Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

AchievingOptimum Nutrition and
Development Potential for Every Child in Rajasthan
The Mission Mode


In collaboration with:
Department of Medical & HealthDepartment of Education
Department for Tribal Area DevelopmentDepartment for Rural Development & Panchayati Raj
Department of Information & Public RelationsDepartment for Ground Water
Department of AgricultureDepartment of Food & Civil Supplies
Salt CommissionerPublic Health Engineering Department
Home Science Departments of Universities
Department of Women and Child DevelopmentGovernment of Rajasthan
AchievingOptimum Nutrition and
Development Potential for Every Child in Rajasthan
The Mission Mode


Message from Chief Minister
Nutrition is the cornerstone that defi nes and affects health and well being. Despite
several policies and plans both at national and state levels, raising the health and
nutritional status of the tribal population remains a challenge. Social and cultural
constraints alongwith little access to health care facilities play a role in the poor
nutritional status of tribal communities which constitute nearly 13 per cent of the
total population of the state.
Malnutrition among children, high infant, child and maternal mortality rates and
a poor nutritional status undermines economic growth and perpetuates poverty.
Micronutrient defi ciencies, especially iron, iodine and vitamin A, among vulnerable
sections are closely related to the poor nutritional status of the entire tribal
community.
Through the State Nutrition Mission, we aspire to address the nutritional problems of
tribal communities, in particular children below 3 years of age, pregnant and nursing
mothers and adolescent girls, in a time-bound and result-oriented manner. In its
fi rst phase, the Mission shall focus on 13 districts of the state, fi ve of which are largely
tribal. It is hoped that the interventions visualized in this Mission would stem the
levels of morbidity and mortality among women and children and lead to a better
quality of life for the vulnerable sections targeted in this Mission.
I take great pleasure in launching this Mission and committing ourselves to the
rights of women and children. I also take this as an opportunity to rededicate our
Government’s commitment to the cause of improving the well being of the people,
especially the women and future generations.
My best wishes are with this Mission.
(Vasundhara Raje)
Vasundhara RajeChief Minister
Government of Rajasthan

The departments of Women and Child Development and Medical and Health have been
implementing various schemes and programmes at the state level, addressing the health
and nutritional needs of women and children in Rajasthan. These schemes and programmes
have to respond even more strongly to the specifi c regional variations and needs of the
state’s vast tribal population by adopting new and innovative approaches to ensure access
to quality services.
It is estimated that nearly 51 per cent of children below 5 years of age suffer from varying
degrees of malnutrition in Rajasthan. In addition, the high prevalence of anemia, vitamin
A defi ciency and iodine defi ciency disorders is crippling development efforts in invisible
ways. While food and nutrition security have come to be recognized as key to tackling the
problem of malnutrition along with community participation, the Government of Rajasthan
recognizes the increasing concern for the survival and protection of the child, and improved
health for the mother and the adolescent girl.
In pursuance of the decisions taken in late 2005 by the Economic Policy and Reform Council,
we commence this Mission by addressing the nutritional needs of critical sections of
population of 13 districts, fi ve of them predominantly tribal, of the State. Subsequently, the
Mission will be extended to include the remaining 19 districts in a phased manner.
Although the Rajasthan State Nutrition Mission is a joint initiative of the departments of
Women and Child Development and Medical and Health and has had the benefi t of the
technical support and guidance of UNICEF Rajasthan, the Mission calls for a convergence
of all concerned departments and sectors who will be actively involved in addressing the
multiplicity of causes and the multiple determinants of nutrition.
We hope that this Mission would serve as an example for achieving health and nutritional
goals through a mission mode, based on specifi c strategies and local initiatives.
Dr Digember SinghMinisterMedical and Health
(Kanak Mal Katara)
Message from Ministers
Kanak Mal KataraMinister
Women and Child Development
(Dr Digember Singh)

R.K. Meena Alka Kala
In recognition of nutrition being vital to development, the Departments of Women and
Child Development and Medical and Health jointly commit to working toward reducing
malnutrition and micronutrient defi ciencies in a mission mode. This Mission Document,
which is the outcome of the collective brainstorming of several departments and experts
facilitated by UNICEF Rajasthan to design a feasible framework for action, not only reviews
the current health and nutritional situation of children, adolescent girls and pregnant and
nursing mothers in the tribal areas of Rajasthan but also sets out the approaches and strategic
interventions to be adopted by the Mission, both multi-pronged and multi-sectoral.
The Mission that will be initiated in 13 districts of the state, fi ve of which are predominantly
tribal, aims to reduce prevalence of malnutrition among children in the 0-3 years age group,
make advances in the prevention of malnutrition, eliminate Vitamin A defi ciency, reduce
prevalence of anaemia and iodine defi ciency disorders among women, adolescent girls and
children.
Ensuring implementation and consistent monitoring along with social mobilization across
sectors and within communities is critical to the success of this mission as is the need for
strengthening partnerships between departments and sectors. UNICEF Rajasthan's support
in developing the vision and technical guidance provided has been both valuable and
critical
Eliminating hunger and malnutrition is a vision that is achievable and feasible. Rajasthan
has not only the political will but also the ability to develop plans of action to ensure their
implementation. We dedicate this Mission to the cause of maternal and child health and
pledge to leave no stone unturned in realising the objectives.
(R.K. Meena) (Alka Kala)Principal Secretary Principal Secretary
Deptt of Medical & Health Deptt of Women and Child Development
Message from Principal Secretaries

AWW : Aangan Wadi Worker
AWC : Aangan Wadi Centre
ANM : Auxiliary Nurse-Midwife
ANC : Ante Natal Check-up
ASHA : Accredited Social Health Activist
BPL : Below Poverty Line
CHC : Community Health Centre
CF : Complementary Feeding
EBF : Exclusive Breast Feeding
FRU : First Referral Unit
GDP : Gross Domestic Product
IMR : Infant Mortality Rate
IFA : Iron and Folic Acid
ICDS : Integrated Child Development
Services
IDD : Iodine Defi ciency Disorders
IYCF : Infant and Young Child Feeding
IEC : Information Education
Communication
MCHN : Maternal and Child Health and
Nutrition
MO : Medical Offi cer
NGO : Non-Governmental Organisation
NFHS : National Family Health Survey
NTFP : Non-Timber Forest Produce
NRHM : National Rural Health Mission
ORS : Oral Rehydration Salts
ORT : Oral Rehydration Therapy
PDS : Public Distribution System
PR : Panchayati Raj
PHE : Public Health Engineering
P&LM : Pregnant & Lactating Mother
PRI : Panchayati Raj Institution
PHC : Primary Health Centre
PNC : Post Natal Check-up
RCH : Reproductive and Child Health
RD : Rural Development
SSA : Sarva Shiksha Abhiyan
SHG : Self Help Group
TBA : Trained Birth Attendant
TT : Tetanus Toxoid
WCD : Women and Child Development
List of abbreviations

Contents
Undernutrition – the silent emergency 1
Rajasthan – The indigenous pointers 11
The mission mode – Responding to the emergency 19
Practising the principles 28
Starting right 34
Firm foundations 41
Caring for the care giver 58
Towards a healthy transition 66
Measuring success 71
References 79
Annexures 80
1. Micronutrients – Defi ciencies and sources
2. Health & nutritional status of Rajasthan vs its tribal districts
3. Target population (rural)
4. Global declarations and conventions recognizing the Right to Nutrition
5. Four options of low-cost latrines


1Undernutrition
The silent emergency
The silent emergency
Undernutrition
The crisis of undernutrition is a harsh
reality, with Asia having the largest number
of malnourished children in the world. In
India, undernutrition is fast turning into an
emergency. It is estimated that one in every three malnourished children in the world lives in India1.
The current situation In India, around 46 per cent of all children
below the age of three are too small for their
age, 47 per cent are underweight and at least
16 per cent are wasted. Many of these children
are severely malnourished.2 In comparison,
Rajasthan has a higher percentage of
underweight children at 50.6 per cent while 52
per cent are too small for their age. With respect
to wasting, Rajasthan's record with 11.5 per
cent is better than the national average.
The prevalence of malnutrition varies across
states, with Madhya Pradesh recording the
highest rate (55 per cent), followed closely by
Rajasthan (51 per cent3) and Kerala among the
lowest (27 per cent).4
As a result of the ongoing interventions of the
ICDS, the percentage of underweight children
has come down (4.1 per cent) as also the
percentage of severely malnourished children
(1.7 per cent). What results also indicate is the
need for urgency and acceleration in order to
achieve improved results quickly.
2.40.0
17.9
14.813.2
20.4
27.5
12.8 13.1 13.2
0.02.3
7.15.1
1.7
0.0
5.0
10.0
15.0
20.0
25.0
30.0
UP Maharashtra Rajasthan Tamil Nadu Kerala
BLS ELS % change
Severely malnourished children
Percent of severly malnourished children
(0-36 months) (<3SD)
58.151.8 50.9
39.5
11.33
44.4 42.639.5
35.4
3.513.7 7.839.2 11.44.1
0
10
20
30
40
50
60
70
UP Maharashtra Tamil Nadu Rajasthan Kerala
BLS ELS % chang
State-wise prevalence of underweight children
Percent of underweight children (0-36 months) (<2SD)
All differences statistically signifi cant [p<0.0001]
In Rajasthan, severe and moderate malnutrition
stood at 50.6 per cent of the population (NFHS
II) against the all-India average of 47 per cent.
Between NFHS I (‘92-’93) and NFHS II (‘98-
’99), there has been an approximate 10 per
cent increase in malnutrition. Most of the
malnourished children are in the 7-36 months
age group. Approximately 80 per cent of the
1 ‘The picture in India’ UNICEF, www.unicef.org/india/nutrition2 Ibid3 NFHS II-1998-994 The picture in India’ UNICEF, www.unicef.org/india/nutrition
Chapter 1
Source: ICDS III – Evaluation 1999-2006, Presentation made at National Consultation on Child Under Nutrition and ICDS in India, May 2006

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode2

3Undernutrition
The silent emergency
malnourished children are in grades I and
II and 20 -30 per cent of the malnourished
children are in grades III and IV. What is
worrying is that there is an increasing trend of
growth faltering - even among children in the
normal grade.
Micronutrient defi ciencies among pregnant
and lactating women and adolescent girls
are of serious concern. Major micronutrient
defi ciencies - iron defi ciency anaemia, iodine
defi ciency diseases, and vitamin A defi ciency
- continue to affect adolescent girls and
women, which in turn affect the growth of the
foetus during their pregnancy. This means that
more children are likely to be born as low birth
weight babies, thus starting life with a severe
handicap.
The Tenth Plan states that “more than half the
women and children are anaemic; reduction
in Vitamin-A defi ciency and iodine defi ciency
disorders (IDD) is sub-optimal”.
The overall prevalence of iron defi ciency
anaemia in children between the ages of 6 and
35 months in the country is 77.7 per cent, while
for Rajasthan, it is as high as 82.3 per cent;
half of the adolescent girls and pregnant and
lactating women suffer from iron defi ciency
anaemia.
Under nutrition also contributes to the person's
inability to fi ght infection and disease. The
under nourished child is not only prone to
childhood illnesses, but once affected takes
The 1990 World Summit for Children singled out defi ciencies of three micronutrients — iron, iodine, and vitamin A — as being particularly common and of special concern for children and women in developing countries.
Malnutrition is low (10-30%) until around 6 months and peaks (50-80%) by about 18 months.
Less than 25% of 6-18 month-old children eat half of what is recommended and fall sick once in every three weeks.

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode4
Why children die?
Source: UNICEF
Under nutrition underlies more than half of
child deaths
that much more time to recover and gain from
the twin attack of infection and nutritional
defi ciency.
Causes of undernutrition and micronutrient defi cienciesUndernutrition is not caused simply by
a dissatisfi ed appetite or household food
insecurity (unavailability and inaccessibility of
food).
It is a consequence of a combination of
inadequate dietary intake and disease.
However, there are certain underlying causes
that lead to inadequate dietary intake and
infectious disease. These are insuffi cient access
to food in a household by the female members,
inadequate maternal and child care practices,
poor water and sanitation facilities and
inadequate health services.
The basic causes at societal level are the
quantity and quality of actual economic,
human and organisational resources which
are further infl uenced by political, cultural,
religious, economic and social systems,
including women’s status, and the limit to the
utilisation of potential resources.
While solutions to larger problems of
poverty and the system are long drawn,
there is no doubt that well-planned high-
impact interventions at the community
and family levels can lead to prevention of
under nutrition and in arresting the progress
of undernutrition and protecting the child
and ensuring his/her healthy growth and
development.
Maternal care, both pre-natal and post-natal,
becomes critical to ensure healthy births and
the child's right to survival. It also reduces the
risk of maternal mortality. All-round healthy
growth and development becomes the natural
corollary.
The multi-stage causal framework of
malnutrition (See next page) explains how and
why malnutrition occurs.
Impact of undernutrition and micronutrient defi cienciesUndernutrition causes direct and indirect
losses in productivity and resources. Low birth
weight, iron defi ciency anaemia and iodine
defi ciency are all known to have a profound
effect on a child’s IQ levels and ability to learn
and educational attainment. Malnourished
children also tend to be enrolled late in school
and drop out early.
• GDP losses 2-3 per cent
• Leads to a >10 per cent potential reduction
in lifetime earnings for each malnourished
individual
• Undernutrition (stunting) in early years is
linked to the following:
4.6 cm loss of height in adolescence
0.7 grades loss of schooling
7 month delay in starting school
45%
10%
20%
25%
Neonatal disorders
Pneumonia
Diarrhoea
Others

5Undernutrition
The silent emergency

Malnutrition
Inadequate dietary intake
Disease
Insuffi cient access to food
Inadequate maternal & child care
practices
Poor water/sanitation & inadequate
health services
Quantity and quality of actual resources – human, economic & organizational –
and the way they are controlled
Potential resources: environment, technology, people
Inadequate and/or inappropriate knowledge
and discriminatoryattitudes limit household
access to actual resourcesaccess to actual resources
Political, cultural, religious,economic and social systems,including women’s status, limit
the utilization of potential resources
Conceptual framework of causes of malnutrition
Immediate causes
Outcome
Underlying causes at household/family level
Basic causes at societal level
Source: Adapted from Nutrition Strategy UNICEF
6Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode

7Undernutrition
The silent emergency
Direct loss in productivity from poor
physical status
Indirect loss in productivity from poor cognitive
development and schooling
Loss in resources from increased health care costs
of ill health
Undernutrition
Undernutrition costs India at least $10 billion annually in terms of lost productivity, illness, and death and is seriously retarding improvements in human development and further reduction of childhood mortality.
Direct and indirect losses as a result of undernutrition

8
The information in the following boxes highlights the impact of micronutrient defi ciencies on
women, adolescent girls and children:
Micronutrient defi ciencies
IRON
Impact of defi ciency• Impairs immunity and reduces physical and
mental capacities
• In infants and young children, even in mild form, can impair intellectual development
• In pregnancy is a major cause of maternal mortality, increasing the risk of haemorrhage and sepsis during childbirth
• Infants born to anaemic mothers often suffer from low birthweight and anaemia themselves. Causes include blood loss associated with menstruation and parasitic infections such as hookworm, but an inadequate intake of iron is the main cause.
Who is affected?• Women, pregnant women
• Children under fi ve
Source: The State of the World’s Children, UNICEF 1998
VITAMIN A
Impact of defi ciency• Makes children especially vulnerable to
infection and worsens the course of many infections
• Heightens a child’s risk of dying
• Single-most important cause of blindness among children
Who is affected?• Pre-school-age children
• Women in their reproductive years
Source: The State of the World’s Children, UNICEF 1998
FOLATE
Impact of defi ciency• Causes birth defects in the developing foetus
during the earliest weeks of pregnancy — before most women are aware that they are pregnant
• Has been found to be associated with a high risk of pre-term delivery and low birthweight
• Also contributes to anaemia, especially in pregnant and lactating women
Who is affected?• Women in their reproductive years
• Young children
Source: The State of the World’s Children, UNICEF 1998
IODINE
Impact of defi ciencyImpact of defi ciencyI• Single-most important cause of preventable
brain damage and mental retardation, most of the damage occurring before birth
• Raises the risk of stillbirth and miscarriage for pregnant women
Who is affected?• People in all ages, specifi cally infants and
young children
Source: The State of the World’s Children, UNICEF 1998
(See Annexure 1 for more details on the four micronutrients)
9Undernutrition
The silent emergency
Causes at the household level include intra-
household food distribution, lack of awareness
regarding correct infant and young child
feeding (IYCF) practices and poor hygiene, all of
which call for improved nutrition and child care
practices at the household level.
Why undernutrition persists in many
food-secure households
Inter-generational cycle Poor nutrition perpetuates itself across
generations. Young girls who grow poorly
become stunted women and are more likely to
give birth to low birthweight infants. If those
infants are girls, they are likely to continue the
cycle by being stunted in adulthood, and so
on, if something is not done to break the cycle.
Adolescent pregnancy heightens the risk of
low birthweight and the diffi culty of breaking
the cycle. Support is needed for good nutrition
at all these stages — infancy, childhood,
adolescence and adulthood — especially for
girls and women.
Thus, what is evident is that undernutrition
impacts the morbidity and mortality of young
children before they reach the 12-24 months
age group. It weakens them and makes them
doubly vulnerable to childhood illnesses.
Rajasthan is facing a child survival protection
and growth and development challenge. Of
every 1,000 children born in the state, 115 die
before the age of 5. Of these, 75 die in the fi rst
year and 48 in the fi rst four weeks.
Such wastage of our future generation and slow
deaths is the SILENT EMERGENCY that needs
immediate and urgent attention.
• Pregnant and nursing women eat too few calories and too little protein, or do not get enough rest.
• Mothers have too little time to take care of their young children or themselves during pregnancy because of repeated pregnancies.
• Short birth intervals and low age at marriage cause undernutrition.
• Mothers of newborns discard colostrum, the fi rst milk, which strengthens the child’s immune system.
• Mothers often feed children under age 6 months foods other than breast milk even though exclusive breastfeeding is the best source of nutrients and the best protection against many infectious and chronic diseases.
• Caregivers start introducing complementary solid foods too late.
• Caregivers feed children under age two years too little food, or foods that are not energy dense.
• Though food is available, because of inappropriate household food allocation, women and young children’s needs are not met and their diets often do not contain enough of the right micronutrients or protein.
• Caregivers do not know how to feed children during and following diarrhoea or fever.
• Caregivers’ poor hygiene contaminates food with bacteria or parasites.
Source: Repositioning nutrition as central to development, A strategy for large-scale action, The World Bank, 2006
High impact interventions that ensure timely prevention of
undernutrition and promote sound health and growth and development of the child, the adolescent and the mother in the natural life cycle process
can defi nitely produce positive results
Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode10
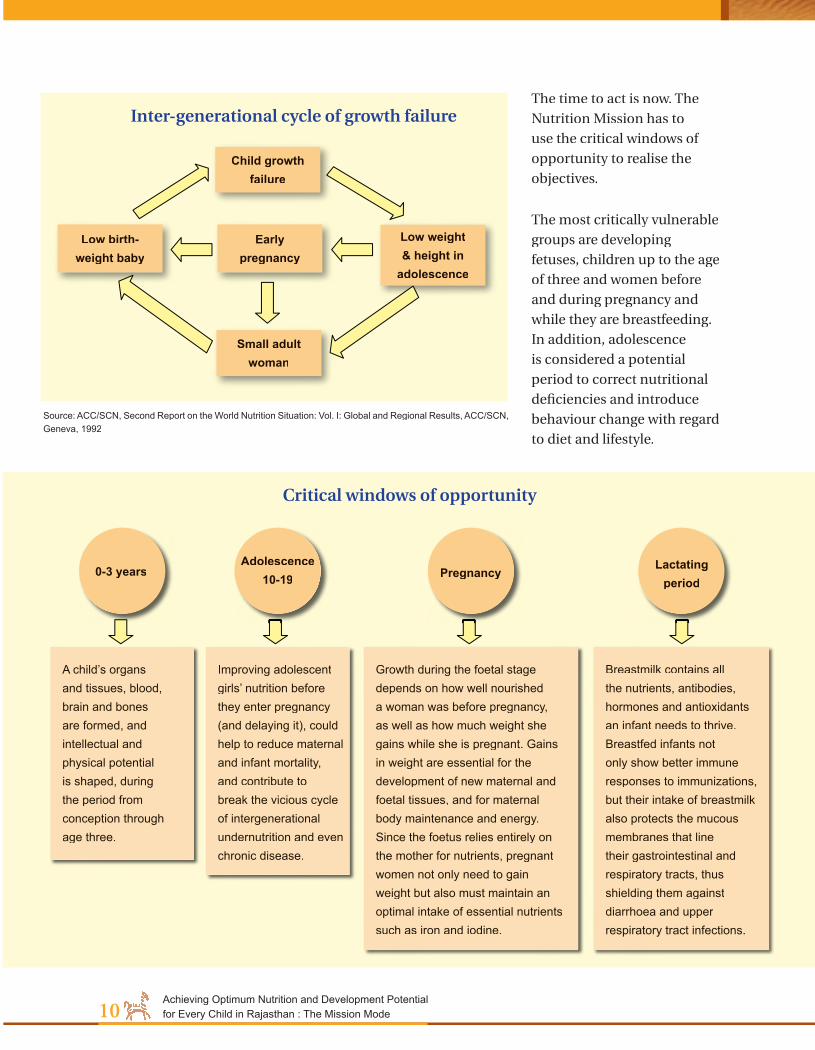
Source: ACC/SCN, Second Report on the World Nutrition Situation: Vol. I: Global and Regional Results, ACC/SCN, Geneva, 1992
Inter-generational cycle of growth failure
Child growth failure
Low weight & height in
adolescence
Early pregnancy
Low birth-weight baby
Small adult woman
A child’s organs and tissues, blood, brain and bones are formed, and intellectual and physical potential is shaped, during the period from conception through age three.
Improving adolescent girls’ nutrition before they enter pregnancy (and delaying it), could help to reduce maternal and infant mortality, and contribute to break the vicious cycle of intergenerational undernutrition and even chronic disease.
Growth during the foetal stage depends on how well nourished a woman was before pregnancy, as well as how much weight she gains while she is pregnant. Gains in weight are essential for the development of new maternal and foetal tissues, and for maternal body maintenance and energy. Since the foetus relies entirely on the mother for nutrients, pregnant women not only need to gain weight but also must maintain an optimal intake of essential nutrients such as iron and iodine.
Breastmilk contains all the nutrients, antibodies, hormones and antioxidants an infant needs to thrive. Breastfed infants not only show better immune responses to immunizations, but their intake of breastmilk also protects the mucous membranes that line their gastrointestinal and respiratory tracts, thus shielding them against diarrhoea and upper respiratory tract infections.
0-3 years Lactating period
PregnancyAdolescence
10-19
The time to act is now. The
Nutrition Mission has to
use the critical windows of
opportunity to realise the
objectives.
The most critically vulnerable
groups are developing
fetuses, children up to the age
of three and women before
and during pregnancy and
while they are breastfeeding.
In addition, adolescence
is considered a potential
period to correct nutritional
defi ciencies and introduce
behaviour change with regard
to diet and lifestyle.
Critical windows of opportunity

11Rajasthan
The indigenous pointers
The indigenous pointers
Rajasthan
The health scenario across the country is
characterised by gender imbalance, low vital
rates and an uneven health care coverage.
Ill-health has a strong correlation to social
variables, in a context where expectant mothers
and girl children are neglected, and women
as a cohort are more vulnerable to diseases
that affl ict the population in general. There
is a general consensus that the health and
nutritional status is the worst among the tribal
population owing to distinct health problems,
mainly governed by multi-dimensional factors
like their habitat, diffi cult terrain, ecologically
variable niches, illiteracy, poverty, livelihood
insecurities, isolation, superstition and
deforestation. These factors make them doubly
vulnerable to disease and undernutrition.
As per Census 2001, Scheduled Tribes account
for approximately 12.6 per cent of the
entire population of Rajasthan. The highest
concentration is noticed in Banswara and
Dungarpur districts where their proportion to
total population of the districts comes to 73.47
per cent and 65.84 per cent, respectively. Other
districts with higher proportion are Udaipur
(46.34%), Sirohi (23.39%), Sawai Madhopur
(22.47%), Bundi (20.25%), Chittorgarh (20.28%)
and Baran (21.13%).
According to the Fifth Schedule of the
Constitution of India, Banswara and Dungarpur
are declared as fully tribal districts and Udaipur,
Chittorgarh and Sirohi as partly tribal.
The prominent Scheduled Tribes are the
Bhils and the Meenas. The Bhils are mostly
concentrated in the hill-locked districts of
Udaipur, Dungarpur and Banswara while
the Meenas are settled mainly in the Jaipur,
Sawai Madhopur and Udaipur districts. Other
Scheduled Tribes are the Garasias and the
Sahariyas. The Garasias are concentrated in the
Pali and Sirohi districts while the Sahariyas are
limited to a pocket of two tehsils in the Kota
district. The most underdeveloped tribal groups
are the Sahariya and the Kathodi. Only 5 percent
of these groups is literate, and they are grossly
underemployed.
Largely due to poverty and heavy burden of
debt, tribals of these districts have failed to
Scheduled Tribes in Rajasthan
Chapter 2
1. Bhil, Bhil Garasia, Dholi Bhil, Dungri Bhil, Dungri Garasia, Mewasi Bhil, Rawal Bhil, Tadvi Bhil, Bhagalia, Bhilala, Pawra, Vasava, Vasave
2. Bhil Mina
3. Damor, Damaria
4. Dhanka, Tadvi, Tetaria, Valvi
5. Garasia (excluding Rajput Garasia)
6. Kathodi, Katkari, Dhor Kathodi, Dhor Katkari, Son Kathodi, Son Katkari
7. Kokna, Kokni, Kukna
8. Koli Dhor, Tokre koli, Kolcha, Kolgha
9. Mina
10. Naikda, Nayaka, Cholivala Nayaka, Kapadia Nayaka, Mota Nayaka, Nana Nayak
11. Patelia
12. Seharia, Sehria, Sahariya
Source: Constitution of India

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode12
optimally use the resources at their disposal
and continue to remain poor.
Several factors contribute to the tribals’
inequitable access and poor status in terms of
health care and nutrition. These include lack
of awareness and social barriers preventing
the utilisation of available health and nutrition
supplementation programme and services,
poor environmental sanitation and lack of safe
drinking water, leading to increased morbidity
from water-borne infections, environmental
conditions that favour vector borne, diseases,
lack of access to health care facilities resulting
in increased severity and/or duration of
illnesses.
The tribal population is largely faced by a
diffi cult and diverse physiography, ranging
from desert and semi-arid to hilly tribal tracts.
Frequent occurrence of droughts coupled with
these geographical barriers has translated
into poor health status for the tribes who
are confi ned to the deserts, forests and hills,
making timely treatment unattainable.
A very large majority of the tribals are engaged
in agriculture; their other economic activities
being food gathering (including hunting),
forestland cultivation, minor forest produce
collection, pastoral and handicrafts. Forests
are an important source of livelihood for the
poor in Rajasthan, and approximately 5 million
TRIBALS Poor accessibility & utilisation of health services
Diffi cult terrain and
sparsely distributed tribal population
in forests and hilly regionsregions
Locational Locational disadvantage
of sub-centres, PHCs, CHCs
Non availability of
service providers due to vacant
posts and lack of residential facilities
Non involvement of the local
traditional faith healers
Lack of suitable Lack of suitable transport facility
for quick referral of emergency cases
Services not being client
friendly in terms of timing, cultural barriers inhibiting
utilization
Inadequate mobilization
of NGOs
IEC activities not tuned to the tribal idioms, beliefs and
practices
Weak monitoring
and supervision systems
mobilization
Lack of integration
with other health programs and
other development sectors

13Rajasthan
The indigenous pointers
tribal people derive seasonal incomes through
the collection, processing, transportation
and marketing of non-timber forest produce
(NTFP). Forests are traditionally a source of
subsistence and livelihoods for the tribals and
are often their only source of fuel wood and
fodder. Animal husbandry is another important
source of livelihood, specially for the poor. The
tribals are also nomadic herders of sheep and
camel.
The tribal’s right to basic resources such
as land, forest and water and their entire
environment have been seriously eroded. Not
only is the landscape changing with the large-
scale soil erosion, making it uncultivable,
water sources are also drying up as a result
of the depletion of forests. The tribals with
their lack of skills are faced with serious
livelihood issues. The tribal-dominated
districts of Udaipur, Dungarpur, Dholpur
and Chittorgarh have the largest incidence of
under-employment. Migration is one of the
mechanisms that help them cope with
poverty.
Water and sanitationWater is a crucial determinant of nutritional
status. Rajasthan is defi cient in water (surface
and ground). Ground water at many places is
unfi t for human and livestock consumption.
Water-borne diseases, especially diarrhoea and
jaundice, are among the frequently occurring
diseases among tribal children.
High concentrations of fl uoride occurring
naturally in groundwater have caused widespread
fl uorosis - a serious bone disease - among local
populations. The districts of Tonk, Sirohi and
Rajsamand are among the worst affected.
Most of the households (85 per cent) in rural
Rajasthan use no latrine and more than than
Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode14
half (57 per cent) had no drainage while 32 per
cent had only kuccha drainage that leads to
widespread clogged, overfl owing and broken
drains. Lack of good drainage is another source
contributing to water-borne diseases. The
coverage of rural areas under sanitation and
hygiene education (under the Total Sanitation
Campaign) is only 14 per cent as per Census
2001.
Food patternsThe main food crops of the state are bajra,
wheat, rice and pulses. The main non-food
crops are oilseeds, pulses and vegetables and
spices.
The district-wise comparison of average food
consumption shows variations. Banswara,
Dungarpur, Chittaurgarh, Rajsmand and Alwar
are districts with inadequate nutrient intake of
50 per cent and higher, with the tribal district
of Dungarpur being inadequate in intake of
cereals, pulses, green leafy vegetables, toots
and tubers, other vegetables, milk and milk
products, fats and oils and sugar. Consumption
of pulses, green leafy vegetables, other
vegetables and sugar are the lowest in the 13
predominantly tribal districts. In a basically
vegetarian state, the low consumption of
pulses, vegetables, sugar and fruits has resulted
in low intake of energy, iron, ribofl avin and
vitamins C and A.
The lifestyles and food habits of the tribals are
different from that of their rural neighbours.
They depend on minor forest produce,
are employed in manual labour and often
do not have adequate income. Their food
consumption pattern is dependent on the
vagaries of nature and varies from extreme
deprivation (in the lean seasons) to high intakes
(in the post harvest period).

15Rajasthan
The indigenous pointers
IMR Districts
<60 per 1000 live births Ganganagar, Hanumangarh, Bikaner, Jhunjhunu, Sikar
60-90 per 1000 live births Churu, Alwar, Bharatpur, Dholpur, Karauli, Sawai Madhopur, Dausa, Jaipur, Nagaur, Jodhpur, Jaisalmer, Barmer, Jalor, Sirohi, Ajmer, Bundi, Kota, Baran, Jhalawar
>90 per 1000 live births Pali, Bhilwara, Rajsamand, Udaipur, Dungarpur, Banswara, Chittorgarh, Tonk
[Source: UNICEF]
Child careInfant mortality rate, which is a parameter
of the society’s ability to provide care for the
children, is high at 94.7 for tribal populations,
while in Rajasthan as a whole too, it fi gures at
97.3. A major proportion (38 per cent) of under-
5 deaths among Scheduled Tribes takes place in
the fi rst year of birth.
The nutritional status of tribal children
in Rajasthan between the ages of 6 and
35 months indicates that 59 per cent are
underweight (Rajasthan 50.6 per cent), 60
per cent are stunted (Rajasthan 52 per cent)
and 17.6 per cent are wasted (11.7 per cent).
It is no surprise that 80.2 per cent of the tribal
children were found to be anaemic (Rajasthan
82.3 per cent). Twenty-one per cent of the
children were suffering from acute respiratory
illnesses out of which only 50 per cent were
taken to a health facility or provider. Twenty-
seven per cent were found suffering from
fever, and out of the 23 per cent suffering from
diarrhoea, nearly 40 per cent were not taken Source: NFHS II 1998-988
Infant & child mortality among STs of Rajasthan
22%
15%
38%
25%
0%
Neonatal
Post-neonatal
IMR
Child mortality
Under 5 mortality
Infant & child mortality among STs of Rajasthan
Infant mortality in districts

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode16
to any health provider or facility. Only 32.7 per
cent of the mothers were found to know about
ORS (Source: NFHS II).
All the districts that show an IMR of >90 per
1000 live births are tribal-dominated except
Pali and Bhilwara, and none of the districts
with an IMR of <60 per 1000 live births are
tribal.
In the tribal dominated districts (see table on
previous page), in the month of October 2005,
incidence of total malnutrition was found to
be 50 percent or more. The total numbers of
children suffering from severe malnutrition in
these districts were as high as 700 and 786 in
Banswara and Udaipur, respectively, and 1,074
and 1,227 in Jhalawar and Baran, respectively.
Eight out of the 13 districts recorded more than
20 deaths each, with Alwar, Chittorgarh and
Udaipur recording deaths as high as 43, 55 and
60, respectively.
Malnutrition in tribal-dominated districts
Tribal-dominated
districts
Total malnutrition* (%)
Moderate & severe
malnutrition** (%)
Total no. of children in
Grades III & IV
Total deaths in 0-5 age group
Dungarpur 59.20 22.17 20 17Banswara 64.38 33.59 700 32Udaipur 63.74 27.45 786 60Chittorgarh 61.93 24.70 517 55Sirohi 60.31 24.24 13 0Sawai Madhopur 62.12 28.00 29 11Jodhpur 50.08 19.11 155 1Baran 60.46 27.64 1227 37Rajsamand 49.24 19.40 15 30Alwar 52.91 21.76 521 43Dholpur 54.72 21.76 402 37Tonk 51.49 22.78 355 14Jhalawar 50.46 22.44 1074 24
Source: ICDS data, October 2005, DWCD, Govt of Rajasthan

17Rajasthan
The indigenous pointers
Lack of care and timely treatment, especially
at the household level, and in acute cases, at
the institutional level, is a major cause of non-
recovery or delayed recovery.
Infant and young child feeding practices in
tribal Rajasthan further throws light on the
poor nutritional status of children. Only 3.7
per cent of the infants were initiated into
breastfeeding within an hour of birth and 27.2
per cent within a day. More appalling is the
fact that colostrum feeding is unpopular and
73.8 per cent of the children were initiated into
breastfeeding after squeezing the fi rst breast
milk.
Adolescent Adolescent girls face more problems than boys,
largely due to socio-cultural factors. Adolescent
girls are deprived of adequate health care,
good nutrition and opportunity for schooling.
Stunted and underweight anaemic girls with
inadequate knowledge of personal care, family
planning or child rearing practices enter into
marriage and motherhood, thus perpetuating
the problems of malnutrition and poverty on to
the coming generation.
The prevalence of iron defi ciency anaemia too
is widespread among tribal adolescent girls.
Maternal care The quality of maternal care is most evident
from the data collected regarding institutional
deliveries, pre-natal and post-natal check-
ups , IFA consumption and TT injections. In
Rajasthan, of every 1,00,000 live births, 670
maternal deaths take place. Among the tribal
population, 58.4 per cent of women in the
reproductive age were found to be anaemic.
Only 15.8 per cent had delivered at a medical
institution. Deliveries assisted by a trained
doctor or a nurse/midwife were slightly higher
at 23.9 per cent though not much. Only 35.8
per cent had received IFA and 42.1 per cent
administered with TT injections. More than half
the tribal mothers and pregnant women (57.9
per cent) had received no ante-natal check-
19
How the probability of underweight increasesfor girls in increasingly vulnerable positions
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ris
k ca
tego
ry
Probabability of under we ight
Girl ST girl ST girl in poorest quintile ST girl in poorest quintile in rural area
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Probability of under weight
Girl ST girls in poorest quintile ST girls in poorest quintile Girl ST girls in poorest quintile ST girls in poorest quintile Girl ST girls in poorest quintile ST girls in poorest quintile
How the probability of underweight increases for
girls in increasingly vulnerable positions

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode18
This is the time to act to end child hunger and
undernutrition.
ups and only 4.7 per cent had received a post-
partum check-up within 2 months of birth.
(It is important to note that out of the 52.5 per
cent of the women who received no ante-natal
check-up, 68.6 per cent cited the reason for not
having received the same as “Not necessary”.)
While it is critical to recognise the challenges
faced in delivering services to tribal
communities, it is equally important to
understand that traditional practices and ways
of living and healing exist and these need to be
appropriately taken into account in order to
adopt sustainable solutions.
(See Annexure 1 for comparative information
on the health and nutrition status of Rajasthan
and its tribal districts.)

19The Mission Mode
Responding to the emergency
Responding to the emergency
The Mission Mode
The nutritional status of the tribal population
of Rajasthan can be improved only through
the adoption of the Mission mode. This move
is initiated by the Department of Women &
Child Development, Government of Rajasthan,
and would involve the active support and
participation of other departments.
Why the ‘Mission Mode’?
because … … the malnutrition crisis in Rajasthan is fast
turning into an emergency
… the interventions need to move on a fast
track
… only well-planned and time-bound efforts
bear fruit
… focus, coordination and convergence
– essential elements of a Mission - are the
pillars of quality service delivery
Objectives of the MissionThe Nutrition Mission would aim to attain the
following by 2011:
With respect to children Reduce prevalence of under-nutrition in 0-6
year-olds
Reduce prevalence specifi cally under the age
of 3 by 60 per cent (from 51 per cent to 30
per cent)
Reduce severe undernutrition in children
below 6 years (weight for age)
Reduce severe undernutrition in children
below 3 years to less than 5 per cent
Reduce prevalence of anaemia in children
below 6 years by 50 per cent of existing level
Eliminate Vitamin A defi ciency as a public
health problem among children in 0-6 years
age group
With respect to adolescent girls Reduce prevalence of anaemia among
adolescent girls by 50 per cent of existing level
Empower adolescent girls with life skills
education
Chapter 3
Article 47 of the Constitution of India states that “the State shall regard raising the level of nutrition and standard of living of its people and improvement in
public health among its primary duties”.
India is among the 191 nations that are committed to achieving the Millennium Development Goals (MDGs), which are the world’s time-bound and quantifi ed targets for dramatically reducing extreme poverty in its many dimensions by 2015 – income poverty, hunger, disease, exclusion, lack of infrastructure and shelter – while promoting gender equality, education, health, and environmental sustainability. The eight MDGs include reduction of child mortality (Goal 5: Reduce under-fi ve mortality rate by two-thirds between 1990 and 2015) and improvement in maternal health (Goal 6: Reduce the maternal mortality ratio by three-quarters between 1990 and 2015). The importance of achieving these goals in Rajasthan gains signifi cance as the state is among the four states (the other three being Madhya Pradesh, Uttar Pradesh and Bihar) that account for more than 50 per cent of infant mortality in India.
Millennium Development Goals:
Child and Maternal Care
Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode20
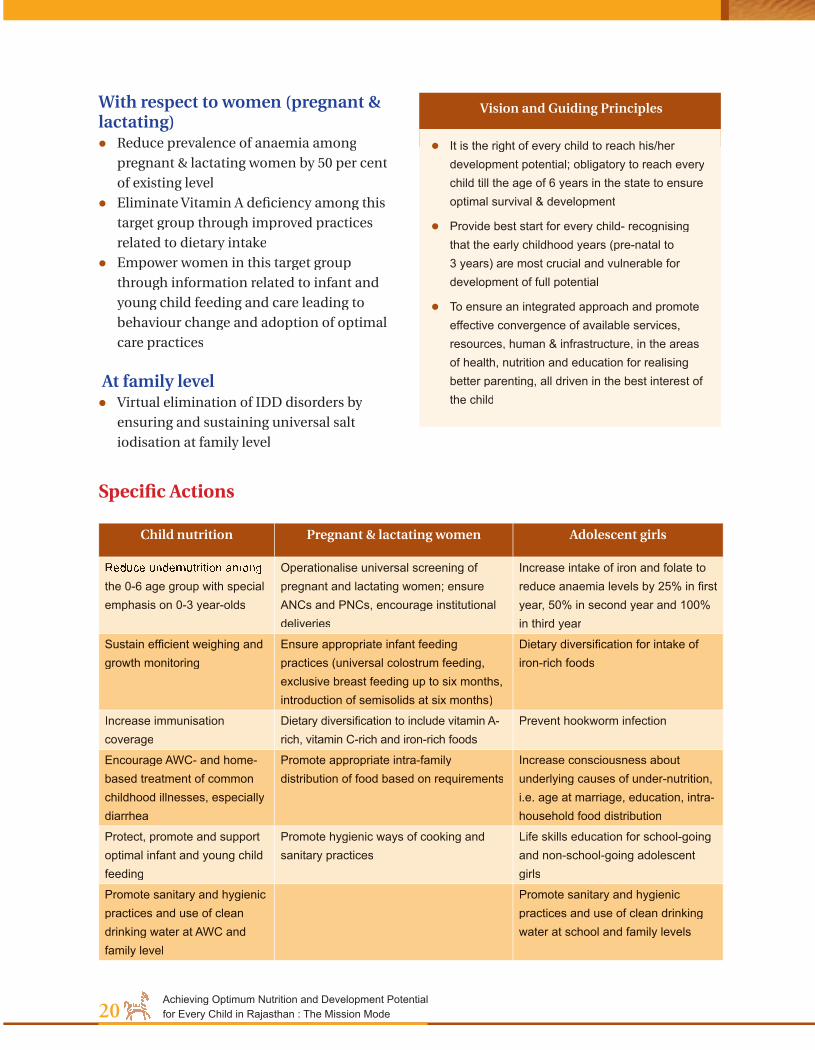
With respect to women (pregnant & lactating) Reduce prevalence of anaemia among
pregnant & lactating women by 50 per cent
of existing level
Eliminate Vitamin A defi ciency among this
target group through improved practices
related to dietary intake
Empower women in this target group
through information related to infant and
young child feeding and care leading to
behaviour change and adoption of optimal
care practices
At family level Virtual elimination of IDD disorders by
ensuring and sustaining universal salt
iodisation at family level
It is the right of every child to reach his/her development potential; obligatory to reach every child till the age of 6 years in the state to ensure optimal survival & development
Provide best start for every child- recognising that the early childhood years (pre-natal to 3 years) are most crucial and vulnerable for development of full potential
To ensure an integrated approach and promote effective convergence of available services, resources, human & infrastructure, in the areas of health, nutrition and education for realising better parenting, all driven in the best interest of the child
Vision and Guiding Principles
Specifi c Actions
Child nutrition Pregnant & lactating women Adolescent girls
Reduce undernutrition among the 0-6 age group with special emphasis on 0-3 year-olds
Operationalise universal screening of pregnant and lactating women; ensure ANCs and PNCs, encourage institutional deliveries
Increase intake of iron and folate to reduce anaemia levels by 25% in fi rst year, 50% in second year and 100% in third year
Sustain effi cient weighing and growth monitoring
Ensure appropriate infant feeding practices (universal colostrum feeding, exclusive breast feeding up to six months, introduction of semisolids at six months)
Dietary diversifi cation for intake of iron-rich foods
Increase immunisation coverage
Dietary diversifi cation to include vitamin A-rich, vitamin C-rich and iron-rich foods
Prevent hookworm infection
Encourage AWC- and home-based treatment of common childhood illnesses, especially diarrhea
Promote appropriate intra-family distribution of food based on requirements
Increase consciousness about underlying causes of under-nutrition, i.e. age at marriage, education, intra-household food distribution
Protect, promote and support optimal infant and young child feeding
Promote hygienic ways of cooking and sanitary practices
Life skills education for school-going and non-school-going adolescent girls
Promote sanitary and hygienic practices and use of clean drinking water at AWC and family level
Promote sanitary and hygienic practices and use of clean drinking water at school and family levels

21The Mission Mode
Responding to the emergency
Time Line The Mission would comprise three phases. The
fi rst phase would begin in 2006 and cover 6
tribal districts (Dungarpur, Banswara, Udaipur,
Chittorgarh, Sirohi and Dholpur) and 7 non-
tribal districts (Jodhpur, Baran, Rajsamand,
Alwar, Sawai Madhopur, Tonk, Jhalawar).
UNICEF is already supporting 7 of the 13 Phase
1 districts through its programme Aanchal se
aangan tak. The second phase would succeed
a year later, in 2007, in which 9 districts would
be included followed by Phase 3 districts in year
2008 to cover the remaining 10 districts of the
state.
Phase 1 Beginning 2006
Phase 2 Beginning 2007
Phase 3 Beginning 2008
Reorientation to targetingSo far, there has been a tendency to target
children between 3 and 6 years as it is
associated with SNP and pre-school education.
Children below 3 years are only targeted
through mothers who happen to be registered
with the AWC. Under the Mission, there would
be a consious reorientation of targeting to
cover the under-3 children. The Mission
will, therefore, give priority to screening all
children from birth to 3 years to ascertain levels
of undernutrition and in a systematic and
planned manner target those who are most
vulnerable.
Target populationThe Mission would aim to achieve its objectives
by targeting the rural population in the critical
age groups, namely the following:
1. Children in the 0-6 years age group with
special focus on 0-3 year-olds
2. Adolescent girls (10-19 year-olds)
3. Pregnant and lactating women
Under 4 Adolescent girls Women Total
Phase 1 2272051 1686692 2980508 6939251
Phase 2 1636890 1243303 2133158 5013351
Phase 3 1923819 1549035 2562105 6034959
Total 5832760 4479030 7675771 17987561
Source: Census 2001
The Mission would target an estimated population of 17,987,561 women, girls and
children in the 0-6 age group.

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode22
Coverage1
*Districts that will receive special focus from the Govt of Rajasthan**UNICEF-supported districts that will continue to receive support from the agency
(See Annexure 3 for district-wise fi gures)
Phase 1
Dungarpur/*Dungarpur/*Dungarpur/*Dungarpur/*Dungarpur/*
Sirohi*Sirohi*Sirohi*Sirohi*Sirohi*Sirohi*
Sawai Madhopur*Sawai Madhopur*Sawai Madhopur*Sawai Madhopur*
Jodhpur** Dhaulpur**Dhaulpur**Dhaulpur**Dhaulpur**Dhaulpur**
S.No. District01. Dungarpur*02. Banswara*03. Udaipur*04. Chittorgarh*05. Sirohi*06. Sawai Madhopur*07. Jodhpur**08. Baran**09. Rajsamand**10. Alwar**11. Dhaulpur**12. Tonk**13. Jhalawar**
Dungarpur/*Dungarpur/*Dungarpur/*Dungarpur/*Dungarpur/*
Target PopulationWomen– 29,80,508Adolescent girls – 16,86,6920-4 – 2272051
1 These fi gures refer to Census 2001. They are being provided only as an estimation of the population that would need to be covered. The fi gures pertain to the rural population only. Adolescent population consists of the population in the 10-19 age group. 'Women' here refers to females in the 20-49 age group. While the Mission will target 0-6 year-olds, fi gures for 0-4 year-olds have been provided.

23The Mission Mode
Responding to the emergency
(See Annexure 3 for district-wise fi gures)
Coverage1
Phase 2
(See Annexure 3 for district-wise fi gures)
Coverage1
1 These fi gures refer to Census 2001. They are being provided only as an estimation of the population that would need to be covered. The fi gures pertain to the rural population only. Adolescent population consists of the population in the 10-19 age group. 'Women' here refers to females in the 20-49 age group. While the Mission will target 0-6 year-olds, fi gures for 0-4 year-olds have been provided.
GanganagarGanganagarGanganagarGanganagar
Jaisalmer
HanumangarhHanumangarhHanumangarhHanumangarh
KarauliKarauliKarauliKarauliKarauliKarauli
BharatpurBharatpurBharatpur
S.No. District01. Nagour02. Pali03. Bhilwara04. Kota05. Barmer06. Jaisalmer07. Jalore08. Bikaner09. Ganganagar
Target PopulationWomen– 21,33,158Adolescent girls – 12,43,3030-4 – 16,36,890
S.No. District01. Hanumangarh02. Dausa03. Jaipur04. Bharatpur05. Ajmer06. Bundi07. Karauli08. Jhunjhunu09. Sikar10. Churu
Phase 3
Target PopulationWomen– 25,62,105
Adolescent girls– 15,49,0350-4– 19,23,819

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode24
Nutrition MissionInter-departmental
convergence
Women & Child
Development
Women &
DevelopmentDevelopment
Medical &health
Ground water
Nutrition Mission
water
Agriculture
Food
Civil
Supplies
Civil
Supplies
EducationEducationInformation & Public Relations
Medical &
Tribal
Area
DevelopmentDevelopment
Information Public Health
Engineering
Inter-departmental convergence in the Mission
Public Health
Salt Commissioner
Salt
Rural
Development
& Panchayati
Raj
ConvergenceThe Mission would involve
the active participation of all
concerned departments of the
Government of Rajasthan. The
determinants of malnutrition, as
we have seen in Chapter 1, include
not just food but also health, water
and sanitation, which imply that
the concerned departments need
to contribute in several ways. several ways. several
Inter-departmental convergence
would be organized in the Mission
in terms of offi cials’ roles and
responsibilities, functionaries,
infrastructure and objectives.
For this, prior agreements would
be made between departments
right from the policy level
to the grassroots in order to
operationalize the convergence on
the fi eld for interventions.
An agreement with ongoing
Missions and schemes/
programmes is necessary as
in each Mission, manpower,
infrastructure and other
resources are being put to use
towards an end. Where there
is convergence of purpose, it
proves to be more benefi cial and
constructive to cross-utilize these
resources. (See illustrations)
Tribal area programmes and
specifi c schemes and institutional
services that are already in place
must be strengthened in tribal
areas, such as public distribution
system, iodised salt distribution
and the employment guarantee
scheme.
Nutrition Mission
RCH IIRCH IITotal
Sanitation campaign
Swajaldhara
National Adolescent Girls
ProgrammeAdolescent Girls
Mid-day meal/ school
lunch
Bharat Nirman
Kishori Shakti Yojna
Nirman
PDS
EmploymentGuaranteeSchemeScheme
Iodised Salt Distribution
meal/ school Iodised Salt Distribution
Tribal Area Development
Inter-scheme convergence in Mission
National Rural Health
MissionRural Health
NutritionMission
Inter-mission convergence

25The Mission Mode
Responding to the emergency
With the objective of ensuring intake of clean water and healthy sanitary practices, while the Dept of WCD would ensure that the AWC staff at the village level is engaged in the transfer of information to women and adolescent girls regarding the importance of safe drinking water and washing hands after defecation and before cooking and eating, the Dept of Medical & Health functionary Sahayogini would spread awareness about water-borne diseases and ways of management at household level and the critical time for referral. The district and block level offi cials of the Public Health Engineering and Panchayati Raj & Rural Development Depts would ensure that all wells, hand pumps, taps and toilets are repaired and maintained. Ground Water Dept would ensure that supply of water is adequate and also oversee the quality of water.
Messages: ‘Drink safe water’, ‘Wash your hands’
Example of Convergence
Sahayogini
AWW
PHEDept.
Panchayati Raj & Rural Develop-
ment Dept.
Tribal Area
Develop-ment Dept.
Ground Water Dept.
Departments that will ensure repair and maintenance of infrastructure for water supply and toilets, supply of water, awareness about clean drinking water, sanitation, hygiene and prevention of water-borne diseases
Drink safe water.
Wash your hands.
Medical & Health Dept.

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode26
Some examples of convergenceThe following example illustrates an area of
a fruitful convergence between the National
Rural Health Mission (in particular, the Janani
Suraksha Yojana) and the Nutrition Mission
in order to achieve the objective of ensuring
safe and healthy pregnancy, delivery and
motherhood.
Note: In Rajasthan, the roles of Sahayogini and ASHA (an NRHM functionary) have been merged, and the Sahayogini is expected to fulfi ll the role of the ASHA.
Ensuring safe and healthy pregnancy,
delivery and motherhood
National Rural Health Mission
Janani Suraksha Yojna Early registration
Early identifi cation of complicated cases
3 ANC & post-delivery visits
Referral and referral transport assistance to Sahayogini and pregnant woman to go to nearest health centre
24/7 delivery services at PHC level providing basic obstetric care
FRUs providing emergency obstetric care
Cash assistance to mother for enabling institutional delivery
Assistance for Caesarean Section
Compensation payment for tubectomy/laparoscopy
Nutrition Mission
Village-level Community-driven mapping of pregnant
and lactating women (weighing, updating & maintenance of records
Door-to-door micronutrient supplementation
Identifi cation of cheap, locally available nutritious foods and demonstrations of nutritive cooking on MCHN Day
Consumption of one nutritious, wholesome meal every day at AWC
Homestead production of vegetables
Support group for employed pregnant & lactating women
Breastfeeding support groups
Cluster counselling on complementary feeding
IEC activities
Fathers' groups
Mothers' groups
Community-based volunteer
teams
Sahayogini
ANM
AWW
Village Health
Committee

27The Mission Mode
Responding to the emergency
Inter-departmental convergence with the
objective of ensuring food security among
adolescent girls and pregnant and lactating
women is illustrated below, wherein the active
involvement of each department is seen as
imperative towards the desired end.
Ensuring food security
Depts of Panchayati Raj & RD and Food and Civil Supplies Ensuring that each BPL family owns a
ration card
Ensuring smooth functioning of and supply at the PDS shop
Local PDS shop
Targeted PDS (10 kg food grain)
Antyodaya Anna Yojana (35 kg food grain)
Aanganwadi Centre
Supplementary Nutrition Programme
National Adolescent Girls Scheme (35 kg food grain for those weighing <35kg)weighing <35kg)
Dept. of Food & Dept. of Food & Civil SuppliesCivil Supplies
Dept. of Women and Dept. of Women and Child DevelopmentChild Development
Depts of Panchayati Raj & Rural Depts of Panchayati Raj & Rural Depts of Panchayati Raj & Rural Development, Food & Civil SuppliesDevelopment, Food & Civil SuppliesDevelopment, Food & Civil Supplies
Inter-departmental convergence to ensure food security to adolescent girls

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode28
Practising the PrinciplesKey approaches & core interventions
Central to the approaches adopted by the
Nutrition Mission is the increased and
maximum interface between the service
provider and the household/family. While the
service provider would ensure the availability
and access to resources and services, the
family would take on increased responsibility
for maternal and child care and thus support
proper utilization of the services.
In every phase of the Mission and through
each intervention, it would embody the
above illustrated principle and display
improved service delivery in all sectors and
institutions involved, increased interaction
between functionaries of all service providing
institutions and the family, improved
accessibility and a system of monitoring
wherein the community and the institutions
are involved, thus leading to transparency and
shared analysis and learning from successes as
well as failures.
Service provider Capacity building on
management of child malnutrition
Use of standard protocols Quality services
FamilyEmpowerment
Involvement of both parents for signifi cant improvement in caring practices
Institutions Political commitment Mobilisation of resources Policy implementation
(targeted PDS; NREG & food fortifi cation)
Rights-basedGender equity
Life cycle
Behaviour change communication
Community-driven, participatory Community
Ownership Local initiative Community-based monitoring Mobilisation for better targeting,
food security
I. Key approachesThe Mission attempts to base its strategies and
interventions on key principles that would pave
Chapter 4

29Practising the Principles
Key approaches & core interventions
the way for achieving several overarching goals,
such as
gender equity,
recognition of people's right to nutrition,
breaking the intergenerational cycle of
growth failure and
community ownership of essential services
and programmes.
The Mission acknowledges the ongoing
involvement and roles of institutions, families,
service providers and communities and
endeavours to synergize existing programmes
and encourage creative initiatives.
a. Rights-basedFreedom from hunger and malnutrition is
a basic human right and their alleviation is
a fundamental prerequisite for human and
national development.
National and state governments, in their
policies, are obliged to promote nutrition
actions and reduce diet-related diseases. They
should do this within the context of respecting,
protecting and fulfi lling the right to adequate
food, and should ensure that these actions are
adequately funded.
The Nutrition Mission, an initiative of the
State government recognizes this right of every
individual, even the most marginalized of all,
and endeavours to empower communities
and families to protect their nutrition, human
rights and entitlements and those of their
Constitution of Food and Nutrition Council in 1997 – On its recommendations, a proposal on National Nutrition Mission, set up under the Prime Minister, was developed with a view to address the problem of malnutrition in a Mission Modeapproach
c. Life cycleGood nutrition is needed for all stages of
life — infancy, childhood, adolescence and
adulthood — especially for girls and women.
When these malnourished children do not
eat well and fall ill frequently, they grow up
to be malnourished adolescent girls who
in turn, in their adulthood, give birth to
babies who are born with low birth weight
and are micronutrient-defi cient. In this way,
malnutrition passes from one generation to
another and becomes a vicious cycle.
children, through knowledge, skills, policies
and regulations.
(See Annexure 4 for key global declarations
and conventions that recognize the Right to
Nutrition)
b. Gender equityInequities in access to and control of assets
have severe consequences for women’s ability
to provide food, care and health and sanitation
services to themselves, their husbands, and
their children, especially their female
children.
Intra-household food distribution has been
recognized as a key cause of nutritional
gender inequity. Even though the primary
burden of the household and the primary
care-giving responsibility of the family is
the woman’s, she is placed in a position that
often fails to address her own nutritional
requirements.
This Mission endeavors to introduce
operationally effective interventions, including
gender-sensitive nutrition education and
involving men and adolescent boys, to improve
the nutrition status of adolescent girls and
pregnant women.
Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode30
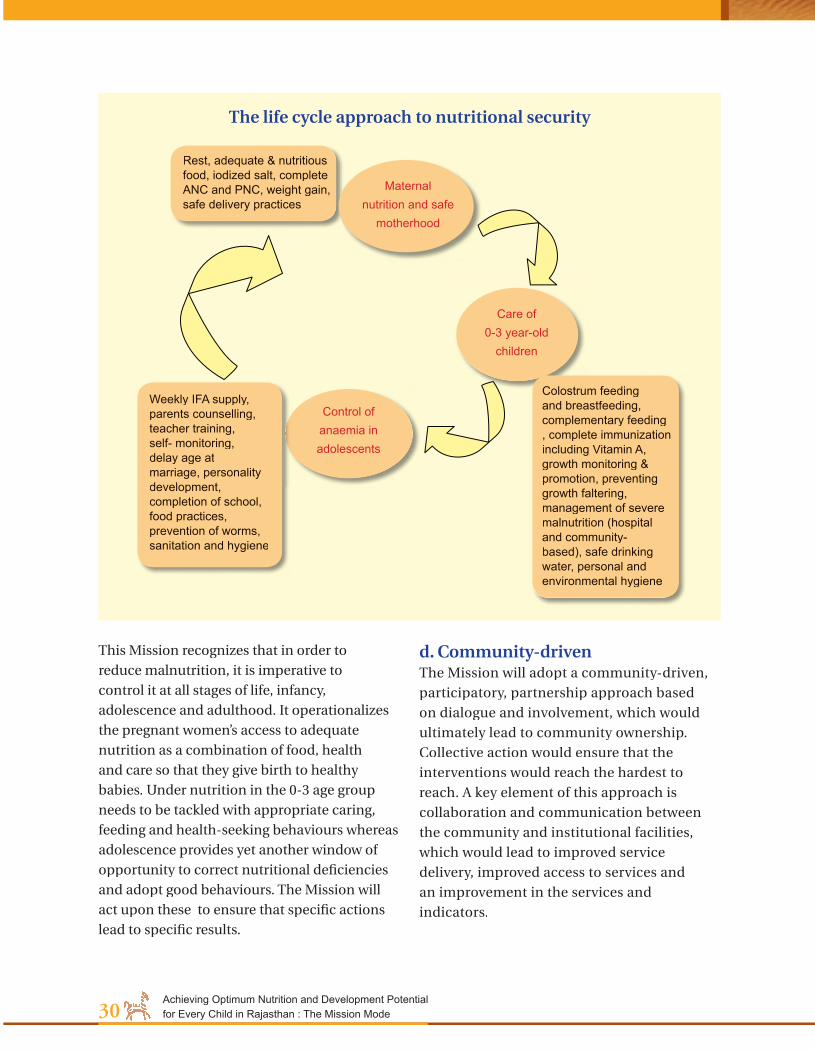
This Mission recognizes that in order to
reduce malnutrition, it is imperative to
control it at all stages of life, infancy,
adolescence and adulthood. It operationalizes
the pregnant women’s access to adequate
nutrition as a combination of food, health
and care so that they give birth to healthy
babies. Under nutrition in the 0-3 age group
needs to be tackled with appropriate caring,
feeding and health-seeking behaviours whereas
adolescence provides yet another window of
opportunity to correct nutritional defi ciencies
and adopt good behaviours. The Mission will
act upon these to ensure that specifi c actions
lead to specifi c results.
Rest, adequate & nutritious food, iodized salt, complete ANC and PNC, weight gain, safe delivery practices
Maternal nutrition and safe
motherhood
Care of 0-3 year-old
children
Control of anaemia in adolescents
Colostrum feeding and breastfeeding, complementary feeding , complete immunization including Vitamin A, growth monitoring & promotion, preventing growth faltering, management of severe malnutrition (hospital and community-based), safe drinking water, personal and environmental hygiene
Weekly IFA supply, parents counselling, teacher training, self- monitoring, delay age at marriage, personality development, completion of school, food practices, prevention of worms, sanitation and hygiene
The life cycle approach to nutritional security
d. Community-drivenThe Mission will adopt a community-driven,
participatory, partnership approach based
on dialogue and involvement, which would
ultimately lead to community ownership.
Collective action would ensure that the
interventions would reach the hardest to
reach. A key element of this approach is
collaboration and communication between
the community and institutional facilities,
which would lead to improved service
delivery, improved access to services and
an improvement in the services and
indicators.

31Practising the Principles
Key approaches & core interventions
Promotion of positive behaviour Promotion and sustaining of individual, community and societal behaviour change Maintenance of appropriate behaviours
Community& Family
Support
groups
Counselling &
home visits
Social mobilisation
& IEC activities
Folk theatre
Positive deviants
The approach would:
address needs identifi ed by community
build on the strengths and resources of the
community
recognise the community as unit of identity
with common interests, shared values and
Community mobilisation
Formation of community-based volunteer teams
Training of volunteer teams
Planning together
Action
Evaluating together The
community-driven,
participatory approach
Community-driven participatory approach
Effecting behaviour change
norms and a commitment to meeting shared
needs
promote local knowledge and practices and
bridge cultural gaps
e. Behaviour change communicationBehaviour change communication is an
interactive process with communities (as
integrated with an overall program) to
develop tailored messages and approaches
using a variety of communication channels
to develop positive behaviours; promote and
sustain individual, community and societal
behaviour change; and maintain appropriate
behaviours.
In this Mission, communication strategies will
address not only individual behaviour change
of the mother and the adolescent girl, but also
the beliefs of those who infl uence them at all
levels: health workers, family members, elders
and community members.
Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode32
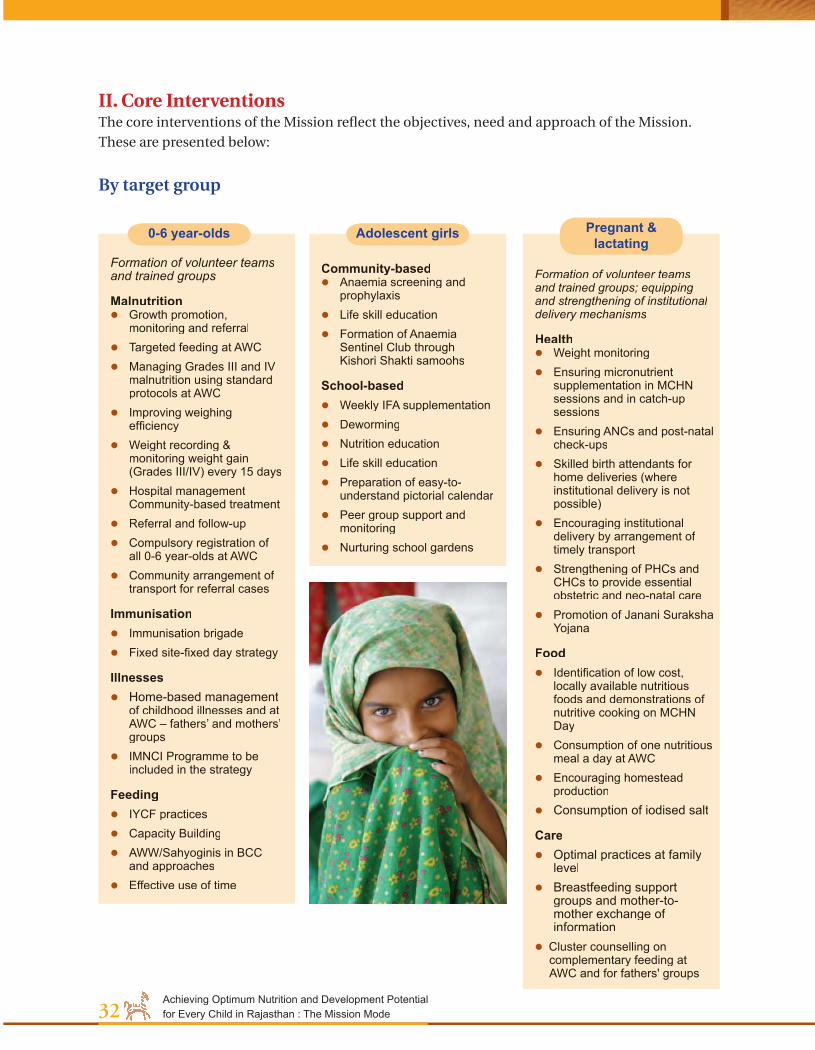
II. Core Interventions The core interventions of the Mission refl ect the objectives, need and approach of the Mission.
These are presented below:
By target group
Formation of volunteer teams and trained groups
Malnutrition Growth promotion,
monitoring and referral Targeted feeding at AWC Managing Grades III and IV
malnutrition using standard protocols at AWC
Improving weighing effi ciency
Weight recording & monitoring weight gain (Grades III/IV) every 15 days
Hospital management Community-based treatment
Referral and follow-up Compulsory registration of
all 0-6 year-olds at AWC Community arrangement of
transport for referral cases
Immunisation Immunisation brigade Fixed site-fi xed day strategy
Illnesses Home-based management
of childhood illnesses and at AWC – fathers’ and mothers’ groups
IMNCI Programme to be included in the strategy
Feeding IYCF practices Capacity Building AWW/Sahyoginis in BCC
and approaches Effective use of time
Community-based Anaemia screening and
prophylaxis Life skill education Formation of Anaemia
Sentinel Club through Kishori Shakti samoohs
School-based Weekly IFA supplementation Deworming Nutrition education Life skill education Preparation of easy-to-
understand pictorial calendar Peer group support and
monitoring Nurturing school gardens
Formation of volunteer teams and trained groups; equipping and strengthening of institutional delivery mechanisms
Health Weight monitoring Ensuring micronutrient
supplementation in MCHN sessions and in catch-up sessions
Ensuring ANCs and post-natal check-ups
Skilled birth attendants for home deliveries (where institutional delivery is not possible)
Encouraging institutional delivery by arrangement of timely transport
Strengthening of PHCs and CHCs to provide essential obstetric and neo-natal care
Promotion of Janani Suraksha Yojana
Food Identifi cation of low cost,
locally available nutritious foods and demonstrations of nutritive cooking on MCHN Day
Consumption of one nutritious meal a day at AWC
Encouraging homestead production
Consumption of iodised salt
Care Optimal practices at family
level Breastfeeding support
groups and mother-to-mother exchange of information
Cluster counselling on complementary feeding at AWC and for fathers' groups
0-6 year-olds Adolescent girls Pregnant & lactating

33Practising the Principles
Key approaches & core interventions
Establishment of cooperative grain banks
Homestead gardening
Revisiting households to ensure that each BPL family owns a ration card
Management of PDS by women's groups
Ensure optimal utilisation of employment and food security schemes
Capacity building and technical support in rain water harvesting/conservation, artifi cial recharge
Promoting use of low-cost latrines (1 for a family)
Communication and education to health workers, families and community on hand-washing, drinking water, hygienic cooking and practices
Distribution of low cost water fi lters (in areas with excess fl uoride in ground water)
Ensuring execution of all works falling under Swajaldhara and Total Sanitation Campaign
Promoting key child care behaviours through community IMNCI
Malnutrition Treatment Centres at CHCs
Improved and well planned home visits for counselling and behaviour change
Strengthening quality of organisation of MCHN days with focus on unreached
Establishing and equipping mini aanganwadi centres for far-fl ung hamlets
Ensuring safe drinking water and sanitation in schools
Life skill education for school and non-school going adolescent girls
Exploring possibilities for nutrition supplementation for out of school adolescent girls
Water & sanitationHealth Food securityEducation
By malnutrition determinant (common for all target groups)

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode34
Starting rightThe Nutrition Mission would function with
the village as the basic unit where all key
interventions would be executed. To facilitate
smooth functioning of the Mission and to
ensure timely monitoring and corrective on-
course action, a fi ve-tiered implementation
structure is proposed.
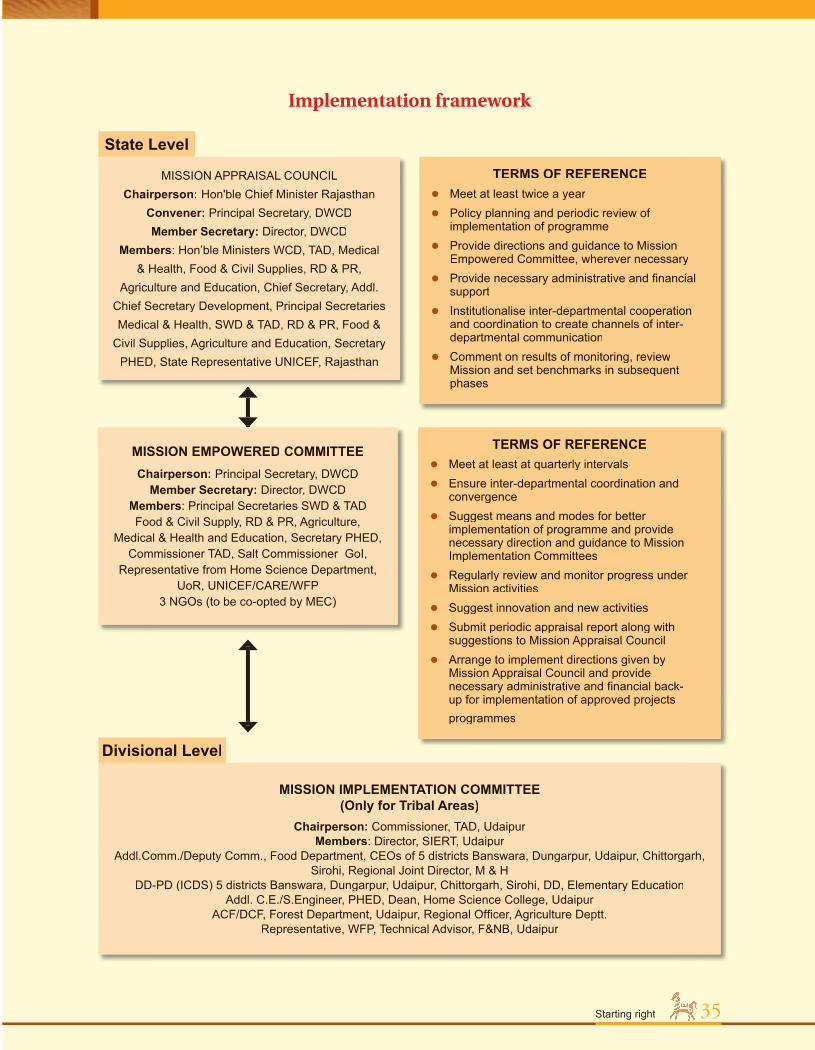
Implementation StructureThe Mission would function through a fi ve-
tiered implementation structure, with a
state-level Mission Appraisal Council headed
by the Honourable Chief Minister. This
body would comprise Ministers, Principal
Secretaries of concerned departments and
UNICEF State Representative along with
Director, DWCD. There would also be a
Mission Empowered Committee at the state-
level headed by Principal Secretary, DWCD
and be constituted by Principal Secretaries
of concerned departments, Secretary PHED,
Commissioner Tribal Area Development,
UNICEF representatives, etc.
At the divisional level, there would be a
Mission Implementation Committee only for
tribal areas headed by Commissioner, TAD,
Udaipur. At the district level, a Mission Review
Committee would be headed by the District
Collector followed by Mission Implementation
Committees at the block and village levels,
which would be chaired by the Pradhan of the
concerned Panchayat Samiti and the Gram
Sarpanch, respectively. The terms of reference
for each of these tiers are provided in the
following pages.
Chapter 5
35
TERMS OF REFERENCE Meet at least twice a year Policy planning and periodic review of
implementation of programme Provide directions and guidance to Mission
Empowered Committee, wherever necessary Provide necessary administrative and fi nancial
support Institutionalise inter-departmental cooperation
and coordination to create channels of inter-departmental communication
Comment on results of monitoring, review Mission and set benchmarks in subsequent phases
MISSION APPRAISAL COUNCILChairperson: Hon'ble Chief Minister Rajasthan
Convener: Principal Secretary, DWCDMember Secretary: Director, DWCD
Members: Hon’ble Ministers WCD, TAD, Medical & Health, Food & Civil Supplies, RD & PR,
Agriculture and Education, Chief Secretary, Addl. Chief Secretary Development, Principal Secretaries Medical & Health, SWD & TAD, RD & PR, Food &
Civil Supplies, Agriculture and Education, Secretary PHED, State Representative UNICEF, Rajasthan
MISSION EMPOWERED COMMITTEEChairperson: Principal Secretary, DWCD
Member Secretary: Director, DWCDMembers: Principal Secretaries SWD & TADFood & Civil Supply, RD & PR, Agriculture,
Medical & Health and Education, Secretary PHED, Commissioner TAD, Salt Commissioner GoI,
Representative from Home Science Department, UoR, UNICEF/CARE/WFP
3 NGOs (to be co-opted by MEC)
State Level
Implementation framework
TERMS OF REFERENCE Meet at least at quarterly intervals Ensure inter-departmental coordination and
convergence Suggest means and modes for better
implementation of programme and provide necessary direction and guidance to Mission Implementation Committees
Regularly review and monitor progress under Mission activities
Suggest innovation and new activities Submit periodic appraisal report along with
suggestions to Mission Appraisal Council Arrange to implement directions given by
Mission Appraisal Council and provide necessary administrative and fi nancial back-up for implementation of approved projects programmes
MISSION IMPLEMENTATION COMMITTEE (Only for Tribal Areas)
Chairperson: Commissioner, TAD, Udaipur Members: Director, SIERT, Udaipur
Addl.Comm./Deputy Comm., Food Department, CEOs of 5 districts Banswara, Dungarpur, Udaipur, Chittorgarh, Sirohi, Regional Joint Director, M & H
DD-PD (ICDS) 5 districts Banswara, Dungarpur, Udaipur, Chittorgarh, Sirohi, DD, Elementary EducationAddl. C.E./S.Engineer, PHED, Dean, Home Science College, Udaipur
ACF/DCF, Forest Department, Udaipur, Regional Offi cer, Agriculture Deptt.Representative, WFP, Technical Advisor, F&NB, Udaipur
Divisional Level
35Starting right

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode36
MISSION REVIEW COMMITTEE Chairperson: District Collector
Member Secretary: DD-PD (ICDS)Members: District-level Offi cers of Line
Departments, Unicef Representative, 2 NGOs
District Level
MISSION IMPLEMENTATION COMMITTEE Chairperson: Pradhan, Panchayat Samiti
concernedMember Secretary: CDPO
Members: BDO, BEO, AEN PHED, Medical Offi cer CHC, Medical Offi cer Incharge PHCs, Enforcement
Inspector, Asst. Agriculture Offi cer Local NGO
Block Level
MISSION REVIEW COMMITTEE Chairperson: Gram Sarpanch
Member Secretary: Secretary PanchayatMembers: Supervisor WCD, ANM, HM
Primary School, Patwari, AWW, Sahayogini, Manager Gram Seva Sahkari Samiti, Social worker/NGO (Depending upon availability),
Gram Sevak
Village Level
TERMS OF REFERENCE Meet once in two months
Make available requirements specifi ed by block-level committee
Analyse data collected and present fi ndings before the state-level offi cials
TERMS OF REFERENCE Meet once in a month
Ensure community participation
Collect data and analyse at block level
Oversee programme implementation in block and suggest modifi cations, if any, for better implementation
TERMS OF REFERENCE Meet once in a month
Discuss operational diffi culties and suggest remedial course of action to block-level implementation committee
Undertake sole responsibility for operationalisation of Mission at grassroots level
Identify/track benefi ciaries for various services
Make available/select various functionaries at grassroots
Regularly inspect AWCs and guide AWW/Sahayogini to improve service delivery

37Starting right
Nodal agency The Dept of Women and Child Development
would be the nodal agency that would
Dept of Medical & Health
Dept of Public Health Engineering
Dept of Tribal Area Development Dept of
Information & PR
Dept of RD &Panchayati Raj
Salt Commissioner
Dept of Food
Dept of Civil SuppliesDept of
Education
Dept of Agriculture
Dept of Ground Water
Village level
State Level
Network Network
CoordinateCoordinate
Organise Organise
IntegrateIntegrate
District
Block level
Divisional N
odal
age
ncy
DW
CD
level
level
coordinate all activities among the identifi ed
departments at the state, district, block and
village levels of the Mission.
Role of nodal agency DWCD

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode38
The launchThe Mission would be launched with a
week-long massive Information-Education-
Communication (IEC) drive in order to ensure
social mobilisation.
Each of the 13 districts will be required to
develop extensive and detailed plans for
implementation of the Mission. A task force
would be set up at the district level involving all
the stakeholders, including departments, active
NGOs, Tribal Council representatives, etc.
Micro-level Action PlansThe Mission recognises the fact that a single
formula for all districts and regions within the
state would not produce the desired change.
Micro-level action plans would be developed by
taking into account the geographical conditions
of the area in focus (hilly, desert etc) and other
area-specifi c factors that infl uence the health
and nutritional status the population. These
micro-level interventions would also need to be
esigned keeping in mind the locally available
resources and ways to maximize their use.
In terms of health and illnesses, illnesses
occurring frequently in those regions would
need to be combated by reviewing the causal
factors. Similarly, appropriate locally available
food would need to be included in the
nutritional diet rather than transporting food
products from far-off markets.
For e.g., with respect to water availability
and quality, the micro-level planning would
incorporate ways of lessening the drudgery
of fetching water from distant sources by
encouraging the revival of traditional systems
of water harvesting (repairing and recharging
of baoris, johads) and water conservation
at the domestic and community levels etc
and ensuring that the water is fi t for human
consumption.
Nutrition Awareness Week
Objectives Spreading the message of the importance of nutrition
Informing about nutritional status of tribal people
Enlisting volunteers for the community-based teams
Key messagesEnsuring healthy children is in our handsCommunities, government and civil society have to work together to ensure thisNutrition care starts before birth and with special attention for children up to 3 yearsThe malnutrition status of the tribal peoples is an emergency. Urgent community-based steps need to be taken.
Key activities Prabhat Pheri involving school children and Nehru Yuvak Kendra Youth
Promotion of local foods through Melas promoting nutritious food cooked at home using locally available items
Health camp for pregnant/nursing women, adolescent girls and children below 3 years
Awareness-raising on hygiene, hand-washing, washing of food items and utensils, clean drinking water
Film shows of the Food and Nutrition Board
Promotional drives on TV, radio, local newspapers and any other local medium of communication
The driving force The Information & Publicity Relations department
would play a key role during this IEC drive.
PRIs at all levels, NGOs, voluntary organizations, youth organizations, school children and teachers, anganwadi functionaries, health workers religious leaders, women workers, etc.

39Starting right
Formation of volunteer teamsDuring the awareness week, Gram Sabha
meetings would be held during which selection
of volunteers would take place and where
the community will actively discuss and
decide on suitable volunteers, the role and
functions of these volunteers, time allocation,
compensation, etc. When volunteers are
selected in this participatory manner, the
community too would appreciate their
efforts and there would be an affi rmation of
the self esteem of volunteers. The leader of
each volunteer team will liaise with the Chief
Executive of the Block Programme Committee.
Capacity building of volunteer teamsAn essential part of the Mission is to impart
training or build capacities of the volunteer
teams. The Mission recommends that in each
village, specifi c teams for specifi c activities are
formed. This would have to be planned and
conducted in a time-bound manner as well as
in stages. The training for all villages in a district
could be conducted in groups, covering a cluster
of villages at convenient spots where training
would be conducive. The volunteers would have
to be brought together from the cluster for about
two days at a time for capacity building.
Preparatory tasks at district and block levels
1. Creating a common understanding about the Mission
2. Orientation and information communication about Mission goals, target populations, sectoral interventions and activities, time-bound results with district- and block-level staff of concerned departments
3. Clearly defi ne roles & responsibilities and tasks related to specifi c interventions
4. Communicate clear objectives and set clear guidelines for all district and block level offi cials of the concerned departments
5. Inform about District-level Review Meetings – once a month for the fi rst six months, once in 3 months subsequently – and the village-level, block level Mission Representatives who will attend these
6. Identifi cation of focal persons within community
7. Rapid assessment of facilities and infrastructure
8. Upgrade infrastructure wherever required – AWCs, PHCs, (For e.g, AWCs to have adequate space, functional weighing machine and other facilities for all activities envisaged, repairing weighing machines )
Preparatory tasks at village level1. Identifi cation of focal persons at village level
2. Identifi cation of persons for volunteer teams
3. Formation of volunteer teams
4. Creating a common understanding among volunteer teams about the Mission, about their role, and the importance of nutrition mapping
5. Capacity building of volunteer teams, on nutrition, IYCF and care, growth monitoring, message transmission, etc

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode40
Understanding nutrition situation among children,
targeted women and adolescents
Learning to conduct participatory exercises for situation analysis of nutrition status
How and what to measure and how to documentUse of simple pictorial monitoring formats
Understanding how to monitor nutrition status through effective growth monitoring and
motivate for optimal practices
IYCF and care ; management of childhood illnesses, especially diarrhoea
Pregnancy and carePreventing anaemia among adolescents
Understanding how to assist in the organisation and
management of health days
Understanding how to plan for community actions - vegetable gardens, water protection,
managing PDS, etc
Capacity building needs for volunteer teams are
suggested below in the fl ow chart:
Understanding how to identify malnourished children and care for them (home management
& referral)
Understanding Mission goals and activities and expected results
Helping villagers help themselvesHaving undergone capacity building in
the areas mentioned in the fl ow chart
above, the community-based volunteer
teams would have acquired information
and skills regarding growth monitoring of
0-6 year-olds and weighing of pregnant
women, care of severely malnourished
children, detection and management (at
community level) of childhood illnesses,
intake and distribution of IFA (women
and adolescents, IYCF practices, healthy
sanitary practices etc.

41Firm foundations
Reducing malnutrition in 0-6 year-olds
Reducing malnutrition in 0-6 year-olds
Firm foundations
Fundamental ObjectiveTo reduce the prevalence of malnutrition
among 0-6 year-old children, with special
focus on 0-3 year-olds, of the Scheduled Tribe
community, and usher in a healthy, disease-free
childhood
Specifi c Goals1. Reduce undernutrition among the 0-6 age
group with special emphasis on 0-3 year-
olds
2. Sustain effi cient weighing and growth
monitoring
3. Increase immunisation coverage
4. Encourage AWC- and home-based treatment
of common childhood illnesses, especially
diarrhoea
5. Protect, promote and support optimal infant
and young child feeding
6. Promote sanitary and hygienic practices
and use of clean drinking water at AWC and
family level
Strategic Interventions
Malnutrition mapping of children in village 1. Growth monitoring of all children in the 0-6
age group by AWW, Sahayogini and Growth
Monitoring Volunteers through home visits
2. Maintenance of village malnutrition record (sex-wise, age-wise, grade-wise) by Growth
Monitoring Volunteer team
Related tasks:
Sharing of information with concerned
families and in health committee meetings
and decisions taken to rectify situations
Chapter 6

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode42
Tasks during home visits (focussing on 0-3 year-olds)a. Nutritional counselling to family
b. Home-based care, advice, support
c. Recording immunisation coverage, types and frequency of other illnesses, such as diarrhoea
d. Categorising the children by malnutrition grades
e. Care of pregnant and lactating women
Recording of weight of all children in 0-6 age group
Plotting of weight on growth chart by AWW, ANM, Growth Monitoring Volunteers
Determine whether or not child is suffering from any grade of malnutrition or has evidence of growth faltering
Normal weight without growth
Grade I
Grade II
Growth faltering
Grades III, IV
Identifi cation of malnourished children in village
Motivating families whose children are
faltering and/or are not in normal grade
Encouraging families whose children are
doing well to maintain positive growth
Planning for information sharing
3. Preparation and monthly updating of Child Nutrition Map of village and associating
households having children by malnutrition
grade by colour (red – grade IV, light blue
– grade III, dark blue – grade II, light green
– grade I, dark green – normal)
Outcomes of home visits are to be shared with
ANM on her monthly/immunisation visits and
if referral is critical, information is to be made
available to the ANM.

43Firm foundations
Reducing malnutrition in 0-6 year-olds
1 Management of severe malnutrition: A manual for physicians and other senior health workers, World Health Organization, Geneva, 1999
I. Management of Grades III and IVChildren falling in grades III and IV are
severely malnourished. Timely and effective
interventions combined with efforts to prevent
further growth failure are crucial for these
children. Successful management of the
severely malnourished child does not require
sophisticated facilities and equipment or highly
qualifi ed personnel. It does, however, require
that each child be treated with proper care and
affection, and that each phase of treatment be
carried out properly by appropriately trained
and dedicated health workers. When this is
done, the risk of death can be substantially
reduced and the opportunity for full recovery
greatly improved1.
1. ANM ReferralIn order to assess how the severely
malnourished child is to be taken care of,
the ANM has to determine (after assessing
symptoms) whether the child can be managed
by the family/AWC level or needs to be referred
to the PHC/CHC/FRU

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode44
Clinical assessment by ANM to be made to determine whether or not the severely malnourished child needs hospital care or community-based care
Once the assessment is made for each of
those children who are severely malnourished
- the management details will have to be
communicated to the concerned families. This
will be done by the ANM with volunteer team
and AWW. The latter will take responsibility
for ensuring follow-up action and volunteer
team will facilitate family to organise if hospital
management is necessary.
Recording of weight of all children in 0-6 age group
Plotting of weight on growth chart by AWW, ANM, Growth Monitoring Volunteers
Determine whether or not child is suffering from any grade of malnutrition or has evidence of growth faltering
Normal weight without growth
Grade I
Grade II
Growth faltering
Grades III, IV
Aangan Wadi Centre/Community
PHC/CHC/FRU
Nutritional status of child:
Grades III & IVTAKE CHILD TO
Grade assessment of children in 0-6 years age group

45Firm foundations
Reducing malnutrition in 0-6 year-olds
Phases Actions Principles
Phase 1 Initial treatment Life threatening problems identifi ed; treated in hospital or community; specifi c defi ciencies corrected; metabolic abnormalities reversed; feeding begun
Treat or prevent thypoglycemia and hypothermia;
Treat or prevent dehydration and restore electrolyte balance;
Treat incipient or developed septic shock, if present;
Start to feed the child; Treat infection; Identify and treat any other problems,
including vitamin defi ciency, severe anemia and heart failure.
Phase 2 Rehabilitation Intensive feeding given to recover most of the lost weight; emotional and physical stimulation increased; mother or carer trained to continue care at home; preparations made for discharge of the child
Encourage the child to eat as much as possible;
Re-initiate and/or encourage breastfeeding as necessary;
Stimulate emotional and physical development; and
Prepare the mother or carer to continue to look after the child after discharge.
Phase 3 Follow-up After discharge, child and family followed to prevent relapse and assure continued physical, mental and emotional development of child
Phases in Management of Severe MalnutritionManagement of the child with severe
malnutrition is divided into three phases. It is
important for all stakeholders - the family, the
AWW and the volunteer team - to understand
and assimilate this. In case the child is referred
to the hospital at the district level, the family
would be assisted by the community, the AWW,
the ANM and the volunteer team.

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode46
2 a. Hospital Management
Primary health centre/Community health centre/District hospital
DAY CARECondition: Presence of infection Child is conscious Accepting oral feed
INPATIENT CARECondition: Listless Presence of severe infection (fever,
diarrhoea, blood in stools, chest drawn in) Child is conscious Accepting oral feed
1. Supervised feeding2. Treatment of infection 1. Supervised feeding
2. Treatment of infection3. Progress monitoring
Follow-up care at AWC
2b. Management at Aangan Wadi Centre/Community-based careIn order to effect successful intervention, the
AWCs need to be equipped to manage severely
malnourished children in terms of the skills
of the functionaries and necessary equipment
and medical supplies. Once the severely
malnourished child is identifi ed, targeted
feeding would begin at the AWC coupled with
monthly prognosis on a fortnightly basis. If
the child is found to not gain weight at the rate
of at least 10 gm per kg (body weight) per day,
she/he would be referred to the PHC or CHC
or the fi rst referral unit. However, if the child
is found to make progress, feeding care at
the family level would follow which would be
supervised by the Sahayogini.
Skill building of the AWW and Sahayogini
through on-the-job training in order to carry
out this intervention effectively is extremely
important for the Mission. Supervision of the
AWW would be conducted at the block level
through the Block Programme Committee (see
Implementation Framework in Chapter 5).
3. Establishing support system for families of children referred to PHC/CHC/FRU in the
event of the primary caregiver in the family
needing to accompany the malnourished child
Counselling to the family for need to take
malnourished child to PHC/CHC/FRU
Children to be taken in groups using a
common vehicle
1 Referral Volunteer per group to accompany
the group
Management at AWW/Community-based care

47Firm foundations
Reducing malnutrition in 0-6 year-olds
Targeted feeding at the Aangan Wadi Centre – minimum 2 feeds
Fortnightly weight recording Visit by Sahayogini for supervised active feeding
at home Maintain warmth by covering the child in
multiplayer with head caps and socks or advice about kangaroo care
Put the child on antibiotics (Cotrimaxazol) for 7 days
Give one course of Mebendazol or Albendazol beyond 2 years
Increase the number of usual feeds and add ghee/oil 1 to 2 tablespoonfuls a day
Continue feeding during illness give supplementary feeding and reinforce correct feeding practice
If the child does not revisit AWC, Referral Volunteer will bring the child to the AWC
Equip AWCs for management of
severely malnourished children
Begin targeted feeding at AWC
Monitor prognosis on fortnightly basis (weight
gain @ 10 gm/kg body weight per day
If yes, continue community-based
care
If no (within 2 weeks)refer to PHC/CHC/FRU
Feeding care at home; supervision
by Sahayogini
Management at AWC/Community-based care
IMPORTANTFrequent causes of failure to
respondProblems with the treatment facility: Poor environment for malnourished children
Insuffi cient or inadequately trained staff
Inaccurate weighing machines
Food prepared or given incorrectly
Problems of individual children: Insuffi cient food given
Vitamin or mineral defi ciency
Malabsorption of nutrients
Rumination
Infections, especially diarrhoea, dysentery, otitis media, pneumonia, tuberculosis, urinary tract infection, malaria, intestinal helminthiasis and HIV/AIDS
Serious underlying disease
Source: ‘Management of Severe Malnutrition – A Manual for Physicians and Other Senior Health Workers’, World Health Organization, 1999

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode48
Normal weight without faltering
Grades I and II
Growth faltering as per established criteria
Praise mother/caregiver
Emphasise on EBF up to 6 months
Complementary feeding at 6 months & reinforce correct feeding practices through nutritional counselling
Advice to continue feeding Advice to continue feeding during illness
Advice on immunization, Advice on immunization, vitamin A supplement and IFA tablet (small)
Advice revisit or ask her Advice revisit or ask her to report early in case of illness
If child does not come for revisit, Sahayogini/AWW/Growth monitoring Volunteer to bring child to centre
Sensory stimulation
Enquire about any illness/alteration of feeding practices
Increase no. of usual feeds and add ghee/oil 1 to 2 tablespoonfuls a day
Continue feeding during illness, give supplementary feeding as per norms and reinforce correct feeding practice
Give advice on immunisation, vitamin A supplement and IFA tablets (small)
Advice revisit or ask her Advice revisit or ask her to report early in case of illness
If child does not come for revisit, Sahayogini/AWW/Growth monitoring Volunteer to bring child to centre
In case of children in Grade II, monitor closely for downward trend
Sensory stimulation
Enquire about any illness/alteration of feeding practices
Increase no. of usual feeds and add ghee/oil 1 to 2 tablespoonfuls a day
Continue feeding during illness, give supplementary feeding as per norms and reinforce correct feeding practice
Give advice on immunisation, vitamin A supplement and IFA tablets (small)
Advice revisit or ask her Advice revisit or ask her to report early in case of illness
If child does not come for revisit, Sahayogini/AWW/Growth monitoring Volunteer to bring child to centre
In case of improve-ment, continue family/community-based care
In case of no improvement, refer to
health facility
Pointer cards to be given to volunteer teams:
Each volunteer team will be given simple
instructions on cards as part of capacity
building to deal with growth monitoring results.
Supporting families

49Firm foundations
Reducing malnutrition in 0-6 year-olds
II. Registration of all births and community-based care of new-born
Register births in the village
Record birth weight
Normal > 2500 gm 2000-2500 gm < 2000 gm
Home care Community management by
preventing: hypothermia hypoglycaemia avoiding infection
Refer newborn to FRU/CHC/PHC
Action to be taken: Feeding colostrum; - Exclusive breastfeeding; - No bathing
for 7 days; - Keeping baby by the side of mother StabilizedNot
stabilized
Action to be taken: Feeding colostrum Exclusive breastfeeding No bathing for 7 days Keeping baby by the side of mother Less handling of baby
Refer to apex institution
Under the Mission, each village volunteer
team will ensure registration of births and
community-based care of the new-born. This
aspect has to be given utmost attention as one-
third of the babies that are born have low birth
weight.
Registration and care of new born

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode50
III. Compulsory registration of all 0-3 year-olds at AWC & optimal utilisation of servicesAs the newborn is followed up closely up to the
fi rst year and thereafter up to 3 years of age, it
is of utmost importance that the family avails
the services at the AWC for the child. The AWW,
therefore, has to inform and make the family
understand the method and signifi cance of the
following:
Monthly weighing and growth monitoring
Immunisation schedule
Danger signs of illness
Importance of adopting hygienic practices
IIIa. Immunisation of all children in the 0-6 age group to be undertaken by /ANM and AWW during growth monitoring visitsGrowth monitoring team and volunteer group
for immunization will communicate the
messages of timely vaccinations through the
use of songs in local dialect
The schedule for immunisation that is provided
in the Mamta card has to be followed as shown
under.
Schedule for 0-3 year-olds' immunisation
YEAR 1 YEAR 2 YEAR 3
Month 1
Month 2 BCG, DPT, Polio
Month 3 DPT
Polio
Month 4 DPT, Polio
Month 5
Month 6 DPT,
Polio,
Vitamin A
Vitamin A
Month 7
Month 8
Month 9 Vitamin A,
Measles
Month 10
Month 11
Month 12 Vitamin A Vitamin A
All mothers need to be motivated to come to
the centre for immunisation at fi xed times.
The volunteer team for growth monitoring
and immunisation needs to inform mothers
accordingly.
In families with severely malnourished or
those in rehabilitation phase have to be
immunised at home. For this, the ANM/
Sahayogini and AWW would need to plan the
home visits.
The volunteer team has to make a list of absent
children so that they too can be covered by the
ANM when the round of home visits are being
planned.
III b. Infant and Young Child Feeding The growth rate in the life of human beings
is maximum during the fi rst year of life
and infant feeding practices comprising
breastfeeding and complementary feeding
plays a major role in determining the

51Firm foundations
Reducing malnutrition in 0-6 year-olds
0-6 month-old 6-36 month-old
Colostrum feeding and exclusive breastfeeding
Preparing for timely and proper initiation of complementary foods
Proper initiation of complementary food Start with small amounts of mashed
cereal, dal, vegetables, fruits
Increase quantity, frequency and thickness of foods gradually
Understand child’s signals for hunger and respond accordingly
Sit with child and feed her/him
Infant and young child feeding
nutritional status of the child. Optimal infant
and young child feeding practices include six
months of exclusive breastfeeding, continued
breastfeeding for two years or beyond,
timely, adequate, safe and appropriate
complementary foods and feeding starting
after six months, and related support for
maternal health, nutrition and birth spacing.
III.c Celebrating a healthy, safe and well-nourished motherhood and childhood: Maternal and Child Health & Nutrition Day (MCHN Day)The Maternal and Child Health and Nutrition
Day is an activity wherein convergence
between the departments of WCD and Medical
& Health is taking place.
It is a fi xed health day held every month at
the AWC to provide antenatal, postnatal,
family planning and child health services. The
AWW, ANM and a Medical offi cer from the
PHC would be in attendance. The AWW and
Sahayogini (and other community volunteers)
would be responsible for ensuring that all
children 0-6 and children for immunization
and other health services be brought to the
AWC on that day, when ANM and MO visit
to provide immunization, and other health
care services. Services to be provided on
the Health Day (by the ANM or PHC MO)
include ANC, newborn check-up, postnatal
care, immunization of mothers and children,
IFA and Vitamin A administration, growth
monitoring, treatment for minor ailments, and
health education.
During the Nutrition Mission, the MCHN Day
would celebrate health and nutrition of the
mother and the child in the 0-6 age group.
Cultural activities, celebrating milestones of
children and other entertaining and festive
events would mark the MCHN Day.
The MCHN Day will help strengthen the
Mission objectives through the reiteration of

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode52
the importance of the health and well being of
mothers and children for society.
Frequency : 1 fi xed day of the month
Participants: All pregnant and lactating womenAll children in the 0-6 age group
Events: Bringing Mamta card for making any enquiriesHealth check up - ANC + infant/young child’s healthGrowth monitoringDemonstrations of nutritive cooking Dialogue between mothers and health & nutrition functionaries and volunteer teams on milestonesHealth and nutrition education
IV. Integrated management of childhood illnesses2
It is seen that in most cases, more than
one underlying cause contributes to the
illness of the child. While the Mission will
focus on treatment, it will also emphasise
prevention of illness through education on the
importance of immunisation, micronutrient
supplementation, and improved nutrition
- especially breastfeeding and infant feeding.
The Mission will also achieve its objective by
improving family and community practices
for the home management of illness, and
improving case management of skills of health
workers.
Detection of symptoms of illnesses, such as diarrhoea, and referral by Childhood Illnesses Volunteers who would be trained on WHO
recommendations.
2 The Integrated Management of Childhood Illness (IMCI) was fi rst developed in 1992 by UNICEF and the World Health Organization (WHO) with the aim of prevention, or early detection and treatment of the leading childhood killers.
Diseases occurring frequently among tribal children in Rajasthan
Pneumonia
Malaria
Jaundice
Diarrhoea
Source: Assessment of ICDS in tribal areas in Rajasthan, IIHMR
Training to Childhood Illnesses Volunteers on
detection of cases of common illnesses
Case treatment by health workers
Fortnightly visits to homes to detect
cases
Management and follow-up of ill children

53Firm foundations
Reducing malnutrition in 0-6 year-olds
In order to accelerate the decline in infant mortality, a special program has been launched in Rajasthan, especially focusing on newborns. This approach is called integrated management of childhood illnesses (IMNCI).
The core IMNCI intervention is integrated case management of the fi ve most important causes of childhood deaths — acute respiratory infections, diarrhoea, measles, malaria and malnutrition. In addition, it ensures that skilled providers visit all newborns at least three times within fi rst week of life. This strategy is likely to increase the survival of newborns in the state.
Integrated case management involves training of a large number of health and nutrition workers in an intensive skill-based program. These trained workers make home visits to newborns and manage sick children in their communities. These workers include the following: Medical offi cers
Auxiliary Nurse-Midwives
Angan Wadi workers
Accredited Social Health Activists
Sahayoginis
Progress so far: In Rajasthan, IMNCI is a core strategy for improving child health under RCH-II. An outlay of Rs 20 cores have been kept for upscaling IMNCI. IMNCI will be implemented in 9 districts in the fi rst phase:
1. Jhalawar, 2. Tonk, 3. Bharatpur, 4. Sawai Madhopur, 5. Dholpur, 6. Baran, 7. Kota, 8. Bundi, 9. Karauli
Kota Medical College and SMS Medical College are acting as regional resource centers. UNICEF provides technical support.
Training of master trainers: State facilitators (consisting of faculty from medical colleges and pediatricians) have been trained in a Master Training Workshop conducted at SMS Medical College and Jaykaylon Hospital. About 20 facilitators have been trained.
Training of trainers: District-level training of trainers has been conducted for the following districts: Baran
Jhalawar
Tonk
Karauli
Training for Bundi is ongoing.
Training of frontline workers: About 400 frontline workers have been trained in the districts of Jhalawar and Tonk. Training in Baran is being initiated. Trained workers have visited more than 2,000 newborns at home after training: more than 90% of births in their fi eld area. Initial results are encouraging.
Keeping illness at bay, the IMNCI way
Encouraging home-based management of childhood illnesses through night classes (by Childhood Illnesses Volunteer Team) for fathers’ groups and day classes for mothers’ groups
1. Diarrhoea Understanding causes, consequences &
symptoms
Home-based care (Application of ORT,
dosage of ORS and other management tips)
2. Malaria Use of treated malaria nets/involve in efforts
targeting breeding of mosquitoes to be taken
up as cleanliness drive
3. Jaundice Understanding causes, consequences &
symptoms

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode54
4. Pneumonia Understanding causes, consequences &
symptoms
V. Establishing community food security systems during lean season and water security systemsAccess to clean water and adequate sanitation
facilities is an essential component for the
success of any nutrition drive. Water supply,
sanitation and hygiene, given their direct
impact on infectious disease, especially
diarrhoea, are important for preventing
malnutrition. In drought-prone Rajasthan with
its scarce water resources, it becomes all the
more important to ensure water supply through
alternate means such as water harvesting and
also the quality of drinking water.
Similarly, seasonal food shortages tend to
recur on an annual basis among the tribal
Some tips for home management of childhood illnesses
Diarrhoea Breastfeed more often Give extra fl uids Give correct dosage of
ORS Continue to give normal diet If loose motions do not
stop, take child to centre
DANGER SIGNS
FeverUse cold, wet sponge on the forehead and limbs during high fever and take child to centre If loose motions do not
stop, take child to centre
centre
Acute Respiratory InfectionTake child immediately to centre if she/he is: breathing fast breathing with diffi culty not able to drink/breastfeed becoming sicker developing fever
DANGER SIGNS
DANGER SIGNS
populations, which have a serious and
damning effect on their nutritional status. In
order to avoid this, through the Mission, in
the focus areas, efforts to maintain adequate
food stock and deliver emergency food will be
promoted.
1. Nutrition Team comprising AWW and Health volunteers to undertake Assessment Drive to:a. Check access and availability of food grain
by households having Grade III & IV children
b. Assessing storage facilities at AWCs
c. Assessing cooking facilities at AWC
2. Establishment of cooperative grain banksLocal-level grain banks (1 per village) operated
by self-help groups supported by a revolving
fund; PDS to be involved; storing of grains for
the lean season

55Firm foundations
Reducing malnutrition in 0-6 year-olds
Fluoride poisoning can be prevented or minimised by using alternative water sources, by removing excessive fl uoride from drinking water, and by improving the nutritional status of populations at risk.
Source: UNICEF http://www.unicef.org/programme/wes/info/fl uor.htm, UNICEF's Position on Water Fluoridation
such tankas and transporting it to their
individual household storage tanks.
Wherever possible individual households
shall be encouraged to construct ground
water recharge dug well/kui so as to use
surplus rain water of their household for
recharge purposes.
Surplus rain water of a village shall be
impounded in an already existing nadi/
johar/local taalaab for storage. The
VWSC shall also arrange to clear any
encroachment of the catchments area of
such structures and shall be responsible for
its maintenance.
The PHED in consultation with other
concerned departments shall take up
construction of anicut, sub-surface barrier
on rivers/streams/nallas and provide
necessary recharge structures. Such
works shall be executed by the relevant
department.
4. Ensuring availability of India Mix/Rajasthan Mix during hungry seasonIndigenously produced, low-cost nutritious
food supplement (blended mix of wheat and
soya, enriched with vitamins and minerals)
5. Construction of low cost latrines These can be constructed even by the families
themselves with a little labour and fi nancial
assistance from UNICEF, Dept of PHE and the
Total Sanitation Campaign (See Annexure 5 for options provided by UNICEF).options provided by UNICEF).options provided by UNICEF
3. Water harvesting and conservationAt department level
Repairing of old pipelines, taps, hand pumps
and other sources in households, schools,
AWCs
Identifying and weeding out ineffi cient
pumping machinery
Distribution of defl uoridation fi lters
– household/community units
At community and departmental level: Rain
water harvesting & artifi cial recharge efforts
Rain water harvesting both in individual houses
and on community basis shall be taken up.
Similarly, massive action for artifi cial recharge
of the ground water aquifer on community
basis in a village shall be required.
Roof top/ground level water harvesting will
be taken up in individual households. The
benefi ciary family shall contribute towards
labour component of the work so that it
develops a sense of ownership of the assets
so created.
Community ‘tankas’ would be constructed
wherever possible so that surplus rainwater
of a village is collected and utilised during
critical period.
The local Village Water and Sanitation
Committee shall look after the up-keep of
such community assets and impose a ban
on taking out or pumping out of water from
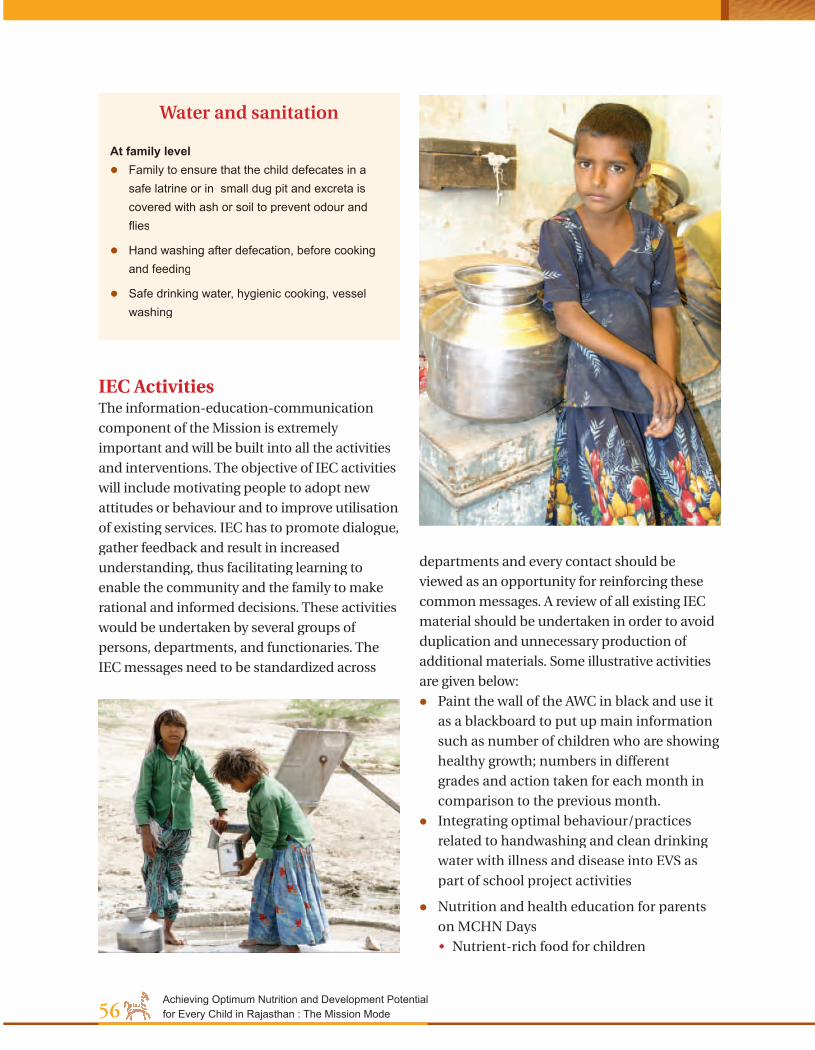
Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode56
IEC Activities The information-education-communication
component of the Mission is extremely
important and will be built into all the activities
and interventions. The objective of IEC activities
will include motivating people to adopt new
attitudes or behaviour and to improve utilisation
of existing services. IEC has to promote dialogue,
gather feedback and result in increased
understanding, thus facilitating learning to
enable the community and the family to make
rational and informed decisions. These activities
would be undertaken by several groups of
persons, departments, and functionaries. The
IEC messages need to be standardized across
departments and every contact should be
viewed as an opportunity for reinforcing these
common messages. A review of all existing IEC
material should be undertaken in order to avoid
duplication and unnecessary production of
additional materials. Some illustrative activities
are given below:
Paint the wall of the AWC in black and use it
as a blackboard to put up main information
such as number of children who are showing
healthy growth; numbers in different
grades and action taken for each month in
comparison to the previous month.
Integrating optimal behaviour/practices
related to handwashing and clean drinking
water with illness and disease into EVS as
part of school project activities
Nutrition and health education for parents
on MCHN Days
Nutrient-rich food for children
Water and sanitation
At family level Family to ensure that the child defecates in a
safe latrine or in small dug pit and excreta is covered with ash or soil to prevent odour and fl ies
Hand washing after defecation, before cooking and feeding
Safe drinking water, hygienic cooking, vessel washing

57Firm foundations
Reducing malnutrition in 0-6 year-olds
Activity Responsibility
Growth monitoring AWW, ANM, Sahayogini
Referral ANM
Drive against mosquito breeding Panchayati Raj and Medical & Health departments
Distribution of treated malaria nets Medical & Health department
Distribution of IEC material on hygiene UNICEF
Facilitation of establishment of Grain Bank and its SHG
Dept of Food & Civil Supplies along with DWCD & Home Science Colleges
Provision of IndiaMix / RajasthanMix DWCD through SHGs
Building capacities of local teams Home Science Colleges, NGOs
using creative learning methods, such as
local mythological characters
using local/vernacular and colloquial
dialect
Household level competitions on
hygiene maintenance in cooking and
feeding
Quiz and other programmes with adolescent
girls in and out of school
Implementing Responsibility & ConvergenceRelevant departments, functionaries and
volunteer teams would converge and be
responsible for the activities and in achieving
the related objectives. The following table
provides information about who will do what:
Helping HandsIt is important to build and strengthen
local level teams, build human resources
at the community level that will result
in local ownership and strengthen local
learning. The interventions related to child
malnutrition would be community-driven
and be implemented at the grassroots by the
community-based volunteer teams
Community-based volunteer teams comprising
Nehru Yuva Kendra members, Mahila Mandal
members, Kishori Balika Mandal members
1. Growth Monitoring VolunteerTeam
2. Referral Volunteer Team
3. Childhood Illnesses Volunteer Team
4. Grain Bank SHGs

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode58
Caring for the care giver
Fundamental Objective To ensure safe and healthy pregnancy and
delivery and pave the way for a healthy
motherhood
Specifi c Goals1. Operationalising universal screening of
pregnant and lactating women; ensuring
ANCs and PNCs, encouraging institutional
deliveries
2. Ensuring appropriate infant feeding
practices (universal colostrum feeding,
exclusive breast feeding up to six months,
introduction of semisolids at six months)
3. Dietary diversifi cation to include vitamin A-
rich, vitamin C-rich and iron-rich foods
4. Promoting appropriate intra-family
distribution of food based on requirements;
5. Promotion of hygienic ways of cooking and
sanitary practices
Strategic Interventions
Strategy: Community-led mapping of all pregnant & lactating women
Actions to be taken1. Identifi cation of all pregnant & lactating
women in village
i) Maintenance of ANC and PNC records
related to:
ii) Preparing easy-to-understand records
iii) Preparing map of village and associating
households having pregnant and
lactating women
iv) Identifi cation of high-risk mothers
v) Weighing and identifi cation of low-
weight mothers (those with less than
40kg body weight)
Chapter 7
Pregnant and lactating women
HealthFood
Care
Elements that infl uence the nutritional status of women

59Caring for the care giver
Pregnant and lactating women
Strategy: Empowering women with knowledge of importance of antenatal check-ups and all elements
Strategy: Door-to-door micronutrient supplementation (IFA, Vitamin A) undertaken by Peer Group of mothers of 1-year olds and above in addition to distribution of IFA at AWCs
ANTENATAL CHECK -UPS
First check-up: Prior to Month 3Second check-up: During Month 7Third check-up: During Month 9
ANTENATAL
Visits the AWC
PregnantWoman
Home visits by AWW/ANC/
Sahayogini
Residingnear AWC
Residing farfrom AWC
Strategy: Women who reside far from the AWC will be visited by a team led by AWW/ ANM/Sahayogini
Care of pregnant woman

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode60
Fortifi cation of common food items, such as salt with iron, to increase the dietary intake of iron and improve the haemoglobin status of the entire population, including girls and women prior to pregnancy
Screening of all pregnant women for anaemia using a reliable method of haemoglobin estimation
Oral iron folate prophylactic therapy for all non-anaemic pregnant women (with haemoglobin more than 11 g/dl);
Iron folate oral medication at the maximum tolerable dose throughout pregnancy for women with haemoglobin level between 8 and 11 g/dl;
Parenteral iron therapy for women with haemoglobin level between 5 and 8 g/dl if they do not have any obstetric or systemic complication;
Hospital admission and intensive personalized care for women with haemoglobin less than 5 g/dl;
Screening and effective management of obstetric and systemic problems in all anaemic pregnant women; and
Improvement in health care delivery systems and health education to the community to promote utilization of available care
Source: Tenth Five-Year Plan Nutrition goals, Govt of India
Danger signsDanger signs
Bleeding during pregnancy/
delivery
Danger signsDanger signsSevere
anaemia with/without breathlessness
Labour pain for more than 12 hours
Danger signs
Bursting of water bag
without labor pain
Danger signsDanger signs
Convulsions or fi ts, blurring of vision, or fi ts, blurring of vision,
headache, sudden swelling of feet
or fi ts, blurring of vision, or fi ts, blurring of vision, headache, sudden
High fever during pregnancy
or within 1 month of delivery
Strategy: Recognition of high risk factors and equipping mothers/
AWWs/Sahayginis and ANMs to manage these
Educating family in understanding danger signs
Multi-pronged strategy for control of anaemia in pregnancy

61Caring for the care giver
Pregnant and lactating women
If delivery conducted at home, it is to be done
only by skilled TBAs, trained dais or ANM
Community arrangement of transport in times of emergency and for deliveryImprove facilities for referral transportation
at panchayat, zilla parishad and primary
health centre levels. At sub-centres, provide
ANMs with soft loans for purchase of mopeds,
to enhance their mobility. This will increase
coverage of ante-natal and post natal
check-ups, which, in turn, and will bring
about reductions in maternal and infant
mortality.
Institutional strategies Strengthen community health centres to
provide comprehensive emergency obstetric
and neo-natal care. These may function as
clinical training centres as well.
Strengthen primary health centres to provide
essential obstetric and neo-natal care
Strengthen sub-centres to provide
a comprehensive range of services,
with delivery rooms, counselling
for contraception, supplies of free
contraceptives, ORS and basic medicines,
together with facilities for immunization
Post-natalStrategy: Ensuring post-natal check-ups and spreading awareness on spacing during the check-ups
During the post-natal check-ups, the
importance of spacing births and the methods
to do so would be conveyed to the new parents.
Easy-to-understand, pictorial IEC material on
this will be provided so that in case the father is
not present, he can appreciate and understand
the same at home.
Health
AntenatalStrategy: AWW/ANM/Sahayogini to ensure
that all pregnant women attend 3 compulsory
antenatal check-ups, which includes weighing
Ensuring safe deliveriesEnsuring safe delivery with assistance of skilled
attendants
Preparation for home delivery Clean hands
Clean surface & surroundings
Clean blade
Clean umbilical cord
Clean thread to tie the cord

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode62
Janani Suraksha Yojana (JSY) integrates cash assistance with antenatal care during pregnancy, institutional care during delivery and immediate post-partum period in a health centre by establishing a system of coordinated care by the fi eld-level health worker. The Nutrition Mission aims to converge with the scheme in its objective to ensure maternal care.
Objectives of JSY To reduce overall maternal mortality ratio and infant
mortality rate
To increase institutional deliveries in BPL families
Target group of JSYAll pregnant women belonging to the below poverty line (BPL) households and Of the age of 19 years or above
Up to two live births
Strategy of JSYLink cash assistance under JSY to institutional delivery by carrying out the following: Early registration of the benefi ciaries with the help
of the village level health workers like ASHA or an equivalent worker
Early identifi cation of complicated cases
Providing at least three antenatal care, and post delivery visits
Organizing appropriate referral and provide referral transport to the pregnant mother
Convergence with Integrated Child Development Services (ICDS) worker by way of involving Angan Wadi worker (AWW) intensively
Devising as well as ensuring transparent and timely disbursement of the cash assistance to the
mother and the incentive to the Accredited Social Health Activist (ASHA) or an equivalent worker with fund available with ANM
The strategy also involves the following: Operationalisation of 24/7 delivery services at PHC
level to provide basic obstetric care
Operationalisation of First Referral Units (FRUs) to provide the emergency obstetric care
Building partnerships through a process of recognition/accreditation with doctors, hospitals/nursing homes/clinics from the private sector specially in the rural areas to provide obstetric services to the JSY benefi ciaries.
Janani Suraksha Helpline was started in April 2006 in Dholpur district by UNICEF Rajasthan’s NGO partner Mangalam Seva Samiti (MSS) with the specifi c objective of developing a 24-hour obstetric helpline. On receiving a call, the helpline staff not only support the transportation of the woman to the health facility, but actually negotiate the health system for admission and hospital stay of the woman. The helpline is truly a community based and supported initiative. The phone number of the helpline has been popularized through wall writings, stickers and by word of mouth. The taxi drivers have been mobilized and sensitized to be ready to transport obstetric emergencies. A standardized fare chart has been prepared after consulting them to ensure there is no delay due to price negotiation. At present, 346 transport vehicles are involved in the project and 105 telephone contact points have been identifi ed which can be used to access the helpline. The Police Department has been brought on board to ensure prompt and safe movement of vehicle carrying women with obstetric emergencies.
Janani Suraksha Yojana
Safe water and sanitation Ensuring intake of clean drinking water and
maintenance of hygiene during and after
pregnancy.
FoodStrategy: Identifi cation of cheap, locally available nutritious foods and demonstrations of nutritive cooking on MCHN Day
Strategy: Consumption of nutritious, wholesome meal every day at the AWC, using locally available, followed by quizzes and songs to make it a fun event
Pregnant and lactating women of the village to
gather at the AWC daily, form groups, cook a
nutritious meal, and consume the same at
the AWC

63Caring for the care giver
Pregnant and lactating women
Vitamin A – rich foodsDark green leafy vegetables like spinach, amaranth,
deep yellow fruits like papaya, mango and melon and milk and milk products, fi sh and eggs
Iron-rich foods Green leafy vegetables, wheat, ragi, jowar, pulses
Vitamin C – rich foodsamla, guava, oranges
Key messages: Hand washing and hygienic preparation of
meals and before eating
Using iodized salt in food
Identifying foods rich in iron and vitamin A
Homestead production Using degraded lands for vegetable
production
Farm wastes as well as food grains unfi t
for human consumption can be used to
feed backyard poultry in order to increase
homestead production of eggs and chicken
and also increase consumption of these at
home
Adolescents can also be involved in this and
school children
A pregnant woman should consume More food
A variety of foods like cereals and whole grains, green leafy vegetables, fruits, lentils and beans, milk and its products, and meat and eggs
Only iodised salt
FIRST FEEDSome important steps
1. Initiate child into breastfeeding within an hour2. Show mothers how to breastfeed and how
to maintain lactation even if they should be separated from their infants
3. Give newborn infants no food or drink other than breastmilk, unless medically indicated
4. Practise rooming-in – allow mothers and infants to remain together – 24 hours a day
5. Encourage breastfeeding on demand
Source: Protecting, Promoting and Supporting Breastfeeding: The special role of maternity services;A Joint WHO/UNICEF Statement (WHO, 1989) and ‘The Global Criteria for the WHO/UNICEF Baby-Friendly Hospital Initiative’ (UNICEF, 1992)
Care
Adequate rest and reduced workload
Strategy: Support group to ensure that the pregnant and lactating women do not take on arduous work
Collective effort for procuring fi rewood
– using boys in the village
Breaks during work

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode64
Infant and young child feeding
Strategy: Formation of breastfeeding & child feeding support groups
Support groups to meet once a week in order to
access information on:
1. Colostrum feeding
2. Exclusive breastfeeding for 6 months
3. Breast hygiene and dietary intake of mother
affecting breastfeeding
4. Young Child Feeding & illness management
The group will share concerns and experiences
and, thereby, help women breastfeed effectively.
The support group will meet at a unanimously
chosen venue, which could either be at the
AWC or at the home of a member.
Strategy: Cluster counselling on complementary feeding at AWC and for fathers’ groups by IYCF Volunteer Team
Counselling on timely, adequate, safe and
appropriate complementary foods and feeding
starting after six months
Strategy: Demonstration of appropriate feeding by lactating women with infants above 6 months of age, peer review and discussions
Thematic discussions : E.g. ‘Breastfeeding - the
right way’, Ensuring proper IYCF”
IEC activities Posters on breastfeeding to be displayed at
the AWC, health centre and using cultural
events/
Development of culturally appropriate
messages
MCHN Day to be used to spread messages n
the following
Important to have that extra, energy-
dense, nutritious meal during pregnancy
Connection between maternal and infant
nutrition and a clean environment and
adequate personal hygiene
MCHN Day – Quizzes on elements of ante-
natal care and prize distribution
Lactating mother’s groups to engage in
dialogue with pregnant women’s groups
(mother-to-mother support)
An easy-to-understand chart:
Antenatal Dangers signs & how to control
Labour & delivery Special care
Immediate newborn Danger signs & care
Postpartum care for new born & mother
Dangers signs & care
Adolescent girls would be encouraged to
develop this chart, using locally available
pictorials.
Another method would be to use positive
deviants within the community as role models.
This could be a woman who is adopting
optimal practices with respect to IYCF or a
family which has collectively ensured healthy
growth and development of the child below 3
years. During the capacity building sessions
for volunteer teams, they could be equipped
to identify steps in developing such role
models.
Helping Hands
Community-based teams/groupsGrowth monitoring team
Breastfeeding support group
Mother-to-mother support group
IYCF Volunteer team comprising Nehru Yuva
Kendra members, Mahila Mandal members,
Kishori Balika Mandal members.

65Caring for the care giver
Pregnant and lactating women
Activity Implementing responsibility
Mapping, monitoring Growth monitoring team
IYCF practices Support groups
Facilities for referral transportation Panchayat
Repairing of taps, common wells Deptts of PHE and PR
Formation of breastfeeding support groups Women’s NGO, post-graduate Home Science students from local institutions
Door-to-door supplementation of IFA AWW, ANM, Sahayogini
Empowering fathers’ groups on CF AWW, ANM
Activities on MCHN Day Dept of Medical and Health
IEC strategy & materials Home Science departments & UNICEF
Implementing responsibility & convergence

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode66
The adolescent girl in focus
Towards a healthy transition
Fundamental ObjectiveTo promote the health and development of
adolescent girls (aged 10-19 years) by reducing
the prevalence of anaemia and making way for
a healthy adulthood
Specifi c Goals1. Increase intake of iron and folate to reduce
anaemia levels by 25% in fi rst year, 50% in
second year and 100% in the third year
2. Dietary diversifi cation for intake of iron-rich
foods
3. Prevent hookworm infection
4. Increase consciousness about underlying
causes of under-nutrition, i.e. age at
marriage, education, intra-household food
distribution
5. Life skills education for school-going and
non-school-going adolescent girls
6. Promote sanitary and hygienic practices and
use of clean drinking water at school and
family level
Adolescents gain 30 per cent of their adult weight and more than 20 per cent of their adult height between 10 and 19 years.
Anaemic: Haemoglobin level <12gm/dL; Severely anaemic: Haemoglobin level <7gm/dL
Chapter 8

67Towards a health transitionThe adolescent girl in focus
Key Strategies & Actions
Nutritional screening of all adolescent girls in village
1. Identify all adolescent girls (13-19 years) in
village, both school-going and non-school-
going
2. Screening of adolescent girls, especially
those who are undernourished or have
menstrual problems, for anaemia and
provide appropriate treatment
The two key approaches to combat anaemia
that the Mission would comprise medicinal
supplementation, i.e., intake of iron and
folic acid tablets or syrup, and dietary
diversifi cation, i.e., intake of foods that
contain vitamin A, such as dark green leafy
vegetables such as spinach, amaranth, cholai,
deep yellow fruits like mango, papaya and
melon, and milk and milk products.
SupplementationMedicinal supplementation requires supplying
the supplements to the adolescent girls. This can
be done through two channels, community and
school either on a weekly or bi-weekly basis.
Screening, counselling to combat anemia
Pregnant adolescentsAdolescents who are pregnant should receive very
high priority for screening and management of anaemia
Community-level activities – for non-school-going adolescents Sentinel Club
Step 1: Formation of Adolescent Sentinel Club – groups
of adolescent boys, each of which is in charge
Medicinal supplementationWeekly/bi-weekly
At community level At school level
School-based, health facility-based and community-based programmes should be considered together
Dietary diversifi cation (Micronutrient-dense
energy foods)
Key approaches
Medicinal supplementation
Combating anaemia
Supplementation
No
n-school going
Sc
hool-going

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode68
of an adolescent girls group, which will ensure
peer group support and monitoring
Step 2: Door-to-door distribution of IFA tablets by
Club members
Step 3: Six-monthly anaemia check-up; group with low
level of anaemia will be rewarded
Inclusion of extension of mid-day meal for out-
of-school girls in select locations
School-level activities – for school-going adolescents
Preparation of easy-to-understand, pictorial
calendar listing benefi ts of taking iron, advice
on where to fi nd them, how families can assist
with compliance; distribution of calendar
among school-going and non-school-going
adolescents
Distribution of IFA at school: The responsibility
for this task would be that of the school
authorities.
Implementing responsibility & convergence
Activity Implementing responsibility
Homestead production Deptts of Panchayati Raj, Food & Civil Supplies
Adolescent Sentinel Club Community, AWW, ANM, Sahayogini
IFA distribution and compliance Adolescent Sentinel Club
Anaemia reduction Departments of Education, Medical & Health
IFA calendar School going adolescent girls
Ensuring toilet and drinking water facilities in schools Depts. of PHE, Education
School gardens Teachers, Dept of Education, PR, WCD
Curriculum development Department of Education
Mid-day meal for non-school going adolescent girls Department of Panchayati Raj

69Towards a health transitionThe adolescent girl in focus
use one day of the week as an
opportunity to cook the vegetables
grown for a meal at the school
Bottom-up educational strategy:
Schoolchildren convey information to their
families. Therefore, families can be sensitized
through information and innovative activities
learned by their children in school.
IEC activities Health education
Promotion of delayed marriage for
girls, not earlier than age 18 and
preferably after 20 years of age
Educating families through drama
and songs about need for equity in
intra-household food distribution
Helping handsAdolescent Sentinel Club comprising village
youth.
Inclusion of life skills topic in Std VI-VII text books and training of teachers for ensuring life skills
Dietary diversifi cation At AWC level
Weighing of all adolescent girls at least four
times in a year, identify those with weight less
than 35 kg and provide food grains for the next
three months or until they weigh more than
35 kg
At school level
Nurture school gardens
Teachers and students nurture gardens at
school to:
learn about the importance of
diversifying the diet, and the
importance of fruits and vegetables
identify space and the vegetables to
be grown
learn how to grow vegetables

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode70
Complementing Nutrition Mission through ongoing Schemes/Programmes/Missions
Provisions in Nutrition Mission Scheme/programme/mission
Institutional delivery (beginning with early registration, identifi cation of complicated cases, ANCs, post-delivery visits, referral, referral transport, active participation of fi eld worker
Janani Suraksha Yojana (National Rural Health Mission)
Janani Suraksha Helpline : 24-hour emergency obstetric care telephone service for referral transport
Janani Suraksha Yojana (National Rural Health Mission)
Immunization, health check-up, referral services and nutrition & health education
Integrated Child Development Services (ICDS) scheme
Nutrition, health, and skill formation for adolescent girls Adolescent Girls’ Scheme/ Kishori Shakti Yojana (ICDS)
Monthly weighing of all adolescent girls in village and provision of grain to low-weight girls
National Adolescent Girls’ Scheme
Integrated Management of Neo and Childhood Illnesses (IMNCI) package
National Rural Health Mission, Reproductive and Child Health Programme II
Capacity building of health & nutrition workers in newborn care
IMNCI package, Reproductive and Child Health Programme II
ANC&PNC services, IFA distribution, delivery by skilled attendant, referral for institutional delivery, immunization, management of childhood illness, de-worming, nutrition and health education for mothers
Tribal component of Reproductive and Child Health Programme II
Grassroots level support for service provision and engagement & training of social workers/link volunteers/Sahayogini for maintaining link between health facility and community
Reproductive and Child Health Programme II (RCH II)
Water harvesting infrastructure Jal Chetna Rath Yatra
Establishment of grain banks Village Grain Bank Scheme, Ministry of Tribal Affairs, Govt of India
Ensure water supply Swajaldhara; Bharat Nirman
Construction of household latrines, AWC toilets, school toilets
Total Sanitation Campaign
School sanitation & hygiene education Total Sanitation Campaign
IEC on hygiene & sanitation Total Sanitation Campaign
School gardens, homestead gardens 20-Point Programme (11B), Ministry of Tribal Affairs, Govt of India
Food security interventions Annapurna Scheme, Mid-day Meal Scheme, Antyodaya Anna Yojana, Targeted Public Distribution Scheme
Drinking water in schools, toilets in schools Sarva Shiksha Abhiyan

71Measuring Success
Participatory monitoring and evaluation
Why Monitor And Evaluate?Participatory monitoring and evaluation is an
essential part of the Mission that will serve twin
purposes:
improve the effi ciency and effectiveness of
the interventions
increase community’s awareness and
understanding of the various factors that
affect their nutritional status
Through the exercise, the community will be
able to assess the progress of their activities
with respect to each target group, identify
gaps, re-examine resources, make mid-course
corrections, if required, and ascertain whether
or not certain strategies are better than others
and draw lessons thereof.
Measuring Success
Monitoring involves more than simply a one-time collection of information. It involves review, which is conducted more frequently.
Implementation
Monitoring
Evaluation
Planning
Review & adjustment
Problem identifi cation
Participatory monitoring and evaluation
Chapter 9
The participatory cycle

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode72
Participatory monitoring is a bottom-up
process. Intrinsic to the community-based
interventions in the Mission is lateral and
vertical feedback both from peers as well as
from the community.
These in-built mechanisms will ensure that
that responses, appraisals and reviews will take
place on a continuous basis.
How to Monitor & Evaluate?Data for monitoring the Mission will be
obtained from the following sources:
1. Family-based, home-retained Mamta Card
The Mamta Card was developed with the
objective of making families in rural areas
informed and well-versed in health and
nutrition. It also helps in accessing services and
generating demand for these.
The Mamta Card is especially useful for
illiterate women and families from rural areas
as it is easy to understand and use. It is meant
for families including a either a pregnant
woman and/or children below the age of 3
years.
The Mamta Card contains information on the
following:
a. For the pregnant woman Frequency and elements of ante-natal
check-up,
Diet and rest requirements
Danger signs to be recognised during
pregnancy and delivery
b. For the 0-3 year-old Weight monitoring
Immunisation
Feeding (breast and complementary)
Signs of childhood illnesses
c. For community Pre-school education at AWC
Spacing of births
Education and upbringing of girls
Age at marriage
Hygiene and sanitary practices
2. Display board at AWCInformation of all children enrolled in the AWC
by their malnutrition grade would be presented
on a display board outside every AWC. This
would make families and communities
conscious of the issues and facilitate dialogue
in appropriate forums.
3. Interviews with community members Data collection for monitoring would emanate
from respondents who would be members of
the community. They would include not just
the target groups members but also families,
community leaders, teachers, AWWs, ANMs,
Sahayoginis etc.
4. Visits to target householdsVisits by health workers and volunteer teams to
the homes of high risk children and pregnant
women would be a part of the review and
monitoring.
5. Independent surveys and evaluationsIn order to study, monitor and evaluate the
Mission, independent surveys and evaluation
studies would be commissioned. Rajasthan-
based credible research organisations having
experience in such work would be taken on for
the assignments.

73Measuring Success
Participatory monitoring and evaluation
6. National Nutrition Monitoring Bureau unitThe National Nutrition Monitoring Bureau
(NNMB) at the National Institute of Nutrition,
Hyderabad assesses the nutrition situation
in the country on a continuous basis. NNMB
measures nutrition status in 10 states. It is
suggested that a state-level NNMB unit be set
up as Rajasthan is not among the 10 states
monitored by NNMB.

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode74
7. Sentinel surveillanceA nutrition surveillance system is already in
place in seven districts where the UNICEF
programme Aanchal se aangan tak is underway. Aanchal se aangan tak is underway. Aanchal se aangan tak
Through this mechanism, quality data, which
would indicate any concerns under conditions
of stress such as severe drought, famines etc, is
continually collected. Sentinel Surveillance is
simple, sensitive, fl exible, acceptable and cost-
effective.
Essential requisites Preparation of protocols (questionnaires) to
be used during the period
Sensitisation of the administrators, training
of the functionaries
Developing a system of regular scrutiny and
compilation of the data generated
Dissemination and feedback of information
To begin with, one AWC per block in the
13 districts can be selected as the sentinel
surveillance centre.
Review and SupervisionIn addition to monitoring, half-yearly
review would take place wherein the district
coordination committee would review all
aspects of the Mission, including performance
of functionaries. Here, the volunteer teams too
would be active.
How to go about?
13 districts
District 1 District 2 District 3
Project 1 Project 2
Project 2
Project 2
Sentinel surveillance could be initiated in a selected area. The sentinel communities could be representative, both spatially and in numbers. Therefore, in each district, 2 ICDS projects may be selected in consultation with the district and state
authorities ensuring that they are not contiguous. From each project, 2 sectors can be randomly selected to serve as sentinel sectors. From each sector, 2 AWCs can be randomly selected.
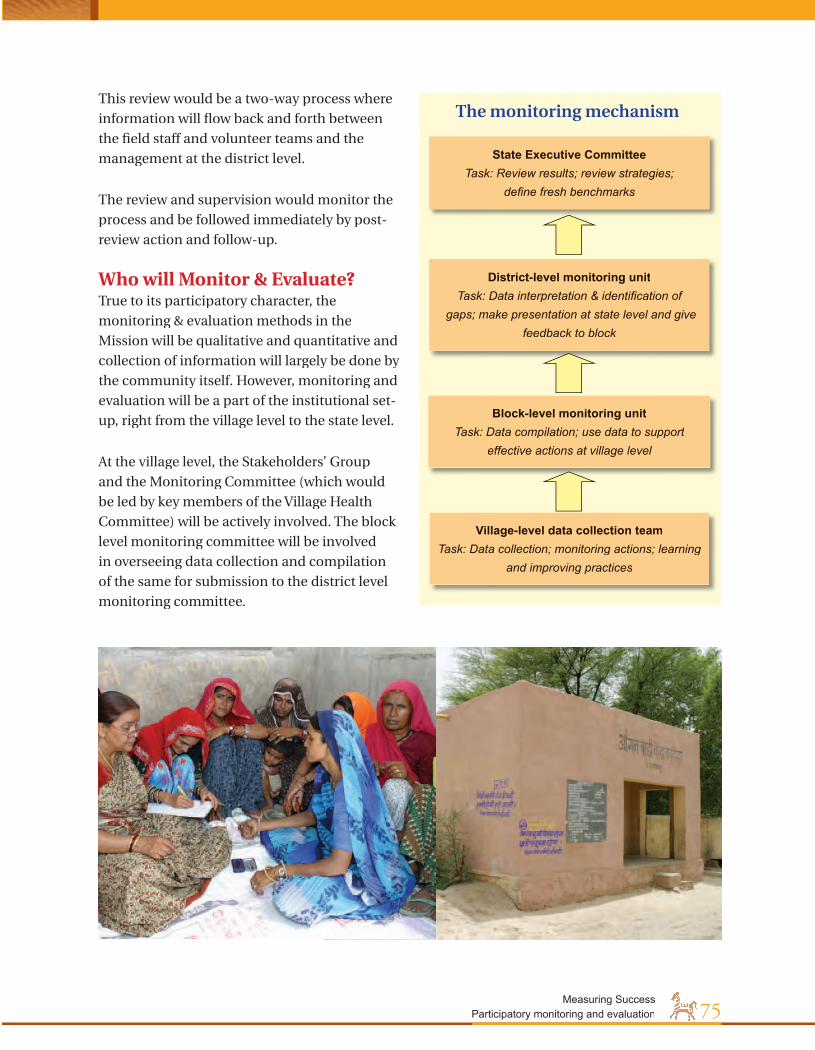
75Measuring Success
Participatory monitoring and evaluation
This review would be a two-way process where
information will fl ow back and forth between
the fi eld staff and volunteer teams and the
management at the district level.
The review and supervision would monitor the
process and be followed immediately by post-
review action and follow-up.
Who will Monitor & Evaluate? True to its participatory character, the
monitoring & evaluation methods in the
Mission will be qualitative and quantitative and
collection of information will largely be done by
the community itself. However, monitoring and
evaluation will be a part of the institutional set-
up, right from the village level to the state level.
At the village level, the Stakeholders’ Group
and the Monitoring Committee (which would
be led by key members of the Village Health
Committee) will be actively involved. The block
level monitoring committee will be involved
in overseeing data collection and compilation
of the same for submission to the district level
monitoring committee.
State Executive Committee Task: Review results; review strategies;
defi ne fresh benchmarks
District-level monitoring unitTask: Data interpretation & identifi cation of
gaps; make presentation at state level and give feedback to block
Block-level monitoring unitTask: Data compilation; use data to support
effective actions at village level
Village-level data collection teamTask: Data collection; monitoring actions; learning
and improving practices
The monitoring mechanism

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode76
Impact indicators Process indicators Behaviour indicatorsChild malnutrition
Malnutrition statusGrowth falteringImmunisationIYCFIllnessesNutritional status of pregnant and lactating womenAdolescent anaemiaIodine defi ciency disorders
Water & sanitation
Food availability, accessibility, dietary practicesCommunity participationGender equityCapacity building
Outcomes to be monitored and evaluated
Target group – Adolescent Girls
December 2007 December 2008 December 2009
IFA supplementation Universalise IFA supplementation in phase 1 districts & sustain coverage
Universalise IFA supplementation in phase II districts & sustain coverage
Universalise IFA supplementation in phase III districts & sustain coverage
Life Skill & Nutrition Education
Coverage of girls (school going 100% and out of school girls -50% out of school) in phase 1 districts.
Coverage of girls (school going 100% and out of school girls -50% out of school) in phase II districts
Coverage of girls (school going 100% and out of school girls -50% out of school) in phase III districts
What To Monitor And Evaluate?What is to be monitored can best be decided
by the community. Essentially, the impact,
process and behaviour will be monitored and
these will be associated with the objectives
framed for the Mission. To this end, relevant
information will need to be collected, which
will be quantitative as well as qualitative. Each
District Mission Management will discuss
and defi ne the impact, process and behaviour
indicators that are to be achieved for their
district.
Some performance indicators are given below:

77Measuring Success
Participatory monitoring and evaluation
Target group – 0-6 year-olds; special focus- 0-3 years
December 2007 December 2008 December 2009
Malnutrition
Weight assessment of all 0-3 year olds; referral of severely undernourished and their management; 20% reduction in malnutrition rates from present levels
Continued growth monitoring of all 0-3 year-olds; strong community-based care; 30% reduction in under-nutrition rates
No cases of severe under-nutrition; total control over growth faltering; strengthened community-based care; 40% reduction in under-nutrition rates
ImmunisationIncrease immunisation coverage to reach 70%
Increase immunisation coverage to 80%
90 % immunisation of 0-3 year-olds
Treatment of illnesses/infections
Universalise IMNCI to Phase 1 districts
Universalisation IMNCI to Phase II districts
Universalisation IMNCI to Phase III districts
Exclusive breastfeeding
Early initiation & exclusive breastfeeding improved to reach 60%
80% mothers giving colostrum within 1st hr of birth; Early initiation & exclusive breastfeeding improved to reach 80%
Early initiation & exclusive breastfeeding improved to reach 90%
Timely complementary feeding
40% children provided appropriate CF and optimal IYCF & care
60% children provided appropriate CF and optimal IYCF & care
80% children provided appropriate CF and optimal IYCF & care
Target group – Pregnant & lactating women
December 2007 December 2008 December 2009
Quality ANCs, PNCs, & safe deliveries
50 % quality ANC, obstetric (institution) & post natal coverage
70 % quality ANC obstetric (institution) & post natal coverage
90 % quality ANC obstetric (institution) & post natal coverage
Micronutrient intake IFA Iodised salt
Ensure 60% IFA consumption; Reduce anemia by 20%; HH level consumption of IS to 80%
Ensure 75% IFA consumption; Reduce anemia by 40%; HH level consumption of IS to 90%
Ensure 90% IFA consumption; Reduce anemia by 60%; HH level consumption of IS to 100%
Exclusive breastfeeding
Early initiation & exclusive breastfeeding improved to reach 60%
80% mothers giving colostrum within 1st hr st hr st
of birth; Early initiation & exclusive breastfeeding improved to reach 80%
Early initiation & exclusive breastfeeding improved to reach 90%

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode78
When to Monitor & Evaluate
Timeline
December 2007 December 2009 December 2011
Wk1 Wk2 Wk3 Wk4 Wk1 Wk2 Wk3 Wk4 Wk1 Wk2 Wk3 Wk4
Data collection
Data compilation
Data interpretation
Presentation at state level
Sharing with community

79Reference
References1. Food Insecurity Atlas of Rural India, WFP and MSSRF 2001
2. NFHS II 1998-99, Rajasthan
3. Census 2001
4. National Rural Health Mission, mohfw.nic.in/nrhm.html
5. Micronutrient Profi le of Indian Population, ICMR 2004
6. ICDS III – Evaluation 1999-2006, Presentation made at National Consultation on Child Under
Nutrition and ICDS in India, May 2006
7. www.unicef.org/india/nutrition
8. The State of the World’s Children, UNICEF 1998
9. Repositioning nutrition as central to development, A strategy for large-scale action, The World
Bank, 2006
10. ACC/SCN, Second Report on the World Nutrition Situation: Vol. I: Global and Regional Results,
ACC/SCN, Geneva, 1992
11. Constitution of India
12. ICDS data, October 2005, DWCD, Govt of Rajasthan
13. Management of severe malnutrition: A manual for physicians and other senior health
workers, World Health Organization, Geneva, 1999
14. Tenth Five-Year Plan Nutrition goals, Govt of India
15. UNICEF and the Global Strategy on Infant and Young Child Feeding (GSIYCF), Understanding
the Past – Planning the Future, UNICEF Working Paper
16. Nutrition and Gender, Ruth Oniang’O and Edith Mukudi, A Foundation for Development,
Brief 7 of 12
17. Nutrition in adolescence – Issues and Challenges for the Health Sector, Issues in Adolescent
Health and Development, World Health Organization 2005
18. Sector Policy for Rural Drinking Water and Sanitation (Draft), Govt of Rajasthan, 2005
19. Guidelines for Participatory Nutrition Projects, Food and Agriculture Organization (FAO)
Corporate Document Repository
20. Rajasthan Human Development Report 2002 (HDRC, UNDP)
21. Background note and recommendations, State Secretaries’ Working Group workshop, Govt of
Rajasthan, July 2005
22. Study on existing system of distribution of nutrition, its quality acceptability of benefi ciaries
and need for alternative cost-effective system - IDS Jaipur
23. Study on effi cacy of pre-school activity in anganwari centres and its relevance in view of DPEP
at RGSJ Pathshala etc. - IIHMR
24. World Bank-assisted ICDS Project Phase III Rajasthan: Baseline Survey - IIHMR
25. World Bank-assisted ICDS Project Phase III Rajasthan: Project Implementation Plan

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode80
Annexure 1
Micronutrients –defi ciencies and sources
IODINEWhat iodine doesIodine is needed by the thyroid gland fornormal mental and physical development.Most commonly and visibly associatedwith goitre (a swelling of the neck as theenlarged thyroid works to collect iodinefrom the blood), iodine defi ciency takes agraver toll in impaired mental acuity.Persons suffering from IDD face a rangeof serious impairments including cretinism,spastic diplegia (a spastic paralysis of thelower limbs) and dwarfi sm. Less severedefi ciencies in both adults and childrencan mean the loss of 10 to 15 intelligencequotient (IQ) points, as well as impairedphysical coordination and lethargy.
Sources of iodineIodized salt is the best source of iodine.Sea fi sh and some seaweed also containiodine, although sea salt does not.
VITAMIN AWhat Vitamin A doesVitamin A, stored normally in the liver, is crucial for effective immune-system functioning, protecting the integrity of epithelial cells lining the skin, the surface of the eyes, the inside of the mouth and the alimentary and respiratory tracts. When this defence breaks down in a vitamin A defi cient child, the child is more likely to develop infections, and the severity of an infection is likely to be greater. Depending on the degree of the defi ciency, a range of abnormalities also appears in the eyes of vitamin A-defi cient children. In the mildest form, nightblindness occurs because the rods in the eye no longer produce rhodopsin, a pigment essential for seeing in the dark. In more severe forms, lesions occur on the conjunctiva and the cornea that if left untreated can cause irreversible damage, including partial or total blindness.
Sources of vitamin AVitamin A is found as retinol in breastmilk, liver, eggs, butter and whole cow’s milk. Carotene, a precursor of vitamin A that is converted to retinol in the abdominal walls, is found in green leafy vegetables,orange and yellow fruits, and red palm oil.
Source: The State of the World’s Children, UNICEF 1998
Source: The State of the World’s Children, UNICEF 1998

81Annexures
IRONWhat iron doesThe body needs iron to produce haemoglobin, the protein in red blood cells responsible for carrying oxygen. Iron is also a component of the many enzymes essential for the adequate functioning of brain, muscle and the immune-system cells. A certain amount of iron is stored in the liver, spleen and bone marrow. Irondefi ciency develops as these stores aredepleted and there is insuffi cient ironabsorption. In anaemia, the iron defi ciencyis so severe that the production ofhaemoglobin is signifi cantly reduced.The main symptoms and signs are paleness of the tongue and inside the lips,tiredness and breathlessness. Defi cienciesof folic acid, vitamin A, ascorbic acid,ribofl avin and various minerals can alsocontribute to anaemia.
SourcesIron is found in liver, lean meats, eggs,wholegrain breads and molasses.
FOLATEWhat folate doesThis B vitamin helps in the formation ofred blood cells. Folate also regulates thenerve cells at the embryonic and foetalstages of development, helping to preventserious neural tube defects (of the brain and/or spinal cord).
SourcesFolate is found in almost all foods, butthe best sources are liver, kidney, fi sh,green leafy vegetables, beans andgroundnuts.
Source: The State of the World’s Children, UNICEF 1998
Source: The State of the World’s Children, UNICEF 1998
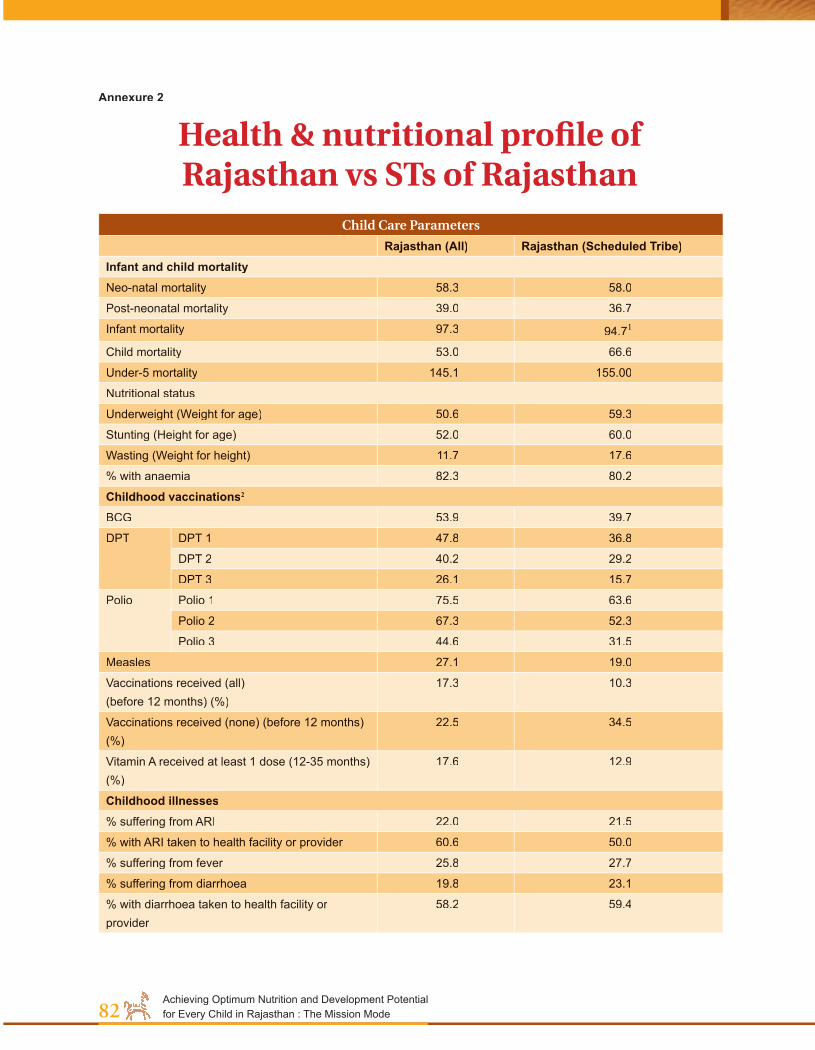
Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode82
Annexure 2
Health & nutritional profi le of Rajasthan vs STs of Rajasthan
Child Care Parameters
Rajasthan (All) Rajasthan (Scheduled Tribe)Infant and child mortalityNeo-natal mortality 58.3 58.0
Post-neonatal mortality 39.0 36.7
Infant mortality 97.3 94.71
Child mortality 53.0 66.6
Under-5 mortality 145.1 155.00
Nutritional status
Underweight (Weight for age) 50.6 59.3
Stunting (Height for age) 52.0 60.0
Wasting (Weight for height) 11.7 17.6
% with anaemia 82.3 80.2
Childhood vaccinations2
BCG 53.9 39.7
DPT DPT 1 47.8 36.8
DPT 2 40.2 29.2
DPT 3 26.1 15.7
Polio Polio 1 75.5 63.6
Polio 2 67.3 52.3
Polio 3 44.6 31.5
Measles 27.1 19.0
Vaccinations received (all) (before 12 months) (%)
17.3 10.3
Vaccinations received (none) (before 12 months) (%)
22.5 34.5
Vitamin A received at least 1 dose (12-35 months) (%)
17.6 12.9
Childhood illnesses% suffering from ARI 22.0 21.5
% with ARI taken to health facility or provider 60.6 50.0
% suffering from fever 25.8 27.7
% suffering from diarrhoea 19.8 23.1
% with diarrhoea taken to health facility or provider
58.2 59.4

83Annexures
% mothers who know about ORS packets 44.8 32.7
% who know two or more signs of medical treatment of diarrhoea
17.9 19.7
Infant and young child feeding (IYCF) practices
*Initiation of breastfeeding (within 1 hour) (%) 4.8 3.7
*Initiation of breastfeeding (within 1 day) (%) 33.6 27.2
*Initiation of breastfeeding after squeezing fi rst breast milk (%)
69.1 73.8
Maternal Care Parameters
Maternal mortality ratio 670 NA
% of ever-married women with anaemia (age 15-49) 48.5 58.4
Deliveries in a medical institution (%) 21.5 15.8
Deliveries assisted by a trained doctor or a nurse/midwife (%)
35.8 23.9
IFA tablet/syrup received (%) 39.3 35.8
Tetanus toxoid (at least 2 injections) received (%) 52.1 42.1
% receiving no ante-natal check-up 52.5 57.9
% with a postpartum check-up within 2 months of birth
6.4 4.7
Iodization of Salt
% household not using iodized salt while cooking 37.1 44.2
1 IMR for Rajasthan, as per SRS 2004, stands at 67.2 Percentage of children aged 12-23 months who received specifi c vaccinations at any time before interview (according to the vaccination card or the mother)Source: NFHS II 1998-99

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode84
Annexure 3
Target Population (Rural)Phase 1 districts
District 0-4 Adolescent girls Women
Total SC ST Total SC ST Total SC STDungarpur 155307 5380 117758 103528 3805 71322 188616 7304 123886Banswara 209447 8181 171069 141136 5345 110602 244681 10066 184640Udaipur 293212 13341 193281 217773 10747 125814 407335 20442 225954Chittorgarh 181030 25589 56665 145999 19369 36267 299761 42546 71473Sirohi 99362 19727 34379 69366 12609 18293 128609 24192 35118Sawai Madhopur
115565 24908 27381 94123 18881 24049 155403 31045 41211
Jodhpur 279926 54268 11329 199979 32881 6091 320697 54024 9512Baran 107528 19101 29361 88333 14867 21505 151230 25753 37684Rajsamand 109322 13928 18633 85128 10400 10761 164741 20037 23486Alwar 351616 67996 29970 270247 49185 23181 436135 78287 39438Dhaulpur 126312 27863 7189 76670 15617 4583 126354 26151 7484
Tonk 120888 25675 19317 96775 19263 14296 171457 33461 25267Jhalawar 122536 20712 19265 97635 14678 13076 185489 28804 23997Total 2272051 326669 735597 1686692 227647 479840 2980508 402112 849150
0-4 includes males and females; adolescent girls comprise 10-19 year-olds; women comprise 20-49 year-olds
(source: Census 2001)
Phase 2 districts
District 0-4 Adolescent girls Women
Total SC ST Total SC ST Total SC ST
Nagaur 296786 70665 736 247241 50736 589 409835 81554 935
Pali 184022 36062 15135 151097 26069 8926 256888 44830 16619
Bhilwara 197730 35186 23193 153680 24088 14204 298368 47869 31146
Kota 86361 20013 19317 76621 15852 14296 133354 28890 25267
Barmer 285579 49878 20588 174049 26713 10792 302116 46639 18484
Jaisalmer 68519 11435 4661 39123 6221 2306 69534 10580 3825
Jalore 198501 38533 21106 141753 24355 11285 233647 39353 19750
Bikaner 163011 44047 315 117026 28134 207 178968 42534 293
Ganganagar 156381 69895 536 142713 55587 411 250448 91435 690
Total 1636890 375714 105587 1243303 257755 63016 2133158 433684 1170090-4 includes males and females; adolescent girls comprise 10-19 year-olds; women comprise 20-49 year-olds
(source: Census 2001)
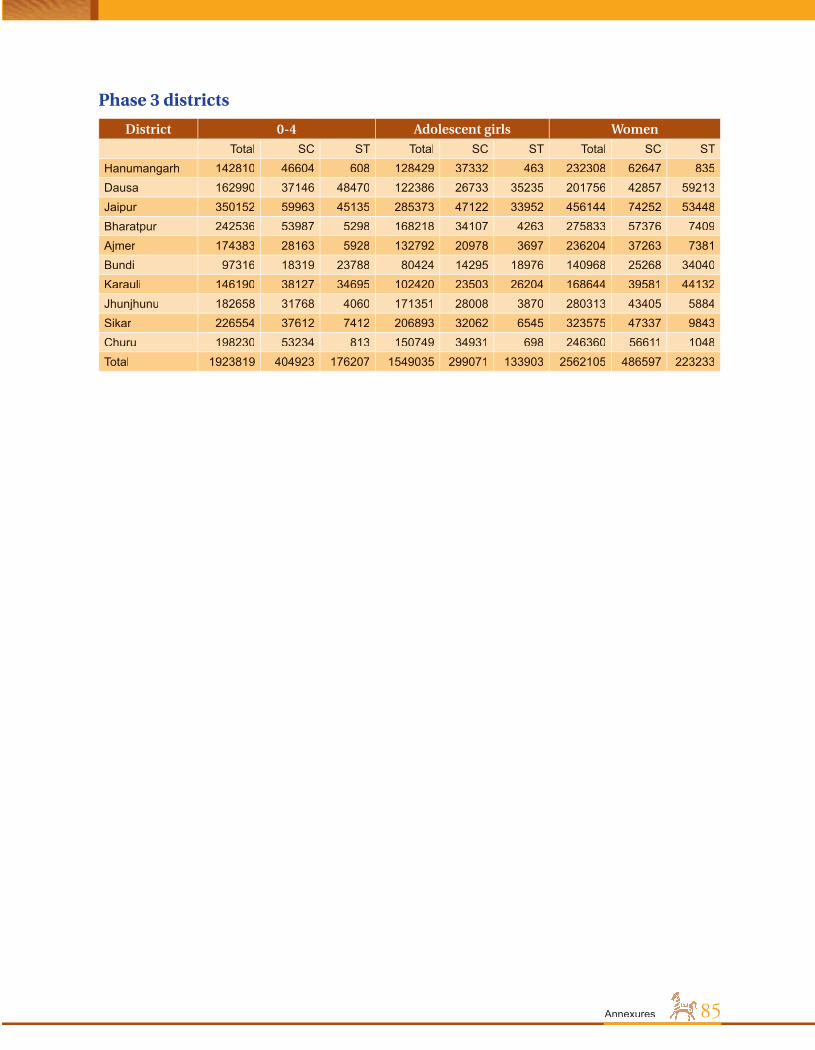
85Annexures
Phase 3 districts
District 0-4 Adolescent girls Women
Total SC ST Total SC ST Total SC STHanumangarh 142810 46604 608 128429 37332 463 232308 62647 835Dausa 162990 37146 48470 122386 26733 35235 201756 42857 59213Jaipur 350152 59963 45135 285373 47122 33952 456144 74252 53448Bharatpur 242536 53987 5298 168218 34107 4263 275833 57376 7409Ajmer 174383 28163 5928 132792 20978 3697 236204 37263 7381Bundi 97316 18319 23788 80424 14295 18976 140968 25268 34040Karauli 146190 38127 34695 102420 23503 26204 168644 39581 44132Jhunjhunu 182658 31768 4060 171351 28008 3870 280313 43405 5884Sikar 226554 37612 7412 206893 32062 6545 323575 47337 9843Churu 198230 53234 813 150749 34931 698 246360 56611 1048Total 1923819 404923 176207 1549035 299071 133903 2562105 486597 223233

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode86
Global declarations and conventions recognizing the Right to Nutrition
Global recognition of the Right to Nutrition
Declaration of the Rights of the Child
1924 The Declaration affi rms that “the child must be given the means needed for its normal development, both materially and spiritually” and states that “the hungry child should be fed.”
Universal Declaration of Human Rights
1948 Article 25 states that “everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care and necessary social services . . . .” This article also affi rms that “motherhood and childhood are entitled to special care and assistance.”
Declaration of the Rights of the Child
1959 The Declaration states in principle 4 that children “shall be entitled to grow and develop in health” and that children “shall have the right to adequate nutrition, housing, recreation and medical services.”
International Covenant on Economic, Social and Cultural Rights
1966 Article 11 affi rms the right of everyone to an adequate standard of living, including adequate food, and the “fundamental right of everyone to be free from hunger.” The Covenant also mandates States parties to take steps to realize this right, including measures “to improve methods of production, conservation and distribution of food.”
Declaration on the Right to Development
1986 Article 1 of the Declaration proclaims that the right to development “is an inalienable human right,” with all people entitled to participate in and enjoy economic, social, cultural and political development “in which all human rights and fundamental freedoms can be fully realized.” Article 8 calls for all States to ensure equal opportunity for all in access to health services and food.
Convention on the Rights of the Child
1989 Article 24 mandates States parties to recognize children’s right to the “highest attainable standard of health” and to take measures to implement this right. Among key steps, States are mandated to provide medical assistance and health care to all children, with an emphasis on primary health care; combat disease and malnutrition, within the framework of primary health care, through the provision of adequate nutritious foods, and safe drinking water and adequate sanitation; and provide families with information about the advantages of breastfeeding.
World Declaration and Plan of Action on the Survival, Protection
and Development of Children
1990 Reducing severe and moderate malnutrition by half of 1990 levels among under-fi ve children by the end of the century is the main nutrition goal. The 7 supporting nutrition goals are: reduction of low-weight births to less than 10 per cent of all births; reduction of iron defi ciency anaemia in women by one third of 1990 levels; virtual elimination of iodine defi ciency disorders; virtual elimination of vitamin A defi ciency; empowerment of all women to exclusively breastfeed their children for about the fi rst six months; institutionalization of growth monitoring and promotion; and dissemination of knowledge and supporting services to increase food production to ensure household food security
Annexure 4
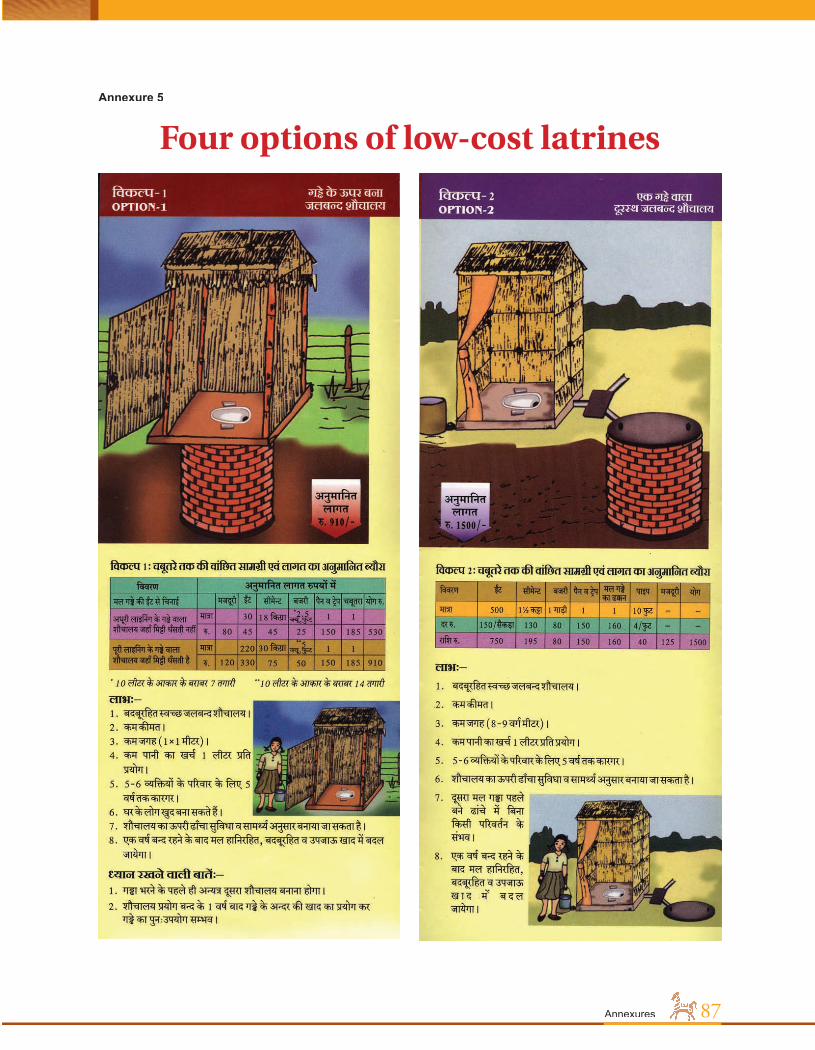
87Annexures
Four options of low-cost latrinesAnnexure 5

Achieving Optimum Nutrition and Development Potential for Every Child in Rajasthan : The Mission Mode88

Related Documents











