Adjuvant occupational therapy for work-related major depression works : randomized trial including economic evaluation AART H. SCHENE 1 *, MAARTEN W. J. KOETER 1 , MARTIJN J. KIKKERT 1 , JAN A. SWINKELS 1 AND PAUL M C CRONE 2 1 Department of Psychiatry, Programme for Mood Disorders, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands ; 2 Health Services Department, Institute of Psychiatry, London, UK ABSTRACT Background. Major depression has far-reaching consequences for work functioning and absen- teeism. In most cases depression is treated by medication and clinical management. The addition of occupational therapy (OT) might improve outcome. We determined the cost-effectiveness of the addition of OT to treatment as usual (TAU). Method. Sixty-two adults with major depression and a mean absenteeism of 242 days were randomized to TAU (out-patient psychiatric treatment) or TAU+OT [6 months, including (i) diagnostic phase with occupational history and work reintegration plan, and (ii) therapeutic phase with individual sessions and group sessions]. Main outcome domains were depression, work resumption, work stress and costs. Assessments were at baseline and at 3, 6, 12 and 42 months. Results. The addition of OT to TAU : (i) did not improve depression outcome, (ii) resulted in a reduction in work-loss days during the first 18 months, (iii) did not increase work stress, and (iv) had a 75 . 5 % probability of being more cost-effective than TAU alone. Conclusion. Addition of OT to good clinical practice does not improve depression outcome, improves productivity without increasing work stress and is superior to TAU in terms of cost-effectiveness. INTRODUCTION Depression-related impairments are similar to or even exceed those of common chronic physical illnesses such as diabetes and heart disease (Hays et al. 1995; Musselman et al. 1998). Globally, depression is responsible for 11% of disability caused by illness (Hirschfeld et al. 2000). Disabilities are not only psychological but also physical and social (Ormel et al. 1999) and have a major impact on number of work days lost through disability (Kouzos & Eaton, 1994, 1997). In the USA, depression was responsible for an annual 20 million work cut-back days and 4 million work-loss days (VonKorff et al. 1992; Spitzer et al. 1995; Kessler & Frank, 1997; Druss et al. 2001), with an annual loss of US$17 billion due to work absenteeism and total costs of US$43.7 billion per year (Greenberg et al. 1993). The relationship between symptoms and impairments is equivocal (Ormel et al. 1999; Judd et al. 2000). Longitudinal studies report that depression is associated with an onset of disability, whereas remission is associated with a reduction or disappearance of disability. Randomized trials suggest that treatment of depression can produce an offset of disability in * Address for correspondence: Professor Dr. Aart H. Schene, Department of Psychiatry, Academic Medical Centre, University of Amsterdam (Room A3.254), PO Box 22700, 1100 DE, Amsterdam, The Netherlands. (Email : [email protected]) Psychological Medicine, 2007, 37, 351–362. f 2006 Cambridge University Press doi:10.1017/S0033291706009366 First published online 20 November 2006 Printed in the United Kingdom 351

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Adjuvant occupational therapy for work-relatedmajor depression works: randomized trial including
economic evaluation
AART H. SCHENE 1*, MAARTEN W. J. KOETER 1, MARTIJN J. KIKKERT 1,JAN A. SWINKELS 1
AND PAUL MCCRONE 2
1 Department of Psychiatry, Programme for Mood Disorders, Academic Medical Centre, University ofAmsterdam, Amsterdam, The Netherlands ; 2 Health Services Department, Institute of Psychiatry, London, UK
ABSTRACT
Background. Major depression has far-reaching consequences for work functioning and absen-teeism. In most cases depression is treated by medication and clinical management. The addition ofoccupational therapy (OT) might improve outcome. We determined the cost-effectiveness of theaddition of OT to treatment as usual (TAU).
Method. Sixty-two adults with major depression and a mean absenteeism of 242 days wererandomized to TAU (out-patient psychiatric treatment) or TAU+OT [6 months, including(i) diagnostic phase with occupational history and work reintegration plan, and (ii) therapeuticphase with individual sessions and group sessions]. Main outcome domains were depression, workresumption, work stress and costs. Assessments were at baseline and at 3, 6, 12 and 42 months.
Results. The addition of OT to TAU: (i) did not improve depression outcome, (ii) resultedin a reduction in work-loss days during the first 18 months, (iii) did not increase work stress, and(iv) had a 75.5% probability of being more cost-effective than TAU alone.
Conclusion. Addition of OT to good clinical practice does not improve depression outcome,improves productivity without increasing work stress and is superior to TAU in terms ofcost-effectiveness.
INTRODUCTION
Depression-related impairments are similar to oreven exceed those of common chronic physicalillnesses such as diabetes and heart disease(Hays et al. 1995; Musselman et al. 1998).Globally, depression is responsible for 11% ofdisability caused by illness (Hirschfeld et al.2000). Disabilities are not only psychologicalbut also physical and social (Ormel et al. 1999)and have a major impact on number of workdays lost through disability (Kouzos & Eaton,
1994, 1997). In the USA, depression wasresponsible for an annual 20 million workcut-back days and 4 million work-loss days(VonKorff et al. 1992; Spitzer et al. 1995;Kessler & Frank, 1997; Druss et al. 2001), withan annual loss of US$17 billion due to workabsenteeism and total costs of US$43.7 billionper year (Greenberg et al. 1993).
The relationship between symptoms andimpairments is equivocal (Ormel et al. 1999;Judd et al. 2000). Longitudinal studies reportthat depression is associated with an onsetof disability, whereas remission is associatedwith a reduction or disappearance of disability.Randomized trials suggest that treatment ofdepression can produce an offset of disability in
* Address for correspondence: Professor Dr. Aart H. Schene,Department of Psychiatry, Academic Medical Centre, University ofAmsterdam (Room A3.254), PO Box 22700, 1100 DE, Amsterdam,The Netherlands.(Email : [email protected])
Psychological Medicine, 2007, 37, 351–362. f 2006 Cambridge University Pressdoi:10.1017/S0033291706009366 First published online 20 November 2006 Printed in the United Kingdom
351

specialty care (Mintz et al. 1992a, b) andprimary care patients (Coulehan et al. 1997;Wells et al. 2000). It is less clear whether patientswith more severe types of depression alsorecover from disabilities when they becomeasymptomatic (Ormel, 2000).
Until recently, employment status and thecapacity to work was a sorely neglected topicin the literature on depression (Mintz et al.1992a ; Timbie et al. 2006). This is surprisingbecause the mutual influence is interesting notonly from an economic (depression contributingto disability in the workplace and work loss)but also from a clinical perspective (work im-pairments contributing to depression or main-taining depression). Neuropsychological andinterpersonal consequences of depression maycreate additional stressors for occupationalfunctioning, which may then contribute to itsrecurrent and chronic nature (Keller et al. 1983,1992; Angst, 1988; Judd et al. 1998).
As clinicians, we know that for those patientsfor whom depression is related to impairment inoccupational functioning, recovery may stag-nate if ‘work’ is not part of the treatment plan.For these patients we developed an interventionto restore and improve occupational function-ing. The content is based on literature andclinical expertise suggesting that return to workand/or recovery from depression is more likelywhen the following occur: (1) early assessmentof occupational history, current occupationalproblems and the possibility of returning tothe workplace, (2) education and training withregard to personal performance in the work-place, (3) intervention provided by staff trainedin the relationship between occupational im-pairment and mental disorders, and (4) durationof the intervention of o6 months (Devereaux &Carlson, 1992; Mintz et al. 1992b ; Simon et al.2000; Dixon et al. 2001).
So far no randomized controlled trials (RCTs)have been undertaken to test interventionswith work reintegration as an outcome measure(Goldberg & Steury, 2001; Timbie et al. 2006).We examined whether it is possible to improvethe treatment of depression by focusing ona relevant and specific life domain such aswork. We conducted an RCT of treatmentas usual (TAU) versus treatment as usual plusoccupational therapy (TAU+OT) for patientswith work-related depression. We hypothesized
that addition of OT to TAU would (1) acceler-ate recovery from depression, (2) acceleratework reintegration and (3) not increase workstress.
METHOD
Setting
The study was conducted as part of the Pro-gramme for Mood Disorders of the Depart-ment of Psychiatry of the Academic MedicalCentre in Amsterdam.
Subjects
Inclusion criteria were: age above 18 years,major depressive disorder, single episode orrecurrent, without psychotic features (DSM-IVcriteria ; APA, 1994), no history of psychosis,manic, hypomanic or cyclothymic features, nohistory of active drug or alcohol abuse or de-pendence, a Beck Depression Inventory (BDI)score >15, work reduction of at least 50%of regular hours worked per week because ofdepression, with a minimum of 10 weeks and amaximum of 2 years (after 2 years patients losetheir right to return to their previous employ-ment). We defined work-related depression asa depressive disorder that is predominantlycaused or evoked by stressful psychologicalcircumstances in the workplace. Senior psy-chiatrists estimated clinically if the contributionof work to the onset and/or continuationof depression was >50% of supposed causalfactors. After a complete description of thestudy to the subjects, written informed consentwas obtained.
Procedure
After telephone screening on inclusion criteria,patients received a regular psychiatric evalu-ation (two visits), including a StructuredClinical Interview for the DSM-IV section ofMood Disorders (Jonghe & Huyser, 1994), bytwo trained senior psychiatrists. They againchecked inclusion criteria. Patients who metthe inclusion criteria were then randomlyassigned to TAU or TAU+OT in blocks of 20(10 : 10) by use of computer-generated cardsstored as concealed assignment codes in con-secutively numbered sealed envelopes underthe responsibility of an independent researchassociate.
352 A. H. Schene et al.

Treatments
After randomization, all patients started TAU.Those randomized to TAU+OT also startedthe diagnostic phase of OT.
TAU was the usual out-patient treatmentfor depression. This consisted of clinicalmanagement according to the APA Guideline(APA, 2000) and antidepressants, if indicatedand accepted by patients, according to ourstandardized stepwise drug treatment algor-ithm. Patients were treated by three supervisedsenior psychiatric residents. Visits lasted 30 minevery 2–3 weeks and consisted of symptomassessment, psycho-education, general supportand cognitive behavioural techniques and, ifindicated, medication prescription. Decisionsregarding treatment type, intensity and durationwere made by patients and treating physicians.
TAU+OT included TAU by the same seniorresidents. OT was developed over the previous5 years, pilot tested in an open study of20 patients and found to be effective, acceptableand appreciated. Two skilled occupationaltherapists were the project’s therapists. OTconsisted of three manual-based phases:
Diagnostic phase (4 weeks) : five contactswith a detailed occupational history, videoobservation in a role-played work situation,contact with an occupational physician fromthe patient’s employer and a plan for work re-integration.
Therapeutic phase (24 weeks) : 24 weeklygroup sessions (8–10 patients) and 12 individualsessions. This phase had three subphases: prep-aration of work reintegration, contacting theplace of work, and if possible starting to work.In individual sessions these three phases werefollowed: further analyses of the relationshipbetween work and depression, exploration ofwork problems, and support and evaluation ofwork resumption. Specific individual issuesfrom the group sessions were discussed further.The first half of these 2-hour group sessionswere spent on discussing and exchanging indi-vidual progress. In the second half, seven themeswere discussed successively : being passive, stresson the workplace, personal bounds and limits,being powerful and powerless, perfectionism,conflicts and prevention.
Follow-up phase (20 weeks) : three individualvisits.
Assessment
We measured psychopathology (depression),behaviour (work resumption), work stress, ser-vice use and costs. The study had two phases.Phase I had assessments at baseline (T1), 3 (T2),6 (T3) and 12 months (T4). Phase II was afollow-up at 42 months (T5). Assessments werecarried out by independent researchers whowere as blind as possible to the treatment group.
Process outcomes
We recorded the number of sessions of occu-pational therapy, primary care contacts (onlythose for mental health-care issues), visits tothe psychiatric out-patient department, use ofpsychotropic medications, and days of partial orfull-time psychiatric hospitalization. Qualitativedata on treatment adherence in OT and satis-faction with OT were gathered by a study-specific questionnaire.
Depression outcomes
Depression was assessed by (1) the StructuredInterview for the Diagnosis of DSM-IV MoodDisorders (Jonghe & Huyser, 1994) and (2)the BDI (Beck et al. 1961, 1988), a self-reportmeasure of severity of depressive symptoms(range 0–63).
Work resumption
At baseline, data regarding work before absen-teeism were collected. Work resumption data(dates and amount of work resumption in daysper week and hours per week) were assessed bya study-specific questionnaire at T2, T3, T4and T5. The T5 questionnaire covered 6-monthperiods from 12 to 42 months. We calculated:(1) time till any work resumption, (2) totalhours worked during each 6-month period, and(3) the proportion of patients working at least2 days or 16 hours per week. Decisions aboutwork resumption were made by the patient’soccupational physician.
Work stress
To assess how stressful patients found theirwork, the 11-item Psychic Strains section of theQuestionnaire Organization Stress (QOS) wasadministered. It measures how often people ex-perience specific mental conditions (e.g. feelingfrustrated, irritated, quiet) during work (Caplan
Adjuvant OT for work-related major depression 353

et al. 1975; Reiche & van Dijkhuizen, 1980;Bergers et al. 1986). The total score runs from 0to 4 (no to much strain). At T1 patients assessedthe last period they had worked.
Economic evaluation
We measured mental health-care costs byattaching unit costs to the measures of serviceuse. Budget-based unit costs were calculated foreach patient over a 12-month period (T1–T4).Regarding medication costs, the actual pre-scription of psychotropics over T1–T4 was as-sessed. Medications for non-psychiatric illnesseswere not included. For OT, costs of individualand group sessions were calculated. The value ofwork time was estimated by combining the totalnumber of hours worked during T1–T4 with theaverage hourly Dutch wage (US$36.88). It wasnot possible to collect valid service use dataretrospectively at T5.
Data analysis
Treatment effect of OT was tested using thet test for continuous measures and the x2 test forcategorical variables (using intention-to-treatanalysis). For the longitudinal analysis we usedthe generalized estimating equations (GEE)method (Zeger & Liang, 1986) for dichotomousoutcomes and a generalized linear modelapproach for continuous outcomes (respectivelyPROC GENMOD and PROC MIXED of SAS 9.1;SAS Institute Inc., Cary, NC, USA). Forboth analyses, time and condition effects weredefined as follows: time=effect over timefor pooled TAU and TAU+OT data; con-dition=effect of condition for pooled time data.The timercondition interaction term tests thedifference in development over time betweenTAU and TAU+OT. In both approaches themodel is
Yt=b0+b1X+Sbiti+SbitiX+b3Yb+COV
for models with time as the categorical variable,the first part being the fixed part of the modelwith X (treatment condition) and time (ti)as categorical independent variables, tiX astimertreatment interaction terms and Yb (base-line value of outcome variable) as covariate.The second part is the random part of the model(COV) and covers the dependent characterof the dependent variables by modelling the
covariance structure. For models with timeas the continuous variable this simplifies to
Yt=b0+b1X+b2t2+b3t3X+b4Yb+COV:
For GEE, the COV should be replaced by R (inGEE the correlation between time is modelled).
Both GEE (assuming missing completely atrandom) and PROC MIXED (assuming missing atrandom) give unbiased effect estimates takinginto account missing data. All non-longitudinalanalyses were performed in SPSS version 12.01(SPSS Inc., Chicago, IL, USA).
Because cost data are usually skewed, we useda bootstrapped regression model with 5000resamples. Bootstrapped analyses allow confi-dence intervals (CIs) to be constructed withoutmaking assumptions about the distribution ofthe data. For comparisons of economic data weused 90% CIs.
To assess cost-effectiveness, the value of workminus service costs was calculated for eachpatient. This ‘net benefit’ was then comparedbetween both groups. The treatment optionwith the highest mean net benefit is preferred.However, the wage rate of US$36.88 doesnot necessarily represent the value of an hourworked. Therefore further net benefit analyseswere conducted to combine cost and outcomedata. Again, net benefit was calculated for eachpatient and defined as the number of hoursworked multiplied by value of a working hourand from this the service cost was subtracted.A range of values of an hour worked wasused (US$0 to US$100 in US$10 increments).Bootstrapped regression analysis (5000 rep-etitions) was used to compare the two groupsfor each of the net benefit statistics andthe proportion of regression coefficients thatwere above zero indicated the likelihood thatTAU+OT was more cost-effective than TAU.
RESULTS
Baseline clinical and demographic characteristics(Table 1)
Of the 88 patients (see Fig. 1) who werescreened, 26 were not randomized; 14 did notmeet study criteria [minor relationship betweendepression and work (n=8), working morethan 50% of typical hours worked (n=4),no depression (n=2)], eight started treatment
354 A. H. Schene et al.

elsewhere and four had other reasons (twounknown; one a medical urgency; one had abereavement).
Sixty-two patients were randomized to TAU(n=32) or TAU+OT (n=30). Complete T4data were obtained on 28 (88%) of TAUpatients and on 29 (97%) of TAU+OTpatients. For T5 these figures were 24 (75%) forTAU and 24 (80%) for TAU+OT.
At T1, five (15.6%) TAU patients andseven (23.3%) TAU+OT patients still worked,although significantly less than they used to do(a mean of 15.3 and 17.6 hours per weekrespectively). The other 50 patients had stoppedwork because of depression. There were, onaverage, 242 (S.D.=170) days taken as sicknessleave [TAU patients 225 (S.D.=162) andTAU+OT patients 263 (S.D.=179) days].
Outcome assessment
Depression outcome
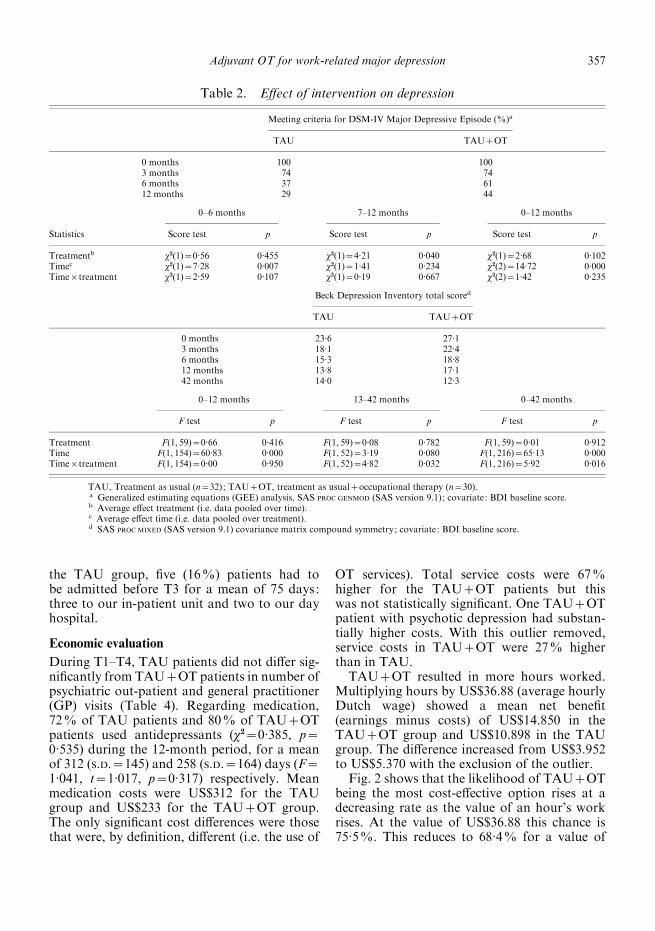
The percentage of patients meeting DSM-IVcriteria for a Major Depressive Episode (MDE)fell from 100% at T1 to 29% at T4 in theTAU group and 44% in the TAU+OT group(Table 2). This recovery was statistically signifi-cant (p=0.000), in particular over the first6 months (p=0.007), but not over the second 6months (p=0.23). It did not differ betweenconditions (p=0.23) (Table 2). The BDI total
score decreased between T1 and T5 from 23.6to 14.0 for TAU and from 27.1 to 12.3 forTAU+OT (Table 2), a significant timercon-dition interaction (p=0.015), which did notshow during the first 12 months (p=0.950), butemerged between months 13 and 42 (p=0.032).
Work resumption
We calculated the time between T1 and themoment of any work resumption for patientswho did not work at T1 (TAU n=27, TAU+OT n=23). For TAU+OT this was a mean of207 days, and 299 days for TAU, a significantdifference [Cox regression, relative risk (RR)=2.71, 95% CI 1.16–6.29, p=0.01]. For the totalpopulation we looked at total hours workedduring each 6-month period up to 42 months.Over the first 18 months (period 1) TAU+OTpatients worked significantly more than TAUpatients (Table 3), which was not the caseduring months 19–42 (period 2). We also calcu-lated for 6-month periods the proportion ofpatients who worked part-time (a mean of atleast 2 days or 16 hours per week) (Table 3). Forthis outcome variable the increase was signifi-cant for both the TAU and the TAU+OTgroups in months 0–18 (p=0.001) but non-significant for months 19–42 (p=0.387). Overmonths 0–18 the timertreatment interactionshowed a trend for significance in favour of the
Table 1. Baseline sociodemographic and clinical characteristics
Characteristic TAU TAU+OT pa
Age, mean (S.D.), years 45.2 (7.5) 46.6 (7.4) 0.48Male, n (%) 15 (47) 15 (50) 0.81Married, n (%) 20 (63) 16 (53) 0.47Living alone, n (%) 9 (28) 12 (40) 0.15Education, n (%) 0.75fHigh school 19 (59) 19 (63)>High school 13 (41) 11 (37)
Employment before illness, hours/week (S.D.) 36.5 (10.4) 36.4 (7.8) 0.97
Baseline clinical statusMajor depressive disorder (MDD), n (%) 0.43Single episode 17 (53) 11 (37)Recurrent, full inter-episode recovery 8 (25) 11 (37)Recurrent, without full inter-episode recovery 6 (19) 5 (17)Chronic 1 ( 3) 3 (10)
MDD severity, n (%) 0.47Mild/moderate 23 (72) 17 (57)Severe 9 (28) 13 (43)
Beck Depression Inventory (BDI) 23.6 (9.1) 27.1 (9.4) 0.15Questionnaire Organization Stress (QOS) 2.7 (0.5) 3.0 (0.6) 0.06
TAU, Treatment as usual (n=32); TAU+OT, treatment as usual+occupational therapy (n=30).a t test independent groups for continuous measures and x2 for percentages and categorical measures.
Adjuvant OT for work-related major depression 355

TAU+OT group (p=0.099). Over the seven6-month periods (months 0–42), the percentagesof patients working part-time in the TAU grouprelative to the TAU+OT group were 11 : 9,15 : 39, 22 : 52, 37 : 52, 37 : 52, 41 : 52 and 41 : 57respectively.
Work stress
With regard to the work stress measure (QOS),two groups of patients were considered: thoseworking a mean of at least half a day (4 h) andthose working at least 2 days (16 h) per weekover a 6-month period. After correction for theinitial QOS score, the QOS for both groupsshowed no increase in work stress betweenT1 and T3 or between T1 and T4. There was nosignificant treatmentrtime interaction.
Service use and qualitative evaluation
Twenty-five patients (83%) completed the OTaccording to protocol. One in seven patientsevaluated the 4-week diagnostic phase of OT asadequate and decided to stop. Of those whocompleted the 24 weeks of OT, one in six foundit too lengthy while half wanted OT to be oflonger duration. Altogether, patients rated OT8.5 on a scale of 1 to 10. The final evaluationshowed no adverse effects of OT.
Two TAU+OT patients (6%) were admittedto the in-patient unit : one (in week 8) for 313days because of a psychotic depression (ex-clusion criterion not clinically manifest duringbaseline evaluation) and another (in week 39)after completing 71 days of OT. One patient leftthe country and was lost to follow-up. Within
T1
T3
T5
T4
88 Patients eligible14 Did not meet inclusion criteria 8 Not randomized 4 Other
32 Assigned to receive treatment as usual (TAU)
30 Assigned to receive treatment as usual + occupational therapy
(TAU + OT)
29 Completed 6-month outcome assessment 30 Completed 6-month outcome assessment
28 Completed 12-month outcome assessment 29 Completed 12-month outcome assessment
1 Lost to follow-up 1 Admitted to in-patient unit 1 Lost to follow-up
32 Received TAU 3 Admitted to in-patient unit 2 Admitted to day hospital 3 Lost to follow-up
25 Received TAU + OT as allocated 4 Received TAU + 4 weeks OT 1 Admitted to in-patient unit
62 Randomized
2 Declined participation 3 Unreachable
4 Declined participation
24 Completed 42-month outcome assessment 24 Completed 42-month outcome assessment
FIG. 1. Trial flow diagram.
356 A. H. Schene et al.
the TAU group, five (16%) patients had tobe admitted before T3 for a mean of 75 days:three to our in-patient unit and two to our dayhospital.
Economic evaluation
During T1–T4, TAU patients did not differ sig-nificantly from TAU+OT patients in number ofpsychiatric out-patient and general practitioner(GP) visits (Table 4). Regarding medication,72% of TAU patients and 80% of TAU+OTpatients used antidepressants (x2=0.385, p=0.535) during the 12-month period, for a meanof 312 (S.D.=145) and 258 (S.D.=164) days (F=1.041, t=1.017, p=0.317) respectively. Meanmedication costs were US$312 for the TAUgroup and US$233 for the TAU+OT group.The only significant cost differences were thosethat were, by definition, different (i.e. the use of
OT services). Total service costs were 67%higher for the TAU+OT patients but thiswas not statistically significant. One TAU+OTpatient with psychotic depression had substan-tially higher costs. With this outlier removed,service costs in TAU+OT were 27% higherthan in TAU.
TAU+OT resulted in more hours worked.Multiplying hours by US$36.88 (average hourlyDutch wage) showed a mean net benefit(earnings minus costs) of US$14.850 in theTAU+OT group and US$10.898 in the TAUgroup. The difference increased from US$3.952to US$5.370 with the exclusion of the outlier.
Fig. 2 shows that the likelihood of TAU+OTbeing the most cost-effective option rises at adecreasing rate as the value of an hour’s workrises. At the value of US$36.88 this chance is75.5%. This reduces to 68.4% for a value of
Table 2. Effect of intervention on depression
Meeting criteria for DSM-IV Major Depressive Episode (%)a
TAU TAU+OT
0 months 100 1003 months 74 746 months 37 6112 months 29 44
Statistics
0–6 months 7–12 months 0–12 months
Score test p Score test p Score test p
Treatmentb x2(1)=0.56 0.455 x2(1)=4.21 0.040 x2(1)=2.68 0.102Timec x2(1)=7.28 0.007 x2(1)=1.41 0.234 x2(2)=14.72 0.000Timertreatment x2(1)=2.59 0.107 x2(1)=0.19 0.667 x2(2)=1.42 0.235
Beck Depression Inventory total scored
TAU TAU+OT
0 months 23.6 27.13 months 18.1 22.46 months 15.3 18.812 months 13.8 17.142 months 14.0 12.3
0–12 months 13–42 months 0–42 months
F test p F test p F test p
Treatment F(1, 59)=0.66 0.416 F(1, 59)=0.08 0.782 F(1, 59)=0.01 0.912Time F(1, 154)=60.83 0.000 F(1, 52)=3.19 0.080 F(1, 216)=65.13 0.000Timertreatment F(1, 154)=0.00 0.950 F(1, 52)=4.82 0.032 F(1, 216)=5.92 0.016
TAU, Treatment as usual (n=32); TAU+OT, treatment as usual+occupational therapy (n=30).a Generalized estimating equations (GEE) analysis, SAS PROC GENMOD (SAS version 9.1); covariate: BDI baseline score.b Average effect treatment (i.e. data pooled over time).c Average effect time (i.e. data pooled over treatment).d SAS PROC MIXED (SAS version 9.1) covariance matrix compound symmetry; covariate: BDI baseline score.
Adjuvant OT for work-related major depression 357

US$20 and to 52.5% when a value of US$10 perhour is used. The probability that TAU+OT isthe most cost-effective option is increased withthe removal of the outlier from the analyses(82.5% at US$36.88).
DISCUSSION
Although depression has a considerableimpact on absenteeism and work loss (Phelanet al. 1991; Lancet, 1998; Claxton et al. 1999;Laitinen-Krispijn & Bijl, 2000), this is, as far aswe know, the first randomized trial evaluatingthe additional effect of OT on TAU with pro-ductivity as an outcome measure (Goldberg &Steury, 2001). Although this small study hasits limitations, it shows that we have to rejectthe first hypothesis : the addition of OT did notaccelerate recovery from depression. We useddifferent methods to measure recovery from
depression – clinician and self-rating (Leon,2001; Thase et al. 2001) – but could not find anydifferences. We did not use a conventional in-terview such as the Hamilton Depression RatingScale (HDRS), which is better for measuringdepressions of greater severity. With the HDRS,stronger effects might have been found.
Although our sample can be described as amore severe population, with long-term de-pression and work absenteeism, the percentageof patients still meeting DSM-IV criteria forMDE at 12 months is in the 30–40% rangedescribed by others on less severe populations(Keitner et al. 1992; Ramana et al. 1995).Between 12 and 42 months, depression severitystabilized in TAU and further reduced inTAU+OT, but we do not place too muchemphasis on this difference. The BDI score atfollow-up showed that a substantial number ofpatients remained symptomatic.
Regarding clinical effectiveness, some pointsneed to be considered. First, for both groupsTAU was of good quality, which might make itdifficult to surpass treatment outcome on thesymptomatic level. Second, OT was not focusedon symptoms but on functioning. From thatpoint of view it would have been surprising tofind a treatment effect on symptoms (Armenianet al. 1998; Paykel & Weismann, 1973). How-ever, others would argue that focusing so in-tensively on a major problem area such aswork is a behavioural intervention for treatingdepression, which should also reduce symptoms(Manninen et al. 1997; Holohan et al. 2000). Ourdata do not, however, support this argument.
We confirmed our second hypothesis : theaddition of OT indeed accelerates and increaseswork resumption. Patients from the exper-imental condition started work approximately3 months earlier. During the first 18 monthssignificantly more TAU+OT patients workedand significantly more worked part-time (atleast 2 days or 16 hours per week). Regardingthe latter, this proportion stabilized from 18 to42 months on 52% in the TAU+OT group,while during that period it increased from 22%to 41% in the TAU group, implying that OThas a long-lasting effect.
Like others, we found that disabilities takemore time to recover than symptoms (Mintzet al. 1992a ; Tweed, 1993; Ormel et al. 1999;Judd et al. 2000). For all patients, symptomatic
Table 3. Effect of intervention on workresumption
Period
Working at least 16 hours per weeka
x2 p
Month 0–18 Treatment b 0.53 0.216Time c 15.81 0.001Timertreatment 6.27 0.099
Month 19–42 Treatment 0.48 0.487Time 3.03 0.387Timertreatment 3.12 0.374
Month 0–42 Treatment 1.34 0.246Time 17.88 0.006Timertreatment 9.56 0.144
Period
Hours worked per 6-month periodd
Median
x2 pTAU TAU+OT
Month 1–6 0.00 20.45 5.24 0.022Month 7–12 0.85 261.75 4.13 0.042Month 13–18 156.42 456.25 4.46 0.035Month 19–24 91.25 456.25 1.42 0.234Month 25–30 0.00 397.58 0.44 0.509Month 31–36 130.35 391.07 1.11 0.293Month 37–42 0.00 404.10 0.62 0.431
TAU, Treatment as usual (n=32); TAU+OT, treatment asusual+occupational therapy (n=30).
a Generalized estimating equations (GEE) analysis, SAS PROC
GENMOD (SAS version 9.1) ; covariate: BDI baseline score.b Average effect treatment (i.e. data pooled over time).c Average effect time (i.e. data pooled over treatment).d Because of the extremely non-normal distribution of hours
worked medians and the median test are presented.
358 A. H. Schene et al.

improvement was stronger during the first6 months of the study, while work resumptioncontinued during the next period. Combiningresults on symptoms and work resumptionshowed that several patients restarted workwhile still symptomatic. At 12 months, the meanBDI score for the total population was stillindicative of a mild depression. To understandthis phenomenon, the distinction within thedepressive syndrome proposed by Mintz et al.(1992a) might be of help. They distinguishedbetween affective impairments (adequacy, dis-interest in the job, being ashamed of one’s work,distress at work) and functional impairments(e.g. absenteeism, poor productivity, inter-personal problems at work). The latter arerelated to a more severe depression whereasthe former can already occur in a mild
Table 4. Cost per capitum (in US dollars) between T1 and T4
VoluminaUnitcosts
Total costs90% CI ofdifferenceTAU TAU+OT TAU TAU+OT
Out-patient treatmentPsychiatric evaluation 2 2 42.5 85 (0) 85 (0) 0 to 0Visit 9.47 10.60 39.2 371 (224) 415 (173) x42 to 128
Occupational therapyIndividual session (45 min) 0 16.63 33.3 0 (0) 554 (229) 481 to 617Group session (120 min) 0 19.24 17.4 0 (0) 335 (169) 280 to 381
Psychotropic medicationa
Actual 312 (303) 233 (211) x207 to 48Imputed drug costs 300 (263) 184 (251) x149 to 34
General practitionerVisit 1.31 2.27 15.8 21 (36) 36 (68) x7 to 39Telephone consultation 0.25 0.17 8.0 2 (11) 1 (4) x4 to 2
Partial/full-time hospitalizationb
Administration 0.16 0.07 609.5 95 (225) 41 (155) x131 to 24Days partial hospitalization 2.91 0.00 79.0 230 (904) 0 (0) x512 to 0Days full-time hospitalization 8.88 12.80 79.0 705 (2.396) 1.017 (4.623) x1.006 to 1.938
ParkingVisits out-patient department 11.47 12.60 1.00 11 (6) 13 (4) x1 to 3Visits occupational therapy 0 55.10 1.00 0 (0) 55 (26) 47 to 62
Travellingc
Visits out-patient department 698.06 766.84 0.10 70 (35) 77 (27) x6 to 20Visits occupational therapy 3350.00 0.10 0 (0) 335 (160) 284 to 379
Total service cost 1.891 (2.619) 3.149 (4.329) x40 to 2.950Earnings 12.777 (23.460) 18.045 (19.017) x3.924 to 13.887Earnings minus cost 10.898 (24.166) 14.850 (20.294) x5.650 to 12.940
Sensitivity analysisd
Total service cost 1.891 (2.619) 2.400 (1.122) x366 to 1.303Earnings 12.777 (23.460) 18.668 (19.040) x3.162 to 14.470Earnings minus cost 10.898 (24.166) 16.268 (19.080) x3.834 to 14.136
CI, Confidence interval ; TAU, treatment as usual (n=32) ; TAU+OT, treatment as usual+occupational therapy (n=30).a Medication: costs of all psychotropic medication prescribed between T1 and T4.b Admissions : TAU: five admissions; TAU+OT: two admissions.c Travelling: volumina in kilometres ; costs in price per kilometre.d The sensitivity analysis was conducted by removing one subject with psychotic depression from the analysis.
0
10
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50 60 70 80 90 100
Value of hour of work ($)
Lik
elih
ood
that
TA
U+
OT
is m
ost
cost
-eff
ectiv
e op
tion
(%)
FIG. 2. Relationship between the value of 1 hour of work (US$) andthe likelihood that treatment as usual plus occupational therapy(TAU+OT) is more effective than TAU alone. –X–, Full sample ;...&..., excluding outlier.
Adjuvant OT for work-related major depression 359

depression. It might be that OT helped patientsto start their work again at the time whenfunctional impairments had more or less disap-peared, although the affective ones were stillthere, while TAU patients postponed this restartjust because affective impairments were stillthere.
Simon et al. (1998) reported that symptomaticchanges may be necessary, but are not sufficient,for improvement in disability and productivity.Depression treatment emphasizing a fasterreturn to productive activities might help toreduce the interval between symptomatic andfunctional recovery. To achieve significantclinical and economic reductions in disability(Stoudemire et al. 1986; Conti & Burton, 1994)may require additional interventions focused onfunctional and behavioural outcomes.
It could be argued that OT is a specific type ofbehavioural therapy focused on functioning inthe workplace. It does not include the cognitivepart of cognitive behavioural therapy (CBT),which might explain why we did not find aneffect on depression. It would be interestingto learn whether a CBT focusing on workfunctioning has better results than the OT westudied. As far as we know such a study has notbeen performed.
A consequence of the earlier work resumptioncould have been a higher level of work-relatedstress in the TAU+OT group (Harding et al.1987; Sauter et al. 1998; Cropley et al. 1999).We did not find that and so confirmed our thirdhypothesis. One possibility is that OT patients,although equally symptomatic, were bettersupported in their coping with work-relatedstressors. We found some evidence for moreadequate and less avoidant coping styles (datanot shown).
Although the benefits of OT have to be seenin terms of an earlier and more satisfactoryreturn to work, it is noteworthy that fewerOT patients had to be admitted for intensivetreatments. A larger study should confirm thistrend. It seems that there is the possibility ofsubstituting more intensive psychiatric treat-ment with OT, which is less stigmatizing andmakes a return to the job market less difficult.A challenging issue for further research wouldbe to assess whether OT reduces the percentageof recurrences of depression because of betterskills and less disruption in someone’s career.
Our 42-month BDI results give some indicationof that.
Others have previously shown the economicbenefit of treating depression, particularly inprimary care patients (Simon et al. 1995, 2001),either in terms of depression-free days or pro-ductivity (Zhang et al. 1999a, b). Our resultssuggest that adding OT to the treatment ofpatients with more severe and longer-lastingdepression can be further improved in terms ofwork days lost (Kessler & Frank, 1997). Theoverall picture showed a median economic gainof about US$4000–5000 per patient, so there arecertainly financial reasons to further investigatethis type of intervention. We showed thatfor TAU+OT to be more cost-effective thanTAU, an hour’s work would need to be valuedat around US$10. This implies that the inter-vention would not be cost-effective for peoplewhose work is valued at less than US$10 perhour. This raises difficult questions of equity.For instance, if the work that someone doesis valued at US$8, should the intervention beprovided? Of course, although some partici-pants will have been paid less than US$10 perhour, the value of their work may well have beenhigher than this amount, and so the number ofparticipants for whom the intervention is notcost-effective may not be high.
Our study has limitations because of the smallnumber of patients and the limited amount offollow-up data, and it would benefit by repli-cation with a much larger population. Given therelatively small sample size, the interpretationof non-significant results, such as those fordepression and depressive symptoms, should becarried out with care. The fact that both theanalysis at syndrome (DSM-IV) and at symp-tom (BDI) level did not show a more favourablecourse for TAU+OT compared to TAU makesit unlikely that using larger samples in the samepopulation and with the same interventionwould have resulted in a statistically significantpositive effect of OT on depression or depressivesymptoms.
Work stress could only be assessed onpatients who had started to work again. Theresults here were tentative and need further re-search, particularly because of the associationbetween that type of stress and coronary heartdisease, hypertension and elevated cortisol con-centrations (Steptoe et al. 2000). We did not
360 A. H. Schene et al.

measure general health services costs, which in alarger replication study should be included.Finally, we could only assess costs over the first12 months.
The qualitative evaluation showed that it isunattractive and sometimes unacceptable thatall RCT patients receive the same treatment(Hotopf et al. 1999). We decided to furtherindividualize OT in three new modules : a4-week diagnostic phase, a 10-week and a26-week module. This evaluation also showedanother clinical limitation: the limited contactbetween TAU and OT staff introduced becausewe wanted to measure the add-on effect objec-tively. Patients evaluated this limited contactnegatively. This is in accordance with recentrehabilitation research that showed that in farmore severe populations, a strong integrationbetween both treatment approaches shows acumulative effect (Drake et al. 1999, 2000).
ACKNOWLEDGEMENTS
We are grateful to Gabe de Vries and MarionAmmeraal for the development and implemen-tation of the occupational intervention. Wethank Drs Jaap van Weeghel, Ronald Blonk,Ingrid Carlier, Jac van der Klink and B. J.Lindeman for their helpful comments on thedesign, intervention, project progress andanalysis and interpretation of data. We are alsograteful to the clinicians and patients who con-tributed their time and effort to the study andto Marianne Haages who contributed so muchto the logistics and administrative progress ofthe trial. This work was funded by LandelijkInstituut Sociale Verzekering (LISV), currentlyUitvoering Werknemersverzekeringen (UWV)Amsterdam, The Netherlands.
DECLARATION OF INTEREST
None.
REFERENCES
Angst, J. (1988). Clinical course of affective disorders. In DepressiveIllness: Predictors of Course and Outcome (ed. T. Helgason andR. J. Daly), pp. 1–44. Springer Verlag: Berlin.
APA (1994). Diagnostic and Statistical Manual of Mental Disorders(4th edn). American Psychiatric Association: Washington, DC.
APA (2000). Practice guideline for the treatment of patientswith major depressive disorder (revision). American PsychiatricAssociation. American Journal of Psychiatry 157 (Suppl.), 1–45.
Armenian, H. K., Pratt, L. A., Gallo, J. & Eaton, W. W. (1998).Psychopathology as a predictor of disability. American Journal ofEpidemiology 148, 269–275.
Beck, A. T., Steer, R. A. & Garbin, M. G. (1988). Psychometricproperties of the Beck Depression Inventory: twenty-five years ofevaluation. Clinical Psychology Review 8, 77–100.
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J. E. &
Erbaugh, J. K. (1961). An inventory for measuring depression.Archives of General Psychiatry 4, 561–571.
Bergers, G. P. A., Marcelissen, F. H. G. & de Wolff, C. J. (1986).VOS-D: Vragenlijst Organisatie Stress [Organization StressQuestionnaire]. Psychologische Laboratorium, Katholieke Uni-versiteit : Nijmegen.
Caplan, R. D., Cobb, S., French, J. R. P., Van Harrison, R. &
Pinneau, S. R. (1975). Job Demands and Worker Health: MainEffects and Occupational Difference, pp. 75–160. US Departmentof Health, Education and Welfare : Washington, DC.
Claxton, A. J., Chawla, A. J. & Kennedy, S. (1999). Absenteeismamong employees treated for depression. Journal of Occupationaland Environmental Medicine 41, 605–611.
Conti, D. & Burton, W. N. (1994). The economic burden of de-pression in a workplace. Journal of Occupational Medicine 36,983–988.
Coulehan, J. L., Schulberg, H. C., Block, M. R., Madonia, M. J. &
Rodriguez, E. (1997). Treating depressed primary care patientsimproves their physical, mental, and social functioning. Archives ofInternal Medicine 157, 1113–1120.
Cropley, M., Steptoe, A. & Joekes, K. (1999). Job strain and psychi-atric morbidity. Psychological Medicine 29, 1411–1416.
Devereaux, E. & Carlson, M. (1992). The role of occupationaltherapy in the management of depression. American Journal ofOccupational Therapy 46, 175–180.
Dixon, L., Goldberg, R., Lehman, A. & McNary, S. (2001). Theimpact of health status on work, symptoms, and functional out-comes in severe mental illness. Journal of Nervous and MentalDisease 189, 17–23.
Drake, R. E., Bond, G. R. & Torrey, W. C. (2000). Psy-chiatry and rehabilitation. Community Mental Health Journal 36,617–619.
Drake, R. E., McHugo, G. J., Bebout, R. R., Becker, D. R.,
Harris, M., Bond, G. R. & Quimby, E. (1999). A randomizedclinical trial of supported employment for inner-city patients withsevere mental disorders. Archives of General Psychiatry 56,627–633.
Druss, B. G., Schlesinger, M. & Allen, H. M. (2001). Depressivesymptoms, satisfaction with health care and 2-year work outcomesin an employed population. American Journal of Psychiatry 158,731–734.
Goldberg, R. J. & Steury, S. (2001). Depression in theworkplace : costs and barriers to treatment. Psychiatric Services52, 1639–1643.
Greenberg, P. E., Stiglin, L. E., Finkelstein, S. N. & Berndt, E. R.
(1993). Economic burden of depression in 1990. Journal of ClinicalPsychiatry 54, 405–418.
Harding, C. M., Strauss, J. S., Hafez, H. & Lieberman, P. B. (1987).Work and mental illness. Toward an integration of the rehabili-tation process. Journal of Nervous and Mental Disease 175,317–326.
Hays, R. D., Wells, K. B., Sherbourne, D. C., Rogers, W. &
Spritzer, K. (1995). Functioning and well-being outcome ofpatients with depression compared with chronic general medicalillnesses. Archives of General Psychiatry 52, 11–19.
Hirschfeld, R. M. A., Montgomery, S. A., Keller, M. B., Kasper, S.,
Schatzberg, A. F., Moller, H. J., Healy, D., Baldwin, D.,
Humble, M., Versiani, M., Montenegro, R. & Bourgeois, M. (2000).Social functioning in depression: a review. Journal of ClinicalPsychiatry 61, 268–275.
Holohan, C. J., Holohan, C. K., Moos, R. H. & Cronkite, R. C.
(2000). Long-term posttreatment functioning among patients withunipolar depression: an integrated model. Journal of Consultingand Clinical Psychology 68, 226–232.
Adjuvant OT for work-related major depression 361

Hotopf, M., Churchill, R. & Lewis, G. (1999). Pragmatic randomisedcontrolled trials in psychiatry. British Journal of Psychiatry 175,217–223.
Jonghe, F. de & Huyser, J. (1994). Diagnosis of Depression:Structured Interview for the Diagnosis of Mood DisordersAccording to DSM-IV. Benecke Consultants : Amsterdam.
Judd, L. L., Akiskal, H. S., Maser, K. D., Zeller, P. J., Endicott, J.,
Coryell, W., Paulus, M. P., Kunovac, J. L., Leon, A. C.,
Mueller, T. I., Rice, J. A. & Keller, M. B. (1998). Major depressivedisorder: a prospective study of residual subthreshold depressivesymptoms as predictor of rapid relapse. Journal of AffectiveDisorder 50, 97–108.
Judd, L. L., Akiskal, H. S., Zeller, P. J., Paulus, M., Leon, A. C.,
Maser, J. D., Endicott, J., Coryell, W., Kunovac, J. L.,
Mueller, T. I., Rice, J. P. & Keller, M. B. (2000). Psychosocialdisability during the long-term course of unipolar major depressivedisorder. Archives of General Psychiatry 57, 375–380.
Keitner, G. I., Ryan, C. E. & Miller, I. W. & Norman, W. H. (1992).Recovery and major depression: factors associated with twelve-month outcome. American Journal of Psychiatry 149, 93–99.
Keller, M. B., Lavori, P. W., Lewis, C. E. & Klerman, G. L. (1983).Predictors of relapse in major depressive disorder. Journal of theAmerican Medical Association 250, 3299–3304.
Keller, M. B., Lavori, P. W., Mueller, T. I., Endicott, J., Coryell, W.,
Hirschfeld, R. M. & Shea, T. (1992). Time to recovery, chronicityand levels of psychopathology in major depression. Archives ofGeneral Psychiatry 49, 809–816.
Kessler, R. D. C. & Frank, R. G. (1997). The impact of psychiatricdisorders on work loss days. Psychological Medicine 27, 861–873.
Kouzis, A. C. & Eaton, W. W. (1994). Emotional disability days:prevalence and predictors. American Journal of Public Health 84,1304–1307.
Kouzis, A. C. & Eaton, W. W. (1997). Psychopathology and the de-velopment of disability. Social Psychiatry and PsychiatricEpidemiology 32, 379–386.
Laitinen-Krispijn, S. & Bijl, R. V. (2000). Mental disordersand employee sickness absence: the NEMESIS study. SocialPsychiatry and Psychiatric Epidemiology 35, 71–77.
Lancet (1998). Prevention and treatment of occupational mentaldisorders [Editorial]. Lancet 352, 999.
Leon, A. C. (2001). Measuring onset of antidepressant action inclinical trials : an overview of definitions and methodology. Journalof Clinical Psychiatry 62 (Suppl. 4), 12–16.
Manninen, P., Heliovaara, M., Ruhimaki, H. & Makela, P. (1997).Does psychological distress predict disability. International Journalof Epidemiology 26, 1963–1970.
Mintz, J., Mintz, L. I. & Arruda, M. J. (1992a). Treatments ofdepression and the functional capacity to work. Archives ofGeneral Psychiatry 47, 761–768.
Mintz, J., Mintz, L. I. & Phipps, C. (1992b). Treatments of mentaldisorders and the functional capacity to work. In Handbook ofPsychiatric Rehabilitation (ed. R. P. Liberman), pp. 290–316.Macmillan Publishing Co. : New York.
Musselman, D. L., Evans, D. L. & Nemeroff, C. B. (1998). Therelationship of depression to cardiovascular disease. Archives ofGeneral Psychiatry 55, 580–592.
Ormel, J. (2000). Synchrony of change in depression and disability.What next? Archives of General Psychiatry 57, 381–382.
Ormel, J., VonKorff, M., Oldehinkel, A. J., Simon, G., Tiemens, B. G.
& Ustun, T. B. (1999). Onset of disability in depressed andnon-depressed primary care patients. Psychological Medicine 29,847–853.
Paykel, E. S. & Weismann, M. M. (1973). Social adjustment anddepression: a longitudinal study. Archives of General Psychiatry28, 659–663.
Phelan, J., Schwartz, J. E., Bromet, E. J., Dew, M. A.,
Parkinson, D. K., Schulberg, H. C., Dunn, L. O., Blane, H. &
Curtis, E. C. (1991). Work stress, family stress and depression inprofessional and managerial employees. Psychological Medicine21, 999–1012.
Ramana, E., Paykel, E. S., Cooper, Z., Hayhurst, M., Saxty, M. &
Surtess, P. G. (1995). Remission and relapse in major depression:a two-year prospective follow-up study. Psychological Medicine25, 1161–1170.
Reiche, H. & van Dijkhuizen, N. (1980). Vragenlijst organisatiestress:testhandleiding deel 1: handleiding voor testafname [OrganizationStress Questionnaire : Test manual part 1]. Katholieke UniversiteitNijmegen: Nijmegen.
Sauter, S. L., Murphy, L. R., Hurrell, J. J. & Levi, L. (1998).Psychosocial and organizational factors. In Encyclopaediaof Occupational Health and Safety, vol. 2 (ed. J. E. Stellman),34.1–34.77. International Labour Organization: Geneva.
Simon, G., Katon, W., VonKorff, M., Lin, E., Robinson, P., Bush, T.,
Walker, E. A., Ludman, E. & Russo, J. (1998). Impact of improveddepression treatment in primary care on daily functioning anddisability. Psychological Medicine 28, 693–701.
Simon, G., VonKorff, M. & Barlow, W. (1995). Health care costs ofprimary care patients with recognized depression. Archives ofGeneral Psychiatry 52, 850–856.
Simon, G. E., Manning, W. G., Katzelnick, D. J., Pearson, S. D.,
Henk, H. J. & Helstad, C. P. (2001). Cost-effectiveness of system-atic depression treatment for high utilizers of general medical care.Archives of General Psychiatry 58, 181–187.
Simon, G. E., Revicki, D., Heiligenstein, J., Grothaus, L., VonKorff,
M., Katon, W. J. & Hylan, T. R. (2000). Recovery from de-pression, work productivity, and health care costs among primarycare patients. General Hospital Psychiatry 22, 153–162.
Spitzer, R., Kroenke, K., Linzer, M., Hahn, S. R., Williams, J. B.,
deGruy 3rd, F. V., Brody, D. & Davies, M. (1995). Health-related quality of life in primary care patients with mental dis-orders. Journal of the American Medical Association 274,1511–1517.
Steptoe, A., Cropley, M., Griffith, J. & Kirschbaum, C. (2000).Job strain and anger expression predict early morning elevationsin salivary cortisol. Psychosomatic Medicine 62, 286–292.
Stoudemire, A., Frank, R., Hedemark, N., Kamlet, M. & Blazer, D.
(1986). The economic burden of depression. General HospitalPsychiatry 8, 387–394.
Thase, M. E., Entsuah, A. R. & Rudolph, R. L. (2001). Remissionrates during treatment with venlafaxine or serotonin reuptake in-hibitors. British Journal of Psychiatry 178, 234–241.
Timbie, J. W., Horvitz-Lennon, M., Frank, R. G. & Normand, S. L.
(2006). A meta-analysis of labor supply effects of interventionsfor major depressive disorder. Psychiatric Services 57, 212–218.
Tweed, D. L. (1993). Depression-related impairment: estimatingconcurrent and lingering effects. Psychological Medicine 23,373–368.
VonKorff, M., Ormel, J., Katon, W. J. & Lin, E. H. B. (1992).Disability and depression among high utilizers of health care.Archives of General Psychiatry 49, 91–100.
Wells, K., Sherbourne, C., Schoenbaum, M., Duan, N., Meredith, L.,
Unutzer, J., Miranda, J., Carney, M. F. & Rubenstein, L. V. (2000).Impact of disseminating quality improvement programs fordepression in managed primary care: a randomized con-trolled trial. Journal of the American Medical Association 283,212–230.
Zeger, S. L. & Liang, K. Y. (1986). Longitudinal data for discreteand continuous outcomes. Biometrics 42, 121–130.
Zhang, M., Rost, K. M. & Fortney, J. C. (1999a). Earnings changesfor depressed individuals treated by mental health specialists.American Journal of Psychiatry 156, 108–114.
Zhang, M., Rost, K. M., Fortney, J. C. & Smith, G. R. (1999b).A community study of depression treatment and employmentearnings. Psychiatric Services 50, 1209–1213.
362 A. H. Schene et al.
Related Documents











