STROKE 0733-8619/00 $15.00 + .OO ACUTE ISCHEMIC STROKE THERAPY Susan L. Hickenbottom, MD, and William G. Barsan, MD After decades of discouragement regarding the treatment of acute stroke, we stand at the horizon of a new era. Advances in the understanding of the epide- miology, pathophysiology, and clinical management of stroke have brought us to the doorstep of significant therapeutic advances. This article summarizes the ur- gent evaluation of the patient with acute ischemic stroke, reviews acute stroke therapies available now, and discusses those that may become available in the future. FUNDAMENTALS OF ACUTE STROKE MANAGEMENT The evaluation of the patient with acute stroke generally begins in the emer- gency department (ED), although efforts are being made to improve care in the prehospital phase. Previously, stroke was not considered a high priority call for most emergency medical services, and emergency medical technicians (EMTs)and paramedics were not provided with much training regarding stroke." With the advent of thrombolytic therapy, acute stroke is now considered a medical emer- gency, and more emphasis is being placed on the prehospital care of the patient. Emergency dispatch service protocols should be designed to quickly recognize potential stroke patients and have priority dispatch with appropriate response teams.76 Eh4Ts and paramedics also should be trained to recognize possible stroke patients in the field in order to begin general, and possibly in the future, specific stroke care. Several easy-to-administer scales, including the Los Angeles Prehos- pita1 StrokeScale and the Cincinnati Prehospital StrokeScale, have been developed for paramedics and EMTs and have been found to be successful in clinical use.4z,43 On arrival in the ED, general therapeutic measures should be undertaken. The patient should have a rapid evaluation to ensure adequate airway, breathing, From the Departments of Neurology (SLH), and Emergency Medicine (WGB), University of Michigan Medical Center, AM Arbor, Michigan NEUROLOGIC CLINICS VOLUME 19 'NUMBER 2 -MAY 2000 379

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

STROKE 0733-8619/00 $15.00 + .OO
ACUTE ISCHEMIC STROKE THERAPY
Susan L. Hickenbottom, MD, and William G. Barsan, MD
After decades of discouragement regarding the treatment of acute stroke, we stand at the horizon of a new era. Advances in the understanding of the epide- miology, pathophysiology, and clinical management of stroke have brought us to the doorstep of significant therapeutic advances. This article summarizes the ur- gent evaluation of the patient with acute ischemic stroke, reviews acute stroke therapies available now, and discusses those that may become available in the future.
FUNDAMENTALS OF ACUTE STROKE MANAGEMENT
The evaluation of the patient with acute stroke generally begins in the emer- gency department (ED), although efforts are being made to improve care in the prehospital phase. Previously, stroke was not considered a high priority call for most emergency medical services, and emergency medical technicians (EMTs) and paramedics were not provided with much training regarding stroke." With the advent of thrombolytic therapy, acute stroke is now considered a medical emer- gency, and more emphasis is being placed on the prehospital care of the patient. Emergency dispatch service protocols should be designed to quickly recognize potential stroke patients and have priority dispatch with appropriate response teams.76 Eh4Ts and paramedics also should be trained to recognize possible stroke patients in the field in order to begin general, and possibly in the future, specific stroke care. Several easy-to-administer scales, including the Los Angeles Prehos- pita1 Stroke Scale and the Cincinnati Prehospital Stroke Scale, have been developed for paramedics and EMTs and have been found to be successful in clinical use.4z,43
On arrival in the ED, general therapeutic measures should be undertaken. The patient should have a rapid evaluation to ensure adequate airway, breathing,
From the Departments of Neurology (SLH), and Emergency Medicine (WGB), University of Michigan Medical Center, AM Arbor, Michigan
NEUROLOGIC CLINICS
VOLUME 19 'NUMBER 2 -MAY 2000 379

380 HICKENBOTTOM & BARSAN
and circulatory status. Vital signs, including temperature, pulse, blood pressure, and oxygen saturation, should be monitored frequently, especially in patients with moderate to severe symptoms. Endotracheal intubation and mechanical ventila- tion should be instituted in those patients who are unable to protect the airway or in those with poor ventilatory drive. Stroke patients with stable respiratory function may receive supplemental oxygen to maintain adequate oxygen satura- tion, because hypoxia may further worsen ischemia.44 Rapid determination of the blood glucose level should be made to rule out hypo- or hyperglycemia as a cause for neurologic deficit; other laboratory studies should also be obtained, including complete blood count, chemistry profiles, and coagulation studies. A toxicology screen should be ordered in young patients and any others suspected of illicit drug use. An electrocardiogram should be obtained to assess for evidence of car- diac ischemia or arrhythmia.
Treatment of hypertension in acute stroke remains controversial. Mild to mod- erate elevation of blood pressure is common in the first hours following stroke; usually this elevation is temporary and gradually resolves without interven- tion.10,33,45 Most recent guidelines have recommended minimal or no initial treat- ment of mild to moderate hypertension in the setting of acute ischemic ~ t r o k e . ~ , ~ ~ , ~ ~ Normal cerebral autoregulation is disrupted in the setting of ischemia, and thus cerebral perfusion in the ischemic areas depends almost entirely on systemic ar- terial blood pressure.59 Overly aggressive treatment of blood pressure to normo- tensive levels may worsen the ischemic insult, particularly in patients with un- derlying essential hy~ertension.",~~ Precipitous lowering of blood pressure, with sublingual nifedipine, for example, is especially to be avoided.26 Antihypertensive therapy should be considered, however, in specific clinical scenarios: before and after thrombolytic therapy, in the presence of myocardial ischemia or aortic dis- section, after significant hemorrhagic conversion of the infarct, or in the setting of hypertensive encephal~pathy.~~
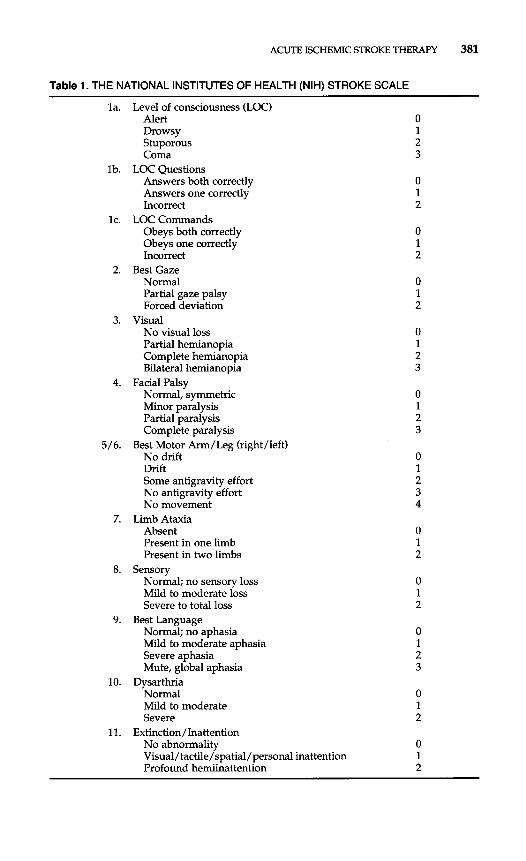
As these general steps are undertaken, specific evaluation for stroke can also begin. The patient's history should be taken in order to establish time of symptom onset and to elucidate any factors that might preclude treatment with thrombo- lytics or other agents. Specific stroke risk factors and potential stroke causes may be identified through the history. Physical examination, including a careful car- diovascular examination, also may suggest a stroke cause. A detailed neurologic examination will establish baseline stroke severity and can be quantified by using the National Institutes of Health Stroke Scale (NIHSS).l1 The NIHSS is summarized in Table 1. This scale has demonstrated reliability when used both by neurologists and nonne~rologists.2~ Finally, emergent neuroimaging with computed tomogra- phy (CT) should be performed to evaluate for the presence of intracerebral hem- orrhage (ICH) and for early signs of cerebral edema. A sample ED protocol for the initial management of acute ischemic stroke is provided.
Emergency Department Protocol for the Initial Management
1. Obtain vital signs including temperature, pulse, blood pressure and oxy-
2. Begin continuous cardiac and oxygen saturation monitoring 3. Ensure adequate airway/respiratory status:
4. IV access: 0.9 normal saline at 50 mL/hr; saline lock in opposite arm 5. STAT laboratory studies:
of Presumed Acute Ischemic Stroke
gen saturation; continue to monitor every 15 minutes
Intubate and initiate mechanical ventilation if necessary Otherwise, begin oxygen at 2 liters per minute via nasal cannula
Serum glucose (may be done at bedside)
ACUTE ISCHEMIC STROKE THERAPY 381
Table 1. THE NATIONAL INSTITUTES OF HEALTH (NIH) STROKE SCALE
la.
lb.
lc.
2.
3.
4.
5/6.
10.
11.
Level of consciousness (LOC) Alert Drowsy Stuporous Coma
LOC Questions Answers both correctly Answers one correctly Incorrect
Obeys both correctly Obeys one correctly Incorrect
Best Gaze Normal Partial gaze palsy Forced deviation
No visual loss Partial hemianopia Complete hemianopia Bilateral hemianopia
Normal, symmetric Minor paralysis Partial paralysis Complete paralysis
No drift Drift Some antigravity effort No antigravity effort No movement
Limb Ataxia Absent Present in one limb Present in two limbs
Normal; no sensory loss Mild to moderate loss Severe to total loss
Normal; no aphasia Mild to moderate aphasia Severe aphasia Mute, global aphasia
Dysarthria Normal Mild to moderate Severe
Extinction/Inattention No abnormality Visual/ tactile/spatial/personal inattention Profound hemiinattention
LOC Commands
Visual
Facial Palsy
Best Motor Arm/Leg (rightheft)
Sensory
Best Language
0 1 2
0 1 2
0 1 2
0 1 2 3
0 1 2
0 1 2
0 1 2
0 1 2

382 HICKENBOTTOM & BARSAN
Complete blood count with platelet count Chemistry profile Coagulation studies (prothrombin time, activated partial thromboplastin
Urine pregnancy test for females of childbearing age Urine toxicology screen
time)
6. Establish patient’s weight (measure or estimate) 7. Obtain IV pump for possible infusion 8. Order STAT head CT without contrast 9. No aspirin or other antiplatelet agents, heparin, or warfarin to be given to
Clearly, the hyperacute evaluation of the stroke patient is a complex process that must proceed efficiently if treatment is to be provided within a therapeutic time window. The need for rapid identification and treatment of other acute dis- orders such as trauma and myocardial infarction has led to the development of systems for the diagnosis and management of these en ti tie^.^,^^ Similar systematic approaches for the rapid evaluation of acute stroke are now being developed. The National Institute of Neurological Disorders and Stroke has issued time guidelines for the evaluation of acute which are summarized in Table 2. Several groups, including the National Institute of Neurological Disorders and Stroke (NINDS) rt-PA Stroke Study Group, have published specific practice protocols to organize prehospital services and emergency departments to assist institutions in meeting the recommended time guideline^?^,^^ Implementation of such protocols often can be accomplished without new investments in either personnel or equip- ment, but merely through an increased commitment to treat acute stroke as an emergency and with reorganization of services already available.32
potential thrombolytic therapy patients
REPERFUSION STRATEGIES
Reperfusion therapy is aimed at improving blood flow to the ischemic region and thus limiting the size of the acute infarction. Thrombolytic agents can re- establish cerebral perfusion by recanalization of acutely occluded arteries and may be delivered either intravenously or intra-arterially. Mechanical therapies to dis- rupt acute thrombus also may be used, either alone or as an adjunct to thrombo- lytic therapy.
Intravenous Thrombolytic Therapy
Although many intravenous (IV) thrombolytic agents exist, only streptokinase (SK) and recombinant tissue plasminogen activator (rt-PA) have been extensively
Table 2. GUIDELINES FOR RAPID EVALUATION OF THE ACUTE STROKE PATIENT
Evaluation Time (min.)
Door-to-stroke team notification 15 Door-to-CT scan initiation 25
Door-to-drug (needle) 60 Door-to-monitored bed 180
Door-to-physician evaluation 10
Door-to-CT scan interpretation 45

ACUTE ISCHEMIC STROKE THERAPY 383
studied in acute stroke. Three large, randomized, double-blind, placebo-controlled trials evaluating cardiac doses of IV SK given up to 6 hours after the onset of stroke symptoms failed to demonstrate a benefit of treatment with the drug and were terminated prematurely because of increased rates of ICH and mortality in the treated groups.20,51,52 As a result of these trials, SK has largely been abandoned as therapy for acute ischemic stroke.
On the other hand, IV rt-PA has been proved to be both safe and effective for use in selected stroke patients and remains the only approved therapy for acute ischemic stroke. Two major trials initially investigated the role of IV rt-PA in acute ischemic stroke: the European Cooperative Acute Stroke Study (ECASS) and the National Institute of Neurological Disorders and Stroke (NINDS) rt-PA Stroke StudyUrX The ECASS trial was a multicenter, randomized, double-blind, placebo- controlled study of 620 patients with acute ischemic hemispheric stroke who pre- sented within 6 hours of symptom onset. Patients were randomized to receive either rt-PA (1.1 mg/kg, maximum dose 100 mg) or placebo. Primary endpoints were scored on the Barthel Index (BI) and the Modified Rankin Scale (MRS) 3 months after stroke. No significant benefit was seen with therapy in the intention- to-treat population as measured by the primary endpoints. Of the 620 patients enrolled, 109 (17.4%) were considered to have had major protocol violations. When these patients were excluded from analysis, a statistically significant benefit to treatment with rt-PA was seen on the M E at 3 months in the remaining target population. The rate of symptomatic ICH was signhcantly higher in the treated patients (19.8% versus 6.5% in the placebo group), but there was no significant difference in mortality at 1 month. The majority of protocol violations occurred in patients with early radiographic signs of major infarction or other CT abnormal- ities; these patients were over-represented in the rt-PA treated group and had higher rates of symptomatic ICH and death than the placebo group. The authors thus concluded that use of rt-PA in unselected ischemic stroke patients was not recommended.
The NINDS rt-PA stroke study was a multicenter, randomized, double-blind, placebo-controlled trial of 624 patients with acute ischemic stroke who presented within 3 hours of symptom onset. Patients were randomized to receive either rt- PA (0.9 mg/kg, maximum dose 90 mg) or placebo. The lower dose of rt-PA used in the NINDS trial was selected after an earlier open label dose-escalation trial demonstrated that ICH occurred at higher dose^.^^,^^ The trial consisted of two parts, which ran consecutively and were reported together. Part I assessed early response to treatment, with the primary endpoint of complete resolution of neu- rologic deficit or a 4-point improvement on the NIHSS at 24 hours. Long-term outcome at 3 months was assessed as a secondary endpoint. Part I1 examined the primary endpoint of outcome at 3 months as determined by four different outcome scales (BI, M E , Glasgow Outcome Scale (GOS), and NIHSS) and a global outcome statistic. In order to demonstrate a sigruficant benefit from rt-PA treatment, scoring of the scales was dichotomized and patients had to return to normal or be left with very minimal deficit to be considered as having a "good outcome. Investi- gators remained blinded to the results of Part I until Part I1 was completed. Part I found no statistically sigruficant difference in early response between the treat- ment and placebo groups; however, there was a trend toward improved outcome in the rt-PA group at 3 months. Part I1 demonstrated significant improvement in the treated group on all four outcome scales and on the global outcome statistic at 3 months, with an 11% to 13% absolute and 30% to 50% relative increase in favorable outcome and an odds ratio for favorable outcome of 1.7 (95% confidence interval, 1.2-2.8; P = 0.008). Treatment with rt-PA was of benefit in all stroke subtypes. Although there was a statistically sigruficant increase in the rate of

384 HICKENBOTTOM & BARSAN
symptomatic ICH in the first 36 hours after treatment in the rt-PA group (6.4% versus 0.6%, p < 0.001), there was no significant difference in mortality at 3 months. As a result of this trial, the Food and Drug Administration (FDA) in June 1996 approved the use of lV rt-PA in acute ischemic stroke within 3 hours of symptom onset. Since then, both the Stroke Council of the American Heart As- sociation and the American Academy of Neurology have issued practice guide- lines for the use of rt-PA in acute ischemic ~ t r o k e . ~ , ~ ~ These guidelines recommend treating ischemic stroke patients who present within 3 hours of symptom onset with rt-PA at a dose of 0.9 mg/kg (maximum dose 90 mg), with 10% of the dose given as a bolus followed by an infusion lasting 60 minutes. They also outline inclusion and exclusion criteria for treatment and include blood pressure control protocols. The inclusion and exclusion criteria are summarized, in Box 1 and a
Box 1. Eligibility Criteria for Treatment of Ischemic Stroke
with Intravenous rt-PA
Inclusion Criteria Age 2 18 years Clinical diagnosis of ischemic stroke with clear symptom onset within
3 hours Noncontrasted CT without evidence for hemorrhage
Exclusion Criteria Medical History
Prior intracranial hemorrhage History of intracranial neoplasm, aneurysm or arteriovenous
Stroke or head trauma within previous 3 months Major surgery or biopsy of parenchymal organ within preceding
Gastrointestinal or urinary bleeding within preceding 21 days Recent myocardial infarction Seizure at onset of stroke History of known hereditary or acquired abnormal hemostasis Current use of oral anticoagulants with prothrombin time > I 5 seconds Use of heparin in previous 48 hours with prolonged partial thrombo-
Neurological signs that are improving rapidly Isolated mild neurological deficits, such as ataxia, dysarthria or
sensory loss alone Systolic blood pressure (BP) >I85 mmHg or diastolic BP
>I 10 mmHg, or aggressive therapy required to control blood pressure
MCA territory)
malformation
14 days
plastin time Clinical Examination
CT or Laboratory Findings Evidence on CT of major hypodensity or sulcal effacement (>1/3 of
Platelet count < 1 O0,000/mm3 Blood glucose <50 mg/dL or >400 mg/dL

ACUTE ISCHEMIC STROKE THERAPY 385
basic protocol for rt-PA administration is provided in Box 2. Blood pressure man- agement guidelines are detailed in Box 3. Adherence to the guidelines for throm- bolytic therapy is vital, as recent studies have indicated that increased risk for ICH occurs when the protocol is ~ i o l a t e d . ~ ~ , ~ ~
When the ECASS intention-to-treat population was analyzed retrospectively using the dichotomized endpoints outlined by the NINDS trial, statistically sig- nificant improvement at 3 months was demonstrated on the MRS, NIHSS, and the global outcome statistic, with an odds ratio for favorable outcome of 1.5 (95% confidence interval, 1.1-2.0; P = 0.008).28 In a post hoc analysis, the patient cohort treated within 3 hours demonstrated an increased rate of favorable outcome.68 To further evaluate the role of dose and timing of thrombolflc therapy, two addi- tional trials were undertaken: the European Cooperative Acute Stroke Study I1 (ECASS 11) and the Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic Stroke (ATLANTIS). ECASS 11, like the ECASS I trial, included patients
Box 2. Protocol for rt-PA Administration
1. Ensure “ED Protocol for Acute Stroke” is initiated 2. Reconfirm exact date and time of stroke onset (or time patient last
seemed normal) 3. Complete brief initial evaluation. Determine if patient has:
a. suspected ischemic stroke b. sufficient time for treatment within 180 minutes from onset
If yes to both, proceed with acute stroke/potential rt-PA evaluation
1. Arrange for STAT head CT; notify CT technician that study is for possible thrombolytic therapy (to ensure scheduling priority)
2. Notify radiology staff of possible thrombolytic therapy and need for emergent CT interpretation
3. Complete history and physical examination 4. Complete NIH Stroke Scale (see Table 1) 5. Re-confirm that all inclusion criteria have been met and no exclusion
criteria are present (see Box 1)
If all inclusion criteria “yes” AND all exclusion criteria “no,” proceed to treatment
1. Obtain informed consent from patient or family (if required by institution) 2. Calculate total dose of rt-PA as 0.9 mg/kg-do not use cardiac dose 3. Give 10% of total dose of rt-PA over 1 minute as IV bolus 4. Start IV infusion of remaining 90% of total dose to infuse over 1 hour 5. Maintain systolic BP<185 mm Hg and diastolic BP<llO mm Hg, per
protocol (see Box 3) 6. Arrange for ICU admission for post-thrombolytic patient 7. Consider possible ICH for any sudden increase in BP, decline in
mental status or neurological function, or complaint of severe headache; obtain STAT repeat head CT as indicated

386 HICKENBOTTOM & BARSAN
Box 3. Emergent Management of Arterial Hypertension for Persons Receiving Thrombolytic Drugs for Acute Ischemic Stroke:
Method Used by the NINDS Study
Monitor arterial blood pressure (BP) during the first 24 hours after starting treatment.
Every 15 minutes for 2 hours after starting the infusion, then Every 30 minutes for 6 hours, then Every 60 minutes until 24 hours after starting treatment.
two or more readings 5-1 0 minutes apart:
Give intravenous labetalol 10 mg over 1-2 minutes. The dose may be
Monitor BP every 15 minutes during labetalol treatment and observe
If systolic BP is 180-230 mm Hg or diastolic BP is 105-120 mm Hg for
repeated or doubled every 10-20 minutes up to a total dose of 150 mg.
for development of hypotension.
If systolic BP is >230 mmHg or diastolic BP is 121 -140 mm Hg for two or more readings 5-10 minutes apart:
Give intravenous labetalol 10 mg over 1-2 minutes. The dose may be repeated or doubled every 10 minutes up to total dose of 150 mg. Monitor BP every 15 minutes during labetalol treatment and observe for development of hypotension. If no satisfactory response is seen, infuse sodium nitroprusside (0.5-1 .O pg/kg/minute).* Continue monitoring BP.
If diastolic BP is <I40 mm Hg for two or more readings 5-10 minutes apart:
Infuse sodium nitroprusside (0.5-1 .O yg/kg/minute).* Monitor BP every 15 minutes during infusion of sodium nitroprusside and observe for development of hypotension.
*Continuous arterial monitoring is advised if sodium nitroprusside is used. The risk of bleed- ing secondary to an arterial puncture should be weighed against the possibility of missing dra- matic changes in blood pressure during infusion.
Data from The National Institute of Neurologic Disorders and Stroke (NINDS) rt-PA Stroke Study Group: Tissue plasminogen activator for acute-ischemic stroke. N Engl J Med 333:i 581 - 1587,1995.
who presented within 6 hours of stroke onset, but used the NINDS dosing regimen of 0.9 mg/kgZ9 More rigorous training for interpretation of CT findings and tighter control of hypertension were emphasized before, during, and after administration of the drug. The primary endpoint was a favorable outcome on the MRS, using the dichotomized method of the NINDS trial. Eight hundred patients were en- rolled, with only 158 treated within 3 hours. Seventy-two protocol violations were reported (34 in the treated group and 38 in the placebo group); most were viola- tions of the CT criteria. A favorable outcome ( M E 0-1) was seen in 40.3% of the rt-PA group and 36.6% of the placebo group, which was not a statistically signifi-

ACUTE ISCHEMIC STROKE THERAPY 387
cant difference (P = 0.277). Post-hoc analysis based on a dichotomized MRS of independence (MRS 0-2) did reveal a statistically sigruficant benefit to treatment with rt-PA, with 54.3% of treated patients returning to independence versus 46.0% of placebo patients (P = 0.024). Symptomatic ICH occurred more frequently in the rt-PA treated group (8.8% versus 3.4% in the placebo group) but there was no difference in mortality between the groups at either 30 days or 90 days. The ECASS I1 investigators concluded that the use of rt-PA in acute ischemic stroke within 6 hours of symptom onset was not supported by the trial, although there might be a trend toward better outcome with treatment. They also recommended conser- vative interpretation of the 0 to 3 hour results, because the number of patients treated within that time window was small.
The ATLANTIS rt-PA Acute Stroke Trial was undertaken to determine whether the benefits of rt-PA given within 3 hours of symptom onset could be extended to a longer time window.'6 Patients were randomized to receive either rt-PA or placebo according to the NINDS protocol; the ECASS CT criteria even- tually were used. Initially, the trial was designed to investigate rt-PA use within 6 hours of stroke onset (Part A), but the time window was changed to 0 to 5 hours (Part B) in December 1995 because of safety concerns about the 5 to 6 hour group. This time window was further modified in February 1996 to 3 to 5 hours after symptom onset following the publication of the NINDS results and the FDA ap- proval of rt-PA use within 3 hours of symptom onset. The primary endpoints for Part A were a 4-point improvement on the NIHSS at 4 days and 30 days. In Part B, efficacy was determined by the percentage of patients with a good outcome (NIHSS = 0 or 1) at 90 days. A total of 142 patients were enrolled in Part A; 619 patients were enrolled in Part B, including 40 within 3 hours. The trial was ter- minated prematurely in July 1998 when Data Monitoring and Safety Board anal- ysis found "treatment was unlikely to prove beneficial"; however, no difference in mortality was seen between the treatment and placebo groups, suggesting that treatment within 5 hours of symptom onset was safe. The ATLANTIS investigators concluded that the use of rt-PA for acute ischemic stroke beyond 3 hours was not recommended.
Other more recent studies have emphasized the importance of time to treat- ment. Post-hoc analysis of the NINDS rt-PA Stroke Study results indicated that better outcome may be linked to earlier treatment within the 3-hour time win- dow." The initial report of the NINDS trial showed no difference in 3-month out- come between patients treated at less than 90 minutes and those treated between 91 and 180 minutes, with an odds ratio for improvement with treatment of 1.9 for both groups. Patients with more severe strokes tended to present earlier within the 3-hour time window, potentially confounding the beneficial effects of earlier treatment. Analysis for time-treatment interactions that adjusted for potential con- founders was performed, and NIHSS score was identified as a masking con- founder for 3-month outcome. With the NIHSS score as a covariate, the odds ratio for a favorable 3-month outcome associated with rt-PA treatment was 2.11 in the 0 to 90 minute group and 1.69 in the 91 to 180 minute group. The odds ratio for a favorable outcome with rt-PA approached 4.0 for treatment within 60 minutes. Post-marketing experience with rt-PA for acute ischemic stroke in Cincinnati found patients were being treated later in the 3-hour time window than in the NINDS trial, with only 10% of post-trial patients treated in fewer than 90 minutes and 75% treated between 2 and 3 ho~rs .3~ Despite the longer time interval to treatment in the Cincinnati study, rates of 24-hour improvement and symptomatic ICH were similar to those in the NINDS trial; however, patients treated earlier had an increased probability of improvement, with an odds ratio of 0.62/hour.

388 HICKENBOTTOM & BARSAN
In summary, the trials of IV rt-PA for acute ischemic stroke demonstrate im- proved outcome following treatment in selected patients treated within 3 hours of stroke onset. Although treatment with IV rt-PA appears to be safe when given up to 6 hours after stroke onset, efficacy data are questionable after 3 hours. Both the NINDS and ECASS investigators have undertaken analyses to identify patients who may be at higher risk for ICH with treatment. The only variables indepen- dently associated with an increased risk of symptomatic ICH were the severity of neurologic deficit at presentation and the presence of brain edema or mass effect on CT before treatment.57 Thus, patients with large areas of acute hypodensity on the baseline CT (ECASS criteria > 1/3 of the middle cerebral artery distribution territory) should not be treated with rt-PA. Patients with very severe strokes at baseline are probably at higher risk for ICH, but also may be considered those with the most to gain from treatment. These patients can still be treated with rt- PA within the 3-hour time window, provided they do not have large areas of hypodensity on baseline CT, but family members or other decision makers should be informed of the added risk of treatment.
lntraarterial Thrombolysis
Direct intraarterial infusion of thrombolytic agents into an occluded blood vessel may serve as an alternative or an adjunct to IV thrombolysis. This approach has the theoretical advantage of delivering higher concentrations of drug directly to the clot and thus minimizing potential systemic complications. Of course, these advantages must be balanced against longer time to treatment, increased cost, and decreased availability of therapy. Nonrandomized studies intraarterial thrombo- lysis in acute ischemic stroke have demonstrated higher recanalization rates than IV therapy; generally, rates of 50% to 71% have been r e p ~ r t e d . ~ , ~ ~ , ~ ~ , ~ , ~ Rates of ICH with intraarterial therapy have ranged from 2% to 11%. The primary agents used in intraarterial infusion are rt-PA, urokinase, and prourokinase. Both rt-PA and urokinase are commercially available but neither has been approved by the FDA for use in the cerebral circulation. Prourokinase (Prolyse) is the inactive single chain precursor of urokinase and has significant fibrin specificity, whereas uroki- nase is not fibrin specific. Prourokinase has recently been evaluated in a series of trials of intraarterial thrombolysis in acute ischemic stroke. The Prolyse in Acute Cerebral Thromboembolism Trial (PROACT) was a Phase I1 trial that enrolled patients who presented within 6 hours of symptom onset and had angiographi- cally documented occlusion of the middle cerebral artery.17 Forty-six patients were randomized in 2:l fashion to receive either 6 mg of intraarterial prourokinase or placebo. No mechanical clot disruption was allowed. Initially, all patients received a bolus of heparin at 100 U/kg followed by a constant heparin infusion at 1000 U/hr for 4 hours. After 16 patients had been treated, the External Safety Com- mittee decreased the heparin dosing to a 2000 U bolus and a 500 U/hr infusion because of concerns about high rates of symptomatic ICH. Overall, partial or com- plete recanalization at 120 minutes after treatment was seen in 58% of the pro- urokinase group and 14% of the placebo group (2P = 0.017), with the highest recanalization rates seen in the prourokinase group that also received high-dose heparin (82%). This group also had the highest rate of symptomatic ICH at 24 hours (27% versus 6.7% for patients that received prourokinase and the low-dose heparin regimen). There were no differences between the prourokinase and pla- cebo groups with regard to 90 day hemorrhagic transformation or mortality rates.

ACUTE ISCHEMIC STROKE THERAPY 389
Following the promising results of the PROACT I trial, PROACT I1 was un- dertaken. This study was a Phase I11 multicenter, randomized, double-blind, pla- cebo-controlled trial; preliminary results have been published.” Patients who pre- sented within 6 hours of symptom onset and had angiographically documented occlusion of the middle cerebral artery were randomized in 2:l fashion to receive either a 120-minute intraarterial infusion of 9 mg of prourokinase or placebo. The low-dose heparin regimen employed in PROACT I was also used, and mechanical clot disruption again was not allowed. The primary outcome measure was a MRS of 2 or less at 90 days, and all patients underwent repeat angiography to assess recanalization. One hundred eighty patients were enrolled. The median NIHSS score was 17 and the median time to treatment was 5.3 hours for both groups. Patients treated with prourokinase were significantly more likely to have a good outcome at 90 days than were placebo-treated patients (40% versus 25%, P = 0.043). The rate of symptomatic ICH at 36 hours in the prourokinase group was 10.2% as compared with 1.8% in the placebo group, but there was no difference in 90-day mortality rates. The results of this trial indicate that intraarterial throm- bolysis may be safe and efficacious for use in selected patients with acute stroke up to 6 hours after symptom onset.
Even if intraarterial therapy proves to be beneficial, several barriers to its widespread adoption exist. One major disadvantage is the delay associated with angiography and delivery of the thrombolytic agent to the clot. In addition, so- phisticated interventional neuroradiology techniques are not universally available. A geographic analysis of the United States indicated that only 37% of the American population would have access to such therapy if a 3-hour time window were to be met,ffi whereas access to IV thrombolysis within the same time window is nearly universal. As a result of the concerns about treatment delay and accessibility with intraarterial therapy, the Emergency Management of Stroke (EMS) investigators performed a small pilot study of combined IV and intraarterial thrombolyhc ther- apy compared with intraarterial therapy This trial was initiated prior to the NINDS rt-PA stroke study and was terminated once that trial began. Thirty- five patients presenting within 3 hours of stroke onset were randomized to receive either 0.6 mg/kg of IV rt-PA or placebo and were then taken immediately to angiography. If acute thrombus was visualized, patients went on to receive intra- arterial rt-PA. The dose was determined by the amount of rt-PA required to es- tablish vessel patency, with a maximum dose of 20 mg over 120 minutes. Me- chanical disruption of the clot by the guidewire or catheter was part of the protocol. If acute thrombus was not visualized at angiography, no further therapy was undertaken. Of the 35 patients enrolled, only 22 had thrombus present at angiography. In the combination IV intraarterial therapy group, 67% had partial or complete recanalization at 2 hours as compared with 60% of the intraarterial only group. Three patients had life-threatening hemorrhages, all in the combina- tion therapy group. Although the small number of patients studied in the EMS trial make it difficult to draw any meaningful conclusions about the efficacy of combination therapy, the trial did demonstrate that such a protocol is feasible and would allow for rapid initiation of IV thrombolytic therapy while arrangements for intraarterial therapy were being made.
Other Thrombolytic Agents and Recanalization Strategies
Several second-generation thrombolytic agents are under investigation. A small dosing safety study of the second-generation thrombolytic E6010, which has

390 HICKENBOTTOM & BARSAN
a prolonged half-life compared with rt-PA, has been performed in stroke patients presenting within 6 hours of symptom Recanalization rates and rates of symptomatic ICH were increased in the higher dosing tier. TNK-t-PA is a more fibrin-specific variant of t-PA that also has a longer half life, with decreased plasma clearance and increased resistance to plasminogen activator inhibitor type 1 (PAI- 1) that allows for dosing as a single Evaluation of this agent in acute ischemic stroke is underway. Mechanical strategies for establishing reperfusion in acute stroke may be adapted from interventions for acute coronary thrombosis. Angioplasty of acutely occluded coronary vessels has demonstrated efficacy in randomized trials.” The use of angioplasty to recanalize acutely occluded cerebral vessels has been rep~r ted .~ An additional catheter strategy would be the use of an AngioJet (Possis Medical Inc., Minneapolis, Minnesota) catheter to perform throm- bectomy of the acutely occluded ~esse1.5~ Angioplasty and other mechanical strat- egies have not been systematically studied in stroke, and any future trials will likely have to await the development of smaller catheters that will be better able to navigate the cerebral vasculature.
ANTlTH ROMBOTIC THERAPIES
Antithrombotic therapies are used to prevent progressive or recurrent throm- bosis; this category includes heparin and heparinoids, aspirin and newer anti- platelet agents, and defibrinogenating drugs. Multiple studies have demonstrated efficacy for various anticoagulation and antiplatelet agents in secondary preven- tion of ischemic stroke, and several recent studies have helped to clarify the role of these agents in the acute treatment of stroke.
Heparins and Heparinoids
Unfractionated (UF) heparin has been used for decades in the treatment of ischemic stroke, but its use remains controversial.z~70 Recently, the International Stroke Trial (IST) examined the benefit of heparin in acute ischemic This unblinded trial randomized 19,435 patients within 48 hours of stroke onset to receive 12,500 U subcutaneous UF heparin twice daily, 5000 U subcutaneous UF heparin, or no heparin for 14 days and aspirin or no aspirin in a 3 x 2 factorial design. Patients receiving heparin had significantly fewer recurrent ischemic strokes (2.9% versus 3.8%, P = 0.005), but this benefit was offset completely by an identical increase in the number of hemorrhagic strokes in the heparin group. Overall, there was no significant difference between the heparin and no heparin groups in death or nonfatal stroke recurrence at 14 days or in 6-month death or dependency rates. Based on these results, the authors did not support the use of heparin in unselected stroke patients.
Various authors have argued for or against the use of heparin in special cir- cumstances, such as partial stroke:’ progressing ~ t r o k e , ’ ~ , ~ , ~ recent or crescendo transient ischemic attacks TIA AS),^.^^,^,^^ cardioembolic s t r ~ k e , ’ ~ , ’ ~ , ~ , ~ ~ and verte- brobasilar syndrome^.*^,^^ Only one of these trials was performed in double-blind, placebo-controlled fashion: a trial of 225 patients who had partial stroke with stable symptoms.21 Patients were randomized to receive either placebo or a con- tinuous IV infusion of UF heparin at a dose adjusted to keep the activated partial thromboplastin time (APTT) between 1.5 and 2.5 times control for 7 days. No significant difference was seen between the treated and placebo groups with re-

ACUTE ISCHEMIC STROKE THERAPY 391
gard to progression of stroke symptoms over 7 days; degree of neurologic change; or functional outcome at 7 days, 3 months, or 1 year after treatment. Unfortunately, the rest of these studies were retrospective, observational, or uncontrolled pro- spective studies often involving small numbers of patients, so that drawing mean- ingful conclusions regarding heparin treatment in these clinical scenarios is diffi- cult. Overall, these trials do not appear to support the use of heparin for acute ischemic stroke. The only prospective trial of progressing stroke involved 36 pa- tients, with 50% of those patients' symptoms continuing to progress despite ade- quate anticoagulation with IV heparin.30 A retrospective study of 289 TIA patients did not demonstrate lower mortality, stroke, or recurrent TIA rates in heparin- treated patient^.^^ In an observational study of 74 patients with TIA, including recurrent or crescendo TIA, 17% continued to have TIAs while receiving adequate anticoagulation with IV heparin and 7% went on to suffer infarction.61 Previous studies of cardioembolic stroke estimated that 12% to 14% of patients would suffer a recurrent embolic event within 2 weeks of the initial event; however, these stud- ies included patients with mechanical valves and thus may have overestimated the rate of re~urrence. '~,~~ More recent estimates of recurrence rates for cardioem- bolic stroke have been in the range of 1% to 2% per week." Given the lower risk for early recurrent embolism and the greater risk for early hemorrhagic transfor- mation in cardioembolic stroke,% the routine use of heparin in presumed car- dioembolic stroke cannot be recommended and should be reserved for cases in which a clear embolic source is identified (e.g., actively mobile or mural throm- bus). Recent megatrials for stroke indicate that the risk for early recurrent stroke in the general stroke population is also low (1.07 recurrent strokes per 100 patients per week), obviating the previously perceived need for urgent anticoagulation with heparin.70
Low-molecular-weight heparin (LMWH) is produced by the chemical or en- zymatic cleavage of UF heparin. LMWH preparations have distinct pharmacoki- netic advantages over UF heparin." Owing to their shorter chain length, they have less affinity for plasma proteins, endothelial cells, and platelets and thus have a longer half-life allowing daily or twice daily administration. In addition, the re- sponse to fixed dose therapy is relatively consistent and predictable, so laboratory monitoring is not required. Finally, the decreased interaction with platelets leads to fewer bleeding complications and there is no risk for heparin-induced throm- bocytopenia. One randomized trial of a LMWH for acute ischemic stroke has been completed;40 306 stroke patients who presented within 48 hours of symptom onset were randomized to receive either high-dose or low-dose LMWH (nadroparin) or placebo for 10 days. The primary endpoint was poor outcome defined as death or dependency at 6 months, with the same outcome at 3 months serving as a sec- ondary endpoint. No significant difference in outcome was seen at 3 months; how- ever, at 6 months, there was a significant dose-dependent reduction in the per- centage of patients left dead or dependent in favor of high-dose nadroparin (P = 0.005). There was no difference between the groups with regard to hemorrhagic transformation or systemic bleeding complications. Further testing of LMWH in stroke is underway.
Heparinoids are natural or semisynthetic glycosaminoglycans that are struc- turally related to heparin and possess similar antithrombotic properties." ORG 10172 (danaproid) is the heparinoid that has been most extensively studied in acute ischemic stroke. In the Trial of ORG 10172 in Acute Stroke Treatment (TOAST), 1281 patients with ischemic stroke who presented within 24 hours of symptom onset were randomized to receive either the drug or placebo intrave- nously for 7 days.60 The primary outcome measure was dichotomized favorable outcome on the GOS and BI at 3 months. No difference between the groups was

392 HICKENBOTTOM & BARSAN
seen at 3 months, although subgroup analysis did suggest benefit to treatment with ORG 10172 in patients with presumed large artery atherothrombotic stroke. The rate of major bleeding events, including ICH, was significantly higher in pa- tients treated with ORG 10172 (P = 0.05).
Antiplatelet Agents
The role of aspirin as acute stroke therapy was recently evaluated in two large trials. In the IST, discussed earlier,= 19,439 patients with ischemic stroke who pre- sented within 48 hours were randomized in unblinded fashion to receive 300 mg of aspirin daily or placebo and moderate-dose or low-dose heparin or no heparin, for 14 days. A statistically sigrdicant reduction in the rate of recurrent ischemic stroke was seen in the group treated with aspirin (2.8% versus 3.9% in the placebo group, P < 0.001) without significant increase in the rate of hemorrhagic stroke. The results of the IST were also combined with those from the Chinese Acute Stroke Trial (CAST).13 This trial was a multicenter, randomized, double-blind, pla- cebo-controlled trial of 21,106 patients with acute ischemic stroke who presented within 48 hours of symptom onset. Patients received either 160 mg of aspirin or placebo daily for 4 weeks. The primary endpoints were death in hospital (up to 4 weeks after stroke) or death or disability at discharge. There was a significant decrease with aspirin treatment, again without increase in the risk for hemorrhagic stroke. Although the absolute risk reduction for recurrent ischemic stroke in the IST and CAST studies was only 1% to 2%, the results were statistically significant and do indicate that aspirin is beneficial in the treatment of acute stroke. When considered on a larger public health scale, a 1% to 2% decline in the number of strokes would result in 7500 fewer strokes per year in the United States, signifi- cantly reducing the personal and economic burden of stroke.
Agents with other antiplatelet effects also have been studied in acute stroke. The results of a Phase I1 dose-escalation safety study of the platelet GpIIJII, re- ceptor inhibitor, abciximab, have been reported recently.' In this trial, patients with ischemic stroke presenting between 3 and 24 hours after symptom onset were randomized in 3:l fashion to either escalating doses of abciximab or placebo, with stratification for stroke onset (3-12 hours and >12 hours) and stroke severity (NIHSS 4-14 and greater than 14). The primary safety endpoint was incidence of major (symptomatic) ICH at 5 days. No patient in either group suffered a major ICH, and preliminary efficacy data suggested a trend toward better outcome with abciximab. A multicenter Phase I11 trial of abciximab for acute ischemic stroke is scheduled to begin soon.
Defibirinogenating Agents
The defibrinogenating agent, ancrod, is extracted from the venom of the Ma- layan pit viper. A Phase I11 trial of ancrod administered within 6 hours of stroke onset did not reveal benefit to treatment, although the lowering of fibrinogen levels was less than de~ired.~ In the more recent Stroke Treatment with Ancrod Trial (STAT), 500 patients with ischemic stroke who presented within 3 hours of symptom onset were randomized to receive a 3-day infusion of ancrod followed by bolus infusions on days 4 and 5, with all doses adjusted according to fibrinogen

ACUTE ISCHEMIC STROKE THERAPY 393
level, or placebo." The target fibrinogen level for the study was 40 to 70 mg/dL, lower than in the aforementioned trial. The primary outcome measure was di- chotomized good outcome on the BI (295) at 3 months. Preliminary results dem- onstrated that the percentage of patients with a good outcome was 41.1% with ancrod treatment and 35.3% with placebo, a statistically significant difference (P = 0.041). The rate of symptomatic ICH were 5.2% with ancrod, as compared with 2.0% with placebo (P = 0.001); ICH rates were increased when the lower fibrinogen target level was overshot. No difference was seen in mortality at any point. It is difficult to compare these results to those of the NINDS trial because different endpoints were used; further evaluation of the preliminary STAT data will need to be performed before any clinical recommendations can be made re- garding the use of ancrod in acute stroke.
SUMMARY
Acute ischemic stroke is a medical emergency that requires rapid diagnosis and treatment. Prehospital and emergency department stroke care can be stream- lined to evaluate and treat the acute stroke patient in a timely fashion. Intravenous thrombolysis with rt-PA is currently the only approved therapy for acute ischemic stroke, but other therapies are on the horizon. Intraarterial thrombolysis with prourokinase has shown promise in treating acute stroke, as has the defibrinogen- ating agent ancrod. Aspirin provides some benefit to patients with acute stroke, and newer antiplatelet agents are under investigation. Other thrombolytic and antithrombotic agents are currently in various stages of development. Pessimistic attitudes toward the treatment of acute ischemic stroke have been slow to give way, but new therapies and emerging proactive attitudes toward stroke care have brought us to the doorstep of a therapeutic revolution. It will be exciting to see what more develops as we move into the next era of acute stroke treatment.
References
1. Adams H Preliminary safety report of an ongoing dose-escalation trial of abciximab in acute ischemic stroke. Stroke 30:244 [abstrl, 1999
2. Adams H, Brott T, Crowell R, et a1 AHA Medical/Scientific Statement: Guidelines for management of patients with acute ischemic stroke: A statement for healthcare profes- sionals from a special writing group of the Stroke Council, American Heart Association. Stroke 251901-1914,1994
3. Adams HP, Brott TG, Furlan AJ, et al: Guidelines for thrombolytic therapy for acute stroke: A supplement for the guidelines for the management of patients with acute is- chemic stroke. A statement for healthcare professionals from a special writing group of the Stroke Council of the American Heart Association. Stroke 271711-1718,1996
4. Ancrod Stroke Study Investigators: Ancrod for the treatment of acute ischemic brain infarction. Stroke 25:1755-1759,1994
5. Balousek P, Knowles H, Higashida R, et al: New interventions in cerebrovascular dis- eases: The role of thrombolytic therapy and balloon angioplasty. Curr Opin Cardiol
6. Barnwell SL, Clark WM, Nguyen TT, et a1 Safety and efficacy of delayed intraarterial urokinase therapy with mechanical clot disruption for thromboembolic stroke. AJNR Am J Neuroradiol151817-1822,1994
11~550-557,1996

394 HICKENBOTTOM & BARSAN
7. Biller J, Bruno A, Adams HP, et al: A randomized trial of aspirin or heparin in hospital- ized patients with recent transient ischemic attacks. A pilot study. Stroke 20:441-447, 1989
8. Bock BF Response system for patients presenting with acute ischemic stroke. In Marler JR, Winters Jones P, Emr M (eds): Proceedings of a National Symposium on Rapid Iden- tification and Treatment of Acute Stroke. Bethesda, MD, The National Institute of Neu- rological Disorders and Stroke, 1997, pp 55-57
9. Broderick JP: Logistics in acute stroke management. Drugs 54(Suppl3): 109-116,1997 10. Broderick J, Brott T, Barsan W, et a1 Blood pressure during the first minutes of focal
cerebral ischemia. Ann Emerg Med 221438-1443,1993 11. Brott T, Adams HP, Olinger CP, et al: Measurements of acute cerebral infarction: A clinical
scale. Stroke 20:864-870,1989 12. Brott TG, Haley EC Jr, Levy DE, et al: Urgent therapy for stroke, part I: Pilot study of
tissue plasminogen activator administered within 90 minutes. Stroke 23:632-640,1992 13. CAST (Chinese Acute Stroke Trial) Collaborative Group: CAST Randomised, placebo-
controlled trial of early aspirin use in 20,000 patients with acute ischemic stroke. Lancet
14. Cerebral Embolism Study Group: Immediate anticoagulation of embolic stroke: A ran- domized trial. Stroke 14:668-676,1993
15. Cerebral Embolism Study Group: Immediate anticoagulation of embolic stroke: Brain hemorrhage and management options. Stroke 15:779-789,1994
16. Clark WM, Albers GW, for the ATLANTIS Stroke Study Investigators: The ATLANTIS rt-PA (Alteplase) acute stroke trial: Final results. Stroke 30:234[abstrl, 1999
17. del Zoppo G, Higashida R, Furlan A, et a1 PROACT A phase I1 randomized trial of recombinant prourokinase by direct arterial delivery in acute middle cerebral artery stroke. Stroke 29:4-11, 1998
18. del Zoppo GJ, Ferbert A, Otis S, et al: Local intra-arterial fibrinolytic therapy in acute carotid territory stroke: A pilot study. Stroke 19:307-313,1988
19. Dobkin BH Heparin for lacunar stroke in progression. Stroke 14:421-423,1983 20. Donnan GA, Davis SM, Chambers BR, et al: Streptokinase for acute ischemic stroke with
relationship to time of administration. JAMA 276961-966,1996 21. Duke RJ, Bloch RF, Turpie AG, et a1 Intravenous heparin for the prevention of stroke
progression in acute partial stable stroke: A randomized controlled trial. Ann Intern Med
22. Emergency Management of Stroke (EMS) Investigators: Combined intra-arterial and in- travenous t-PA for stroke. Stroke 28:273[abstr], 1997
23. The European Cooperative Acute Stroke Study (ECASS): Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. JAMA 274:1017- 1025,1995
24. Furlan AJ, Higashida F, Wechsler L, et al: PROACT 11: Recombinant prourokinase (r-Pro- UK) in acute cerebral thromboembolism. Initial trial results. The PROACT I1 Investiga- tors. Stroke 30234[abstr], 1999
25. Goldstein LB, Samsa GI? Reliability of the National Institutes of Health Stroke Scale. Extension to non-neurologists in the context of a clinical trial. Stroke 28:307-310, 1997
26. Grossman E, Messerli F, Grodzicki T, et a1 Should a moratorium be placed on sublingual nifedipine capsules given for hypertensive emergencies and pseudoemergencies? JAMA
27. Hachinski V, Norris J: The deteriorating stroke. In The Acute Stroke. Philadelphia; FA Davis, 1985, p 123
28. Hacke W, Bluhmki E, Steiner T, et al: Dichotomized efficacy end points and global end- point analysis applied to the ECASS intention-to-treat data set: Post-hoc analysis of ECASS I. Stroke 29:2073-2075,1998
29. Hacke W, Kaste M, Fieshci C, et a1 Randomised, double-blind, placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischemic stroke. (ECASS 11). Second European-Australian Acute Stroke Study investigators. Lancet 352:1245-1251, 1998
30. Haley EC, Jr, Kassell NF, Torner JC: Failure of heparin to prevent progression in pro- gressive ischemic infarction. Stroke 19:lO-14,1988
349:1641-1649,1997
1052325-828,1986
276:1328-1331,1996

ACUTE ISCHEMIC STROKE THERAPY 395
31. Haley EC Jr, Levy DE, Brott TG, et a1 Urgent therapy for stroke, part 11: Pilot study of tissue plasminogen activator administered 91-180 minutes after onset. Stroke 23:641- 645,1992
32. Haley EC Jr, Lewandowski C, Tilley BC, et al: Myths regarding the NINDS rt-PA stroke trial Setting the record straight. Ann Emer Med 30:676-682,1997
33. Harper G, Castleden CM, Potter J F Factors affecting changes in blood pressure after acute stroke. Stroke 25:1726-1729,1994
34. Hart RG, Easton J D Hemorrhagic infarcts. Stroke 17586-589,1986 35. International Stroke Trial Collaborative Group: The International Stroke Trial (IST): A
randomized trial of aspirin, subcutaneous heparin, both or neither among 19,435 patients with acute ischaemic stroke. Lancet 349:1569-1581,1997
36. Jones HR, Millikan CH, Sandok BA Temporal profile of acute vertebrobasilar system cerebral infarction. Stroke 11:173-177,1980
37. Kanter DS, Kohtari R, Pancioli A, et al: The greater Cincinnati t-PA experience after the NINDS trial: Does a longer time to treatment within the current three-hour window reduce efficacy? Stroke 30244[abstr], 1999
38. Kasner SE, Grotta JC: Ischemic stroke. Neurol Clin 16:355-372,1998 39. Katzen IL, Furlan AJ, Way LE, et a1 A systematic audit of IV tPA use in Cleveland area
hospitals. Stroke 30:266[abstr], 1999 40. Kay R, Wong KS, Yu YL, et al: Low-molecular-weight heparin for the treatment of acute
ischemic stroke. N Engl J Med 333:1588-1593,1995 41. Keith DS, Phillips SJ, Whisnant JF', et a1 Heparin therapy for recent transient cerebral
ischemia. Mayo Clin Proc 58637-641,1987 42. Kidwell CS, Saver JL, Eckstein M, et a1 High accuracy of emergency medical technician
identification of stroke using the Los Angeles Prehospital Stroke Scale (LAPSS). Stroke 29313,1998
43. Kothari RU, Pancioli A, Liu T, et a1 Cincinnati Prehospital Scale: Validity and repro- ducibility. Stroke 29:313,1998
44. Kwiatkowski TG, Libman RB Emergency strategies. In Welch KMA, Caplan LR, Reis DJ, Siesjo BK, Weir B (eds): Primer on Cerebrovascular Diseases. San Diego, Academic Press, 1997, pp 671-675
45. Lisk DR, Grotta JC, Lamki LM, et al: Should hypertension be treated after acute stroke? A randomized controlled trial using single photon emission computed tomography. Arch Neurol50:855-862,1993
46. Lopez-Yunez AM, Bruno A, Z u m C, et al: Protocol violations in community-based rt- PA use are associated with symptomatic intracerebral hemorrhage. Stroke 30:264[abstrl, 1999
47. Marler JR, Tilley B, Lu M, et al: Earlier treatment associated with better outcome in the NINDS TPA stroke study. Stroke 30:244[abstrl, 1999
48. Miller VT, Hart RG: Heparin anticoagulation in acute brain ischemia. Stroke 19:403-406, 1988
49. Mori E, Tabuchi M, Yoshida T, et a1 Intracarotid urokinase with thromboembolic occlu- sion of the middle cerebral artery. Stroke 19:802-812,1988
50. Mori E, Takakura K, Yamaguchi T, et al: Multicenter trial of a novel modified t-PA, E6010, by JY bolus injection in patients with acute carotid artery territory stroke. Cerebrovasc Dis 639, 1996
51. The Multicenter Acute Stroke Trial-Europe Study Group: Thrombolytic therapy with streptokinase in acute ischemic stroke. N Engl J Med 335:145-150,1996
52. Multicentre Acute Stroke Trial-Italy (MAST-I) Group: Randomised controlled trial of streptokinase, aspirin, and combination of both in treatment of acute ischemic stroke. Lancet 3461509-1514,1995
53. Nakagawa Y, Matsuo S, Kimura T, et al: Thrombectomy with AngioJet catheter in native coronary arteries for patients with acute or recent myocardial infarction. Am J Cardiol
54. The National Institute of Neurologic Disorders and Stroke (NINDS) rt-PA Stroke Study Group: Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 333:1581- 1587,1995
55. The National Institute of Neurologic Disorders and Stroke (NINDS) rt-PA Stroke Study
83~994-999,1999

396 HICKENBOTTOM & BARSAN
Group: A systems approach to immediate evaluation and management of hyperacute stroke: Experience at eight centers and implications for community practice and patient care. Stroke 28:1530-1540,1997
56. Nehler M, Moneta G, McConnell D, et a1 Anticoagulation followed by elective carotid surgery in patients with repetitive transient ischemic attacks and high grade carotid stenosis. Arch Surg 128:1117-1123, 1993
57. The NINDS t-PA Stroke Study Group: Intracerebral hemorrhage after intravenous t-PA therapy for ischemic stroke. Stroke 282109-2118,1997
58. Phillips SJ: An alternative view of heparin anticoagulation in acute focal brain ischemia. Stroke 20:295-298,1989
59. Powers W Acute hypertension after stroke: The scientific basis for treatment decisions. Neurology 43:461-467,1993
60. The Publications Committee for the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) Investigators: Low molecular weight heparinoid, ORG 10172 (danaproid), and outcome after acute ischemic stroke. A randomized controlled trial. JAMA 279:1265- 1272,1998
61. Putnam SF, Adams HP: Usefulness of heparin in initial management of patients with recent transient ischemic attacks. Arch Neurol42:960-962,1985
62. Report of the Quality Standards Subcommittee of the American Academy of Neurology: Practice advisory: Thrombolytic therapy for acute ischemic stroke-summary statement. Neurology 47835-839,1996
63. Sasaki 0, Takeuchi S, Koike T, et a1 Fibrinolytic therapy for acute embolic stroke: Intra- venous, intracarotid and intra-arterial local approaches. Neurosurgery 361581-1587, 1995
64. Sayre MR, Honeycutt LK, Swor RA: Prehospital identification and treatment. In Marler JR, Winters Jones P, Emr M (eds): Proceedings of a National Symposium on Rapid Iden- tification and Treatment of Acute Stroke. Bethesda, MD, The National Institute of Neu- rological Disorders and Stroke, 1997, pp 35-43
65. Scott PA, Lowell MJ, Longstreth K Analysis of U.S. population with geographic access to interventional neuroradiology and intra-arterial thrombolysis for acute ischemic stroke. Stroke 28:266[abstrl, 1997
66. Sherman DG, for the STAT Writers Group: Defibrinogenation with Viprinex (ancrod) for the treatment of acute, ischemic stroke. Stroke 30:234[abstr], 1999
67. Smalling RW A fresh look at the molecular pharmacology of plasminogen activators: From theory to test tube to clinical outcomes. Am J Health-System Pharm 54(Suppl
68. Steiner T, Bluhmki E, Kaste M, et al: The ECASS 3-hour cohort. Secondary analysis of ECASS data by time stratification. ECASS Study Group. European Cooperative Acute Stroke Study. Cerebrovasc Dis 8198-203,1998
69. Strandgaard 5 Autoregulation of cerebral blood flow in hypertensive patients. Circu- lation 53:720-727,1976
70. Swanson RA: Intravenous heparin for acute stroke. What can we learn from the mega- trials? Neurology 521746-1750,1999
71. Tilley BC, Lyden PD, Brott TG, et al: Total quality improvement method for reduction of delays between emergency department admission and treatment of acute ischemic stroke. Arch Neurol54:1466-1474,1997
72. Trunkey D D Trauma: A public health problem. In Moore EE, et a1 (eds): Early Care of the Injured Patient. Toronto, BC Decker, 1990, pp 3-11
73. Weaver W, Simes J, Betriu A, et al: Comparison of primary coronary angioplasty and intravenous thrombolytic therapy for acute myocardial infarction. JAMA 2782093-2098, 1997
74. Weaver WD, Kennedy JW: Myocardial infarction: Thrombolytic therapy in the prehos- pita1 setting. In Furster, Verstraebe M (eds): Thrombosis in Cardiovascular Disorders. Philadelphia, WB Saunders, 1992, pp 275-287
l):S17-S22,1997
75. Wietz JI: Low-molecular-weight heparins. N Engl J Med 337688-698,1997 76. Zachariah BS, Van Cott CC, Dunford J: Dispatch life support and the acute stroke patient:
Making the right call. In Marler JR, Winters Jones P, Emr M (eds): Proceedings of a National Symposium on Rapid Identification and Treatment of Acute Stroke. Bethesda, MD, The National Institute of Neurological Disorders and Stroke, 1997, pp 29-33

ACUTE ISCHEMIC STROKE THERAPY 397
77. Zeumer H, Freitag HJ, Zanella F, et a1 Local intra-arterial fibrinolytic therapy in patents with stroke: Urokinase versus recombinant tissue plasminogen activator (r-TPA). Neu- roradiology 35:159-162, 1993
Address reprint requests to
William G . Barsan, MD Department of Emergency Medicine
University of Michigan Medical Center TC B1354/0303
1500 E. Medical Center Dr. Ann Arbor MI 48109
e-mail: [email protected]
Related Documents











