http://cat.sagepub.com Clinical and Applied Thrombosis/Hemostasis DOI: 10.1177/1076029607306807 2008; 14; 428 originally published online Dec 26, 2007; Clin Appl Thromb Hemost Florencia Vargas-Vorackova, Jorge Vela-Ojeda and Jaime García-Chávez Majluf-Cruz, Rodolfo Guardado-Mendoza, Irma Molina-Ávila, Irma Isordia-Salas, Norma Corona-de la Peña, Abraham Majluf-Cruz, Manuel Moreno-Hernández, Adriana Ruiz-de-Chávez-Ochoa, Rosario Monroy-García, Karim Activated Protein C Resistance and Factor V Leiden in Mexico http://cat.sagepub.com/cgi/content/abstract/14/4/428 The online version of this article can be found at: Published by: http://www.sagepublications.com can be found at: Clinical and Applied Thrombosis/Hemostasis Additional services and information for http://cat.sagepub.com/cgi/alerts Email Alerts: http://cat.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: http://cat.sagepub.com/cgi/content/refs/14/4/428 SAGE Journals Online and HighWire Press platforms): (this article cites 53 articles hosted on the Citations by Abraham Majluf-Cruz on October 1, 2008 http://cat.sagepub.com Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

http://cat.sagepub.com
Clinical and Applied Thrombosis/Hemostasis
DOI: 10.1177/1076029607306807 2008; 14; 428 originally published online Dec 26, 2007; Clin Appl Thromb Hemost
Florencia Vargas-Vorackova, Jorge Vela-Ojeda and Jaime García-Chávez Majluf-Cruz, Rodolfo Guardado-Mendoza, Irma Molina-Ávila, Irma Isordia-Salas, Norma Corona-de la Peña,
Abraham Majluf-Cruz, Manuel Moreno-Hernández, Adriana Ruiz-de-Chávez-Ochoa, Rosario Monroy-García, Karim Activated Protein C Resistance and Factor V Leiden in Mexico
http://cat.sagepub.com/cgi/content/abstract/14/4/428 The online version of this article can be found at:
Published by:
http://www.sagepublications.com
can be found at:Clinical and Applied Thrombosis/Hemostasis Additional services and information for
http://cat.sagepub.com/cgi/alerts Email Alerts:
http://cat.sagepub.com/subscriptions Subscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://cat.sagepub.com/cgi/content/refs/14/4/428SAGE Journals Online and HighWire Press platforms):
(this article cites 53 articles hosted on the Citations
by Abraham Majluf-Cruz on October 1, 2008 http://cat.sagepub.comDownloaded from

Activated Protein C Resistanceand Factor V Leiden in Mexico
Abraham Majluf-Cruz, MD, Manuel Moreno-Hernández, MSc,Adriana Ruiz-de-Chávez-Ochoa, MSc, Rosario Monroy-García, ScT,Karim Majluf-Cruz, MD, Rodolfo Guardado-Mendoza, MD,Irma Molina-Ávila, MD, Irma Isordia-Salas, MD,Norma Corona-de la Peña, PhD, Florencia Vargas-Vorackova, MD, PhD,Jorge Vela-Ojeda, MD, and Jaime García-Chávez, MD
anticoagulant effect of activated protein C, or acti-vated protein C resistance (APCR), is recognized inmany countries as the single most common cause ofhereditary thrombophilia.6-11 Most cases of APCRare thought to be due to factor V Leiden mutation(FV Leiden) or to several other mutations in thegene of this hemostatic factor,12 but in a few cases,the genetic explanation for the APCR phenotyperemains unclear.
On the other hand, the occurrence of APCR phe-notype has also been described as associated with sev-eral nonhereditary morbid states. The importance ofthese specific associations appears cumbersomebecause these pathologic phenomena are widely asso-ciated with thrombotic events. Moreover, APCR maybe present in an individual without being known, andthe morbid states carry a high thrombogenic risk forthese individuals. Therefore, an acquired variant ofAPCR may be an important although unrecognizedfactor for thrombosis.13
Owing to the importance of APCR and FV Leidenin the pathogenesis of thrombosis, and because the
Thrombotic disease is the leading cause ofmorbidity and mortality worldwide.1,2 Causesof thrombosis may be genetic or acquired.
Although several abnormalities that induce geneticpredisposition to thrombosis have been described,and most are inherited or acquired deficiencies ofnaturally occurring anticoagulants, these cannotexplain all thrombotic events.3-5 Resistance to the
A common cause of hereditary thrombophilia is activatedprotein C resistance (APCR), and most cases resultfrom factor V Leiden mutation. An APCR phenotypewithout association with factor V Leiden has beendescribed. This transversal, observational, nonrandomizedstudy evaluated these 2 phenomena in healthy indigenousand mestizo Mexican subjects (n = 4345), including600 Mexican natives. No indigenous subjects hadAPCR, but 82 mestizo subjects did. After retesting, 50subjects had a negative test. The remaining 32 subjectshad factor V Leiden, giving a 0.85% prevalence of
factor V Leiden in the mestizo Mexican population.Only 31% of APCR carriers had factor V Leiden. Theseresults show a very low prevalence of APCR and factorV Leiden in Mexico. Except for factor V Leiden, thereare no other mutations in the factor V gene responsiblefor the APCR phenotype. Acquired APCR is nearlytwice as prevalent as the inherited variant.
Keywords: factor V Leiden; activated protein C resist-ance; thrombosis; Native Americans
From the Unidad de Investigación Médica en Trombosis,Hemostasia y Aterogénesis, Instituto Mexicano del SeguroSocial (IMSS), Mexico City, Mexico (AMC, MMH, ARDCO,RMG, KMC, RGM, IMA, IIS, NCDLP), Departamento deGastroenterología, Instituto Nacional de la Nutrición SalvadorZubirán, Mexico City, Mexico (FVV), and Departamento deHematología, Hospital de Especialidades, Centro Médico LaRaza, IMSS, Mexico City, Mexico (JVO, JGC).
Address correspondence to: Abraham Majluf-Cruz, MD, FACP,Apdo. Postal 12-1100, México 12, DF, México; Phone/fax: (+52)55-5688-5417; e-mail: [email protected] and [email protected].
This work was sponsored by contract grant sponsor ConsejoNacional de Ciencia y Tecnología, CONACYT (México); contractgrant number, M-12891.
Clinical and AppliedThrombosis/Hemostasis
Volume 14 Number 4October 2008 428-437
© 2008 Sage Publications10.1177/1076029607306807
http://cath.sagepub.comhosted at
http://online.sagepub.com
428 by Abraham Majluf-Cruz on October 1, 2008 http://cat.sagepub.comDownloaded from

epidemiologic impact of such prothrombotic stateshas not been clearly established in Mexico, we decidedto evaluate the characteristics of these 2 pathologicphenomena in the country.
Subjects and Methods
Subjects
We conducted a cross-sectional, observational, non-randomized study of indigenous and mestizoMexican populations. To collect the whole numberof blood samples according to the calculated samplesize, we recruited subjects from 3 main sources,namely, governmental blood banks, universities, andnongovernmental organizations. In every case, directcontact with the source of individuals started beforesampling. We provided the blood banks with carefulinformation about the study the same day of blooddonation and then asked the blood donors to partic-ipate. We obtained the sample immediately beforeblood donation. For universities and nongovernmen-tal organizations, appropriate information was sentand distributed to the candidates to participate sev-eral weeks before blood drawing was performed. Theday of blood collection, participants were informedagain about the nature of the study. A total of 136nongovernmental organizations helped us in thisstudy, including syndicates and health-related, envi-ronmental, cultural, sporting, medical, ambientalist,professional, religious, and social groups. Theseorganizations were very important, especially for thecollection of samples in indigenous communities.
We included healthy men and women agedbetween 18 and 70 years. For indigenous and mestizopopulations, we included only 1 family member. To bestudied, indigenous subjects had to belong to one ofthe several ethnic groups living throughout Mexico.These were considered as indigenous when they ful-filled all of the following criteria: (1) speaking a nativelanguage as first language (with Spanish as a secondlanguage), (2) living in an indigenous village, (3) con-sidering themselves as indigenous, and (4) beingcarriers of blood group O Rh(o)D-positive.14 If aninterethnic indigenous mixture was demonstrated,the subject continued to be eligible. All mestizo indi-viduals living in Mexico were included. We excludedsubjects with no evidence of mestizaje (mixing ofraces) in at least 1 of the parents. In addition, weexcluded individuals with a history of thromboticevents or hemophilia, individuals with a family history
of thrombosis or hemorrhagic diseases, and individu-als with liver disease, moderate-to-severe alcoholism,or moderate-to-severe malnutrition. Finally, weexcluded all women taking oral contraceptives.
Sample Collection
From each subject, 3 mL of blood was drawn in a sil-iconized glass tube containing 0.109M sodium citrate(9:1, vol:vol) as well as 5 mL of blood in a glass tubecontaining ethylenediaminetetraacetic acid (EDTA;Vacutainer, Beckton Dickinson, Franklin Lakes, NewJersey). After withdrawal, samples were centrifugedimmediately at 2000 g for 15 minutes to obtain 2aliquots of citrated plasma and 1 aliquot of buffy coatfrom the tube with EDTA. Aliquots were maintainedin 1.5-mL Eppendorf tubes (Eppendorf AG,Hamburg, Germany) and frozen with dry ice as soonas possible. On arrival at our center, the aliquots weremaintained frozen at −70°C until processing. Bloodgroup was determined by means of blood cells.
Activated Protein C Resistance Assay
This test was performed according to the techniquepreviously described in the literature, using a com-mercially available kit (Stago APC-R, DiagnosticaStago, Ansnieres, France) that measures clottingtime after venom activation of factor X in the pres-ence of activated protein C (APC); test plasma wasdiluted (1:20) in FV-deficient plasma. We used STA-Compaq equipment (Diagnostica Stago). Plasmaswere thawed on the day of the test. Results areexpressed as clotting times, without reference tobaseline without APC.
We considered the test positive for APCR whenclotting time was less than 120 seconds. WheneverAPCR was reported as positive, the test was conductedagain with a second assay performed after dilution(1:4) of test plasma in a FV plasma reagent (Coatest,APC Resistance V, Instrumentation Laboratory,Milan, Italy). Using this assay, APCR was positivewhen the ratio of clotting times was 0.84 or less.Whenever a subject was positive after both assays,lupus anticoagulant was excluded using a commer-cially available test (Staclot LA,Diagnostica Stago).
In all APCR-positive patients, a new sample wasobtained at least 3 months after the first sample toconfirm the result and to identify those who werelikely acquired-APCR carriers. During this secondstudy phase, APCR was again investigated using the
FV Leiden and APCR in Mexico / Majluf-Cruz et al 429
by Abraham Majluf-Cruz on October 1, 2008 http://cat.sagepub.comDownloaded from

2 previously mentioned assays. Acquired APCR wasconsidered according to previously published crite-ria as the presence of APCR in the absence of FVLeiden mutation.13,15
Factor V Leiden Assay
We followed the internationally accepted procedurefor establishing the presence of this mutation.16 Weused the buffy coat obtained from the blood samplecollected in EDTA. Genomic DNA was isolatedaccording to the manufacturer’s instructions with aQIAamp blood kit (QIAGEN, Hilden, Germany).Polymerase chain reaction (PCR) was performed ina PerkinElmer thermocycler (PerkinElmer Life andAnalytical Sciences, Inc. Waltham, Massachusetts)for 30 cycles consisting of 9°C for 40 seconds, 58°Cfor 40 seconds, and 71°C for 2 minutes, this cyclerepeated 35 times. After allele-specific restrictionenzyme digestion of the amplified DNA with therestriction enzyme Mnl-l for 6 hours at 37°C, the FVLeiden genotype was identified on 3% agarose gels.These were stained with 1-μg/mL ethidium bromideand visualized under ultraviolet light. Individualswithout FV Leiden mutation were identified bybands at 163 bp, 67 bp, and 37 bp. Whenever FVLeiden was present, 2 bands were visualized: one at200 bp and the other at 67 bp.
Statistical Analysis
To detect frequencies of 2% with a 95% confidenceinterval and considering the entire Mexican popula-tion of 100 million, a sample of 4200 subjects wascalculated; we collected and analyzed 4345 samples.Because approximately 12% of the Mexican popula-tion is indigenous,17 we attempted to study 504 nativeindividuals. Because 85% of the mestizaje in Mexicohave Spanish origin, we attempted to sample the pop-ulation while maintaining this proportion. Data areexpressed as frequencies, medians, and ranges.
Because this was a nonrandomized study, weanalyzed the distribution of the participating indi-viduals to determine if there were differences amongthe populations that could affect the study results.We therefore analyzed the results according to the 3main sources of recruitment of the participatingindividuals (universities, nongovernmental organiza-tions, and governmental blood banks) in terms ofage, sex, and prevalence of acquired APCR and FVLeiden. A χ2 test was used to identify differences
among these 3 sources of individuals. To demonstratedifferences among the 3 groups in terms of age, ananalysis of variance test was used. Results were sig-nificant at P < .05.
Ethics Aspects
Before blood withdrawal, all individuals received oraland written information about the study characteris-tics. If they agreed to participate, we requested writ-ten consent from each person. We ensured therestricted nature of results information and sampleuse according to Declaration of Helsinki principles.This project was approved by the Ethics Committeesof our respective institutions.
Results
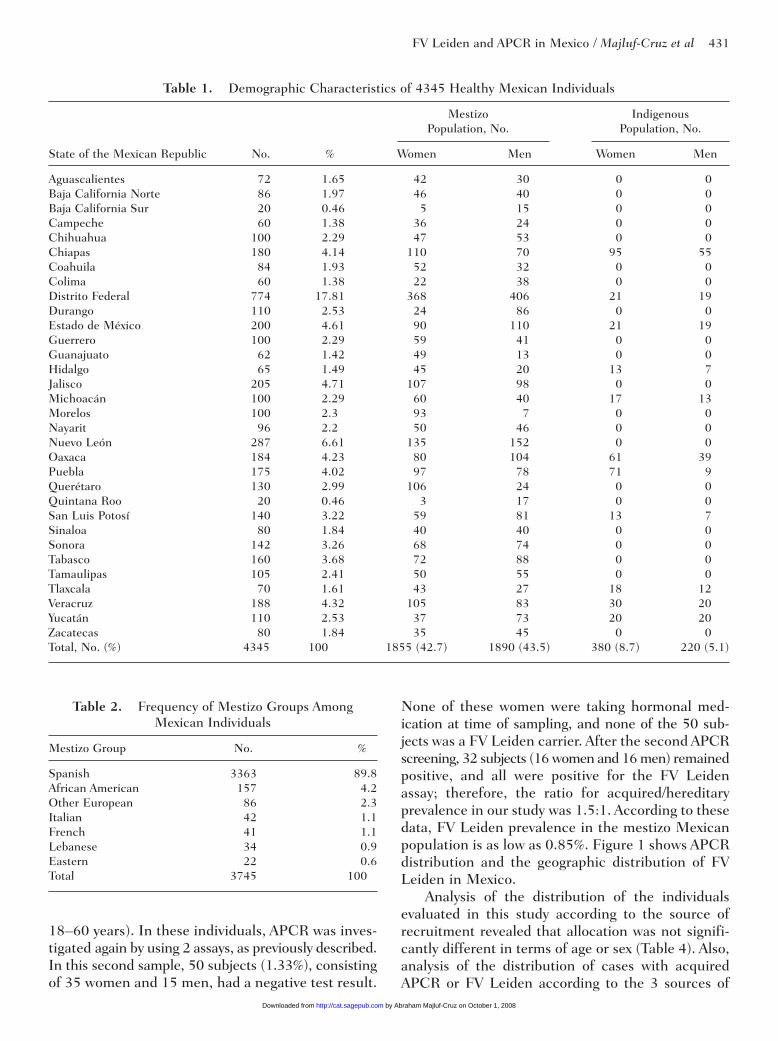
After 5026 healthy Mexican individuals were directlyinvited to participate, we obtained blood samplesfrom 4345 subjects from throughout Mexico. Generalcharacteristics of these subjects are summarized inTable 1. We covered all the states of the MexicanRepublic, collecting blood samples from subjects in647 cities, towns, and villages. Percentages of womenand men were 51.4 and 48.6%, respectively. Themedian ages were 38.5 years (range, 18-68 years) forwomen and 40.0 years (range, 18-69 years) for men.We obtained 600 blood samples from Mexican indige-nous persons residing in 11 states of the MexicanRepublic and 3745 blood samples from mestizos. Weobtained samples from 380 native women and 220men, with a respective median age of 35.5 years(range, 18-56 years) and 39 years (range, 19-57years). For mestizo individuals, median age was 40years (range, 18-68 years) for women and 41 years(range, 18-69 years) for men. Absolute numbers andpercentages of individuals sampled from each mestizogroup are presented in Table 2.
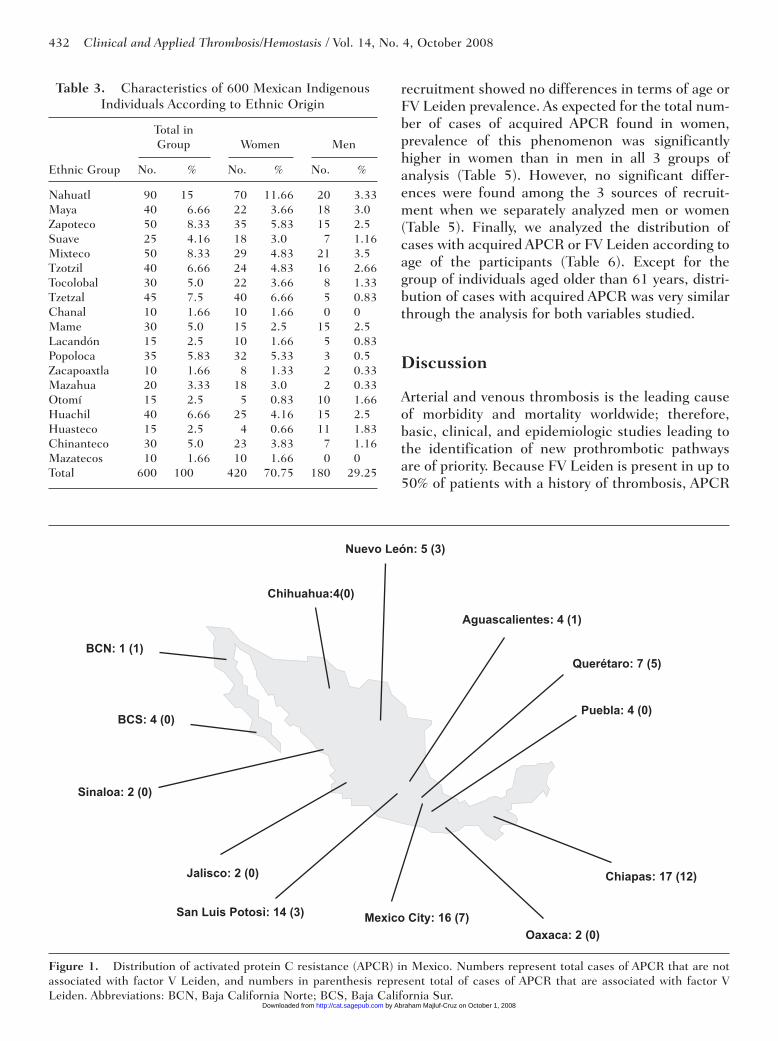
General demographic data of indigenous Mexicanpopulations studied are presented in Table 3. Weobtained samples from 19 ethnic groups. More sam-ples from women were obtained because they weremore accessible than men, mainly because of workconditions. The O-positive blood group was found in100% of our indigenous sample.
The APCR prevalence was 0% in the indigenouspopulation studied. Among 3745 mestizos, APCR wasfound in 82 individuals (2.18%) by using 2 APCRassays. This group, which consisted of 51 womenand 31 men, had a median age of 37 years (range,
430 Clinical and Applied Thrombosis/Hemostasis / Vol. 14, No. 4, October 2008
by Abraham Majluf-Cruz on October 1, 2008 http://cat.sagepub.comDownloaded from
FV Leiden and APCR in Mexico / Majluf-Cruz et al 431
18–60 years). In these individuals, APCR was inves-tigated again by using 2 assays, as previously described.In this second sample, 50 subjects (1.33%), consistingof 35 women and 15 men, had a negative test result.
None of these women were taking hormonal med-ication at time of sampling, and none of the 50 sub-jects was a FV Leiden carrier. After the second APCRscreening, 32 subjects (16 women and 16 men) remainedpositive, and all were positive for the FV Leidenassay; therefore, the ratio for acquired/hereditaryprevalence in our study was 1.5:1. According to thesedata, FV Leiden prevalence in the mestizo Mexicanpopulation is as low as 0.85%. Figure 1 shows APCRdistribution and the geographic distribution of FVLeiden in Mexico.
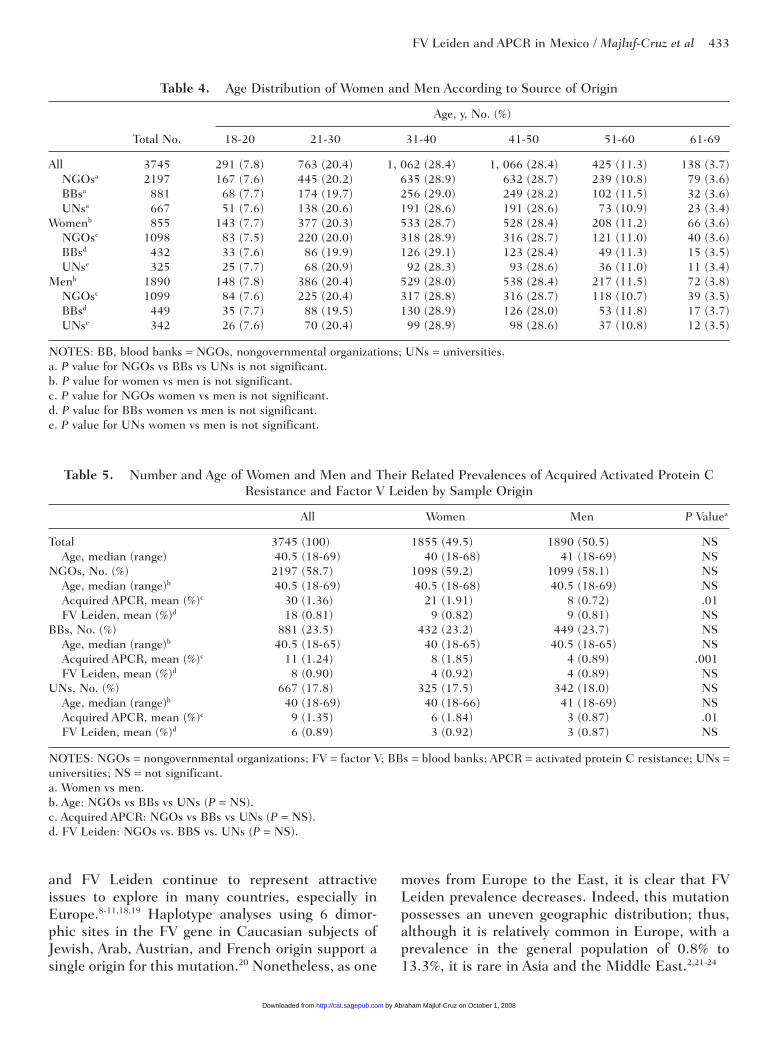
Analysis of the distribution of the individualsevaluated in this study according to the source ofrecruitment revealed that allocation was not signifi-cantly different in terms of age or sex (Table 4). Also,analysis of the distribution of cases with acquiredAPCR or FV Leiden according to the 3 sources of
Table 1. Demographic Characteristics of 4345 Healthy Mexican Individuals
Mestizo Indigenous Population, No. Population, No.
State of the Mexican Republic No. % Women Men Women Men
Aguascalientes 72 1.65 42 30 0 0Baja California Norte 86 1.97 46 40 0 0Baja California Sur 20 0.46 5 15 0 0Campeche 60 1.38 36 24 0 0Chihuahua 100 2.29 47 53 0 0Chiapas 180 4.14 110 70 95 55Coahuila 84 1.93 52 32 0 0Colima 60 1.38 22 38 0 0Distrito Federal 774 17.81 368 406 21 19Durango 110 2.53 24 86 0 0Estado de México 200 4.61 90 110 21 19Guerrero 100 2.29 59 41 0 0Guanajuato 62 1.42 49 13 0 0Hidalgo 65 1.49 45 20 13 7Jalisco 205 4.71 107 98 0 0Michoacán 100 2.29 60 40 17 13Morelos 100 2.3 93 7 0 0Nayarit 96 2.2 50 46 0 0Nuevo León 287 6.61 135 152 0 0Oaxaca 184 4.23 80 104 61 39Puebla 175 4.02 97 78 71 9Querétaro 130 2.99 106 24 0 0Quintana Roo 20 0.46 3 17 0 0San Luis Potosí 140 3.22 59 81 13 7Sinaloa 80 1.84 40 40 0 0Sonora 142 3.26 68 74 0 0Tabasco 160 3.68 72 88 0 0Tamaulipas 105 2.41 50 55 0 0Tlaxcala 70 1.61 43 27 18 12Veracruz 188 4.32 105 83 30 20Yucatán 110 2.53 37 73 20 20Zacatecas 80 1.84 35 45 0 0Total, No. (%) 4345 100 1855 (42.7) 1890 (43.5) 380 (8.7) 220 (5.1)
Table 2. Frequency of Mestizo Groups AmongMexican Individuals
Mestizo Group No. %
Spanish 3363 89.8African American 157 4.2Other European 86 2.3Italian 42 1.1French 41 1.1Lebanese 34 0.9Eastern 22 0.6Total 3745 100
by Abraham Majluf-Cruz on October 1, 2008 http://cat.sagepub.comDownloaded from
432 Clinical and Applied Thrombosis/Hemostasis / Vol. 14, No. 4, October 2008
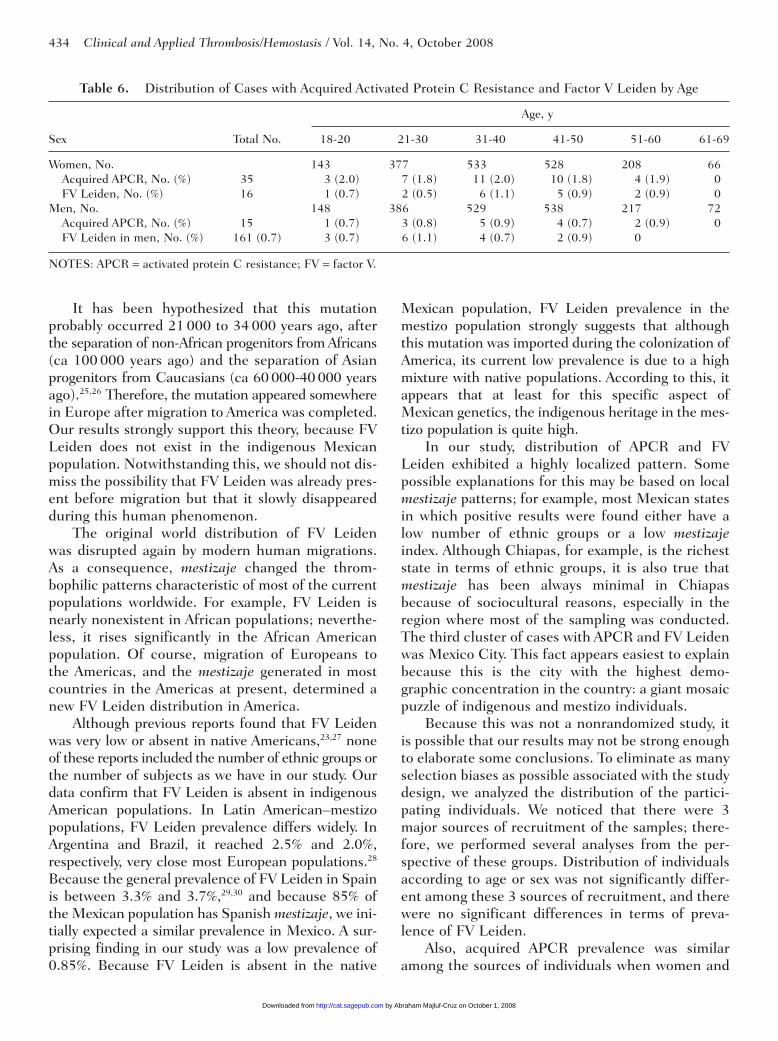
recruitment showed no differences in terms of age orFV Leiden prevalence. As expected for the total num-ber of cases of acquired APCR found in women,prevalence of this phenomenon was significantlyhigher in women than in men in all 3 groups ofanalysis (Table 5). However, no significant differ-ences were found among the 3 sources of recruit-ment when we separately analyzed men or women(Table 5). Finally, we analyzed the distribution ofcases with acquired APCR or FV Leiden according toage of the participants (Table 6). Except for thegroup of individuals aged older than 61 years, distri-bution of cases with acquired APCR was very similarthrough the analysis for both variables studied.
Discussion
Arterial and venous thrombosis is the leading causeof morbidity and mortality worldwide; therefore,basic, clinical, and epidemiologic studies leading tothe identification of new prothrombotic pathwaysare of priority. Because FV Leiden is present in up to50% of patients with a history of thrombosis, APCR
Table 3. Characteristics of 600 Mexican IndigenousIndividuals According to Ethnic Origin
Total in Group Women Men
Ethnic Group No. % No. % No. %
Nahuatl 90 15 70 11.66 20 3.33Maya 40 6.66 22 3.66 18 3.0Zapoteco 50 8.33 35 5.83 15 2.5Suave 25 4.16 18 3.0 7 1.16Mixteco 50 8.33 29 4.83 21 3.5Tzotzil 40 6.66 24 4.83 16 2.66Tocolobal 30 5.0 22 3.66 8 1.33Tzetzal 45 7.5 40 6.66 5 0.83Chanal 10 1.66 10 1.66 0 0Mame 30 5.0 15 2.5 15 2.5Lacandón 15 2.5 10 1.66 5 0.83Popoloca 35 5.83 32 5.33 3 0.5Zacapoaxtla 10 1.66 8 1.33 2 0.33Mazahua 20 3.33 18 3.0 2 0.33Otomí 15 2.5 5 0.83 10 1.66Huachil 40 6.66 25 4.16 15 2.5Huasteco 15 2.5 4 0.66 11 1.83Chinanteco 30 5.0 23 3.83 7 1.16Mazatecos 10 1.66 10 1.66 0 0Total 600 100 420 70.75 180 29.25
Mexico City: 16 (7)
Chiapas: 17 (12)
Querétaro: 7 (5)
Chihuahua:4(0)
San Luis Potosì: 14 (3)
BCN: 1 (1)
Puebla: 4 (0) BCS: 4 (0)
Jalisco: 2 (0)
Aguascalientes: 4 (1)
Sinaloa: 2 (0)
Oaxaca: 2 (0)
Nuevo León: 5 (3)
Figure 1. Distribution of activated protein C resistance (APCR) in Mexico. Numbers represent total cases of APCR that are notassociated with factor V Leiden, and numbers in parenthesis represent total of cases of APCR that are associated with factor VLeiden. Abbreviations: BCN, Baja California Norte; BCS, Baja California Sur.
by Abraham Majluf-Cruz on October 1, 2008 http://cat.sagepub.comDownloaded from
FV Leiden and APCR in Mexico / Majluf-Cruz et al 433
and FV Leiden continue to represent attractiveissues to explore in many countries, especially inEurope.8-11,18,19 Haplotype analyses using 6 dimor-phic sites in the FV gene in Caucasian subjects ofJewish, Arab, Austrian, and French origin support asingle origin for this mutation.20 Nonetheless, as one
moves from Europe to the East, it is clear that FVLeiden prevalence decreases. Indeed, this mutationpossesses an uneven geographic distribution; thus,although it is relatively common in Europe, with aprevalence in the general population of 0.8% to13.3%, it is rare in Asia and the Middle East.2,21-24
Table 4. Age Distribution of Women and Men According to Source of Origin
Age, y, No. (%)
Total No. 18-20 21-30 31-40 41-50 51-60 61-69
All 3745 291 (7.8) 763 (20.4) 1, 062 (28.4) 1, 066 (28.4) 425 (11.3) 138 (3.7)NGOsa 2197 167 (7.6) 445 (20.2) 635 (28.9) 632 (28.7) 239 (10.8) 79 (3.6)BBsa 881 68 (7.7) 174 (19.7) 256 (29.0) 249 (28.2) 102 (11.5) 32 (3.6)UNsa 667 51 (7.6) 138 (20.6) 191 (28.6) 191 (28.6) 73 (10.9) 23 (3.4)
Womenb 855 143 (7.7) 377 (20.3) 533 (28.7) 528 (28.4) 208 (11.2) 66 (3.6)NGOsc 1098 83 (7.5) 220 (20.0) 318 (28.9) 316 (28.7) 121 (11.0) 40 (3.6)BBsd 432 33 (7.6) 86 (19.9) 126 (29.1) 123 (28.4) 49 (11.3) 15 (3.5)UNse 325 25 (7.7) 68 (20.9) 92 (28.3) 93 (28.6) 36 (11.0) 11 (3.4)
Menb 1890 148 (7.8) 386 (20.4) 529 (28.0) 538 (28.4) 217 (11.5) 72 (3.8)NGOsc 1099 84 (7.6) 225 (20.4) 317 (28.8) 316 (28.7) 118 (10.7) 39 (3.5)BBsd 449 35 (7.7) 88 (19.5) 130 (28.9) 126 (28.0) 53 (11.8) 17 (3.7)UNse 342 26 (7.6) 70 (20.4) 99 (28.9) 98 (28.6) 37 (10.8) 12 (3.5)
NOTES: BB, blood banks = NGOs, nongovernmental organizations; UNs = universities.a. P value for NGOs vs BBs vs UNs is not significant.b. P value for women vs men is not significant.c. P value for NGOs women vs men is not significant.d. P value for BBs women vs men is not significant.e. P value for UNs women vs men is not significant.
Table 5. Number and Age of Women and Men and Their Related Prevalences of Acquired Activated Protein CResistance and Factor V Leiden by Sample Origin
All Women Men P Valuea
Total 3745 (100) 1855 (49.5) 1890 (50.5) NSAge, median (range) 40.5 (18-69) 40 (18-68) 41 (18-69) NS
NGOs, No. (%) 2197 (58.7) 1098 (59.2) 1099 (58.1) NSAge, median (range)b 40.5 (18-69) 40.5 (18-68) 40.5 (18-69) NSAcquired APCR, mean (%)c 30 (1.36) 21 (1.91) 8 (0.72) .01FV Leiden, mean (%)d 18 (0.81) 9 (0.82) 9 (0.81) NS
BBs, No. (%) 881 (23.5) 432 (23.2) 449 (23.7) NSAge, median (range)b 40.5 (18-65) 40 (18-65) 40.5 (18-65) NSAcquired APCR, mean (%)c 11 (1.24) 8 (1.85) 4 (0.89) .001FV Leiden, mean (%)d 8 (0.90) 4 (0.92) 4 (0.89) NS
UNs, No. (%) 667 (17.8) 325 (17.5) 342 (18.0) NSAge, median (range)b 40 (18-69) 40 (18-66) 41 (18-69) NSAcquired APCR, mean (%)c 9 (1.35) 6 (1.84) 3 (0.87) .01FV Leiden, mean (%)d 6 (0.89) 3 (0.92) 3 (0.87) NS
NOTES: NGOs = nongovernmental organizations; FV = factor V; BBs = blood banks; APCR = activated protein C resistance; UNs =universities; NS = not significant.a. Women vs men.b. Age: NGOs vs BBs vs UNs (P = NS).c. Acquired APCR: NGOs vs BBs vs UNs (P = NS).d. FV Leiden: NGOs vs. BBS vs. UNs (P = NS).
by Abraham Majluf-Cruz on October 1, 2008 http://cat.sagepub.comDownloaded from
434 Clinical and Applied Thrombosis/Hemostasis / Vol. 14, No. 4, October 2008
It has been hypothesized that this mutationprobably occurred 21 000 to 34 000 years ago, afterthe separation of non-African progenitors from Africans(ca 100 000 years ago) and the separation of Asianprogenitors from Caucasians (ca 60 000-40 000 yearsago).25,26 Therefore, the mutation appeared somewherein Europe after migration to America was completed.Our results strongly support this theory, because FVLeiden does not exist in the indigenous Mexicanpopulation. Notwithstanding this, we should not dis-miss the possibility that FV Leiden was already pres-ent before migration but that it slowly disappearedduring this human phenomenon.
The original world distribution of FV Leidenwas disrupted again by modern human migrations.As a consequence, mestizaje changed the throm-bophilic patterns characteristic of most of the currentpopulations worldwide. For example, FV Leiden isnearly nonexistent in African populations; neverthe-less, it rises significantly in the African Americanpopulation. Of course, migration of Europeans tothe Americas, and the mestizaje generated in mostcountries in the Americas at present, determined anew FV Leiden distribution in America.
Although previous reports found that FV Leidenwas very low or absent in native Americans,23,27 noneof these reports included the number of ethnic groups orthe number of subjects as we have in our study. Ourdata confirm that FV Leiden is absent in indigenousAmerican populations. In Latin American–mestizopopulations, FV Leiden prevalence differs widely. InArgentina and Brazil, it reached 2.5% and 2.0%,respectively, very close most European populations.28
Because the general prevalence of FV Leiden in Spainis between 3.3% and 3.7%,29,30 and because 85% ofthe Mexican population has Spanish mestizaje, we ini-tially expected a similar prevalence in Mexico. A sur-prising finding in our study was a low prevalence of0.85%. Because FV Leiden is absent in the native
Mexican population, FV Leiden prevalence in themestizo population strongly suggests that althoughthis mutation was imported during the colonization ofAmerica, its current low prevalence is due to a highmixture with native populations. According to this, itappears that at least for this specific aspect ofMexican genetics, the indigenous heritage in the mes-tizo population is quite high.
In our study, distribution of APCR and FVLeiden exhibited a highly localized pattern. Somepossible explanations for this may be based on localmestizaje patterns; for example, most Mexican statesin which positive results were found either have alow number of ethnic groups or a low mestizajeindex. Although Chiapas, for example, is the richeststate in terms of ethnic groups, it is also true thatmestizaje has been always minimal in Chiapasbecause of sociocultural reasons, especially in theregion where most of the sampling was conducted.The third cluster of cases with APCR and FV Leidenwas Mexico City. This fact appears easiest to explainbecause this is the city with the highest demo-graphic concentration in the country: a giant mosaicpuzzle of indigenous and mestizo individuals.
Because this was not a nonrandomized study, itis possible that our results may not be strong enoughto elaborate some conclusions. To eliminate as manyselection biases as possible associated with the studydesign, we analyzed the distribution of the partici-pating individuals. We noticed that there were 3major sources of recruitment of the samples; there-fore, we performed several analyses from the per-spective of these groups. Distribution of individualsaccording to age or sex was not significantly differ-ent among these 3 sources of recruitment, and therewere no significant differences in terms of preva-lence of FV Leiden.
Also, acquired APCR prevalence was similaramong the sources of individuals when women and
Table 6. Distribution of Cases with Acquired Activated Protein C Resistance and Factor V Leiden by Age
Age, y
Sex Total No. 18-20 21-30 31-40 41-50 51-60 61-69
Women, No. 143 377 533 528 208 66Acquired APCR, No. (%) 35 3 (2.0) 7 (1.8) 11 (2.0) 10 (1.8) 4 (1.9) 0FV Leiden, No. (%) 16 1 (0.7) 2 (0.5) 6 (1.1) 5 (0.9) 2 (0.9) 0
Men, No. 148 386 529 538 217 72Acquired APCR, No. (%) 15 1 (0.7) 3 (0.8) 5 (0.9) 4 (0.7) 2 (0.9) 0FV Leiden in men, No. (%) 161 (0.7) 3 (0.7) 6 (1.1) 4 (0.7) 2 (0.9) 0
NOTES: APCR = activated protein C resistance; FV = factor V.
by Abraham Majluf-Cruz on October 1, 2008 http://cat.sagepub.comDownloaded from

FV Leiden and APCR in Mexico / Majluf-Cruz et al 435
men were separately analyzed. We believe that allthese data support the assumption that the studydesign did not affect the final results of the study. Onthe other hand, it should be noticed that a higherprevalence of acquired APCR was found in womenthan in men. This significantly higher prevalence ofacquired APCR in women not associated with a sim-ilar increase in the prevalence of FV Leiden suggeststhat the mechanism(s) responsible for this phenom-enon is likely associated with specific factors presentin women.
The significance of APCR occurring in theabsence of mutations of the FV gene, also calledacquired APCR, is well recognized, although infor-mation about it remains scarce. Owing to the num-ber of potential confounders, only a few studies haveanalyzed APCR as an independent thrombotic riskfactor. Subjects within the highest quintile of APCRhave an increased risk of stroke compared withthose in the lowest quintile, without significantchanges after correction for FV Leiden status.31 Apopulation study observed a relationship betweenquintiles of APCR and peripheral artery disease;again, no difference was observed after adjustmentfor FV Leiden.32 This finding was not unexpectedowing to the association between APCR and throm-bosis in nonwhite populations in which FV muta-tions are nearly absent.33 Two additional surveys alsoobserved increased risk of venous thrombosis amongsubjects with acquired APCR.34,35
Although acquired APCR prevalence hasbeen underestimated, a study representative of aCentral European population found APCR preva-lence was at least as frequent as FV Leiden itself.32
In the population-based Vicenza Thrombophilia andArteriosclerosis Project, FV Leiden and APC ratiosof 0.84 and below occurred at a ratio of 1:4.36 It there-fore appears that APCR in itself is an independentprothrombotic phenotype and that the thrombophilicstate it induces should receive greater emphasis inclinical practice in the future.
Several mechanisms have been proposed toexplain the phenomenon of acquired APCR in differentclinical settings; however, a clear explanation is notyet available. Conditions such as lupus anticoagulant,anticardiolipin and anti-β2-glycoprotein I antibod-ies,37,38 systemic lupus erythematosus,39 pregnancy,40-42
acquired immunodeficiency syndrome,43 arterial hyper-tension,44 oral contraceptive intake,45-47 oral hormonereplacement therapy,48 multiple myeloma,15,49 andcancer50-52 can induce acquired APCR; thus, the plasmaassay can afford misleading results additionally in
the absence of FV Leiden.53,54 Because the originallydescribed test based on the activated partial throm-boplastin time is not specific for FV Leiden, manystrategies have been devised to render coagulation-based APCR assays more specific for FV Leiden.55
The nature of our research led us to use an FV-specificassay as global screening, and in subjects with a pos-itive test result, a second assay using a differenttechnical principle was chosen. No woman with a pos-itive test result for APCR was taking hormonal drugs.
It is noteworthy that only 31% of APCR carrierswere also FV Leiden carriers. It has been suggestedthat a high number of healthy individuals without afamily history of thrombosis may be carriers of thisphenotype. Of course, the non-FV Leiden APCR phe-notype can be due to other rare FV mutations or to atrue acquired condition. However, the prevalence ofother FV mutations responsible for the inherited APCRis so low that they may be considered irrelevant.15
In our transversal analysis, prevalence ofacquired APCR reached 1.33%. We consider theseindividuals as true carriers of acquired APCRbecause (1) they had an initial positive test as evalu-ated by 2 different assays; (2) they had a negativetest at least 3 months after the first assay, againusing the same 2 assays (undoubtedly, these 2 factsstrongly support the transient and noninheritablenature of the phenomenon); (3) as expected, allcases with APCR in the first and second studyphases were FV Leiden carriers; and (4) all patientswith transient APCR had a negative FV Leiden testresult. Absence of known diseases when APCR waspositive confirms that this phenomenon may bepresent with moderate prevalence during brief timeperiods in healthy subjects.
Conclusion
Our results show a very low prevalence of APCR andFV Leiden in Mexico. Based on the number of nativeAmerican individuals from several ethnic groups, weconfirmed that neither APCR nor FV Leiden affectnative Americans. This fact strongly supports thehypothesis of the appearance of FV Leiden aftermigration from Europe began. We have shown thatin the general population in Mexico, there exist noFV gene mutations that are different from the Leidenabnormality. Mutations in the FV gene are responsiblefor solely 31% of cases with APCR, signifying thatacquired APCR is nearly twice as prevalent as theinherited variant. Of course, the clinical importance of
by Abraham Majluf-Cruz on October 1, 2008 http://cat.sagepub.comDownloaded from
this data requires clarification in specifically designedstudies to evaluate its impact on thrombosis. On thebasis of our data, it is possible to suggest that at leastfor ACPR and FV Leiden, there is a profoundindigenous effect on mestizo population in Mexico.
References
1. Goldhaber SZ. Epidemiology of pulmonary embolism anddeep vein thrombosis. In: Bloom AL, Forber CD, ThomasDP, Tuddenham ED, eds. Haemostasis and Thrombosis.New York, NY: Churchill Livingstone; 1994:66-79.
2. Dahlbäck B. Inherited thrombophilia: resistance to acti-vated protein C as a pathogenic factor of venous throm-boembolism. Blood. 1995;85:607-614.
3. Malm J, Laurell M, Nilsson IM, Dahlbäck B. Thromboem-bolic disease: critical evaluation of laboratory investiga-tion. Thromb Haemost. 1992;68:7-13.
4. Miletich JP, Prescott SM, White R, Majerus PW, BovillEG. Inherited predisposition to thrombosis. Cell. 1993;72:477-480.
5. Tabernero MD, Tomas JF, Alberca I, Orfao A, LópezBorrasca A, Vicente V. Incidence and clinical character-istics of hereditary disorders associated with venousthrombosis. Am J Hematol. 1991;36:249-254.
6. Dahlbäck B. New molecular insights into the genetics ofthrombophilia. Resistance to activated protein C causedby Arg506 to Gln mutation in factor V as a pathogenicrisk factor for venous thrombosis. Thromb Haemost.1995;74:139-148.
7. Faioni EM, Franchi F, Asti D, Sacchi E, Bernardi F,Mannucci PM. Resistance to activated protein C in ninethrombophilic families: Interference in a protein S func-tional assay. Thromb Haemost. 1993;70:1067-1071.
8. Voorberg J, Roelse J, Koopman R, et al. Association of idio-pathic venous thromboembolism with single point-mutationat Arg506 of factor V. Lancet 1994;343:1535-1536.
9. Koster T, Rosendaal FR, de Ronde H, Briet E,Vandenbroucke JP, Bertina RM. Venous thrombosis due topoor anticoagulant response to activated protein C: Leidenthrombophilia study. Lancet 1993;342:1503-1506.
10. Griffin JH, Evatt B, Wideman C, Fernandez JA.Anticoagulant protein C pathway defective in a majorityof thrombophilic patients. Blood. 1993;82:1989-1993.
11. Halbmayer WM, Haushofer A, Schon R, Fischer M. Theprevalence of poor anticoagulant response to activatedprotein C (APC resistance) among patients sufferingfrom stroke or venous thrombosis and among healthysubjects. Blood Coagul Fibrinolysis. 1994;5:51-57.
12. Dahlbäck B. Factor V gene mutation causing inheritedresistance to activated protein C as a basis for venousthromboembolism. J Intern Med. 1995;237:221-227.
13. Clark P, Walker ID. The phenomenon known asacquired activated protein C resistance. Br J Haematol.2001;115:767-773.
14. Lisker R, Ramírez E, Babinsky V. Genetic structure ofautochthonous populations of Meso-America: Mexico.Hum Biol. 1996, 68:395-404.
15. Elice F, Fink L, Tricot G, Barlogie B, Zangari M.Acquired resistance to activated protein C (aAPCR) inmultiple myeloma is a transitory abnormality associatedwith an increased risk of venous thromboembolism. Br JHaematol. 2006;134:399-405.
16. Bertina RM, Koeleman BP, Koster T, et al. Mutation inblood coagulation factor V associated with resistance toactivated protein C. Nature. 1994;369:64-67.
17. Instituto Nacional de Estadística, Geografía e Informática.XII Censo Nacional de Población y Vivienda. 2000.Available at: www.inegi.gob.mx. Accessed July 19, 2007.
18. Dahlbäck B, Carlsson M, Svensson PJ. Familial throm-bophilia due to a previously unrecognized mechanismcharacterized by poor anticoagulant response to acti-vated protein C: prediction of a cofactor to activated pro-tein C. Proc Natl Acad Sci U S A. 1993;90:1004-1008.
19. Kisiel W, Canfield WM, Ericsson LH, Davie EW.Anticoagulant properties of bovine plasma protein Cfollowing activation by thrombin. Biochemistry. 1977;16:5824-5831.
20. Zivelin A, Griffin JH, Xu X, et al. A single genetic originfor a common Caucasian risk factor for venous throm-bosis. Blood. 1997;89:397-402.
21. Nemerson Y. The tissue factor pathway of blood coagu-lation. Semin Hematol. 1992;29:170-176.
22. Kane WH, Davie EW. Blood coagulation factors V andVIII: structural and functional similarities and theirrelationship to hemorrhagic and thrombotic disorders.Blood. 1988;71:539-555.
23. Rees DC, Cox M, Clegg JB. World distribution of factorV Leiden. Lancet 1995;346:1133-1134.
24. Hallam PJ, Millar DS, Krawczak M, Kakkar VV,Cooper DN. Population differences in the frequency ofthe factor V Leiden variant among people with clinicallysymptomatic protein C deficiency. J Med Genet 1995;32:543-545.
25. Cox MJ, Rees DC, Martinson JJ, Clegg JB. Evidence fora single origin of factor V Leiden. Br J Haematol. 1996;92:1022-1025.
26. Castoldi E, Lunghi B, Mingozzi F, Ioannou P, Marcheti G,Bernardi F. New coagulation factor V gene polymorphismsdefine a single and infrequent haplotype underlying thefactor V Leiden mutation in Mediterranean populationsand Indians. Thromb Haemost. 1997;78:1037-1041.
27. Pepe G, Rickards O, Camacho Vanegas O, et al. Prevalenceof factor V Leiden mutation in non-European popula-tions. Thromb Haemost. 1997;77:329-331.
28. Hepner M, Roldan A, Pieroni G, et al. Frequency of fac-tor V Arg506 to Gln mutation (FV Leiden) and activatedprotein C resistance in blood donors in Argentina. A pre-liminary study. Thromb Haemost. 1997;78(suppl):226.
29. Martinez E, Tirado I, Vallve C, et al. Prevalenceof resistance to activated protein C in patients with
436 Clinical and Applied Thrombosis/Hemostasis / Vol. 14, No. 4, October 2008
by Abraham Majluf-Cruz on October 1, 2008 http://cat.sagepub.comDownloaded from
FV Leiden and APCR in Mexico / Majluf-Cruz et al 437
thrombosis in Spanish population. Thromb Haemost.1997;78(suppl): 223.
30. Garcia-Gala JM, Alvarez V, Pinto CR, et al. Factor VLeiden (R506Q) and risk of venous thromboembolism:a case-control study based on the Spanish population.Clin Genet 1997;52:206-210.
31. van der Bom JG, Bots ML, Haverkate F, et al. Reducedresponse to activated protein C is associated withincreased risk for cerebrovascular disease. Ann InternMed. 1996;125:265-269.
32. Kiechl S, Muigg A, Santer P, et al. Poor response toactivated protein C as a prominent risk predictor ofadvanced atherosclerosis and arterial disease. Circulation.1999;99:614-619.
33. Sakata T, Kario K, Katayama Y, Matsuyama T, Kato H,Miyata T. Clinical significance of activated protein Cresistance as a potential marker for hypercoagulablestate. Thromb Res. 1996;82:235-244.
34. De Visser MC, Rosendaal FR, Bertina RM. A reducedsensitivity for activated protein C in the absence of fac-tor V Leiden increases the risk of venous thrombosis.Blood. 1999;93:1271-1276.
35. Rodeghiero F, Tosetto A. Activated protein C resistanceand factor V Leiden mutation are independent risk factorsfor venous thromboembolism. Ann Intern Med. 1999;130:643-650.
36. Tosetto A, Castaman G, Cappellari A, Rodeghiero F. TheVITA Project: inheritability of resistance to activatedprotein C. Thromb Haemost. 2000;84:811-814.
37. Gennari L, Blanco A. Alberto MF, Grosso S, Lazzari MA.The concomitant presence of lupus anticoagulant, anti-cardiolipin and anti-[beta]2-glycoprotein I antibodiescould be associated with acquired activated protein Cresistance in non-systemic lupus erythematosuspatients. Br J Haematol. 2003;121:527-529.
38. Male C, Mitchell L, Julian J, et al. Acquired activatedprotein C resistance is associated with lupus anticoagu-lants and thrombotic events in pediatric patients withsystemic lupus erythematosus. Blood. 2001;97:844-849.
39. Nojima J, Kuratsune H, Suehisa E, et al. Acquired acti-vated protein C resistance is associated with the co-exis-tence of anti-prothrombin antibodies and lupusanticoagulant activity in patients with systemic lupuserythematosus. Br J Haematol. 2002;118:577-583.
40. Benedetto C, Marozio L, Tavella AM, Maulà V,Carmignani D, Curti A. Response to activated protein Cdecreases throughout pregnancy. Acta Obstet GynecolScand. 2002;81:1028-1032.
41. Samama MM, Rached RA, Horellou MH, et al.Pregnancy-associated venous thromboembolism (VTE)in combined heterozygous factor V Leiden (FVL) andprothrombin (FII) 20210 A mutation and in heterozy-gous FII single gene mutation alone. Br J Haematol.2003;123:327-334.
42. Robertson L, Wu O, Langhorne P, et al. Thrombophiliain pregnancy: a systematic review. Br J Haematol. 2005;132:171-196.
43. Majluf-Cruz A, Silva-Estrada M, Sanchez-Barboza R, et al.Venous thrombosis among patients with AIDS. Clin ApplThromb Hemost. 2004;10:19-25.
44. Makris TK, Krespi PG, Hatzizacharias AN, et al. Resistanceto activated protein C and FV Leiden mutation inpatients with a history of acute myocardial infarction orprimary hypertension. Am J Hypertens. 2000;13:61-65.
45. Olivieri O, Friso S, Manzato F, et al. Resistance to acti-vated protein C in healthy women taking oral contra-ceptives. Br J Haematol. 1995;91:465-470.
46. van Vliet HA, Frolich M, Christella M, et al. Associationbetween sex hormone-binding globulin levels and acti-vated protein C resistance in explaining the risk ofthrombosis in users of oral contraceptives containingdifferent progestogens. Hum Reprod. 2004;20:563-568.
47. Gardiner C, Mackie IJ, Furs SA, Piegsa K, Guillebaud J,Machin SJ. Acquired resistance to activated protein C ismore pronounced in women receiving combined oral con-traceptives containing desogestrel than levonorgestrel andis associated with low protein S levels. Br J Haematol.2003;121(suppl 1):62.
48. Post MS, Rosing J, Van Der Mooren MJ, et al; AgeingWomen and the Institute for Cardiovascular Research-Vrije Universiteit (ICaR-VU). Increased resistance toactivated protein C after short-term oral hormone replace-ment therapy in healthy post-menopausal women. Br JHaematol. 2002;119:1017-1023.
49. Zangari M, Saghafifar F, Anaissie E, et al. Activated pro-tein C resistance in the absence of FV Leiden mutationis a common finding in multiple myeloma and is associ-ated with an increased risk of thrombotic complications.Blood Coagul Fibrinolysis. 2002;13:187-192.
50. De Lucia D, de Vita F, Orditura M, et al. Hypercoagulablestate in patients with advanced gastrointestinal cancer:evidence for an acquired resistance to activated proteinC. Tumori. 1997;83:948-952.
51. Green D, Maliekel K, Sushko E, Akhtar R, Soff GA.Activated protein C resistance in cancer patients.Haemostasis. 1997;27:112-118.
52. Haim N, Lanir N, Hoffman R, Haim A, Tsalik M,Brenner B. Acquired protein C resistance is common incancer patients and is associated with venous throm-boembolism. Am J Med. 2001;110:91-96.
53. De Stefano V, Leone G. Resistance to activated proteinC due to mutated factor V as a novel cause of inheritedthrombophilia. Haematologica. 1995;80:344-356.
54. Dahlbäck B. Protein S and C4b-binding protein: com-ponents involved in the regulation of the protein C anti-coagulant system. Thromb Haemost. 1991;66:49-61.
55. Guerrero F, Arnaud C, Nguyen F, Boneu B, Sié P.Comparison of three activated protein C resistance testsin the risk assessment of venous thrombosis in non-car-riers of the factor V Leiden mutation. Thromb Haemost.2006;95:728-734.
by Abraham Majluf-Cruz on October 1, 2008 http://cat.sagepub.comDownloaded from
Related Documents











