Prostate Cancer Activation of the Thromboxane A 2 Pathway in Human Prostate Cancer Correlates with Tumor Gleason Score and Pathologic Stage Thibaut Dassesse a,1 , Xavier de Leval b,1 , Laurence de Leval c , Bernard Pirotte b , Vincent Castronovo a,2 , David Waltregny a,d, * ,2 a Metastasis Research Laboratory, Center of Experimental Cancer Research, University of Lie `ge, B-4000 Lie `ge, Belgium b Natural and Synthetic Drugs Research Center, Laboratory of Medical Chemistry, University of Lie `ge, B-4000 Lie `ge, Belgium c Department of Pathology, University of Lie `ge, B-4000 Lie `ge, Belgium d Department of Urology, University of Lie `ge, B-4000 Lie `ge, Belgium european urology 50 (2006) 1021–1031 available at www.sciencedirect.com journal homepage: www.europeanurology.com Article info Article history: Accepted January 15, 2006 Published online ahead of print on February 23, 2006 Keywords: Prostate Cancer Cyclooxygenase Thromboxane Prognosis Please visit www.eu-acme.org/ europeanurology to read and answer questions on-line. The EU-ACME credits will then be attributed automatically. Abstract Objective: We investigated the potential involvement of the thrombox- ane A 2 (TXA 2 ) pathway in human prostate cancer (PCa). Methods: Expression of cyclooxygenase-2 (COX-2), TXA 2 synthase (TXS), and TXA 2 receptors (TPRs), the main actors of the TXA 2 pathway, was analyzed on serial tissue sections from 46 human PCa specimens. Results: The expression levels of COX-2, TXS, and TPRs were signifi- cantly higher in malignant than in corresponding nontumoral prostatic epithelial cells. Increased immunoreactivity for these antigens was also observed in high-grade prostate intraepithelial neoplasia (HGPIN) glands. COX-2, TXS, and TPR proteins usually displayed a coordinated overexpression pattern in PCa lesions, as assessed in serial tissue sections. Increased levels of these proteins in the tumors were all significantly associated with higher Gleason scores and pathologic stages. Conclusions: Proteins specifically involved in the TXA 2 pathway are up- regulated in human PCa and their level of expression is associated with tumor extraprostatic extension and loss of differentiation. Our study is the first to examine simultaneously all key proteins involved in this pathway including TXA 2 receptors and results suggest that the TXA 2 pathway may be a potential target for PCa prevention/therapy. # 2006 European Association of Urology. Published by Elsevier B.V. All rights reserved. * Corresponding author. Department of Urology, University Hospital of Lie ` ge, Bloc Central, 1, Bat. B35, CHU Sart Tilman Lie ` ge, B-4000 Lie ` ge, Belgium. Tel. +32 4 366 7251; Fax: +32 4 366 7258. E-mail address: [email protected] (D. Waltregny). 1 T.D. and X.dL. contributed equally to this work. 2 V.C. and D.W. codirected this work. 0302-2838/$ – see back matter # 2006 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2006.01.036

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Prostate Cancer
Activation of the Thromboxane A2 Pathway in HumanProstate Cancer Correlates with Tumor Gleason Scoreand Pathologic Stage
Thibaut Dassesse a,1, Xavier de Leval b,1, Laurence de Leval c, Bernard Pirotte b,Vincent Castronovo a,2, David Waltregny a,d,*,2
aMetastasis Research Laboratory, Center of Experimental Cancer Research, University of Liege, B-4000 Liege, BelgiumbNatural and Synthetic Drugs Research Center, Laboratory of Medical Chemistry, University of Liege, B-4000 Liege, BelgiumcDepartment of Pathology, University of Liege, B-4000 Liege, BelgiumdDepartment of Urology, University of Liege, B-4000 Liege, Belgium
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 1 0 2 1 – 1 0 3 1
avai lab le at www.sciencedi rect .com
journa l homepage: www.europeanurology.com
Article info
Article history:Accepted January 15, 2006Published online ahead ofprint on February 23, 2006
Keywords:ProstateCancerCyclooxygenaseThromboxanePrognosis
Please visitwww.eu-acme.org/europeanurology to read andanswer questions on-line.The EU-ACME credits willthen be attributedautomatically.
Abstract
Objective: We investigated the potential involvement of the thrombox-ane A2 (TXA2) pathway in human prostate cancer (PCa).Methods: Expression of cyclooxygenase-2 (COX-2), TXA2 synthase (TXS),and TXA2 receptors (TPRs), the main actors of the TXA2 pathway, wasanalyzed on serial tissue sections from 46 human PCa specimens.Results: The expression levels of COX-2, TXS, and TPRs were signifi-cantly higher in malignant than in corresponding nontumoral prostaticepithelial cells. Increased immunoreactivity for these antigens was alsoobserved in high-grade prostate intraepithelial neoplasia (HGPIN)glands. COX-2, TXS, and TPR proteins usually displayed a coordinatedoverexpression pattern in PCa lesions, as assessed in serial tissuesections. Increased levels of these proteins in the tumors were allsignificantly associated with higher Gleason scores and pathologicstages.Conclusions: Proteins specifically involved in the TXA2 pathway are up-regulated in human PCa and their level of expression is associated withtumor extraprostatic extension and loss of differentiation. Our study isthe first to examine simultaneously all key proteins involved in thispathway including TXA2 receptors and results suggest that the TXA2
pathway may be a potential target for PCa prevention/therapy.# 2006 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. Department of Urology, University Hospital of Liege, Bloc Central, 1,Bat. B35, CHU Sart Tilman Liege, B-4000 Liege, Belgium. Tel. +32 4 366 7251;Fax: +32 4 366 7258.E-mail address: [email protected] (D. Waltregny).1 T.D. and X.dL. contributed equally to this work.2 V.C. and D.W. codirected this work.
0302-2838/$ – see back matter # 2006 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2006.01.036

e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 1 0 2 1 – 1 0 3 11022
1. Introduction
Intake of nonsteroidal anti-inflammatory drugs(NSAIDs), which act as inhibitors of cyclooxy-genases, has been associated in humans with asignificantly reduced risk of developing severaltypes of cancer including prostate cancer (PCa)[1–4]. A recent comprehensive review of 91 epide-miologic studies, assessing the impact of dailyintake of NSAIDs, has indicated that such atreatment may result in cancer development riskreduction of 39% for PCa [1]. Use of NSAIDs has alsobeen associated with a significantly reduced inci-dence of colon, breast, lung, esophageal, stomach,and ovarian cancers [1]. For most patients, NSAIDanticancer preventive effects become apparentafter �5 yr of use, with a positive associationbetween intake duration and the importanceof risk reduction [1]. These data support theobservations that prostanoids, which are derivedfrom arachidonic acid (AA) through the activityof cyclooxygenases (COXs), usually display anti-apoptotic, growth- promoting, and proangiogenicproperties [5]. It is thus assumed that the chemo-preventive effects of COX inhibitors are predomi-nantly achieved as a result of the inhibition ofAA conversion into prostanoids (see Fig. 1 for aschematic description of the prostanoid pathway).However, prostanoids may exert opposing roles intumor development/progression. For example, inthe study by Pradono et al., retroviral vectorscarrying thromboxane A2 (TXA2) synthase (TXS)
Fig. 1 – Schematic description of the prostanoid pathway
starting from the conversion of arachidonic acid into
endoperoxide prostaglandin H2 (PGH2) under the catalytic
activities of cyclooxygenases. PGH2, a highly unstable
prostanoid, is the substrate of several isomerases,
synthases, and reductases leading to the formation of five
primary prostanoids: PGD2, PGE2, PGF2a, PGI2
(prostacyclin), and TXA2 (thromboxane A2).
cDNA, or prostacyclin (PGI2) synthase cDNA weretransduced to colon cancer cells and each trans-formant was inoculated to mice. Tumors derivedfrom TXA2 synthase transformants grew almostthree times faster and showed more abundantvasculature, whereas tumors from PGI2 synthasetransformants presented opposite effects. Theseeffects were reversed by administration of specificinhibitors [6]. Therefore, the profile of COX meta-bolites in cancer cells can be a significant determi-nant for tumor development. Results from severalother studies have largely supported the implica-tion of TXA2 in tumor invasiveness, angiogenesis,and metastasis [7–15]. TXA2 is thus currentlyconsidered as a valuable anticancer target [11–13,15,16]. In this respect, it is important to considerthat the selective targeting of downstream COX-2pathways, such as the TXA2 pathway, may appearas a promising strategy bearing the potential ofavoiding COX-2 inhibitors cardiovascular toxicitywhile maintaining their anticancer properties.
Several studies on the human prostate haveyielded contradictory results regarding the possibleoverexpression of COX-2 in PCa lesions [17–29]. Onthe other hand, TXS has been shown to be up-regulated in PCa and its increased expression hasbeen associated with advanced disease [8]. To thebest of our knowledge, no data on expression ofTXA2 receptors (TPRs) in PCa are currently available.Two different TPRs, named TPa and TPb receptors,have been identified and are generated by alter-native splicing [30]. TPRs are transmembrane recep-tors belonging to the G protein-coupled receptorsuperfamily. Although no differences were observedin ligand binding and coupling of TPa and TPb
receptors, the b splice variant becomes internalizedto a greater extent than the a variant on exposure toagonist. TPa and TPb form homo- and heterodimers/oligomers [31].
The present study investigated whether the TXA2
pathway may be activated in PCa. The expression ofthe main proteins involved in TXA2 biosynthesis andactivity (COX-2, TXS, and TPR) was assessed usingimmunohistochemistry in serial tissue sections ofhuman PCa samples.
2. Methods
2.1. Tissue samples
Tissue samples from human PCa were surgically obtained
from 46 patients who had undergone a radical retropubic
prostatectomy for localized PCa. All radical prostatectomy
specimens used in this study had been entirely submitted
for histopathologic examination (complete sampling), as

e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 1 0 2 1 – 1 0 3 1 1023
Table 1 – Characteristics of 46 patients with clinicallylocalized prostate cancer treated by retropubic radicalprostatectomy
Gleason score
2–4 5–7 8–10 Total
No. of patients 7 29 19 46
Age, yr
Mean 67.1 65.9 67.2 66.7
SD 6.2 4.3 4.5 4.7
Pathologic stage, %
Organ confined (pT2) 100 55.2 0 50.0
Extracapsular (pT3a) 0 31.9 40.0 28.3
Seminal vesicle invasion (pT3b) 0 13.8 60.0 21.7
SD = standard deviation.
previously described [32]. Most of the tissue sections analyzed
in our study contained portions of both peripheral and
transitional zones. No patient who had received prior
hormonal therapy, chemotherapy, or radiation therapy was
included in the investigation. The age of the patients and the
pathologic stage of their disease are shown in Table 1.
2.2. Antibodies
Polyclonal anti-TXS and anti-TPR antibodies, their correspond-
ing blocking peptide, and monoclonal antihuman COX-2
antibodies were purchased from Cayman Chemical (Ann Arbor,
MI). TXS- and TPR-blocking peptides correspond to the peptides
against which their respective antibodies were raised. TXS-
blocking peptide corresponds to amino acids 359–377
(TNPDCQEKLLREVDVFKEK) of human TXS. TPR blocking pep-
tide corresponds to amino acids 275–279 (VMSFSGQLLRATEHQ)
of the murine TPR (third extracellular domain common to both
TPa and TPb receptors). According to the information given by
the manufacturer, the polyclonal anti-TPR antibody used in this
study cross-reacts with human TPR.
Table 2 – Analysis of expression of COX-2, TXS, and TPR level
I score
Anti-COX-2 immunostaining
N (n = 45) 0.51 � 0.51 (0–1)
HGPIN (n = 22) 2.0 � 0.52 (1–3)
C (n = 46) 2.06 � 0.64 (1–3)
Anti-TXS immunostaining
N (n = 45) 1.36 � 0.48 (1–2)
HGPIN (n = 22) 2.17 � 0.58 (1–3)
C (n = 46) 2.09 � 0.73 (1–3)
Anti-TPR immunostaining
N (n = 45) 0.82 � 0.39 (0–1)
HGPIN (n = 22) 1.39 � 0.72 (0–2)
C (n = 46) 1.39 � 0.88 (0–3)
COX-2 = cyclooxygenase-2; TXS = thromboxane synthase; TPR = thromb
HGPIN = high-grade prostatic intraepithelial neoplasia; C = cancer. I sco
ranging from 0 to 4; IE score is intensity � extent score ranging from 0 to 1
to maximum).
2.3. Immunohistochemistry
One tissue block per patient containing the most representa-
tive tumor-bearing areas was selected considering the
capsular status (pathologic stage) and the Gleason score
stated in the pathologic report, as previously described [33–35].
Serial tissue sections, 5 mm thick, were cut from paraffin
blocks and placed on silane-coated slides for immunohisto-
chemical analysis. Immunoperoxidase staining was per-
formed as previously described [33,35] with the use of the
ABC Vectastain Kit (Vector Laboratories, Burlingame, CA). For
antigen retrieval, slides were heated in a water-bath at 95 8Cfor 40 min in 10 mM citrate buffer. Anti-COX-2 antibody (1:60),
anti-TXS antibody (1:300), or anti-TPR antibody (1:200) was
applied onto the slides and incubated overnight at 4 8C.
Control experiments included omission of the first antibody
and preincubations of anti-TXS and anti-TPR antibodies with
their corresponding blocking peptide prior to their use in the
immunoperoxidase assay.
2.4. Evaluation of immunohistochemical staining
The immunohistochemically stained sections were reviewed
by two independent observers. All discrepancies were
resolved by joint review of the slides. The importance of
anti-COX-2, anti-TXS, and anti-TPR immunoreactivity in
noncancerous and non–high-grade intraepithelial neoplasia
(HGPIN) epithelial cells (herein referred to as ‘‘nontumoral’’)
was analyzed without segregating the expression data
between benign prostatic hyperplasia (BPH) glands from the
transitional zone and histologically normal glands that are
adjacent to cancer cells in the peripheral zone. Anti-COX-2,
anti-TXS, and anti-TPR immunoreactivity was scored in
nontumoral and HGPIN glands when at least 10 glands were
present in the tissue sections. Scoring of the staining was done
according to immunostaining intensity and extent using
arbitrary scales ranging from 0 to 3 and 0 to 4, respectively,
as previously described [33,35,36].
s using immunohistochemistry in human prostate tissues
E score IE score
1.29 � 1.39 (0–4) 1.29 � 1.39 (0–4)
3.87 � 0.46 (2–4) 7.73 � 2.28 (4–12)
3.72 � 0.65 (2–4) 7.79 � 2.87 (2–12)
1.36 � 0.48 (1–2) 2.07 � 1.45 (1–4)
4.00 � 0.00 (4–4) 8.70 � 2.30 (4–12)
4.00 � 0.00 (4–4) 8.35 � 2.90 (4–12)
1.22 � 0.74 (0–2) 1.22 � 1.22 (0–2)
1.91 � 0.90 (0–4) 3.09 � 1.88 (0–8)
1.98 � 1.22 (0–4) 3.48 � 3.24 (0–12)
oxane receptor; n = number of cases; N = normal prostatic glands;
re is an intensity score ranging from 0 to 3; E score is extent score
2. All values are expressed as mean � standard deviation (minimum

e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 1 0 2 1 – 1 0 3 11024
Fig. 2 – Detection of cyclooxygenase 2 (COX-2), thromboxane synthase (TXS), and thromboxane A2 receptors (TPRs) using
immunoperoxidase in human prostate tissues. (A) Immunohistochemical detection of COX-2 in human prostate cancer
(PCa) cells. The inset in the upper right corner shows a higher magnification of the COX-2–expressing PCa cells. (B) Control
experiment using the same tissue sample (serial section) as in panel A, in which anti-COX-2 antibody was omitted in the
immunoperoxidase assay. (C) Detection of TXS in PCa cells (same tissue sample as in panel A). (D) Control experiment in
which the anti-TXS antibody was incubated with an excess of the corresponding peptide prior to its use in the
immunoperoxidase assay. Note the markedly reduced level of anti-TXS immunoreactivity in tumor cells. (E) Detection of
TPR in PCa cells. (F) Control experiment in which the anti-TPR antibody was incubated with an excess of the corresponding
peptide prior to its use in the immunoperoxidase assay. Note the markedly reduced level of anti-TPR immunoreactivity in
tumor cells. Representative examples of moderately (G) and poorly (H) differentiated prostate adenocarcinoma (c) showing
strong anti-TPR immunoreactivity. No or a weak detectable level of TPR was found in adjacent nontumoral prostate glands

e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 1 0 2 1 – 1 0 3 1 1025
2.5. Statistical analysis
A paired t test was used to compare the immunostaining
scores between cancer, HGPIN, and normal prostate glands.
The Spearman rank correlation test was performed to evaluate
the degree of association between the specific staining scores
and the clinicopathologic features of the tumors. A p < 0.05
was considered as statistically significant. Statistical analyses
were carried out using the StatView 5.0 software (Abacus
Concepts, Berkeley, CA).
3. Results
3.1. The two main TXA2 biosynthetic enzymes, COX-2 and
TXS, and its receptors are overexpressed and colocalized in
human PCa
We examined the expression of the main compo-nents of the TXA2 pathway in human PCa cells. Theexpression of the TPRs and that of the 2 enzymesinvolved in its synthesis, COX-2 and TXS, wasevaluated using immunohistochemistry in aseries of human PCa lesions. Among the enzymesresponsible for TXA2 synthesis, no detectable or aweak level of expression of COX-2 and TXS wasobserved in nontumoral glands, whereas adjacentcancer cells usually expressed high levels of theenzymes (Fig. 2A and C). All tumor lesions showeda detectable level (intensity score of 1+, 2+, or 3+)of TXS and COX-2 expression (Table 2). Inaddition, among the 46 PCa lesions analyzed, 39(85%) and 37 (78%) expressed moderate to stronglevels (intensity score of 2+ or +3) of COX-2 and TXS,respectively. Increased levels of TXS and COX-2expression were also usually observed in HGPINglands as compared with nontumoral glands (datanot shown).
Positive staining was abolished or stronglyreduced by omission of the primary antibodies orpreincubation of the primary antibodies with thecorresponding synthetic peptides (Fig. 2A–D). Aspreviously described [20,25,26], COX-2 expressionwas systematically detected in the epithelium liningejaculatory ducts and seminal vesicles when pre-sent in the tissue sections, was observed in scatteredinflammatory cells, including macrophages andlymphocytes, but was not detected in endothelial
(n). (I) Moderately differentiated prostate adenocarcinoma and ad
Note absence of TPR expression in nontumoral prostate glands
immunoreactivity. (K) Strong anti-TPR immunoreactivity in mo
low detectable level of TPR expression in well differentiated can
showing strong anti-TPR reactivity. c = cancer; p = HGPIN; n = no
(Gleason score 4); m = moderately differentiated adenocarcinom
A–D, I, and K, �100; E–G and J, �200; H and L, �400.
cells (data not shown). Anti-COX-2, anti-TXS, andanti-TPR immunostaining was prominently cyto-plasmic.
Fig. 2E–L shows representative photomicrographsof anti-TPR immunoreactivity. Epithelial cells fromnontumoral glands usually exhibited no or a lowdetectable level of TPRs. In contrast, TPR expressionlevels in HGPIN and cancer glands/cells weregenerally increased as compared with those foundin nontumoral cells (Fig. 2G–J). Most PCa lesionsstudied (38 of 45, 74.4%) expressed detectable levelsof TPR (intensity score of 1+, 2+, or 3+). TPRexpression was heterogeneous within the sametumor and the highest levels of immunoreactivitywere frequently observed in the most undifferen-tiated and infiltrating areas (Fig. 2K). In casesshowing perineural invasion, neoplastic cells fre-quently exhibited strong TPR expression (Fig. 2L).Positive TPR staining was abolished by preincuba-tion of the primary antibody with the correspondingsynthetic peptide (Fig. 2E and F).
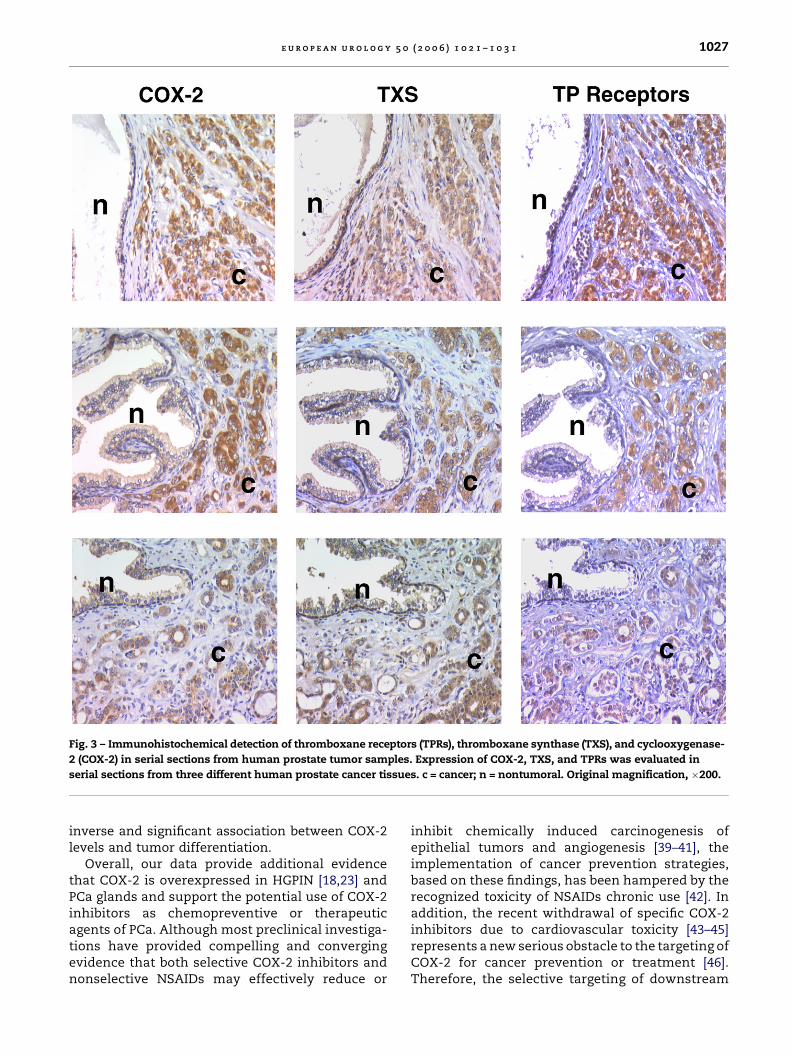
Results of anti-COX2, anti-TXS, and anti-TPRstaining intensity and extent scoring are summar-ized in Table 2. Immunostaining extent and inten-sity for the proteins tested was higher in cancer cellsand HGPIN glands than in nontumoral prostateglands (paired t test, p < 0.005). No significantdifference in anti-COX-2, anti-TXS, or anti-TPRimmunostaining intensity or extent was foundbetween cancer cells and HGPIN glands. As shownin representative examples in Fig. 3, all proteinsexamined also appeared to be coordinately up-regulated within the same tumor. Indeed, all tumorsexhibiting detectable levels of TPR also expressedCOX-2 and TXS. In addition, among tumors expres-sing moderate to strong levels (2+ and 3+ intensityscores) of TPR expression, 95% and 90% of them alsoexpressed moderate to strong levels (2+ and 3+intensity scores) of COX-2 and TXS, respectively(data not shown).
3.2. The expression levels of COX-2, TXS, and TPR are
significantly associated with extraprostatic extension and loss
of differentiation of human PCa
We then compared COX-2, TXS, and TPR expressionlevels in tumors with 2 major histopathologic
jacent HGPIN glands (p) expressing moderate levels of TPR.
. (J) HGPIN glands exhibiting strong anti-TPR
derately differentiated adenocarcinoma glands (m) with a
cer glands (w). (L) Focus of perineural invasion by PCa cells
rmal; w = well differentiated adenocarcinoma glands
a glands (Gleason score 6). Original magnification: panels

e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 1 0 2 1 – 1 0 3 11026
Table 3 – Evaluation of the associations betweenpathologic parameters (pathologic state and Gleasonscore) and anti-COX-2, anti-TXS or anti-TPR stainingintensity and extent in human prostate cancer
Associated tests p value (Spearman rankcorrelation)
COX-2 TXS TPRs
Pathologic stage vs I score 0.0011 0.0037 0.0012
Pathologic stage vs E score 0.0016 NA 0.1885
Pathologic stage vs IE score 0.0029 0.0037 0.0165
Gleason score vs I score 0.0010 0.0184 0.0020
Gleason score vs E score 0.0003 NA 0.0803
Gleason score vs IE score 0.0009 0.0184 0.0207
COX-2 = cyclooxygenase-2; TXS = thromboxane synthase;
TPR = thromboxane receptor; NA = not applicable because all
tumors contained a high percentage of cancer sells showing
detectable anti-TXS immunoreactivity (immunostaining extent
score 4), regardless of their pathologic stage or Gleason score. I
score = intensity score ranging from 0 to 3; E score = extent score
ranging from 0 to 4; IE score = intensity � extent score ranging
from 0 to 12.
prognostic indicators of PCa progression: the Glea-son score and the pathologic stage. Gleason scoreswere stratified into well-differentiated (Gleasonscores 2–4), moderately differentiated (Gleasonscores 5–7), and poorly differentiated (Gleason scores8–10). With the use of the Spearman rank correla-tion test, we found that anti-COX-2, anti-TXS, andanti-TPR staining intensity scores were signifi-cantly associated with the Gleason scores of thetumors (Table 3). Almost two thirds of the poorlydifferentiated adenocarcinomas analyzed showedmoderate (2+) or strong (3+) anti-TP stainingintensity, whereas none of the well differentiatedtumors exhibited such staining intensities (Fig. 2K).In addition, staining intensity � extent scores forthe proteins tested were also significantly corre-lated with the Gleason scores of the tumors. Similarresults were obtained when Gleason score 7 tumorswere included in the group of poorly differentiatedtumors (in extenso comparison between Gleasonscores 2–4 versus 5–6 versus 7–10 tumors; data notshown).
We further observed a significant associationbetween staining intensity or staining intensi-ty � extent scores and the pathologic stage of theprostate tumors (Table 3). As shown in Fig. 4,increased TPR expression was associated withextracapsular extension (pT3A) and invasion ofthe seminal vesicles by the tumors (pT3B). Nosignificant association between the Gleason scoreor pathologic stage of the tumors and the extent ofanti-TXS immunoreactivity was observed becausethe majority of cancer cells within each tumorexpressed the protein (staining extent score of 4).
4. Discussion
A detailed analysis of the key actors of the TXA2
pathway is definitely warranted to justify the use ofexisting or future inhibitors of this pathway aspreventive or therapeutic agents. Indeed, theadministration of such inhibitors would obviouslynot be recommended if the enzymes belonging tothis pathway are not expressed in the targetedtissue.
It is generally accepted that COX-2, an inducibleenzyme as opposed to the more constitutivelyexpressed COX-1, is normally undetectable in mosttissues. Its expression in certain cell types has beenshown to be induced by proinflammatory ormitogenic agents [37,38]. It is also widely recognizedthat COX-2 expression is up-regulated in manyepithelial cancers such as colon, breast, gastro-intestinal, and lung cancers.
Whether COX-2 is overexpressed in human PCacells, as determined by immunohistochemistry,remains a subject of debate at this time. Our studyis one among many others that have found an up-regulation of COX-2 expression in human PCa cells.We have searched PubMed for studies in whichCOX-2 expression was evaluated by immunohisto-chemistry in human PCa tissues. Strikingly, among13 identified articles dealing with this issue [17–29],researchers in 11 studies concluded that COX-2 isoverexpressed in PCa cells as compared withnontumoral prostate glands [17–19,21–27,29]. Onepaper showed ‘mixed’ results suggesting that, ascompared with nontumoral prostate glands, COX-2transcript and protein in PCa cells may be under-expressed and overexpressed, in moderately andpoorly differentiated PCas, respectively [28]. Wehave found only one study, in which COX-2 isdescribed to be expressed neither by PCa cells nor bynormal secretory cells, unless they are involved inan inflammatory process (or postinflammatoryatrophy areas) [20]. In this latter study, Zha et al.have tested the same antibody as the one that wasused in our study [20]. Intriguingly, in their hands,this antibody has generated a striking plasmamembrane staining pattern, which we have notseen in our analysis of COX-2 expression. Similarlyto Zha et al. [20], we have found high levels of COX-2expression in the epithelial lining of ejaculatoryducts and seminal vesicles. It is likely that contra-dictory data may have been the result of thedifferent methodologies used (eg, various antibodiesor different batches of the same antiserum, hormo-nal status, tissue processing, immunohistochemis-try procedures used). In our study, we have furtherfound, as previously described [19,24,26,28], an
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 1 0 2 1 – 1 0 3 1 1027
Fig. 3 – Immunohistochemical detection of thromboxane receptors (TPRs), thromboxane synthase (TXS), and cyclooxygenase-
2 (COX-2) in serial sections from human prostate tumor samples. Expression of COX-2, TXS, and TPRs was evaluated in
serial sections from three different human prostate cancer tissues. c = cancer; n = nontumoral. Original magnification, �200.
inverse and significant association between COX-2levels and tumor differentiation.
Overall, our data provide additional evidencethat COX-2 is overexpressed in HGPIN [18,23] andPCa glands and support the potential use of COX-2inhibitors as chemopreventive or therapeuticagents of PCa. Although most preclinical investiga-tions have provided compelling and convergingevidence that both selective COX-2 inhibitors andnonselective NSAIDs may effectively reduce or
inhibit chemically induced carcinogenesis ofepithelial tumors and angiogenesis [39–41], theimplementation of cancer prevention strategies,based on these findings, has been hampered by therecognized toxicity of NSAIDs chronic use [42]. Inaddition, the recent withdrawal of specific COX-2inhibitors due to cardiovascular toxicity [43–45]represents a new serious obstacle to the targeting ofCOX-2 for cancer prevention or treatment [46].Therefore, the selective targeting of downstream

e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 1 0 2 1 – 1 0 3 11028
Fig. 4 – Thromboxane receptor (TPR) expression levels in human prostate cancer (PCa). Scores of intensity (A) and extent (B)
of anti-TPR immunostaining in PCas according to the pathologic stage of the lesions. Scores of intensity (C) and extent (D) of
anti-TPR immunostaining in PCas according to the Gleason score of the lesions. The scores were defined according to the
scoring method described in the ‘‘Materials and methods’’ section.
COX-2 metabolites, such as TXA2, may appear morejudicious. TXA2, a powerful aggregation mediatorinvolved in thrombotic disorders, has been recentlydemonstrated to participate in cancer progression[7–10]. TXA2 is a key mediator of cancer cell-inducedplatelet aggregation, a process that favors blood-borne metastasis [11]. It also acts as a potentangiogenesis stimulator, both directly and byinducing platelet vascular endothelial growth fac-tor (VEGF) and platelet derived growth factor (PDGF)secretion following platelet aggregation [12–15]. Ourdata indicate that human PCas overexpress TXS andreceptors, with a significant association betweenthe expression levels of these proteins and higherGleason score and pathologic stage of the tumors.We have also observed that TXS and TPR are usuallyup-regulated in HGPIN glands, indicating thatoverexpression of these proteins may be an earlyevent in prostate carcinogenesis. In addition,because these proteins are predominantly coex-
pressed, they may contribute to PCa development inan autocrine manner.
Anti-TPR immunoreactivity was observed to bemainly cytoplasmic. This result is not unexpectedbecause previous studies have shown that TPRsbecome internalized on agonist exposure [47–49]. Infact, our observation that TPRs are mainly found inthe cytoplasmic compartment of PCa cells supportsthe hypothesis of an autocrine loop, in which thecells synthesize TXA2 that subsequently binds andactivates its receptors. Another explanation for thecytoplasmic localization of TPRs is that TPRs canalso been found in the endoplasmic reticulum andthe Golgi complex [50]. It has also been shown thatTPb receptor can be constitutively endocytosed andthat constitutive endocytosis of TPb receptors mayform a pool of receptors in perinuclear recyclingendosomes from which they recycle to the cellsurface, a process involved in preserving receptorsensitivity to agonist stimulation [51].

e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 1 0 2 1 – 1 0 3 1 1029
The mechanisms by which COX-2–derived pros-tanoids might contribute to carcinoma developmentor progression are not precisely defined, but poten-tially include protection against apoptosis [52] andcontribution to tumor angiogenesis [53–55]. Further-more, at this time it is not known why PCa cells dooverexpress enzymes participating in the TXA2
pathway. Accumulating evidence suggests a rolefor inflammation in prostate carcinogenesis [56].Epidemiology data have correlated prostatitis withincreased PCa risk and intake of anti-inflammatorydrugs with decreased PCa risk. Proliferative inflam-matory atrophy lesions containing activated inflam-matory cells and proliferating epithelial cells mayalso be precursors to HGPIN lesions and PCa. COX-2has been linked to inflammation in the normal andmalignant prostate [20]. It has been recently shownthat elevated COX-2 expression levels in PCa cellsmay be associated with increased inflammatory celldensity, both of T lymphocytes and macrophages,suggesting that COX-2 expression may be up-regulated focally in tumor areas with chronicinflammation [26]. It has therefore been proposedthat proinflammatory cytokines, released byT-lymphocytes and macrophages, may up-regulateCOX-2 in adjacent tumor cells. In line with thisconcept, mutations of one of the putative PCasusceptibility genes, MSR1 (encoding macrophagescavenger receptor-1), may contribute to prostatecarcinogenesis through a macrophage-mediatedeffect [57–61]. Regarding TXS and TPRs, their over-expression in PCa cells may obviously be the resultof epigenetic or genetic alterations, which remain tofurther investigated. Whether expression of TXSand TPRs in prostate epithelial cells may be affectedby cytokines should be the focus of further studies.
5. Conclusions
In conclusion, the results of the present studyindicate for the first time that the expression ofthe key proteins involved in the TXA2 pathway areup-regulated in HGPIN and PCa cells. In PCa lesions,overexpression of these proteins is associated withtumor extraprostatic extension and loss of differ-entiation. Overall, these findings identify the TXA2
pathway as a potential target for PCa prevention ortreatment or both.
Acknowledgments
The authors thank Pascale Heneaux for technicalassistance. D. Waltregny and L. de Leval are
Research Associates and T. Dassesse is a Televieresearch Fellow at the National Fund for ScientificResearch (FNRS, Belgium).
Grant sponsors: National Fund for ScientificResearch (Belgium), Centre Anti-Cancereux de l’Uni-versite de Liege, Fonds Leon Fredericq, TELEVIE,European Union FP6 LSHC-CT-2003-503233, Inter-university Attraction Pole (IAP-P5/31) and the sup-port of European Commission through contacts CEELSHC-CT-2004-503049 and CEE LSHC-CT-2003-505233.
References
[1] Harris RE, Beebe-Donk J, Doss H, Burr Doss D. Aspirin,
ibuprofen, and other non-steroidal anti-inflammatory
drugs in cancer prevention: a critical review of non-selec-
tive COX-2 blockade (review). Oncol Rep 2005;13:559–83.
[2] Koehne CH, Dubois RN. COX-2 inhibition and colorectal
cancer. Semin Oncol 2004;31:12–21.
[3] Nelson JE, Harris RE. Inverse association of PCa and non-
steroidal anti-inflammatory drugs (NSAIDs): results of a
case-control study. Oncol Rep 2000;7:169–70.
[4] Terry MB, Gammon MD, Zhang FF, et al. Association of
frequency and duration of aspirin use and hormone recep-
tor status with breast cancer risk. JAMA 2004;291:2433–40.
[5] Rodrigues S, Bruyneel E, Rodrigue CM, Shahin E, Gespach
C. Cyclooxygenase 2 and carcinogenesis. Bull Cancer
2004;91:S61–76.
[6] Pradono P, Tazawa R, Maemondo M, et al. Gene transfer of
thromboxane A(2) synthase and prostaglandin I(2)
synthase antithetically altered tumor angiogenesis and
tumor growth. Cancer Res 2002;62:63–6.
[7] Nie D, Lamberti M, Zacharek A, et al. Thromboxane A(2)
regulation of endothelial cell migration, angiogenesis,
and tumor metastasis. Biochem Biophys Res Commun
2000;267:245–51.
[8] Nie D, Che M, Zacharek A, et al. Differential expression of
thromboxane synthase in prostate carcinoma: role in
tumor cell motility. Am J Pathol 2004;164:429–39.
[9] Nanji AA. Thromboxane synthase and organ preference
for metastases. N Engl J Med 1993;329:138–9.
[10] Daniel TO, Liu H, Morrow JD, Crews BC, Marnett LJ.
Thromboxane A2 is a mediator of cyclooxygenase-2-
dependent endothelial migration and angiogenesis.
Cancer Res 1999;59:4574–7.
[11] Jurasz P, Alonso-Escolano D, Radomski MW. Platele–can-
cer interactions: mechanisms and pharmacology of
tumour cell-induced platelet aggregation. Br J Pharmacol
2004;143:819–26.
[12] Atkinson S, Fox SB. Vascular endothelial growth factor
(VEGF)-A and platelet-derived growth factor (PDGF) play a
central role in the pathogenesis of digital clubbing.
J Pathol 2004;203:721–8.
[13] Rhee JS, Black M, Schubert U, et al. The functional role
of blood platelet components in angiogenesis. Thromb
Haemost 2004;92:394–402.

e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 1 0 2 1 – 1 0 3 11030
[14] Arisato T, Hashiguchi T, Sarker KP, et al. Highly accumu-
lated platelet vascular endothelial growth factor in coagu-
lant thrombotic region. J Thromb Haemost 2003;1:2589–93.
[15] Ross JA, Potter JD, Severson RK. Platelet-derived growth
factor and risk factors for colorectal cancer. Eur J Cancer
Prev 1993;2:197–210.
[16] Liu XH, Kirschenbaum A, Yao S, Lee R, Holland JF, Levine
AC. Inhibition of cyclooxygenase-2 suppresses angiogen-
esis and the growth of PCa in vivo. J Urol 2000;164:820–5.
[17] Yoshimura R, Sano H, Masuda C, et al. Expression of
cyclooxygenase-2 in prostate carcinoma. Cancer
2000;89:589–96.
[18] Kirschenbaum A, Liu X, Yao S, Levine AC. The role of
cyclooxygenase-2 in PCa. Urology 2001;58:127–31.
[19] Lee LM, Pan CC, Cheng CJ, Chi CW, Liu TY. Expression of
cyclooxygenase-2 in prostate adenocarcinoma and
benign prostatic hyperplasia. Anticancer Res 2001;21:
1291–4.
[20] Zha S, Gage WR, Sauvageot J, et al. Cyclooxygenase-2 is
up-regulated in proliferative inflammatory atrophy of the
prostate, but not in prostate carcinoma. Cancer Res
2001;61:8617–23.
[21] Rubio J, Ramos D, Lopez-Guerrero JA, et al. Immunohis-
tochemical expression of Ki-67 antigen, Cox-2 and Bax/
Bcl-2 in PCa: prognostic value in biopsies and radical
prostatectomy specimens. Eur Urol 2005;48:745–51.
[22] Zang T, Sun F, Li Y. Expression of COX-2 in prostatic
cancer and benign prostatic hyperplasia. Zhonghua Wai
Ke Za Zhi 2001;39:702–3.
[23] Uotila P, Valve E, Martikainen P, Nevalainen M, Nurmi M,
Harkonen P. Increased expression of cyclooxygenase-2
and nitric oxide synthase-2 in human PCa. Urol Res
2001;29:23–8.
[24] Madaan S, Abel PD, Chaudhary KS, et al. Cytoplasmic
induction and over-expression of cyclooxygenase-2 in
human PCa: implications for prevention and treatment.
BJU Int 2000;86:736–41.
[25] Gupta S, Srivastava M, Ahmad N, Bostwick DG, Mukhtar
H. Over-expression of cyclooxygenase-2 in human pros-
tate adenocarcinoma. Prostate 2000;42:73–8.
[26] Wang W, Bergh A, Damber JE. Cyclooxygenase-2 expres-
sion correlates with local chronic inflammation and
tumor neovascularization in human PCa. Clin Cancer
Res 2005;11:3250–6.
[27] Edwards J, Mukherjee R, Munro AF, Wells AC, Almushatat
A, Bartlett JM. HER2 and COX2 expression in human PCa.
Eur J Cancer 2004;40:50–5.
[28] Shappell SB, Manning S, Boeglin WE, et al. Alterations in
lipoxygenase and cyclooxygenase-2 catalytic activity and
mRNA expression in prostate carcinoma. Neoplasia
2001;3:287–303.
[29] Tanji N, Kikugawa T, Yokoyama M. Immunohistochem-
ical study of cyclooxygenases in prostatic adenocarci-
noma; relationship to apoptosis and Bcl-2 protein
expression. Anticancer Res 2000;20:2313–9.
[30] Kinsella BT. Thromboxane A2 signalling in humans: a
‘Tail’ of two receptors. Biochem Soc Trans 2001;29:641–54.
[31] Laroche G, Lepine MC, Theriault C, et al. Oligomerization
of the alpha and beta isoforms of the thromboxane A2
receptor: relevance to receptor signaling and endocytosis.
Cell Signal 2005;17:1373–83.
[32] Bostwick DG, Montironi R. Evaluating radical prostatect-
omy specimens: therapeutic and prognostic importance.
Virchows Arch 1997;430:1–16.
[33] Waltregny D, Bellahcene A, Van Riet I, et al. Prognostic
value of bone sialoprotein expression in clinically loca-
lized human PCa. J Natl Cancer Inst 1998;90:1000–8.
[34] van den Brule FA, Waltregny D, Liu FT, Castronovo V.
Alteration of the cytoplasmic/nuclear expression pattern
of galectin-3 correlates with prostate carcinoma progres-
sion. Int J Cancer 2000;89:361–7.
[35] Chaplet M, Waltregny D, Detry C, Fisher LW, Castronovo
V, Bellahcene A. Expression of dentin sialophosphopro-
tein in human PCa and its correlation with tumor aggres-
siveness. Int J Cancer 2006;118:850–6.
[36] Sjogren S, Inganas M, Norberg T, et al. The p53 gene in
breast cancer: prognostic value of complementary DNA
sequencing versus immunohistochemistry. J Natl Cancer
Inst 1996;88:173–82.
[37] Taketo MM. Cyclooxygenase-2 inhibitors in tumorigen-
esis (part I). J Natl Cancer Inst 1998;90:1529–36.
[38] Vane JR, Bakhle YS, Botting RM. Cyclooxygenases 1 and 2.
Annu Rev Pharmacol Toxicol 1998;38:97–120.
[39] Gately S, Li WW. Multiple roles of COX-2 in tumor angio-
genesis: a target for antiangiogenic therapy. Semin Oncol
2004;31:2–11.
[40] Wei D, Wang L, He Y, Xiong HQ, Abbruzzese JL, Xie K.
Celecoxib inhibits vascular endothelial growth factor
expression in and reduces angiogenesis and metastasis
of human pancreatic cancer via suppression of Sp1 tran-
scription factor activity. Cancer Res 2004;64:2030–8.
[41] Rao CV, Reddy BS. NSAIDs and chemoprevention. Curr
Cancer Drug Targets 2004;4:29–42.
[42] Fortun PJ, Hawkey CJ. Nonsteroidal antiinflammatory
drugs and the small intestine. Curr Opin Gastroenterol
2005;21:169–75.
[43] Bannwarth B. Do selective cyclo-oxygenase-2 inhibitors
have a future? Drug Saf 2005;28:183–9.
[44] Bresalier RS, Sandler RS, Quan H, et al. Cardiovascular
events associated with rofecoxib in a colorectal adenoma
chemoprevention trial. N Engl J Med 2005;352:1092–102.
[45] Levesque LE, Brophy JM, Zhang B. The risk for myocardial
infarction with cyclooxygenase-2 inhibitors: a population
study of elderly adults. Ann Intern Med 2005;142:481–9.
[46] Vanchieri C. Vioxx withdrawal alarms cancer prevention
researchers. J Natl Cancer Inst 2004;96:1734–5.
[47] Walsh MT, Foley JF, Kinsella BT. The alpha, but not the
beta, isoform of the human thromboxane A2 receptor is a
target for prostacyclin-mediated desensitization. J Biol
Chem 2000;275:20412–23.
[48] Walsh M, Foley JF, Kinsella BT. Investigation of the role of
the carboxyl-terminal tails of the alpha and beta isoforms
of the human thromboxane A(2) receptor (TP) in mediat-
ing receptor:effector coupling. Biochim Biophys Acta
2000;1496:164–82.
[49] Breyer RM, Bagdassarian CK, Myers SA, Breyer MD. Pros-
tanoid receptors: subtypes and signaling. Annu Rev Phar-
macol Toxicol 2001;41:661–90.

e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 1 0 2 1 – 1 0 3 1 1031
[50] Valentin F, Field MC, Tippins JR. The mechanism of oxi-
dative stress stabilization of the thromboxane receptor in
COS-7 cells. J Biol Chem 2004;279:8316–24.
[51] Theriault C, Rochdi MD, Parent JL. Role of the Rab11-asso-
ciated intracellular pool of receptors formed by constitu-
tive endocytosis of the beta isoform of the thromboxane A2
receptor (TP beta). Biochemistry 2004;43:5600–7.
[52] Tsujii M, DuBois RN. Alterations in cellular adhesion and
apoptosis in epithelial cells overexpressing prostaglandin
endoperoxide synthase 2. Cell 1995;83:493–501.
[53] Tsujii M, Kawano S, Tsuji S, Sawaoka H, Hori M, DuBois
RN. Cyclooxygenase regulates angiogenesis induced by
colon cancer cells. Cell 1998;93:705–16.
[54] Sawaoka H, Tsuji S, Tsujii M, et al. Cyclooxygenase inhi-
bitors suppress angiogenesis and reduce tumor growth in
vivo. Lab Invest 1999;79:1469–77.
[55] Masferrer JL, Leahy KM, Koki AT, et al. Antiangiogenic and
antitumor activities of cyclooxygenase-2 inhibitors. Can-
cer Res 2000;60:1306–11.
Editorial Comment
Arno van Leenders, Rotterdam, The [email protected]
Clinical, epidemiological and molecular biolo-gical studies all imply involvement of inflamma-tory pathways in prostate cancer [1]. Intake ofNSAIDs is generally associated with an inverseassociation with prostate cancer development [2].The mechanisms underlying these chemopreven-tive effects are still poorly understood.
First, inhibition of inflammatory pathwaysmight directly affect prostate cancer cells. Thedata currently presented by Dassesse et al. supportthis hypothesis as they clearly demonstrate over-expression of cyclo-oxygenase-2, thromboxane A2synthase and its receptors in malignant prostateepithelium. Inhibition of these enzymes or recep-tors by NSAIDs would accordingly have apoptoticor anti-proliferative effects, resulting in remissionof latent tumours. Concomitantly, anti-inflamma-tory drugs potentially prevent progression of pre-malignant lesions. The authors namely demon-strate expression of these inflammatory pathwaysin PIN, which is generally assumed to represent theprecursor of prostate cancer.
Second, besides direct effects on tumourcells, reduction of prostatic inflammation mightcontribute to the chemoprevention of prostatecancer. Although prostatitis is generally consid-ered a clinical diagnosis, microscopic prostaticinflammatory foci are almost invariably encoun-tered in normal patients. These foci are oftenassociated with morphologic atrophy of adjacentepithelial glands, which paradoxically demonstrate
[56] Nelson WG, De Marzo AM, DeWeese TL, Isaacs WB. The
role of inflammation in the pathogenesis of PCa. J Urol
2004;172:S6–11, discussion S2.
[57] DeMarzo AM, Nelson WG, Isaacs WB, Epstein JI. Patholo-
gical and molecular aspects of PCa. Lancet 2003;361:955–
64.
[58] Xu J, Zheng SL, Komiya A, et al. Germline mutations and
sequence variants of the macrophage scavenger receptor
1 gene are associated with PCa risk. Nat Genet 2002;32:
321–5.
[59] Dong JT. Prevalent mutations in PCa. J Cell Biochem
2005;97:433–47.
[60] Porkka KP, Visakorpi T. Molecular mechanisms of
prostate cancer. Eur Urol 2004;45:683–91.
[61] Rennert H, Zeigler-Johnson CM, Addya K, et al. Associa-
tion of susceptibility alleles in ELAC2/HPC2, RNASEL/
HPC1, and MSR1 with PCa severity in European American
and African American men. Cancer Epidemiol Biomarkers
Prev 2005;14:949–57.
enhanced proliferative activity and have thereforebeen referred to as ‘proliferative inflammatoryatrophy’ [3]. Although these lesions are not con-sidered to be malignant precursors per se, early(epi)genetic alterations are identified in subsetsof atrophic epithelial glands presumably in conse-quence of their continuous exposure to inflamma-tory oxidants such as nitric oxide and superoxide[4]. Direct targeting of the inflammatory responsesby anti-oxidative and -inflammatory drugs wouldtherefore logically represent another chemopre-ventive mechanism.
Unfortunately, the authors did not specificallyconsider atrophic lesions in their analysis of thethromboxane A2 pathway in the prostate. Char-acterisation of key-members of this pathway as iscurrently reported, offers a rationale for the furtherdevelopment of chemopreventive targets in pros-tate cancer.
References
[1] Nelson WG, De Marzo AM, DeWeese TL, Isaacs WB. The
role of inflammation in the pathogenesis of prostate
cancer. J Urol 2004;172:S6–11.
[2] Mahmud S, Franco E, Aprikian A. Prostate cancer and
use of nonsteroidal anti-inflammatory drugs: systema-
tic review and meta-analysis. Br J Cancer 2004;90:93–9.
[3] De Marzo AM, Marchi VL, Epstein JI, Nelson WG. Prolif-
erative inflammatory atrophy of the prostate: implica-
tions for prostatic carcinogenesis. Am J Pathol
1999;155:1985–92.
[4] Shah R, Mucci NR, Amin A, Macoska JA, Rubin MA.
Postatrophic hyperplasia of the prostate gland: neoplas-
tic precursor or innocent bystander? Am J Pathol 2001;
158:1767–73.
Related Documents
![Bt354 as a new STAT3 signaling pathway inhibitor against ...download.xuebalib.com/38cqWocZQRSY.pdf · carcinoma, prostate cancer, melanoma, multiple myeloma, and leukemia [3]. Aberrant](https://static.cupdf.com/doc/110x72/5c873e1809d3f2d8348badbc/bt354-as-a-new-stat3-signaling-pathway-inhibitor-against-carcinoma-prostate.jpg)










