INSTITUTE OF PHYSICS PUBLISHING PHYSICS IN MEDICINE AND BIOLOGY Phys. Med. Biol. 49 (2004) 2053–2067 PII: S0031-9155(04)72062-X Acquiring 4D thoracic CT scans using a multislice helical method P J Keall 1 , G Starkschall 2 , H Shukla 3,5 , K M Forster 2 , V Ortiz 2 , C W Stevens 4 , S S Vedam 1 , R George 1 , T Guerrero 4 and R Mohan 2 1 Departments of Radiation Oncology and Biomedical Engineering, Virginia Commonwealth University, Richmond, Virginia, USA 2 Department of Radiation Physics, The University of Texas M D Anderson Cancer Center, Houston, Texas, USA 3 Philips Medical Systems, Cleveland, Ohio, USA 4 Department of Radiation Oncology, The University of Texas M D Anderson Cancer Center, Houston, Texas, USA E-mail: [email protected] Received 16 November 2003 Published 4 May 2004 Online at stacks.iop.org/PMB/49/2053 DOI: 10.1088/0031-9155/49/10/015 Abstract Respiratory motion degrades anatomic position reproducibility during imaging, necessitates larger margins during radiotherapy planning and causes errors during radiation delivery. Computed tomography (CT) scans acquired synchronously with the respiratory signal can be used to reconstruct 4D CT scans, which can be employed for 4D treatment planning to explicitly account for respiratory motion. The aim of this research was to develop, test and clinically implement a method to acquire 4D thoracic CT scans using a multislice helical method. A commercial position-monitoring system used for respiratory-gated radiotherapy was interfaced with a third generation multislice scanner. 4D cardiac reconstruction methods were modified to allow 4D thoracic CT acquisition. The technique was tested on a phantom under different conditions: stationary, periodic motion and non-periodic motion. 4D CT was also implemented for a lung cancer patient with audio-visual breathing coaching. For all cases, 4D CT images were successfully acquired from eight discrete breathing phases, however, some limitations of the system in terms of respiration reproducibility and breathing period relative to scanner settings were evident. Lung mass for the 4D CT patient scan was reproducible to within 2.1% over the eight phases, though the lung volume changed by 20% between end inspiration and end expiration (870 cm 3 ). 4D CT can be used for 4D radiotherapy, respiration-gated radiotherapy, ‘slow’ CT acquisition and tumour motion studies. 5 Present address: Siemens Oncology Care Systems, Concord, California, USA. 0031-9155/04/102053+15$30.00 © 2004 IOP Publishing Ltd Printed in the UK 2053

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

INSTITUTE OF PHYSICS PUBLISHING PHYSICS IN MEDICINE AND BIOLOGY
Phys. Med. Biol. 49 (2004) 2053–2067 PII: S0031-9155(04)72062-X
Acquiring 4D thoracic CT scans using a multislicehelical method
P J Keall1, G Starkschall2, H Shukla3,5, K M Forster2, V Ortiz2,C W Stevens4, S S Vedam1, R George1, T Guerrero4 and R Mohan2
1 Departments of Radiation Oncology and Biomedical Engineering, Virginia CommonwealthUniversity, Richmond, Virginia, USA2 Department of Radiation Physics, The University of Texas M D Anderson Cancer Center,Houston, Texas, USA3 Philips Medical Systems, Cleveland, Ohio, USA4 Department of Radiation Oncology, The University of Texas M D Anderson Cancer Center,Houston, Texas, USA
E-mail: [email protected]
Received 16 November 2003Published 4 May 2004Online at stacks.iop.org/PMB/49/2053DOI: 10.1088/0031-9155/49/10/015
AbstractRespiratory motion degrades anatomic position reproducibility during imaging,necessitates larger margins during radiotherapy planning and causes errorsduring radiation delivery. Computed tomography (CT) scans acquiredsynchronously with the respiratory signal can be used to reconstruct 4DCT scans, which can be employed for 4D treatment planning to explicitlyaccount for respiratory motion. The aim of this research was to develop,test and clinically implement a method to acquire 4D thoracic CT scansusing a multislice helical method. A commercial position-monitoring systemused for respiratory-gated radiotherapy was interfaced with a third generationmultislice scanner. 4D cardiac reconstruction methods were modified to allow4D thoracic CT acquisition. The technique was tested on a phantom underdifferent conditions: stationary, periodic motion and non-periodic motion. 4DCT was also implemented for a lung cancer patient with audio-visual breathingcoaching. For all cases, 4D CT images were successfully acquired from eightdiscrete breathing phases, however, some limitations of the system in termsof respiration reproducibility and breathing period relative to scanner settingswere evident. Lung mass for the 4D CT patient scan was reproducible to within2.1% over the eight phases, though the lung volume changed by 20% betweenend inspiration and end expiration (870 cm3). 4D CT can be used for 4Dradiotherapy, respiration-gated radiotherapy, ‘slow’ CT acquisition and tumourmotion studies.
5 Present address: Siemens Oncology Care Systems, Concord, California, USA.
0031-9155/04/102053+15$30.00 © 2004 IOP Publishing Ltd Printed in the UK 2053

2054 P J Keall et al
1. Introduction
Respiratory motion degrades anatomic position reproducibility during imaging (Shepp et al1979, Mayo et al 1987, Tarver et al 1988, Ritchie et al 1992, 1994, Balter et al 1996, Shimizuet al 2000, 2001, Keall et al 2002, Ford et al 2003, Vedam et al 2003a, Allen et al 2004),necessitates larger margins during radiotherapy planning (ICRU 1993, 1999) and causeserrors during radiation delivery (Yu et al 1998, Keall et al 2001, Bortfeld et al 2002, Chui et al2003, George et al 2003, Jiang et al 2003). Clinically significant lung tumour motioncannot be predicted by any known clinical parameters (Stevens et al 2001), suggestingthat tumour motion must be explicitly determined for each patient. Methods to accountfor respiratory motion during CT imaging include breath-hold, respiratory gating andfour-dimensional (4D) CT, the subject of the current research. 4D thoracic CT imagesaccounting for respiratory motion have successfully been acquired using single slice scanners(Ford et al 2003, Vedam et al 2003a), however, the authors of these works acknowledgethe temporal and spatial limitations of 4D acquisition with current single slice technology.Multislice 4D CT scans have been acquired using an axial/cine method at WashingtonUniversity (Low et al 2003), Memorial Sloan Kettering Cancer Center (Mageras 2002) andMassachusetts General Hospital (Rietzel et al 2003a, 2003b, Pan et al 2004). 4D cone-beam CT scans have been acquired using a benchtop system by Taguchi (2003) as wellas clinically at the Netherlands Cancer Institute (Sonke et al 2003). To date, there has beenno literature on the acquisition of 4D thoracic CT scans using a helical method on a multislicescanner.
The aim of this research was to develop, test and clinically implement a method to acquire4D thoracic CT scans using a multislice helical method.
2. Method
2.1. System design
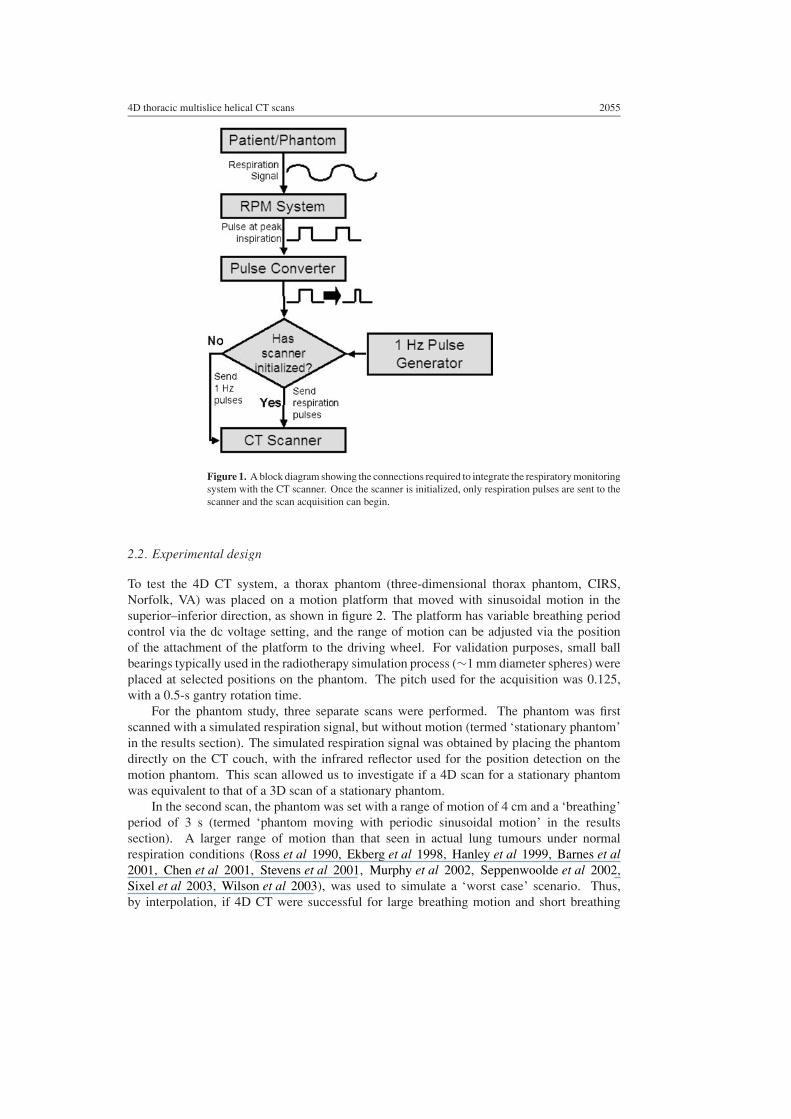
The scanner used for the CT data acquisition was a 16-slice helical CT scanner (MX8000IDT version 2.5 scanner, Philips Medical Systems, Cleveland, OH) with a standard physicalaperture 70 cm in diameter. The respiration signal was acquired by monitoring the motion ofan infrared reflecting marker box placed on the abdomen of the phantom or patient (real-timeposition management (RPM) version 1.5.1 system, Varian Medical Systems, Palo Alto, CA).The CT scanner currently supports 4D CT using a cardiac signal. A description of the cardiacimplementation on the same hardware is given by Grass et al (2003). However, to integrate theCT scanner with the respiration signal for thoracic 4D CT, two modifications were required.First, the cardiac input expected a pulse frequency of approximately 1 Hz to initiate the CTscanner. Since the respiratory period is typically 0.1–0.3 Hz, it was necessary to use a pulsegenerator to initialize the scanner, with a switch to use the respiratory pulses once the scannerwas initialized. Second, the output pulse from the RPM system has a 500-ms length, so it wasnecessary to design a pulse converter to obtain a 50-ms 5 V pulse, which was subsequentlysent to the CT scanner. A block diagram of the steps required to integrate the respiratorymonitoring system with the CT scanner in order to achieve 4D thoracic image acquisition isshown in figure 1. Note that both upgrades to the CT scanner and the RPM system since thesedata were acquired have obviated the need for both the pulse converter and the pulse generatorshown in figure 1.
4D thoracic multislice helical CT scans 2055
Figure 1. A block diagram showing the connections required to integrate the respiratory monitoringsystem with the CT scanner. Once the scanner is initialized, only respiration pulses are sent to thescanner and the scan acquisition can begin.
2.2. Experimental design
To test the 4D CT system, a thorax phantom (three-dimensional thorax phantom, CIRS,Norfolk, VA) was placed on a motion platform that moved with sinusoidal motion in thesuperior–inferior direction, as shown in figure 2. The platform has variable breathing periodcontrol via the dc voltage setting, and the range of motion can be adjusted via the positionof the attachment of the platform to the driving wheel. For validation purposes, small ballbearings typically used in the radiotherapy simulation process (∼1 mm diameter spheres) wereplaced at selected positions on the phantom. The pitch used for the acquisition was 0.125,with a 0.5-s gantry rotation time.
For the phantom study, three separate scans were performed. The phantom was firstscanned with a simulated respiration signal, but without motion (termed ‘stationary phantom’in the results section). The simulated respiration signal was obtained by placing the phantomdirectly on the CT couch, with the infrared reflector used for the position detection on themotion phantom. This scan allowed us to investigate if a 4D scan for a stationary phantomwas equivalent to that of a 3D scan of a stationary phantom.
In the second scan, the phantom was set with a range of motion of 4 cm and a ‘breathing’period of 3 s (termed ‘phantom moving with periodic sinusoidal motion’ in the resultssection). A larger range of motion than that seen in actual lung tumours under normalrespiration conditions (Ross et al 1990, Ekberg et al 1998, Hanley et al 1999, Barnes et al2001, Chen et al 2001, Stevens et al 2001, Murphy et al 2002, Seppenwoolde et al 2002,Sixel et al 2003, Wilson et al 2003), was used to simulate a ‘worst case’ scenario. Thus,by interpolation, if 4D CT were successful for large breathing motion and short breathing

2056 P J Keall et al
Figure 2. The experimental design showing the power supply that drives the electric motor, whichin turn moves the motion platform and phantom sinusoidally in the superior–inferior direction asit moves through the CT bore.
periods, this technique would be applicable to smaller motions and longer breathing periods,as observed clinically.
In the third experiment, the range of motion was 4 cm, however, the period was manuallychanged between 1.5 s and 6 s (40–10 breaths per minute) to represent variable respirationperiods (termed ‘phantom moving with non-periodic sinusoidal motion’ in the results section).
For 4D CT, it is important to ensure that each section of the anatomy is imaged throughoutthe entire breathing cycle, otherwise, the anatomy will not be present in each respiration phase,leaving apparent gaps or missing slices in the reconstructed volume. This means that to avoidundersampling of the object and missing data, for helical 4D CT acquisition the followingsettings are required:
Gantry rotation time
Pitch� Breathing period. (1)
For the motion phantom, the rotation time used was 0.5 s, and the pitch 0.125. With thesesettings ∼20 breathing cycles were completed throughout the entire scan (which completedin ∼60 s).
Phase tracking of the respiration signal was used, and the phase signal trigger was set at endinspiration. The end-inspiration value was chosen, as this point, is the most clearly defined inthe respiration cycle; inspiration is, in general, shorter than expiration. The pulse for the RPMsignal at end inspiration is received by the CT scanner as a ‘tag.’ These tags are synchronizedwith the sinogram acquisition. To reconstruct at the tags, corresponding in this case to endinspiration, only sinogram data recorded within ±180◦ gantry rotation (±0.25 s) of the tagsare used; the rest of the sinogram data is ignored. To reconstruct CT images at other pointsof the respiratory cycle the time between the tags is linearly interpolated, so, for example, toacquire the end expiration image set, the sinogram data acquired within ±180◦ gantry rotationof the mid-time point between each tag is used for the reconstruction. Note that using thesinogram-based 4D CT method means that the patient dose is not affected by the desirednumber of respiratory phases to be reconstructed. With this method, an arbitrary numberof phases can be reconstructed. However, with the finite temporal resolution, if too many

4D thoracic multislice helical CT scans 2057
phases are reconstructed then there will be overlap between the data used for reconstructionin successive phases.
2.3. Experimental analysis
The image sinograms, the respiration signals from the RPM system and the time tags at whichthe respiration pulses were sent to the CT scanner to indicate end inspiration were recorded.Following the method of Vedam (Vedam et al 2003a), the 4D CT scan was reconstructedinto eight discrete breathing phases: end inspiration, early expiration, mid expiration, lateexpiration, end expiration, early inspiration, mid inspiration and late inspiration. From thereconstructed data sets, the lung volumes and the positions of the external fiducial markers forthe phantom case were recorded.
Several recent publications have shown the benefit of ‘slow CT’ (Lagerwaard et al 2001,van Sornsen de Koste et al 2001, 2003, de Koste et al 2003). In the absence of methods toexplicitly account for respiratory motion (e.g., gating, breath hold or 4D techniques), slowCT is a useful technique for thoracic scanning, with the caveat that the benefits of includingthe entire range of tumour motion are somewhat negated by the subsequent reduction in thetumour/mediastinal boundary contrast when there is tumour extension into this area. However,using the above-described scanning parameters, reconstruction of slow CT is possible usingthe 4D CT data. The tags are simply ignored, and the entire sinogram is used for the imagereconstruction. For a 0.5-s rotation speed and a 0.125 pitch, each image is acquired over 4 s.This slow CT scan was used for comparison during the experimental analysis.
2.4. Patient case
The system described above was implemented clinically under MDACC protocol ID 00-202‘assessing three-dimensional tumour motion and treatment volume in radiotherapy of lungcancers using CT and MRI’. The patient was a 53-year old male with stage IIIB T4N2M0adenocarcinoma of the right lung.
For the patient implementation, the RPM system was adapted to allow audio-visualrespiratory coaching (Kini et al 2003). The audio ‘breathe in . . . breathe out’ instructiontiming was adapted for the patient’s comfort using in-house developed software (Kini et al2003, Vedam et al 2003b). The patient was trained until comfortable with the visual feedback.The training process takes several minutes. A picture of the visual coaching set-up is given infigure 3.
4D CT image data sets for the phantom cases and patient case were transferred toa commercial radiation treatment-planning system (Pinnacle3, Philips Medical Systems,Milpitas, CA) for analysis. Lung contours were obtained using a thresholding algorithmon the treatment-planning system. Threshold CT numbers were 0 for the lower threshold(corresponding with a density of 0.00 g cm−3), with an upper threshold of 800 (density of0.82 g cm−3).
3. Results
Described here are the results of the phantom and patient measurements. Typically, morethan 1000 CT slices are reconstructed for a 4D CT scan. The respiration traces for thephantom and patient experiments are given in figure 4. As expected, the periodic motionphantom has the most reproducible respiration trace. The non-periodic phantom case exhibitsreproducible peak-to-peak positions, but varies from period to period. The patient trace
2058 P J Keall et al
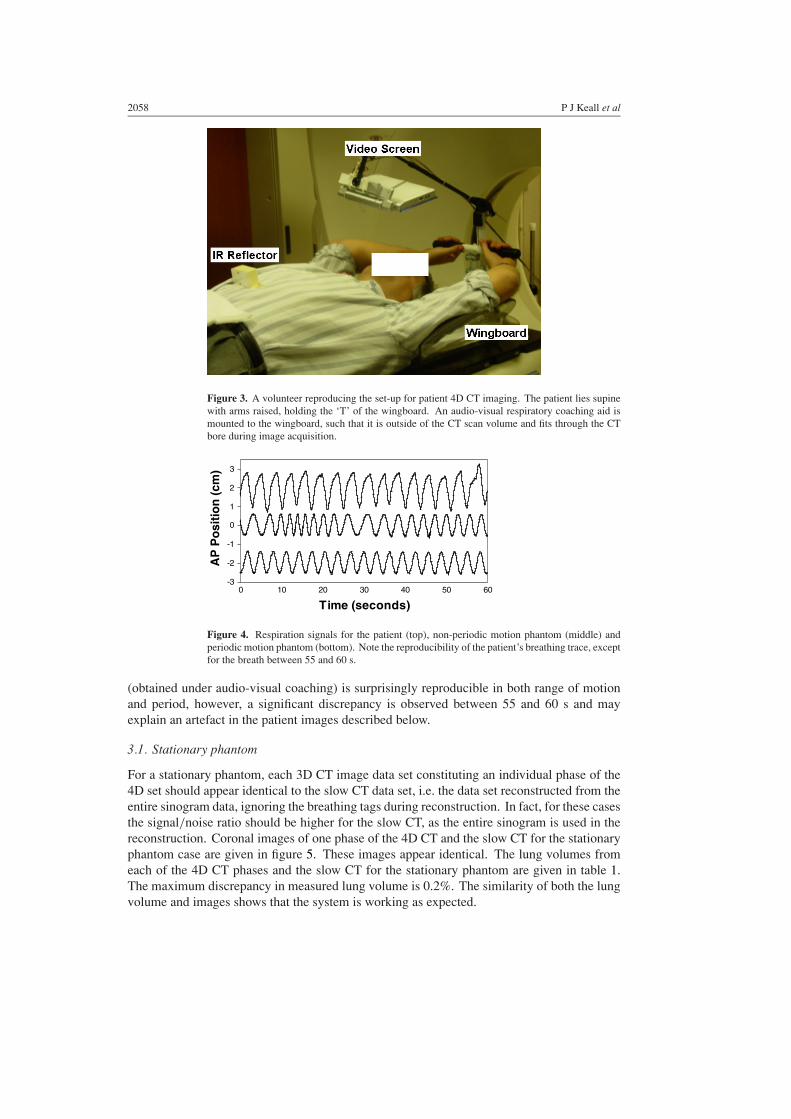
Figure 3. A volunteer reproducing the set-up for patient 4D CT imaging. The patient lies supinewith arms raised, holding the ‘T’ of the wingboard. An audio-visual respiratory coaching aid ismounted to the wingboard, such that it is outside of the CT scan volume and fits through the CTbore during image acquisition.
-3
-2
-1
0
1
2
3
0 10 20 30 40 50 60
Time (seconds)
AP
Po
siti
on
(cm
)
Figure 4. Respiration signals for the patient (top), non-periodic motion phantom (middle) andperiodic motion phantom (bottom). Note the reproducibility of the patient’s breathing trace, exceptfor the breath between 55 and 60 s.
(obtained under audio-visual coaching) is surprisingly reproducible in both range of motionand period, however, a significant discrepancy is observed between 55 and 60 s and mayexplain an artefact in the patient images described below.
3.1. Stationary phantom
For a stationary phantom, each 3D CT image data set constituting an individual phase of the4D set should appear identical to the slow CT data set, i.e. the data set reconstructed from theentire sinogram data, ignoring the breathing tags during reconstruction. In fact, for these casesthe signal/noise ratio should be higher for the slow CT, as the entire sinogram is used in thereconstruction. Coronal images of one phase of the 4D CT and the slow CT for the stationaryphantom case are given in figure 5. These images appear identical. The lung volumes fromeach of the 4D CT phases and the slow CT for the stationary phantom are given in table 1.The maximum discrepancy in measured lung volume is 0.2%. The similarity of both the lungvolume and images shows that the system is working as expected.

4D thoracic multislice helical CT scans 2059
(a) (b)
Figure 5. Coronal images of the (a) end-inspiration phase of the 4D CT and (b) the slow CT forthe stationary phantom. As expected, the images appear almost identical.
Table 1. Lung volume (cm3) for each of the eight 4D CT phases and ‘slow CT’ for the phantomstudies.
End Early Mid Late End Early Mid Late 4D SlowMotion exp. insp. insp. insp. insp. exp. exp. exp. mean 1 SD CT
Stationary 3202 3202 3196 3200 3200 3198 3194 3196 3199 3 3202Periodic 3212 3093 3098 3092 3199 3130 3058 3134 3127 54 2944sinusoidalmotionNon-periodic 3135 2992 3046 3116 1480a 3052 2952 3108 3057 68 2919sinusoidalmotion
CT: computed tomography; exp.: expiration; insp.: inspiration; SD: standard deviation.a Note that this value corresponds with a CT set where only half of the image was reconstructed and that this valuewas not included in the calculation of the mean.
3.2. Phantom moving with periodic sinusoidal motion
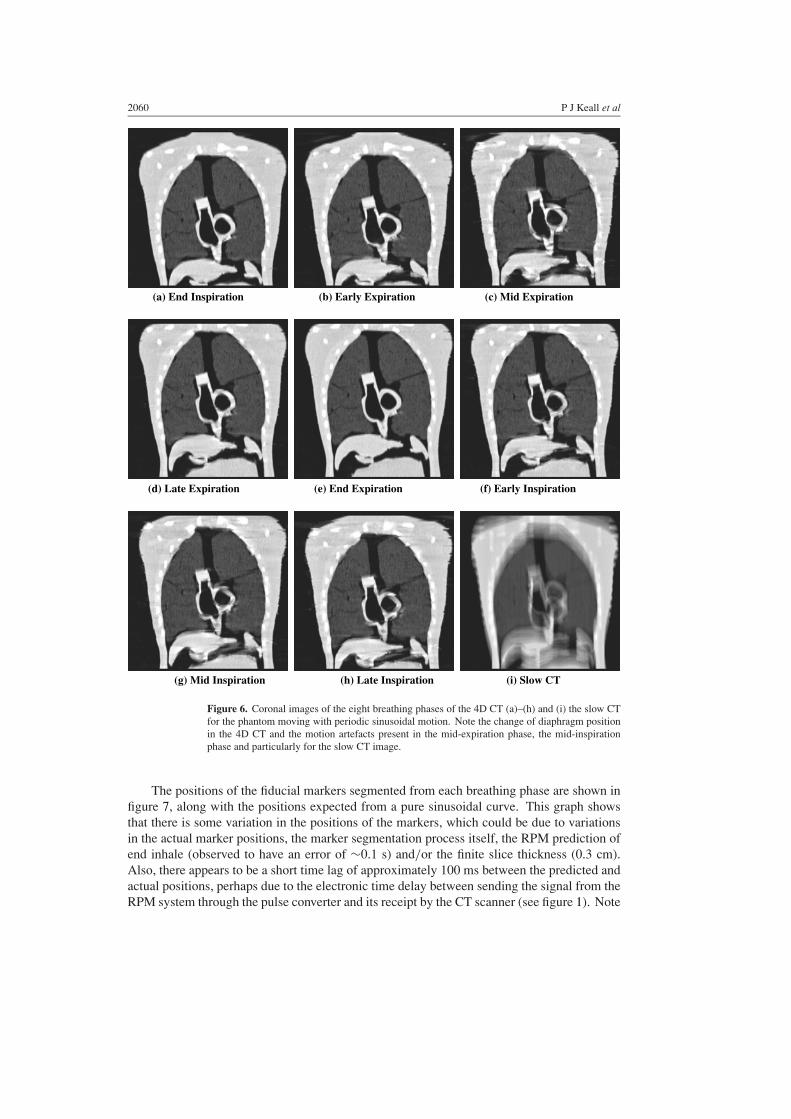
Coronal images of each phase of the 4D CT scan from the phantom moving with periodicsinusoidal motion are shown in figure 6. Also shown for comparison is the ‘slow’ 3D CT scan,reconstructed using the entire sinogram data, ignoring the respiratory tags. It is evident fromthese images that image quality is highest at end inspiration and end expiration (figures 6(a)and (e), respectively), where the motion of the phantom during image acquisition is minimal.However, there are apparent artefacts near the liver in mid-cycle (figures 6(c) and (g)), showingthat there is still a temporal resolution limitation when motion is maximal.
When the 4D CT images (figures 6(a) to (h)) are compared with the slow CT image(figure 6(i)), it is evident that even the worst-case mid-cycle 4D images are considerablyclearer than the slow CT images, where the motion significantly blurs even the sharpest highcontrast areas. The lung volumes for each of the phases are quantified in table 1. The lungvolumes are closest to the stationary volume at the end-respiratory phases and diminish as themotion during the scan acquisition is increased. However, all of the lung volumes from eachphase of the 4D CT are closer to the stationary CT lung volume than the slow CT value.
2060 P J Keall et al
(a) End Inspiration (b) Early Expiration (c) Mid Expiration
(d) Late Expiration (e) End Expiration (f) Early Inspiration
(g) Mid Inspiration (h) Late Inspiration (i) Slow CT
Figure 6. Coronal images of the eight breathing phases of the 4D CT (a)–(h) and (i) the slow CTfor the phantom moving with periodic sinusoidal motion. Note the change of diaphragm positionin the 4D CT and the motion artefacts present in the mid-expiration phase, the mid-inspirationphase and particularly for the slow CT image.
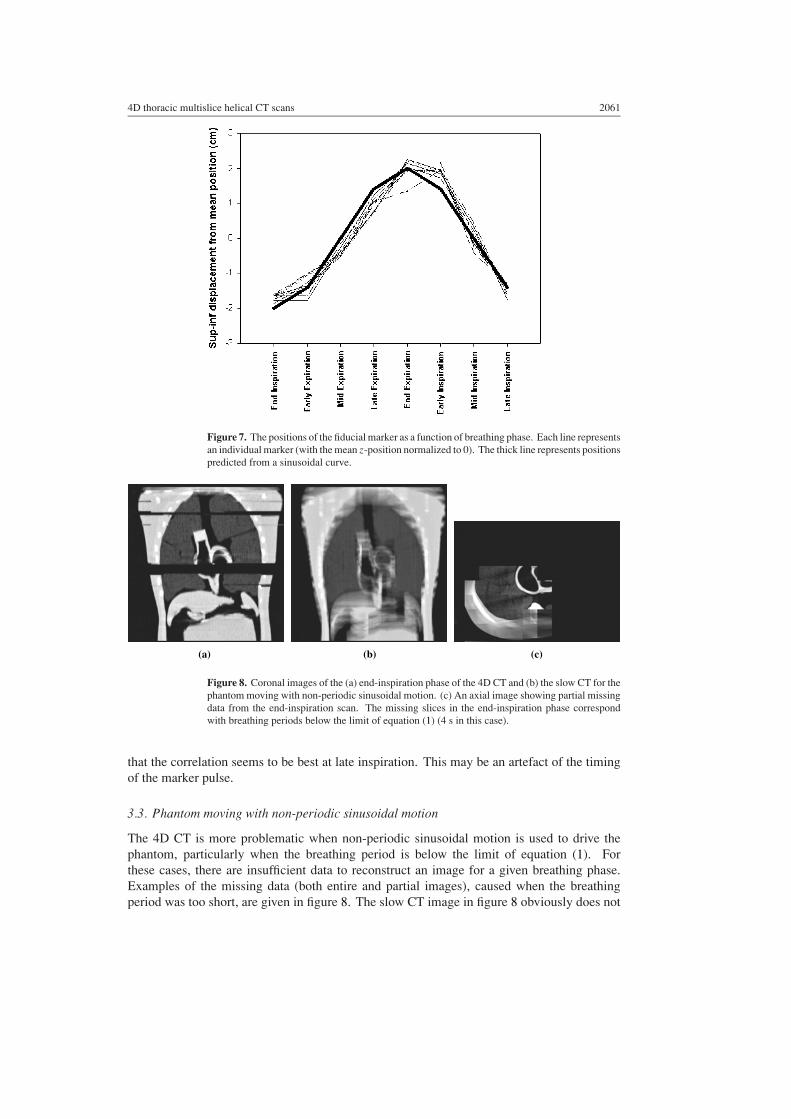
The positions of the fiducial markers segmented from each breathing phase are shown infigure 7, along with the positions expected from a pure sinusoidal curve. This graph showsthat there is some variation in the positions of the markers, which could be due to variationsin the actual marker positions, the marker segmentation process itself, the RPM prediction ofend inhale (observed to have an error of ∼0.1 s) and/or the finite slice thickness (0.3 cm).Also, there appears to be a short time lag of approximately 100 ms between the predicted andactual positions, perhaps due to the electronic time delay between sending the signal from theRPM system through the pulse converter and its receipt by the CT scanner (see figure 1). Note
4D thoracic multislice helical CT scans 2061
Figure 7. The positions of the fiducial marker as a function of breathing phase. Each line representsan individual marker (with the mean z-position normalized to 0). The thick line represents positionspredicted from a sinusoidal curve.
(a) (b) (c)
Figure 8. Coronal images of the (a) end-inspiration phase of the 4D CT and (b) the slow CT for thephantom moving with non-periodic sinusoidal motion. (c) An axial image showing partial missingdata from the end-inspiration scan. The missing slices in the end-inspiration phase correspondwith breathing periods below the limit of equation (1) (4 s in this case).
that the correlation seems to be best at late inspiration. This may be an artefact of the timingof the marker pulse.
3.3. Phantom moving with non-periodic sinusoidal motion
The 4D CT is more problematic when non-periodic sinusoidal motion is used to drive thephantom, particularly when the breathing period is below the limit of equation (1). Forthese cases, there are insufficient data to reconstruct an image for a given breathing phase.Examples of the missing data (both entire and partial images), caused when the breathingperiod was too short, are given in figure 8. The slow CT image in figure 8 obviously does not

2062 P J Keall et al
exhibit the missing data artefacts, however, as with figure 6(i), substantial loss of contrast andblurring are evident. In cases where the breathing period is within the limit of equation (1),non-periodic breathing will still affect the reconstruction in that essentially the same shapefor each respiratory cycle is assumed with the current approach of interpolating between tags,with each tag sent once per breathing cycle.
The lung volumes for each of the phases are quantified in table 1. To obtain the lungvolumes, the lung contours were interpolated between the missing slices (see figure 8). Asignificant discrepancy in lung volume is shown for the end-inspiration breathing phase intable 1. This discrepancy occurred, because, for this phase, only half of the image could bereconstructed. Apart from this outlier, the lung volumes for all of the other phases were closerto the stationary value than that of the slow CT. The absolute and relative volumes shown herewill be affected by the choice of autocontouring threshold. The value used here (correspondingto a density of 0.82 g cm−3) was chosen as it is the value used clinically at MDACC.
3.4. Patient case
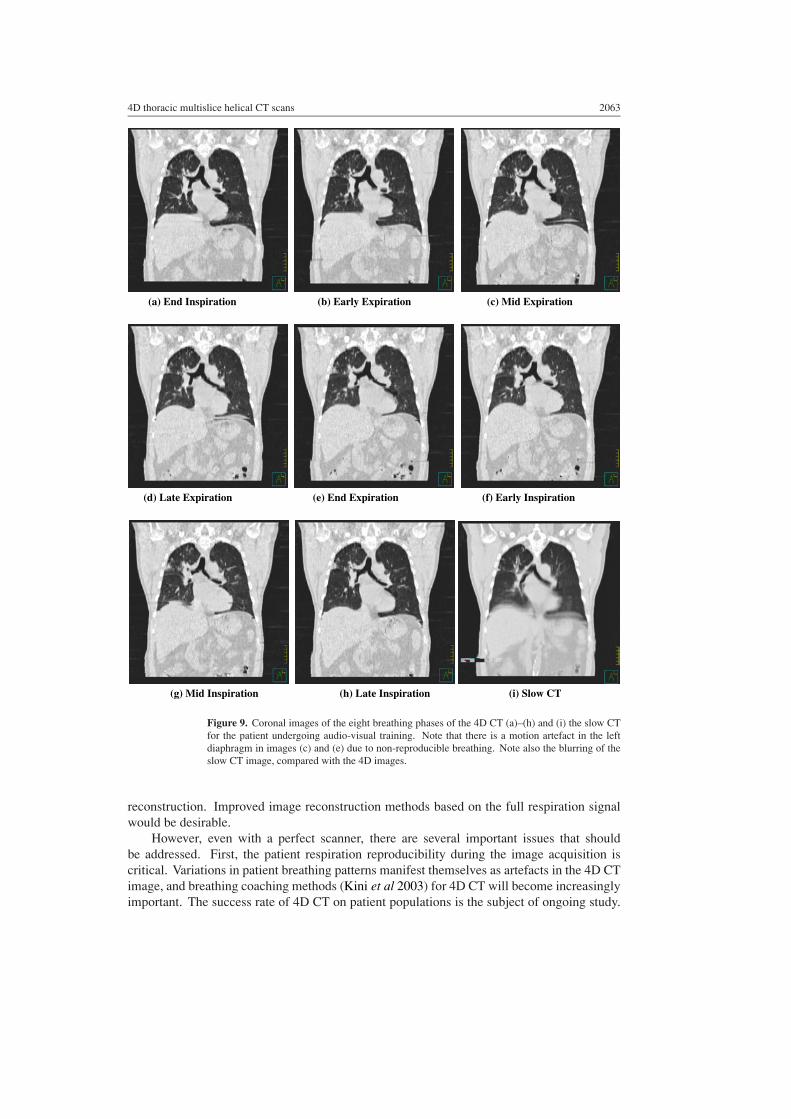
The 4D CT acquisition technique was applied to a patient case. Coronal reconstructed imagesof each phase and the slow CT are given in figure 9. The contrast of each phase of the 4D CTis high, however, a motion artefact in the left diaphragm is apparent in figures 9(c) and (d).This artefact was caused by the variability of the patient’s respiratory pattern, even though hehad received audio-visual breathing coaching, as seen in figure 4 (note the variable respiratorycycle between 55 and 60 s).
Blurring is again evident on the slow CT image; however, the image is clearer where thereis little motion, e.g., the humeral head area, as compared with areas of significant motion,such as both diaphragms. It can be observed that contrast for slow CT becomes progressivelyworse from the superior to the inferior part of the lung.
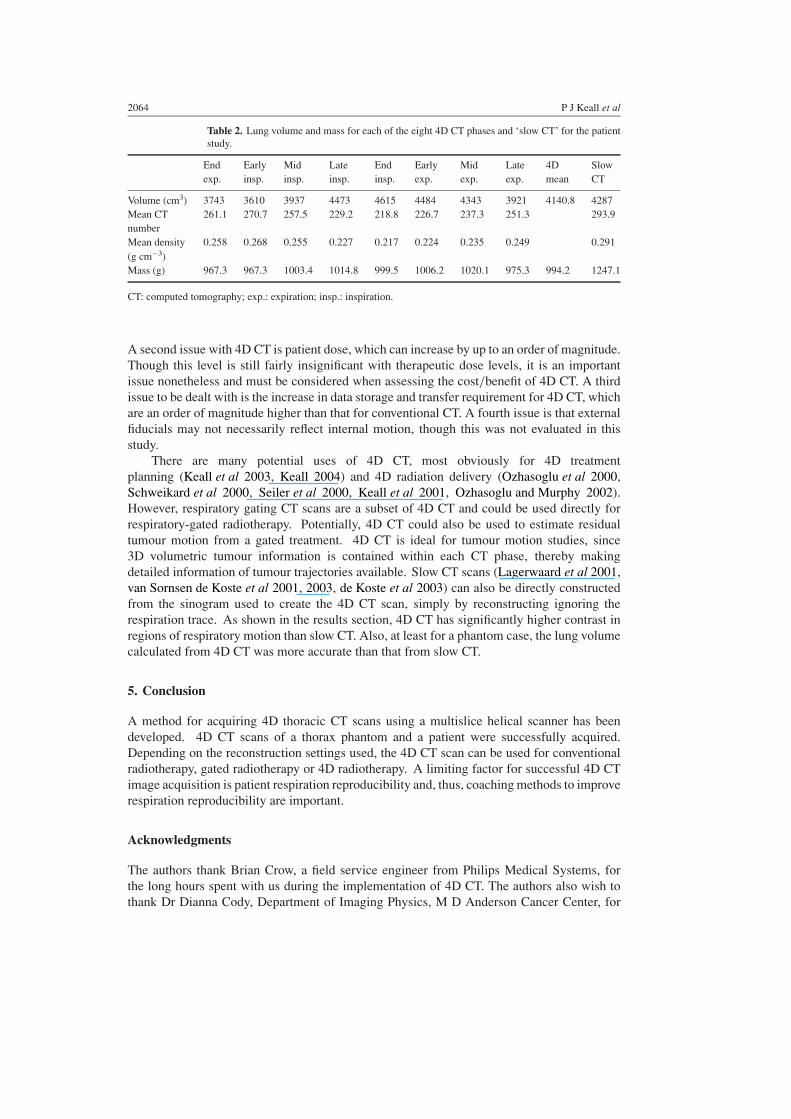
Total lung volumes and lung masses for each of the eight 4D CT phases are listed intable 2, where they are compared with the volume and mass obtained from the slow CT dataset. For the eight phases, the mean lung mass is 994.2 g with a standard deviation of only2.1%, indicating good consistency among the eight data sets. The lung volume changed by20% between end inspiration and end expiration (870 cm−3).
4. Discussion
A method for acquiring 4D thoracic CT scans using a multislice helical technique has beendeveloped and tested on a thorax phantom and a patient. The system worked well fora sinusoidally moving phantom and a patient undergoing audio-visual breathing coachingduring scan acquisition; however, for non-periodic sinusoidal motion, missing phantom datacaused gaps in both individual slices and the volumetric reconstruction. This is particularlymarked if the displacement is large.
As with all new methods, there are many opportunities for improvement. Reducing thepitch, slowing the gantry rotation or increasing the number of detector rows can resolve themissing data issue. Reducing the pitch or slowing the gantry rotation speed increases scanacquisition time, which is currently of the order of a minute, placing increasing onus on thepatient to maintain a regular breathing pattern. Slowing the gantry rotation also has a negativeimpact on the temporal resolution of the image. Increasing the number of detector rows(currently 16) allows the image to be acquired more quickly and addresses the missing dataissue. A further limitation of the current method is that it linearly interprets the breathing phasebased on the tags and does not continually input this data into the sinogram acquisition for
4D thoracic multislice helical CT scans 2063
(a) End Inspiration (b) Early Expiration (c) Mid Expiration
(d) Late Expiration (e) End Expiration (f) Early Inspiration
(g) Mid Inspiration (h) Late Inspiration (i) Slow CT
Figure 9. Coronal images of the eight breathing phases of the 4D CT (a)–(h) and (i) the slow CTfor the patient undergoing audio-visual training. Note that there is a motion artefact in the leftdiaphragm in images (c) and (e) due to non-reproducible breathing. Note also the blurring of theslow CT image, compared with the 4D images.
reconstruction. Improved image reconstruction methods based on the full respiration signalwould be desirable.
However, even with a perfect scanner, there are several important issues that shouldbe addressed. First, the patient respiration reproducibility during the image acquisition iscritical. Variations in patient breathing patterns manifest themselves as artefacts in the 4D CTimage, and breathing coaching methods (Kini et al 2003) for 4D CT will become increasinglyimportant. The success rate of 4D CT on patient populations is the subject of ongoing study.
2064 P J Keall et al
Table 2. Lung volume and mass for each of the eight 4D CT phases and ‘slow CT’ for the patientstudy.
End Early Mid Late End Early Mid Late 4D Slowexp. insp. insp. insp. insp. exp. exp. exp. mean CT
Volume (cm3) 3743 3610 3937 4473 4615 4484 4343 3921 4140.8 4287Mean CT 261.1 270.7 257.5 229.2 218.8 226.7 237.3 251.3 293.9numberMean density 0.258 0.268 0.255 0.227 0.217 0.224 0.235 0.249 0.291(g cm−3)Mass (g) 967.3 967.3 1003.4 1014.8 999.5 1006.2 1020.1 975.3 994.2 1247.1
CT: computed tomography; exp.: expiration; insp.: inspiration.
A second issue with 4D CT is patient dose, which can increase by up to an order of magnitude.Though this level is still fairly insignificant with therapeutic dose levels, it is an importantissue nonetheless and must be considered when assessing the cost/benefit of 4D CT. A thirdissue to be dealt with is the increase in data storage and transfer requirement for 4D CT, whichare an order of magnitude higher than that for conventional CT. A fourth issue is that externalfiducials may not necessarily reflect internal motion, though this was not evaluated in thisstudy.
There are many potential uses of 4D CT, most obviously for 4D treatmentplanning (Keall et al 2003, Keall 2004) and 4D radiation delivery (Ozhasoglu et al 2000,Schweikard et al 2000, Seiler et al 2000, Keall et al 2001, Ozhasoglu and Murphy 2002).However, respiratory gating CT scans are a subset of 4D CT and could be used directly forrespiratory-gated radiotherapy. Potentially, 4D CT could also be used to estimate residualtumour motion from a gated treatment. 4D CT is ideal for tumour motion studies, since3D volumetric tumour information is contained within each CT phase, thereby makingdetailed information of tumour trajectories available. Slow CT scans (Lagerwaard et al 2001,van Sornsen de Koste et al 2001, 2003, de Koste et al 2003) can also be directly constructedfrom the sinogram used to create the 4D CT scan, simply by reconstructing ignoring therespiration trace. As shown in the results section, 4D CT has significantly higher contrast inregions of respiratory motion than slow CT. Also, at least for a phantom case, the lung volumecalculated from 4D CT was more accurate than that from slow CT.
5. Conclusion
A method for acquiring 4D thoracic CT scans using a multislice helical scanner has beendeveloped. 4D CT scans of a thorax phantom and a patient were successfully acquired.Depending on the reconstruction settings used, the 4D CT scan can be used for conventionalradiotherapy, gated radiotherapy or 4D radiotherapy. A limiting factor for successful 4D CTimage acquisition is patient respiration reproducibility and, thus, coaching methods to improverespiration reproducibility are important.
Acknowledgments
The authors thank Brian Crow, a field service engineer from Philips Medical Systems, forthe long hours spent with us during the implementation of 4D CT. The authors also wish tothank Dr Dianna Cody, Department of Imaging Physics, M D Anderson Cancer Center, for

4D thoracic multislice helical CT scans 2065
use of the thoracic phantom. The therapy simulation, physics and physician lung service staffat the M D Anderson Cancer Center are thanked for their patience and scheduling changesduring the experimental phase of the project. Thank you to Devon Murphy for improvingthe clarity of the manuscript. Paul Keall acknowledges the support of NIH/NCI R01 grant#93626, 4D IMRT: Imaging, Planning and Delivery, and the financial support of the John HBlaffer visiting professorship programme at the M D Anderson Cancer Center.
References
Allen A M, Siracuse K M, Hayman J A and Balter J M 2004 Evaluation of the influence of breathing on the movementand modeling of lung tumors Int. J. Radiat. Oncol. Biol. Phys. 58 1251–7
Balter J M, Ten Haken R K, Lawrence T S, Lam K L and Robertson J M 1996 Uncertainties in CT-based radiationtherapy treatment planning associated with patient breathing Int. J. Radiat. Oncol. Biol. Phys. 36 167–74
Barnes E A, Murray B R, Robinson D M, Underwood L J, Hanson J and Roa W H 2001 Dosimetric evaluation oflung tumor immobilization using breath hold at deep inspiration Int. J. Radiat. Oncol. Biol. Phys. 50 1091–8
Bortfeld T, Jokivarsi K, Goitein M, Kung J and Jiang S B 2002 Effects of intra-fraction motion on IMRT dose delivery:statistical analysis and simulation Phys. Med. Biol. 47 2203–20
Chen Q S, Weinhous M S, Deibel F C, Ciezki J P and Macklis R M 2001 Fluoroscopic study of tumor motion due tobreathing: facilitating precise radiation therapy for lung cancer patients Med. Phys. 28 1850–6
Chui C S, Yorke E and Hong L 2003 The effects of intra-fraction organ motion on the delivery of intensity-modulatedfield with a multileaf collimator Med. Phys. 30 1736–46
de Koste J R, Lagerwaard F J, de Boer H C, Nijssen-Visser M R and Senan S 2003 Are multiple CT scans required forplanning curative radiotherapy in lung tumors of the lower lobe? Int. J. Radiat. Oncol. Biol. Phys. 55 1394–9
Ekberg L, Holmberg O, Wittgren L, Bjelkengren G and Landberg T 1998 What margins should be added to theclinical target volume in radiotherapy treatment planning for lung cancer? Radiother. Oncol. 48 71–7
Ford E C, Mageras G S, Yorke E and Ling C C 2003 Respiration-correlated spiral CT: a method of measuringrespiratory-induced anatomic motion for radiation treatment planning Med. Phys. 30 88–97
George R, Keall P J, Kini V R, Vedam S S, Siebers J V, Wu Q, Lauterbach M H, Arthur D W and Mohan R2003 Quantifying the effect of intrafraction motion during breast IMRT planning and dose delivery Med. Phys.30 552–62
Grass M, Manzke R, Nielsen T, Koken P, Proksa R, Natanzon M and Schecter G 2003 Helical cardiac cone beamreconstruction using retrospective ECG gating Phys. Med. Biol. 48 3069–84
Hanley J, Debois M M, Mah D, Mageras G S, Raben A, Rosenzweig K, Mychalczak B, Schwartz L H, Gloeggler P J,Lutz W, Ling C C, Leibel S A, Fuks Z and Kutcher G J 1999 Deep inspiration breath-hold technique for lungtumors: the potential value of target immobilization and reduced lung density in dose escalation Int. J. Radiat.Oncol. Biol. Phys. 45 603–11
ICRU 1993 Prescribing, Recording and Reporting Photon Beam Therapy ICRU Report No 50 (Bethesda, MD:International Commission on Radiation Units and Measurements)
ICRU 1999 Prescribing, Recording and Reporting Photon Beam Therapy (Supplement to ICRU Report 50) ICRUReport No 62 (Bethesda, MD: International Commission on Radiation Units and Measurements)
Jiang S B, Pope C, Al Jarrah K M, Kung J H, Bortfeld T and Chen G T 2003 An experimental investigation onintra-fractional organ motion effects in lung IMRT treatments Phys. Med. Biol. 48 1773–84
Keall P 2004 Four-dimensional computed tomography imaging and treatment planning Semin. Radiat. Oncol.14 81–90
Keall P J, Joshi S, Tracton G, Kini V, Vedam S and Mohan R 2003 Four-Dimensional radiotherapy planning Int. J.Radiat. Oncol. Biol. Phys. 57 S233
Keall P J, Kini V, Vedam S S and Mohan R 2001 Motion adaptive x-ray therapy: a feasibility study Phys. Med. Biol.46 1–10
Keall P J, Kini V R, Vedam S S and Mohan R 2002 Potential radiotherapy improvements with respiratory gatingAustralas. Phys. Eng. Sci. Med. 25 1–6
Kini V R, Vedam S S, Keall P J, Patil S, Chen C and Mohan R 2003 Patient training in respiratory-gated radiotherapyMed. Dosim. 28 7–11
Lagerwaard F J, Van Sornsen de Koste J R, Nijssen-Visser M R, Schuchhard-Schipper R H, Oei S S, Munne A andSenan S 2001 Multiple ‘slow’ CT scans for incorporating lung tumor mobility in radiotherapy planning Int. J.Radiat. Oncol. Biol. Phys. 51 932–7
2066 P J Keall et al
Low D A, Nystrom M, Kalinin E, Parikh P, Dempsey J F, Bradley J D, Mutic S, Wahab S H, Islam T, Christensen G,Politte D G and Whiting B R 2003 A method for the reconstruction of four-dimensional synchronized CT scansacquired during free breathing Med. Phys. 30 1254–63
Mageras G S 2002 Respiration correlated CT techniques for gated treatment of lung cancer Radiother. Oncol. 64 75Mayo J R, Muller N L and Henkelman R M 1987 The double-fissure sign: a motion artifact on thin-section CT scans
Radiology 165 580–1Murphy M J, Martin D, Whyte R, Hai J, Ozhasoglu C and Le Q T 2002 The effectiveness of breath-holding to stabilize
lung and pancreas tumors during radiosurgery Int. J. Radiat. Oncol. Biol. Phys. 53 475–82Ozhasoglu C and Murphy M J 2002 Issues in respiratory motion compensation during external-beam radiotherapy
Int. J. Radiat. Oncol. Biol. Phys. 52 1389–99Ozhasoglu C, Murphy M J, Glosser G, Bodduluri M, Schweikard A, Forster K, Martin D P and Adler J R 2000
Real-time tracking of the tumor volume in precision radiotherapy and body radiosurgery—a novel approach tocompensate for respiratory motion Computer Assisted Radiology and Surgery (San Francisco) pp 691–6
Pan T, Lee T Y, Rietzel E and Chen G T 2004 4D-CT imaging of a volume influenced by respiratory motion onmulti-slice CT Med. Phys. 31 333–40
Rietzel E, Chen G T, Doppke K P, Pan T, Choi N C and Willett C G 2003a 4D computed tomography for treatmentplanning Int. J. Radiat. Oncol. Biol. Phys. 57 S232–3
Rietzel E, Doppke K, Pan T, Choi N, Willett C and Chen G 2003b 4D computer tomography for radiation therapy(abstract) Med. Phys. 30 1365–6
Ritchie C J, Godwin J D, Crawford C R, Stanford W, Anno H and Kim Y 1992 Minimum scan speeds for suppressionof motion artifacts in CT Radiology 185 37–42
Ritchie C J, Hseih J, Gard M F, Godwin J D, Kim Y and Crawford C R 1994 Predictive respiratory gating: a newmethod to reduce motion artifacts on CT scans Radiology 190 847–52
Ross C S, Hussey D H, Pennington E C, Stanford W and Doornbos J F 1990 Analysis of movement of intrathoracicneoplasms using ultrafast computerized tomography Int. J. Radiat. Oncol. Biol. Phys. 18 671–7
Schweikard A, Glosser G, Bodduluri M, Murphy M J and Adler J R 2000 Robotic motion compensation for respiratorymovement during radiosurgery Comput. Aided Surg. 5 263–77
Seiler P G, Blattmann H, Kirsch S, Muench R K and Schilling C 2000 A novel tracking technique for the continuousprecise measurement of tumour positions in conformal radiotherapy Phys. Med. Biol. 45 N103–10
Seppenwoolde Y, Shirato H, Kitamura K, Shimizu S, van Herk M, Lebesque J V and Miyasaka K 2002 Precise andreal-time measurement of 3D tumor motion in lung due to breathing and heartbeat, measured during radiotherapyInt. J. Radiat. Oncol. Biol. Phys. 53 822–34
Shepp L A, Hilal S K and Schulz R A 1979 The tuning fork artifact in computerized tomography Comput. GraphImage Process. 10 246–55
Shimizu S, Shirato H, Kagei K, Nishioka T, Bo X, Dosaka-Akita H, Hashimoto S, Aoyama H, Tsuchiya K andMiyasaka K 2000 Impact of respiratory movement on the computed tomographic images of small lung tumorsin three-dimensional (3D) radiotherapy Int. J. Radiat. Oncol. Biol. Phys. 46 1127–33
Shimizu S, Shirato H, Ogura S, Akita-Dosaka H, Kitamura K, Nishioka T, Kagei K, Nishimura M and Miyasaka K2001 Detection of lung tumor movement in real-time tumor-tracking radiotherapy Int. J. Radiat. Oncol. Biol.Phys. 51 304–10
Sixel K E, Ruschin M, Tirona R and Cheung P C 2003 Digital fluoroscopy to quantify lung tumor motion: potentialfor patient-specific planning target volumes Int. J. Radiat. Oncol. Biol. Phys. 57 717–23
Sonke J, Remeijer P and van Herk M 2003 Respiration-correlated cone beam CT: obtaining a four-dimensional dataset (abstract) Med. Phys. 30 1415
Stevens C W, Munden R F, Forster K M, Kelly J F, Liao Z, Starkschall G, Tucker S and Komaki R 2001 Respiratory-driven lung tumor motion is independent of tumor size, tumor location, and pulmonary function Int. J. Radiat.Oncol. Biol. Phys. 51 62–8
Taguchi K 2003 Temporal resolution and the evaluation of candidate algorithms for four-dimensional CT Med. Phys.30 640–50
Tarver R D, Conces D J and Godwin J D 1988 Motion artifacts on CT simulate bronchiectasis Am. J. Roentgenol.151 1117–9
van Sornsen de Koste J R, Lagerwaard F J, Nijssen-Visser M R, Graveland W J and Senan S 2003 Tumor locationcannot predict the mobility of lung tumors: a 3D analysis of data generated from multiple CT scans Int. J.Radiat. Oncol. Biol. Phys. 56 348–54
van Sornsen de Koste J R, Lagerwaard F J, Schuchhard-Schipper R H, Nijssen-Visser M R, Voet P W, Oei S Sand Senan S 2001 Dosimetric consequences of tumor mobility in radiotherapy of stage I non-small cell lungcancer—an analysis of data generated using ‘slow’ CT scans Radiother. Oncol. 61 93–9

4D thoracic multislice helical CT scans 2067
Vedam S S, Keall P J, Kini V R, Mostafavi H, Shukla H P and Mohan R 2003a Acquiring a four-dimensional computedtomography dataset using an external respiratory signal Phys. Med. Biol. 48 45–62
Vedam S S, Kini V R, Keall P J, Ramakrishnan V, Mostafavi H and Mohan R 2003b Quantifying the predictabilityof diaphragm motion during respiration with a noninvasive external marker Med. Phys. 30 505–13
Wilson E M, Williams F J, Lyn B E, Wong J W and Aird E G 2003 Validation of active breathing control in patientswith non-small-cell lung cancer to be treated with CHARTWEL Int. J. Radiat. Oncol. Biol. Phys. 57 864–74
Yu C X, Jaffray D A and Wong J W 1998 The effects of intra-fraction organ motion on the delivery of dynamicintensity modulation Phys. Med. Biol. 43 91–104
Related Documents











