vast
majority of ADRs

ADR Classifications• A number of schemes have been proposed• Unfortunate and common use of the term
allergy• Patterson, DeSwarte and Greenberger
(1986)– Predictable– Unpredictable
• New England Review of Allergy Proceedings, 1986, 7: 325-42

Predictable ADRs
• Predicated on and predictable from the drug’s pharmacology– Side Effects– Secondary Effects– Interactions– Toxicity
Unpredictable ADRs
• Not known to be related to the drug’s pharmacology– Intolerance– Allergic - Pseudoallergic– Idiosyncratic– Psychogenic

Predictable ADRs• Side Effects
– Fine tremor associated with inhaled salbutamol (albuterol)
• Secondary Effects– Pseudomembranous colitis after lincomycin
therapy• Interactions
– Bleeding when coumadin and cimetadine are given concurrently
• Toxicity– Metabolic acidosis in salicylate overdose

Unpredictable ADRs• Intolerance
– Intractable vomiting associated with erythromycin therapy
• Allergic - Pseudoallergic– Anaphylaxis or urticaria associated with pencillin
therapy• Idiosyncratic
– Stevens-Johnson Syndrome associated with sulphonamides
• Psychogenic– Environmental Hypersensitivity

Commonly Used Drugs
• Penicillins• Opiates• Local Anaesthetics• Acetaminophen • NSAIDs
Penicillins
• Can cause all four types of Gell & Coombs reactions
• Commonest is Type I (hypersensitivity)
• Said to occur in as many as 10% of patients

Penicillins
• Most common ADRs are skin rash and diarrhoea
• Diarrhoea usually self resolving• Rash may be allergic or may be
drug-disease interaction
Penicillins
• Stated incidence of allergy 10%• Actual incidence probably much
lower• ADRs described probably represent
viral-drug interactions• Can be verified or refuted with skin
testing
Penicillins
• Penicillin skin testing available at selected centres
• Testing requires use of both minor and major determinants
• Accurate in even small infants• Often deferred until several years
after an event

Time
Percentage

Opiates
• Commonly used for severe pain• Dose-related respiratory
depression in high doses• About 5% of the population
develops urticaria on usual doses• NOT an allergy - reflects sensitivity• Crosses the class

Local Anaesthetics
• Commonly and widely used• Two common problems -
inadvertent intravenous injection and allergy
• Allergy tends to be unique to class (amide or ester)
• Can be tested for

Skin Testing
• Commonly used• Role is to determine safety, not
causation• Hence, usually uses agents of the
other class

Local Anaesthetic Sensitivity
• Ocassionally involves both classes• A considerable problem for the
practicing dentist• Benadryl may be used instead -
modestly effective

Acetaminophen
• Commonly used• Very safe in usual therapeutic
doses• Only dangerous in overdoses• Can occur in setting of repeated
suproatherapeutic dosing

NSAIDs
• Commonly used and increasingly used among children and adolescents
• Associated with GI bleeds, gaastrointestinal discomfort
• Can be associated with hypersensitivity
NSAIDs
• Can be cross-class• In this case, may need to use
therapeutic alternatives

Other Agents
• Macrolides - can be associated with vomiting and GI upset
• Most common with erythromycin, less common (but not unknown) with newer agents
• Clindamycin - diarrhoea more common than with other agents

Special Cases• Drug Substitution• 10 fold errors
– Unique problem in Paediatrics– More common among certain staff
• Drug Errors– Probably more common in children than
adults– Again, may be more common among
certain staff

Medication Errors in a Paediatric ER - One Month’s
ExperienceType of error Number %Wrong dose 133 (49.1%)Wrong f requency 117 (43.2%)Wrong route 7 (2.6%)Wrong drug 5 (1.8%)I nf ormation 7 (2.6%)Other 2 (0.7%)
Total 271 (100%)

Medication Errors
• Paediatric doses need to be individualized
• Knowledge of paediatric doses often much less than optimal
• Certain staff - trainees, those unused to working with children, mathematically inept - at higher risk

Unique Cases
• Special cases arise in which ADR patterns are not the same in children as in adults
Cefaclor-associated serum sickness - seen in 1% of childrentreated, but probably 0.1 to 0.01%of adults-Can J Clin Pharmacol 1999; 6: 197-201

Pre-Marketing Research
• Pre-clinical use often includes juvenile animals
• Classically, Phase I - III trials include 300 to 5000 patients
• Hence, will NOT detect rare but potentially serious events (e.g. most drug-induced hypersensitivities)

Limitations of Usual Data
• Use of usual data sources for ADR assessment (e.g. CPS) significant
• However, usual data sources (e.g. CPS) are poor sources of ADR information– Common events not reported– Rare events over-stated
Implications
• Novel or serious ADR patterns to new drugs may not be appreciated based on the pre-marketing data available
• The CPS may not help you much• Vigilance is important, especially
for novel agents

Approach to an Undesired Event
• Careful Clinical Approach• Evaluation of therapeutic goals
– Have we achieved the goal?– If not, how are we going to achieve
the goal?– Do we need to revise our goals or do
we need to revise our strategy?

Clinical Approach to a Possible ADR (I)
• History and Physical Examination– Drug, dose, timing, rationale, other
events
• Analysis of Drug Exposure• Differential Diagnosis• Obtaining Information• Coming to a Clinical Opinion

Clinical Approach to a Possible ADR (II)
• Confirmation• Communication• Treatment • Reporting• Coping
– Patient– Patient-physician relationship

References
• Patterson R, DeSwartre RD, Greenberger PA et al.: Drug allergy and protocols for management of drug allergies. New England Review of Allergy Proceedings 1896; 7: 325-42
• Rieder MJ: In vitro and in vivo testing for adverse drug reactions. Pediatric Clinics of North America 1997; 44: 93-111
• Gupta A, Waldhauser L: Adverse drug reactions from birth to early childhood. Pediatric Clinics of North America 1997; 44: 79-92

What About Maria?• Stevens-Johnson Syndrome• Pathogenesis related to bioactivation of drug to a
reactive intermediate and then (probably) immune propagation
• Issues - multi-organ involvement, risk of infection• Therapy - supportive, monitoring for
complications, possible use of pulse corticosteroids
QuickTime™ and aPhoto - JPEG decompressor
are needed to see this picture.

Take Home Message
• Know the drugs that you are using• Be vigilant• When in doubt, ask• When faced with a dilemma, seek
expert opinion
Acknowledgments• Canadian Institutes of Health Research -
MRC• Kidney Foundation of Canada• Hospital for Sick Children Foundation• Drs. Gideon Koren, Doreen Matsui, Shinya
Ito, Greg Kearns, Bruce Carleton, • Drs. Sanford Cohen, Neil Shear, Ralph
Kauffman, Stuart MacLeod
Related Documents











