ADVANCES IN LUNG CANCER DIAGNOSIS 3 rd Annual Southeastern Pathology Conference Greenville, South Carolina Saturday, November 3, 2018 William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ADVANCES IN LUNG CANCER DIAGNOSIS
3rd Annual Southeastern Pathology
ConferenceGreenville, South Carolina
Saturday, November 3, 2018
William D. Travis, M.D.Attending Thoracic Pathologist
Memorial Sloan Kettering Cancer Center
New York, NY

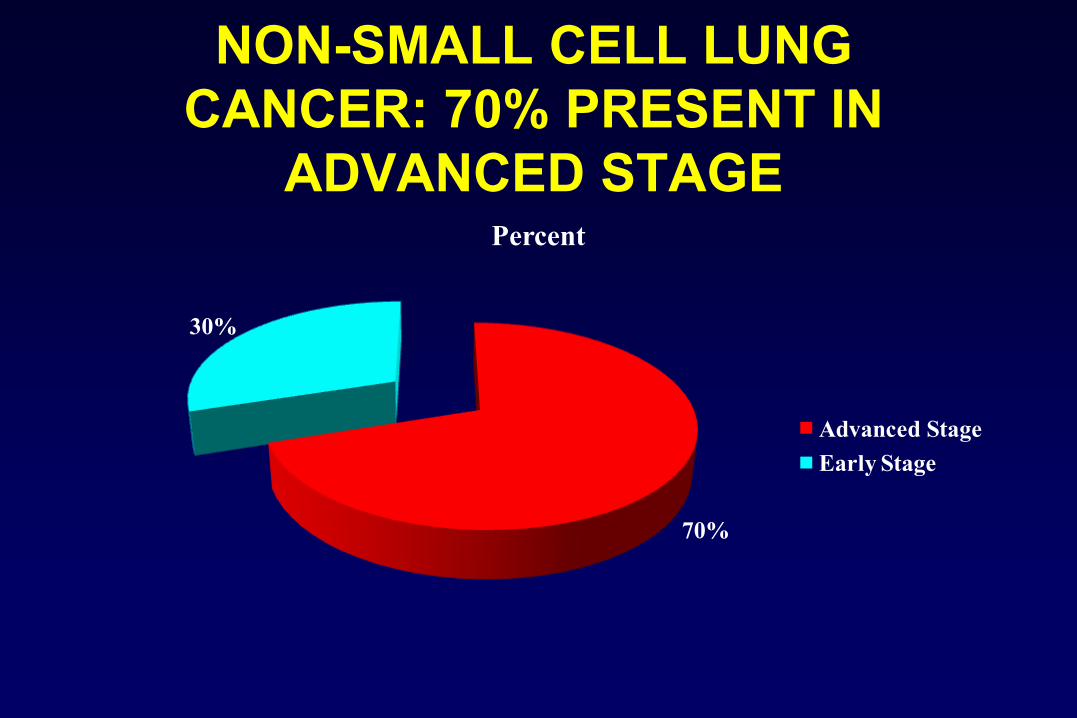
NON-SMALL CELL LUNG CANCER: 70% PRESENT IN
ADVANCED STAGE
70%
30%
Percent
Advanced StageEarly Stage

Results in EGFR mutation positive and negative patients ( All Asian, 94% Never Smokers)
–EGFR mutation positive –EGFR mutation negative
–HR (95% CI) = 0.48 (0.36, 0.64) p<0.0001
–No. events gefitinib: 97No. events Chemo: 111
Gefitinib (n=132)Carboplatin / paclitaxel (n=129)
–HR (95% CI) = 2.85 (2.05, 3.98)p<0.0001
–No. events gefitinib: 88No. events Chemo: 70
–132 –71 –31 –11 –3 –0–129 –37 –7 –2 –1 –0
–108–103
–0 –4 –8 –12 –16 –20 –24
–Gefitinib–C / P
–0.0
–0.2
–0.4
–0.6
–0.8
–1.0
–Pro
babi
lity
of p
rogr
essi
on-fr
ee s
urvi
val
–At risk :–91 –4 –2 –1 –0 –0–85 –14 –1 –0 –0 –0
–21–58
–0 –4 –8 –12 –16 –20 –24–0.
0
–0.2
–0.4
–0.6
–0.8
–1.0
–Pro
babi
lity
of p
rogr
essi
on-fr
ee s
urvi
val
Gefitinib (n=91)Carboplatin / paclitaxel (n=85)
–Months –Months
–Gefitinib CR/PR Rate 71%–CBP/PTX CR/PR Rate 47%
–Gefitinib CR/PR Rate 1%–CBP/PTX CR/PR Rate 24%
–Mok N Engl J Med 361: 947-57, 2009

Initial Therapy of Advanced Adenoca or NSCLC-NOS–Adenocarcinoma–Large cell ca–NSCLC-NOS
–EGFR Mutation–Exon 19 del
–Exon 21 L858R, L861X–Exon 18 G719A/S
–Unknown EGFR
Mutation & ALKStatus
–Neg EGFR mut
–Pos ALK fusion
–Erlotinib/Gefitinib–±
–Pem/Bev/Cis
–Pemetrexed–Bevacizumab–Cisplatin
Modified from Mark Kris, Thoracic Oncology, MSKCC
–Crizotinib
–Neg EGFR mut
–Neg ALK fusion

CLASSIFICATION OF LUNG CANCER NOW REQUIRES GENETIC TESTING
MSK-IMPACT NGD data, 2017 – now includes 468 genesCourtesy of Marc Ladanyi
–Jordan EJ Ca Discovery 7:596-609, 2017

MOLECULAR TARGETED THERAPYTarget Drug
EGFRErlotinibAfatinib
ALK fusions CrizotinibCeritinib, Alectinib
BRAF V600E DabrafenibROS1 fusions Loatinib, CrizotinibRET fusions Cabozantinib
MET splice site Exon 14 mutations
Cabozantinib (and crizotinib)
Courtesy of Greg Riely
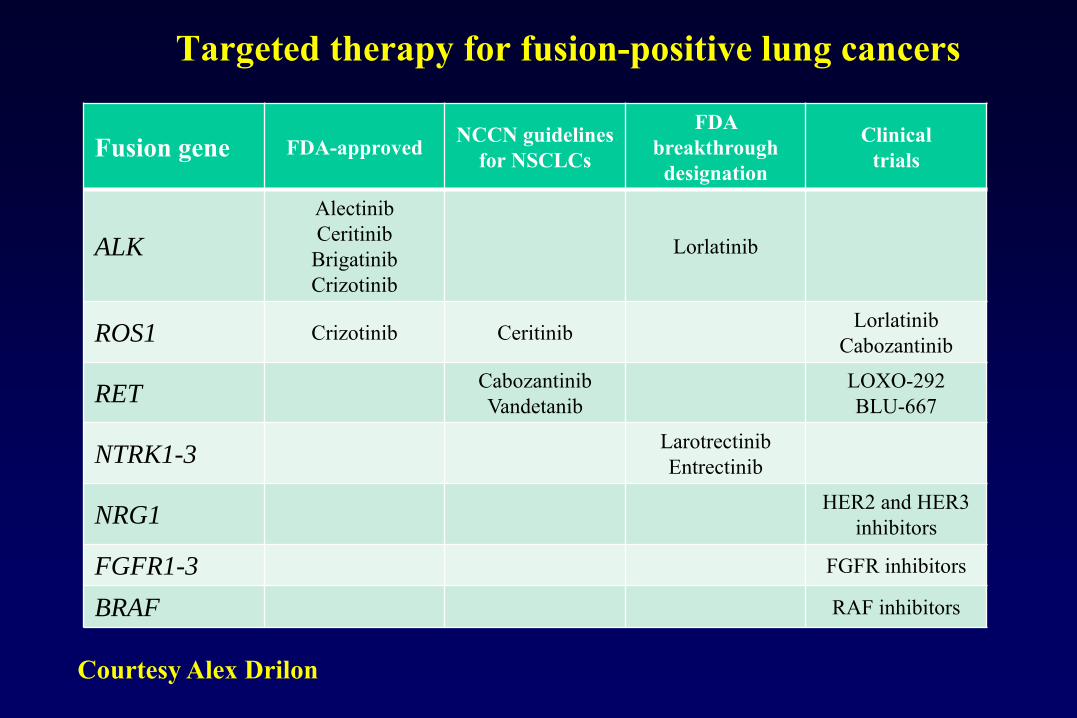
Targeted therapy for fusion-positive lung cancers
Fusion gene FDA-approved NCCN guidelines for NSCLCs
FDA breakthrough
designation
Clinical trials
ALK
AlectinibCeritinib
BrigatinibCrizotinib
Lorlatinib
ROS1 Crizotinib Ceritinib LorlatinibCabozantinib
RETCabozantinibVandetanib
LOXO-292BLU-667
NTRK1-3LarotrectinibEntrectinib
NRG1HER2 and HER3
inhibitors
FGFR1-3 FGFR inhibitors
BRAF RAF inhibitors
Courtesy Alex Drilon

Initial Therapy of Advanced Adenoca or NSCLC-NOS–Adenocarcinoma–Large cell ca–NSCLC-NOS
–EGFR Mutation–Exon 19 del
–Exon 21 L858R, L861X–Exon 18 G719A/S
–Unknown EGFR
Mutation & ALKStatus
–Neg EGFR mut
–Pos ALK fusion
–Erlotinib/Gefitinib–±
–Pem/Bev/Cis
–Pemetrexed–Bevacizumab–Cisplatin
Modified from Mark Kris, Thoracic Oncology, MSKCC
–Crizotinib
–Neg EGFR mut
–Neg ALK fusion
Could add ROS1 fusion, BRAF mutation, RET fusion, MET splice site exon14 mutation to this algorithm

2015 WHO Classification of Lung Tumors
NEW CHAPTER:CLASSIFICATION IN SMALL
BIOPSY AND CYTOLOGY SPECIMENS

SMALL BIOPSY/CYTOLOGY LUNG CANCER DIAGNOSIS: IN USA OVER 139,000 CASES IN 2018
▪ 2018: ACS estimates for USA: • 234,030 Lung Cancers• Sigel RA et al: CA Cancer J Clin 2018:68:7-30
85% NSCLC = 198,926 (15% SCLC)▪ 70% Advanced Stage = 139,248
• Unresectable: Diagnosed by small biopsies/cytology

PHASE III STUDY COMPARING CISPLATIN PLUS GEMCITABINE WITH CISPLATIN &
PEMETREXED IN ADVANCED NSCLC
Scagliotti G, et al: JCO 26:3543-51, 2008
50%
29%
9%
12%
Percent
Adenoca Squamous Ca Large cell Ca NSCLC, NOS

PHASE III STUDY COMPARING CISPLATIN PLUS GEMCITABINE WITH CISPLATIN &
PEMETREXED IN ADVANCED NSCLC
Scagliotti G, et al: JCO 26:3543-51, 2008
50%
29%
9%
12%
Percent
Adenoca Squamous Ca Large cell Ca NSCLC, NOS
–IN THIS STUDY APPROXIMATELY 20% OF CASES REPRESENT NSCLC-NOS
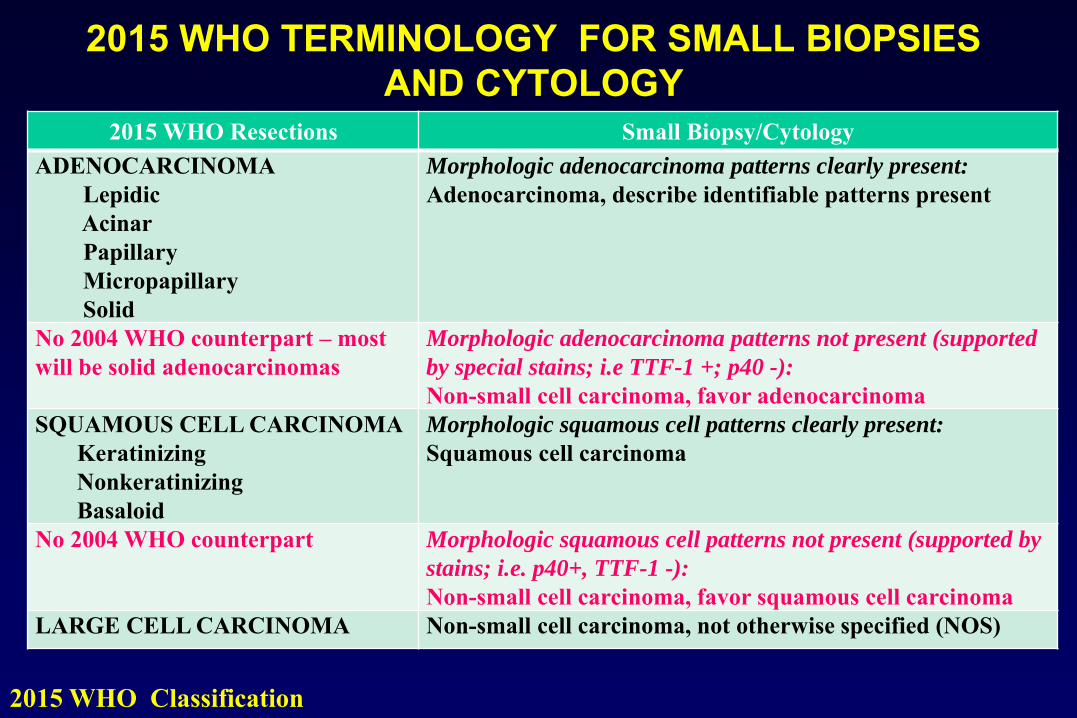
2015 WHO TERMINOLOGY FOR SMALL BIOPSIES AND CYTOLOGY
2015 WHO Resections Small Biopsy/CytologyADENOCARCINOMA
LepidicAcinarPapillaryMicropapillarySolid
Morphologic adenocarcinoma patterns clearly present:
Adenocarcinoma, describe identifiable patterns present
No 2004 WHO counterpart – most will be solid adenocarcinomas
Morphologic adenocarcinoma patterns not present (supported
by special stains; i.e TTF-1 +; p40 -):
Non-small cell carcinoma, favor adenocarcinomaSQUAMOUS CELL CARCINOMA
KeratinizingNonkeratinizingBasaloid
Morphologic squamous cell patterns clearly present:
Squamous cell carcinoma
No 2004 WHO counterpart Morphologic squamous cell patterns not present (supported by
stains; i.e. p40+, TTF-1 -):
Non-small cell carcinoma, favor squamous cell carcinomaLARGE CELL CARCINOMA Non-small cell carcinoma, not otherwise specified (NOS)
2015 WHO Classification
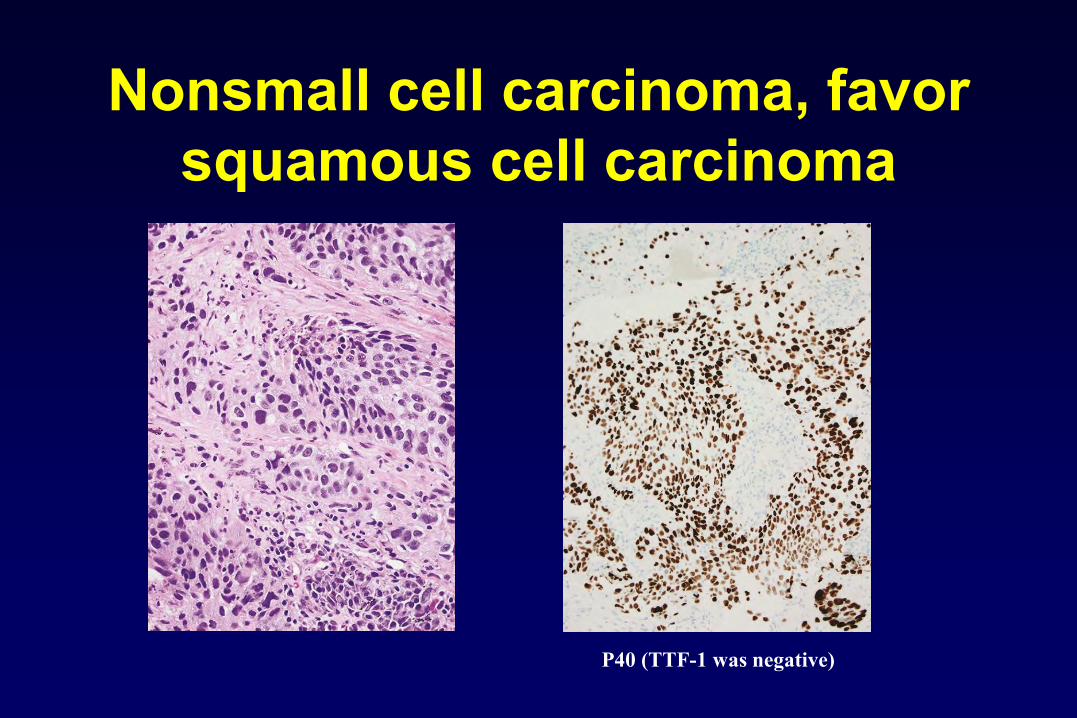
Nonsmall cell carcinoma, favor squamous cell carcinoma
P40 (TTF-1 was negative)

NONSMALL CELL CARCINOMA, FAVOR ADENOCARCINOMA
TTF-1 (p40 was negative)

IMMUNOHISTOCHEMICAL MARKERS
▪ ADENOCARCINOMA (ONE MARKER)• TTF-1 (best), Napsin, PE-10
▪ SQUAMOUS CARCINOMA (ONE MARKER)• p40 (best), p63, CK5/6, 34βE12• Desmocolin-3 (need more testing)
▪ Cocktails – nuclear/cytoplasmic antibodies• Adenoca – TTF-1/Napsin• Squamous – p63/CK5/6
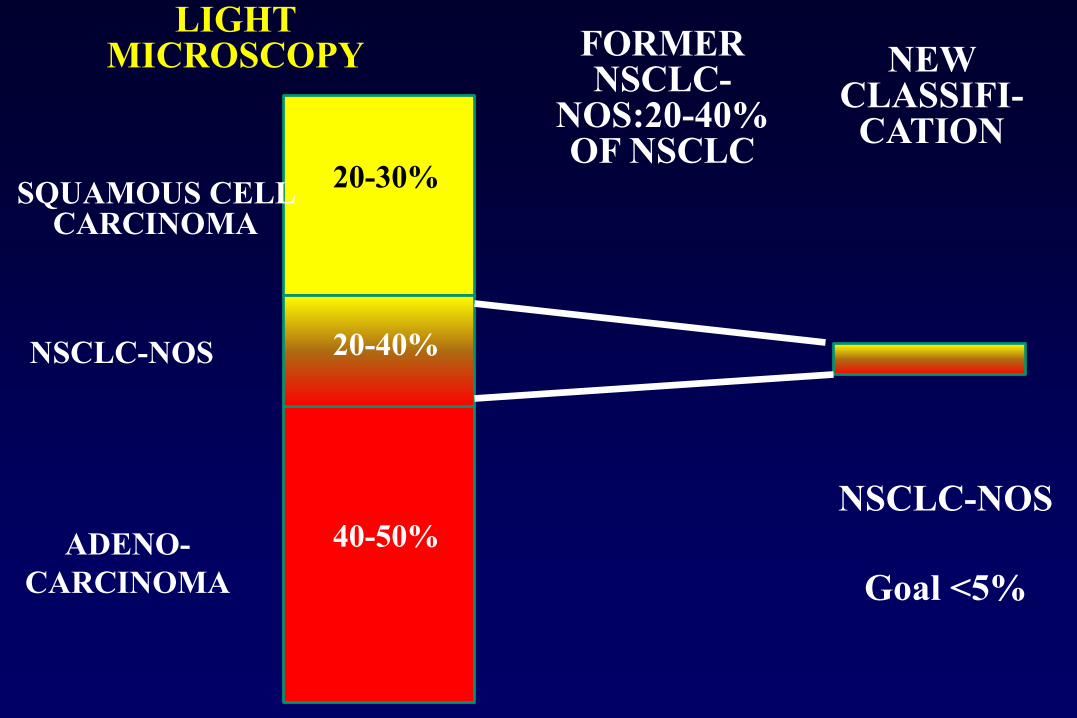
LIGHT MICROSCOPY
ADENO-CARCINOMA
NSCLC-NOS
20-30%
20-40%
40-50%NSCLC-NOS
Goal <5%
FORMER NSCLC-
NOS:20-40% OF NSCLC
SQUAMOUS CELL CARCINOMA
NEW CLASSIFI-
CATION

TISSUE MANAGEMENT▪ Each group of thoracic physicians
(clinicians, radiologists, surgeons, pathologists, molecular biologists) must develop a strategy to manage tissues
▪ Obtaining biopsies or cytology samples▪ Optimal processing by
laboratories/pathologists for diagnosis AND molecular studies
▪ Pathologists are the ideal leader of this
PERSONALIZED MEDICINE IN ADVANCED LUNG CANCER
PATIENTS IS DRIVEN BY HISTOLOGY AND GENETICS
BELLAGIO CENTERROCKEFERLLER
FOUNDATION
WRITINGCOMMITTEE

INCREASING COMPLEXITY▪ 1967 WHO▪ 1981 WHO▪ 1999 WHO▪ 2004 WHO
▪ 2015 WHO
▪ H&E▪ H&E & Mucin▪ H&E, EM & IHC▪ H&E, EM, IHC &
Genetics▪ H&E, Cytology, IHC,
Genetics, Mucin, Radiology
INCREASING RELEVANCE FORPERSONALIZED MEDICINE
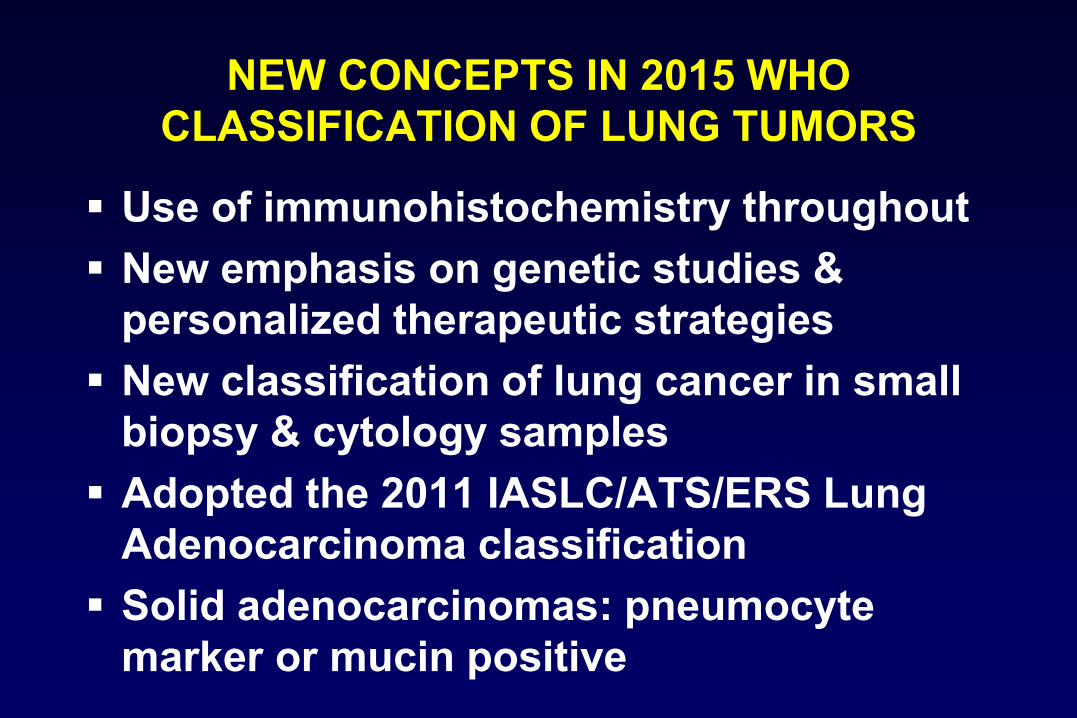
NEW CONCEPTS IN 2015 WHO CLASSIFICATION OF LUNG TUMORS
▪ Use of immunohistochemistry throughout▪ New emphasis on genetic studies &
personalized therapeutic strategies▪ New classification of lung cancer in small
biopsy & cytology samples▪ Adopted the 2011 IASLC/ATS/ERS Lung
Adenocarcinoma classification▪ Solid adenocarcinomas: pneumocyte
marker or mucin positive

▪ Restrict large cell carcinoma to tumors lacking clear differentiation by both IHC and morphology
▪ Reclassify squamous cell ca: keratinizing, nonkeratinizing and basaloid
▪ Diagnosis of nonkeratinizing squamous cell carcinoma requires IHC (p40+, TTF1-)
▪ Group NE tumors together (TC,AC, LCNEC, SCLC)
NEW CONCEPTS IN 2015 WHO CLASSIFICATION OF LUNG TUMORS
LARGE CELL CARCINOMA
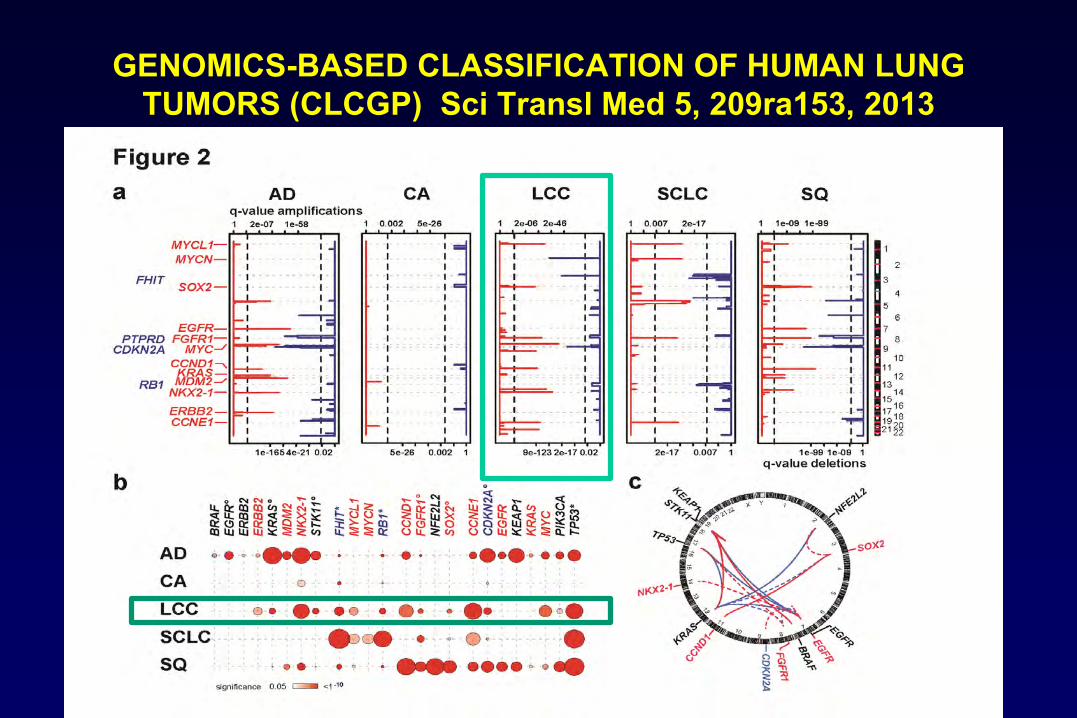
GENOMICS-BASED CLASSIFICATION OF HUMAN LUNG TUMORS (CLCGP) Sci Transl Med 5, 209ra153, 2013

SEER DATA BY HISTOLOGIC TYPE: RATES PER 100,000 PY
–Lewis D et al; Cancer 2014; 120: 2883-92

LARGE CELL CARCINOMA1999 & 2004 WHO Classification
▪ Large cell carcinoma▪ Large cell neuroendocrine carcinoma• Combined LCNEC
▪ Basaloid carcinoma▪ Lymphoepithelioma-like carcinoma▪ Clear cell carcinoma▪ Large cell carcinoma with rhabdoid
phenotype
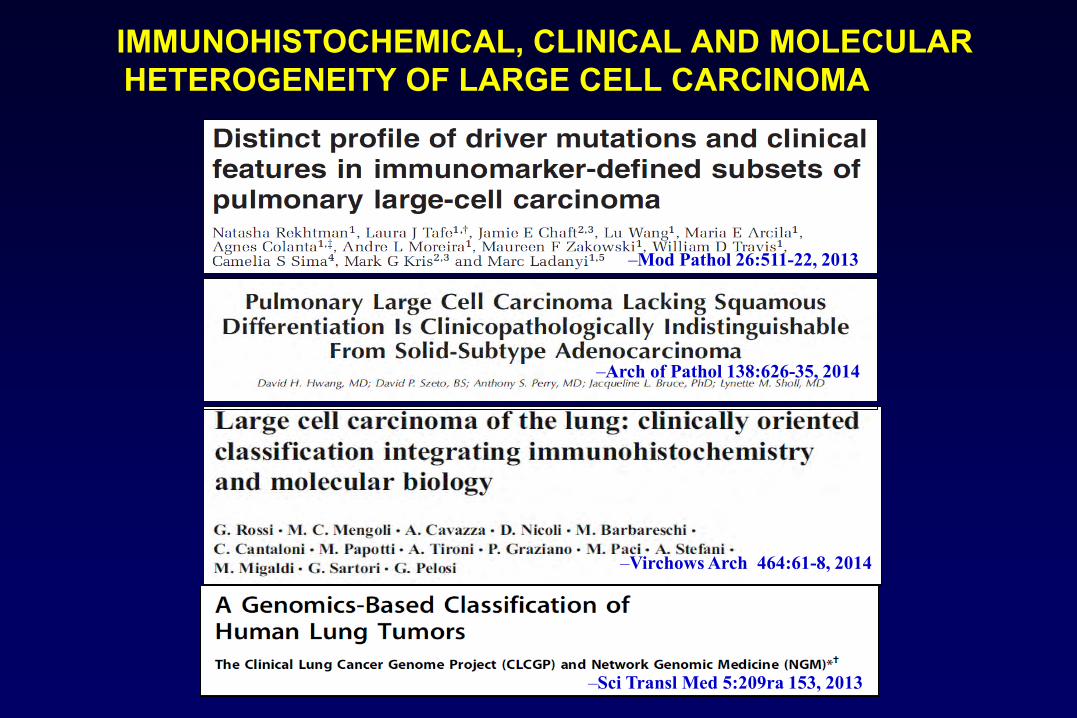
IMMUNOHISTOCHEMICAL, CLINICAL AND MOLECULAR HETEROGENEITY OF LARGE CELL CARCINOMA
–Virchows Arch 464:61-8, 2014
–Mod Pathol 26:511-22, 2013
–Arch of Pathol 138:626-35, 2014
–Sci Transl Med 5:209ra 153, 2013

–Rekhtman et al Mod Pathol 26:511-22, 2013
DISTRIBUTION OF MUTATIONS AND IMMUNOMARKER DEFINED TYPES OF LARGE CELL CARCINOMA

2015 WHO CLASSIFICATION: WHERE WILL THE LARGE CELL CARCINOMAS GO?
▪ Pneumocyte marker (TTF-1) positive LCC solid adenoca
▪ Squamous marker positive (p40) LCC nonkeratinizing squamous cell ca
▪ Large cell neuroendocrine carcinoma• Combined LCNEC NE tumors
▪ Basaloid carcinoma Squamous ca
2015 WHO CLASSIFICATION: WHERE WILL THE LARGE CELL CARCINOMAS GO?
▪ Lymphoepithelioma-like carcinoma Other carcinomas
▪ Clear cell carcinoma (Cytologic pattern not subtype)
▪ Large cell carcinoma with rhabdoid phenotype (Cytologic pattern not subtype)

LARGE CELL CARCINOMA2015 WHO Classification
▪ Large cell carcinoma with null immunohistochemical features and no mucin
▪ Large cell carcinoma with unclear immunohistochemical features
▪ Large cell carcinoma with no stains available

PSEUDOSQUAMOUS SOLID ADENOCARCINOMA
TTF-1 Mucicarmine
EGFR Exon 19 Deletion

PSEUDOKERATINIZING ADENOCARCINOMA
TTF-1 p40

2015 WHO CLASSIFICATION SQUAMOUS CELL CARCINOMA
▪ Keratinizing
▪ Non-keratinizing
▪ Basaloid carcinoma
now need IHC –P40 positive,
TTF-1 negative
now need IHC –(+p40, -TTF1 & NE markers) r/o
LCNEC & SCLC

52%
40%
8%
NK SqC 86%
LCNEC 1%
Adenoca7%
Adc 4%
LCC 2%
K SqC 99.6%
AdSq 0.4%
SCLC & LCNEC 5% each
B Sq 90%
–Kadota K et al; AJSP 39:1170-80, 2015
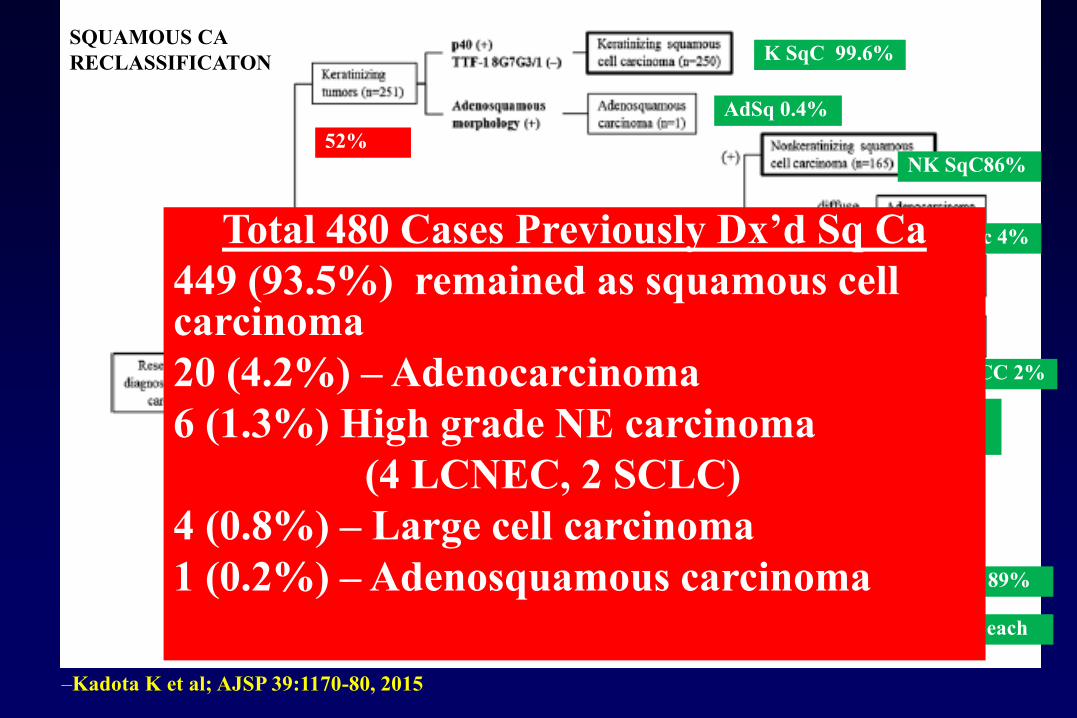
SQUAMOUS CARECLASSIFICATON
Two TTF-1 Abs–8G7G3 – more specific–SPT24 – more sensitive, less specific
52%
40%
8%
NK SqC86%
LCNEC 1%
Adenoca7%
Adc 4%
LCC 2%
K SqC 99.6%
AdSq 0.4%
SCLC & LCNEC 5% each
B Sq 89%
SQUAMOUS CARECLASSIFICATON
Total 480 Cases Previously Dx’d Sq Ca449 (93.5%) remained as squamous cell carcinoma20 (4.2%) – Adenocarcinoma6 (1.3%) High grade NE carcinoma
(4 LCNEC, 2 SCLC)4 (0.8%) – Large cell carcinoma1 (0.2%) – Adenosquamous carcinoma
–Kadota K et al; AJSP 39:1170-80, 2015

KEY ISSUESSQUAMOUS CELL CARCINOMA
▪ Tumor budding and tumor nest size are the most significant histologic prognostic factors
▪ Histologic subtyping (keratinizing, nonkeratinizing, basaloid) not clearly prognostically important

SQUAMOUS CELL CARCINOMATUMOR BUDDING AND NEST SIZE
SINGLE CELL INVASION
TUMOR BUDDING AND NEST SIZE < 5 CELLS
Kadota K et al: JTO 9:1126-39, 2014
Maeshima AM: Lung Ca 52:53-58, 2006Masuda R: Mol Med Rep 6:937-43, 2012Taira T: Lung Ca 76:423-30, 2012Weichert W et al; ERJ 47:938-46, 2015Zhao Y: Medicine 94:e1634, 2015Kadota K: AJSP 41: 750-60, 2017
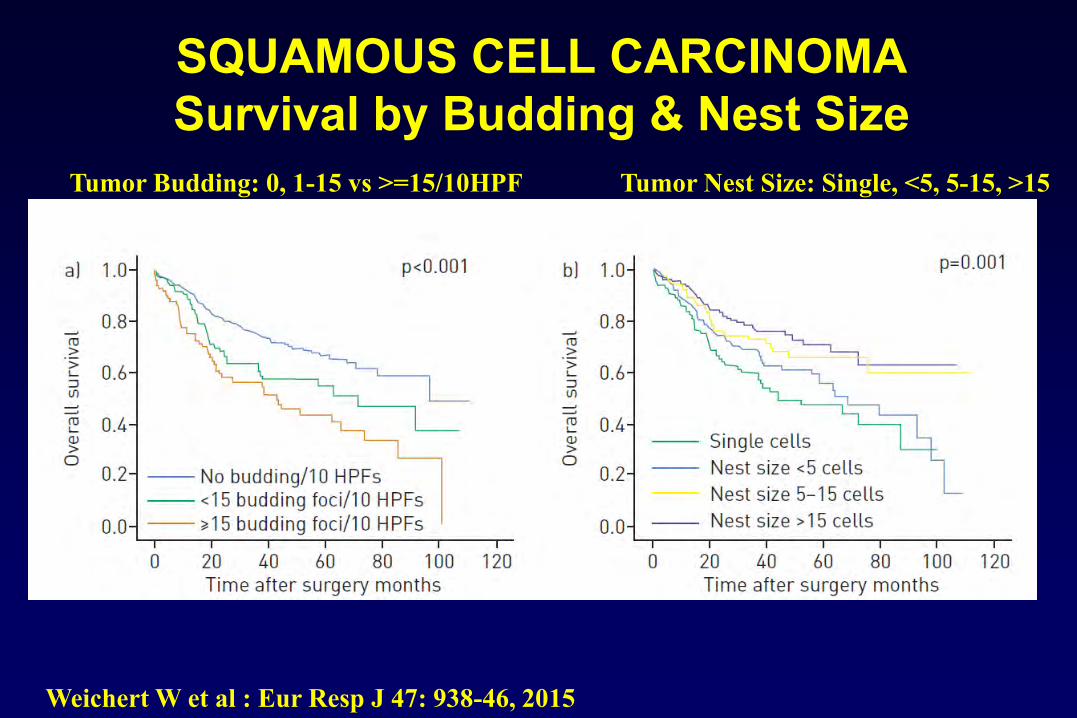
SQUAMOUS CELL CARCINOMASurvival by Budding & Nest Size
Weichert W et al : Eur Resp J 47: 938-46, 2015
Tumor Budding: 0, 1-15 vs >=15/10HPF Tumor Nest Size: Single, <5, 5-15, >15

SUMMARY▪ 2015 WHO Classification provides diagnostic
criteria and terminology to be used in small bxand cytology
▪ Need strategic approach to use of small specimens not only for diagnosis but for molecular testing
▪ Rapidly evolving field requires following new technology (IHC, molecular)
▪ Need multidisciplinary team▪ Large cell carcinoma – largely reclassified▪ Squamous cell ca – tumor budding/nest size is
prognostic

Related Documents











