PAIN MEDICINE Volume 4 • Number 1 • 2003 ABSTRACTS 19 TH ANNUAL AAPM MEETING ABSTRACTS © American Academy of Pain Medicine 1526-2375/03/$15.00/91 91–112 500 Clinical A Case Report of Pulsed Radiofrequency Lesioning for Greater Occipital Neuralgia Annu Navani, MD, Paul Kreis, MD, Gagan Mahajan, MD, Scott M. Fishman, MD Division of Pain Medicine, University of California, Davis Introduction: Greater occipital nerve blockade (GONB) utilizing local anesthetic and/or steroid has been safely and successfully performed to manage greater occipital neuralgia (GON). We report a case of occipital neuralgia where pulsed radiofrequency lesioning (RFL) of the greater occipital nerve (GON) was used to achieve long- term pain relief. Case Study: A sixty-two year old male with a forty-three year history of left suboccipital pain, which was suboptimally relieved with naproxen, a TENS unit and GONB with local anesthetic and steroid, under- went pulsed RFL (20 ms bursts in intervals of 0.5 seconds for four minutes at 42°C) of the left GON. After obtaining 70% pain relief lasting for four months, pulsed RFL was repeated and resulted in 70% pain relief lasting for 5 months. Discussion: GONB with local anesthetic has been proposed to reduce the pool of exaggerated sensory input and antagonize the putative “wind-up-like effect” felt to be responsible for inducing occipital neuralgia. 1 Continuous RFL of the GON at 90°C for 90–120 seconds has been described in the treatment of occipital neuralgia to offer atleast 6 months of pain relief. 2 We consider pulsed RFL an alternative to continuous RFL with the proposed advantage of mitigating pain, as in continous RFL, but without the potential risk of deafferentation pain associ- ated with neurolytic procedures. While placebo and other non-specific analgesic effects cannot be ruled out, the apparent safety profile and potential efficacy of pulsed RFL makes it a compelling option to consider before irre- versible neuroablative therapies are applied. References 1 Vincent MB, et al. Arq Neuropsiquiatr 1998;56(4): 720–5. 2 Blume H et al. Eds. Updating in Headache. Berlin: Springer Verlag, 1985:17–23. 501 Research (Clinical) A Comparison of Outcomes Using the Treatment Outcomes in Pain Survey (TOPS) Between Patients with Cancer-related Pain and Chronic Nonmalignant Pain Rosemary C. Polomano,Vitaly Gordin, Harold A. Harvey, and Fredrick K. Orkin, Milton S. Hershey Medical Center, Penn State University College of Medicine; Hershey, Pennsylvania Treatment Outcomes in Pain Survey (TOPS) is a comprehensive, multidimensional tool developed at New England Medical Center to measure physical and psychosocial outcomes associated with chronic nonma- lignant pain (CNMP). 1,2 TOPS comprises 8 subscales derived from SF-36 Health Survey and 14 TOPS domains. TOPS was administered to 52 outpatients from our oncology clinic with advanced cancer reporting average pain >3 (0–10 Scale) and compared their results to TOPS data collected from 94 patients with CNMP referred to our Pain Management Clinic. Internal con- sistency reliability (Cronbach’s alpha) was calculated for each of the 8 SF-36 subscales separately for each group: SF-36 subscales had reliability coefficients ≥0.70 and were similar for most subscales, with differences between groups <0.12. Social Functioning was the lowest for the cancer group, 0.70. TOPS domains also demonstrated acceptable reliability for both groups, except for Passive Coping (0.62, cancer group; 0.77, CNMP). Scores from SF-36 subscales and TOPS domains were compared (Student’s t-test). Cancer group had less Body Pain (p < 0.001) but poorer General Health (p < 0.01). For TOPS domains, cancer group reported better percep- tions of Health Care Satisfaction (p < 0.01) and Work Limitations (p < 0.05), less Total Pain Experience (p < 0.05), and poorer perceptions in Solicitous Response (p < 0.001), a measure of extent to which a significant other assumes role functions. Mean score for Perceived Family, 1 Rogers WH, et al. Using the “TOPS,” an outcome instrument for multidisciplinary outpatient pain treatment. Pain Med 2001;1:55–67. 2 Rogers WH, et al. Assessing individual outcomes during outpatient multidisciplinary chronic pain treatment by means of an augmented SF-36. Pain Med 2001;1:44–54. Downloaded from https://academic.oup.com/painmedicine/article/4/1/91/1816761 by guest on 30 May 2022

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PAIN MEDICINEVolume 4 • Number 1 • 2003
ABSTRACTS
19TH ANNUAL AAPM MEETING ABSTRACTS
© American Academy of Pain Medicine 1526-2375/03/$15.00/91 91–112
500Clinical
A Case Report of Pulsed RadiofrequencyLesioning for Greater Occipital Neuralgia
Annu Navani, MD, Paul Kreis, MD, Gagan Mahajan,MD, Scott M. Fishman, MD Division of PainMedicine, University of California, DavisIntroduction: Greater occipital nerve blockade (GONB)utilizing local anesthetic and/or steroid has been safely andsuccessfully performed to manage greater occipital neuralgia (GON). We report a case of occipital neuralgiawhere pulsed radiofrequency lesioning (RFL) of thegreater occipital nerve (GON) was used to achieve long-term pain relief. Case Study: A sixty-two year old malewith a forty-three year history of left suboccipital pain,which was suboptimally relieved with naproxen, a TENSunit and GONB with local anesthetic and steroid, under-went pulsed RFL (20 ms bursts in intervals of 0.5 secondsfor four minutes at 42°C) of the left GON. After obtaining70% pain relief lasting for four months, pulsed RFL was repeated and resulted in 70% pain relief lasting for 5 months. Discussion: GONB with local anesthetic hasbeen proposed to reduce the pool of exaggerated sensoryinput and antagonize the putative “wind-up-like effect”felt to be responsible for inducing occipital neuralgia.1
Continuous RFL of the GON at 90°C for 90–120 secondshas been described in the treatment of occipital neuralgiato offer atleast 6 months of pain relief.2 We consider pulsedRFL an alternative to continuous RFL with the proposedadvantage of mitigating pain, as in continous RFL, butwithout the potential risk of deafferentation pain associ-ated with neurolytic procedures. While placebo and othernon-specific analgesic effects cannot be ruled out, theapparent safety profile and potential efficacy of pulsedRFL makes it a compelling option to consider before irre-versible neuroablative therapies are applied.
References
1 Vincent MB, et al. Arq Neuropsiquiatr 1998;56(4):720–5.
2 Blume H et al. Eds. Updating in Headache. Berlin:Springer Verlag, 1985:17–23.
501Research (Clinical)
A Comparison of Outcomes Using the TreatmentOutcomes in Pain Survey (TOPS) Between Patientswith Cancer-related Pain and ChronicNonmalignant Pain
Rosemary C. Polomano,Vitaly Gordin, Harold A.Harvey, and Fredrick K. Orkin, Milton S. HersheyMedical Center, Penn State University College ofMedicine; Hershey, PennsylvaniaTreatment Outcomes in Pain Survey (TOPS) is a comprehensive, multidimensional tool developed at NewEngland Medical Center to measure physical and psychosocial outcomes associated with chronic nonma-lignant pain (CNMP).1,2 TOPS comprises 8 subscalesderived from SF-36 Health Survey and 14 TOPSdomains. TOPS was administered to 52 outpatients from our oncology clinic with advanced cancer reportingaverage pain >3 (0–10 Scale) and compared their resultsto TOPS data collected from 94 patients with CNMPreferred to our Pain Management Clinic. Internal con-sistency reliability (Cronbach’s alpha) was calculated foreach of the 8 SF-36 subscales separately for each group:SF-36 subscales had reliability coefficients ≥0.70 andwere similar for most subscales, with differences betweengroups <0.12. Social Functioning was the lowest for thecancer group, 0.70. TOPS domains also demonstratedacceptable reliability for both groups, except for PassiveCoping (0.62, cancer group; 0.77, CNMP). Scores fromSF-36 subscales and TOPS domains were compared(Student’s t-test). Cancer group had less Body Pain (p < 0.001) but poorer General Health (p < 0.01). ForTOPS domains, cancer group reported better percep-tions of Health Care Satisfaction (p < 0.01) and WorkLimitations (p < 0.05), less Total Pain Experience (p <0.05), and poorer perceptions in Solicitous Response (p< 0.001), a measure of extent to which a significant otherassumes role functions. Mean score for Perceived Family,
1 Rogers WH, et al. Using the “TOPS,” an outcomeinstrument for multidisciplinary outpatient pain treatment.Pain Med 2001;1:55–67.2 Rogers WH, et al. Assessing individual outcomes duringoutpatient multidisciplinary chronic pain treatment bymeans of an augmented SF-36. Pain Med 2001;1:44–54.
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

a measure of the ability to perform family and social roles,was significantly better for cancer subjects (p < 0.05).Interestingly, the CNMP group indicated much greaterPain Symptoms (p < 0.001). We conclude that the TOPScan make important contributions to the measurement oftreatment outcomes for persons with cancer-related pain.More studies are needed to establish its validity and sen-sitivity for evaluating physical and psychosocial dimen-sions of the cancer-pain experience and to refine theinstrument to reduce the item burden for persons withadvanced cancer.
502Clinical
A Pilot Trial of Intravenous Pamidronate forChronic Mechanical Spine Pain
Brenda Breuer PhD, MPH; Kevin Sperber MD, AaronSchneider NP, Seth Stoller MD, Noah Rosen MD andMarco Pappagallo MD; Comprehensive PainTreatment Center, Hospital for Joint Diseases,Orthopaedic Institute, New York; Department ofNeurology, New York University School of Medicine,New YorkChronic low back pain is a costly worldwide public healthproblem, responsible for suffering, lost workdays, andmedical treatment costs. We administer, on a compas-sionate basis, pamidronate infusions to patients havingmechanical, debilitating, chronic spinal pain. Our motiva-tion includes the palliative analgesic effect of pamidronatein metastatic bone pain, the possibility that mechanismsresponsible for cancer-related- and non-cancer-spinal-painare similar, and the success of bisphosphonate treatmentfor painful conditions unrelated to cancer or osteoporosis;e.g., ankylosing spondylitis, complex regional pain syn-drome, inflammatory bone and joint conditions, rheuma-toid arthritis; and visceral pain in animals. There are nopublications on pamidronate’s effect on spinal pain.
We administered 90 mg pamidronate infusions over 4hours to 25 patients, 41 to 84 years old. According to ourprotocol, patients receive 3 infusions, with an interval of 1 month between infusions. Based on a 0–10 numericrating scale (NRS), after completion of treatment, 91%of the patients reported some degree of pain relief. Themean pain change was a decrease of 3.6 points on theNRS, and a percentage score decrease of 41% (P <0.0001). There was no increase in opioid or non-opioidanalgesic medications associated with pain relief. A ran-domized, placebo-controlled, double blind clinical trial is needed to confirm these benefits of pamidronate formechanical spinal pain.
505Research (Clinical)
An Analysis of Pain Outcomes Using the Brief Pain Inventory in a Sample of Chronic Pain Patients
Vitaly Gordin, Cindy Baer, Michael Weaver, andKavita Gupta; Milton S. Hershey Medical Center,Penn State University College of Medicine, Hershey,PennsylvaniaPain outcomes are reported from a consecutive series ofboth new and repeat visits from 723 patients (mean age50.1 yr. ± 14.8) with chronic pain syndromes, evaluatedin our Pain Medicine Center using the Brief Pain Inven-tory (BPI). Initial completion of the BPI showed a meanaverage pain score (0–10 analog scale) since the last visitof 5.7 ± 2 and worst pain, 8.4 ± 1.8. Percent pain relief(0-no relief to 100-complete relief ) was 47.5 ± 29.2. Paininterference (0-none to 10-complete) was greatest forNormal Work (6.8 ± 2.7) and lowest for Relationships(4.8 ± 3.2). The mean score for General Activity was 6.6± 2.6. Worst pain levels were higher in women (p < 0.05).Data were also collected on whether patients were onworkman’s compensation, taking opioids, and had a com-ponent of neuropathic pain. Comparisons using Studentt-test revealed that patients taking opioids (n = 282) hadhigher average pain (p < 0.05) and greater General Activ-ity interference (p < 0.001), but significantly better painrelief (p < 0.01) compared to those who were not (n = 257). There were no differences in pain levels, painrelief, and General Activity interference betweenpatients with neuropathic pain (n = 269) and nonneuro-pathic pain (n = 272). Overall, patients on workman’scompensation had poorer outcomes. On a subset ofpatients (n = 192) with 2 and 3 visits, we were unable todetect significant differences in any of the BPI outcomes;however, mean scores for pain relief improved over time.Our analyses show that the BPI may be a useful measureto assess differences among chronic nonmalignant painpopulations. Summary data of patient-reported pain out-comes from repeated visits can provide useful informa-tion about the effectiveness of pain interventions overtime.
506Research (Clinical)
Analgesic Efficacy of Rofecoxib Compared withMultidose Oxycodone/Acetaminophen for theTreatment of Acute Pain: A Randomized Controlled Trial
David J. Chang, MD1, Paul J. Desjardins, DMD, PhD2,Steven R. Bird, MS1, Erluo Chen, MS1, Sandra H.Mockoviak1, and Gregory P. Geba, MD, MPH1
92 Abstracts
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022
1Merck & Co.,West Point, Pennsylvania,2SCIREX Corporation, Austin,Texas
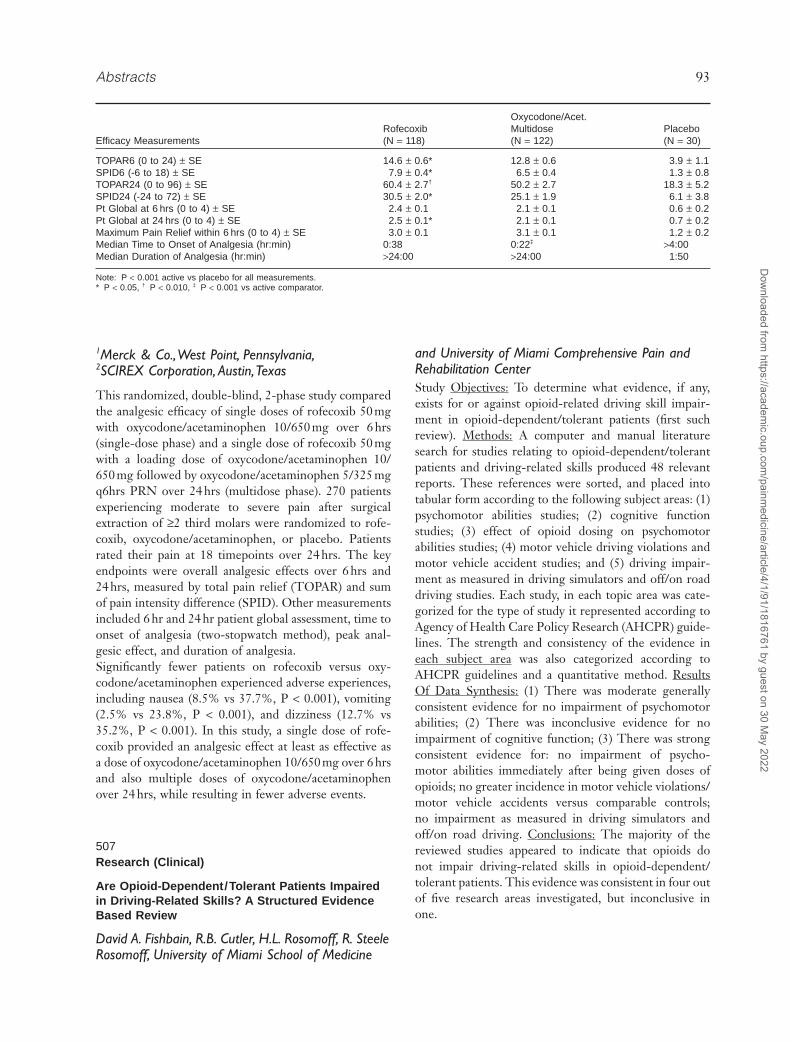
This randomized, double-blind, 2-phase study comparedthe analgesic efficacy of single doses of rofecoxib 50 mgwith oxycodone/acetaminophen 10/650 mg over 6 hrs(single-dose phase) and a single dose of rofecoxib 50 mgwith a loading dose of oxycodone/acetaminophen 10/650 mg followed by oxycodone/acetaminophen 5/325 mgq6hrs PRN over 24 hrs (multidose phase). 270 patientsexperiencing moderate to severe pain after surgicalextraction of ≥2 third molars were randomized to rofe-coxib, oxycodone/acetaminophen, or placebo. Patientsrated their pain at 18 timepoints over 24 hrs. The keyendpoints were overall analgesic effects over 6 hrs and 24 hrs, measured by total pain relief (TOPAR) and sumof pain intensity difference (SPID). Other measurementsincluded 6 hr and 24 hr patient global assessment, time toonset of analgesia (two-stopwatch method), peak anal-gesic effect, and duration of analgesia.Significantly fewer patients on rofecoxib versus oxy-codone/acetaminophen experienced adverse experiences,including nausea (8.5% vs 37.7%, P < 0.001), vomiting(2.5% vs 23.8%, P < 0.001), and dizziness (12.7% vs35.2%, P < 0.001). In this study, a single dose of rofe-coxib provided an analgesic effect at least as effective asa dose of oxycodone/acetaminophen 10/650 mg over 6 hrsand also multiple doses of oxycodone/acetaminophenover 24 hrs, while resulting in fewer adverse events.
507Research (Clinical)
Are Opioid-Dependent/Tolerant Patients Impairedin Driving-Related Skills? A Structured EvidenceBased Review
David A. Fishbain, R.B. Cutler, H.L. Rosomoff, R. SteeleRosomoff, University of Miami School of Medicine
and University of Miami Comprehensive Pain andRehabilitation CenterStudy Objectives: To determine what evidence, if any,exists for or against opioid-related driving skill impair-ment in opioid-dependent/tolerant patients (first suchreview). Methods: A computer and manual literaturesearch for studies relating to opioid-dependent/tolerantpatients and driving-related skills produced 48 relevantreports. These references were sorted, and placed intotabular form according to the following subject areas: (1)psychomotor abilities studies; (2) cognitive functionstudies; (3) effect of opioid dosing on psychomotor abilities studies; (4) motor vehicle driving violations andmotor vehicle accident studies; and (5) driving impair-ment as measured in driving simulators and off/on roaddriving studies. Each study, in each topic area was cate-gorized for the type of study it represented according toAgency of Health Care Policy Research (AHCPR) guide-lines. The strength and consistency of the evidence ineach subject area was also categorized according toAHCPR guidelines and a quantitative method. ResultsOf Data Synthesis: (1) There was moderate generallyconsistent evidence for no impairment of psychomotorabilities; (2) There was inconclusive evidence for noimpairment of cognitive function; (3) There was strongconsistent evidence for: no impairment of psycho-motor abilities immediately after being given doses ofopioids; no greater incidence in motor vehicle violations/motor vehicle accidents versus comparable controls; no impairment as measured in driving simulators andoff/on road driving. Conclusions: The majority of thereviewed studies appeared to indicate that opioids do not impair driving-related skills in opioid-dependent/tolerant patients. This evidence was consistent in four outof five research areas investigated, but inconclusive inone.
Abstracts 93
Oxycodone/Acet.Rofecoxib Multidose Placebo
Efficacy Measurements (N = 118) (N = 122) (N = 30)
TOPAR6 (0 to 24) ± SE 14.6 ± 0.6* 12.8 ± 0.6 3.9 ± 1.1SPID6 (-6 to 18) ± SE 7.9 ± 0.4* 6.5 ± 0.4 1.3 ± 0.8TOPAR24 (0 to 96) ± SE 60.4 ± 2.7† 50.2 ± 2.7 18.3 ± 5.2SPID24 (-24 to 72) ± SE 30.5 ± 2.0* 25.1 ± 1.9 6.1 ± 3.8Pt Global at 6 hrs (0 to 4) ± SE 2.4 ± 0.1 2.1 ± 0.1 0.6 ± 0.2Pt Global at 24 hrs (0 to 4) ± SE 2.5 ± 0.1* 2.1 ± 0.1 0.7 ± 0.2Maximum Pain Relief within 6 hrs (0 to 4) ± SE 3.0 ± 0.1 3.1 ± 0.1 1.2 ± 0.2Median Time to Onset of Analgesia (hr:min) 0:38 0:22‡ >4:00Median Duration of Analgesia (hr:min) >24:00 >24:00 1:50
Note: P < 0.001 active vs placebo for all measurements.* P < 0.05, † P < 0.010, ‡ P < 0.001 vs active comparator.
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

509Clinical
Botulinum Toxin Type B (Myobloc®) in theTreatment of Refractory CervicothoracicMyofascial Pain Syndrome
Terry Millette, MD, Pascagoula, MSCervical Thoracic Myofascial Pain Syndrome (MPS) is a common chronic regional pain syndrome defined by the presence of trigger points and referred pain patternsremote from the involved area. Botulinum toxin has demonstrated efficacy in a variety of conditions associated with muscle spasm. A retrospective review of patients receiving Botulinum toxin Type B(MYOBLOC®, Elan Pharmaceuticals, Inc.) for the treat-ment of MPS refractory to extensive conservative therapywas performed. A total of 20 patients (age range: 32–79years, F/M: 19/01) received injections into affected cer-vical, thoracic and facial muscles. The injections wereperformed as standard trigger point injections by palpa-tion alone using MYOBLOC, starting dose of up to20,000 units directly into the trigger point and into thesurrounding taut band of muscle. Patients were followed-up at one month and periodically thereafter. In additionto individual responses and overall response rate, treat-ment evaluations included the assessment of medicationusage, physical examination findings, neurotoxin dosage,and side effects of treatment. Response to injection wasdefined as poor relief (<20% symptom reduction), fair(≥20% reduction), good (≥50% reduction), and excellent(85% to total reduction). Of the 20 patients for whichrecords were available for review, 65% had a response ofat least good to excellent and 90% reported at least a fairresponse. As most of the patients only had one to twofollow-up visits, duration data was insufficient to quan-tify. Onset of maximum symptomatic improvementvaried from one to three weeks post-injection. Injectionswere well tolerated and patients reported non-seriousadverse events of muscle weakness (06), moderate tosevere dry mouth (02), dysphagia (05) and visual distur-bances (01) all of which were in patients who received20,000 units. Those who received less than 15,000 unitsexperienced no adverse events, indicating that a conser-vative approach suggests a starting dose of MYOBLOC10,000 units should be chosen to avoid adverse events.Botulinum toxin injection appears to be a promisingmethod for managing refractory MPS.
References
1 Childers MK, Wilson DJ, Galae JF, Smith BK. Treat-ment of painful muscle syndromes with botulinumtoxin: a review. J Back Musculoskeletal Rehabil.1998;10:89–96.
2 Simpson LL. Peripheral actions of the botulinumtoxins, in: Simpson LL ed. Botulinum neurotoxin and tetanus toxin. San Diego: Academic Press;1983:153–78.
3 Travell JG, Simons DG. Myofascial pain and dys-function: the trigger point manual. Vol. I. Baltimore,MD: Williams & Wilkins;1983.
4 Wolfe F, Simons DG, Friction J, et al. Thefibromyalgia and myofascial pain syndromes: a pre-liminary study of tender points and trigger points inpersons with fibromyalgia, myofascial pain syndromeand no disease. J Rheumatol 1992;19:944–51.
512Research (Clinical)
Can Patients Taking Opioids Drive Safely? A Structured Evidence-Based Review
David A. Fishbain, R.B. Cutler, H.L. Rosomoff,R. Steele Rosomoff, University of Miami School ofMedicine and University of Miami ComprehensivePain and Rehabilitation CenterA structured evidence-based literature review was com-pleted to determine if there was epidemiological evidencefor an association between opioid use and intoxicateddriving, motor vehicle accidents (MVA) and MVA fatali-ties. References relating to intoxicated driving, MVA andMVA fatalities were retrieved and reviewed in detail. Ofthese, references addressing opioid use were isolated andresearch information from these references was placedinto tabular form under three major headings: Intoxi-cated driving; MVA; and MVA fatalities. Data wereextracted from these references according to the follow-ing format: research question addressed, sample size, statistical analysis and results. The type of evidence eachstudy represented was categorized according to theAgency for Health Care Policy and Research (AHCPR)type of evidence categories scale. Each research area represented by all the studies in each table was also categorized by the strength and consistency of evidenceAHCPR scale. Of the 6 reports addressing intoxicateddriving, all reported a prevalence for opioid use whichwas approximately 1/10 that of the point prevalence usefor opioids in the general population indicating thatopioids probably are not associated with intoxicateddriving. Of the 9 studies addressing MVA all except oneindicated that opioids are not associated with MVA. Of the 10 studies addressing MVA fatalities the vastmajority demonstrated a prevalence percentage for anopioid association with MVA fatalities which was 1/5 thatof the point prevalence percentage for opioid usereported in the general population. Only 1 studyreported a possible association between opioid use andMVA fatalities. Although the comparison of point preva-
94 Abstracts
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

lence rates to point prevalence may be problematic,overall this evidence indicated that opioids do not appearto be associated with intoxicated driving, MVA and MVAfatalities.
513Research (Clinical)
Central Hypogonadism in Cancer Survivors onChronic Opioid Medications
Arun Rajagopal M.D., Rena Vassilopoulou-Sellin M.D.,Eduardo Bruera M.D., MD Anderson Cancer CenterA sizable number of cancer survivors require chronicopioid therapy for cancer-related pain. Recently, therehave been a number of articles demonstrating the devel-opment of central hypogonadism in patients receivingintrathecal opioid therapy for non-malignant pain syn-dromes (1–4). The purpose of this study was to identifywhether a similar phenomenon existed for patientsreceiving high-dose oral opioid therapy. Our data setincludes 20 patients so far. Male cancer survivors whosemorphine-equivalent daily dose was at least 200 mg wereincluded. Patients who had prior treatment that mightdisrupt the hypothalamic/pituitary axis were excluded(eg, prior cranial radiation or surgery, prior testosteronereplacement). We studied the hypothalamic/pituitary/gonadal axis by assessing serum levels of follicle-stimulating hormone (FSH), luteinizing hormone (LH),and testosterone (T). Eighteen out of 20 patients (90%)had abnormally low total T in the setting of low to low-normal FSH and LH, consistent with central hypogo-nadism (see Table). This finding confirms our hypothesisthat there may be an association between chronic high-dose opioid therapy and the development of centralhypogonadism. Our initial study has some limitations.We have not yet studied a control group to identifywhether this problem exists in cancer survivors not onchronic opioid therapy. We have also not studied otherfactors that may lead to central hypogonadism in thecancer survivor group. More research is justified in thisarea.
Study Group, n = 20 Normal Values
Testosterone (T) 170 +/- 94 ng/dL 241–827 ng/dLFSH 5.9 +/- 6.7 1.4–18.1LH 2.4 +/- 1.8 1.5–9.3
References
1 Paice JA, Penn RD, Ryan WG. Altered sexual func-tion and decreased testosterone in patients receiving
intraspinal opioids. J Pain Symp Management, 1994,9:126–31.
2 Chaney MA. Side effects of intrathecal and epidural opioids. Can J Anaesth, 1995;42(10):891–903.
3 Abs R, Verhelst J, Maeyaert J, van Buyten J, OpsomerF, Adriaensen H, Verlooy J, van Havenbergh T, SmetM, van Acker K. Endocrine consequences of long-term intrathecal administration of opioids. J. ClinEndocrinol Metab, 2000, 85:2215–22.
4 Finch PM, Roberts LJ, Price L, Hadlow NC, Pullan PT. Hypogonadism in patients treated withintrathecal morphine. Clin J. Pain, 2000;16(3):251–4.
514Education
Cevicogenic Headache and the Fibromyalgia Examination
John W. McFadden, Maryland;Tupelo Pain Clinic,Tupelo, MississippiObjective: The objective of the study is to describe theuse of the upper body fibromyalgia examination in thepatient with cervicogenic headache and to differentiatebetween cervicgenic headache and non-cervicogenicheadache. Methods: Two hundred patiets meeting the full criteria for the fibromyalgia examination werestudied. The fibromyalgia examination plus very carefullyexpanded examination of the cervical spine help deter-mine the presence or absence of neck pain. Digital pressure over the disc and positional maneuvers of thecervical spine by the patient increase or decrease theintradiscal pressure to aid in localizing the painful disc ordiscs. The patients were in pain when examined andfamiliar pain was produced during the examination.Results: Patients presented in the study reported an asso-ciation between their neck pain and headache. No patientwas found by x-ray, MRI or discography to have evidenceof pain of origin other than the cervical intertebral disc.After the examinations the patient is more oriented to therelationship between neck pain and headache and is morereceptive to treatment of the neck pain. Options for treat-ment include medical and/or surgical interventions. Inthis series of 200 patients 11 had no headache, 37 hadmild headache, 57 had moderately severe headache, and94 had severe headache. There were 40 men and 160women. The average age of the men was 44.8 and thewomen was 43.9 years. Conclusions: The upper bodyfibromyalgia examination is a useful tool in examining thepatients reporting headache. If the examination revealsevidence of cervical disc pain the chance that theheadache is of cervical origin increases.
Abstracts 95
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

515Research
Changes in Outpatient Narcotic PrescribingPatterns in the National Ambulatory Medical CareSurvey, 1996–99
Elliot B. Bodofsky M.D., UMDNJ-Cooper UniversityHospital, Camden, NJSeveral local studies have documented a significantincrease in the use of narcotic analgesics in recent years.The U.S. National Ambulatory Medical Care Survey(NAMCS) is a clustered survey of outpatient physicianvisits in all specialties, conducted by the National Centerfor Health Statistics (NCHS). The survey was analyzed todetermine whether narcotic prescription is increasingnationally, and whether this increase is consistent bygender, race, and physician specialty. In 1996, there werean estimated 20,496,860 total outpatient narcotic pre-scriptions (95% confidence interval 18.5–22.5 million),rising 24% (95% confidence interval –3% to 57%) by1999 to 25,476,743 (95% confidence interval 21.8–29.1million) (Z = 1.7, p = .09). At the same time, total medicalprescriptions in the U.S. rose only 3%. However, duringthis time, total narcotic prescriptions for Females rosefrom 12,227,149 to 14,337,732, a 17% increase, while forMales, the total rose from 8,269,711 to 11,139,011, amuch larger 35% increase. The rate of narcotic analgesicprescription in Blacks was lower than Whites in 1996, butby 1999 this had disappeared due to a much larger rise innumber of prescriptions (17% for Whites and 126% forBlacks). In both studies, the largest number of narcoticprescriptions were written by Family Practioners andInternists (46% of total in 1996 and 54% in 1999). Mostspecialties with large numbers of prescriptions showedsimilar increases between 1996 and 1999. Overall, this studyshows a moderate increase in outpatient narcotic prescrip-tions in the U.S. between 1996 and 1999. The increase wassimilar for major specialties. Groups that had a lower rateof narcotic prescription in 1996 showed a greater increaseby 1999.
516Clinical
Chemical Burns Following Accidental PhenolExposure: A Call for Use of Luer-Lock ExtensionTubing During Phenol Neurolysis
B.Todd Sitzman, MD, MPH,Vitaliy Y. Domashevich,MD, Kristen M. Zeller, MD,Tim J. Lamer, MD andDouglas S. Fenton, MD, Division of Pain Medicine,Mayo Clinic, Jacksonville, Florida
Abstract Text:Introduction: Phenol neurolysis is a widely used tech-nique for the relief of intractable cancer-related pain.Neuronal exposure to dilute phenol (6 to 10% carbolicacid) results in cell wall destruction and protoplasmicprotein denaturation, with subsequent disruption ofafferent nociceptive pathways. The majority of seriousadverse effects from phenol neurolysis involve inadver-tent intravascular injection and subarachnoid spread. We describe a case of dermal chemical burns from acci-dental skin exposure to phenol. Additionally, we presenta simple method of preventing the occurrence of suchevents by use of Luer-lock connection tubing. Case Report: J.R., a 72 yo with severe abdominal painfrom unresectable mesenteric carcinoid tumor, under-went celiac plexus phenol neurolysis using a left-sidedposterior single needle approach (22 G, 20 cm Chibaneedle; B-D, Franklin Lakes, NJ). Correct needle tipposition and sufficient spread of contrast involving bilateral celiac plexuses was confirmed using CT-guidance. Injection of contrast agent and 10% phenol wasperformed using small-bore extension tubing (B.BraunMedical Inc., Bethlehem, PA), such that the tubing wasattached to the needle with a slip-tip connection [Figure1]. There was little resistance during contrast injection;however, during phenol injection there was a discon-nection of the extension tubing and needle. Thisresulted in a spray of 10% phenol onto the exposed skinof the patient’s back and the physician’s wrist. Both thepatient and physician experienced a burning sensationwithin 30 seconds of phenol contact. The exposed skinwas washed with copious isopropyl alcohol solutionwithout delay and the procedure was completed withoutcomplication. The skin areas exposed to phenol subse-quently revealed second-degree chemical burns [Figures2 and 3]. These sites were treated with silver sulfadi-azine ointment with resultant healing. Additionally, twodays following the procedure the patient reported amarked reduction of his abdominal pain (VAS pain scoredecreased from 8 to 1).Discussion: Dermal exposure to phenol, even in lowconcentrations, can result in severe burns and dermaltoxicity. Systemic absorption may lead to serious, evenlethal, adverse effects.1 These potential effects are wellreported in the occupational health and toxicology literature; however, little is written on this topic in thepain literature. The use of a Luer-lock connectionbetween the extension tubing and needle tip would haveprevented the inadvertent disconnection and skin expo-sure to phenol [Figure 4]. Should skin exposure occur,OSHA advises that polyethylene glycol or isopropylalcohol be applied prior to washing with large quanti-ties of water.2
96 Abstracts
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

Summary: We recommend the use of extension tubingwith Luer-lock connectors during all phenol neurolyticprocedures.
References
1 Hathaway GJ, et al. Proctor and Hughes (Eds):Chemical Hazards of the Workplace. 3rd ed. VanNostrand Reinhold Company, New York, NY 1991.pp 468–9.
2 OSHA. Occupational safety and health guideline for phenol. http://www.osha-slc.gov/SLTC/healthguidelines/phenol/recognition.html.
518Research
Citalopram in the Treatment of Fibromyalgia
William G. Kee, Arthur R. Smith, Jeffrey W. Folk:Medical University of South CarolinaAbstract Text: The efficacy of citalopram in the treat-ment of primary idiopathic fibromyalgia was evaluatedusing 22 subjects, 11 who scored in the minimal (<14)and 11 who scored in the moderate to severe (≥19) rangeon the Beck Depression Inventory II (BDI). Prior tostarting the medication trial, subjects had one week ofwashout from all medications for pain, sleep or depres-sion. Subjects were treated for 6 weeks with citalopram20–40 mg. Measures taken at baseline, end of washoutweek and end of study included: BDI, Visual AnalogScale for pain, McGill Pain Questionnaire (MPQ), SleepQuestionnaire, Fibromyalgia Impact Questionnaire(FIQ), Pressure Threshold Gauge for Tender Points, andActivity Diary. During the study patients were prohib-ited from taking usual medications and provided with arescue medication. Results indicated no consistent dif-ferences on demographic variables between depressedand non-depressed subjects. Regression analyses did notindicate any consistent relationship between subject variables and outcome measures. Changes during the 6week medication trial showed significant (0.01 to 0.05)improvement on: VAS scores, MPQ, FIQ, sleep, 4tender points, 2 control points and pooled tender pointscore. Depressed subjects showed greater improvementthan non-depressed. Pearson correlation coefficients ofchange indicated a correlation between changes indepression and changes in pain, sleep and FIQ symptomseverity. However, change in depression scoresaccounted for 37.3% to 41.9% of the change in painscores with >50% attributable to other factors. In con-clusion, subjects taking citalopram showed a marked
improvement in pain, fibromyalgia symptoms, sleep andtender points compared to baseline. The study indicatesthat citalopram is effective in making changes in thesymptoms of fibromyalgia beyond changes seen in mood.Study supported by Forest Laboratories
519Research
Comparison of Healthcare Service Use and CostsAmong Patients with any Mention of ArthritisInitiating Therapy on Oxycontin® Tablets orControlled-Release Morphine Sulfate Tablets
Objective: Comparison of pharmacy and healthcare serv-ices costs among patients with any mention of arthritis initiating therapy with OxyContin® Tablets or controlled-release morphine sulfate (CRMS) tablets. Methods: Patientswith any mention of arthritis and newly prescribed Oxy-Contin or CRMS were identified using the MEDSTATMarketScan® database (1997–2000). Ordinary leastsquare regression models calculated adjusted total andpharmacy costs. An intent-to-treat analysis comparedhealthcare resource utilization and costs over the 6 monthsfollowing therapy initiation. Models controlled for co-morbid pain conditions, previous healthcare utilizationand cost, non pain-related co-morbidities, patient demo-graphic characteristics, and type of health plan. Results arereported as per-member costs. Results: A total of 4,384OxyContin and 623 CRMS “new starters” with anymention of arthritis were identified. Adjusted total andpharmacy costs in the six months following were signifi-cantly lower for OxyContin “new starters” (total—$4,518,pharmacy—$1,532; p < 0.01) compared with CRMS(total—$6,117, pharmacy—$2,200) “new starters”. Nodifferences were noted in either inpatient or outpatientcosts. Inpatient costs for OxyContin “new starters” were$1,061 compared with CRMS “new starters” $1,263. Out-patient costs were $1,716 for OxyContin “new starters”compared with $1,560 for CRMS “new starters”. Withinpharmacy costs, long-acting and short-acting opioid costsover the 6 months were lower for OxyContin “newstarters” ($263 p < 0.01; $215 p < 0.05, respectively) thanCRMS “new starters” ($310; $263, respectively). Con-comitant non-steroidal anti-inflammatory drug costs overthe 6 months were $121 for OxyContin “new starters”while CRMS “new starters” were $97 (p < 0.01). Conclu-sion: Total and pharmacy costs, specifically long-actingand short-acting opioid costs, in OxyContin “newstarters” were significantly less over a 6-month periodcompared to CRMS “new starters”. Results suggest differ-ences in pharmacy costs impact total costs.
Abstracts 97
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

520Research (clinical)
Comparison of the Analgesic Efficacy of Rofecoxib50 mg and Placebo in Acute Pain: A CombinedAnalysis of 13 Clinical Studies
Donald R. Mehlisch, MD, DDS1, David J. Chang, MD2,David Krupa, MS3, Adam B. Polis, MA2, Richard A.Petruschke, PharmD2, and Gregory P. Geba, MD, MPH2
1SCIREX Corporation, Austin,Texas, 2Merck & Co.,West Point, Pennsylvania, 3Merck ResearchLaboratories, Rahway, New Jersey
The objective of this study was to assess the overall anal-gesic efficacy across 13 similarly designed acute painstudies of a single dose of rofecoxib 50 mg, a selectivecyclooxygenase (COX)-2 inhibitor approved for acuteanalgesia. A combined analysis was performed on the 13 randomized, double-blind, placebo-controlled studiesinvolving patients experiencing moderate to severe painafter surgical extraction of ≥2 third molars. Patientstreated with rofecoxib 50 mg (N = 1,329) or placebo (N= 568) were included in the analysis. The overall anal-gesic effect was determined by patient global assessmentat 24 hours based on responders (excellent, very good,good) versus non-responders (poor, fair). Total pain reliefover 8 hours (TOPAR8), the time-weighted sum of painrelief scores, ranging from 0 (no relief) to 4 (completerelief), during the first 8 hours was also analyzed. TheTOPAR8 scores ranged from 0 to 32. Patient character-istics were similar between rofecoxib and placebo in eachstudy. Overall, about 60% were females, mean age was21 years, and 68% had moderate pain at baseline. Basedon patient global assessment at 24 hours, 72% of rofe-coxib-treated patients were responders compared with16% of placebo-treated patients (P < 0.001). Results ofrofecoxib versus placebo by TOPAR8 (17.4 vs 4.4, P <0.001) confirmed the robust overall analgesic efficacy ofrofecoxib. In this combined analysis involving over 1,300patients treated with a single dose of rofecoxib 50 mg,approximately three of every four patients experienced a good, very good, or excellent response at 24 hours. The overall demonstrated analgesic efficacy of rofecoxibshown in global patient-reported endpoints is consistentwith desired characteristics of analgesics used in the treat-ment of acute pain.
522Research (clinical)
Effect of Lidocaine Patch 5% on Pain Intensity andPain Relief When Used in Combination withGabapentin in 3 Chronic Pain States
Joseph Gimbel, MD, Arizona Research Center,Phoenix, Arizona; Bradley S. Galer, MD, Arnold R.Gammaitoni, PharmD, Endo Pharmaceuticals Inc.,Chadds Ford, PennsylvaniaPostherpetic neuralgia (PHN), low back pain (LBP), andpainful diabetic neuralgia (DN) are all complex and difficult-to-treat chronic pain conditions that are likely torequire administration of multiple analgesics to achieveclinically meaningful pain relief. These pain states maybe perpetuated by both peripheral and central painprocesses. Therefore, a rational pharmacotherapy ap-proach in patients with PHN, LBP, or painful DN iscombining a targeted peripheral analgesic with one ormore centrally acting agents. This open-label, nonran-domized, multicenter trial assessed the effectiveness,safety, and tolerability of lidocaine patch 5% (Lido-derm®), a targeted peripheral analgesic, administeredq24h for 2 weeks in the treatment of PHN, DN, and LBPin patients who had experienced an incomplete or partialresponse to their current analgesic regimen containinggabapentin. Partial response was defined as average dailypain intensity >4 on a 0–10 numeric pain intensity scale.Patients were maintained on their current analgesicregimen, including gabapentin, throughout the study,with no adjustments other than addition of lidocainepatch. Interim analyses of the first 50 patients (PHN, n = 6; DN, n = 13; LBP, n = 31) who completed 2 weeksof treatment revealed significant improvements in all painintensity parameters and pain relief measured by the BriefPain Inventory (BPI) for all patients combined (P < .001)and the LBP group (P < .05), composite BPI pain inter-ference with quality-of-life score for all patients com-bined (P < .0001); and all 4 Neuropathic Pain Scalesubscores for all patients combined (P < .0001), the DNgroup (P < .01), and the LBP group (P < .002). Lidocainepatch was found to be safe and well tolerated with rela-tively few clinical adverse events, most of which weremild or moderate. Final analyses will be presented at themeeting. The support of Endo Pharmaceuticals Inc. forthis study is gratefully acknowledged.
523Research (Clinical)
Effects of AvinzaTM, A New Once-Daily Extended-Release Morphine Formulation, and Twice-Daily MsContin on Sleep Variables in Patients with ChronicModerate-to-Severe Osteoarthritis Pain
Jacques R. Caldwell, M.D., Radiant Research;Jeffrey C. Davis, M.D., Capstone Clinical Trials Inc.;Howard L. Offenberg, M.D., Radiant Research;Howard W. Marker, M.D., Memphis MedicalSpecialists; Ronald J. Rapoport, M.D.,Turesdale
98 Abstracts
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

Clinic; Sanford H. Roth, M.D., ArthoCare; Lise Eliot,Ph.D., Elan Pharmaceuticals Inc.; Cynthia R. King,Ph.D., Ligand Pharmaceuticals Inc.; Patrick Kenny,Elan Drug Delivery Inc.; Najib Babul, Pharm.D.,Theraquest Biosciences, LLC.Introduction: The objective of this assessment was to eval-uate the effects of a new, once-daily extended-release mor-phine sulfate formulation (AVINZATM) and twice-dailycontrolled-release morphine sulfate (MS Contin®; MSC)on several sleep variables, as part of an analgesic efficacystudy in patients with chronic moderate-to-severeosteoarthritis (OA) pain. Methods: Patients in this multi-center, randomized placebo-controlled, double-blind,parallel-group trial received either AVINZA 30 mg QAM(n = 73), AVINZA 30 mg QPM (n = 73), MSC 15 mgQ12H (n = 76), or placebo Q12H (n = 73) for 4 wks.Patients completed a sleep questionnaire at baseline andweekly to evaluate the following: trouble falling asleep(TFA) because of pain, need for sleep medication to fallasleep (NSM), frequency of awakening by pain during themorning (FAAM) or night (FAPM), duration of sleep in hours (DOS) and overall quality of sleep (QOS). Allassessments, except DOS, were scored on a 100-mm scale.Results: 184 patients completed the study. Improvementsin all sleep variables were demonstrated with active treatments in comparison to placebo; however, not allimprovements were statistically significant (p = 0.05).AVINZA QAM provided statistically significant (p = 0.05)improvements versus placebo on multiple occasions forseveral sleep variables at weeks 1 to 4 and provided a sig-nificant improvement in QOS versus MSC on weeks 1 and4. Significant improvements (p = 0.05) relative to placebowere also observed for AVINZA QPM for QOS on weeks1, 2, and 4, and DOS on week 1 and by MSC BID for QOSat week 2 and TFA at weeks 3 & 4. The majority of adverseevents (AEs) were mild to moderate, those generally asso-ciated with opioids, and similar between AVINZA andMSC. Conclusions: AVINZA once-daily administeredeither in the morning or evening improves several sleepvariables in patients with chronic moderate-to-severe OApain. AVINZA QAM demonstrated a significant improve-ment in overall QOS relative to MSC.
** The support of Ligand Pharmaceuticals Inc. for this researchproject is gratefully acknowledged.
525Research
Fibromyalgia of Intervertebral Disc Origin: A Report of 200 Cases
John W. McFadden. MD,Tupelo Pain Clinic,Tupelo,MS
Aim of Investigation: To study the findings in patientswith anterior cervical spine tenderness and pain of discorigin meeting the full criteria for the fibromyalgia syn-drome. Methods: Two hundred patients with disc paincomplaints requiring daily medication for pain controlwere chosen between January 2000 and January 2001. Allhad 11 or more painful sites and had a complaint of neckand low back pain. All patients are examined with the indexfinger up and down the anterior cervical spine on the rightand left. Results: The average age of the female patient was43.9 years. The average age of the male patient was 44.8years. The average duration of disabling pain was 7.3 yearsin the female patients and in the male patients was 6.5years. Pain was found on one side of the cervical spine in55% and in both sides in 45% of the female patients. In themale patients pain was found on one side in 75% and onboth sides in 25%. Headaches were reported by 95% ofthe patients. A diagnosis of depression and/or anxiety wasmade in 75%. In those having 15 or more painful sites,93% had anxiety, depression, or both. Painful sites werefound from C2 to C6 and L3 to L5. The usual pain was re-created in enough of the familiar pattern to convincethe patient that the pain was of disc origin in the cervicalarea frequently. No patient achieved 24 hour pain relief.Undertreatment of pain was reported with an average ofonly 4.4 hours of pain relief out of 24. Conclusions:Fibromyalgia of intervertebral origin is sorted out by amore careful examination. The fibromyalgia examinationshould include anterior cervical spine examination of C2through C7disc levels. The data suggests that the anteriorcervical spine portion of the fibromyalgia examinationshould be carried out more carefully.
526Research (clinical)
Improvement of Sleep in Diabetics withNeuropathic Pain Treated with Controlled-ReleaseOxycodone
Edward Liao, Purdue Pharma L.P.; Patricia Richards,Purdue Pharma L.P.; Michael Friedman, PurduePharma L.P.; Russell Portenoy, Beth Israel MedicalCenterBACKGROUND: Pain associated with diabetic neuropa-thy (DN) may persist or worsen at night and interfere withsleep. The present study evaluated whether controlled-release (CR) oxycodone improved sleep in patients withpainful DN. OBJECTIVE: To evaluate the efficacy andsafety of CR oxycodone in providing analgesia, improvingquality of sleep, and reducing pain interference with sleepin patients with painful DN. METHODS: Diabetics withpainful polyneuropathy were enrolled in a randomized,double-blind, parallel-group, 6-week study. Subjects initi-
Abstracts 99
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

ated therapy with CR oxycodone 10 mg q12h or matchingplacebo. Blinded dose titration ensued until patientsreported adequate pain relief or intolerable side effects, or a maximum CR oxycodone dose of 60 mg q12h wasreached. Among other measures, pain interference withsleep (0 = does not interfere, 10 = completely interferes)was assessed using an item from the Brief Pain Inventory atbaseline and on days 14, 28, and 42, and quality of sleep (0= poor sleep, 10 = excellent sleep) was assessed by dailydiary. Treatments were compared using repeated meas-ures analysis of covariance. RESULTS: 159 subjects (CRoxycodone = 82, placebo = 77; mean age = 58.9 years) com-prised the intent-to-treat population. There were no significant differences in demographics between the treat-ment groups. CR oxycodone provided significantly betteranalgesia than placebo (p = 0.002). The following tablesummarizes the sleep findings:
Placebo CR Oxycodone
Change Change Post- from Post- fromBaseline Baseline Baseline BaselineMean (SE) (SE) Mean (SE) (SE) p-value
Interference 5.3 (0.31) -1.5 (0.32) 3.6 (0.32) -3.3 (0.32) <0.001with Sleep
Quality of 5.4 (0.24) 0.5 (0.24) 6.1 (0.24) 1.2 (0.24) 0.024Sleep
Adverse events were typical for opioids and wereobserved more frequently with CR oxycodone thanplacebo. None of the serious adverse events were con-sidered related to study treatment.CONCLUSION: Compared to placebo, treatment withCR oxycodone provided better analgesia, improved sleepquality, and reduced pain interference with sleep inpatients with painful DN.
527Clinical
Injections of the Past that Reveal ThemselvesUnder Fluoroscope Today: Fluoroscopic Evidenceof Remote Injections of Radiopaque Substances
Annu Navani, MD, Carmen L. Dominguez, MD,John K. Hald, MD, PhD, Scott M. Fishman, MD
Division of Pain Medicine, Department ofAnesthesiology and Radiology, University of California,Davis
Introduction: It is not unusual to encounter residualeffects of contrast agents used from the remote past. Thisis such a case. Our goal through this discussion is to intro-duce and alert clinicians to the implications of residual oil-based ionic contrast agents in the intrathecal space. Case
Report: A 70 y/o female with evidence of lumbar degen-erative disc disease underwent series of lumbar epiduralsteroid injections with significant relief of pain. Fluo-roscopy during the procedure revealed diffuse residualintrathecal pantopaque dye. We were able to demonstrateunrestricted epidural spread of 1 ml omnipaque 180 downto S1 vertebral level with a L2–3 translaminar approach.Discussion: The goal of this case report is to highlight thepotential of residual myelographic dye to complicateinterventional procedures. Such residual dyecan increasethe level of technical difficulty in performing the proce-dure and the rate of complications associated with theprocedure, such as, dural puncture during epidural injec-tion. Pantopaque (iophendylate) has a slow clearancefrom the cerebrospinal fluid (0.5–3 cc per year) and mayproduce arachnoiditis, meningeal reactions, and completeadherence of the pia, arachnoid and duramater.1 Theissues related to the efficacy of the lumbar epidural blockand detrimental effects of epidural steroids in terms ofworsening the preexisting arachnoiditis are concerning.The presence of intrathecal pantopaque also raises thepossibility of misinterpretation of the dye droplets forintraspinal lipoma or hemorrhage leading to unnecessarydiagnostic and therapeutic interventions. The medicole-gal ramifications of new-onset neurological symptoms inthe face of ongoing interventional pain management in apatient with residual intrathecal contrast agent cannot beoveremphasized.
References
1 Mason MS, Raaf J. Complications of Pantopaquemyelography- case report and review. J Neurosurg1962;19:302–11.
528Research (Clinical)
Is Pain Fatiguing? A Structured Evidence Based Review
David A. Fishbain, Brandly Cole, R.B. Cutler, H.L.Rosomoff, R. Steele Rosomoff, University of MiamiSchool of Medicine, Departments of Psychiatry,Neurological Surgery, and Anesthesiology. Universityof Miami Comprehensive Pain and RehabilitationCenter at South Shore HospitalStudy Objectives: To determine what evidence, if any,exists for or against an association between fatigue andpain. Summary of Background Data: Previous studieshave reported the association of fatigue and pain.Methods: A computer and manual literature search relat-ing to fatigue and pain produced 23 reports. Informationrelating to the above problem was abstracted and placed
100 Abstracts
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

into tabular form. Each report was categorized for thetype of study it represented according to Agency forHealth Care Policy and Research (AHCPR) guidelinesand was rated for quality independently by two of theauthors. Only studies having a quality score of 75% orgreater were utilized to formulate the conclusions of thisreview. The strength and consistency of the evidence rep-resented by the remaining studies was categorized utiliz-ing the AHCPR guidelines. Conclusions of this reviewwere based on these results. Results Of Data Synthesis:Of the 23 reports, 17 had quality scores of 75% orgreater. Of these 17 reports, 94.1% indicated that therewas an association between fatigue and pain. In addition,100% of a subgroup of thirteen reports indicated thatthere might be an etiological relationship between painand fatigue. The overall strength and consistency of thisevidence according to AHCPR guidelines was thereforecategorized as A (highly consistent findings from multi-ple studies). Conclusions: There is an associationbetween fatigue and pain and there may be an etiologi-cal relationship between pain and fatigue.
529Clinical
Management of Post-Operative Pain Secondary toIleus Utilizing Neuroanatomic Acupuncture
Ronald Reimer, MD, Division of Neurosurgery, MayoClinic, Jacksonville, FloridaIntroduction: A common cause of post-operative pain is paralytic ileus. This can be seen after any procedurerequiring general anesthesia, particularly after abdominaland transplant surgery.Methods: We present a series of twelve cases managedwith neuroanatomic acupuncture. All patients failedmaximal medical therapy including nasogastric drainage,maximal intravenous antiemetic therapy and the use ofprokinetics, including reglan and erythromycin. Radi-ographs were obtained to exclude evidence of bowelobstruction, and metabolic abnormalities were ruled out.The gastroenterologists were consulted, and had nofurther recommendations. All patients were experiencingincessant nausea, vomiting, obstipation and abdominalpain secondary to ileus, for up to two weeks precedingconsultation. Many were requiring parenteral nutritionto diminish weight loss and were unable to be ambulate,markedly slowing their postoperative recovery. Results:We designed a neuroanatomic acupuncture input focus-ing on equilibration of autonomic imbalance. This input included needle placement bilaterally at standardacupuncture points MH-6, LI-4, HT-3, ST-25, ST-36,LR-3, SP-6, and centrally at GV-20 and CV-12. Low fre-quency electrical stimulation was utilized in a crossed
fashion, linking LI-4 and ST-36. Treatment was per-formed for only 12 minutes and all but two patientsresponded dramatically after the initial treatment. Ten oftwelve patients (83%) noted immediate peristalsis, withborborygmus and improved bowel function with dimin-ished nausea and no further vomiting. They resumednormal diets and were discharged within 24–36 hours.Acupuncture treatments were well tolerated with noadverse sequalae. In all cases, the patient’s length of staywas significantly shortened with the utilization of neu-roanatomic acupuncture. Conclusion: The NIH consen-sus statement of 1997 accepted the use of acupuncturefor the treatment of postoperative and chemotherapy-induced nausea & vomiting, as well as dental pain. Wehave seen dramatic results in treating more extensiveautonomic dysfunction and propose the use of neu-roanatomic acupuncture for the management of re-fractory ileus.
530Research
Medications and Healthcare Services Costs Among Neuropathic Pain Patients Receiving Long-Acting Opioids
Objective: To examine the economic impact on total andpharmacy costs on patients newly prescribed transdermalfentanyl (TDF) or controlled-release oxycodone (CRO)for neuropathic pain. Methods: Patients diagnosed withneuropathic pain who were prescribed TDF or CROwere identified using the MEDSTAT MarketScan® data-bases (1997–2000). Total medical and pain-related phar-macy costs were compared six months following therapyinitiation. Analyses controlled for co-morbid condi-tions (both pain-related and non-pain-related), previoushealthcare utilization and cost, patient demographiccharacteristics, and health plan type. Results are reportedas per-member costs. Results: A total of 506 TDF and2,299 CRO patients were identified for the analyses.Total and pharmacy costs in newly prescribed CROpatients (total—$4,860, pharmacy—$1,636) were lowerin the six months following compared with those newlystarted on TDF (total—$5,378 p < 0.05; pharmacy—$2,026 p < 0.01). Within pharmacy costs, long-actingopioid (LAO) and short-acting opioid (SAO) costs forTDF were $367 and $337 respectively. LAO and SAOcosts for CRO were $340 and $281 (p < 0.05), respec-tively. Concomitant non-steroidal anti-inflammatory(NSAID) costs over the 6 months were $109 for TDFand $134 (p < 0.05) for CRO. Conclusion: Neuropathicpain patients newly started on CRO are overall less costlyin the areas of total and pharmacy costs compared toTDF. Findings suggest pharmacy costs impact total costfor neuropathic pain patients.
Abstracts 101
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

531Clinical
Methadone and the Hospice Patient: PrescribingTrends in the Home Care Setting
Douglas J.Weschules PharmD, excelleRx Inc. JillMcMath PharmD excelleRx Inc., Rollin GallagherMD Medical College of Pennsylvania/HahnemannSchool of Medicine/excelleRx Inc., Calvin J. Alt RPhexcelleRx Inc., and Calvin H. Knowlton PhD excelleRxInc.Methadone is enjoying a resurgence in popularity for thetreatment of cancer pain. However, many clinicians arehesitant to use methadone due to it’s complex pharma-cokinetics, potential drug interactions, and dynamicopioid conversion ratios. Methadone also continues toremain stigmatized by its association with the treatmentof heroi addiction. Despite these issues, methadone is avery effective opioid in the treatment of nociceptive andneuropathic pain, and is very cost effective. The latterpoint is especially important in the hospice setting, whereproviding cost-effective symptom relief is of utmostimportance. To understand more about patterns ofmethadone use in our hospice patients, we reviewed the pharmacy dispensing data for all hospice pa-tients managed by our pharmacy over one year(11/1/00–10/31/01) to identify all patients for whommethadone was prescribed. Four hundred and thirty fourpatients were prescribed methadone during this timeperiod (m = 204, f = 229, unknown = 1). When comparedto other long-acting opioids, only 2.5–2.7% of hospicepatients/month were prescribed methadone as theprimary analgesic. This underscores the need for educa-tion and familiarity with its unique characteristics. Toaddress this need, we will outline methadone usage cri-teria, opioid equianalgesic ratios based on literaturereview, and a proactive monitoring system that is phar-macist driven. After implementation with the proposedprotocol, we will monitor for outcomes datapoints suchas pain scales, sedation scores, and breakthrough dose uti-lization. A case presentation will illustrate this protocol.The collection of this data will increase the clinician’sfamiliarity and confidence in methadone as a long actingopioid.
532Clinical
Modafinil for Excessive Daytime SleepinessSecondary to Chronic Opiate Use: A Case Report
The use of chronic opiates leading to daytime sedationand fatigue is well documented. (1) Numerous medica-tions have been used to counteract these side effects
such as CNS stimulants (e.g., amphetamines, caffeine,methylphenidate). They all work to varying degrees ofsuccess but demonstrate significant side effects such ascardiac irregularities and gastric disturbances. Chronicuse often results in insomnia, hyperactivity, irritability,and aggressive behavior. (2) Modafinil, a benzhydrylsulfinylacetamide derivative, is a schedule IV CNS stim-ulant that is structurally and pharmacologically distinctfrom other currently available CNS stimulants such asamphetamines, caffeine, cocaine, and methylphenidate.Modafinil promotes vigilance and wakefulness anddecreases the number of daytime sleep episodes associ-ated with narcolepsy. Modafinil is FDA approved for thesymptomatic treatment of narcolepsy to improve wake-fulness in patients with excessive daytime sleepiness(EDS). Narcolepsy is a CNS disorder characterized bysomnolence, often accompanied by sudden attacks ofweakness (cataplexy). 10 patients were selected with avariety of pain conditions with the use of chronic opiatesand daytime sedation being the one common qualifier.The Epworth Sleepiness Scale (ESS) and the FatigueSeverity Scale (FSS) was used to measure the level offatigue and sedation. Initial dosing was started at 100 mgdaily and was titrated upward every 5 days to 200 mg. Thefollowing results were obtained: excellent = 30%, good =60%, fair = 10%, and poor = 0%. Overall improvementin ESS and FSS scores are significant and reflect 90% ofpatients studied were no longer in the pathologic category. One patient was discontinued due to nausea.Modafinil has no impact on plasma melatonin and corti-sol profiles, which suggest that acute modafinil adminis-tration is devoid of short-term side-effects. (3) Modafinilis a pharmacologically and clinically promising agent forthe treatment of medication induced daytime somno-lence. Placebo-controlled trials are needed to assess thesafety and efficacy of this agent.
References
1 Barker LR, Burton JR, Zieve PD. Principles ofambulatory medicine. 4th ed. Philadelphia: Williamsand Wilkins; 1995.
2 Barnhart ER, publisher. Physicians’ desk reference.45th ed. Oradell, NJ: Medical Economics Inc;1991:513–4.
3 Brun J, Chamba G, Khalfallah Y, Girard P, Boissy I,Bastuji H, Sassolas G, Claustrat B. Effect ofmodafinil on plasma melatonin, cortisol and growthhormone rhythms, rectal temperature and perform-ance in healthy subjects during a 36 h sleep depriva-tion. J Sleep Res 1998 Jun;7(2):105–14.
102 Abstracts
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

533Clinical
National Osteoporosis Foundation (NOF) ClinicalPractice Parameters on Medical RehabilitationManagement of Patients with Osteoporosis and its Sequela with Emphasis on Pain and Disability
Martin Grabois, M.D., Baylor College of Medicine;Rollin Gallagher, M.D., MCP Hahnemann Universityand Francis J. Bonner, Jr., M.D.This poster will present the rationale, organizationalstructure, writing and finally implementation of the NOFClinical Parameters on Rehabilitation of patients withosteoporosis. These practice parameters are an outgrowthof the rehabilitation area being inadequately addressed ina medical practice parameters previously developed.
The NOF is the national organization representingconsumers concerned about osteoporosis. While con-sumer based it is has a medical advisory committee andan interspecialty medical council with representatives of many osteoporosis related professional organizationincluding the American Academy of Pain Medicine. Aspecial panel was empowered to write the clinical prac-tice parameters with input from the interspecialtymedical council, the medical advisory board, approved bythe Board of Directors and endorsed by the interspecialtymedical council individual representative organizations.
Following a critical review of the literature on the following areas: exercise, pain, modalities and assistivedevices, articles were ranked in an evidence-basedmanner. The Practice Parameter Task Force meeting inperson and by e-mail wrote and reviewed each sectionbased on evidence-based and/or consumer based information.
The review of the literature found limited evidence-based information in the area of pain secondary to osteo-porosis and its treatment with medications or modalities,but with some evidence in the exercise area.
It is expected these guidelines, to be published in late2002 or early 2003, will provide healthcare practitionersa road map to better manage patients with osteoporosisboth in presentation and treatment areas. Appropriateuse of pain medication combined with appropriate phys-ical modalities and exercises as well as assistive devicesshould increase function and improved quality of life inpatients with osteoporosis mainly based on the consen-sus rather than evidence-based literature.
Implications for evidence-based research in the treatment of pain in patients with osteoporosis will bepresented.
534Research (Clinical)
Onset of Analgesic Efficacy of Rofecoxib 50 mg: ACombined Analysis of 11 Clinical Studies
Paul J. Desjardins, DMD, PhD1, David J. Chang, MD2,David Krupa, MS3, Adam B. Polis, MA2, Richard A.Petruschke, PharmD2, and Gregory P. Geba, MD,MPH2
1SCIREX Corporation, Austin,TX, 2Merck & Co.,WestPoint, PA, 3Merck Research Laboratories, Rahway, NJ
The objective of this study was to determine the rapidityand consistency of the onset of analgesic efficacy with asingle dose of rofecoxib 50 mg, a selective cyclooxygenase(COX)-2 inhibitor approved for acute analgesia, across11 similarly designed acute pain studies. A combinedanalysis was performed on the 11 randomized, double-blind, placebo-controlled studies involving patients expe-riencing moderate to severe pain after surgical extractionof ≥2 third molars. Onset of analgesic efficacy was deter-mined by time to confirmed perceptible pain relief (thetime to perceptible pain relief for patients achievingmeaningful pain relief), using the two-stopwatch method.Two studies were excluded from the analysis since thismethodology was not used. The percent of patientsachieving confirmed perceptible pain relief was alsodetermined. 1219 patients treated with rofecoxib 50 mgwere included in the analysis. Overall, 60% were females,mean age was 21 years, and 66% had moderate pain atbaseline. The median time to confirmed perceptible painrelief was 34 minutes (95% CI, 31 to 38 minutes). Sta-tistical tests of the hazard ratio did not detect significantheterogeneity across studies (P = 0.126), and estimates ofmedian time to confirmed perceptible pain relief in 10 of 11 studies were within 10 minutes of the combinedestimate. Seventy seven percent of rofecoxib patientsachieved confirmed perceptible pain relief. In this com-bined analysis, a single dose of rofecoxib 50 mg providedanalgesic efficacy with onset in approximately a half hourdemonstrated across numerous studies. These resultssupport the notion that once daily rofecoxib acts rapidly,consistent with a desired characteristic of a drug used inthe treatment of acute pain.
535Research (Clinical)
Onset of Efficacy with Rofecoxib, Celecoxib, andAcetaminophen in Osteoarthritis: the Vact-2 Trial
GP Geba, MD, MPH1, AL Weaver, MD2, AB Polis, MA1,RA Petruschke, PharmD1,TJ Schnitzer, MD, PhD3
Abstracts 103
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

1Merck and Co., Inc.West Point, PA, 2Arthritis Centerof Nebraska, Lincoln, NE, 3Northwestern University,Chicago, IL.We compared onset of efficacy over the first 6 days of therapy of the selective inhibitors of cyclooxygenase(COX)-2, rofecoxib (ROF) and celecoxib (CEL), and acet-aminophen (ACET) as a secondary endpoint in a random-ized, double-blind trial of osteoarthritis (OA) patients,VACT-2. 1578 patients with OA of the knee wereenrolled. Patients received treatment with ROF 12.5 mg(n = 259), ROF 25 mg (n = 527), CEL 200 mg (n = 523), orACET 4000 mg (n = 269) daily for 6 weeks. Time-to-eventanalysis was performed using Wilcoxon’s rank test to eval-uate time patients first reported Good or Excellent PatientGlobal Assessment of Response to Therapy (PGART)during Days 1 to 6. Response during the onset period was also analyzed comparing time-weighted meanchanges from baseline of Western Ontario and McMasterUniversities (WOMAC) OA Index (visual analog scale[VAS], 0 “no pain” to 100 “extreme pain”) for PainWalking on a Flat Surface, Night Pain, Rest Pain, andMorning Stiffness. Demographics were similar acrosstreatment groups. The majority of patients were Cau-casian (88%), female (67%), median age of 62 years.Median time to a Good or Excellent PGART response wasDay 3, 4, 5, and 6 for ROF 25 mg, ROF 12.5 mg, CEL, andACET, respectively. Time to a Good or Excellent PGARTresponse was significantly quicker (p = 0.01) for ROF 25mg compared to CEL. All coxibs had significantly quickertime to response than ACET (p-values £0.035). For thefour WOMAC endpoints, both ROF 12.5 mg and ROF 25mg had significantly greater reductions compared to CEL(p-values <0.05) and ACET (p-values <0.01). In conclu-sion, ROF 25 mg provided significantly quicker onset ofOA efficacy compared to CEL 200 mg based on PGART.All coxibs provided quicker onset than ACET 4000 mgbased on PGART. Response during the onset period withboth ROF doses was superior to response with CEL orACET based on WOMAC assessments.
536
Oral Transmucosal Fentanyl Citrate Used toReduce Emergency Department Visits in MigrainePatients: A Prospective Open Label Trial
A recent study using the 1998 National Hospital Ambulatory Medical Care Survey (NHAMCS) looked at100.4 million emergency department (ED) visits isolat-ing patients presenting with the diagnosis of migraine.811,419 patients were diagnosed having migraine and of these patients (84.8%) received a parenteral agent. The most commonly used medication was meperidine.Adjunct anti-emetics were commonly administered with
parenteral opioids (89.8%) of the time. Opioid use, par-ticularly meperidine, exceeds that of recommended nono-pioid abortive migraine medications. (1) The impact ofthese visits translates to an estimated cost of lost produc-tivity ranging from $1.2 billion to $17.2 billion. (2) Wefollowed 20 patients (16 female and 4 male) with migrainefor 6 months with pre-study average monthly ED visits of2.8. Home Administration of a single Oral transmucosalfentanyl lozenge was used as a rescue medication in lieu of parenteral opioids normally administered at an ED.Patient subjective response was measured to assess effi-cacy and average visits to the ED were revisited after theinitiation of therapy. Patients were followed for 24 weeks.The dosage was not changed unless the patients related noefficacy at the starting dose of 400 mcg. Increases weremade in 400 mcg increments. No one received greaterthan 1600 mcg with and average dose of 700 mcg. 16patients had no ED visits in 24 weeks, 2 patients had 1visit. 1 patient self discontinued due to nausea and seda-tion and 1 self discontinued due to disorientation. Noanti-emetics were used. In summary oral transmucosalfentanyl citrate (Actiq ® Cephalon Inc.) appears to be anexcellent rescue medication for migraine and in this studydrastically reduced ED visits. Additional placebo-controlled studies are clearly needed to elucidate the fentanyl citrate lozenges place in the treatment ofmigraine.
References
1 Vinson DR. Treatment patterns of isolated benignheadache in US emergency departments. Ann EmergMed 2002 Mar;39(3):215–22.
2 Lipton RB, Stewart WF. Prevalence and impact ofmigraine. Neurol Clin. 1997;15:1–13.
537Clinical
Oxycodone HCl + Ibuprofen CombinationSignificantly Improves Analgesia Compared withOxycodone or Ibuprofen Alone
Steven E. Christensen, Jean Brown Associates,Inc.; Hugh Kenneth Findlay, JBA Research; MindiTurpin, JBA Research; Hongjie Zheng, ForestLaboratories, Inc.; Kenneth Newman, ForestLaboratories, Inc.Objectives: To compare the efficacy and safety of singledoses of an oral combination of oxycodone and ibuprofento that of either drug alone and placebo for the treatmentof postoperative pain. Methods: In a multi-site, double-blind, parallel-group study, patients with moderate tosevere pain following dental surgery were randomized to asingle dose of oxycodone/ibuprofen 5/400mg, oxycodone/
104 Abstracts
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

ibuprofen 10/400 mg, oxycodone 5 mg, oxycodone 10 mg,ibuprofen 400mg, or placebo, and evaluated for 6 hours post-dose. Primary efficacy parameters were Total Pain Relief(TOTPAR) and Sum of Pain Intensity Difference (SPID).Results: The 5/400 mg combination achieved a significantincrease in primary efficacy parameters compared with 5 mg oxycodone or ibuprofen alone, and the 10/400 mgcombination compared with 10 mg oxycodone or ibupro-fen alone (TOTPAR and SPID over 6 hours, all P < 0.05).There were no significant differences in TOTPAR and SPID values between the two combination treat-ments. The median times to onset of pain relief for oxycodone/ibuprofen 5/400 mg, 10/400 mg, ibuprofen400 mg, oxycodone 5 mg, and oxycodone 10 mg were~25.4, 22.5, 28.0, 67.3, and 63.4 minutes, respectively.Patients in the 5/400 mg group indicated a significantlyhigher degree of satisfaction on the global evaluation (GE)scale compared with those in the oxycodone 5 mg orplacebo groups (P < 0.001). GE scores in the 10/400 mggroup were significantly greater than those in the ibupro-fen (P < 0.05) or oxycodone 10 mg groups (P < 0.001). Themost common treatment-emergent adverse events, higherin the 10/400 mg than in the 5/400 mg combination, werenausea, vomiting, and somnolence. There were no seriousadverse events. Conclusions: Both drug combinationsprovided significantly and clinically superior analgesiacompared with each component alone or placebo. The5/400 mg combination was as effective as the 10/400 mgcombination and resulted in a lower incidence of adverse events. Both combinations were safe and well tolerated.
538Research
Patient Demographics and Treatment Patterns Associated with Fibromyalgia in aMedicaid Database
Jeff S. Markowitz, Health Data Analytics; Jeff R.Schein, Janssen Pharmaceutica, Inc.; Chureen Carter,Thomas Jefferson University/Janssen Pharmaceutica,Inc.; Norman R. Rosenthal, Ortho-McNeilPharmaceutical, Inc.Background: Fibromyalgia is associated with pain andmuscle tenderness. Sleep disturbance, chronic fatigue,and depression are common symptoms. Fibromyalgiapatients are likely to exhibit high consumption of health-care resources, including pain medications. However,there is limited knowledge about their prescription uti-lization. Objective: The objective of this descriptive studywas to characterize the demographics and treatment pat-terns of fibromyalgia patients. Methods: A retrospectivedatabase analysis was performed on Medi-Cal beneficiar-
ies having at least one index claim with a primary or sec-ondary fibromyalgia diagnosis from January 1996 to June2001. Patients with continuous enrollment for at least sixmonths after the index claim were included. Prescriptionclaims occurring after the index claim were analyzed.Results: A total of 25,984 subjects were diagnosed withfibromyalgia during the study period. The majority ofsubjects were female (69%) and 55% were younger than44 years of age. A total of 76% of subjects received painmedications; of these subjects, the mean number of pre-scriptions per year was 4.7 (SD = 6.1). Using the claim asthe unit of analysis, the four most commonly prescribedpain medications were acetaminophen with codeine(33%), ibuprofen (19%), tramadol (9%), and celecoxib(9%). More than half of all fibromyalgia subjects (51.6%)had at least one short-acting opioid prescribed; only 3.2%had a long-acting opioid prescribed. Antidepressant pre-scribing was common. About 43% of all subjects wereprescribed an antidepressant; 94% received a prescriptionfor a pain medication or an antidepressant, and nearly40% were prescribed both. Paroxetine, amitriptyline, and fluoxetine were the most frequently prescribed antidepressants. Conclusions: Fibromyalgia is a condi-tion with a high burden on patients and the healthcaresystem. A retrospective analysis of a Medi-Cal populationrevealed that fibromyalgia primarily affects females, and individuals in their most productive work-years.Treatment with analgesics and antidepressants iscommon.
539Research (Clinical)
Patient Global Assessment and Womac ResponseAmong Osteoarthritis Patients Treated withRofecoxib, Celecoxib, or Acetaminophen in theVact-2 Trial
GP Geba, MD, MPH1,TJ Schnitzer, MD, PhD2,AB Polis, MA1, RA Petruschke, PharmD1, and AL Weaver, MD3
1Merck and Co., Inc.,West Point,PA, 2Northwestern University, Chicago, IL, 3ArthritisCenter of Nebraska, Lincoln, NE.We evaluated the efficacy of selective inhibitors of COX-2, rofecoxib (ROF) and celecoxib (CEL), and acetamin-ophen (ACET) in osteoarthritis (OA) patients. 1578patients with OA of the knee (ROF 12.5 mg qd [n = 259],ROF 25 mg qd [n = 527], CEL 200 mg qd [n = 523], and ACET 1000 mg qid [n = 269]) were enrolled in a randomized, double-blind, 6 week trial. Patient GlobalAssessment of Response to Therapy (PGART) was ana-lyzed using two methods: 1) logistic regression analysis
Abstracts 105
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

comparing percentage of patients with Good or Excellent PGART at 2, 4, and 6 weeks, with PGART atWeek 6 as the primary endpoint and 2) cumulativeregression analysis of PGART at 2, 4, and 6 weeksaccounting for ordered categorical data (none, poor, fair,good, and excellent). Comparison of treatment groups interms of Western Ontario and McMaster Universities(WOMAC) OA Index’s Pain, Stiffness, and PhysicalFunction Subscales was also performed. Demographicswere similar across treatment groups. The percentage ofpatients with Good or Excellent PGART was numeri-cally, but not significantly greater with ROF 25 mg com-pared to CEL at Week 6 (55.4% vs. 50.6%, p = 0.11).Significantly greater response was observed with ROF 25mg compared to CEL at Weeks 2 (55.5% vs. 48.6%, p =0.02) and 4 (57.5% vs. 50.8%, p = 0.03). Cumulativeregression analysis of PGART was significantly greaterwith ROF 25 mg compared to CEL (p = 0.035). TheROF 12.5 mg dose was not significantly different fromCEL. The coxibs provided significantly greater (p-values<0.05) PGART to ACET at each time point. For all threeWOMAC subscales, improvement over 6 weeks was sig-nificantly greater with ROF 25 mg compared to CEL.Improvements in WOMAC subscales over 6 weeks weresignificantly greater with all coxibs versus ACET (p-values £ 0.01). Given the totality of endpoints, ROF 25 mg provided greater improvement compared to CEL200 mg among OA patients in this study. ROF 12.5 mgand CEL were not significantly different. All coxibsdemonstrated superior efficacy to ACET. All treatmentswere generally well tolerated.
540Clinical
PDPH Following Intrathecal Pump Placement:Treatment with Fluoroscopy-Guided Blood Patch
Eduardo M. Fraifeld, MD. Medical Director DanvillePain Referral Center. Danville,VAIntroduction: Usage of intrathecal drug delivery systemshas significantly increased over the last decade. Thesesystems provide effective analgesia and control of spasticdisorders but are also know to cause complications.Reported complications include infection, fibrosis,catheter failure, persisted cerebrospinal fluid leak(PCSFL) and post-dural puncture headache (PDPH).Epidural blood patch (EBP) is considered the gold stan-dard treatment for PDPH and advocated for PCSFL;however, its use in patients with PDPH after intrathecalpump placement carries significant risk includingindwelling catheter damage or displacement. This casereport describes the successful treatment of a persistentPDPH in a young woman who underwent placement of
an intrathecal drug delivery system with development ofincapacitating persistent PDPH. Case Report: Describesthe case in detail, including level of insertion, type ofradiopaque catheter, contrast was injected to verifycorrect level of distal catheter tip prior to autologousblood injection, how much blood was injected time toresolution of headache, complications, etc. Conclusion:The technique is a safely and easily performed methodto obviate the risk of catheter damage when performingan EBP in the presence of an indwelling intrathecalcatheter.
542Research
Risk Factors Associated with Opioid Abuse in aMedicaid Population: A Case-Control Approach
Jeff S. Markowitz, Health Data Analytics; Jeff R.Schein, Janssen Pharmaceutica, Inc.; Nathaniel Katz;Chureen Carter,Thomas Jefferson University/JanssenPharmaceutica, Inc.Background: Addiction is a dysfunctional neurobiologi-cal disease with genetic, psychosocial, and environmen-tal factors. Characteristic behaviors include impairedcontrol over drug use, compulsive use, continued usedespite harm, and preoccupation with opioid use.Methods: This retrospective case-control study wasbased on a 20% random sample of subjects within theCalifornia Medicaid system (Medi-Cal) during the period1996 through June 2001. Inclusion criteria for cases werean ICD-9 diagnosis of opioid abuse with an observationperiod of at least three months prior to this index diagnosis. An equal number of controls were randomlyselected without a diagnosis (primary or secondary) ofopioid abuse. Variables examined as possible risk factorsduring the observation period, included demographics,clinical variables (surgery, hospitalization, depression,and number of comorbid conditions), history of otherdrug abuse, and use of short-and long-acting opioids.Independent study variables were entered into a logisticregression model with opioid abuse as the outcome.Results: 429 subjects with a diagnosis of opioid abuse metthe study criteria. Subjects younger than age 65 had agreater risk of abuse compared with those over age 65.Ages 30 to 44 had the highest risk of abuse (adjusted oddsratio [AOR] = 12.1, 95% CI = 6.8, 21.5). Other signifi-cant risk factors for abuse were male gender (AOR = 2.2,95% CI = 1.6, 3.1), depression (AOR = 1.8, CI = 1.2, 2.8),hospitalization (AOR = 2.4, 95% CI = 1.7, 3.4), and useof short-acting opioids (AOR = 1.7, 95% CI = 1.2, 2.4).Risk of abuse with short-acting opioids appeared to occurin a dose-response manner; adjusted odds ratios were 1.3 (95% CI = 0.8, 2.1), 1.8 (95% CI = 1.1, 2.9), and 2.3(95% CI = 1.4, 3.8), for low-, medium, and high-dose
106 Abstracts
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

short-acting opioid use, respectively. Conclusions: Malegender, younger age, depression, hospitalization, and useof short-acting opioids were significant risk factors inunadjusted and adjusted analyses. Additional research iswarranted to further characterize determinants of opioidabuse.
543Research (Clinical)
Sexual Dysfunction in Cancer Survivors onChronic Opioid Medications
Arun Rajagopal M.D., Rena Vassilopoulou-Sellin M.D.,Eduardo Bruera M.D., MD Anderson Cancer CenterSexual dysfunction is a common problem in cancer survivors. Causes are disparate, including the effects ofcancer therapy, negative self-image, chronic anxiety, ordepression (1,2). Chronic opioid therapy as a cause ofsexual dysfunction has not been studied. The purpose of this study was to estimate the prevalence of sexual dysfunction in cancer survivors consuming chronic high-dose opioid medications for cancer-related painsyndromes. We chose the Sexual Desire Inventory (SDI)since it is a validated tool that specifically addresses sexualdesire in the absence of consummatory behavior andspecifically assesses dyadic (activity with another person)vs. solitary (engaging in sexual behavior by oneself)desire(3). Our data set includes 20 patients. Male cancersurvivors whose morphine-equivalent daily dose was atleast 200 mg were included. The results of our study areshown in the table. Although the SDI questionnaire hasnot been previously used in the cancer survivor popula-tion, it has been used to assess sexual desire in a healthyadult population(4). Our data demonstrates a significantdegree of sexual dysfunction in this population. Ourmean dyadic score is approximately two standard devia-tions and our solitary score is approximately one standarddeviation below the mean for healthy adults. We postu-late that chronic opioid therapy may lead to a centralhypogonadic state. This is currently being assessed in aparallel study. Our study has some limitations. Sexualdysfunction is inherently difficult to assess and in thecancer population, there are many factors. In order todemonstrate a stronger association between opioid con-sumption and sexual dysfunction, a control group ofcancer survivors not using chronic opioid therapy willneed to be studied.
Study Group, Healthy Adults(4), n = 20 n = 90
SDI, Dyadic Score 23.9 +/- 15.7 42.8 +/- 8.9SDI, Solitary Score 1.3 +/- 1.9 6.5 +/- 4.8
References
1 McKee AL, Schover LR. Sexuality Rehabilitation.Cancer 2001;92:1008–12.
2 Schover LR, Montague DK, Lakin MM. Sexualproblems. In: DeVita VT, Hellman S, Rosenberg SA,editors. Cancer: principles and practice of oncology.5th ed. Philadelphia: Lippincott-Raven:1997:2857–72.
3 Spector IP, Carey MP, Steinberg L. The SexualDesire Inventory: Development, Factor Structure,and Evidence of Reliability. J Sex & Marital Ther.22(3):175–90, Fall 1996.
4 King BE, Allgeier ER. The Sexual Desire Inventoryas a Measure of Sexual Motivation in College Students. Psych Reports 2000;86:347–50.
544
Single-Dose Parecoxib Sodium, a Novel COX-2Selective Inhibitor, Improved Analgesic Efficacyand Length of Stay Following LaparoscopicCholecystectomy
H. Minkowitz, MD;1 G. Joshi, MD;2 T. J. Gan, MD;3 E.Viscusi, MD;4 R. Cheung, PhD;5 R. C. Hubbard, MD;6
C. Chen, Pharm.D.;6 J. G. Fort, MD5
1Memorial Hermann–Memorial City Hospital,Houston,TX; 2University of Texas, SouthwesternMedical Center, Dallas,TX; 3Duke University MedicalCenter, Durham, NC; 4Jefferson Medical College,Thomas Jefferson University, Philadelphia, PA;5Pharmacia Corporation, Peapack, NJ; 6PharmaciaCorporation, Skokie, IL
Objectives: To assess the impact of a single preopera-tive 40 mg dose of parecoxib sodium (parecoxib), theprodrug of valdecoxib, on fentanyl use and maximal pain scores following laparoscopic cholecystectomy.Methods: This multicenter, randomized, double-blind,parallel-group trial assessed the efficacy and safety ofparecoxib. Parecoxib 40 mg IV or placebo was adminis-tered 30 to 45 min preoperatively. Patients received standard-of-care (SOC) fentanyl on demand for painduring the immediate postoperative period. The amount of fentanyl consumed from the time of wakingthrough each of the first 4 h (0–60, 0–120, 0–180, 0–240 min) was recorded and compared between treatmentgroups using ANOVA with treatment as a factor.“Maximal Pain” scores were measured at 240 min usinga categorical scale, and compared between groups using Fisher’s Exact Test. Actual time, and time to “eli-gibility for discharge” from the postanesthesia care unit(PACU) and step-down unit, was recorded by clinicians.Results: From 0 to 240 min, patients in the parecoxibgroup required significantly less fentanyl (P = 0.011)than those receiving placebo. “Maximal Pain” was
Abstracts 107
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022
108 Abstracts
characterized as less severe in the parecoxib group (P = 0.031). Step-down unit length of stay (LOS) was shorter in the parecoxib group than in the placebogroup, with similar trends for PACU LOS (Table). Clinicians judged more patients “eligible” for transfer(from PACU to step-down unit) after 30 min in thePACU (25% in the parecoxib group versus 13% in theplacebo arm; p = 0.02). Conclusions: Preoperativeadministration of a single dose of parecoxib 40 mg IV,as an adjunct to SOC, resulted in significant reductionsin opioid requirements and reduced maximal pain levelspostoperatively. Parecoxib-treated patients also dem-onstrated improvements in measures of LOS and eligibility for transfer/discharge following laparoscopiccholecystectomy.
In-hospital Analgesic Efficacy and Length of Stay
Parecoxib40 mg Placebo(n = 119) (n = 104) p value
Fentanyl consumption,mcg (SD)
0–240 min 152.8 (106.4) 192.9 (127.8) 0.0110–60 min 107.7 (70.0) 125.5 (81.6) 0.0820–120 min 133.4 (83.2) 160.0 (100.6) 0.0320–180 min 145.3 (98.6) 179.1 (114.8) 0.019
Step-down unit LOS, 6.9 (8.4) 9.8 (11.7) 0.04hours (SD)
PACU LOS, 125 (80) 129 (76) 0.74min (SD)
Sponsored by Pharmacia Corporation and Pfizer Inc
545Research
Surface EMG Signal Intensity Correlation withSeverity of Symptoms in Chronic Paraspinal Pain
Alex Ambroz, MD,VA Medical Center and FirstPriority Medical Choice, Martinsburg,WV, EugeneBenjamin, MD,VA Medical Center, Martinsburg,WVand Clara Ambroz, MD, Disability Evaluation Service,Romney,WV.Objective validation of the complaint of pain is a majorproblem in treating chronic spinal area pain, and chronicpain in general. While patient symptom description andimaging studies help to refine pain assessment, there is need for an objective test of pain perception, and measurement of pain magnitude.
The degree of paravertebral muscle spasm can cor-relate with pain magnitude, but manual assessment ofspasm on physical examination, is imprecise. Staticsurface electromyographic (EMG) signals are believed tobe a form of objective measurement of myospasm.
In our study, we correlated surface EMG signal inten-sity with mild to severe pain levels reported in patientswith paraspinal pain. Two groups of 30 patients were categorized as having mild or severe pain based upon a scoring system. Subjective symptoms, range of motionmeasurements, pain inventories, imaging studies,employment status, drug seeking behavior, and use ofmedications were assessed in determining an overallpicture of pain severity.
Paraspinal surface EMG measurements were takenwith a Myovision 3000 apparatus and patients were exam-ined in a standing position. The mean electrical signal inmicrovolts of the “mild” pain group was 234.8 microvoltsand the mean signal for the “severe” pain group was1361.7 microvolts. A chi square analysis of the results,indicated that surface EMG (sEMG) signal intensity cor-related with pain complaints at a p level <0.01.
We found that sEMG measurements are a usefulobjective parameter in the evaluation of chronic spinalpain. This test is very inexpensive for patients, non-invasive, and a potential avenue for routine evaluation of chronic paraspinal pain.
546
Clinical Research
Symptomatic Hypogonadism Among Men onChronic Opioid Therapy for Pain
Elizabeth Miller PharmD, Daniel Brookoff MD, RogerCicala MD, Jefferey Jernigan MD, Brigitte Messenger;Methodist University Pain InstituteOpioid therapy has been associated with hypogonadismin males being treated with intrathecal morphine forchronic pain or with oral methadone for opioid depend-ence. We assessed the incidence of symptomatic hy-pogonadism among men being treated with oral ortransdermal opioids for chronic pain. In this case series,54 consecutive adult males treated with daily opioids for chronic pain for greater than three months wereassessed for symptoms of hypogonadism using validatedquestionnaires. Subjects who screened positive forsymptoms had serum measured for total testosterone,FSH, LH, prolactin and thyroid function tests. Forty ofthe 54 subjects (74%) reported symptoms of hypogo-nadism. Twenty-four of the 40 symptomatic patients(60%) had total serum testosterone levels below 300 ng/dL. Hypotestosteronism was not associated withage, alcohol use, medical or psychiatric diagnosis or theuse of other testosterone-lowering medications. FSHand LH levels were normal or low in all 24 patientswith symptomatic hypogonadism. Only two patients hadabnormal prolactin levels and these were less than 50%above the top normal value. Over the entire group of
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

patients, symptomatic hypogonadism was found in 56%on morphine (5/9), 55% on oxycodone (11/20), 45% ontransdermal fentanyl (4/9), and 43% on methadone(3/7). No patients on hydrocodone (0/6) or oral trans-mucosal fentanyl (0/1) reported symptoms of hypo-gonadism. Two patients were on combinations oflong-acting opioids. Symptomatic hypogonadsim didnot appear to be correlated to opioid dose. Symptomatichypogonadism is common among males with chronicpain on opioid therapy. Endocrine tests suggest that thisis more likely due to primary suppression of the releaseof gonadotropin-releasing factors by the hypothalamusor selective suppression of gonadotropins rather thanprimary gonadal failure or hypersecretion of prolactin.The causal role for opioids or for chronic pain itself inthe genesis of symptomatic hypogonadism has yet to beelaborated.
549Research
The Impact of Aging in Caucasian AmericansPresenting for Chronic Pain Management
Carmen R. Green, M.D., University of Michigan;Andrew M. Nagrant, MPH, University of Michigan;Tamara A. Baker, Ph.D., University of MichiganOlder adults may be more adversely affected by chronicpain than younger people, but differences based upon agehave not been well defined. Physical and psychologicalwell-being in persons with chronic pain are importantconsiderations for an aging population. We evaluated theimplications of chronic pain on Caucasian Americans presenting for initial treatment at a tertiary care paincenter. A secondary analysis of a database, which containsthe McGill Pain Questionnaire, Beck Depression Inven-tory, Pain Disability Index, and Post Traumatic ChronicPain Test was performed. Caucasian Americans <50 years(n = 3392) and 50+ years (n = 1906) were compared. Themajority of the sample were women. Chi-square analysisshowed that increasing age was associated with increasedpain severity in the week prior to the initial visit to the paincenter, better control of pain, better overall mood,decreased irritability, decreased tenseness/anxiety, increasedcoping success, greater enjoyment of work, and less fatiguein the morning (p < 0.05). Increasing age was associatedwith less reported limitation of activities due to pain, a smaller reported change in satisfaction from social/recreational activities due to pain, a smaller reportedchange in ability for social/recreational activities due topain, a greater reported change in ability for householdchores due to pain, and a smaller reported change in rela-tionship with spouse, family, or significant other due topain (p < 0.05). No significant differences were observedwith level of pain at the time of the visit, suffering, fatigue,
and ability to work. Logistic regression analysis showedthat after adjustment for gender, marital status, education,and duration of pain, older Caucasians reported lower levelsof pain, depression, and PTSD than younger Caucasians(p < 0.05). However, there were no differences in level ofdisability. Prospective studies are needed to determine thedirectionality of time between reported conditions.
550Research—Clinical
The Impact of Opioid Analgesic Use onFunctioning and Distress in Patients with Chronic Headaches
Jeffrey Rome, M.D., Barbara Bruce, Ph.D., ChrisSletten, Ph.D., Jaxon Hodgson, M.A., CynthiaTownsend, Ph.D., and Connie Luedtke, R.N., MayoClinic Comprehensive Pain Rehabilitation CenterControversy exists regarding the use of chronic opioidsfor treating intractable headaches. Concern about analgesic dependence and analgesic rebound headachesmakes the use of opioids in this population problematic.The present study examined chronic headache patientsreferred to the Mayo Comprehensive Pain RehabilitationCenter. Pain severity, functional status and distress wereexamined in patients using and not using opioids. Subjects consisted of 142 patients (73% female) withchronic headaches. The patients completed question-naires related to functioning (MPI), depression (CES-D),and coping responses (CSQ) at admission and upon discharge. Of this population, nearly half (n = 72) weretaking opioids at admission and the remaining population(n = 70) were not taking opioids. Upon discharge, noneof the patients were taking opioids which is a typical reha-bilitation goal. Analysis of variance revealed that com-pared to headache sufferers who were not using opioidsat admission, patients using opioids reported significantlygreater levels of pain severity (p < 0.01), interference in daily activities (p < 0.01), and catastrophic coping (p < 0.05). The patients did not differ in level of depres-sion, perceived self-control over life or general activitylevel. Additionally, repeated measures ANOVAs to com-pare admission and discharge data revealed both groupsreported significant decreases in pain severity (p < 0.01),interference in daily activities (p < 0.01), catastrophizing(p < 0.01) and depression (p < 0.01) with significantincreases in perception of life control (p < 0.01) andgeneral activity level (p < 0.01). Discharge data revealedno significant differences on any of the measures betweenthe patients who had previously taken or not takenopioids after completing pain rehabilitation treatment.These findings suggest intractable headache suffererstreated with chronic opioids have greater pain severityand interference in functioning due to pain than
Abstracts 109
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

headache patients who do not take opioids. Also, the datasuggests that pain rehabilitation appears to be as effica-cious in the treatment of headache patients on chronicopioids as those without.
551Research
The Incidence of Constipation in Chronic PainPatients Taking Long-Acting Opioids
Peter S. Staats, Johns Hopkins Medical Institute; JeffS. Markowitz, Health Data Analytics; Jeff R Schein,Janssen Pharmaceutica, Inc.; Gary Vorsanger,Janssen Pharmaceutica, Inc.Background: Constipation is a common side effect ofopioid therapy that may be persistent. While rarely fatal,constipation may lead to severe decrements in patients’quality of life. Objective: To determine the incidence ofconstipation in chronic pain patients taking three differ-ent long-acting opioids for malignant or nonmalignantpain. Methods: Claims data were analyzed from theMedi-Cal database from January1996 through March2001. A retrospective cohort design was used to studythree groups of adult subjects with at least 3 months oftreatment with one of the following long-acting opioids(LAOs): transdermal fentanyl system, oxycodone HClcontrolled release (CR), or morphine sulfate controlled-release (CR). The main outcome variable was a primaryor secondary ICD-9 diagnosis of constipation. Controlvariables included demographics, cancer diagnosis,surgery, depression diagnosis, and morphine equivalentsfor short- and long-acting opioids. Logistic regressionwas used to control for potential confounding variables.An alpha level of <0.05 (2-tailed) was used. Results: Atotal of 1,836 subjects (601 on transdermal fentanyl, 721on oxycodone CR, and 514 on morphine sulfate CR) meteligibility criteria and were analyzed. Subjects averaged58.8 years and 63% were female. Crude (unadjusted)rates of constipation were 3.7% for transdermal fentanyl,6.1% for oxycodone CR, and 5.1% for morphine sulfateCR. When potential confounding variables were con-trolled in logistic regression using transdermal fentanylas the reference group, the adjusted odds ratio for oxycodone CR was 1.78 (95% CI = 1.05, 3.03; p = 0.0337)and for morphine CR, 1.44 (95% CI = 0.80, 2.60; NS).Conclusions: Relative to transdermal fentanyl and afteradjusting for potential confounders, a significant increase(78%) in the risk of constipation was observed in chronicpain patients prescribed oxycodone CR and an increasednonsignificant (44%) risk for morphine sulfate CR. Additional studies are recommended in other populationsto aid in the generalizability of these findings.
552
The MIND Registry: An Observational Database ofPatients Treated with MYOBLOC® (Botulium ToxinType B)
1C. O’Brien, MD, 1M. Royal, MD, 1C.Towey, 1D. BeversObjective: The MIND (Medical Index for Neuromus-cular Data) Registry captures the “real-world” usage ofMYOBLOC® (Botulium Toxin Type B) by physiciansacross the United States. Through the MIND Registry,data are collected, evaluated and provided on a quarterlybasis to participating physicians. Methods: Investigatorsreceive information about the MIND Registry throughElan Medical Affairs, the MIND Helpdesk and a neurology website. There are no restrictive criteria, as ina clinical trial. Any patient treated with MYOBLOC maybe enrolled in the MIND Registry. The Data CollectionForms capture the following key data: demographics,primary condition and diagnosis, MYOBLOC treatmentinjection (e.g. muscle selection; dose units per muscle;total number of injections per diagnoses), patient satis-faction and outcome assessments, and serious adverseevents. Results: As of November 05, 2002 patient enroll-ment equals 534. The tables below contain data regard-ing the following indications: spasmodic torticollis,idiopathic torsion dystonia, other focal dystonias(approximately 50% of the total patient enrollment). Themean dose of MYOBLOC was 9,150 units/ml over 2,566muscles. MYOBLOC reduced the severity of patientrated signs and symptoms, including pain and “bother”levels at follow-up visits. Based on, 160 follow-up visits,70.6% of patients rated at least a one-point reduction inpain scores and 45.0% of patients rated a two-pointreduction in pain scores. (See table below). Conclusions:Data captured in the MIND Registry provide valuablemedical and safety information to clinicians. Physiciansmay benchmark their use of MYOBLOC against thenational aggregate data. To date, we know MYOBLOCis used in a wide range of focal dystonia syndromes witha high degree of patient satisfaction. Dose and muscleselection vary from center to center. Through thisresearch initiative, an understanding of practice patternsmay lead to improved treatment algorithms. Future data-base analyses will reveal any alteration of dose over time,differences in response by patient type (e.g., A-responsive vs. A-resistant) and other clinical questionsraised by the scientific advisory group.
1 Elan Pharmaceuticals, Inc., 7475 Lusk Boulevard, San Diego,California.
110 Abstracts
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

553Clinical
The Role of Gadolinium in Interventional PainManagement as an Alternative to IodinatedContrast Agents
Annu Navani, MD, Gagan Mahajan, MD, Paul Kreis,MD, Scott M. Fishman, MD
Division of Pain Medicine, University of California,DavisSummary: Gadolinium contrast was used instead of an iodinated contrast in patients with a history of allergic reaction to iodinated compounds. Preliminaryresults suggest gadolinium is a safe alternative that can be used to verify correct needle placement during fluoroscopically-guided interventional pain managementprocedures. Methods: We injected 2–4 ml of gadolinium(gadodiamide [Omniscan]) 0.5 mmol/ml into fourpatients to confirm a cervical epidurogram (two), alumbar epidurogram (one) and a piriformis myogram(one). Results: Gadolinium localized successful needleplacement in all four patients. None reported any imme-diate or delayed side effects. Discussion: Gadoliniumcontrast is used as an alternative in interventional proce-dures in patients with an iodine allergy. More recently,gadolinium-based contrast agents have been used suc-cessfully in discography.1,2 There is decreased risk ofadverse reactions with contrast agents containinggadolinium versus iodine. The reported incidence ofadverse effects with intravenous gadolinium is 1–3%.1,3
Theoretically, the high KeV of contrasts containinggadolinium versus iodine allows for the use of higher kVpimaging without the loss of image enhancement, result-ing in less radiation exposure to the patient and opera-tor.3,4 However, the primary difficulty with usinggadolinium contrast relates to its inferior fluoroscopicimaging quality secondary to the low concentration ofgadolinium (0.5 mmol/mL).3 However, a larger volumeor higher concentration of gadolinium can be used tocompensate for this. We successfully demonstrated anepidurogram or myogram using only 2–4 ml of contrast.Finally, because of concerns of neurotoxicity related toGd-DTPA when used in the vicinity of the neuraxis,caution is warranted in terms of the dose and the preciseplacement of Gd-DTPA.1
References
1 Slipman CW, et al. Pain Medicine 2002;3:1:23–9.2 Huang TS et al. Spine 2002;27:839–43.3 Spinosa DJ, et al. Journal of vascular and interven-
tional radiology 2000;11:8:985–90.4 Spinosa DJ, et al. American journal of Radiology
1999;173:1403–9.
554Clinical Research
Trans-Biceps Femoris Knee Block in OperativeFoot and Ankle Patients after General Anesthesia:Results in 475 Patients
Muir JJ, Mayo Clinic Scottsdale; Keyarash AB,TucsonOrthopedic Institute; Kile TA, Mayo Clinic Scottsdale;Claridge RJ, Mayo Clinic Scottsdale, Quach TD,Mayo Clinic Scottdale:Weinmeister KP. Mayo Clinic ScottsdaleFoot and ankle surgical patients often have severe post-operative pain. Traditionally, this pain has been managedwith parenteral narcotic analgesics. The need for effec-tive perioperative pain control following foot and ankleprocedures has lead many centers to use nerve blocks tomanage post operative pain in these patients. Currentlymost centers perform an ankle block or popliteal blockfor post operative analgesia. With few reported excep-tions, popliteal nerve blocks are performed in awakepatients using an insulated catheter with a nerve stimu-lator. No study to date has addressed the efficacy andsafety of lateral popliteal blocks in fully anesthetizedpatients.
The purpose of our study was to determine the effi-cacy and safety of performing the lateral block followingadministration of general anesthesia in a large group offoot and ankle surgical patients. 475 consecutive patientsreceived a popliteal block, after general anesthesia wasinduced, using a modification of the lateral technique ofMcLeod et. al.(1). Following surgery all patients, with theexception of those receiving hind foot or mid footarthrodesis, were discharged home. They were then seenon the first or third postoperative day for dressing changeand the effective duration of the block was noted.Patients were then followed at 1, 6, and 12 weeks and afinal time at 6 months postoperatively and all complaintsrelated to the blocks were noted in the chart. Post oper-ative pain control was present for a minimum of 12 hoursafter the procedure. (Range 12–26 hours)
On average, patients needed 4 narcotic analgesictablets by mouth during the first 24 hours. 464 of our 475(97%) reported being highly satisfied with their post-operative pain control. There were no reported cases ofneurologic injury at the six-month follow-up visit.
Reference
1 Lateral Popliteal Sciatic Nerve Block ComparedWith Ankle Block For Analgesia Following FootSurgery. McLeod DH;Wong DHW;VaghadiaH;Claridge RJ; Canadian Journal of Anaesthesia vol42 p. 765–69, 1995.
Abstracts 111
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022

555Clinical
Treatment of Carpal Tunnel Syndrome
Marco Pappagallo, MD; Brenda Breuer, PhD, MPH;Kevin Sperber, MD; Kiril Kiprovski, MD; Barry Snow,PhD; Hospital for Joint Diseases, Mount Sinai NewYork University Health, NYCMyobloc (botulinum toxin type B), FDA-approved fortreatment of neck pain and abnormal neck position incervical dystonia, is also used “off-label” for other painfulconditions, including migraines and backaches. While itsanalgesic mechanism remains undetermined, Myobloc-associated improvement in pain and paresthesias suggestit may alleviate carpal tunnel syndrome (CTS)-associatedinvoluntary painful muscular hand spasms. We were thusmotivated to conduct a randomized, double-blind,placebo-controlled clinical trial of Myobloc in patientswith a clinical diagnosis suggestive of, and nerve con-duction velocity abnormalities consistent with, CTS. Asour hypothesis is that Myobloc alleviates pain/discomfortnot associated with nerve injury, subjects with severeCTS were excluded. We also excluded patients withrheumatoid arthritis, connective tissue diseases, vasculi-tis, untreated hypothyroidism, and acromegaly.
We report results for the first two patients, TR andYS, both white females, whose data were unblindedbecause of adverse events described below. TR received5000 units of Myobloc; YS received 7500 units. The dosewas divided into three 0.5 ml doses, each injected, respec-tively, into the 3 hypothenar muscles (palmaris brevis,opponens digiti minimi, and flexor digiti minimi)anatomically fixed to the transverse ligament, the roof ofthe CT.
Each patient complained of 5th finger stiffness andweakness. YS reported these symptoms also in the 4th
finger. Additionally, she was unable to adduct her 5th
finger. All adverse events were resolved within 6 weeks.On an 11-point pain rating scale TR reported a decreaseof 6 points by week5 post-injection, and YS a decrease of3 points by week3. Pain reductions were stable throughthe end of follow-up; i.e., week12. Each subject indicatedthat her pain relief more than compensated for theadverse events. We continue our trial, but limit theMyobloc dose to 2500 units and the volume to 1.0 ml.There have been no more adverse events.
556Clinical
Use of Gadolinium for Discography in Iodine-Allergic Patients
Douglas S. Fenton, MD1, B.Todd Sitzman, MD,MPH2, Leo F. Czervionke, MD1, Divisions of
Neuroradiology1 and Pain Medicine2; Mayo Clinic,Jacksonville, FLIntroduction: Discography is a widely utilized techniqueto assess intervertebral disc pathology. It is most oftenperformed with iodinated contrast agents, allowing forexcellent fluoroscopic visualization and post-discographyCT evaluation. However, in patients with documentedsevere allergic reactions to iodinated contrast, the efficacyof alternative contrast agents (e.g., gadolinium) fordiscography is unknown. Gadolinium, a paramagneticcontrast agent originally approved for clinical use inMRI, has a significantly lower rate of severe allergic reac-tions than iodinated contrast agents: 1 : 400,000 versus 1: 500 for ionic iodinated and 1 : 2,500 for non-ionic iodinated contrast agents. We report on the efficacy ofgadolinium for discography in six patients with historiesof allergic reactions to iodinated contrast agents.Methods: Six patients with documented iodinated con-trast allergic reactions were scheduled for discographyand post-discography CT evaluation. Premedication(steroid, H1- and H2-blockers) as prophylaxis againstcontrast allergy was administered. Lumbar discs wereinjected with either Iohexol 300 mg/mL (Omnipaque®)or gadolinium 287 mg/mL (Omniscan®), such that bothcontrast agents were used in each patient. Subjective flu-oroscopic visualizations of the discs were performed andradiographs of each disc were obtained for later evalua-tion as to the adequacy of contrast visualization. Allpatients underwent post-discography CT evaluation.The CT images were evaluated for adequacy of contrastvisualization and for relative density, measured inHounsfield units (HU). Results: The gadolinium injecteddiscs were less well visualized fluoroscopically than theiodine injected discs. However, gadolinium was sufficientto demonstrate intranuclear filling and annular morphol-ogy. Fluoroscopic visualization of the lower lumbar leveldiscs in the lateral projection was poorer, regardless ofthe contrast used, due to decreased X-ray penetrance asa result of increased soft tissue and iliac bones. CTdemonstrated the relative density of gadolinium to be 43% that of the iodinated contrast (797 HU versus1870 HU). However, this density was more than adequateto demonstrate disc anatomy and annular tears. Nopatient experienced an adverse reaction to the intradiscalgadolinium. Conclusion: Gadolinium is an acceptablealternative to iodinated contrast agents for discographyin those patients with a history of previous severe allergic reactions to iodine. Given the relative decreasedvisualization of gadolinium fluoroscopically, we recom-mend the use of high quality fluoroscopy units in patientsundergoing gadolinium-contrast discography. In selectcases, it may be necessary to arrange for a post-discography CT to demonstrate subtle intradiscal fillingpatterns and disc annulus morphology.
112 Abstracts
Dow
nloaded from https://academ
ic.oup.com/painm
edicine/article/4/1/91/1816761 by guest on 30 May 2022
Related Documents











