ACUTE NORMOVOLEMIC HEMODILUTION Aryeh Shander, MD, FCCM, FCCP Chief, Department of Anesthesiology, Critical Care and Hyperbaric Medicine Englewood Hospital and Medical Center, Englewood, New Jersey Clinical Professor of Anesthesiology, Medicine and Surgery Mount Sinai School of Medicine, New York

ACUTE NORMOVOLEMIC HEMODILUTION Aryeh Shander, MD, FCCM, FCCP Chief, Department of Anesthesiology, Critical Care and Hyperbaric Medicine Englewood Hospital.
Dec 11, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ACUTE NORMOVOLEMIC HEMODILUTIONAryeh Shander, MD, FCCM, FCCP
Chief, Department of Anesthesiology, Critical Care and Hyperbaric Medicine
Englewood Hospital and Medical Center,Englewood, New Jersey
Clinical Professor of Anesthesiology, Medicine and SurgeryMount Sinai School of Medicine, New York

ANH
• The technique• Formula or other targets• Fluid resuscitation, is there a
difference?• Induced anemia – safe or risk?• Anemia, perfusion and organ
function• ANH and PBM- outcomes

ANH
• As a blood conservation technique it cannot stand alone and must be accompanied by– Treatment of ANEMIA– Cell salvage and possible fractionation– Post operative management of anemia
and coagulation

ANH – The Debate
• ANH – controversial• ANH – variety of methods• ANH – unclear indications• ANH – risk not quantified• ANH – more work

Acute Normovolemic Acute Normovolemic Hemodilution (ANH)Hemodilution (ANH)
ANHANHNormovolemicHemodilution
NormovolemicHemodilution
Surgery(1- 6 hours)
Surgery(1- 6 hours)
He
mo
glo
bin
(g
/dL
)
14
11
8
5
PostoperativePostoperative
ANHANH

Practical Issues
• ANH– Key Points:
•Vascular access - IV or arterial•Monitoring•GA and/or Regional•Fluid replacement

ANH indications and concerns• Relative Indications
•Preop normal Hemoglobin levels•Anticipated intraop blood loss > ~1000ml•Moderate anticipated blood loss in patient
refusing allogeneic transfusion•Ability to draw blood after anesthetic induction
+ before commencement of surgical bleeding• Concerns
– Ability to tolerate blood withdrawal– Recurarization* (Br J Anaesth. 2006;97(4):482-8)– Coagulation– Fluid overload
Hobisch-Hagen P et al. BJA;82(4):503-9

Outcome Measurement in Blood Conservation (ANH)
• Reduced blood loss– Statistically significant reduction of blood loss– Clinically significant reduction of blood loss
• Reduced blood loss and or eliminate patient’s exposure to allogeneic transfusions
• Reduced or eliminate transfusions alone• Morbidity – perioperative infection, SIRS or MOF• Mortality

The Effect of Two Levels of Hypotension on Intraoperative Blood Loss During Total Hip
Arthroplasty Performed Under Lumber Epidural
Anesthesia
Shanrrock NE, et al.Anesth Analg. 1993 Mar;76(3):580-4.

Intraoperative – ANHEffectiveness of acute normovolemic
hemodilution to minimize allogeneic blood transfusion in major liver resections
• Liver resection – at least 30% transfusion requirements
• Prospective, randomized• N = 78• ANH to target Hct 24% vs. controls• Transfuse at 20% Matot I, et al.
Anesthesiology 2002;97:794-800.

Intraoperative – ANHIntraoperative – ANH
36
10
0
5
10
15
20
25
30
35
40
Control ANH
% t
ran
sfu
se
d a
llog
en
eic
blo
od
Matot I. et al. Anesthesiology 2002;97:794-800

ANH
• The technique• Formula or other targets• Fluid resuscitation, is there a
difference?• Induced anemia – what’s the limit?• Anemia, perfusion and organ function• ANH and blood conservation -
outcomes

V=EBV x Hi – Hf / Hav
ANH

Weiskopf R.B. Anesthesiology 2001;94:439-46

ANH
• The technique• Formula or other targets• Fluid resuscitation, is there a
difference?• Induced anemia – what’s the limit?• Anemia, perfusion and organ function• ANH and blood conservation -
outcomes

Choice of Fluid
• Crystalloid• ‘Normal’ Saline• Physiologic solutions
• Colloid• HA• Penta-Starch• Solute

Normal Saline vs. LR in Gyn Surgery
Total n = 24
Scheingraber et al. Anesthesiology 1999
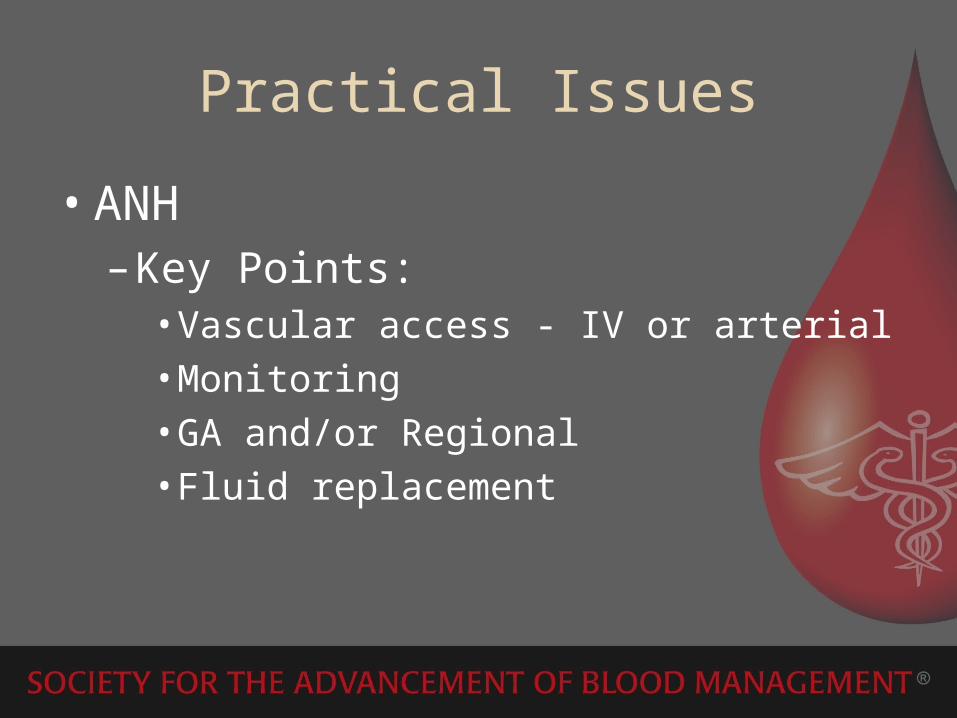
Anemia, viscosity and tissue oxygenation
OX
YG
EN
TE
NS
ION
, mm
/hg
Tsai AG. Tsai AG. Biorheology 38 (2000) 229-237Biorheology 38 (2000) 229-237

Acid-Base Changes Caused by 5% Albumin versus 6% Hydroxyl Starch Solution in Patients Undergoing ANHRehm M, et. Al. Anesthesiology 2000;93:1174-83
• N=20 Gyn surgery • ANH to HCT 22%• 10 HES and 10 HA in NaCl solution• Blood volume well maintained in
both groups• Metabolic acidosis (SID) with both
after ANH

ANH
• The technique• Formula or other targets• Fluid resuscitation, is there a
difference?• Induced anemia – safe or risk?• Anemia, perfusion and organ function• ANH and blood conservation -
outcomes

VO2 vs. DO2
DO2 ml/m2/min
VO2
Critical point of DO2
E.C.S.M. van Woerkens A&A 75, 1992

Normovolemic Anemia N=33
Weiskopf et.al. JAMA 279, #3 1998

Critical Oxygen Delivery in Conscious Humans
0
5
10
15
Esmolol Hemodilution Baseline
timetime
DO2
andVO2
ml O2 Kg-1
min-1
N=8N=8Hb. 4.7+/- 0.2 g/dlHb. 4.7+/- 0.2 g/dl
Lieberman JA Lieberman JA AnesthesiologyAnesthesiology 2000; 92:407-13 2000; 92:407-13
****

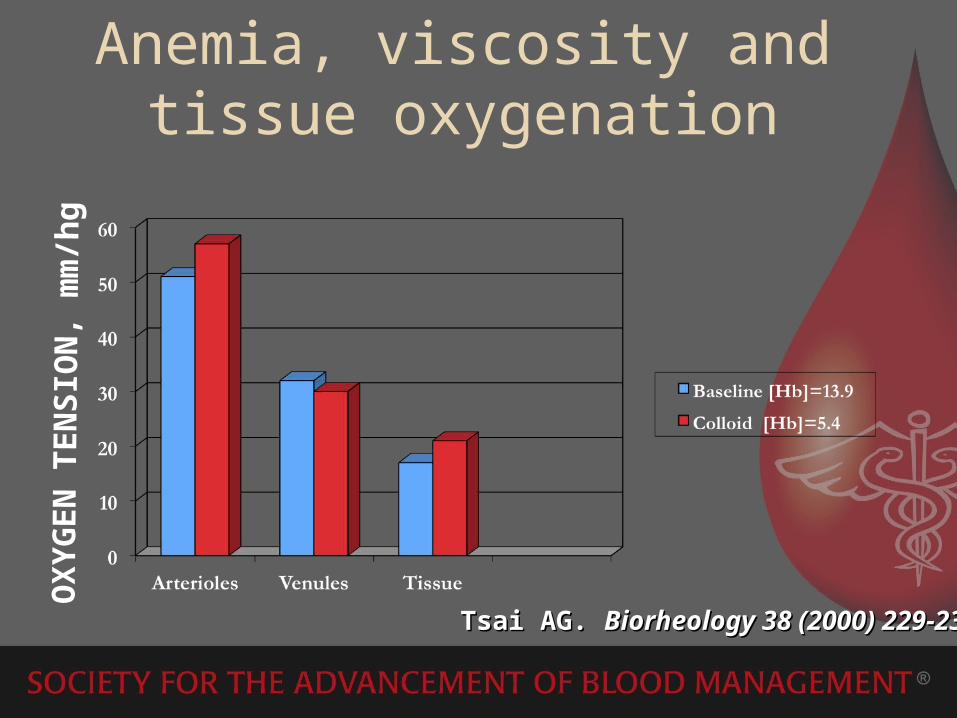
ANH & Coagulation
• aPT, INR, aPTT, platelets and fibrinogen• No significant change at 500, 1000 ml• 1500 ml, aPT and INR increased without
increased in nonsurgical bleeding
Figure 1: Coagulation Studies in ANH
60
70
80
90
100
110
120
130
Baseline 1000cc 1500 cc
% o
f Cha
nge
Platelets
Fibgn.
INR
PT
PTT
Hemoglobin

TEG values in ANH
0
10
20
30
40
50
60
70
80
pre-ANH post-ANH post return
mm
/ d
eg
. R
K
MA
Ang

Acute Severe Isovolemic Anemia Impairs Cognitive Function and Memory in Humans
Weiskopf R.B. et.al., Anesthesiology 2000;92:1646-1652 N=9 volunteers - reaction time and calculation
were impaired at Hb of 5.0gm/dl but not 7.0gm/dl
No PET scan, tests 10-15 min after anemia induction
Impaired vs. protectiveOxygen Reverses Deficits of Cong. Function
and Memory and Increased Heart Rate Induced by Acute Severe Isovolemic Anemia
Weiskopf R.B. et.al. Anesthesiology 2002;96:871-877
Acute Isovolemic Anemia Does Not Impair Peripheral or Central Nerve Conduction
Weiskopf R.B., et.al. Anesthesiology 2003;99(3):546-551
Peripheral conduction but no CNS effect at 5.0gm/dl

Cardiovascular Disease

Coronary Flow• Flow resistance is primarily reduced by
reduction of viscosity• Coronary flow is markedly increased with
ANH - Subendo and Subepicardial, improved oxygen utilization– Increased myocardial O2 extraction– Active coronary vasodilatation– MVO2 (myocardial BF X CaO2) remain stable
• Extraction ratio in severe ANH is UNCHANGED until Hct drops below 12.5% (Hgb 4.5)
Jan KM, Am J Physiol 1977;233:H106Levy PS et al. Am J Physiol 1993;265:H340-9

Cardioprotective effects of acute normovolemic hemodilution in patients with
severe aortic stenosis undergoing valve replacement
• N = 40 patients scheduled for elective AVR - randomly assigned to a control group (standard care) or an ANH group (target hematocrit level of 28%)
• In the ANH group:– Postoperative release of troponin I (1.7 ng/mL) and myocardial fraction
of creatine kinase (22 U/L) was significantly lower than in the control group (3.6 ng/mL and 45 [U/L, respectively)
– Circulating levels of erythropoietin (EPO) were higher than in control patients (13.6 +/- 4.2 mUI/mL vs. 7.3 +/- 2.4 mUI/mL; p < 0.05).
• Fewer hemodiluted patients presented adverse cardiac events
• Preoperative ANH further attenuates myocardial injuries• ANH-induced cardioprotection:
– Optimization of preischemic myocardial oxygen delivery and/or consumption
– Postconditioning effects of endogenous EPOLicker M. et al. Transfusion. 2007 Feb;47(2):341-50

Perioperative time course of serum concentrations of total CPK (A), CK-MB (B), and cTnI (C) in the control ( ) and ANH ( )
groups. *p < 0.05, between the two groups; #p < 0.05, compared with baseline
Licker M. et al. Transfusion. 2007 Feb;47(2):341-50

ANH & CARDIAC DISEASE
Anh.jpg

Significant Intraoperative Predictors of TransfusionBased on Patients With a Preoperative Estimated Risk of
Transfusion 5%a
Risk Factors OR CI Multivariate p Value
CPB time 1.013 1.005–1.020 0.001No. of bypass grafts (3) 0.381 0.138–1.052 0.0626Total crystalloid (2,500 mL) 4.732 1.181–18.961 0.0282
Total ANH 0.999 0.998–0.999 0.0049
n 145 observations; 5 were excluded because of missing values for acovariate; Hosmer-Lemeshow statistic for lack of fit of this model has a p
value of 0.72, and the c statistic 0.802.ANH acute normovolemic hemodilution; CI confidence interval;
Moskowitz D, Klein J.J, Shander A et.al. Ann Thorac Surg 2004;77:626–34

Blood ConservationEnglewood Hospital and Medical Center

CABG OutcomesPBMP vs Non-PBMP
Moskowitz et al Ann Thorac Surg 2010
N=586

Outcome of ANH• Cost effective
– Monk TG, et al. Transfusion 1996;36(6):849-50ANH cost effective vs PAD in rad prostate surgery– Monk TG, et al. A&A 1997;85(5):953-8ANH replaces PAD– Monk TG, et al. Anesthesiology 1999;(1):24-33EPO, ANH and PAD – ANH least costly– Goodnough LT, et al. Vox Sang 1999;77(1):11-6RT of ANH vs PAD TKA – ANH less costly– Goodnough LT, et al. Transfsion
2000;40(9):1054-7RT ANH vs PAD in THA – ANH less $$
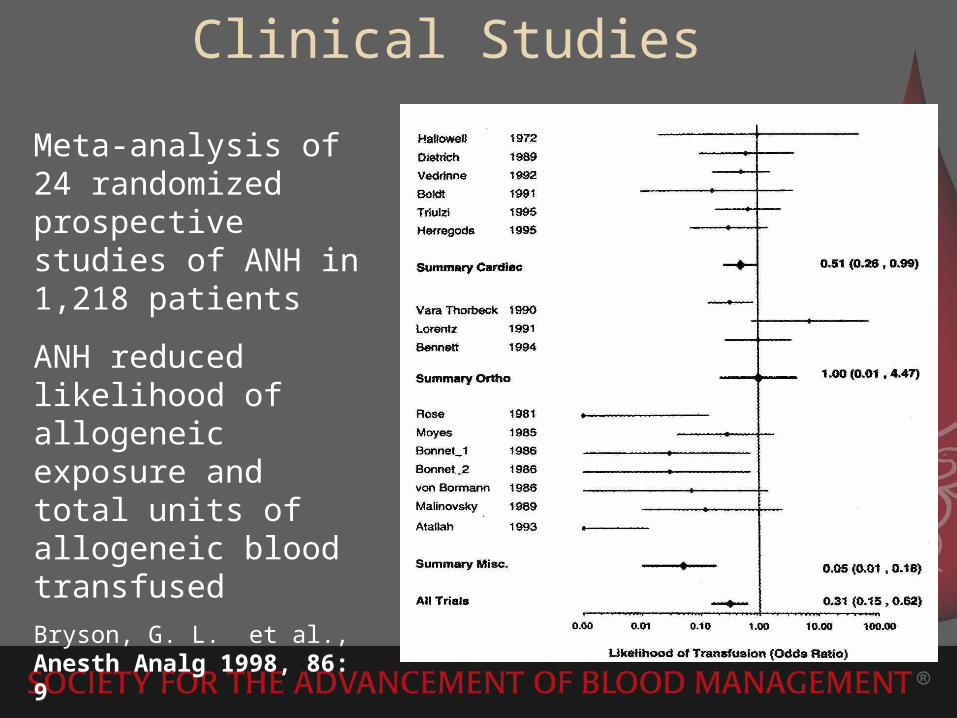
Clinical Studies
Meta-analysis of 24 randomized prospective studies of ANH in 1,218 patients
ANH reduced likelihood of allogeneic exposure and total units of allogeneic blood transfused
Bryson, G. L. et al., Anesth Analg 1998, 86: 9

Evaluation of Acute Normovolemic Hemodilution and Autotransfusion in
Neurosurgical Patients Undergoing Excision of Intracranial Meningiom
• Prospective randomized study• N = 40 (over 2 years)• Group I (Control Group) - Group II (ANH Group)
– Surgical blood loss in group I was 835.29 ± 684.37 ml vs 865 + 409.78 ml in group II
– Mean blood transfused in group I was 864.71 ± 349.89 ml vs. 165 ± 299.6 ml in group II [statistically significant (p<0.05)]
• ANH up to a target hematocrit of 30% is safe and effective in reducing the need for allogeneic blood
Naqash IA. Et al. J Anaesthesiol Clin Pharmacol. 2011 Jan;27(1):54-8

Relationship Between Intraoperative Fluid Administration and Perioperative Outcome After
Pancreaticoduodenectomy Management
• N = 130 (July 2005 to May 2009) randomized to ANH or standard management (STDM)– Transfusion rates were similar (ANH = 16.9%, 30 units vs STD =
18.5%, 33 units; P = 0.82)– Morbidity (ANH = 49.2% vs STD = 47%, P = 0.86)– More grade-3 complications in patients undergoing ANH (32% vs
23.1% STD, P = 0.17)– Pancreatic anastomosis complications higher in the ANH group
(21.5% vs 7.7%, P = 0.045)
• ANH did not reduce allogeneic transfusions• Restrictive intravenous fluid management
during PD may help improve postoperative outcome
Fischer M. et al. Ann Surg. 2010 Dec;252(6):952-8

Acute normovolemic hemodilution in moderate blood loss surgery: a randomized controlled trial
• N = 155 patients undergoing elective hip surgery • Groups "ANH" (n = 78) or "standard transfusion" (n
= 77)• Allogeneic transfusion was necessary in 22 (29%)
standard transfusion patients and 15 (19%) ANH patients
• Postoperative complications:– 30 (38%) standard transfusion patients compared with 14
(18%) assigned to ANH group (OR, 0.3; 95% CI, 0.14-0.65; p = 0.009)
• The major difference between the groups was the frequency of infective complications
• ANH reduced postoperative complicationsBennett J. et al. Transfusion. 2006 Jul;46(7):1097-103

Acute Normovolemic Hemodilution (ANH)
• Safely reduces allogeneic transfusions and associated complications
• Cost effective procedure • Effective in all surgical procedures –
method dependent • Dramatically underutilized• No standard approach to date


THANK YOU
Related Documents











