Adolescent Gynecology Mike Guyton, MD Assistant Clinical Professor/Academic Faculty in General Pediatrics

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Adolescent Gynecology
Mike Guyton, MD
Assistant Clinical Professor/Academic Faculty in General Pediatrics
Objectives
• The Pelvic Exam and Vaginal Discharge– Indications and Technique
• Gynecologic Abdominal Pain– Acute vs Chronic
• Dysfunctional Uterine Bleeding– Causes, Eval, and Treatment
• Amenorrhea/Dysmenorrhea– Primary vs Secondary Amenorrhea
– Causes of Dysmenorrhea
• PCOS
• **This Material Represents ~ 4% of the material on the Boards**

The Menstrual Cycle

The Pelvic exam
• Valuable (and necessary) for many reasons• Begin with the Basics!!!
– Vitals, Height, Weight, and Symptoms!!
• Provide explanation of the procedure and devices early in the visit– Sometimes helps to have a diagram of the female anatomy
handy
• Give the adolescent a choice of who can stay in the room
• Position is key for an adequate exam• Your goal is to complete a exam tailored to the
complaint and provide comfort to the patient
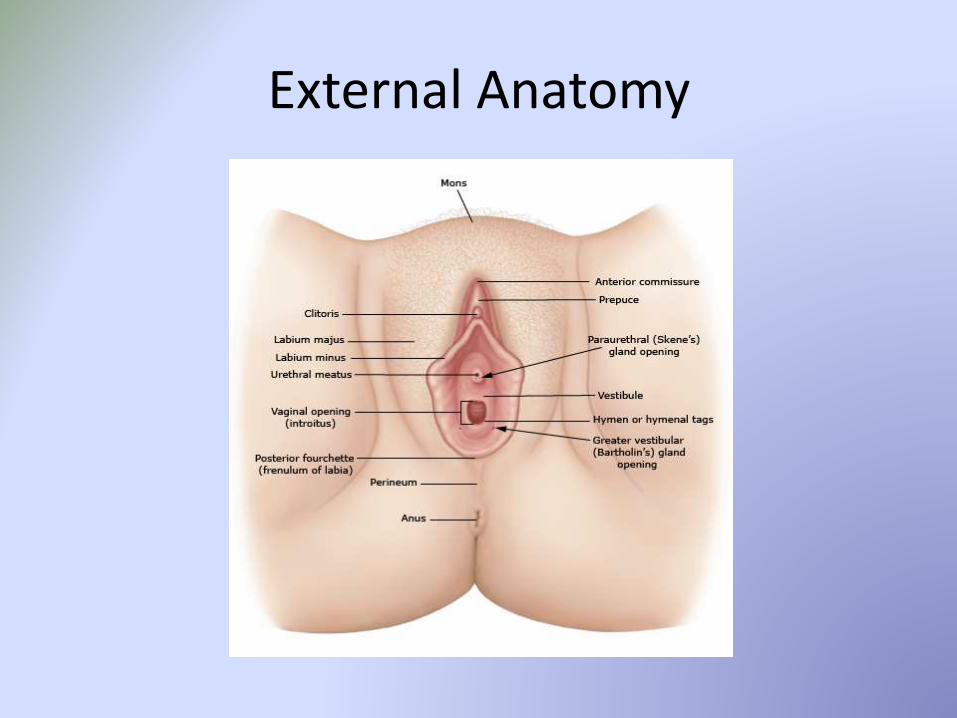
External Anatomy

Indications for Exam
• Cervical Cancer Screening• STI Testing and evaluation• Pregnancy or postpartum• Pain• Discharge• Itching• Swelling• Bleeding• Menstrual Abnormalities• Less common (Trauma, abnormalities of development)

What to look for
• Presence/absence of pubic hair• Clitoral size
– Premenarchal is 3mm
• Configuration of the Hymen• Signs of Estrogenization
– Moist, thick, and dull pink
• Hygiene• Abnormalities from Normal
– Discharge– Discoloration– Trauma– Anatomical Defects
Vaginal Discharge
• Can be physiologic or Inflammatory Leukorrhea
– Physiologic tends to be more clear/slightly yellow and creamy in consistency 2
– Begins at onset of puberty and ends after menopause, due to estrogen influence
• Often, color and consistency are clues to diagnosis
• Important to be able to distinguish which discharge needs which treatment

Adapted from Zitelli Atlas of Pediatric Diagnosis
Physiologic Candida Chlamydia Gonorrhea Trichomonas Bacterial Vaginosis
HSV
Appearance White/Gray/Clear/ Mucoid
White, curdlike, plaques
Mucopus at cervix, clear/bloody discharge
Yellow/greenish discharge
Gray/yellow/green,malodorous, frothy
Gray/white/homogenous, thin
Serous
Vaginal Irritation
None, typically yes Not usual Not usual yes rare yes
pH <4.5 <4.5 variable <4.5 >4.5 >4.5 <4.5
Micro Epithelial cells, lactobacilli, few WBC
WBC’s, pseudohyp-hae with budding yeast
Increased WBC
Greatly increased WBC
Greatly increased WBC, motiletrichomonads
Few WBC, but clue cells present
Greatly increased WBC
Clinical Symptoms
none Itching, dysuria,dy-spareunia
Urethritis, PID, perihepatitis
Urethritis, PID, systemic illness, proctitis
Vulvar itching, prominent dysuria, pelvic discomfort
Fish-like odor LAN, pain
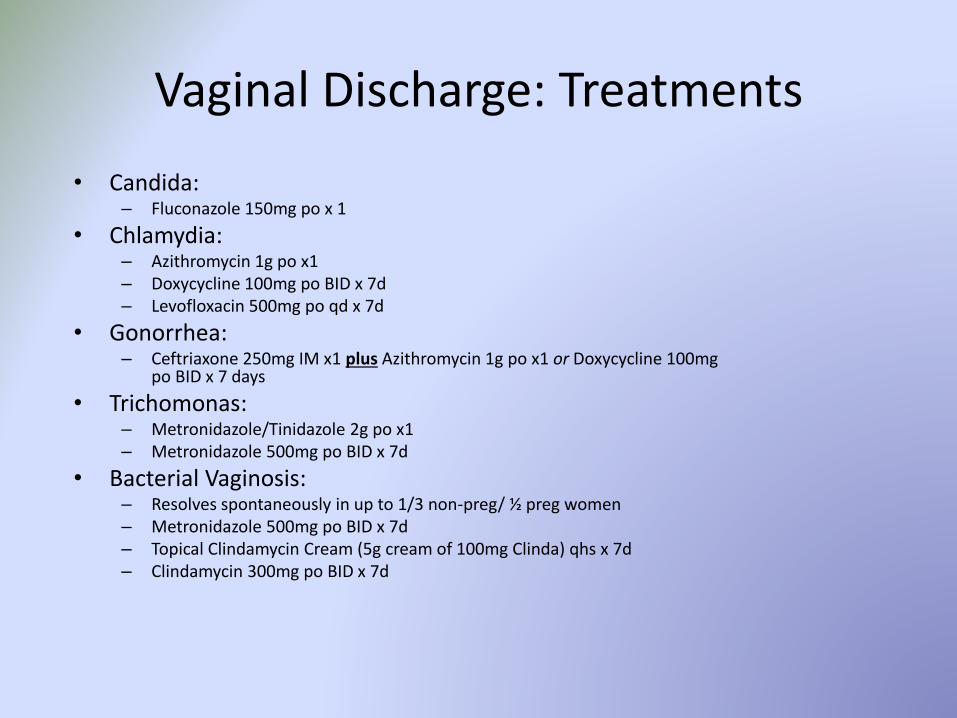
Vaginal Discharge: Treatments
• Candida:– Fluconazole 150mg po x 1
• Chlamydia:– Azithromycin 1g po x1– Doxycycline 100mg po BID x 7d– Levofloxacin 500mg po qd x 7d
• Gonorrhea:– Ceftriaxone 250mg IM x1 plus Azithromycin 1g po x1 or Doxycycline 100mg
po BID x 7 days
• Trichomonas:– Metronidazole/Tinidazole 2g po x1– Metronidazole 500mg po BID x 7d
• Bacterial Vaginosis:– Resolves spontaneously in up to 1/3 non-preg/ ½ preg women– Metronidazole 500mg po BID x 7d– Topical Clindamycin Cream (5g cream of 100mg Clinda) qhs x 7d– Clindamycin 300mg po BID x 7d

Gynecologic abdominal (Pelvic) pain
• Response to many conditions within the body– Distension, stretching, compression, irritation, ischemia,
neuritis, necrosis
• Best classified/discussed as Acute vs Chronic causes
• In pre-pubertal girls, most often involves the GI or Urinary tracts– Gynecologic causes more likely in late adolescence
• Adolescent female with abdominal/pelvic pain warrants a full evaluation and external genital exam, often including a pelvic exam– Indicated for sexually active females


Ovarian Cyst
• Very common between menarche and 18yo– Mature follicles that fail to
ovulate (follicular) or involute (CL)
• Classified as functional vsNon-functional– Functional = part of the
menstrual cycle
• Most asymptomatic and found incidentally– Could cause mentrual irreg.,
pain, urinary frequency, constipation, or pelvic heaviness
Ovarian Cyst Evaluation and Management
• Evaluation
– Detailed menstrual and sexual history• Dysmenorrhea? OCP’s?
– UPT +/- CBC (ie, worried about bleeding)
– Ultrasound• Calcification = think
teratoma
• Management
– Follicular• Usually resolve in 1-2
months
• <6cm = observe +/- OCP
• >6cm = observe vscystectomy (not aspiration!)
– Corpus Luteum• Observe 2wks-3mos (1st
Line) +/- OCP
• Persistent = cystectomy
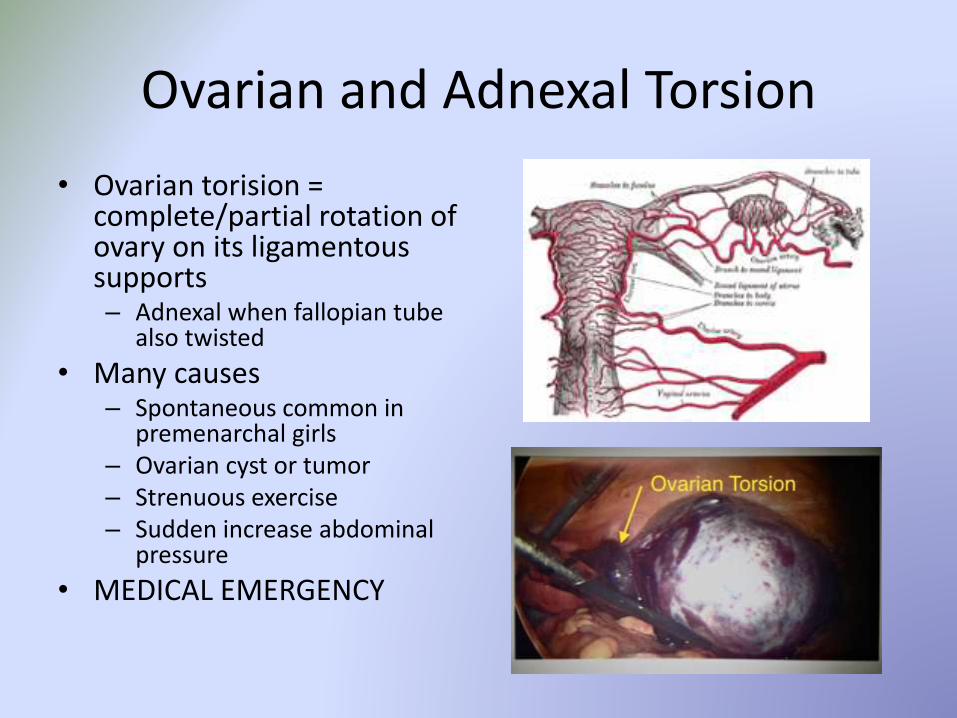
Ovarian and Adnexal Torsion
• Ovarian torision = complete/partial rotation of ovary on its ligamentous supports– Adnexal when fallopian tube
also twisted
• Many causes– Spontaneous common in
premenarchal girls– Ovarian cyst or tumor– Strenuous exercise– Sudden increase abdominal
pressure
• MEDICAL EMERGENCY

Evaluation and Management of Torsion
• Clinical Presentation/Eval– Typical is ACUTE onset of
mod/severe pelvic pain with nausea +/- vomiting with an adnexal mass
– Fever and bleeding sometimes present
– Serum Hcg, CBC, and BMP
– Ultrasound is 1st line DI
• Management– Immediate surgical
intervention• Necrosis possible after
~36 hours
• Now prefer to save rather than remove the ovary
– Can reoccur• High dose OCP’s can help
suppress cyst formation
• Oophoropexy done in children without evidence of mass

Ectopic Pregnancy
• Developing blastocyst implants somewhere other than the uterus
• Incidence ranges from 6-16% and has increased and plateaued since the mid-20th century
• 876 maternal deaths associated with ectopic pregnancy between 1980 and 2007
• Sites of occurrence vary– Almost all occur in the fallopian tube (~98%, most in
the ampullary)– Other sites include: Cervix, Ovary,
Abdominal
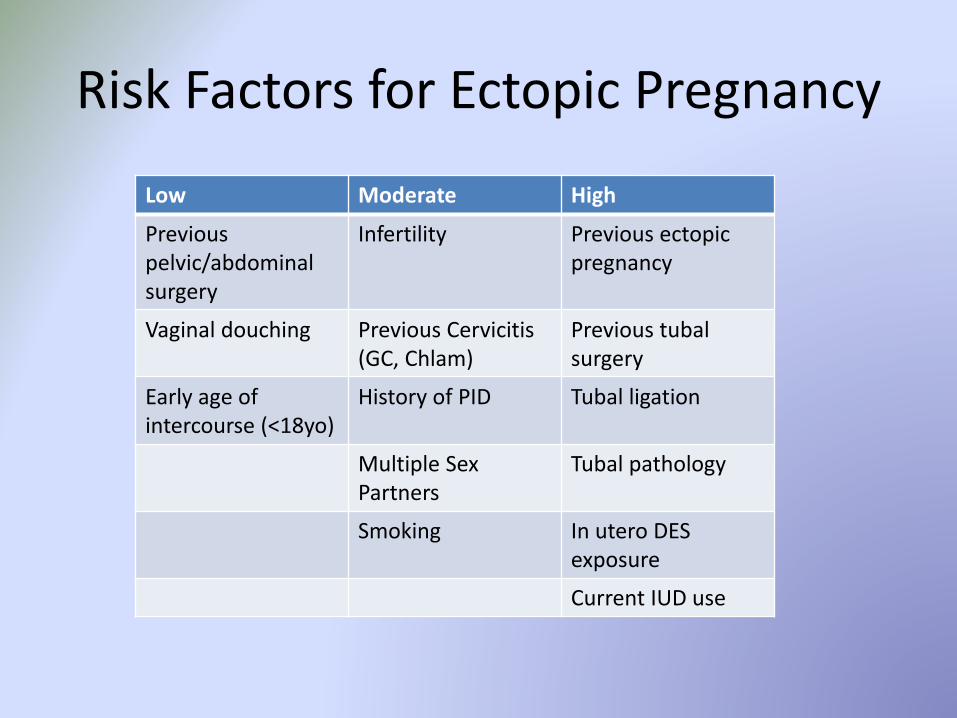
Risk Factors for Ectopic Pregnancy
Low Moderate High
Previous pelvic/abdominal surgery
Infertility Previous ectopic pregnancy
Vaginal douching Previous Cervicitis (GC, Chlam)
Previous tubal surgery
Early age of intercourse (<18yo)
History of PID Tubal ligation
Multiple Sex Partners
Tubal pathology
Smoking In utero DES exposure
Current IUD use

Clinical Presentation
• Most common: 1st trimester vaginal bleeding and/or abdominal pain– Usually 6-8 weeks after LMP– Bleeding quality and quantity varies– Abdominal pain usually pelvic, but quality and timing can vary
• May be ruptured or unruptured at time of presentation, and may even be asymptomatic
• Must be considered in all women of reproductive age who present with vaginal bleeding and/or abdominal pain and:– Are pregnant but IUP not confirmed– Have unknown pregnancy status but amenorrhea >4 weeks
prior to episode– Present with HD instability and an acute abdomen

Evaluation
• Obtain complete history and preform complete physical– Detailed medical/menstrual history, sexual history, and past surgical
history– Complete pelvic exam with bi-manual
• Confirm pregnancy– Serum quantitative HcG level: measured serially every 48-72 hours,
usual doubling time is 1-2 days– HcG that does not rise appropriately can be indicative of an
ectopic/abnormal pregnancy– Transvaginal ultrasound (TVUS)
• Determine location of pregnancy– TVUS
• Further assess stability of patient and consult with appropriate specialists
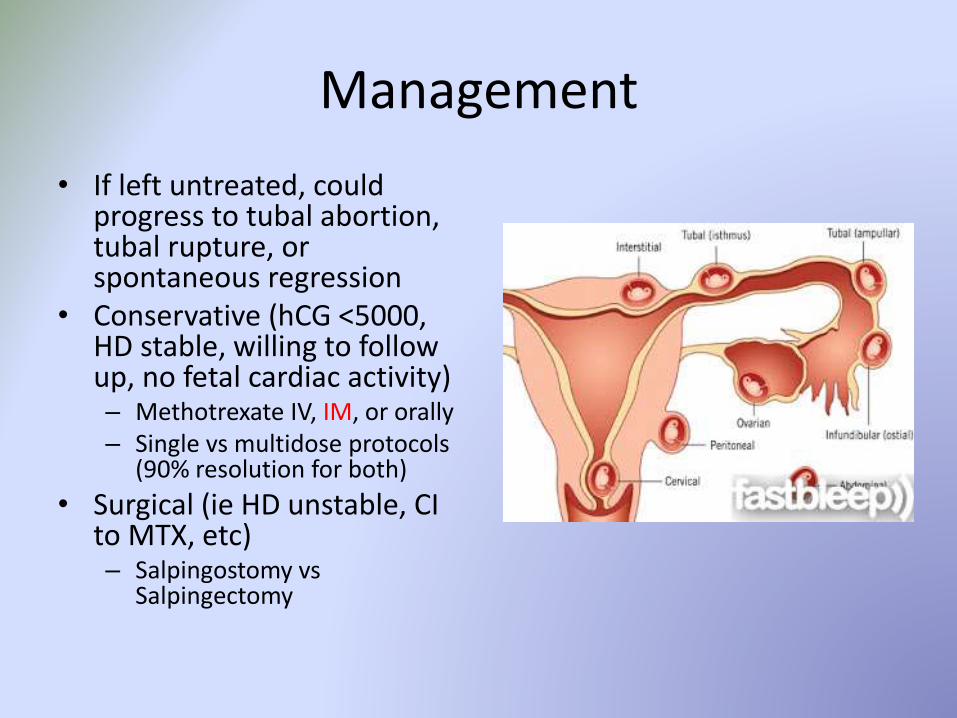
Management
• If left untreated, could progress to tubal abortion, tubal rupture, or spontaneous regression
• Conservative (hCG <5000, HD stable, willing to follow up, no fetal cardiac activity)– Methotrexate IV, IM, or orally– Single vs multidose protocols
(90% resolution for both)
• Surgical (ie HD unstable, CI to MTX, etc)– Salpingostomy vs
Salpingectomy
Chronic Pelvic Pain
• Usually defined as 3-6 months of pain• Prevalence as high as 3.8% in women 15-73yo• For adolescents, can potentially lead to missed school
days and inability to participate in social interactions• Investigation into non-gynecologic organ systems very
important• Often proceeds to laparoscopic investigation and
interventions• Key Point!!!!
– Offer support and empathy, be non-judgmental, and most of all be THOROUGH!!!

Age related incidence of laparoscopic findings in 129 adolescent patients with chronic pelvic pain (Children’s Hospital Boston, 1980-1983)
Number of patients (%)
Diagnosis Age 11-13 Age 14-15 Age 16-17 Age 18-19 Age 20-21
Endometriosis
2 (12) 9 (28) 21 (40) 17 (45) 7 (54)
Postop Adhesions
1 (6) 4 (13) 7 (13) 5 (13) 2 (15)
Serositis 5 (29) 4 (13) 0 (0) 2 (5) 0 (0)
Ovarian Cyst 2 (12) 2 (6) 3 (5) 2 (5) 0 (0)
Uterine Malformation
1 (6) 0 (0) 1 (2) 0 (0) 1 (8)
Other 0 (0) 1 (3) 2 (4) 1 (3) 0 (0)
No Path Found
6 (35) 12 (37) 19 (36) 11 (29) 3 (23)
Reproduced from Pediatric and Adolescent Gynecology 5th Edition, Emans et al

Endometriosis
• Endometrial tissue located at sites outside the uterus– Often discovered incidentally
• Chronic estrogen-dependent disorder, potentially debilitating symptoms– Pelvic pain, dysmenorrhea, dyspareunia, infertility
• Occurs in women of reproductive age (25-25 often)– Rare in pre-pubertal and post-menopausal girls and women
• Negative risk factors and protective factors exist– Negative: Nulliparity, early menarche/late menopause, short
cycles, prolonged menses, mullerian anormalities– Protective: Multiple births, extended intervals of lactation, late
menarche

Endometriosis: Clinical Presentation
• Classic symptoms are Dysmenorrhea (79%), Pelvic pain (69%), dyspareunia (45%), and/or infertility (26%)
• Pain is typically chronic, dull, crampy, and occuring 1-2 days prior to menses, then through menses
• Can occur in the urinary or lower GI tract, leading to bladder/bowel symptoms as well
• ~1/4 of women will present as infertility, 20% as an ovarian mass, or again found completely incidentially.

Endometriosis: Diagnosis
• History and PE– Often no abnormal
findings, but pelvic indicated
– Tenderness in posterior vaginal fornix
• Labs– None useful
• Diagnostics– Pelvic US
• Surgery– Laparoscopy (visual or
histologic diagnosis)

Endometriosis: Treatment
• Chronic condition = lifelong management plan• Expectant Management• Analgesia• Hormonal Therapy
– Combo OCP– GnRH agonists– Progestins– Danazol– Aromatase inhibitors
• Surgery• Combination

Abnormal Uterine Bleeding
• Bleeding that is excessive or occurs outside the normal cyclic menstruation
• Most common cause during initial ~2 years of menstruation is anovulatorycycles
• Specific definitions exist– Duration >8 days– Flow >80ml/cycle (or subjective impression of heavy flow)– Occur >every 24 days or <every 38 days– Intermenstrual bleeding/postcoital spotting– Absence of menses
• Terminology– Amenorrhea– Irregular bleeding– Heavy menstrual bleeding– Acute bleeding

AUB: Specific Board Differential
• Pregnancy Related Bleeding– Threatened abortion (or spontaneous, incomplete, or missed)– Iatrogenic (problems with termination procedures)– Tubal pregnancy
• Pelvic Inflammatory Disease• Endocrinopathies
– Anovulatory Uterine Bleeding– Hyperthyroidism– Adrenal Disorders– Hyperprolactinemia– PCOS– Ovarian Failure
• Coagulopathies– Von Willebrand Disease
AUB: Evaluation
• ALWAYS start with the history and PE– History with and without parent; detailed menstrual history with focus
on symptoms, medical history, medicines, FH, and social factors– External Genital and Pelvic exam, in addition to tanner staging general
PE parameters
• Pelvic Ultrasound– Indicated if PE limited or to evaluate internal structures
(present/absent)
• Laboratory evaluation– UPT– CBC– TSH– Other: Prolactin, type and cross
AUB: Treatment
• Observation and reassurance (mild)• OCP’s
– Combination or Progestin Only– Can be taken as much as TID x 48 hours if moderate-severe bleeding
• Iron Supplements– Often can lead to iron deficiency
• Hemostatic Agents– Desmopressin and Amicar
• Surgery– D&C
• Hospitalization– Hgb<10 + Heavy Bleeding, Initial Hgb <7, or Orthostatic Hypotension

Amenorrhea
• Absence of Menses
• Primary vs Secondary– Primary amenorrhea defined
as the lack of menses by age 15 or 2 years after sexual maturation has occurred
– If no sexual characteristics by age 13, then begin workup
– Short Stature + Amenorrhea (primary or secondary) = THINK TURNER SYNDROME

Causes of Amenorrhea
Primary• Hypothalamic/Pituitary Disease
– Functional Hypothalamic Amenorrhea
• Congenital GnRH Deficiency– Idio. Hypogonadotropic Hypogonadism
• Constitutional Delay of Puberty– Later occurring menses
• Hyperprolactinemia (Rare)• Ovarian etiologies
– Gonadal Dysgenesis– Turner Syndrome– PCOS
• Congenital Anatomic Lesions– Imperforate Hymen– Transverse Vaginal Septum– Vaginal Agenesis
Secondary• PREGNANT UNTIL PROVEN
OTHERWISE!!!!!• Hypothalamic Causes
– Idiopathic/Meds– Endocrinopathies– Stress/Exercise/Eating Disorders– Weight Loss– Chronic Illness– Hypothalmic Failure– PCOS
• Pituitary Causes– Lesions
• Ovarian Causes– Premature Ovarian Failure– Asherman Syndrome
Amenorrhea Work-Up
Primary• Start with Physical Exam
• Uterus Absent:– Karyotype
– Serum Testosterone
• Uterus Present:– Serum hCG
– Serum FSH
• Other– Prolactin
– TSH
– DHEA-S
– 17-alpha-hydroxylase
Secondary
• RULE OUT PREGNANCY– Urine/serum hCG
• Minimal Testing– Prolactin
– FSH
– TSH
• Hyperandrogenism– Morning 17-OH Progesterone
– DHEA-S

Amenorrhea Treatment
Primary
• Education/Counseling
• Cause Specific– Anatomic Lesion/Y
chromosome Material = Surgery
– Primary OF = HRT
– PCOS = TBA/Goal Oriented
– Hypothalamic Amenorrhea = weight gain, stress/exercise modification, GnRH (help infertility issues)
Secondary• Directed at the underlying
pathology• Hypothalamic
– Lifestyle Change– CBT– Leptin Administration (experimental)
• Hyperprolactinemia– Depends on cause and goals
• Premature OF– Estrogen therapy (OCP or HRT)
• PCOS– TBA/Goal Oriented
• Asherman Syndrome– Hysteroscopic lysis of adhesions, long
term estrogen therapy
Dysmenorrhea
• Recurrent, crampy lower abdominal pain during menstruation– Responsible for episodic school absence in girls/young women– Prevalence 60-93% in adolescent females, only 15% seek medical
advice– Does not occur until menstrual cycles are established
• Primary vs Secondary– Primary = no obvious organic disease– Secondary = IUD, PID, Endometriosis, other organic disease
• Pathophysiology– Believed to be caused by excess production of endometrial
prostaglandin F2 alpha– Leads to dysrhythmic uterine contractions and increased muscle tone uterine ischemia
– Also see nausea, vomiting, and diarrhea due to GI tract stimulation

Dysmenorrhea
• Clinical Symptoms– Abdominal Pain (lower quadrant) several hours prior to
menses, lasting for several days
– Nausea, Vomiting, Diarrhea, HA, dizziness, or back pain
– Can impact daily activities
• Treatment– 1st line: NSAID’s
• Ibuprofen, Naproxen
– 2nd line: Birth Control (can combine with NSAID’s)
– Exercise, APAP, healthy diet, and rest are overly ineffective

What’s in a name?
• Pre-Menstrual Syndrome– The occurrence of at least one affective (emotional
labiality, depression) or physical (breast pain, bloating) symptom associated with economic or social dysfunction during the 5 days preceding a menstrual cycle and present in at least 3 cycles
• Pre-Menstrual Dysphoric Syndrome– Symptoms present for most of the preceding year, and 5 or
more of the symptoms being present during the week prior to menses and resolving shortly after menses• Must have significant distress or impairment of daily activities
PMDD: A Psychiatric Diagnosis
1+ must be present
• Mood swings, sudden sadness, increased sensitivity to rejection
• Anger, irritability
• Sense of hopelessness, depressed mood, self-critical thoughts
• Tension, anxiety, feeling on edge
1+ must be present to reach total of 5 symptoms• Difficulty concentrating• Change in appetite, food cravings,
overeating• Diminished interest in usual
activities• Easy fatigability, decreased
energy• Feeling overwhelmed, or out of
control• Breast tenderness, bloating,
weight gain, or joint/muscles aches
• Sleeping too much or not sleeping enough

Polycystic Ovarian Syndrome
• Disorder of the H-P-O System temporary/persistent anovulation and androgen excess
• Requires 2/3 Criterion (2003 Rotterdam Consensus)– Oligo and/or anovulation
– Clinical and/or biochemical signs of hyperandrogenism
– Polycystic Ovaries by US

PCOS
• Very common cause of amenorrhea (Primary and Secondary)• Most common cause of hyperandrogenism in women and girls
– Affects 5-10% of premenopausal girls
• Close association with diabetes– Insulin resistance increased metabolic and cardiovascular risks
• Pathophysiology is unclear– Abnormal H-P function– Abnormal Ovarian function– Abnormal adrenal androgen metabolism– Insulin resistance hyper insulinemic state excessive ovarian
androgen production by theca cells

PCOS: Clinical Symptoms/Diagnosis
• Cutaneous Findings– Hirsutism
• Vs Hypertrichosis
– Acne– Balding
• Ovarian Findings– Anovulation
• Primary/Secondary Amenorrhea, Oligomenorrhea, DUB
– Polycystic Ovaries with pelvic pain
• Metabolic Associations– Obesity– Manifestations of Insulin Resistance
• Acanthosis Nigricans, Metabolic Syndrome, Sleep Disordered Breathing, Nonalcoholic Fatty Liver Disease
PCOS: Treatment
• Hormonal Therapy– Combined OCP or cyclic progestin– GnRH agonist therapy (if unresponsive to above)– Glucocorticoid therapy (non-obese, solely adrenal
hyperandrogenism)
• Metformin– Indication: abnormal glucose tolerance– Reduces insulin concentrations– Promotes ovulation– Lowers androgen levels
• Antiandrogens– Spironolactone (Aldactone), Finasteride (Propecia)
• Weight Loss
Take Home Messages
• Don’t be afraid of the pelvic exam
• More information is better than no information for our patients
• Consider pregnancy in any reproductive age female with abdominal pain or odd presenting symptoms
• Do not underestimate the social or psychological impairments of gynecologic disease

Related Documents











