N.A.OTHIENO-ABINYA, FRCP DEPARTMENT OF CLINICAL MEDICINE AND THERAPEUTICS, UNIVERSITY OF NAIROBI ACUTE LEUKAEMIAS: THE HARD FACTS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

N.A.OTHIENO-ABINYA, FRCPDEPARTMENT OF CLINICAL MEDICINE AND
THERAPEUTICS,UNIVERSITY OF NAIROBI
ACUTE LEUKAEMIAS: THE HARD FACTS
CONFLICT OF INTEREST
Life as a medical oncologist used to be so simple before 2000! (EricP.Winer:(19/09/2014),
But first things first!
I have got no conflict of interest to declare.
EVERYTHING OLD IS NEW AGAIN Cora B Sternberg and Andrea B Apolo on: Modified M-VAC in neoadjuvant treatment of muscle
invasive bladder cancer
How about Jazz?Today cancer treatments have gone high-tech.AML too?

CONTINUATION FROM 27/11/14
ACUTE MYELOID LEUKAEMIA
Unbridled proliferation of haematopoietic stem cells of myeloid lineage resulting in marrow failure and patient death unless successfully treated.
Cause of acute leukaemias is largely unknown but malignant transformation is unlikely to be the result of a single event, rather, multistep process.

BackgroundMultiple processes producing genetic damage secondary to
physical or chemical exposure in susceptible progenitor cells.Incidence in the US is approximately 4.9/100,000
population/year. About 75% of new acute leukaemia cases are in adults.
What causes you? Risks Ionizing radiationOccupational exposure to benzene and other chemicalsCytotoxic chemotherapy, especially with alkylating agents
and topoisomease II inhibitors - AVOID DOING IT THE AFRICAN WAY
Most patients have no credible aetiologic factors

PresentationMainly result of bone marrow failure:FatigueSpontaneous bleedingFever Others are: Weight loss, night sweats and lethargy. Effects of tissue infiltration or circulating leukaemia cells.Metabolic abnormalities

Physical examinationPallorBleeding tendenciesSigns of infectionInfiltrations.
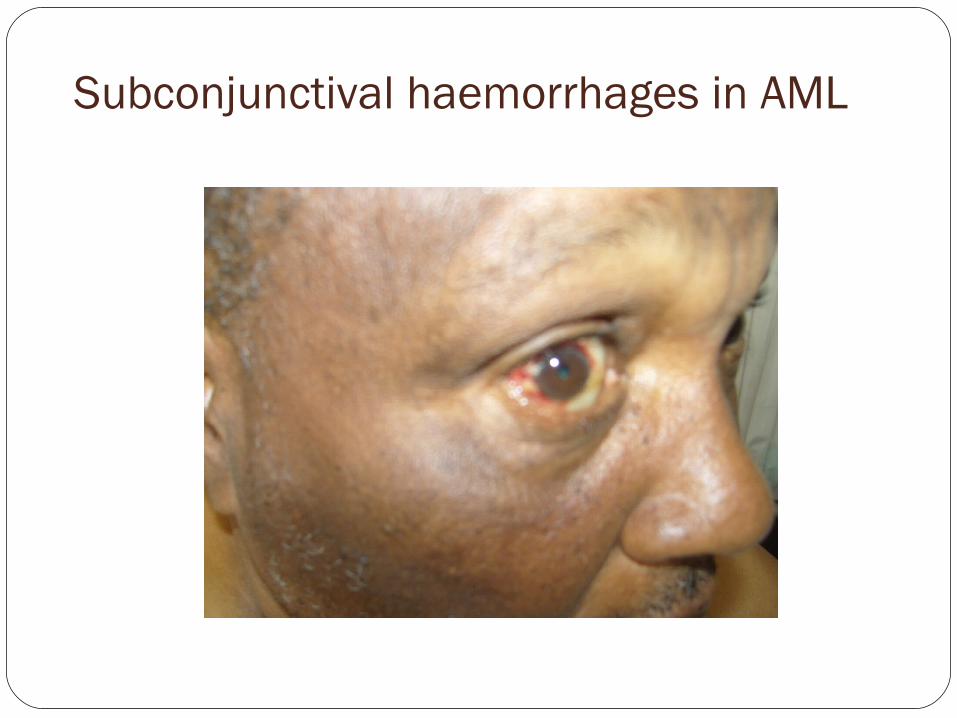
Subconjunctival haemorrhages in AML

Myeloblastic sarcoma

Sepsis
WHO Classification: Can we apply it? Is it important? Can we improvise?
Acute myeloid leukemia with recurrent genetic abnormalities
Acute myeloid leukemia with t(8;21)(q22;q22); RUNX1-RUNX1T1
Acute myeloid leukemia with inv(16)(p13.1q22) or t(16;16)(p13.1;q22), CBF /MYH11β
Acute promyelocytic leukemia with t(15;17)(q22;q12); PML/RARA
Acute myeloid leukemia with t(9;11)(p22;q23); MLLT3-MLL
Acute myeloid leukemia with t(6;9)(p23;q34); DEK-NUP214

Acute myeloid leukemia with inv(3)(q21q26.2) or t(3;3)(q21;q26.2), RPN1-EVI1
Acute myeloid leukemia (megakaryoblastic) with t(1;22)(p13;q13); RBM15-MKL1
Acute myeloid leukemia with t(9;11)(p22;q23); MLLT3-MLL
Provisional entity: Acute myeloid leukemia with mutated NPM1
Provisional entity: Acute myeloid leukemia with mutated CEBPA

Acute myeloid leukemia with myelodysplasia-related changes
Therapy-related myeloid neoplasmsAcute myeloid leukemia, not otherwise specifiedAcute myeloid leukemia with minimal differentiationAcute myeloid leukemia without maturationAcute myeloid leukemia with maturationAcute myelomonocytic leukemiaAcute monoblastic/monocytic leukemia

Acute erythroid leukemiaPure erythroid leukemiaErythroleukemia, erythroid/myeloid
Acute megakaryoblastic leukemiaAcute basophilic leukemiaAcute panmyelosis with myelofibrosisMyeloid sarcoma

Diagnostic procedures: Are they available to us all? Baseline evaluation involves routine blood work: complete blood count with differential comprehensive metabolic profile, and coagulation studies.
This is necessary for determining diagnosis and prognosis. Additional studies:
Chest radiography and echocardiography to determine a patient's ability to receive potentially cardiotoxic chemotherapy.
A cautious lumbar puncture may be needed if CNS symptoms are identified.
Human leukocyte antigen (HLA) typing is needed if bone marrow transplantation is being considered, and it should be performed prior to myeloablation

Diagnostic evaluationHigh index of suspicionPhysical evaluationBlood and bone marrow20% blasts, not 30% required for diagnosisA bone marrow aspiration and biopsy should be evaluated by: . cytochemistryImmunophenotypingFlow cytometryCytogenetics

Things used to be very simple! TODAY
Flow cytometry immunophenotype CD 34, 33,13,117 11b, 14
CytogeneticsMolecular profiling
Cytogenetic risk stratification for overall survival; Do we need it in Africa?
Favorable RiskBalanced structural rearrangementst(15;17) PMLRARAt(8;21) RUNX1-RUNXT1inv(16) CBFB-MYH11Normal karyotypeMutated NPM1 without FLT3-ITDMutated CEBPA

Intermediate riskBalanced structural rearrangementst(9;22) MLLT3-MLLCytogenetics abnormalities not classified as favorable or adverseAdverse/Unfavorable RiskComplex karyotypeBalanced structural rearrangementsinv(3) RPN1-EVI1t(6;9) DEK-NUP214t(v;11) MLL rearranged
Unbalanced structural rearrangement del(5q)Numerical aberrations−5−7abnl(17p)
Treatment stepsInduction = THE YOUNGER BROTHER OF MURDER.ConsolidationPostconsolidation therapy
NCCN classifies patients into those <60 years and those ≥ 60 years.
This is controversial.
Views AML should always be considered a medical emergency in
younger (age <60 years) adults, in whom each day of delay in instituting definitive chemotherapy may compromise survival.
? CONTROVERSIAL

Give me CR with frontline chemotherapy if you care for me.

Should we send all to clinical trials?2013 NCCN guidelines - all cases of AML excluding APL
should be treated in the setting of an appropriate clinical trial.
t-AML - poor prognosis, with median survival of only 8 months and 5-year survival less than 10%.
Humble request pleaseGood hygieneAvailability of platelets and blood at very short noticeAvailability of effective antimicrobialsDedicated, well-informed personnelLaboratory capability to recognize bone marrow in
remission.
ON AVERAGE 30 UNITS OF BLOOD IN FIRST 21 DAYS

Induction chemotherapy(Attempted murder)The goal is to reduce the number of leukemic cells, as well as
to return proper function to the bone marrow.Treatment of older AML patients is controversial.They often cannot tolerate the toxicities of intensive
remission induction chemotherapy.Ordinarily, the treatment-related mortality is between 15%
and 30%. Other less intensive regimens that may be used are oral
agents (such as hydroxyurea), low dose cytarabine, or one of the hypomethylating agents (azacitidine or decitabine
3/7For 4 decades - a combination of an
anthracycline/anthracenedione and cytosine arabinoside, the 3/7 protocol.
An anthracycline ie:- daunorubicin at 45-90 mg/m2 days 1-3- Doxorubicin 30-35 mg/m2 iv days 1-3-Cytarabine at 100-200 mg/m2 civi days 1-7 consecutive
days. Idarubicin or mitoxantrone at doses of 10-12 mg/m2.

Caveats
AMLs are quite heterogeneous and the prognosis remains poor.
Substituting daunorubicin with another anthracycline, or addition of 6-thioguanine or etoposide has not been demonstrated to improve outcome.
Current mechanism targeted therapies are not changing the outlook for AML significantly.
Moreover, 3/7 is quite toxic and support after its administration is highly costly: KShs1.7 M in 21 days

Treatment-related statistics for AML stratified by age Age (years) <60 ≥60Induction chemotherapy 7 + 3 7 + 3Postremission chemotherapy HiDAC 5 or 5 + 2Complete response rates (%) 60-85 40-55Treatment-related mortality (%) 5-10 20-305-year disease-free survival (%) 30 5-10
Those are responses from the west and North

Is 3/7 optimized?Factors that appear to have been ignored in formulation of
AML protocols are numerous Cell cycle kinetics appear to have been given blackout in
formulation of these protocols The AML stem cell tends to be resistant to chemotherapy. At any one time there are about 20% of myeloid leukaemia
stem cells (G0) cells.

Participation of Cyclin-dependent Kinases (CDKs), Cyclin-dependent Kinase Inhibitors (CKIs) and Retinoblastoma protein (RB) in cell cycle control.
(+) CDKS (cyclins D1, D2, D3, and E) P53 BRAKES
D/Cdk4 CAK activation induction
D/Cdk6 (-) CKIs Kip/cip (p21, p27, p57)
Rb pRb INK4(P15, p16, p18, p19)
DRIVE E2F release
cdc25+ D/cdk5 p16
Release of transcription factor E2F cdk1 M D/cdk4 p15
E2F response cyc A/B cyc D1
genes transcribed G2 G1 Rb p21 p53
S D/cdk2 p27
Cell cycle E/cdk2
Progression cdk7+ cdk1/2 cyc E
(G1-S exit) cyc H Cyc A +cdc25

Post remission therapyAims to eradicate any residual disease in an attempt at cure. Includes HiDAC for patients younger than 60 year - yields a
4-year disease-free survival rate of 44%, but carries with it a 5% treatment-related mortality.
HiDAC failed to improve the outcome of patients older than 60 years
Can be associated with cerebellar, ophthalmologic, and gastrointestinal toxicity, particularly in patients over the age of 60 years.

Allogeneic bone marrow transplantation: No free rides!Is an additional option for postremission therapy in adults
with AML. For adverse cytogenetics in patients < 60 years and for
whom an HLA-matched sibling or matched unrelated donor is available.
This procedure is not without risk; it has an associated 20% to 25% treatment-related mortality rate.

For paediatric ALL, survival outcomes have dramatically improved over the last several decades mainly due to:
- advances in the understanding of the molecular genetics and pathogenesis of the disease
- incorporation of risk-adopted therapy -availability of new targeted agents.
With current treatment regimens, the cure rate among children with ALL is about 80%.
The long-term prognosis for adults with ALL however
remains poor, with cure rates of only 30-40%.

Outcome of AMLPoor in older people because of: Poor stem cell reserve Higher frequency of co-morbidities Intrinsic resistance to chemotherapy Dismal in our country because of total lack of even the bare
minimum.
WHAT IS THE WAY FORWARD?
Related Documents