SPECIAL ARTICLE ACC/AHA Task Force Report Special Report: Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Perioperative Cardiovascular Evaluation for Noncardiac Surgery) Committee Members Kim A. Eagle, MD, FACC, Chair; Bruce H. Brundage, MD, FACC; Bernard R. Chaitman, MD, FACC; Gordon A. Ewy, MD, FACC; Lee A. Fleisher, MD, FACC; Norman R. Hertzer, MD, FACC; Jeffrey A. Leppo, MD, FACC; Thomas J. Ryan, MD, FACC; Robert C. Schlant, MD, FACC; William H. Spencer Ill, MD, FACC; John A. Spitteli, Jr, MD, FACC; Rmhard D. Twiss, MD, FACC Task Force Members James L. Rttchte, MD, FACC, Chmr; Melvin D. Cheitlin, MD, FACC; Kim A. Eagle, MD, FACC; Timothy J. Gardner, MD, FACC; Arthur Garson, Jr, MD, MPH, FACC; Raymond J. Gibbons, MD, FACC; Robert A. O'Rourke, MD, FACC; Thomas J. Ryan, MD, FACC CONTENTS Preamble Executive Summary Guidelines for Perioperatwe Cardiovascular Evaluation for Noncardiac Surgery I. Definition of the Problem Purpose of These Gmdehnes Epidemiology Practice Patterns Financial Implications Role of the Consultant II. General Approach to the Patient History Physical Exammatlon Comorbld Diseases Ancillary Studms III. Disease-Specific Approaches Coronary Artery Disease Hypertension Congestive Heart Failure Cardiomyopathy Valvular Heart Disease Arrhythmms and Conduction Defects Pulmonary Vascular Disease IV. Type of Surgery Urgency Surgical Risk V. Supplemental Preoperative Evaluation Resting Left Ventricular Function Assessment of Risk for Coronary Artery Disease and Functional Capacity Functional Capacity Exercise Stress Testing for Myocardial Ischemia and Functional Capacity Nonexercise Stress Testing Myocardial Perfusion Imaging Methods Dobutamine Stress Echocardlography Stress Testing in the Presence of Left Bundle Branch Block Ambulatory Electrocardxographic Monitoring VI. Implications of Risk Assessment Strategies on Costs VII. Preoperative Therapy Rationale for Surgical Coronary Revascularization and Summary of Evidence Medical Therapy Valve Surgery Arrhythmia/Conduction/Device Preoperative Intensive Care Venothromboembolism/Peripheral Arterial Disease "GuMehnes for Penoperatlve Cardtovascular Evaluatton for Noncard~ac Surgery" was appl oved by the American College of Cardtology Board of Trustees on October 15, 1995, and by the Amencan Heart Assoctatlon SA C C / Steenng Comrntttee on October 19, I995. Repnnted wah permtsston from the Amencan Heart Assoctatton, Inc The entire contents of the Gutdehnes ate pubhshed m Journal of the American College of Cardtology 27 910-948, 1996, and Clrculatmn 93 1996 Address repnnt requests to the Office of Sctenttfic Affatrs, American Heart Assoctanon, 7272 Gteenvdle Ave, Dallas, 7X 75231-4596 Copyrtght © 1996 Amencan Heart Assoctatton, Inc 1053-0771/96/1004-002250 00/0 540 Journal of Cardlothoracm and VascularAnesthesla, Vo110, No 4 (June), 1996 pp 540-552

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

SPECIAL ARTICLE
ACC/AHA Task Force Report Special Report: Guidelines for Perioperative Cardiovascular Evaluation for
Noncardiac Surgery Report of the American College of Cardiology/American Heart Association Task
Force on Practice Guidelines (Committee on Perioperative Cardiovascular Evaluation for Noncardiac Surgery)
Committee Members Kim A. Eagle, MD, FACC, Chair; Bruce H. Brundage, MD, FACC; Bernard R. Chaitman, MD, FACC; Gordon A. Ewy,
MD, FACC; Lee A. Fleisher, MD, FACC; Norman R. Hertzer, MD, FACC; Jeffrey A. Leppo, MD, FACC; Thomas J. Ryan, MD, FACC; Robert C. Schlant, MD, FACC; William H. Spencer Ill, MD, FACC;
John A. Spitteli, Jr, MD, FACC; Rmhard D. Twiss, MD, FACC Task Force Members
James L. Rttchte, MD, FACC, Chmr; Melvin D. Cheitlin, MD, FACC; Kim A. Eagle, MD, FACC; Timothy J. Gardner, MD, FACC; Arthur Garson, Jr, MD, MPH, FACC; Raymond J. Gibbons, MD, FACC; Robert A. O'Rourke, MD, FACC;
Thomas J. Ryan, MD, FACC
CONTENTS
Preamble Executive Summary Guidelines for Perioperatwe Cardiovascular Evaluation for
Noncardiac Surgery I. Definition of the Problem
Purpose of These Gmdehnes Epidemiology Practice Patterns Financial Implications Role of the Consultant
II. General Approach to the Patient History Physical Exammatlon Comorbld Diseases Ancillary Studms
III. Disease-Specific Approaches Coronary Artery Disease Hypertension Congestive Heart Failure Cardiomyopathy Valvular Heart Disease Arrhythmms and Conduction Defects Pulmonary Vascular Disease
IV. Type of Surgery Urgency Surgical Risk
V. Supplemental Preoperative Evaluation Resting Left Ventricular Function Assessment of Risk for Coronary Artery Disease
and Functional Capacity Functional Capacity Exercise Stress Testing for Myocardial Ischemia
and Functional Capacity Nonexercise Stress Testing
Myocardial Perfusion Imaging Methods Dobutamine Stress Echocardlography Stress Testing in the Presence of Left Bundle
Branch Block Ambulatory Electrocardxographic Monitoring
VI. Implications of Risk Assessment Strategies on Costs VII. Preoperative Therapy
Rationale for Surgical Coronary Revascularization and Summary of Evidence
Medical Therapy Valve Surgery Arrhythmia/Conduction/Device Preoperative Intensive Care Venothromboembolism/Peripheral Arterial Disease
"GuMehnes for Penoperatlve Cardtovascular Evaluatton for Noncard~ac Surgery" was appl oved by the American College of Cardtology Board of Trustees on October 15, 1995, and by the Amencan Heart Assoctatlon SA C C / Steenng Comrntttee on October 19, I995.
Repnnted wah permtsston from the Amencan Heart Assoctatton, Inc The entire contents of the Gutdehnes ate pubhshed m Journal of the American College of Cardtology 27 910-948, 1996, and Clrculatmn
93 1996 Address repnnt requests to the Office of Sctenttfic Affatrs, American Heart Assoctanon, 7272 Gteenvdle Ave, Dallas, 7X 75231-4596 Copyrtght © 1996 Amencan Heart Assoctatton, Inc 1053-0771/96/1004-002250 00/0
540 Journal of Cardlothoracm and VascularAnesthesla, Vo110, No 4 (June), 1996 pp 540-552

ACC/AHA TASK FORCE REPORT 541
VIII. Anesthetic Considerations and Intraoperatlve Management
Choice of Anesthetic Technique and Agent Perioperatlve Pain Management Intraoperative Nitroglycerin Use of Transesophageal Echocardiography Intra-aortic Balloon Counterpulsation Dewce
IX. Perioperative Surveillance Intraoperative and Postoperatlve Use of Pulmonary
Artery Catheters Intraoperative and Postoperative Use of ST-Segment
Monitoring Surveillance for Penoperative Myocardml Infarction Arrhythmm/Conduction Disease
X. Postoperative Therapy/Future Management XI. Conclusions
XII. Cardiac Risk of Noncardiac Surgery: Areas m Need of Further Research
Appendixes
PREAMBLE
C learly it ts important that the medical profession play a sigmficant role in critically evaluating the use of
diagnostic procedures and therapies in the management or prevention of disease states. Rigorous and expert analysis of the available data documenting relative benefits and risks of those procedures and therapies can produce helpful guide- lines that improve the effectiveness of care, optimize patient outcomes, and impact the overall cost of care favorably by focusing resources on the most effectave strategies.
The American College of Cardiology (ACC) and the American Heart Association (AHA) have produced such guidelines in the area of cardiovascular disease jointly since 1980. This report was directed by the ACC/AHA Task Force on Practice Gmdelines, which has as its charge to develop and revise practice guidelines for important cardio- vascular diseases and procedures. Experts in a given field are selected from both orgamzations to examine subject- specific data and write guidelines. Addmonal representa- tives from other medical practitioner and specialty groups are included in the wrmng process when appropriate. Each writing group is specifically charged to perform a formal hterature review, weigh the strength of evidence for or against a particular treatment or procedure, and include estimates of expected health outcomes where data exist Patient-specific modifiers, comorbldities, and issues of pa- tient preference that might influence the choice of particu- lar tests or therapies are considered along with frequency of follow-up and cost-effectiveness.
These practice guidelines are intended to assist physi- cians in clinical decision making by describing a range of generally acceptable approaches for the diagnosis, manage- ment, or prevention of specific diseases or condaions. These guidelines attempt to define practices that meet the needs of most patients in most c~rcumstances The ultimate judgment regarding care of a particular patient must be made by the physicmn and patient in light of all of the circumstances presented by that patient.
The ACC/AHA classifications I, II, and III are used in
this report to summarize indications for a particular therapy or treatment as follows:
Class I" Conditions for which there is evidence for and/or general agreement that a procedure be performed or a treatment is of benefit.
Class II: Conditions for which there is a divergence of evidence and/or opinion about the treatment.
Class IIL Conditions for wfuch there is evidence and/or general agreement that the procedure/treatment is not necessary.
The Committee to Develop Gmdellnes on Perioperative Cardiovascular Evaluation for Noncardiac Surgery was chaired by Kim A. Eagle, MD, and included the following members: Bruce H. Brundage, MD, Bernard R. Chaitman, MD, Gordon A. Ewy, MD, Lee A. Flelsher, MD, Norman R. Hertzer, MD, Jeffrey A. Leppo, MD, Thomas J. Ryan, MD, Robert C. Schlant, MD, William H. Spencer III, MD, John A. Splttell, Jr, MD, and Richard D. Twiss, MD. This document was approved by the ACC Board of Trustees and the AHA SACC/Steermg Committee and as being pub- lished simultaneously in the Journal of the Amertcan College of Cardiology and Circulation in March 1996. The document was also endorsed by the Sooety for Cardiovascular Anes- thesiologists, the Society for Vascular Surgery, and the North American Chapter of the International Society for Cardiovascular Surgery.
This document was reviewed by three outside reviewers nominated by the ACC and by three outside reviewers nominated by the AHA, as well as reviewers nominated by the American Academy of Family Physicians, the Society for Vascular Surgery, the American Society of Anesthesiolo- gists, and the Society of Cardiovascular Anesthesiologists The document will be reviewed 2 years after the date of publication and yearly thereafter and considered current unless the Task Force publishes a revision or withdrawal.
James L. Rttchze, MD, FACC Chatr, ACC /AHA Task Force on Practice GuMehnes
EXECUTIVE SUMMARY
Purpose of These Guidel ines
These guidelines are intended for physicians involved in the preoperative, operative, and postoperative care of patients undergoing noncardiac surgery. They provide a framework for considering cardiac risk of noncardiac sur- gery m a variety of patient and operative situations. The overriding theme of these gmdelines is that intervention is rarely necessary to lower the risk of surgery. The goal of the task force is the rational use of testing in an era of cost containment
General Approach
Successful perioperative evaluation and treatment of cardiac patients undergoing noncardiac surgery requires careful teamwork and commumcatlon between patient, primary care phys~oan, anesthesiologist, and surgeon. In general, indications for further cardiac testing and treat- ments are the same as those in the nonoperative setting, but

542 ACC/AHA TASK FORCE REPORT
their timing is dependent on such factors as the urgency of noncardiac surgery, the patient's risk factors, and specific surgical considerations. Coronary revascularlzation before noncardiac surgery to enable the patient to "get through" the noncardiac procedure is appropriate only for a small subset of patients at very high risk. Preoperative testing should be limited to circumstances in which the results will affect patient treatment and outcomes. A conservatwe approach to use of expensive tests and treatments is recommended.
Preoperative Clinical Evaluation
The initial history, physical examination, and electrocar- diographic (ECG) assessment should focus on identifica- tion of potentially serious cardiac disorders, including coronary artery disease (CAD) (eg, prior myocardial infarc- tion [MI], angina pectoris), congestive heart failure (CHF), and electrical instability (eg, symptomatic arrhythmlas).
In addition to identifying the presence of preexisting manifested heart disease, it is essential to define disease severity, stabdity, and prior treatment. Other factors that help determine cardiac risk include functional capacity, age, comorbid conditions (eg, diabetes mellitus, peripheral vas- cular disease, renal dysfunction, chronic pulmonary dis- ease), and type of surgery (vascular procedures and pro- longed, complicated thoracic, abdominal, and head and neck procedures considered higher risk).
Further Preoperative Testing to Assess Coronary Risk
Which patients are most likely to benefit from preopera- tive coronary assessment and treatment? The lack of adequately controlled or randomized clinical trials to define the optimal evaluation strategy has led to the proposed algorithm based on collected observational data and expert opinion. A step-wise Bayesian strategy that rehes on assess- ment of clinical markers, prior coronary evaluation and treatment, functional capacity, and surgery-specific risk is outlined below. A framework for determining which pa- tients are candidates for cardiac testing is presented in algorithmic form. Successful use of the algorithm requires an appreciation for different levels of risk attributable to certain clinical circumstances, levels of functional capacity, and types of surgery. These are defined below, after which the step-by-step algorithm is reviewed.
Climcal Markers
The major chnical predictors of increased perioperative cardiovascular risk are unstable coronary syndromes such as recent MI with evidence of important ischemic risk and unstable or severe angina; decompensated CHF, significant arrhythmias (high-grade atrioventricular block, symptom- atic arrhythmias in the presence of underlying heart dis- ease, supraventricular arrhythmias with uncontrolled ven- tricular rate), and severe valvular disease.
Intermediate predictors of increased risk are mild angina pectoris, prior MI, compensated or prior CHF, and diabe- tes mellitus. Mmor predictors of risk are advanced age, abnormal electrocardiogram, rhythm other than sinus, low
functional capacity, history of stroke, and uncontrolled systemic hypertension.
Functional Capactty
This measurement can be expressed in metabolic equiva- lent (MET) levels. Multiples of the baseline MET value can be used to express aerobic demands for specific activities. Perioperative cardiac and long-term risk is increased in patients unable to meet a 4-MET demand during most normal daily activities. The Duke Activity Status Index and other activity scales provide the clinician with a set of questions to determine a patient's functional capacity. Energy expenditure for activities such as eating, dressing, walking around the house, and dishwashing can range from 1 to 4 METs. Climbing a flight of stairs, walking on level ground at 6.4 kin/h, running a short distance, scrubbing floors, or playing a game of golf equals 4 to 10 METs. Strenuous sports such as swimming, singles tennis, and football exceed 10 METS.
Surgery-Specific Risk
Surgery-specific cardiac risk of noncardiac surgery is related to two important factors: the type of surgery itself and the degree of hemodynamic stress associated with surgery-specific procedures. The duration and intensity of coronary and myocardial stressors can be helpful in estimat- ing the likelihood of perioperative cardiac events, particu- larly for emergency surgery. Surgery-specific risk for noncar- diac surgery can be stratified as high, intermediate, and low. Htgh-risk surgery includes major emergency surgery, particu- larly in the elderly; aortic and other major vascular surgery; peripheral vascular surgery; and anticipated prolonged procedures associated with large flmd shifts and/or blood loss. Intermediate-risk procedures include carotid endarter- ectomy, head and neck surgery, intraperitoneal and intratho- racic, orthopedic, and prostate surgery. Low-risk proce- dures include endoscopic and superficial procedures, cataract surgery, and breast surgery.
Indicatzons for Angiography
Indications for coronary angiography are designated as Class I, conditions for which there is evidence for and/or general agreement that a procedure be performed or a treatment is of benefit; Class II, conditions for which there is a divergence of evidence and/or opinion about the treatment; and Class III, conditions for which there is evidence and/or general agreement that the procedure is not necessary.
Class I indications (helpful), for patients with suspected or proven CAD, are high-risk results during noninvasive testing; angina pectoris unresponsive to medical therapy; unstable angina pectoris in most patients; and nondiagnos- tic or equivocal nonmvasive test in a high-risk patient undergoing a high-risk procedure.
Class II indications (may be helpful) are intermediate- risk results during noninvasive testing; nondiagnostic or equivocal noninvasive test in a patient at lower risk under-

ACC/AHA TASK FORCE REPORT 543
going a higher risk procedure; urgent noncardiac surgery in a patient recovering from acute MI; and perioperative MI.
Class III indications (not necessary) are low-risk non- cardiac surgery In patients with known CAD and low-risk results on noninvasive testing; screenmg for CAD without appropriate noninvasive testing; patients who are asymptom- atic after coronary vascularization and have excellent exer- case capacity; mild, stable angina in patients with good left ventncular function and low-risk noninvasive test results; patients who are not candidates for revascularizatzon be- cause of concomitant illness; prior technically adequate normal coronary anglogram within 5 years; severe left ventricular dysfuncUon an patients not considered candi- dates for revascularization; and panents unwilhng to un- dergo revascularization
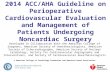
The following steps correspond to the algorithm pre- sented in Fig 1.
Step 1. What is the urgency of noncardmc surgery? Certain emergencies do not allow time for preoperative cardmc evaluation. Postoperative risk stratification may be appropriate for some patients who have not had such an assessment before.
Step 2: Has the patient undergone coronary revasculariza- tion in the past 5 years? If so, and if clinical status has remained stable without recurrent symptoms/sagns of lsCh- emia, further cardiac testing is generally not necessary.
Step 3: Has the patient had a coronary evaluation in the past 2 years? If coronary risk was adequately assessed and the findmgs were favorable, at is usually not necessary to
~ urgt~ar rl~k
~ N00r0.~,~o,0,,,o°
Abno~a l ~C~
Fig 1, Stepwlse approach to preoperative cardiac assessment, Steps are discussed in text *Subsequent care may include cancella- tion or delay of surgery, coronary revascularization followed by noncardiac surgery, or intensified care
repeat testing unless the patient has experienced a change or new symptoms of coronary ischemia since the previous evaluation.
Step 4: Does the patient have an unstable coronary syndrome or a major climcal predictor of risk? When elective noncardiac surgery is being considered, the pres- ence of unstable coronary disease, decompensated CHF, symptomatic arrhythmias, and/or severe valvular heart disease usually leads to cancellation or delay of surgery until the problem has been identified and treated.
Step 5: Does the patient have intermediate chnical predtc- tors of risk? The presence or absence of prior MI by history or ECG, angina pectoris, compensated or prior CHF, and/or diabetes melhtus helps further stratify clinical risk for perioperative coronary events. Consideration of func- nonal capactty and level of surgery-spectfic risk allows a rational approach to identifying patients most likely to benefit from further noninvasive testing.
Step 6: Patients without major but with intermediate predictors of clinical risk and moderate or excellent func- tional capacity can generally undergo intermediate-risk surgery with little likehhood of penoperative death or MI. Conversely, further nomnvasive testing as often considered for patients with poor functional capacity or moderate functional capacity but higher-risk surgery and especmlly for patients with two or more intermediate predictors.
Step 7" Noncardiac surgery is generally safe for patients with neather major nor intermediate predactors of clinical risk and moderate or excellent functional capacity (4 METs or greater). Further testing may be considered on an individual basis for patients without clinical markers but poor functional capacity who are facing higher-risk opera- tions, pamcularly those with several minor clinical predic- tors of risk who are to undergo vascular surgery.
Step 8." The results of noninvasive testing can be used to determine further preoperative management. Alterna- twely, the results may lead to a recommendation to proceed with surgery. In some panents, the risk of coronary interven- tion or corrective cardiac surgery may approach or even exceed the risk of the proposed noncardmc surgery. This approach may be appropriate, however, if it also slgnifi- candy improves the patient's long-term prognosis.
For some panents, a careful considerataon of clinical, surgery-specific, and functional status attributes leads to a decision to proceed to coronary angiography.
Management of Specific Preoperative Cardiovascular Condittons
Hypertension. Severe hypertension should be controlled before surgery when possible. The decision to delay surgery because of elevated blood pressure should take into ac- count the urgency of surgery and potennal benefit of more intensive medical therapy. Continuation of preoperative antihypertenswe treatment through the perioperatwe pe- riod is critical.
Valvular heart dasease: Indications for evaluation and treatment of valvular heart disease are identical to those in the nonoperative setting. Symptomatac stenonc lesions are

544 ACC/AHA TASK FORCE REPORT
associated with risk of perioperatlve severe CHF or shock and often require percutaneous valvotomy or valve replace- ment before noncardiac surgery to lower cardiac risk. Symptomatic regurgitant valve disease is usually better tolerated perloperatively and may be stabilized preopera- tively with intensive medical therapy and monitoring. Regur- gitant valve disease is then treated definitively with valve repair or replacement after noncardiac surgery. This is appropriate when a walt of several weeks or months before noncardlac surgery may have severe consequences. Excep- tions may include severe valvular regurgitation with re- duced left ventricular function, in which overall hemody- namIc reserve is so limited that destabilization during perloperative stresses is very likely.
Myoeardzal disease. Dilated and hypertrophic cardiomy- opathy are associated with increased incidence of perioper- ative CHF. Management is aimed at maximizing preopera- tive hemodynamic status and prowding intensive postoperative medical therapy and surveillance. An esti- mate of hemodynamic reserve IS useful for anticipating potential complications from mtraoperative and/or postop- erative stress.
Arrhythmtas and conduction abnormahties: The presence of an arrhythmia or cardiac conduction disturbance should provoke a careful evaluation for underlying cardiopulmo- nary disease, drug toxictty, or metabolic abnormality. Therapy should be initiated for symptomatic or hemody- namically significant arrhythmias, first to reverse an under- lying cause and second to treat the arrhythmia. Indications for antiarrhythmic therapy and cardiac pacing are identical to the nonoperative setting.
Supplemental Preoperatlve Evaluation
No specific recommendations can be made for individual patients. The following should be considered appropriate as indicated In specific situations: resting left ventricular function, exercise stress testing, pharmacological stress testing, ambulatory ECG monitoring, and coronary angiog- raphy. In most ambulatory patients the test of choice is
exercise ECG testing, which can both provide an estimate of functional capacity and detect myocardial ischem~a through changes in the ECG and hemodynamlc response. In patients with important abnormalities on their resting ECG (left bundle branch block, left ventricular hypertro- phy with strain pattern, digitalis effect, etc), other tech- niques such as exercise echocard~ography or exercise myo- cardial perfusion imaging should be considered.
lmphcatzons of Risk Assessment Strategzes on Costs
The degree of variation surrounding preoperatwe testing before noncardiac surgery is substantial. Cost-effectiveness analyses of various methods of preoperative testing and treatments have also yielded highly varied results. It is important for the clinician to consider the cost ~mplicatlons of screening strategies and, when possible, to rely on generally accepted strategies for treating patients in the nonoperative setting (Table 1).
Preoperative Coronary Revascularlzation
Coronary artery bypass graft (CABG) surgery: Indications for CABG before noncardiac surgery are identical to those reviewed in the ACC/AHA guidelines for CABG. CABG is rarely indicated to simply "get a patient through." How- ever, when the stress of elective noncardiac surgery is likely to exceed the stress of daily life, it may be reasonable to consider CABG before noncardiac surgery.
Coronary angtoplasty: There are no controlled trials comparing perIoperative cardiac outcome after noncardlac surgery for patients treated with preoperative PTCA versus medical therapy. Several small observational series have suggested that cardiac death is infrequent in patients who have coronary angioplasty before noncardlac surgery. Sev- eral studies have also demonstrated a number of complica- tions from angioplasty, including emergency CABG in some patients. Until further data are available, indications for PTCA in the perioperatlve setting are similar to those in the ACC/AHA guidelines for use of PTCA in general.
Table 1 Cost Assessment of a Screening Strategy for Major Vascular Surgery Patients
Cost per Test or per Procedure Accumulated Costs for Each Algortthm Step Progression of Chmcal Care At Each Step m Total for Screenmg/Treatmg 201 Pat=ents
201 consecuttve patients
Exerctse and/or dipyrldamole stress test (CPT codes 78465 and 93015) 58 patients (29%)
Cardiac catheterization and coronary angiography 16 patients (8%)
Coronary revascularization PTCA' 2 patients (6 5%) CABG 11 pattents
Total perloperatlve cardiac death 1 patient (0 5%)
Nuclearstresstestlng $ 32,886 $457 + 110 = $5671
Cardiac catheterization w~thout angioplasty or bypass surgery $9,2002
$ 27,600
Cardiac catheterization with PTCA $21,7603 $ 43,520
Cardiac catheterization w~th CABG $44,2004 $486,200
$590,206

ACC/AHA TASK FORCE REPORT 545
Medical Therapy for Coronary Artery Dtsease
There are very few randomized trials from which firm conclusions or recommendations can be drawn. However, ff patients require 13-blockers, calcium channel blockers, and/or nitrates before surgery, continuation of the preop- erative medical regimen into the operative and postopera- tive period may also protect against ischemic tendencies caused by perioperative stresses. The same is true for therapies to control symptoms of CHF. Observational studies also suggest that B-blockers reduce frequency of postoperative ischemia, and in one study reduced incidence of peroperatwe MIs. Protection against ischemia may also reduce risk of MI.
Anesthetic Considerations and Intraoperative Management
Anesthettc agent: All anesthetic techniques and drugs have known cardiac effects that should be considered in the perioperatwe plan. There appears to be no one best myocardial protective anesthetic technique. Therefore, the choice of anesthesia and intraoperative monitors is best left to the discretion of the anesthesia care team, which will consider the need for postoperative ventdation; cardiovas- cular effects, including myocardial depression; sympathetic blockade; and dermatomal level of the procedure. Advo- cates of monitored anesthesia, in which local anesthesia is supplemented by intravenous sedation/analgesia, have ar- gued that use of this techmque avoids the undesirable effects of general or neuraxial techniques, but no studies have established this. Failure to produce complete local anesthesia/analgesia can lead to increased stress response, myocardial ischemia, or depression.
Penoperattve pain management: Patient-controlled intra- venous and/or epidural analgesia is a popular method for reducing postoperative pain. Several studies suggest that effective pain management leads to a reduction m postop- erative catecholamine surges and hypercoagulability.
Intraoperattve nttroglycerm: There are insufficient data about the effects of prophylactic intraoperative intravenous nitroglycerin in panents at high risk. Nitroglycerin should be used only when the hemodynamic effects of other agents in use are considered.
Transesophageal echocardzography (TEE): There are few data on the value of TEE-detected transient wall motion abnormalities to predict cardiac morbidity in noncardiac surgical patients. Experience to date suggests that the incremental value of this techmque for risk prediction is small. Guidelines for appropriate use of TEE are being developed by the American Society of Anesthesiologists and the Society of Cardiovascular Anesthesiologists.
Perioperative Surveillance
Pulmonary artery catheters: Although very few studies that have been reported compare patient outcomes after treat- ment with or without pulmonary artery catheters, the following three variables are particularly important in
assessing benefit versus risk of pulmonary artery catheter use: disease severity, magnitude of anticipated surgery, and practice setting. The extent of expected fired shifts is a primary concern. Patients most likely to benefit from perioperative use of a pulmonary artery catheter appear to be those with a recent MI comphcated by CHF, those with sigmficant CAD who are undergoing procedures associated with significant hemodynamic stress, and those with systolic or diastolic left ventricular dysfunction, cardiomyopathy, and valvular disease undergoing high-risk operations.
Intraoperative and postoperattve ST-segment monitoring: Intraoperative and postoperative ST changes indicating myocardial ischemia are strong predictors of perioperative MI in patients at high risk who undergo noncardiac surgery. Similarly, postoperative lschemia is a significant predictor of long-term MI and cardiac death. Conversely, in patients at low risk who undergo noncardiac surgery, ST depression may occur and often is not associated with regional wall motion abnormalities. Accumulating evidence suggests that proper use of computerized ST-segment analysis m appro- priately selected patients at h~gh risk may improve sensitiv- ity for myocardial ischemia detection.
Surveillance for penoperative MI: Few studies have exam- ined the optimal method for diagnosing a perioperative MI. Clinical symptoms, postoperative ECG changes, and eleva- tion of the MB fraction of creatine kinase (CK) have been most extensively studied. Newer myocardial-specific en- zyme elevations such as troponin-I, troponin-T, or CK-MB isoforms may also have value. In patients with known or suspected CAD undergoing high-risk procedures, ECGs obtained at baseline, immediately after surgery, and the first 2 days after surgery appear to be cost-effective. Use of cardiac enzymes is best reserved for patients at high risk and those with clinical, ECG, or hemodynamic evidence of cardiovascular dysfunction.
Postoperative Therapy and Long-Term Management
When possible, postoperatwe management should in- clude assessment and management of modifiable risk fac- tors for CAD, heart failure, hypertension, stroke, and other cardiovascular diseases. For many patients, the proposed noncardiac surgery may be the first opportunity for a systematic cardiovascular evaluation. Assessment for hyper- cholesterolemia, smoking, hypertension, diabetes, physical inactivity, peripheral vascular disease, cardiac murmur(s), arrhythmms, conduction abnormalities, perioperative isch- emia, and postoperative MI may lead to further evaluation and treatments that reduce future cardiovascular risk. In particular, patients who sustain a perioperative MI and/or experience repetitive postoperative myocardial ischemia are at substantially high risk for MI or cardiac death during long-term follow-up. These patients should be a particular focus for risk factor interventions and future risk stranfica- non and therapy.

546 ACC/AHA TASK FORCE REPORT
D e v e l o p m e n t of Guide l ines
These guidelines are based on a Medline search of the English literature from 1975 through 1994, review of selected journals from 1995, and the expert opinions of 12 committee members representing various disoplines of cardiovascular care, including general cardiology, noninva- sive testing, vascular medicine, vascular surgery, anesthesi- ology, and arrhythmia management. In addition, draft guide- lines were submitted for critical review and amendment to physicians representing internal medicine, family practice, nuclear cardiology, general surgery, and anesthesiology as well as executive officers representing the American College of Cardiology and the American Heart Association. The final document represents the eighth iteration over 18 months, which included six drafts in committee and two additaonal drafts to incorporate key findings from external rewew.
A large proport ion of the data used to develop these guidelines is based on observational or retrospective studies
or knowledge of management of cardiovascular disorders in the nonoperative setting. While the collective knowledge surrounding the identification of high- and low-risk patients using perioperative clinical and noninvasive evaluation is substantial, very few prospective or randomized studies have been performed that establish the value of tests or treatments on perioperatlve outcomes. Therefore, data are presented in a tabular format, and whenever possible reflect the value of a test or intervention for similar outcomes of a perioperative MI or cardiac death. Because the studies were rarely randomized controlled trials, defini- tions of a penoperat ive event varied, investigators were rarely blinded, and many inherent selection biases existed, the task torce has chosen not to provide an aggregate synthesis of the data in the form of a point estimate or meta-analysis. On the other hand, presentation of the original data provides substantial support for these recom- mendations.
REFERENCES
1 Mangano DT- Perioperatwe cardiac morbidity Anesthesiol- ogy 72.153-184, 1990
2. Lubltz J, Deacon R: The rise in the incidence of hosp~tahza- tions for the aged, 1967 to 1979 Health Care Fmancing Review 3.21-40, 1982
3. Fleisher LA, Beattle C' Current practice in the preoperatwe evaluation of patients undergoing major vascular surgery' A survey of cardiovascular anesthesiologists. J Cardiothorac Vasc Anesth 7:650-654, 1993
4 Wells PH, Kaplan JA' Optimal management of patients with lschemlc heart disease for noncardiac surgery by complementary anesthesiologist and cardiologist interaction. Am Heart J 102:1029- 1037, 1981
5 Roger VL, Ballard D J, Hallett JW Jr, et al. Influence of coronary artery disease on morbidity and mortahty after abdominal aortic aneurysmectomy' A population-based study, 1971-1987. J Am Coil Cardlol 14"1245-1252, 1989
6 Hertzer NR' Basic data concerning associated coronary disease in peripheral vascular patients. Ann Vasc Surg 1:616-620, 1987
7 Hlatky MA, Bomeau RE, Hlgglnbotham MB, et al' A brief self-administered questionnaire to determine functional capacity (the Duke Actwity Status Index) Am J Cardlol 64.651-654, 1989
8. Gersh BJ, Rihal CS, Rooke TW, et al' Evaluation and management of patients with both peripheral vascular and coro- nary artery disease J Am Coil Cardlol 18'203-214, 1991
9 Jamleson WRE, Janusz MT, Miyagishima RT, et al' Influence of ischemlc heart disease on early and late mortahty after surgery for peripheral occlusive vascular disease Circulation 66 1-92-I-97, 1982 (suppl 1)
10. Ewy GA The abdominojugular test: Technique and hemody- namic correlates Ann Intern Med 109:456-460, 1988
11. Butman SM, Ewy GA, Standen JR, et al. Bedside cardiovas- cular examination in paUents with severe chromc heart failure: Importance of rest or inducible jugular venous distension. J Am Coll Cardio122:968-974, 1993
12. Goldman L, Caldera DL, Nussbaum SR, et al' Multifactorml index of cardiac risk m noncardmc surgical procedures. N Engl J Med 297'845-850, 1977
13 Dajanl AS, Bisno A.L, Chung KJ, et al Prevention of
bacterial endocardltis recommendations by the American Heart Assooatlon JAMA 264.2919-2922, 1990
14 Nelson AH, Fleisher LA, Rosenbaum SH: Relationship between postoperatwe anemia and cardiac morbidity in high-risk vascular patients m the intenswe care unit Crlt Care Med 21:860-866, 1993
15. Ashton CM, Petersen NJ, Wray NP, et al: The inodence of penoperative myocardial infarction in men undergoing noncardiac surgery. Ann Intern Med 118"504-510. 1993
16. Hollenberg M, Mangano DT, Browner WS, et al: Predmtors of postoperatwe myocardial lschemm in patients undergoing non- cardiac surgery: The Study of Perloperative Ischemia Research Group JAMA 268.205-209, 1992
17. Hubbard BL, Gibbons RJ, Lapeyre AC III, et al. Identifica- tion of severe coronary artery disease using simple chnlcal param- eters. Arch Intern Med 152.309-312. 1992
18. Lette J, Waters D, Bernier H. et al' Preoperatwe and long-term cardiac risk assessment. Predlctwe value of 23 clinical descriptors, 7 multivariate scoring systems, and quantxtative dipyrl- damole ~maging in 360 patients. Ann Surg 216.192-204, 1992
19 Mangano DT, Browner WS, Hollenberg M, et al' Associa- tion of perloperatwe myocardial ischemla with cardiac morbidity and mortality in men undergoing noncardlac surgery The Study of Penoperatwe Ischemla Research Group. N Engl J Med 323 1781- 1788, 1990
20 Michel LA, Jamart J, Bradpiece HA, et al. Prediction of risk In noncardlac operations after cardiac operations. J Thorac Cardlo- vasc Surg 100:595-605, 1990
21 Eagle KA, Coley CM. Newell JB, et al: Combining clinical and thalhum data optimizes preoperative assessment of cardiac risk before major vascular surgery Ann Intern Med 110:859-866, 1989
22. Detsky AS, Abrams HB, McLaughhn JR, et al' Predicting cardmc complications m patients undergoing non-cardiac surgery. J Gen Intern Med 1'211-219, 1986
23 Foster ED, Davis KB. Carpenter JA, et al: Risk of noncar- dIac operation in patients with defined coronary disease The Coronary Artery Surgery Study (CASS) registry experience Ann Thorac Surg 41.42-50, 1986
24. Cooperman M, Pflug B, Martin EW Jr, et al. Cardiovascular

ACC/AHA TASK FORCE REPORT 547
risk factors in patients with peripheral vascular disease. Surgery 84:505-509, 1978
25. Tarhan S, Moffitt EA, Taylor WF, et al Myocardml infarc- tion after general anesthesm JAMA 220'1451-1454, 1972
26. Gunnar RM, Passamani ER, Bourddlon PD, et al. Grade- lines for the early management of patients with acute myocardial infarction: a report of the American College of Cardiology/ American Heart Association Task Force on Assessment of Diagnos- tic and Therapeutic Cardiovascular Procedures (Subcommittee to Develop Guidelines for the Early Management of Patients with Acute Myocardial Infarction) J Am Coil Cardiol 16.249-292, 1990
27. Fletcher GF, Balady G, Froelicher VF, et al: Exercise standards: A statement for healthcare professionals from the American Heart Association: Writing Group. Circulation 91:580- 615, 1995
28. Steen PA, Tinker JH, Tarhan S: Myocardml relnfarctlon after anesthesm and surgery. JAMA 239:2566-2570, 1978
29 Rao TL, Jacobs KH, E1-Etr AA' Reinfarctlon following anesthesm in patients with myocardial infarction Anesthesiology 59"499-505, 1983
30. Hertzer NR: Fatal myocardml infarction following periph- eral vascular operations' A study of 951 patients followed 6 to 11 years postoperatively Cleve Chn Q 49'1-11, 1982
31 Mahar LJ, Steen PA, Tinker JH, et al" Perioperatwe myocardml infarction in patients w~th coronary artery &sease with and without aorta/-coronary artery bypass grafts. J Thorac Cardio- vasc Surg 76:533-537, 1978
32. Wemer DA, Ryan TJ, McCabe CH, et al Prognostic importance of a clinical profile and exerose test in medically treated patients with coronary artery &sease J Am Coll Cardlol 3.772-779, 1984
33. Nelson CL, Herndon JE, Mark DB, et al: Relation of chnical and ang~ographic factors to functional capacity as measured by the Duke Activity Status Index. Am J Cardlo168:973-975, 1991
34. Myers J, Do D, Herbert W, et al: A nomogram to predict exerose capacity from a specific actwlty questionnaire and clinical data. Am J Cardio173'591-596, 1994
35 Eagle KA, Rihal CS, Foster ED, et al Long-term survival in patients with coronary artery &sease' Importance of peripheral vascular disease. The Coronary Artery Surgery Study (CASS) Investigators. J Am Coil Cardio123"1091-1095, 1994
36. Guidelines for coronary anglography. A report of the Ameri- can College of Car&ology/Amencan Heart Assocmtlon Task Force on Assessment of Diagnostic and Therapeutic Cardiovascu- lar Procedures (Subcommittee on Coronary Angiography). J Am Coil Cardiol 10:935-950, 1987
37 Morns CK, Ueshima K, Kawaguchl T, et al: The prognostic value of exercise capacity. A review of the literature. Am Heart J 122:1423-1431, 1991
38. Chaltman BR: The changing role of the exercise electrocar- diogram as a diagnostic and prognostic test for chronic lschemic heart disease. J Am Coll Cardlol 8.1195-1210, 1986
39. Glanrossi R, Detrano R, Mulvihlll D, et al Exercise-reduced ST depression m the diagnosis of coronary artery disease: A meta-analysxs Czrculatlon 80:87-98, 1989
40. Detrano R, Gianrossl R, Mulvihlll D, et al' Exerose-lnduced ST segment depression in the diagnosis of multivessel coronary disease: A meta analysls. J Am Coil Cardiol 14:1501-1508, 1989
41 Mark DB, Hlatky MA, Harrell FE Jr, et al. Exercise treadmill score for predicting prognosis m coronary artery disease Ann Intern Med 106:793-800, 1987
42. Mark DB, Shaw L, Harrell FE Jr, et al. Prognostic value of a treadmill exercise score m outpatients with suspected coronary artery disease N Engl J Med 325"849-853, 1991
43. Guldehnes for exercise testing: A report of the American
College of Cardiology/American Heart Association Task Force on Assessment of Cardiovascular Procedures (Subcommittee on Exer- cise Testing). J Am Coil Cardiol 8:725-738, 1986
44. Alpert JS, Chipkln SR, Aronln N. Diabetes melhtus and silent myocardial lschemia. Adv Cardlo137:279-303, 1990
45. Shindo T, Nosaka H, Kimura T, et al: Anglography of silent myocar&ol lschemla. J Cardio121:761-769, 1991
46. Titus BG, Sherman CT' Asymptomatic myocardial ischemia during percutaneous transluminal coronary angioplasty and impor- tance of prior Q-wave infarction and diabetes mellitus. Am J CardIo168'735-739, 1991
47 Olivetti G, Melissari M, Capasso JM, et al' Cardiomyopathy of the aging human heart: Myocyte loss and reactwe cellular hypertrophy Carc Res 68:1560-1568, 1991
48. GISSI-3' Effects of lisinopril and transdermal glyceryl tnm- trate singly and together on 6-week mortality and ventricular function after acute myocardml infarction. Gruppo Italiano per lo Studio della Sopravvwenza nell'infarto Miocar&co. Lancet 343: 1115-1122, 1994
49 Castella WP Epldemlology of coronary heart disease" The Framlngham study Am J Med 76:4-12, 1984
50. Becker RC, Terrm M, Ross R, et al: Comparison of clinical outcomes for women and men after acute myocardial infarction Ann Intern Med 120'638-645, 1994
51 Raby KE, Barry J, Creager MA, et al Detection and significance of mtraoperative and postoperative myocardial isch- emia in peripheral vascular surgery. JAMA 268:222-227, 1992
52. Detsky AS, Abrams HB, Forbath N, et al: Cardmc assess- ment for patients undergoing noncardlac surgery: A multi-factorial chnical risk index. Arch Intern Med 146:2131-2134, 1986
53. The fifth report of the Joint National Committee on Detec- tion, Evaluation. and Treatment of High Blood Pressure (JNCV). Arch Intern Med 153:154-183, 1993
54 Charlson ME, MacKenzie CR, Gold JP, et al- Preoperatwe characteristics predlctmg lntraoperative hypotension and hyperten- sion among hypertenswes and diabetics undergoing noncardiac surgery. Ann Surg 212.66-81, 1990
55 Stone JG, Foex P, Sear JW, et al. Myocardial ischemia in untreated hypertenswe patients: Effect of a single small oral dose of a beta-adrenergic blocking agent Anesthesiology 68:495-500, 1988
56. Stone JG, Foex P, Sear JW, et al: Risk of myocardial ischaemla during anaesthesia in treated and untreated hyperten- swe patients Br J Anaesth 61.675-679, 1988
57. Prys-Roberts C, Meloche R, Foex P. Studies of anaesthesia in relation to hypertension, I: Cardiovascular responses of treated and untreated patients. Br J Anaesth 43'122-137, 1971
58 Pasternack PF, Grossi EA, Baumann FG, et al: Beta blockade to decrease sdent myocardial lschemia during peripheral vascular surgery. Am J Surg 158' 113-116, 1989
59 Cucchiara RF, Benefiel DJ, Matteo RS, et al: Evaluation of esmolol in controlhng increases in heart rate and blood pressure during endotracheal intubat~on In patients undergoing carotid endarterectomy. Anesthesiology 65:528-531, 1986
60. Magnusson J, Thulin T, Werner O, et al' Haemodynamlc effects of pretreatment with metoprolol in hypertenswe patients undergoing surgery Br JAnaesth 58:251-260, 1986
61. Slogoff S, Keats AS: Does perioperative myocardial lsch- emla lead to postoperatwe myocardial infarction? Anesthesiology 62:107-114, 1985
62 Bedford RF, Femstem B' Hospital admission blood pres- sure: A predictor for hypertension following endotracheal lntuba- tlon Anesth Analg 59'367-370, 1980
63 Goldman L, Caldera DL" Risks of general anesthesia and

548 ACC/AHA TASK FORCE REPORT
electwe operation in the hypertensive patient. Anesthesiology 50:285-292, 1979
64 Thompson RC, Llberthson RR, LowensteIn E' Perlopera- tire anesthetic risk of noncardlac surgery in hypertrophic obstruc- tive cardiomyopathy, lAMA 254:2419-2421, 1985
65. Reyes VP, Raju BS, Wynne J, et al: Percutaneous balloon valvuloplasty compared with open surgical commlssurotomy for mltral stenosis N Engl J Med 331.961-967, 1994
66 Stein PD, Alpert JS, Copeland J, et al Antithrombotic therapy in patients with mechanical and biological prosthetic heart valves Chest 102.445S-455S, 1992 (suppl)
67. Goldman L, Caldera DL, Southwick FS, et al' Cardiac risk factors and complications in non-cardiac surgery. Medicine (Balti- more) 57:357-370, 1978
68 O'Kelly B, Browner WS, Massle B, et al' Ventncular arrhythmias in patients undergoing noncardiac surgery: The Study of Perioperative Ischemia Research Group lAMA 268.217-221, 1992
69. Fisher FD, Tyroler HA: Relationship between ventrIcular premature contractions on routine electrocardiography and subse- quent sudden death from coronary heart disease Circulation 47'712-719, 1973
70 Kennedy HL, Whitlock JA, Sprague MK, et al Long-term follow-up of asymptomatlc healthy subjects with frequent and complex ventricular ectopy. N Engl J Med 312:193-197, 1985
71. Pastore JO, Yurchak PM, Jams KM, et al: The risk of advanced heart block in surgical patients with right bundle branch block and left axis deviation Circulation 57"677-680, 1978
72. Webb GD, Burrows FA: The risks of noncardlac surgery. J Am Coil Cardiol 18:323-325, 1991
73 Lueker RD, Vogel JH, Blount SG Jr Cardiovascular abnor- mahties following surgery for left-to-right shunts: Observations in atrial septal defects, ventricular septal defects, and patent ductus arteriosus Circulation 40'785-801, 1969
74. Maron BJ, Humphrles JO, Rowe RD, et al- Prognosis of surgically corrected coarctation of the aorta' A 20-year postopera- tive appraisal Circulation 47'119-126, 1973
75. James FW, Kaplan S, Schwartz DC, et al: Response to exercise in patients after total surgical correction of tetralogy of Fallot. Circulation 54'671-679, 1976
76 Nellson G, Galea EG, Blunt A. Elsenmenger's syndrome and pregnancy. Med J Aust 1:431-434, 1971
77. Taylor LM Jr, Porter JM. Basic data related to clinical decision-making in abdominal aortic aneurysms Ann Vasc Surg 1'502-504, 1987
78 Backer CL, Tinker JH, Robertson DM, et al: Myocardial reInfarction following local anesthesia for ophthalmic surgery. Anesth Analg 59 257-262, 1980
79 Warner MA, Shields SE, Chute CG' Major morbidity and mortality within 1 month of ambulatory surgery and anesthesia lAMA 270 1437-1441, 1993
80 Greenburg AG, Saik RP, Pridham D. Influence of age on mortahty of colon surgery Am J Surg 150.65-70, 1985
81 Plecha FR, Bertm VJ, Plecha El, et al: The early results of vascular surgery m patients 75 years of age and older: An analysis of 3259 cases J Vasc Surg 2.769-774, 1985
82 Goldman L Cardiac risks and comphcatlons of noncardlac surgery. Ann Intern Med 98 504-513, 1983
83. Pedersen T, Ehasen K, Henriksen E. A prospective study of risk factors and cardiopulmonary comphcatlons associated with anaesthesia and surgery risk indicators of cardlopulmonary morbid- lty Acta Anaesthesiol Scand 34 144-155, 1990
84 Marsch SC, Schaefer HG, Skarvan K, et al Perloperatwe myocardial ischemia in patients undergoing elective hip arthro-
plasty during lumbar regional anesthesia Anesthesiology 76.518- 527, 1992
85. Krupskl WC, Layug EL, Rellly LM, et al: Comparison of cardiac morbidity rates between aortic and mfralnguinal opera- tions' two-year follow-up. Study of Perioperatlve Ischemia Re- search Group J Vasc Surg 18'609-615, 1993
86 L'Itahen GJ, Cambria RP, Cutler BS, et al' Comparative early and late cardiac morbidity among patients requiring different vascular surgery procedures. J Vasc Surg 21:935-944, 1995
87 Hsla DC, Krushat WM, Moscoe LM Epidemlology of carotid endarterectomles among Medicare beneficiaries J Vasc Surg 16.201-208, 1992
88 Fisher ES, Malenka DJ, Solomon NA, et al' Risk of carotid endarterectomy in the elderly Am J Public Health 79"1617-1620, 1989
89 Pilcher DB, Davis JH, Ashikaga T, et al. Treatment of abdominal aortic aneurysm in an entire state over 71/z years. Am J Surg 139:487-494, 1980
90 Richardson JD, Mare KA: Repair of abdominal aortic aneurysms' A statewide experience Arch Surg 126:614-616, 1991
91 Hannan EL, Kflburn H Jr, O'Donnell JF, et al A longitudi- nal analys~s of the relationship between in-hospital mortality m New York State and the volume of abdominal aortic aneurysm surgeries performed Health Serv Res 27:517-542, 1992
92, Glllum RF. Peripheral arterial occlusive disease of the extremities in the United States Hospitahzation and mortality. Am Heart J 120(pt 1)'1414-1418, 1990
93 Chassln MR, Park RE, Lohr KN, et al: Differences among hospitals in Medicare patient mortality Health Serv Res 24 1-31, 1989
94. Hobson RW II, Weiss DG. Fields WS, et al' Efficacy of carotid endarterectomy for asymptomatlc carotid stenosis The Veterans Affairs Cooperative Study Group. N Engl J Med 328'221- 227, 1993
95 Fleisher LA, Barash PG' Preoperative cardiac evaluation for noncardiac surgery: A functional approach Anesth Analg 74"586- 598, 1992
96. Fletcher JP, Antlco VF, Gruenewald S, et al: Risk of aortic aneurysm surgery as assessed by preoperative gated heart pool scan Br J Surg 76 26-28, 1989
97 Pedersen T, Kelbaek H, Munck O. Cardlopulmonary comph- cations in high-risk surgical patients' The value of preoperative radionuclide cardiography Acta Anaestheslol Scand 34:183-189, 1990
98. Lazor L, Russell JC, DaSilva J, et al' Use ot the multiple uptake gated acquisition scan for the preoperatwe assessment of cardiac risk. Surg Gynecol Obstet 167.234-238, 1988
99 Pasternack PF. Imparato AM, Bear G, et al: The value of radaonuchde anglography as a predictor of perioperatwe myocar- dml infarction in patients undergoing abdominal aortic aneurysm resectmn J Vasc Surg 1 320-325, 1984
100 Mosley JG, Clarke JM, Ell PJ, et al. Assessment of myocardial funcnon before aortic surgery by radionuchde anglocar- dlography. Br J Surg 72.886-887, 1985
101. Pasternack PF, Imparato AM~ Riles TS, et al. The value of the radIonuclide anglogram in the prediction of perloperatwe myocardial Infarction in patients undergoing lower extremity revascularizatlon procedures Circulation 72(suppl 2, pt 2):I1-13-I1- 17, 1985
102. Kazmers A, Cerqueira MD, Zlerler RE' The role of preoperatwe radionuchde ejection fraction in direct abdominal aortic aneurysm repair J Vasc Surg 8:128-136, 1988
103 Flser WP, Thompson BW, Thompson AR, et al Nuclear cardiac election fraction and cardiac index in abdominal aortic surgery Surgery 94 736-739, 1983

ACC/AHA TASK FORCE REPORT 549
104 Hostetler MD, Dunn MI: Penoperatwe evaluation of a patient with abdominal aortic aneurysm. JAMA 269:295, 1993
105. Poldermans D, Fiorettl PM, Forster T, et al: Dobutamlne stress echocardiography for assessment of perloperatlve cardiac risk in patients undergoing major vascular surgery Circulation 87.1506-1512, 1993
106. McCabe CJ, Reldy NC, Abbott WM, et al. The value of electrocardiogram monitoring during treadmill testing for periph- eral vascular disease Surgery 89 183-186, 1981
107. Cutler BS, Wheeler HB, Paraskos JA, et al' Apphcabdity and Interpretation of electrocardiographic stress testing m patients with peripheral vascular disease Am J Surg 141 501-506, 1981
108. Arous EJ, Baum PL, Cutler BS" The ischemlc exercise test m patients with peripheral vascular disease: Imphcatlons for management Arch Surg 119 780-783, 1984
109, Gardlne RL, McBride K, Greenberg H, et al. The value of cardmc momtormg during peripheral arterial stress testing In the surgical management of peripheral vascular disease. J Cardmvasc Surg (Torino) 26:258-261, 1985
110. yon Knorrmg J, Lepantalo M. Prediction of penoperatlve cardiac complications by electrocar&ographac momtorlng during treadmill exercise testing before peripheral vascular surgery Sur- gery 99'610-613, 1986
111. Leppo J, Plaja J, Glonet M, et al Nomnvasive evaluation of cardiac risk before electwe vascular surgery J Am Coll Cardiol 9.269-276, 1987
112 Hanson P, Pease M, Berkoff H, et al' Arm exercise testing for coronary artery d~sease in patients with peripheral vascular disease Chn Cardlol 11:70-74, 1988
113 McPhall N, Calwn JE, Shariatmadar A, et al' The use of preoperative exerose testing to predict cardiac comphcatlons after arterial reconstruction J Vasc Surg 7 60-68, 1988
114. Carhner NH, Fisher ML, Plotnick GD, et al: Routine preoperatwe exercise testing in patients undergoing major noncar- diac surgery Am J Car&o156.51-58, 1985
115 Gerson MC, Hurst JM, Hertzberg VS, et al: Prediction of cardmc and pulmonary comphcatlons related to electwe abdominal and noncardmc thoracic surgery in geriatric patients. Am J Med 88'101-107, 1990
116 Kopecky SL, Gibbons RJ, Holher LH. Preoperatwe suplne exerose radlonuclide anglogram predicts perloperatlve car&ovas- cular events m vascular surgery. J Am Coil Cardml 7'226A, 1986
117. Urbmatl S, D1 Pasquale G, Andreoli A, et al: Preoperatwe nonlnvaswe coronary risk stratification in candidates for carotid endarterectomy Stroke 25.2022-2027, 1994
118. Chaaman BR" Exercise stress testing, m Braunwald E (ed). Heart Disease' A Textbook of Cardiovascular Me&one (ed 4) Phlladelphm, PA, Saunders, 1992, p 168
119 Boucher CA, Brewster DC, Darling RC, et al Determina- tion ol cardiac risk by dipyridamole-thalhum imaging before peripheral vascular surgery. N Engl J Med 312'389-394, 1985
120 Cutler BS, Leppo JA: Dipyrldamole thallium 20l scmtlgra- phy to detect coronary artery disease before abdominal aortic surgery. J Vasc Surg 5-91-100, 1987
121 Fletcher JP, Antlco VF, Gruenewald S, et al' Dlpyridamole- thalhurn scan for screening of coronary artery &sease prior to vascular surgery J Cardlovasc Surg (Tormo) 29"666-669, 1988
122 Sachs RN, Telher P. Larmlgnat P, et al Assessment by dlpyridamole-thallium-201 myocardml sclntlgraphy of coronary risk before peripheral vascular surgery. Surgery 103:584-587, 1988
123. McEnroe CS, O'Donnell RF Jr, Yeager A, et al Compari- son of ejection fraction and Goldman risk factor analysis of dlpyridamole-thalllum 201 stu&es in the evaluation of cardiac morbidity after aortic aneurysm surgery J Vasc Surg 11.497-504, 1990
124 Younls LT, Agulrre F, Byers S, et al. Perioperatwe and long-term prognostic value of intravenous dlpyrldamole thallium scintlgraphy in patients with peripheral vascular disease. Am Heart J 119'1287-1292, 1990
125. Mangano DT, London MJ, Tubau JF, et al. Dlpyrldamole thalhum-201 scintigraphy as a preoperative screening test' A reexamination of its predictive potential. Study of Perloperative Ischemia Research Group. Circulation 84'493-502, 1991
126. Strawn DJ, Guernsey JM. Dlpyrldamole thallium screening in the evaluation of coronary artery disease m elective abdommal aomc surgery. Arch Surg 126:880-884, 1991
127. Watters TA, Botvmlck EH, Dae MW, et al' Comparison of the findings on preoperatwe dlpyridamole perfuslon scmtlgraphy and lntraoperatlve transesophageal echocardlography: lmphca- tlons regarding the identification of myocardlum at ischemlc risk J Am Coil Cardxol 18 93-100, 199l
128 Hendel RC, Whltfield SS, Vlllegas BJ, et al: Prediction of late cardiac events by &pyrldamole thallium imaging In patients undergoing elective vascular surgery. Am J Car&ol 70"1243-1249, 1992
129. Lette J, Waters D, Cermo M, et al' Preoperatwe coronary artery disease risk stratification based on dlpyndamole imaging and a simple three-step, three-segment model for patients undergo- mg noncar&ac vascular surgery or major general surgery. Am J Cardlol 69 1553-1558, 1992
130 Madsen PV, VIssing M, Munck O, et al: A comparison of dlpyrldamole thallium 201 scintlgraphy and clinical examination m the determination of cardiac risk before arterial reconstruction. Anglology 43:306-311, 1992
13l Brown KA, Rowen M. Extent ofjeopar&zed viable myocar- dlum determined by myocardial perfuslon imaging best predicts perxoperative cardmc events in patients undergoing noncardlac surgery J Am Coll Car&o121.325-330, 1993
132. Kresowlk TF, Bower TR, Garner SA, et al. Dlpyndamole thallium imaging In patients being considered for vascular proce- dures Arch Surg 128.299-302, 1993
133 Baron JF, Mundler O, Bertrand M, et al Dlpyrldamole- thalhum scmtlgraphy and gated radlonuclide angiography to assess cardmc risk before abdominal aortic surgery. N Engl J Med 330 663-669, 1994
134 Bry JD, Belkm M, O'Donnell TF Jr, et al An assessment of the pOsltlve predlctwe value and cost-effectiveness of &pyrldamole myocardial scintigraphy in patients undergoing vascular surgery. J Vasc Surg 19:112-121, 1994
135 Camp AD, Garvln PJ, Hoff J, et al' Prognostic value of intravenous dlpyndamole thallium imaging in patients with diabe- tes mellltus considered for renal transplantation. Am J Cardlol 65 1459-1463, 1990
136 Iqbal A, Gibbons RJ, McGoon MD, et al: Nonlnvaswe assessment of cardiac risk in insuhn-dependent diabetic patients being evaluated for pancreatic transplantation using thallium-201 myocardial perfusion sclntlgraphy. Transplant Proc 23(pt 2) 1690- 1691, 1991
137 Coley CM, Field TS, Abraham SA, et al. Usefulness of dlpyndamole-thalhum scanning for preoperatwe evaluation of cardiac risk for nonvascular surgery. Am J Cardlol 69 1280-1285, 1992
138, Shaw L, Miller DD, Kong BA, et al Determination of perloperatlve cardiac risk by adenosine thalhum-201 myocardial imaging Am Heart J 124:861-869, 1992
139. Takase B, Younis LT, Byers SL, et al' Comparative prognostic value of clinical risk indexes, restmg two-dlmenslonal echocardlography, and dlpyrldamole stress thallium-201 myocar- dial imaging for perioperatlve cardmc events in major nonvascular surgery patients. Am Heart J 126:1099-1106, 1993

550 ACC/AHA TASK FORCE REPORT
140 Youms L, Stratmann H, Takase B, et al: Preoperatwe climcal assessment and dipyrldamole thallium-201 scintigraphy for prediction and prevention of cardmc events in patients having major noncardlovascular surgery and known or suspected coronary artery disease. Am J Cardio174"311-317, 1994
141. Ritchie JL, Bateman TM, Bonow RO, et al" Guidehnes for chnical use of cardiac radionuclide lmagmg: A report of the American College of Cardiology/American Heart Association Task Force on Assessment of DmgnosUc and Therapeutic Cardio- vascular Procedures (Committee on Radionuclide Imagmg), devel- oped m collaboration with the American Society of Nuclear Cardiology. J Am Coll Cardio125:521-547, 1995
142. Berthe C, Plerard LA, Hiernaux M, et al' Predicting the extent and location of coronary artery disease m acute myocardial infarction by echocardlography during dobutamme infusion. Am J Cardlo158:1167-1172, 1986
143. Cohen JL, Greene TO, Ottenweller J, et al Dobutamlne digital echocardiography for detecting coronary artery disease Am J Cardlo167:1311-1318, 1991
144. Sawada SG, Segar DS, Ryan T, et al: Echocardiographlc detection of coronary artery disease durmg dobutamine infusion Circulation 83:1605-1614, 1991
145. Martin TW, Seaworth JF, Johns JP, et al' Comparison of adenosine, dipyridamole, and dobutamine in stress echocardlogra- phy. Ann Intern Med 116:190-196, 1992
146. Marwick T, Willemart B, D'Hondt AM, et al' Selection of the optimal nonexerose stress for the evaluation of lschemlc regional myocardial dysfunction and malperfusion: comparison of dobutamine and adenosine using echocardlography and 99mTc- MIBI single photon emission computed tomography. Circulation 87:345-354, 1993
147. Lane RT, Sawada SG, Segar DS, et al: Dobutamine stress echocardiography for assessment of cardiac risk before noncardlac surgery Am J Cardlo168:976-977, 1991
148. Lalka SG, Sawada SG, Dalsing MC, et al: Dobutamine stress echocardlography as a predictor of cardiac events associated with aortic surgery. J Vasc Surg 15:831-840, 1992
149 Elchelberger JP, Schwarz KQ, Black ER, et al' Predictive value of dobutamine echocardlography just before non-cardiac vascular surgery. Am J Cardio172:602-607, 1993
150 Langan EM III, Youkey JR, Franklin DP, et al: Dobuta- mine stress echocardlography for cardiac rtsk assessment before aortic surgery J Vasc Surg 18'905-911, 1993
151. Dfivila-Rom~in VG, Waggoner AD, Slcard GA, et al: Dobutamine stress echocardlography predicts surgical outcome in patients with an aortic aneurysm and peripheral vascular disease. J Am Coll Cardio121'957-963, 1993
152. DePuey EG, Guertler-Krawczynska E, Robbins WL: Thai- hum-201 SPECT in coronary artery disease patients with left bundle branch block. J Nucl Med 29'1479-1485, 1988
153. Larcos G, Gibbons RJ, Brown ML: Dmgnostlc accuracy of exercise thalhum-201 single-photon emission computed tomogra- phy in patients with left bundle branch block. Am J Cardlol 68:756-760, 1991
154. Rockett JF, Wood WC, Moinuddm M, et al: Intravenous dlpyrldamole thalhum-201 SPECT imaging in patients with left bundle branch block Chn Nucl Med 15:401-407, 1990
155. O'Keefe JH Jr, Bateman TM, Barnhart CS. Adenosine thallium-201 is superior to exercise thallium-201 for detecting coronary artery disease m patients with left bundle branch block. J Am Coil Cardio121:1332-1338, 1993
156. Hirzel HO, Senn M, Nuesch K, et al: ThaUium-201 scintig- raphy in complete left bundle branch block Am J Cardlol 53 764- 769, 1984
157. Tighe DA, Hutchinson HG, Park CH, et al: False-positwe
reversible perfusion defect during dobutamine-thalhum imaging in left bundle branch block J Nucl Med 35:1989-1991, 1994
158. Flelsher LA, Rosenbaum SH, Nelson AIt, et al: The predictive value of preoperatwe sdent ischemla for postoperatwe lschemlc eardmc events in vascular and nonvascular surgery pa- tients. Am Heart J 122(pt 1):980-986, 1991
159. Kirwin JD, Ascer E, Gennaro M, et al' Sdent myocardial lschemia is not predictwe of myocardial infarction m peripheral vascular surgery patients. Ann Vasc Surg 7:27-32, 1993
160. McPhail NV, Ruddy TD, Barber GG, et al' Cardiac risk stratification using dipyndamole myocardial perfuslon imaging and ambulatory ECG monitormg prior to vascular surgery Eur J Vasc Surg 7:151-155, 1993
161. Raby KE, Goldman L, Creager MA, et al Correlation between preoperative lschemia and major cardiac events after peripheral vascular surgery. N Engl J Med 321:1296-1300, 1989
162. Pasternack PF, Grossl EA, Baumann FG, et al: The value of silent myocardial lschemia momtorlng in the prediction of penoperatwe myocardial infarction in patients undergoing periph- eral vascular surgery J Vasc Surg 10:617-625, 1989
163. Flelsher LA, Rosenbaum SH, Nelson, et al: Preoperative dlpyridamole thallium imaging and Holter monitoring as a predic- tor of perioperatwe cardiac events and long term outcome. Anesthesiology (m press)
164. Mantha S, Rolzen MF, Barnard J, et al. Relatwe effective- ness of tour preoperative tests for predicting adverse cardiac outcomes after vascular surgery: A meta-analysls. Anesth Analg 79'422-433, 1994
165 Cambria RP, Brewster DC, Abbott WM, et al The impact of selective use of dlpyndamole-thallium scans and surgical factors on the current morbidity of aortic surgery J Vasc Surg 15:43-51, 1992
166. Rlhal CS, Eagle KA, Mlckel MC, et al' Surgical therapy for coronary artery disease among patients with combined coronary artery and peripheral vascular disease. Circulation 91:46-53, 1995
167 Coley CM, Eagle KA, Singer DE, et al: Decision analysis for preoperative cardiac risk evaluation before vascular surgery Chn Res 35'342A, 1987
168. Flelsher LA, Skolmck ED, Holroyd KJ, et al: Coronary artery revascularlzation before abdominal aortic aneurysm surgery a decision analytic approach. Anesth Analg 79:661-669, 1994
169. Mason JJ, Owens DK, Harris RA, et al: The role of coronary angiography and coronary revascularization before non- cardmc vascular surgery. JAMA 273.1919-1925, 1995
170. Dlehl JT, Cali RF, Hertzer NR, et al: Complications of abdominal aortic reconstruction: An analysis of penoperatwe risk factors in 557 patients. Ann Surg 197.49-56, 1983
171. Crawford ES, Morris GC Jr, Howell JF, et al Operatwe risk in patients with prevmus coronary artery bypass. Ann Thorac Surg 26:215-221, 1978
172. Reul GJ Jr, Cooley DA, Duncan JM, et al: The effect of coronary bypass on the outcome of peripheral vascular operations m 1093 patients J Vasc Surg 3 788-798, 1986
173. Nielsen JL, Page CP, Mann C, et al: Risk of major elective operation after myocardial revasculanzatlon. Am J Surg 164:423- 426, 1992
174. Hertzer NR, Beven EG, Young JR, et al' Coronary artery disease m peripheral vascular patients: a classification of 1000 coronary anglograms and results of surgical management. Ann Surg 199:223-233, 1984
175. Hertzer NR, Young JR, Beven EG, et al. Late results of coronary bypass in patients with peripheral vascular disease, I: Five-year survival according to age and clinical cardmc status Cleve Chn Q 53:133-143, 1986
176 European Coronary Surgery Study Group' Long-term re-

ACC/AHA TASK FORCE REPORT 551
suits of prospective randomised study of coronary artery bypass surgery in stable angina pectoris. Lancet 2:1173-1180, 1982
177 Hertzer NR, Young JR, Beven EG, et al: Late results of coronary bypass in patients with peripheral vascular disease, II: Fwe-year survival according to sex, hypertension, and diabetes. Cleve Clin J Med 54:15-23, 1987
178. Guidelines and indications for coronary artery bypass graft surgery: A report of the American College of Cardiology/ American Heart Association Task Force on Assessment of Dmgnos- tic and Therapeutic Cardiovascular Procedures (Subcommittee on Coronary Artery Bypass Graft Surgery). J Am Coll Cardiol 17"543-589, 1991
179 Huber KC, Evans MA, Bresnahan JF, et al Outcome of noncardlac operations in patients with severe coronary artery disease successfully treated preoperatively with coronary angIo- plasty Mayo Clin Proc 67:15-21, 1992
180. Elmore JR, HaUett JW Jr, Gibbons RJ, et al Myocardial revascularization before abdominal aomc aneurysmorrhaphy- Ef- fect of coronary angioplasty. Mayo Clin Proc 68"637-641, 1993
181 Allen JR, Helhng TS, Hartzler GO: Operatwe procedures not involving the heart after percutaneous transluminal coronary angioplasty. Surg Gynecol Obstet 173"285-288, 1991
182. Guidelines for percutaneous transluminal coronary anglo- plasty: A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Committee on Percutaue- ous Transluminal Coronary Angioplasty). J Am Coil Cardiol 22:2033-2054, 1993
183. Corlat P, Daloz M, Bousseau D, et al' Prevention of intraoperatwe myocardial lschemm during noncardiac surgery with intravenous nitroglycerin. Anesthesiology 61.193-196, 1984
184 Dodds TM, Stone JG, Coromilas J, et al" Prophylactic mtroglycerln infusion during noncardiac surgery does not reduce perioperatwe lschemla. Anesth Analg 76 705-713, 1993
185 Godet G, Coriat P, Baron JF, et al: Prevention of intraop- eratwe myocardial lschemia during noncardiac surgery with intra- venous dlltlazem: A randomized trial versus placebo Anesthesiol- ogy 66:241-245, 1987
186 Pasternack PF, Imparato AM, Baumann FG, et al' The hemodynamics of beta-blockade in patients undergoing abdominal aortic aneurysm repair Circulation 76:1II-1-111-7, 1987 (suppl 3)
187. Hayes SN, Holmes DR Jr, Nishimura RA, et al. Palliative percutaneous aortic balloon valvuloplasty before noncardlac opera- tions and lnvaswe dmgnostlc procedures. Mayo Clin Proc 64'753- 757, 1989
188 Rahlmtoola SH" Catheter balloon valvuloplasty of aortic and mltral stenosis in adults. Circulation 75:895-901, 1987
189 Marcus FI, Ewy GA, O'Rourke RA, et al: The effect of pregnancy on the murmurs of mltral and aortic regurgitation. Orculation 41'795-805, 1970
190. Waller TJ, Kay HR, Spielman SR, et al. Reduction in sudden death and total mortality by antiarrhythmlc therapy evalu- ated by electrophyslologic drug testing criteria of efficacy in patients with sustamed ventricular tachyarrhythmla. J Am Coll Cardlol 10:83-89, 1987
191 Swerdlow CD, Wmkle RA, Mason JW. Prognostic signifi- cance of the number of induced ventricular complexes during assessment of therapy for ventricular tachyarrhythmms Circula- tion 68.400-405. 1983
192. Guidelines for implantation of cardiac pacemakers and antlarrhythmia devices. A report of the American College of Cardiology/American Heart Association Task Force on Assess- ment of Diagnostm and Therapeutic Cardiovascular Procedures (Committee on Pacemaker Implantation). J Am Coll Cardlol 18 1-13, 1991
193. Berlauk JF, Abrams JH, Gilmour IJ, et al: Preoperatwe optimization of cardiovascular hemodynam]cs improves outcome in peripheral vascular surgery: A prospective, randomized clinical trial. Ann Surg 214 289-297, 1991
194. Clagett GP, Anderson FA Jr, Levine MN, et al: Prevention of venous thromboembohsm Chest 102'391S-407S, 1992 (suppl 4)
195. Verstraete M" The diagnosis and treatment of deep-vein thrombosis. N Engl J Med 329"1418-1420, 1993 (Editorial com- ment)
196. Mohr DN, SIlversteln MD, Ilstrup DM, et al' Venous thromboembohsm associated with hip and knee arthroplasty' current prophylactic practices and outcomes Mayo Chn Proc 67'861-870, 1992
197. Heljboer H, Cogo A, Buller HR, et al: Detection of deep vein thrombosis with impedance plethysmography and real-time compression ultrasonography in hospitalized patients. Arch Intern Med 152:1901-1903, 1992
198. Moser KM, Fedullo PF' The diagnosis of deep vein thrombosis. N Engl J Med 330:863-864, 1994 (letter)
199. Bergqvist D, Jendteg S, Llndgren B, et al The economics of general thromboembohc prophylaxis. World J Surg 12:349-355, 1988
200 Crlqui MH, Fronek A, Barrett-Connor E, et al: The prevalence of peripheral arterial disease in a defined population. Circulation 71'510-515, 1985
201. Friedman SA, Pandya M, Grelf E. Peripheral arterial occlusion in patients with acute coronary heart disease. Am Heart J 86:415-419, 1973
202 Cohen MM, Duncan PG, Tate RB: Does anesthesia contribute to operative mortality? JAMA 260"2859-2863, 1988
203. Leung JM, Goehner P, O'Kelly BF, et al. Isoflurane anesthesia and myocardial ischemla: comparative risk versus sufen- tani1 anesthesia in patients undergoing coronary artery bypass graft surgery. The SPI (Study of Perloperative Ischemia) Research Group. Anesthesiology 74 838-847, 1991
204 Baron JF, Bertrand M, Barre E, et al" Combined epldural and general anesthesia versus general anesthesia for abdominal aortic surgery. Anesthesiology 75'611-618, 1991
205. Christopherson R, Beattie C, Frank SM, et al' Periopera- tive morbidity In patients randomized to epidural or general anesthesia for lower extremity vascular surgery: Perloperatwe Ischemla Randomized Anesthesia Trial Study Group Anesthesiol- ogy 79.422-434, 1993
206. Slogoff S, Keats AS Randomized trial of primary anes- thetic agents on outcome of coronary artery bypass operations Anesthesiology 70 179-188, 1989
207. Tuman K J, McCarthy R J, Spiess BD Epidural anaesthesia and analgesia decreases postoperative hypercoagulabihty in high- risk vascular patients Anesth Analg 70 $414, 1990
208. Gallagber JD, Moore RA, Jose AB, et al" Prophylactic nitroglycerin infusions during coronary artery bypass surgery Anesthesiology 64"785-789, 1986
209. Thomson IR, Mutch WA, Culligan JD Failure of Intrave- nous mtroglycerln to prevent Intraoperatwe myocardial lschemia during fentanyl-pancuronmm anesthesm Anesthesiology 61:385- 393, 1984
210. Elsenberg M J, London MJ, Leung JM, et al" Monitoring for myocardial ischemia during noncardlac surgery A technology assessment of transesophageal ecbocardiography and 12-lead elec- trocardiography. The Study of Perioperatlve Ischemia Research Group JAMA 268:210-216, 1992
211 London MJ, Tubau JF, Wong MG, et al: The natural history of segmental wall motion abnormahtles In patients undergo- Ing noncardiac surgery- SPI Research Group. Anesthesiology 73'644-655, 1990

552 ACC/AHA TASK FORCE REPORT
212. SIu SC, Kowalchuk G J, Welty FK, et al: Intraaortlc balloon counterpulsation support in the high-risk cardiac patient undergo- ing urgent noncardlac surgery. Chest 99:1342-1345, 1991
213. Grotz RL, Yeston NS: Intra-aortic balloon counterpulsa- tion in high-risk cardiac patients undergoing noncardiac surgery. Surgery 106:1-5, 1989
214. Mangano DT, Browner WS, Hollenberg M, et al: Long- term cardiac prognosis following noncardiac surgery' The Study of Perioperative Ischemla Research Group. JAMA 268'233-239, 1992
215. Yeager RA, Moneta GL, Edwards JM, et al' Late survwal after perioperative myocardial Infarction complicating vascular surgery J Vasc Surg 20:598-606, 1994
216 Isaacson IJ, Lowdon JD, Berry AJ, et al: The value of pulmonary artery and central venous monitoring In patients under- going abdominal aortic reconstructwe surgery: a comparatwe study of two selected, randomized groups. J Vasc Surg 12'754-760, 1990
217. Joyce WP, Provan JL, Ameh FM, et al: The role of central haemodynamlc monitoring in abdominal aortic surgery: A prospec- tive randomlsed study. Eur J Vasc Surg 4"633-636, 1990
218. Practice guidelines for pulmonary artery catheterization: A report by the American Society of Anesthesiologists Task Force on Pulmonary Artery Catheterization. Anesthesiology 78:380-394, 1993
219. Landesberg G, Luria MH, Cotev S, et al' Importance of long-duration postoperatwe ST-segment depression in cardiac morbidity after vascular surgery. Lancet 341:715-719, 1993
220. Fleisher LA, Nelson AH, Rosenbaum SH. Postoperative myocardial ischemia, etiology of cardiac morbidity or manlfesta- tlon of underlying &sease? J Chn Anesth 7:97-102, 1995
221 Mathew JP, Fleisher LA, Rinehouse JA, et al: ST segment depression during labor and delivery. Anesthesiology 77'635-641, 1992
222 Breslow MJ, Miller CF, Parker SD, et al: Changes In T-wave morphology following anesthesia and surgery: A common recovery-room phenomenon. Anesthesiology 64:398-402, 1986
223. Adams JE III, Sicard GA, Allen BT, et al: Diagnosis of perioperative myocardial infarction with measurement of cardiac troponin I. N Engl J Med 330'670-674, 1994
224. Charlson ME, MacKenzie CR, Ales K, et al: Surveillance for postoperative myocardial infarction after noncardiac opera- tions. Surg Gynecol Obstet 167:404-414, 1988
225. Rettke SR. Shub C, Naessens JM, et al: Significance of mildly elevated creatine kinase (myocardial band) activity after electwe abdominal aortic aneurysmectomy. J Cardiothorac Vasc Anesth 5:425-430, 1991
226. Nordrehaug JE' Malignant arrhythrnla in relation to serum potassium in acute myocardial infarction. Am J Cardiol 56.20D- 23D, 1985
227. Hollifield JW: Thiazlde treatment of systemic hyperten- sion: Effects on serum magnesium and ventricular ectopic activity. Am J Cardio163:22G-25G, 1989
228 Wong KC, Schafer PG, Schultz JR: Hypokalemia and anesthetic implications. Anesth Analg 77:1238-1260, 1993
229. Summary of the second report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evalua- tion, and Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel II). JAMA 269'3015-3023, 1993
Related Documents