9 Advances in alcoholic liver disease Gavin Arteel PhD Assistant Professor of Pharmacology and Toxicology University of Louisville Medical Center, Building A, Room 1319, Louisville, KY 40292, USA Luis Marsano MD Professor of Internal Medicine Christian Mendez MD Fellow in Gastroenterology Department of Internal Medicine, University of Louisville Medical Center, 550 S. Jackson Street, ACB 3rd Floor, Louisville, KY 40292, USA Frederick Bentley MD Associate Professor of Surgery University of Louisville Medical Center, 550 S. Jackson Street, ACB 3rd Floor, Louisville, KY 40292, USA Craig J. McClain * MD Vice Chair for Research, Professor of Internal Medicine, Pharmacology and Toxicology Department of Internal Medicine, University of Louisville Medical Center, 550 S. Jackson Street, ACB 3rd Floor, Louisville, KY 40292, USA Alcoholic liver disease (ALD) remains a major cause of morbidity and mortality worldwide. For example, the Veterans Administration Cooperative Studies reported that patients with cirrhosis and superimposed alcoholic hepatitis had a 4-year mortality of . 60%. Interactions between acetaldehyde, reactive oxygen and nitrogen species, inflammatory mediators and genetic factors appear to play prominent roles in the development of ALD. The cornerstone of therapy for ALD is lifestyle modification, including drinking and smoking cessation and losing weight, if appropriate. Nutrition intervention has been shown to play a positive role on both an inpatient and outpatient basis. Corticosteroids are effective in selected patients with alcoholic hepatitis and pentoxifylline appears to be a promising anti-inflammatory therapy. Some complementary and alternative medicine agents, such as milk thistle and S-adenosylmethionine, may be effective in alcoholic cirrhosis. Treatment of the complications of ALD can improve quality of life and, in some cases, decrease short-term mortality. Key words: alcoholic liver disease; diagnosis; aetiology; treatment. 1521-6918/03/$ - see front matter Published by Elsevier Science Ltd. Best Practice & Research Clinical Gastroenterology Vol. 17, No. 4, pp. 625–647, 2003 doi:10.1053/ybega.2003.400, www.elsevier.com/locate/jnlabr/ybega * Corresponding author. Tel.: þ1-502-852-6991; Fax: þ1-502-852-0846. E-mail address: [email protected] (C. J. McClain).

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

9
Advances in alcoholic liver disease
Gavin Arteel PhD
Assistant Professor of Pharmacology and Toxicology
University of Louisville Medical Center, Building A, Room 1319, Louisville, KY 40292, USA
Luis Marsano MD
Professor of Internal Medicine
Christian Mendez MD
Fellow in Gastroenterology
Department of Internal Medicine, University of Louisville Medical Center, 550 S. Jackson Street, ACB 3rd Floor,
Louisville, KY 40292, USA
Frederick Bentley MD
Associate Professor of Surgery
University of Louisville Medical Center, 550 S. Jackson Street, ACB 3rd Floor, Louisville, KY 40292, USA
Craig J. McClain* MD
Vice Chair for Research, Professor of Internal Medicine, Pharmacology and Toxicology
Department of Internal Medicine, University of Louisville Medical Center, 550 S. Jackson Street, ACB 3rd Floor,
Louisville, KY 40292, USA
Alcoholic liver disease (ALD) remains a major cause of morbidity and mortality worldwide. Forexample, the Veterans Administration Cooperative Studies reported that patients with cirrhosisand superimposed alcoholic hepatitis had a 4-year mortality of .60%. Interactions betweenacetaldehyde, reactive oxygen and nitrogen species, inflammatory mediators and genetic factorsappear to play prominent roles in the development of ALD. The cornerstone of therapy for ALDis lifestyle modification, including drinking and smoking cessation and losing weight, if appropriate.Nutrition intervention has been shown to play a positive role on both an inpatient and outpatientbasis. Corticosteroids are effective in selected patients with alcoholic hepatitis and pentoxifyllineappears to be a promising anti-inflammatory therapy. Some complementary and alternativemedicine agents, such as milk thistle and S-adenosylmethionine, may be effective in alcoholiccirrhosis. Treatment of the complications of ALD can improve quality of life and, in some cases,decrease short-term mortality.
Key words: alcoholic liver disease; diagnosis; aetiology; treatment.
1521-6918/03/$ - see front matter Published by Elsevier Science Ltd.
Best Practice & Research Clinical GastroenterologyVol. 17, No. 4, pp. 625–647, 2003doi:10.1053/ybega.2003.400, www.elsevier.com/locate/jnlabr/ybega
* Corresponding author. Tel.: þ1-502-852-6991; Fax: þ1-502-852-0846.E-mail address: [email protected] (C. J. McClain).

In Western countries, up to 50% of cases of end-stage liver disease have alcohol as a mainaetiological factor.1 In the USA, end-stage liver disease is the 9th leading cause of death.Between 1978 and 1988, alcohol was responsible for 44% of the deaths from cirrhosis inthe USA.2 The mortality from alcoholic cirrhosis is higher than that of non-alcoholiccirrhosis and the survival rate at 5 and 10 years is only 23 and 7%, respectively, in somestudies.3 Thus, the mortality of this liver disease is more than that of many major forms ofcancer, such as breast, colon and prostate.4 This chapter will review three major aspectsof alcoholic liver disease (ALD): (i) diagnosis, (ii) aetiology and (iii) treatment.
DIAGNOSIS OF ALD
Risk factors
In order to develop liver disease, a ‘threshold’ regarding daily amount and length of timeof alcohol intake has to be exceeded. Daily intake of alcohol for 10–12 years with dosesin excess of 40–80 g/day for males and of 20–40 g/day for females are generally neededto cause ALD.5–8 Because alcoholic beverages have different alcohol content, it isimportant to convert ‘usual serving’ sizes to g of alcohol. Thus, 12 oz of beer (5% v/valcohol) provides 13.85 g of alcohol versus 4 oz of wine (12% v/v alcohol), whichprovides 10.7 g, whereas 2 oz of fortified wine (20% v/v alcohol) and 1 oz of ‘spirits’(40% v/v alcohol) provide 8.9 g of alcohol each. Thus, daily drinking of 3–6 cans (12 ozeach) of beer/day for males or 1.5–3 cans of beer/day for females for 10 years or longercan cause ALD.
Despite the need for a threshold with respect to dose and length of time for thedevelopment of ALD, there is not a particular amount of alcohol that will predictablycause ALD. Among heavy, long-term alcohol drinkers, 90–100% develop fatty liver butonly 10–35% develop alcoholic hepatitis and 8–20% will develop alcoholic cirrhosis.9
Thus, alcohol probably works as a ‘potential hepatotoxin’, with the development ofliver disease depending on the balance of host attributes and co-existing externalfactors, such as gender, polymorphism of alcohol-metabolizing enzymes, immunologicalfactors, exposures to other substances/drugs, hepatic viral infections, nutritionaldeficiencies, obesity, etc.
Diagnosis
The diagnosis of ALD is established with a history of habitual alcohol intake of sufficientlength and intensity together with physical signs and/or laboratory evidence of liverdisease. The diagnosis can be made difficult because patients frequently minimize ordeny alcohol abuse. In addition, physical examination findings may be absent andlaboratory abnormalities may be non-specific.10–12 The severity of injury spans thespectrum, from fatty liver (steatosis) to steatohepatitis to cirrhosis. Cirrhosis andsteatohepatitis often co-exist. The tool most frequently used to assess alcoholdependency is the CAGE questionnaire, which explores the lifetime occurrence of, orneed for, Cutting down on drinking, Annoyance when others express concern about theamount of drinking, Guilt about drinking and need of alcohol as an Eye opener. Twopositive answers indicate alcohol dependency with a sensitivity of more than 70% andspecificity of more than 90%.13,14 An important caveat is that alcohol dependency is nota pre-requirement for the development of ALD because some people are exquisitelysensitive to the effects of alcohol.
626 G. Arteel et al

Ambulatory patients with alcoholic fatty liver are usually asymptomatic15 but 70% ofhospitalized patients with steatosis have hepatomegaly and one-third have laboratoryabnormalities.16 Patients with alcoholic steatohepatitis may be asymptomatic, have onlyhepatomegaly, or have a full-blown picture of alcoholic hepatitis with tenderhepatomegaly, jaundice, fever, ascites, hepatic encephalopathy, anorexia, malaise andeven leukaemoid reactions and hepatorenal syndrome. Portal hypertension may bepresent, even in the absence of cirrhosis. Once a patient has alcoholic hepatitis, theprobability of developing cirrhosis is 10–20% per year, and up to 70% will eventuallydevelop cirrhosis.17 The patients at higher risk for the development of cirrhosis arethose who continue drinking, have severe alcoholic hepatitis and who are female.18
Some patients who abstain may still develop cirrhosis, but others will have completeclinical and histological recovery. We do not know if, in older studies, other poorly-recognized liver disorders at that time (hepatitis C, non-alcoholic fatty liver disease,etc) were contributing factors in the patients who had progressive liver disease despitealcohol abstinence.
Patients with well-compensated alcoholic cirrhosis may be asymptomatic and havenormal physical examinations. Alcoholic steatosis or steatohepatitis are often co-existent and the patient may have hepatomegaly and/or splenomegaly. In thosecirrhotics with severe alcoholic hepatitis, hepatomegaly and/or splenomegaly maydominate the clinical features; in other patients, the signs and symptoms of portalhypertension may dominate. As the disease advances, the liver decreases in size, the lefthepatic lobe becomes more prominent and the entire liver has a hard and nodularconsistency. Splenomegaly of varying degree is frequent. In decompensated disease,patients have muscle wasting, ascites and venous collateral circulation. Spiderangiomata, palmar erythema and Dupuytren’s palmar contractures are common.Parotid and lacrimal gland enlargement is often seen. Some patients with severehypoalbuminaemia have Muercke’s nails or have white nails. Clubbing of the fingers maybe found in patients who have meaningful arterio-venous pulmonary shunting.Oesophageal varices, gastric varices and portal hypertensive gastropathy are frequentlyfound during endoscopy. When hepatic encephalopathy is present, patients have slowreaction time and may have asterixis. None of the physical signs and symptoms arepathognomonic for ALD.
Laboratory data
For habitual alcohol consumption (more than 50 g/day with liver injury), aspartatetransaminase (AST) is more sensitive (50% sensitivity) than alanise transaminase (ALT)(35% sensitivity) but ALT elevation is a little more specific (86% specificity) than ASTelevation (82% specificity).19 Almost all patients will have elevation of AST .ALTwithboth below 300 IU/ml.20–22 When the AST:ALT ratio is greater than two, the mostlikely diagnosis is ALD; in some studies, more than 80% of patients reach this ratio.23,24
Elevation of g glutamyltransferase (GGT) is more sensitive (70%) but less specific(65–80%) than elevation of AST or ALT for excessive alcohol consumption. BecauseGGT is ubiquitous in many organs and drugs that induce the microsomal enzymes causeGGTelevation, the specificity of GGTelevation is limited. In addition, GGT is increasedin most forms of liver injury. Because alcohol causes mitochondrial damage,mitochondrial AST (mAST) is a very sensitive marker of alcohol consumption.However, this test is not routinely used in clinical care.
Chronic alcohol consumption is also often associated with hypertriglyceridaemia,hyperurecaemia, hypokalaemia and hypomagnesaemia, as well as elevated mean
Advances in alcoholic liver disease 627
corpuscular erythrocyte volume (MCV).25 Hyperuricaemia and hypertriglyceridaemiaoften normalize with abstinence and hypokalaemia normalizes with adequatereplacement. Elevated MCV is often found in persons ingesting more than 50 gmalcohol/day, with a sensitivity of 27–52% and specificity of 85–90%.14,19,26
Carbohydrate-deficient transferrin is frequently used to detect current or recentalcohol abuse, especially in excess of 60 g/day.27,28 However, there are no ideal tests toidentify continuing ethanol intake.
Leukocytosis and thrombocytopaenia are common in alcoholic hepatitis. Occasion-ally patients have leukaemoid reactions with counts of 100 000 white blood cells(WBC)/mm3 in the absence of infection. Thrombocytopaenia may be transitory, but inpatients with concomitant cirrhosis, it is persistent. Elevation of bilirubin, prolongationof prothrombin time (PT) and hypoalbuminaemia are markers of severe alcoholichepatitis and/or cirrhosis. The most commonly used prognostic index in alcoholichepatitis is the ‘Maddrey’s Discriminant Function’, which is calculated using theequation: 4.6 £ (PT patient 2 PT control) þ total bilirubin (mg/dl). If this value exceeds32, the mortality during the current hospitalization is in excess of 50%.29,30 There is alsoevidence that serum concentrations of tumour necrosis factor-a (TNF-a), interleukin-6 (IL-6) and interleukin-8 (IL-8) correlate with mortality in patients with alcoholichepatitis31, but levels of these cytokines are not used in routine clinical practice.
Histology
Clinical diagnosis of ALD is sensitive (91%) and specific (96%) with a positive predictivevalue of 88% and negative predictive rate of 97%, at least in an educated population.32 Inanother study, clinical diagnosis was 79% sensitive but 98% specific.33 Because clinicaldiagnosis is very specific and has a high positive predictive value, liver biopsy is rarelyused just to establish the diagnosis. Its main use is to clarify atypical cases, to betterdefine the alcohol contribution in patients with possible co-existing conditions and tostage the severity of liver disease.
Most persons who habitually drink more than 60 g/day of alcohol will develop fattyliver in the centrilobular or perivenular region. Subjects who have severe mixedmicro/macrovesicular pattern, and/or giant mitochondria are more likely to developfibrosis and evolve to cirrhosis.34,35
Alcoholic hepatitis is characterized by ballooning degeneration of hepatocytes withpolymorphonuclear cell infiltration (97%), moderate to severe fatty infiltration (82%),Mallory bodies (76%), sclerosing hyaline necrosis (68%) and increased fibrosis (54%) withperivenular fibrosis (19%).36 Of interest, in contrast with alcoholic fatty liver, thepresence of megamitochondria in alcoholic hepatitis appears to improve its prognosis.37
Alcoholic cirrhosis is usually micronodular (less often mixed micro- and macro-nodular). If the patient has co-existing alcoholic hepatitis, Mallory bodies are almostuniversal (95%), while sclerosing hyaline necrosis and moderate to severe fattyinfiltration are common (44 and 43%, respectively).36
Practice points
† ALD ranges from steatosis to steatohepatitis to cirrhosis† AST . ALT is important in diagnosis and an AST:ALT .2 is highly suggestive
of ALD
628 G. Arteel et al
MECHANISMS OF LIVER INJURY
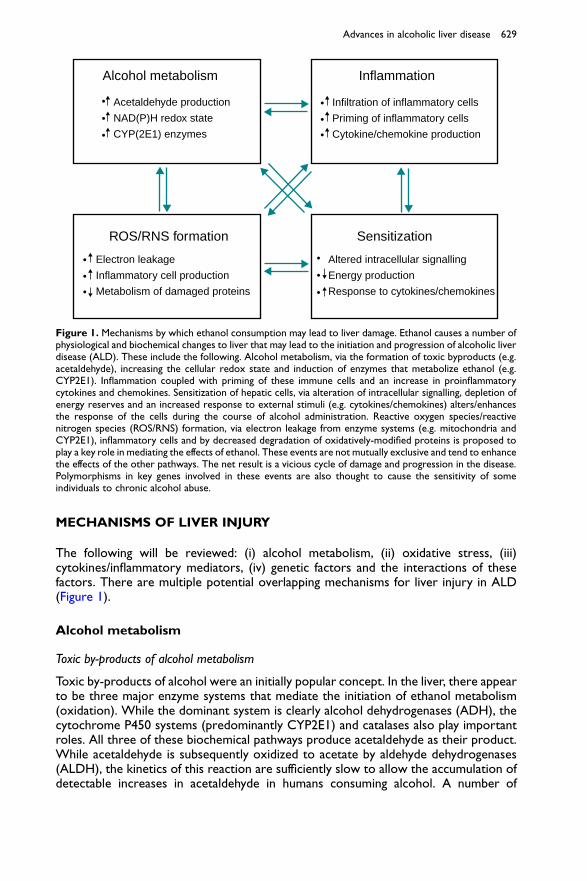
The following will be reviewed: (i) alcohol metabolism, (ii) oxidative stress, (iii)cytokines/inflammatory mediators, (iv) genetic factors and the interactions of thesefactors. There are multiple potential overlapping mechanisms for liver injury in ALD(Figure 1).
Alcohol metabolism
Toxic by-products of alcohol metabolism
Toxic by-products of alcohol were an initially popular concept. In the liver, there appearto be three major enzyme systems that mediate the initiation of ethanol metabolism(oxidation). While the dominant system is clearly alcohol dehydrogenases (ADH), thecytochrome P450 systems (predominantly CYP2E1) and catalases also play importantroles. All three of these biochemical pathways produce acetaldehyde as their product.While acetaldehyde is subsequently oxidized to acetate by aldehyde dehydrogenases(ALDH), the kinetics of this reaction are sufficiently slow to allow the accumulation ofdetectable increases in acetaldehyde in humans consuming alcohol. A number of
Alcohol metabolism
ROS/RNS formation Sensitization
Inflammation
Acetaldehyde production
NAD(P)H redox state
CYP(2E1) enzymes
Electron leakage
Inflammatory cell production
Metabolism of damaged proteins
Altered intracellular signalling
Energy production
Response to cytokines/chemokines
Infiltration of inflammatory cells
Priming of inflammatory cells
Cytokine/chemokine production
Figure 1. Mechanisms by which ethanol consumption may lead to liver damage. Ethanol causes a number ofphysiological and biochemical changes to liver that may lead to the initiation and progression of alcoholic liverdisease (ALD). These include the following. Alcohol metabolism, via the formation of toxic byproducts (e.g.acetaldehyde), increasing the cellular redox state and induction of enzymes that metabolize ethanol (e.g.CYP2E1). Inflammation coupled with priming of these immune cells and an increase in proinflammatorycytokines and chemokines. Sensitization of hepatic cells, via alteration of intracellular signalling, depletion ofenergy reserves and an increased response to external stimuli (e.g. cytokines/chemokines) alters/enhancesthe response of the cells during the course of alcohol administration. Reactive oxygen species/reactivenitrogen species (ROS/RNS) formation, via electron leakage from enzyme systems (e.g. mitochondria andCYP2E1), inflammatory cells and by decreased degradation of oxidatively-modified proteins is proposed toplay a key role in mediating the effects of ethanol. These events are not mutually exclusive and tend to enhancethe effects of the other pathways. The net result is a vicious cycle of damage and progression in the disease.Polymorphisms in key genes involved in these events are also thought to cause the sensitivity of someindividuals to chronic alcohol abuse.
Advances in alcoholic liver disease 629
the systemic toxic effects of ethanol abuse (e.g. flushing, headaches and nausea) aremediated, at least in part, by the direct or indirect effects of elevated acetaldehydelevels. At the more local level, it is proposed that acetaldehyde may also play anaetiological role in ALD.38 For example, acetaldehyde can form adducts with reactiveresidues on proteins or small molecules (e.g. cysteines). These chemical modificationscan alter and/or interfere with normal biological processes and be directly toxic to thecell. Modified biological molecules may also stimulate the host’s immune response andcause an autoimmune-like disease. Antibodies against such oxidatively modifiedproteins have been reported in both humans and animal models of ALD.39,40 Forexample, a hybrid adduct of malondialdehyde and acetaldehyde (MMA) unique toalcohol exposure has been shown to induce an immune response both in humanalcoholics and in animal models of ALD.41
An indirect mechanism by which alcohol metabolism may contribute to ALD is theinduction of the cytochrome P450, CYP2E1. The co-localization of CYP2E1 in thehepatic lobule regions of liver damage after alcohol consumption led to the hypothesisthat CYP2E1 plays a causal role in ALD. Inhibitors of CYP2E1 partially blocked hepaticpathology caused by ethanol in animal models42, supporting this hypothesis. While themechanism(s) by which CYP2E1 induction may play a role in ALD are unclear, it isproposed that this enzyme is a source of oxidative stress (see below). For example,CYP2E1 has been shown to be loosely coupled with cytochrome reductase, leakingelectrons to oxygen to form O2
z2 or to catalyze lipid peroxidation.43 However, sincecultured hepatocytes have relatively low CYP2E1 activity, these questions were difficultto evaluate in the intact cell. To address this problem, HepG2 cells that overexpressCYP2E1 were developed. The work to date with these cells has supported thehypothesis that CYP2E1 is involved in hepatocyte damage due to alcohol.44 However,mice lacking CYP2E1 developed liver injury analogous to their wild-type counter-parts.45 It has been suggested that other isoforms of CYP (e.g. CYP4A) may play acompensatory role in the initiation of early alcohol-induced liver injury in the absenceof CYP2E1 in the knockouts.46 Nevertheless, it appears that CYP2E1 is not required forthe initiation of alcohol-induced liver injury in mice. This observation does not precludea role for CYP2E1 in later stages of disease progression in mice or in other species.Much work remains to be done to address these issues.
Biochemical effects of alcohol metabolism
In addition to forming cytotoxic byproducts, ethanol metabolism can alter the cellularredox state, which can indirectly be involved in liver damage. Specifically, the oxidationof ethanol to acetaldehyde by ADH and its subsequent oxidation to acetate by ALDHutilizes NADþ as an electron acceptor, causing a shift in the NADH:NADþ ratio to amore reduced state. This change in the redox state can impair normal carbohydrate andlipid metabolism, which has multiple effects, including decreasing the supply of ATP tothe cell.47 The increase in the reduced state of pyridine nucleotides has also beenproposed as being involved in the accumulation of lipids during alcohol ingestion(steatosis), which appears to be critical for the progression to more severe damage inthe disease.48
Oxidative stress
Reactive oxygen and nitrogen intermediates (ROS and RNS, respectively) can beproducts of normal cellular metabolism and have beneficial effects (e.g. cytotoxicity
630 G. Arteel et al
against invading bacteria). However, since these molecules also have the potential todamage normal tissue, the balance between pro-oxidants and antioxidants is critical forthe survival and function of aerobic organisms. If the balance is tipped in favour ofoverproduction of these species, oxidative stress can occur. Oxidative stress has beenproposed to be critically involved in ALD.49,50 Oxidative stress associated with clinicalALD is most probably not due to an increase in pro-oxidant formation alone.Alcoholics replace up to 50% of their total daily calories with ethanol51, leading tonutritional deficiencies that can be further complicated by nutrient malabsorption.52
The net effect is that alcoholics often have lower levels of key dietary antioxidantmolecules (see Lieber47 for a review) and a decreased overall antioxidant status.Therefore, oxidative stress in ALD is most probably mediated by both an increase inpro-oxidant production and a decrease in antioxidant defences.
In support of the hypothesis that oxidative stress is involved in ALD, numerousantioxidants have been shown to protect against the damaging effects of ethanol inboth in vitro and in vivo models of ALD.53–55 Although important advances have beenmade in understanding the role of pro-oxidants in experimental alcohol-induced liverinjury, this work has yet to translate into an accepted antioxidant therapy for ALD.With a better understanding of the mechanisms by which oxidative stress leads toliver damage during alcohol exposure, antioxidant therapies that are targeted to thespecific cellular/molecular effects of ethanol may be applied in the clinic withpotentially greater success.
ROS: a role for superoxide
Superoxide (O2z2) can come from many sources within the cell, including direct
production from enzymes (e.g. xanthine oxidase and NA(D)PH oxidases), as well aselectron leakage from enzyme systems not specifically designed to produce the radical(e.g. mitochondria and CYP2E1). Support for the role of O2
z2 in ALD comespredominantly from correlations between injury and levels of superoxide dismutase(SOD), an enzyme that catalytically reduces O2
z2 to hydrogen peroxide (H2O2).56
For example, levels of SOD correlated inversely with pathological changes in theenteral alcohol model of experimental ALD.57 Furthermore, exogenous SOD hasshown protective/antioxidant effects in both in vitro and in vivo models of alcoholexposure. Furthermore, gene delivery of either cytosolic Cu/Zn-SOD or mitochondrialMn-SOD by adenoviral vectors has also been shown to prevent alcohol-induced liverinjury in rats in the enteral model of alcohol injury.58,59 While there is clear experimentalevidence that pro-oxidant formation is dependent on the production of O2
z2, this radicalis itself not a potent oxidant. O2
z2 can alternatively react through catalytic pathways inthe cell to form more potent oxidants, such as the hydroxyl radical (OH; the Fentonreaction)60 and hypochlorous acid (HOCl).61 An additional pathway for O2
z2-dependentoxidative stress involves the enzyme-independent reaction of O2
z2 with NOz to formperoxynitrite (ONOO2), another strong oxidizing and nitrating species.62,63 All of theabove-mentioned pathways form pro-oxidants with the redox potential to lead to theformation of the a-hydroxyethyl radical. Therefore, O2
z2 can be considered to be a key‘starting point’ of oxidative stress during alcohol exposure.
RNS: a role for nitric oxide
Like O2z2 for ROS, it is likely that NOz serves as the ‘parent’ molecule for other RNS.
Unlike O2z2, NOz has pleotropic effects that obscure whether it predominantly plays
Advances in alcoholic liver disease 631
a protective or a damaging role in ALD.64 For example, it is well known that thedisregulation of vascular tone after acute alcohol intake and in alcoholic cirrhosis ismediated, in part, by a decrease in NOz production.65,66 It has also been shown thatNOz is anti-apoptotic in hepatocytes and is required for normal liver regeneration.67,68
However, high levels of NOz can also play a potentially damaging role in ALD by theproduction of RNS, such as ONOO2. RNS derived from NOz can cause nitrationreactions (e.g. 3-nitrotyrosine formation) and nitrosation reactions (e.g. nitrosothiolformation), as well as oxidation reactions during alcohol exposure. Thus, NOz may playa dual role in ALD, mediating both protective effects and tissue damage byoverproduction of RNS. Which of these events predominates in vivo may depend onthe cell type, NOS isoform and stage of disease studied.
Alcohol-induced modifications in cellular redox balance independent of pro-oxidant formation
Alcohol also causes modifications to the cell that can lead to oxidative stressindependent of increased pro-oxidant production per se. Lower antioxidant levels inalcoholics due to the nutritional deficiencies are an example. The mobilization of freeiron caused by alcohol can also lead to an increase in transition-metal catalysis to potentoxidants (e.g. the Fenton reaction). Indeed, experiments have shown that ironsupplementation enhances damage due to alcohol.44,69 Another example is theinhibition by alcohol of the 26 S proteosome in hepatocytes.42 This critical complex isresponsible for degrading oxidatively modified proteins; therefore, its inhibition leadsto the accumulation of these damaged proteins, possibly even in the absence of a realincrease in pro-oxidants.70 Finally, there exist a host of proteins and systems involved inthe ‘antioxidant network’. This family does not directly intercept pro-oxidants, but theyserve instead as ancillary reductants and maintain the catalytic activity of antioxidantproteins or small molecules. These reactions require cellular energy to maintain suchcycles. The depletion by ethanol of both cytosolic and mitochondrial energy supplies(see above) can thus indirectly impair cellular antioxidant defences.
How are oxidants involved in alcoholic liver injury?
One mechanism by which oxidative stress is proposed to cause cellular injury is bychemical modification of biological molecules, which can alter and/or interfere withnormal processes within the cell. Also, antibodies against oxidatively modified proteinshave been shown to be produced in both humans and animal models of ALD.39,41 Theseantibodies have the potential to stimulate an autoimmune-like disease in the liver. It isnow clear that pro-oxidants can also mediate and/or amplify their signal by modifyingsignalling cascades within the cell. Many recent reviews have focused on the role ofsignalling cascades in damage due to oxidative stress.71274 Oxidant sensitive signallingcascades include small molecules (e.g. intracellular Caþþ )75, stress-activated proteinkinases (SAPK), (e.g. C-Jun N-terminal kinase (JNK), endoplasmic reticulum kinase 1and /or 2 (ERK 1/2) and p38)76, transcription factors (e.g. activator protein-1 (AP-1),hypoxia-inducible factor-1 (HIF-1) and nuclear factor which binds to the kB site onDNA (NFkB))77, and modulators of apoptosis signalling (e.g. caspases, Bad and Bcl-2).78
Ethanol has been shown to modulate the signal of many of these cascades in vitro and/or in experimental ALD; however, whether or not these effects are mediated byoxidative stress per se is often unclear.
632 G. Arteel et al
Cytokines and inflammatory mediators
Priming and sensitization of inflammation during ALD
A key concept in alcoholic liver injury is priming and sensitization. As mentioned above,the natural history of ALD is characterized by chronic inflammation in the liver.This activation of the immune response can be at least partially attributed to increasedlevels of activators of this response, such as lipopolysaccharides (LPS).79,80 However,the elevated levels of LPS found in alcoholics and in experimental ALD are relatively lowcompared to those found in endotoxaemia. Furthermore, damage to liver caused byalcohol cannot be mimicked by chronic low-dose LPS in the absence of ethanol.81
Instead, inflammatory cells appear to be primed to activation by alcohol administration.For example, peripheral blood monocytes obtained from patients with alcoholichepatitis spontaneously produce proinflammatory mediators (e.g. TNF-a) and theyproduce more of these mediators in response to LPS than do control monocytes.82
Other cytokines and chemokines that have been shown to be elevated in ALD patientsinclude IL-683, IL-884, monocyte chemoattractant protein 1 (MCP-1)85, and macrophageinflammatory protein 1 (MIP-1).86 In addition to cytokine/chemokine production, thereare a host of other mediators of inflammation that are increased in ALD, such asadhesion molecule expression, ROS/RNS (see above), and cytokine receptors (e.g.tumour necrosis factor receptor 1 (TNFR1)) to mention only a few. Moreover, anumber of the systemic effects of ALD (e.g. muscle wasting, increased gut permeabilityand fever) are thought to be mediated by elevated levels of proinflammatorymediators.87
In addition to priming inflammatory cells, liver cells appear to be sensitized toinflammatory stimuli by alcohol administration. For example, although TNF-a isnormally pro-proliferative in hepatocytes isolated from naı̈ve animals, it is pro-apoptotic in cells isolated from ethanol-treated animals.88 Furthermore, HepG2 cellsoverexpressing CYP2E1 are more sensitive to TNF-a-induced cell killing afterexposure to alcohol.89,90 This appears to be mediated through the cellular ‘deathdomain’ pathways.90 Other cell types (e.g. stellate cells) also appear to be primed/sensitized during alcohol administration.91,92
The concept of priming and sensitization also implies that there may be a series ofsequential events in the progression of liver injury during alcohol exposure. Specifically,the priming of inflammatory cells by ethanol leads to a more robust cell-killing responsethat is exacerbated in sensitized hepatocytes. This pattern explains why blocking theactivation of Kupffer cells or employing knockouts with an impaired Kupffer cellresponse protects against damage in hepatocytes. For example, knocking out the LPSserum carrier protein, LPS binding protein (LBP), blocked liver damage but did notprevent induction of CYP2E1.93 Such cell-to-cell signalling is also proposed to underliethe mechanism(s) by which some proteins appear to have both damaging and protectiveroles in ALD. For example, the transcription factor NFkB is a key mediator in theinflammatory response in Kupffer cells by upregulating proinflammatory genes (e.g.TNF-a). However, NFkB inhibition causes apoptosis after addition of TNF-a or amembrane receptor mediating apoptosis (Fas) to cultured hepatocytes.94,95 When ratswere transfected with adenoviral vectors containing the inhibitor of kB (IkB) super-repressor, liver damage due to enteral alcohol was prevented.96 Furthermore, theproduction of TNF-a in the liver was also blunted. It is, therefore, likely that underthese conditions, the potentially damaging/proinflammatory effects of NFkB activation,such as TNF-a production in Kupffer cells, precede any protective/anti-apoptoticeffects in the hepatocyte.
Advances in alcoholic liver disease 633

Effects of proinflammatory cytokines in ALD beyond inflammation
An interesting observation regarding antioxidants and knockout mice in studies ofexperimental ALD is that many of these conditions blunt the steatosis caused byalcohol.53–55,58,59,97 As mentioned above, steatosis due to alcohol is generallyconsidered to be the result of NADH redox inhibition of mitochondrial b-oxidationcaused by alcohol metabolism. While redox changes are likely to be necessary foralcohol-induced steatosis, the data obtained with antioxidants bring into questionwhether this redox shift is sufficient in and of itself. Specifically, none of the conditionsmentioned above had any apparent effect on alcohol metabolism. A factor that thesestudies have in common is that the increase in cytokine (e.g. TNF-a) production causedby alcohol was blunted. TNF-a (and other cytokines) can indeed influence lipidmetabolism both in the liver and the periphery (see Pessayre et al98, for a review). Forexample, TNF-a increases free fatty acid release from adipocytes in the periphery99,increases lipogenesis in hepatocytes100, and inhibits b-oxidation of fatty acids.101 Othercytokines induced by alcohol (e.g. IL-1 and IL-6) may also impair transport andsecretion of triglycerides.102 The net consequence during alcohol exposure is thatcytokines increase the supply of fatty acids to the liver while simultaneously impairingthe ability of the hepatocytes to metabolize and secrete them. In support of thishypothesis, TNFR1 knockout mice are protected against alcohol-induced fataccumulation in experimental ALD.103 It is proposed that these effects work in tandemwith alcohol-induced shifts in the NADH redox state to lead to steatosis.
Genetic polymorphisms and the risk of ALD
It is clear that the risk for the development of ALD increases with the time- and dose-dependent consumption of alcohol.104 However, even in populations that consume highlevels of ethanol (e.g. .80 g/day), only a fraction of individuals develop severe forms ofthe disease (e.g. alcoholic hepatitis and cirrhosis). Even when other risk factors (e.g.diet composition, concomitant hepatitis C virus (HCV) or hepatitis B virus (HBV)infection, etc) are taken into account, there is no combination of environmental riskthat leads to a 100% incidence of the disease. Furthermore, some individuals developALD while consuming much less alcohol. For these reasons, it has long been proposedthat in addition to environmental risk factors, there are genetic risk factors thatincrease the risk for the development of ALD.105
It is now clear that many gene products are polymorphic in the human population;polymorphisms in these genes give rise to structural and functional variations in theresultant proteins. It has been proposed that polymorphisms in key genes hypothesizedto be involved in the development of ALD may be the basis of the apparent genetic riskfor the development of the disease. Indeed, many of the above-described pathwaysthought to be involved in ALD are known to be polymorphic. For example, ethanol-metabolizing systems (e.g. ADH, ALDH and CYP2E1) have been shown to bepolymorphic.106 Indeed it is now clear that polymorphisms in ALDH gene products areresponsible for alcohol sensitivity, especially in Asian populations, and that theseindividuals develop ALD while consuming less alcohol.107 ROS/RNS formation anddamage are also clear candidates, but have yet to be clearly shown in large case–controlled studies. As mentioned above, iron catalysis of oxidative stress may be criticalin ALD; indeed, there is a strong link between disregulated iron homeostasis (e.g.haemochromatosis) and alcohol-induced liver disease.108 Lastly, polymorphisms in pro-inflammatory (e.g. TNF-a) and anti-inflammatory (e.g. IL-10) cytokines have also been
634 G. Arteel et al
linked to increased risk for ALD.109,110 It should be mentioned that, as withenvironmental risk factors, there is no genetic variation identified thus far that leads toa 100% incidence of ALD in individuals who drink. Instead it is likely that multipleenvironmental and genetic factors combine to determine the risk of the individual. Thegoal of future work is to better delineate these factors.
THERAPY FOR ALCOHOLIC LIVER DISEASE
We have reviewed the major advances that have been made in our understanding ofmechanisms of alcohol-induced liver injury, and these concepts are being translated intoclinical trials. Moreover, we are now in a position to better understand some ofthe mechanisms of actions of some traditionally-used therapies for ALD, ranging fromsteroids to antioxidant therapy. This section on therapy will touch on the importance of:(i) life-style change, including abstinence; (ii) nutrition; (iii) drug therapy (conventionaland alternative therapies) and (iv) the role of liver transplantation (Table 1).
Life-style change
Abstinence from alcohol is vital in order to prevent further ongoing liver injury, fibrosisand possibly hepatocellular carcinoma. Abstinence causes total resolution of alcoholicsteatosis. There are limited studies evaluating the effects of abstinence from alcohol onthe progression of ALD and these are retrospective, non-randomized trials. However,virtually all studies show beneficial effects of abstinence. Early studies from Klatskin’sprogramme showed that, in particular, patients with jaundice or ascites benefited fromabstinence.111 Merkel et al112 in a recent small series of patients having alcoholiccirrhosis who were followed for 4 years or until death, showed that the cumulativeprobability of survival was 87% in persistent abstainers and only 55% in persistentdrinkers. Patients with compensated or decompensated cirrhosis benefit fromabstinence. Moreover, unpublished data from recent Veterans Health Administration
Research agenda
† determine specific and sensitive biomarkers for alcohol consumption and ALD† determine how alcohol primes and sensitizes cells to cytokine injury† determine interactions between factors such as oxidative stress, cytokines and
genetic variations in ALD† translate new insights on mechanisms of liver injury into treatment
Table 1. Therapy for alcoholic liver disease (ALD).
† Lifestyle modification ( # EtOH, smoking, obesity)
† Proper nutrition/nutritional support
† Consider pentoxifylline or prednisone for alcoholic hepatitis
† Consider silymarin or SAMe for cirrhosis
† Correct metabolic disturbances/complications
† Transplantation in selected abstinent patients with end-stage disease
EtOH, alcohol; SAMe, S-adenosylmethionine.
Advances in alcoholic liver disease 635

(VA) Co-operative Studies suggest that reducing, but not stopping, ethanolconsumption also improves projected survival in ALD (Drs C. Lieber and T. Morgan,pers. comm.). Thus, abstinence, or a major reduction in drinking, should be encouragedin all patients with ALD. Newer agents to improve abstinence, such as Naltrexone andAcamprosate, have been shown to have efficacy in some chronic alcoholics; however,there are no large multicentre studies evaluating these drugs in patients with ALD.
Many subjects who drink alcohol also smoke cigarettes. Smoking cigarettes has beenshown in European studies to increase the rate of progression of fibrosis in ALD.113,114
Moreover, hepatitis C patients who drink also have accelerated disease progression ifthey smoke cigarettes.115 Cigarette smoking causes oxidative stress and this may beanother mechanism for the observed accelerated liver disease in smokers.
Obesity is associated with the development of fatty liver and non-alcoholicsteatohepatitis (NASH). Body mass index (BMI) has been shown to be an independentrisk factor for the development of ALD.116 Thus, similar to many other gastrointestinaldisorders (e.g. gastro-oesophageal reflux disease), the initial approach to ALD is lifestylemodification related to issues of alcohol consumption, cigarette smoking and obesity.
Nutrition therapy
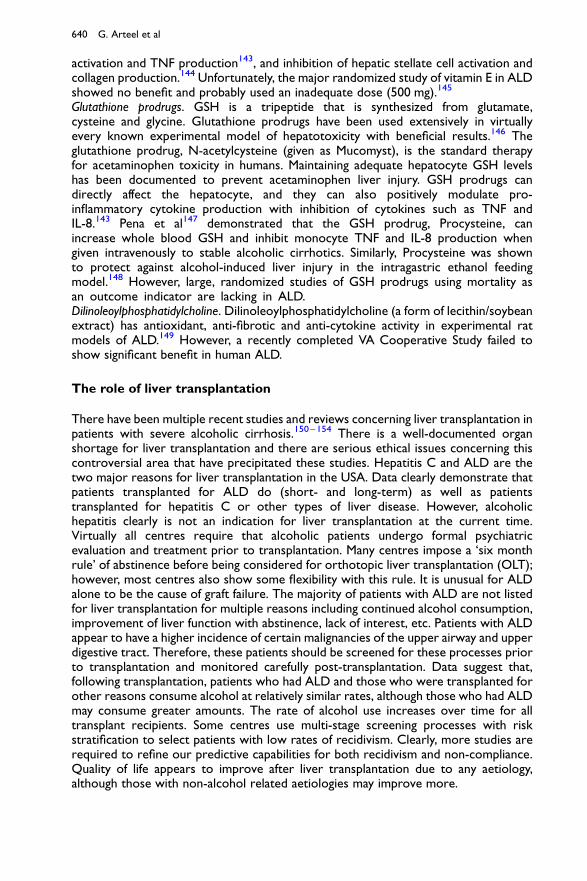
Malnutrition is prevalent in liver disease, especially in the more severe forms of chronicliver disease. Probably the most extensive studies of nutritional status in patients withliver disease are large studies in the VA Cooperative Studies Program dealing withpatients having alcoholic hepatitis.117 The first of these studies118 demonstrated thatvirtually every patient with alcoholic hepatitis had some degree of malnutrition. Patientshad a mean alcohol consumption of 228 g/day (with almost 50% of energy intake comingfrom alcohol). The severity of liver disease generally correlated with the severity ofmalnutrition. Similar data were generated in a follow-up VA study on alcoholichepatitis.119 In both of these studies, patients were given a balanced 2500-kcal hospitaldiet, monitored carefully by a dietitian, and were encouraged to consume the diet. Inthe second study, patients in the therapy arm of the protocol also received an enteralnutritional support product high in branched-chain amino acids (BCAAs), as well as theanabolic steroid oxandrolone (80 mg/day). Patients were not fed by tube if voluntaryoral intake was inadequate in either study (probably a study design flaw, in retrospect).Voluntary oral food intake correlated in a stepwise fashion with 6-month mortality data.Thus, patients who voluntarily consumed .3000 kcal/day had virtually no mortality,whereas those consuming ,1000 kcal/day had .80% 6-month mortality (Figure 2).117
Moreover, the degree of malnutrition correlated with the development of seriouscomplications such as encephalopathy, ascites and hepatorenal syndrome.117
Interest in nutrition therapy for cirrhosis was stimulated when Patek et al120
demonstrated that a nutritious diet improved the 5-year outcome of patients withalcoholic cirrhosis compared with patients consuming an inadequate diet. Several recentstudies have further supported the concept of improved outcome with nutritionalsupport in patients with cirrhosis. Hirsch et al121 demonstrated that outpatients takingan enteral nutritional support product (1000 kcal, 34 g protein) had significantlyimproved protein intake and significantly fewer hospitalizations. These sameinvestigators subsequently gave an enteral supplement to outpatients with alcoholiccirrhosis and observed an improvement in nutritional status and immune function.122 Inthe VA Cooperative Study No. 275 on nutritional support in ALD using both an anabolicsteroid and an enteral nutritional supplement, improved mortality was seen withthe combination of oxandrolone plus supplement in patients who had moderate
636 G. Arteel et al

protein–energy malnutrition.117 Those with severe malnutrition did not significantlybenefit from therapy, possibly because their malnutrition was so advanced that nointervention, including nutrition, could help. Studies by Kearns et al123 showed thatpatients with ALD hospitalized for treatment and given an enteral nutritionalsupplement via tube feeding had significantly improved serum bilirubin levels and liverfunction as assessed by anti-pyrine clearance. Moreover, a major randomized study ofenteral nutrition versus steroids in patients with alcoholic hepatitis showed similaroverall initial outcomes and fewer long term infections in the nutrition group.124 Thus,traditional nutritional supplementation clearly improves nutritional status and, in someinstances, hepatic function and other outcome indicators in alcoholic hepatitis/cirrhosis.
Drug therapy (conventional and alternative therapies)
Although ALD remains a major cause of morbidity and mortality in the USA, there is noFood and Drug Administration (FDA) approved therapy for either alcoholic cirrhosis oralcoholic hepatitis. However, there are several drugs that have been widely used. Wewill discuss only therapies available in the USA for which there generally have been largerandomized human studies.
Propylthiouracil
Chronic alcohol feeding in experimental animals produces a hypermetabolic state withincreased oxygen consumption. This may lead to relative hypoxia, especially in thecentral lobular area, or Zone 3, of the liver. Propylthiouracil (PTU) has been postulatedto attenuate this hypermetabolic state, to function as an anti-oxidant and to improveportal blood flow. This prompted a long-term study of PTU therapy by Orrego and
Energy intake (kcal/day)
100
80
60
40
20
0
>3000 2500-3000 2000-2499 1500-1999 1000-1499 <1000
Mor
talit
y (%
)
Figure 2. A direct relationship was noted between voluntary caloric intake in Veterans Health Administrationstudies in patients with moderate and severe alcoholic hepatitis. It is not known whether providing enteralfeeding to patients with inadequate caloric intake would have improved mortality.
Advances in alcoholic liver disease 637

co-workers in over 300 patients with a variety of types of liver disease, includingALD.125 In the total study population, mortality was reduced by nearly 50% in patientsreceiving PTU.125 A recent Cochrane review evaluated PTU therapy for ALD, includingalcoholic steatosis, alcoholic fibrosis, alcoholic hepatitis and/or cirrhosis.126 Combiningthe results of six randomized clinical trials, which included 710 patients, no significanteffects of PTU versus placebo on mortality or liver-related mortality, complications ofliver disease, or liver histology were shown.126 The negative results of this review, aswell as hepatologists’ natural aversion to render metabolically-compromised patientshypothyroid, limit enthusiasm for PTU in ALD.
Colchicine
Colchicine has been suggested as a treatment for ALD because of its anti-fibroticeffects. It has many potential therapeutic mechanisms of action including inhibition ofcollagen production, enhancement of collagenase activity and anti-inflammatoryfunctions. Initial positive studies by Kershenobich et al127 led to a large VA CooperativeStudy evaluating colchicine therapy in alcoholic cirrhosis that has recently beencompleted. Results showed no beneficial effect on either overall mortality or liver-related mortality.128 A recent smaller study from Europe also showed no beneficialeffects of colchicine.129 Thus, despite initial enthusiasm and biochemical rationale foruse of this drug, it does not appear to be effective in ALD.
Corticosteroids
Corticosteroids have been the most extensively-studied form of therapy for alcoholichepatitis, but their role remains limited.130 The rationale for steroid use is to decreasethe immune response and proinflammatory cytokine response. Most randomizedstudies have supported the use of corticosteroids in moderate/severe alcoholichepatitis, but the large multicentre VA study headed by Mendenhall yielded negativeresults.30,131 Most meta-analyses support the use of steroids for severe acute alcoholichepatitis including the most recent study.132 This study reported significantly improvedsurvival at 28 days (85% versus 65%) in severely ill alcoholic hepatitis patients having adiscriminant function (DF) of .32. This survival advantage may extend to 1 year, butnot 2. Independent prognostic factors associated with death at 28 days in this meta-analysis were steroid treatment, age and creatinine. It is important to note that thepatients studied were highly selected and infections (e.g. spontaneous bacterialperitonitis), gastro-intestinal bleeding and many other common complications wereexclusions for entry into these studies. Most investigators agree that if corticosteroidsare to be used, they should be reserved for those with relatively severe liver disease(DF . 32), and possibly those with hepatic encephalopathy. Steroids have well-documented side effects, including enhancing the risk of infection, which is alreadysubstantial in patients with alcoholic hepatitis. Thus, a major disadvantage tocorticosteroids is their lack of applicability in many patients with alcoholic hepatitis.
Pentoxifylline
Pentoxifylline (PTX) is a non-selective phosphodiesterase inhibitor that increasesintracellular concentrations of adenosine 30,50-cyclic monophosphate (cAMP) andguanosine 30,50-cyclic monophosphate (cGMP) and decreases production of pro-inflammatory chemokines/cytokines including TNF. Akriviadis et al133 from theUniversity of Southern California Liver Unit performed a prospective, randomized,double-blind clinical trial of PTX in severe alcoholic hepatitis (DF . 32). Forty-nine
638 G. Arteel et al

patients received 400 mg of PTX orally 3 times daily and 52 received placebo (vitaminB12) for 4 weeks. PTX treatment improved survival. Twelve PTX patients died (24.5%)compared with 24 (46%) placebo patients. PTX also decreased hepatorenal syndromeas a cause of death. Six out of the 12 (50%) PTX-treated patients who died did so ofrenal failure compared with 22 out of the 24 (92%) control patients who died of renalfailure. Multivariate analysis revealed age, serum creatinine at randomization andtreatment with PTX as independent factors associated with survival. Our groupcurrently uses PTX in patients with alcoholic hepatitis and with alcoholic cirrhosisbecause of its anti-inflammatory properties, its protective effects against hepatorenalsyndrome and its excellent safety profile.
Silymarin (milk thistle)
Silymarin is probably the most widely used form of complementary and alternativemedicine (CAM) in the treatment of liver disease in the USA. It has anti-oxidantactivities, it protects against lipid peroxidation and it has anti-inflammatory and anti-fibrotic effects. Large controlled trials of Silymarin have been performed in Europe, withvarying results. Ferenci et al134 evaluated 170 patients with cirrhosis in a treatmentprogramme (140 mg t.i.d.) having a mean duration of 41 months. They observed apositive beneficial effect, especially in patients with alcoholic cirrhosis and in those withmilder disease (Child’s A category). However, a study by Pares et al135 found nobeneficial effects (150 mg silymarin t.i.d.) in a study of 200 patients with alcoholiccirrhosis, some of whom also had hepatitis C. Both of these trials had majorshortcomings, including high drop-out rates and compliance issues. In all studiesperformed thus far, the drug appears to be quite safe.
S-Adenosylmethionine
S-Adenosylmethionine (SAMe or AdoMet), is an obligatory intermediate in theconversion of methionine to cysteine in the hepatic trans-sulphuration pathway. SAMeis a precursor for the synthesis of polyamines, choline and glutathione (GSH) and it isthe major methylating agent for a vast number of molecules via specific methyltrans-ferases.136 Patients with ALD have elevated plasma methionine levels, markedly delayedclearance of an oral methionine load and decreased hepatic methionine adenosyl-transferase (MAT) activity (the enzyme responsible for conversion of methionine toSAMe). Hepatic-specific MAT is highly sensitive to oxidative stress and it is likely thatthe subnormal hepatic MAT activity reported in ALD is due to oxidation of the activesite.137 Studies from our laboratories have shown that SAMe downregulatesproduction of the cytotoxic pro-inflammatory cytokine, TNF, in animal models ofliver injury and in peripheral blood monocytes or macrophage cell lines in vitro.138,139
Mato et al140 recently reported that patients with alcoholic liver cirrhosis who wererandomized to receive SAMe (1200 mg/day orally) for 2 years had decreased livermortality/liver transplantation (16% versus 30%) compared to the placebo treatedgroup.
Antioxidants
Vitamin E. Vitamin E deficiency has been well documented in ALD.141 Vitamin E has beenused extensively with hepatoprotective effects in experimental models of liver injurysuch as that induced by carbon tetrachloride or ischaemia. Vitamin E has multiplepotential beneficial effects including membrane stabilization142, reduced NFkB
Advances in alcoholic liver disease 639
activation and TNF production143, and inhibition of hepatic stellate cell activation andcollagen production.144 Unfortunately, the major randomized study of vitamin E in ALDshowed no benefit and probably used an inadequate dose (500 mg).145
Glutathione prodrugs. GSH is a tripeptide that is synthesized from glutamate,cysteine and glycine. Glutathione prodrugs have been used extensively in virtuallyevery known experimental model of hepatotoxicity with beneficial results.146 Theglutathione prodrug, N-acetylcysteine (given as Mucomyst), is the standard therapyfor acetaminophen toxicity in humans. Maintaining adequate hepatocyte GSH levelshas been documented to prevent acetaminophen liver injury. GSH prodrugs candirectly affect the hepatocyte, and they can also positively modulate pro-inflammatory cytokine production with inhibition of cytokines such as TNF andIL-8.143 Pena et al147 demonstrated that the GSH prodrug, Procysteine, canincrease whole blood GSH and inhibit monocyte TNF and IL-8 production whengiven intravenously to stable alcoholic cirrhotics. Similarly, Procysteine was shownto protect against alcohol-induced liver injury in the intragastric ethanol feedingmodel.148 However, large, randomized studies of GSH prodrugs using mortality asan outcome indicator are lacking in ALD.Dilinoleoylphosphatidylcholine. Dilinoleoylphosphatidylcholine (a form of lecithin/soybeanextract) has antioxidant, anti-fibrotic and anti-cytokine activity in experimental ratmodels of ALD.149 However, a recently completed VA Cooperative Study failed toshow significant benefit in human ALD.
The role of liver transplantation
There have been multiple recent studies and reviews concerning liver transplantation inpatients with severe alcoholic cirrhosis.150–154 There is a well-documented organshortage for liver transplantation and there are serious ethical issues concerning thiscontroversial area that have precipitated these studies. Hepatitis C and ALD are thetwo major reasons for liver transplantation in the USA. Data clearly demonstrate thatpatients transplanted for ALD do (short- and long-term) as well as patientstransplanted for hepatitis C or other types of liver disease. However, alcoholichepatitis clearly is not an indication for liver transplantation at the current time.Virtually all centres require that alcoholic patients undergo formal psychiatricevaluation and treatment prior to transplantation. Many centres impose a ‘six monthrule’ of abstinence before being considered for orthotopic liver transplantation (OLT);however, most centres also show some flexibility with this rule. It is unusual for ALDalone to be the cause of graft failure. The majority of patients with ALD are not listedfor liver transplantation for multiple reasons including continued alcohol consumption,improvement of liver function with abstinence, lack of interest, etc. Patients with ALDappear to have a higher incidence of certain malignancies of the upper airway and upperdigestive tract. Therefore, these patients should be screened for these processes priorto transplantation and monitored carefully post-transplantation. Data suggest that,following transplantation, patients who had ALD and those who were transplanted forother reasons consume alcohol at relatively similar rates, although those who had ALDmay consume greater amounts. The rate of alcohol use increases over time for alltransplant recipients. Some centres use multi-stage screening processes with riskstratification to select patients with low rates of recidivism. Clearly, more studies arerequired to refine our predictive capabilities for both recidivism and non-compliance.Quality of life appears to improve after liver transplantation due to any aetiology,although those with non-alcohol related aetiologies may improve more.
640 G. Arteel et al
CONCLUSIONS
In summary, all patients should stop or markedly decrease alcohol intake and employother lifestyle modifications where appropriate (Table 1). Proper nutrition andnutritional support have consistently been shown to be important. Certain drugs (e.g.corticosteroids or pentoxifylline) may be effective in selected patients. While no FDA-approved therapies are available, many new agents, such as anti-TNF antibody, areunder investigation. Transplantation is life-saving in certain abstinent patients with end-stage liver disease.
Complications of ALD are important events in more advanced liver disease.Diagnosing and appropriately treating complications is vital for maintaining quality of lifeand decreasing morbidity and mortality. Some major complications include: (i) ascites,(ii) spontaneous bacterial peritonitis, (iii) hepatorenal syndrome, (iv) hepaticencephalopathy and (v) oesophageal varices. Various therapies can attenuate orreverse these complications but are often only palliative. Liver transplantation iscurative. A discussion of these complications is beyond the scope of this chapter.However, the reader is directed to the following references, which review theseimportant topics.155–161
REFERENCES
1. Orholm M, Sorensen TI, Bentsen K et al. Mortality of alcohol abusing men prospectively assessed inrelation to history of abuse and degree of liver injury. Liver 1985; 5: 253–260.
2. Grant BF, DeBakey S & Zobeck TS. Surveillance Report No. 18: Liver Cirrhosis Mortality in the United States,1973–1988. Rockville, MD: National Institute on Alcohol Abuse and Alcoholism, Division of Biometryand Epidemiology, 1991.
3. Propst A, Propst T, Zangerl G et al. Prognosis and life expectancy in chronic liver disease. DigestiveDiseases and Sciences 1995; 40: 1805–1815.
4. Chedid A, Mendenhall CL, Gartside P et al. Prognostic factors in alcoholic liver disease. VA CooperativeStudy Group. American Journal of Gastroenterology 1991; 86: 210–216.
5. Becker U, Deis A, Sorensen TI et al. Prediction of risk of liver disease by alcohol intake, sex, and age: aprospective population study. Hepatology 1996; 23: 1025–1029.
6. Fuchs CS, Stampfer MJ, Colditz GA et al. Alcohol consumption and mortality among women. New EnglandJournal of Medicine 1995; 332: 1245–1250.
7. Thun MJ, Peto R, Lopez AD et al. Alcohol consumption and mortality among middle-aged and elderly U.S.adults. New England Journal of Medicine 1997; 337: 1705–1714.
8. Grant BF, Dufour MC & Harford TC. Epidemiology of alcoholic liver disease. Seminars in Liver Disease1988; 8: 12–25.
9. McCullough AJ. Alcoholic liver disease. In Schiff ER, Sorrell MF & Maddrey WC (eds.) Schiff ’s Diseases ofthe Liver. vol. 2, 8th edn, pp. 941–971. Philadelphia: Lippincott, Raven, 1999.
10. Espinoza P, Ducot B, Pelletier G et al. Interobserver agreement in the physical diagnosis of alcoholic liverdisease. Digestive Diseases and Sciences 1987; 32: 244–247.
Practice points
† lifestyle changes—stop or reduce drinking, stop smoking, lose weight (if obese)† nutrition intervention—adequate diet (calories and composition)† drug therapy—as yet no FDA-approved therapy for alcoholic cirrhosis or
alcoholic hepatitis† some CAM agents hold promise for cirrhosis; pentoxyfilline appears effective
for alcoholic hepatitis† liver transplantation corrects liver failure and disease complications
Advances in alcoholic liver disease 641
11. Rosman AS. Utility and evaluation of biochemical markers of alcohol consumption. Journal of SubstanceAbuse 1992; 4: 277–297.
12. Conigrave KM, Saunders JB & Whitfield JB. Diagnostic tests for alcohol consumption. Alcohol andAlcoholism 1995; 30: 13–26.
13. Buchsbaum DG, Buchanan RG, Welsh J et al. Screening for drinking disorders in the elderly using theCAGE questionnaire. Journal of the American Geriatrics Society 1992; 40: 662–665.
14. Girela E, Villanueva E, Hernandez-Cueto C & Luna JD. Comparison of the CAGE questionnaire versussome biochemical markers in the diagnosis of alcoholism. Alcohol and Alcoholism 1994; 29: 337–343.
15. Bruguera M, Bordas JM & Rodes J. Asymptomatic liver disease in alcoholics. Archives of Pathology andLaboratory Medicine 1977; 101: 644–647.
16. Leevy CB. Fatty liver: a study of 720 patients with biopsy proven fatty liver and a review of the literature.Medicine 1962; 41: 249.
17. Bird GL & Williams R. Factors determining cirrhosis in alcoholic liver disease. Molecular Aspects ofMedicine 1988; 10: 97–105.
18. Pares A, Caballeria J, Bruguera M et al. Histological course of alcoholic hepatitis. Influence of abstinence,sex and extent of hepatic damage. Journal of Hepatology 1986; 2: 33–42.
19. Bell H, Tallaksen CM, Try K & Haug E. Carbohydrate-deficient transferrin and other markers of highalcohol consumption: a study of 502 patients admitted consecutively to a medical department. Alcohol,Clinical and Experimental Research 1994; 18: 1103–1108.
* 20. Cohen JA & Kaplan MM. The SGOT/SGPTratio—an indicator of alcoholic liver disease. Digestive Diseasesand Sciences 1979; 24: 835–838.
21. Himmelstein DU, Woolhandler SJ & Adler RD. Elevated SGOT/SGPT ratio in alcoholic patients withacetaminophen hepatotoxicity. American Journal of Gastroenterology 1984; 79: 718–720.
22. Matloff DS, Selinger MJ & Kaplan MM. Hepatic transaminase activity in alcoholic liver disease.Gastroenterology 1980; 78: 1389–1392.
23. Galambos J. Alcoholic Hepatitis. New York: Intercontinental Medical Book Co, 1974.24. Skude G & Wadstein J. Amylase, hepatic enzymes and bilirubin in serum of chronic alcoholics. Acta Medica
Scandinavica 1977; 201: 53–58.25. Morse RM & Hurt RD. Screening for alcoholism. Journal of the American Medical Association 1979; 242:
2688–2690.26. Yersin B, Nicolet JF, Dercrey H et al. Screening for excessive alcohol drinking. Comparative value of
carbohydrate-deficient transferrin, gamma-glutamyltransferase, and mean corpuscular volume. Archievesof Internal Medicine 1995; 155: 1907–1911.
27. Nilssen O, Huseby NE, Hoyer G et al. New alcohol markers—how useful are they in population studies:the Svalbard Study 1988–89. Alcohol, Clinical and Experimental Research 1992; 16: 82–86.
28. Litten RZ, Allen JP & Fertig JB. Gamma-glutamyltranspeptidase and carbohydrate deficient transferrin:alternative measures of excessive alcohol consumption. Alcohol, Clinical and Experimental Research 1995;19: 1541–1546.
29. Maddrey WC, Boitnott JK, Bedine MS et al. Corticosteroid therapy of alcoholic hepatitis. Gastroenterology1978; 75: 193–199.
30. Carithers RL Jr., Herlong HF, Diehl AM et al. Methylprednisolone therapy in patients with severe alcoholichepatitis. A randomized multicenter trial. Annals of Internal Medicine 1989; 110: 685–690.
31. McClain C, Hill D, Schmidt J & Diehl AM. Cytokines and alcoholic liver disease. Seminars in Liver Disease1993; 13: 170–182.
32. Van Ness MM & Diehl AM. Is liver biopsy useful in the evaluation of patients with chronically elevated liverenzymes? Annals of Internal Medicine 1989; 111: 473–478.
33. Talley NJ, Roth A, Woods J & Hench V. Diagnostic value of liver biopsy in alcoholic liver disease. Journal ofClinical Gastroenterology 1988; 10: 647–650.
34. Teli MR, Day CP, Burt AD et al. Determinants of progression to cirrhosis or fibrosis in pure alcoholic fattyliver. Lancet 1995; 346: 987–990.
35. Fromenty B, Grimbert S, Mansouri A et al. Hepatic mitochondrial DNA deletion in alcoholics: associationwith microvesicular steatosis. Gastroenterology 1995; 108: 193–200.
36. MacSween RN & Burt AD. Histologic spectrum of alcoholic liver disease. Seminars in Liver Disease 1986; 6:221–232.
37. Chedid A, Mendenhall CL, Tosch T et al. Significance of megamitochondria in alcoholic liver disease.Gatroenterology 1986; 90: 1858–1864.
38. Lieber CS. Metabolic effects of acetaldehyde. Biochemical Society Transactions 1988; 16: 241–247.39. Klassen LW, Tuma D & Sorrell MF. Immune mechanisms of alcohol-induced liver disease. Hepatology 1995;
22: 355–357.40. Niemela O. Distribution of ethanol-induced protein in vivo: relationship to tissue injury. Free Radical
Biology and Medicine 2001; 31: 1533–1538.
642 G. Arteel et al

41. Thiele GM, Worrall S, Tuma DJ et al. The chemistry and biological effects of malondialdehyde-acetaldehydeadducts. Alcohol, Clinical and Experimental Research 2001; 25(5th supplement ISBRA): 218S–224S.
42. Bardag-Gorce F, Yuan QX, Li J et al. The effect of ethanol-induced cytochrome p4502E1 on the inhibitionof proteasome activity by alcohol. Biochemical and Biophysical Research Communications 2000; 279: 23–29.
43. Ekstrom G & Ingelman-Sundberg M. Rat liver microsomal NADPH-supported oxidase activity and lipidperoxidation dependent on ethanol-cytochrome P-450 (P-450IIE1). Biochemical Pharmacology 1989; 38:1313–1319.
44. Cederbaum AI, Wu D, Mari M & Bai J. CYP2E1-dependent toxicity and oxidative stress in HepG2 cells.Free Radical Biology and Medicine 2001; 31: 1539–1543.
45. Kono H, Bradford BU, Yin M et al. CYP2E1 is not involved in early alcohol-induced liver injury. AmericanJournal of Physiology 1999; 277: G1259–G1267.
46. Maher J. The CYP2E1 knockout delivers another punch: first ASH, now NASH. Alcoholic steatohepatitis.Nonalcoholic steatohepatitis. Hepatology 2001; 33: 311–312.
47. Lieber CS. ALCOHOL: its metabolism and interaction with nutrients. Annual Review of Nutrition 2000; 20:395–430.
48. Day CP & James OF. Hepatic steatosis: innocent bystander or guilty party? Hepatology 1998; 27:1463–1466.
49. Di Luzio NR. A mechanism of the acute ethanol-induced fatty liver and the modification of liver injury byantioxidants. American Journal of Pharmacy and the Sciences Supporting Public Health 1966; 15: 50–63.
50. Shaw S, Jayatilleke E, Ross WA et al. Ethanol-induced lipid peroxidation: potentiation by long-termalcohol feeding and attenuation by methionine. Journal of Laboratory and Clinical Medicine 1981; 98:417–424.
51. Patek Jr. AJ. Alcohol, malnutrition, and alcoholic cirrhosis. American Journal of Clinical Nutrition 1979; 32:1304–1312.
52. Bujanda L. The effects of alcohol consumption upon the gastrointestinal tract. American Journal ofGastroenterology 2000; 95: 3374–3382.
53. Kono H, Rusyn I, Bradford BU et al. Allopurinol prevents early alcohol-induced liver injury in rats. Journalof Pharmacology and Experimental Therapeutics 2000; 293: 296–303.
* 54. Kono H, Rusyn I, Uesugi Tet al. Diphenyleniodonium sulfate, an NADPH oxidase inhibitor, prevents earlyalcohol-induced liver injury in the rat. American Journal of Physiology: Gastrointestinal and Liver Physiology2001; 280: G1005–G1012.
55. Kono H, Arteel GE, Rusyn I et al. Ebselen prevents early alcohol-induced liver injury in rats. Free RadicalBiology and Medicine 2001; 30: 403–411.
56. McCord JM & Fridovich I. Superoxide dismutase. An enzymic function for erythrocuprein (hemocuprein).Journal of Biological Chemistry 1969; 244: 6049–6055.
57. Polavarapu R, Spitz DR, Sim JE et al. Increased lipid peroxidation and impaired antioxidant enzymefunction is associated with pathological liver injury in experimental alcoholic liver disease in rats fed dietshigh in corn oil and fish oil. Hepatology 1998; 27: 1317–1323.
58. Wheeler MD, Kono H, Yin M et al. Delivery of the Cu/Zn-superoxide dismutase gene with adenovirusreduces early alcohol-induced liver injury in rats. Gastroenterology 2001; 120: 1241–1250.
59. Wheeler MD, Nakagami M, Bradford BU et al. Overexpression of manganese superoxide dismutaseprevents alcohol-induced liver injury in the rat. Journal of Biological Chemistry 2001; 276:36664–36672.
60. Fridovich I. Superoxide radical and superoxide dismutases. Annual Review of Biochemistry 1995; 64:97–112.
61. Klebanoff SJ. Myeloperoxidase-halide-hydrogen peroxide antibacterial system. Journal of Bacteriology 1968;95: 2131–2138.
62. Beckman JS, Beckman TW, Chen J et al. Apparent hydroxyl radical production by peroxynitrite:implications for endothelial injury from nitric oxide and superoxide. Proceedings of the National Academy ofSciences of the USA 1990; 87: 1620–1624.
63. Beckman JS. The physiological and pathophysiological chemistry of nitric oxide. In Lancaster J (ed.) NitricOxide: Principles and Actions. pp 1–82, San Diego, CA: Academic Press, 1996.
64. Hon WM, Lee KH & Khoo HE. Nitric oxide in liver diseases: friend, foe, or just passerby? Annals of theNew York Academy of Science 2002; 962: 275–295.
65. Oshita M, Takei Y, Kawano S et al. Endogenous nitric oxide attenuates ethanol-induced perturbation ofhepatic circulation in the isolated perfused rat liver. Hepatology 1994; 20: 961–965.
66. Wiest R & Groszmann RJ. The paradox of nitric oxide in cirrhosis and portal hypertension: too much, notenough. Hepatology 2002; 35: 478–491.
67. Kim YM, Kim TH, Chung HT et al. Nitric oxide prevents tumor necrosis factor alpha-induced rathepatocyte apoptosis by the interruption of mitochondrial apoptotic signaling through S-nitrosylation ofcaspase-8. Hepatology 2000; 32: 770–778.
Advances in alcoholic liver disease 643
68. Rai RM, Lee FY, Rosen A et al. Impaired liver regeneration in inducible nitric oxide synthase deficient mice.Proceedings of the National Academy of Sciences of the USA 1998; 95: 13829–13834.
69. Tsukamoto H, Horne W, Kamimura S et al. Experimental liver cirrhosis induced by alcohol and iron.Journal of Clinical Investigation 1995; 96: 620–630.
* 70. Donohue TM Jr. The ubiquitin–proteasome system and its role in ethanol-induced disorders. AddictionBiology 2002; 7: 15–28.
71. Allen RG & Tresini M. Oxidative stress and gene regulation. Free Radical Biology and Medicine 2000; 28:463–499.
72. Droge W. Free radicals in the physiological control of cell function. Physiological Reviews 2002; 82: 47–95.73. Forman HJ & Torres M. Redox signaling in macrophages. Molecular Aspects of Medicine 2001; 22: 189–216.74. Kamata H & Hirata H. Redox regulation of cellular signalling. Cellular Signalling 1999; 11: 1–14.75. Ermak G & Davies KJ. Calcium and oxidative stress: from cell signaling to cell death. Molecular Immunology
2002; 38: 713–721.76. Suzuki YJ, Forman HJ & Sevanian A. Oxidants as stimulators of signal transduction. Free Radical Biology and
Medicine 1997; 22: 269–285.77. D’Angio CT & Finkelstein JN. Oxygen regulation of gene expression: a study in opposites. Molecular
Genetics and Metabolism 2000; 71: 371–380.78. Hoek JB & Pastorino JG. Ethanol, oxidative stress, and cytokine-induced liver cell injury. Alcohol 2002; 27:
63–68.79. Spencer S, Rubin K & Lieber CS. Depressed hepatic glutathione and increased diene conjugates in
alcoholic liver disease: evidence of lipid peroxidation. Digestive Diseases and Sciences 1983; 28: 585–589.80. Bigatello LM, Broitman SA, Fattori L et al. Endotoxemia, encephalopathy, and mortality in cirrhotic
patients. American Journal of Gastroenterology 1987; 82: 11–15.81. Deaciuc IV, Fortunato F, D’Souza NB et al. Modulation of caspase-3 activity and Fas ligand mRNA
expression in rat liver cells in vivo by alcohol and lipopolysaccharide. Alcohol, Clinical and ExperimentalResearch 1999; 23: 349–356.
* 82. MaClain CJ & Cohen DA. Increased tumor necrosis factor production by monocytes in alcoholic hepatitis.Hepatology 1989; 9: 349–351.
83. Hill DB, Marsano L, Cohen D et al. Increased plasma interleukin-6 concentrations in alcoholic hepatitis.Journal of Laboratory and Clinical Medicine 1992; 119: 547–552.
84. Hill DB, Marsano LS & McClain CJ. Increased plasma interleukin-8 concentrations in alcoholic hepatitis.Hepatology 1993; 18: 576–580.
85. Devalaraja MN, McClain CJ, Barve S et al. Increased monocyte MCP-1 production in acute alcoholichepatitis. Cytokine 1999; 11: 875–881.
86. Fisher NC, Neil DA, Williams A & Adams DH. Serum concentrations and peripheral secretion of the betachemokines monocyte chemoattractant protein 1 and macrophage inflammatory protein 1 alpha inalcoholic liver disease. Gut 1999; 45: 416–420.
* 87. McClain CJ, Hill DB, Song Z et al. Monocyte activation in alcoholic liver disease. Alcohol 2002; 27: 53–61.88. Colell A, Garcia-Ruiz C, Miranda M et al. Selective glutathione depletion of mitochondria by ethanol
sensitizes hepatocytes to tumor necrosis factor. Gastroenterology 1998; 115: 1541–1551.89. Pastorino JG & Hoek JB. Ethanol potentiates tumor necrosis factor-alpha cytotoxicity in hepatoma cells
and primary rat hepatocytes by promoting induction of the mitochondrial permeability transition.Hepatology 2000; 31: 1141–1152.
90. Liu H, Jones BE, Bradham C & Czaja MJ. Increased cytochrome P-450 2E1 expression sensitizeshepatocytes to c-Jun-mediated cell death from TNF-alpha. American Journal of Physiology: Gastrointestinaland Liver Physiology 2002; 282: G257–G266.
91. Kim KY, Rhim T, Choi I & Kim SS. N-acetylcysteine induces cell cycle arrest in hepatic stellate cells throughits reducing activity. Journal of Biological Chemistry 2001; 276: 40591–40598.
92. Reeves HL, Dack CL, Peak M et al. Stress-activated protein kinases in the activation of rat hepatic stellatecells in culture. Journal of Hepatology 2000; 32: 465–472.
93. Uesugi T, Froh M, Arteel GE et al. Role of lipopolysaccharide-binding protein in early alcohol-induced liverinjury in mice. Journal of Immunology 2002; 168: 2963–2969.
94. Bradham CA, Qian T, Streetz K et al. The mitochondrial permeability transition is required for tumornecrosis factor alpha-mediated apoptosis and cytochrome c release. Molecular and Cellular Biology 1998;18: 6353–6364.
95. Hatano E, Bradham CA, Stark A et al. The mitochondrial permeability transition augments Fas-inducedapoptosis in mouse hepatocytes. Journal of Biological Chemistry 2000; 275: 11814–11823.
96. Uesugi T, Froh M, Arteel GE et al. Delivery of IkappaB superrepressor gene with adenovirus reduces earlyalcohol-induced liver injury in rats. Hepatology 2001; 34: 1149–1157.
97. McKim SE, Konno A, Gabele E et al. Cocoa extract protects against early alcohol-induced liver injury inthe rat. Archives of Biochemistry and Biophysics 2002; 406: 40–46.
644 G. Arteel et al
* 98. Pessayre D, Mansouri A & Fromenty B. Nonalcoholic steatosis and steatohepatitis. V. Mitochondrialdysfunction in steatohepatitis. American Journal of Physiology: Gastrointestinal and Liver Physiology 2002; 282:G193–G199.
99. Hardardottir I, Doerrler W, Feingold KR & Grunfeld C. Cytokines stimulate lipolysis and decreaselipoprotein lipase activity in cultured fat cells by a prostaglandin independent mechanism. Biochemical andBiophysical Research Communications 1992; 186: 237–243.
100. Feingold KR & Grunfeld C. Tumor necrosis factor-alpha stimulates hepatic lipogenesis in the rat in vivo.Journal of Clinical Investigation 1987; 80: 184–190.
101. Nachiappan V, Curtiss D, Corkey BE & Kilpatrick L. Cytokines inhibit fatty acid oxidation in isolated rathepatocytes: synergy among TNF, IL-6, and IL-1. Shock 1994; 1: 123–129.
102. Navasa M, Gordon DA, Hariharan N et al. Regulation of microsomal triglyceride transfer protein mRNAexpression by endotoxin and cytokines. Journal of Lipid Research 1998; 39: 1220–1230.
103. Yin M, Wheeler MD, Kono H et al. Essential role of tumor necrosis factor alpha in alcohol-induced liverinjury in mice. Gastroenterology 1999; 117: 942–952.
104. Lelbach WK. Liver damage in chronic alcoholism. Results of a clinical, clinical-chemical and bioptic-histological study in 526 alcoholic patients during a low-calorie diet in an open drinking sanatorium. ActaHepato-splenologica 1966; 13: 321–349.
105. Day CP. Who gets alcoholic liver disease: nature or nurture? Journal of the Royal College of Physicians,London 2000; 34: 557–562.
106. Agarwal DP. Genetic polymorphisms of alcohol metabolizing enzymes. Pathologie-Biologie (Paris) 2001;49: 703–709.
107. Eriksson CJ. The role of acetaldehyde in the actions of alcohol (update 2000). Alcohol, Clinical andExperimental Research 2001; 25(5 supplement ISBRA): 15S–32S.
108. Adams PC & Agnew S. Alcoholism in hereditary hemochromatosis revisited: prevalence and clinicalconsequences among homozygous siblings. Hepatology 1996; 23: 724–727.
109. Grove J, Daly AK, Bassendine MF & Day CP. Association of a tumor necrosis factor promoterpolymorphism with susceptibility to alcoholic steatohepatitis. Hepatology 1997; 26: 143–146.
* 110. Grove J, Daly AK, Bassendine MF et al. Interleukin 10 promoter region polymorphisms and susceptibilityto advanced liver disease. Gut 2000; 46: 540–545.
111. Powell WJ Jr. & Klatskin G. Duration of survival in patients with Laennec’s cirrhosis. Influence of alcoholwithdrawal, and possible effects of recent changes in general management of the disease. American Journalof Medicine 1968; 44: 406–420.
112. Merkel C, Marchesini G, Fabbri A et al. The course of galactose elimination capacity in patients withalcoholic cirrhosis: possible use as a surrogate marker for death. Hepatology 1996; 24: 820–823.
113. Klatsky AL & Armstrong MA. Alcohol, smoking, coffee and cirrhosis. American Journal of Epidemiology1992; 136: 1248–1257.
114. Corrao G, Lepore AR, Torchio P et al. The effect of drinking coffee and smoking cigarettes on the risk ofcirrhosis associated with alcohol consumption. A case–control study. Provincial Group for the Study ofChronic Liver Disease. European Journal of Epidemiology 1994; 10: 657–664.
115. Pessione F, Ramond MJ, Njapoum C et al. Cigarette smoking and hepatic lesions in patients with chronichepatitis C. Hepatology 2001; 34: 121–125.
116. Raynard B, Balian A, Fallik D et al. Risk factors of fibrosis in alcohol-induced liver disease. Hepatology2002; 35: 635–638.
117. Mendenhall C, Roselle GA, Gartside P & Moritz T. Relationship of protein calorie malnutrition toalcoholic liver disease: a reexamination of data from two Veterans Administration Cooperative Studies.Alcohol, Clinical and Experimental Research 1995; 19: 635–641.
118. Mendenhall CL, Anderson S, Weesner RE et al. Protein calorie malnutrition associated with alcoholichepatitis. Veterans Administration Cooperative Study Group on Alcoholic Hepatitis. American Journal ofMedicine 1984; 76(2): 211–222.
119. Mendenhall CL, Moritz TE, Roselle GA, Morgan TR, Nemchausky BA, Tamburro CH, Schiff ER, McClainCJ, Marsano LS, Allen JI, Samanta A, Weesner RE, Henderson W, Gartside P, Chen TS, French SW,Chedid A, and the Veterans Affairs Cooperative Study Group 275. A study of oral nutritional supportwith oxandrolone in malnourished patients with alcoholic hepatitis: results of a Department of VeteransAffairs Cooperative study. Hepatology 1993; 17(4): 564–576.
120. Patek AJ, Post J & Ralnoff OD. Dietary treatment of cirrhosis of the liver. Journal of the American MedicalAssociation 1948; 139: 543–549.
121. Hirsch S, Bunout D, de la Maza P et al. Controlled trial on nutrition supplementation in outpatients withsymptomatic alcoholic cirrhosis. Journal of Parenteral and Enteral Nutrition 1993; 17: 119–124.
122. Hirsch S, de la Maza MP, Gattas V et al. Nutritional support in alcoholic cirrhotic patients improves hostdefenses. Journal of the American College of Nutrition 1999; 18: 434–441.
Advances in alcoholic liver disease 645
123. Kearns PJ, Young H, Garcia G et al. Accelerated improvement of alcoholic liver disease with enteralnutrition. Gastroenterology 1992; 102: 200–205.
* 124. Cabre E, Rodriguez-Iglesias P, Caballeria J et al. Short- and long-term outcome of severe alcohol-inducedhepatitis treated with steroids or enteral nutrition: a multicenter randomized trial. Hepatology 2000; 32:36–42.
125. Orrego H, Blake JE, Blendis LM et al. Long-term treatment of alcoholic liver disease withpropylthiouracil. New England Journal of Medicine 1987; 317: 1421–1427.
126. Rambaldi A & Gluud C. Propylthiouracil for alcoholic liver disease. Cochrane Database of SystematicReviews 2002; 2: CD002800.
127. Kershenobich D, Vargas F, Garcia-Tsao G et al. Colchicine in the treatment of cirrhosis of the liver. NewEngland Journal of Medicine 1988; 318: 1709–1713.
128. Morgan T, Nemchausky N, Schiff ER et al. Colchicine does not prolong life in patients with advancedalcoholic cirrhosis: results of a prospective, randomized, placebo-controlled, multicenter VA trial (Csp352). Gastroenterology 2002; 122(supplement): 641(abstract).
129. Cortez-Pinto H, Alexandrino P, Camilo ME et al. Lack of effect of colchicine in alcoholic cirrhosis: finalresults of a double blind randomized trial. European Journal of Gastroenterology and Hepatology 2002; 14:377–381.
130. Fulton F & McCullough AJ. Treatment of alcoholic hepatitis. Clinics in Liver Disease 1998; 4:799–819.
131. Mendenhall CL, Anderson S, Garcia-Pont P et al. Short-term and long-term survival in patients withalcoholic hepatitis treated with oxandrolone and prednisolone. New England Journal of Medicine 1984;311: 1464–1470.
132 Mathurin P, Mendenhall CL, Carithers RL Jr. et al. Corticosteroids improve short-term survival inpatients with severe alcoholic hepatitis (AH): individual data analysis of the last three randomizedplacebo controlled double blind trials of corticosteroids in severe AH. Journal of Hepatology 2002;36: 480–487.
* 133. Akriviadis E, Botla R, Briggs Wet al. Pentoxifylline improves short-term survival in severe acute alcoholichepatitis: a double-blind, placebo-controlled trial. Gastroenterology 2000; 119: 1637–1648.
134. Ferenci P, Dragosics B, Dittrich H et al. Randomized controlled trial of silymarin treatment in patientswith cirrhosis of the liver. Journal of Hepatology 1989; 9: 105–113.
135. Pares A, Planas R, Torres M et al. Effects of silymarin in alcoholic patients with cirrhosis of the liver:results of a controlled, double-blind, randomized and multicenter trial. Journal of Hepatology 1998; 28:615–621.
136. Mato JM, Alvarez L, Ortiz P & Pajares MA. S-adenosylmethionine synthesis: molecular mechanisms andclinical implications. Pharmacology and Therapeutics 1997; 73: 265–280.
* 137. Sanchez-Gongora E, Ruiz F, Mingorance J et al. Interaction of liver methionine adenosyltransferase withhydroxyl radical. FASEB Journal 1997; 11: 1013–1019.
138. Chawla RK, Watson WH, Eastin CE et al. S-adenosylmethionine deficiency and TNF-alpha inlipopolysaccharide-induced hepatic injury. American Journal of Physiology 1998; 275: G125–G129.
139. McClain CJ, Hill DB, Song Z et al. S-adenosylmethionine, cytokines, and alcoholic liver disease. Alcohol2002; 27: 185–192.
* 140. Mato JM, Camara J, Fernandez de Paz J et al. S-adenosylmethionine in alcoholic liver cirrhosis: arandomized, placebo-controlled, double-blind, multicenter clinical trial. Journal of Hepatology 1999; 30:1081–1089.
141. McClain C, Hill D, Kugelmas M & Marsano L. Nutrition and liver disease. In RM B (ed.) Present Knowledgein Nutrition. pp 483–496, Washington, DC: International Life Sciences Institute, 2001.
142. Evstigneeva RP, Volkov IM & Chudinova VV. Vitamin E as a universal antioxidant and stabilizer ofbiological membranes. Membrane and Cell Biology 1998; 12: 151–172.
143. Hill DB, Devalaraja R, Joshi-Barve S et al. Antioxidants attenuate nuclear factor-kappa B activation andtumor necrosis factor-alpha production in alcoholic hepatitis patient monocytes and rat Kupffer cells, invitro. Clinical Biochemistry 1999; 32: 563–570.
144. Lee KS, Buck M, Houglum K & Chojkier M. Activation of hepatic stellate cells by TGF alpha and collagentype I is mediated by oxidative stress through c-myb expression. Journal of Clinical Investigation 1995; 96:2461–2468.
145. de la Maza MP, Petermann M, Bunout D & Hirsch S. Effects of long-term vitamin E supplementation inalcoholic cirrhotics. Journal of the American College of Nutrition 1995; 14: 192–196.
146. Meister A. Glutathione metabolism and its selective modification. Journal of Biological Chemistry 1988;263: 17205–17208.
147. Pena LR, Hill DB & McClain CJ. Treatment with glutathione precursor decreases cytokine activity. Journalof Parental and Enteral Nutrition 1999; 23: 1–6.
646 G. Arteel et al
148. Iimuro Y, Bradford BU, Yamashina S et al. The glutathione precursor L-2-oxothiazolidine-4-carboxylicacid protects against liver injury due to chronic enteral ethanol exposure in the rat. Hepatology 2000; 31:391–398.
149. Cao Q, Mak KM & Lieber CS. Dilinoleoylphosphatidylcholine decreases LPS-induced TNF-alphageneration in Kupffer cells of ethanol-fed rats: respective roles of MAPKs and NF-kappaB. Biochemicaland Research Communications 2002; 29: 849–853.
150. Veldt BJ, Laine F, Guillygomarc’h A et al. Indication of liver transplantation in severe alcoholic livercirrhosis: quantitative evaluation and optimal timing. Journal of Hepatology 2002; 36: 93–98.
151. Bravata DM, Olkin I, Barnato AE et al. Employment and alcohol use after liver transplantation foralcoholic and nonalcoholic liver disease: a systematic review. Liver Transplantation 2001; 7: 191–203.
152. Neuberger J, Schulz KH, Day C et al. Transplantation for alcoholic liver disease. Journal of Hepatology2002; 36: 130–137.
153. Bellamy CO, DiMartini AM, Ruppert K et al. Liver transplantation for alcoholic cirrhosis: long termfollow-up and impact of disease recurrence. Transplantation 2001; 72: 619–626.
154. Gish RG, Lee A, Brooks L et al. Long-term follow-up of patients diagnosed with alcohol dependence oralcohol abuse who were evaluated for liver transplantation. Liver Transplantation 2001; 7: 581–587.
155. Garcia-Tsao G. Current management of the complications of cirrhosis and portal hypertension: varicealhemorrhage, ascites, and spontaneous bacterial peritonitis. Gastroenterology 2001; 120: 726–748.
156. Burroughs AK & Vangeli M. Transjugular intrahepatic portosystemic shunt versus endoscopic therapy:randomized trials for secondary prophylaxis of variceal bleeding: an updated meta-analysis. ScandinavianJournal of Gastroenterology 2002; 37: 249–252.
157. Arroyo V, Gines P, Gerbes AL et al. Definition and diagnostic criteria of refractory ascites andhepatorenal syndrome in cirrhosis. International Ascites Club. Hepatology 1996; 23: 164–176.
158. Angeli P, Volpin R, Gerunda G et al. Reversal of type 1 hepatorenal syndrome with the administration ofmidodrine and octreotide. Hepatology 1999; 29: 1690–1697.
159. Mitzner SR, Stange J, Klammt S et al. Improvement of hepatorenal syndrome with extracorporealalbumin dialysis MARS: results of a prospective, randomized, controlled clinical trial. Liver Transplantation2000; 6: 277–286.
160. Blei AT & Cordoba J. Hepatic encephalopathy. American Journal of Gastroenterology 2001; 96: 1968–1976.161. Burroughs AK & Patch D. Transjugular intrahepatic portosystemic shunt. Seminars in Liver Disease 1999;
19: 457–473.
Advances in alcoholic liver disease 647
Related Documents











