Acute Management of Acute Management of Traumatic Brain Injury Traumatic Brain Injury Dr N. Vairavan Dr N. Vairavan Neurosurgery Unit Neurosurgery Unit Department of Surgery Department of Surgery Faculty of Medicine Faculty of Medicine University Malaya University Malaya

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 1/32
Acute Management of Acute Management of
Traumatic Brain InjuryTraumatic Brain InjuryDr N. VairavanDr N. Vairavan
Neurosurgery Unit Neurosurgery UnitDepartment of SurgeryDepartment of Surgery
Faculty of MedicineFaculty of Medicine
University MalayaUniversity Malaya

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 2/32
Traumatic Brain InjuryTraumatic Brain Injury
2% of population/year 2% of population/year 43,000 people/yr 43,000 people/yr
1010 ± ± 15 % severe injury15 % severe injury
65% of mortality due to severe TBI65% of mortality due to severe TBI
Major cause of death and disability amongMajor cause of death and disability among
productive age group productive age group
Major socioeconomic effect on the family,Major socioeconomic effect on the family,
society and countrysociety and country

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 3/32

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 4/32

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 5/32

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 6/32
Prehospital ManagementPrehospital Management
Transport direct to nearest facility with theTransport direct to nearest facility with theresources to intervene and optimise ptresources to intervene and optimise pt
AirwayAirway
BreathingBreathing
CirculationCirculation
Cervical Spine ImmobilisationCervical Spine Immobilisation
Supplemental Oxygen/ Endotracheal intubationSupplemental Oxygen/ Endotracheal intubation Level III evidence of improved survivalLevel III evidence of improved survival
Winchell RJ, Hoyt DB. Endotracheal intubation in the field improves survivalin patients with severe head injury. Arch Surgery 132: 592- 597, 1997

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 7/32
Prehospital hypotension (SBP <90), hypoxemiaPrehospital hypotension (SBP <90), hypoxemia(SpO2< 90 )(SpO2< 90 )
± ± independent predictors of outcomeindependent predictors of outcome
Prehospital measurement of GCS, pupillary response-- predictors of outcomepredictors of outcome
Chestnut RM. Role of secondary brain injury in determining outcome in severehead injury. J Trauma. 34: 216 ± 222, 1993
Baxt WG. Impact of advanced prehospital emergency care on the mortality of
severely brain injure patients. J Trauma. 27:365 -369, 1987

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 8/32
Prehospital Brain targeted therapyPrehospital Brain targeted therapy
HyperventilationHyperventilation
MannitolMannitol
SedationSedation
AnalgesicAnalgesic ParalyticParalytic
Only hyperventilation recommended on Level IIIOnly hyperventilation recommended on Level IIIevidence in presence of brain herniationevidence in presence of brain herniation
Raichle M. Hyperventilation and cerebral blood flow. Stroke 3:965Raichle M. Hyperventilation and cerebral blood flow. Stroke 3:965 ± ± 972, 1972972, 1972

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 9/32
Imaging GuidelinesImaging GuidelinesBrainBrain

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 10/32
Imaging GuidelinesImaging Guidelines
Cervical SpineCervical Spine

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 11/32
Hypotension & HypoxemiaHypotension & Hypoxemia
Morbidity & Mortality Morbidity & Mortality
Single episode of SBP < 90 mmHgSingle episode of SBP < 90 mmHg
Apneic cyanosis or SpOApneic cyanosis or SpO22 < 90 or PaO< 90 or PaO22 < 60< 60
Level III evidence onlyLevel III evidence only Miller et al ¶78, Chestnut et al ¶93, Manley et al ¶01, Struchen et al µ01Miller et al ¶78, Chestnut et al ¶93, Manley et al ¶01, Struchen et al µ01
?? Treatment threshold, Optimal resuscitation?? Treatment threshold, Optimal resuscitation
protocals, Target values, treatment impact on protocals, Target values, treatment impact on
outcomeoutcome

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 12/32
Hyperosmolar TherapyHyperosmolar Therapy
Mannitol 0.25 to 1 gm/kg BWMannitol 0.25 to 1 gm/kg BW Single shotSingle shot ± ± buy time for diagnostic or interventional buy time for diagnostic or interventional
procedure procedure ± ± Level III recommendationLevel III recommendation
Prolonged therapyProlonged therapy ± ± for control of persistently raisedfor control of persistently raised
ICPICP Arterial hypotension should be avoidedArterial hypotension should be avoided
??Infusion vs bolus, Risks of prolonged??Infusion vs bolus, Risks of prolonged
administrationadministration
Becker and Vries ¶72, Mendelow et al ¶85, Eisenberg et al ¶88Becker and Vries ¶72, Mendelow et al ¶85, Eisenberg et al ¶88
Roberts I et al Cochrane Syst RV 2003Roberts I et al Cochrane Syst RV 2003

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 13/32
Hyperosmolar TherapyHyperosmolar Therapy
Hypertonic SalineHypertonic Saline
Reduce ICP without compromising BP, CPP or causingReduce ICP without compromising BP, CPP or causing
cerebral vasoconstrictioncerebral vasoconstriction
Osmotic mobilisation, microcirculatory effect, reducedOsmotic mobilisation, microcirculatory effect, reducedleukocyte adhesionleukocyte adhesion
3% saline 0.1 to 1.0mL/kg BW/ Hr on a sliding scale3% saline 0.1 to 1.0mL/kg BW/ Hr on a sliding scale
Level III recommendationLevel III recommendation
HS bolus infusionHS bolus infusion -- effective adjuvant / alternative toeffective adjuvant / alternative to
mannitolmannitol
??Dose, concentration, method??Dose, concentration, method Shackford et al ¶98, Quereshi et al µ99Shackford et al ¶98, Quereshi et al µ99

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 14/32
ProphylacticHypothermiaProphylacticHypothermia Target cooling 32Target cooling 32 --3333ºCºC
Duration of 48HDuration of 48H
Rate of rewarming 1ºC /H or slower Rate of rewarming 1ºC /H or slower
Meta Analysis of 6 RCTMeta Analysis of 6 RCT All cause mortality not different from control groupAll cause mortality not different from control group
46% increased chance of good outcome (GOS 4 or 5)46% increased chance of good outcome (GOS 4 or 5)
Avoid HyperthermiaAvoid Hyperthermia
??Target, duration??Target, duration Abiki et al 2000, Jiang et al 2000, Qiu et al 2003Abiki et al 2000, Jiang et al 2000, Qiu et al 2003

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 15/32
Infection ProphylaxisInfection Prophylaxis Periprocedural antibiotics for intubationPeriprocedural antibiotics for intubation
No change in LOS or mortality (1) No change in LOS or mortality (1)
Early tracheostomyEarly tracheostomy Reduce mechanical ventilation daysReduce mechanical ventilation days
No change in mortality or nosocomial pneumonia rates (2) No change in mortality or nosocomial pneumonia rates (2)
No support for routine catheter changes to prevent No support for routine catheter changes to preventinfection (Linfection (L--III) (3)III) (3)
No support for routine systemic prophylaxis in No support for routine systemic prophylaxis inventilatedTBI patients (LventilatedTBI patients (L--III)III)
Periprocedural prophylaxis does decrease pneumoniaPeriprocedural prophylaxis does decrease pneumonia(L(L--III)III)
1.Poon et al Acta Neur 1998, 2. Sugerman RJ J Trauma 1997, 3. Holloway1.Poon et al Acta Neur 1998, 2. Sugerman RJ J Trauma 1997, 3. Hollowayet al J Neuro 2000,et al J Neuro 2000,

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 16/32
DVT ProphylaxisDVT Prophylaxis 20% pt with TBI develop DVT20% pt with TBI develop DVT
0.38% incidence of PE in TBI pt0.38% incidence of PE in TBI pt
Graduated compression stockings (LGraduated compression stockings (L--III) (1)III) (1)
LMWH used in combination with mechanical prophylaxis (LLMWH used in combination with mechanical prophylaxis (L± ± III) (2)III) (2)
Lower risk of DVT, no difference in mortalityLower risk of DVT, no difference in mortality
Risk of intracranial h¶ghe expansionRisk of intracranial h¶ghe expansion
?? Dose, agent, timing of prophylaxis?? Dose, agent, timing of prophylaxis
1. Black et al Neuro 1986, 2. Gerlach et al Neuro 20031. Black et al Neuro 1986, 2. Gerlach et al Neuro 2003

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 17/32
Indication for ICP MonitoringIndication for ICP Monitoring
ICP in all pt with severe TBI ( GCS 3ICP in all pt with severe TBI ( GCS 3--8) and8) andabnormal CT scan (Labnormal CT scan (L--II)II)
ICP in severe TBI and normal CT scan if ICP in severe TBI and normal CT scan if >40 yrs age>40 yrs age
Unilat or bilat posturingUnilat or bilat posturing SBP < 90mmHgSBP < 90mmHg
ICP monitoring allowsICP monitoring allows Prediction of outcome and worsening intracranial pathologyPrediction of outcome and worsening intracranial pathology
Calculate and manage CPPCalculate and manage CPP
Allow therapeutic CSF drainage in ventricular monitorsAllow therapeutic CSF drainage in ventricular monitors Restrict potentially delterious ICP reduction therapiesRestrict potentially delterious ICP reduction therapies
NarayanRK et al J Neuro 1982 NarayanRK et al J Neuro 1982

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 18/32

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 19/32
ICP Monitoring TechnologyICP Monitoring Technology
Ventricular catheter + ext strain gaugeVentricular catheter + ext strain gauge Parenchymal ICP monitor Parenchymal ICP monitor
Subarachnoid, subdural, epidural monitorsSubarachnoid, subdural, epidural monitors
Pressure range 0Pressure range 0 --100 mmHg100 mmHg
AccuracyAccuracy 2mm Hg in 02mm Hg in 0--20 range20 range
Max error 100% in 20Max error 100% in 20 100 range100 range
ComplicationComplication Hemorhage, Malfunction,Hemorhage, Malfunction,
InfectionInfection
Lundberg et al Acta Psych 1960, Narayan R et al JLundberg et al Acta Psych 1960, Narayan R et al J
Neurosurg 1982, Stendel R et al Acta Neur 2003 Neurosurg 1982, Stendel R et al Acta Neur 2003

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 20/32
ICP ThresholdICP Threshold
Treatment should be commenced at ICP > 20 mmHgTreatment should be commenced at ICP > 20 mmHg(L(L± ±II) (1)II) (1)
Treatment threshold > 25 without craniectomy and >Treatment threshold > 25 without craniectomy and >
15 post craniectomy ( L15 post craniectomy ( L--II) (2)II) (2)
?? Herniation threshold pressure?? Herniation threshold pressure As little as 18mmHgAs little as 18mmHg
?? ICP interaction with CPP, CBF, Sjo2?? ICP interaction with CPP, CBF, Sjo2
1. Marmarou et al J Neuro 1991, 2. Eisenberg et al J Neuro 19881. Marmarou et al J Neuro 1991, 2. Eisenberg et al J Neuro 1988

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 21/32

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 22/32
Brain Oxygen Monitoring andBrain Oxygen Monitoring and
ThresholdThreshold
Jugular venous saturation or brain tissue oxygenJugular venous saturation or brain tissue oxygen
monitoring measure cerebral oxygenationmonitoring measure cerebral oxygenation
SjOSjO22 < 50% (1), P< 50% (1), P br br OO22 < 15mmHg (2) are threshold for < 15mmHg (2) are threshold for
interventionintervention
Cerebral microdialysis, thermal diffusion probe, transcranialCerebral microdialysis, thermal diffusion probe, transcranial
doppler, near infrared spectroscopydoppler, near infrared spectroscopy
1. Robertson CS et al J Neurotrauma 1995 2. Valadka et al 19981. Robertson CS et al J Neurotrauma 1995 2. Valadka et al 1998

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 23/32

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 24/32
BarbituratesBarbiturates
BarbituratesBarbiturates Cerebral protective alteration in vascular tone and resistanceCerebral protective alteration in vascular tone and resistance
Suppression of metabolismSuppression of metabolism
Inhibition of lipid peroxidationInhibition of lipid peroxidation
Inhibition of excitotoxicityInhibition of excitotoxicity
Prophylactic barbiturate to induce burst suppression notProphylactic barbiturate to induce burst suppression notrecommended (1)recommended (1)
High dose barbiturate recommended to control elevated ICPHigh dose barbiturate recommended to control elevated ICPrefractory to standard medical and surgical treatment (2)refractory to standard medical and surgical treatment (2)
Cochrane Systematic Review (2004)Cochrane Systematic Review (2004)µNo evidence that barbiturate therapy in patients with acute severe headµNo evidence that barbiturate therapy in patients with acute severe headinjury improves outcome¶injury improves outcome¶
1. Ward JD et al J Neuro 1985, 2.Eisenberg HM et al J Neuro 1988,1. Ward JD et al J Neuro 1985, 2.Eisenberg HM et al J Neuro 1988,3.Robert I et al. Cochrane Library 20053.Robert I et al. Cochrane Library 2005

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 25/32
NutritionNutrition
Patients should be fed to attain full caloricPatients should be fed to attain full caloricreplacement by day 7 post injury (1)replacement by day 7 post injury (1)
Start gastric or jejunal feed by day 3Start gastric or jejunal feed by day 3
Hyperglycemia should be controlled (2)Hyperglycemia should be controlled (2)
Zinc supplementation may be beneficial (3)Zinc supplementation may be beneficial (3)
1. Taylor SJ et al Crit Care Med.1999, 2. Lam AM et al J Neuro 1991,1. Taylor SJ et al Crit Care Med.1999, 2. Lam AM et al J Neuro 1991,3.Young B et al J Neurotrauma 19963.Young B et al J Neurotrauma 1996

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 26/32
Anti Seizure ProphylaxisAnti Seizure Prophylaxis
Prophylactic anticonvulsants are notProphylactic anticonvulsants are notrecommended for preventing laterecommended for preventing late
posttraumatic seizures (1) posttraumatic seizures (1)
Anticonvulsants are indicated to decreaseAnticonvulsants are indicated to decrease
incidence of early PTS (2)incidence of early PTS (2)
?? Benefit vs compication?? Benefit vs compication
1. Manaka S et al J Psych Neur 1992, 2. Temkin N et al N Eng J Med 19901. Manaka S et al J Psych Neur 1992, 2. Temkin N et al N Eng J Med 1990

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 27/32
HyperventilationHyperventilation
Prophylactic hyperventilation ( PaCO2 < 25) isProphylactic hyperventilation ( PaCO2 < 25) isnot recommended (1)not recommended (1)
Hyperventilation may be used as a temporizingHyperventilation may be used as a temporizingmeasure to reduce ICP (1)measure to reduce ICP (1)
Hyperventilation should be avoided in first 24Hyperventilation should be avoided in first 24hrs of injury (3)hrs of injury (3)
1. Muizellar JP J Neuro 1991, 2. 3. Bouma GJ J Neuro 19921. Muizellar JP J Neuro 1991, 2. 3. Bouma GJ J Neuro 1992

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 28/32
SteroidsSteroids
Steroids is not recommended for improvingSteroids is not recommended for improvingoutcome or reducing ICP (1)outcome or reducing ICP (1)
In moderate to severe TBI, high dose methylIn moderate to severe TBI, high dose methyl
pred is assoc with increased mortality (2) pred is assoc with increased mortality (2)
1. Alderson P Br Med J 1997, 2. Roberts I MRC CRASH Trial Lancet1. Alderson P Br Med J 1997, 2. Roberts I MRC CRASH Trial Lancet20042004

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 29/32
Decompressive CraniectomyDecompressive Craniectomy
Removal of a large portion of skull to provideRemoval of a large portion of skull to provide
spacefor brain expansionspacefor brain expansion
Reduction of refractory ICP due to severe TBIReduction of refractory ICP due to severe TBI
or malignant MCA infarctor malignant MCA infarct Observational studies provide LObservational studies provide L--III evidenceIII evidence
of good outcome (1,2)of good outcome (1,2)
On going LOn going L--I trialsmay provide answers (3,4)I trialsmay provide answers (3,4)
1. Kunze E et al Acta Neuro 1998, 2. Polin RS Neurosurg 1997,1. Kunze E et al Acta Neuro 1998, 2. Polin RS Neurosurg 1997,
3.Hutchinson PJ R ESCUEicp trial, 4. Cooper DJ et al DECRA trial3.Hutchinson PJ R ESCUEicp trial, 4. Cooper DJ et al DECRA trial

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 30/32
GCS<8
CT Brain
Insert ICP Monitor
Maintain CPP
(Age Appropriate)
oICP
Sedation & Analgesia
Head up 300
oICP
Drain CSF if Ventriculostomy
is present
oICP
Neuromuscular Blockade
oICPMannitol PRN HTS 3%
Mild Hyperventilation PaCO2 30-35 mm Hg
May continue if S. Osm<360May continue if
S. Osm<320
oICP
Second Tier
Therapy
Consider CTCarefully withdraw
ICP treatment
NO
NO
NO
NO

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 31/32
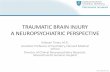
Second Tier TherapySecond Tier Therapy
o ICP despite first tier Rx
Evidence of Hyperemia ?Evidence of Hyperemia ?
No Evidence of IschemiaNo Evidence of Ischemia
Consider HyperventilationConsider Hyperventilation
To PaCO2 < 30 mm HgTo PaCO2 < 30 mm Hg
Consider monitoring CBF,Consider monitoring CBF,SjO2, AFDO2SjO2, AFDO2
Evidence of Ischemia?Evidence of Ischemia?
No evidence of No evidence of
contraindicationcontraindication
to Hypothermia?to Hypothermia?
Consider moderateConsider moderate
hypothermiahypothermia
Working VentriculostomyWorking Ventriculostomy
Consider lumbar drainConsider lumbar drain
Active EEG?
No contraindication to
Barb
Consider high dose BarbConsider high dose BarbSalvageable patientSalvageable patient
Consider decompressiveConsider decompressive
craniectomycraniectomy

8/8/2019 Acute Management of Traumatic Brain Injury
http://slidepdf.com/reader/full/acute-management-of-traumatic-brain-injury 32/32
Thank YouThank You
for for
your kind attention your kind attention
Related Documents