ACUTE KIDNEY INJURY - an update - Dr Pooran Kumar Kohistani FCPS Nephrology Liaquat university of medical and health sciences, Jamshoro

ACUTE KIDNEY INJURY - an update - Dr Pooran Kumar Kohistani FCPS Nephrology Liaquat university of medical and health sciences, Jamshoro.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ACUTE KIDNEY INJURY- an update -
Dr Pooran Kumar Kohistani FCPS NephrologyLiaquat university of medical and health
sciences, Jamshoro
What are the major functions of kidneys
?
Functions of Kidney
1. Excretion of metabolic end products & foreign substances like,urea,creatinine,toxins and drugs. (Function of glomerulus)
2. Maintenance of body composition:o Electrolytes balance o Volume regulation (Sodium balance)o Water balance & tonicity regulation
3. Production & secretion of enzymes & hormones:o Renin –– an enzyme from JGCo Erythropoiten — glycoprotein hormone secreted by
cortical interstitial cells.
o 1,25 dihydroxyvitamin D3 (active form) by prox.tubular cells, responsible for calcium & phosphate balance

Glomerular Filtration rateGlomerular Filtration rate
Both kidneys receive ~= 20% of the cardiac output (~= 1200 ml / min)
On average Glomerular Filtration rate is
~= 125 ml / min.
Filtration rate is relatively constant – auto regulation
Final urine output is ~= 1 ml / min.
So ~99% fluid of the filtrate is missing. And also other solutes are missing too. (So, Where this filtrate of blood is ???)
Reabsorption

TUBULAR FUNCTION:Basic principles
Absorption & secretion in the Renal Tubules
• The glomerular filtrate undergoes a series of modifications before becoming the final urine. These changes are:
1. Absorption, the movement of solutes & water from tubular lumen to blood e.g. Na+,Cl¯,H2O,HCO3
¯, glucose, amino acids, proteins, phosphates, Ca2+, Mg2+, urea, uric acid and other
2. Secretion, the movement of solutes from the blood or cell interior to tubular lumen e.g. H+,NH4
+,K+ and a number of organic acids and bases.

MEASURE OF KIDNEY FUNCTION - 1
NKF CKD Guidelines ‘clinicians should not use serum creatinine concentration as the sole means to assess the level of kidney function’
S. Creatinine reflects muscle mass –Different kits may give a different result - up to 0.3 mg/dl
Estimate creatinine clearance via equations that take into account variables as age, sex, race, body size.

MEASURE OF KIDNEY FUNCTION – 2
Timed collection of urine for creatinine clearance U x V ( urinary creatinine x volume ) P plasma creatinineCockcroft-Gault equation
140 - age x weight / 72 x s. creatinine [ x .85 for females ]
MDRD modified186 x [Cr.] -1.154 x [age] -0.203 x [0.742 for
females] x [1.210 for blacks]
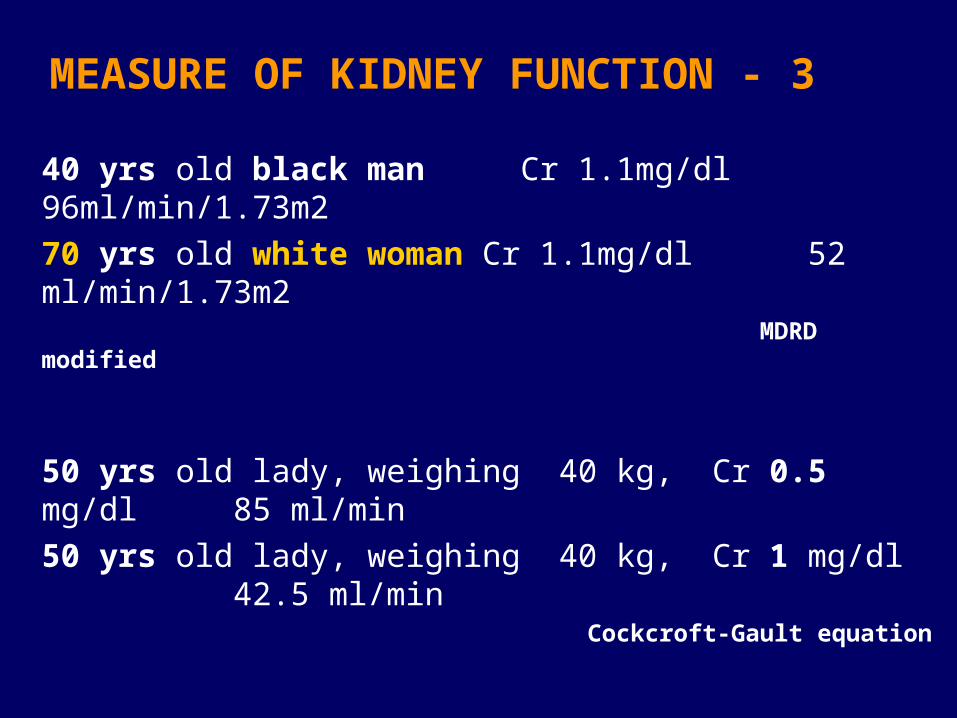
MEASURE OF KIDNEY FUNCTION - 3
40 yrs old black man Cr 1.1mg/dl 96ml/min/1.73m270 yrs old white woman Cr 1.1mg/dl 52 ml/min/1.73m2
MDRD modified
50 yrs old lady, weighing 40 kg, Cr 0.5 mg/dl 85 ml/min50 yrs old lady, weighing 40 kg, Cr 1 mg/dl 42.5 ml/min
Cockcroft-Gault equation
50 yrs old lady, weighing 40 kg, Cr 4.0 mg/dl 10.6 ml/min50 yrs old lady, weighing 40 kg, Cr 4.5 mg/dl 9.44 ml/min
Cockcroft-Gault equation
ACUTE kidney Injury - Definition
• Traditionally defined as the abrupt decrease of renal function sufficient to result in retention of nitrogenous waste products, as well as loss of regulation of extracellular volume and electrolytes

Reduction in GFR that is often reversible.there has been no agreement on how
much serum creatinine has to increase and over
what period of time for it to constitute AKIProposed definition for AKI: •0.5 mg/dl within 48 hours•50 % increase to at least 2 mg/dl.•Urine out put (oliguria).•Urea level

The RIFLE Criteria - Critical Care Clin. 2005; 21:223-237 The International Acute Dialysis Quality Initiative Group
GFR Urine output
S. Creatinine x 1.5 < 0.5 ml/kg/hour GFR >25% x 6 hours
S. Creatinine x 2 < 0.5 ml/kg/hour GFR >50% x 12 hours
S. Creatinine x 3 < 0.3 ml/kg/hour x 24 h GFR >75% anuria x 12 hrs S. Creatinine 4 mg/dl acute 0.5 mg/dl
Persistant ARF = complete loss of kidney function > 4 weeks
End Stage Renal Disease > 3 moths
Risk
Injury
Failure
Loss
ESRD
Acute Kidney Injury Network: Report of an Initiative to Improve Outcomes in Acute
Kidney Injury. Critical care 2007: 11 R 31
18 Nephrology Societies, 7 Critical Care Societies
Acute Kidney Injury (AKI) to reflect entire spectrum
Diagnostic Criteria:Abrupt (within 48 h) reduction in kidney
functionAbsolute S. Creatinine 0.3 mg/dlPercentage S. Creatinine 50% (1.5 fold)Reduction in urine output
< 0.5 ml/kg BW/hour for > 6 hours
Acute Kidney Injury Network: Report of an Initiative to Improve Outcomes in Acute Kidney
Injury. Critical Care 2007: 11 R 31
Classification/ Staging system for Acute Kidney Injury
1 S. Creatinine 0.3 mg/dl or < 0.5 ml/kg BW/hour S. Creatinine 1.5-2 fold from baseline for > 6 hours
2 S. Creatinine >2-3 fold from baseline < 0.5 ml/kg BW/hour
for > 12 hours
3 Creatinine 4 mg/dl with an acute 0.5 < 0.3 ml/kg BW/hour S. Creatinine >3 fold from baseline for > 24 hrs or anuria for 24 hrs.RRT irrespective of any of the above criteria is stage 3
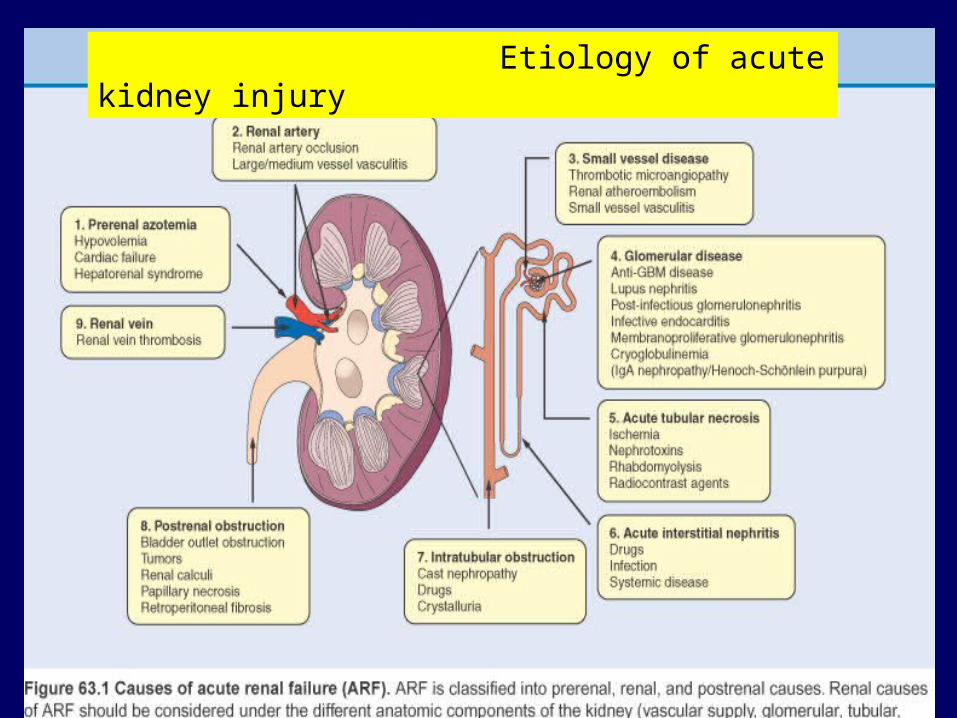
Etiology of acute kidney injury

ACUTE RENAL FAILURE - etiology
Pre Renal Failure Volume depletion Hypotension congestive cardiac failure Hemodynamic causes
(intrarenal vasoconstriction)
Radiocontrast PGinhibitors(NSAIDs) CNI inhibitors ACE inhibitors, ARBs Amphotericin
Hypercalcemia Hepato renal syndrome
intrinsic / intra Renal Vascular
Renal infarction,renal artery or vein thrombosis
Malignant hypertension
Tubular Ischemia nephrotoxic
Glomerular Acute GN Vasculitis Thrombotic microangiopathy
Interstitium Drugs tumor infilteration
ACUTE RENAL FAILURE - etiology
Postrenal:
a)Intra renal (tubular):
precipitation of insoluble crystals (phosphates, methotraxate, acyclovir,sulfonamides,uric acid), or protein hemoglobin , myoglobin, paraprotein.
b) Obstruction of extra renal collecting system:Prostate hypertophy
Neurogenic bladder
Intraureteral obstruction:( stones,tumor, clot, crystal ie uric acid,acyclovir,indinavir )
Extra ureteral obstruction: tumor , retroperitoneal fibrosis
CLINICAL EVALUATION OF PATIENT WITH AKI
•Is injury acute, Chronic or acute on Chronic?
•Is there hypovolemia/ effective arterial blood volume?
•Has there been a major vascular occlusion?
•Evidence of parenchymal renal disease other than ATN?
•Is there renal tract obstruction?

AKI vs. CHRONIC KIDNEY DISEASE
•History•Serial record of serum creatinine (drug therapies/interventions) •Laboratory tests.
•Normochromic, normocytic anemia•Hyperphosphatemia.•Hypocalcemia
•Ultrasound of kidneys.•Normal – does not exclude CRF (DM, amyloid Polycystic)•Bilateral small, echogenic – consistent with CRF. ( acute on chronic)
CLINICAL EVALUATION – History
•DM, HTN, CCF•Liver disease (pre renal, renal, hepato-renal)•Health checks•Urinary symptoms, recurrent UTI•Systemic illness•Recent surgery/ procedures •Radiocontrasts. •Arterial catheterization involving aorta, AF•Drug history, NSAIDS, ACE, ARB, Herbal, Hakim, Recreational•Volume loss/ sequestration.•Muscle pain weakness, rhabdomyolysis, muscle trauma drugs.
CLINICAL EVALUATION–Physical Examination 2
Intravascular Volume Depletion
History Thirst, dry mucosae, Oliguria
Record Excessive fluid loss, I/O chart,
Weight Record
Physical skin turgor,dry mucosa, JVP
Examination Postural hypotension,Orthostatic tachycardia.
Volume Overload
Ankle swellingWeight gain, PND,Orthopnea,
Pitting edema, ↑ JVP,
S3, Pulmonarycrackles, pleuraleffusion
INTAKE/ OUTPUT CHART, WEIGHT RECORD
CLINICAL EVALUATION–Laboratory Tests
•Urinalysis
–Significant proteinuria, glomerular disease.–RBC and RBC cast suggest glomerular cause.–Large number of WBC and WBC cast pyelonephritis, interstitial nephritis.–Eoisinophils > 1% of WBC, allergic interstitial nephritis, cholesterol embolism.
–Lack of RBC despite large Hb on dipstick,
myoglobinuria, hemoglobinuria.

CLINICAL EVALUATION–Laboratory Tests
•Urine Volume–Oliguria < 500ml/day, < 20 ml/hour.–Anuria < 100 ml/day.
–Non-oliguric better prognosis–Anuria:
RPGN, Acute cortical necrosis, Total renal arterial or venous occlusion, Complete urinary tract obstruction
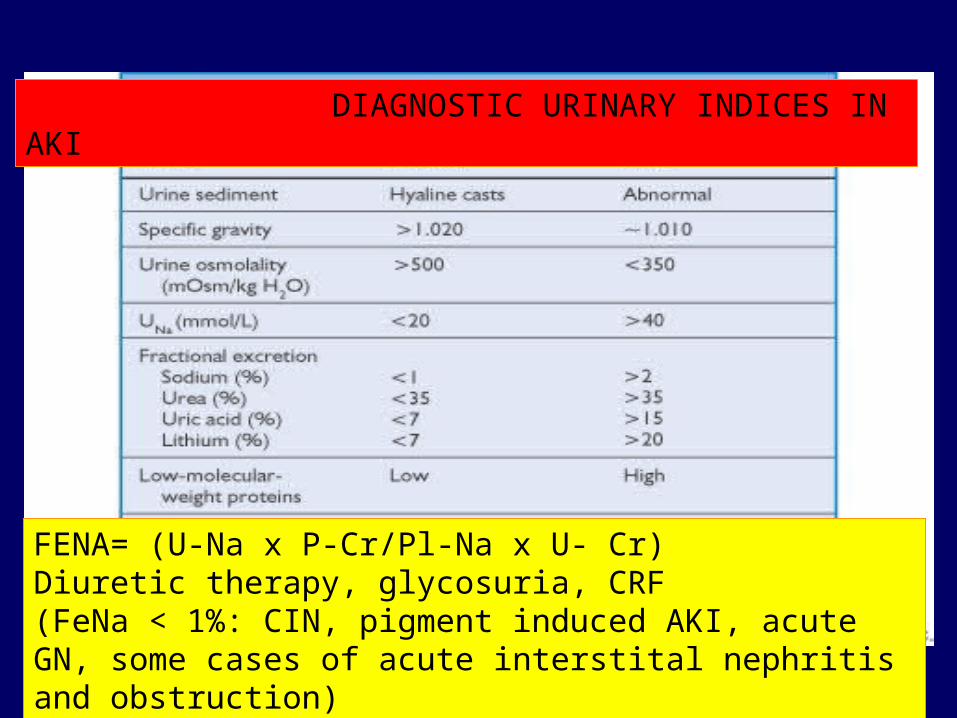
Pre renal
Urine Osmolality > 500U- Na (meq/L) < 20FENA* < 1%
Renal
< 350> 40> 2%
FENA= (U-Na x P-Cr/Pl-Na x U- Cr)Diuretic therapy, glycosuria, CRF(FeNa < 1%: CIN, pigment induced AKI, acute GN, some cases of acute interstital nephritis and obstruction)
DIAGNOSTIC URINARY INDICES IN AKI
CLINICAL EVALUATION–Laboratory Tests
Serum Creatinine•in complete absence of GFR S. Creatinine es by 1-1.5 mg/day.
•When an abrupt and complete interruption in GFR is followed by progressive recovery, S. creatinine will increase with peak on day 3-5.
•After nephrotoxic insult, no. of days that serum creatinine continues to increase has prognostic value.

CLINICAL EVALUATION– Ultrasonography
Observation Clue to diagnosis
Shrunken Kidneys Chronic intrinsic renal disease.Normal sizes
Echogenic Acute GN, ATNNormal Echo Pre renal AKI, Ac.
Renal artery obstructionEnlarged Malignant infiltration, Amyloid, Renal vein thrombosis,, HIV associatedPelviicalyceal dilatation Obstructive nephropathy

STRATEGIES TO DECREASE AKI

STRATEGIES TO DECREASE AKIVolume Expansion
risk of AKI, radio contrast agentsisotonic soda bicab@ 3ml/kg BW x 6 hrs superior
• risk of AKI, surgery of aorta, of obstructive jaundice, renal Tx
• early fluid resuscitation in critically ill é sepsis in ER. mortality & risk of AKI
• Crush syndrome-myoglobin induced AKI hydration as early as possible. 1-1.5 L first hr, 10 L/day. UO > 300 ml/hr.
• ??? ICU patients with multiple risk factors, third-space loss.
• Cardiac failure with renal perfusion, precipitate pulmonary edema.
Evaluation and Initial Management of Acute Kidney Injury. Clin J Am Soc Nephrol 2008
Volume – responsive AKI
Volume – unresponsive AKI
Volume responsive of the kidney
Volume responsive patient

STRATEGIES TO DECREASE AKIThe main effect of protein C is to • Reduce the production of thrombin, by inactivating
factors Va and VIII.• Inhibits the influence of tissue factor on the clotting
system• Reduces the production of IL-1, IL-6, and TNF-α by
monocytes, and has profibrinolytic properties by inactivating PAI-1 (it inactivates the inhibitor of the activator of the agent that converts plasminogen into plasmin)
• There is now compelling evidence that the exogenous administration of activated protein C to patients, in severe sepsis, improves outcome.
• Drotrecogin alpha (Xigris) 24 mcg/hr 96 hrs• Risk of increased bleeding
DOPAMINE (low dose) in ARF Meta-analysis - 261 trials 3359 patients identified.
Meta-analysis showed no effect of low dose dopamine on
Mortality RR 0.96 (95% CI 0.78-1.19)Need for RRT RR 0.93 (95% CI 0.76-
1.15)Adverse events RR 1.13 (95% CI 0.90-1.41)
Low dose dopamine urine out-put by (on day 1) 24% (CI
14-35%)improvement in S creatinine 4%
(CI 1-7%)e Creatinine clearance 6% (CI 1-
11%)
Ann. Int. Med 2005;142:510-524

FRUESEMIDE to prevent or treat ARF: Meta-analysis 4
Frusemide is NOT associated with any significant clinical benefits in the prevention and treatment of acute kidney injury in adults. High doses may be associated with an increased risk of ototoxicity.
BMJ 2006; 333:420
Timing of Initiation & Discontinuation of
RRT in AKI: Unanswered Key Questions. Clin J Am Soc Nephrol 3: 876-880, 2008 Indication – clinical or biochemical conditidion that defines the need for RRT in the presence of AKI Absolute – each indication can represent a stand-alone condition making RTT mandatory.
Relative – requires concomitant conditions without which RRT can only be suggested or recommended but not considered mandatory.
Timing of Initiation & Discontinuation of
RRT in AKI: Unanswered Key Questions. Clin J Am Soc Nephrol 3: 876-880, 2008
Timing – time in which RRT is initiated in patients with AKI
Early/ Late
RIFLE/AKI staging system.Severity score – no. and severity of
comorbidities.Trends – rate of biochemical changes.Illness trajectory – pace of clinical
evolution of the patient
Timing of Initiation & Discontinuation of
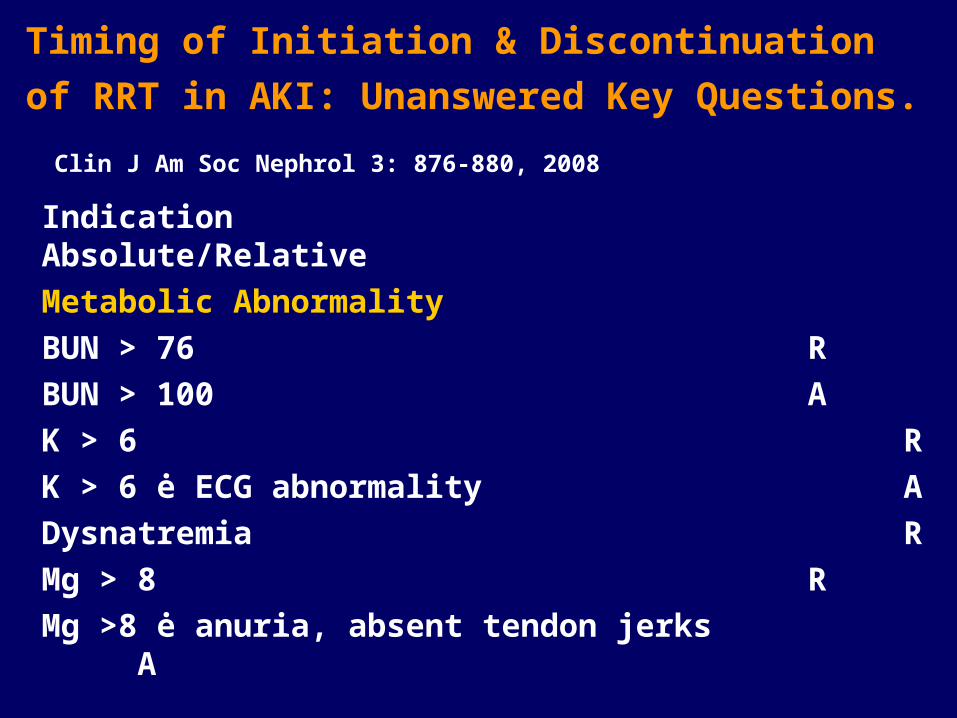
RRT in AKI: Unanswered Key Questions. Clin J Am Soc Nephrol 3: 876-880, 2008 Indication Absolute/RelativeMetabolic AbnormalityBUN > 76 RBUN > 100AK > 6RK > 6 ė ECG abnormalityADysnatremiaRMg > 8 RMg >8 ė anuria, absent tendon jerksA
Timing of Initiation & Discontinuation of
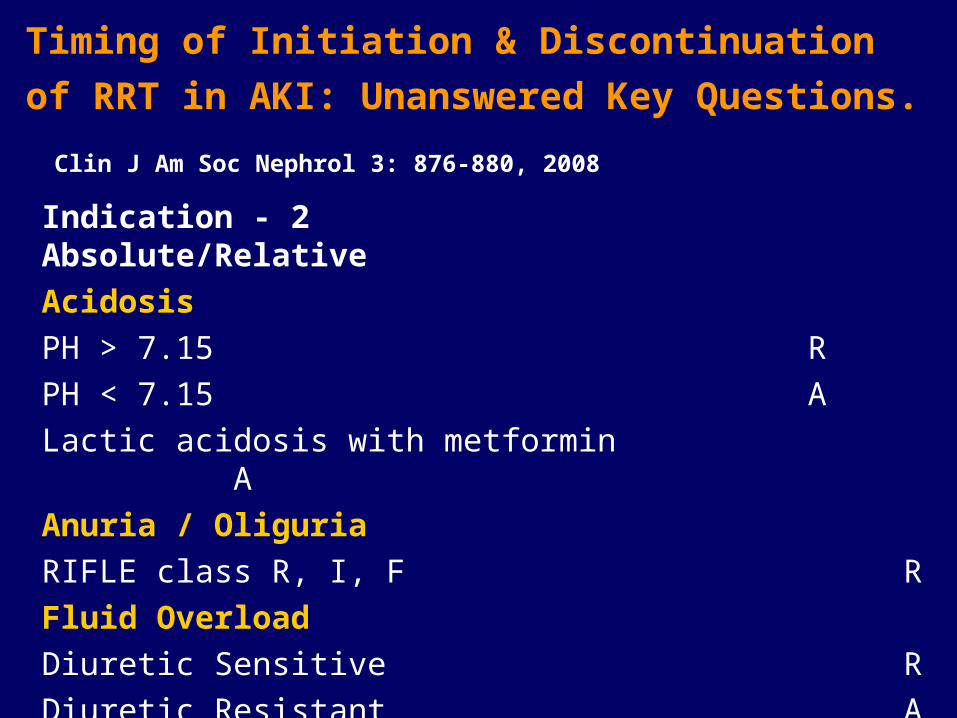
RRT in AKI: Unanswered Key Questions. Clin J Am Soc Nephrol 3: 876-880, 2008 Indication - 2 Absolute/RelativeAcidosisPH > 7.15 RPH < 7.15 ALactic acidosis with metformin
AAnuria / OliguriaRIFLE class R, I, FRFluid OverloadDiuretic SensitiveRDiuretic ResistantA
Timing of Initiation & Discontinuation of
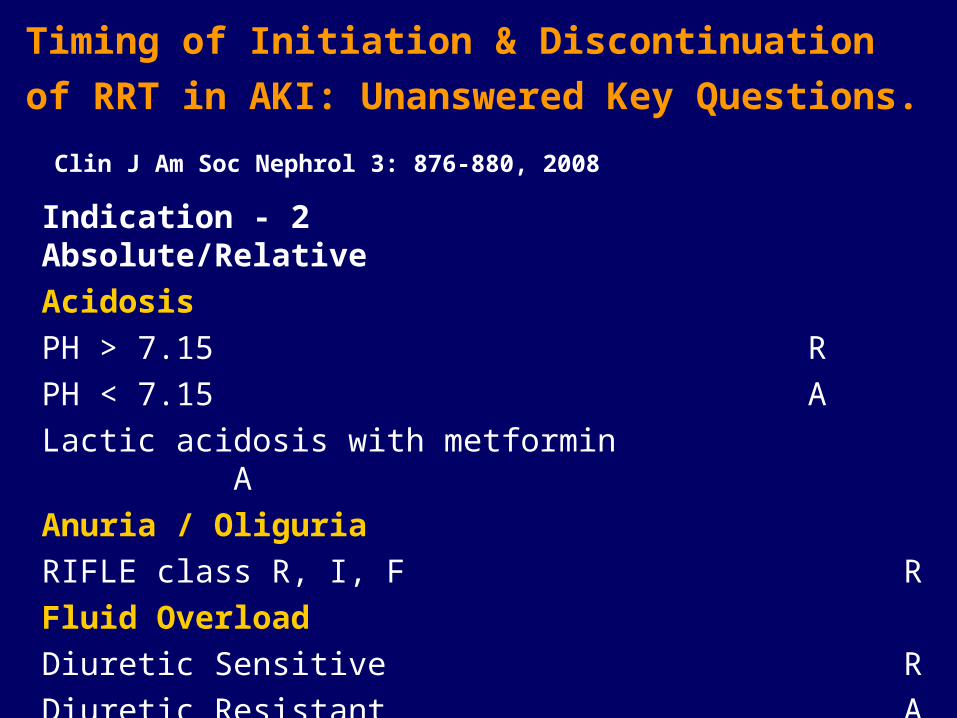
RRT in AKI: Unanswered Key Questions. Clin J Am Soc Nephrol 3: 876-880, 2008 Indication - 2 Absolute/RelativeAcidosisPH > 7.15 RPH < 7.15 ALactic acidosis with metformin
AAnuria / OliguriaRIFLE class R, I, FRFluid OverloadDiuretic SensitiveRDiuretic ResistantA

Timing of Initiation & Discontinuation of
RRT in AKI: Unanswered Key Questions. Clin J Am Soc Nephrol 3: 876-880, 2008 Research Questions
1 Timing of initiation of RRTWhat are the indications of RRT in in AKI?What factors determine timing of initiation of RRT?Does the timing of initiation of RRT influence outcome in AKI?
2 Does the timing of discontinuation of RRT in AKI influence renal recovery and out come?

Delivery of RRT in AKI: What are the key
issues. Clin J Am Soc Nephrol 3: 876-880, 2008 • Data on optimal dosage of RRT for AKI in
IHD, Hybrid techniques, and PD are limited. • An UF flow rate of 35 ml/kg /hr in CVVH and
dialysate clearance of 18 ± 5 ml/kg/hr – superior outcome compared with 20-25 ml/kg/hr.
• Current data do not suggest that any specific modality of RRT in AKI is superior, PD may be inferior.
• Benefit with less bioincompatible dialysis membrane in AKI is uncertain.
• Heparin is the most common anticoagulant, yet citrate may offer certain advantages during CRRT..

Take home message
• AKI , most of the time reversible.
• Furosimide (lasix) no more recommended.
• Renal dose dopamine no more validated.
END
Related Documents










