1 Acquired Disease of the Aortic Valve Normal aortic valve anatomy ในหัวใจของคนปกติทั่วไปจะมีชุดของลิ้นหัวใจ (cardiac valve) รวม 2 ชุด ชุดแรกได้แก่ atrioventricular valves (AV valves) อันประกอบไปด้วย tricuspid valve และ mitral valve ส่วนชุด ที่สองได้แก่ semilunar valves ซึ่งประกอบไปด้วย pulmonic valve และ aortic valve Aortic valve ถือเป็นลิ้นหัวใจด่านสุดท้ายก่อนที่จะให้เลือดออกไปสู่ร่างกาย หน้าที่สาคัญ ของ aortic valve ก็คือการป้องกันการเกิดเลือดไหลย้อน (backflow) จาก aorta มายัง left ventricle สาหรับ aortic valve จะประกอบไปด้วย 3 leaflets คือ left coronary, right coronary และ noncoronary leaflets โดย leaflet แต่ละอันก็จะยึดติดกับแต่ละด้านของ sinus of Valsava นอกจากนี้ aortic valve leaflets จะมี fibrous skeleton ซึ่งมีลักษณะเป็น U-shape คอยพยุงแต่ละ leaflet ของ aortic valve โดยพบว่ามีส่วนที่ต่อเนื่องไปถึง anterior leaflet ของ mitral valve อีกด้วย บริเวณใต้ต่อ noncoronary leaflet (cusp) จะมี atrioventricular conduction system ฝังตัวอยู่ ซึ่งขณะทาการผ่าตัดจะต้องระมัดระวังเป็นอย่างยิ่ง โดยเฉพาะการผ่าตัดเปลี่ยนลิ้นหัวใจ (aortic valve replacement : AVR) สาหรับส่วนของ valve leaflets พบว่ามีโครงสร้างเป็น fibrous tissue และคลุมด้วย endothelium อีกชั้น โดยไม่พบว่ามี specific vascular supply ส่วน free edge ของทั้ง 3 leaflets จะพบมีลักษณะเนื้อที่นูนขึ้นมาบริเวณกึ่งกลาง เรียกว่า nodule of Arantius ในช่วง systole พบว่า leaflets ทั้ง 3 จะถูกดันออกข้างๆ และด้วยลักษณะเฉพาะของ sinus of Valsava จะเป็นกลไกสาคัญที่ป้องกันไม่ให้ leaflets ถูกดันไปแนบกับด้านข้าง (sidewall) ของ aorta ซึ่งจะเป็นการป้องกันการเกิด coronary ostia occlusion สาหรับในช่วง diastole นั้น พบว่า free edge ของ aortic valve ทั้ง 3 leaflets ก็จะเคลื่อนเข้ามาชนกันตรงกลาง โดยมีส่วนที่เป็น coaptation surface ประมาณ 1-2 mm. เท่านั้น Aortic stenosis Causes สาเหตุของการเกิด aortic stenosis ที่พบได้บ่อยในประเทศไทย ได้แก่ 1. Rheumatic aortic stenosis (Figure 1) 2. Bicuspid aortic stenosis (Figure 2) 3. Degenerative calcific aortic stensois

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Acquired Disease of the Aortic Valve Normal aortic valve anatomy ในหัวใจของคนปกติทั่วไปจะมีชุดของลิ้นหัวใจ (cardiac valve) รวม 2 ชุด ชุดแรกได้แก่ atrioventricular valves (AV valves) อันประกอบไปด้วย tricuspid valve และ mitral valve ส่วนชุดที่สองได้แก่ semilunar valves ซึ่งประกอบไปด้วย pulmonic valve และ aortic valve Aortic valve ถือเป็นลิ้นหัวใจด่านสุดท้ายก่อนที่จะให้เลือดออกไปสู่ร่างกาย หน้าที่ส าคัญของ aortic valve ก็คือการป้องกันการเกิดเลือดไหลย้อน (backflow) จาก aorta มายัง left ventricle ส าหรับ aortic valve จะประกอบไปด้วย 3 leaflets คือ left coronary, right coronary และ noncoronary leaflets โดย leaflet แต่ละอันก็จะยึดติดกับแต่ละด้านของ sinus of Valsava นอกจากนี้ aortic valve leaflets จะมี fibrous skeleton ซึ่งมีลักษณะเป็น U-shape คอยพยุงแต่ละ leaflet ของ aortic valve โดยพบว่ามีส่วนที่ต่อเน่ืองไปถึง anterior leaflet ของ mitral valve อีกด้วย บริเวณใต้ต่อ noncoronary leaflet (cusp) จะมี atrioventricular conduction system ฝังตัวอยู่ ซึ่งขณะท าการผ่าตัดจะต้องระมัดระวังเป็นอย่างยิ่ง โดยเฉพาะการผ่าตัดเปลี่ยนลิ้นหัวใจ (aortic valve replacement : AVR) ส าหรับส่วนของ valve leaflets พบว่ามีโครงสร้างเป็น fibrous tissue และคลุมด้วย endothelium อีกชั้น โดยไม่พบว่ามี specific vascular supply ส่วน free edge ของทั้ง 3 leaflets จะพบมีลักษณะเนื้อที่นูนขึ้นมาบริเวณกึ่งกลาง เรียกว่า nodule of Arantius ในช่วง systole พบว่า leaflets ทั้ง 3 จะถกูดันออกข้างๆ และด้วยลักษณะเฉพาะของ sinus of Valsava จะเป็นกลไกส าคัญที่ป้องกันไม่ให้ leaflets ถูกดันไปแนบกับด้านข้าง (sidewall) ของ aorta ซึ่งจะเป็นการป้องกันการเกิด coronary ostia occlusion ส าหรับในช่วง diastole นั้น พบว่า free edge ของ aortic valve ทั้ง 3 leaflets ก็จะเคลื่อนเข้ามาชนกันตรงกลาง โดยมีส่วนที่เป็น coaptation surface ประมาณ 1-2 mm. เท่านั้น Aortic stenosis Causes
สาเหตุของการเกิด aortic stenosis ที่พบได้บ่อยในประเทศไทย ได้แก่ 1. Rheumatic aortic stenosis (Figure 1) 2. Bicuspid aortic stenosis (Figure 2) 3. Degenerative calcific aortic stensois

2
Figure 1 Calcific aortic stenosis
(From Michael KB : Acquired aortic valve disease. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)
ส าหรับในประเทศที่เจริญแล้ว (industrialized nations) ก็จะพบสาเหตุของ aortic stenosis ที่เกิดจาก rheumatic causes ค่อนข้างน้อย โดยพบว่าลิ้นหัวใจที่มีสาเหตุจากไข้รูมาติกนี้จะเร่ิมต้นจากการที่มี valvulitis ก่อน จากนั้นจะมี edema, lymphocytic infiltration และ neovascularization of the leaflets หลังจากนั้นลิ้นหัวใจก็จะหนาตัว (leaflet thickening) มี commissural fusion และ valvular calcification ซี่งส่งผลให้ลิ้นหัวใจมีการตีบ(stenosis)ในที่สุด
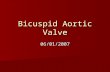
Figure 2 Calcific bicuspid aortic stenosis
(From Michael KB : Acquired aortic valve disease. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)

3
Pathophysiology เวลาที่เกิด aortic stenosis พบว่าส่งผลท าให้เกิด left ventricular afterload เพิ่มขึ้น ซึ่งจะมีผลกระทบอย่างมากต่อ left ventricular emptying ในจังหวะหดตัวของหัวใจ (systole) โดยปกติแล้ว aortic valve ที่ปกติจะไม่พบมี pressure gradient ในช่วง systole แต่ส าหรับผู้ป่วยที่มีการตีบตันของลิ้น (severe aortic stenosis) จะสามารถตรวจพบว่าจะมี peak pressure gradient > 40 mmHg ส าหรับผู้ป่วยที่เป็น aortic stenosis ที่อยู่ในระยะ well-compensated heart อาจตรวจพบว่ามี peak pressure gradient > 100 mmHg ในคนทั่วไปจะมีค่าปกติของ aortic valve cross-sectional area ประมาณ 2-4 cm2 ส าหรับผู้ป่วยที่มี severe aortic stenosis จะมี aortic valve cross-sectional area < 0.8 cm2 (< 0.5 cm2/m2 of body surface area) และเมื่อมีการตีบตันของลิ้นหัวใจในต าแหน่งนี้จะมีผลท าให้ left ventricular pressure สูงขึ้น ทั้งนี้เพื่อที่จะพยายามรักษา perfusion pressure ใน ascending aorta ให้คงที่หรือปกติ ผลกระทบต่อมาจะมี increased left ventricular wall stress, increased left ventricular wall thickness จนเกิด left ventricular hypertrophy ที่มีลักษณะเรียกว่า concentric hypertrophy ภาวะที่มี chronic left ventricular wall stress elevation นี้เองจะมีผลท าให้มี left ventricular failure, decreased ventricular contractility, decreased left ventricular ejection fraction (LVEF) และ มี progressive left ventricular dilatation ในที่สุด การรักษาภาวะ severe aortic stenosis โดยวิธีการผ่าตัดเปลี่ยน/ซ่อมลิ้นหัวใจ จะช่วยลด left ventricular afterload ลด capillary wedge pressure ลด left ventricular end-diastolic volume ซึ่งจะสามารถท าให้ left ventricular ejection fraction (LVEF) ดีขึ้น ส่วนภาวะ left ventricular hypertrophy นั้นพบว่าจะดีขึ้นหลังการผ่าตัดรักษา แตอ่าจต้องใช้เวลา 6-12 เดือน Clinical findings ในช่วงระยะแรกของผู้ป่วยที่เป็น aortic stenosis อาจไม่แสดงอาการ แต่หลังจากนั้นเมื่อมีการตีบมากขึ้นก็พบว่ามักจะมาด้วยกลุ่มอาการได้ 3 ลักษณะคือ exertional dyspnea, angina และ syncope ส าหรับการตรวจร่างกายก็จะไดัยินเสียงหัวใจผิดปกติเป็นแบบ systolic ejection murmur ที่บริเวณ second intercostal space ทางด้านขวาของ sternum โดยมีเสียง murmur ที่ radiate ไปยัง carotid arteries ทั้ง 2 ด้าน นอกจากนี้อาจตรวจพบ palpable thrill ได้ แต่อย่างไรก็ตาม palpable thrill และเสียง murmur อาจลดน้อยลงได้ถ้าพบว่าผู้ป่วยมี severe left ventricular failure การท า electrocardiogram จะพบมี left ventricular hypertrophy with strain บางรายอาจพบว่าเป็น atrial fibrillation หรือมี intraventricular conduction defect เช่น right bundle branch block, atrioventricular nodal block

4
การส่งตรวจ chest X-ray พบว่า เงาหัวใจมักไม่ค่อยโต, อาจเห็น calcified aortic valve, dilated ascending aorta (post-stenotic dilation), อย่างไรก็ตามผู้ป่วยที่เป็นมานาน และหรือไม่ยอมรักษาก็อาจพบว่ามี severe left ventricular failure ตรวจ chest X-ray ก็จะพบว่ามีหัวใจโตได้ (left ventricular dilation) ซึ่งถือว่าเป็นระยะที่ผลการท านายของโรค (prognosis)ไม่ดี และความเสี่ยงจากการผ่าตัดรักษาก็จะสูงขึ้นด้วย ในผู้ป่วย severe aortic stenosis บางรายที่มี heavily calcified aortic valve การส่งตรวจ chest X-ray อาจพบเห็นcalcium ที่ aortic valve โดยเฉพาะอย่างยิ่งให้สังเกตในท่า lateral view ของ chest X-ray Diagnosis การส่งตรวจด้วย Doppler echocardiography จะให้ผลการวินิจฉัยที่แม่นย า สามารถบอกถึง peak pressure gradient (across aortic valve), degree of stenosis, causes of stenosis, aortic regurgitation detection, associated other valve lesions และ ที่ส าคัญคือ ค่า left ventricular ejection fraction การส่งตรวจ cardiac catheterization ส าหรับผู้ป่วยที่เป็น aortic stenosis แนะน าให้ตรวจเป็นเฉพาะรายดังนี้
- aortic stenosis ในผู้ป่วยอายุ > 40 ป ี- ผู้ป่วยที่พบมีปัจจัยเสี่ยงต่อโรค coronary heart disease - borderline degree ของผู้ป่วย aortic stenosis ที่พบว่ามี impaired left ventricular
function Natural history ผู้ป่วยที่เป็น mild aortic stenosis อาจยังไม่พบว่ามีอาการอยู่หลายปี ทั้งนี้ขึ้นอยู่กับว่ายังอยู่
ในช่วงที่มี compensatory left ventricular hypertrophy หรือไม่ และ progression ของโรคเองก็ไม่แน่นอน (variable) แต่เมื่อเป็น moderate to severe aortic stenosis ส่วนใหญ่ก็จะมาด้วยอาการเหนื่อยง่าย (congestive heart failure) เจ็บอก (angina) หรือ เป็นลมหมดสติ (syncope) มีการศึกษาในเร่ืองของ survival rate ในผู้ป่วย severe aortic stenosis หลังจากที่เร่ิมมีอาการและไม่ได้รับการรักษาที่เหมาะสม พบว่า average survival ของผู้ป่วยกลุ่มอาการเจ็บอกเท่ากับ 3-5 ปี average survival ของผู้ป่วยกลุ่มอาการเป็นลมหมดสติเท่ากับ 3 ปี และ average survival ของผู้ป่วยกลุ่มอาการเหนื่อยง่ายและมีภาวะหัวใจวายร่วมด้วยเท่ากับ 1.5-2 ปี โดยในกลุ่มหลังนี้พบว่าผู้ป่วยจ านวนมากมีอุบัติการณ์ของการเกิด sudden death อันเนื่องมาจากภาวะ ventricular arrhythmia และที่ส าคัญพบว่า successful rate ของการท า CPR ในผู้ป่วยประเภทนี้ค่อนข้างต่ า

5
Management การให้ medical treatment ในผู้ป่วย symptomatic aortic stenosis พบว่ามีข้อจ ากัดมากและเป็นเพียงบรรเทาหรือควบคุมอาการเพียงชั่วคราว ดังนั้น ผู้ป่วย aortic stenosis ทุกคนที่มีอาการควรจะได้รับการผ่าตัดเปลี่ยน/ซ่อมลิ้นหัวใจ ส าหรับในรายที่มีอาการน้อยหรือไม่มีอาการ ก็ควรจะผ่าตัดรักษาหากพบว่ามี peak aortic gradient > 40 mmHg, aortic valve area < 0.8 cm2 หรือมี impaired left ventricular function แล้ว จากพยาธิสภาพของลิ้นหัวใจในผู้ป่วย severe aortic stenosis ส่วนใหญ่พบว่ามีการท าลายของ aortic leaflet ค่อนข้างมากแล้ว จึงมักจะต้องเปลี่ยนลิ้นหัวใจมากกว่าการซ่อมลิ้นหัวใจ ส่วนการท า percutaneous balloon aortic valvuloplasty ได้ผลไม่ค่อยดีนัก ปัจจุบันจึงเลือกรักษาโดยวิธีนี้น้อยลง Aortic regurgitation Causes
สาเหตุของการเกิด aortic regurgitation ที่พบได้บ่อยในประเทศไทย ได้แก่ 1. Rheumatic caused 2. Infective endocarditis 3. Annuloaortic ectasia เช่น Marfan syndrome เป็นต้น
สาเหตุอ่ืนๆที่อาจพบได้ ได้แก่ myxoid degeneration, aortic dissection, aortitis from rheumatoid arthritis ankylosing spondylitis and Reiter’s syndrome และ blunt and penetrating chest injuries Pathophysiology ผู้ป่วยที่เป็น aortic regurgitation จะพบว่าเกิดภาวะ volume overload ต่อ left ventricle มี increased diastolic filling pressure, increased diastolic volume and diastolic wall stress และ increased cardiac output ซึ่งส่งผลให้มี left ventricular dilatation (cor bovinum) และ ภาวะ eccentric hypertrophy และเช่นเดียวกันกับในกลุ่มผู้ป่วย aortic stenosis ผู้ป่วยที่เป็น chronic aortic regurgitation จะมี progressive left ventricular dilation, increased wall stress, increased pulmonary venous pressure, increased left ventricular diastolic pressure, subendocardial ischemia จนเกิดภาวะ impaired left ventricular function ในที่สุด

6
Clinical findings ผู้ป่วยมักมีอาการของ congestive heart failure โดยอาจพบอาการในลักษณะ dyspnea on exertion, orthopnea และ paroxysmal nocturnal dyspnea ก็ได้แล้วแต่ความรุนแรงของโรค นอกจากนี้อาจพบมีอาการ angina ได้ แต่ไม่ค่อยมาพบแพทย์ด้วยอาการ syncope การตรวจร่างกาย จะพบมี decreased diastolic aortic pressure (มักจะพบว่า < 60 mmHg), wide pulse pressure, “water hammer” pulse, Traube sign (pistol shot sounds), Muller sign (systolic pulsation of the uvula), Quincke sign (capillaries pulsations) ส าหรับเสียง murmur มักจะฟังได้เป็น diastolic blowing murmur ที่ต าแหน่ง AVA หรือ left parasternal area (3rd & 4th ICS) และในราย severe aortic regurgitation จะฟังได้ mid diastolic Austin Flint murmur ที่ left ventricular apex Diagnosis การส่งตรวจ chest X-ray มักจะพบมี left ventricular enlargement, dilatation of ascending aorta และ pulmonary venous congestion บางรายอาจถึงขั้นเป็น pulmonary edema การส่งตรวจ electrocardiogram ก็จะพบ left ventricular hypertrophy with strain การตรวจด้วย echocardiography ให้ผลการตรวจที่แม่นย า สามารถบอกถีง สาเหตุและความรุนแรงของโรค ดู associated pathology เช่น aortic root dilatation โดยเฉพาะกลุ่มที่เป็น aortic root disease (annuloaortic ectasia) และการประเมิน left ventricular ejection fraction ส าหรับผู้ป่วย aortic regurgitation ที่อายุ >50 ปีหรือพบมีปัจจัยเสี่ยงต่อการเป็นโรค coronary heart disease ควรพิจารณาท า coronary arteriography Natural history พบว่าในผู้ป่วย severe chronic aortic regurgitation อาจจะไม่มีอาการหรืออาการน้อยได้หลายปี จนกระทั่งเร่ิมมี elevated left ventricular end-diastolic pressure, left ventricular dilatation และ depressed left ventricular contractility อาการของผู้ป่วยก็จะชัดเจนและรุนแรงขึ้น ในผู้ป่วย asymptomatic aortic regurgitation, normal left ventricular function และรักษาด้วยยา มีการศึกษาพบว่ามี survival rate 81 % ที่ 5 ปี หลังจากผู้ป่วยเร่ิมมีอาการ จะพบว่า left ventricular contractility จะทรุดลงอย่างรวดเร็ว
ส าหรับผู้ป่วยในกลุ่ม acute onset ของ severe aortic regurgitation เช่น aortic valve endocarditis จะมีอาการค่อนข้างรุนแรง ทั้งนี้เนื่องจากภาวะ left ventricular decompensation และหากไม่รักษาให้เหมาะสมและทันการณ์ ผู้ป่วยอาจจะเสียชีวิตอย่างรวดเร็ว

7
Management เน่ืองจากผู้ป่วยกลุ่มนี้ไม่ค่อยมีปัญหาการเกิด sudden death เหมือนในผู้ป่วย aortic stenosis
ผู้ป่วย asymptomatic aortic regurgitation ที่มี normal left ventricular function แนะน าให้รักษาด้วยยา medical treatment และควรจะพิจารณาผ่าตัดในผู้ป่วย aortic regurgitation เมื่อผู้ป่วยมีอาการ, impaired left ventricular function, left ventricular dilatation หรือ มี significantly elevated left ventricular end-diastolic pressure
Figure 3 Surgical incision for aortic valve surgery
(From Michael KB : Acquired aortic valve disease. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)
Results of surgical therapy (Figure 3-5) ปัจจุบันน้ีพบว่าการผ่าตัดเปลี่ยน/ซ่อมลิ้นหัวใจมีความปลอดภัยมาก อัตราการเสียชีวิตจาก
การผ่าตัดค่อนข้างต่ า พบว่า 30-day mortality ส าหรับการท า isolated aortic valve replacement ประมาณ 2-5 % เพิ่มเป็น 6-15 % หากเป็นการผ่าตัดคร้ังที่ 2 (re-sternotomy) เพิม่เป็น 10 % หากท าผ่าตัด mitral valve replacement ร่วมด้วย (double valve replacement)
มีรายงานถึงปัจจัยเสี่ยงต่ออัตราการเสียชีวิตของการผ่าตัด primary isolated aortic valve replacement มีดังนี้
- increased age - decreased left ventricular function - poor preoperative functional status - renal insufficiency - atrial fibrillation นอกจากนี้ยังมีรายงานถึงสาเหตุการตายที่พบบ่อยในการผ่าตัด primary isolated aortic
valve replacement มีดังนี ้

8
- 58 % cardiac failure or infarction - 11 % hemorrhage - 7 % infection - 5 % arrhythmia - 4% stroke
Figure 4 Aortic valve replacement using the bioprosthesis (tissue valve)
(From Michael KB : Acquired aortic valve disease.Sabistion & Spencer Surgery of the Chest.
Philadelphia:Elsevier Saunders, 2005)
Figure 5 Aortic valve replacement using the allograft root technique
(From Michael KB : Acquired aortic valve disease.Sabistion & Spencer Surgery of the Chest.
Philadelphia:Elsevier Saunders, 2005)

9
Acquired Disease of the Mitral Valve Surgical Anatomy การท างานของ mitral valve เป็นการท างานที่ค่อนข้างซับซ้อนและต้องอาศัยส่วนประกอบหลายๆ ส่วนที่ต้องท างานร่วมกันอย่างมีประสิทธิภาพ ความผิดปกติในส่วนใดส่วนหนึ่งจะส่งผลให้การปิด-เปิดของลิ้นผิดปกติได้ ส่วนประกอบของ mitral valve ได้แก่
1. Leaflets (valvular tissue) 2. Mitral annulus 3. Chordae tendineae 4. Papillary muscle 5. Left ventricle
ส าหรับส่วนที่เรียกว่า subvalvular apparatus ของ mitral valve นั้น จะหมายถึง chordae tendineae และ papillary muscle Leaflets (valvular tissue) ของ mitral valve จะประกอบไปด้วย anterior leaflet, posterior leaflet, anterolateral และ posteromedial commissures โดยทั้งหมดนี้จะยึดล้อมรอบ mitral annulus ลักษณะของ anterior leaflet (aortic leaflet) จะมีลักษณะ semicircular shape โดยยึดติด 2 ใน 5 ส่วนของ annular circumference และ ตัว leaflet นีย้ังเชื่อมต่อไปถึง left และ noncoronary cusps ของ aortic valve ส าหรับ posterior leaflet (mural leaflet) จะเป็นลักษณะ quadrangular shape โดยยึดติด 3 ใน 5 ส่วน ของ annular circumference (Figure 6)
Figure 6 Surgical anatomy of the mitral valve
(From Farzan F et al : Acquired Disease of the Mitral Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)

10
ปัจจุบัน มีการแบ่ง Mitral valve แบบที่เรียกว่า anatomical nomenclature ซึ่งเป็นการก าหนด segmental valve analysis เพื่อเป็นการบอกต าแหน่งหรือบริเวณที่ผิดปกติที่ท าให้ลิ้นตีบหรือร่ัว เพื่อเป็นแนวทางในการวางแผนการผ่าตัดลิ้นหัวใจโดยเฉพาะอย่างยิ่งในการพิจารณาท า mitral valve reconstructive surgery โดยจะแบ่ง mitral valve เป็น 8 segments ดังนี ้(Figure 7) - Anterolateral commissure - Posteromedial commissure - Three scallops of the posterior leaflet (P1: anterior scallop, P2 : middle scallop, และ P3 : posterior scallop) - Three corresponding segments of anterior leaflet (A1 : anterior segment, A2 : middle segment, และ A3 : posterior segment)
Figure 7 Segmental mitral valve analysis
(From Farzan F et al : Acquired Disease of the Mitral Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)
ส าหรับ mitral annulus ถือว่าเป็นส่วนที่เชื่อม (junction) ระหว่าง left atrium และ left ventricle ขณะเดียวกันก็เป็น insertion site ของ valvular tissue ส่วนของ mitral annulus จะยึดติดกับ fibrous trigones โดยยังแบ่งออกเป็น right และ left fibrous trigones พบว่า right fibrous trigone ถือเป็น dense junctional area ของ annulus ระหว่าง mitral annulus, tricuspid annulus, noncoronary cusp of aortic annulus และ membranous septum ส่วน left fibrous trigone จะอยู่ตรง junction ระหว่าง left fibrous borders ของ aortic valve และ mitral valve นอกจากนี้ยังพบว่า mitral annulus บริเวณ posterior leaflet จะค่อนข้างบางและไม่มีส่วนที่เป็น rigid structure ให้ยึด จึงพบว่ามักจะเป็นบริเวณที่ขยายออก (annular dilation) ได้ง่ายเวลาที่เป็นโรคลิ้นหัวใจร่ัว

11
ส าหรับ chordae tendineae ซึ่งเป็นส่วนที่ยึดระหว่าง papillary และ leaflet ของ mitral valve สามารถแบ่งออกได้เป็น 3 กลุ่มด้วยกัน โดยดูจากบริเวณจุดยึด (site of insertion) ระหว่าง free margin และ base ของตัว leaflet ดังนี้ (Figure 8)
Figure 8 Subvalvular apparatus of the mitral valve
(From Farzan F et al : Acquired Disease of the Mitral Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)
- Marginal chordae (primary chordae) ยึดที่ free margin ของ leaflet โดยหน้าที่ส าคัญคือป้องกันการเกิด prolapsed valve - Intermediate chordae (secondary chordae) ยึดที่ ventricular surface ของ leaflet โดยมีหน้าที่ relieve the valvular tissue of excess tension - Basal chordae (tertiary chordae) จะพบที่ posterior leaflet เท่านั้น โดยยึดที่ leaflet base และยังเชื่อมกับ mitral annulus และ surrounding myocardial tissue ส าหรับ papillary muscles นั้นสามารถแบ่งเป็น anterolateral papillary muscle และ posteromedial papillary muscle ซึ่งเป็นที่ให้ chordae tendineae ยึดเพื่อไปยัง mitral leaflet ทั้งสองอัน anterolateral papillary muscle เลี้ยงโดย left anterior descending artery และ marginal branch ของ circumflex artery ส่วน posterior papillary muscle นั้นเลี้ยงโดย left circumflex artery หรือ right coronary artery โดยพบว่า posteromedial papillary muscle มักจะเป็นบริเวณที่ necrosis (single system of blood supply) เวลาเกิดภาวะ ischemic cardiomyopathy ซึ่งเป็นสาเหตุของการน าไปสู่การเกิด ischemic mitral regurgitation ได้

12
Mitral stenosis Causes สาเหตุของการเกิด mitral stenosis ที่พบบ่อยที่สุดได้แก่ rheumatic fever โดยเฉพาะอย่างยิ่งในประเทศด้อยพัฒนาหรือก าลังพัฒนารวมทั้งประเทศไทยด้วย พบว่ามีอุบัติการณ์คิดเป็น 25 % ของผู้ป่วยที่เป็น rheumatic heart disease (pure mitral stenosis) แต่อย่างไรก็ตามในทางคลินิกแล้วมักจะพบเป็นลักษณะ combined mitral stenosis และ regurgitation เป็นส่วนใหญ่ หลังการเป็น rheumatic disease จะมีผลท าให้เกิดการเปลี่ยนแปลงที่ลิ้นหัวใจ โดยท าให้มี fibrosis และตามมาด้วย fibroretractive transformation ของ mitral valve เกิดเป็น leaflet thickening, chordal thickening, shortening & fusion, commissural fusion จนเกิด leaflet calcification ในที่สุด ซึ่งท าให้มี restrictive motion ของ valve leaflets โดยเฉพาะในช่วง diastole ในรายที่เป็น advanced stage ก็จะพบมี calcification บริเวณ commissural edges ด้วย ท าให้เห็น mitral valve มีลักษณะที่เรียกว่า “fish mouth” Pathophysiology โดยปกติ normal mitral valve area (MVA) = 4-6 cm2 โดยถือว่าจะเป็น mitral stenosis ก็ต่อเมื่อมี MVA < 2 cm2 และถือเป็น critical stenosis เมื่อ MVA < 1cm2 ผู้ป่วยที่เป็น severe mitral stenosis จะท าให้เกิด left atrial hypertension ซึ่งจะน าไปสู่ภาวะ pulmonary hypertension, pulmonary interstitial edema ในระยะยาวอาจมีผลท าให้ right ventricular dilatation and dysfunction นอกจากนี้ จากปัญหา left atrial hypertension ก็จะท าให้เกิด left atrial enlargement และตามมาด้วย cardiac arrhythmia ซึ่งเกือบทั้งหมดจะเป็น atrial fibrillation เชื่อว่าเกิดจากไปรบกวน atrial conducting system ในหัวใจ และด้วยจากปัญหานี้ที่พบร่วมกับ mitral stenosis จึงมีผลท าให้ผู้ป่วยอาจมี thrombus formation หรือ clot ใน left atrial chamber ได้ ส าหรับ left ventricular function ในผู้ป่วย mitral stenosis ส่วนใหญ่จะปกติ อย่างไรก็ตามพบว่าประมาณ 25 % ของผู้ป่วย severe, chronic mitral stenosis โดยสันนิษฐานว่าอาจจะเป็นด้วยสาเหตุ prolonged reduction ของ preload และหรือ การเกิด scar ซึ่ง extend จากตัว mitral valve ไปยัง myocardium นอกจากนี้ ยังเชื่อว่าภาวะที่ผู้ป่วยเป็น chronic atrial fibrillation ก็อาจส่งผลท าให้มี cardiomyopathy (AF induced cardiomyopathy) ได้เช่นกัน
Clinical findings and Diagnosis การวินิจฉัย mitral stenosis ต้องอาศัยการซักประวัติ ตรวจร่างกาย chest X-ray
electrocardiogram (ECG) และ echocardiography ผู้ป่วยบางรายอาจตรวจพบความผิดปกติของเสียงหัวใจโดยที่ไม่มีอาการก็ได้ อาการที่มักจะน าผู้ป่วยมาพบแพทย์ได้แก่ fatigue, dyspnea หรือ

13
hemoptysis ในรายที่เป็นรุนแรงและพบเป็น acute pulmonary edema ผู้ป่วยบางรายอาจมาด้วยอาการใจสั่นจากภาวะ atrial fibrillation และอาจมีประวัติของ embolic event ก็ได ้
การตรวจร่างกายจากการฟังเสียงหัวใจ (auscultation) อาจฟังได้ auscultatory triad ดังนี ้- loud first heart sound - diastolic rumbling murmur (low pitch) at apex - opening snap (preserved leaflet mobility) การตรวจ chest X-ray ในผู้ป่วย mitral stenosis มักจะมีขนาดของหัวใจที่ปกติ อาจพบเห็น
เพียง left atrial enlargement และ มี pulmonary congestion ในผู้ป่วยที่เป็น severe, chronic mitral stenosis ก็จะเห็น right atrium และ right ventricle โตได้
ส าหรับการตรวจ electrocardiogram (ECG) อาจพบว่ามี normal sinus rhythm พร้อมกับเห็น p-mitrale ซึ่งบ่งบอกถึงว่ามี left atrial enlargement แต่โดยประสบการณ์แล้วพบว่าผู้ป่วยที่เป็นโรคน้ีและเข้ามารักษาด้วยการผ่าตัดหัวใจ ส่วนใหญ่จะเป็น atrial fibrillation ไปแล้ว และอาจพบว่ามี right ventricular hypertrophy ได้ ซึ่งจะท าให้ผู้รักษาควรจะพิจารณาการให้ anticoagulant drug และ ยาที่ควบคุม ventricular rate ในกรณีเป็น atrial fibrillation ด้วย
ส าหรับ diagnostic stool ที่ดีที่สุดในขณะนี้ส าหรับการวินิจฉัย mitral stenosis ได้แก่ การท า two-dimension (2D) color-doppler echocardiogram ซึ่งการตรวจวิธีนี้สามารถบอกและประเมินถึง
- mobility of mitral leaflets - commissures - subvalvular apparatus - severity of mitral stenosis (การวัด mitral valve area และ mitral valve score) - transmitral gradient - pulmonary artery pressure - associated other valves lesion (aortic and/or tricuspid diseases) - evaluation of right and left ventricular function
Indication for Surgery ปัจจุบันน้ีหลายสถาบันมีการท า percutaneous balloon mitral valvulotomy (PBMV) เพื่อรักษาผู้ป่วย mitral stenosis โดยพิจารณาเลือกผู้ป่วย ดังนี้ - symptomatic patients (NYHA II, III, และ IV) with isolated moderate to severe mitral stenosis (MVA < 1.5 cm2) - favorable valve morphology (low mitral valve score)

14
- asymptomatic patients with isolated moderate to severe mitral stenosis and pulmonary hypertension at rest > 50 mmHg PBMV ไม่ควรท าในผู้ป่วยที่มี left atrial thrombus, at least moderate mitral regurgitation, inadequate valve morphology (high mitral valve score) ข้อบ่งชี้ในการผ่าตัด - symptomatic patients (NYHA III และ IV) with moderate to severe mitral stenosis (MVA < 1.5cm2) และไม่เหมาะสมที่จะท า PBMV - asymptomatic patients with severe mitral stenosis with severe pulmonary hypertension and inadequate valve morphology ผู้ป่วย mild symptomatic mitral stenosis ที่มี MVA > 1.5 cm2 และ วัดว่ามี mean gradient < 5mmHg พบว่าจะมีอาการคงที่และสามารถด าเนินชีวิตปกติได้หลายปี โดยเพียงให้ medical treatment และ ติดตามการรักษาอย่างใกล้ชิดก็เพียงพอแล้ว Mitral regurgitation Causes
1. Degenerative disease (fibroelastic deficiency, Barlow’s disease, Marfan’s syndrome) 2. Rheumatic heart disease 3. Endocarditis 4. Trauma 5. Ischemic cardiomyopathy 6. Dilated cardiomyopathy 7. Calcified disease of the annulus 8. Endomyocardial fibrosis (EMF)
Pathophysiology
ในผู้ป่วยที่เป็น mitral regurgitation พบว่าจะมี retrograde regurgitation ของเลือดจาก left ventricle เข้าไปยัง left atrium ในช่วง systole ซึ่งท าให้เกิด volume overload ใน left ventricular chamber โดยในช่วงแรกๆ ที่หัวใจยัง compensate ได้อยู่ left ventricle จะยังไม่มีการเปลี่ยนแปลงรูปร่างและขนาด แต่หลังจากที่เป็นอยู่นานๆ volume overload ดังกล่าวจะท าให้มีภาวะ myocardial remodeling ของ left ventricle เกิด increased left ventricular wall stress ท าให้เกิดภาวะ left ventricular dilatation และ hypertrophy รวมทั้งตามด้วย left atrial enlargement ซึ่งก็จะท าให้เกิด atrial fibrillation ในที่สุดเช่นเดียวกัน ปัจจัยของ regurgitation flow จาก mitral regurgitation และ

15
atrial fibrillation จะเป็นตัวก าหนด onset ของ pulmonary hypertension โดยพบว่าในระยะแรกของการเกิด pulmonary hypertension จะยังคงเป็น reversible process แต่ถ้าหากปล่อยโรคไว้โดยไม่รักษาจนกลายเป็น severe chronic mitral regurgitation จะพบเป็น fixed pulmonary hypertension และภาวะ severe left ventricular dysfunction ซึ่งจะถือว่าเป็นกลุ่มที่มีความเสี่ยงสูงหากต้องผ่าตัดรักษา และยังถือว่าเป็นที่เป็นกลุ่มที่มี poor prognosis และมี low survival rate การที่จะเข้าใจถึง valve pathology ส าหรับผู้ป่วย mitral valve disease นิยมใช้ Carpentier’s functional classification ที่เรียกว่าเป็น “pathophysiological triad” โดย Dr. Carpentier ศัลยแพทย์ชาวฝรั่งเศส ดังนี้ - etiology (cause of the disease) - valve lesions (resulting from the disease) - valve dysfunction (resulting from the lesion) Carpentier’s functional classification (Figure 9) -Type I dysfunction : normal leaflet motion, mitral regurgitation is due to annular dilatation or leaflet perforation (e.g. ischemic cardiomyopathy, dilated cardiomyopathy, endocarditis) - Type II dysfunction : increased leaflet motion, the free edge of the leaflet overriding the plane of the annulus during systole : leaflet prolapse (e.g. fibroelastic deficiency, Barlow’s syndrome, Marfan’s syndrome) - Type IIIA dysfunction : restricted leaflet motion during both diastole and systole (e.g. rheumatic disease) - Type IIIB dysfunction : restricted leaflet motion during systole (e.g. ischemic cardiomyopathy, dilated cardiomyopathy)
Figure 9 Carpentier's functional classification
(From Farzan F et al : Acquired Disease of the Mitral Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)

16
Clinical findings and diagnosis ผู้ป่วยที่เป็น mitral regurgitation นั้น จะใช้เวลาหลายปีกว่าจะมีอาการโดยอาการจะค่อยเป็นค่อยไป ส าหรับกลุ่มที่มีอาการก็จะมาด้วยอาการ fatigue, decreased exercise capacity, shortness of breath, หรือ มาด้วยอาการ congestive heart failure โดยมักจะพบ atrial fibrillation ร่วมด้วย การตรวจร่างกายก็จะพบ high-pitch systolic murmur ที่ apex โดยเสียง murmur จะ radiate ไปที่รักแร้ Chest X-ray ก็จะพบมี left atrial และ left ventricular enlargement อาจพบมี pulmonary trunk enlargement ในกรณีที่มี pulmonary hypertension แล้ว ส าหรับ electrocardiogram อาจพบ left atrial enlargement, left and right ventricular hypertrophy และในผู้ป่วย chronic mitral regurgitation มักจะพบว่ามี atrial fibrillation แล้ว การท า 2D color-doppler echocardiogram ถือเป็น diagnostic tool ที่ดีที่สุด โดยสามารถบอกถึง - etiology of mitral regurgitation - severity of mitral regurgitation (scale 1+ to 4+) - location of valve dysfunction using segmental valve analysis - associated other valve lesions - left ventricular function (LVEF) - evaluate for pulmonary hypertension Indication for surgery เน่ืองด้วยปัจจุบันนี้การผ่าตัดซ่อม/เปลี่ยนลิ้นหัวใจ ในผู้ป่วย mitral regurgitation มีอัตราการเสียชีวิตที่ต่ ามาก เป็นผลท าให้การก าหนดข้อบ่งชี้ในการผ่าตัดรักษาจึงมีการปรับเปลี่ยนอยู่ตลอดเวลา กล่าวคือจะมีแนวโน้มผ่าตัดที่เร็วขึ้นแม้กระทั่งในกลุ่มที่ไม่มีอาการ การจะพิจารณาผ่าตัดหรือไม่ให้ค านึงถึง - severity of mitral regurgitation - left ventricular function - symptomatic or asymptomatic patients - etiology of mitral regurgitation - overall surgical risks (age, comorbid risk factors) - likelihood of valve repair

17
ส าหรับ severe symptomatic mitral regurgitation ควรจะรักษาโดยการผ่าตัดทุกรายถึงแม้จะมี poor left ventricular function ส าหรับผู้ป่วยที่เป็น severe mitral regurgitation แต่ยังไม่มีอาการ ก็ควรจะพิจารณาท า early surgery ก่อนที่จะมี impaired left ventricular function ส าหรับผู้ป่วยที่เป็น moderate asymptomatic mitral regurgitation (regurgitation volume 45-60 ml, 3+ mitral regurgitation, effective regurgitation orifice 30-39 mm2) แนะน าให้ผ่าตัดหากพบว่าเร่ิมมี left ventricular dysfunction หรือ มี supraventricular arrhythmia เป็นลักษณะ repairable valve โดยเฉพาะอย่างยิ่งที่มีสาเหตุจาก degenerative disease ข้อบ่งชี้ในการผ่าตัดส าหรับผู้ป่วยที่เป็น native mitral valve endocarditis มีดังนี้ 1. significant mitral regurgitation with or without symptoms of congestive heart failure 2. uncontrolled sepsis despite proper antibiotic therapy 3. presence of an antibiotic resistant organism 4. fungal, S. aureus, or gram negative bacilli endocarditis 5. evidence of mitral annular abscess 6. extension of infection to intervalvular fibrous body 7. formation of intracardiac fistulas 8. onset of a new conduction disturbance 9. large vegetations (> 1cm), particularly those that are mobile and located on the anterior leaflet, at high risk for embolic complications 10. multiple emboli after appropriate antibiotic therapy Surgical incisions ส าหรับการผ่าตัด mitral valve surgery มี surgical incisions ที่นิยมมี 4 วิธี ได้แก่ (ดังภาพ) A. full sternotomy B. upper hemisternotomy C. lower hemisternotomy D. right minithoracotomy โดยส าหรับการผ่าตัดในวิธีที่ B, C และ D จะเลือกใช้ส าหรับการผ่าตัด mitral valve surgery ที่เป็น minimally invasive approach ซึ่งขณะนี้ได้รับความนิยมมากขึ้น (Figure 10)

18
Figure 10 Surgical incisions for the mitral valve surgery
(From Farzan F et al : Acquired Disease of the Mitral Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)
Exposure of the mitral vavle (Figure 11) ส าหรับการผ่าตัด mitral valve surgery ปัจจุบันสามารถเลือกการลงแผลผ่าตัดเพื่อเข้าถึง mitral valve ได้ ที่นิยมมี 3 วิธี ได้แก่ A. interatrial approach through the Sondergaard’s groove B. horizontal biatrial transseptal approach C. superior biatrial trannseptal approach
Figure 11 Exposure of the mitral valve
(From Farzan F et al : Acquired Disease of the Mitral Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)

19
Fundamental of reconstructive surgery for the mitral valve โดยหลักการแล้วก่อนการผ่าตัด mitral valve reconstructive surgery ศัลยแพทย์จะต้องพิจารณาดู mitral valve apparatus ทั้งหมด เพื่อตรวจดูถึง กลไกการเกิด mitral regurgitation ความยากง่ายต่อการท า mitral valve repair เพื่อจะได้พิจารณาว่าควรจะเปลี่ยนหรือซ่อมลิ้นหัวใจ และหากจะซ่อมลิ้นหัวใจจะได้เลือกเทคนิคหรือวิธีการซ่อมได้อย่างเหมาะสม โดยสรุปการจะท า mitral valve reconstructive surgery ส าหรับ mitral regurgitation ควรพิจารณาหลัก 3 ข้อ ดังนี้ 1. valve analysis (โดยอาศัยหลักของ Carpentier’s functional classification) 2. remodeling ring annuloplasty 3. assessment of repair (quality of repair) Surgical techniques of reconstructive surgery for the mitral valve 1. Valve repair in type I dysfunction (Figure 12) โดยส่วนใหญ่แล้ว ผู้ป่วย mitral regurgitation ในกลุ่มนีจ้ะมีสาเหตุจาก annular dilatation ซึ่งเทคนิคการผ่าตัดจะนิยมใช้วิธี remodeling annuloplasty (ring annuloplasty technique)
Figure 12 Mitral valve repair using ring annuloplasty technique
(From Farzan F et al : Acquired Disease of the Mitral Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)
2. Valve repair in type II dysfunction (Figure 13-15) ในกลุ่มนี้ mitral regurgitation เกิดจากภาวะ leaflet prolapse ซึ่งเป็นได้ทั้ง anterior leaflet prolapse และหรือ posterior leaflet prolapse โดยมีเทคนิคต่างๆที่ปัจจุบันน้ีนิยมใช้มีดังนี้ - triangular/quadrangular resection - chordal transfer - chordal transposition - artificial chordoplasty

20
- papillary muscle sliding plasty - papillary muscle shortening
Figure 13 Mitral valve repair : Quadrangular resection and sliding plasty
(From Farzan F et al : Acquired Disease of the Mitral Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)
Figure 14 Mitral valve repair : Chordal transfer
(From Farzan F et al : Acquired Disease of the Mitral Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)

21
Figure 15 Mitral repair : Artificial chordoplasty
(From Farzan F et al : Acquired Disease of the Mitral Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)
3. Valve repair in type IIIA dysfunction (Figure 16) วิธีการซ่อมลิ้นในกลุ่มนี้มีหลากหลายวิธี ซึ่งส่วนใหญ่มักจะต้องใช้ร่วมกัน ทั้งนี้เนื่องจากเป็นกลุ่มที่มี leaflet restriction จาก chordal thickening retraction และ fusion นอกจากนี้ลักษณะของลิ้นหัวใจเองก็พบว่ามี leaflet retraction ส าหรับโรคที่มักเป็นสาเหตุคือ rheumatic valvular heart disease ส าหรับเทคนิคการผ่าตัดซ่อมลิ้นหัวใจได้แก่ - resection of secondary chordae - chordal fenestration - triangular wedge resection - commissurotomy - pericardial patch enlargement

22
Figure 16 Open mitral commissurotomy or valvulotomy
(From Farzan F et al : Acquired Disease of the Mitral Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)
4. Valve repair in type IIIB dysfunction จะเป็นความผิดปกติที่มักจะพบในกลุ่มผู้ป่วย ischemic cardiomyopathy และ dilated
cardiomyopathy การซ่อมลิ้นหัวใจในกลุ่มนี้ ปัจจุบันแนะน าให้ท า remodeling annuloplasty โดยใช้ undersized ring ประมาณ เบอร์ 24-28 mm
อย่างไรก็ตาม ส าหรับลิ้นหัวใจที่ช ารุดมากๆ (extensive leaflet destruction) เช่น severe endocarditis, heavy calcification of the leaflets or subvalvular apparatus โดยเฉพาะอย่างยิ่งกลุ่ม rheumatic disease หรือหลังการพยายามซ่อมลิ้นหัวใจแล้วพบว่าได้ผลไม่ดี (unacceptable residual regurgitation) ก็ควรตัดสินใจเปลี่ยนลิ้นหัวใจโดยใช้ลิ้นหัวใจเทียม โดยการเลือกชนิดของลิ้นหัวใจเทียมไม่ว่าจะเป็นแบบโลหะ (mechanical valve) หรือ แบบเนื้อเยื่อ (bioprosthesis / tissue valve) ก็แล้วแต่ข้อบ่งชี้และความเหมาะสมของผู้ป่วยแต่ละราย
Results Open commissurotomy for mitral stenosis มี operative risk < 0.5 % ได้ผลการผ่าตัดค่อนข้างดี (good early and late outcome) แต่
อย่างไรก็ตามผู้ป่วยกลุ่มนี้ก็จะต้องเผชิญกับภาวะ disease progression จนกลับมามี restenosis แทบทุกรายซึ่งจะต้องมีการผ่าตัดซ้ าเพื่อมาเปลี่ยนลิ้นหัวใจในภายหลัง

23
Hickey และคณะ ได้รายงานผู้ป่วยกลุ่ม young patients จ านวน 339 รายที่ได้รับการผ่าตัด open mitral commissurotomy พบว่ามี overall survival rate 95 %, 87 % และ 59 % ที่ 5, 10 และ 20 ปี ตามล าดับ โดยมี freedom from reoperation 78 % และ 47 % ที่ 10 และ 20 ปี ตามล าดับ
Herrera และคณะ ได้รายงาน actuarial survival 89 % และ 75 % ที่ 15 และ 18 ปีตามล าดับโดยมี freedom from reoperation 92 % ที่ 18 ปีของการติดตามผู้ป่วยหลังผ่าตัด
Mitral valve repair for mitral regurgitation ปัจจุบัน operative mortality ส าหรับการท า mitral valve repair surgery ค่อนข้างต่ า
ประมาณ 2-4 % แต่ในบางแห่งที่เป็น advanced cardiac centers พบว่ามี operative mortality น้อยกว่า 0.5 % นอกจากนี้จากการศึกษาที่ผ่านมาหลายสิบปียืนยันเหมือนกันว่า การผ่าตัด mitral valve repair ได้ผลที่ดีกว่าการผ่าตัด mitral valve replacement ซึ่งเชื่อว่าเหตุผลส าคัญข้อหนึ่งได้แก่ การที่ได้ให้ความส าคัญของการมี preservation of postoperative left ventricular function อย่างไรก็ตาม มีการศึกษาพบว่าปัจจัยที่อาจเป็นตัวก าหนดอัตราการตายจากการผ่าตัดประเภทนี้ มีดังต่อไปนี้
- onset of mitral regurgitation (acute or chronic) - etiology of mitral regurgitation (ischemic vs nonischemic) - impaired left ventricular function (preoperative low ventricular ejection fraction) - advanced age - high functional class (NYHA III-IV) - associated coronary heart disease พบว่า long-term survival ในผู้ป่วย mitral valve repair กลุ่ม nonischemic patients จะ
ประมาณ 68-94 % ที่ 10 ปี Mitral valve replacement ส าหรับ operative mortality ในผู้ป่วยที่ได้การผ่าตัด mitral valve replacement จะประมาณ
2-4 % โดยเฉพาะอย่างยิ่ง พบว่าการผ่าตัดเปลี่ยนลิ้นหัวใจจะมีความปลอดภัยยิ่งขึ้น หากใช้เทคนิคการผ่าตัดที่มีการท า preservation of posterior leaflet และ chordal sparing valve replacement ซึ่งพบว่าช่วยลดอุบัติการณ์การเกิด left ventricular disrupture และ การที่ยังคงไว้ซึ่ง ventriculoannular continuity นี้เองถือเป็นปัจจัยส าคัญในการที่ท าให้มี conservation of postoperative ventricular function

24
มีการศึกษารวบรวมข้อมูลของ Jamieson และคณะ โดยการเก็บข้อมูลผู้ป่วยจ านวน 13,936 ราย จาก STS National Database ที่ได้รับการผ่าตัดหัวใจ isolated mitral valve replacement พบว่ามี operative mortality 6.4 % โดยมี independent predictors of operative mortality ได้แก่
- age - urgent/emergent of the operation - renal failure (dialysis vs non dialysis dependent) - functional class - multiple reoperation - previous myocardial infarction - associated coronary disease นอกจากนี ้Jamieson และคณะยังพบอีกว่า survival rate ส าหรับผู้ป่วยที่ผ่าตัด mitral valve
replacement มีประมาณ 50-60 % ที่ 10 ปี ส าหรับชนิดของ prosthetic valve มี 2 ประเภท ด้วยกัน ได้แก่
- Mechanical prosthetic valve (ลิ้นแบบโลหะ) - Bioprosthetic valve or tissue valve (ลิ้นแบบเนื้อเยื่อ)
Mechanical prosthetic valve
Bioprosthetic valve

25
Acquired Disease of the Tricuspid Valve Surgical anatomy Tricuspid valve ประกอบไปด้วย 3 leaflets โดยยึดติดที่ tricuspid annulus และถือว่าเป็นลิ้นหัวใจที่มี valvular area Tricuspid annulus ส่วนฐาน (base) ของ anterior และ posterior leaflets ของ tricuspid valve พบว่ายึดติดกับ free wall ของ right ventricle แต่ส าหรับ septal leaflet จะเชื่อมติดกับส่วนฐานของ interventricular septum โดยลักษณะตามธรรมชาติของ tricuspid annulus จะไม่มี encircling fibrotic structure ท าให้เกิด annular dilatation ได้โดยง่าย Tricuspid leaflets ประกอบไปด้วย 3 leaflets ได้แก่ septal, anterior และ posterior leaflets ซึ่ง leaflet ทั้ง 3 ถูกแยกโดย commissures 3 commissures เช่นกัน ได้แก่ anteroseptal, anteromedial และ posteroseptal commissures พบว่า anterior leaflet มีขนาดใหญ่ที่สุด ตามมาด้วย posterior leaflet โดยมี septal leaflet มีขนาดเล็กที่สุด Chordae tendineae and papillary muscle Leaflets ของ tricuspid valve จะถูกยึดด้วย marginal และ basal chords โดยพบว่า marginal chords จะเกาะที่ free margin ของ leaflet ส่วน basal chords จะยึดกับ ventricular surface ของ leaflets หากมี elongation หรือ rupture ของ marginal chords จะท าให้เกิด leaflet prolapse ส่วน tricuspid basal chords จะช่วยในการดูแลเร่ือง valve และ ventricular geometry ส าหรับ papillary muscles มี 3 มัดด้วยกัน ได้แก่ anterior, posterior และ septal papillary muscles พบว่า anterior papillary muscle มีขนาดใหญ่ที่สุด และมักเป็นลักษณะ single head โดยเป็น papillary muscle ที่มี chordae มาเกาะมากที่สุดเช่นกัน นอกจากนี้ยังพบว่า มีจ านวน 20 % ที่อาจไม่มี septal papillary muscle โดยที่ลิ้นสามารถท างานได้ปกติ (Figure 17)

26
Figure 17 Surgical anatomy of the tricuspid valve
(From Carlos MG Duran : Acquired Disease of the Tricuspid Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)
Physiopathology Tricuspid valve lesions แบ่งเป็นได้ 2 ลักษณะ คือ organic tricuspid valve disease และ functional tricuspid regurgitation Organic tricuspid valve disease ส าหรับในประเทศด้อยพัฒนาหรือก าลังพัฒนาซึ่งรวมทั้งประเทศไทยด้วย พบว่าสาเหตุของ organic tricuspid valve disease ที่พบบ่อยได้แก่จาก rheumatic disease โดยจะท าให้ลิ้นหัวใจมีการหนาตัว (tricuspid valve leaflets thickening) และ พบมี commissural fusion แต่ก็มีข้อสังเกตเมื่อเปรียบเทียบกับ rheumatic mitral disease พบว่า rheumatic tricuspid disease จะไม่ค่อยพบว่ามี subvalvular stenosis หรือภาวะ valve calcifications อย่างไรก็ตาม ได้มีการศึกษาเพื่อค้นหาอุบัติการณ์ของการเกิด rheumatic tricuspid disease ที่พบร่วมกับ rheumatic mitral disaease จะพบว่าอยู่ระหว่าง 10-30 % ทั้งนี้ขึ้นอยู่กับว่าการศึกษาอุบัติการณ์ดังกล่าวได้ท าการศ฿กษาอ้างอิงกับผลการตรวจจาก echocardiography จาก surgical findings หรือ จาก postmortem Tricuspid valve endocarditis ถึงแม้ในประเทศที่เจริญแล้วจะมีอุบัติการณ์เพียง 5-10 % แต่ส าหรับในแถบภาคพื้นบ้านเรายังถือว่าพบค่อนจะบ่อยกว่า โดยเฉพาะอย่างยิ่งในกลุ่ม intravenous drug abuse ลักษณะของ lesions เป็นได้ตั้งแต่เป็นเพียง isolated vegetations ไปจนถึงพบว่ามี destruction ของ valve และ annulus และที่น่าสนใจใน vegetations ที่พบใน tricuspid valve endocarditis พบว่ามักจะเห็นอยู่บริเวณ free edge ของ tricuspid valve leaflets ซึ่งไม่ค่อยเหมือนใน mitral valve endocarditis ด้วยเหตุนี้เองท าให้เวลารักษาผู้ป่วย tricuspid valve endocarditis with vegetations มักจะมีโอกาส conservative treatment ในความหมายนี้ก็คืออาจไม่ต้องผ่าตัด มากกว่าในกลุ่มผู้ป่วย mitral valve endocarditis ส าหรับเชื้อที่เป็นสาเหตุที่พบบ่อยได้แก่ Staphylococcus aureus โดยเฉพาะอย่างยิ่งในกลุ่ม drug addicts ตามมาด้วยกลุ่ม gram negatives และ Candida

27
ส าหรับ fungal infections พบว่ามีอุบัติการณ์มากขึ้นในกลุ่มผู้ป่วยที่ต้องใส่ invasive monitoring โดยเฉพาะผู้ป่วยในภาวะ multiple organ failure และต้องอยู่ใน intensive care unit เป็นเวลานาน สาเหุตอ่ืนที่อาจพบได้ คือ
- degenerative change (myxomatous) - trauma - postinfarction - carcinoid - endocardial fibroelastosis - lupus erythematosus - tumors (myxoma) - mediastinal fibrosis Functional tricuspid regurgitation สาเหุตหลักจะเกิดจากภาวะ annular dilatation มีการศึกษาของ Waller และคณะ พบวา่ในผู้ป่วยที่มี tricuspid regurgitation จะมีสาเหตุจาก functional regurgitation อยู่ประมาณ 50 % โดยปกติขนาดของเส้นรอบวง (perimeter) ของ tricuspid annulus จะวัดได้ประมาณ 100-120 mm. แต่ส าหรับในผู้ป่วยที่มี functional tricuspid regurgitation ขนาดของเส้นรอบวงพบว่าอาจจะขยายมากถึง 150-170 mm. นอกจากนี้ Carpentier และคณะ ได้ศึกษาพบว่าการขยายของ tricuspid annulus ดังกล่าว บริเวณ anterior และ posterior segments ของ annulus มีการขยายมากกว่าบริเวณ septal segment ซึ่งจาการศึกษานี้น ามาสู่การพัฒนาเทคนิคของการท า annuloplasty ส าหรับสาเหตุที่พบบ่อยของการเกิด functional tricuspid regurgitation เกิดจากการที่มี right ventricular pressure overload ที่เป็นผล (secondary effect) จาก chronic mitral valve disease ซึ่งพบได้ทั้งใน mitral stenosis และ mitral regurgitation อย่างไรก็ตาม ก็มีข้อสังเกตที่น่าสนใจว่าในกลุ่มผู้ป่วยที่เป็น congenital heart disease ที่มี severe pulmonary hypertension แต่กลับไม่ค่อยพบว่ามีภาวะ functional tricuspid regurgitation ท าให้แพทย์หลายคนเชื่อว่าปัญหาดังกล่าวน่าจะเป็นผลจากการมี right ventricular failure เป็นสาเหตุจริงๆ มากกว่าจะเป็นจาก right ventricular pressure overload (Figure 18)

28
Figure 18 Diagram of the tricuspid valve annulus showing normal (inner ellipse)
and myxomatous (outer ellipse) valve
(From Carlos MG Duran : Acquired Disease of the Tricuspid Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)
Diagnosis ในปัจจุบันนี้เป็นที่ยอมรับว่า 2D color Doppler echocardiography เป็น investigation tool ที่ดีที่สุด มีความน่าเชื่อถือ (reliability) ผู้ป่วยไม่ต้องเจ็บตัว (noninvasiveness) ไม่ต้องเสี่ยงต่อการรับรังสีหรือสารทึบรังสี โดยสามารถบอกถึง สาเหตุและความรุนแรงของโรคได้ด้วย ในกรณีของ surgical point of view เมื่อขณะท า 2D color Doppler echocardiography ควรจะสามารถบอกข้อมูลต่อไปนี้ - whether or not the patient has tricuspid disease - whether it is organic, functional, or mixed - quantification of the degree regurgitation and direction of regurgitation jet - pulmonary artery peak and mean pressures - presence and quantification of transvalvular pressure gradients - maximum and minimum tricuspid annulus diameter and systolic shortening - anatomical features of the valve, such as leaflet thickness, mobility, billowing of
the leaflet body, and location of the prolapsing free edge toward the right atrium - absence or presence of a patent foramen ovale (PFO) Surgical indications โดยส่วนใหญ่แล้วเทคนิคการซ่อมลิ้นหัวใจในผู้ป่วย tricuspid valve disease ไม่ค่อยยุ่งยากและได้ผลค่อนข้างดี ยกเว้นในรายที่เป็น severe disease ที่อาจมีผลการผ่าตัดที่ไม่ดีซึ่งอาจถึงกับ

29
ต้องพิจารณาเปลี่ยนลิ้นหัวใจไปเลย อย่างไรก็ตามที่มักจะเป็นประเด็นปัญหาในขณะนี้คือ การที่มีสมมติฐานที่ว่าในกลุ่ม functional tricuspid regurgitation พบว่าการร่ัวของลิ้นจะดีขึ้นเมื่อได้แก้ไขปัญหาของ mitral valve disease หรือแม้แต่ในกลุ่มที่มีเพียง mild tricuspid valve regurgitation ที่ตัดสินใจไม่ได้ซ่อมลิ้นหลังการผ่าตัด mitral valve surgery ซึ่งมีการศึกษาของ King และคณะ พบว่าเมื่อศึกษากลุ่มผู้ป่วยที่ต้องกลับมาผ่าตัด tricuspid valve surgery หลังจากที่ได้ผ่าตัดท า mitral valve replacement ไปแล้ว มีถึง 66 % ที่พบว่าขณะผ่าตัดคร้ังแรก tricuspid valve disease เป็นแค่เพียง mild regurgitation เท่านั้น Porter และคณะ ท าการศึกษาติดตามกลุ่มผู้ป่วยจ านวน 65 คนที่เป็น rheumatic heart disease และได้ท าการผ่าตัด mitral valve replacement โดยที่ไม่ได้ท า tricuspid valve surgery แต่อย่างไร เมื่อติดตามไปประมาณ 30 ปี (mean 11.3 years) โดยน าผู้ป่วยกลุ่มนี้มาตรวจ echocardiography พบว่ามี significant tricuspid regurgitation ถึง 67 % และหนึ่งในสามเป็น organic tricuspid valve disease ข้อมูลเหล่านี้แสดงให้เห็นถึงว่ามีความล าบากพอสมควรในการประเมินและตัดสินใจว่าผู้ป่วยคนใดที่มี tricuspid regurgitation ว่าควรจะพิจารณาซ่อมหรือไม่ อย่างไรก็ตาม ข้อมูลของการตรวจและการวินิจฉัยที่แม่นย าก่อนการผ่าตัด (preoperative assessment and diagnosis) ถือว่าเป็นหัวใจส าคัญส าหรับศัลยแพทย์ในการตัดสินใจและวางแผนการรักษาได้อย่างเหมาะสมในผู้ป่วยแต่ละราย Tricuspid valve surgery ส าหรับ surgical approach ในการผ่าตัด tricuspid valve surgery นั้น สามารถผ่าตัดผ่าน incision ได้ 2 วิธี คือ median sternotomy และ right thoracotomy โดยผ่านทาง right atriotomy incision ก็สามารถเข้าถึง tricuspid valve ได้โดยง่าย (Figure 19)
Figure 19 Surgical view of the tricuspid valve
(From Carlos MG Duran : Acquired Disease of the Tricuspid Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)

30
ส าหรับ เทคนิคการผ่าตัด tricuspid valve disease (stenosis/regurgitation) พอสรุปได้ 3 วิธีด้วยกัน ดังน้ี 1. tricuspid commissurotomy 2. tricuspid annuloplasty 3. tricuspid replacement Tricuspid commissurotomy เป็นการผ่าตัดโดยใช้มีดกรีดตามแนว commissures ซึ่งโดยปกติถึงแม้ tricuspid valve จะมี 3 commissures แต่โดยทั่วไปมักจะมีเพียง 1-2 commissures ที่จะมี fusion โดยพบว่า anteroseptal commissure จะพบว่ามี fusion บ่อยที่สุด จุดส าคัญข้อหนึ่งของการท า tricuspid commissurotomy ก็คือแนวมีดกรีดตรง commissure เมื่อท าแล้วขอบทั้งสองด้านต้องมี chordae ยึดติดด้วยเพื่อป้องกันการเกิด regurgitation อย่างไรก็ตามหลังท า tricuspid commissurotomy มักจะต้องท า tricuspid annuloplasty ร่วมด้วย เนื่องจากมักจะมีปัญหา lack of leaflet tissue และ annular dilatation (Figure 20)
Figure 20 Tricuspid valve commissurotomy
(From Carlos MG Duran : Acquired Disease of the Tricuspid Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)
Tricuspid annuloplasty จุดประสงค์ของการท า tricuspid annuloplasty ก็เพื่อลดขนาดเส้นรอบวงของ tricuspid annulus หรือลดขนาดของ tricuspid orifice นั่นเอง ปัจจุบันเทคนิคที่นิยมท าคือการ DeVega semicircular suture annuloplasty โดยการท า double suture ที่เย็บบริเวณ base ของ anterior และ posterior leaflets จาก aneteroseptal commissure ไปจนถึง posteroseptal commissure สาเหตุที่ไม่เย็บครบวงเนื่องจาก ที่ base ของ septal leaflet มี conductive tissue (AV node) ฝังอยู่ข้างในนั่นเอง

31
แต่อย่างไรก็ตาม เมื่อติดตามผู้ป่วยหลังท า DeVega tricuspid annuloplasty พบว่ามีปัญหา recurrent regurgitation ในภายหลังโดยเชื่อว่าเกิดจาก sutures cutting through/breaking ซึ่งมีรายงานต้ังแต่ 15-25 % Carpentier จึงได้เสนอการใช้ rigid prosthetic ring (Carpentier annuloplasty ring) เพื่อลดขนาดของ annulus อย่างไรก็ตามก็มีแพทย์จ านวนมากนิยมใช้แบบ flexible prosthetic ring (Duran annuloplasty ring) ซึ่งถือได้ว่าการใส่ prosthetic ring ทั้ง 2 แบบ ให้ผลการผ่าตัดที่ดีใกล้เคียงกัน (Figure 21)
Figure 21 Tricuspid valve annuloplasty
(From Carlos MG Duran : Acquired Disease of the Tricuspid Valve. Sabistion & Spencer Surgery of the Chest.
Philadelphia : Elsevier Saunders, 2005)
Tricuspid valve replacement โดยส่วนใหญ่แล้ว tricuspid lesion มักจะซ่อมลิ้นได้ ยกเว้นในรายที่ลิ้นเสียหายมากๆ เช่น severe endocarditis ที่มี valve destruction มากๆ ก็คงต้องท า tricuspid valve replacement ส าหรับชนิดของลิ้นหัวใจเทียมที่จะใช้ไม่ว่าจะเป็น mechanical prosthetic valve หรือ bioprosthesis ปัจจุบันพบว่าไม่มีความแตกต่างกัน ทั้งในประเด็น survival rate และ reoperation rate อย่างไรก็ตาม ศัลยแพทย์จ านวนมากยังกังวลในเร่ืองของ prosthetic valve thrombosis ในกลุ่ม mechanical valve และการที่ผู้ป่วยกลุ่มนี้ต้องได้รับ anticoagulation (warfarin) ตลอดชีวิต มีผลให้ในปัจจุบัน การท า tricuspid valve replacement มีแนวโน้มจะเลือกใช้ bioprosthesis (tissue valve) เพิ่มมากขึ้น
DeVega technique Ring annuloplasty

32
Results มีรายงานส าหรับการท าผ่าตัด tricuspid valve surgery ในภาพรวมทั้งการเปลี่ยนหรือซ่อมลิ้นหัวใจพบว่ามี hospital mortality ประมาณ 15-20 % แต่ถ้าหากศึกษาดูเฉพาะในกลุ่มที่ท า tricuspid valve replacement พบว่ามี hospital mortality เพิ่มถึงเกือบ 40 % และบางรายงานยังพบว่าหากท า tricuspid valve replacement ในกลุ่มที่เคยผ่าตัดหัวใจมาก่อน (reoperation case) พบว่ามี hospital mortality ถึง 50 % ท าให้ศัลยแพทย์หัวใจในปัจจุบันต่ืนตัวมากขึ้นในเร่ืองของการท า preoperative evaluation ของ tricuspid lesion ที่ละเอียดและแม่นย าขึ้น รวมทั้งการพัฒนาเทคนิคการซ่อมลิ้นหัวใจ tricuspid valve ที่ดีขึ้น เพื่อหลีกเลี่ยงการท า tricuspid valve replacement และจะได้ไม่ต้องมาเผชิญกับปัญหาการเกิด prosthetic valve thrombosis และ ภาวะแทรกซ้อนที่มักจะเกิดขึ้นจากการที่ผู้ป่วยต้องได้รับ permanent anticoagulation สิ่งส าคัญอีกสิ่งหนึ่งที่ศัลยแพทย์หัวใจควรค านึงถึงคือสาเหตุอ่ืนๆ ของ tricuspid pathology ที่นอกเหนือจาก rheumatic lesion ที่อาจเป็นสาเหตุของโรค เช่น myxomatous, ischemic หรือ cardiomyopathic tricuspid regurgitation ที่อาจจะต้องอาศัยเทคนคิการรักษาและการผ่าตัดที่แตกต่างกัน __________________________________________________________
References
1. Michael K. Banbury: Acquired Aortic Valve Disease: In Frank W. Sellke editor-in-chief: Sabiston & Spencer Surgery of the Chest 7th edition. Philadelphia: Elsevier Saunders, 2005, pp.1285-1297.
2. Farzan Filsoufi, Sacha P. Salzberg, Lishan Aklog, David H. Adams: Acquired Disease of the Mitral Valve: In Frank W. Sellke editor-in-chief: Sabiston & Spencer Surgery of the Chest 7th edition. Philadelphia: Elsevier Saunders, 2005, pp.1299-1333.
3. Carlos M.G. Duran: Acquired Disease of the Tricuspid Valve: In Frank W. Sellke editor-in-chief: Sabiston & Spencer Surgery of the Chest 7th edition. Philadelphia: Elsevier Saunders, 2005, pp.1335-1354.
4. Catherine M. Otto: Valvular Heart Disease: In Peter L, Robert OB, Douglas LM, Douglas PZ editors: Braunwald’s Heart Disease 8th edition. Philadelphia: Elsevier Saunders, 2008, pp.1625-1712.

33
5. Nicholas TK, Eugene HB, Donald BD, Frank LH, Robert BK: Acquired Valvar Heart Disease: In Nicholas TK editor: Kirklin/Barratt/Boyes Cardiac Surgery 3rd edition. Philadelphia: Churchill Livingstone, 2003, pp.483-671.
6. Fedak PWM, Verma S, David TE, et al: Clinical Update: Clinical and pathophysiological implications of a bicuspid aortic valve. Circulation 106: 900-904, 2002.
7. Banbury MK, Cosgrove DM, Thomas JD, et al: Hemodynamic stability during 17 years of the Carpentier-Edwards aortic pericardial bioprosthesis. Ann Thorac Surg 73: 1460-1465, 2002.
8. Carpentier A: Cardiac valve surgery-the “French correction.” J Thorac Cardiovasc Surg 86(3): 323-337, 1983.
9. David TE, Feindel CM, Armstrong S, et al: Reconstruction of the mitral annulus. A ten-years experience. J Thorac Cardiovasc Surg 110(5): 1323-1332, 1995.
10. Bolling SF, Pagani FD, Deeb GM, et al: Intermediate-term outcome of mitral reconstruction in cardiomyopathy. J Thorac Cardiovasc Surg 115: 381-386, 1998.
11. Duran CM, Gometza B, De Vol EB: Valve repair in rheumatic mitral disease. Circulation 84 (suppl 5): III 125 - III 132, 1991.
12. Onada K, Yasuda F, Takao M, et al: Long term follow-up after Carpentier-Edwards ring annuloplasty for tricuspid regurgitation. Ann Thorac Surg 70: 796-799, 2000.
13. Holper K, Haehnel JC, Augustin N, et al: Surgery for tricuspid insufficiency: long-term follow up after DeVega annuloplasty, Thorac Cardiovasc Surg 41: 1-8, 1993.
14. De Paulis R, Bobbio M, Ottino G, et al: The DeVega tricuspid annuloplasty. Perioperative mortality and long-term follow up. J Cardiovasc Surg 31: 512-517, 1990.
__________________________________________________
ผศ.นพ.ศุภชัย เชื้อรัตนพงษ ์ หน่วยศัลยกรรมทรวงอก หัวใจ และหลอดเลือด ภาควิชาศัลยศาสตร ์คณะแพทยศาสตร์ มหาวิทยาลัยเชียงใหม่
Related Documents