3/8/2014 1 ACTION Registry ACTION Registry ACTION Registry ACTION Registry – GWTG GWTG GWTG GWTG Version 2.4 Version 2.4 Version 2.4 Version 2.4 Dr. Joanne Foody Kim Hustler The following relationships exist: Dr. Foody:Janssen, Sanofi, Genzyme, Aegerion, Amarin, BristolMeyersSquibb, Abbott, Gilead, ACC, Pfizer, Merck Kim Hustler: No Disclosures Session Objectives • Outline the data points that will be changing for ACTION Registry – GWTG Version 2.4 • Discuss the rationale and implications for the changes in the data elements

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

3/8/2014
1
ACTION Registry ACTION Registry ACTION Registry ACTION Registry –––– GWTG GWTG GWTG GWTG
Version 2.4Version 2.4Version 2.4Version 2.4
Dr. Joanne Foody
Kim Hustler
The following relationships exist:
Dr. Foody:Janssen, Sanofi, Genzyme, Aegerion,
Amarin, BristolMeyersSquibb, Abbott, Gilead,
ACC, Pfizer, Merck
Kim Hustler: No Disclosures
Session Objectives
• Outline the data points that will be changing
for ACTION Registry – GWTG Version 2.4
• Discuss the rationale and implications for
the changes in the data elements

3/8/2014
2
Disclosures
• Dr. Joanne Foody
– No Disclosures to report
• Kim Hustler
– No Disclosures to report
Version 2.4 Update - Why Change?
• New therapies/medications
• Research/Clinical Guidelines
• Collaborative/Integrated Care
• Improved quality of data in registry
• Public reporting
– Physician reporting
• Aligning with other NCDR Registries
ARS Question #1
Who Who Who Who did we include in the process of did we include in the process of did we include in the process of did we include in the process of
determining what fields to adddetermining what fields to adddetermining what fields to adddetermining what fields to add????
1. Email suggestions
2. RSM calls
3. Focused RSM teleconferences
4. Physician committee meetings
5. All of the above

3/8/2014
3
ARS Question #2
How did we determine what fields to remove?How did we determine what fields to remove?How did we determine what fields to remove?How did we determine what fields to remove?
1. Frequency of fields being answered
2. Current practice
3. Core data elements
4. Enough data already captured
5. All of the above
ACTION -GWTG Q.I.
Subcommittee Members
• Dr. Joanne Foody – Chair
• Dr. Karen Alexander
• Dr. Donald Casey
• Dr. Shahriar Dadkhah
• Dr William French
• Dr. Michael Ho
• Dr. Mauro Moscucci
• Dr. Gregg Fonarow
• Dr. Judith Lichtman
• Dr. Nurcan Illksoy
• Dr. James Jollis
• Dr. Mikhail Kosiborod
Process
• SQOC – Science & Quality Oversight
Committee
• ACTION Registry – GWTG Steering
Committee
• Stakeholder feedback
• NCDR Management Board
•

3/8/2014
4
Registry Site Manager Calls
• Calls were specifically to obtain feedback
from users
• Two Teleconferences
�September 27, 2011
�October 6, 2011
Be Careful What
You Ask For!
Version 2.4 Changes
New therapies/medicationsNew therapies/medicationsNew therapies/medicationsNew therapies/medications
• Medications
– Dabigatran
– Rivaroxaban
– Apixaban
– Statin therapy at discharge, new fields
• Hypothermia Protocol

3/8/2014
5
Section E- Medications
New medication: Xarelto (Rivaroxaban)
Documentation:Documentation:Documentation:Documentation:
• History of Atrial fibrillation
• Presents with symptoms of ACS
• Positive Troponins- NSTEMI
• Physician discharges patient on Xarelto
ARS Question # 32
How will How will How will How will you enter you enter you enter you enter the Xarelto in the data the Xarelto in the data the Xarelto in the data the Xarelto in the data
collection tool?collection tool?collection tool?collection tool?
1.Do not include
2.Answer Warfarin at discharge Seq. #6220
as “contraindicated”
3.Answer Warfarin at discharge Seq. #6220
as “yes”
3/8/2014
6
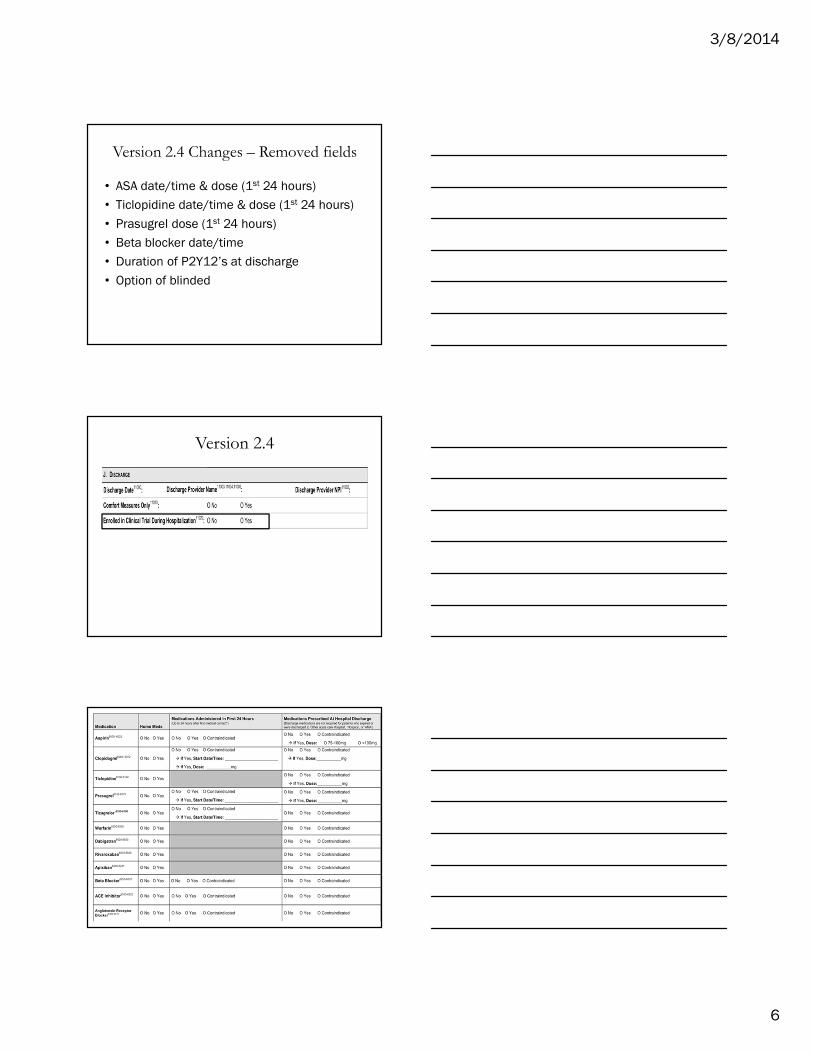
Version 2.4 Changes – Removed fields
• ASA date/time & dose (1st 24 hours)
• Ticlopidine date/time & dose (1st 24 hours)
• Prasugrel dose (1st 24 hours)
• Beta blocker date/time
• Duration of P2Y12’s at discharge
• Option of blinded
Version 2.4

3/8/2014
7
Version 2.4 Changes
• New field for Statin therapy at discharge
• “Less than Intensive” Statin Therapy
• “Intensive” Statin Therapy
Version 2.4 Changes
• Unfractionated Heparin
Version 2.4 Changes
• GP IIB/IIIA Inhibitors

3/8/2014
8
Version 2.4 Changes
• Anticoagulants removed
Section E- Medications
Excessive dosing UFH- no PCI
Documentation:Documentation:Documentation:Documentation:
• Presents with N/V, left arm pain
• 12 lead ECG- STEMI
• To cath lab for primary PCI- 5000 units UFH
given in cath lab
• Coronary arteries- clean
• No PCI is performed
Excessive dosing UFH- no PCIThe data collection form would be completed as:
• Reperfusion Candidate #8000 “yes”
• Primary PCI #8015 “no” Reason no PCI #8030- Anatomy
not suitable to primary PCI
• Thrombolytic “no”, reason #8035- Expected DTB <90 min- if
was expected

3/8/2014
9
ARS Question # 4
Would this patient be included in the UFH Would this patient be included in the UFH Would this patient be included in the UFH Would this patient be included in the UFH
Excessive dosing report as we are currently Excessive dosing report as we are currently Excessive dosing report as we are currently Excessive dosing report as we are currently
entering itentering itentering itentering it????
1. No
2. Yes
Answer: #1 (No)
• As of October 1, 2013 discharges “Diagnostic
Angiography Time” Seq. #7022 is the identifying
time for UFH doses administered in the cath lab
• If date/time of UFH Seq. #6852/6853 is prior to prior to prior to prior to
Angiography time, it is included
• If afterafterafterafter Angiography time- dose is excluded
Section E- Medications
Excessive dosing UFH
DocumentationDocumentationDocumentationDocumentation::::
• Presents with N/V, left arm pain at 04:00
• 12 lead ECG- negative
• Cardiac Biomarkers elevated- NSTEMI
• Weight 100 kg
• ED starts UFH infusion at 1000 U at 05:00
• To cath lab at 08:00
• 5000 U IV bolus in cath lab administered at 08:15

3/8/2014
10
ARS Question # 5
Would this patient be included in the UFH Would this patient be included in the UFH Would this patient be included in the UFH Would this patient be included in the UFH
Excessive dosing report as we are currently Excessive dosing report as we are currently Excessive dosing report as we are currently Excessive dosing report as we are currently
entering itentering itentering itentering it????
1. No
2. Yes
V2.4 Excessive dose UFH • V2.4 will capture date/time for both initial doses (bolus &
infusion)
• The dates/times provide verification of administration prior
to or after arrival in cath lab
• Patient can only ‘fail’ the Excessive Dosing metric once
Version 2.4 Changes
Aligning RegistriesAligning RegistriesAligning RegistriesAligning Registries
• PCI Indications
• Arterial access site
• Demographics/Race Fields
• Mobile ICU
3/8/2014
11
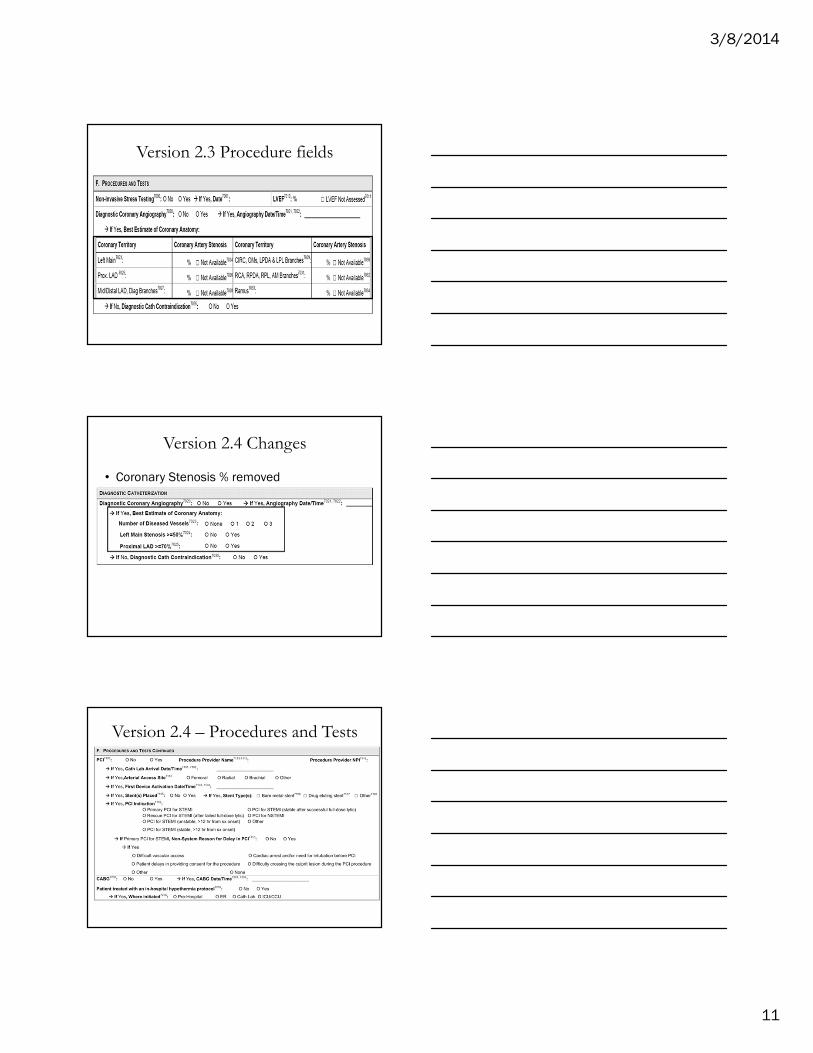
Version 2.3 Procedure fields
Version 2.4 Changes
• Coronary Stenosis % removed
Version 2.4 – Procedures and Tests

3/8/2014
12
Version 2.4 Changes
PCI Indications & arterial access sitePCI Indications & arterial access sitePCI Indications & arterial access sitePCI Indications & arterial access site
Version 2.4 Changes
Hypothermia therapyHypothermia therapyHypothermia therapyHypothermia therapy
Section F- Procedures & Tests
PCI Indication V2.4
Documentation:Documentation:Documentation:Documentation:
• Presents with N/V & chest pressure
• Chest pressure started 2 days ago
• Vomiting started at 08:00, worsening CP
• ECG- ST elevation
• Emergently to cath lab at 09:45

3/8/2014
13
ARS Question # 62
What would you select for PCI Indication?What would you select for PCI Indication?What would you select for PCI Indication?What would you select for PCI Indication?
1.1.1.1. Primary PCI for STEMIPrimary PCI for STEMIPrimary PCI for STEMIPrimary PCI for STEMI
2.2.2.2. PCI for STEMI (unstable, >12 PCI for STEMI (unstable, >12 PCI for STEMI (unstable, >12 PCI for STEMI (unstable, >12 hrhrhrhr from from from from sxsxsxsx onset)onset)onset)onset)
3.3.3.3. PCI for STEMI PCI for STEMI PCI for STEMI PCI for STEMI (stable(stable(stable(stable, >12 , >12 , >12 , >12 hrhrhrhr from from from from sxsxsxsx onsetonsetonsetonset))))
Version 2.4 Additions
DemographicsDemographicsDemographicsDemographics---- Race detail linesRace detail linesRace detail linesRace detail lines
Section A- Demographics
Hispanic or Latino Ethnicity
Documentation:Documentation:Documentation:Documentation:
• Presents meeting criteria for NSTEMI
• Noted in town visiting family, home Mexico
• Her last name is Garcia
• Primary language: English
• Secondary language: Spanish
• No documentation of race/ethnicity in medical
record

3/8/2014
14
ARS Question #72
How How How How would you would you would you would you answer Hispanic or Latino answer Hispanic or Latino answer Hispanic or Latino answer Hispanic or Latino
Ethnicity Seq. #2076?Ethnicity Seq. #2076?Ethnicity Seq. #2076?Ethnicity Seq. #2076?
1. No
2. Yes
3. Yes, Mexican
Version 2.4 Changes
Research/Clinical GuidelinesResearch/Clinical GuidelinesResearch/Clinical GuidelinesResearch/Clinical Guidelines
• Additional In-Hospital Clinical events
• Home Functioning/Cognitive Status
In-Hospital Clinical Events

3/8/2014
15
Version 2.4 Changes
Home FunctioningHome FunctioningHome FunctioningHome Functioning
Version 2.4 Changes• Cocaine use
• COPD
• Atrial fib or flutter- “past 2 weeks” “past 2 weeks” “past 2 weeks” “past 2 weeks” removed
Version 2.4 Changes
• Cancer history added
• Detail under Cerebrovascular disease

3/8/2014
16
Version 2.4 Changes
Collaborative/Integrated CareCollaborative/Integrated CareCollaborative/Integrated CareCollaborative/Integrated Care
• Two FMC fields to capture non-EMS FMC
• Non-system reason for delay for First
Medical Contact
• Additional EMS fields & cath lab activation
Two FMC fields to capture nonTwo FMC fields to capture nonTwo FMC fields to capture nonTwo FMC fields to capture non----EMS FMCEMS FMCEMS FMCEMS FMC
NonNonNonNon----system system system system reason for delay for First Medical reason for delay for First Medical reason for delay for First Medical reason for delay for First Medical
ContactContactContactContact
Version 2.4 Changes for FMC
Section B- Admission
Means of Transport to First Facility
Documentation:Documentation:Documentation:Documentation:
• EMS called to home of female with symptoms of ACS
• BLS unit dispatched, ALS unit arrived 5 minutes later
• 12 Lead ECG read- ST elevation
• ASA is administered
• ECG reading phoned into ED
• ALS unit transported to primary PCI hospital

3/8/2014
17
ARS Question # 8
What would you enter for Means of What would you enter for Means of What would you enter for Means of What would you enter for Means of
Transport to First Facility?Transport to First Facility?Transport to First Facility?Transport to First Facility?
1. Self/Family
2. Ambulance
3. Mobile ICU
Section B- Admission
First Medical Contact time Seq. #3106
Documentation: Documentation: Documentation: Documentation:
• Presented to physician office at 11:30 with 2 hours
of epigastric pain, and pain radiating down left arm
• ECG- STEMI
• EMS patient contact time 11:50- transported by
ambulance to PCI hospital
• Immediate Primary PCI
ARS Question # 9
What time would you enter in for First What time would you enter in for First What time would you enter in for First What time would you enter in for First
Medical Contact time Seq. #3106?Medical Contact time Seq. #3106?Medical Contact time Seq. #3106?Medical Contact time Seq. #3106?
1. 11:30 Physician Office contact time
2. 11:50 EMS contact time
3. Leave time blank

3/8/2014
18
Data Collection FormStarting with January 1, 2014 discharges
Enter into Auxiliary field 4 the response to question:
Was EMS the first medical contact?
Data Collection ToolEnter “Y” or “N” into Auxiliary field 4 under Discharge
Note- answer “N” when no first medical contact
Additional EMS fields & Additional EMS fields & Additional EMS fields & Additional EMS fields & cathcathcathcath lab activationlab activationlab activationlab activation
Version 2.4 Changes

3/8/2014
19
Version 2.4 Changes
Improved quality of data in registry Improved quality of data in registry Improved quality of data in registry Improved quality of data in registry
• Non-system reason for delay for ECG’s
• Geographic concerns with D2B patients
• Initial and peak lab values
Version 2.4 Changes
NonNonNonNon----system system system system reason for delay for ECG’sreason for delay for ECG’sreason for delay for ECG’sreason for delay for ECG’s
V2.4 Changes
Door to ECG Quality Metric #22
Documentation: Documentation: Documentation: Documentation:
• EMS arrives at scene patient in cardiac arrest
• Code ran 11 minutes- Defib, CPR, meds-
resuscitated
• Transported to hospital- presented in cardiac arrest
at 11:05
• Coded for 10 minutes-resuscitated
• ECG- at 11:20- STEMI
• Immediate Primary PCI
3/8/2014
20
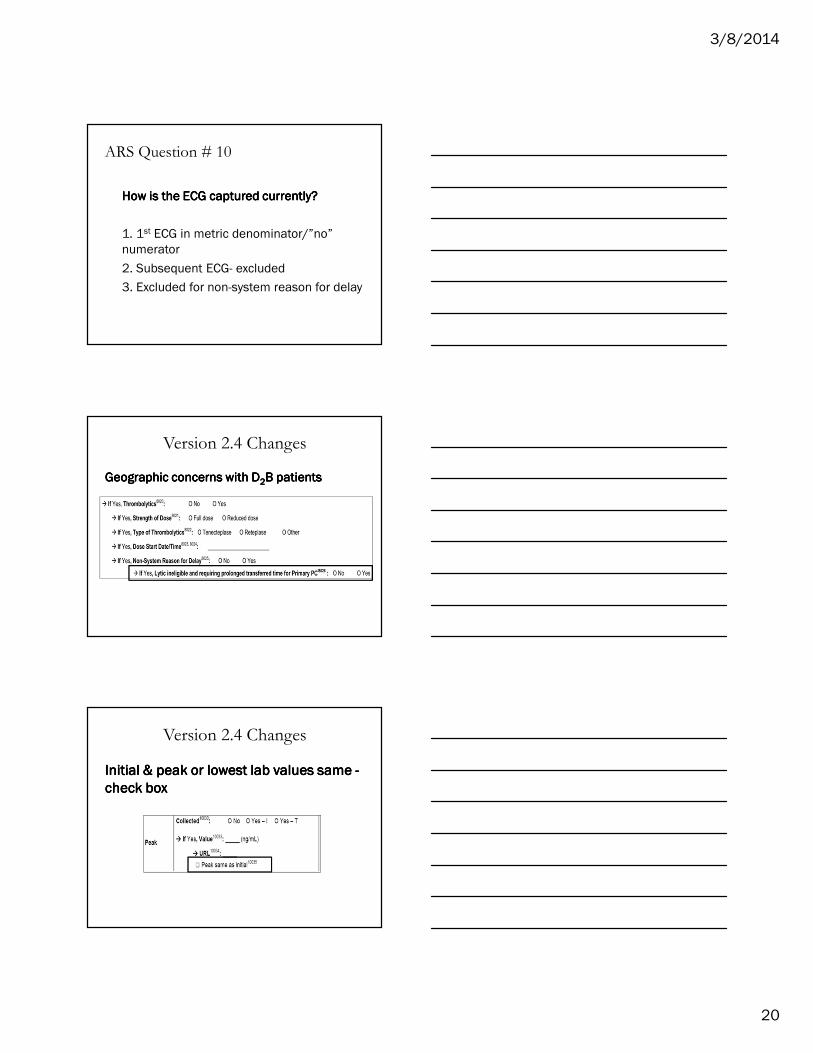
ARS Question # 10
How is the ECG captured currently?How is the ECG captured currently?How is the ECG captured currently?How is the ECG captured currently?
1. 1st ECG in metric denominator/”no”
numerator
2. Subsequent ECG- excluded
3. Excluded for non-system reason for delay
Version 2.4 Changes
Geographic concerns with DGeographic concerns with DGeographic concerns with DGeographic concerns with D2222B patientsB patientsB patientsB patients
Version 2.4 Changes
Initial Initial Initial Initial & peak or lowest lab values same & peak or lowest lab values same & peak or lowest lab values same & peak or lowest lab values same ----
check boxcheck boxcheck boxcheck box

3/8/2014
21
Version 2.4 Changes
Troponin & CKTroponin & CKTroponin & CKTroponin & CK----MB MB MB MB initial initial initial initial and and and and peak peak peak peak –––– date/time date/time date/time date/time
fields removedfields removedfields removedfields removed
Version 2.4 Changes
Public reporting/ Core MeasuresPublic reporting/ Core MeasuresPublic reporting/ Core MeasuresPublic reporting/ Core Measures
• LVEF measured after discharge
Version 2.4 Changes
Public reportingPublic reportingPublic reportingPublic reporting
• Physician Provider Number (NPI)
�Admitting
�Procedure
�Discharge

3/8/2014
22
Physician Level Dashboard Reporting
Physician Quality Reporting System
(PQRS)
• Reimbursement
– Promotes reporting of quality information by
eligible providers
– Providers identified by NPI #
Limited and Premier Forms- Current
140 fields in Limited vs. 280 fields in Premier
– Simple/Avg pt = 60 - 80 fields vs. 100 - 150 in Premier
– Complicated pt = 80 - 100 fields vs. 150 - 200 in
Premier
– Non PCI centers 60 fields vs. 100 in Premier
Strongly encourage participants to use Premier
data set, especially P-PCI capable centers

3/8/2014
23
Limited and Premier Forms- V 2.4
• 160 fields in Limited vs. 260 fields in
Premier
– Addition of fields in Limited include:
• EMS fields (Mission Lifeline reporting)
• Reasons for no Reperfusion
• Location of First Evaluation
• “Value out of range” for LDL
Limited and Premier Forms – V2.4
• 25% fewer date/time fields
• “Set to no” functionality in ACC
data collection tool
Limited and Premier Forms – V2.4
• Limited form – answering “no” to many
parent fields will ‘close’ child fields
– As few as 75 fields for Limited, 120 for Premier
• Referring hospitals can review their
performance on care measures provided
3/8/2014
24
Contact NCDR for questions at Contact NCDR for questions at Contact NCDR for questions at Contact NCDR for questions at
[email protected] or call [email protected] or call [email protected] or call [email protected] or call 800----257257257257----4737473747374737
Related Documents











