ADHD- and medication-related brain activation effects in concordantly affected parent–child dyads with ADHD Jeffery N. Epstein, 1 B.J. Casey, 2 Simon T. Tonev, 3 Matthew C. Davidson, 2 Allan L. Reiss, 4 Amy Garrett, 4 Stephen P. Hinshaw, 5 Laurence L. Greenhill, 6 Gary Glover, 4 Keith M. Shafritz, 7 Alan Vitolo, 5 Lisa A. Kotler, 6 Matthew A. Jarrett, 3 and Julie Spicer 2 1 Department of Pediatrics, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, USA; 2 Sackler Institute, Weill Medical College of Cornell University, New York, USA; 3 Department of Psychiatry and Behavioral Sciences, Duke University Medical Center, Durham, NC, USA; 4 Department of Psychiatry, Stanford University Medical Center, Palo Alto, CA, USA; 5 Department of Psychology, University of California, Berkeley, CA, USA; 6 Division of Child Psychiatry, Columbia University Medical Center/New York State Psychiatric Institute, New York, USA; 7 Department of Psychology, Hofstra University, Hempstead, NY, USA Background: Several studies have documented fronto-striatal dysfunction in children and adolescents with attention deficit/hyperactivity disorder (ADHD) using response inhibition tasks. Our objective was to examine functional brain abnormalities among youths and adults with ADHD and to examine the relations between these neurobiological abnormalities and response to stimulant medica- tion. Method: A group of concordantly diagnosed ADHD parent–child dyads was compared to a matched sample of normal parent–child dyads. In addition, ADHD dyads were administered double- blind methylphenidate and placebo in a counterbalanced fashion over two consecutive days of testing. Frontostriatal function was measured using functional magnetic resonance imaging (fMRI) during performance of a go/no-go task. Results: Youths and adults with ADHD showed attenuated activity in fronto-striatal regions. In addition, adults with ADHD appeared to activate non-fronto-striatal regions more than normals. A stimulant medication trial showed that among youths, stimulant medication increased activation in fronto-striatal and cerebellar regions. In adults with ADHD, increases in activa- tion were observed in the striatum and cerebellum, but not in prefrontal regions. Conclusions: This study extends findings of fronto-striatal dysfunction to adults with ADHD and highlights the importance of frontostriatal and frontocerebellar circuitry in this disorder, providing evidence of an endophenotype for examining the genetics of ADHD. Keywords: ADHD, adolescence, adulthood, brain imaging, devel- opment, fMRI, methylphenidate, neuropsychology, children, parents. Abbreviations: MTA: Multimodal Treatment Study of ADHD; LNCG: local normative comparison group; CAADID: Conners Adult ADHD Diagnostic Interview for DSM-IV. Attention-deficit/hyperactivity disorder (ADHD) is a common developmental disorder of childhood with a prevalence rate of approximately 5–8% in the US (American Psychiatric Association, 1994; Centers for Disease Control, 2005). ADHD and related impair- ments frequently persist into adolescence and adulthood (Biederman, Mick, & Faraone, 2000; Rasmussen & Gillberg, 2000; Weiss & Hechtman, 1993). Beyond the defining behavioral character- istics of ADHD (i.e., inattention, impulsivity, and hyperactivity), a large neuropsychological literature has documented several areas of cognitive impair- ment. Most notably, deficits in response inhibition (i.e., suppression of a prepotent response in favor of an appropriate response; Nigg, 2001) have been reported for children, adolescents, and adults with ADHD using a variety of neuropsychological tasks (Hervey, Epstein, & Curry, 2004; Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005). Deficits in response inhibition are hypothesized to result from some form of abnormality in the fronto- striatal circuitry in the brains of ADHD patients. Evidence for this hypothesis comes from several sources. First, imaging studies with normal particip- ants clearly demonstrate the role of the prefrontal cortices in tasks involving response inhibition (Casey et al., 1997b; Konishi et al., 1999; Konishi, Nakaj- ima, Uchida, Sekihara, & Miyashita, 1998; Menon, Adleman, White, Glover, & Reiss, 2001; Rubia et al., 2001; Tamm, Menon, & Reiss, 2002). Second, patients with frontal lobe lesions have response inhibition deficits similar to those seen in patients with ADHD (Stuss, Murphy, Binns, & Alexander, 2003). Third, several studies have shown corre- lations between behavioral performance on response inhibition tasks and MRI-based measures of Conflict of interest statement: No conflicts declared. Journal of Child Psychology and Psychiatry 48:9 (2007), pp 899–913 doi:10.1111/j.1469-7610.2007.01761.x Ó 2007 The Authors Journal compilation Ó 2007 Association for Child and Adolescent Mental Health. Published by Blackwell Publishing, 9600 Garsington Road, Oxford OX4 2DQ, UK and 350 Main Street, Malden, MA 02148, USA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ADHD- and medication-related brain activationeffects in concordantly affected parent–child
dyads with ADHD
Jeffery N. Epstein,1 B.J. Casey,2 Simon T. Tonev,3 Matthew C. Davidson,2 AllanL. Reiss,4 Amy Garrett,4 Stephen P. Hinshaw,5 Laurence L. Greenhill,6 Gary
Glover,4 Keith M. Shafritz,7 Alan Vitolo,5 Lisa A. Kotler,6 Matthew A. Jarrett,3
and Julie Spicer21Department of Pediatrics, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, USA; 2Sackler Institute,Weill Medical College of Cornell University, New York, USA; 3Department of Psychiatry and Behavioral Sciences,
Duke University Medical Center, Durham, NC, USA; 4Department of Psychiatry, Stanford University Medical Center,Palo Alto, CA, USA; 5Department of Psychology, University of California, Berkeley, CA, USA; 6Division of Child
Psychiatry, Columbia University Medical Center/New York State Psychiatric Institute, New York, USA; 7Departmentof Psychology, Hofstra University, Hempstead, NY, USA
Background: Several studies have documented fronto-striatal dysfunction in children and adolescentswith attention deficit/hyperactivity disorder (ADHD) using response inhibition tasks. Our objective wasto examine functional brain abnormalities among youths and adults with ADHD and to examine therelations between these neurobiological abnormalities and response to stimulant medica-tion. Method: A group of concordantly diagnosed ADHD parent–child dyads was compared to amatched sample of normal parent–child dyads. In addition, ADHD dyads were administered double-blind methylphenidate and placebo in a counterbalanced fashion over two consecutive days of testing.Frontostriatal function was measured using functional magnetic resonance imaging (fMRI) duringperformance of a go/no-go task. Results: Youths and adults with ADHD showed attenuated activity infronto-striatal regions. In addition, adults with ADHD appeared to activate non-fronto-striatal regionsmore than normals. A stimulant medication trial showed that among youths, stimulant medicationincreased activation in fronto-striatal and cerebellar regions. In adults with ADHD, increases in activa-tion were observed in the striatum and cerebellum, but not in prefrontal regions. Conclusions: Thisstudy extends findings of fronto-striatal dysfunction to adults with ADHD and highlights the importanceof frontostriatal and frontocerebellar circuitry in this disorder, providing evidence of an endophenotypefor examining the genetics of ADHD. Keywords: ADHD, adolescence, adulthood, brain imaging, devel-opment, fMRI,methylphenidate, neuropsychology, children, parents. Abbreviations: MTA:MultimodalTreatment Study of ADHD; LNCG: local normative comparison group; CAADID: Conners Adult ADHDDiagnostic Interview for DSM-IV.
Attention-deficit/hyperactivity disorder (ADHD) is acommon developmental disorder of childhood with aprevalence rate of approximately 5–8% in the US(American Psychiatric Association, 1994; Centers forDisease Control, 2005). ADHD and related impair-ments frequently persist into adolescence andadulthood (Biederman, Mick, & Faraone, 2000;Rasmussen & Gillberg, 2000; Weiss & Hechtman,1993). Beyond the defining behavioral character-istics of ADHD (i.e., inattention, impulsivity, andhyperactivity), a large neuropsychological literaturehas documented several areas of cognitive impair-ment. Most notably, deficits in response inhibition(i.e., suppression of a prepotent response in favor ofan appropriate response; Nigg, 2001) have beenreported for children, adolescents, and adults withADHD using a variety of neuropsychological tasks
(Hervey, Epstein, & Curry, 2004; Willcutt, Doyle,Nigg, Faraone, & Pennington, 2005).
Deficits in response inhibition are hypothesized toresult from some form of abnormality in the fronto-striatal circuitry in the brains of ADHD patients.Evidence for this hypothesis comes from severalsources. First, imaging studies with normal particip-ants clearly demonstrate the role of the prefrontalcortices in tasks involving response inhibition (Caseyet al., 1997b; Konishi et al., 1999; Konishi, Nakaj-ima, Uchida, Sekihara, & Miyashita, 1998; Menon,Adleman, White, Glover, & Reiss, 2001; Rubia et al.,2001; Tamm, Menon, & Reiss, 2002). Second,patients with frontal lobe lesions have responseinhibition deficits similar to those seen in patientswith ADHD (Stuss, Murphy, Binns, & Alexander,2003). Third, several studies have shown corre-lations between behavioral performance on responseinhibition tasks and MRI-based measures ofConflict of interest statement: No conflicts declared.
Journal of Child Psychology and Psychiatry 48:9 (2007), pp 899–913 doi:10.1111/j.1469-7610.2007.01761.x
� 2007 The AuthorsJournal compilation � 2007 Association for Child and Adolescent Mental Health.Published by Blackwell Publishing, 9600 Garsington Road, Oxford OX4 2DQ, UK and 350 Main Street, Malden, MA 02148, USA

prefrontal and striatal regions (Casey et al., 1997a;Hill et al., 2003; Rubia, 2002). Taken together, con-siderable evidence supports fronto-striatal networkabnormalities as contributing to observed behavioraldeficits in response inhibition in ADHD.
Several functional imaging studies have examineddifferences in brain activity between ADHD andnormal participants on response inhibition tasks(Durston et al., 2003; Pliszka et al., 2006; Rubiaet al., 1999; Schulz et al., 2004; Smith, Taylor,Brammer, Toone, & Rubia, 2006; Tamm, Menon,Ringel, & Reiss, 2004; Vaidya et al., 1998). A numberof these studies have shown lower levels of striatalactivation (e.g., caudate nucleus) among childrenwith ADHD relative to controls (Booth et al., 2005;Durston et al., 2003; Rubia et al., 1999; Vaidyaet al., 1998, 2005) . The majority of studies havefound less prefrontal activation in children withADHD (Booth et al., 2005; Rubia et al., 1999; Rubia,Smith, Brammer, Toone, & Taylor, 2005; Smithet al., 2006; Vaidya et al., 2005), although at leastone study has reported the opposite (Durston et al.,2003; Schulz et al., 2004). In those investigationsshowing less prefrontal activity in ADHD, the patternhas been isolated predominantly within the inferiorfrontal gyri (IFG; Booth et al., 2005; Durston,Mulder, Casey, Ziermans, & van Engeland, in press;Rubia et al., 1999; Rubia et al., 2005). This patternof decreased IFG activation has been shown in bothchildren and adolescents with ADHD and hasrecently been reported in medication-naı̈ve childrenwith ADHD on a mental rotation task (Silk et al.,2005). On the other hand, patterns of activation inregions such as the anterior cingulate cortex havebeen mixed, with some groups reporting greateractivity (Pliszka et al., 2006; Schulz et al., 2004) andothers showing less activity (Bush et al., 1999; Rubiaet al., 1999; Tamm et al., 2004) in ADHD samples.
In addition to examining brain activation differ-ences between patients with ADHD and normal re-search participants, the effects of stimulantmedications have also been examined using brainimaging. A review of previous imaging studiesexamining the effects of MPH on brain functionyields mixed results across adult and pediatricsamples. In adults with ADHD, MPH has beenassociated with increased activation in the cerebellarvermis (Schweitzer et al., 2003), right thalamus(Schweitzer et al., 2004), and precentral gyrus(Schweitzer et al., 2004), and decreased activation inthe prefrontal cortex (Schweitzer et al., 2004), pre-central gyri (Schweitzer et al., 2003), right claustrum(Schweitzer et al., 2003), and striatum (Matochik,1994; Schweitzer et al., 2003). These studies haveprimarily used working memory tasks.
In pediatric samples, the pattern of results issomewhat different. Vaidya et al. (1998) found thatstimulants increased frontal activation on aresponse inhibition task in children with ADHD.MPH-related increases in activation in the cerebellar
vermis (Anderson, Polcari, Lowen, Renshaw, & Tei-cher, 2002) and striatum (Shafritz, Marchione, Gore,Shaywitz, & Shaywitz, 2004; Vaidya et al., 1998)have also been noted. However, others have reportedMPH-related decreases in striatal activity (Lee et al.,2005).
Inconsistencies within the literature and acrossdevelopmental stages may result from multiple fac-tors. One reason is the broad range of imagingmethods (e.g., positron emission tomography (PET),functional magnetic resonance imaging [fMRI]) andbehavioral paradigms (e.g., stop signal task, go/no-go task) utilized across studies. In particular, pedi-atric and adult studies are largely different in thatadult studies utilize primarily PET while pediatricstudies have utilized fMRI. To date, no ADHD ima-ging study has used the same behavioral paradigmswith similar imaging methods across pediatric andadult samples.
In addition, the sample composition across studieshas been quite heterogeneous. A wide variety ofinclusion criteria have been used (e.g., multipleADHD subtypes vs. a single ADHD subytpe; requir-ing only past evidence of ADHD symptomatology vs.current ADHD symptomatology; samples withmedication history vs. medication-naı̈ve patients). Todate, samples have been study-specific, serving toincrease heterogeneity within most experimentalsamples. One method for decreasing sampleheterogeneity is to utilize an existing, compre-hensively defined, and well-studied sample, which(a) allows for accurate description of the studysample (e.g., comorbid disorders), (b) documents thepersistence of ADHD symptomatology over time, and(c) ensures common developmental trajectoriesamong the sample. One such existing study sampleincludes the youths who participated in the Multi-modal Treatment Study of ADHD (MTA; MTACooperative Group, 1999). This sample is one of themost well-defined and comprehensively studiedpediatric ADHD samples available.
Because children with ADHD symptoms can pos-sess a variety of genetic and/or non-genetic riskfactors (Biederman, 2005), another method forincreasing homogeneity within an ADHD sample isto utilize a family history of ADHD to select studypatients. Seidman and colleagues (Seidman et al.,1995; Seidman, Biederman, Faraone, Weber, &Ouellette, 1997) have shown that adolescents with afamily history of ADHD have more neuropsycho-logical deficits, particularly on response inhibitionmeasures, than children without such a familyhistory. Selecting participants based on a familyhistory of ADHD has the capability to produce amore biologically-at risk group of ADHD patients,which would serve to increase the power to detectbetween-group differences.
With this method, an innovative study designmay be used in which both youths with ADHD andtheir affected parents are studied. This design
900 Jeffery N. Epstein et al.
� 2007 The AuthorsJournal compilation � 2007 Association for Child and Adolescent Mental Health.

affords examination of ADHD-specific functionaldeficits at two different developmental stages.Behaviorally, symptom patterns change with devel-opment (Biederman et al., 2000). Also, brain mor-phology of key brain regions changes over time(Castellanos et al., 2002). By using both youths andtheir parents, differences across developmentalstages may be qualitatively examined which mayfurther our understanding of the developmentalcourse of ADHD-related brain abnormalities andthe possible developmental changes in the brain’sresponse to stimulant medication.
In the present study, youths from the MTA studyserve as the patient sample, and a matched com-parison group of normal youths recruited as part ofthe MTA study serve as controls. To obtain a two-generation sample, we selected probands based onthe presence of an ADHD diagnosis in both the youthand at least one biological parent. Further, the pres-ent study utilizes both youths and parents as studyparticipants, allowing analyses of between-groupeffects and medication effects at two differentdevelopmental stages. Our chief objectives were toexamine deficits compared to control subjects andmedication-related changes in ADHD-related fronto-striatal brain circuitry using fMRI. Based on previ-ous studies, we predicted between-group differencesin fronto-striatal and frontocerebellar circuits,parietal cortices, and anterior cingulate for theADHD parent–child dyads compared to the controldyads. Stimulant medication was predicted toproduce brain activation changes especially in thestriatal region.
Overall study design
Sample
An initial sample of twenty ADHD youth–parentdyads were recruited from 3 of the 7 geographicalrecruiting sites for the MTA study (i.e., Duke Uni-versity Medical Center, University of California atBerkeley, and New York State Psychiatric Institute).All children in the MTA study received a diagnosisof ADHD, Combined Type at the time of studyrecruitment when children were 7–9 years of age(see MTA Cooperative Group, 1999 for MTA studymethods and total sample description). At the timeof entry into the present study, a DISC-P (version4.0; Shaffer, Fisher, Lucas, Dulcan, & Schwab-Stone, 2000) was administered. Youths were re-quired to meet DSM-IV ADHD diagnostic criteria forany ADHD subtype based on the current DISC to beincluded in the study. Biological parents meetingDSM-IV ADHD criteria using the Conners AdultADHD Diagnostic Interview for DSM-IV (CAADID;Epstein, Johnson, & Conners, 2001; Epstein &Kollins, 2006) were included in the study. Youthsand their parents in both groups were excluded ifthey had an estimated IQ below 80, suffered from
any neurological disease, had a diagnosis of bipolardisorder, psychosis, or pervasive developmentaldisorder, or had any history of head trauma. Forthose participants taking stimulant medication, awashout period (5 multiplied by the half-life of themedication) was required. Participants had to befree of neuroleptic medications for 6 months priorto the study.
Nine healthy control dyads matched to theseADHD youths’ age and sex were recruited from aLocal Normative Comparison Group (LNCG) thathad been recruited for the MTA study (MTACooperative Group, 1999). LNCG children wereliving in the same communities and attending thesame schools as the MTA children at baselineassessment. For the purposes of this study, chil-dren in the LNCG group had to have fewer than 3ADHD symptoms within each DSM-IV ADHDsymptom domain as assessed by the DISC parentreport. In addition, parents in the LNCG groupwere matched on gender to the ADHD parent andwere required to have fewer than 3 symptoms ineach DSM-IV ADHD symptom domain as measuredby the CAADID. All youths and their parents in theLNCG groups met the same exclusion criteriaas those in the MTA group except for diagnosticstatus.
Imaging protocol
After description of the study, written informedconsent was obtained for all subjects. All particip-ants were acclimated to the scanning environmenton the first day of image acquisition using a mockscanner. See Epstein et al. (in press) for a fulldescription of the simulator protocol.
Dyads were scanned on consecutive days. Usinga counterbalanced and double-blinded design, dy-ads were assigned to receive either placebo orimmediate-release methylphenidate on the first dayof image acquisition; dyads received the comple-mentary condition on the second day of imageacquisition. Medication dosage was determinedusing a 0.3 mg/kg formula with a maximum of20 mg. Using this formula, all of the participantsreceived a 20 mg dosage except for two youths whoreceived a 17.5 mg dose. The dosage taken was notnecessarily the optimal dosage for each individualparticipant nor was it necessarily equivalent to thedosage regularly taken by some participants priorto study entry. Functional imaging using thebehavioral paradigm described above beganbetween 60 and 120 minutes after ingestion andended between 100 and 160 minutes after inges-tion. Dyads engaged in the identical behavioralparadigm on both days of image acquisition. Thefunctional images were collected in 28–32 minuteseach session.
The study was approved by Institutional ReviewBoards at each of the participating institutions.
ADHD frontostriatal dysfunction 901
� 2007 The AuthorsJournal compilation � 2007 Association for Child and Adolescent Mental Health.

Behavioral paradigm
The behavioral paradigm was a go/no-go task. Par-ticipants were required to press the response buttonwith the right index finger for each letter that ap-peared on the screen except for the letter X. The taskconsisted of five groups (runs) of 128 trials each run.Each run lasted 5 min, 20 sec. Each letter,approximately 2.5 cm in size, appeared for500 milliseconds with an inter-stimulus interval of2000 ms. The letter ‘X’ occurred on approximately20% of all trials (n ¼ 125), which were presentedrandomly throughout the run. Other letters wererandomly selected from the alphabet.
Performance measures on the go/no-go task weremean reaction time and standard deviation forcorrect go trials, errors of omission, errors of com-mission, and d-prime. The signal detection meas-ure, d-prime, reflects the subject’s perceptualsensitivity to targets; it is the distance between thesignal distribution and noise distribution in stand-ard score units. Higher d-prime values indicatehigher levels of signal detection relative to noise(i.e., better discrimination between targets andnontargets).
Image acquisition and analysis
Subjects were scanned with General Electric 1.5Tesla fMRI scanners (General Electrical MedicalSystems, Milwaukee, Wisconsin) at Duke UniversityMedical Center, Stanford University School of Medi-cine and Cornell University Medical College.1
A whole brain high resolution T1 weighted an-atomic scan (256 · 256 in-plane resolution, 240 mmfield of view; 124 slices at 1.5 mm per slice) wasacquired for each subject for transformation andlocalization of functional data into Talairach space.Functional data were collected with a spiral in-and-out sequence (Glover & Law, 2001) (TR ¼2500 msec, TE ¼ 40 msec, flip angle ¼ 90, FOV ¼240 mm, 64 · 64 matrix). Each volume contained 33oblique slices (3.2 mm thick with 1 mm skip) with anin-plane resolution of 3.75 · 3.75 mm covering theentire brain. Although the time series samplinginterval of TR ¼ 2.5 secs was thus equal to theinterstimulus presentation interval, signal detectionefficiency was not compromised because the average
hemodynamic response delay of 5–6 secs is well-sampled at this rate.
The BrainVoyager QX software package (BrainInnovations, Maastricht, The Netherlands) was usedto perform random effects analyses of the functionaldata. Preprocessing of the functional data involvedthree-dimensional motion detection and correction(spatial alignment of all volumes to the first volumeby rigid transformation) and linear trend removal.Estimated translation and rotation movements wereless than 3 mm for all runs used in the analyses.Subjects who did not have at least 3 runs of usabledata were excluded from the study. Functional datawere co-registered to the anatomic volume by align-ment of corresponding points and manual adjust-ments to obtain registration. Functional data werethen transformed into Talairach space with standardlandmarks and were interpolated to a resolution of1 mm.
Signal values in each time course were normalizedto z-scores representing a change from the meansignal for that run. The signal values for the correctno-go trials were considered to be the effects ofinterest and were modeled with a convolution of anideal boxcar response (assuming a value of 1 for thevolume of the no-go task presentation and a value of0 for the remaining time points) with a linear modelof the hemodynamic response (Boynton, Engel,Glover, & Heeger, 1996). These predictors were usedto build a design matrix for each time course in theexperiment. Only correct trials were included in thematrices and subsequent analyses. Hence, correctno-go trials were contrasted with correct go trials toidentify response inhibition-related activation pat-terns which were compared within groups. A wholebrain analysis was conducted, but contrasts wereexamined only in hypothesized ROIs identifiedbelow.
Three-dimensional statistical maps were gener-ated by assigning an F value to each voxel corres-ponding to the correct no-go trials and calculatedon the basis of the least mean squares solution ofthe GLM. Contrast analyses were then performedbased on t-score differences between the betaweights of this predictor relative to the mean betaweights for that subject. A p level of .05 was usedand multiple comparisons were corrected using acontiguity threshold of 5 acquisition-based voxels(Forman et al., 1995). Analyses were conductedseparately for youths and adults to examinebetween-group and medication effects at two dif-ferent developmental stages. Analyses could not befeasibly conducted combining or comparing thesetwo developmentally different groups due to thenumber of differences between parents and childrenin gender, stimulant medication histories, andmethods of recruitment across the youths and adultgroups (see Table 1) which could result in errone-ous interpretations about developmental differ-ences.
1
In order to ensure comparability across sites, all sites used
identical scanners and software for imaging. Prior to image
acquisition, the same individuals were scanned at all sites in
order to ensure similar signal to noise and contrast to noise
across sites. Further, all sites scanned identical phantoms on a
monthly basis to check and guard against any drift during the
course of the study. Lastly, all data were normalized during
preprocessing to correct for any small signal to noise variations
across site. This cross-site methodology was developed and
based on a similar multi-site functional imaging study (Casey
et al., 1998).
902 Jeffery N. Epstein et al.
� 2007 The AuthorsJournal compilation � 2007 Association for Child and Adolescent Mental Health.
Study #1: Between-group effects
Methods
Subjects. Nine youth–parent dyads who were ran-domly assigned to take placebo on the first day ofscanning and the 9 matched LNCG dyads were usedto test for between-group differences. ADHD dyadswho were randomly assigned to take stimulantmedication on the first day of testing were excludedbecause of the effects ofmedication onbrain function.
Demographic data for the matched ADHD andLNCG groups, including gender, ethnicity, age,handedness, diagnostic status, and comorbid dis-orders, are presented in Table 1. There were no sta-tistically significant differences between the twomatched samples (parents or youths) on gender,ethnicity, age, or handedness (all p values > .2).
Analyses. Participants were required to performwith greater than 70% accuracy on the behavioralparadigm and have less than a voxel (i.e., less than3 mm) of head movement for at least three runs to be
included in the analyses. The 70% accuracy criterionwas derived based on the need to have enough goand no-go trials to obtain a stable hemodynamicresponse function for each of these trial types. Thehalf voxel of motion criterion is based on Krings et al.(2001). The exclusion of one dyad member excludedthe entire dyad from the analyses because ofmatching criteria. As such, 9 ADHD and 9 normalcontrol dyads (n ¼ 36 subjects) described above metthese inclusion criteria. Diagnostic groups werematched on number of runs used in the analysis toprevent differences in statistical power betweengroups.
Awhole brain analysis was conducted, but post hoccontrasts were examined in ROIs that have beenassociated with response inhibition or have beenidentified in previous imaging studies as being dif-ferent between ADHD and comparison groups. Theseareas included the striatum, frontal gyri, anteriorcingulate cortex, cerebellum, and posterior parietalgyrus. In ROIs where between-group differences werepresent, mean beta weights were generated for the
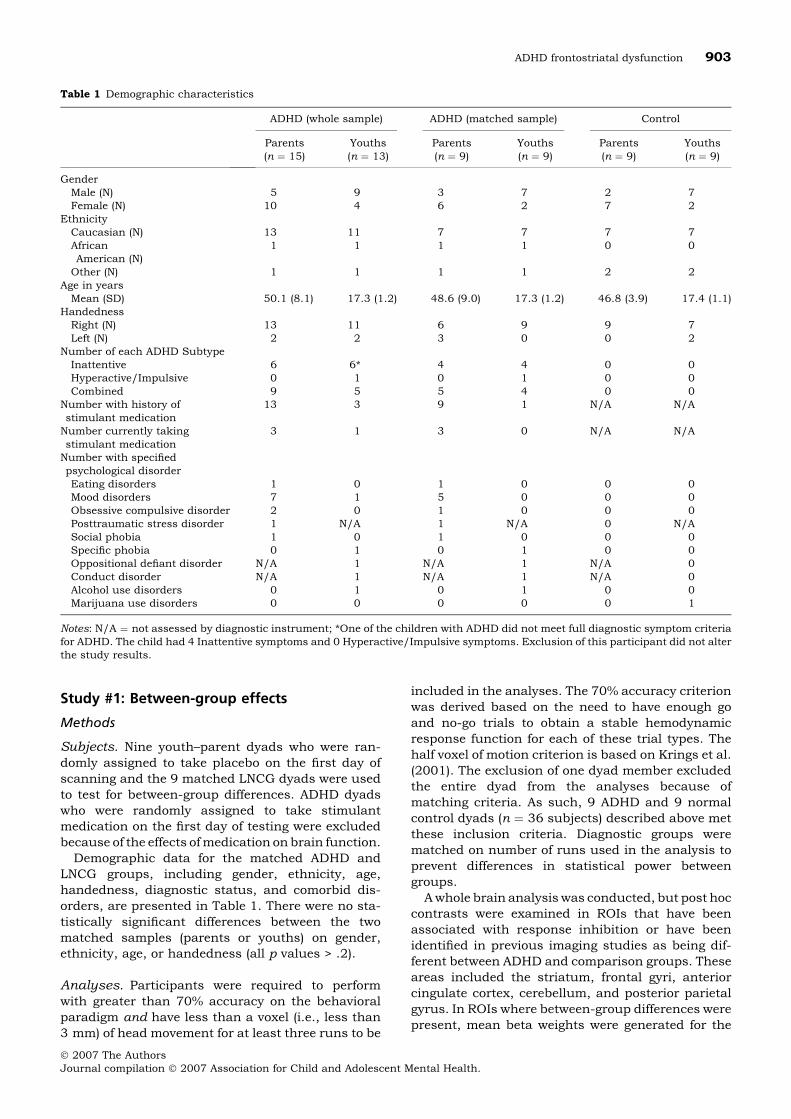
Table 1 Demographic characteristics
ADHD (whole sample) ADHD (matched sample) Control
Parents(n ¼ 15)
Youths(n ¼ 13)
Parents(n ¼ 9)
Youths(n ¼ 9)
Parents(n ¼ 9)
Youths(n ¼ 9)
GenderMale (N) 5 9 3 7 2 7Female (N) 10 4 6 2 7 2
EthnicityCaucasian (N) 13 11 7 7 7 7AfricanAmerican (N)
1 1 1 1 0 0
Other (N) 1 1 1 1 2 2Age in yearsMean (SD) 50.1 (8.1) 17.3 (1.2) 48.6 (9.0) 17.3 (1.2) 46.8 (3.9) 17.4 (1.1)
HandednessRight (N) 13 11 6 9 9 7Left (N) 2 2 3 0 0 2
Number of each ADHD SubtypeInattentive 6 6* 4 4 0 0Hyperactive/Impulsive 0 1 0 1 0 0Combined 9 5 5 4 0 0
Number with history ofstimulant medication
13 3 9 1 N/A N/A
Number currently takingstimulant medication
3 1 3 0 N/A N/A
Number with specifiedpsychological disorderEating disorders 1 0 1 0 0 0Mood disorders 7 1 5 0 0 0Obsessive compulsive disorder 2 0 1 0 0 0Posttraumatic stress disorder 1 N/A 1 N/A 0 N/ASocial phobia 1 0 1 0 0 0Specific phobia 0 1 0 1 0 0Oppositional defiant disorder N/A 1 N/A 1 N/A 0Conduct disorder N/A 1 N/A 1 N/A 0Alcohol use disorders 0 1 0 1 0 0Marijuana use disorders 0 0 0 0 0 1
Notes: N/A ¼ not assessed by diagnostic instrument; *One of the children with ADHD did not meet full diagnostic symptom criteriafor ADHD. The child had 4 Inattentive symptoms and 0 Hyperactive/Impulsive symptoms. Exclusion of this participant did not alterthe study results.
ADHD frontostriatal dysfunction 903
� 2007 The AuthorsJournal compilation � 2007 Association for Child and Adolescent Mental Health.

ROI using activation maps to define the ROI borders.These beta weights were then correlated with the be-havioral measures to examine relations betweenfunctional brain activation and performance.
Results and discussion
Table 2 shows differences between the ADHD andLNCG group’s behavioral performance on the go/no-go task conducted in the scanner. Children withADHD had slower and more variable reaction times(RTs) than children in the LNCG group, but no stat-istically significant differences were found betweenparents with ADHD and parents without ADHD.
Youths with ADHD showed less brain activationthan youths with no history of ADHD during no-gotrials in bilateral middle frontal gyrus (Brodmann’sareas 9 & 46), right inferior frontal gyrus (Brod-mann’s areas 45 & 47), right inferior parietal lobule(Brodmann’s area 40), anterior cingulate (Brod-mann’s area 32), and bilateral caudate nucleus(Figure 1). Youths with ADHD did not show higheractivation compared to LNCG youths in anypre-identified regions of interest.
Parents with ADHD also had less activation thancontrols in right inferior frontal gyrus (Brodmann’sarea 45) and left caudate nucleus. Less activationamong parents with ADHD vs. controls was alsoobserved in the left inferior frontal gyrus (Brod-mann’s area 44). On the other hand, parents withADHD showed more activation in the left inferiorparietal lobule (Brodmann’s area 40) and anteriorcingulate (Brodmann’s area 32) than parents with-out ADHD.2 See Table 3 for regions of interest,maximum t-value, and Talaraich coordinates. SeeTables 6 and 7 for the main effect of condition foreach group separately.3
The relation between behavioral task performanceand corresponding brain activation was examinedusing correlational analyses. Because the trials ofinterest were no-go trials (i.e., inhibition trials), onlyerrors of commission and d-prime were utilized asperformance indicators. Performance on these indic-ators was correlated with individual beta weights foreach individual ROI that was identified in the be-tween-group fMRI analyses. Correlations betweenerrors of commission and the various ROIs inparents and children were all non-significant (all pvalues > .05). However, d-prime was positively cor-related with brain activation in the right inferiorfrontal gyrus in children (r ¼ .47, p ¼ .048; Brod-mann’s area 47) and parents (r ¼ .66, p ¼ .003;Brodmann’s area 45). Scatter plots (see Figure 2) ofthese correlations indicate that the association be-tween right IFG and d-prime was consistent acrossADHD and control youths, but was confined to theADHD participants in the adult sample. D-prime wasalso positively correlated with left caudate nucleusactivation in parents (r ¼ .71, p ¼ .001). Note thathigher values of d-prime indicate better discrimin-ation; hence the more activation in these regions, thebetter the discrimination.
The novel use of concordantly-affected parent–child dyads allowed a cross-sectional examination offronto-striatal abnormalities in manifestations ofADHD at two different ages. We found that youthsdiagnosed with ADHD showed lower brain activationin fronto-striatal regions on a response inhibitiontask than comparison youths. Parents of the ADHDsample who themselves met criteria for ADHDshowed similar fronto-striatal abnormalities to theirchildren as well as some interesting differences.Consistent with research reporting similar neuro-psychological deficits (see reviews by Pennington &Ozonoff, 1996 and Hervey et al., 2004) acrosschildhood and adulthood, these study findings sup-port similar fronto-striatal abnormalities in ADHDpatients across youth and adult samples. Further,because the adults and youths in this sample werebiologically related, the current pattern of resultssuggests a possible biologically-based mechanism oftransmission (i.e., heritability).
Using a family history of ADHD as the basis forinclusion resulted in robust between-group differ-
Table 2 T-test results, means and standard deviations for ADHD and LNCG youths and parents on the behavioral task
Youths Parents
ADHD (n ¼ 9) LNCG (n ¼ 9)Effectsize (d) t-tests
ADHD(n ¼ 9)
LNCG(n ¼ 9)
Effectsize (d) T-tests
Errors of omission 6.44 (8.59) 2.34 (3.03) .64 1.35 7.52 (8.87) 2.10 (3.30) .77 1.72Errors of commission 23.37 (14.95) 19.98 (7.74) .28 .60 10.50 (10.56) 8.78 (9.08) .17 .37Reaction time 439 (69) 352 (30) 1.56 3.44** 450 (52) 440 (85) .14 .30Reaction time SD 157.3 (56.7) 73.3 (22.5) 1.85 4.13*** 120.1 (51.4) 108.5 (35.9) .25 .56D-prime 2.70 (1.03) 3.08 (.61) .43 .96 3.11 (.99) 3.86 (.52) .90 2.01
Note: **p < .01; ***p < .001.
2
Post hoc correlational analysis showed no within-dyad cor-
relation between levels of activation (i.e., beta values) in youths
with levels of activation in their parents (all p values > .05) for
any identified region of interest.3
Whole brain between-group analyses revealed increased right
parahippocampal gyrus (BA 20) and decreased left thalamic
activation for ADHD youths compared to normal controls.
However, these regions did not survive our contiguity thresh-
old. No additional regions of interest were different among
parents in whole brain analyses.
904 Jeffery N. Epstein et al.
� 2007 The AuthorsJournal compilation � 2007 Association for Child and Adolescent Mental Health.

ences in brain activation in our youth sample andalso served to identify at least two regions, leftcaudate nucleus and right inferior frontal gyrus,showing diminished activation among children andparents with ADHD. Right IFG activation was alsocorrelated with performance on the behavioraltask. Indeed, the IFG has been repeatedly found tobe involved in response inhibition tasks amongboth control and disordered populations (see re-view by Aron & Poldrack, 2005). Decreased IFGand caudate activation has also been one of themost consistent ADHD-related findings in fMRIstudies comparing children with ADHD to normal
controls (Booth et al., 2005; Durston et al., 2003;Rubia et al., 1999, 2005; Smith et al., 2006; Vai-dya et al., 1998; Vaidya et al., 2005). Also, a recentstudy report (Sowell et al., 2003) and a review ofthe structural literature (Swanson, Castellanos,Murias, LaHoste, & Kennedy, 1998) demonstratesignificant structural differences in right IFGbetween children with and without ADHD. Giventhese past and current findings, IFG functionalactivation seems to be a candidate endophenotypein examining phenotype-genotype relations inADHD. Indeed, Durston et al. (in press) haveshown a similar concordance in IFG functional
The right side of the image corresponds to the left side of the brain.
Figure 1 Diagnosis-based activation differences (control–ADHD) during response inhibition for parent and youthparticipants. For parents, controls show significantly greater activation than ADHD participants in left caudatenucleus and bilaterally in inferior frontal gyrus whereas ADHD participants show greater activation in anteriorcingulate and precuneus. For youths, controls show greater activation in anterior cingulate, right inferior frontalgyrus, and bilaterally in caudate nucleusa
Table 3 Regions of interest showing significant differences in brain activation between ADHD and normal controls
Region of interest Brodmann’s area
Talairachcoordinates
Contrast t-value Maximum Volume (mm3)x y z
YouthMiddle frontal gyrus –R 46/9 21 46 31 Control>ADHD 3.59 421L 46/9 )21 48 33 Control>ADHD 4.93 747
Inferior frontal gyrus (R) 47 32 43 4 Control>ADHD 3.91 1150Anterior cingulate 32 -2 37 31 Control>ADHD 4.21 6533Inferior frontal gyrus (R) 45 34 18 4 Control>ADHD 3.77 896Caudate nucleus –R 10 1 16 Control>ADHD 3.71 302L )13 5 15 Control>ADHD 3.06 364
Inferior parietal lobule (R) 40 42 )43 42 Control>ADHD 4.95 1858ParentsAnterior cingulate 32 )7 33 21 ADHD>Control )2.82 229Inferior frontal gyrus –R 45 38 24 15 Control>ADHD 2.94 154L 44 )45 11 12 Control>ADHD 3.47 960
Caudate nucleus (L) )7 13 16 Control>ADHD 4.03 620Inferior parietal lobule (L) 40 )47 )67 27 ADHD>Control )3.35 937Precuneus 7 0 )70 33 ADHD>Control )4.15 3107
ADHD frontostriatal dysfunction 905
� 2007 The AuthorsJournal compilation � 2007 Association for Child and Adolescent Mental Health.

abnormalities among children with ADHD and theirunaffected siblings.
Although some brain regions showed similar pat-terns of activity across youths with ADHD and theirparents, the parents had fewer regional differencesfrom the control parents than did their children withrespect to control children. In addition, some brainregions showed higher activation in the parents withADHD versus the control parents. The differentpattern of neurofunctional deficits across youthsand adults is quite interesting and raises the ques-tion of whether such disparities are evidence of adevelopmental phenomenon or, rather, an artifact ofthe experimental methods used for this study. Therewere several characteristics that differentiated theyouth and adult ADHD samples in this study. Mostnotably, adults were less likely to have receivedmedication for ADHD. Furthermore, parents in thestudy were recruited based on their child’s ADHDstatus; as a result, the non-referred adult ADHDsample used in this study may have been lessseverely impaired than the child sample and possiblyless severe than adult ADHD samples used in pre-vious studies. There were also differences betweenthe youth and adult samples in terms of genderdistribution (more males in youth sample), presenceof mood disorders (more mood disorders in the adultsample), history of stimulants (lower usage in theadult sample), and equality of handedness acrossADHD and control groups (not a matching variable).Any or all of these variables can be consideredconfounds in inferring developmental differencesfrom our results. However, in regard to a history ofstimulant usage as a confound, at least three fMRIstudies using medication-naı̈ve children with ADHDhave shown activation differences in similar regionsof interest as those reported in this paper (e.g., IFG;
Rubia et al., 2005; Silk et al., 2005; Smith et al.,2006).
It appears that adults with ADHD may recruitalternative brain regions to perform task-relatedinhibition. Namely, task-related activation in theanterior cingulate was higher for parents with ADHDthan control parents. Coupled with the absence ofbetween-groups behavioral deficits, it may be thatthe adults with ADHD are relying on alternative brainregions to successfully inhibit responses during thetask. Recruitment of the anterior cingulate cortexmay be an attempt to recruit attentional mechanismsto improve performance (Peterson et al., 1999), per-haps related to response conflict or error monitoring.Interestingly, the finding of increased anterior cin-gulate cortex activity during successful no-go trials isconsistent with results reported by Pliszka et al.(2006) using a pediatric sample. However, Bush et al.(1999) report lower activation in anterior cingulatecortex for adults with ADHD when performing aCounting Stoop task. Our finding of increased acti-vation in anterior cingulate cortex on a behavioralinhibition task should be treated with caution giveninconsistency across paradigms.
Another developmental difference was the lateral-ity of observed activation differences across youthsand adults. Neurobiological models and previousfindings largely support a right-lateralized deficitamong patients with ADHD (see review by Giedd,Blumenthal, Molloy, & Castellanos, 2001). In ouryouth sample, most of the differences in brain acti-vation were right lateralized and for those thatappeared on the left (e.g., MFG, caudate), there werecorresponding differences on the right side. For theadults, however, deficits were observed predomin-antly on the left side (i.e., lower activation in caudatenucleus and IFG). These findings may suggest
Youths Parents
r=.4 5
r=.45 r=.82
r=-.15
Overall r=.47, p<.05 Overall r=.66, p<.01
Figure 2 Correlations (and associated regression lines) between d-prime and right inferior frontal gyrus beta valuesoverall, and as a function of diagnostic group (ADHD, control) for both parent and youth participants
906 Jeffery N. Epstein et al.
� 2007 The AuthorsJournal compilation � 2007 Association for Child and Adolescent Mental Health.

involvement of bilateral fronto-striatal circuitry inresponse inhibition, rather than simple right later-alization of this function due to strategic differences(e.g., use of language to help refrain from making afalse alarm) in performing the task.
The primary limitation of this study is small sam-ple size. First, because of the decision to use the well-defined and comprehensively assessed MTA sample,potential participants were limited to the MTA sam-ple. The effective sample was further limited to thosechildren who continued to have ADHD into adoles-cence and who also had a parent with ADHD. Fur-ther, the number of data collection sites was limitedto three in order to reduce heterogeneity introducedby using multiple scanners. The resulting samplesize was small but comparable to other ADHDfunctional imaging studies. Nevertheless, this smallsample may have limited power to detect between-group behavioral and brain activation differences.Another limitation was the use of a cross-sectionaldesign to examine possible developmental differ-ences in contrast to using a longitudinal designwhich would allow within-subjects comparison ofdevelopmental changes over time. Also, as com-mented on above, the youth and parent groups werenot matched and displayed several baseline differ-ences on key measures such as medication usehistory and gender.
Study #2: Medication effects
Methods
Subjects. Of the 20 ADHD dyads, 7 youths and 5parents were excluded because they were unable toperform with greater than 70% accuracy on the be-havioral paradigm and have less than 3 mm of headmovement for at least three runs. The remaining 13youths and 15 parents comprised the sample. SeeTable 1 for demographic and diagnostic character-istics of the parent and youth samples.
Analyses. On- and off-medication contrasts wereconducted with a random effects analysis. Placeboand medication data sets were matched on numberof runs used in the analysis to prevent differences in
statistical power between the two conditions. Awhole brain analysis was conducted, but contrastswere examined only in hypothesized ROIs that havebeen associated with methylphenidate response (i.e.,striatum, prefrontal and posterior parietal cortices,and the cerebellum).
Results and discussion
Table 4 presents the results of paired t-tests exam-ining medication effects on go/no-go task perform-ance. Medication decreased reaction time (RT)variability and improved stimulus discrimination(i.e., d-prime) in both youths and their parents. Inaddition, medication reduced the number of errors ofomission made by parents with ADHD.
Comparisons of brain activation during perform-ance of no-go trials showed that ADHD youths, whileon MPH compared to placebo, showed a consistentpattern of increased activity across multiple regions.These task-related increases in activity were in theleft middle frontal gyrus (Brodmann’s area 9), leftinferior frontal gyrus (Brodmann’s area 45), rightinferior parietal lobule (Brodmann’s area 40), anter-ior cingulate (Brodmann’s area 32), right caudatenucleus and left cerebellum (Figure 3). No regions ofinterest showed increased activation during placebodays compared to MPH days in the ADHD youths.Correlations between changes in behavioral per-formance on- and off-medication and brainactivation beta values on- and off-medication inactivation-defined regions of interest, where medi-cation effects were noted, were non-significant (all pvalues > .05).
Effects of medication on brain activation in par-ents with ADHD were less widespread. Increasedactivation was observed for the MPH conditioncompared to placebo in left caudate nucleus. How-ever, increased activation was observed for placebovs. MPH in the right inferior parietal lobule (Brod-mann’s area 40) and left middle frontal gyrus(Brodmann’s area 46). See Table 5 for identifiedregions, volumes, and Talaraich coordinates.
There appears to be a benefit of methylphenidatefor youths with ADHD as evidenced by betterbehavioral performance and increased brain activa-
Table 4 Paired t-test results, means and standard deviations for the behavioral performance of the ADHD youths and parents onplacebo compared to on methylphenidate
Youths Parents
Placebo(n ¼ 13) MPH (n ¼ 13)
Effectsize (d) t-tests
Placebo(n ¼ 15)
MPH(n ¼ 15)
Effectsize (d) t-tests
Errors of omission 6.18 (8.27) 3.35 (7.52) .36 2.02 8.97 (11.13) 1.44 (2.01) .92 2.85*Errors of commission 20.98 (14.64) 14.99 (13.65) .42 1.75 9.32 (9.27) 7.72 (6.64) .19 1.11Reaction time 434 (80) 407 (42) .42 1.72 430 (57) 403 (51) .49 2.00Reaction time SD 154.3 (69.2) 108.2 (40.5) .81 3.14** 103.3 (44.9) 78.0 (19.0) .71 2.27*D-prime 2.82 (.92) 3.37 (.84) .62 2.52* 3.12 (.78) 3.83 (.59) 1.03 4.22***
Note: *p < .05; **p < 01; ***p < .001.
ADHD frontostriatal dysfunction 907
� 2007 The AuthorsJournal compilation � 2007 Association for Child and Adolescent Mental Health.
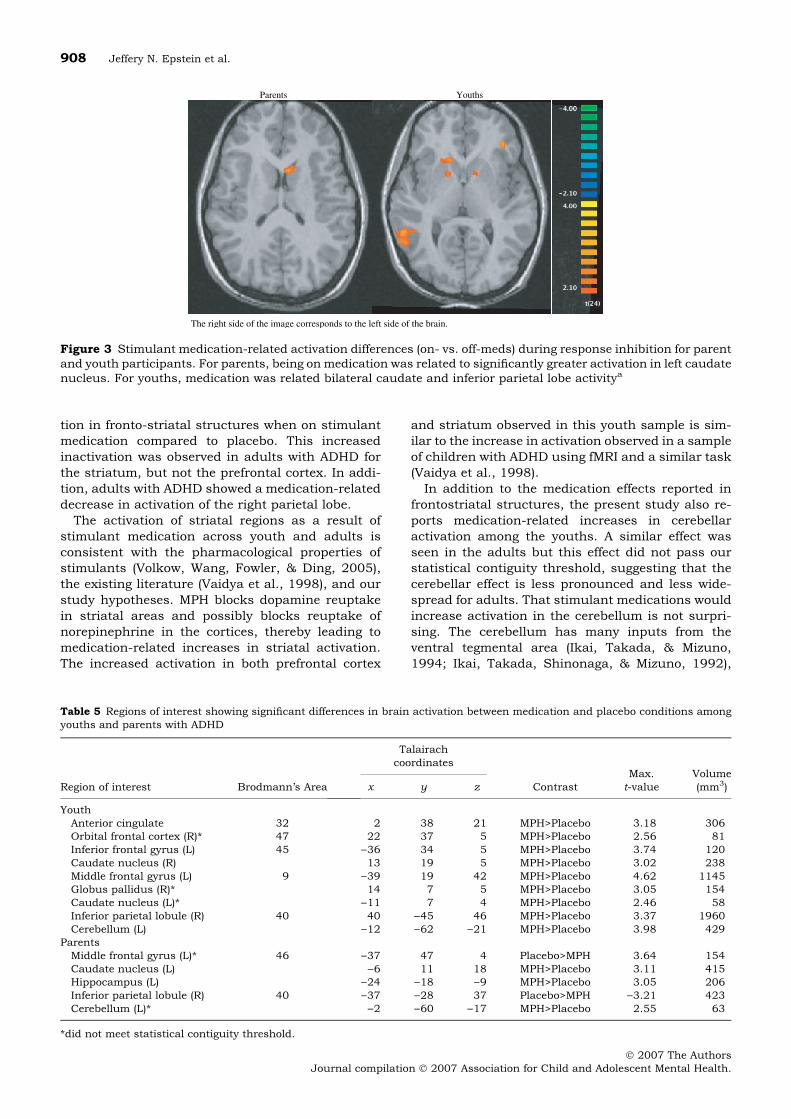
tion in fronto-striatal structures when on stimulantmedication compared to placebo. This increasedinactivation was observed in adults with ADHD forthe striatum, but not the prefrontal cortex. In addi-tion, adults with ADHD showed a medication-relateddecrease in activation of the right parietal lobe.
The activation of striatal regions as a result ofstimulant medication across youth and adults isconsistent with the pharmacological properties ofstimulants (Volkow, Wang, Fowler, & Ding, 2005),the existing literature (Vaidya et al., 1998), and ourstudy hypotheses. MPH blocks dopamine reuptakein striatal areas and possibly blocks reuptake ofnorepinephrine in the cortices, thereby leading tomedication-related increases in striatal activation.The increased activation in both prefrontal cortex
and striatum observed in this youth sample is sim-ilar to the increase in activation observed in a sampleof children with ADHD using fMRI and a similar task(Vaidya et al., 1998).
In addition to the medication effects reported infrontostriatal structures, the present study also re-ports medication-related increases in cerebellaractivation among the youths. A similar effect wasseen in the adults but this effect did not pass ourstatistical contiguity threshold, suggesting that thecerebellar effect is less pronounced and less wide-spread for adults. That stimulant medications wouldincrease activation in the cerebellum is not surpri-sing. The cerebellum has many inputs from theventral tegmental area (Ikai, Takada, & Mizuno,1994; Ikai, Takada, Shinonaga, & Mizuno, 1992),
Parents Youths
The right side of the image corresponds to the left side of the brain.
Figure 3 Stimulant medication-related activation differences (on- vs. off-meds) during response inhibition for parentand youth participants. For parents, being on medication was related to significantly greater activation in left caudatenucleus. For youths, medication was related bilateral caudate and inferior parietal lobe activitya
Table 5 Regions of interest showing significant differences in brain activation between medication and placebo conditions amongyouths and parents with ADHD
Region of interest Brodmann’s Area
Talairachcoordinates
ContrastMax.t-value
Volume(mm3)x y z
YouthAnterior cingulate 32 2 38 21 MPH>Placebo 3.18 306Orbital frontal cortex (R)* 47 22 37 5 MPH>Placebo 2.56 81Inferior frontal gyrus (L) 45 )36 34 5 MPH>Placebo 3.74 120Caudate nucleus (R) 13 19 5 MPH>Placebo 3.02 238Middle frontal gyrus (L) 9 )39 19 42 MPH>Placebo 4.62 1145Globus pallidus (R)* 14 7 5 MPH>Placebo 3.05 154Caudate nucleus (L)* )11 7 4 MPH>Placebo 2.46 58Inferior parietal lobule (R) 40 40 )45 46 MPH>Placebo 3.37 1960Cerebellum (L) )12 )62 )21 MPH>Placebo 3.98 429
ParentsMiddle frontal gyrus (L)* 46 )37 47 4 Placebo>MPH 3.64 154Caudate nucleus (L) )6 11 18 MPH>Placebo 3.11 415Hippocampus (L) )24 )18 )9 MPH>Placebo 3.05 206Inferior parietal lobule (R) 40 )37 )28 37 Placebo>MPH )3.21 423Cerebellum (L)* )2 )60 )17 MPH>Placebo 2.55 63
*did not meet statistical contiguity threshold.
908 Jeffery N. Epstein et al.
� 2007 The AuthorsJournal compilation � 2007 Association for Child and Adolescent Mental Health.

which is a dopaminergic center of the brain. UsingPET, increased cerebellar activity as a result of MPHhas been shown with normal adults (Volkow et al.,1998). This study’s documentation of increases incerebellar activation as a result of MPH administra-tion does differ from previous studies in that thiseffect was shown using task-related BOLD response.Typically, fMRI studies have not included cerebellarregions in their imaging field of view. Hence, thepresent findings emphasize the importance of col-lecting whole brain images when examining activa-tion patterns, and especially medication effects, inpatients with ADHD.
A limitation of the current study is that childrenand adults with ADHD did not necessarily take anindividually-determined optimal dose of MPH on the
day of scanning. Rather, a mg/kg formula (with amaximum cut-off of 20 mg MPH) was used to assigndosages to individual participants. Because weightdoes not correlate with optimal dose (Rapport, Du-Paul, & Kelly, 1989) and because patients havevariable dose response curves (Rapport et al., 1987),dosing according to weight does not always result inan optimal dosage for each individual.
General discussion
Results from the above studies support prevailingtheoretical notions that ADHD is caused by a neuro-biological deficit localized to prefrontal and striatalregions of the brain. Several studies have been
Table 6 Regions of interest showing significant differences inbrain activation in control participants
Region of interestBrodmann’s
area
Talairachcoordinates
Maximumt-valuex y z
YouthInferior frontal gyrusR 45 38 19 11 5.61R 45 35 24 1 7.47L 45 )28 23 7 2.76
Middle frontal gyrusR 9 34 42 26 11.83L 9 )32 40 25 7.42
Caudate nucleus (L) – )12 13 13 6.92Globus PallidusR – 15 1 1 5.66L – )18 )1 7 6.50
Inferior parietal lobule (R)R 40 47 )41 39 8.26L 40 )46 )39 43 5.40
Cerebellum (L) )27 )65 )26 8.15Anterior cingulateR 32 12 30 23 8.42L 32 )10 26 20 8.23
Orbital (R) – – – – –Hippocampus (L) – – – – –
ParentsInferior frontal gyrusR 46 31 38 12 9.16R 45 35 24 1 8.21L 46 )33 38 7 4.95
Middle frontal gyrusR 9 34 42 25 13.03L 9 )33 42 36 8.82
Caudate nucleus (R) – 11 2 17 7.38Globus PallidusR – 15 1 1 5.66L – )11 7 4 6.20
Inferior parietal lobule (R)R 40 47 )42 39 7.87L 40 )40 )52 40 4.79
Cerebellum (L) – )27 )64 )26 7.86Anterior cingulateR 32 3 20 35 7.17L 32 )2 36 28 8.14
Orbital (L) 11 20 33 )7 7.27Hippocampus (L) – 31 )22 )14 5.22
Table 7 Regions of interest showing significant differences inbrain activation in participants with ADHD
Region of interestBrodmann’s
area
Talairachcoordinates
Maximumt-valuex y z
YouthInferior frontal gyrusR 47 42 31 5 5.35R 46 37 41 7 7.07L 45 )26 22 13 5.52
Middle frontal gyrusR 46 32 38 16 7.55L 9 )23 38 32 9.18
Caudate nucleus (R) – 13 5 21 5.75Globus PallidusR – 20 6 6 15.08L – )19 4 6 7.78
Inferior parietal lobule (R)R 40 45 )46 24 6.68L 40 )45 )40 30 9.51
Cerebellum (L) – )22 )52 )28 9.72Anterior cingulateR 32 11 15 38 13.29L 32 )9 15 42 5.68
Orbital (R) 11 26 33 )5 7.85Hippocampus (L) – 29 )29 )9 6.24
ParentsInferior frontal gyrusR 44 46 15 20 7.00R 46 41 38 14 5.97L 45 )33 22 11 9.16
Middle frontal gyrusR 9 31 40 30 12.48L 46 )31 44 21 8.42
Caudate nucleus (R) – 15 2 20 6.71Globus PallidusR – 14 6 2 7.55L – )13 1 0 7.49
Inferior parietal lobule (R)R 40 47 )53 39 12.59L 40 )53 )46 35 7.42
Cerebellum (L) – )36 )55 )32 5.86Anterior cingulateR 32 7 34 24 6.75L 32 )6 24 27 6.14
Orbital (R) – – – – –Hippocampus (L) – )26 39 0 8.40
ADHD frontostriatal dysfunction 909
� 2007 The AuthorsJournal compilation � 2007 Association for Child and Adolescent Mental Health.

conducted examining response inhibition-relatedbrain activation in children with ADHD. This studyextends findings of fronto-striatal dysfunction toadults with ADHD and in individuals with geneticvulnerability for the disorder. A stimulant medicationtrial among the ADHD youths and their parentsshowed that among youths, stimulant medicationincreases activation in the striatum, as well as incerebellar regions. Increases in activation wereobserved in prefrontal regions in the youth, butnot the adults. In addition, there was a medication-related increase in activation in hippocampus for theadults, unlike the youths.
A clear strength of this study was the use of theMTA sample for recruitment of participants. All ofthe MTA participants with ADHD had a documentedhistory of an ADHD, Combined Type diagnosis be-tween 7 and 9 years of age. Further, children in thissample were assessed approximately every 2 yearsuntil the present so that persistence of ADHDsymptomatology has been documented. This differsfrom most ADHD imaging samples where studyinclusion is usually, but not always, based uponsymptoms present at the time of the study. Such asingle time point diagnosis may yield increasedsample heterogeneity, with the likelihood of multipleetiologies (Biederman, 2005). Our study sample wasfurther restricted to youths and parents with afamily history of ADHD. This recruitment strategyincreases the likelihood that the observed findingsrepresent the effects of stimulant medications onyouths and adults whose ADHD symptomatology isbiologically based and shared within dyads.
Because the sample used for the present studywas selected based on genetic association, the studyresults provide several clues as to possible endo-phenotypic characteristics that may be used to studythe genetics and pharmacogenetics of ADHD. In-deed, several investigators (e.g., Doyle et al., 2005)have described the advantages of using endopheno-types to search for genetic associations with ADHD.In addition, several research studies report on therelationships between specific candidate genes andresponse to stimulant medication among patientswith ADHD (see McGough, 2005 for review). Some ofthe outcomes in the present study (i.e., d-prime on aresponse inhibition task, fronto-striatal activation)demonstrated between-group and medication-related effects across developmentally differentsamples. Relating these endophenotypes to geneticmarkers has the potential to identify genetic predic-tors of ADHD and possibly stimulant response.
Acknowledgements
The grant was supported by a set of NIH collaborat-ive grants: MH064179 (Epstein), MH064166 (Casey),MH064177 (Reiss), MH064182 (Hinshaw), andMH064176 (Greenhill) as well as grant #RR09784(Glover).
Correspondence to
Jeffery N. Epstein, Cincinnati Children’s HospitalMedical Center, 3333 Burnet Ave, ML 10006, Cin-cinnati, OH 45229; Tel: (513)636-8296; Fax: (513)636-0755; Email: [email protected]
References
American Psychiatric Association. (1994). Diagnosticand statistical manual for mental disorders, 4th edn.Washington, DC: Author.
Anderson, C.M., Polcari, A., Lowen, S.B., Renshaw,P.F., & Teicher, M.H. (2002). Effects of methylpheni-date on functional magnetic resonance relaxometry ofthe cerebellar vermis in boys with ADHD. AmericanJournal of Psychiatry, 159, 1322–1328.
Aron, A.R., & Poldrack, R.A. (2005). The cognitiveneuroscience of response inhibition: Relevance forgenetic research in Attention-Deficit/HyperactivityDisorder. Biological Psychiatry, 57, 1285–1292.
Biederman, J. (2005). Attention-deficit/hyperactivitydisorder: A selective overview. Biological Psychiatry,57, 1215–1220.
Biederman, J., Mick, E., & Faraone, S.V. (2000). Age-dependent decline of symptoms of attention deficithyperactivity disorder: Impact of remission definitionand symptom type. American Journal of Psychiatry,157, 816–818.
Booth, J.R., Burman, D.D., Meyer, J.R., Lei, Z., Trom-mer, B.L., Davenport, N.D., et al. (2005). Largerdeficits in brain networks for response inhibitionthan for visual selective attention in attention deficithyperactivity disorder (ADHD). Journal of ChildPsychology and Psychiatry, 46, 94–111.
Boynton, G.M., Engel, S.A., Glover, G.H., & Heeger,D.J. (1996). Linear systems analysis of functionalmagnetic resonance imaging in human V1. Journal ofNeuroscience, 16, 4207–4221.
Bush, G., Frazier, J.A., Rauch, S.L., Seidman, L.J.,Whalen, P.J., Jenike, M.A., et al. (1999). Anteriorcingulate cortex dysfunction in attention-deficit/hyperactivity disorder revealed by fMRI and countingStroop. Biological Psychiatry, 45, 1542–1552.
Casey, B.J., Castellanos, F.X., Giedd, J.N., Marsh,W.L., Hamburger, S.D., Schubert, A.B., et al.(1997a). Implication of right frontostriatal circuitryin response inhibition and attention-deficit/hyperactivity disorder. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 36,374–383.
Casey, B.J., Cohen, J.D., O’Craven, K., Davidson,R.J., Irwin, W., Nelson, C.A., et al. (1998). Repro-ducibility of fMRI results across four institutionsusing a spatial working memory task. Neuroimage,8, 249–261.
Casey, B.J., Trainor, R.J., Orendi, J.L., Schubert, A.B.,Nystrom, L.E., Giedd, J.N., et al. (1997b). A develop-mental functional MRI study of prefrontal activationduring performance of a go-no-go task. Journal ofCognitive Neuroscience, 9, 835–847.
Castellanos, F.X., Lee, P.L., Sharp, W., Jeffries, N.O.,Greenstein, D.K., Clasen, L.S., et al. (2002). Develop-mental brain trajectories of brain volume abnormal-
910 Jeffery N. Epstein et al.
� 2007 The AuthorsJournal compilation � 2007 Association for Child and Adolescent Mental Health.
ities in children and adolescents with ADHD. Journalof the American Medical Association, 288, 1740–1748.
Centers for Disease Control. (2005). Mental health inthe United States. Prevalence of diagnosis and medi-cation treatment for attention-deficit/hyperactivitydisorder – United States, 2003. MMWR Morbidityand Mortality Weekly Report, 2, 842–847.
Doyle, A.E., Willcutt, E.G., Seidman, L.J., Biederman,J., Chouinard, V., Silva, J., et al. (2005). Attention-deficit/hyperactivity disorder endophenotypes. Bio-logical Psychiatry, 57, 1324–1335.
Durston, S., Mulder, M., Casey, B.J., Ziermans, T., &van Engeland, H. (in press). Activation in ventralprefrontal cortex is sensitive to genetic vulnerabilityfor attention deficit hyperactivity disorder. BiologicalPsychiatry.
Durston, S., Tottenham, N.T., Thomas, K.M., Davidson,M.C., Eigsti, I.M., Yang, Y., et al. (2003). Differentialpatterns of striatal activation in young children withand without ADHD. Biological Psychiatry, 53,871–878.
Epstein, J.N., Casey, B.J., Tonev, S.T., Davidson, M.,Reiss, A., Garrett, A., et al. (in press). Assessment andprevention of head motion during imaging of patientswith attention deficit hyperactivity disorder. Psychi-atry Research: Neuroimaging.
Epstein, J.N., Johnson, D.E., & Conners, C.K. (2001).Conners’ Adult ADHD Diagnostic Interview for DSM-IV. North Tonawanda, NY: Multi-Health Systems, Inc.
Epstein, J.N., & Kollins, S.H. (2006). Psychometricproperties of an adult ADHD diagnostic interview.Journal of Attention Disorders, 9, 504–514.
Forman, S.D., Cohen, J.D., Fitzgerald, M., Eddy, W.F.,Mintun, M.A., & Noll, D.C. (1995). Improved assess-ment of significant activation in functional magneticresonance imaging (fMRI): Use of a cluster-sizethreshold. Magnetic Resonance in Medicine, 33,636–647.
Giedd, J.N., Blumenthal, J., Molloy, E., & Castellanos,F.X. (2001). Brain imaging of ADHD. Annals of theNew York Academy of Sciences, 931, 33–49.
Glover, G.H., & Law, C.S. (2001). Spiral-in/out BOLDfMRI for increased SNR and reduced susceptibilityartifacts. Magnetic Resonance in Medicine, 46,515–522.
Hervey, A.S., Epstein, J.N., & Curry, J.F. (2004). Theneuropsychology of adults with attention deficithyperactivity disorder: A meta-analytic review.Neuropsychology, 18, 485–503.
Hill, D.E., Yeo, R.A., Campbell, R.A., Hart, B., Vigil, J.,& Brooks, W. (2003). Magnetic resonance imagingcorrelates of attention-deficit/hyperactivity disorderin children. Neuropsychology, 17, 496–506.
Ikai, Y., Takada, M., & Mizuno, N. (1994). Singleneurons in the ventral tegmental area that project toboth the cerebral and cerebellar cortical areas by wayof axon collaterals. Neuroscience, 61, 925–934.
Ikai, Y., Takada, M., Shinonaga, Y., & Mizuno, N.(1992). Dopaminergic and non-dopaminergic neu-rons in the ventral tegmental area of the rat project,respectively, to the cerebellar cortex and deep cere-bellar nuclei. Neuroscience, 51, 719–728.
Konishi, S., Nakajima, K., Uchida, I., Kikyo, H.,Kameyama, M., & Miyashita, Y. (1999). Commoninhibitory mechanism in human inferior prefrontal
cortex revealed by event-related fMRI. Brain, 122,981–991.
Konishi, S., Nakajima, K., Uchida, I., Sekihara, K., &Miyashita, Y. (1998). No-go dominant brain activity inhuman inferior prefrontal cortex revealed by func-tional magnetic resonance imaging. European Journalof Neuroscience, 10, 1209–1213.
Krings, T., Reinges, M.H.T., Erberich, S., Kemeny, V.,Rohde, V., Spetzger, U., et al. (2001). Functional MRIfor presurgical planning: Problems, artefacts, andsolutions strategies. Journal of Neurology Neurosur-gery Psychiatry, 70, 749–760.
Lee, J., Kim, B., Kang, E., Lee, D., Kim, Y., Chung, J.,et al. (2005). Regional cerebral blood flow in childrenwith attention deficit hyperactivity disorder: Compar-ison before and after methylphenidate treatment.Human Brain Mapping, 24, 157–164.
Matochik, J. (1994). Cerebral glucose metabolism inadults with attention deficit hyperactivity disorderafter chronic stimulant treatment. American Journalof Psychiatry, 151, 658–664.
McGough, J.J. (2005). Attention-deficit/hyperactivitydisorder pharmacogenomics. Biological Psychiatry,57, 1367–1373.
Menon, V., Adleman, N.E., White, C.D., Glover, G.H., &Reiss, A.L. (2001). Error-related brain activationduring a go/nogo response inhibition task. HumanBrain Mapping, 12, 131–143.
MTA Cooperative Group. (1999). A 14-month random-ized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. The MTA CooperativeGroup. Multimodal Treatment Study of Childrenwith ADHD. Archives of General Psychiatry, 56,1073–1086.
Nigg, J.T. (2001). Is ADHD a disinhibitory disorder?Psychological Bulletin, 127, 571–598.
Pennington, B., & Ozonoff, S. (1996). Executivefunctions and developmental psychopathology.Journal of Child Psychology and Psychiatry, 37,51–87.
Peterson, B.S., Skudlarski, P., Gatenby, J.C., Zhang,H., Anderson, A.W., & Gore, J.C. (1999). An fMRIstudy of Stroop word-color interference: Evidence forcingulate subregions subserving multiple distributedattentional systems. Biological Psychiatry, 45,1237–1258.
Pliszka, S.R., Glahn, D.C., Semrud-Clikeman, M.,Franklin, C., Perez, R., Xiong, J., et al. (2006). Neu-roimaging of inhibitory control areas in children withattention deficit hyperactivity disorder who weretreatment naı̈ve or in long-term treatment. AmericanJournal of Psychiatry, 163, 1052–1060.
Rapport, M.D., DuPaul, G.J., & Kelly, K.L. (1989).Attention deficit hyperactivity disorder and methyl-phenidate: The relationship between gross bodyweight and drug response in children. Psychophar-macology Bulletin, 25, 285–290.
Rapport, M.D., Jones, J.T., DuPaul, G.J., Kelly, K.L.,Gardner, M.J., Tucker, S.B., et al. (1987). Attentiondeficit disorder and methylphenidate: Group andsingle-subject analyses of dose effects on attentionin clinic and classroom settings. Journal of ClinicalChild Psychology, 16, 329–338.
Rasmussen, P., & Gillberg, C.G. (2000). Natural out-come of ADHD with developmental coordination
ADHD frontostriatal dysfunction 911
� 2007 The AuthorsJournal compilation � 2007 Association for Child and Adolescent Mental Health.

disorder at age 22 years: A controlled, longitudinal,community-based study. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 39,1424–1431.
Rubia, K. (2002). The dynamic approach to neurodevel-opmental psychiatric disorders: Use of fMRI com-bined with neuropsychology to elucidate thedynamics of psychiatric disorders, exemplified inADHD and schizophrenia. Behavioural Brain Re-search, 130, 47–56.
Rubia, K., Overmeyer, S., Taylor, E., Brammer, M.,Williams, S.C., Simmons, A., et al. (1999). Hypo-frontality in attention deficit hyperactivity disorderduring higher-order motor control: A study withfunctional MRI. American Journal of Psychiatry,156, 891–896.
Rubia, K., Russell, T., Overmeyer, S., Brammer, M. J.,Bullmore, E. T., Sharma, T., et al. (2001). Mappingmotor inhibition: Conjunctive brain activationsacross different versions of go/no-go and stop tasks.Neuroimage, 13, 250–261.
Rubia, K., Smith, A.B., Brammer, M.J., Toone, B., &Taylor, E. (2005). Abnormal brain activation duringinhibition and error detection in medication naiveadolescents with ADHD. American Journal of Psy-chiatry, 162, 1067–1075.
Schulz, K.P., Fan, J., Tang, C.Y., Newcorn, J.H., Buc-hsbaum, M.S., Cheung, A.M., et al. (2004). Responseinhibition in adolescents diagnosed with attentiondeficit hyperactivity disorder during childhood: Anevent-related fMRI study. American Journal of Psy-chiatry, 161, 1650–1657.
Schweitzer, J.B., Lee, D.O., Hanford, R.B., Tagamets,M.A., Hoffman, J.M., Grafton, S.T., et al. (2003). Apositron emission tomography study of methylphen-idate in adults with ADHD: Alterations in restingblood flow and predicting treatment response. Neuro-psychopharmacology, 28, 967–973.
Schweitzer, J.B., Lee, D.O., Hanford, R.B., Zink, C.F.,Ely, T.D., Tagamets, M.A., et al. (2004). Effect ofmethylphenidate on executive functioning in adultswith attention-deficit/hyperactivity disorder: Normal-ization of behavior but not related brain activity.Biological Psychiatry, 56, 597–606.
Seidman, L.J., Biederman, J., Faraone, S.V., Milber-ger, S., Norman, D., Seiverd, K., et al. (1995). Effectsof family history and comorbidity on the neuro-psychological performance of children with ADHD:Preliminary findings. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 34,1015–1024.
Seidman, L.J., Biederman, J., Faraone, S.V., Weber, W.,& Ouellette, C. (1997). Toward defining a neuro-psychology of attention deficit-hyperactivity disorder:Performance of children and adolescents from a largeclinically referred sample. Journal of Consulting andClinical Psychology, 65, 150–160.
Shaffer, D., Fisher, P., Lucas, C.P., Dulcan, M.K., &Schwab-Stone, M.E. (2000). NIMH DiagnosticInterview Schedule for Children Version IV (NIMHDISC-IV): Description, differences from previous ver-sions, and reliability of some common diagnoses.Journal of the American Academy of Child andAdolescent Psychiatry, 39, 28–38.
Shafritz, K.M., Marchione, K.E., Gore, J.C., Shaywitz,S.E., & Shaywitz, B.A. (2004). The effects of methyl-phenidate on neural systems of attention in attentiondeficit hyperactivity disorder. American Journal ofPsychiatry, 161, 1990–1997.
Silk, T., Vance, A., Rinehart, N., Egan, G., O’Boyle,M., Bradshaw, J.L., et al. (2005). Fronto-parietalactivation in attention-deficit hyperactivity disorder,combined type: Functional magnetic resonanceimaging study. British Journal of Psychiatry, 187,282–283.
Smith, A.B., Taylor, E., Brammer, M.J., Toone, B., &Rubia, K. (2006). Task specific hyperactivation inprefrontal and temporo-parietal brain regions inmedication-naive children and adolescents withattention deficit/hyperactivity disorder during motorinhibition and tasking switching. American Journal ofPsychiatry, 163, 1044–1051.
Sowell, E.R., Thompson, P.M., Welcome, S.E., Henken-ius, A.L., Toga, A.W., & Peterson, B.S. (2003). Corticalabnormalities in children and adolescents with atten-tion-deficit/hyperactivity disorder. Lancet, 362,1699–1707.
Stuss, D.T., Murphy, K.R., Binns, M.A., & Alexander,M.P. (2003). Staying on the job: The frontal lobescontrol individual performance variability. Brain,126, 2363–2380.
Swanson, J., Castellanos, F.X., Murias, M., LaHoste,G., & Kennedy, J. (1998). Cognitive neuroscience ofattention deficit hyperactivity disorder and hyper-kinetic disorder. Current Opinions in Neurobiology, 8,263–271.
Tamm, L., Menon, V., Ringel, J., & Reiss, A.L. (2004).Event-related fMRI evidence of frontotemporal invol-vement in aberrant response inhibition and taskswitching in attention deficit/hyperactivity disorder.Journal of the American Academy of Child andAdolescent Psychiatry, 43, 1430–1440.
Tamm, L., Menon, V., & Reiss, A.L. (2002). Matu-ration of brain function associated withresponse inhibition. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 41,1231–1238.
Vaidya,C.J.,Austin,G.,Kirkorian,G.,Ridlehuber,H.W.,Desmond, J.E., Glover, G.H., et al. (1998). Selectiveeffects of methylphenidate in attention deficithyperactivity disorder: A functional magnetic reson-ance study. Proceedings of the National Academyof Sciences of the United States of America, 95,14494–14499.
Vaidya,C.J.,Bunge,S.A.,Dudukovic,N.M.,Zalecki,C.A.,Elliott, G.R., & Gabrieli, J.D.E. (2005). Alteredneural substrates of cognitive control in childhoodADHD: Evidence from functional magnetic resonanceimaging. American Journal of Psychiatry 162,1605–1613.
Volkow, N.D., Wang, G., Fowler, J.S., & Ding, Y. (2005).Imaging the effects of methylphenidate on braindopamine: New model on its therapeutic actions forattention-deficit/hyperactivity disorder. BiologicalPsychiatry, 57, 1410–1415
Volkow, N.D., Wang, G.J., Fowler, J.S., Hitzemann, R.,Gatley, J., Ding, Y.S., et al. (1998). Differences inregional brain metabolic responses between single
912 Jeffery N. Epstein et al.
� 2007 The AuthorsJournal compilation � 2007 Association for Child and Adolescent Mental Health.

and repeated doses of methylphenidate. PsychiatryResearch, 83, 29–36.
Weiss, G., & Hechtman, L. (1993). Hyperactive childrengrown up: ADHD in children, adolescents, and adults.New York: Guilford.
Willcutt, E.G., Doyle, A.E., Nigg, J.T., Faraone, S.V., &Pennington, B.F. (2005). Validity of the executive
function theory of attention-deficit/hyperactivity dis-order: A meta-analytic review. Biological Psychiatry,57, 1336–1346.
Manuscript accepted 29 January 2007
ADHD frontostriatal dysfunction 913
� 2007 The AuthorsJournal compilation � 2007 Association for Child and Adolescent Mental Health.
Related Documents











