Massachusetts Patient-Centered Medical Home Initiative (MA PCMHI): Impact on Clinical Quality at 30 Months Judith Steinberg, M.D., M.P.H. Sai Cherala, M.D., M.P.H. Ann Lawthers, S.M., Sc.D. Christine Johnson, Ph.D. Commonwealth Medicine UMass Medical School

Academy Health-Annual Research Meeting Presentation
Jul 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Massachusetts Patient-Centered Medical Home Initiative (MA PCMHI): Impact on Clinical Quality at 30 Months
Judith Steinberg, M.D., M.P.H.Sai Cherala, M.D., M.P.H. Ann Lawthers, S.M., Sc.D. Christine Johnson, Ph.D.
Commonwealth Medicine UMass Medical School
Introduction The Patient‐Centered Medical Home (PCMH) offers an
innovative model of care: comprehensive primary care, quality improvement, care management, and enhanced access in a patient centered environment
PCMH evaluations have shown variable impact
Aims:
To assess data trends of clinical quality measures from participating practices in the Massachusetts Patient-Centered Medical Home Initiative
To evaluate practice and staff level factors that may impact clinical quality performance

Background: Massachusetts Patient Centered Medical Home Initiative
Multi-payer, statewide initiative
Sponsored by Massachusetts Health & Human Services; legislatively mandated
46 participating practices
3-year demonstration: March, 2011 − March, 2014
Includes payment reform and technical assistance

MA PCMHI Evaluation Questions
Question 1:
To what extent and how do practices become medical homes?
• Extent
• Patient-family centeredness
• Care management
• Care coordination
• Access
• Teamwork
• Information technology
• Leadership
• Barriers and Facilitators
Question 2:
To what extent do patients become partners in their health care?
•Perceived self-management efficacy
•Patient-family centeredness by chronic and non-chronic
Question 3:
What is the initiative’s impact on utilization, cost, clinical quality, patient and provider outcomes?
•Emergency Department use
•Hospitalizations
•Cost
•Clinical quality measures
•Staff satisfaction
•Patient satisfaction
Methods
Design: Quality improvement study using practices’ self-reported monthly data on 22 clinical quality measures from June 2011 through February 2014
Methods
Linear Mixed Model
Analysis
Data were divided into three-month periods:
Time 1 (June – August, 2011) ... to Time 11 (December, 2013 – February, 2014)
Analysis of Change over Time: Baseline (Time 1 or Time 2 or Time 6) vs. Time 11

Clinical Quality MeasuresAdult Diabetes
HbgA1c Control (<8%) HbgA1c Control (>9%) BP < 140/90 mmHg LDL Control < 100mg/dL Screened for Depression Self-Management Goal
Adult Prevention Adult Weight Screening and
Follow-up Tobacco Use Assessment Tobacco Cessation Intervention
Other Adult Target Blood Pressure Control Hypertension with Documented
Self-Management Goal Depression with Documented
PHQ-9 Score Depression with Documented Self-
Management Goal
Childhood Prevention Immunization Status Multiple
vaccines Weight Assessment and Counseling
for Children and Adolescents
Pediatric Asthma Use of Appropriate Medications for
Asthma Persistent Asthma Patients with
Action Plan
Other Pediatric Target Follow-up Care for Children
Prescribed ADHD Medication Management Plan for Children
Prescribed ADHD Medication
Care Coordination/ Care Management Follow-up after Hospital Discharge Highest Risk Patients with Care Plan

Results: Study Participants Practice Characteristics Percentage
Geography
Rural (<10,000 town population) 9%
Suburban (Between 10,000 and 50,000) 20%
Urban (>= 50,000) 71%
Practice Size (Based on Number of Full Time Practitioners)
Small (< 6 FTE practitioners) 31%
Medium (Between 6 and 11 FTE practitioners) 29%
Large (> 11 FTE practitioners) 40%
Type of Practice
Community Health Center 56%
Residency or Academic Practice 11%
Group Practice 29%
Solo Practice 4%
Payer Mix (Practices with Financial Incentives N=31)
Commercial 12%
Health Safety Net 15%
Medicaid 72%
Medicare 1%
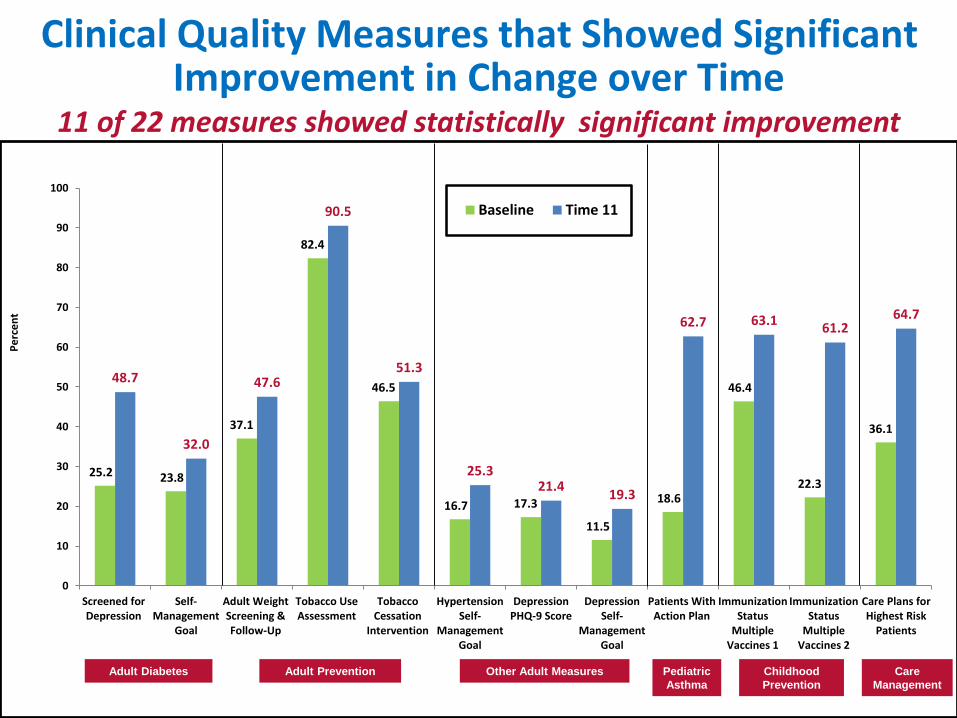
Clinical Quality Measures that Showed Significant Improvement in Change over Time
25.2 23.8
37.1
82.4
46.5
16.7 17.3
11.5
18.6
46.4
22.3
36.1
48.7
32.0
47.6
90.5
51.3
25.321.4
19.3
62.7 63.161.2
64.7
0
10
20
30
40
50
60
70
80
90
100
Screened forDepression
Self-Management
Goal
Adult WeightScreening &Follow-Up
Tobacco UseAssessment
TobaccoCessation
Intervention
HypertensionSelf-
ManagementGoal
DepressionPHQ-9 Score
DepressionSelf-
ManagementGoal
Patients WithAction Plan
ImmunizationStatus
MultipleVaccines 1
ImmunizationStatus
MultipleVaccines 2
Care Plans forHighest Risk
Patients
Pe
rce
nt
Baseline Time 11
11 of 22 measures showed statistically significant improvement
Adult Diabetes Adult Prevention Other Adult Measures Pediatric
Asthma
Childhood
Prevention
Care
Management

Values met the study’s definition of statistical significance p<.05.
Care Coordination/Care Management Measures: Change over Time
63.3
36.1
66.5 64.7
0
10
20
30
40
50
60
70
Follow-Up After Hospital Discharge Care Plans for Highest Risk Patients
Ave
rage
Rat
e
Measures
Baseline Time 11

Drilling Deeper on Change: Methods
Correlation analysis
Variables included: Performance on clinical measures in the last three months, change in clinical performance over the demonstration, practice characteristics and staff perceptions/attitudes towards the change
Data sources: Clinical data submission, Medical Home Implementation Quotient (MHIQ), staff survey

Results of Correlation Analysis: Care Plan for Highest Risk Patients
Change over Three Years Performance in Last Three Months
Leadership at Baseline(staff survey) (r=0.42, p=0.01)
Leadership at Baseline(staff survey) (r=0.45, p=0.009)
Strong team(staff survey) (r=0.41, p=0.01)
Quality improvement culture at Baseline(staff survey) (r=0.39, p=0.02)
Quality improvement culture at Baseline(staff survey) (r=0.36, p=0.04)
Strong team(staff survey) (r=0.32, p=0.05)
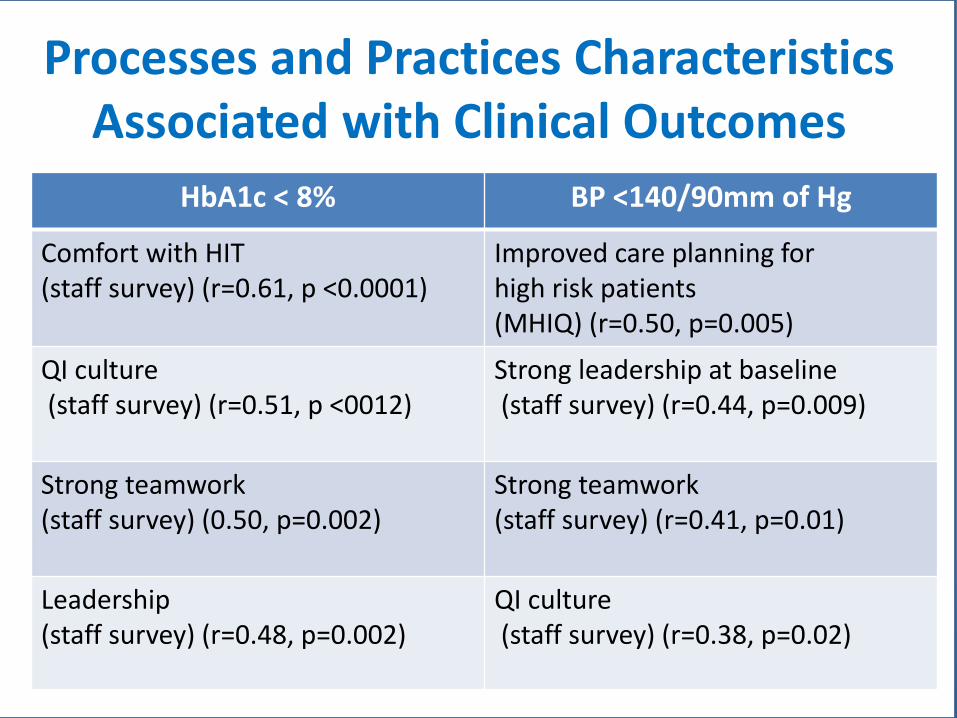
Processes and Practices Characteristics Associated with Clinical Outcomes
HbA1c < 8% BP <140/90mm of Hg
Comfort with HIT (staff survey) (r=0.61, p <0.0001)
Improved care planning for high risk patients (MHIQ) (r=0.50, p=0.005)
QI culture(staff survey) (r=0.51, p <0012)
Strong leadership at baseline(staff survey) (r=0.44, p=0.009)
Strong teamwork (staff survey) (0.50, p=0.002)
Strong teamwork(staff survey) (r=0.41, p=0.01)
Leadership (staff survey) (r=0.48, p=0.002)
QI culture(staff survey) (r=0.38, p=0.02)

Quality Improvement Study
No Comparison Group
Small Sample Size
Correlation Analysis
Limitations
At the close of the MA PCMHI initiative (3 years), 11 of 22 clinical measures showed statistically significant improvement
Measures that showed significant improvement: Process measures
New or newly documented processes
A solid practice QI culture, leadership and strong team functioning were positively correlated with performance and improvement in high risk care planning
Factors that correlated with performance on clinical outcome measures were: QI culture, strong leadership and teamwork, comfort with HIT
Summary

Conclusion and Implications for Policy and Practice
Quality of care in the management of chronic diseases, prevention and screening, and high risk care management was significantly improved in this PCMH demonstration that had a preponderance of safety net practices
Implementation of foundational elements of the PCMH − QI, leadership engagement, teamwork and HIT − may foster improvement in clinical quality
Understanding factors that are correlated with clinical performance can focus transformation efforts
Acknowledgments
We would like to acknowledge the Massachusetts Executive Office of Health and Human Services (EOHHS), the MA PCMHI Leadership and Medical Home Facilitator Teams, as well as MA PCMHI participating practices without whom this work would not be possible.
Contact Information:
Judith Steinberg, M.D., M.P.H.Deputy Chief Medical OfficerCommonwealth MedicineUMass Medical [email protected]
Sai Cherala, M.D., M.P.H.Senior Clinical AnalystCommonwealth MedicineUMass Medical [email protected]
Related Documents