i ADDIS ABABA UNIVERSITY COLLEGE OF HEALTH SCIENCE SCHOOL OF PUBLIC HEALTH THE ROLE OF HOUSEHOLD FUEL EXPOSURE AND HOUSING CHARACTERISTICS ON ASTHMA IN SELECTED PUBLIC HOSPITALS OF ADDIS ABABA, ETHIOPIA: MATCHED CASE CONTROL STUDY DESIGN By Yonas Abebe (Bsc) A THESIS SUBMITTED TO THE SCHOOL OF PUBLIC HEALTH OF GRADUATE STUDIES ADDIS ABABA UNIVERSITY, IN PARTIAL FULFILLMENT OF THE REQUIREMENT FOR MASTER DEGREE OF PUBLIC HEALTH IN EPIDEMIOLOGY AND BIOSTATISTICS. Addis Ababa, Ethiopia October 2020

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
i
ADDIS ABABA UNIVERSITY
COLLEGE OF HEALTH SCIENCE
SCHOOL OF PUBLIC HEALTH
THE ROLE OF HOUSEHOLD FUEL EXPOSURE AND
HOUSING CHARACTERISTICS ON ASTHMA IN SELECTED
PUBLIC HOSPITALS OF ADDIS ABABA, ETHIOPIA:
MATCHED CASE CONTROL STUDY DESIGN
By Yonas Abebe (Bsc)
A THESIS SUBMITTED TO THE SCHOOL OF PUBLIC HEALTH
OF GRADUATE STUDIES ADDIS ABABA UNIVERSITY, IN
PARTIAL FULFILLMENT OF THE REQUIREMENT FOR MASTER
DEGREE OF PUBLIC HEALTH IN EPIDEMIOLOGY AND
BIOSTATISTICS.
Addis Ababa, Ethiopia
October 2020
ii
ADDIS ABABA UNIVERSITY
COLLEGE OF HEALTH SCIENCE
SCHOOL OF PUBLIC HEALTH
DEPARTMENT OF PREVENTIVE MEDICINE
MASTER OF PUBLIC HEALTH
RESEARCH PROJECT SUBMISSION FORM
Name of investigator Yonas Abebe (BSC.)
Name of Advisor(s) Prof. Ahmed Ali (MPH., PhD)
Dr. Adamu Addissie (MD., PhD)
Dr. Tewodros Haile (MD., Pulmonologist)
Full title of the research project The role of household fuel exposure and housing
characteristics on asthma in selected public hospitals of
Addis Ababa, Ethiopia, 2020.
Matched Case control study design
Duration of project September 2019 – September 2020
Study Area Addis Ababa, Ethiopia
Address of investigator Tel: +251944162181
Mail: [email protected]
iii
Examiners’ Approval Sheet
We, the undersigned, members of the Board of Examiners of the final open defense by Yonas
Abebe Mezemir , have read and evaluated his thesis entitled “The role of household fuel
exposure and housing characteristics on asthma in selected public hospitals of Addis Ababa,
Ethiopia ,2020.” This is to verify that the thesis has been accepted in partial fulfillment of the
requirements for the Master of Public Health Degree in “Epidemiology and Biostatistics”
Name of internal examiner:
Signature ___________
Date:
Name of external examiner:
Date
Signature ___________

iv
Acknowledgment
Above all I would like to thank God, who has helped me through the whole time and
then my deepest gratitude goes to AAU, College of Health Science, and School of
Public Health, Department of Preventive Medicine for giving the chance to take part
in this interesting program and valuable support in academic and research process. It
is also my pleasure to thank my Advisors, Prof. Ahmed Ali, Dr. Adamu Adissie and
Dr. Tewoderos Haile for their encouragement and guidance for conducting this
Thesis Research. My special thanks go to Dr. Abera Kumi and Mulugeta Tamir for
their comments, suggestions and support. I would also like to thank Tikur Anbessa
Specialized Hospital, Saint Paul Hospital Millennium Medical College and Yekatite
12 Hospital for their kindest collaboration for allowing us to conduct the data
collection process in their chest clinic and internal medicine outpatient departments.
Last, but not least, I would like to acknowledge data collectors, families and friends
for their support to the study.
v
Table of Contents Examiners’ Approval Sheet ......................................................................................................................... iii
Acknowledgment ......................................................................................................................................... iv
List of tables ............................................................................................................................................... viii
List of figures ............................................................................................................................................... ix
List of annexes .............................................................................................................................................. x
List of abbreviation and acronyms ............................................................................................................... xi
Abstract ...................................................................................................................................................... xii
1. Introduction ........................................................................................................................................... 1
1.1 Background ......................................................................................................................................... 1
1.2 Statement of the problem .................................................................................................................. 2
1.3 Rationale of the study ......................................................................................................................... 4
1.4 Significance of the study ..................................................................................................................... 4
2. Literature review ................................................................................................................................... 5
2.1 Magnitude of asthma .......................................................................................................................... 5
2.2 Factors associated with asthma .......................................................................................................... 6
2.2.1 Socio economic and demographic characteristics and asthma ................................................... 6
2.2.2 Behavioural factors and asthma .................................................................................................. 8
2.2.3 Household fuel exposure and asthma ......................................................................................... 8
2.2.4 Housing characteristics and asthma .......................................................................................... 10
2.2.5 Other factors and asthma .......................................................................................................... 11
2.3 Conceptual frame work .................................................................................................................. 13
3. Research question and objectives ....................................................................................................... 14
3.1 Research question ............................................................................................................................. 15
3.2 Research Hypothesis ......................................................................................................................... 15
3.2.1 Null hypothesis ........................................................................................................................... 15
3.2.2 Alternative hypothesis ............................................................................................................... 15
3.3 Objective ........................................................................................................................................... 15
3.3.1 General objective ........................................................................................................................... 15
3.3.2 Specific objectives .......................................................................................................................... 15
4. Methods and materials ........................................................................................................................ 16
4.1 Study area ......................................................................................................................................... 16
vi
4.2 population ......................................................................................................................................... 17
4.2.1 Target population....................................................................................................................... 17
4.2.2 Source population ...................................................................................................................... 17
4.2.3 Study population ........................................................................................................................ 17
4.2.4 Study unit ................................................................................................................................... 17
4.2.5 Inclusion criteria ......................................................................................................................... 17
4.2.6 Exclusion criteria ........................................................................................................................ 17
4.3 Study Design and study period ...................................................................................................... 18
4.4 Sample size calculation................................................................................................................... 18
4.5 Sampling procedure .......................................................................................................................... 20
4.6 Study variables .................................................................................................................................. 22
4.6.1 Dependent variable .................................................................................................................... 22
4.6.2 Independent variables ............................................................................................................... 22
4.6.2.1 Socio-demographic characteristics ......................................................................................... 22
4.6.2.2 Main exposure variables ......................................................................................................... 22
4.6.2.3 Confounding variables ............................................................................................................ 22
4.7 Data collection procedure ................................................................................................................. 23
4.8 Data Quality management ................................................................................................................ 23
4.9 Data analysis procedure .................................................................................................................... 24
4.10 Operational definitions ................................................................................................................. 25
4.11 Ethical consideration ....................................................................................................................... 27
4.12 Dissemination of findings ................................................................................................................ 28
5. Results ................................................................................................................................................. 29
5.1 Descriptive analysis ........................................................................................................................... 29
5.2 Association of different Characteristics of participant with Asthma ................................................ 48
6. Discussions ......................................................................................................................................... 53
7. Strengths and limitations of the study ................................................................................................. 57
7.1. Strengths .............................................................................................................................................. 57
7.2 Limitations ............................................................................................................................................ 57
8. Conclusions and recommendations ..................................................................................................... 58
8.1 Conclusions ........................................................................................................................................... 58
8.2 Recommendations ................................................................................................................................ 58

vii
9. References .......................................................................................................................................... 59
viii
List of tables
Table 1- Sample size determination for objective 1…….………………………………………18
Table 2- Sample size determination for objective 2…….………………………………………19
Table 3- Sample size determination for objective 3………….…………………………………19
Table 4- Socio-demographic characteristics of participants in selected public hospitals of Addis
Ababa, Ethiopia, 2020 …………………………………………………………………………..29
Table 5: Characteristics [mean (±SD)] of participants in selected public hospitals of Addis
Ababa, Ethiopia, 2020…………………………………………………………………………...30
Table 6: Housing characteristics of participants in selected public hospitals of Addis Ababa,
Ethiopia, 2020…………………………………………………………………………………....31
Table 7: Cooking room characteristics of participants in selected public hospitals of Addis
Ababa, Ethiopia, 2020………………………………………………………………………….32
Table 8: stove type characteristics of participants in selected public hospitals of Addis Ababa,
Ethiopia, 2020 ………………………………………………………………………………....34
Table 9: Current household fuel characteristics of participants in selected public hospitals of
Addis Ababa, Ethiopia, 2020 …………………………………………………………………35
Table 10: Lifetime household fuel characteristics of participants in selected public hospitals of
Addis Ababa, Ethiopia, 2020………………………………………………………………….36
Table 11: Pet characteristics, life style and nutritional status of participants in selected public
hospitals of Addis Ababa, Ethiopia, 2020…………………………………………………….40
Table 12: Medical condition characteristics of participants in selected public hospitals of Addis
Ababa, Ethiopia, 2020…………………………………………………………………………41
Table 13: Conditional multivariable logistic regression analysis of factors associated with asthma
among participants in selected public hospitals of Addis Ababa, Ethiopia, 2020…………….45

ix
List of figures
Figure 1- Conceptual frame work on factors that affect asthma taken from different works of
literature…………….……………………………………………………………………………14
Figure 2- Map of study area ……………………………………...…………………………….16
Figure 3; Schematic presentation of sampling procedure ………………………………………21
Figure 4: Door opening practice while cooking among participants in selected hospitals of Addis
Ababa, Ethiopia, 2020 …………………………………………………………………………33
Figure 5: Life time agricultural residues using status for household fuel among participants in
selected hospitals of Addis Ababa, Ethiopia, 2020 ……………………………………………37
Figure 6: Life time wood using status for household fuel among participants in selected hospitals
of Addis Ababa, Ethiopia, 2020 ………………………………………………………………38
x
List of annexes
Annex 1- Information sheet (English version)…………………………………………..………58
Annex 2- Informed consent (English version)…………………………………………………..61
Annex 3- Screening questionnaire (English version)…………………………………………...62
Annex 4- Survey questionnaire (English version)………………………………………………63
Annex 5- Information sheet (Amharic version)…………………………………………………69
Annex 6- Informed consent (Amharic version)…………………………………………………71
Annex 7- Screening questionnaire (Amharic version)………………………………………….72
Annex 8- Survey questionnaire (Amharic version)…………………………………………..…73
Annex 9: A manual for training of data collectors and supervisors …………………………….78
Annex 10: Curriculum vitae ……………………………………………………………………85
Annex 11: Assurance of principal investigator………………………………………………….88
xi
List of abbreviation and acronyms
ATS- American Thoracic Society
BMI- Body Mass Index
COPD- Chronic Obstructive Pulmonary Disease
CI- Confidence Interval
COR- Crude Odds Ratio
CRD- Chronic Respiratory Diseases
DALYS- Disability Adjusted Life Years
ECRHS II- European Community Respiratory Health Survey II
FMHACA- Food Medicine Health Care Administration and Control Authority
FMOH- Federal Ministry of Health
GBD- Global Burden of Disease
GINA- Global Initiative for Asthma
IAQ- Indoor Air Quality
ISAAC- International Study of Asthma and Allergies in Childhood
LRTI- Lower Respiratory Tract Infectious
MMMF- Man Made Mineral Fibers
MOR- Matched Odd Ratio
NCDs- Non Communicable Diseases
OPD- Out Patient Department
OR- Odds Ratio
PTB- Pulmonary Tuberculosis
SD- Standard Deviations
SPHMMC- St, Paul Hospital millennium medical college
SPSS- Statistical Package for Social Sciences
TASH- Tikur Anbessa Specialized Hospital
UK- United Kingdom
USA- United States of America
VIF- Variance Inflation Factor
VOC- Volatile Organic Compound
WHO- World Health Organization
xii
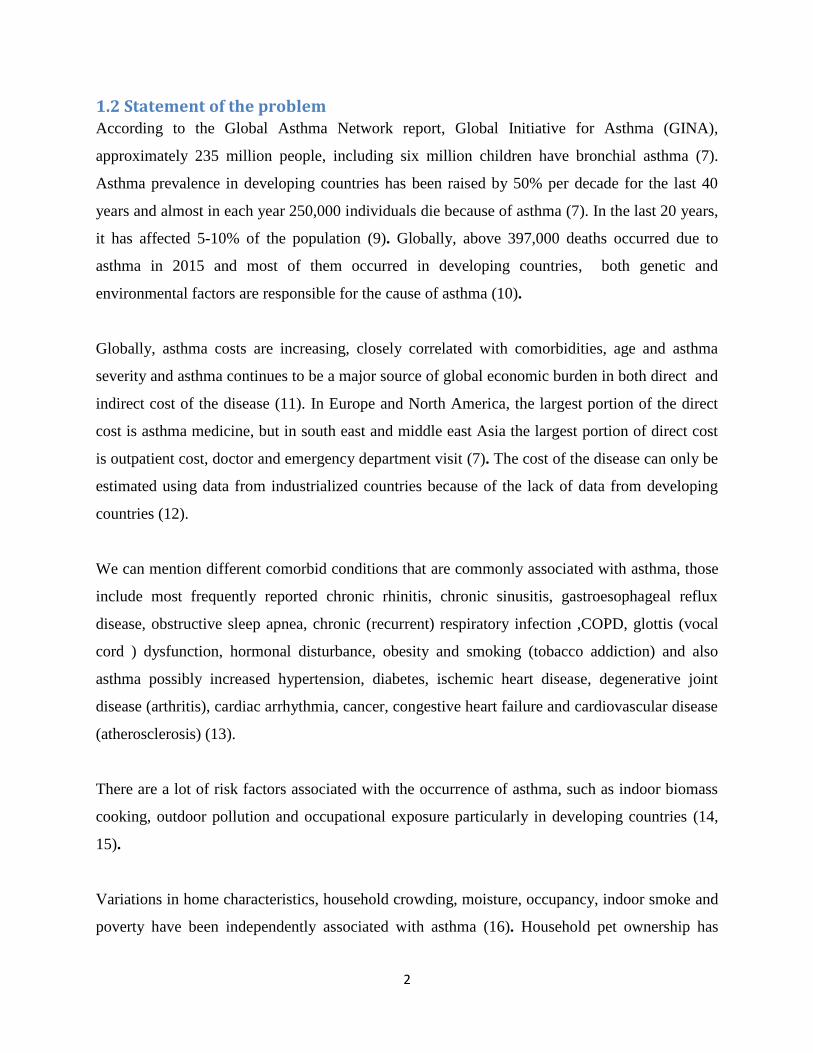
Abstract Introduction: Asthma is a chronic inflammatory disorder characterized by airway obstruction
and hyper responsiveness. Studies have suggested that household fuel exposure; either biomass
or fossil fuel and housing characteristics have been associated with allergy. Recent analysis has
also shown an increase in asthma among residential determinants of allergy. But there remains
considerable uncertainty about whether this reflects an association with asthma. Hence this study
was conducted to elucidate selected factors associated with asthma.
Objective: To examine whether there is an association between household fuel exposure and
housing characteristics with asthma at selected public hospitals in Addis Ababa, Ethiopia.
Methods: Hospital-based case-control study design, matched with age and sex was done.
Among four hundred eighty three participants, 161 were cases and 322 were controls selected
using consecutive sampling technique from selected public hospitals in Addis Ababa, Ethiopia.
Double population proportions formula with a 2:1 control to case ratio was used to calculate
sample size with 95% confidence interval and 80% power. Data were collected between
February and August, 2020 using structured questionnaire, entered into EPI info version 7.2 and
then analyzed using SPSS version 24. Chi-square test was used to assure statistical significance.
Conditional logistic regression model was applied to see the determinants of asthma. Both crude
and adjusted odds ratios with 95% confidence interval (CI) were used to identify the strength,
direction and significance of the association.
Results: Among study subjects the odds of developing asthma was 4 times higher among those
who used agricultural residues for cooking (AOR: 3.809, 95% CI: 1.052, 13.79). , 5 times higher
among those who used wood for cooking (AOR: 4.954, 95% CI: 2.1, 11.686). 5 times higher
among those who had family history of asthma (AOR: 4.725, 95% CI: 1.544, 14.454), 6 times
higher among those who smoke tobacco (AOR: 6.16, 95% CI: 1.304, 29.098) and 10 times
higher among those who don’t practice door opening, while cooking (AOR: 10.254, 95% CI:
3.969, 26.49).
Conclusion: To reduce the risk of asthma development, people should practice door opening,
while cooking, and must avoid using wood and agricultural residues for cooking and tobacco for
smoking. Family history of asthma was also noted to be another risk factor for asthma.
Key words: Household fuel exposure, Housing characteristic, TASH, SPHMMC, Asthma,
Ethiopia

1
1. Introduction
1.1 Background
Globally, around three billion people and 90% of rural households in developing countries rely
on kerosene, biomass and coal as primary source of cooking energy, those are typically burnt
indoors in open fires or poorly functioning stoves, often causing extreme pollution most of the
time women spent many hours breathing smoke, while cooking (1, 2) . Household air pollution
from inefficient cooking practices with solid fuels and kerosene causes non-communicable
diseases, including chronic respiratory diseases (1).
Chronic respiratory diseases (CRD) could broadly be classified in to two, bronchial asthma and
chronic pulmonary disease. Chronic pulmonary disease is classified in to three, chronic
obstructive pulmonary diseases (COPD), chronic occupational lung diseases and chronic
interstitial lung diseases (3).
Asthma is a chronic disease that affects the airways of the lungs. Airways are the breathing tubes
that are responsible for the movement of air in and out of the lung (4). The inflammation of the
airway causes swelling and the swelling causes the airways to make thick, sticky secretions
called mucus. Asthma causes the muscles in and around the airways to get very tight or constrict,
those three physiological changes on the airway, including swelling, mucus secretion, and tight
muscles can make the airways narrower than normal and it becomes very hard to get air into and
out of the lungs (5). It features variable airway obstruction and bronchial hyper responsiveness.
Clinically, asthmatics exhibit upper respiratory symptoms, like cough and lower respiratory
symptom like recurrent episodes of wheeze, chest tightness, and shortness of breath (6). The
2018 global asthma report states that asthma affects 339 million people in the world (7).
Asthma can be classified in to two persistent or intermittent based on the occurrence of the
symptom and also it can be classified in to seven based on the exacerbation factors, including
allergic asthma, non-allergic asthma, mixed asthma, occupational asthma, exercise-induced
asthma, cough variant asthma and aspirin-induced asthma (8).
2
1.2 Statement of the problem According to the Global Asthma Network report, Global Initiative for Asthma (GINA),
approximately 235 million people, including six million children have bronchial asthma (7).
Asthma prevalence in developing countries has been raised by 50% per decade for the last 40
years and almost in each year 250,000 individuals die because of asthma (7). In the last 20 years,
it has affected 5-10% of the population (9). Globally, above 397,000 deaths occurred due to
asthma in 2015 and most of them occurred in developing countries, both genetic and
environmental factors are responsible for the cause of asthma (10).
Globally, asthma costs are increasing, closely correlated with comorbidities, age and asthma
severity and asthma continues to be a major source of global economic burden in both direct and
indirect cost of the disease (11). In Europe and North America, the largest portion of the direct
cost is asthma medicine, but in south east and middle east Asia the largest portion of direct cost
is outpatient cost, doctor and emergency department visit (7). The cost of the disease can only be
estimated using data from industrialized countries because of the lack of data from developing
countries (12).
We can mention different comorbid conditions that are commonly associated with asthma, those
include most frequently reported chronic rhinitis, chronic sinusitis, gastroesophageal reflux
disease, obstructive sleep apnea, chronic (recurrent) respiratory infection ,COPD, glottis (vocal
cord ) dysfunction, hormonal disturbance, obesity and smoking (tobacco addiction) and also
asthma possibly increased hypertension, diabetes, ischemic heart disease, degenerative joint
disease (arthritis), cardiac arrhythmia, cancer, congestive heart failure and cardiovascular disease
(atherosclerosis) (13).
There are a lot of risk factors associated with the occurrence of asthma, such as indoor biomass
cooking, outdoor pollution and occupational exposure particularly in developing countries (14,
15).
Variations in home characteristics, household crowding, moisture, occupancy, indoor smoke and
poverty have been independently associated with asthma (16). Household pet ownership has
3
attracted considerable attention as an early life environment exposure, which might play a role in
the development of asthma and allergy (17).
Combustion indoors produces both gases (e.g. nitrogen dioxide, carbon monoxide) and
particulate matter that may affect the development or exacerbation of asthma (18). Researches
done in Nigeria and India show that biomass fuel is associated with increase in the risk of
developing of asthma by increasing the concentration of indoor air pollutants (19, 20). Not only
biomass fuel, but also indoor cooking with gas stoves were positively associated with both
allergy and asthma prevalence (21). In contrast to the above studies, research done in Bangladesh
concludes that there is no significant association between indoor air pollutants from biomass fuel
use and respiratory diseases especially with asthma (22).
The risk factors for asthma have been identified, but the cause of asthma is not known. Women
are at risk for developing severe asthma because of many conditions (23). Social, psychological
and physical factors in the environment may increase the risk for Asthma, including poverty,
housing condition and indoor allergen exposures(24). There are conflicting evidences regarding
the association between selected factors (indoor fuel exposure and housing characteristics) and
asthma (21, 22, 25).
Most of the researches on this area are done in developed countries as a way of understanding
the effect of household fuel exposure on asthma(21, 25). In Africa, only few studies exist(19,
25). And in Ethiopia, few studies tried to assess the risk factors for asthma(26). And yet there are
no published studies on the association between household fuel exposure with housing
characteristics and asthma in Ethiopia.
It is inappropriate to assume that previously observed relationships between household fuel
exposure with housing characteristics and chronic respiratory disease applied in all contexts (27).
Therefore, this study is intended to fill the information gap particularly in Ethiopia, in this area
of, which the association between selected factors (such as household fuel exposure and housing
characteristics) and asthma in the study area.

4
1.3 Rationale of the study Despite the large population at risk worldwide, the effect of exposure to indoor solid fuel smoke
has not been adequately studied (28). This study added knowledge on asthma and factors
associated with it, such as household fuel exposure, housing characteristics, pet ownership,
obesity, smoking, alcohol drinking, family history of asthma and physical activity. There are
many types of research that describe the relation between chronic respiratory disease and their
risk factors. But only a few researches explore the potential risk factor for asthma particularly in
Ethiopia (29). So, this study could provide more information about selected factors and their
contribution towards asthma and it may be important for researchers who are interested in this
area.
1.4 Significance of the study The findings from this study could give insight on selected factors including, household fuel
exposure and housing characteristics and its association with asthma. Then the results used to
influence governmental and non-governmental organizations by performing different actions that
may reduce air pollution from biomass fuel. And also the data obtained from the study may have
its own contribution to policy makers, such as FMOH and regulatory organization, by designing
environmental policy which enforces better ventilation system in cooking rooms. such as
FMHACA for planning and evaluating the management of asthma. And also to help individuals
to understood the effect of household fuel exposure on asthma in Ethiopia.

5
2. Literature review
2.1 Magnitude of asthma
Death from non-communicable diseases scores around 41 million people each year that accounts
for 71% of all deaths globally (30). Based on the prevalence rate, NCDs could be ordered, with
the first being cardiovascular diseases accounting for most NCD deaths, or 17.9 million people
annually, followed by cancers (9.0 million), respiratory diseases (3.9million), and diabetes (1.6
million) (31).
In Ethiopia, NCDs are estimated to account for 39% of all deaths, which include, 16%
Cardiovascular diseases, 7% Cancers, 2% Chronic respiratory diseases, 2% Diabetes, 12% Other
NCDs, and the other 49% represent for Communicable, maternal, perinatal and nutritional
conditions, and 12% for Injuries (32).
The Global Burden of Disease (GBD) study estimated that there were 339.4 million people
worldwide affected by asthma globally and asthma is ranked 16th among the leading causes of
years lived with disability and 28th among the leading causes of burden of disease (7). The
worldwide number of asthma death is about 180,000 per year, with a wide variation between
continents, regions, age and economic groups (11). The highest prevalence (≥20%) was
generally observed in English speaking countries of Australasia, Europe and North America, and
in parts of Latin America and the lowest prevalence (<5%) was observed in the Indian
subcontinent, Asia-Pacific, Eastern Mediterranean, and Northern and Eastern Europe (33).
The prevalence of asthma in younger adults, aged 18-45 years, overall, 4.3% of the global
population in this age group reported a doctor’s diagnosis of asthma, 4.5% reported either a
doctor’s diagnosis or that they were taking treatment for asthma, and 8.6% reported that they had
experienced attacks of wheezing or whistling breath (symptoms of asthma) in the preceding 12
months in Australia, Northern and Western Europe, and Brazil had the highest prevalence (7).
Almost 44 million people in the East Asia or Pacific Region have asthma, although the
prevalence rates vary markedly throughout the Region (33). The age distribution of the burden of
asthma, represented as DALYs per 100,000 persons, follows a bimodal distribution with peaks at
age 10-14 years and at age 75-79 years and the lowest burden occurs at age 30-34 years. The
6
burden is similar in males and females at ages below 30-34 years. However, in older adults, the
burden is higher in males and increases with age (7). The prevalence of clinical asthma were
different in different countries, Australia 21.5%, Sweden 20.2%, UK 18.2%, Netherland 15.3%
and Brazil at 13.0% (34).
In Africa, intercountry prevalence data are limited to the International Study of Asthma and
Allergies in Childhood (ISAAC) in which seven African countries participated (English-
speaking regions: Ethiopia 9.1%, Kenya 15.8%, Nigeria 13.0%, and South Africa 20.3%; and
French-speaking regions: Algeria 8.7%, Morocco 10.4%, and Tunisia 11.9% . Symptom rates are
lower than in industrialized countries (35). The prevalence of asthma in sub-Saharan Africa
among adults is less studied or understood (36).
In Ethiopia, according to the latest WHO data published in 2017 asthma death reached 6,269 or
0.99% of total death (37). The age-adjusted death rate is 11.98% per 100,000 of population ranks
Ethiopia 50th
in the world. Among the leading causes of death in Ethiopia, asthma is ranking 24th
(37). The prevalence of asthma in different Ethiopian cities have different values ,for instance, a
study done in Addis Ababa, reported that 18.2% have had wheezing and 2.8% reported to have
bronchial asthma among school children (38), In Debre Berhan, the prevalence of bronchial
asthma among adult patient was 29.6% (26) . In Gonder, 2.2% children claimed to have a label
of bronchial asthma (39) , another study state that the prevalence of asthma in urban and rural
Ethiopia is 3.6% and 1.3% respectively (40) and also the prevalence of wheeze in urban and rural
parts of Butajira is 9.5% and 11.5% respectively (41).
2.2 Factors associated with asthma
2.2.1 Socio economic and demographic characteristics and asthma
Parental history, female sex, low physical activity, and malnutrition, have been described as risk
factors together with pesticides, insecticides, wood or kerosene heating, grass mats, mud and
cow dung, smoking, and car and truck diesel exhaust (4).
Demographic factors
Age
Based on the research conducted in Nigeria, increasing age was associated with a reduced risk of
ever wheezing, current wheeze, and any respiratory symptoms evaluated (19). Another cross-

7
sectional study of 7649 people aged 5 years or more from the Butajira Rural Health Project
Database, suggested that the prevalence of both wheeze and asthma increased significantly with
age (41). In contrast to this, study conduct in Nigeria reported that age was not significantly
associated with asthma symptoms or signs (42). Based on the study conducted to assess
prevalence and determinants of asthma in adults in Kinshasa, state that the distribution of asthma
was similar for various age groups (43).
Gender
Asthma prevalence and risk factors study in Northern Portugal conclude that asthma prevalence
was higher for boys than for girls (44). In contradiction to that, study in Ethiopia suggest that
there was no significant difference in the prevalence of allergic disorders between gender (45).
Biomass fuel exposure and asthma symptoms assessment research in Nigeria says that the
prevalence of current wheeze and any of the asthma symptoms were significantly higher in
females than males (19). Another cross sectional community survey in Nigeria, reported that
female respondents were more likely to have ‘probable asthma’ than their male counterparts
(36). Beside this the study in Debre Berhan Referral Hospital, report that sex didn’t show
significant association with bronchial asthma (9).
Socio economic factors
Economic states
Low SES and low household income appear to play a role in adult-onset asthma. Based on the
study in Debre Berhan Referral Hospital, monthly income of the households, was significantly
associated with bronchial asthma (income of household less than 1000 Et.Br/month (26).
Level of education
There was a significant association between mother’s levels of education and asthma based on a
study conduct in Nigeria (46). Also an epidemiological study has shown educational level has no
association with an increase in the prevalence and incidence of asthma (47). And also another
study suggest that level of education was not found to be statistically significant risk factors for
asthma (48).
Occupational
Occupational factors that potentially increase the risk of asthma include high-risk jobs, exposure
to sensitizing agents, exposure to low-level irritants in the workplace, the mode and route of
exposure, the level of exposure, as well as concomitant exposures to pollutants at the workplace
8
(49). In the occupational setting, isocyanate and latex sensitivity have been reported as risk
factors, and poultry workers, hairdressers, gold miners, and wood choppers are reported as
having increased risk of asthma and annual rainfall seems to have an influence on symptom
presentation (35).
2.2.2 Behavioural factors and asthma
Smoking
Epidemiological evidence for the association between active cigarette smoking and asthma has
been inconsistent. Smoking at baseline was shown to significantly increase the risk of incident
asthma in adults (50). In another study, significant associations were found between asthma and
smoking (51), whereas no significant association was reported in a follow-up cross-sectional
analysis (48).
Physical activity
Based on a cross-sectional analysis exercise/sport was not found to be statistically significant
risk factors for asthma (48).
Obesity
Obesity, a major component of metabolic syndrome, is a risk factor for incident asthma in adults.
Asthma and obesity are frequently associated, and obesity may contribute to the development
and severity of asthma (52). Another study also support that obesity has been associated with
asthma (15). However, an epidemiological study has shown that obesity has no association with
an increase in the prevalence and incidence of asthma (47).
2.2.3 Household fuel exposure and asthma
According to the WHO guidelines for indoor air quality there are nine basic pollutants that can
cause serious health problem; those include benzene, carbon monoxide, formaldehyde,
naphthalene, nitrogen dioxide, poly cyclic aromatic hydrocarbons, radon, trichloroethylene, and
tetrachloroethylene (53).
Generally, those pollutants have serious health effects, like acute myeloid leukaemia, ischemic
heart disease, sensory irritation, respiratory inflammation and malignancy, respiratory infection,
lung cancer and carcinogenicity effect on liver, kidney, bile duct and non-Hodgkin’s lymphoma
(53). There are different parameters to measure indoor air quality, comprising of animal
allergens (dust mite, dog, cat), bacteria (gram negative) count endotoxin, mould identification
9
and counts ergo-sterol, volatile organic compound (VOCs), carbon dioxide, man-made mineral
fibers (MMMF) (54).
Indoor cooking using biomass fuel and asthma
There are uncertainties in different literatures on the relationship between the effects of indoor
cooking from the use biomass fuel and respiratory illness. Studies have yielded inconsistent
results, with some studies showing an association between indoor cooking, using biomass fuel
and asthma (27, 46, 55, 56). Including the study undertaken in India on 3456 children to
identifying the effects of the indoor air pollutants SO2, NO2 and total suspended particulate
matter (SPM) generated from fuel used for cooking on respiratory allergy suggests that biomass
fuels increased the concentrations of indoor air pollutants that cause asthma, rhinitis and URTI in
children (27).
Another study on 38,595 elderly persons included in India’s second National Family Health
Survey conducted in 1998–1999; indicate that elderly men and women living in households
using biomass fuels have a significantly higher prevalence of asthma than do those living in
households using cleaner fuels (55).
Other studies in Nigeria and Turkey have similar findings. i.e. A cross-sectional survey, in three
rural communities in Nigeria concludes that the use of biomass fuel for cooking is associated
with an increased risk of severe asthma symptoms (46). Another epidemiological cross-sectional
study in Turkey reported a significant association between symptoms of chronic bronchitis-
asthma and biomass fuel usage (56).
In contrast to the above studies, other studies have shown lack of association between indoor
cooking using biomass fuel and asthma (15, 28, 42). A cross-sectional study in North Central
Nigeria reported that biomass fuel smoke exposure was not associated with an increased risk of
asthma symptoms or airway obstruction (42).
10
Based on a population-based study on 2953 participants in Peru state that indoor cooking using
biomass fuel exposures were not associated with adult asthma (28). Current daily exposure to
biomass fuel smoke and smoking were not associated with asthma (15).
Despite the large population at risk worldwide, the effect of exposure to indoor solid fuel smoke
has not been adequately studied. Indoor air pollution from solid fuel use is strongly associated
with COPD (both emphysema and chronic bronchitis), acute respiratory tract infections, and lung
cancer (primarily coal use) and weakly associated with asthma, tuberculosis, and interstitial lung
disease (28).
Indoor cooking using fossil fuel and asthma
Studies have different association between indoor cooking using fossil fuel and asthma. A study
conducted on 600 households from six urban neighbourhoods in Bangalore, India, found
associations between kerosene use and wheezing, difficulty in breathing and asthma in adults and
cough and wheezing in children, though those associations were not statistically significant (57).
A cross-sectional systematic survey of households in Jimma, Ethiopia suggest that domestic
combustion of refined fossil fuels increases the risk of allergic sensitization and symptoms, and
may have contributed to the increasing prevalence of allergic diseases (58).
A birth cohort study, including 3000 children on development of allergy and asthma did not
show a relationship between gas cooking and any of the respiratory or allergy outcomes (59) .
2.2.4 Housing characteristics and asthma
Housing characteristics can be defined in many ways, but the major focus areas are three, the
first is internal environment, such as adequate ventilation, adequate lighting, floor surface free
from tripping hazards, indoor air quality and moisture level (dampness). The second is internal
structure, such as water supply, sewage disposal, power supply, and other internal components,
as for instance (e.g. doors close, electrical wiring etc). The third is external structure, such as
structural integrity (e.g. building code followed), weather tightness (e.g. Roof/window do not
leak), securing (e.g. Doors lock),external materials have integrity (not broken/rotten),insulation.
In general, in order to say that housing characteristics have high quality, the house must be able

11
to protect from cold, damp, heat, rain, wind, structural hazards, disease vectors and other threats
to health (60).
Poor housing characteristics, such as crowding, need for major repairs, and compromised indoor
air quality have been associated with respiratory conditions (61). Housing disarray are associated
with increased early childhood asthma. Exposure to multiple stressors (i.e. poor housing quality)
may increase children’s risk of developing asthma more than a single stressor. Also poor housing
quality for example, presence of cockroaches, rats and water leaks are associated with asthma
(62). Poor housing characteristics (i.e. high moisture and low occupancy rate) has its own effect
on indoor microbial ecology including fungi this has significant association with development of
asthma (63, 64).
2.2.5 Other factors and asthma
Pet ownership and asthma
Based on the research done in the United kingdom, the prevalence of pet ownership is high
among asthmatics, even those in regular contact with respiratory clinics, and is higher still in
asthmatics managed in primary care (65). The study further suggests that pet ownership is
associated with significant morbidity in asthmatic patients, the burden falling primarily on
younger, atopic individuals (65). Another research suggests that Pet ownership during pregnancy
and childhood is consistently associated with a reduced risk of aeroallergen sensitization and
atopic asthma , but tended to be associated with an increased risk of non-atopic asthma (25). The
opposing effects on atopy vs. non-atopic asthma might be considered by parents when they are
deciding whether to acquire a pet(25). Another cohort study which is done in UK state that there
is no association between cat exposure and wheezing and lung function among children(25).
Well-known allergens in Africa are house dust mite, cockroach, and cat and dog dander; a less
well known allergen is washing soap (35). Study done in Hispanic school children living in a
U.S.-Mexico border city found that ant and spider pest problems, pet dogs, fire place heat,
central air conditioning, humidifier use, and cooking with wood stoves are positively associated
with both allergy and asthma prevalence (21).
12
Family history of asthma
Family history of asthma has been reported as a risk factor for adult-onset asthma (9, 15, 66).
A study in Thailand, revealed that family history of asthma and history of atopy were
significantly associated with an increased risk of developing asthma (OR= 13.62; 95% CI 5.91,
31.43 and OR= 8.54; 95% CI 5.47, 13.33 respectively) (66). A study in Debre Berhan Referral
Hospital, Ethiopia concluded that family history of asthma is significantly associated with
bronchial asthma (9). Another study also supports that family history of asthma was associated
with asthma prevalence (15).
Most of the studies have shown that the association between indoor cooking, housing
characteristics, and asthma are population based secondary data, cross sectional household
studies; with limited information on controlling of confounding. No study has been conducted to
assess the association of selected factors (household fuel exposure and housing characteristics)
and asthma in Ethiopia using hospital based case control study design matched with age.
13
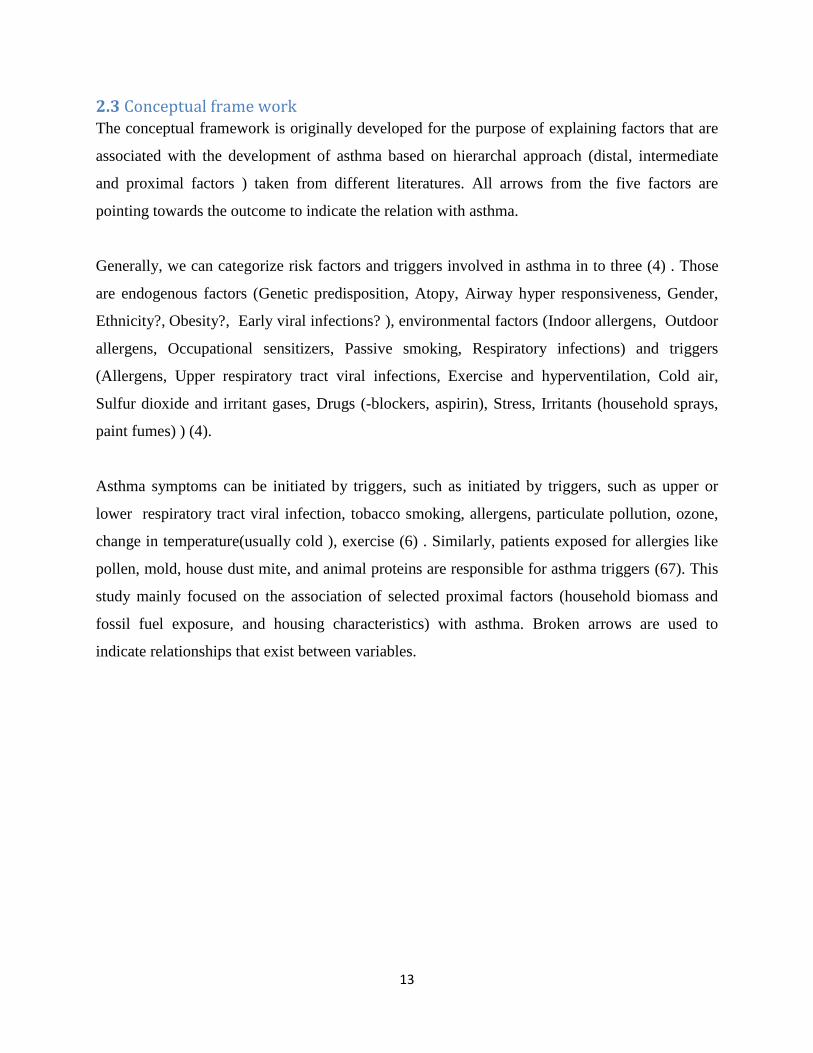
2.3 Conceptual frame work The conceptual framework is originally developed for the purpose of explaining factors that are
associated with the development of asthma based on hierarchal approach (distal, intermediate
and proximal factors ) taken from different literatures. All arrows from the five factors are
pointing towards the outcome to indicate the relation with asthma.
Generally, we can categorize risk factors and triggers involved in asthma in to three (4) . Those
are endogenous factors (Genetic predisposition, Atopy, Airway hyper responsiveness, Gender,
Ethnicity?, Obesity?, Early viral infections? ), environmental factors (Indoor allergens, Outdoor
allergens, Occupational sensitizers, Passive smoking, Respiratory infections) and triggers
(Allergens, Upper respiratory tract viral infections, Exercise and hyperventilation, Cold air,
Sulfur dioxide and irritant gases, Drugs (-blockers, aspirin), Stress, Irritants (household sprays,
paint fumes) ) (4).
Asthma symptoms can be initiated by triggers, such as initiated by triggers, such as upper or
lower respiratory tract viral infection, tobacco smoking, allergens, particulate pollution, ozone,
change in temperature(usually cold ), exercise (6) . Similarly, patients exposed for allergies like
pollen, mold, house dust mite, and animal proteins are responsible for asthma triggers (67). This
study mainly focused on the association of selected proximal factors (household biomass and
fossil fuel exposure, and housing characteristics) with asthma. Broken arrows are used to
indicate relationships that exist between variables.
14
Conceptual frame work
Fig 1; conceptual framework to identify factors associated with asthma (4, 6, 67)
Demographic and socio economic
factors
Demographic: Age, Gender
Socio economic: educational
states, occupational states
Behavioural factors
Smoking
Alcohol
drinking
Physical activity
Triggers
Allergens (atopic
dermatitis or
allergic rhinitis )
Pet ownership
Environmental factors
Air pollution
Biomass fuel user
Fossil fuel user
Housing
characteristics
Kitchen
characteristics
Asthma
Distal
Factors
Intermediate
factors
Proximal
factors
Outcome
Endogenous factors
Genetic
predisposition
Obesity
Viral respiratory infection
Respiratory problem
during infancy and
childhood
Occupational exposure
Exposure to
dusts(industrial or
wood dusts)
Chemical fumes and
vapors
Molds
15
3. Research question and objectives
3.1 Research question Is there any association between selected factors (household biomass fuel exposure,
household fossil fuel exposure and housing characteristics) and asthma?
3.2 Research Hypothesis
3.2.1 Null hypothesis
Household fuel exposure and housing characteristics have no association with asthma.
3.2.2 Alternative hypothesis
Household fuel exposure and housing characteristics have association with asthma.
3.3 Objective
3.3.1 General objective To investigate the association between household fuel exposure and housing
characteristics, with asthma.
3.3.2 Specific objectives To assess the association between household biomass fuel exposure and asthma.
To determine the association between household fossil fuel exposure and asthma.
To evaluate the role of housing characteristics on asthma.
16
4. Methods and materials
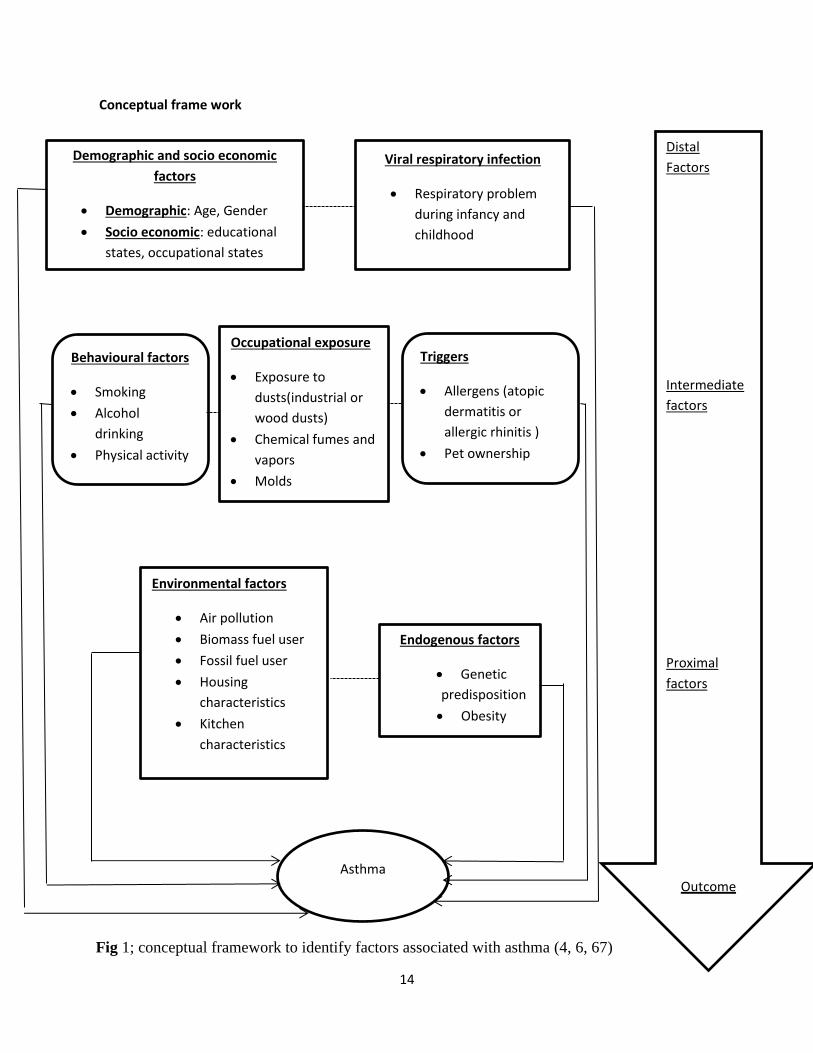
4.1 Study area The study area was Addis Ababa, the Capital City of Ethiopia. Addis Ababa lies at an elevation
of 2,200 meters (7,200 ft.) and is located at 9’1’48”N 38’44’24”E / 9.03000’N 38.74000’E.(68).
In Addis Ababa there were 96 health centers, 12 public hospitals, 28 private hospitals and 882
clinics (69). Among the available 12 government run hospitals, the study was conducted in two
public hospitals, including Tikur Anbessa Specialized Hospital and St. Paul Hospital Millennium
Medical College (SPHMMC). The hospitals were selected for this study on the basis of
spirometry using status, case load (from all over the country) and various specialized units (chest
clinic and internal medicine OPD). TASH is the largest Teaching Hospital of the country which
is found in Lideta sub-city, Addis Ababa. Originally, TASH was built to accommodate 500 beds
and currently has more than 600 beds. It serves about 250,000 patients per year in its outpatient
department and about 24,000 in the inpatient (70). Chest clinic is one of the 16 clinics in the
hospital. On average, 500 patients with respiratory diseases are seen each month in the clinic;
asthma patients account for one-third of all cases. On the other hand, Saint Paul Hospital
Millennium Medical College is one of the specialized referral public hospitals in Addis Ababa
with, bed capacity of about 350. The Hospital has outpatient and inpatient wards that provide
different services. The hospital receives referrals from all over the country (71).
Figure 2; Map of study area
17
4.2 population
4.2.1 Target population
The target population for the study were all patients who visited public hospitals in Addis
Ababa between February and August 2020.
4.2.2 Source population
The source population were all patients who visited study hospitals between February and
August 2020.
4.2.3 Study population
The study population were all patients attending study hospitals (chest clinic and internal
medicine OPD) in the study period and those who fulfilled the eligibility criteria.
4.2.4 Study unit
Single participant selected based on inclusion criteria and sampling techniques during the
study period.
4.2.5 Inclusion criteria
Cases
Spirometry confirmed asthmatic patients who were diagnosed and enrolled in the study
hospitals chest clinic of internal medicine OPD.
Age 18 years or older.
Controls
Attendees of study hospitals non chest clinic of internal medicine OPD for non-asthma
health problems.
Matched with sex and age, we have chosen two controls in the same five year age group.
(i.e. control age =case age ± 2 years )
4.2.6 Exclusion criteria
Cases and controls suffering from COPD, lung cancer, PTB and pneumonia were
excluded.
Controls with clinical sign or symptom suggestive of asthma were excluded.
18
4.3 Study Design and study period A hospital based matched case control study design was employed in individuals with asthma
and without asthma at Tikur Anbessa Specialized Hospital and St. Paul hospital from February to
August 2020.
4.4 Sample size calculation Sample size was calculated using Epi info 7 statistical software package with the assumption of
double population, n=(r+1)/r. (p)(1-p)(zβ+zα/2)2/(p1-p2)
2 formula. The assumptions are two-
sided significance level (α=5%), power (1-β) =80% to detect how much exposure difference
between cases and controls , 95% confidence level, ratio of control to case (R) 2:1. The largest
sample size was taken. The prevalence of exposure (selected determinants, such as indoor
cooking using biomass fuel, indoor cooking using fossil fuel and household crowding index)
among controls are estimated from previous studies that are 10%, 19.5% and 34% respectively
(72-74). Then, the sample size required for main variable with control to case ratio of 2:1 by
considering the three main variable percent of control exposed was 296 (99 cases and 197
controls), 464 (155 cases and 309 controls) and 35 (12 cases and 23 controls) respectively
without considering non response rate. The minimum sample size required for the study was
independently established.
19
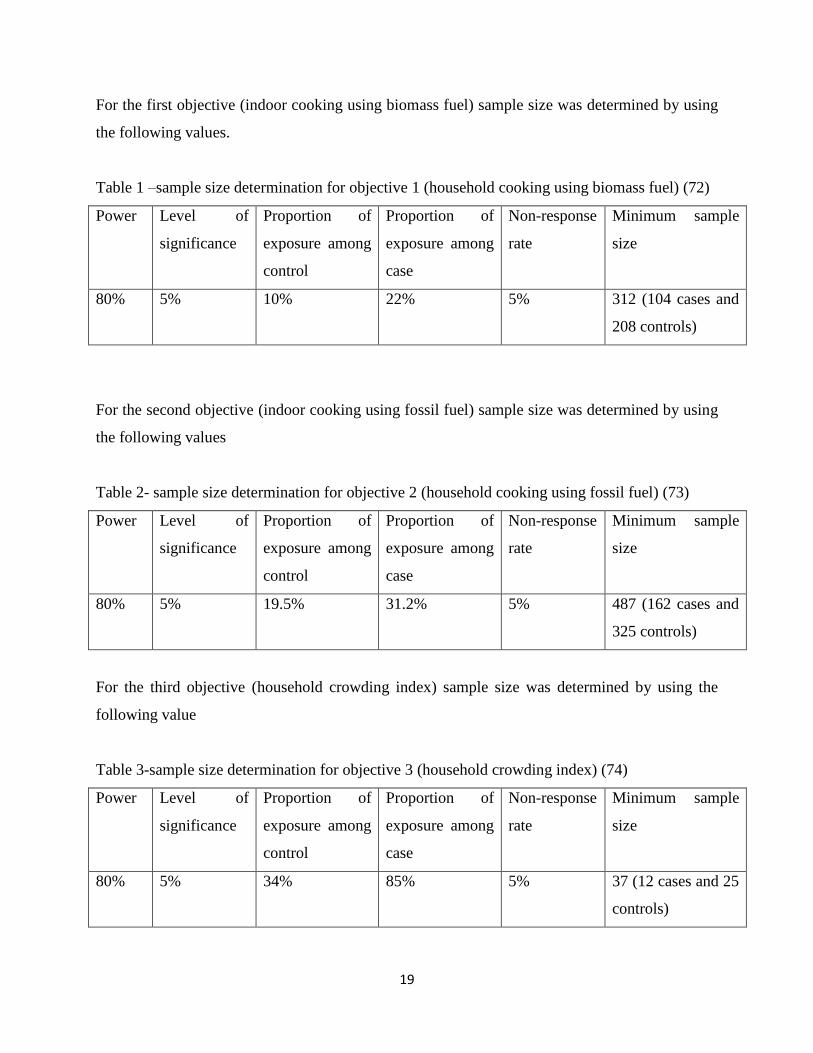
For the first objective (indoor cooking using biomass fuel) sample size was determined by using
the following values.
Table 1 –sample size determination for objective 1 (household cooking using biomass fuel) (72)
Power Level of
significance
Proportion of
exposure among
control
Proportion of
exposure among
case
Non-response
rate
Minimum sample
size
80% 5% 10% 22% 5% 312 (104 cases and
208 controls)
For the second objective (indoor cooking using fossil fuel) sample size was determined by using
the following values
Table 2- sample size determination for objective 2 (household cooking using fossil fuel) (73)
Power Level of
significance
Proportion of
exposure among
control
Proportion of
exposure among
case
Non-response
rate
Minimum sample
size
80% 5% 19.5% 31.2% 5% 487 (162 cases and
325 controls)
For the third objective (household crowding index) sample size was determined by using the
following value
Table 3-sample size determination for objective 3 (household crowding index) (74)
Power Level of
significance
Proportion of
exposure among
control
Proportion of
exposure among
case
Non-response
rate
Minimum sample
size
80% 5% 34% 85% 5% 37 (12 cases and 25
controls)
20
Then, the maximum sample size was taken. Accordingly, the sample size corresponding to
indoor cooking using fossil fuel objective 2 was taken (73). Finally, the calculated sample size
was 464. After adjusting for 5% non-response rate, the minimum required sample size was 487
which was 162 cases and 325 controls.
4.5 Sampling procedure
Selection criteria used to select study hospitals were first, spirometry using status for the
diagnosis of asthma, second, case load (referee from Addis and other rural regions of the
country) and third, various specialized units (chest unit and internal medicine OPD). Among the
available 12 government run hospitals, the study was conducted on two public hospitals,
including Tikur Anbessa Specialized Hospital and St. Paul Hospital millennium medical college
based on the selection criteria.
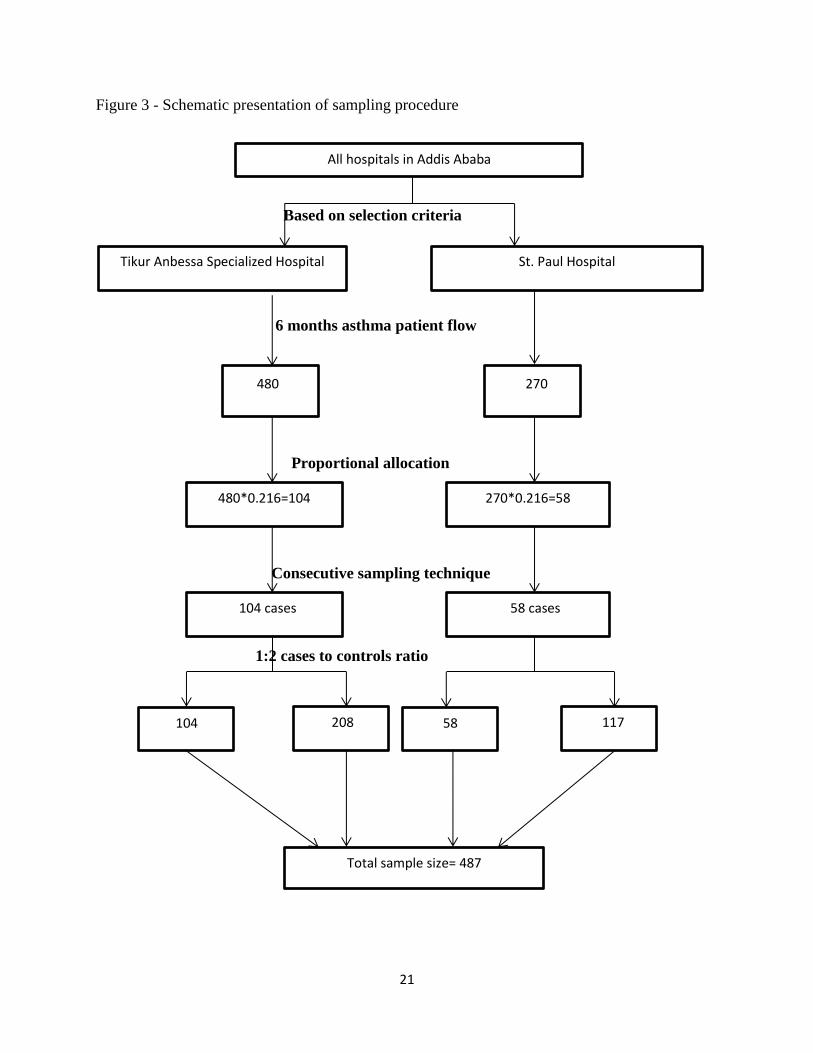
From each hospital, participants were selected by consecutive/sequential sampling technique
based on the proportion of selected hospitals total patient flow as denominator. The total number
of asthma patients at study hospitals based on last year data on similar time with the data
collection period three months report was totally 750 asthma patient; 480 from Tikur Anbessa
Specialized Hospital and 270 from St. Paul Hospital.
Proportional allocation was used to select the sample size (sampling fraction=sample size/total
patient flow=162/750=0.216). Based on the proportional allocation total number of patients were
162, including 104 (0.216*480) from Tikur Anbessa Specialized Hospital and 58(0.216*270)
from St. Paul Hospital.
During selection of participants based on sampling technique if the person was not eligible to be
included or not willing to participate, then data collectors proceeded to the next person. The
detail description of the sampling techniques is presented below.
21
Figure 3 - Schematic presentation of sampling procedure
Based on selection criteria
6 months asthma patient flow
Proportional allocation
Consecutive sampling technique
1:2 cases to controls ratio
All hospitals in Addis Ababa
Tikur Anbessa Specialized Hospital
St. Paul Hospital
480 270
480*0.216=104
270*0.216=58
104 208 58 117
Total sample size= 487
104 cases
58 cases
22
4.6 Study variables
4.6.1 Dependent variable
Asthma status (cases and controls)
4.6.2 Independent variables
4.6.2.1 Socio-demographic characteristics
Age, Residence, Sex, Marital status, Educational status, Occupational status, Monthly
income , Religion
4.6.2.2 Main exposure variables
Housing characteristics: number of rooms, number of persons, household crowding
index, lighting source , cooking area, cooking room floor material, cooking room wall
material, cooking room roof material, window in cooking room, window opening, door
opening, smoke extraction, cooking time
Household fuel exposure characteristics: stove type (three stone fire, shielded mud
stove, wood burning metal stove, improved charcoal stove, kerosene stove, LPG(gas)
stove, solar cooker, grid powered electric stove), current household fuel type (wood,
charcoal, kerosene, dung, agricultural residues, solar, grid electricity, batteries) and life
time household fuel type(wood, charcoal, kerosene, dung, agricultural residues, solar,
grid electricity, batteries) ,
4.6.2.3 Confounding variables
Pet ownership (pet )
Life style characteristics (Tobacco Smoking status, shisha smoking status, alcohol
drinking, chat chewing status, drug using status, family history of asthma, physical
activity)
Nutritional status (body mass index, weight, height)
Co morbidities (cardiac, hypertension, diabetes, nerve, kidney disease, liver disease,
HIV)
23
4.7 Data collection procedure
Data collectors were waiting until the study unit’s physicians complete their consultation. After
they finish, the interviewers explained the objective of the study and got written informed
consent to conduct the interview. Data were collected through questionnaire based on face to
face interview by eight nurses in selected units, who received data collection training with
appropriate measure to avoid risk of COVID-19 transmission such as sanitizing their hands,
wearing mask properly and keeping their physical distance. The data collection tool used in this
study was adopted from the previously peer reviewed studies, European Community Respiratory
Health Survey II (ECRHS II) questionnaires and American Thoracic Society division of lung
disease (ATS-DLD-78) questionnaires, and appropriate modifications were made to serve our
purpose (75, 76). The final format had two major parts. The first part was demographic and
socioeconomic characteristics items (age, gender, marital states, educational states, occupational
states and family income), while the second part included items related to potentials risk factor
predictors, including indoor cooking, housing characteristics, cooking room characteristics,
smoking status, alcohol drinking, family history of asthma, pet ownership, physical activity and
obesity. This hospital based, case control study including face to face interviews was performed
by trained data collectors. A screening questionnaire was used to exclude any one with asthmatic
symptoms from the control groups. The survey questionnaire was used for both case and control
subjects. Data regarding patient’s medical information were extracted from patient cards.
4.8 Data Quality management Data collectors were experienced nurses that work in study hospitals. Data quality assurance was
done at three steps, before, during and after data collection period. First, before data collection
period, two days training was given for data collectors based on the content of questionnaire,
data collection methods, ethical concerns and the purpose of the study. The training was given by
the principal investigator. The questionnaire prepared in English was translated to Amharic and
back to English to keep the consistency of the questions. Pre testing of the questionnaire was
made to ensure the quality of data in Yekatit 12 Hospital on 25 patients, 5% of study population.
Second during data collection, completeness and consistency of the questionnaire were assessed
daily by field supervisors and the principal investigator. Supervisors and the principal
investigator revisited the questionnaire to check the accuracy of information collected by data
collectors. Third after data collection period, data were entered in to a template prepared on Epi-

24
Info software and inconsistencies of the entered data were reconciled by checking the
questionnaire. Data cleaning was done by running frequencies and cross-tabulating with the main
outcome variables. Before analysis, missing values and outliers were checked, The data were
exported to SPSS version 24 for analysis.
4.9 Data analysis procedure First, descriptive statistics were computed using frequency distribution and proportions for
categorical variables and, mean and standard deviations (SD) for continuous variables (Age,
monthly income, no of rooms, no of person, household crowding index, time spent for cooking
weight , height and body mass index) was described. Generally, results were presented, using
frequencies, cross tabulations and percentages. Chi-square test was used to assess the level of
significant differences. A threshold p value of less ≤ 0.05 was used to declare significant
association between asthma and its predictors in the chi-square test. Since we have used matched
case control study design conditional logistic regression were performed. Hence, variables which
were found to be associated with asthma were included in the conditional binary logistic
regression. Furthermore, different variables were included in the conditional multivariable
logistic regression to single out the effect of each covariate with asthma and adjusted odds ratios,
with 95% confidence interval was consider to see the association. Co-founders, interaction and
multi-collinearity were checked to minimize bias. Multi-collinearity between independent
variables was checked to ensure that inserting as many variables did not introduce statistically
significant multicollinearity, which was confirmed by the assumption of VIF<10 as no
multicollinearity. and the model goodness of the test was checked by Hosmer - Lemeshow
goodness of fit test. The model is fit at x2
=3.711 and p-value of 0.882. A 95% confidence
interval for crude and adjusted ORs and a threshold p-value of ≤ 0.05 were used to decide
significance of association.
25
4.10 Operational definitions
Asthma – based on spirometry result we should have (reversibility of airway obstruction)
i.e. (greater than 12% and 200 ml increase in FEV1) following inhalation of
bronchodilator.
Biomass fuel user- In the questionnaire, an individual was considered as biomass fuel
user, if he/she used fuel, including wood, charcoal, plant residues or agricultural waste
and animal dung, mainly from domesticated animals for cooking or heating purposes.
Pertaining to user classification, former biomass user means previously used biomass
fuel, but stop now or not used biomass fuel with in the last 12 months, current biomass
user means that uses biomass fuel with in the last 12 months and if users either current,
former or both called life time user for Q.402 and Q.403 (77, 78).
Fossil fuel user - In the questionnaire, an individual considered as fossil fuel if he/she,
uses fuel such as oil, coal, natural gas, kerosene and liquid petroleum gas for cooking.
Regarding user classification, former fossil fuel user means previously used fossil fuel
but stop now or not used fossil fuel with in the last 12 months, current fossil fuel user
means that used fossil fuel with in the last 12 months and if users either current, former or
both called life time user for Q.402 and Q.403 (77, 79) .
Indoor Cooking:- any type of Home cooking, either in kitchen or part of main living
area, using both heating devices (eg, fireplaces, woodstoves, kerosene heaters, flued [i.e.
vented] or non-flued gas heaters) and gas stoves for cooking for Q.206 (18).
Household crowding index: - denoted by the number of co-residents per room. i.e
number of co residents (excluding newborn) divided by number of rooms (excluding
kitchen and bathroom) based on this it can be categorized in to three, low when it is less
than one, medium when it is between one and two, and high when it is greater than three
for Q.203 (80).
26
Window characteristics- Cooking room shall have at least one window, the minimum
total window size shall be at least eight percent of the floor area of the room. If this
requirement is fellfield our answer would be yes for Q.304 about having window and if it
is not fellfield the answer would be no (81).
Door characteristics; the environment has an opening in the windward façade and a
door in the leeward façade and the minimum requirement door characteristics are width
of 0.80 meter and height of 2,10 meter. If this requirement is fellfield our answer would
be yes for Q.306 about having window and if it is not fellfield the answer would be no
(82) .
Pet ownership:-having any pet that includes, cat, dog, and bird and assess contact with
them and contacts can be categorized in to regular contact (at least once a day and five
times per week) and some contact (less than once a day and five times per week) for
Q.501.
Physical activity: this question is measured by considering as any bodily movement
produced by skeletal muscles that results in energy expenditure, it can be categorized in
to occupational, sports, conditioning, household, or other activies (83). In order to say a
person has normal physical activity, he/she must engage in moderate physical activity for
at least 30 minutes per day for 5 or more days per week or vigorous physical activity for
at least 20 minutes per day for 3 or more days per week for Q.615 (84).
Alcohol drinking: Behaviors can be measured in different ways, but for this
questionnaire it was defined as follows; A person who had ever drunk any alcoholic
beverage during his/her life was called an ever drinker. An ever drinker who had not
drink alcohol with in the last 12 months was designated as an ex-drinker. An ever drinker
who had drunk alcohol with in the last 12 months was labled as a current drinker for
Q.607 (85).
27
Smoking states: In this study an individual smoking status was defined as follows: A
person who had smoked at least 20 packs of cigarettes or 12 oz (360 grams) of tobacco in
a lifetime, or at least one cigarette per day or one cigar a week for one year was labelled
an ever smoker (76). An ever smoker who had not smoked with in the last 12 months or
with in the last 6 months was called an ex- smoker. An ever smoker who had smoked
with in the past 30 days was called a current smoker for Q.601 (86).
Body mass index (BMI) in this study, subjects are characterized by body mass index
(BMI), divided in to four subgroups, Underweight (BMI less than 19.8 kg/m2), Normal (
19.8 -25 kg/m2), overweight (BMI 25.1-30 kg/m2) and obese (BMI greater than
30kg/m2) for Q.703 (87).
Cooking time: cooking time in this study was measured by asking the following question
“how many minutes on average do you spend preparing, cooking and cleaning up each
time per day?” And the answer were recorded in to three categories, less than 60 minutes,
between 60and 120 minutes, and greater than 120 minutes for Q.207 (88).
4.11 Ethical consideration Before conducting the study ethical clearance was secured from the Research Ethical Committee
of the School of Public Health, College of Health Sciences of the Addis Ababa University. Then,
formal letters were written to study hospitals, including Yekatit 12 hospital, Tikur Anbessa
Specialized Hospital and St. Paul Hospital from Addis Ababa University, School of Public
Health to inform them about the study. The data collectors got written consent from the
participants and informed them clearly the aim of the study and the fact that it has no invasive
procedure and harm. Respondents were informed that they could refuse or discontinue
participation at any time and they were informed of the fact that Information is recorded without
their names being mentioned. Only codes were used to keep it anonymous and maintain
confidentiality and privacy of respondents.

28
4.12 Dissemination of findings The result of this study was disseminated to the School of Public Health, College of Health
Sciences, Addis Ababa University. Furthermore, it is also planned to share the information with
Ethiopia Food Medicine Health Care Administration and Control Authority, of the Federal
Ministry of Health through hard and soft copies. The finding of the research shall be
communicated through workshops. The findings shall be published in peer-reviewed journal.
29
5. Results
5.1 Descriptive analysis
Socio-demographic characteristics of study participant
From those patients who came for different services at TASH and SPHMMC, 487 participants
that were approached, four people were excluded (1 case and 3 controls) due to failure to get age
and sex matched controls. A total of 483 patients were enrolled in the study, which makes the
response rate 99.17%. Age and sex were the matching variables in the study. For each case we
had plus or minus two years old controls.
Socio demographic characteristics of cases and controls are depicted in Table 4. The proportion
of ages less than 20, 20-40, 41-60, 61-80 and greater than 80 years were found to be 4%. 28.6%,
49.5%, 19.7% and 1.9% respectively. From total participants, 98(60.9%) cases and 202(62.7%)
controls were females.
With regard to place of residents, more cases 7(4.3%) than controls (7(2.2%) were from rural
area. Most of participants were female 98(60.9%) of cases and 196(60.9%) of controls. Majority
97(60.2%) cases and 225(69.9%) controls were married. And, 25(15.5%) cases and 45(14%)
controls were single, 30(18.6%) cases and 46(14.3%) controls were widowed and 9(5.6%) cases
and 6(1.9%) controls were Separated /divorced.
Among study participants with respect to education, 51(31.7%) of cases and 95 (29.5%) controls
attained primary education. Further 18(11.2%) of cases and 37 (11.5%) of controls, 4(2.5%)
cases and 10 (3.1%) of controls and 48(29.8%) of cases and 94 (29.2%) of controls completed
secondary, preparatory and above diploma educational status respectively. However, 40(24.8%)
of cases and 86 (26.7%) of controls were unable to read and write.
With respect to occupational status, majority of participants were employed either in
government, private or self 87(54%) of cases and 193(59.9%) of controls. And also 55(34.2%) of
cases and 106(32.9%) of controls, 18(311.2%) of cases and 21(6.5%) of controls, and 1(0.6%) of
cases and 2(0.6%) of controls were unemployed, retired and student respectively.
With regard to monthly income, majority of participant 68(42.2%) of cases and 127(39.4%) of
controls earned above 2500 EB. And 41(25.5%) of cases and 84(26.1%) of controls, 35(21.7%)

30
of cases and 54(16.8%) of controls and 17(10.6%) of cases and 57(17.7%) of controls got below
500 ETB, between 500 and 1500 ETB, between 1501 and 2500 ETB respectively.
Majority 104(64.6%) of cases and 218(67.7%) controls were orthodox and the rest 19(11.8%)
cases and 42(13%) controls, 35(21.7%) cases and 46(14.3%) controls, and 3(1.9%) cases and16
(5%) controls were Muslim, Protestants and Catholics respectively.
31
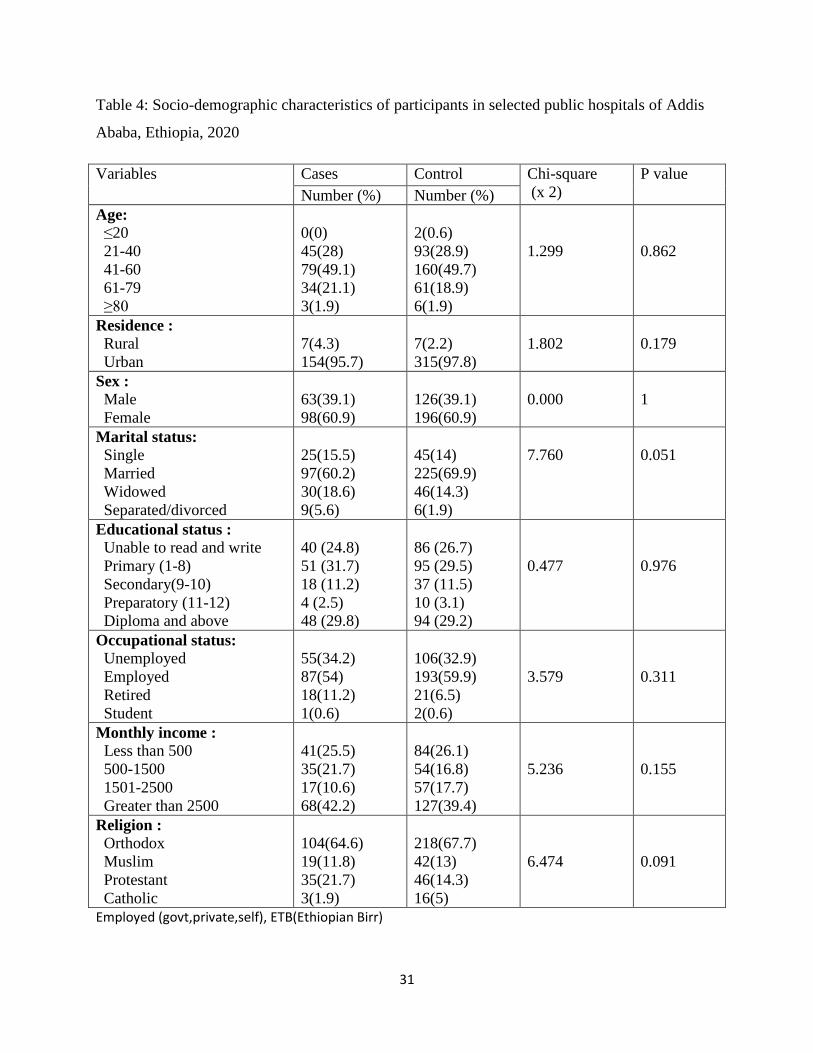
Table 4: Socio-demographic characteristics of participants in selected public hospitals of Addis
Ababa, Ethiopia, 2020
Variables Cases Control Chi-square
(x 2)
P value
Number (%) Number (%)
Age:
≤20
21-40
41-60
61-79
≥80
0(0)
45(28)
79(49.1)
34(21.1)
3(1.9)
2(0.6)
93(28.9)
160(49.7)
61(18.9)
6(1.9)
1.299
0.862
Residence :
Rural
Urban
7(4.3)
154(95.7)
7(2.2)
315(97.8)
1.802
0.179
Sex :
Male
Female
63(39.1)
98(60.9)
126(39.1)
196(60.9)
0.000
1
Marital status:
Single
Married
Widowed
Separated/divorced
25(15.5)
97(60.2)
30(18.6)
9(5.6)
45(14)
225(69.9)
46(14.3)
6(1.9)
7.760
0.051
Educational status :
Unable to read and write
Primary (1-8)
Secondary(9-10)
Preparatory (11-12)
Diploma and above
40 (24.8)
51 (31.7)
18 (11.2)
4 (2.5)
48 (29.8)
86 (26.7)
95 (29.5)
37 (11.5)
10 (3.1)
94 (29.2)
0.477
0.976
Occupational status:
Unemployed
Employed
Retired
Student
55(34.2)
87(54)
18(11.2)
1(0.6)
106(32.9)
193(59.9)
21(6.5)
2(0.6)
3.579
0.311
Monthly income :
Less than 500
500-1500
1501-2500
Greater than 2500
41(25.5)
35(21.7)
17(10.6)
68(42.2)
84(26.1)
54(16.8)
57(17.7)
127(39.4)
5.236
0.155
Religion :
Orthodox
Muslim
Protestant
Catholic
104(64.6)
19(11.8)
35(21.7)
3(1.9)
218(67.7)
42(13)
46(14.3)
16(5)
6.474
0.091
Employed (govt,private,self), ETB(Ethiopian Birr)
32
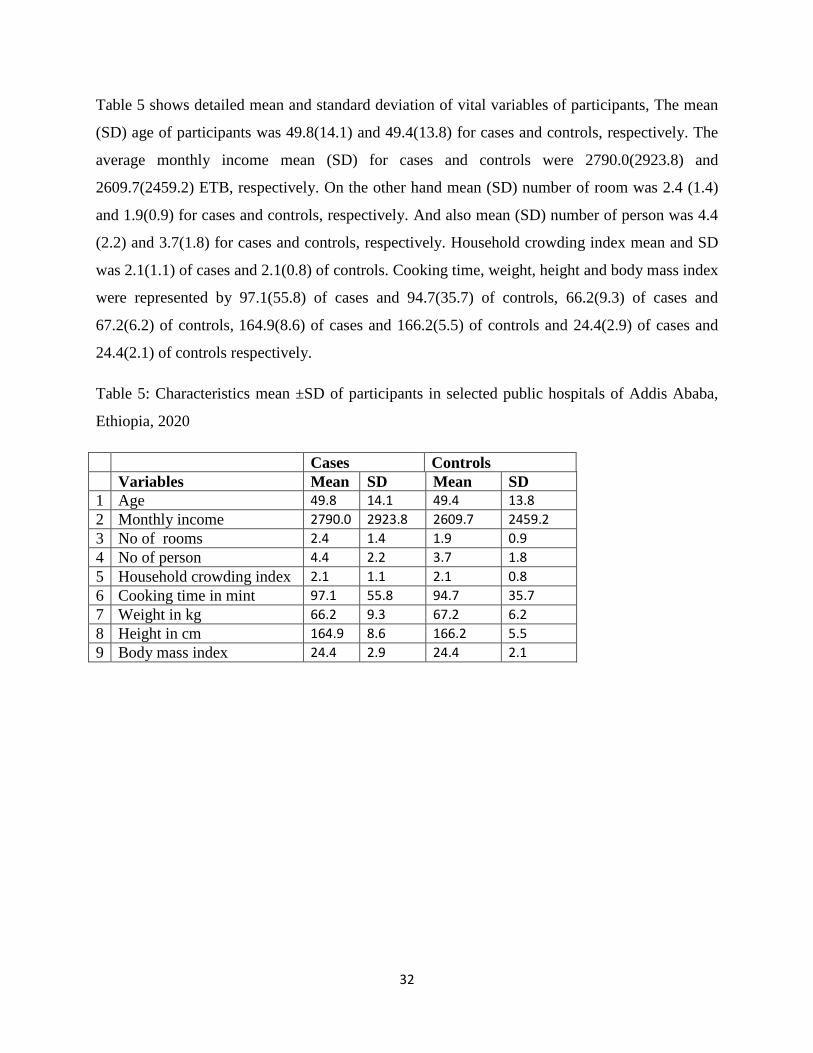
Table 5 shows detailed mean and standard deviation of vital variables of participants, The mean
(SD) age of participants was 49.8(14.1) and 49.4(13.8) for cases and controls, respectively. The
average monthly income mean (SD) for cases and controls were 2790.0(2923.8) and
2609.7(2459.2) ETB, respectively. On the other hand mean (SD) number of room was 2.4 (1.4)
and 1.9(0.9) for cases and controls, respectively. And also mean (SD) number of person was 4.4
(2.2) and 3.7(1.8) for cases and controls, respectively. Household crowding index mean and SD
was 2.1(1.1) of cases and 2.1(0.8) of controls. Cooking time, weight, height and body mass index
were represented by 97.1(55.8) of cases and 94.7(35.7) of controls, 66.2(9.3) of cases and
67.2(6.2) of controls, 164.9(8.6) of cases and 166.2(5.5) of controls and 24.4(2.9) of cases and
24.4(2.1) of controls respectively.
Table 5: Characteristics mean ±SD of participants in selected public hospitals of Addis Ababa,
Ethiopia, 2020
Cases Controls
Variables Mean SD Mean SD
1 Age 49.8 14.1 49.4 13.8
2 Monthly income 2790.0 2923.8 2609.7 2459.2
3 No of rooms 2.4 1.4 1.9 0.9
4 No of person 4.4 2.2 3.7 1.8
5 Household crowding index 2.1 1.1 2.1 0.8
6 Cooking time in mint 97.1 55.8 94.7 35.7
7 Weight in kg 66.2 9.3 67.2 6.2
8 Height in cm 164.9 8.6 166.2 5.5
9 Body mass index 24.4 2.9 24.4 2.1
33
Housing characteristics
Housing characteristics of cases and controls are shows detailed of the total study population in
Table 6, majority of person have 2 rooms 59(36.6%) of cases and 104(32.3%) of controls
respectively. And also persons living in the house were four or greater than four which were
represented by 102(63.4%) cases and 164(50.9%) controls, the rest 13(8.1%) cases and
44(13.7%) controls, 15(9.3%) cases and 30(9.3%) controls and finally 31(19.3%) cases and
84(26.1%) controls were represented by 1, 2 and 3 persons in the household respectively. Among
those participant household crowding index value lies between 1 and 2 were 70(43.5%) of cases
and 151(46.9%) of controls. Majority of participant use electricity for lighting source
157(97.5%) of cases and 317(98.4%)of controls. A high proportion of cases and controls had
enclosed area (kitchen) for cooking purpose reported among 117(72.7%) of cases and 241
(74.8%) of controls. On the other hand 38(23.6%) cases and 70 (21.7%) controls, 6(3.7%)cases
and 11 (3.4%) controls, used part of main living area and semi- open area for cooking
respectively. When we try to see smoke extraction, majority of participant use door opening
practice 76(47.2%) of cases and 162(50.3%) of controls. Further 3(1.9%) of cases and 0(0%) of
controls, 1(0.6%) of cases and 2(0.6%) of controls, 5(3.1%) of cases and 3(0.9%) of controls,
4(2.5%) of cases and 12(3.7%) of controls, 0(0%) of cases and 0(0%) of controls, 70(43.5%) of
cases and 138(42.9%) of controls, 2(1.2%) of cases and 5(1.6%) of controls were represent
permanent hole n roof, eaves spaces, chimney, windows opening, fan or air condition , door and
window opening and open area. On the other hand majority of participants 74(46%) cases and
304(94.4) controls spent 60-120 minutes for cooking a day. And the rest, 71(44.1%) of cases
and 2(0.6%) of controls and 16(9.9%) of cases and 16(5%) of controls spent below 60 min and
above 120 min respectively.
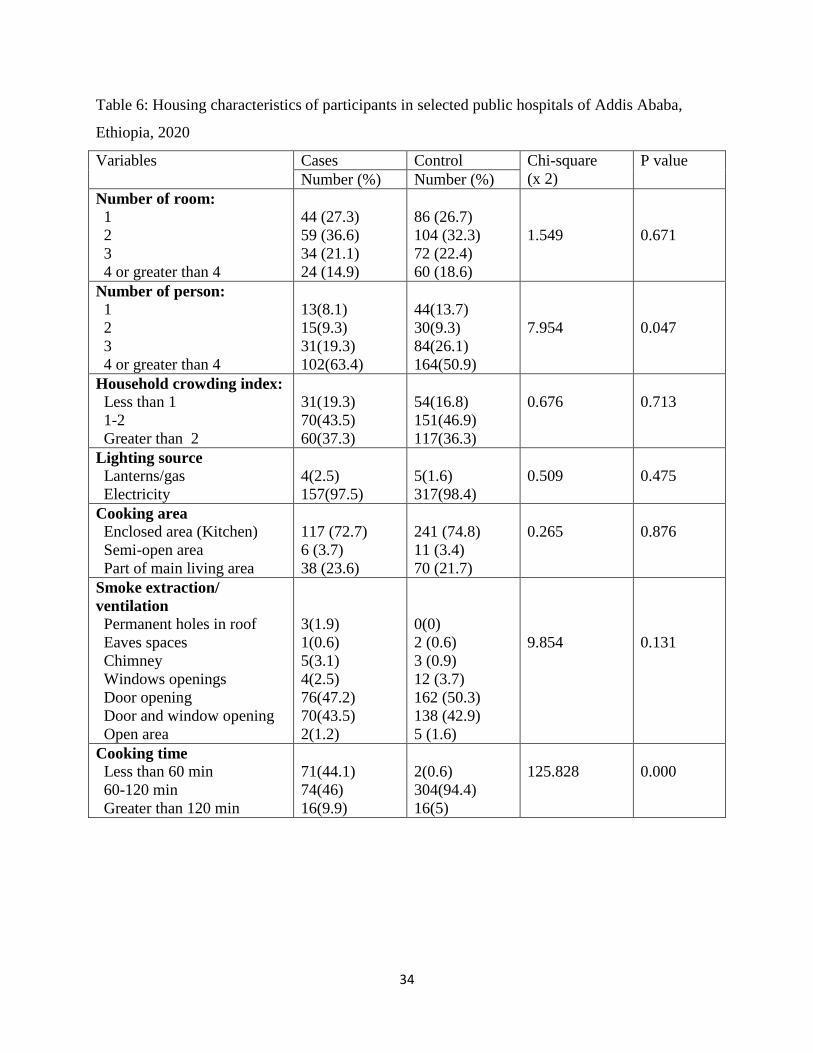
34
Table 6: Housing characteristics of participants in selected public hospitals of Addis Ababa,
Ethiopia, 2020
Variables Cases Control Chi-square
(x 2)
P value
Number (%) Number (%)
Number of room:
1
2
3
4 or greater than 4
44 (27.3)
59 (36.6)
34 (21.1)
24 (14.9)
86 (26.7)
104 (32.3)
72 (22.4)
60 (18.6)
1.549
0.671
Number of person:
1
2
3
4 or greater than 4
13(8.1)
15(9.3)
31(19.3)
102(63.4)
44(13.7)
30(9.3)
84(26.1)
164(50.9)
7.954
0.047
Household crowding index:
Less than 1
1-2
Greater than 2
31(19.3)
70(43.5)
60(37.3)
54(16.8)
151(46.9)
117(36.3)
0.676
0.713
Lighting source
Lanterns/gas
Electricity
4(2.5)
157(97.5)
5(1.6)
317(98.4)
0.509
0.475
Cooking area
Enclosed area (Kitchen)
Semi-open area
Part of main living area
117 (72.7)
6 (3.7)
38 (23.6)
241 (74.8)
11 (3.4)
70 (21.7)
0.265
0.876
Smoke extraction/
ventilation
Permanent holes in roof
Eaves spaces
Chimney
Windows openings
Door opening
Door and window opening
Open area
3(1.9)
1(0.6)
5(3.1)
4(2.5)
76(47.2)
70(43.5)
2(1.2)
0(0)
2 (0.6)
3 (0.9)
12 (3.7)
162 (50.3)
138 (42.9)
5 (1.6)
9.854
0.131
Cooking time
Less than 60 min
60-120 min
Greater than 120 min
71(44.1)
74(46)
16(9.9)
2(0.6)
304(94.4)
16(5)
125.828
0.000
35
Cooking room characteristics
Cooking room characteristics of cases and controls are presented in Table 7. Majority of
participant cooking room floor material were cement represented by 91(56.5%) of cases and
187(58.1%) of controls. Further cooking room floor material 52(32.3%) of cases and 99(30.7%)
of controls, 9(5.6%) of cases and 21(6.5%) of controls and 9(5.6%) of cases and 15(4.7%) of
controls were clay/mud, ceramic and wood respectively. With respect to cooking house wall
material 63(39.1%) of cases and 94(29.2%) of controls, 38(23.6%) of cases and 82(25.5%) of
controls, 59(36.6%) of cases and 146(45.3%) of controls, and 1(0.6%) of cases and 0(0%) of
controls were iron sheet, burned bricks, wattle and daub and plastic respectively. On the other
hand most of participants cooking room roof material were iron sheet 154(95.7%) of cases and
304(94.4%) of controls. And the rest were tiles 7(4.3%) of cases and 18(5.6%) of controls. Based
on participants report, 77(47.8%) of cases and 276(85.7%) of controls has windows in cooking
room. Among those who haves it 76(47.2%) cases and 273(84.6%) controls practice window
opening during cooking time. The detail of cooking room characteristics of the study participants
is presented in the following table 7.
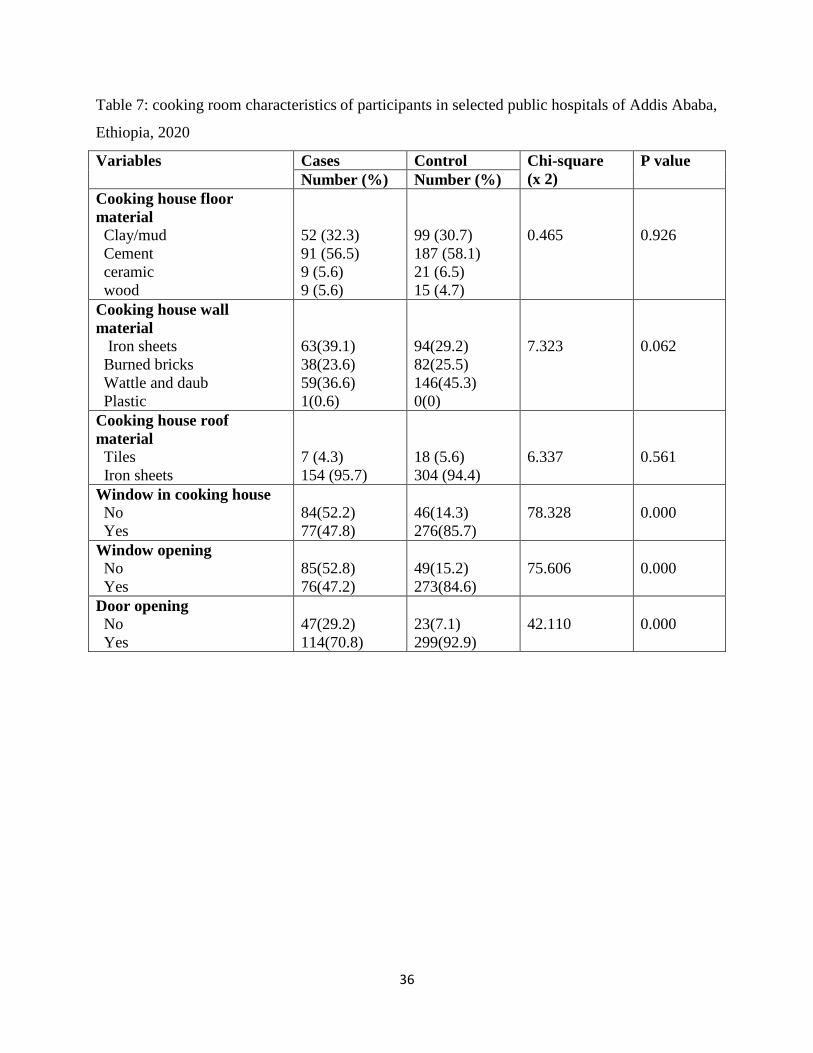
36
Table 7: cooking room characteristics of participants in selected public hospitals of Addis Ababa,
Ethiopia, 2020
Variables Cases Control Chi-square
(x 2)
P value
Number (%) Number (%)
Cooking house floor
material
Clay/mud
Cement
ceramic
wood
52 (32.3)
91 (56.5)
9 (5.6)
9 (5.6)
99 (30.7)
187 (58.1)
21 (6.5)
15 (4.7)
0.465
0.926
Cooking house wall
material
Iron sheets
Burned bricks
Wattle and daub
Plastic
63(39.1)
38(23.6)
59(36.6)
1(0.6)
94(29.2)
82(25.5)
146(45.3)
0(0)
7.323
0.062
Cooking house roof
material
Tiles
Iron sheets
7 (4.3)
154 (95.7)
18 (5.6)
304 (94.4)
6.337
0.561
Window in cooking house
No
Yes
84(52.2)
77(47.8)
46(14.3)
276(85.7)
78.328
0.000
Window opening
No
Yes
85(52.8)
76(47.2)
49(15.2)
273(84.6)
75.606
0.000
Door opening
No
Yes
47(29.2)
114(70.8)
23(7.1)
299(92.9)
42.110
0.000
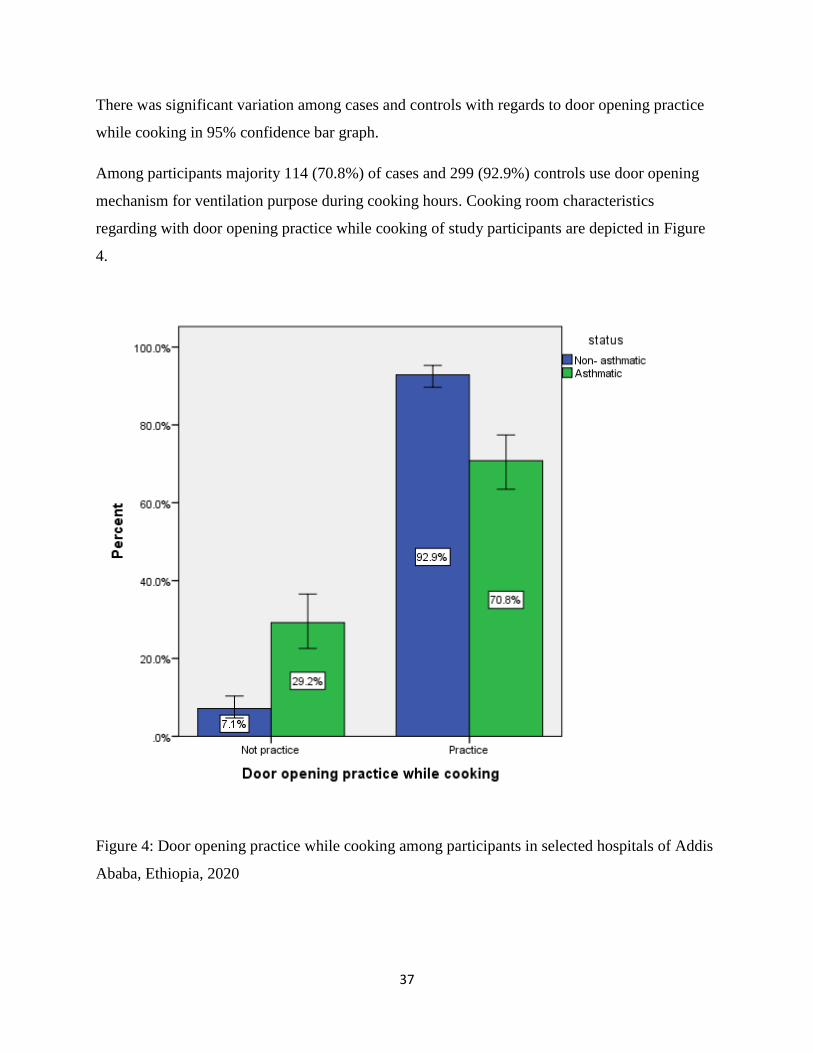
37
There was significant variation among cases and controls with regards to door opening practice
while cooking in 95% confidence bar graph.
Among participants majority 114 (70.8%) of cases and 299 (92.9%) controls use door opening
mechanism for ventilation purpose during cooking hours. Cooking room characteristics
regarding with door opening practice while cooking of study participants are depicted in Figure
4.
Figure 4: Door opening practice while cooking among participants in selected hospitals of Addis
Ababa, Ethiopia, 2020
38
Household fuel exposure characteristics
The participant household fuel exposure characteristics were described in the following table
with different section. In household fuel exposure characteristics we have three categories.
Stove type, current household fuel exposure and life time household fuel exposure.
Stove type
Among total participant of cases in the study 19(11.8%) use three-stone fire, 12(7.5%) use
shielded mud stove, 7(4.3%) use wood-burning metal stove, 108(67.1%) use improved charcoal
stove, 53(32.9%) use kerosene stove, 1(0.6%) use solar cooker and 154(95.7%) use Grid
powered electric stove. On the other side among controls 6(1.9%) use three-stone fire, 20(6.2%)
use shielded mud stove, 19(5.9%) use wood-burning metal stove, 199(61.8%) use improved
charcoal stove, 227(70.5%) use kerosene stove, 1(0.3%) use solar cooker and 310(96.3%) use
Grid powered electric stove. The detail of stove type of the study participants is presented in the
following Table 8.
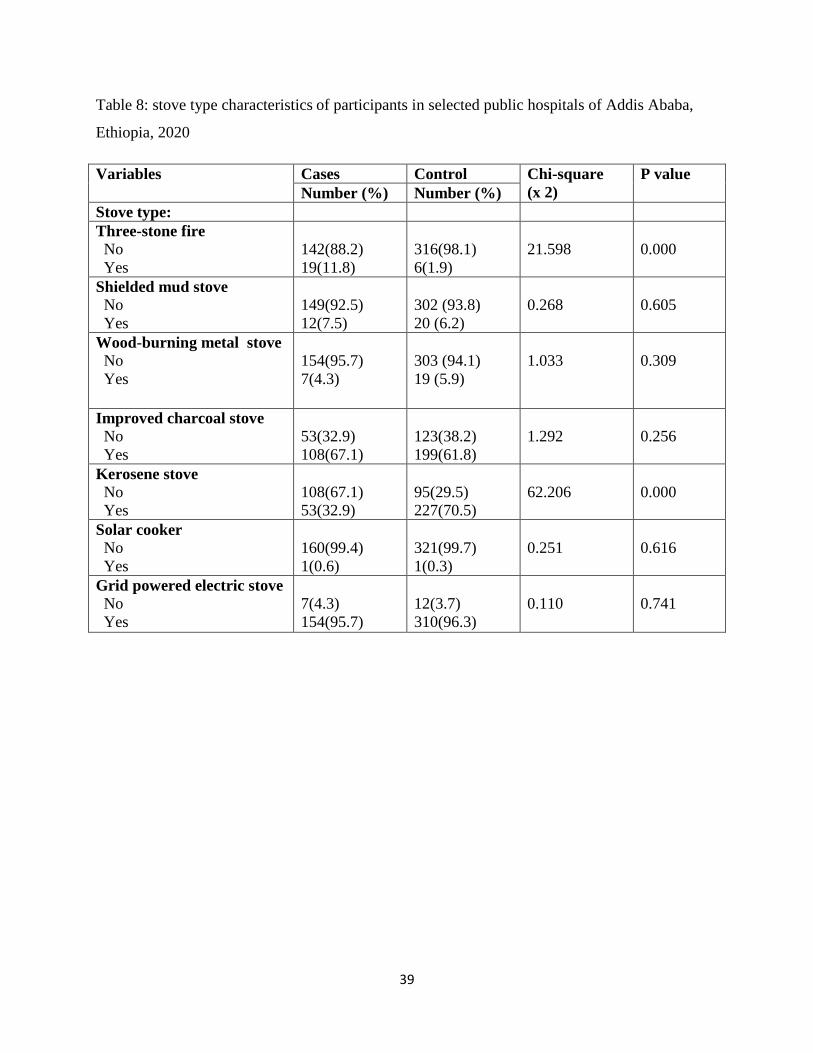
39
Table 8: stove type characteristics of participants in selected public hospitals of Addis Ababa,
Ethiopia, 2020
Variables Cases Control Chi-square
(x 2)
P value
Number (%) Number (%)
Stove type:
Three-stone fire
No
Yes
142(88.2)
19(11.8)
316(98.1)
6(1.9)
21.598
0.000
Shielded mud stove
No
Yes
149(92.5)
12(7.5)
302 (93.8)
20 (6.2)
0.268
0.605
Wood-burning metal stove
No
Yes
154(95.7)
7(4.3)
303 (94.1)
19 (5.9)
1.033
0.309
Improved charcoal stove
No
Yes
53(32.9)
108(67.1)
123(38.2)
199(61.8)
1.292
0.256
Kerosene stove
No
Yes
108(67.1)
53(32.9)
95(29.5)
227(70.5)
62.206
0.000
Solar cooker
No
Yes
160(99.4)
1(0.6)
321(99.7)
1(0.3)
0.251
0.616
Grid powered electric stove
No
Yes
7(4.3)
154(95.7)
12(3.7)
310(96.3)
0.110
0.741
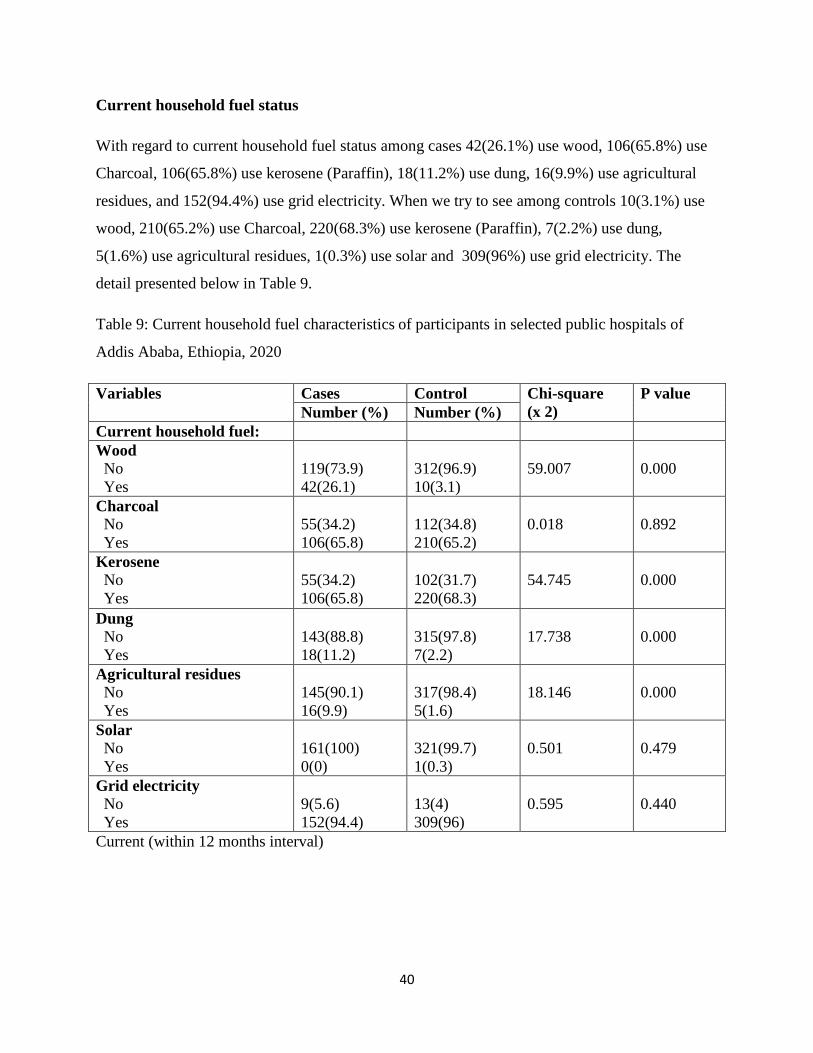
40
Current household fuel status
With regard to current household fuel status among cases 42(26.1%) use wood, 106(65.8%) use
Charcoal, 106(65.8%) use kerosene (Paraffin), 18(11.2%) use dung, 16(9.9%) use agricultural
residues, and 152(94.4%) use grid electricity. When we try to see among controls 10(3.1%) use
wood, 210(65.2%) use Charcoal, 220(68.3%) use kerosene (Paraffin), 7(2.2%) use dung,
5(1.6%) use agricultural residues, 1(0.3%) use solar and 309(96%) use grid electricity. The
detail presented below in Table 9.
Table 9: Current household fuel characteristics of participants in selected public hospitals of
Addis Ababa, Ethiopia, 2020
Variables Cases Control Chi-square
(x 2)
P value
Number (%) Number (%)
Current household fuel:
Wood
No
Yes
119(73.9)
42(26.1)
312(96.9)
10(3.1)
59.007
0.000
Charcoal
No
Yes
55(34.2)
106(65.8)
112(34.8)
210(65.2)
0.018
0.892
Kerosene
No
Yes
55(34.2)
106(65.8)
102(31.7)
220(68.3)
54.745
0.000
Dung
No
Yes
143(88.8)
18(11.2)
315(97.8)
7(2.2)
17.738
0.000
Agricultural residues
No
Yes
145(90.1)
16(9.9)
317(98.4)
5(1.6)
18.146
0.000
Solar
No
Yes
161(100)
0(0)
321(99.7)
1(0.3)
0.501
0.479
Grid electricity
No
Yes
9(5.6)
152(94.4)
13(4)
309(96)
0.595
0.440
Current (within 12 months interval)
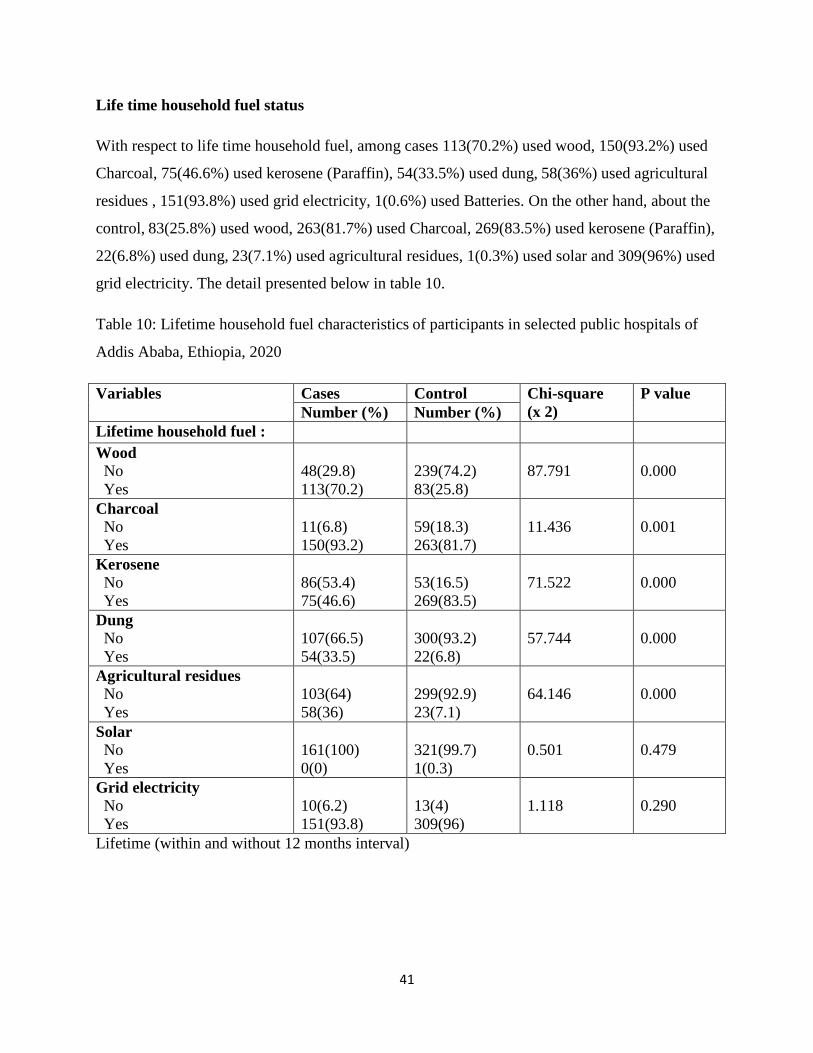
41
Life time household fuel status
With respect to life time household fuel, among cases 113(70.2%) used wood, 150(93.2%) used
Charcoal, 75(46.6%) used kerosene (Paraffin), 54(33.5%) used dung, 58(36%) used agricultural
residues , 151(93.8%) used grid electricity, 1(0.6%) used Batteries. On the other hand, about the
control, 83(25.8%) used wood, 263(81.7%) used Charcoal, 269(83.5%) used kerosene (Paraffin),
22(6.8%) used dung, 23(7.1%) used agricultural residues, 1(0.3%) used solar and 309(96%) used
grid electricity. The detail presented below in table 10.
Table 10: Lifetime household fuel characteristics of participants in selected public hospitals of
Addis Ababa, Ethiopia, 2020
Variables Cases Control Chi-square
(x 2)
P value
Number (%) Number (%)
Lifetime household fuel :
Wood
No
Yes
48(29.8)
113(70.2)
239(74.2)
83(25.8)
87.791
0.000
Charcoal
No
Yes
11(6.8)
150(93.2)
59(18.3)
263(81.7)
11.436
0.001
Kerosene No
Yes
86(53.4)
75(46.6)
53(16.5)
269(83.5)
71.522
0.000
Dung
No
Yes
107(66.5)
54(33.5)
300(93.2)
22(6.8)
57.744
0.000
Agricultural residues
No
Yes
103(64)
58(36)
299(92.9)
23(7.1)
64.146
0.000
Solar
No
Yes
161(100)
0(0)
321(99.7)
1(0.3)
0.501
0.479
Grid electricity
No
Yes
10(6.2)
151(93.8)
13(4)
309(96)
1.118
0.290
Lifetime (within and without 12 months interval)

42
There was significant difference between cases and controls with respect to life time agricultural
residues using status for household fuel.
Of the total respondents, 58(36%) and 23(7.1%) were used agricultural residues among cases and
controls respectively. Life time household biomass fuel exposure characteristics with respect to
agricultural residues using status of study participants are presented in Figure 5.
Figure 5: Life time agricultural residues using status for household fuel among participants in
selected hospitals of Addis Ababa, Ethiopia, 2020
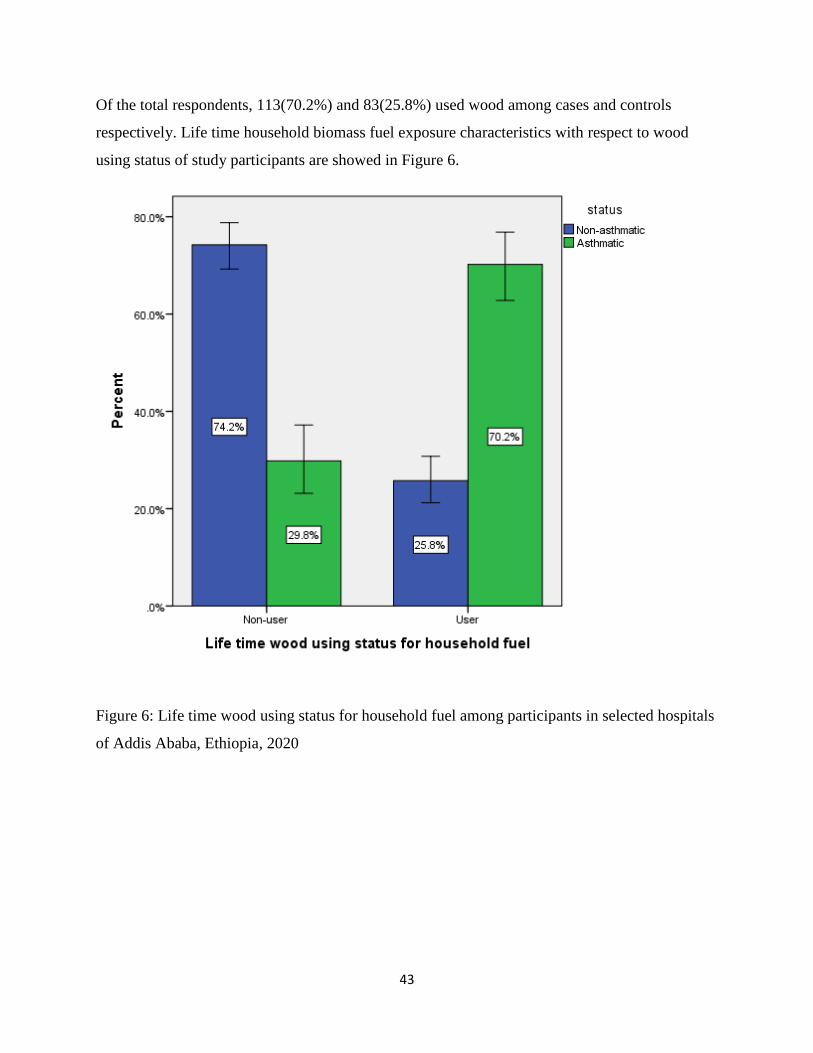
43
Of the total respondents, 113(70.2%) and 83(25.8%) used wood among cases and controls
respectively. Life time household biomass fuel exposure characteristics with respect to wood
using status of study participants are showed in Figure 6.
Figure 6: Life time wood using status for household fuel among participants in selected hospitals
of Addis Ababa, Ethiopia, 2020
44
Pet characteristics, life style and nutritional characteristics
Pet characteristics, life style and nutritional characteristics together were presented in the
following Table 11. From a total of 487 patients, a high proportion of cases 77(47.8%) and
73(22.7%) of controls has pet. Among cases 44(57.1%) were cat owner, 12(15.6%) were dog
owner, 2(2.6%) were bird owner and 19(24.7%) were both cat and dog owner. On the other hand
among controls 55(75.3%) were cat owner, 6(8.2%) were dog owner and 12(16.4%) were both
cat and dog owner Over all magnitude of ever tobacco smoking status was 22(13.7%) of cases
and 7(2.2%) of controls. Similarly, alcohol drinking status was 18(11.2) of cases and 30 (9.3) of
controls. Chat chewing status and shisha smoking status has very low magnitude based on
participants report 10(6.2%) and 1(0.6%) among cases and 19 (5.9) and 7(2.2%) among controls.
There were no drug using status in current and past time among case, but there were among
controls which are 2(0.6%). Most of participants were inactive to participate in physical activity
145(90.1%) of cases and 284(88.2%)of controls. With regard to body mass index most of the
participants had normal weight 95 (59.0%) of cases and 184(57.1%) of controls. Further
underweight, over weight and obesity can be described 6 (3.7%) of cases and 17(5.3%) of
controls, 54(33.5%) of cases and 110(34.2%) of controls and 6(3.7%) of cases and 11(3.4%) of
controls respectively.
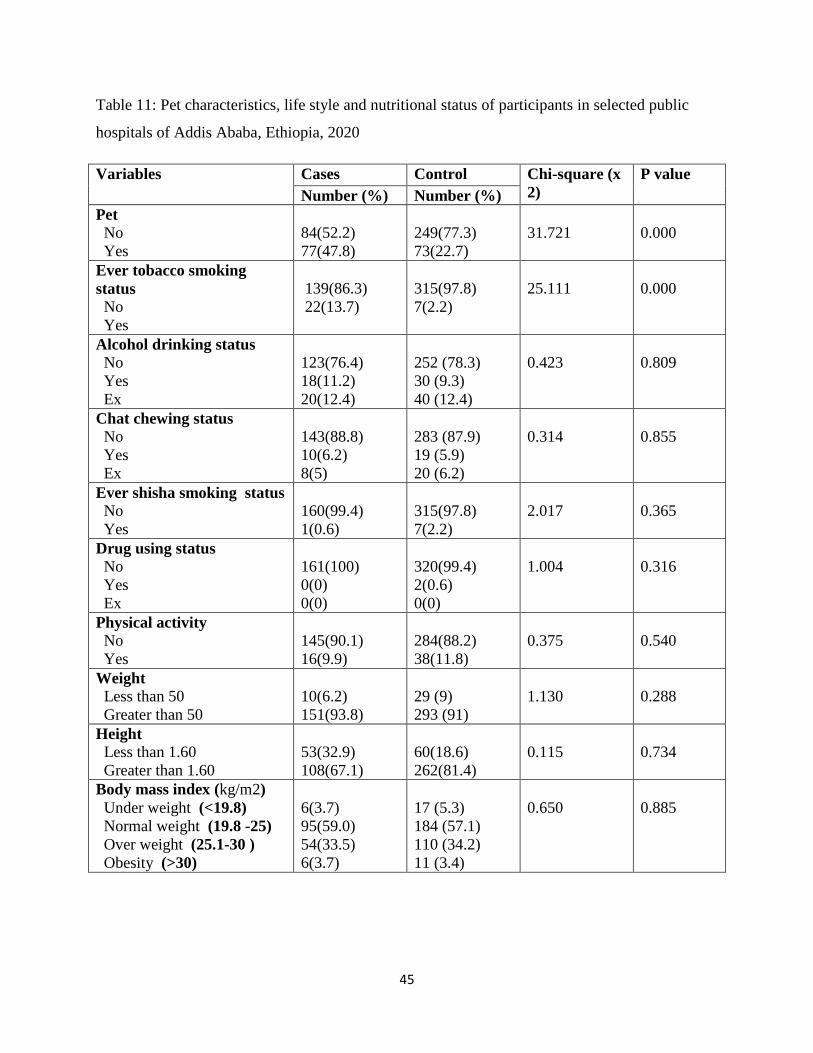
45
Table 11: Pet characteristics, life style and nutritional status of participants in selected public
hospitals of Addis Ababa, Ethiopia, 2020
Variables Cases Control Chi-square (x
2)
P value
Number (%) Number (%)
Pet
No
Yes
84(52.2)
77(47.8)
249(77.3)
73(22.7)
31.721
0.000
Ever tobacco smoking
status
No
Yes
139(86.3)
22(13.7)
315(97.8)
7(2.2)
25.111
0.000
Alcohol drinking status
No
Yes
Ex
123(76.4)
18(11.2)
20(12.4)
252 (78.3)
30 (9.3)
40 (12.4)
0.423
0.809
Chat chewing status
No
Yes
Ex
143(88.8)
10(6.2)
8(5)
283 (87.9)
19 (5.9)
20 (6.2)
0.314
0.855
Ever shisha smoking status
No
Yes
160(99.4)
1(0.6)
315(97.8)
7(2.2)
2.017
0.365
Drug using status
No
Yes
Ex
161(100)
0(0)
0(0)
320(99.4)
2(0.6)
0(0)
1.004
0.316
Physical activity
No
Yes
145(90.1)
16(9.9)
284(88.2)
38(11.8)
0.375
0.540
Weight
Less than 50
Greater than 50
10(6.2)
151(93.8)
29 (9)
293 (91)
1.130
0.288
Height
Less than 1.60
Greater than 1.60
53(32.9)
108(67.1)
60(18.6)
262(81.4)
0.115
0.734
Body mass index (kg/m2)
Under weight (<19.8)
Normal weight (19.8 -25)
Over weight (25.1-30 )
Obesity (>30)
6(3.7)
95(59.0)
54(33.5)
6(3.7)
17 (5.3)
184 (57.1)
110 (34.2)
11 (3.4)
0.650
0.885

46
Medical characteristics
With regards to medical characteristics of the study participants, presented in the following Table
12. Among the total participant 28(17.4%) of cases and 13(4.0%) of controls had family history
of asthma. Similarly, 24(14.9%) of cases and 47(14.6%) of controls have cardiac problems. On
the other hand 39(24.2%) of cases and 73(22.7%) controls had history of hypertension and
24(14.9%) of cases and 46(14.3%) of controls have diabetes. And also chronic kidney disease
and chronic liver disease reported based on participants are 13(8.1%) and 3(1.9%) of cases, and
16(5%) and 18(5.6%) of controls. The detail is presented in the table below. Further 2(1.2%) of
cases and 12(3.7%) of controls, 0(0) of cases and 7(2.2%) of controls and 5(3.1%) of cases and
8(2.5%) of controls had cancer, HIV and neurologic problem respectively.

47
Table 12: Medical condition characteristics of participants in selected public hospitals of Addis
Ababa, Ethiopia, 2020
Variables Cases Control Chi-square
(x 2)
P value
Number (%) Number (%)
Family asthma history
No
Yes
133(82.6)
28(17.4)
309(96)
13(4)
24.640
0.000
Cardiac problem
No
Yes
137(85.1)
24(14.9)
275(85.4)
47(14.6)
0.008
0.928
Hypertension
No
Yes
122(75.8)
39(24.2)
249(77.3)
73(22.7)
0.145
0.703
Diabetes
No
Yes
137(85.1)
24(14.9)
276(85.7)
46(14.3)
0.033
0.855
Chronic kidney disease
No
Yes
148(91.9)
13(8.1)
306(95)
16(5)
1.834
0.176
Chronic liver disease
No
Yes
158(98.1)
3(1.9)
304(94.4)
18(5.6)
3.584
0.058
Cancer disease
No
Yes
159(98.8)
2(1.2)
310(96.3)
12(3.7)
2.354
0.125
HIV
No
Yes
161(100)
0(0)
316(97.8)
7(2.2)
3.551
0.059
Neurologic problem
No
Yes
156(96.9)
5(3.1)
314(97.5)
8(2.5)
0.158
0.691

48
5.2 Association of different Characteristics of participant with Asthma
Multi-collinearity between independent variables were checked. The Hosmer-Lemeshow
goodness of fit test was used to assess the fitness of the final model. The final model was fit well
with X2 = 3.711 and P value of 0.882.
A comparison was done between cases and controls based on different factors, such as socio
demographic, housing , household fuel exposure , nutritional, life style , pet ownership and
medical factors. Differences between cases and controls were analyzed using chi-square test.
Then, variables found to be statistically significant with asthma in the chi-square test were
entered in the conditional bi-variable and multi-variable logistic regression analysis to identify
the independent predictors of asthma among study participants.
Variables, such as number of persons, window in cooking, window opening, door opening,
cooking time, three stone fire, kerosene stove, current wood user, current kerosene (Paraffin)
user , current dung user, current agricultural residues user, life time wood user , life time
charcoal user ,life time kerosene (Paraffin) user ,life time dung user , life time agricultural
residues user , pet ownership , ever tobacco smoking status and family asthma history were
found to be significantly associated with asthma in the conditional binary logistic regression
analysis. Such variables were included in the final model. The detail presented in the following
Table 13.
With respect to number of persons living in the house status of the study participants, four or
greater than four persons living in the house was found to be a statistically significant risk factor
for asthma. The conditional bi-variable analysis indicate that the odds of developing asthma was
found to be 2.52 times higher among patients with four or greater than four persons compared
with patients with one person living in the house, (COR: 2.525 (1.199, 5.315)). however, the
association vanished when adjusted for confounders.
Window in cooking house and window opening practice were found to be associated with
asthma in the conditional bi-variable analysis. The odds of developing asthma was found to be
lower among patients who have windows in cooking houses and window opening practice
compared to those who have not window in cooking house and window opening practice , (COR:
49
6.734(4.103, 11.051) and (COR: 6.418(3.947, 10.435) ) respectively. But the association
vanished when adjusted for confounders.
With regard to door opening practice, the conditional multiple logistic regression analysis
provided that people who didn’t practice door opening, while cooking were at high risk to
develop asthma compared with people who had door opening practice while cooking. The odds
of developing asthma was found to be 10 times higher among people who don’t have door
opening practice compared to people who have door opening practice while cooking,
(AOR:10.254, 95% CI, (3.969, 26.49))
Life time use of charcoal and dung were found to be significantly associated with asthma in the
crude analysis in our study (COR: 3.452 (1.731, 6.885)) and (COR: 7.893 (4.199, 14.838))
respectively. However, factors were not found to be statistically significant when adjusted for
confounders.
Participants who were life time wood user were at high risk to develop asthma. The conditional
multivariable analysis indicated that people who use wood in their life time for cooking were 4
times at risk of developing asthma compared to people who didn’t use, (AOR:4.954, 95% CI,
(2.1, 11.686)).
On the other hand, people who use agricultural residues for cooking throughout their life time
were found to be at risk to develop asthma compared to those who didn’t use agricultural
residues for cooking in their life time. The odds of developing asthma was found to be 3 times
higher among people who use agricultural residues for cooking compared to people who didn’t
use agricultural residues throughout their life time for cooking, (AOR:3.809, 95% CI, (1.052,
13.79)).
Participants who have pet were found to be at high risk of developing asthma in conditional bi-
variable analysis (COR: 3.188 (2.087, 4.87)), however, the association disappeared when
adjusted for confounders.
With regard to ever tobacco smoking status, the conditional bi variable analysis identified that,
tobacco use as significant risk factor to develop asthma (COR: 8.234 (3.105, 21.837) ). Its
association also existed when adjusted for confounders.
50
Current and life time kerosene users were found to be associated with asthma in the conditional
bi-variable analysis. The odds of developing asthma were found to be lower among patients who
use kerosene in current and life time exposure compared to those who didn’t use kerosene in
current and lifetime (COR: 0.226 (0.147, 0.347)) and (COR: 0.167 (0.104, 0.27) ) respectively,
but the association was not apparent when adjusted for confounders.
With regard to current wood user, using wood for cooking was found to be statistically
significant risk factor for asthma. The conditional bi-variable analysis indicated that the odds of
developing asthma was found to be 8.4 times higher among patients who use it compared with
patients who don’t use (COR: 8.406 (4.213, 16.773)), however the association vanished when
adjusted for confounders.
As we hold all other factors in the model constant, the odds of developing asthma was found to
be 6 times more likely among smoker compared to non-smokers, (AOR:6.16, 95% CI, (1.304,
29.098)).
Compared to people who hadn’t family history of asthma , people who had family history of
asthma were 5 times more likely to develop asthma, after keeping all independent variables
constant, (AOR:4.725, 95% CI, (1.544, 14.454)).

51
Table 13: Conditional multivariable logistic regression analysis of factors associated with asthma
among participants in selected public hospitals of Addis Ababa, Ethiopia, 2020
Variables Cases Control COR at 95%, CI AOR 95%, CI
Number
(%)
Number
(%)
Number of person:
1
2
3
4 or greater than 4
13(8.1)
15(9.3)
31(19.3)
102(63.4)
44(13.7)
30(9.3)
84(26.1)
164(50.9)
1
2.079 (0.827, 5.229)
1.389 (0.627, 3.078)
2.525 (1.199, 5.315)
1
4.104 (0.709, 23.762)
2.544 (0.598, 10.819)
1.425 (0.298, 6.811)
Window in cooking
house
No
Yes
84(52.2)
77(47.8)
46(14.3)
276(85.7)
6.734 (4.103, 11.051)
1
1.916 (0.008,
477.767)
1
Window opening
No
Yes
85(52.8)
76(47.2)
49(15.2)
273(84.6)
6.418 (3.947,10.435)
1
2.174 (0.009,
520.665)
1
Door opening
No
Yes
47(29.2)
114(70.8)
23(7.1)
299(92.9)
5.127 (2.933, 8.963)
1
10.254 (3.969, 26.49)*
1
Cooking time
Less than 60 mint
60-120 mint
Greater than 120 mint
71(44.1)
74(46.0)
16(9.9)
2(0.6)
304(94.4)
16(5)
1
1.028 (0.656, 1.611)
2.312 (1.048, 5.103)
1
0.687 (0.297, 1.589)
1.605 (0.313, 8.234)
Stove type:
Three-stone fire
No
Yes
142(88.2)
19(11.8)
316(98.1)
6(1.9)
1
5.615 (2.358,13.372)
1
0.202 (0.014, 2.924)
Kerosene stove
No
Yes
108(67.1)
53(32.9)
95(29.5)
227(70.5)
1
0.213 (0.139, 0.326)
1
0.203 (0.031, 1.338)
Current household fuel:
Wood
No
Yes
119(73.9)
42(26.1)
312(96.9)
10(3.1)
1
8.406 (4.213, 16.773)
1
5.479 (0.432, 69.516)
Kerosene (Paraffin)
No
Yes
55(34.2)
106(65.8)
102(31.7)
220(68.3)
1
0.226 (0.147, 0.347)
1
3.392 (0.454, 25.346)
Dung
No
Yes
143(88.8)
18(11.2)
315(97.8)
7(2.2)
1
5.77 (2.283, 14.581)
1
0.621 (0.06, 6.461)
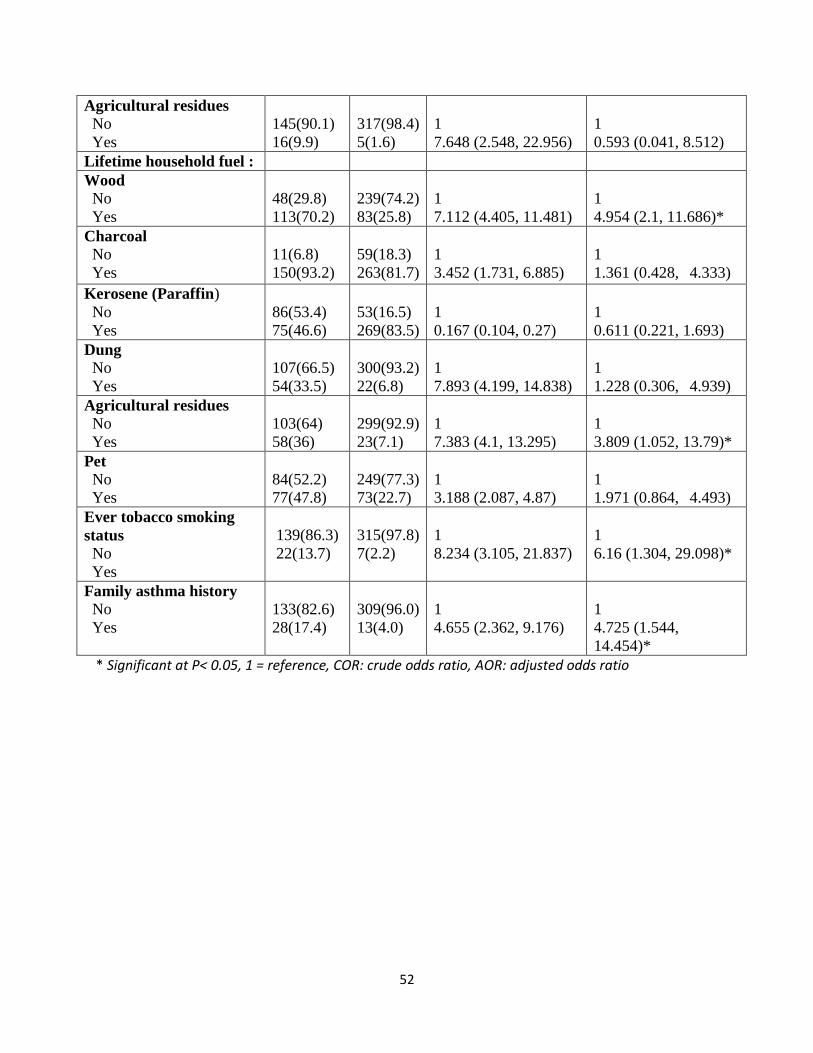
52
Agricultural residues
No
Yes
145(90.1)
16(9.9)
317(98.4)
5(1.6)
1
7.648 (2.548, 22.956)
1
0.593 (0.041, 8.512)
Lifetime household fuel :
Wood
No
Yes
48(29.8)
113(70.2)
239(74.2)
83(25.8)
1
7.112 (4.405, 11.481)
1
4.954 (2.1, 11.686)*
Charcoal
No
Yes
11(6.8)
150(93.2)
59(18.3)
263(81.7)
1
3.452 (1.731, 6.885)
1
1.361 (0.428, 4.333)
Kerosene (Paraffin)
No
Yes
86(53.4)
75(46.6)
53(16.5)
269(83.5)
1
0.167 (0.104, 0.27)
1
0.611 (0.221, 1.693)
Dung
No
Yes
107(66.5)
54(33.5)
300(93.2)
22(6.8)
1
7.893 (4.199, 14.838)
1
1.228 (0.306, 4.939)
Agricultural residues
No
Yes
103(64)
58(36)
299(92.9)
23(7.1)
1
7.383 (4.1, 13.295)
1
3.809 (1.052, 13.79)*
Pet
No
Yes
84(52.2)
77(47.8)
249(77.3)
73(22.7)
1
3.188 (2.087, 4.87)
1
1.971 (0.864, 4.493)
Ever tobacco smoking
status
No
Yes
139(86.3)
22(13.7)
315(97.8)
7(2.2)
1
8.234 (3.105, 21.837)
1
6.16 (1.304, 29.098)*
Family asthma history
No
Yes
133(82.6)
28(17.4)
309(96.0)
13(4.0)
1
4.655 (2.362, 9.176)
1
4.725 (1.544,
14.454)*
* Significant at P< 0.05, 1 = reference, COR: crude odds ratio, AOR: adjusted odds ratio
53
6. Discussions
The aim of the study was to assess factors associated with asthma, with special reference to
household fuel exposure and housing characteristics in selected public hospitals in Addis Ababa,
Ethiopia. We found that door opening practice while cooking as a protective factor for asthma.
On the other hand, life time uses of wood and agricultural residues for cooking purpose and
tobacco for smoking purpose were found to be significant risk factors for asthma. Family history
of asthma was also noted to be another risk factor for asthma.
In this study, 483 subjects participated, among them high proportion of controls had door
opening practice during cooking hours 299 (92.9%) compared to cases 76(47.2%). The odds of
developing asthma was 10 times higher among individuals who practice door opening while
cooking compared with individuals who don’t practice (AOR: 10.254, 95% CI:3.969, 26.49 ).
The association may be due to overcrowding and inadequate ventilation for the presence of
smoke measured by elevated CO2 level, high level of benzene and other VOCs (16). This may
take the responsibility for the development of asthma. The finding on this study supported by
different studies like that of the study which was conducted in Alaska (16), in Japan (89) and
Southern New England (63). In contrast to that, another study conducted in Peru provides
unequivocal report which state there is no association between door opening practice and asthma
(90). This variation may occur due to area of cooking room and other smoke extraction system.
The finding of the study demonstrated that (36%) among cases and (7.1%) among controls were
using agricultural residues as a source of household fuel in their life time. Those subjects who
used agricultural residues in their life time were almost four times more likely to develop asthma
compared to people, who don’t use agricultural residues in their life time for cooking (AOR:
3.809, 95% CI: 1.052, 13.79).
Similarly the use of wood in their life time for cooking purpose was found to be important
predictor for the acquiring of asthma in this study. The odds of developing asthma was almost
five times higher among subjects who use wood for cooking compared to subjects who don’t use
wood (AOR: 4.954, 95% CI: 2.1, 11.686). Finding from this study suggest that the risk of wood
smoke exposure for asthma may be confined due to their duration of exposure to the smoke and
compromised respiratory system from cooking smoke.

54
The association between biomass fuel smoke exposure and asthma are confirmed by different
researches for instance a cross-sectional studies conducted in Turkey (56), in Nigeria (46) and in
India (27, 55). The justification for this may be smoke emanating from burning biomass fuels
contains toxic pollutants called oxidants, which include volatile organic compound (VOCs),
particulate matter (PM), carbon monoxide (CO), and oxides of nitrogen, sulfur and Florine (91).
Because of this oxidative stress, which is imbalance between biological pro-oxidants and anti-
oxidant defense system, some changes observed like initiate cytokine production and depression
of protective membrane and mediates inflammatory response or worsen asthma due to a
compromised anti-oxidant defense system (91).
On the other hand, study conducted in Peru (15) and in Nigeria (42) have showed lack of
association between biomass fuel smoke exposure and asthma. The discrepancies between
studies may be possible due to variations in cooking area, ventilation system, as well as in type,
duration and intensity of biomass fuel smoke exposure.
Smoking has also been identified as important risk factor for developing asthma by six times
(AOR: 6.16, 95% CI: 1.304, 29.098). Our study produce similar finding with the study
conducted in Thailand which state that there is a significant association between smoking and
asthma (66). The justification for this may be the effect of smoking on airway i.e. tobacco smoke
flow inward to inflammatory cell like neutrophils, lymphocytes, eosinophils, mast cell and
macrophages (92). Due to this various inflammatory mediators are released which include lipids,
chemokines, cytokines and growth factor and those proteolytic enzymes cause inflammatory
damage and bronchial hyper responsiveness which is hall mark of asthma (92). On the other
hand studies conducted in Britain (48) and Uganda (93) are in contrast with our finding by
stating there is no significant association between tobacco smoking and asthma. This could be
due to variation in the study population, magnitude of cigarette smoking.
Patients who had family history of asthma were more than four times more likely to develop
asthma compared to those who had no family history of asthma (AOR: 4.725, 95% CI: 1.544,
14.454). The possible explanation for this association could be either due to hereditary factors or
a shared environment by the member of a family contributes to the pathogenesis of asthma (15).
The finding of our study is supported by other studies which were conducted in Australia (66),
Thailand (94), Uganda (95), New Zealand (96) and California (97) , which conclude that family

55
history of asthma is one of the major risk factor for the development of asthma. The justification
for the similarity might be the study setting in which most of the studies were conducted in a
hospital setting. However, another study conducted in Britain is not in agreement with our
finding, which states that there is no significant relationship between family history of asthma
and asthma (93). This may be due to study design and population characteristics.
On the other hand, conditional multivariable analysis showed that there is no statistically
significant difference between cases and controls related to number of person living in a
household (AOR:4.104, 95% CI, (0.709, 23.762)), (AOR:2.544, 95% CI, (0.598, 10.819)) and
(AOR:1.425, 95% CI, (0.298, 6.811)) despite a significant association was found in conditional
bi-variable analysis.
In our study, statistical significant association was not found between both having window in
cooking house and window opening practice during cooking time with the risk of asthma when
adjusted for confounders ((AOR:1.916, 95% CI, (0.008, 477.767)) and (AOR:2.174, 95% CI,
(0.009, 520.665)) ) respectively. Despite significant association was found in the crude analysis.
With regard to cooking time, the conditional multivariable analysis yield that there is no
statistically significant association between cooking time and asthma (AOR: 0.687, 95% CI,
(0.297, 1.589)) and (AOR: 1.605, 95% CI, (0.313, 8.234)). Despite significant association was
found in crude analysis.
According to this study regarding stove type, statistically significant association was not found
between both three stone fire stove and kerosene stove with the risk of asthma when adjusted for
confounders (AOR:0.202, 95% CI, (0.014, 2.924)) and (AOR:0.203, 95% CI, (0.031, 1.338))
respectively. Despite significant association was found in conditional bi-variable analysis.
With respect to current household fuel type such as wood, kerosene, dung and agricultural
residues have no relationship with the risk of asthma after adjusted for covariates (AOR:5.479,
95% CI, (0.432, 69.516)), (AOR:3.392, 95% CI, (0.454, 25.346)), (AOR:0.621, 95% CI, (0.06,
6.461)) and (AOR:0.593, 95% CI, (0.041, 8.512)) respectively though statistically significant
association was found in the crude analysis.

56
Except wood and agricultural residues , life time household fuel type such as charcoal, kerosene
and dung on conditional multivariable analysis revealed that statistically significant was not
found between life time house hold fuel type (charcoal, kerosene and dung) and asthma ((AOR:
1.361, 95% CI, (0.428, 4.333)), (AOR: 0.611, 95% CI, (0.221, 1.693)) and (AOR: 1.228, 95%
CI, (0.306, 4.939)) respectively.
Likewise, no relationship was observed between asthma and pet ownership after adjusted for
covariates (AOR: 1.971, 95% CI, (0.864, 4.493)) though statistically significant was not found in
the conditional bi-variable analysis. This finding is comparable with a study conducted in united
kingdom (25). Nevertheless , the finding of our study is in contrast to the study in united
kingdom (65). The possible explanation could be due to difference in method of assessment of
pet contact, genetically and environmental factor.
On the contrary , such variables, among socio demographic characteristics age (41), sex (44),
residences , marital status, educational status (46), occupational status (49), monthly income (9)
and religion) , among housing characteristics (number of rooms, household crowding index,
lighting source , cooking area, cooking house floor material, cooking house wall material,
cooking house roof martial, smoke extraction (46), ), among stove type (shielded mud stove (46),
wood burning metal stove (27), improved charcoal stove (27), solar cooker, grid powered
electric stove), among current household fuel type (charcoal (27), solar, grid electricity), among
life time household fuel type (solar, grid electricity), among life style characteristics (alcohol
drinking status, chat chewing status, shisha smoking status, drug using status, physical activity )
(48), among nutritional status (weight, height, body mass index) (15) , among chronic medical
condition (cardiac problem, hypertension, diabetes mellitus, chronic kidney disease, chronic liver
disease, cancer disease, HIV, neurologic problem ) were not significantly associated with
asthma in the conditional bi-variable analysis. Because of this these variables were not selected
as a candidate for the final model however significant associations were reported in previous
studies.
Most of the studies on asthma and its risk factors employed by cross sectional method, which has
a limitation of statistical power by comparing the groups internally. When we compare the
introduction of bias, matched case control study design has lower bias than cross sectional study.
Because of this it is assumed that to generate valid data among main exposure variables.
57
7. Strengths and limitations of the study
7.1. Strengths
Cases included in the study were selected based on spirometry results. This may reduce
wrong diagnosis of the asthma.
Using trained nurses who work in the selected hospitals as data collectors helped to keep
the privacy of the respondents because of this they can provide the required information
comfortably.
Investigating the effect of multiple risk factors of Asthma simultaneously could be the
strength of the study.
Cases and controls were recruited at the same facility, to control for the context
difference in the study participants.
To control the influence of using matched design, matched analysis (conditional logistic
regression analysis) was employed which is one of the strengths of the study.
Representative sample size was taken.
7.2 Limitations
Assessment of housing characteristics information was obtained by interview, but it
would be better if we obtain it through direct physical observation.
Since the study was done in institutions, it might not be generalized to the general
population with asthma.
58
8. Conclusions and recommendations
8.1 Conclusions
This study demonstrated some of the factors associated with asthma. For instance, using wood
and agricultural residues for cooking purpose in their life time were found to be significant risk
factors for asthma. Tobacco smoking was also considered to be another risk for asthma. On the
other hand, opening door while cooking was found to be preventive for asthma. Family history
of asthma was noted to have its own contribution for the development of asthma.
8.2 Recommendations Based on factors identified in the study we provide the following recommendations
For the public
It will be better if the people avoid using wood and agricultural residues as household
fuel for cooking or other purposes.
It will be of great help in order to prevent asthma by practicing door open practice while
cooking for better ventilation.
People should avoid tobacco smoking in order to prevent asthma development.
For FMHACA
Prepare trainings for health professionals, who work in, to widen their understanding
about factors associated with asthma special reference to household fuel exposure and
housing characteristics.
FMHACA should include door open practice in the checklist, which they use to control
food and drink establishment institutes, as mandatory /critical requirement in order to
provide a licence.
For health care providers
Health professionals should counsel patients by providing risk and preventive factors that
are associated with asthma.
For the researcher
It would be great if a study is conducted by direct observation in the house of the patient
to check the exact housing characteristics and different observation may they hide in
interview.
Further study shall be conducted in cohort study design to show a cause and effect
relationship between asthma and its risk factor.
59
9. References 1. WHO. Household air pollution and health (Fact sheets ): World Health Organization; 2018 [cited 2018 8 May ]. 2. MORTEN A. SCHEI, JENS O. HESSEN, KIRK R. SMITH, NIGEL BRUCE, JOHN McCRACKEN, LOPEZ. V. Childhood asthma and indoor woodsmoke from cooking in Guatemala. Journal of Exposure Analysis and Environmental Epidemiology. 2004;14:110-7. 3. health FdroEmo. National strategic action plan (NSAP) for prevention and control of non communicable disease in Ethiopia. Addis Ababa, Ethiopia 2016. 4. Lango, Fauci, Kasper, Hauser, Jameson, Loscalzo. HARRISONS principle of internal medicine 8, editor. 5. Mary Spitak Bilitski Msn, Sally Wonzel, Vitari C. what is asthma? patient education serious, American thoracic society. 2013. 6. Mims Jw. Asthma defination and pathophysiology Int forum Allergy Rhinol. 2015:52-6. 7. The Global Asthma Report 2018. Auckland, New Zealand: Global Asthma Network; 2018. 8. S.Romanet Manent, D. Charpin, A. Magnan, A. Lanteaume, vervloet D. Allergic vs Non allergic Asthma: What makes the diffrence? Blackwell Munksgard. 2002;57:607-13. 9. Sisay Shine, Sindew Muhamud, Demelash. A. Prevalence and associated factors of bronchial asthma among adult patients in debreberhan referral hospital, Ethiopia BMC research note 2019;608. 10. Asnakew Achaw Ayele, Tegegn. HG. Non adherence to inhalational medications and associated factors among patients with asthma in a referral hospital in Ethiopia, using validated tool TAI. Asthma research and practice 2017:1186. 11. Carlos Nunes, Ana Margarida Pereira, Morais-Almeida2 M. Asthma costs and social impact. Asthma Research and Practice 2017;3:1. 12. Nadia Aı¨t-Khaled, Donald Enarson, Bousquet. J. Chronic respiratory diseases in developing countries: the burden and strategies for prevention and management. Bulletin of the World Health Organization. 2001;79:10. 13. Louis-Philippe Boulet, Boulay. M-È. Asthma-related comorbidities. Expert reviws respiratory medicine. 2011;5(3):377-93. 14. Colin L Robinson, Lauren M Baumann, Karina Romero, Juan M Combe, Alfonso Gomez, Robert H Gilman, et al. Effect of urbanisation on asthma, allergy and airways inflammation in a developing country setting. Thorax. 2011;66:1051e7. 15. Chelsea Gaviola, Catherine H Miele, Robert A Wise, Robert H Gilman, Devan Jaganath, J Jaime Miranda, et al. Urbanisation but not biomass fuel smoke exposure is associated with asthma prevalence in four resource-limited settings. Thorax 2016;71:154–60. 16. Rosalyn Singleton, Aaron J Salkoski, Lisa Bulkow, Chris Fish, Jennifer Dobson, al. LAe. Housing characteristics and indoor air quality in households of Alaska native children with chronic lung conditions. Anchorage 2016. 17. Damtew Dagoye, al. ZBe. wheezing, allergy and parasite infection in children in urban and rural ethiopia critical care medicine 2003;167:1369-73. 18. Kathleen belanger, Elizabeth W. triche. Indoor combustion and asthma National inistitute of health public access. 2008;28(3):507. 19. Oluwafemi Oluwole, Ganiyu O. Arinola, Dezheng Huo, O.Olopade. C. Biomass fuel exposure and asthma symptoms among rural school children in Nigeria. journal of asthma 2016. 20. Raj Kumar, Jitendra K. Nagar, Neelima Raj, Pawan Kumar, Alka S. Kushwah, Mahesh Meena, et al. Impact of Domestic Air Pollution from Cooking Fuel on Respiratory Allergies in Children in India. ASIAN PACIFIC JOURNAL OF ALLERGY AND IMMUNOLOGY 2008;26:213-22.
60
21. Erik R. Svendsen, Melissa Gonzales, Adwoa Commodore. The role of indoor enviroment :Residential determinant of allergy,asthma and plumonary function Science of total enviroment 2018:616-27. 22. M. khaleguzzaman, M. Kamijima, K.sakai, N. hamajima, Nakajima T. Indoor air pollution and its impact on children under five years old in bangladish. Blackwell Munksgard. 2007;17:297=304. 23. Marianne Frieri, Maeve O’Connor, Nassef. M. Asthma, stress, and depression in women. (Allergy Asthma Proc 2015;36:256 –61. 24. Elizabeth W. Holt, Katherine P. Theall, Rabito. FA. Individual, Housing, and Neighborhood Correlates of Asthma among Young Urban Children. Journal of Urban Health: Bulletin of the New York Academy of Medicine. 2012;90:1. 25. S.M.Collin, R. Granell, C. Westgarth, J. murray, Paul E, C. Sterne, et al. Pet ownership is associated with increased risk of non-atopic asthma and reduced risk of atopy in childhood. Clinical & Experimental Allergy. 2015;45:200-10. 26. Sisay Shine, Sindew Muhamud, Demelash. A. Prevalence and associated factors of bronchial asthma among adult patients in Debre Berhan Referral Hospital, Ethiopia 2018: a cross‑sectional study. BMC research note. 2018;12:608. 27. Raj Kumar, K. J, Nagar, Neelima Raj, Pawan Kumar, Alka S. Kushwah, et al. Impact of Domestic Air Pollution from Cooking Fuel on Respiratory Allergies in Children in India. ASIAN PACIFIC JOURNAL OF ALLERGY AND IMMUNOLOGY. 2008;26:213-22. 28. Akshay Sood. Indoor fuel exposure and the lung in both developing and developed countries:. NIH Public Access. 2012;33(4) 649–65. 29. Frederik van Gemerta, Thys van der Molena, Rupert Jonesb, Chavannesc. N. The impact of asthma and COPD in sub-Saharan Africa. Primary Care Respiratory journal 2011;20(3):240-8. 30. Non communicable disease Geneva, Switzerland: World health organization
2018. 31. Awoke Misganaw, Damen Haile Mariam, Ahmed Ali, Araya. T. Epidemiology of Major Non-communicable Diseases in Ethiopia: A Systematic Review. INTERNATIONAL CENTRE FOR DIARRHOEAL DISEASE RESEARCH. 2014;32:1-13. 32. organization Wh. Non communicable disease country profile 2018. 33. Braman SS. The Global Burden of Asthma. Chest 2006 2006;130:4s-12s. 34. Croisant S. Epidemiology of Asthma: Prevalence and Burden of Disease. In: Brasier AR, editor. Advances in Experimental Medicine and Biology. New York: Springer Science+Business Media 2014. 35. Wjst M, Boakye D. Asthma in africa PLOS med 2007. 36. Daniel O. Obaseki, Francis O. Awoniyi, Olayemi F. Awopeju, Erhabor GE. Low prevalence of asthma in sub Saharan Africa: A cross sectional community survey in a suburban Nigerian town. Respiratory Medicine 2014;108:1581-8. 37. Ethiopia health profile World healthorganization
2017. 38. Melaku K , Y. B. Prevalence of wheeze and asthma related symptoms among school children in Addis Ababa, Ethiopia. Ethiopian medicine journal. 1999;37:247-54. 39. Sirak Hailu, Tesfaye Tessema, Silverman. M. Prevalence of Symptoms of Asthma and Allergies in Schoolchildren in Gondar Town and Its Vicinity, Northwest Ethiopia
Pediatric Pulmonology 2003;35:427-32. 40. Haile Yemaneberhan, Zegaye Bekele, Andrea Venn, Sarah Lewis, Eldryd Parry, Britton. J. Prevalence of wheeze and asthma and relation to atopy in urban and rural Ethiopia. THE LANCET. 1997;350.
61
41. G. Davey, A. Vennw, H. Belete, Y. Berhane, Brittonw J. Wheeze, allergic sensitization and geohelminth infection in Butajira, Ethiopia. Clinical and Experimental Allergy. 2005;35:301–7. 42. Jesse D. Thacher, Anders Emmelin, Aboi J.K. Madaki, Thacher. TD. Biomass fuel use and the risk of asthma in Nigerian children. Respiratory Medicine. 2013;107:1845-51. 43. Kabengele Benoit Obel1, Kayembe Jean Marie Ntumba, Kayembe Patrick Kalambayi, Akilimali Pierre Zalagile, kaba Didine Kinkodi, Munogolo. KZ. Prevalence and determinants of asthma in adults in Kinshasa. PLOS ONE. 2017:1-13. 44. P.T.B.S. Brancoa, R.A.O. Nunesa, M.C.M. Alvim-Ferraza, F.G. Martinsa, C. Ferrazb, L.G. Vazb, et al. Asthma prevalence and risk factors in early childhood at Northern Portugal. Rev Port Pneumol. 2016;22(3):146-50. 45. Nezar Mehanna, Nader Mohamed, Moges Wordofa, Dessie Abera, Abiyot Mesfin, al. MWe. Allergy-related disorders (ARDs) among Ethiopian primary school-aged children: Prevalence and associated risk factors. PLOS one 2018;13(9). 46. Oluwafemi Oluwole, Ganiyu O. Arinola, Dezheng Huo, Olopade4. CO. Household biomass fuel use, asthma symptoms severity, and asthma underdiagnosis in rural schoolchildren in Nigeria: a cross-sectional observational study. BMC Pulmonary Medicine. 2017;17:3. 47. Imane Ghanname, Ahmed Chaker, Abha Cherkani Hassani, Laila Herrak, Serge Arnaul Ebongue, Mustapha Laine, et al. Factors associated with asthma control: MOSAR study (Multicenter Observational Study of Asthma in Rabat-Morocco). BMC Pulmonary Medicine. 2018;18:61. 48. Richard E Sanya, Bruce J Kirenga, William Worodria, Okot-Nwang. M. Risk factors for asthma exacerbation in patients presenting to an emergency unit of a national referral hospital in Kampala, Uganda. African Health Sciences 2014;14:707-15. 49. Mohamed F. Jeebhay, Dorothy Ngajilo, Moual. Nl. Risk factors for nonwork-related adult-onset asthma and occupational asthma: a comparative review. Wolters Kluwer Health. 2014;14:84-94. 50. Dorothy Ngajilo, Tanusha Singh, Edith Ratshikhopha, Payal Dayal, Onnicah Matuka, Roslynn Baatjies, et al. Risk factors associated with allergic sensitization and asthma phenotypes among poultry farm workers. aMERICAN jOURNAL oF INDUSTRIAL MEDICINE 2018:1-9. 51. Bruce J. Kirenga , Corina de Jong, Winceslaus Katagir, Samuel Kasozi, Levicatus Mugenyi, Marike Boezen, et al. Prevalence and factors associated with asthma among adolescents and adults in Uganda: a general population based survey. BMC Public Health. 2019;19:227-36. 52. Boulet L-P. Influence of obesity on the prevalence and clinical features of asthma. Clin Invest Med. 2008;31:386-90. 53. WHO guidelines for indoor air quality: selected pollutants. World Health Organization
2010. 54. S Kirchner, N Pasquier, D Cretier, S Gauvin, F Golliot, D Pietrowski , et al. THE FRENCH PERMANENT SURVEY ON INDOOR AIR QUALITY SURVEY DESIGN IN DWELLINGS AND SCHOOLS. INDOOR AIR. 2002:449-54. 55. Mishra V. Effect of Indoor Air Pollution from Biomass Combustion on Prevalence of Asthma in the Elderly. Environmental Health Perspectives. 2003;111. 56. Kürsat UZUN, Bülent ÖZBAY, Erkan CEYLAN, Mehmet GENCER, ZEHIR. I. Prevalence of Chronic Bronchitis-Asthma Symptoms in Biomass Fuel Exposed Females. Environmental Health and Preventive Medicine. 2003;8:13-7. 57. Jae-Young Choi, Jill Baumgartner, Sarah Harnden, Bruce H Alexander, Robert J Town, George D’Souza, et al. Increased risk of respiratory illness associated with kerosene fuel use among women and children in urban Bangalore, India. Occup Environ Med. 2015;72:114–22.
62
58. ANDREA J. VENN, HAILE YEMANEBERHAN, ZEGEYE BEKELE, SARAH A.LEWIS, ELDRYD PARRY, BRITTON. J. Increased Risk of Allergy Associated with the Use of Kerosene Fuel in the Home. AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE. 2001;164:1660-5. 59. S. M. Willers, B. Brunekreef, M. Oldenwening, H. A. Smit, M. Kerkhof, H. De Vries, et al. Gas cooking, kitchen ventilation, and asthma, allergic symptoms and sensitization in young children – the PIAMA study. 2006;61:563–8. 60. Zealand SN. Measuring housing quality: Potential ways to improve data collection on housing quality in New Zealand. Statistics New Zealand. 2015. 61. Gisele M carriere, Rochelle garner, sanmarti C. Housing condition and respiratory hospitalizations among first nation people in canada. Statistics canada 2017. 62. Jennifer Northridae, Olivia F. Ramirez, Jeanette A. stingone, claudio L. The role of housing type and housing quality in urban children with asthma The new york academy of medicine 2010;87. 63. Karen C. Dannemiller, Janneane F. Gent, Brian P. Leaderer, Peccia. J. Influence of housing characteristics on bacterial and fungal communities in homes of asthmatic children. yale edu. 2009:432-8. 64. Tugba Arikoglu, Sehra Birgul Batmaz, Taner Coşkun, Feza Otag, Didem Derici Yildirim, Kuyucu. S. The characteristics of indoor and outdoor fungi and their relation with allergic respiratory diseases in the southern region of Turkey. crossvmark. 2016;188:380. 65. A.J simpson, S.P Mstusiewicz, A.P Greening, Crompton GK. Pet ownership and asthma morbidity Respiratory medicine 2000;94:91-2. 66. Darika Wortong, Naesinee Chaiear, Boonsawat. W. Risk of asthma in relation to occupation: A hospitalbased case-control study. Asian Pac J Allergy Immunol. 2015;33:152-60. 67. Alan P. Koterba, Carol A. Saltoun. Asthma classification Ocean side publication. 2012;33:3. 68. Adugna A. HEALTH INSTITUTIONS AND SERVICES. 2014. 69. Ethiopia National Health Insurance Scale-Up Assessment on Medicines Financing, Use, and Benefit Management: Findings, Implications, and Recommendations. Ethiopia federal ministry of health, 2016. 70. G. Hadgu, S. Almaz, Tsehay. S. Assessment of Nurses’ Perceptions and Barriers on Evidence Based Practice in Tikur Anbessa Specialized Hospital Addis Ababa Ethiopia. American Journal of Nursing Science 2015;4(3):73-83. 71. Abate Bane, Tola Bayisa , Fetene Adamu, Abdissa. SG. Medical Admissions and Outcomes at Saint Paul’s Hospital, Addis Ababa, Ethiopia: a retrospective study. Ethiop J Health Dev. 2016;30:1. 72. Nashila Mohamed, Lucy ngang, Joseph odhiambo, Janet nyamways, menzies R. Home enviroment and asthma in kenya Thorax. 1995;50:74-8. 73. Harriet Mpairwe, Milly Namutebi, Gyaviira Nkurunungi, Pius Tumwesige, Irene Nambuya , Mike Mukasa1, et al. Risk factors for asthma : a case-control study in urban Uganda. 74. Doyin Fagbule , Ekanem. EE. Some environmental risk factors for childhood asthma: a case-control study. Annals of Tropical Paediatrics. 1994. 75. society At. Recommended respiratory disease questionnaires for use with adults and children epidemiological research 76. Peter Burney, Jarvis D. THE EUROPEAN COMMUNITY RESPIRATORY HEALTH SURVEY II. European Commission. 77. R. Albertyn, H. Rode, A.J.W. Millar, Peck. MD. The domestication of fire: The relationship between biomass fuel, fossil fuel and burns. Burns. 2012;38:7 9 0 – 7 9 5. 78. H. W. DE KONING, K. R. SMITH, LAST. JM. Biomass fuel combustion and health. Bulletin ofthe WorldHealth Organization. 1985;63 (1):11 - 26. 79. R. Saidura, E.A. Abdelaziza, A. Demirbasb, M.S. Hossaina, Mekhilefc. S. A review on biomass as a fuel for boilers. Renewable and Sustainable Energy Reviews 2011;15:2262–89.
63
80. I S Melki, H A Beydoun, M Khogali, H Tamim, Yunis. KA. Household crowding index: a correlate of socioeconomic status and inter-pregnancy spacing in an urban setting. Journal of Epidemiology & Community Health. 2004;58:476–80. 81. Mood EW. APHA -CDC RECOMMENDED MINIMUM HOUSING STANDARDS. 1015 Fifteenth Street, NW Washington, DC 200051986. 82. Helenice Sacht, Lukiantchuki MA. Windows Size and the Performance of Natural Ventilation. Procedia Engineering 2017;196 972 – 9. 83. CARL J. CASPERSEN, KENNETH E. POWELL, CHRISTENSON. GM. Physical Activity, Exercise, and Physical Fitness: Definitions and Distinctions for Health-Related Research. Public Health Reports. 1985;100:129. 84. Chong Y, Klein R, Plepys C. Operational definitions for year 2010 objectives: Physical Activity and Fitness. Healthy People 2000 Statistical Notes; National Center for Health Statistics. 2008. 85. JOSE DE LEON, M. D, RENDON, FELIPE AIZPURU, ANA GONZALEZ-PINTO, CECILIA ANITUA , et al. ASSOCIATION BETWEEN SMOKING AND ALCOHOL USE IN THE GENERAL POPULATION: STABLE AND UNSTABLE ODDS RATIOS ACROSS TWO YEARS IN TWO DIFFERENT COUNTRIES. Alcohol & Alcoholism. 2007;42:252–7. 86. Kishor Khanal1, Chataut. J. Association between Alcohol Consumption and Smoking Habit in the General Population of Rural Nepalese Community. ACCLM. 2017;3(1):22-9. 87. Boulet L-P. Influence of obesity on the prevalence and clinical features of asthma. Clin Invest Med. 2008;31 (6): E386-E90. 88. Pablo Monsivais, Anju Aggarwal, Drewnowsk. A. Time Spent on Home Food Preparation and Indicators of Healthy Eating. American Journal of Preventive Medicine. 2014;47(6):796–802. 89. Shi Cong, Atsuko Araki, Shigekazu Ukawa, Yu Ait Bamai, Tajima. S. Association of Mechanical Ventilation and Flue Use in Heaters With Asthma Symptoms in Japanese Schoolchildren: A Cross-Sectional Study in Sapporo, Japan. J Epidemiol 2014;;24(3)::230-8. 90. Suzanne L Pollard, D’Ann L Williams, Patrick N Breysse, Patrick A Baron, Laura M Grajeda, Gilman RH. A cross-sectional study of determinants of indoor environmental exposures in households with and without chronic exposure to biomass fuel smoke. Environmental Health ,. 2014;13:21. 91. Roehr B. Environmentalists seek to set research agenda on indoor air pollution BMJ 2011;d 3062:342. 92. S.K. Jindal DG. The relationship between tobacco smoke & bronchial asthma. Indian J Med Res November 2004;120, :443-53. 93. P M Sturdy CRV, H R Anderson, J M Bland, B K Butland, B D W Harrison, C Peckitt, J C Taylor. Psychological, social and health behaviour risk factors for deaths certified as asthma: a national case-control study. Thorax 2002;;57::1034–9. 94. Simone Accordini LC, Ane Johannessen, Laura Portas, Bryndis Benediktsd ottir,Randi Jacobsen Bertelsenet.al A three-generation study on the association of tobacco smoking with asthma. International Journal of Epidemiology. 2018:1106–17. 95. Harriet Mpairwe MN, Gyaviira Nkurunungi, Pius Tumwesige, Irene Nambuya, Mike Mukasa, Caroline Onen, Marble Nnaluwooza. Risk factors for asthma among schoolchildren who participated in a case- control study in urban Uganda. eLife 2019;8(49496.). 96. Kristin Wickens JC, Trudi Kemp, Simon Lewis, Wendyl D’Souza, Gillian Sawyer, Louise Stone, Sarah Tohill, Jo Kennedy, Tania Slater, Natalie Rains. A case-control study of risk factors for asthma in New Zealand children. AUSTRALIAN AND NEW ZEALAND JOURNAL OF PUBLIC HEALTH. 2001;25:1. 97. Lisa A. Croen JKG, Cathleen K. Yoshida, Roxana Odouli, Judy Van de Water,. Maternal Autoimmune Diseases, Asthma and Allergies, and Childhood Autism Spectrum Disorders. Arch Pediatr Adolesc Med 2005;159::151-7.

64
ANNEXES
Annex 1- Information sheet (English version)
Background
Good morning / good afternoon
My name is __________________i am data collector for master of public health student project
in Addis Ababa University. We are conducting a research about “Assessment of the role of
household fuel exposure and housing characteristics on asthma in selected public hospitals of
Addis Ababa, Ethiopia; unmatched Case control study design.” Respiratory disease is the
commonest public health burden across the globe. Among them asthma is a widely spread
chronic condition. Today more than 200 million people worldwide are experiencing asthmatic
attack resulting in more than 0.18 million people death per year. A worldwide prevalence study
on asthma and allergies indicates that prevalence rate in Ethiopia 9.1%.Among the top 50 cause
of death in Ethiopia asthma is 24th
by the 11.98 age standardized death rate per 100,000
population. It imposes a global burden of impaired quality of life and health care costs.
Individual susceptibility to asthma is likely to be determined by interacting heritable and
environmental risk factors. Studies that have been investigated on this area suppose
environmental exposure have generated inconsistent and inconclusive finding. This study is
designed to fill the gap on the investigation of indoor cooking, housing characteristics and pet
ownership association with asthma among women. This study will examine the relationship
between housing characteristics and indoor cooking on asthma at public hospitals in Addis
Ababa, Ethiopia. The information I collect will help in implementing possible and important
intervention and to plan better supportive care provision system for patients. Now you are chosen
by chance to participate for the survey. The benefits, procedure and what is expected from you
will be explained in the following sections.
Objective
Aim of the study is to investigate whether household fuel exposure and housing characteristics
are associated with asthma or not at public hospitals in Addis Ababa, Ethiopia.
65
Study procedures
The study involves a face-to-face interview. You will be asked set of questions using a
structured questionnaire. After signing the consent form, you will then be asked relevant
questions and your responses will be written on the questionnaire. The interview will take
about 20 minutes.
Benefit of the study
The study will have important value to determine the association between selected factors (i.e.
housing characteristics and indoor cooking) and asthma and also it has contribution to take
appropriate intervention towards the establishment of prevention and control strategy of asthma.
There will not be any incentives that will be given. But when you participate in this study you
will have long and short term benefits. The long term benefit would be, the result of the study
will be useful to expand and implement a good health control and prevention method towards
asthma and your response will be used as baseline data to develop and implement new strategies.
This could be very beneficiary for the patients and also for the overall community.
Harm/risks of the study
You might feel discomfort able talking about your personal information and part of your time
(average of 20 minutes) will be consumed to answer the questions.
Rights of Participants
You have full right either to participate or refuse as well as to quit at the middle or at any time
you want after you start participation in this study. You may respond to all the questions or you
may not answer questions you don’t want to answer. You can ask any question which is not clear
for you.
Protection of privacy during data collection and analysis
Any data with personal information will be handled with confidentiality, and the privacy of
subjects respected at all stages of the project. Respondents' privacy will be respected through the
66
informed consent process and the procedures during the data collection. Personal identifiers
(including name) will not be recorded. Primary data will be handled only by the researchers, and
the database will be password protected. During data analysis, again data will be stored through a
password protected system and data is analyzed using codes, without personal identifiers.
Data Sharing:
During the study only the study PIs will have access to the study data including consent
documents. If you have any question about all things I explained to you now please forward it
before we procced to the next step?
Are you willing to participate in the study?
1- Yes (take informed consent)
2- No I don’t want to participate in the study (Thank you)
If you want to ask the principal investigator about the research at any time, you can contact
through:
Email: [email protected]
phone number: +251 944162181
If you want to ask the primary advisor about the research at any time, you can contact through:
Email : [email protected]
Phone number: +251911684399
If you want to ask the co-advisor about the research at any time, you can contact through:
Email : [email protected]
Phone number: +251911404954

67
Annex 2- Informed consent (English version)
Centre Number: :______________
Subject identification Number for this trial:___________
I agree to take part in the above study by considering the following statement.
1. I confirm that I have received and understand the information sheet detail for the above
study and have had the opportunity to ask question.
2. I understand that my participation is voluntary and that I am free to withdraw at any time,
without giving any reason, without my medical care or legal rights being affected.
3. I understand that the information I give may be looked at by responsible individuals from
the research team or from regulatory authorities where it is relevant.
What does your signature on this consent form mean?
Your signature on this form means:
You have been informed about this study’s purpose, procedures, and possible benefits.
You have been given the chance to ask questions before you sign.
You have voluntarily agreed to be in this study.
Signature of the Participant _________________
Name of the interviwer __________________ Signature______________
Date of interview ________________

68
Annex 3- Screening questionnaire for control (English version)
1. Have you had wheezing or whistling in your chest at any time in the last 12 months?
A. No
B. Yes
2. Have you woken up with a feeling of tightness in your chest at any time in the last 12
months?
A. No
B. Yes
3. Have you had an attack of shortness of breath that came on during the day when you
were at rest or following strenuous activity at any time in the last 12 months?
A. No
B. Yes
4. Have you been woken by an attack of coughing at any time in the last 12 months?
A. No
B. Yes

69
Annex 4- Survey questionnaire (English version)
Thank you for your willingness to participate, you were selected by a scientific sampling
procedure, and your cooperation is very important to the success of the study. This is a
questionnaire you are asked to answer, please answer the questions as frankly and accurately as
possible. All information obtained in the study will be kept confidential and used for public
health research only.
"Assessment of the role of indoor fuel exposure and housing characteristics on asthma in
selected public hospitals of Addis Ababa, Ethiopia"
Center _________________________________
Card number ____________________________
Code __________________________________
Address ________________________________
Telephone number ________________________
Date ____________________________________
PART I: Demographic and socioeconomic characteristics
SN Question Option Skip
pattern
101 How old are you? ______ years
102 Where do you live? A. Rural
B. Urban
103 sex? A. Male
B. Female
104 What is your marital status? A. Single
B. Married
C. Widowed
D. Separated /divorced
105 What is your educational status? A. Unable to read and write
B. Primary (1-8)
C. Secondary (9-10)
D. Preparatory (11-12)
E. Diploma and above
106 What is your occupational status? A. Unemployed
B. Employed (government, private,
self )
C. Retired
D. Student
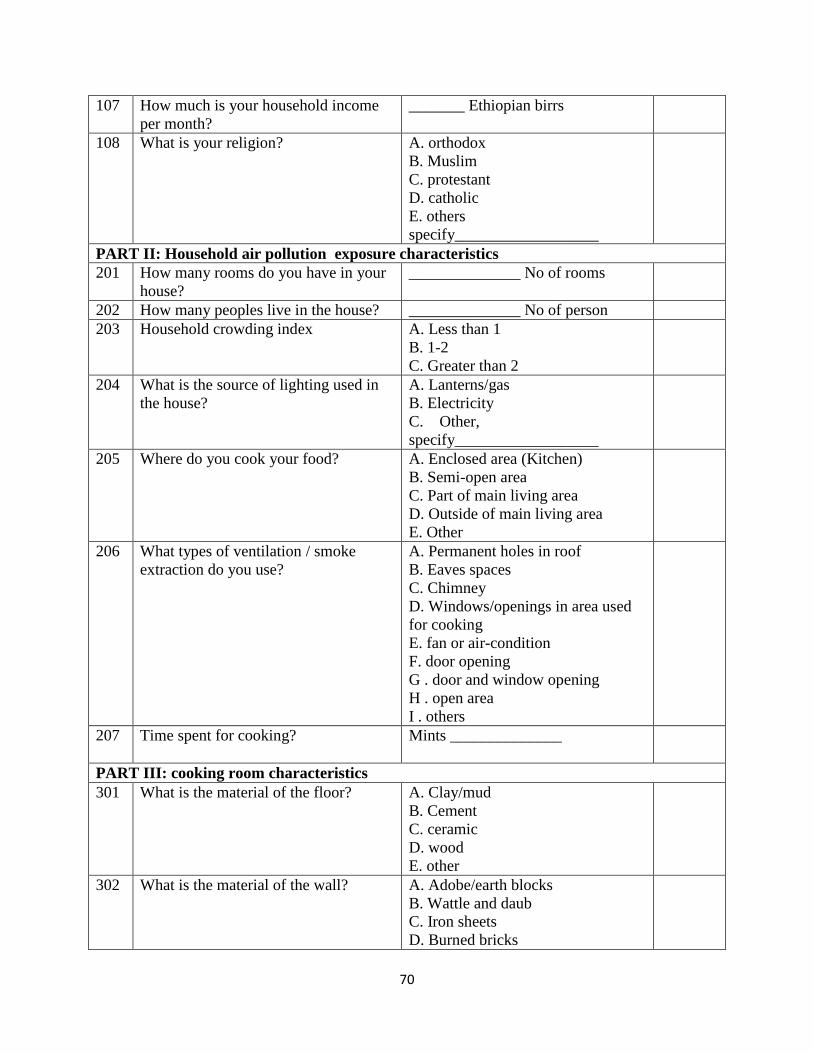
70
107 How much is your household income
per month?
_______ Ethiopian birrs
108 What is your religion? A. orthodox
B. Muslim
C. protestant
D. catholic
E. others
specify__________________
PART II: Household air pollution exposure characteristics
201 How many rooms do you have in your
house?
______________ No of rooms
202 How many peoples live in the house? ______________ No of person
203 Household crowding index A. Less than 1
B. 1-2
C. Greater than 2
204 What is the source of lighting used in
the house?
A. Lanterns/gas
B. Electricity
C. Other,
specify__________________
205 Where do you cook your food? A. Enclosed area (Kitchen)
B. Semi-open area
C. Part of main living area
D. Outside of main living area
E. Other
206 What types of ventilation / smoke
extraction do you use?
A. Permanent holes in roof
B. Eaves spaces
C. Chimney
D. Windows/openings in area used
for cooking
E. fan or air-condition
F. door opening
G . door and window opening
H . open area
I . others
207 Time spent for cooking? Mints ______________
PART III: cooking room characteristics
301 What is the material of the floor? A. Clay/mud
B. Cement
C. ceramic
D. wood
E. other
302 What is the material of the wall? A. Adobe/earth blocks
B. Wattle and daub
C. Iron sheets
D. Burned bricks
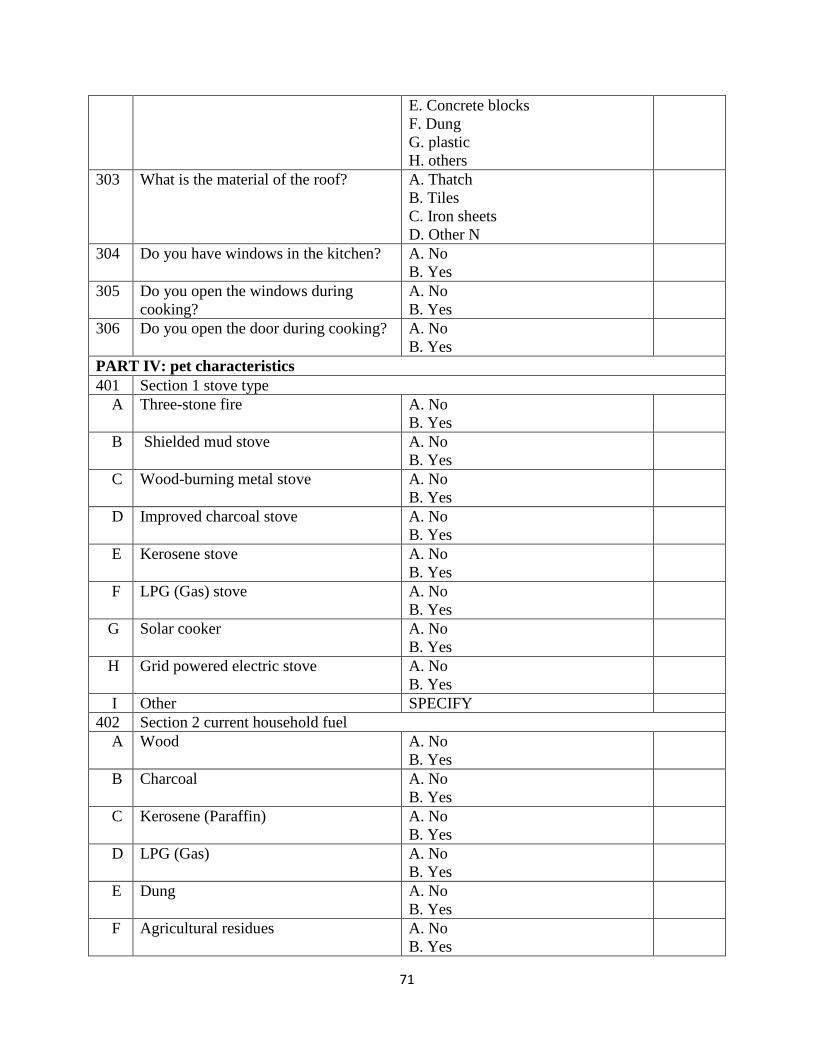
71
E. Concrete blocks
F. Dung
G. plastic
H. others
303 What is the material of the roof? A. Thatch
B. Tiles
C. Iron sheets
D. Other N
304 Do you have windows in the kitchen? A. No
B. Yes
305 Do you open the windows during
cooking?
A. No
B. Yes
306 Do you open the door during cooking? A. No
B. Yes
PART IV: pet characteristics
401 Section 1 stove type
A Three-stone fire A. No
B. Yes
B Shielded mud stove A. No
B. Yes
C Wood-burning metal stove A. No
B. Yes
D Improved charcoal stove A. No
B. Yes
E Kerosene stove A. No
B. Yes
F LPG (Gas) stove A. No
B. Yes
G Solar cooker A. No
B. Yes
H Grid powered electric stove A. No
B. Yes
I Other SPECIFY
402 Section 2 current household fuel
A Wood A. No
B. Yes
B Charcoal A. No
B. Yes
C Kerosene (Paraffin) A. No
B. Yes
D LPG (Gas) A. No
B. Yes
E Dung A. No
B. Yes
F Agricultural residues A. No
B. Yes

72
G Solar A. No
B. Yes
H Grid electricity A. No
B. Yes
I Batteries A. No
B. Yes
J Wax candle A. No
B. Yes
K Other SPECIFY
403 Section 3 life time household fuel
A Wood A. No
B. Yes
B Charcoal A. No
B. Yes
C Kerosene (Paraffin) A. No
B. Yes
D LPG (Gas) A. No
B. Yes
E Dung A. No
B. Yes
F Agricultural residues A. No
B. Yes
G Solar A. No
B. Yes
H Grid electricity A. No
B. Yes
I Batteries A. No
B. Yes
J Wax candle A. No
B. Yes
K Other SPECIFY
PART V: pet characteristics
501 Do you keep a pet? A. No
B. Yes
If' No`,
go to
601
502 if 'Yes' which one? A. Cat
B. Dog
C. Bird
D. Cat and dog
E. Dog and bird
F. Cat and bird
G. Cat, dog and bird
H. If other
503 Do pets have contact with inhabitants? A. No
B. Yes
If' No`
skip 601
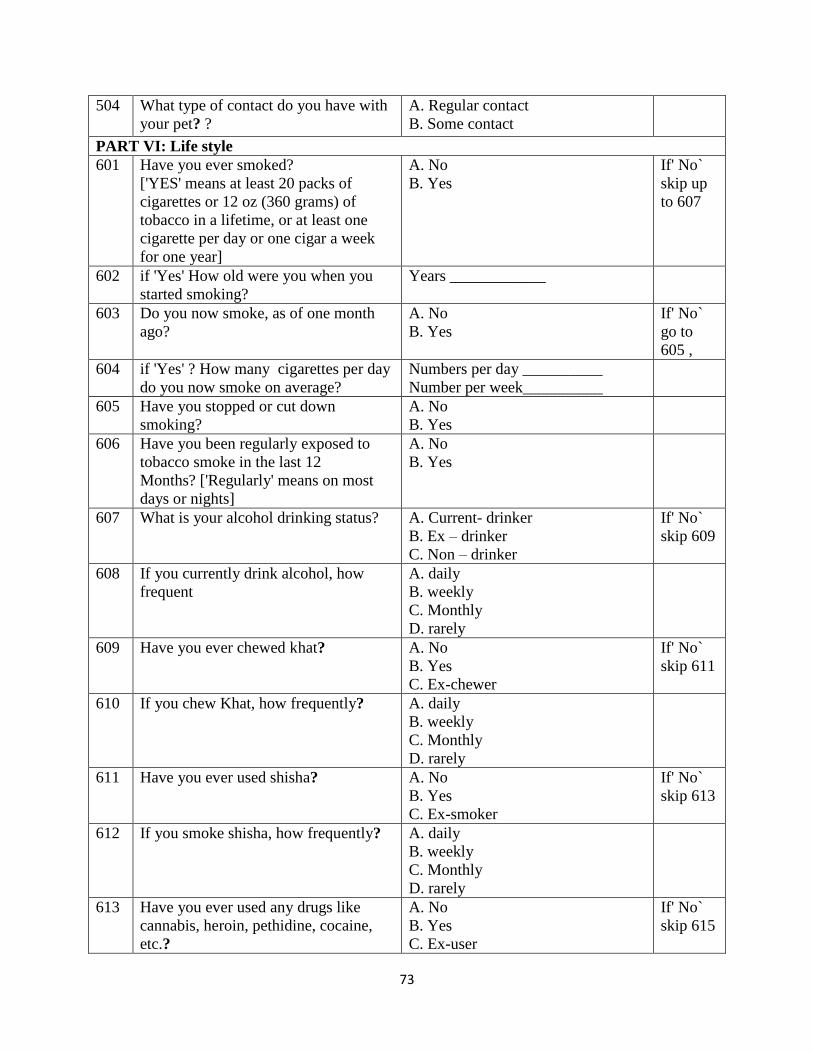
73
504 What type of contact do you have with
your pet? ?
A. Regular contact
B. Some contact
PART VI: Life style
601 Have you ever smoked?
['YES' means at least 20 packs of
cigarettes or 12 oz (360 grams) of
tobacco in a lifetime, or at least one
cigarette per day or one cigar a week
for one year]
A. No
B. Yes
If' No`
skip up
to 607
602 if 'Yes' How old were you when you
started smoking?
Years ____________
603 Do you now smoke, as of one month
ago?
A. No
B. Yes
If' No`
go to
605 ,
604 if 'Yes' ? How many cigarettes per day
do you now smoke on average?
Numbers per day __________
Number per week__________
605 Have you stopped or cut down
smoking?
A. No
B. Yes
606 Have you been regularly exposed to
tobacco smoke in the last 12
Months? ['Regularly' means on most
days or nights]
A. No
B. Yes
607 What is your alcohol drinking status? A. Current- drinker
B. Ex – drinker
C. Non – drinker
If' No`
skip 609
608 If you currently drink alcohol, how
frequent
A. daily
B. weekly
C. Monthly
D. rarely
609 Have you ever chewed khat? A. No
B. Yes
C. Ex-chewer
If' No`
skip 611
610 If you chew Khat, how frequently? A. daily
B. weekly
C. Monthly
D. rarely
611 Have you ever used shisha? A. No
B. Yes
C. Ex-smoker
If' No`
skip 613
612 If you smoke shisha, how frequently? A. daily
B. weekly
C. Monthly
D. rarely
613 Have you ever used any drugs like
cannabis, heroin, pethidine, cocaine,
etc.?
A. No
B. Yes
C. Ex-user
If' No`
skip 615
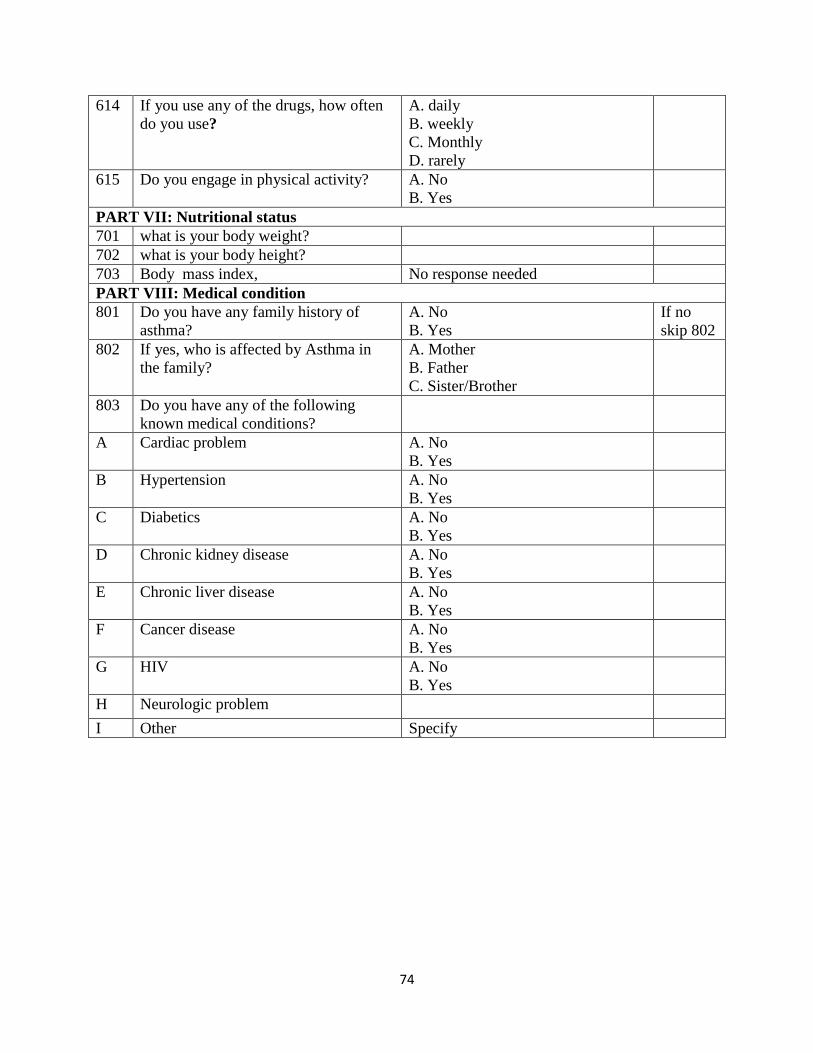
74
614 If you use any of the drugs, how often
do you use?
A. daily
B. weekly
C. Monthly
D. rarely
615 Do you engage in physical activity? A. No
B. Yes
PART VII: Nutritional status
701 what is your body weight?
702 what is your body height?
703 Body mass index, No response needed
PART VIII: Medical condition
801 Do you have any family history of
asthma?
A. No
B. Yes
If no
skip 802
802 If yes, who is affected by Asthma in
the family?
A. Mother
B. Father
C. Sister/Brother
803 Do you have any of the following
known medical conditions?
A Cardiac problem A. No
B. Yes
B Hypertension A. No
B. Yes
C Diabetics A. No
B. Yes
D Chronic kidney disease A. No
B. Yes
E Chronic liver disease A. No
B. Yes
F Cancer disease A. No
B. Yes
G HIV A. No
B. Yes
H Neurologic problem
I Other Specify
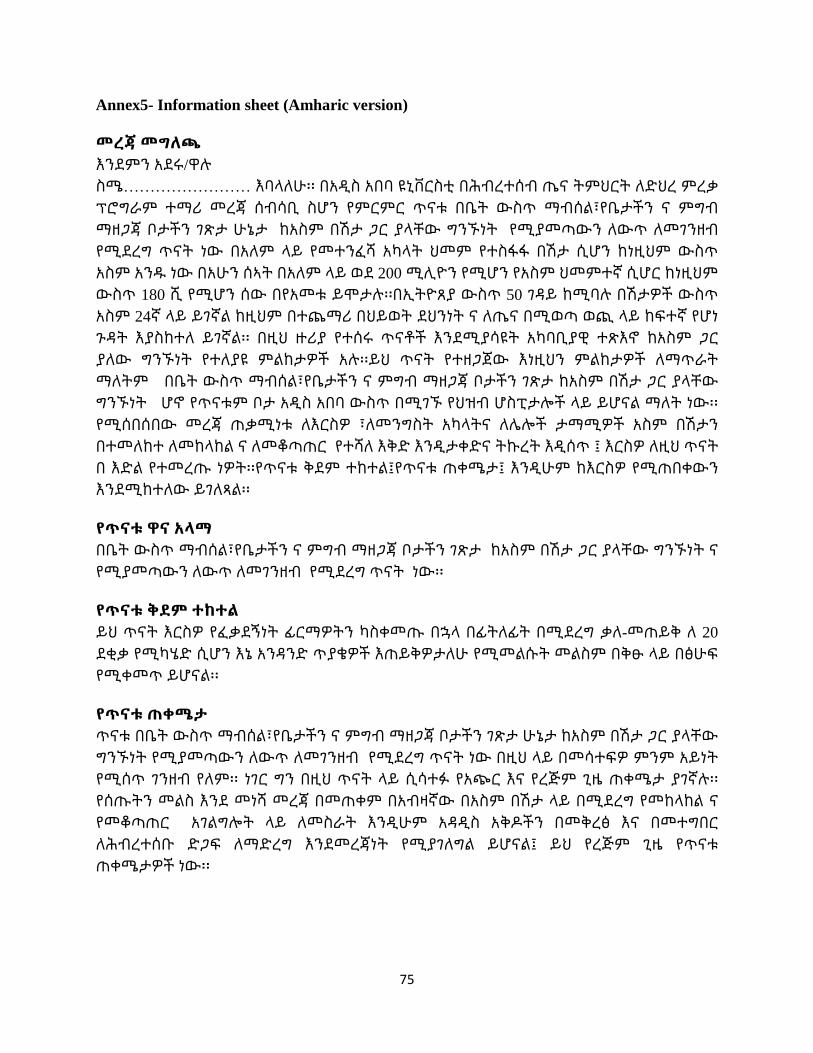
75
Annex5- Information sheet (Amharic version)
መረጃ መግለጫ
እንደምን አደሩ/ዋሉ
ስሜ…………………… እባላለሁ፡፡ በአዲስ አበባ ዩኒቨርስቲ በሕብረተሰብ ጤና ትምህርት ለድህረ ምረቃ
ፕሮግራም ተማሪ መረጃ ሰብሳቢ ስሆን የምርምር ጥናቱ በቤት ውስጥ ማብሰል፣የቤታችን ና ምግብ
ማዘጋጃ ቦታችን ገጽታ ሁኔታ ከአስም በሽታ ጋር ያላቸው ግንኙነት የሚያመጣውን ለውጥ ለመገንዘብ
የሚደረግ ጥናት ነው በአለም ላይ የመተንፈሻ አካላት ህመም የተስፋፋ በሽታ ሲሆን ከነዚህም ውስጥ
አስም አንዱ ነው በአሁን ሰኣት በአለም ላይ ወደ 200 ሚሊዮን የሚሆን የአስም ህመምተኛ ሲሆር ከነዚህም
ውስጥ 180 ሺ የሚሆን ሰው በየአመቱ ይሞታሉ፡፡በኢትዮጸያ ውስጥ 50 ገዳይ ከሚባሉ በሽታዎች ውስጥ
አስም 24ኛ ላይ ይገኛል ከዚህም በተጨማሪ በህይወት ደህንነት ና ለጤና በሚወጣ ወጪ ላይ ከፍተኛ የሆነ
ጉዳት እያስከተለ ይገኛል፡፡ በዚህ ዙሪያ የተሰሩ ጥናቶች እንደሚያሳዩት አካባቢያዊ ተጽእኖ ከአስም ጋር
ያለው ግንኙነት የተለያዩ ምልከታዎች አሉ፡፡ይህ ጥናት የተዘጋጀው እነዚህን ምልከታዎች ለማጥራት
ማለትም በቤት ውስጥ ማብሰል፣የቤታችን ና ምግብ ማዘጋጃ ቦታችን ገጽታ ከአስም በሽታ ጋር ያላቸው
ግንኙነት ሆኖ የጥናቱም ቦታ አዲስ አበባ ውስጥ በሚገኙ የህዝብ ሆስፒታሎች ላይ ይሆናል ማለት ነው፡፡
የሚሰበሰበው መረጃ ጠቃሚነቱ ለእርስዎ ፣ለመንግስት አካላትና ለሌሎች ታማሚዎች አስም በሽታን
በተመለከተ ለመከላከል ና ለመቆጣጠር የተሻለ እቅድ እንዲታቀድና ትኩረት እዲሰጥ ፤ እርስዎ ለዚህ ጥናት
በ እድል የተመረጡ ነዎት፡፡የጥናቱ ቅደም ተከተል፤የጥናቱ ጠቀሜታ፤ እንዲሁም ከእርስዎ የሚጠበቀውን
እንደሚከተለው ይገለጻል፡፡
የጥናቱ ዋና አላማ
በቤት ውስጥ ማብሰል፣የቤታችን ና ምግብ ማዘጋጃ ቦታችን ገጽታ ከአስም በሽታ ጋር ያላቸው ግንኙነት ና
የሚያመጣውን ለውጥ ለመገንዘብ የሚደረግ ጥናት ነው፡፡
የጥናቱ ቅደም ተከተል
ይህ ጥናት እርስዎ የፈቃደኝነት ፊርማዎትን ካስቀመጡ በኋላ በፊትለፊት በሚደረግ ቃለ-መጠይቅ ለ 20
ደቂቃ የሚካሄድ ሲሆን እኔ አንዳንድ ጥያቄዎች እጠይቅዎታለሁ የሚመልሱት መልስም በቅፁ ላይ በፅሁፍ
የሚቀመጥ ይሆናል፡፡
የጥናቱ ጠቀሜታ
ጥናቱ በቤት ውስጥ ማብሰል፣የቤታችን ና ምግብ ማዘጋጃ ቦታችን ገጽታ ሁኔታ ከአስም በሽታ ጋር ያላቸው
ግንኙነት የሚያመጣውን ለውጥ ለመገንዘብ የሚደረግ ጥናት ነው በዚህ ላይ በመሳተፍዎ ምንም አይነት
የሚሰጥ ገንዘብ የለም፡፡ ነገር ግን በዚህ ጥናት ላይ ሲሳተፉ የአጭር እና የረጅም ጊዜ ጠቀሜታ ያገኛሉ፡፡
የሰጡትን መልስ እንደ መነሻ መረጃ በመጠቀም በአብዛኛው በአስም በሽታ ላይ በሚደረግ የመከላከል ና
የመቆጣጠር አገልግሎት ላይ ለመስራት እንዲሁም አዳዲስ አቅዶችን በመቅረፅ እና በመተግበር
ለሕብረተሰቡ ድጋፍ ለማድረግ እንደመረጃነት የሚያገለግል ይሆናል፤ ይህ የረጅም ጊዜ የጥናቱ
ጠቀሜታዎች ነው፡፡

76
የጥናቱጉዳቶች
የሰአትዎን በአማካኝ 20 ደቂቃ በጥናቱ ላይ ያሳልፋሉ፡፡ እንዲሁም ስለ ግል ህይወትዮ በሚወሩበት ሰአት
ምናልባት የመረበሽ ስሜት ሊኖርዎት ይችላል፡፡
የተሳታፊዎች መብት
በጥናቱ ላይ የመሳተፍም ሆነ ያለመሳተፍ ሙሉ መብት አልዎት፣ ጥናቱ ውስጥ ተሳታፊ ሆነው ቢሆን
እንኳን አቋርጦ መውጣት ይችላሉ ፣ ሁሉንም ጥያቄዎች መመለስ አሊያም አለመመለስ ይችላሉ ፡፡
ያልገባዎትን ማንኛውንም ጥያቄ መጠየቅ ይችላሉ፡፡
ሚስጥር ጠባቂነት በመረጃ አሰባሰብ እና ትንተና ወቅት
ከዝህ ጥናት የሚሰበሰበው መረጃ በጥናቱ አጥኚ የሚያዝ ሲሆን መረጃውም በ ሚስጥር ቁጥር የሚዘጋ
ይሆናል፡፡ የግለሰቦች መግለጫ (ስም) አይመዘገብም በተመሳሳይ ጥናቱ ባለቀ ወቅትም የግለሰቦች
ማንነት(ስም) በሪፖርት ላይ ማይገለጽና ማጠቃለያ ጽሁፉም በሚስጥር ቁጥር የሚዘጋ ይሆናል፡፡
መረጃ ክፍፍል
በጥናቱ ወቅት የተሰበሰበው መረጃ የጥናቱ ባለቤት ብቻ ይኖርዋል፡፡ ይህ የፈቃደኝነት መግለጫውንም
ያካትታል፡፡ እባክዎ ከላይ ስለተዘረዘረው ነገር ወደቀጣዩ ክፍል ሳንገባ ማንኛውም ጥያቄ ካልዎት?
በጥናቱ ለመሳተፍ ፈቃደኛ ነዎት ?
1- አዎ (በመረጃ ለይ የተደገፈ የፍቃደኝነት ቅጽ ይውሰዱ)
2- በጥናቱ ለመሳተፍ ፈቃደኛ ካልሆኑ (እናመሰግናለን)
ጥናቱን በተመለከተ ሊብራራልዎት የሚፈልጉት ነገር ካለ መጠየቅ ይችላሉ። ለበለጠ መረጃ የጥናቱን ዋና
አጥኚበሚከተለዉ አድራሻ ማግኝት ይችላሉ።
እሜል፡ [email protected] ወይም
ሞባይል ስልክ ቁጥር +251 944162181.
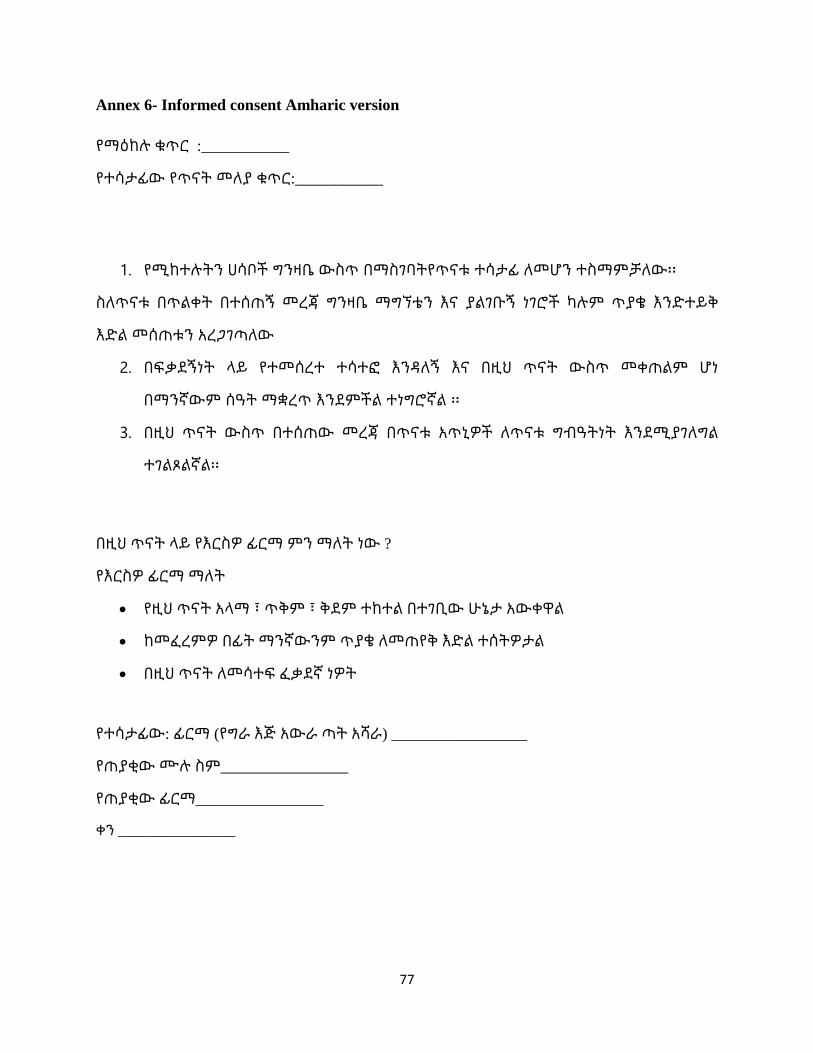
77
Annex 6- Informed consent Amharic version
የማዕከሉ ቁጥር :___________
የተሳታፊው የጥናት መለያ ቁጥር:___________
1. የሚከተሉትን ሀሳቦች ግንዛቤ ውስጥ በማስገባትየጥናቱ ተሳታፊ ለመሆን ተስማምቻለው፡፡
ስለጥናቱ በጥልቀት በተሰጠኝ መረጃ ግንዛቤ ማግኘቴን እና ያልገቡኝ ነገሮች ካሉም ጥያቄ እንድተይቅ
እድል መሰጠቱን አረጋገጣለው
2. በፍቃደኝነት ላይ የተመሰረተ ተሳተፎ እንዳለኝ እና በዚህ ጥናት ውስጥ መቀጠልም ሆነ
በማንኛውም ሰዓት ማቋረጥ እንደምችል ተነግሮኛል ፡፡
3. በዚህ ጥናት ውስጥ በተሰጠው መረጃ በጥናቱ አጥኒዎች ለጥናቱ ግብዓትነት እንደሚያገለግል
ተገልጾልኛል፡፡
በዚህ ጥናት ላይ የእርስዎ ፊርማ ምን ማለት ነው ?
የእርስዎ ፊርማ ማለት
የዚህ ጥናት አላማ ፣ ጥቅም ፣ ቅደም ተከተል በተገቢው ሁኔታ አውቀዋል
ከመፈረምዎ በፊት ማንኛውንም ጥያቄ ለመጠየቅ እድል ተሰትዎታል
በዚህ ጥናት ለመሳተፍ ፈቃደኛ ነዎት
የተሳታፊው: ፊርማ (የግራ እጅ አውራ ጣት አሻራ) _________________
የጠያቂው ሙሉ ስም________________
የጠያቂው ፊርማ________________
ቀን ________________

78
Annex 7- Screening questionnaire for control (Amharic version)
ጥ1. ባለፉት 12 ወራት የማፉጨት ወይም የማንኮራፋት አይነት ድምጽ በደረት አካባቢ ሰምተው
ያውቃሉ?
A. አይ አላቅም
B. አዎ አቃለው
ጥ2.ባለፉት 12 ወራት በማንኛውም ሰዓት ከእንቅልፍ ሲነቁ ደረት አካባቢ የህመም ስሜት ይሰማዎታል?
A. አይ አይሰማኝም
B. አዎ ይሰማኛል
ጥ3. ባለፉት 12 ወራት በማንኛውም ሰዓት የሰውነት እንቅስቃሴ ካደረጉ በኃላ ወይም አረፍ ብለው ሳለ
ትንፋሽ አጥሮት ያውቃል?
A. አይ አያቅም
B. አዎ ያውቃል
ጥ4. ባለፉት 12 ወራት በማንኛውም ሰዓት በሳል ምክንያት ከእንቅልፍ ነቅተው ያውቃሉ?
A. አይ አላቅም
B. አዎ አቃለው

79
Annex 8 - Survey questionnaire (Amharic version)
በቅድሚያ ይህን መጠይቅ ለመመለስ ፈቃደኛ ስለሆኑ እናመሰግናለን በዚህ ጥናት ላይ ለመሳተፍ እርስዎ
የተመረጡት በሳይንሳዊ ዘዴ ነው በመሆኑም የእርሶ ትብብር ለጥናቱ ውጤታማነት አስፈላጊ ነው፡፡ በዚህ
መጠይቅ ላይ የሚሞሉት መረጃ ሚስጥራዊነቱ የተጠበቀ መሆኑን ና አገልግሎቱም ለጥናቱ ብቻ መሆኑን
እየገለጽን ጥያቄዎቹን በታማኝነት ና በሀቀኝነት እንዲመልሱ እንጠይቃለን፡፡
ማእከል ________________________________________
የካርድ ቁጥር _____________________________
መለያ ቁጥር _____________________________
አድራሻ _________________________________
ስልክ ቁጥር ______________________________
ቀን __________________________________
ክፍል 1፡ ህዝበ-ነክ፣ማህበራዊና እኮኖሚያዊ ሁኔታ
ቁ ጥያቄ ምርጫ እለፍ 101 ስንት አመትህ/ሽ ነው? ______ አመት
102 የት ነው የምትኖረው/ሪው? ሀ. ገጠር
ለ. ከተማ
103 ጾታህ/ሽ ምንድነው? ሀ. ወንድ
ለ. ሴት
104 የሚገኙበት የጋብቻ ሁኔታ? ሀ. ያላገባ
ለ. ያገባ
ሐ. የሞተበት / የሞተችበት
መ.የፈታ / የፈታች
105 የሚገኙበት የትምህርት ሁኔታ? ሀ. መጻፍ ና ማንበብ የማይችል
ለ. የመጀመሪያ ደረጃ ትምህርት
ሐ. ሁለተኛ ደረጃ ትምህርት
መ. መሰናዶ ትምህርት
ሠ.ዲፕሎማ ና ከዛበላይ
106 የሚገኙበት የስራ ሁኔታ? ሀ. ስራ የሌለው
ለ. ስራ ያለው (የመንግስት፣ የግል፣የራስ)
ሐ. ጡረታ የወጣ
መ. ተማሪ
107 ምን ያህል የወር ገቢ አላቹ? _______ ብር
108 እምነትህ/ሽ ምንድና? ሀ.ኦርቶዶክስ
ለ. ሙስሊም
ሐ ፕሮቴስታንት
መ. ካቶሊክ
ሠ. ሌላ ካለ
ይግለጹ__________________
80
ክፍል 2: የመኖሪያ ቤቱ የቤት ውስጥ ጭስ ሁኔታ
201 በቤት ውስጥ ስንት ክፍል አለ? ______________ ክፍል በቁጥር
202 በቤት ውስጥ ምን ያህል ሰው ይኖራል? ______________ ሰው በቁጥር
203 አማካኝ ምን ያህል ሰው በአንድ ክፍል ውስጥ
ይኖራል?
ሀ. ከ አንድ በታች
ለ. ከአንድ -ሁለት
ሐ. ከሁለት በላይ
204 በቤት ውስጥ ለመብራትነት
የምትጠቀሙበት የሀይል ምንጭ?
ሀ. ፋኖስ / ጋዝ
ለ. ኤሌክትሪክ
ሐ..ሌሎች ይግለጹ__________________
205 ምግብ የምታበስሉት የት ነው? ሀ. ከዋናው ክፍል ጋር ያልተገናኘ ማብሰያ
ውስጥ (ኩሽና)
ለ. በከፊል ክፍት የሆነ ቦታላይ
ሐ. መኖሪያ ቤት ውስጥ
መ. ከመኖሪያ ቤት ውጪ
ሠ. ሌላ ካለ፣ይግለጹ
ኩሽናን
ከመረጣቹ(If
ከ306-3011
ስለዚ ኩሽና
ይሆናል)
206 ምን አይነት የማናፈሻ ስርዓት ትጠቀማላቹ? ሀ. ጣሪያውን በመቅደድ ክፍተት
በመፍጠር
ለ. ከጣሪያው በታች ግንቡን በመብሳት
ክፍተት በመፍጠር
ሐ. ጭስ ማውጫ በመጠቀም
መ. በምናበስልበት ሰዓት መስኮት
በመክፈት
ሠ. አየር ማቀዝቀዢያ በመጠቀም
ረ. ሌላ ካለ ፣ይገለጹ
207 ምግብ ለማብሰል ምን ይህል ሰአት
ታሳልፋላቹ?
ደቂቃ ______________
ክፍል 3: የማብሰያ ክፍሉ ገዕታ ሁኔታ
301 ወለሉ የተሰራው ከምንድነው? ሀ. ሸክላ አፈር / ጭቃ
ለ. ሲሚንቶ / ሴራሚክ
ሐ. ሌላ ካለ፣ይግለጹ
302 ግድግዳው የተሰራው ከምንድነው? ሀ. ከጡብ
ለ. ከጭቃ ወይም ሸክላ
ሐ. ቆርቆሮ
መ. ብሎኬት
ሠ. ኮንክሪት
ረ. ፍግ
ሰ. ሌላ ካለ፣ይግለጹ
303 ጣሪያው የተሰራው ከምንድነው? ሀ. ከሳር
ለ. ከፕላስቲክ
ሐ. ከቆርቆሮ
መ.ሌላ ካለ፣ይግለጹ
304 ኩሽናው መስኮት አለው? ሀ. አይ
81
ለ. አዎ
305 ምግብ በምታዘጋጁ ግዜ መስኮት ይከፈታል? ሀ. አይ
ለ. አዎ
306 ምግብ በምታዘጋጁ ግዜ በር ይከፈታል? ሀ. አይ
ለ. አዎ
ክፍል 4 ፤: የጭስ ተጋላጭነትን በተመለከተ
401 1 - ምን አይነት የማብሰያ ምድጃ ነው ያላቹ?
ሀ. ባለ ሶስት ጉልቻ ምድጃ ሀ. አይ
ለ. አዎ
ለ ዙሪያውን በጭቃ የተለሰነ ምድጃ ሀ. አይ
ለ. አዎ
ሐ አንጨት በማንደድ የሚሰራ የብረት ምድጃ ሀ. አይ
ለ. አዎ
መ የተሻሻለው የከሰል ምድጃ ሀ. አይ
ለ. አዎ
ሠ. ቡታ ጋዝ ምድጃ ሀ. አይ
ለ. አዎ
ረ. ቤንዚን ምድጃ
ሀ. አይ
ለ. አዎ
ሰ. በጸሀይ በርሃን የሚሰራ ምድጃ ሀ. አይ
ለ. አዎ
ሸ. በኤሌክትሪክ የሚሰራ ምድጃ በኤሌክትሪክ የሚሰራ ምድጃ
ቀ. ሌላ ካለ፣ ይግለጹ_
402 2- በአሁን ሰዓትለምግብ ማብሰያነት በመጀመሪያ ደረጃ የምትጠቀሙበት የነዳጅ አይነት
ሀ. እንጨት ሀ. አይ
ለ. አዎ
ለ ከሰል ሀ. አይ
ለ. አዎ
ሐ ነጭ ጋዝ ሀ. አይ
ለ. አዎ
መ ቤንዚን ሀ. አይ
ለ. አዎ
ሠ. ፍግ ሀ. አይ
ለ. አዎ
ረ. ሰብለ-ቀር ሀ. አይ
ለ. አዎ
ሰ. የጸሀይ ብርሀን ሀይል ሀ. አይ
ለ. አዎ
ሸ. የኤሌክትሪክ ሀይል ሀ. አይ
ለ. አዎ
ቀ. ባትሪ ሀ. አይ
82
ለ. አዎ
በ. የሰም ሻማ ሀ. አይ
ለ. አዎ
ተ ሌላ ካለ፣_ ይግለጹ_
403 3- በህይወት ዘመንዎ ለምግብ ማብሰያነት በመጀመሪያ ደረጃ የምትጠቀሙበት የነዳጅ አይነት
ሀ. እንጨት ሀ. አይ
ለ. አዎ
ለ ከሰል ሀ. አይ
ለ. አዎ
ሐ ነጭ ጋዝ ሀ. አይ
ለ. አዎ
መ ቤንዚን ሀ. አይ
ለ. አዎ
ሠ. ፍግ ሀ. አይ
ለ. አዎ
ረ. ሰብለ-ቀር ሀ. አይ
ለ. አዎ
ሰ. የጸሀይ ብርሀን ሀይል ሀ. አይ
ለ. አዎ
ሸ. የኤሌክትሪክ ሀይል ሀ. አይ
ለ. አዎ
ቀ. ባትሪ ሀ. አይ
ለ. አዎ
በ. የሰም ሻማ ሀ. አይ
ለ. አዎ
ተ ሌላ ካለ፣_ ይግለጹ_
ክፍል 5 ፡ የቤት ውስጥ እንስሳ 501 በቤታችሁ ውስጥ ለማዳ እንስሳ አለ? ሀ. አይ
ለ. አዎ
አይ ካሉ ወደ
601 ይለፉ
502 'አዎ' ከሆነ ? የቱ? ሀ. ድመት
ለ. ውሻ
ሐ. ወፍ
መ. ድመት ና ውሻ
ሠ. ድመት ና ወፍ
ረ. ውሻ ና ወፍ
ሰ. ድመት፣ውሻ ና ወፍ
ሸ. ሌሎች
503 ከለማዳ እንስሳቶቹ ጋ ንክኪ አላችሁ? ሀ. አይ
ለ. አዎ
አይ ካሉ ወደ
601 ይለፉ
504 'አዎ' ከሆነ ለምን ያህል ግዜ? ሀ. ሁል ግዜ
ለ. አልፎ አልፎ
83
ክፍል 6፣ የአኗኗር ዘይቤ 601 በህይወት ዘመንህ/ሽ አጭሰህ/ሽ ታቃለህ/ሸ?
['አዎ' ማለት በያንስ 20 እሽግ ሲጃራ ወይም
(360 ግ.ም) የሚመዝን ቶባኮ በህይወት
ዘመን ወይም ቢያንስ አንድ ሲጃራ በቀን
ወይም አንድ ሰጃራ በሳምንት ለአመት ]
ሀ. አይ
ለ. አዎ
አይ ካሉ
607ን ይለፉ
602 ማጨስ ስትጀምር ስንት አመትህ/ሽ ነበር? እድሜ ____________
603 በአንድ ወር ገዜ ውስጥ አጭሰህ ታቃለህ/ሽ? ሀ. አይ
ለ. አዎ
604 በአማካኝ ምን ያህል ሲጃራ በቀን ያጨሳሉ? ቁጥር በቀን __________
ቁጥር በሳምንት__________
605 ሲጃራ ማጨስ አቁመህ ወይም ቀንሰህ
ታቃለህ/ሽ?
ሀ. አይ
ለ. አዎ
606 ላለፉት 12 ወራት ለትንባሆ ጭስ በየጊዜው
ተጋላጭ ሆነው ያውቃሉ ? ['በየጊዜው' ማለት
በአብዛኛው ቀን ና ማታ ማለት ነው ]
ሀ. አይ
ለ. አዎ
607 የአልኮል መጠጥ የመጠጣት ሁኔታ? ሀ. አሁንም እጠጣለው
ለ. በፊት እጠጣ ነበር
ሐ. ጠጥቼ አላቅም
አይ ካሉ
608ን ይለፉ
608 አሁን የሚጠጡ ከሆን መቼ መቼ? ሀ. በቀን
ለ. በሳምንት
ሐ. በወር
መ.አልፎ አልፎ
609 ጫት ቅመው ያውቃሉ? ሀ. አይ
ለ. አዎ
ሐ.በፊት
አይ ካሉ
610ን ይለፉ
610 አሁን የሚቅሙ ከሆን መቼ መቼ? ሀ. በቀን
ለ. በሳምንት
ሐ. በወር
መ.አልፎ አልፎ
611 ሺሻ አጭሰው ያውቃሉ? ሀ. አይ
ለ. አዎ
ሐ.በፊት
አይ ካሉ
612ን ይለፉ
612 አሁን የሚያጨሱ ከሆን መቼ መቼ? ሀ. በቀን
ለ. በሳምንት
ሐ. በወር
መ.አልፎ አልፎ
613 እንደ ካናቢስ፣ሄሮኢን፣ፔቲዲን፣ኮኬን
የመሳሰሉ መድሀኒቶችን ተጠቅመው
ያውቃሉ ?
ሀ. አይ
ለ. አዎ
ሐ.በፊት
አይ ካሉ
614ን ይለፉ
614 የሚጠቀሙ ከሆነ በምን ያህል ግዜ? ሀ. በቀን
ለ. በሳምንት
84
ሐ. በወር
መ.አልፎ አልፎ
615 የአካል ብቃት እንቅስቃሴ ታደርጋለህ? ሀ. አይ
ለ. አዎ
ክፍል 7፣ የሰውነት ሁኔታ 701 ክብደትህ/ሽ ስንት ነው?
702 ቁመትህ/ሽ ስንት ነው?
703 የሰውነት ክብደት ጠቋሚ ምላሽ አያስፈልገውም
ክፍል 8፣ የጤና ሁኔታ 801 በቤተሰብ ውስጥ አስም የሚያመው ሰው
አለ?
ሀ. አይ
ለ. አዎ
አይ ካሉ
803ን ይለፉ
802 አዎ ካላቹ ማን ነው የታመመው? ሀ. እናት
ለ. አባት
ሐ. እህት/ ወንድም
803 የሚከተሉት የህመም አይነቶች አሉባቸሁ?
ሀ. የልብ ህመም ሀ. አይ
ለ. አዎ
ለ ግፊት ሀ. አይ
ለ. አዎ
ሐ ስኳር ሀ. አይ
ለ. አዎ
መ ኩላሊት ሀ. አይ
ለ. አዎ
ሠ. ጉበት ሀ. አይ
ለ. አዎ
ረ. ካንሰር ሀ. አይ
ለ. አዎ
ሰ. ኤች አይ ቪ ሀ. አይ
ለ. አዎ
ሸ. የነርቨ ህመም ሀ. አይ
ለ. አዎ
ቀ. ሌላ ካለ ይግለጹ_
85
Annex 9: A manual for training data collectors and supervisors
ADDIS ABABA UNIVERSITY
COLLEGE OF HEALTH SCIENCE
SCHOOL OF PUBLIC HEALTH
Data collectors and supervisors training manual
Principal investigator – Yonas Abebe (Bsc)
Advisores- prof, Ahemed Ali (PhD)
Dr. Adamu Addissie (MD, PhD)
Dr, Tewodros Haile (MD, Pulmonologist)
February 2020
Addis Ababa, Ethiopia
86
Contents
1. Introduction
2. Objective
3. Method of the training
4. Training schedule
5. Equipment for data collection procedure
6. Payment
7. Responsibility for participants in the data collection process
A. Data collectors responsibility
B. Supervisor responsibility
8. Description for cases and controls
9. Description for questionnaire
10. Data collection procedure

87
1. Introduction
Asthma is a chronic inflammatory disorder characterized by airway obstruction and hyper
responsiveness. Studies have suggested that household fuel exposure; either biomass or
fossil fuel and housing characteristics have been associated with allergy. Recent analysis
has also shown an increase in asthma among residential determinants of allergy. But there
remains considerable uncertainty about whether this reflects an association with asthma.
2. Objective of the training
The main objective of this training is to provide basic information about the research and
data collection process basically how to select the study unit and interview participants
with the exact and appropriate way.
3. Method of the training
Participatory presentation
Group discussion
Practical training
4. Training schedule
Activity Time
1 Introduction 20 mint
2 Description for data collection procedure 40 mint
3 Description for cases and controls 40 mint
4 Description for questionnaire 20 mint
5. Equipment for data collection procedure
Information sheet
Informed consent
Questionnaire
Patient card
Pen
Pencil
Summary sheet

88
6. Payment
Data collectors and supervisors in the study have payment per questionnaire. The
payment is done after the data collection process is completed. The payment is
paid by the principal investigator.
7. Responsibility for participants in the data collection process
A. Data collectors responsibility
Before data collection process data collectors should take training.
Identify cases and controls based on selection criterias.
Informed consent should sign based on the informed information sheet.
Doing interview for study participants based on questionnaire.
Take basic information of the participant from system card or patient card.
B. Supervisor responsibility
Before data collection process supervisors should take training.
Help data collectors if needed.
Follow data collection process
Check completeness of the questionnaire and if there is a problem aware the data
collectors to solve it.
Provide materials for data collectors in order to perform the data collection
process.
8. Description for selection of cases and controls
Cases in this study took based on medical history, physical examination and pulmonary
function test
1. Medical history
Cough (worse at night)
Chest tightness
Wheezing
Difficulty breathing
2. Physical examination finding
Thoracic hyper expansion
Wheezing during normal breathing
Prolonged phase of forced exhalation
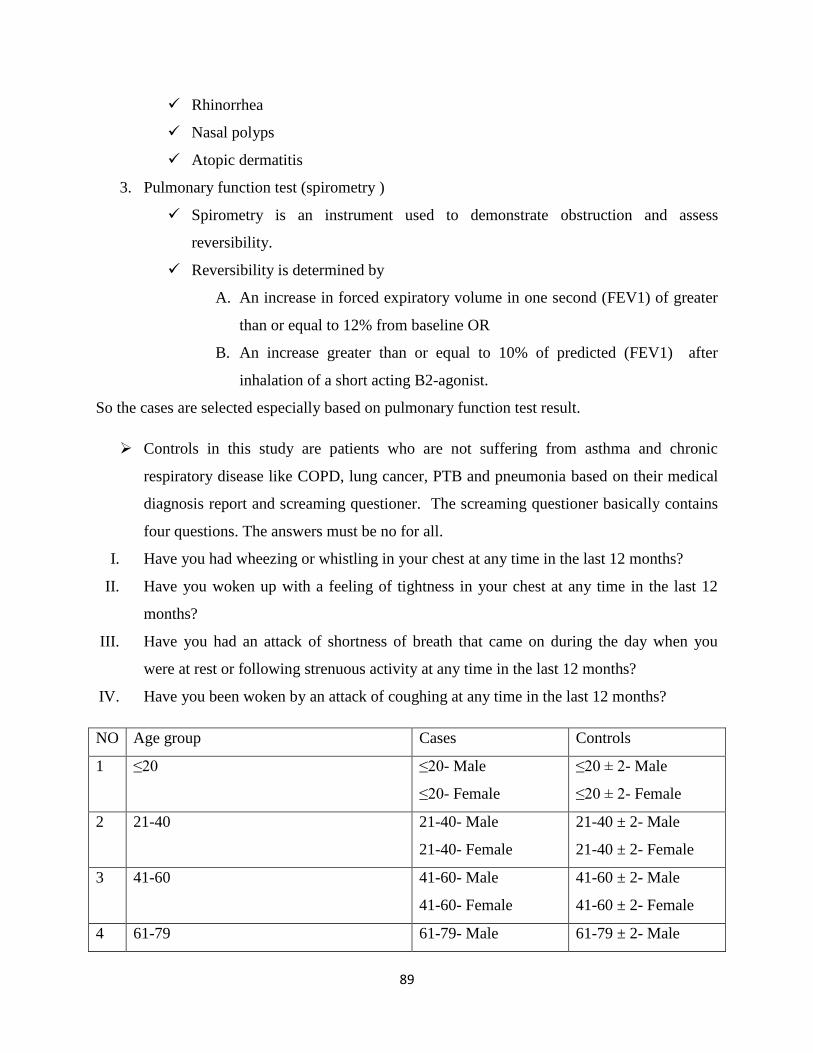
89
Rhinorrhea
Nasal polyps
Atopic dermatitis
3. Pulmonary function test (spirometry )
Spirometry is an instrument used to demonstrate obstruction and assess
reversibility.
Reversibility is determined by
A. An increase in forced expiratory volume in one second (FEV1) of greater
than or equal to 12% from baseline OR
B. An increase greater than or equal to 10% of predicted (FEV1) after
inhalation of a short acting B2-agonist.
So the cases are selected especially based on pulmonary function test result.
Controls in this study are patients who are not suffering from asthma and chronic
respiratory disease like COPD, lung cancer, PTB and pneumonia based on their medical
diagnosis report and screaming questioner. The screaming questioner basically contains
four questions. The answers must be no for all.
I. Have you had wheezing or whistling in your chest at any time in the last 12 months?
II. Have you woken up with a feeling of tightness in your chest at any time in the last 12
months?
III. Have you had an attack of shortness of breath that came on during the day when you
were at rest or following strenuous activity at any time in the last 12 months?
IV. Have you been woken by an attack of coughing at any time in the last 12 months?
NO Age group Cases Controls
1 ≤20 ≤20- Male
≤20- Female
≤20 ± 2- Male
≤20 ± 2- Female
2 21-40 21-40- Male
21-40- Female
21-40 ± 2- Male
21-40 ± 2- Female
3 41-60 41-60- Male
41-60- Female
41-60 ± 2- Male
41-60 ± 2- Female
4 61-79 61-79- Male 61-79 ± 2- Male
90
61-79- Female 61-79 ± 2- Female
5 ≥80 ≥80- Male
≥80- Female
≥80 ± 2- Male
≥80 ± 2- Female
9. Description for questionnaire
The questionnaire has 5 sub sections these are
A. Sub-section 1- Demographic and socio economic characteristics
B. Sub-section 2- Housing characteristics
C. Sub-section 3- House hold fuel exposure characteristics
D. Sub-section 4- Pet characteristics
E. Sub-section 5-Life style
F. Sub-section 6- Medical condition
Question description
Based on our data collection procedure we categorize household fuel in to three
1. Biomass fuel- which include wood, charcoal, agricultural residues and dung.
2. Fossil fuel- which include kerosene(paraffin), LPG
3. Cleaner fuel- which include grid electricity, batteries and solar
And if there is the use of such fuel with in the last 12 months considered like current user . on
the other hand if there is the use of such fuel previously in their life time considered like life
time user.
Age is considered like as right censored i.e. we count in years when the month is
completed. For example, if an individual whose age was 20 years with six month we took
it like 20 year.
Time spent for cooking present approximately in minute.
Pet contact categorized in to two regular and some contact.
1. Regular contact – a contact with a pet at least once a day and five times per week.
2. Some contact- a contact with a pet less than once a day and five times per week.
Alcohol drinking status categorized in to three
1. Ever drinker – a person who had ever drink alcoholic beverage during his/her life.
2. Ex-drinker- an ever drinker who had not drink alcohol with in the last 12 months.
3. Current drinker- an ever drinker who had drunk alcohol with in the last 12 months.
91
Physical activity categorized in to two
1. Physically active – a person who engage in moderate physical activity for at least 30
minute per day , 5 or more days per week or vigorous physical activity for at least 20
minute per day 3 or more days per week.
2. Physically inactive – a person who didn’t engage in moderate physical activity for at
least 30 minute per day , 5 or more days per week or vigorous physical activity for at
least 20 minute per day 3 or more days per week.
Smoking in this study categorized in to three.
1. Ever smoker - A person who had smoked at least 20 packs of cigarettes or 12 oz (360
grams) of tobacco in a lifetime, or at least one cigarette per day or one cigar a week
for one year was called an ever smoker.
2. Ex-smoker - An ever smoker who had not smoked with in the last 12 months or with
in the last 6 months.
3. Current smoker- An ever smoker who had smoked with in the past 30 days.
Weight of an individual in this study is expressed in a unit called kilogram.
Height of an individual in this study is expressed in a unit called centimeter.
10. Data collection procedure
Introduce yourself to participants after greetings
Read the information sheet for participants
Ensure participants understanding about research and data collection process.
Answering politely if there is any question which participants want to elaborate.
Ask their permission to engage in the study without any enforcement.
If they are agree to participate in the study , then we will sign them on the
informed consent form.
Finally start the interview
Thank you
92
Annex 10: curriculum vitae
CURRICULUM VITAE 1
1. GENERAL INFORMATION
- YONAS ABEBE MEZEMIR
- MALE
- 19/03/1987 EC
- SINGLE
- ETHIOPIAN
- E-MAIL- [email protected]
MOBILE- 0944162181
ADDIS ABABA, ETHIOPIA
2. EDUCATIONAL BACKGROUND
Education Study Area Obtain From Points Graduation
year
Certificate Primary
education
Mesrak Jegnoch primary
school Dire Dawa
97.9% 2000 E.C
Certificate Secondary
education
Sabeyan secondary school
Dire Dawa
3.8 2002 E.C
Preparatory
education
Natural science Sabeyan preparatory school
Dire Dawa
461 2004 E.C
Bachelor of
science
Public health
officer
Addis Ababa university 3.61 2008 E.C
3. LANGUAGE ABILITY
language Reading Writing Speaking Understanding
Amharic Fluent Fluent Fluent fluent
English Very good Very good Very good Very good
4. TRAINING
1 .Basic computer skill (EXCEL, WORD, POWER POINT, )
2. Basic journalism and communication skill
93
5. WORK EXPERIENCE
NO POSTION PLACE OF WORK DATE OF
WORK
1 Junior public health professional Arsi zone, munesa woreda,
kenchere health center
25/01/2009-
25/09/2009
2 Junior food , health related and
health facilities inspection and
licencing officer
Arada subcity woreda 09 Food,
Medicine, Health Care
Administration and Control
Authority (FMHACA)
15/09/2009-
27/09/2010
3 Assistance lecturer (part-timer) Alkan health science , business
and technology college
1/10/2010-
1/2/2011
1. Arsi zone, munesa woreda, kenchere health center , Junior public health professional.
The main duties and responsibility is
Work in both OPD and IPD (i.e treatment of patients and decision on referral)
Work in emergency (trauma management, drainage…)
Provide health education (communicable disease, personal and environmental hygiene,
STI, and first aid)
Organize and document different patient data for different purpose.
2. Arada subcity woreda 09 Food, Medicine, Health Care Administration and Control Authority
(FMHACA), Junior food , health related and health facilities inspection and licencing officer
The main activities and responsibility is
Provide technical support and health education in different areas for example hygienic,
standard operating procedure, solid and liquid waste management ,food handling,
medicine preservation….)
Monitor and evaluate institutions then issue, renew, suspend and revoke certificate of
competence for health, health related and food processing institutes.
Design and develop different plans, programs, strategies, techniques…in order to create
awareness in food and health related institutions.
Ensure proper disposal of expired medicine and foods and their raw material.
Ensure that handling and disposal of solid and liquid wastes from different institutions
are not harmful to public health.
Control illegal food, medicine and health services and take appropriate measure.
Ensure the availability of necessary hygienic requirement in controllable health related
institution.

94
Serve as medicine, food, health professional and health and controllable health related
institutions information center.
3. Alkan health science , business and technology college, Assistance lecturer (part-timer)
The main activities and responsibility is
Teaching different subjects like environmental health, health promotion.
Assist other instructors in different activities.
Coordinate college activities.
6. REFERENCE
No
NAME JOB TELL NO
1 Mr. Werissaw h/Selassie Head, under graduate
department of public health
officer, AAU
+251912005718
2 Mr. Debebe Yosef Kenchere health center manager +251904115919
3 Mr. Kumela Fufi Arada subcity woreda 9
FMHACA Manger
+251910393505
4 Mr Dawit Tadesse AHSBTC Community health
faculty dean
+251911466091
95
Annex 11: Assurance of principal investigator
ASSURANCE OF PRINCIPAL INVESTIGATOR
The undersigned agrees to accept responsibility for the scientific ethical and technical
Conduct of the research project and for provision of required progress reports as
Per terms and conditions of the Research Publications Office in effect at the time of
Grant is forwarded as the result of this application.
Name of the student: _______________________________________
Date.____________________ Signature _________________
Approval of the primary Advisor
Name of the primary advisor : _________________________________
Date.____________________ Signature _________________
Related Documents











