-
8/20/2019 ACLS Class Packet 2015
1/9
ACLS Cardiac Arrest Algorithm
Neumar, R. W. et al. Circulation 2010;122:S729-S767
-
8/20/2019 ACLS Class Packet 2015
2/9
ACLS Cardiac Arrest Circular Algorithm
Neumar, R. W. et al. Circulation 2010;122:S729-S767
-
8/20/2019 ACLS Class Packet 2015
3/9
Bradycardia Algorithm
Neumar, R. W. et al. Circulation 2010;122:S729-S767
-
8/20/2019 ACLS Class Packet 2015
4/9
Neumar, R. W. et al. Circulation 2010;122:S729-S767
Tachycardia Algorithm
-
8/20/2019 ACLS Class Packet 2015
5/9
Post-cardiac arrest care algorithm
Peberdy, M. A. et al. Circulation 2010;122:S768-S786
-
8/20/2019 ACLS Class Packet 2015
6/9
O'Connor, R. E. et al. Circulation 2010;122:S787-S817
Acute Coronary Syndromes Algorithm
-
8/20/2019 ACLS Class Packet 2015
7/9
Goals for management of patients with suspected stroke
auch, E. C. et al. Circulation 2010;122:S818-S828J
-
8/20/2019 ACLS Class Packet 2015
8/9
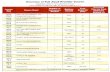
ACLS Code DrugsDrug Indications Dosage Administration
Adenosine/
Adenocard
Narrow PSVT/SVTWide QRS Tachy of
uncertain cardiac origin
6 mg followed by 12mg in 1-2min.
Rapid IV push close to thehub followed by a saline
bolus.
Amiodarone Vfib/pulseless VT,VT with a pulse. May be
used for rate control of
WPW or atrial tachycardias.
300mg IVP for cardiac arrest.
Consider repeating with 150mg
in 3-5 min.
150mg over 10 min for stableVT, may repeat 150mg every 10
min as needed. Cumulative dose
of 2.2 IV in 24 hrs.
Slow infusion 360mg IV over 6hrs, maintenance 540mg over 18
hrs. (0.5mg/min)
Draw up with filtered
needle. Administer drip with
filtered tubing.
Gtt infusion mixed
900mg/500 D5W.
1mg/min = 33.3cc/hr
.5mg/min = 16.6cc/hr
Half life is up to 40 days.
Atropine Symptomatic sinus bradycardia.
.5 mg IV every 3-5 min for
bradycardia, not to exceed 3 mg
Tracheal 2-3mg diluted in 10cc NS.
Do not give less than 0.5mg
IV.
May be given IV, IO, or ET
Does not work with heart
transplant patients due todenervation.
Calcium Chloride Known or suspectedhyperkalemia (renal fx).Hypocalcemia after multiple
blood tx. Antidote forcalcium channel blockers or
beta blocker overdose
8-16mg/kg IV for hyperkalemia
and calcium channel blockeroverdose.
Do not mix with sodium
bicarbonate.
Dopamine Used for hypotension withsigns and symptoms of
shock or bradycardia
Mixed 400mg/250D5W
2-10mcg/kg/min.
IV line must be a good one.Will cause extravasation
with infiltration
Do not mix with sodium
bicarbonate.
Epinephrine Cardiac arrest, VF, pulselessVT, asystole, PEA
Symptomatic bradycardia,
severe hypotension,anaphylaxis
Cardiac arrest: 1mg of the1:10,000 administered q 3-5 min
follow each dose with IV flush.
Bradycardia or hypotension usea gtt.
1mg/250cc: 1mcg/min = 15cc/hr.
May be given IV, IO or ET
-
8/20/2019 ACLS Class Packet 2015
9/9
Drug Indications Dosage AdministrationMagnesium Sulfate Torsades de pointes or
suspected hypomagnesemia.
Life threatening arrhythmiasdue to dig toxicity.
1-2 gm diluted in 10 cc D5W
IVP if in cardiac arrest.
If not in cardiac arrest mix 1-2
gm in; 50 to 100 cc D5W to
infuse over 5 to 60 min.
May cause fall in BP with
rapid administration.
Use with caution if renal
failure is present.
Morphine Sulfate Used for treatment ofischemic chest pain, acutecardiogenic pulmonary
edema, anxiety
Decreases the myocardial
preload and causes
peripheral venous pooling.
Dosage should be in 1 to 2 mg
increments up to 10 mg max
Given slow IV over 1-2 min
Precautions: respiratory
depression and hypotension
Narcan/Naloxone Used to reverse respiratorydepression that results from
narcotics
Also used for coma of
unknown etiology
Dosage – 0.4 mg to 2 mg IV or
IO and may be given ET
IV or IO meds should be
given over 1 min.
Precautions: If given rapidly
IV/IO can cause projectile
vomiting
Patient may become
agitated or violent
Procainamide Anti-arrhythmic for stablewide QRS Tachycardia
20-50 mg/min End Points: Arrhythmia
suppressed, hypotension
ensues, QRS duration
increase >50%, max dose17 mg/kg
Sotalol Hemodynamically StableMonomorphic Ventricular
Tachycardia
3rd Line Anti-Arrhythmic
100 mg over 5 min or1.5 mg/kg over 5 min
Avoid if prolonged QT
Sodium Bicarbonate Preexisting hyperkalemia,metabolic acidosis,
prolonged resuscitation.
1 meq/kg IV bolus.Repeat half dose q 10 min
Not recommended forroutine use in cardiac arrest
patients.
Vasopressin May be used as analternative pressor to epi in
the treatment of CardiacArrest instead of 1st or 2nd
dose of epi
IV, IO 40 U IV push X 1 dose
only.
ET 80U X 1 dose only
Do not give any epi for
10 min after vosopressin is
given.
Compiled by:Rebecca Cass NREMT-P
innovative solutionsin healthcare education, llc
5923 cherrycrest lane
charlotte, nc 28217
704-527-5119 www.innosols.com