Acute Appendicitis

Acute Appendicitis. Epidemiology The incidence of appendectomy appears to be declining due to more accurate preoperative diagnosis. Despite newer imaging.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Acute Appendicitis

Epidemiology
• The incidence of appendectomy appears to be declining due to more accurate preoperative diagnosis.
• Despite newer imaging techniques, acute appendicitis can be very difficult to diagnose.
Appendicitis:
• The most common surgical condition of the abdomen
• Lifetime occurrence of 7%
• Peak incidence 10-30y
• The most common nonobstetric surgical intervention during pregnancy

Pathogenesis:• Appendiceal lumen obstruction : lymphoid hyperplasia fecaliths parasites foreign bodies crohn’s disease metastatic cancer carcinoid syndrome

Pathophysiology
• Acute appendicitis is thought to begin with obstruction of the lumen
• Obstruction can result from food matter, adhesions, or lymphoid hyperplasia
• Mucosal secretions continue to increase intraluminal pressure

Pathophysiology
• Eventually the pressure exceeds capillary perfusion pressure and venous and lymphatic drainage are obstructed.
• With vascular compromise, epithelial mucosa breaks down and bacterial invasion by bowel flora occurs.

Pathophysiology
• Increased pressure also leads to arterial stasis and tissue infarction
• End result is perforation and spillage of infected appendiceal contents into the peritoneum

Pathophysiology
• Initial luminal distention triggers visceral afferent pain fibers, which enter at the 10th thoracic vertebral level.
• This pain is generally vague and poorly localized.
• Pain is typically felt in the periumbilical or epigastric area.

Pathophysiology
• As inflammation continues, the serosa and adjacent structures become inflamed
• This triggers somatic pain fibers, innervating the peritoneal structures.
• Typically causing pain in the RLQ

Pathophysiology
• The change in stimulation form visceral to somatic pain fibers explains the classic migration of pain in the periumbilical area to the RLQ seen with acute appendicitis.
Pathophysiology
• Exceptions exist in the classic presentation due to anatomic variability of the appendix
• Appendix can be retrocecal causing the pain to localize to the right flank
• In pregnancy, the appendix ca be shifted and patients can present with RUQ pain
Pathophysiology
• In some males, retroileal appendicitis can irritate the ureter and cause testicular pain.
• Pelvic appendix may irritate the bladder or rectum causing suprapubic pain, pain with urination, or feeling the need to defecate
• Multiple anatomic variations explain the difficulty in diagnosing appendicitis
symptoms :
• Pain – RLQ / RUQ / Flank• Anorexia• Vomiting• Nausea • Pain migration• Fever

Physical examination:
• Tenderness – RLQ• Rebound & Guarding (peritoneal signs)• Rovsing sign• Dunphy’s sign• Psoas sign (retroperitoneal retrocecal appendix) • Obturator sign (pelvic appendix)• Rectal examination tenderness (cul-de-sac)• Low grade fever
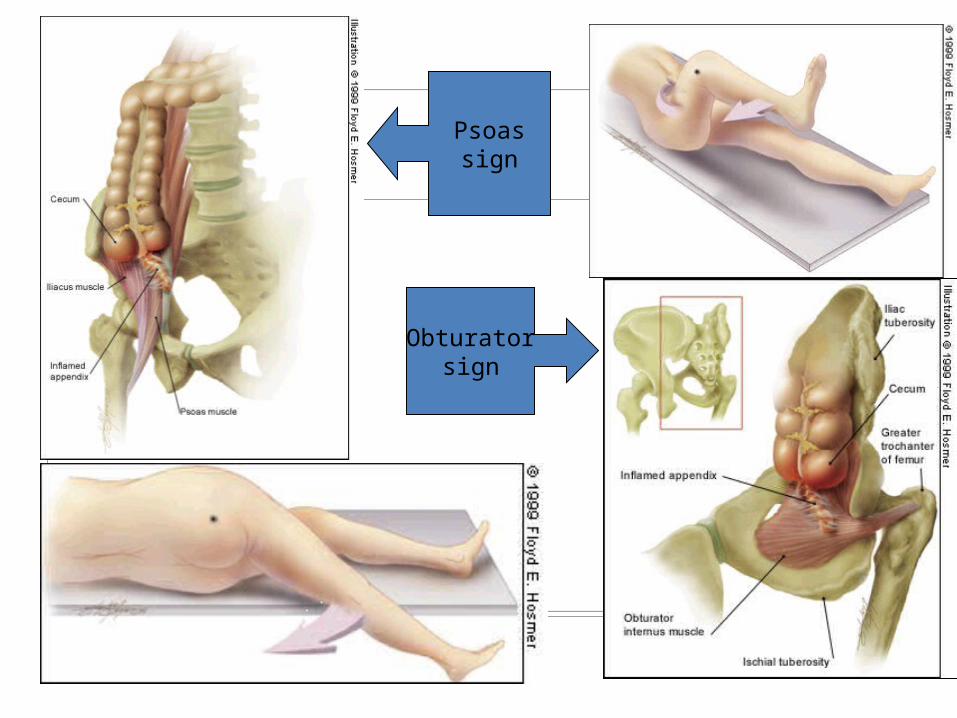
Psoassign
Obturatorsign

History
• Primary symptom: abdominal pain• ½ to 2/3 of patients have the classical
presentation• Pain beginning in epigastrium or periumbilical
area that is vague and hard to localize

History
• Associated symptoms: indigestion, discomfort, flatus, need to defecate, anorexia, nausea, vomiting
• As the illness progresses RLQ localization typically occurs
• RLQ pain was 81 % sensitive and 53% specific for diagnosis
History
• Migration of pain from initial periumbilical to RLQ was 64% sensitive and 82% specific
• Anorexia is the most common of associated symptoms
• Vomiting is more variable, occuring in about ½ of patients
Physical Exam
• Findings depend on duration of illness prior to exam.
• Early on patients may not have localized tenderness
• With progression there is tenderness to deep palpation over McBurney’s point
Physical Exam
• McBurney’s Point: just below the middle of a line connecting the umbilicus and the ASIS
• Rovsing’s: pain in RLQ with palpation to LLQ• Rectal exam: pain can be most pronounced if
the patient has pelvic appendix
Physical Exam
• Additional components that may be helpful in diagnosis: rebound tenderness, voluntary guarding, muscular rigidity, tenderness on rectal
Physical Exam
• Psoas sign: place patient in L lateral decubitus and extend R leg at the hip. If there is pain with this movement, then the sign is positive.
• Obturator sign: passively flex the R hip and knee and internally rotate the hip. If there is increased pain then the sign is positive
Physical Exam
• Fever: another late finding.• At the onset of pain fever is usually not found.
• Temperatures >39 C are uncommon in first 24
h, but not uncommon after rupture
Lab:
• CBC – WBC ( 80% 45% )• CRP • Urinalysis - mild pyuria mild proteinuria mild hematuria

D.D.:surgical: gyneco:
• Renal stone • Gastroenteritis• Pancreatitis• Cholecystitis• Mesenteric adenitis• Hernia• Bowel obstruction
• Preterm labor• Placenta abruptio• Chorioamnionitis• Adnexal torsion • Ectopic pregnancy• Pelvic inflammatory• Round lig. pain
Diagnostic problems:
• Position of appendix: normally 70% intraperitoneal
30% pelvic, retroileal, retrocolic
pregnancy – anatomical changes
gravid uterus displacement upward &
outward flank pain (3rd trimester) (Baer,1932)
increased separation of peritoneum decreased perception of somatic pain and localization

Diagnostic problems:
• Symptoms complex – physical changes anorexia, nausea & vomiting in normal pregnancy• Lab – relative leukocytosis• Imaging techniques
Diagnosis
• Acute appendicitis should be suspected in anyone with epigastric, periumbilical, right flank, or right sided abd pain who has not had an appendectomy

Diagnosis
• Women of child bearing age need a pelvic exam and a pregnancy test.
• Additional studies: CBC, UA, imaging studies
Diagnosis
• CBC: the WBC is of limited value. • Sensitivity of an elevated WBC is 70-90%, but
specificity is very low.• But, +predictive value of high WBC is 92% and
–predictive value is 50%• CRP and ESR have been studied with mixed
results

Diagnosis
• UA: abnormal UA results are found in 19-40%• Abnormalities include: pyuria, hematuria,
bacteruria• Presence of >20 wbc per field should increase
consideration of Urinary tract pathology
Imaging:
• KUB• Barium enema• Graded compression ultrasonography• Helical CT scan
Diagnosis
• Imaging studies: include X-rays, US, CT• Xrays of abd are abnormal in 24-95%• Abnormal findings include: fecalith,
appendiceal gas, localized paralytic ileus, blurred right psoas, and free air
• Abdominal xrays have limited use b/c the findings are seen in multiple other processes

Graded compression ultrasound:• Normal appendix (<6mm) rules out
appendicitis. • Nonpregnant – Sensitivity 85% specificity 92%• Pregnant – cecal displacement & uterine
imposition makes precise examination difficult (Williams,21 edition)
Diagnosis
• Graded Compression US: reported sensitivity 94.7% and specificity 88.9%
• Basis of this technique is that normal bowel and appendix can be compressed whereas an inflamed appendix can not be compressed
• DX: noncompressible >6mm appendix, appendicolith, periappendiceal abscess
Diagnosis
• Limitations of US: retrocecal appendix may not be visualized, perforations may be missed due to return to normal diameter
Diagnosis
• CT: best choice based on availability and alternative diagnoses.
• In one study, CT had greater sensitivity, accuracy, -predictive value
• Even if appendix is not visualized, diagnose can be made with localized fat stranding in RLQ.
Diagnosis
• CT appears to change management decisions and decreases unnecessary appendectomies in women, but it is not as useful for changing management in men.

Special Populations
• Very young, very old, pregnant, and HIV patients present atypically and often have delayed diagnosis
• High index of suspicion is needed in the these groups to get an accurate diagnosis

Treatment
• Appendectomy is the standard of care• Patients should be NPO, given IVF, and
preoperative antibiotics • Antibiotics are most effective when given
preoperatively and they decrease post-op infections and abscess formation






Treatment
• There are multiple acceptable antibiotics to use as long there is anaerobic flora, enterococci and gram(-) intestinal flora coverage
• One sample monotherapy regimen is Zosyn 3.375g or Unasyn 3g
• Also, short acting narcotics should be used for pain management
Disposition
• Abdominal pain patients can be put in 4 groups
• Group 1: classic presentation for Acute appendicitis- prompt surgical intervention
• Group 2: suspicious, but not diagnosed appendicitis- benefit from imaging and 4-6h observation with surgical consult if serial exam changes or imaging studies confirm
Disposition
• Group 3: remote possibility of appendicitis- observe in ED for serial exams; if no change and course remains benign patient can D/C with dx of nonspecific abd pain
• Patients are given instructions to return if worsening of symptoms, and they should be seen by PCP in 12-24 h
• Also advised to avoid strong analgesia
Disposition
• Group 4: high risk population(including elderly, pediatric, pregnant and immunocomprimised)- require high index of suspicion and low threshold for imaging and surgical consultation
Prognosis:
• Generally good : Disease found Surgery complications
The end
Related Documents











