2007;13:3968-3976. Clin Cancer Res Xuefeng Zhang, Jianfeng Xu, Jack Lawler, et al. Endostatin Therapy with Thrombospondin-1 Type 1 Repeats and Mediated Antiangiogenic Gene - Adeno-Associated Virus Updated version http://clincancerres.aacrjournals.org/content/13/13/3968 Access the most recent version of this article at: Cited Articles http://clincancerres.aacrjournals.org/content/13/13/3968.full.html#ref-list-1 This article cites by 43 articles, 19 of which you can access for free at: Citing articles http://clincancerres.aacrjournals.org/content/13/13/3968.full.html#related-urls This article has been cited by 3 HighWire-hosted articles. Access the articles at: E-mail alerts related to this article or journal. Sign up to receive free email-alerts Subscriptions Reprints and . [email protected] Department at To order reprints of this article or to subscribe to the journal, contact the AACR Publications Permissions . [email protected] Department at To request permission to re-use all or part of this article, contact the AACR Publications Cancer Research. on September 11, 2013. © 2007 American Association for clincancerres.aacrjournals.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

2007;13:3968-3976. Clin Cancer Res Xuefeng Zhang, Jianfeng Xu, Jack Lawler, et al. EndostatinTherapy with Thrombospondin-1 Type 1 Repeats and
Mediated Antiangiogenic Gene−Adeno-Associated Virus
Updated version
http://clincancerres.aacrjournals.org/content/13/13/3968
Access the most recent version of this article at:
Cited Articles
http://clincancerres.aacrjournals.org/content/13/13/3968.full.html#ref-list-1
This article cites by 43 articles, 19 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/13/13/3968.full.html#related-urls
This article has been cited by 3 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
To request permission to re-use all or part of this article, contact the AACR Publications
Cancer Research. on September 11, 2013. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from

Adeno-AssociatedVirus^Mediated Antiangiogenic Gene TherapywithThrombospondin-1Type 1Repeats and EndostatinXuefeng Zhang,1Jianfeng Xu,2 Jack Lawler,3 ErnestTerwilliger,2 and Sareh Parangi1
Abstract Purpose: Recombinant adeno-associated virus (rAAV)-mediated antiangiogenic gene therapyoffers a powerful strategy for cancer treatment, maintaining sustained levels of antiangiogenicfactors with coincident enhanced therapeutic efficacy.We aimed to develop rAAV-mediatedantiangiogenic gene therapy delivering endostatin and 3TSR, the antiangiogenic domain ofthrombospondin-1.Experimental Design: rAAV vectorswere constructed to express endostatin (rAAV-endostatin)or3TSR(rAAV-3TSR).Theantiangiogenicefficacyof thevectorswascharacterizedusingavascularendothelial growth factor (VEGF)-induced mouse ear angiogenesis model. To evaluate theantitumor effects of the vectors, immunodeficientmicewere pretreatedwith rAAV-3TSRor rAAV-endostatin and receivedorthotopic implantationof cancer cells into the pancreas.Tomimic clinicalsituations, mice bearing pancreatic tumors were treatedwith intratumoral injection of rAAV-3TSRor rAAV-endostatin.Results: rAAV-mediated i.m. gene delivery resulted in expression of the transgene in skeletalmuscle with inhibition ofVEGF-induced angiogenesis at a distant site (the ear). Local delivery ofthe vectors into the mouse ear also inhibited VEGF-induced ear angiogenesis. Pretreatment ofmice with i.m. or intrasplenic injection of rAAV-endostatin or rAAV-3TSR significantly inhibitedtumor growth. A single intratumoral injection of each vector also significantly decreased thevolume of large established pancreatic tumors. Tumor microvessel density was significantlydecreased in each treatment group andwaswell correlatedwith tumor volume reduction.Greaterantiangiogenic and antitumor effects were achievedwhen rAAV-3TSRand rAAV-endostatinwerecombined.Conclusions: rAAV-mediated 3TSR and endostatin gene therapy showed both localized andsystemic therapeutic effects against angiogenesis and tumor growth and may provide promisefor patients with pancreatic cancer.
Tumor growth beyond 1 to 2 mm depends on angiogenesis,the formation of new blood vessels (1, 2). The homeostaticprocesses regulating tumor angiogenesis have become morethoroughly understood in recent years. In the tumor microen-vironment, angiogenic stimulators outbalance angiogenicinhibitors, generating a proangiogenic response and anincreased blood vessel density (3, 4), which in turn is relatedto decreased survival in cancer patients (5, 6). To restore the
tightly regulated angiogenesis balance in the tumor microen-vironment, antiangiogenic therapy can be aimed at up-regulation of antiangiogenic factors or down-regulation ofproangiogenic factors or both.Among endogenous angiogenic inhibitors, endostatin,
angiostatin, and thrombospondin-1 (TSP-1) are the mostimportant and have been studied extensively (1, 7–9). TSP-1is a multifunctional extracellular matrix protein with pivotalroles in the regulation of vascular development and angiogen-esis (7, 8). The discrete antiangiogenic domain of TSP-1, theTSP-1 type 1 repeats, designated 3TSR, is an attractive candidatefor antiangiogenic treatment. We previously have shown theantiangiogenic and antitumor efficacy of recombinant 3TSR inseveral preclinical studies (10–13). A TSR-derived mimeticpeptide, ABT-510, has been tested in clinical trials for patientswith advanced cancers (14–16). Recombinant endostatin, aCOOH-terminal proteolytic fragment of collagen XVIII, has alsoentered clinical trials for patients with solid tumors (17, 18).Evidence suggests that a consistent level of angiogenic
inhibitors might improve the therapeutic potency and efficacyof cancer treatment (19–23). We and others have shown thatcontinuous delivery of angiogenic inhibitors, including 3TSR,endostatin, and angiostatin, was more effective than daily bolusinjections (19–23), indicating the therapeutic benefits of
Cancer Therapy: Preclinical
Authors’Affiliations: Departments of 1Surgery, 2Medicine, and 3Pathology, BethIsrael Deaconess Medical Center, Harvard Medical School, Boston, MassachusettsReceived1/31/07; revised 4/6/07; accepted 4/19/07.Grant support: Medical Foundation/DolphinTrust Grant, American College ofSurgeons Faculty Research Fellowship, National Cancer Institute grant K08CA88965-01A1 (S. Parangi), NIH grants CA 92644 and HL 68003 (J. Lawler),and Susan Komen Foundation award (E.Terwilliger).The costs of publication of this article were defrayed in part by the payment of pagecharges.This article must therefore be hereby marked advertisement in accordancewith18 U.S.C. Section1734 solely to indicate this fact.Requests for reprints: Sareh Parangi, Department of Surgery, Beth IsraelDeaconess Medical Center, Harvard Medical School, 330 Brookline Avenue,Stoneman 934, Boston, MA 02215. Phone: 617-667-2442; Fax: 617-667-2978;E-mail: [email protected].
F2007 American Association for Cancer Research.doi:10.1158/1078-0432.CCR-07-0245
www.aacrjournals.orgClin Cancer Res 2007;13(13) July1, 2007 3968
Cancer Research. on September 11, 2013. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from

sustained levels of angiogenic inhibitors. Gene therapy providesa way to achieve sustained delivery of antiangiogenic factors tothe tumor site from a single or small number of treatments andto maintain the continuous production of angiogenic inhib-itors for a set period of time. Gene therapy strategies directlytargeting tumor cells with genes encoding prodrug-converting
enzymes or cytokines/chemokines for oncolysis require high-efficiency transduction of cancer cells by gene vectors. Incontrast, antiangiogenic gene therapy does not require high-efficient cancer cell transduction, and may target nontumorcells as well as tumor cells, using both tissues to provide stableplatforms for expression of secreted proteins.
Fig. 1. Characterization of rAAV vector expression in vitro and in vivo. A, structure of the rAAV vectors expressing different transgenes.The inserted gene expressionwas under the control of the human cytomegalovirus immediate early (CMV-IE) promoter. ITR, inverted terminal repeat sequences of AAV. B, expression of GFP at 48 hafter pancreatic cancer cells were transduced with rAAV-GFP.Top, images from green fluorescence channel; bottom, phase-contrast images from the same visual field.C,Western blot for 3TSR with supernatant of rAAV-3TSR ^ transduced cells.The cultural media were changed 48 h after transduction and collected forWestern blot 24 hlater. D, immunofluorescence staining of 3TSR in mouse skeletal muscle after rAAV-3TSR i.m. injection.Top, images from green fluorescence microscopy; bottom,light-microscopic images from the same visual field.The ink marked the distribution of injected agents. Bar, 0.2 mm.
Antiangiogenic GeneTherapy withTSP-1and Endostatin
www.aacrjournals.org Clin Cancer Res 2007;13(13) July1, 20073969
Cancer Research. on September 11, 2013. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from
The potential of antiangiogenic gene therapy in cancer iscurrently being evaluated using both viral and nonviral vectors(24–27). Antiangiogenic vectors need to be capable ofsustained, long-term expression without vector-associated
toxicity or immunity. Compared with other gene therapyvectors, adeno-associated virus (AAV) vectors are highlyadvantageous for antiangiogenic gene therapy. AAV-mediatedtransgene persists in host cells primarily as stable episomes,
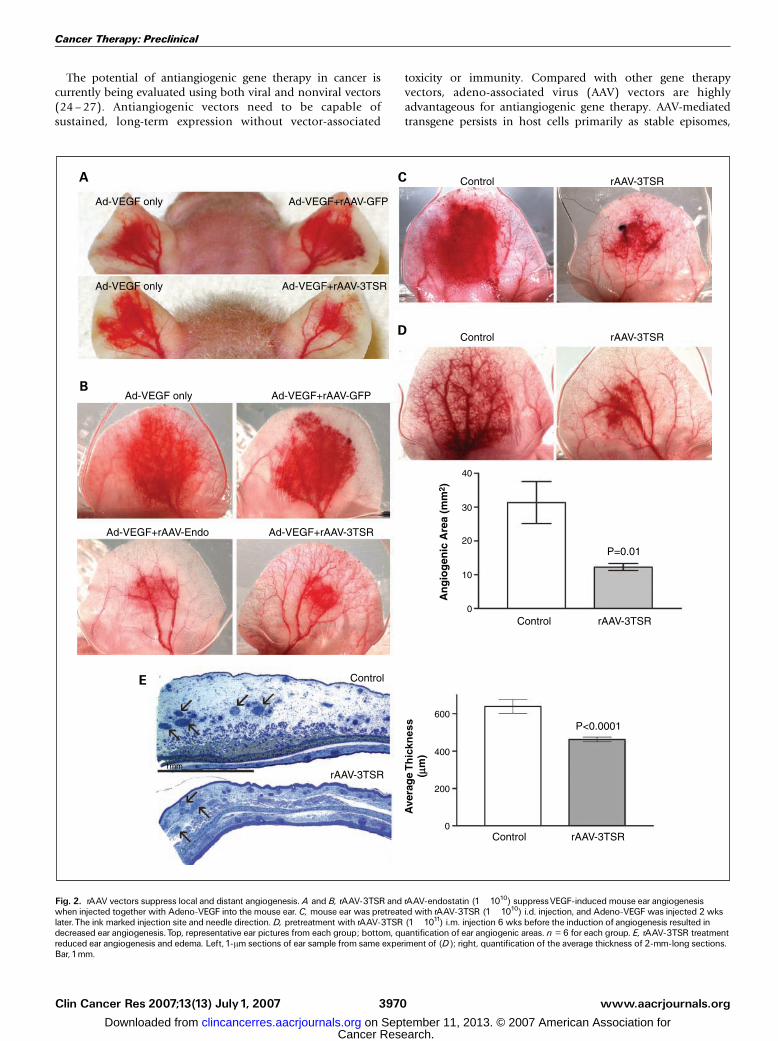
Fig. 2. rAAV vectors suppress local and distant angiogenesis. A and B, rAAV-3TSR and rAAV-endostatin (1 �1010) suppressVEGF-induced mouse ear angiogenesiswhen injected together with Adeno-VEGF into the mouse ear. C, mouse ear was pretreated with rAAV-3TSR (1 �1010) i.d. injection, and Adeno-VEGF was injected 2 wkslater.The ink marked injection site and needle direction. D, pretreatment with rAAV-3TSR (1 �1011) i.m. injection 6 wks before the induction of angiogenesis resulted indecreased ear angiogenesis.Top, representative ear pictures from each group; bottom, quantification of ear angiogenic areas. n = 6 for each group. E, rAAV-3TSR treatmentreduced ear angiogenesis and edema. Left, 1-Am sections of ear sample from same experiment of (D); right, quantification of the average thickness of 2-mm-long sections.Bar, 1mm.
Cancer Therapy: Preclinical
www.aacrjournals.orgClin Cancer Res 2007;13(13) July1, 2007 3970
Cancer Research. on September 11, 2013. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from

thus resulting in prolonged but not permanent transgeneexpression, with low risk of insertional mutagenesis. AAVs arenonpathogenic vectors with a limited host immune responseand have been used in humans with no adverse effects (28).AAV-expressing endostatin has been used in several preclinicalcancer models showing long-term endostatin expression andsignificant protective effects against tumor growth (26, 29, 30).In the present study, we engineered vectors derived from
AAV2, the most commonly used serotype, to express either3TSR or endostatin and characterized the antiangiogenicefficacy of these vectors in a vascular endothelial growth factor(VEGF)-induced mouse ear angiogenesis model. The antitumoreffects of the viral vectors were then studied in a murineorthotopic pancreatic cancer model with direct relevance to thedisease seen in humans. We find that AAV-mediated antiangio-genic gene therapy can be used to express transgenes in normaltissue, such as skeletal muscle and liver, to inhibit tumorgrowth at distant sites. Direct intratumoral delivery of therecombinant AAV (rAAV) vectors also significantly inhibitedthe growth of established pancreatic tumors. Furthermore,more significant antiangiogenic and antitumor effects wereachieved when the AAV vectors expressing 3TSR and endostatinwere used in combination.
Materials and Methods
Cell culture. Human pancreatic cancer cells AsPC-1 and MiaPaCa-2(American Type Culture Collection) were grown in RPMI 1640 (LifeTechnologies, Inc.) supplemented with 10% fetal bovine serum andpenicillin-streptomycin. Cells were grown in 5% CO2/95% air at 37jCin a humidified incubator.
rAAV construction and production. rAAV vectors expressing endo-statin (rAAV-endostatin) or 3TSR (rAAV-3TSR) were constructed usingmethods described previously (31). For rAAV-endostatin, a fragmentcontaining a 250-bp segment encoding the endogenous murinecollagen XVIII signal sequence fused to a 600-bp cDNA fragmentencoding the COOH-terminal noncollagenous domain (NC1) of theprotein, identical to endostatin, was inserted into an AAV-basedplasmid. A cDNA encoding the three type 1 repeats of TSP-1 wascloned as described previously (10) and subcloned into the same AAVplasmid to generate rAAV-3TSR. In each case, transcription of theinserted gene was under the control of the human cytomegalovirusimmediate early promoter. Isogenic rAAV encoding green fluorescentprotein (GFP) or LacZ was used as control in these studies. Figure 1Ashows the structure of the rAAV vectors. The rAAV vectors werepackaged in 293 cells and functional viral titers were estimated by real-time PCR as described previously (31).
In vitro transduction and Western blot for 3TSR. Pancreatic cancercells were transduced with rAAV-3TSR as described previously (31).Fresh medium was added to transduced cells 48 h after transduction.Twenty-four hours later, the culture medium was collected andprecipitated with ammonium sulfate. The 3TSR protein was detectedvia Western blotting with a customized chicken anti-TSR antibody (AvesLabs, Inc.). To produce chicken antibody against TSR, recombinanthuman TSR2 (the second TSP-1 type 1 repeat) protein was used asimmunogen. Hens were injected with TSR2 protein on days 3, 24, 38,and 52, and immune eggs were collected 1 week after the last injection.Chicken IgY was purified from the immune eggs.
Tumor models. All animal work was done in accordance withfederal, local, and institutional guidelines as described previously (12).Male severe combined immunodeficient mice (Taconic), 4 to 6 weeksof age, were used. The orthotopic pancreatic cancer model was made viasurgically implanting a suspension of 1 � 106 AsPC-1 cells into thebody of the pancreas (12).
rAAV-mediated gene therapy. rAAV vectors were delivered via i.m.,intrasplenic, or intratumoral injections. In mice receiving i.m. orintrasplenic rAAV delivery, rAAV particles (1 � 1011) in 100 AL wereinjected. Four weeks after vector administration, each mouse receivedsurgical implantation of cancer cells into the pancreas. The followinggroups were included: I, control, mice received rAAV-GFP i.m. injection;II, rAAV-3TSR i.m. injection; III, rAAV-3TSR intrasplenic injection; IV,rAAV-endostatin i.m. injection; and V, rAAV-3TSR plus rAAV-endostatini.m. injection. Intrasplenic injection was done using a similar regimenas described above. For i.m. injection, viral vectors were injected intothe quadriceps muscle of the hind limbs.
For intratumoral gene therapy, tumor cells were implanted into thepancreas and allowed to grow for 3 weeks. Tumor-bearing micewere then randomized and received single intratumoral gene transfer of1 � 1011 (in 100 AL) rAAV-GFP, rAAV-endostatin, or rAAV-3TSR. Fivemice were used in each group. Mice in all groups were sacrificed andunderwent necropsy 31 days after tumor cell implantation. Tumorvolume was calculated as p/6 � length � width � height.
Mouse ear angiogenesis assay. The mouse ear angiogenesis assay wasdone using VEGF-expressing adenoviral vectors (Adeno-VEGF) as de-scribed by Nagy et al. (32). Briefly, Adeno-VEGF (1 � 107 or 2 � 107)in 10 AL was injected i.d. into the ear of male nu/nu mice (NationalCancer Institute, Bethesda, MD) to induce angiogenesis. To test theantiangiogenic efficacy of the rAAV vectors, the ear angiogenesisassay was done in three experimental settings: I, a mixture of 2 � 107
Adeno-VEGF and 1 � 1010 rAAV-3TSR (or rAAV-endostatin) in 10 ALwas injected into the mouse ear; II, mice were pretreated with
Fig. 3. Antiangiogenic gene therapy inhibited the growth of orthotopic pancreatictumors. A, severe combined immunodeficient mice first received rAAV i.m. orintrasplenic injections, and tumor cells were implanted 4 wks later. B, mice receivedtumor implantation first, and tumors were allowed to grow for 3 wks.Then,rAAV vectors were injected into the pancreatic tumors. All mice were sacrificed1mo after tumor implantation. 3TSR, rAAV-3TSR; Endo, rAAV-endostatin; IM,intramuscular; IT, intratumoral; IS, intrasplenic. *, P < 0.05 versus control; “ , P < 0.05versus other i.m. groups.
Antiangiogenic GeneTherapy withTSP-1and Endostatin
www.aacrjournals.org Clin Cancer Res 2007;13(13) July1, 20073971
Cancer Research. on September 11, 2013. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from

rAAV-3TSR or rAAV-endostatin (1 � 1010 in 10 AL) ear injection andreceived Adeno-VEGF ear injection in the same sites 2 weeks later; andIII, mice were pretreated with rAAV-3TSR or rAAV-endostatin (1 � 1011
in 100 AL) i.m. injection and received Adeno-VEGF ear injection 2, 4, 6,and 8 weeks later. rAAV-GFP was used as negative control. To study thecombinatory effects of rAAV-3TSR and rAAV-endostatin, mice werepretreated with rAAV-3TSR and/or rAAV-endostatin (1 � 109) earinjection, and Adeno-VEGF (1 � 107) was injected into the same sites2 weeks later. Five days after Adeno-VEGF injection, the ear pictureswere captured with a dissection microscope, and the angiogenic area ofthe mouse ear was measured using IPLab software (Scanalytics, Inc.).Ear samples were collected, fixed in paraformaldehyde-glutaraldehyde,and processed for 1-Am Epon sections as described by Nagy et al. (33).
Immunohistochemistry. Immunohistochemistry was done as de-scribed previously (12) using anti-CD31 antibody (BD PharMingen),anti-endostatin antibody (kindly provided by Dr. Kashi Javaherian,Children’s Hospital, Boston, MA), or anti-TSR antibody.
Image processing and quantification. Microscopic pictures werecaptured using a Spot digital camera mounted to a Nikon TE300microscope. IPLab software was used for quantification of the images.
Tumor microvessel density was quantified via calculating the percentageof total vascular area in a given �20 visual field (0.584 � 0.438 mm2),40 fields for each group. Endostatin staining was quantified bymeasuring the absorbance value of 10 visual fields (�20) for eachgroup. To quantify angiogenesis and edema of the mouse ear 1-Amsections, the area of a 2-mm (from center) ear section was measured.The average thickness of the ear was calculated as the area (in mm2)divided by 2 mm.
Statistics. All tumor volumes and quantified variables wereexpressed as the mean F SE. Statistics was done with GraphPad Prismsoftware (GraphPad Software, Inc.). Student’s t test was used tocompare variables of treated tumors versus untreated control. Samplesize and power of all the analysis were calculated with PS Power andSample Size Program (34). Differences were considered statisticallysignificant when P V 0.05.
Results
Expression of rAAV-3TSR in pancreatic cancer cells and mouseskeletal muscle. Our previous published data showed in vitroexpression of endostatin in rAAV-endostatin–transduced cells(31). Increased endostatin levels were detected in the culturemedium of rAAV-endostatin–transduced human tumor cells,and conditioned medium from those transduced cells signifi-cantly inhibited capillary endothelial cell proliferation (31).Here, we tested the expression of rAAV-3TSR both in vitro andin vivo. Human pancreatic cancer cells (AsPC-1 and MiaPaCa-2)were transduced with rAAV-GFP (control vector) or rAAV-3TSR.Forty-eight hours after transduction, GFP expression wasobserved in rAAV-GFP–transduced cells (Fig. 1B). Culturemedium was changed 48 h after transduction and collected24 h later for 3TSR protein detection. In this way, we verifiedthat the detected 3TSR was secreted by the transduced cellsfollowing de novo synthesis and did not arise from preexistingprotein within the virus preps. Figure 1C shows the secretion of3TSR protein by the rAAV-3TSR–transduced MiaPaCa-2 andAsPC-1 pancreatic cancer cells. 3TSR production was consistentwith the transduction efficiency observed in the control rAAV-GFP transduction. In vivo expression of rAAV-3TSR was detectedvia immunofluorescence staining in mouse skeletal muscle at 5and 9 weeks after a single i.m. injection (Fig. 1D). In controlmice receiving only a rAAV-LacZ injection, no positive 3TSRstaining was observed in the injection sites (Fig. 1D). Theexpression of rAAV-endostatin was tested in wild-type FVBmice. Plasma endostatin level was elevated 2 weeks after i.m.injection and peaked at 4 weeks, and the elevated endostatinlevels persisted at least until 8 weeks after rAAV-endostatininjection.In vivo antiangiogenic efficacy of rAAV-3TSR and rAAV-
endostatin. The antiangiogenic efficacy of rAAV-endostatinand rAAV-3TSR in vivo was studied using an Adeno-VEGF–induced mouse ear angiogenesis model in three experimentalsettings (Fig. 2). Injecting the ears simultaneously with acontrol rAAV-GFP vector did not alter the proangiogenic effectsof Adeno-VEGF (Fig. 2A). In contrast, when Adeno-VEGF wasinjected simultaneously with rAAV-endostatin or rAAV-3TSR,VEGF-induced ear angiogenesis was significantly inhibited(Fig. 2A and B). Pretreatment of mouse ears with i.d. injectionof rAAV-3TSR followed by induction of ear angiogenesis2 weeks later by injection of Adeno-VEGF at the same sitesalso resulted in significant inhibition of ear angiogenesis in therAAV-3TSR pretreated but not control ears (Fig. 2C).
Fig. 4. Expression of endostatin after rAAV-endostatin gene therapy.Tumor tissueand plasma samples were collectedwhen tumor-bearingmicewere sacrificed at theend of the experiments. A, increased endostatin expression in tumor tissue afterintratumoral rAAV-endostatin delivery. Endostatin staining was quantified bymeasuring the intensity of the staining of 10 visual fields (�20) from each group.Bar, 100 Am. B, plasma endostatin levels were elevated in mice treated withrAAV-endostatin.
Cancer Therapy: Preclinical
www.aacrjournals.orgClin Cancer Res 2007;13(13) July1, 2007 3972
Cancer Research. on September 11, 2013. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from

To show the systemic effects of rAAV-3TSR treatment, weinjected rAAV-3TSR i.m. and then induced angiogenesis in themouse ear with the Adeno-VEGF. No significant inhibition of earangiogenesis was seen if the Adeno-VEGF was given 2 weeksafter i.m. injection of rAAV-3TSR. However, at 4, 6, and 8 weeksafter rAAV-3TSR i.m. injection, Adeno-VEGF–induced earangiogenesis was significantly inhibited in the rAAV-3TSR–treated mice compared with control. Figure 2D shows a typicalresult at 6 weeks. Quantification of themouse ear angiogenic areashowed a 61.0% reduction in mice treated with a single i.m.injection of rAAV-3TSR 6 weeks before induction of ear angio-genesis with Adeno-VEGF (Fig. 2D). Adeno-VEGF–inducedmouse ear angiogenesis is characterized by enlarged,thin-walled, serpentine, pericyte-poor, hyperpermeable, andsinusoid-appearing mother vessels, which arise from the enlarge-ment of preexisting microvessel, primarily venules (35). In micepretreated with rAAV-3TSR i.m. injection, the VEGF-inducedmother vessels were limited to the center of the angiogenic areas,and the average thickness of the ear was significantly decreasedcompared with the control animals (Fig. 2E).
Inhibition of orthotopic pancreatic tumor growth after rAAV-3TSR and/or rAAV-endostatin treatment. An orthotopic animalmodel of pancreatic cancer was chosen to evaluate both theantiangiogenic and antitumor efficacy of our novel genetherapy vectors. Figure 3A shows the average tumor volumeand the volume of each individual tumor from control anddifferent treatment groups. There was a significant protectiveeffect against tumor growth in immunocompromised micepretreated with a single i.m. injection of either rAAV-3TSRor rAAV-endostatin 4 weeks before implantation of humanAsPC-1 pancreatic cancer cells into the mouse pancreas. Theaverage tumor volume was decreased by 45.7% (rAAV-3TSR)and 36.2% (rAAV-endostatin), respectively (P < 0.01 versuscontrol). The rAAV-3TSR and rAAV-endostatin pretreatmentswere equally effective; there was no significant differencebetween the average tumor volume of rAAV-3TSR–treatedand rAAV-endostatin–treated mice. Of note, a greater inhibi-tory effect on tumor growth was observed when mice receivedinjections of both rAAV-3TSR and rAAV-endostatin. The aver-age tumor volume was significantly smaller in this combinedtreatment group (60.8% reduction) comparing with those inany single treatment group (P < 0.02).Intrasplenic injection of rAAV-3TSR was also done to allow
uniform hematogenous distribution and expression of thevectors in the liver. Intrasplenic injection with the rAAV-3TSRvector resulted in comparable tumor inhibitory effects as i.m.injection of the same vector.
Treatment of established pancreatic tumors with localizedadministration of rAAV-3TSR and rAAV-endostatin. To mimicthe more clinically relevant situation, when tumors are alreadyestablished, we also treated mice bearing sizable orthotopicpancreatic tumors with intratumoral injection of rAAV-endo-statin or rAAV-3TSR and sacrificed the mice 10 days later. Micein the control group received an intratumoral rAAV-GFPinjection, which showed no effect on tumor volume comparedwith mice receiving rAAV-GFP i.m. As shown in Fig. 3B, a singleintratumoral injection of either rAAV-3TSR or rAAV-endostatinsignificantly decreased the volume of established orthotopicpancreatic tumors (57.1% and 48.8% reduction, respectively).
Detection of endostatin in mouse plasma and tumor tissue afterrAAV-endostatin gene therapy. Due to the high background inELISA assay with mouse plasma and in immunostaining onhuman tumor tissue, we were unable to detect 3TSR protein inmouse plasma or the orthotopic human tumor xenograft fromthe mouse model. Detection of endostatin was used to examinethe pattern of expression of secreted proteins following rAAV-mediated tumor gene therapy. Significantly enhanced endo-statin immunohistochemical staining was observed in tumorsafter injection with rAAV-endostatin; the absorbance value ofthe staining was increased 2.6-fold (Fig. 4A). Plasma endostatinlevels were also elevated in mice treated with rAAV-endostatincompared with control or rAAV-3TSR–treated mice (Fig. 4B).
rAAV-3TSR and rAAV-endostatin gene therapy decreased tumormicrovessel density. We further analyzed change in pancreatictumor microvessel density after treatment with rAAV-endostatinand/or rAAV-3TSR. The average microvessel density wasbetween 7.2% and 7.7% in the i.m. and intratumoral injectioncontrol tumors. As shown in Fig. 5, the tumor microvessel den-sity was significantly decreased in each treatment group. Con-sistent with the decreases noted in tumor volume, mice treatedwith the combination of rAAV-3TSR and rAAV-endostatin
Fig. 5. Antiangiogenic gene therapy decreased tumor microvessel density.Microvessel density (MVD) was defined as the percentage of total microvesselarea in a given �20 (0.582� 0.437 mm2) visual area [region of interest (ROI)].A, severe combined immunodeficient mice first received rAAV i.m. or intrasplenicinjections, and tumor cells were implanted 4 wks later. B, mice received tumorimplantation first, and tumors were allowed to grow for 3 wks.Then, rAAVvectors were injected into the pancreatic tumors. All mice were sacrificed1moafter tumor implantation. 3TSR, rAAV-3TSR; Endo, rAAV-endostatin; IM,intramuscular; IS, intrasplenic; IT, intratumoral. *, P < 0.05 versus control; “ , P < 0.05versus other i.m. groups.
Antiangiogenic GeneTherapy withTSP-1and Endostatin
www.aacrjournals.org Clin Cancer Res 2007;13(13) July1, 20073973
Cancer Research. on September 11, 2013. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from

showed a significantly lower tumor microvessel densitycompared with mice treated with either vector alone, indicatinga stronger antiangiogenic efficacy when the two vectors werecombined.A combination of rAAV-3TSR and rAAV-endostatin exhibited
stronger antiangiogenic efficacy in the mouse ear angiogenesismodel. To further study the combinatorial effects of rAAV-3TSRand rAAV-endostatin, we pretreated mouse ears with a lowerdosage of the rAAV vectors and induced ear angiogenesis withAdeno-VEGF 2 weeks later in the same injection sites. The lowerdose was given to make the detection of any combinatorialeffects easier. Figure 6 shows representative pictures of earangiogenesis from each group. At this lower dosage, neitherrAAV-3TSR nor rAAV-endostatin alone showed significantinhibitory effects on VEGF-induced angiogenesis. However, thecombination of rAAV-3TSR and rAAV-endostatin significantlyinhibited ear angiogenesis induced by Adeno-VEGF (Fig. 6).
Discussion
Antiangiogenic gene therapy offers a powerful strategy forcancer treatment with its capability to maintain sustained levelsof antiangiogenic factors, thereby enhancing their antiangio-genic and antitumor efficacy (19–23, 27). Gene therapy is alsohighly flexible, offering the option of custom tailoring eitherhighly localized or systemic treatments, and is more costeffective than expensive recombinant proteins.
rAAV offers highly efficient as well as long-term in vivoexpression without progressive silencing over time (27) andprovides distinct advantages for antiangiogenic gene therapies.AAV2-mediated in vivo gene transduction has been reported tobe most efficient in skeletal muscle and brain followed byhepatocytes. Consequently, i.m. and intraportal vein injectionhave been the most widely used delivery methods for AAV-mediated systemic therapies, including systemic cancer genetherapy (27). After i.m. or intraportal vein delivery, it takes 4 to6 weeks for rAAV-mediated transgenes to reach steady-stateexpression levels in the circulation (26, 27, 29), and transducedskeletal muscle cells or hepatocytes will persistently synthesize asecreted factor for a prolonged period and thus maintain asustained plasma level of the protein.In the present study, we show that rAAV-mediated delivery of
3TSR or endostatin significantly inhibited the growth oforthotopic pancreatic tumors. The direct antiangiogenic effectof these vectors was clearly shown by decreased ear angiogen-esis in response to VEGF in a mouse ear model and bydecreased tumor microvessel density in the tumor model. Wedelivered rAAV-3TSR via both i.m. and intrasplenic injection,which is used here as a substitute for intraportal vein delivery.Comparable antitumor efficacy was observed in the i.m. andintrasplenic treatment groups. From the clinical perspective,i.m. delivery of rAAV vectors is easier and less invasive, whereasthe potential advantage of overexpressing antiangiogenicfactors in hepatocytes may lie in preventing liver metastasisafter surgical removal of a primary pancreatic tumor, forexample. To our knowledge this is the first time that a TSR-based gene therapy approach has been used successfully toinhibit angiogenesis and tumor progression in a mousepancreatic tumor model or that a combination antiangiogenicapproach using TSP-1 and endostatin has been reported. It alsorepresents the first occasion where we have seen this mouse earangiogenesis model used to screen antiangiogenic gene vectors.Increased antitumor and antiangiogenic efficacy were ob-
served when mice were treated with the combination of rAAV-3TSR and rAAV-endostatin. When the two rAAV vectors wereused in combination, more significant angiogenic inhibitionwas observed in the ear angiogenesis model. Mice treated withthe combination of rAAV-3TSR and rAAV-endostatin alsoshowed significantly decreased tumor volume and tumormicrovessel density compared with mice that received eithervector alone. This is consistent with their possessing distinctmechanisms of action. The antiangiogenic effects of TSP-1 arereportedly mediated by interaction of the TSRs with CD36 onthe endothelial cell membrane (36). 3TSR binds CD36 andsequentially activates p59 fyn, caspase-3, and p38 mitogen-activated protein kinase, triggering apoptosis of microvesselendothelial cells (37). By contrast, endostatin acts by binding totropomyosin, integrins, and matrix metalloproteinases (38–40).The half-lives of 3TSR4 and endostatin are different, complica-ting drug scheduling with recombinant proteins. Stable genetherapy approaches such as described here can overcome theselimitations by maintaining stable systemic levels of both 3TSRand endostatin.To mimic the clinical situation, we also treated established
tumors using localized gene delivery and showed significant
Fig. 6. The combination of rAAV-3TSR and rAAV-endostatin resulted in moresignificant inhibitory effects onVEGF-induced mouse ear angiogenesis. rAAV-3TSRand/or rAAV-endostatin (1 �109) were injected into the mouse ears, and 2 wkslater, Adeno-VEGFwas injected into the same sites. Note lower dose of viral vectorswas used in this experiment to make the detection of any combinatorial effectseasier.The ink marked injection site and needle direction. A, presentative earpictures from each group. B, quantification of ear angiogenesis. 4 Unpublished data.
Cancer Therapy: Preclinical
www.aacrjournals.orgClin Cancer Res 2007;13(13) July1, 2007 3974
Cancer Research. on September 11, 2013. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from

tumor volume reductions after intratumoral rAAV-3TSR orrAAV-endostatin treatment. Similarly, intratumoral delivery ofrAAV vectors expressing angiostatin or tissue inhibitor ofmetalloproteinase-1 has been reported to have significantantitumor efficacy, inhibiting tumor angiogenesis in animalsbearing either Kaposi’s sarcoma or orthotopic glioma (41, 42).Our data also indicate the therapeutic importance of local
levels of antiangiogenic factors. Although it requires f4 weeksfor AAV2-mediated gene expression to reach the steady-statelevel, expression of a transgene commences shortly after thesingle-stranded genome of AAV is converted into a double-stranded structure (27, 43). This is in line with our in vitro datathat production of endostatin and 3TSR could be detectedat 48 to 72 h after transduction (31). A potential advantageof intratumoral gene delivery is that, in a given cell type,expression from an AAV-delivered transgene may be higher incells that are actively dividing because in actively dividing cells,such as tumor cells, the enhanced metabolic rate may pro-mote DNA replication and gene expression (27). In our study,the increased levels of 3TSR and endostatin in the tumormicroenvironment, although not reaching steady-state or peaklevels, were sufficient to shift the angiogenic balance toward theantiangiogenic side, decrease tumor microvessel density, andconsequently inhibit tumor growth. This notion is also supported
by the data from the mouse ear angiogenesis model. Significantinhibition of angiogenesis was observed when rAAV-3TSR andAdeno-VEGF were injected together into the ear. However, whenwe injected rAAV-expressing antiangiogenic factors i.m., signifi-cant inhibition of VEGF-induced ear angiogenesis was observedonly when rAAV was injected at least 4 weeks before the Adeno-VEGF ear injection.In summary, rAAV vectors expressing 3TSR and endostatin
showed significant antiangiogenic efficacy in vivo . Usingexperimental settings that closely mimic clinical situations, weconclude that rAAV-mediated 3TSR and endostatin antiangio-genic gene therapy could provide a promising regimen forpatients with pancreatic cancer as well as other gastrointestinaltumors. The antiangiogenic vector can be delivered i.m. andintratumorally in patients with unresectable pancreatic tumorsusing radiologic guidance or injected into the portal vein aftersurgical removal of the primary tumors.
Acknowledgments
We thank Drs. Harold F. Dvorak and Janice A. Nagy for providing Adeno-VEGFand the mouse ear angiogenesis model and Eleanor Manseau for processing the1-Am ear sections.
References1. FolkmanJ. Role of angiogenesis in tumor growth andmetastasis. Semin Oncol 2002;29:15^8.
2. Folkman J. Tumor angiogenesis: role in regulation oftumor growth. Symp Soc Dev Biol 1974;30:43^52.
3.HanahanD, FolkmanJ. Patterns and emergingmech-anisms of the angiogenic switch during tumorigene-sis. Cell 1996;86:353^64.
4. Hanahan D,Weinberg RA. The hallmarks of cancer.Cell 2000;100:57^70.
5. Khan AW, Dhillon AP, Hutchins R, et al. Prognosticsignificance of intratumoural microvessel density(IMD) in resected pancreatic and ampullary cancersto standard histopathological variables and survival.EurJ Surg Oncol 2002;28:637^44.
6. Ikeda N, Adachi M, Taki T, et al. Prognostic signifi-cance of angiogenesis in human pancreatic cancer.BrJCancer1999;79:1553^63.
7. Lawler J. The functions of thrombospondin-1and-2.Curr Opin Cell Biol 2000;12:634^40.
8. Lawler J, Detmar M. Tumor progression: the effectsof thrombospondin-1and -2. Int J Biochem Cell Biol2004;36:1038^45.
9. Folkman J. Endogenous angiogenesis inhibitors.APMIS 2004;112:496^507.
10.MiaoWM, SengWL, Duquette M, Lawler P, Laus C,Lawler J. Thrombospondin-1 type 1 repeat recombi-nant proteins inhibit tumor growth through transform-ing growth factor-h-dependent and -independentmechanisms. Cancer Res 2001;61:7830^9.
11.Yee KO, Streit M, HawighorstT, Detmar M, LawlerJ.Expressionof the type-1repeats of thrombospondin-1inhibits tumor growth through activation of transform-ing growth factor-h. AmJPathol 2004;165:541^52.
12. Zhang X, Galardi E, Duquette M, Delic M, LawlerJ,Parangi S. Antiangiogenic treatment with the threethrombospondin-1type 1repeats recombinant proteinin an orthotopic human pancreatic cancer model. ClinCancer Res 2005;11:2337^44.
13. Zhang X, Galardi E, Duquette M, Lawler J, ParangiS. Antiangiogenic treatment with three thrombospon-din-1 type 1 repeats versus gemcitabine in an ortho-topic human pancreatic cancer model. Clin CancerRes 2005;11:5622^30.
14. Westphal JR. Technology evaluation: ABT-510,Abbott. Curr Opin MolTher 2004;6:451^7.
15. Hoekstra R, de Vos FY, Eskens FA, et al. Phase Istudy of the thrombospondin-1-mimetic angiogene-sis inhibitor ABT-510 with 5-fluorouracil and leuco-vorin: a safe combination. Eur J Cancer 2006;42:467^72.
16. Hoekstra R, de Vos FY, Eskens FA, et al. Phase Isafety, pharmacokinetic, and pharmacodynamic studyof the thrombospondin-1-mimetic angiogenesis inhib-itorABT-510 in patients with advanced cancer. J ClinOncol 2005;23:5188^97.
17. Herbst RS, Hess KR, Tran HT, et al. Phase I studyof recombinant human endostatin in patients withadvanced solid tumors. J Clin Oncol 2002;20:3792^803.
18.ThomasJP, Arzoomanian RZ, Alberti D, et al. PhaseI pharmacokinetic and pharmacodynamic study ofrecombinant human endostatin in patients withadvancedsolid tumors. JClinOncol 2003;21:223^31.
19. Kisker O, Becker CM, Prox D, et al. Continuousadministration of endostatin by intraperitoneallyimplanted osmotic pump improves the efficacy andpotency of therapy in amouse xenograft tumormodel.Cancer Res 2001;61:7669^74.
20. Capillo M, Mancuso P, Gobbi A, et al. Continuousinfusion of endostatin inhibits differentiation,mobiliza-tion, and clonogenic potential of endothelial cell pro-genitors. Clin Cancer Res 2003;9:377^82.
21.Morishita T, Mii Y, Miyauchi Y, et al. Efficacy of theangiogenesis inhibitor O-(chloroacetyl-carbamoyl)-fumagillol (AGM-1470) on osteosarcoma growthand lung metastasis in rats. Jpn J Clin Oncol 1995;25:25^31.
22. Drixler TA, Borel Rinkes IH, Ritchie ED, vanVroonhovenTJ, Gebbink MF,Voest EE. Continuousadministration of angiostatin inhibits acceleratedgrowth of colorectal liver metastases after partialhepatectomy.CancerRes2000;60:1761^5.
23. ZhangX,ConnollyC,DuquetteM, LawlerJ, ParangiS. Continuous administration of the three throm-bospondin-1 type 1 repeats recombinant proteinimproves the potency of therapy in an orthotopic
human pancreatic cancer model. Cancer Lett2007;247:143^9.
24. Feldman AL, Restifo NP, Alexander HR, et al. Anti-angiogenic gene therapy of cancer utilizing a recombi-nant adenovirus to elevate systemic endostatin levelsin mice. Cancer Res 2000;60:1503^6.
25. Ding I, SunJZ, Fenton B, et al. Intratumoral admin-istrationof endostatin plasmid inhibits vascular growthand perfusion in MCa-4 murine mammary carcino-mas. Cancer Res 2001;61:526^31.
26. NoroT, Miyake K, Suzuki-Miyake N, et al. Adeno-associated viral vector-mediated expression of endo-statin inhibits tumor growth and metastasis in anorthotropic pancreatic cancer model in hamsters.Cancer Res 2004;64:7486^90.
27. Ponnazhagan S, Curiel DT, Shaw DR, Alvarez RD,Siegal GP. Adeno-associated virus for cancer genetherapy. Cancer Res 2001;61:6313^21.
28. Li C, Bowles DE, van DykeT, Samulski RJ. Adeno-associated virus vectors: potential applications forcancer gene therapy. Cancer Gene Ther 2005;12:913^25.
29. ShiW,Teschendorf C, Muzyczka N, Siemann DW.Adeno-associated virus-mediated gene transfer ofendostatin inhibits angiogenesis and tumor growthin vivo. Cancer GeneTher 2002;9:513^21.
30. Subramanian IV, Ghebre R, Ramakrishnan S.Adeno-associated virus-mediated delivery of a mu-tant endostatin suppresses ovarian carcinoma growthin mice. Gene Ther 2005;12:30^8.
31. Nguyen JT,Wu P, Clouse ME, Hlatky L,TerwilligerEF. Adeno-associated virus-mediated delivery of anti-angiogenic factors as an antitumor strategy. CancerRes1998;58:5673^7.
32. Nagy JA,Vasile E, Feng D, et al. VEGF-A inducesangiogenesis, arteriogenesis, lymphangiogenesis,and vascular malformations. Cold Spring Harb SympQuant Biol 2002;67:227^37.
33. Nagy JA, Morgan ES, Herzberg KT, Manseau EJ,Dvorak AM, DvorakHF. Pathogenesis of ascites tumorgrowth: angiogenesis, vascular remodeling, and stro-ma formation in the peritoneal lining. Cancer Res1995;55:376^85.
Antiangiogenic GeneTherapy withTSP-1and Endostatin
www.aacrjournals.org Clin Cancer Res 2007;13(13) July1, 20073975
Cancer Research. on September 11, 2013. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from

34. Dupont WD, PlummerWD. PS power and samplesize program available for free on the Internet. ControlClinTrials 1997;18:274.
35. Dvorak HF. Rous-Whipple Award Lecture. Howtumors make bad blood vessels and stroma. Am JPathol 2003;162:1747^57.
36. Lawler J. Thrombospondin-1as an endogenous in-hibitor of angiogenesis and tumor growth. J Cell MolMed 2002;6:1^12.
37. Jimenez B, Volpert OV, Crawford SE, FebbraioM, Silverstein RL, Bouck N. Signals leading toapoptosis-dependent inhibition of neovasculariza-
tion by thrombospondin-1. Nat Med 2000;6:41^8.
38. Dhanabal M, Ramchandran R,Waterman MJ, et al.Endostatin induces endothelial cell apoptosis. J BiolChem1999;274:11721^6.
39. HanaiJ,DhanabalM,KarumanchiSA,etal.Endosta-tin causes G1arrest of endothelial cells through inhibi-tionofcyclinD1. JBiolChem2002;277:16464^9.
40. Lee SJ, JangJW, KimYM, et al. Endostatin binds tothe catalytic domain of matrix metalloproteinase-2.FEBSLett 2002;519:147^52.
41. Ma HI, Lin SZ, ChiangYH, et al. Intratumoral gene
therapy of malignant brain tumor in a rat model withangiostatin delivered by adeno-associated viral(AAV) vector. GeneTher 2002;9:2^11.
42. ZacchignaS,ZentilinL,MoriniM,etal.AAV-mediatedgene transfer of tissue inhibitor of metalloproteinases-1inhibits vascular tumorgrowthandangiogenesis invivo.CancerGene Ther2004;11:73^80.
43.TeramotoS,BartlettJS,McCartyD,XiaoX,SamulskiRJ,BoucherRC.Factors influencingadeno-associatedvirus-mediated gene transfer to human cystic fibrosisairway epithelial cells: comparison with adenovirusvectors. JVirol1998;72:8904^12.
Cancer Therapy: Preclinical
www.aacrjournals.orgClin Cancer Res 2007;13(13) July1, 2007 3976
Cancer Research. on September 11, 2013. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from
Related Documents











