ADVANCED AIRWAY ADVANCED AIRWAY MANAGEMENT MANAGEMENT Nazri B. Aiwan @ Ismail Nazri B. Aiwan @ Ismail Pengajar Pengajar Kolej Pembantu Perubatan Ulu Kolej Pembantu Perubatan Ulu Kinta Kinta

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ADVANCED AIRWAY ADVANCED AIRWAY MANAGEMENTMANAGEMENT
Nazri B. Aiwan @ IsmailNazri B. Aiwan @ Ismail
PengajarPengajar
Kolej Pembantu Perubatan Ulu Kolej Pembantu Perubatan Ulu KintaKinta
EAM
Airway and ventilation are the Airway and ventilation are the first priorities in managingfirst priorities in managing
the emergency patient.the emergency patient.

Early preventable deaths from airway Early preventable deaths from airway problems include:problems include:
Failure to recognise the partially obstructed Failure to recognise the partially obstructed airway and/or inadequate ventilation.airway and/or inadequate ventilation.
Delay in providing an airway when it is Delay in providing an airway when it is needed.needed.
Delay in providing assisted ventilation when Delay in providing assisted ventilation when it is neededit is needed
Technical difficulties in securing a definitive Technical difficulties in securing a definitive airway.airway.
Aspiration of gastric contents.Aspiration of gastric contents.
Problems with emergency airway Problems with emergency airway managementmanagement
Unavailability or inadequate history.Unavailability or inadequate history. Intoxication and drug overdose.Intoxication and drug overdose. Inadequate time for thorough assessment of the Inadequate time for thorough assessment of the
airway.airway. Unstable haemodynamic and respiratory Unstable haemodynamic and respiratory
parameters.parameters. Patient must undergo multiple therapeutic and Patient must undergo multiple therapeutic and
diagnostic intervention while airway assessment diagnostic intervention while airway assessment & management take place.& management take place.
Danger of aspiration due to “full stomach”.Danger of aspiration due to “full stomach”. Critical illness increase OCritical illness increase O22 demand. demand.

Assessment, identification and management Assessment, identification and management of airway and ventilatory compromiseof airway and ventilatory compromise
A.A. Establish responsivenessEstablish responsiveness
B.B. Assessment of airwayAssessment of airway
C.C. Opening and maintenance of airwayOpening and maintenance of airway
D.D. Assessment of ventilationAssessment of ventilation
E.E. Maintenance of ventilationMaintenance of ventilation
F.F. Definitive airwayDefinitive airway

Supplemental oxygenSupplemental oxygen should be provided should be provided before and immediately after airway measures before and immediately after airway measures are instituted.are instituted.
Protection of the cervical spineProtection of the cervical spine must be must be provided in patients who are unconscious, provided in patients who are unconscious, patients with injuries above the clavicle and patients with injuries above the clavicle and multi system trauma.multi system trauma.
In trauma patients, cIn trauma patients, care must be taken to are must be taken to maintain in linemaintain in line immobilisation of the cervical immobilisation of the cervical spinespine during airway management.during airway management.
Assessment, identification and management Assessment, identification and management of airway and ventilatory compromiseof airway and ventilatory compromise
A. Establish responsivenessA. Establish responsiveness
If the patient is able to speak and If the patient is able to speak and answer appropriately, it can be answer appropriately, it can be assumed:assumed:
* the airway is unobstructed* the airway is unobstructed
* cerebral perfusion adequate* cerebral perfusion adequate
1.1. LOOKLOOK
2.2. LISTENLISTEN
3.3. FEELFEEL
B. Assessment of the AirwayB. Assessment of the Airway
CAUSES OF AIRWAY CAUSES OF AIRWAY OBSTRUCTIONOBSTRUCTION
1.1. Soft tissue obstructionSoft tissue obstruction Floppy tongue (main cause of airway obstruction)Floppy tongue (main cause of airway obstruction) maxillofacial or airway injuriesmaxillofacial or airway injuries Oedema or haematoma occluding the airwayOedema or haematoma occluding the airway
2.2. Foreign body obstructionForeign body obstruction TeethTeeth SecretionSecretion BloodBlood foreign debrisforeign debris
3.3. Laryngospasm / bronchospasmLaryngospasm / bronchospasm
Main cause of airway obstruction is due to the Main cause of airway obstruction is due to the floppy tongue especially in patients with floppy tongue especially in patients with altered sensorium. altered sensorium.
Obstructed airway can often be cleared by:Obstructed airway can often be cleared by:– chin lift or jaw thrust chin lift or jaw thrust or head tilt chin lift or head tilt chin lift and the use and the use
of airway adjuncts (obstruction by the floppyof airway adjuncts (obstruction by the floppy tongue).tongue).
– removing and suctioning secretion and foreign removing and suctioning secretion and foreign bodybody
C. OPENING AND MAINTENANCE OF AIRWAY
1.1. Manual manoeuvresManual manoeuvres chin liftchin lift/head tilt/head tilt jaw thrustjaw thrust
2.2. Airway adjunctsAirway adjuncts oropharyngeal airwayoropharyngeal airway nasopharyngeal airwaynasopharyngeal airway
3.3. EEndotracheal intubationndotracheal intubation4.4. SSurgical airwayurgical airway
cricothyroidotomycricothyroidotomy
Manoeuvres to open and maintain the airway
5.5. Other airway mx technique;Other airway mx technique;
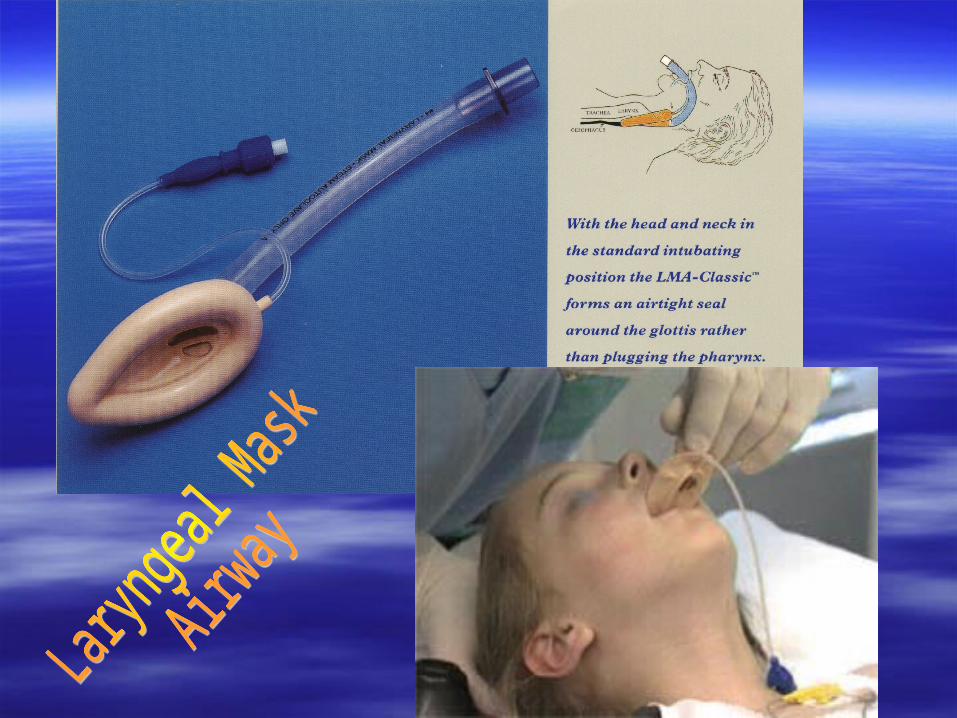
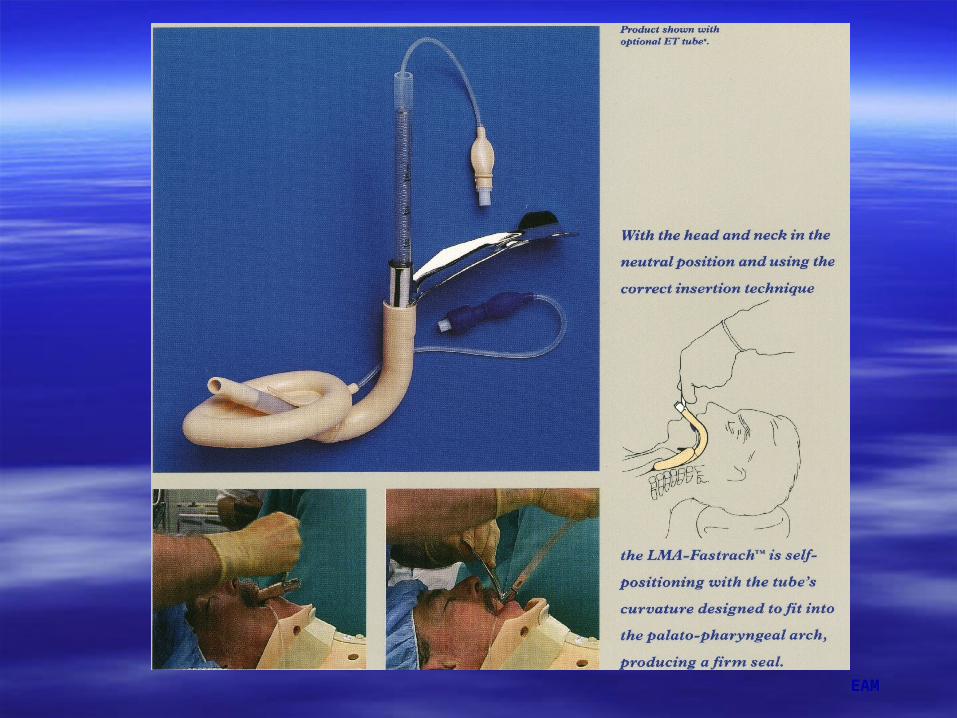
– Laryngeal mask/tracheal tube– Fastrach– Fibreoptic intubation– Illuminating stylet– combitube
Manoeuvres to open and maintain the airway
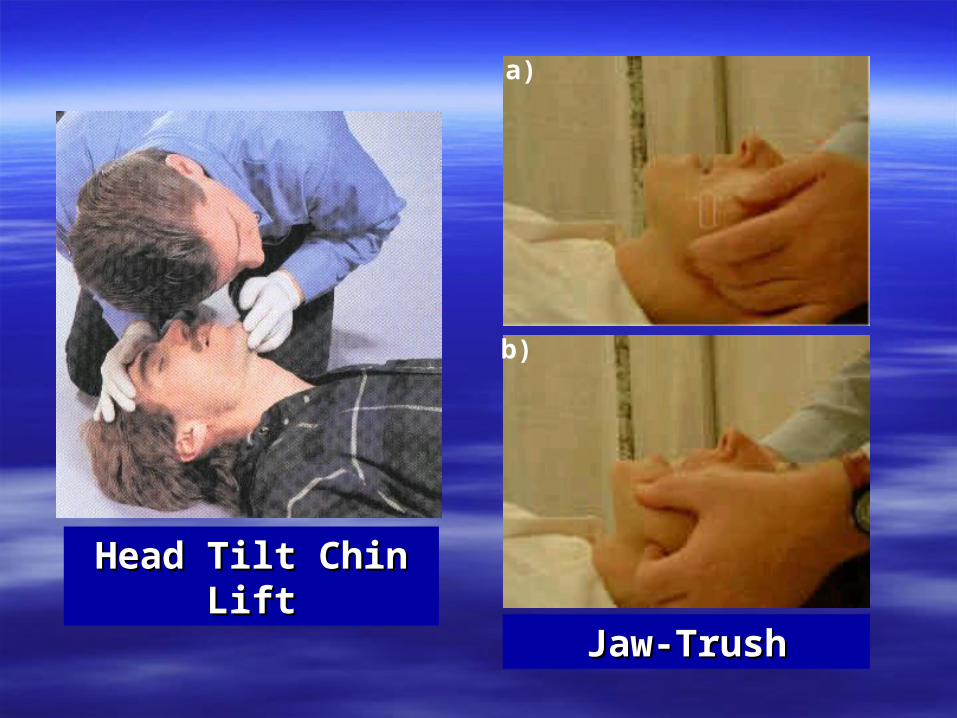
Head Tilt Chin LiftHead Tilt Chin Lift
Jaw-TrushJaw-Trush
a)
b)

The assessment of ventilation The assessment of ventilation (breathing) and airway go hand-in-hand (breathing) and airway go hand-in-hand because their outcome may depend on because their outcome may depend on one another.one another.
1)1) Expose the chestExpose the chest2)2) Determine the rate, depth, symmetry and Determine the rate, depth, symmetry and
regularity of respiration;regularity of respiration; rapid respiratory rate may indicate hypoxia and rapid respiratory rate may indicate hypoxia and
impending respiratory failureimpending respiratory failure Irregular respiration may indicate severe head Irregular respiration may indicate severe head
injuryinjury
D. ASSESSMENT OF VENTILATIOND. ASSESSMENT OF VENTILATION

InspectionInspection

4. Auscultation– air entry– abnormal breath sounds– heart sounds– displaced apical beat
ASSESSMENT OF VENTILATIONASSESSMENT OF VENTILATION
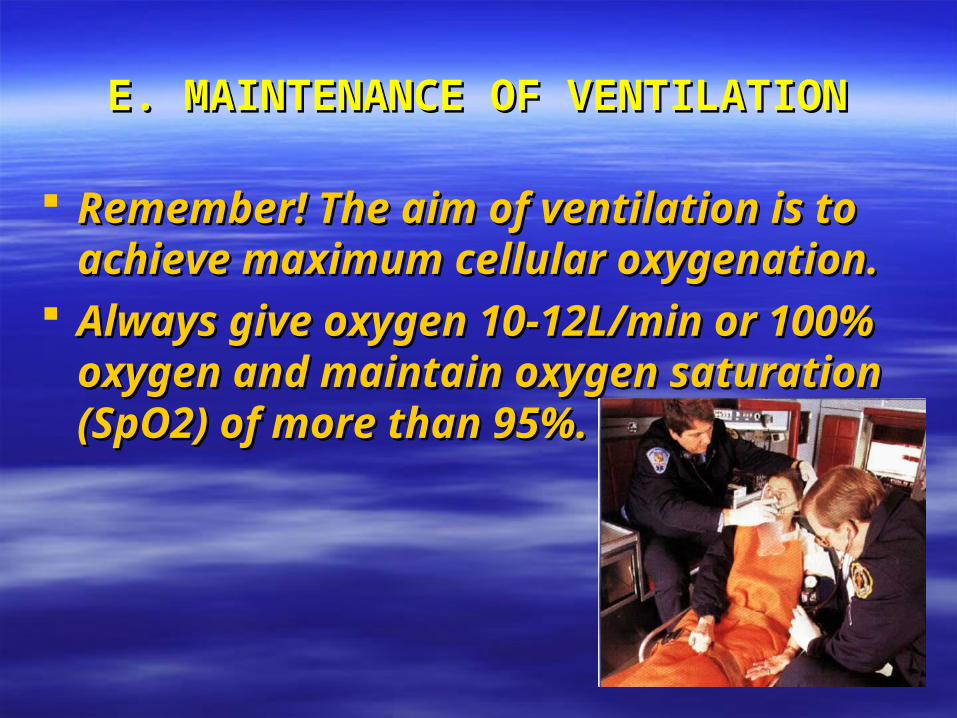
E. MAINTENANCE OF VENTILATIONE. MAINTENANCE OF VENTILATION
Remember! The aim of ventilation is to Remember! The aim of ventilation is to achieve maximum cellular oxygenation.achieve maximum cellular oxygenation.
Always give oxygen 10-12L/min or 100% Always give oxygen 10-12L/min or 100% oxygen and maintain oxygen saturation oxygen and maintain oxygen saturation (SpO2) of more than 95%.(SpO2) of more than 95%.
EAM

INDICATIONS FOR VENTILATIONINDICATIONS FOR VENTILATION
1. Apnoea1. Apnoea
2. Respiratory failure2. Respiratory failure- PaO2 < 60 mmHg- PaO2 < 60 mmHg- PaCO2 > 60 mmHg- PaCO2 > 60 mmHg
3. Severe head injury requiring cerebral 3. Severe head injury requiring cerebral - resuscitation- resuscitation
4. Cardiopulmonary arrest4. Cardiopulmonary arrest
F. DEFINITIVE AIRWAYF. DEFINITIVE AIRWAY
Requires a tube in the trachea with the cuff Requires a tube in the trachea with the cuff inflated and oxygen delivered to the patient.inflated and oxygen delivered to the patient.
The gold standard for a definitive airway is the The gold standard for a definitive airway is the presence of a cuffed endotracheal tube in the presence of a cuffed endotracheal tube in the trachea.trachea.
Achieved by:Achieved by:a) Endotracheal intubationa) Endotracheal intubationb) Surgical airwayb) Surgical airway
- - cricothyroidotomycricothyroidotomy- percutaneous needle - percutaneous needle - surgical- surgical
INDICATIONS FOR DEFINITIVE AIRWAYINDICATIONS FOR DEFINITIVE AIRWAY(ENDOTRACHEAL INTUBATION)(ENDOTRACHEAL INTUBATION)
1.1. Inability to maintain an adequately patent Inability to maintain an adequately patent airway by jaw thrust or oro/nasopharyngeal airway by jaw thrust or oro/nasopharyngeal airway.airway.
2.2. Prevention of aspiration by blood or gastric Prevention of aspiration by blood or gastric content.content.
3.3. Impending or potential airway compromise eg Impending or potential airway compromise eg in maxillofacial injury.in maxillofacial injury.
4.4. Head injury requiring cerebral resuscitation.Head injury requiring cerebral resuscitation.5.5. Failure to maintain adequate oxygenation by Failure to maintain adequate oxygenation by
face mask oxygen supplementation. face mask oxygen supplementation. 6.6. ApnoeaApnoea
Endotracheal Intubation
1.1. Preoxygenate the patient with 100% oxygen.Preoxygenate the patient with 100% oxygen.2.2. Attempts at intubation should not exceed 30 seconds Attempts at intubation should not exceed 30 seconds
and 2 attempts. Get expert help if you are unable to and 2 attempts. Get expert help if you are unable to intubate.intubate.. REMEMBER! IF ONE ENCOUNTERS DIFFICULT OR FAILED REMEMBER! IF ONE ENCOUNTERS DIFFICULT OR FAILED INTUBATION DO NOT CONTINUE THE INTUBATION ATTEMPT INTUBATION DO NOT CONTINUE THE INTUBATION ATTEMPT BUT PROVIDE VENTILATION AND OXYGENATION VIA THE BUT PROVIDE VENTILATION AND OXYGENATION VIA THE BAG-VALVE MASKBAG-VALVE MASK
3.3. Manual in-line stabilisation of the cervical spine must Manual in-line stabilisation of the cervical spine must be maintained at all times in patients with suspected be maintained at all times in patients with suspected cervical spine injury.cervical spine injury.
4.4. ETT size 8 - 9 mm in male and 7 - 8 mm in female.ETT size 8 - 9 mm in male and 7 - 8 mm in female.5.5. Always maintain cricoid pressure until ETT is Always maintain cricoid pressure until ETT is
confirmed confirmed in place.in place.

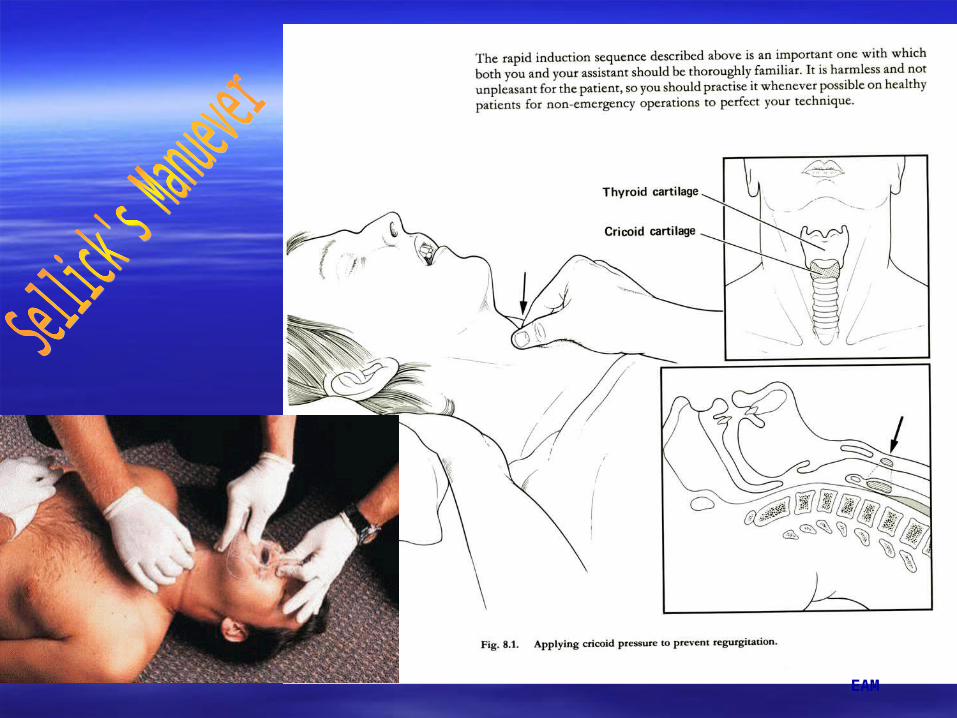
Cricoid PressureCricoid Pressure (Sellick’s Maneuver) (Sellick’s Maneuver)
It is the pressure on the cricoid cartilageIt is the pressure on the cricoid cartilage (requires 10lb of pressure)(requires 10lb of pressure)
Pressure is applied firmly backwards with Pressure is applied firmly backwards with finger and thumbfinger and thumb
The cartilage forms a complete ring and will The cartilage forms a complete ring and will thus occlude the oesophagus preventing thus occlude the oesophagus preventing regurgiregurgittation into the pharynx.ation into the pharynx.
Cricoid pressure is maintained until you have Cricoid pressure is maintained until you have confirmed placement of the ETTconfirmed placement of the ETT
EAM
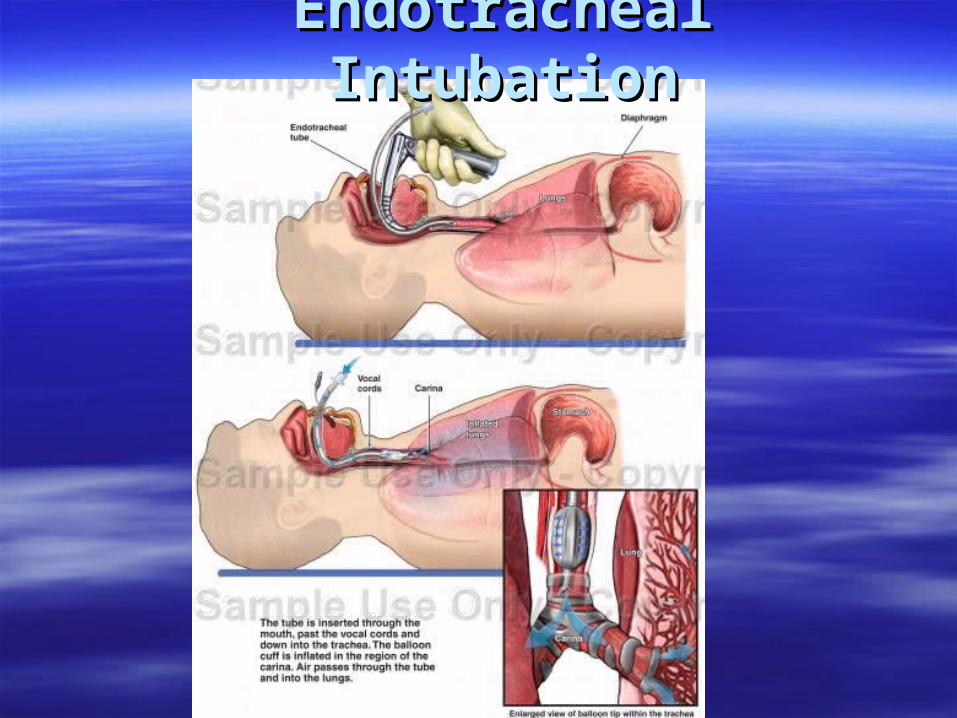
Endotracheal IntubationEndotracheal Intubation
EAM
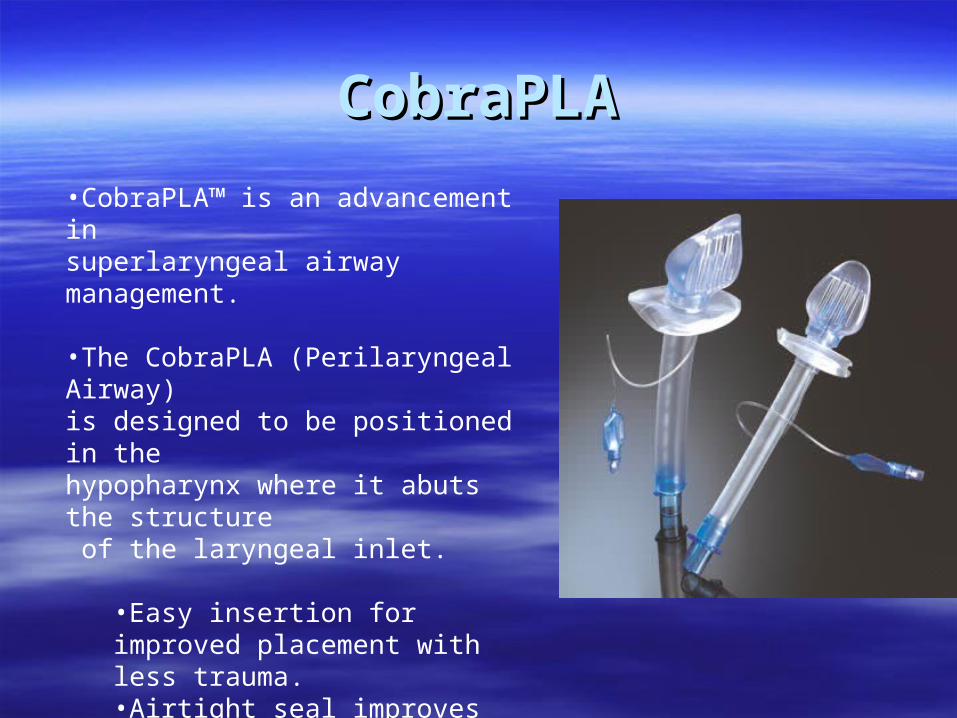
CobraPLACobraPLA
•CobraPLA™ is an advancement in superlaryngeal airway management. •The CobraPLA (Perilaryngeal Airway) is designed to be positioned in the hypopharynx where it abuts the structure of the laryngeal inlet.
•Easy insertion for improved placement with less trauma. •Airtight seal improves positive pressure ventilation. •Eight sizes provide a complete adult and paediatric range.
COMPLICATIONS OF ENDOTRACHEAL COMPLICATIONS OF ENDOTRACHEAL INTUBATIONINTUBATION
1.1. Physiological response ie hypertension, Physiological response ie hypertension, tachycardia, dysrhythmia, increase ICP tachycardia, dysrhythmia, increase ICP and IOP, layngospasm and and IOP, layngospasm and bronchospasm.bronchospasm.
2.2. Oesophageal intubation.Oesophageal intubation.3.3. Endobronchial intubation (usually right Endobronchial intubation (usually right
mainstem)mainstem)4. Failed intubation
EAM

COMPLICATIONS OF ENDOTRACHEAL COMPLICATIONS OF ENDOTRACHEAL INTUBATIONINTUBATION
5. Induction of vomiting leading to aspiration
6. Trauma teeth, lips, tongue, mucosa - dislocation of mandible, arytenoid cartilage
7. Conversion of a cervical spine injury without neurological deficit to one with neurological deficit.

FAILED INTUBATIONFAILED INTUBATION
EAM
• Failed intubation drillFailed intubation drill– CALL FOR HELPCALL FOR HELP– maintain cricoid pressuremaintain cricoid pressure– maintain oxygenation via the bag-valve maskmaintain oxygenation via the bag-valve mask– head down position or lateralpositionhead down position or lateralposition
wait for patient to reawake if sedation is given wait for patient to reawake if sedation is given for intubation.for intubation.
Think of other intubation choices.Think of other intubation choices.– other difficult airway mx technique.

Techniques for Techniques for Failed/Failed/Difficult AirwayDifficult Airway
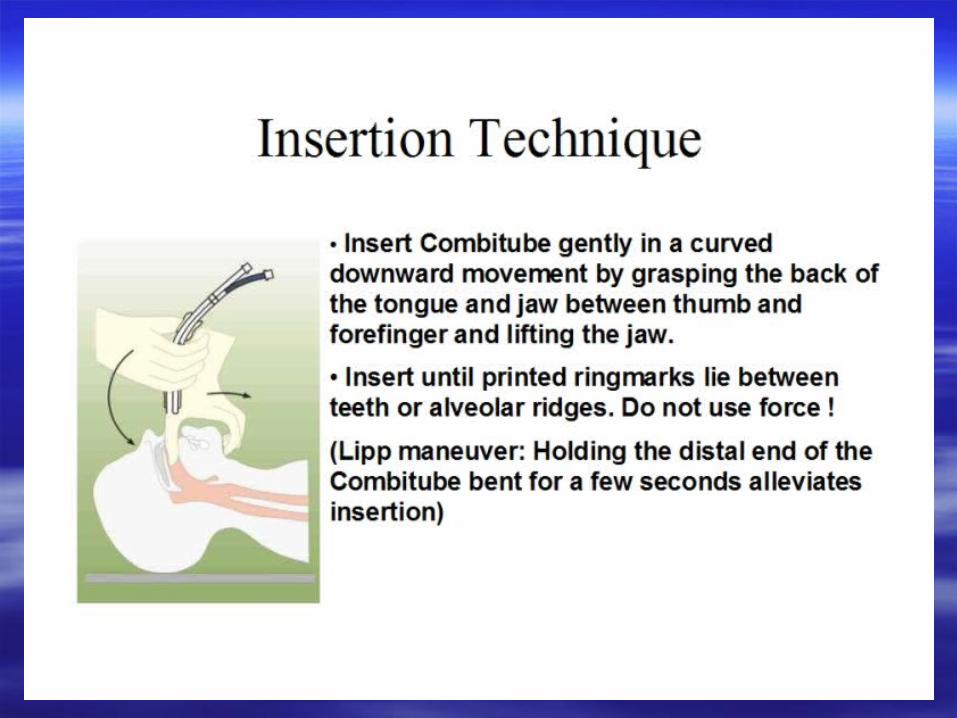
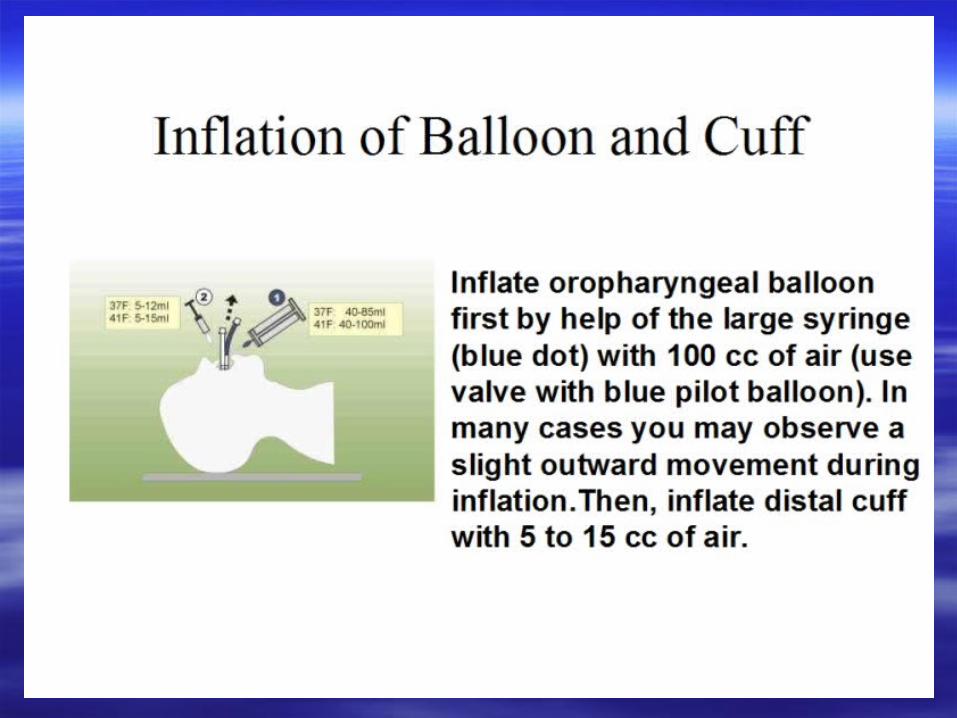
a)a) Non surgicalNon surgical– different laryngoscopic bladesdifferent laryngoscopic blades– FibreopticFibreoptic– illuminating styletilluminating stylet– Combitube (oesophageal tracheal airway)Combitube (oesophageal tracheal airway)– laryngeal masklaryngeal mask/fastrach/laryngeal tube/fastrach/laryngeal tube– retrograde techniqueretrograde technique
b)b) SurgicalSurgical– percutaneous cricothyroidotomypercutaneous cricothyroidotomy– surgical cricothyroidotomysurgical cricothyroidotomy
EAM
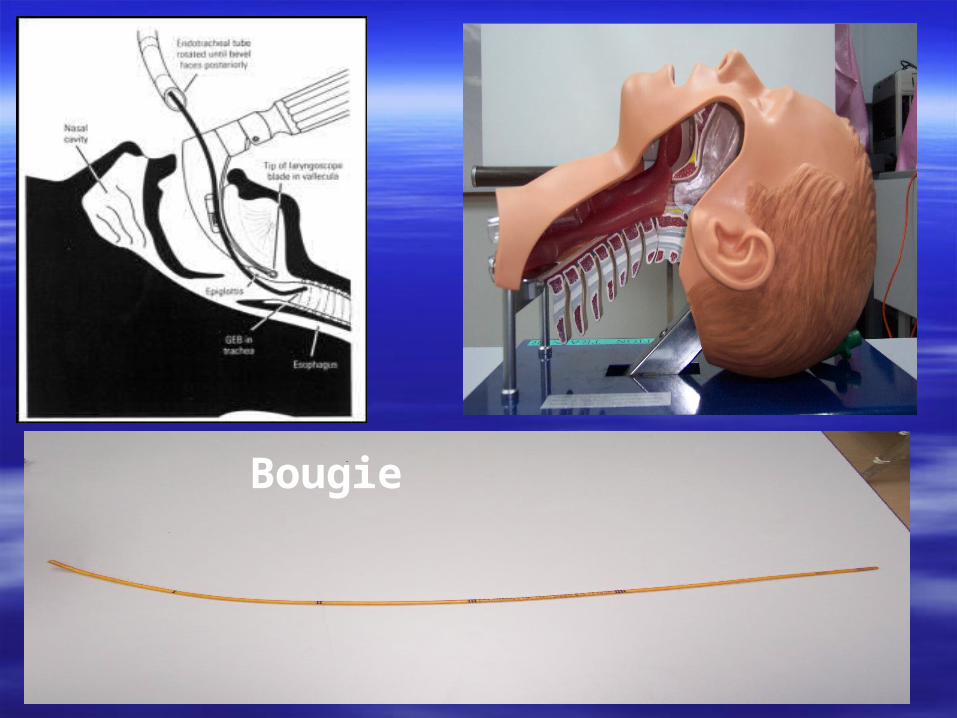
Bougie

ETTETT




EAM
LARYNGEAL TUBE
EAM
SURGICAL AIRWAYSURGICAL AIRWAY
1. Cricothyroidotomy1. Cricothyroidotomy
- percutaneous needle cricothyroidotomy- percutaneous needle cricothyroidotomy
- surgical cricothyroidotomy- surgical cricothyroidotomy
2. Tracheostomy2. Tracheostomy
- too time consuming in the emergency - too time consuming in the emergency
setting. Not usually done.setting. Not usually done.

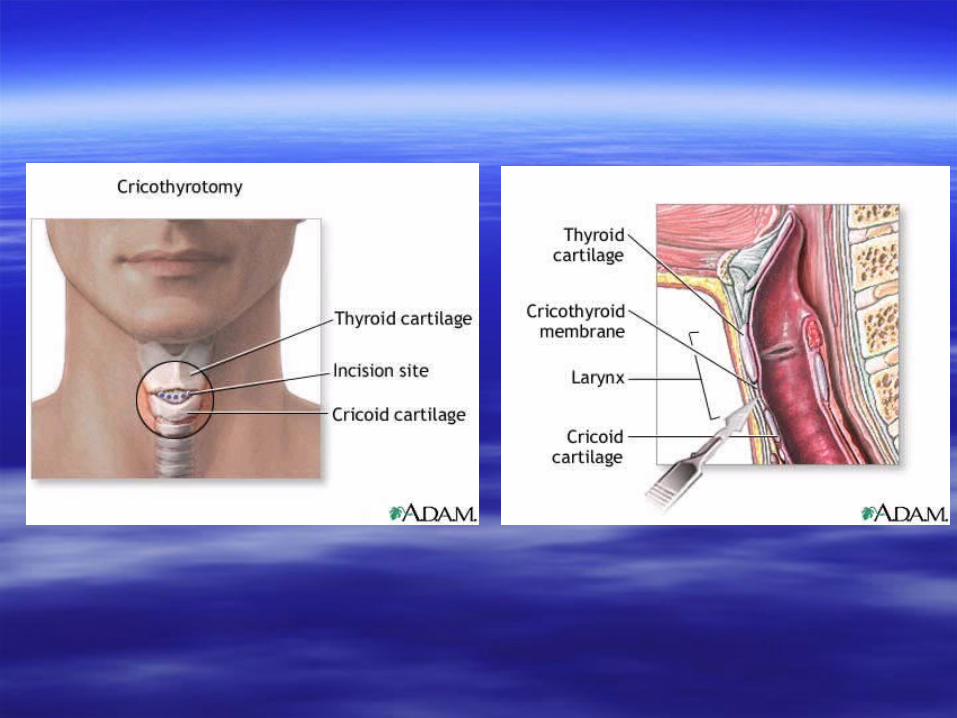
CricothyroidotomyCricothyroidotomy

SURGICAL AIRWAYSURGICAL AIRWAY
- An emergency surgical airway is only indicated - An emergency surgical airway is only indicated when there is an inability to when there is an inability to secure an airwaysecure an airway in the in the presence of an unrelieved airway obstruction.presence of an unrelieved airway obstruction.
- Indications for surgical airway- Indications for surgical airway1. Failure of ETT insertion due to laryngeal 1. Failure of ETT insertion due to laryngeal oedemaoedema2. Severe maxillofacial injury that distorts the2. Severe maxillofacial injury that distorts the anatomyanatomy3. Severe oropharyngeal haemorrhage that 3. Severe oropharyngeal haemorrhage that prevents vocal cord visualisationprevents vocal cord visualisation

Maxilofacial injuryMaxilofacial injury

TracheostomyTracheostomy

LIGHTED STILLETLIGHTED STILLET

VIDEO INTUBATION VIDEO INTUBATION LARYNGEOSCOPELARYNGEOSCOPE

ATLATL

VIDEO LARYNGEOSCOPEVIDEO LARYNGEOSCOPE
EAM
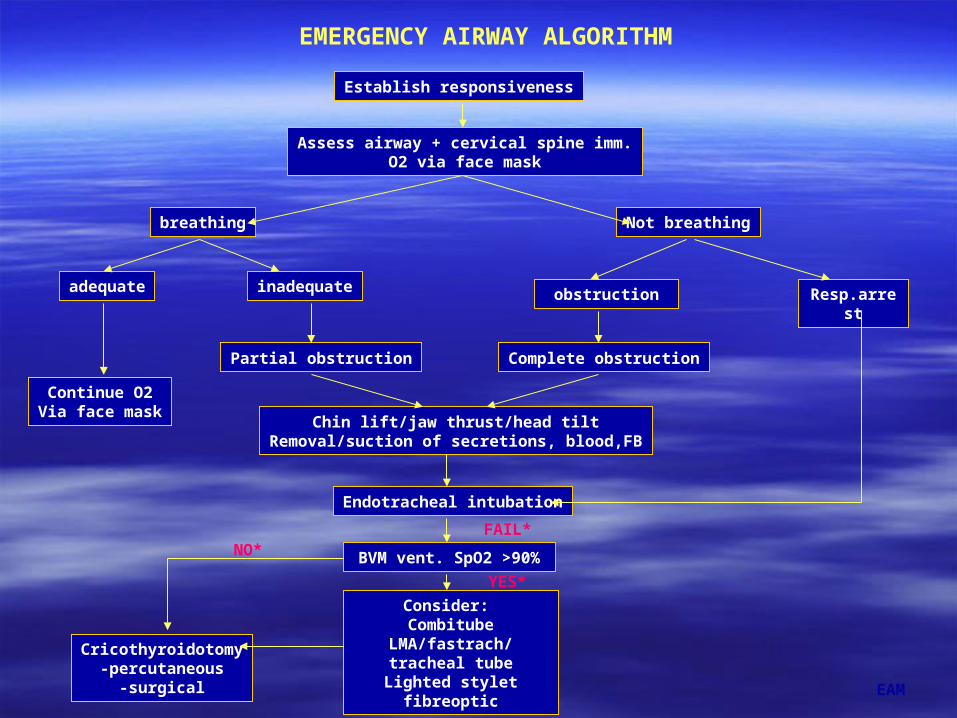
EMERGENCY AIRWAY ALGORITHM
Establish responsiveness
Assess airway + cervical spine imm.O2 via face mask
breathing
adequate inadequate
Continue O2Via face mask
Not breathing
obstruction Resp.arrest
Partial obstruction Complete obstruction
Chin lift/jaw thrust/head tiltRemoval/suction of secretions, blood,FB
Endotracheal intubation
BVM vent. SpO2 >90%
Cricothyroidotomy-percutaneous
-surgical
Consider: Combitube
LMA/fastrach/tracheal tube
Lighted styletfibreoptic
FAIL*NO*
YES*
EAM
SUMMARYSUMMARY
• assessment of the airway, recognising the problem and prompt action to maintain and secure the airway is the first priority in resuscitation
• be prepared for a difficult intubation
IF YOU FAIL TO PLAN, THEN YOU PLAN TO FAIL!

Related Documents