R econstitution of the T- cell C ompartment P ost - A llogeneic H aematopoietic C ell T ransplantation A thesis submitted in fulfilment of the requirements for the degree of Doctor o f Philosophy by Paul Raymond Fallen Anthony Nolan Research Institute Royal Free and University College Medical School F ebruary 2002

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

R e c o n st it u t io n of the T -cell C o m pa r t m e n t P o s t -
A llo g eneic H a em ato po ietic C ell T r a n sp l a n t a t io n
A thesis submitted in fulfilment of the requirements for
the degree of Doctor o f Philosophy
by
Paul Raymond Fallen
Anthony Nolan Research Institute
Royal Free and University College Medical School
February 2002

ProQuest Number: 10011221
All rights reserved
INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted.
In the unlikely event that the author did not send a complete manuscript and there are missing pages, these will be noted. Also, if material had to be removed,
a note will indicate the deletion.
uest.
ProQuest 10011221
Published by ProQuest LLC(2016). Copyright of the Dissertation is held by the Author.
All rights reserved.This work is protected against unauthorized copying under Title 17, United States Code.
Microform Edition © ProQuest LLC.
ProQuest LLC 789 East Eisenhower Parkway
P.O. Box 1346 Ann Arbor, Ml 48106-1346

Abstract
The effective reconstitution o f the T-cell compartment post-haematopoietic cell transplantation
(HCT) is essential for the re-establishment o f immunity to infectious pathogens. The primary
aim o f this thesis is to analyse the kinetics and quality o f T-cell reconstitution in HCT
recipients. This has been achieved using T-cell phenotyping to enable identification o f naïve,
memory and effector T-cells and by measuring the number o f circulating thymic emigrants
using the TREC assay.
We know that there are at least two pathways by which T-cell regeneration can occur after
HCT, thymic-dependent and thymic-independent. The results presented in this thesis
demonstrate that thymic-independent pathways rapidly regenerate the memory and effector T-
cell pool within 6 months post-HCT. Thymic-dependent T-cell regeneration was detected by 3
months post-HCT in some patients but generally, detection o f circulating thymic emigrants
was delayed until 6-9 months post-HCT. In addition, the number o f circulating thymic
emigrants was highly variable between different individuals.
In an analysis o f the factors affecting thymic-dependent T-cell regeneration, increasing patient
age and the presence o f clmical graft-versus-host disease (GVHD; either acute or chronic)
were the two most important factors predicting low or absent thymic output. Cord blood
transplant recipients also had reduced levels o f thymic emigrants compared with age-matched
recipients o f peripheral blood or bone marrow transplants raising concerns over the
reconstitution potential o f cord blood cell grafts. Further results from a cohort o f severe
combined immunodeficiency (SCID) patients suggest that the administration o f some form o f
pre-transplant conditioning is essential for the engraftment o f donor stem cells and long term
maintenance o f thymic output.
Taken together, these results suggest that the thymus is capable o f repopulating the T-cell
compartment post-HCT in a diverse group o f patients. Furthermore, these results suggest that
strategies aimed at reactivating the thymus may be beneficial for older HCT recipients and
patients who have experienced episodes o f GVHD. Larger studies are essential to analyse the
effect o f post-transplant immunosuppression, individual conditioning regimens and the clinical
correlation between level o f thymic emigrants and susceptibility to infection.

Acknowledgements
I would like to thank my supervisor Dr. Paul Travers (my walking immunology textbook) for
his encouragement, advice and support during the last three years. I have particularly enjoyed
our conversations that were frequently ridiculous but often sublime. 1 would also like to thank
Prof. Alejandro Madrigal for giving me the opportunity to carry out my PhD at the ANRI and
for constantly pushing me further than I thought I could go. Thanks also go to Dr. Shara
Cohen for her help and support during the first year o f my project.
This project would not have been possible without the co-operation and input o f the clinical
staff from a variety o f transplant centres. Special thanks go to Prof. Grant Prentice and Dr.
Mike Potter for critically reviewing manuscripts; Dr. Mark Ethel and the rest o f the clinical
staff on Crowley Ward for collecting blood samples and for help in collecting and analysing
the necessary clinical data. 1 would also like to acknowledge Dr. Andrew Gennery, Dr. Adrian
Thrasher, Dr. Franco Locatelli, Dr. Susanne Matthes-Martin, Dr. Gerhard Fritsch and Dr.
Colin Michie for their input and ideas and for providing valuable blood samples from little
people with not much blood to give. 1 would also like to thank Dr. Antonio Guimares for
providing blood samples and clinical data.
Thank you to everyone at the Anthony Nolan Research Institute who made my time so
enjoyable. Special thanks go to Dr. Louise McGreavey (my partner in crime) for constant help
in organising and processing samples and for making sure there was never a dull moment. I
would like to thank Drs. Steve Marsh, Anthony Dodi, Ann Margaret Little and Linda Barber
for help, advice and guidance and to Pauline Dodi and Marjorie Lawton for proof-reading this
thesis. A big thank you also goes to the people who made evenings in the White Horse
bearable (while their absence would have made an evening in the White Horse enjoyable):
Neema (get a recording contract); Christian (for protecting the Mexican way o f life); Bronwen
(my Tunisian sock-merchant); Angus (for Rawhide and for laughing at any old rubbish);
Rafael (for being the first Matador preppie) and Sylvie (Ruskekiavich).
1 am especially grateful to my Mum and Dad for their support, enthusiasm and for being a
constant source o f inspiration; and to my sister for her friendship and for keeping me in line!
Finally, to Karen, thank you for being you.

This thesis is dedicated to my Grandparents
James and Elizabeth Reavey
and
Raymond and Agnes Fallen

Contents
C hapter 1; Introduction........................................................................................................ 1
The immune system ........................................................................................... 1
Thymic T-cell development............................................................................. 4
Phenotypic changes associated with thymocyte maturation into
CD4^ and CD8^ T -cells..................................................................................... 4
The thymic microenvironment and signals that drive thymocyte
maturation............................................................................................................. 6
Identification o f recent thymic emigrants................................................... 8
Thymic emigration and T-cell homing to secondary lymphoid organs 12
T-cell activation: mechanisms and requirements...................................... 13
Differentiation o f naïve T-cells into memory and effector ce lls 17
Differentiation o f naïve CD4^ T-cells to polarised Thl or Th2 subsets 19
Homeostatic control o f T-cell numbers and diversity............................... 20
Ageing and the T-cell compartment................................................................ 24
Haematopoietic cell transplantation (HCT)................................................. 27
HLA-matching and Graft-ver5W5-host disease (G V H D ).......................... 28
Current strategies for the prevention and control o f G VH D................... 30
Establishing antigen-specific peripheral tolerance..................................... 32
Graft-versus-leukaemia (G VL)......................................................................... 34
Immune reconstitution post-HCT...................................................................... 35
Thymic-dependent and thymic-independent T-cell recovery after HCT 37
A im s o f this th esis.................................................................................................. 39
C hapter 2: M aterials and M ethods........................................................................................ 41
Patients........................................................................................................................ 41
Processing o f peripheral blood samples............................................................ 42
Control blood and serum samples....................................................................... 42
Isolation o f peripheral blood mononuclear cells (PBM C s)......................... 42
Cryopreservation o f PBM Cs.................................................................................. 42

Positive selection o f CD4 and CDS subsets from PBM Cs........................ 43
Preparation o f cell lysates.................................................................................... 44
DNA extraction from whole blood................................................................... 45
DNA quantification by spectrophotometry................................................... 46
Flow cytometric analysis o f lymphocyte subsets......................................... 46
Measurement o f absolute lymphocyte and T-cell number in whole
blood......................................................................................................................... 46
Flow cytometric analysis o f T-cell subsets in PBMC populations 47
Additional antibodies........................................................................................... 49
Detection and quantification o f T-cell receptor rearrangement excision
Circles by radiolabelled quantitative, competitive PCR........................... 49
Detection o f signal joint TREC in healthy control blood samples 49
Polyacrylamide gel electrophoresis................................................................. 50
Preparation o f internal TREC standard for radiolabelled QC-PCR 51
Transformation o f the TREC standard plasmid........................................... 51
Miniprep DNA extraction................................................................................... 51
Restriction digestion o f miniprep D N A .......................................................... 52
Agarose gel electrophoresis................................................................................ 52
Maxiprep o f TREC standard plasmid.............................................................. 53
Dilution o f TREC standards................................................................................ 53
Radiolabelled quantitative-competitive PCR................................................. 54
Calculation o f TREC frequency by densitometry......................................... 55
Detection and quantification o f TREC by Real-Time PCR...................... 56
Transformation o f the Taqman® TREC standard plasmid......................... 56
Miniprep, maxiprep and restriction digestion analysis o f the Taqman®
TREC standard plasmid........................................................................................ 56
Optimisation o f the Taqman® standard curve................................................ 57
Real-Time quantitative PCR............................................................................... 57
Quantification o f TREC using Real-Time quantitative PCR.................... 58
T-cell functional assays......................................................................................... 58
Preparation o f T-cell lines.................................................................................... 58
Mixed lymphocyte reactions............................................................................... 59
Stimulation o f T-cell lines with anti-CD3 antibody or IL-2...................... 59
Analysis o f CD25 expression............................................................................. 59
Analysis o f the frequency o f IL-2 producing T -cells.................................. 60

Intracellular cytokine staining............................................................................. 60
Buffers and solutions............................................................................................. 60
C hapter 3: T hym ic-dependent versus thym ic-independent T -cell reconstitution
post-H C T ................................................................................................................... 63
Introduction............................................................................................................... 63
Results......................................................................................................................... 65
Recovery o f C D 3 \ CD4" and CD8^ T-cells post-HCT................................ 65
Development o f T-cell phenotyping to detect circulating naïve, memory
and effector T-cell subsets..................................................................................... 67
T-cell phenotyping strategy................................................................................... 73
Recovery o f naïve CD4^ T-cell numbers.......................................................... 74
Recovery o f memory and effector CD4^ T -cells............................................ 74
Recovery o f naïve CD8^ T -cells........................................................................... 76
Direct quantification o f thymic-dependent pathways.................................... 79
Detection o f TREC molecules in peripheral blood samples........................ 80
Quantification o f TREC molecules in CD4^ and CD8^ T-cells in 26
allogeneic HCT recipients...................................................................................... 80
Relationship between TREC and naïve T-cell numbers............................... 83
CD4^CD45RO*CD27' T-cells and thymic output........................................... 84
The recovery o f naïve CD4^CD45RO'CD27^ T-cells is dependent on
thymic output, whereas non-naïve CD4^CD45RO'CD27" T-cells evolve
in the absence o f thymic output........................................................................... 87
D iscussion................................................................................................................... 87
C hapter 4: Factors affecting T-cell reconstitution ........................................................... 92
Introduction................................................................................................................. 92
Results.......................................................................................................................... 96
Factors affecting thymic output in recipients o f allogeneic HCT 96
Age o f transplant recipient..................................................................................... 96
Graft-ver5W5-host disease........................................................................................ 98
T-cell depletion.......................................................................................................... 100
T-cell dose................................................................................................................... 103
Stem cell source: Peripheral blood versus bone marrow.............................. 104
Donor leukocyte infusions..................................................................................... 104

Pre-transplant conditioning regimens................................................................ 105
Campath-IH.............................................................................................................. 106
Total body irradiation (TBI).................................................................................. 107
Immunosuppression................................................................................................. 108
Cyclosporin A ............................................................................................................ 108
Corticosteroids........................................................................................................... 110
Factors affecting the recovery o f memory and effector T-cell subsets
post-allogeneic HCT................................................................................................ I l l
Age o f transplant recipient..................................................................................... I l l
Graft-ver5w^-host disease........................................................................................ 113
T-cell depletion.......................................................................................................... 113
T-cell dose................................................................................................................... 114
Stem cell source: Peripheral blood versus bone marrow............................... 114
Campath-IH............................................................................................................... 115
Total body irradiation.............................................................................................. 117
Immunosuppression................................................................................................. 117
Cyclosporin A ............................................................................................................ 117
Corticosteroids........................................................................................................... 118
Post-transplant infection......................................................................................... 119
CMV-infected individuals versus non-infected individuals.......................... 119
Discussion................................................................................................................... 120
Chapter 5: Cord blood im m unobiology and transp lantation ........................................ 124
Introduction................................................................................................................. 124
Cord blood (CB) immunobiology: The CB microenvironment................... 130
The effect o f adult and CB serum on the mixed lymphocyte reaction 130
The effect o f adult and CB serum on the proliferation o f human T-cell
lines................................................................................................................................ 131
The expression o f CD25 on adult PBMC following stimulation in the
presence o f adult and CB serum.............................................................................134
The effect o f adult and CB serum on IL-2 production from T-cells in a
stimulated T-cell population.................................................................................... 136
Measurement o f cytokines in adult and CB serum........................................... 137
The role o f M-CSF in CB serum............................................................................. 138
Summary and discussion o f CB immunobiology.............................................. 141

CB transplantation: Reconstitution o f the T-cell compartment.................. 142
Discussion................................................................................................................... 146
C hapter 6: Thym ic function in paediatric prim ary im m unodeficiency patients 150
Introduction................................................................................................................. 150
Results........................................................................................................................... 153
HCT for the treatment o f SCID.............................................................................. 153
The SCID thymus: detection o f thymic activity post-HCT........................... 153
Case study o f a non-conditioned SCID.................................................................. 155
Thymic output and the DiGeorge syndrome.........................................................157
Discussion....................................................................................................................... 159
Chapter 7 ; C onclusion ..................................................................................................................... 161
A ppendix....................................................................................................................................................... 166
Study proposal sent to the Royal Free Hospital Ethical Practices
Subcommittee.................................................................................................................171
Aims and objective o f the project............................................................................ 171
Scientific background o f the study........................................................................ 171
Participant consent form............................................................................................. 172
Participant information sheet.....................................................................................173
Publications.................................................................................................................... 174
Abstracts.......................................................................................................................... 175
B ibliography................................................................................................................................................ 176

List of Figures
Figure 1.1: Molecular model o f aP-TCR recognition o f a class I MHC-peptide
com plex........................................................................................................................ 3
Figure 1.2 Phenotypic changes associated with thymocyte maturation......................... 5
Figure 1.3 Localisation o f thymocytes to specific thymic microenvironments
during T-cell maturation.......................................................................................... 7
Figure 1.4 TCR rearrangement at the TCR-ct/ô locus........................................................ 10
Figure 1.5 Formation o f the immunological synapse during T-cell activation 15
Figure 1.6 Proposals for the differentiation o f naïve to memory and effector T-cells. 18
Figure 1.7 Pathways o f T-cell regeneration post-HCT........................................................... 37
Figure 2.1 Purity o f CD4^ and CDS^ populations after positive selection....................... 44
Figure 2.2 Sequence o f the signal joint region in each TREC..............................................55
Figure 2.3 Representative standard curve for detection o f TREC using Real-Time
PCR................................................................................................................................... 57
Figure 3.1 Recovery o f C D 3 \ CD4^ and CDS^ T-cells subsets after HCT......................66
Figure 3.2 Subsets o f CD4^ and CDS^ T-cells defined by CD45RA and CD45RO
expression in patients 3 months post-HCT........................................................... 69
Figure 3.3 Subsets o f CD4^ and CDS^ T-cells defined by CD27 and CD45RO
expression in patients 3 months post-HCT........................................................... 71
Figure 3.4 T-cell phenotyping to monitor the reconstitution o f naïve, memory and
effector T-cells in patients after HCT.................................................................. 73
Figure 3.5 Recovery o f naïve, memory and effector CD4^ T-cell subsets...................... 75
Figure 3.6 Recovery o f naïve, memory and effector CDS^ T-cell subsets........................ 77
Figure 3.7 Increases in number o f TREC^ T-cells in patients after HCT......................... 81
Figure 3.8 Analysis o f absolute TREC numbers in individual patients post-HCT 82
Figure 3.9 Reconstitution o f naïve T-cells after HCT is dependent on thymic output 84
Figure 3.10 Direct quantification o f thymic output in T-cell replete HCT recipients... 86
Figure 4.1 Effect o f patient age on thymic output.....................................................................97
Figure 4.2 Effect o f patient age on naïve T-cell recovery...................................................... 98
Figure 4.3 Effect o f GVHD on thymic output............................................................................99

Figure 4.4 Naïve T-cell numbers at 12 months post-HCT in patients with or
without cG VH D......................................................................................................... 100
Figure 4.5 Effect o f T-cell depletion on naïve T-cell numbers after HCT..................... 101
Figure 4.6 Effect o f T-cell depletion on the detection o f thymic output......................... 102
Figure 4.7 Effect o f donor leukocyte infusions on thymic output.................................... 105
Figure 4.8 Effect o f Campath-IH administration on T-cell recovery at 3 months
post-HCT...................................................................................................................... 107
Figure 4.9 Effect o f Cyclosporin A on thymic output and naïve T-cell recovery
post-HCT...................................................................................................................... 109
Figure 4.10 Reconstitution o f naïve, memory and effector T-cell subsets in
Patient 183................................................................................................................... 110
Figure 4.11 Effect o f patient age on recovery o f differentiated effector T-cells
post-HCT...................................................................................................................... 112
Figure 4.12 Effect o f Campath-IH administration on memory CD4^ and non-naïve
CD8^ T-cell recovery at 3 months post-HCT..................................................... 115
Figure 4.13 Effect o f Campath-IH administration on reconstitution o f total C D 3 \
CD4^ and CD8^ T-cells at 3 months post-HCT................................................ 116
Figure 4.14 Effect o f Cyclosporin A on memory and effector T-cell recovery
post-HCT...................................................................................................................... 118
Figure 5.1 Allogeneic stimulation o f PBMCs in the presence o f adult and
CB serum...................................................................................................................... 131
Figure 5.2 Effect o f different sera on the mitogen specific proliferation o f a
T-cell line..................................................................................................................... 132
Figure 5.3 Effect o f different sera on the IL-2 specific proliferation o f a human
T-cell line..................................................................................................................... 133
Figure 5.4 Expression o f the IL-2 receptor a chain (CD25) on adult PBMCs
following allostimulation in the presence o f adult and CB sera.................. 134
Figure 5.5 The effect o f different sera on CD25 expression on T-cells stimulated
with PHA..................................................................................................................... 135
Figure 5.6 Analysis o f the percentage o f IL-2 producing T-cells after stimulation
in the presence o f CB or adult serum.................................................................. 137
Figure 5.7 Concentration o f cytokines in adult and CB serum.......................................... 138
Figure 5.8 M-CSF inhibits the human MLR........................................................................... 139
Figure 5.9 The role o f M-CSF in cord blood (CB) sera....................................................... 140

Figure 5.10 Thymie output and naïve T-cell recovery in recipients o f CB transplants
compared with age-matched recipients o f BM or PBSC transplants 144
Figure 6.1 TREC levels in SCID patients after HCT............................................................ 154
Figure 6.2 TREC levels in SCID patients at different time points after HCT 155
Figure 6.3 TREC and T-cell subsets in Patient 42 before and after peripheral
blood infusions........................................................................................................... 156
Figure 6.4 Thymic output in patients with DiGeorge syndrome...................................... 158
Figure A1 TREC standard construct for radiolabelled QC-PCR..................................... 166
Figure A2 Standard construct for the detection o f TREC using Real-Time PCR 167
Figure A3 Age-matched healthy control TREC values....................................................... 168

List of Tables
Table 2.1 Optimal antibody dilutions for staining PBMC populations......................... 48
Table 2.2 Antibody combinations enabling identification o f naïve, memory and
effector T-cell subsets by flow cytometry.......................................................... 48
Table 3.1 Phenotypic definitions o f naïve, memory and effector T -cells.................... 68
Table 3.2 Summary o f reconstitution o f naïve, memory and effector CD4^
T-cell subsets.............................................................................................................. 76
Table 3.3 Summary o f reconstitution o f naïve, memory and effector CD8^
T-cell subsets.............................................................................................................. 78
Table 3.4 Relationship between TREC and naïve T-cell numbers................................. 83
Table 3.5 Patient characteristics................................................................................................ 85
Table 3.6 Ratio o f naïve: non-naïve CD4^CD45RA^ T-cells post-HCT........................ 86
Table 3.7 Correlation o f thymic output with CD4^CD45RA^ subsets.......................... 87
Table 4.1 Clinical characteristics o f patients enrolled in the study................................ 94
Table 4.2 T-cell related clinical data....................................................................................... 95
Table 5.1 Phenotypic differences between cord blood and adult T -cells..................... 127
Table 5.2 A comparison o f cytokine production by CB and adult T -cells................... 128
Table 5.3 Soluble factors detected in adult and CB sera.................................................... 129
Table 5.4 Transplant related clinical data on recipients o f CB, BM and PBSC
Transplants................................................................................................................... 143
Table 6.1 T-cell phenotyping and TREC levels in 5 DiGeorge syndrome patients... 158
Table A1 Factors affecting overall reconstitution o f the T-cell compartment
post-HCT...................................................................................................................... 169
Table A2 Factors affecting reconstitution o f naïve CD4^ T-cells and CD4 TREC... 169
Table A3 Factors affecting reconstitution o f naïve CD8^ T-cells and CD8 TREC... 170
Table A4 Factors affecting reconstitution o f memory and effector CD4^ T-cell
subsets.......................................................................................................................... 170
Table A5 Factors affecting reconstitution o f non-naïve and CD8^CD57^CD28’
subsets......................................................................................................................... 170

C h a p t e r 1
C h a p t e r 1
Introduction
The immune system
Since Edward Jenner’s discovery of the smallpox vaccine in 1796, the study o f the
immune system has revealed a complex defence mechanism that has evolved to protect us
against the myriad of infectious agents to which we are exposed each day.
Immune responses to pathogens can be broadly classified into the innate or adaptive
immune response. The innate immune response describes a system of non-specific
barriers which pathogens must penetrate before the adaptive response is activated. The
simplest way to avoid infection is to prevent pathogens gaining access to the body.
Therefore, physical barriers such as the skin, mucosal linings and bodily fluids such as
saliva, gastric juice and lysosyme provide the first layer o f protection. If these physical
barriers are penetrated two other non-specific mechanisms are activated, these being the
complement pathway and phagocytosis of foreign particles by phagocytes and cells o f the
reticuloendothelial system (RES).
As well as forming a series of non-specific barriers, the innate immune system is now
known to have considerable specificity in its recognition of pathogens (Aderem and
Ulevitch, 2000; Hoffmann et a l , 1999; Medzhitov and Jane way, 1997). In fact, the innate
immune system is very probably the key to the question that has troubled immunologists
for many years i.e. how does the immune system identify foreign pathogens and respond
appropriately without causing unnecessary destruction to self-tissues. The specificity o f
the innate arm of the immune system is conferred by a group of receptors that recognise
conserved motifs on pathogens that are not found in higher eukaryotes (Reviewed in
(Aderem and Ulevitch, 2000)). These receptors are highly conserved across different
species and bind to motifs that are essential for the biology of pathogens. The group o f
receptors which bind these pathogen-specific motifs are termed pattern recognition
receptors (PRRs) and have generated much recent interest (Reviewed in (Aderem and
Ulevitch, 2000; Akira gf al., 2001)). Professional antigen presenting cells (APCs) such as

___________________________________________________________________________________________________________________________________________ C h a p t e r 1
dendritic cells and macrophages have distinct patterns of expression of PRRs, which is
thought to facilitate distinct immune responses to different invading pathogens
((Kadowaki et a l , 2001); also discussed later). Critically, signalling events through PRRs
activate professional APCs to express costimulatory molecules and cytokines (Hertz et al.,
2001; Kadowaki et al., 2001; Kaisho and Akira, 2001). The exact structure, function and
signalling through PRRs is outwith the scope o f this thesis. However, it is essential for the
following discussion to mention that the initial discrimination between self- and non-self
(in terms o f pathogen recognition) is probably dependent on signals (or lack of) via
PRRs.
Whereas the innate immune system responds to pathogens in the same way upon re
infection, the adaptive immune system (as the name suggests) is able to adapt so that upon
subsequent infections, the response is faster and of greater magnitude than after the initial
pathogen exposure. This represents an important observation in terms of the evolution o f
the immune system. The innate immune system while able to provide some protective
immunity in its own right, is limited in its clonal expansion capabilities and therefore
unable to completely eliminate rapidly dividing bacteria and viruses. However, the
adaptive response (capable of clonal expansion, pathogen-specific recognition and
elimination) is activated by cells of the innate immune system.
T- and B-cells are the major lymphocyte components of the adaptive arm of the immune
system and represent the main effectors of the immune system. B-cells upon activation
proliferate and produce large quantities o f antibodies that neutralise extracellular
pathogens resulting in clearance by phagocytes or complement-mediated lysis. The
function o f pathogen-specific T-cells is either to provide “help” (in the form o f cytokine
production) for the activation of B-cells or direct killing o f pathogen infected cells.
Both T- and B-cells originate in the bone marrow, but while B-cells develop and mature in
the bone marrow, T-cells migrate to the thymus to undergo their maturation. By contrast
to the highly conserved PRRs of the innate immune system, T- and B-cells express
receptors that have been produced by random rearrangement during their maturation
from bone marrow-derived precursors. The ligands that bind to rearranged T-cell
receptors (TCRs) and provide the antigen-specific activation signal are peptides from
foreign pathogens presented in the context o f self-major histocompatability com plex
(MHC) molecules (Figure 1.1; (Babbitt et al., 1985; Zinkemagel and Doherty, 1974)).

C h a i t ü r 1
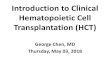
Figure 1.1: Molecular model o f af5-TCR recognition o f a class / MHC-peptide complex T h e specif ic i ty and d ivers i ty o f pa thogen recognit ion by T -cel ls is mediated by virtue o f TCR r e c o g n i t io n o f
M H C -p e p t id e com plexes . T h e a l and (31 dom ains o f an M H C class 1 m olecu le ( a -h e l i c e s and p-p lea ted s h e e t s )
a re s h o w n in light b lue and the bound pep tide is show n in white with am in o acid side c h a in s rep resen ted in
b lue and red. T he M H C -pep t ide com plex is bound by the C D R l (green), C D R 2 (beige) and C D R 3 (p ink) l o o p s
o f the a - chain and the C D R l (dark blue) , C D R 2 (yellow) and C D R 3 (red) loops o f the P -c h a in o f the T -cell
recep tor . T h e specific i ty and d iversi ty o f p a thogen reco g n i t io n is conferred as fo llow s: T he M H C is h i g h l y
p o l y m o rp h ic , but the m ajor ity o f the p o ly m o rp h is m s are w ith in the pep t ide b ind in g pocke t and not in
reg ions o f the M H C that will be recognised by the C D R l and C D R 2 loops. T hus sp ec if ic i ty is via C D R l and
C D R 2 b in d in g to the M H C molecule itself . The b ind ing o f pep t ides by M H C m olecu les is depen d en t o n
severa l anchor res idues , but there is f lexibil i ty in the am in o acid sequence for the re m a in in g residues in each
p ep t ide i.e. for a n in e -m er peptide , 2 anchor residues would bind w ith in specif ic pock e ts in the p e p t id e
b in d in g g roove o f the M H C m olecule and the rem ain ing residues would fit in to o ther pock e ts w hich are le s s
s t r in g en t in their spatia l requ irem ents . T h is sys tem a l low s a h igh ly d iverse array o f pep t ides to be p re s e n te d
b y each M H C m olecu le . The d iversi ty in peptide b ind in g by M H C m olecu les is m irrored by T C R b i n d i n g
s ince the C D R 3 loops (w hich m ake con tact with the peptides) represent the m ost variable reg ion o f the T C R .

______________________________________________________________________________________________________________________________________ C h a p t e r 1
However, as part of normal cellular function, MHC molecules also present self-peptides
that are structurally similar to foreign peptides (Reviewed in (Klein and Sato, 2000; Klein
and Sato, 2000)) necessitating mechanisms that prevent T-cells from reacting against self
tissues. The primary mechanism that prevents aberrant T-cell activation to self-tissues is
thymic selection, a process also known as central tolerance. In addition, peripheral
tolerance mechanisms exist to prevent T-cell clones that “escaped” thymic selection from
being inappropriately activated. Therefore, the primary objective of T-cell development is
to provide each individual with a repertoire of T-cells capable o f responding to any one
of the thousands of environmental pathogens while preventing aberrant destruction o f
self-tissues. How this is achieved merits some consideration.
Thymic T-cell development
Historically, the role of the thymus in the immune system has been a matter o f some
debate. Even as late as 1963, many researchers believed that the thymus did not have a
significant influence on lymphocyte development. Around this time however. Miller
demonstrated that removing the thymus from newborn mice adversely affected their
immunological responses (Discussed in (Miller, 2001)). Since then, not only has the
thymus been demonstrated to be o f crucial importance in T-cell development, but an
enormous amount of data has been generated describing the mechanism of T-cell
development.
Thymocytes begin life in the bone marrow where they develop from pluripotent
haematopoietic stem cells to become common lymphoid progenitors (CLP; (Galy et a i ,
1995)); both o f these expressing the CD34 antigen (Berenson et a i , 1988; Terstappen et
a i , 1991). The common lymphoid progenitor (CLP) then migrates from the bone
marrow via the blood circulation into the thymus, where it enters through high endothelial
venules at the corticomedullary junction (Donskoy and Goldschneider, 1992). Once in
the thymic microenvironment, thymocyte development follows a series o f developmental
stages (Figure 1.2) driven by cytokine signals and interactions between developing
precursors and thymic stromal cells.
Phenotypic changes associated with thymocyte maturation into CD4*
or CD8* T-cells
The most immature cells within the thymus are CD34^CD38 (Marquez et a i , 1995; Res et
al., 1996; Schmitt et a i , 1993) and progress to a more mature developmental stage via an
intermediate C D 34‘“' phenotype which is paralleled by the acquisition of other markers

_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ C h a i t i ^r 1
such as CD la and CD5 (Galy et al., 1993; Spits, 1994). These cells remain C D 3C D 4C D 8
and are therefore defined as triple negative (TN) or double negative (DN) thymocytes.
Such TN thymocytes can be further subdivided on the basis of expression of c-kit, CD44
and CD25 (Zuniga-Pflucker and Lenardo, 1996). These cells are defined (in order o f
maturation) as C D 44T D 25 c-kit\ CD44TD 25"c-kit\ CD44 CD25"c-kit'"", and CD44
CD25 c -k i t . During this TN phase of thymocyte development, a number of crucial
checkpoints are reached particularly in the commitment of thymocytes to the T-cell
lineage and also commitment to the ocp or yô T-cell lineage (Capone et al., 1998; Dudley
et al., 1995; Livak et al., 1995). Productive TCR(3 rearrangements are thought to favour
differentiation of a(3 T-cells whereas productive yô rearrangements are required to divert
a(3 T-cells from their default pathway (Mallick et al., 1993; von Boehmer and Fehling,
1997).
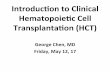
PeripheryMarrow Thymus
Mature
CD4Immature CD8^
CD8+ early44+25c-kit+
44 25c-kit+
44-25-c-kit-
M ature
C D 3 - y,8 ,e
p T a l
T C R -B
T C R -a
Figure 1.2; Phenotypic changes associated with thymocyte maturationT he d e v e lo p m e n ta l p a th w ay for m urine T -ce l ls is show n. B one m arrow derived co m m i t te d l y m p h o i d
p ro g e n i to r s (CLP) c o lo n i se the thym us and subsequen t ly dev e lo p into C D 4 or CDS s ing le p o s i t iv e (SP)
t h y m o c y te s w h ich exit the thym us and jo in the per iphera l T-cell pool as naïve C D T or CDS" T -ce l ls . T he
d e v e lo p m e n ta l ly regu la ted ex p ress io n o f cer ta in surface p ro te in s that are crucial for a p - T C R " T-cell
m a tu ra t io n is sh o w n .
Progression to the next developmental stage is dependent on the surface expression of,
and signalling through, a pre-TCR consisting of a productively rearranged TCR-(3 chain
and an invariant surrogate a chain (pTa; (Groettrup and von Boehmer, 1993; Kishi et al.,
1991 ; Shinkai et al., 1993; Shores et al., 1993)). Signals through the pre-TCR complex
trigger a wave of proliferation, rearrangement of the T C R -a locus and expression of CD4
and CD8 molecules (Fehling and von Boehmer, 1997; von Boehmer and Fehling, 1997).
These double positive (DP) CD4 CD8^ thymocytes represent the major thymocyte
population in the thymus. Such large, dividing DP thymocytes develop into small non

___________________________________________________________________________________________________________________________________________ C h a p t e r 1
dividing thymocytes which progressively differentiate from TCR/CD3’"' to TCR/CD3'"‘
cells.
DP thymocytes are then tested for their reactivity to self-MHC-peptide com plexes in
processes known as positive and negative selection. During these selective processes DP
thymocytes have three options: death by neglect, death by negative selection and life by
positive selection, all three of which are determined by TCR affinities for self-MHC-
peptide complexes. Therefore, cells expressing a TCR which fail to bind self-MHC die by
neglect (passive cell death, discussed later); cells expressing a TCR with high affinity for
self-MHC-peptide complexes undergo negative selection (activation induced cell death,
discussed later); whereas cells with an ‘intermediate’ affinity for self-MHC-peptide
com plexes are rescued from apoptosis by positive selection (Reviewed in (Jameson and
Bevan, 1998)). In this way, the majority of self-reactive T-cells are deleted from the
repertoire. Indeed, only -5% of developing thymocytes survive this rigorous selection
process.
During the final stage of a p T-cell development in the thymus, immature CD4^CD8^ DP
thymocytes shut down expression o f either CD4 or CD8 to give rise to mature CD8'" or
CD4^ single positive (SP) cells (Reviewed in (Basson and Zamoyska, 2000)).
The thymic m icroenvironm ent and signals that drive th y m o c y te
m a tu ra t io n
The development of immature TN (CD3 C D 4C D8 ) thymocytes to DP CD4"^CD8
thymocytes involves a number of crucial events that are regulated by interactions with
thymic stromal cells. In addition, the integrity of thymic architecture is dependent on the
presence o f thymocyte subsets (Sano et al., 2001; van Ewijk et a i , 2000). The maturation
o f TN to DP thymocytes depends on the simultaneous presence of MHC class IP thymic
epithelial cells and mesenchyme (Anderson et al., 1993). Furthermore, experiments have
shown that MHC class IT thymic epithelial cells are unique in their ability to mediate
positive selection of DP thymocytes whereas negative selection can be induced by several
different stromal cell types (Anderson et a i , 1997; Volkmann et al., 1997). However,
additional signals other than TCR-MHC interactions are also required for positive
selection (Ernst et al., 1996). The nature of these signals is currently unknown but has
been suggested to involve the production of glucocorticoids by thymic epithelium which
would prevent TCR-mediated thymocyte apoptosis (Vacchio and Ashwell, 1997).
The release of soluble factors by thymic stromal cells may also be involved in thym ocyte
development (Reviewed in (Zlotnik and Moore, 1995)). Thymic derived hormones such

_____________________________________________________________________________________________ C h a it iik 1
as thymulin and the thymosins are released by subcapsular and medullary epithelium
(Ritter and Crispe, 1992) and are thought to influence thymocyte differentiation. Perhaps
the best characterised cytokine influencing thymocyte differentiation is IL-7, a cytokine
that acts as a crucial driving force in the first phase of thymocyte proliferation (Maki et
al., 1996; Peschon e ta !., 1994; von Freeden-Jeffry et al., 1995). Therefore, mice lacking
either IL-7 (von Freeden-Jeffry et al., 1995), IL-7R common gamma chain (Gao et al.,
1995; DiSanto et al., 1995; Ohbo et al., 1996); or components of the IL-7R signalling
pathway such as Jak3 (Nosaka et al., 1995; Park et al., 1995; Thomis et al., 1995) or Jakl
(Rodig et al., 1998) all have a profound reduction in thymic cellularity.
Although a substantial proportion of these cytokine signals and the exact interactions
between thymic stromal cells and developing thymocytes remain to be discovered, it is
clear that the process of thymocyte differentiation is a highly regulated process. This was
further demonstrated in a recent publication by Lind et al. describing the migration of
developing thymocytes and their requirement for distinct stromal microenvironments and
developmental signals (Lind et al., 2001). Using fluorescent microscopy and thymic
tissue sections, they demonstrated that thymocytes enter the thymus at the
corticomedullary junction, then migrate to the outer region of the cortex while developing
from DN 1 to DN4 subsets. DN4 cells then develop into DP cells in the outer region of the
cortex and DP cells then undergo positive and negative selection (Figure 1.3).
region 4proliferation
positive and negative selection
region 3
®T-lineage commitment, T(TCRB recombination
O region 2
loss of B andNK potential, proliferation
region 1proliferation
Figure 1.3: Localisation o f thymocytes to specific thymic microenvironments during T-cell m aturationT h y m o c y te d e v e lo p m e n t is localised to certain regions with in the th y m u s . An a p p ro x im a te m ap o f th e
cor t ica l reg ions and the m atura tion stages that occur with in these r eg ions is show n . T h is m ig ra t io n p a t t e rn
su g g e s t s spec if ic r equ irem en ts for so lub le factors and cell-cell in te rac t io n s for the d e v e lo p m e n t o f s p e c i f i c
t h y m o c y t e subse ts .

___________________________________________________________________________________________________________________________________________C h a p t e r 1
This data demonstrates a requirement for developing thymocytes to localise within
specific stromal environments and further suggests that chemotactic factors may play a
role in thymocyte migration and maturation. In support of this hypothesis, unpublished
data from Petrie et al. (personal communication) suggests that DN2 (CD44"’CD25^c-kif)
thymocyte migration is mediated via adhesion of a4-containing integrins (a4 |3 l and
a4(37) to a matrix of VCAM -T cortical epithelial cells. Furthermore, the chem okine
receptors CCR7 and CCR8 are differentially expressed on deep cortical precursors
(DN1/DN2 thymocytes) implicating a role for chemokines in attracting DN cells to a
particular stromal environment.
The previous observations suggest that thymocyte differentiation is dependent on
numerous soluble and cellular components of the thymus. Such stringently regulated
thymocyte development ensures that the majority of self-reactive T-cell clones are deleted
in the thymus. The concept of age-related thymic involution will be discussed later, but
undoubtedly, therapeutic intervention and the reversal of age-related thymic involution in
a variety of clinical settings will be dependent on a detailed knowledge o f thymocyte
development. This will include a detailed knowledge of thymocyte-stromal cell
interactions, soluble factors necessary for thymocyte differentiation and the migratory
patterns of T-cell precursors, both entering the thymus as CLPs and exiting the thymus as
naïve CD4" or CDS'" T-cells. In addition, the development o f methods to detect thymic
emigrants in the circulation remains a high priority.
Identification o f thymic emigrants
Before discussing the migration of thymic emigrants from the thymus to peripheral
lymphoid organs, a consideration o f the identification of thymic emigrants is necessary.
It has been estimated that approximately 1% of the cells produced in the murine thymus
migrate to the periphery as immature T-cells (Egerton et al., 1990; Scollay et al., 1980).
However, detailed analysis of these thymic emigrants in terms o f their migration patterns,
number and differentiation to mature T-cells {i.e. naïve CD4" or CD8"' T-cells) has been
hampered by the lack of a reliable marker that differentiates such thymic emigrants from
circulating naïve T-cells.
The first study to identify a phenotypic marker specific for thymic emigrants was
published by Kong et al. (Kong et al., 1998). Prior to this study, the chTl antigen (on
avian cells) was considered to be thymocyte-specific (Chen et al., 1984). Kong et al.
extended these observations to demonstrate that chTD T-cells produced by chicken
thymic lobes represented recent thymic emigrants. These conclusions were based on the
fact that the number of peripheral chT D T-cells decreased as thymic lobes (of which

___________________________________________________________________________________________________________________________________________ C h a p t e r I
chickens have 14) were removed, the number of chT T T-cells decreased with increasing
age and that chT T T-cells were enriched for TCR rearrangement deletion circles (which
will be discussed later) compared with chTT T-cells.
However, such a reliable phenotypic marker that distinguishes human thymic emigrants
from circulating naïve T-cells has not been identified to date. It would seem that there is
still considerable debate on the phenotypic markers that reliably discriminate between
naïve and non-naïve T-cells (De Rosa et a l , 2001), much less naïve T-cells from thymic
emigrants. Nevertheless, McFarland et al. suggested that CD 103 (in combination with
CD45RO, CD27 and CD62L) discriminates CD8^CD4 thymic emigrants from CD8^ naïve
T-cells. By their proposal, CD8^ recent thymic emigrants are CD45ROCD27^
CD62L+CD103" while circulating naïve CD8" T-cells are CD45RO C D 27 T D 6 2 L T D 1 0 3
(McFarland et al., 2000).
Clearly, an assay that would enable evaluation of the number o f circulating thymic
emigrants would be beneficial both in terms of basic research and clinical applications.
The lack o f a specific thymic emigrant phenotype prior to McFarland’s observations
prompted the development of a different approach to measuring thymic emigrants.
Douek et al. (Douek et al., 1998) translated the results o f Livak and Schatz (Livak and
Schatz, 1996) into an assay that could detect recent thymic emigrants based on the
maintenance (in peripheral T-cells) of episomal fragments of DNA excised from the
genome during TCR rearrangement in the thymus. Before discussing this assay, a
description of the formation of such episomes is necessary.
The T-cell receptor is expressed on the cell surface as a heterodimer composed of either
a-(3 or y -0 chains. During T-cell development in the thymus, these genes undergo a
process o f random rearrangement termed V(D)J recombination (For reviews see (Alt et
al., 1992; Krangel et al., 1998)), during which segments of V, D and J genes recombine to
form the a - or 5-chains and V and J genes recombine to form the (3- or y-chains o f the
TCR. These newly formed TCRs are then tested for their specificity and self-restriction by
positive and negative selection. Although random, in that any TCR V, D or J segment can
be used in any given recombination event, TCR V(D)J recombination is highly specific
and restricted to developing thymocytes. The specificity of V(D)J recombination depends
on heptamer and nonamer recombination signal sequences (RSSs) as well as enzym es
including the lymphoid-cell-specific recombinase proteins RAG-1 and RAG-2 and a
ubiquitous set o f double-strand break-repair proteins (Jackson and Jeggo, 1995; Lewis,
1994). D NA cleavage occurs at the junction of the individual coding (i.e. V, D or J)
segments and its flanking RSS to generate signal ends (Schlissel et al., 1993) and coding
ends (Roth et al., 1992; Roth et al., 1992). The recombination process is then com pleted
by ligation o f both coding ends and signal ends generating an episome of unwanted DNA

C H A i m : K I
and a coding joint that will ultimately form part of the TCR (Figure 1.4; (de Villartay et
al., 1988; de Villartay et a i , 1987; Livak and Schatz, 1996; Verschuren et al., 1997)).
V a a n d VÔ VÔ DÔ JÔ CÔ VÔ TEA Jcx C a
ÔREC
5REC
EXCISIONAND
SPLICING
S ig n a l joint
+
0 - e n h a n c e r
V g g I Y 6 2 D | D 5 2 D 8 3 J S l J S 4 J 5 2 J 6 3 Q g V 5 2 TEA
a - e n h a n c e r
J a 6 0
ÔREC T JaVÔ5 I '
Figure 1.4: TCR rearrangement at the TCR-a/5 locusT h e re a r ra n g e m e n t o f the T C R - a chain results in excision o f the TCR-Ô locus f rom the t h y m o c y te g e n o m e , an
even t thought to be im portan t in T C R - a P versu s T C R -yô co m m itm en t . T h e rea r ran g em en t even t that o ccu rs at
the h ig h es t f requency in human and m urine th y m o cy tes is the rea r ran g em en t o f the 6 -Rec to the Y J a RSS
(show n) . E x c is io n o f the TCR-Ô locus genera tes an ex trach rom osom al e p is o m e (TCR re a r ra n g e m e n t e x c i s i o n
c irc le (T R E C )) c o n ta in ing unw an ted TCR-Ô sequences. The splicing o f the ô-Rec to the Y J a RSS is f o l lo w ed
by further re a r ra n g e m e n t events that even tual ly genera tes a functional T C R - a chain. T R E C s can be detec ted in
pe r iphe ra l b lood T-cells using a PC R -based method. P rim er b ind ing si tes and d irec t ion are ind ica ted by th e
g reen arrow s . T h e p r imers were pos i t ioned on ei ther side o f the j o in in g reg ion to p reven t a m p l i f i c a t io n o f
P C R produc ts in T-cel ls that have not rearranged their T C R - a chain.
Although these episomal DNA circles were discovered some time ago (Takeshita et al.,
1989), Livak and Schatz were the first to report that such by-products of TCR
rearrangement were maintained in thymocytes and mature T-cells (Livak and Schatz,
10

___________________________________________________________________________________________________________________________________________ C h a p t e r 1
1996). Following this report, Kong et al. utilised these observations to suggest that these
products could be used to identify and quantify thymic emigrants in the peripheral T-cell
pool in chickens (Kong et al., 1998; Kong et al., 1999).
Douek et al. were the first investigators to demonstrate that such gene deletion circles
could be used to measure thymic output in humans (Douek et al., 1998). In this ground
breaking report, Douek et al. named these episomes “T-cell receptor rearrangement
excision circles” (TRECs). They demonstrated that TRECs are stable, do not replicate
with cell division and decrease with increasing age. The TREC assay is a PCR-based
method that detects the most abundant TREC in human thymocytes (the ôREC to Y Ja
rearrangement event) which is present in -70% of ap TCR"" thymic emigrants (Verschuren
et al., 1997). Therefore, the TREC assay is designed to detect the export o f a p T-cells
from the thymus, each aP-TCR^ thymic emigrant containing 1 TREC for each TCR-a
locus that has been rearranged during T-cell development.
The frequency of TREC in the peripheral T-cell pool represents a balance between thymic
output and peripheral expansion. However, it is not an exact measurement o f thymic
output i.e. because TRECs are stable, they will be maintained in naïve T-cells until they
undergo cell division. Also, since TREC measurements only quantify T-cells that have
rearranged aP T-cell receptors, this assay does not conclusively rule out the possibility
that extrathymic T-cell development also contributes to the T-cell pool (Antica and
Scollay, 1999; Howie et al., 1998; Lefrancois and Puddington, 1995; Wang and Klein,
1994). However, in the absence of thymic output i.e. where the peripheral T-cell pool is
maintained by peripheral expansion in the case of thymectomised individuals, TREC
levels decline over time but do not immediately disappear (Douek et al., 1998; Kong et
a/., 1998).
Nevertheless, since the initial publication, TRECs have been utilised in a number o f
different applications, demonstrating that elderly humans maintain thymic function until
very late in life (Douek et al., 1998; Jamieson et al., 1999; Poulin et al., 1999) as well as
enabling analysis of thymic function in HIV infected individuals (Douek et al., 1998;
Hatzakis et al., 2000; Zhang et al., 1999); haematopoietic cell transplant recipients
(Douek et al., 2000; Hochberg et al., 2001; Patel et al., 2000; Storek et al., 2001 ;
Weinberg et al., 2001); primary immunodeficiency patients (Markert et al., 1999) and
other patient cohorts.
While this assay was clearly a breakthrough enabling thymic function to be assessed in
humans, there are currently no methods, on a cell by cell basis that can discriminate
thymic emigrants from circulating naïve T-cells.
11

C h a p t e r 1
Thymic emigration and T-cell homing to secondary lymphoid organs
The previous observations notwithstanding, a number o f groups have used alternative
approaches to study the biology o f recent thymic emigrants.
Upon maturation into SP CD4^ or CDS'’ thymocytes, cells are programmed to exit the
thymus and migrate to secondary lymphoid organs (such as the lymph nodes and spleen)
where they can begin to participate in the fight against foreign pathogens.
While the process of naïve T-cell homing to secondary lymphoid organs is fairly well
characterised, the mechanism and timing of SP thymocyte emigration from the thymus is
unclear. Lee et al. demonstrated using foetal thymic organ culture (FTOC) that SP
thymocytes were able to exit the thymus less than 24 hours after positive selection
(although SP thymocyte residency time in the thymus has been estimated to be up to 8
days; (Lucas et a i , 1994)). Furthermore, thymocyte emigration in this system was
inhibited by cytochalasin D, pertussis toxin and Clostridium dijficile toxin B, implicating
an active motility process and G-protein coupled receptors in thymic emigration (Lee et
a i , 2001). However, no reports of chemokine receptor expression by thymic emigrants
have been published as yet. It seems likely however, that the pattern of chem okine
receptor and adhesion molecule expression on recent thymic emigrants will be similar to
that of naïve T-cells.
By contrast to recent thymic emigrants, a significant amount of data has been published
on naïve T-cell chemokine receptor expression, migration and homing (Reviewed in (von
Andrian and Mackay, 2000)).
Naïve T-cells continuously migrate from the blood into secondary lymphoid tissues and
back into the blood (Butcher and Picker, 1996). Cells migrate into secondary lymphoid
tissues through high endothelial venules (HEV) which express adhesion molecules and
chemokines that selectively recruit lymphocyte subsets. The physical stresses involved in
arresting T-cell flow in the blood necessitates the use of adhesion receptors to form stable
bonds with their respective ligands on the HEV wall (Carlos and Harlan, 1994; Springer,
1994). The first step in this adhesion “cascade” is the binding o f the leukocyte specific
selectin (L-selectin; CD62L) to its respective ligand (peripheral node addressin (PNAd) on
HE Vs in the lymph node; mucosal addressin cell adhesion molecule (MadCAM) on HEVs
in Peyer’s patches; (Kansas, 1996)). However, these bonds are short-lived and the pressure
exerted by the blood flow causes dissociation of this interaction resulting in a rolling
motion of the T-cell along the vascular wall. To allow extravasation (diapedesis) o f the T-
cell into the lymph node, the movement of the cell must be arrested. The rolling T-cell
must therefore engage additional adhesion molecules such as LFA-1, or integrins such as
12

C h a p t e r 1
VLA-4 or a4p 7 (Lawrence and Springer, 1991; von Andrian et al., 1991). While L-
selectin is constitutively expressed on naïve T-cells, expression of members o f the integrin
family is dependent on activation signals. These signals can be provided by chem okines
immobilised on endothelial cell surfaces (Cyster, 1999). The chemokines SLC and ELC
can perform this task by binding to the chemokine receptor CCR7, following which
activation o f integrins, arrest and subsequent migration of naïve T-cells into lymph nodes
occurs. The chemotactic gradients of SLC, ELC and a third chemokine BCA-1 then attract
naïve T-cells further into the lymph node (For a review see (Moser and Loetscher, 2 0 01))
where they localise with dendritic cells (DCs). Upon recruitment into the appropriate
region o f the secondary lymphoid organ, naïve T-cells then begin to “scan” a large
number of professional APCs (mostly DCs with some B-cells and macrophages) for signs
o f invading pathogens. The recognition of foreign antigen by the TCR in the presence o f
costimulation then triggers a cascade of events leading to T-cell activation and
differentiation.
T-cell activation: mechanisms and requirements
T-cell activation occurs when the TCR is engaged by its ligand, a complex o f MHC-
peptide (Babbitt et at., 1985) presented on the surface of antigen presenting cells
(Unanue, 1984). For activation of naïve T-cells, we now know that the peptide-MHC
complex must be presented on the surface of mature dendritic cells (Banchereau et al.,
2000; Steinman, 1991). However, there are several basic physical problems that the T-cell
must overcome before sustained TCR-MHC/peptide interactions can stimulate T-cell
activation.
First, the TCR has a relatively low affinity for MHC/peptide ligands with dissociation
constants ranging from 10 '* to lO'^M (Alam et al., 1996; Corr et al., 1994; Lyons et al.,
1996; Matsui et al., 1994). This binding is relatively weak compared with antibodies
which often have dissociation constants o f <10^M (Mason and Williams, 1980). Second,
that the number of activating MHC/peptide complexes {i.e. foreign agonist peptides) on
any given APC is very low and can be as few as 100 molecules per APC (Demotz et al.,
1990; Harding and Unanue, 1990; Valitutti et al., 1995). The question therefore arises as
to how 100 molecules of MHC/peptide can activate signals through 30,000-40,000 T-cell
receptors? The third problem that the T-cell has to overcome is steric hindrance since the
TCR and the MHC/peptide complex are small compared with other membrane proteins
such CD45 and CD43 (Shaw and Dustin, 1997).
Only recently have we begun to understand how the T-cell deals with these problems. In
essence, the T-cell deals with these problems by forming an “immunological synapse” at
the point of contact between the T-cell and the APC, very probably the same phenom enon
13

___________________________________________________________________________________________________________________________________________ C h a p t e r 1
of capping which was observed some 25 years ago (Raff, 1973). Since the affinity o f
TCR-MHC/peptide interactions are weak and the number of appropriate MHC/peptide
complexes on each APC is low, contact between the T-cell and APC is initiated through
LFA-l/ICAM -1 and CD2/CD58 interactions. Therefore, when the T-cell makes contact
with the APC, many interactions of CD2/CD58 and LFA-l/ICAM -1 take place (Dustin et
al., 1996; Lollo et al., 1993). The net result o f these interactions is that CD2/CD58 forms
a central area o f contact and LFA-l/ICAM-1 is pushed out of this area to form an outer
ring (Grakoui et al., 1999; Monks et al., 1998). Other large molecules such as CD43 and
the tyrosine phosphatase CD45 are also pushed out of the central contact area (Figure
1.5). Therefore, with this initial interaction, numerous problems associated with initiating
T-cell activation are overcome. The binding o f CD2/CD58 and LFA-l/ICAM -1 “spreads
the load” so that cell contact is not dependent on TCR-MHC/peptide interactions. In
addition, the inner contact zone of CD2/CD58 interactions provides a region that is
favourable in terms of size (~15nm) that enables the TCR to engage MHC/peptide
complexes (Grakoui et al., 1999; Monks et a i , 1998). Also, a number of signalling
molecules (p 56‘"‘‘ and p59 ‘ ") are dependent on tyrosine phosphorylation for activation.
The exclusion of CD45 from the central contact zone enables signals via the TCR to be
transduced to the nucleus via numerous signalling pathways (Leo and Schraven, 2001;
Tomlinson et al., 2000; Ward and Cantrell, 2001). This gross rearrangement o f surface
receptors is driven by the actin cytoskeleton (Reviewed in (Dustin and Cooper, 2000;
Penninger and Crabtree, 1999)) and it has become apparent recently that this is an active
process that may be directly dependent on signals via the TCR (Delon et a i , 2001).
Once the central contact area is established, T-cell activation is thought to be dependent
on crossing a number of pre-set thresholds. This brings forward the third problem
mentioned previously, that there are relatively few appropriate MHC/peptide ligands on
each APC. A serial triggering model was proposed by Lanzavecchia’s group (Valitutti et
al., 1995) to provide a solution to this problem. According to this model, a single
MHC/peptide complex can trigger up to 100 TCRs with these results being extended to
demonstrate that internalisation of 8000 TCRs (a surrogate marker for the number o f
TCRs that have been engaged) was sufficient to enable T-cell activation (Viola et al.,
1999).
14

C h a i t ü r 1
TCR engagement and signalling, protein clustering, cytoskeleton-driven membrane reorganisation, mature synapse formation within 30 mins leading to T-cell activation
40nm
C D 48/CD58
CD2
ICAM-1
LFA-1
I C D 80/CD86 MHC/peptide
CD28TCR/CD3
CD45
CD4
L CD43
Figure 1.5: Formation o f the immunological synapse during T-cell activationBefore co n tac t with the A PC, surface receptors on both the APC and T-cell have a r e la t ive ly h o m o g e n e o u s
d is t r ib u t io n . W ith in seconds of cel l-cell con tac t , T C R tr ig g e r in g occurs and pro te in c lu s te r in g t ak es p la c e .
W ith in severa l m inu tes , cy to s k e le to n driven m em b ran e p ro te in r e o rg a n is a t io n occurs such that la rge
m olecu les such as C D 43 , C D 45, LFA-1 and ICAM-1 are transported out o f the core synapse reg ion . F o r m a t i o n
o f the m ature synapse is com ple te with in 30 m inutes o f cel l-cell con tac t and must be m a in ta in ed for se vera l
hours for full T -cell act ivation to occur.
15

___________________________________________________________________________________________________________________________________________ C h a p t e r 1
W e know from in vitro studies of T-cell activation using anti-CD3 antibodies and from in
vivo mouse studies (Bluestone, 1995; Freeman et a i , 1993; Kundig et al., 1993;
Shahinian et al., 1993) that T-cell activation can be achieved by sustained stimulation
through the TCR alone. However, a number of other studies demonstrated that signalling
through the TCR alone induced a state of tolerance or anergy that could only be reversed
by exogneous IL-2 (Bluestone, 1995; Schwartz, 1990). A more recent study demonstrated
that the duration of TCR stimulation determined additional activation requirements for T -
cells (Kundig et al., 1996). Therefore, only those antigens that persist for many days and
provide a sustained, strong stimulus to the T-cell via the TCR would enable T-cell
activation and initiation o f an effective immune response (Kundig et al., 1996). To enable
T-cells to respond more effectively to antigenic peptides (but also to prevent abberant
activation o f T-cells by normal healthy cells), mature APCs (primarily dendritic cells)
provide additional signals to T-cells in the form of cytokine signals and costimulation via
CD28-B7, IC0S-B7h and CD40-CD40L interactions (Salomon and Bluestone, 2001; Yu
et al., 2001). CD28 is often considered the paradigm for the mechanism of costimulation.
For many years the “two signal” hypothesis was thought to be sufficient to explain the
mechanisms o f costimulation and why allogeneic tissue transplants were not always
rejected (Lafferty et al., 1983; Lafferty and Woolnough, 1977). In this model, signals are
transmitted to the nucleus via the TCR (signal one) and these signals are enhanced by
signals via a separate CD28-dependent signalling cascade resulting in effective T-cell
activation, cytokine gene transcription and proliferation (Babcock et al., 1987; Jenkins
and Schwartz, 1987; Thompson et al., 1989). Further evidence that signals via CD28
enable more effective T-cell activation was provided by Lanzavecchia et al who
demonstrated that the number of TCRs that needed to be engaged for T-cell activation
was reduced from 8000 to 2000 when CD28 costimulation was provided (Valitutti et a i ,
1995).
However, recent studies suggest that the two-signal hypothesis might be an
oversimplification of costimulation. Viola et al. demonstrated that CD28 engagem ent
recruited membrane microdomains (or lipid rafts) rich in signalling molecules to the
immunological synapse thereby increasing the availability o f signalling molecules in the
region o f the synapse (Viola et al., 1999). In addition, Bromley et al. (Bromley et a i ,
2001) demonstrated that CD28 was not recruited en masse to the synapse but that only a
fraction of cellular CD28 was engaged in the synapse during activation. Their proposal
holds that T-cell activation is dependent on an increasingly complicated series o f
thresholds that the T-cell must cross before it becomes fully activated (Bromley et a i ,
2001). Furthermore, the recent discovery o f the inducible costimulator (ICOS) adds
another level of complexity to the costimulatory requirements for T-cell activation (D ong
et a i , 2001; Hutloff et al., 1999; McAdam et a i , 2000; Tamura et al., 2001; Yoshinaga et
al., 1999).
16

___________________________________________________________________________________________________________________________________________ C h a p t e r 1
From the previous observations, it is clear that many aspects o f T-cell activation remain to
be discovered. This is also apparent in our current knowledge o f the intracellular
signalling pathways activated during T-cell stimulation. We already know these to be
extremely complicated networks and far too complex to be summarised here (Reviewed in
(Kane et al., 2000; Myung et at., 2000; Tomlinson et at., 2000)).
Differentiation o f naïve T~cells into memory and e f f e c t o r c e l l s
Upon receiving the appropriate stimulus, naïve T-cells begin their differentiation into
memory and effector T-cells. The way in which this differentiation process occurs
remains the matter o f some debate. The opinion held by many investigators is that during
the course o f the immune response, naïve T-cells acquire effector functions, clear the
infection then revert back to a resting state and are maintained in the body as long-lived
memory cells (Ahmed and Gray, 1996; Busch et al., 1998; Grayson et al., 2000; Jacob
and Baltimore, 1999; Murali-Krishna et al., 1998; Opferman et al., 1999). This model is
further supported by recent data from Swain et al. (Hu et al., 2001; Swain et al., 1999)
demonstrating that adoptive transfer o f effector Thl or Th2 cells into irradiated mice was
followed by reversion o f these cells to long-lived small resting T-cells. A second model o f
effector and memory cell generation from naïve cells was proposed by Lanzavecchia et al
(Lanzavecchia and Sallusto, 2000). In this model, naïve CD4" T-cells, upon stimulation
with antigen, differentiate first into non-polarised cells with characteristics o f memory
cells and then become polarised towards either Thl or Th2 effector cells (Figure 1.6).
Both in vivo models provide viable evidence for each differentiation pathway. However,
each o f these publications utilised in vivo model systems that were subject to experimental
limitations. Swain et al. were unable to address the possibility that populations of non
polarised memory cells exist and that cells do not have to acquire effector function then
revert back to a resting-memory state. Equally, lezzi et al. using a different in vivo model,
were unable to demonstrate that resting populations of polarised Thl and Th2 cells form
a significant portion o f the memory pool (lezzi et al., 2001). It seems likely, given the
heterogeneity of T-cell responses in a normal individual, that both of these populations
would exist. As a protective mechanism, this would allow the individual to mount a rapid
response to re-infection by mobilising differentiated effector cells to the site o f infection.
However, if these cells constituted the only memory population, the pool of T-cells to any
particular antigen could be exhausted quite rapidly (Hayflick and Moorhead, 1961). This
might be particularly important for the ongoing immune responses necessary to prevent
reactivations of latent viruses such as CMV and EBV and indeed, exhaustion o f CD8" T-
cells in HIV-infected individuals has been demonstrated (Effros et al., 1996). Therefore,
the maintenance of a pool of less differentiated memory cells would allow long term
immunological memory to be maintained.
17

C h a i >t i ; r 1
C ontinuous TCR engagem ent + co-stim ulatory signals
centralmemory
effectormemory
end-stage effector
naïve apoptos IS
pathogenclearance
pathogenclearance
non-polansed central memory
T h l, Th2, Tc polarised effector memory
pathogenclearance
antigenstimulation re-challenge
activated effector T hl.T h Z , Tc
activated effector T h l,T h 2 , Tc
restingmemory
Figure 1.6: Proposals for the differentiation of naïve to memory and effector T-cells(A) M odel p roposed by L anzavecch ia et al. where the extent o f T-cell d i f fe ren t ia t ion is con t ro l le d by th e
d ura t ion o f T C R signall ing. In this model, individual T-cells have individual ac t iv a t io n th re sh o ld s and du r ing
the cou rse o f an im m une response , m em ory cells , effec tor ce lls and en d -s tag e effec to r ce l ls are g e n e ra ted
d e p e n d in g on the dura tion o f s t im u la t ion o f individual T-cells . (B) P roposa l by Sw ain et al. where e f fe c to r
cells are genera ted as a first stage in the T-cell response . Once the p a th o g en is c leared , the m a jo r i ty o f
re sp o n d in g c lones die but a proport ion o f ce lls are rescued from a p o p to s is and are m a in ta ined as l o n g - l i v e d ,
res t ing , m e m o ry T -ce l ls which can respond rapidly upon re-infection.
Regardless of the exact pathway of differentiation, it appears that the most basic
requirements for naïve to memory and effector cell differentiation are appropriate
MHC/peptide, costimulation and cytokine signals all of which can be provided by mature
dendritic cells (Reviewed in (Lanzavecchia and Sallusto, 2000)). A number of other
studies have analysed additional requirements for cells to differentiate from naïve to
memory and effector T-cells.
First, does differentiation from naïve to memory and effector T-cells require T-cell
activation followed by proliferation? While there is evidence that naïve T-cell activation
and differentiation to memory and effector cells does require proliferation (Bird et al.,
1998; Gudmundsdottir et al., 1999; Hu et al., 2001; Laouar and Crispe, 2000; Richter et
1 8

___________________________________________________________________________________________________________________________________________ C h a p t e r 1
al., 1999; Wells et al., 2000), the most compelling argument to the contrary was provided
by Laouar and Crispe (Laouar and Crispe, 2000). These investigators argued that
proliferation was not required for differentiation into memory or effector cells. Thus,
while cells might proliferate during the process of differentiation, the lack of requirement
for cell proliferation allows flexibility in the CD4 response. Therefore, under normal
conditions when ‘space’ might limit proliferation, differentiation o f naïve T-cells to
effector cells is not limited by a lack o f proliferation (Laouar and Crispe, 2000).
Second, a recent study by Reinhardt et al. viewed the generation of memory CD4 T-cells
from naïve T-cells in tissue sections o f whole mice (Reinhardt et al., 2001). Using this
system, they were able to demonstrate that another basic requirement for memory T-cell
generation was that the peptide be coinjected with adjuvant (lipopolysaccharide),
consistent with other studies (Kearney et al., 1994; Mitchell et al., 2001; Vella et al.,
1995). Furthermore, they were able to show conclusively that naive T-cells resided
primarily in secondary lymphoid tissues and that chronic stimulation (over 3-11 days)
generated populations o f memory cells which migrated to other tissues such as the liver
and lungs.
Differentiation o f naïve CD4^ T-cells to polarised Thl or TH2 subsets
The continued stimulation of naïve CD4" T-cells during an immune response can lead to
differentiation into Thl or Th2 subsets (Abbas et al., 1996; Romagnani, 1994). Naïve
CD4* T-cells that receive prolonged stimulation through the TCR in the presence o f IL-12
develop into Thl T-cells which produce IFN-y and are responsible for directing immune
responses leading to eradication of intracellular pathogens (Sher and Coffman, 1992). On
the other hand, naïve CD4^ T-cells that receive prolonged TCR stimulation in the presence
of IL-4 differentiate into Th2 cells which produce IL-4, IL-5 and IL-13 and direct
immune responses towards antibody mediated immunity against helminths and allergens
(Abbas et al., 1996; Mosmann and Sad, 1996; O'Garra, 1998; Romagnani, 1994).
Given that Thl and Th2 cells mediate responses to very different pathogens and that
differentiation is controlled by IL-12 and IL-4, how is Thl and Th2 development
regulated?
At the molecular level, differentiation into Thl or Th2 cells is thought to be regulated by
activation o f different transcription factors such as NF-AT, NF-kB, STAT molecules and
G ATA-3 (Reviewed in (Rengarajan et al., 2000)). However, what are the signals that
determine whether cells will begin a developmental programme biased towards Thl or
Th2 differentiation?
19

___________________________________________________________________________________________________________________________________________ C h a p t e r 1
These signals have been the topic of several reviews (See (Lanzavecchia and Sallusto,
2000; O'Garra, 1998)), Lanzavecchia proposes that signals from the environment
(whether this be pathogen binding to PRRs, adjuvants, inflammatory cytokines or
prostaglandins) drives the differentiation of dendritic cells down a particular pathway
which subsequently drives T-cells down a similar pathway. Therefore, DCs primed in the
presence of pathogens that induce IL-12 production will elicit Thl responses. DCs which
are stimulated to mature in the presence of inflammatory cytokines, cholera toxin or
prostaglandin E2 (Braun et a l , 1999; Gagliardi et al., 2000) are thought to elicit Th2
responses (Lanzavecchia and Sallusto, 2000). O’Garra highlights the importance o f
several other factors including the genetic background of the host as well as the dose and
route o f immunisation as important in driving Thl and Th2 differentiation (O'Garra,
1998).
In contrast to the relative difficulty of driving CD4"' T-cells to differentiate to effector
cells, recent experiments indicate that CD8^ T-cells have much less stringent
differentiation requirements. Indeed, it appears that once activated, CD8^ T-cells can
acquire effector function in the absence o f further antigenic stimulation (Kaech and
Ahmed, 2001; van Stipdonk et at., 2001; Wong and Pamer, 2001). This implies that
differentiation of CD8 cells to effectors is pre-programmed and that recognition o f
antigenic peptides (in the presence of costimulation) is sufficient to drive terminal
differentiation. This may reflect the differential functions of CD4^ and CD8" T-cells.
While CD4’' T-cells are refulatory in that they orchestrate the immune response, CD8^ T-
cells are required to proliferate rapidly, then differentiate into effector cells and clear the
infection (Foulds et at., 2002). The results presented later in this thesis demonstrate that a
high proportion of CD8^ T-cells in haematopoietic stem cell transplant recipients are
highly differentiated. The less stringent requirements of CD8 T-cells to achieve terminal
differentiation may help to explain these results.
Homeostatic control o f T-cell numbers and diversity
From the moment of birth, we are continuously exposed to foreign pathogens
necessitating a continuous evolution of the immune system to provide appropriate
responses to these infections. The previous discussions demonstrate that during the course
o f an adaptive immune response, clones of T-cells become activated then proliferate and
differentiate into memory and effector cells. If such proliferation were to continue
unabated, the entire T-cell compartment would be filled with expanded clones and the
diversity o f the T-cell compartment would be extremely restricted. However, current
estimates o f between 10* and 10“ individual TCR-expressing clones in a normal
individual have been made (Arstila et a l , 2000). Due to the cross-reactivity o f TCR-
recognition, the number of clones specific for any given antigen is in the order o f 1 in 10^
20

___________________________________________________________________________________________________________________________________________C h a p t e r 1
(Van Parijs and Abbas, 1998). During the course of an immune response, clonal
expansion occurs and the frequency o f specific T-cells can increase to 1 in 1000 or more
(McHeyzer-Williams and Davis, 1995; Mondino et a i , 1996; Sprent and Tough, 1994;
Zinkernagel, 1996). The most extreme case of clonal expansion in humans yet observed
is illustrated in patients experiencing episodes o f acute infectious mononucleosis, where
EBV-specific CDS^ T-cells can constitute up to 50% of the total CDS^ T-cell pool (Callan
et al., 1998). Clearly, this gross clonal expansion of cells reactive to one epitope (while
necessary to fight the infection) if left unchecked would have serious consequences for
the diversity of the T-cell pool.
It is now well documented that the T-cell compartment is strictly regulated and maintains
T-cell numbers, ratios and diversity at a fairly constant level throughout life. Upon
resolution of an infection, death of the majority of the responding clones ensues and the
T-cell compartment is restored to baseline levels between 4 and 12 weeks post-infection
(McHeyzer-Williams and Davis, 1995; Mondino et al., 1996; Zinkernagel, 1996). Even in
the absence of thymic output, homeostatic mechanisms maintain both the naïve and
memory T-cell pool with naïve and memory cells having the ability to divide in the
periphery in the absence of overt antigen stimulation (Sprent and Tough, 1994). Further
evidence o f homeostatic control of T-cell numbers is provided by studies in T-cell
deficient mice. Following transfer into SCID, nude or sublethally irradiated RAG^' mice,
T-cells divide slowly to fill up the peripheral T-cell pool (Bell et al., 1987; Bruno et al.,
1996; Oehen and Brduscha-Riem, 1999; Pereira and Rocha, 1991; Rocha et al., 1989).
What then are the signals that exert homeostatic control over T-cell numbers?
Many suggestions have been made that resources, whether these be in the form of MHC-
peptide complexes, cytokine signals or growth factors, are present in limited amounts and
that T-cells must compete for these signals to survive or proliferate (Freitas and Rocha,
2000; Freitas et al., 1995; Marrack et al., 2000). It is also thought that these resources are
specific for each component of the immune system (Tanchot et al., 1997). Therefore,
peripheral B- and T-cells occupy separate niches and compete for different resources, a
conclusion based on observations that T-cell deficient mice have normal numbers o f B-
cells (Mombaerts et al., 1992) and vice-versa (Kitamura et al., 1991). This proposal has
been extended to suggest that naïve and memory cells also occupy separate niches since
memory cells, when transferred to T-cell deficient mice, expand to form a pool equivalent
in size to the memory pool in normal animals (Tanchot and Rocha, 1995). This
observation partly explains the maintenance of repertoire diversity and memory/recall
responses. Thus memory cells with a restricted repertoire would not occupy the niche
reserved for the diverse naive T-cell pool. Neither would thymic emigrants affect
immunological memory by directly feeding into the memory T-cell pool (Tanchot et al.,
1997).
21

___________________________________________________________________________________________________________________________________________C h a p t e r 1
Consistent with the ‘niche’ and ‘resource limitation’ hypotheses, numerous studies have
shown that naïve and memory T-cells differ in their signal requirements for survival and
proliferation. For survival, naïve T-cells require signals from self-MHC molecules (but not
their selecting peptides) whereas memory T-cells can survive for extended periods in the
absence of any MHC signals (Murali-Krishna et al., 1999; Swain et at., 1999; Tanchot et
at., 1997). To undergo homeostatic proliferation, naïve T-cells require self-MHC (Bender
et al., 1999; Goldrath and Bevan, 1999; Goldrath and Bevan, 1999; Murali-Krishna et al.,
1998; Viret et al., 1999) and their positively selecting peptide (Ernst et al., 1999;
Goldrath and Bevan, 1999; Viret et al., 1999). On the other hand, when memory
polyclonal or TCR transgenic monoclonal CD4^ T-cell populations are transferred to T-
cell depleted syngeneic hosts, they divide without their positively selecting peptide, but
still depend on TCR-MHC class II interactions (Bender et al., 1999; Ernst et al., 1999;
Viret et al., 1999). The homeostatic proliferation of CDS^ polyclonal or TCR transgenic
cells in wild type hosts is also dependent on class I interactions (Goldrath and Bevan,
1999; Kieper and Jameson, 1999; Murali-Krishna et al., 1998). Furthermore, in the
concept of resource limitation, the number of MHC-peptide binding sites on professional
APCs may be a limiting factor controlling T-cell numbers in a T-cell replete individual
(Kedl et al., 2000). These results suggest that one of the basic requirements for T-cell
homeostasis is a signal via the TCR. Suggestions have also been made that the T-cell
receives and processes signals for survival, homeostatic proliferation and activation via the
TCR and that the response is dependent on the strength of the signal. That TCR signal
strength might be important was investigated by Seddon et al. (Seddon et a i , 2000). The
results from this study demonstrated that recruitment and activation of p 56‘‘"‘‘ during TCR
stimulation by MHC-peptide was a crucial step governing the outcome of TCR-MHC
interactions. In this model, survival signals (provided by antagonist peptides) were not Ick-
dependent, homeostatic proliferation (driven by moderate TCR stimulation by partial
agonist peptides) was /cA-dependent and T-cell activation (strong agonist signals provided
by CD3 crosslinking) was highly /c/c-dependent.
Other resources that might be important in regulating T-cell homeostasis are cytokines
and growth factors. IL-4, IL-6 and IL-7 are known to prolong naïve T-cell survival (Boise
et al., 1995; Kishimoto and Sprent, 1999; Vella et al., 1997) whereas activated T-cells can
be sustained by any member of the IL-2 subfamily of cytokines (IL-2, IL-4, IL-7, IL-9
and IL-15 but not IL-6; (Marrack et al., 2000; Soares et a l , 1998)). In addition, activated
but not naïve T-cells can be maintained in vitro by type I interferons (Marrack et al.,
2000). With regard to homeostatic proliferation in vivo, IL-7 is perhaps the most
important cytokine driving this process (Marrack et al., 2000; Tan et al., 2001; Webb et
al., 1999) although IL-12 (Kieper et al., 2001) and IL-15 (Kennedy et al., 2000; Ku et
al., 2000; Lodolce et al., 1998) may also be involved.
22

___________________________________________________________________________________________________________________________________________ C h a p t e r 1
The maintenance o f homeostasis in the T-cell compartment is also dependent on
mechanisms that switch off T-cell responses, either at the end of an immune response,
preventing autoimmune reactions, or any other inappropriate T-cell responses. Such
mechanisms can be broadly described in two categories. First, the absence or loss o f
stimuli that provide survival and differentiation signals to T-cells leads to functional
inactivation or programmed cell death (passive cell death). Second, T-cell activation itself
activates regulatory pathways whose function is to exert control over T-cell activation and
differentiation (activation induced cell death).
Passive cell death is consistent with the “resource limitation” hypothesis since it is
primarily reliant on growth factor withdrawal at the end of the immune response or lack
of appropriate activating signals in the first place. The requirement o f T-cells for signals
via the TCR and co-stimulatory molecules such as CD28 was described previously. A
number of pathogens prevent T-cell responses by down-regulating their MHC-peptide
complexes resulting in a lack of stimulation via the TCR and lack o f T-cell activation
(Reviewed in (Ploegh, 1998)). In this instance, T-cells do not recognise the invading
pathogen and no immune response is made. On the other hand, if T-cells are exposed to
antigen in the presence of B7 (CD80 or CD86) antagonists or if CD28-deficient T-cells
are exposed to antigen (i.e. TCR engagement in the absence o f co-stimulatory signals),
the cells fail to become activated and undergo rapid apoptosis (Boise et al., 1995;
Kearney et al., 1995; Khoruts et al., 1998; Sperling et al., 1996; Van Parijs et al., 1996).
Such a mechanism is also crucial for the prevention of immune responses to self-antigens.
Activated T-cells undergo apoptosis by both passive and activation-induced cell death. At
the end of an immune response, expanded effector cells begin to die and T-cell numbers
gradually decline to baseline levels. Activated T-cells that are deprived o f survival stimuli,
such as co-stimulatory signals and cytokines, lose expression o f anti-apoptotic proteins
such as Bcl-2 and Bcl-xL and the cells die of neglect (Reviewed in (Van Parijs and Abbas,
1998)). Activation-induced cell death (AICD) on the other hand is purposefully induced
by T-cells as a mechanism of self-regulation. AICD is primarily mediated via the Fas-FasL
pathway. Activated T-cells up-regulate the expression o f both Fas and FasL. Cell-cell
interaction of activated T-cells expressing Fas-FasL leads to apoptosis o f the interacting
cells (Nagata and Suda, 1995; Van Parijs et al., 1998). This pathway is induced by
repeated activation, is potentiated by lL-2, is not prevented by expression of Bcl-2 or Bcl-
xL and is thought to be important in preventing T-cell responses to self-antigens (Van
Parijs et al., 1998; Welsh et al., 1995).
A second mechanism that is designed to down-regulate T-cell responses is the
transduction of signals to activated T-cells via cytotoxic T-lymphocyte antigen-4 (CTLA-
4; (Chambers et al., 2001; Chambers et al., 1997)). CTLA-4 is recruited to the region o f
contact between T-cell and APC but is retained within the cell during the initial phases o f
23

___________________________________________________________________________________________________________________________________________ C h a p t e r 1
T-cell activation and synapse formation (Egen and Allison, 2002). CTLA-4 is then
expressed on the cell surface after continued stimulation where it binds to its ligand
(CD80 or CD86) and transduces signals that inhibit IL-2 transcription and the progression
of T-cells into cell cycle (Calvo et al., 1997; Krummel and Allison, 1996). However, the
precise molecular mechanism leading to CTLA-4-mediated inhibition o f IL-2 production
is not clear.
Clearly then, homeostasis of the T-cell compartment is an active, ongoing process
controlled to a certain extent by resource limitation. Although significant advances have
been made in defining the nature of these resources, the exact mechanisms responsible for
maintaining T-cell numbers at a constant number in normal individuals remain unclear.
Furthermore, homeostasis o f T-cell numbers is maintained throughout life even though
the ageing process affects pathways feeding into the T-cell compartment.
Ageing and the T-cell compartment
The effects o f ageing on the T-cell compartment can be considered as two ongoing
processes. First, the effects of ageing o f the organism and how general age-related
changes in the immune system affect the T-cell compartment. Second, it is necessary to
consider ageing o f individual T-cell clones and the concept of replicative senescence.
During the normal process of ageing, almost every component of the immune system
undergoes changes, resulting in either diminution or enhancement of responses (Reviewed
in (Globerson and Effros, 2000)). The age-related decline in the immune system
manifests ultimately as increased rates o f morbidity and mortality in the elderly due to
infection. This is also apparent as diminished protective immunity after influenza
vaccination, reduced reactivity to tuberculin skin tests and re-emergence o f latent viral
infections such as Varicella zoster (Globerson and Effros, 2000)).
The most significant and commonly described change in the T-cell compartment during
ageing is a shift in phenotype from naïve CD45RA^ T-cells to memory CD45R0^ T-cells
(Globerson, 1995). This shift away from a population of naïve T-cells most likely results
from two ongoing processes. First, the influences of cumulative exposure to foreign
pathogens over time. The second possibility relates to the previously described
phenomenon of T-cell homeostasis. It is known that thymic output decreases with
increasing age (Douek et a i , 1998; Jamieson et a i , 1999), therefore, the increasing
number o f memory cells may represent homeostatic compensation for reduced thymic
output (Timm and Thoman, 1999). The argument against this is that naïve and memory
cells supposedly occupy separate niches (Tanchot et al., 1997), but the possibility remains
24

___________________________________________________________________________________________________________________________________________C h a p t e r 1
that the size of the available niche for memory cells increases as part of the ageing
process.
As well as an increased number of memory T-cells during ageing, investigators have
noted qualitative changes in T-cell responses (Mu and Thoman, 1999). Thus despite aged
mice maintaining some level of thymic output (Mackall et al., 1998) a recent study
suggested that the majority of the CD4^ T-cell pool were o f a memory
(CD44'’‘®'’CD45R B‘°' ) phenotype and produced mRNA for IL-4, IL-5 and IFNy (Mu and
Thoman, 1999; Timm and Thoman, 1999). In contrast, CD4^ T-cells from young mice
produced only IL-2. Age related changes in the CDS^ T-cell compartment are also
apparent. Clonal expansions of CDS^ T-cells during the ageing process have been noted
(Effros and Pawelec, 1997; LeMaoult et al., 2000; Posnett et al., 1994). These clonally
expanded CDS'” T-cells have a characteristic CD8^CD28' phenotype and have been
suggested on the basis o f telomere length and proliferative capacity to represent end-stage
cells that have reached a state of replicative senescence (Reveiwed in (Effros et al., 1994;
Effros and Pawelec, 1997)).
Replicative senescence represents the second process of ageing that is apparent within the
T-cell compartment. Therefore, in addition to ageing of the organism as a whole, T-cells
themselves have a finite life-span. Replicative senescence was first noted in fibroblast
cultures by Hayflick and Moorhead (Hayflick and Moorhead, 1961). These investigators
were the first to report that cells can only undergo a certain number o f cell divisions and
called this the ‘Hayflick Limit’. For a population such as T-cells, that are reliant on clonal
expansion, the Hayflick limit could have serious consequences on their ability to
continuously fight infections. In fact, exhaustion of CTL clones in the face o f high level,
continuous stimulation has been demonstrated by Zinkernagel’s group (Gallimore et al.,
1998; Hunziker et al., 2002; Moskophidis et al., 1993). In these studies, CTL clones
responding to epitopes from lymphocytic choriomeningitis virus (LCMV) were exhausted
and mice were unable to clear the infection when high doses of LCMV were administered.
CD4^ and CD8^ T-cells appear to reach replicative senescence after 17 to 35 cell divisions
depending on the model system used (Adibzadeh et al., 1995; Grubeck-Loebenstein et
al., 1994; Pawelec et al., 1996; Perillo et al., 1989; Weng et al., 1995). Nevertheless, these
cells are still able to function within the immune system. Senescent cells are able to
upregulate CD25 expression after antigen stimulation, CD8^ cells are able to carry out
antigen-specific cytotoxicity and senescent CD4" cells secrete cytokines after stimulation
via the TCR (Adibzadeh et al., 1995; Perillo et al., 1989). Cell surface markers have not
proved significantly different on senescent cells compared with non-senescent cells with
the exception of CD28 (Adibzadeh et al., 1995; Effros et al., 1994). CD28 is expressed
on progressively fewer CD8‘" cells after each cell division such that 95% of senescent cells
are CD28 (Effros et al., 1994). CD4^ T-cell clones also show marked reduction in CD28
25

_________________________________________________________________________________________________________________________________ C h a p t e r 1
expression after repeated rounds of stimulation (Adibzadeh et a i , 1995; Pawelec et al.,
1996). The limiting factor that prevents infinite cell division is telomere length. The
dynamics of telomere length are discussed elsewhere (Blackburn, 2001).
Perhaps the most important aspect o f ageing that affects maintenance o f the T-cell
compartment is age-related thymic involution. The process of thymic involution begins
approximately 1 year after birth and is characterised by a gradual deposition o f adipose
tissue in the thymus resulting in a greatly decreased volume of useful lymphoepithelial
tissue and decreased T-cell production throughout life (Douek et a l , 1998; Steinmann et
at., 1985). With regard to cellular changes during thymic involution, changes occur in
both thymic stromal elements and bone marrow-derived thymocyte progenitors (Yu et al.,
1997). Thus, with increasing age there is a reduced proliferative capacity o f thym ocyte
precursors and an attenuated interaction of developing thymocytes with the thymic
stroma. In addition, aged bone marrow has been shown to contain reduced numbers o f
progenitors and to have a reduced capacity to seed fetal thymic epithelium (Fridkis-Hareli
et al., 1992; Globerson et al., 1992). Thymic involution is also affected by circulating
hormones and other soluble factors. IL-7 production by stromal cells is significantly
decreased in the aged thymus and administration of exogenous IL-7 can significantly
increase thymic output (Aspinall and Andrew, 2000; Mackall et al., 2001). The
concentration o f noradrenalin and noradrenergic receptors increases significantly during
ageing (Madden et al., 1997). In addition, growth hormone and insulin growth factor-1
levels are reduced with age and administration o f these factors seems to influence bone
marrow cells that settle in the thymus (Montecino-Rodriguez et al., 1998). There is also
some evidence that sex hormones influence thymic involution (Leposavic et al., 2001 ;
Olsen et al., 1998) and furthermore that removal of these hormones by castration can
reverse age-related thymic involution to some extent (Olsen et al., 2001 ; Windmill and
Lee, 1999).
Only recently have we begun to appreciate that the thymus maintains some level o f
activity until late in life. Direct evaluation o f thymic output in aged mice and humans
(Douek et al., 1998; Jamieson et al., 1999; Mackall et al., 1998) and recipients o f
chemotherapy followed by HSCT (Douek et al., 2000; Weinberg et al., 2001) has
demonstrated a significant contribution of thymic-dependent pathways to T-cell
reconstitution. These observations have generated significant interest in the mechanism o f
thymic involution. However, although proposals have been made as to the causes,
evolutionary advantages and necessities of thymic involution (George and Ritter, 1996;
Turke, 1997), strategies to reverse thymic involution have only been marginally successful
(Weinberg et al., 1995; Mackall et al., 2001; Min et al., 2000). Clearly, thymic involution
is a multi-faceted process and we need a better understanding of how it is regulated before
successful approaches can be designed.
26

C h a p t e r I
Haematopoietic cell transplantation (HCT)
The previous descriptions have highlighted some of the advances we have made in
understanding the biology of T-cells. The possibility o f utilising T-cells in
immunotherapy approaches for the treatment o f cancers has generated significant interest
over the last 5-10 years. The transplantation of haematopoietic cells represents perhaps
the most basic form of immunotherapy (when considered among some of today’s elegant
approaches), but the initiation of haematopoietic stem cell transplant research was
motivated by very different circumstances.
Towards the end of World War II, the populations o f Hiroshima, Nagasaki and the
surrounding areas were exposed to lethal doses of radiation. A number o f investigators
proceeded to study the effects o f irradiation in mice and demonstrated that mice could be
rescued from lethal doses of irradiation by transplantation o f syngeneic bone marrow. It
was not long after this that the first studies demonstrated the existence o f pluripotent
haematopoietic stem cells (Reviewed in (Weissman, 2000)).
The transplantation of bone marrow was subsequently utilised as a rescue strategy that
allowed physicians to increase chemotherapy and radiotherapy doses to lethal levels as a
method o f killing cancerous cells. The first successful bone marrow transplant was
reported in 1959 and was carried out between identical twins (Thomas et al., 1959). Since
the late 1970s and early 1980s, autologous and allogeneic HCT (which includes bone
marrow, peripheral blood and cord blood as a source of cells) has been used in the
treatment o f an increasing spectrum of diseases including haematological malignancies,
primary immunodeficiency diseases, bone marrow failure syndromes, autoimmune
diseases and some solid tumours. To date over 125,000 allogeneic HCTs have been
performed worldwide.
There are many factors that influence the outcome of HCT and many problems to
resolve. Graft-vgrjw.y-host disease (GVHD), relapse of the primary malignancy, infections
and immune reconstitution all remain significant obstacles to the success of HCT. Since
the main aim o f this thesis is to analyse T-cell reconstitution post-HCT, the next section
outlines the general causes and the pivotal role that T-cells play in each of these processes.
27

___________________________________________________________________________________________________________________________________________ C h a p t e r 1
HLA-matching and Graft-versus-host disease (GVHD)
With the increasing popularity o f HCT coupled with advances in graft engineering and
HLA matching, the potential donor pool has increased significantly. Before 1980 virtually
all HCT were carried out between HLA-matched siblings (Cleaver, 1993; Hansen et al.,
1981; Hansen et al., 1980). However, only -30% of patients in need o f a transplant have
this option available to them. Since 1980, the donor pool has expanded to include HLA-
matched and mismatched unrelated, haploidentical and related and unrelated cord blood
donors. The unrelated donors have been recruited by a number o f bone marrow donor
registries such that approximately 7-7.5 million unrelated donors are now available. The
net result of this unrelated donor recruitment is that >50% of patients lacking an HLA-
identical sibling donor now have the option of a transplant from an unrelated donor.
However, even HCT administered between HLA-identical siblings and identical twins can
be accompanied by immunological reactions of the graft against the foreign tissues of the
host (GVHD) and the residual host immune system against the graft (graft failure or
rejection). The development of GVH reactions is determined largely by the degree o f
HLA-disparity between donor and patient (Klein and Sato, 2000; Klein and Sato, 2000).
Until recently, selection of unrelated donors for transplant was reliant on matching for
HLA-A, -B and -DR antigens. However, it has become increasingly obvious in recent
years that it is essential to match donor and recipient for HLA-A, -B and -C (class I); and
HLA-DRB1, -DQ Bl and -DPBl (class II) antigens (Erlich et al., 2001; Madrigal et al.,
1997). These realisations have arisen due to the advances in HLA-typing technologies
(Reviewed in (Erlich et al., 2001)) which to date have enabled the identification o f more
than 125 HLA-A, 260 HLA-B, 75 HLA-C, 225 HLA-DRB 1 and 40 H LA-DQ Bl alleles.
The advances in tissue-typing technologies have also enabled analyses of the number o f
truly HLA matched unrelated donor transplants. Previously published work has reported
that over 30% of serologically matched donor-recipient pairs were HLA mismatched
when tested by Sequence Based Typing (Petersdorf et al., 1998). The results from the
Anthony Nolan Research Institute using Reference Strand-mediated Conformational
Analysis (RSCA), are in agreement with these previously published results (Arguello et al.,
1998; Scott et al., 1998), are in agreement with these previously published results. In
addition, the discovery of minor histocompatability antigens (MiHA) has led to the
realisation that HLA-identical sibling have some degree o f genetic disparity (Goulmy,
1997; Warren et al., 1998).
That T-cells are involved in the pathology of GVHD is now undisputed. However, the
activation o f alloreactive T-cells does not represent aberrant T-cell activation, but rather
reflects a lack of donor T-cell education to the host’s tissues (Reviewed in (Garcia et al.,
1999; Jameson and Bevan, 1998)). The discussion earlier in this chapter was focused on
the activation of T-cells by foreign peptides presented in the context o f self-MHC
28

___________________________________________________________________________________________________________________________________________ C h a p t e r I
molecules. The specificity of this process and maintenance of self-tolerance is dependent
upon education of the T-cell population in the thymus (and also in the periphery). In the
context o f HCT however, T-cells have not been tolerised to either host MHC molecules (in
the case of HLA-mismatched transplants) or the peptides that they present. Therefore,
subsets of T-cells (termed alloreactive T-cells) can recognise these host MHC molecules as
foreign (Garcia et al., 1999) and become activated to initiate GVHD. Even when the
HLA-antigens between donor and patient are fully matched (as in sibling or identical twin
transplants) the self-peptides (minor histocompatibility antigens) presented by MHC
molecules can invoke strong T-cell responses.
GVHD can be described as a cell-mediated attack of donor T-cells against host tissues, the
effects of which can be devastating. The transfer of allogeneic T-cells into
immunodeficient mice results in diarrhoea, skin lesions, severe wasting and death within 1
to 3 weeks (Allen et at., 1993; De Wit et a i , 1993). In addition, 80% of patients who
received allogeneic transplants in the absence o f immunosuppression rapidly developed
severe acute GVHD (Sullivan et a i , 1986). GVHD in humans is described as either acute
(manifesting less than 100 days post-transplant) or chronic (>100 days post-transplant).
Acute GVHD is also graded in terms of severity on a five-point scale from 0-IV, taking
into consideration skin, liver and gut involvement (Glucksberg et at., 1974; Thomas et at.,
1975; Thomas et al., 1975). Grade 0 indicates no GVHD, grade I is the least severe form
indicating a localised skin rash and grade IV indicates life-threatening or lethal GVHD
and frequently involves multiple target organs. The risk factors associated with developing
GVHD have been assessed by numerous investigators. HLA matching is of crucial
importance. HLA identical siblings and identical twins have the lowest rates o f GVHD
(between 10-60% depending on the transplant centre) with the relative risk o f developing
GVHD increasing with increasing HLA disparity between donor and patient (Ash et al.,
1990; Beatty et al., 1991; Keman et al., 1993; Martin, 1991). The composition o f the
stem cell graft represents another important risk factor with recipients o f T-cell replete
grafts experiencing significantly higher rates o f GVHD than T-cell depleted grafts. Older
patients also experience increased frequencies o f GVHD compared with younger patients
although the reason is currently unknown (Ringden et al., 1995). Also, sex-mismatching
is associated with increased GVHD thought to result from peptides processed from Y-
chromosome associated proteins (Bross et al., 1984; Doney et al., 1997).
The development of GVHD involves cytokine networks, T-cell activation and activation o f
non-T-cell populations such as NK-cells and macrophages. The initiation o f GVHD is
known to be dependent on the transfer o f donor T-cells. Indeed T-cell depletion has been
well documented to prevent GVHD (Antin et al., 1991; Fahey et al., 1987; Marmont et
al., 1991; Prentice et al., 1984). Donor T-cells expand rapidly upon transfer to an
allogeneic host. Within the first hours of exposure to host alloantigens, donor T-cells
become activated and begin to produce cytokines such as IL-2 and IFNy (Allen, 1993;
29

_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ C h a p t e r I
Troutt and Kelso, 1993; Via, 1991). The production of such Thl type cytokines appears
crucial to the development o f GVHD since modulating the production o f IL-2 and IFNy
prevents GVHD in some models (Fowler et al., 1994; Fowler et al., 1994; Szebeni et al.,
1994). In addition to T-cell involvement in the initiation and exacerbation o f GVHD,
other effectors that cause GVHD-associated tissue damage are NK-cells and macrophages
activated by T-cell derived pro-inflammatory cytokines (reviewed in (Hakim, 1997)).
Murine models demonstrated that NK-cells infiltrate the tissues damaged during GVHD,
particularly epithelial cells o f the skin, liver and colon (Guillen et al., 1986). NK-cell
infiltrates are also associated with tissue damage in the thymus and pancreas (Ghayur et
al., 1987; Ghayur et al., 1988; Ghayur et al., 1987). Increased NK-cell activation and
subsequent production o f IFNy (Sher et al., 1993) TNFa, IL-1 and NO (Garside et al.,
1992; Murphy et al., 1993) may also be important for the development of GVHD. Donor
and host macrophages also increase in number during the first few weeks of GVHD and
play a crucial role in GVHD development. They present host alloantigens to donor T-cells
and subsequently become activated by T- and NK-cell cytokines. In addition, when
stimulated by bacterial products such as endotoxin, macrophages also produce high levels
of TNFa, IL-1, IL-6 and NO (Nestel et al., 1992; Smith et al., 1991).
Therefore, the combination of activated T-cells, NK-cells and macrophages can lead to
systemic activation of the immune system, elaboration of pro-inflammatory cytokines and
in severe cases, mortality due to septic shock (Nestel et al., 1992). Such systemic
activation of the immune system makes effective treatment of GVHD difficult and it
would clearly be of benefit to prevent rather than control GVHD. However, one o f the
main problems facing clinicians is that in the absence of GVHD, patients with malignant
diseases are more likely to relapse (Marmont et al., 1991). It was subsequently realised
that T-cells also play a role in eliminating residual leukaemic cells, a phenomenon known
as Graft-v^r5M.s-Leukaemia (GvL) or Graft-ver^w^-Tumour (GvT). Before discussing the
immunotherapeutic potential of haemopoietic cell grafts, a description o f the current
methods of GVHD prophylaxis and immunosuppression is needed.
Current strategies fo r the prevention and control o f GVHD
Current strategies of GVHD prophylaxis rely on non-specific immunosuppressants such
as Cyclosporin A, FK506 and rapamycin; antimetabolites such as mycophenolate and
azathioprine and cell cycle inhibitors such as methotrexate (Reviewed in (Vander Woude,
1997)). The main problem with all of these agents is the lack of specificity of their
actions. Such global immunosuppression increases the transplant recipient’s susceptibility
to infections and increases the risk of relapse of their primary malignancy. The realisation
that T-cells were crucial for the initiation of GVHD led to the development o f T-cell
depletion strategies as alternative GVHD prophylaxis, demonstrating that the risk o f
30

_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ C h a p t e r I
developing GVHD could be significantly reduced by T-cell depletion. Furthermore, it was
realised that appropriate T-cell depletion {i.e. >2 log depletion of T-cells from the graft)
in animal models circumvented the need for non-specific post-transplant
immunosuppression (Antin et al., 1991; Lowenberg et al., 1986; Young et al., 1992).
However, recipients of T-cell depleted grafts experienced a higher incidence of graft
failure, leukaemic relapse and delayed immune reconstitution compared with recipients o f
T-cell replete grafts (Apperley et al., 1988; Daley et al., 1987; Goldman et al., 1988;
Maraninchi et al., 1987; Small et al., 1997). Therefore, T-cell depletion suffers from
some of the same problems as non-specific immunosuppressants.
T-cell depletion strategies represent perhaps the earliest attempt to engineer
haematopoietic stem cell grafts. The problems associated with depletion o f all T-cells
prompted investigation of alternative methods of graft engineering and GVHD
prevention. The problem of graft failure results from the rejection o f donor
haematopoietic cells by residual host T-cells that have survived pre-transplant
conditioning (Bunjes et al., 1987; Keman et al., 1987). This problem has been
circumvented by administration of Campath antibodies in vivo prior to transplant, thereby
removing residual host T-cells and alleviating the problem of graft rejection (Hale et al.,
1998). The increased relapse rates in recipients of T-cell depleted grafts led to the
development of donor leukocyte infusion (DLI) protocols (Drobyski et al., 1999; Kolb et
al., 1990; Kolb et al., 1995; Mackinnon et al., 1995). T-cell depletion followed by DLI
has been successful in treating or preventing relapse in CML patients with responses also
noted in patients with acute leukaemia, CLL, myeloma and lymphoma (Mandigers et al.,
1998). Although DLI protocols limit the risk of GVHD, they do not abolish the risk
completely and GVHD remains a significant hazard associated with administration o f
DLIs (Collins et al., 1997; Drobyski et al., 1993; Kolb et al., 1990; Kolb et al., 1995;
Mackinnon et al., 1995; Porter et al., 1994).
More recently, a number o f groups have investigated the possibility of ex vivo gene
therapy to insert dmg-inducible suicide genes into donor lymphocytes (Bonini et al.,
1997; Bordignon et al., 1995; Drobyski et al., 2001; Thomis et al., 2001; Tiberghien et
al., 1997). The herpes simplex vims thymidine kinase (HSV-r/:)/ganciclovir (GCV)-based
suicide strategy has been most widely adopted. In this system, cells are engineered to
express HSW-tk such that administration of GCV leads to cell death through r/:-catalysed
metabolism of the dmg to a lethal metabolite. Because the YlSY-tk gene is only active in
cycling cells, the administration of GCV to patients at strategic time-points after transplant
eliminates only proliferating cells (probably alloreactive, but potentially cells involved in
homeostatic proliferation). This system has been used effectively to prevent GVHD
although problems remain with the immunogenicity o f the viral transduced T-cells
(Thomis et al., 2001).
31

________________________________________________________________________________________________________________________ C h a p t e r I
A more simplified graft-engineering protocol was developed by Koh et al. (Koh et at.,
1999). These investigators incubated donor and patient lymphocytes in an MLR, then
depleted the cultures of CD69" , and hence alloreactive, T-cells. In 2° MLRs, the
allospecific proliferation was -10% of the original value while S"' party allospecific
proliferation was maintained (-77% of the original value). Furthermore, CMV antigen-
specific responses were maintained, raising hopes that GVHD would be prevented while
maintaining the GVL potential of the grafts. Intelligent ex vivo graft engineering may
therefore represent the most feasible short-term prospect for GVHD prevention.
Nevertheless, numerous other strategies are currently under investigation.
Blocking antibodies against CD3 (Yu et al., 2001), CD28 (Yu et al., 2000), and CD40L
(Blazar et al., 1997; Durham et al., 2000; Durie et al., 1994; Ito et al., 2001; Wekerle et
al., 2000) as well as CTLA4-lg (Wekerle et al., 2000; Wekerle et al., 1998) are all
proposed to prevent GVHD and in some cases lead to the induction o f peripheral
tolerance. The prevention o f GVHD by manipulating cytokine networks has also been
attempted but with limited success and conflicting results. It has been suggested that acute
GVHD is a Thl-mediated process whereas chronic GVHD has been suggested to be Th2-
mediated (Allen, 1993; De Wit et al., 1993; Fowler et al., 1994; Garlisi et al., 1993;
Krenger and Ferrara, 1996). There is some evidence that acute GVHD can be inhibited by
Th2 cells (Krenger and Ferrara, 1996). However, IL-12 (thought to represent a Thl type
cytokine) can protect against (Sykes et al., 1995) or augment (Via et al., 1994;
Williamson et al., 1996) GVHD. A recent publication by Liu et al. using a suicide gene-
based T-cell depletion method demonstrated that acute GVHD can be prevented to a
certain extent by removing either type 1 or type 2 cells (Liu et al., 2001).
E stablish ing antigen-specific peripheral tolerance
The ultimate GVHD prevention strategy would be the prevention o f alloreactive T-cell
activation with maintenance of all anti-leukaemic and anti-pathogen T-cell responses.
However, the induction o f peripheral tolerance in an antigen-specific manner has proven
difficult to achieve in the allogeneic transplant setting. This is in no small part due to our
lack o f understanding of the basis of TCR cross-reactivity and the exact mechanisms
governing the establishment of peripheral tolerance. We know that central tolerance is
conferred by thymic selection such that thymocytes strongly reactive to self-M HC-self-
peptide com plexes are deleted during negative selection. However, it is unlikely that all
self-antigens are presented by intrathymic APCs. Therefore, to prevent inappropriate
peripheral T-cell activation, peripheral tolerance mechanisms must also exist. As
mentioned previously, the binding of pathogens by pattern recognition receptors (PRRs)
upregulates costimulatory molecule and cytokine expression by DCs and other
professional APCs. Costimulation is known to significantly reduce the activation threshold
32

__________________________________________________________________________________________________________________________________________ C h a p t e r 1
of T-cells (Viola and Lanzavecchia, 1996; Viola et al., 1999). Therefore, in the absence o f
costimulatory signals, TCR-MHC-peptide binding would have to be o f high affinity, slow
off-rate and with a continuous source of antigen to activate a T-cell response (Kundig et
at., 1996). However, T-cells with receptors with such affinities for self antigens are
unlikely to escape thymic selection due to TCR cross-reactivity. Thus low or moderate
affinity interactions would be insufficient to activate a T-cell response to self-peptides in
the absence o f costimulatory signals. Therefore, in its simplest form, peripheral tolerance
is thought to rely on engagement o f the TCR on peripheral T-cells in the absence o f
costimulatory signals (Reviewed in (Foy et a i , 1996; Lenschow et at., 1996)). This
hypothesis has prompted a number of approaches to achieving antigen-specific tolerance
in the allogeneic transplant setting.
First, soluble MHC has been proposed to be a tolerogen (Buelow et at., 1995; King et al.,
1989) although its efficacy in suppressing alloresponses when in monomeric form has
been limited (Arnold et al., 1988; Wang et al., 1996). O'Herrin et al. suggested that such
lack o f potency was due to the low affinity o f binding of soluble monomeric MHC-
peptide com plexes and therefore designed and utilised soluble dimeric MHC-peptide
complexes to achieve peripheral tolerance in the allogeneic transplant setting (O'Herrin et
al., 2001). A rather different approach to achieving peripheral tolerance was the injection
of immature dendritic cells (which lack the costimulatory molecules necessary for fully
activating a T-cell response). These immature DCs were loaded with the influenza matrix
peptide and subsequently injected into mice (Dhodapkar et al., 2001). This approach also
led to the inhibition of T-cell responses to the influenza matrix peptide and the
establishment o f peripheral tolerance, this time in human subjects.
However, the main problem with such antigen-specific tolerance induction approaches is
that the antigens that drive the alloresponse have not been defined and are very probably
different for each individual. Therefore, a number o f investigators have developed
alternative methods of achieving antigen-specific peripheral tolerance. Perhaps the most
popular approach has been the blockade of coreceptor molecules such as CD2 and CD4
and costimulatory molecules such as CD28 and CD40 (Carteron et al., 1989; Chavin et
al., 1994; Guckel et al., 1991; Gutstein et al., 1986; Ito et al., 2001; Taylor et al., 2001;
Wekerle et al., 2000). Although the majority o f these approaches have been developed to
establish bone marrow microchimerism prior to solid organ transplants it seems likely that
similar approaches to peripheral tolerance induction would be beneficial for some
haematological disorders.
Although the prevention o f GVHD remains an elusive goal in HCT biology, patients
transplanted for some leukaemias, lymphomas and myelomas are more likely to relapse in
the absence o f GVHD. This has initiated great interest in the immunotherapeutic potential
33

C h a p t e r 1
of haematopoietic cells grafts and the ability of transplanted allogeneic T-cells to
eliminate leukaemic target cells.
G raft-versus-leukaem ia (GVL)
Barnes et al. in 1956 using a mouse model were the first to suggest that GVL effects
existed (Barnes et al., 1956). Since these initial observations, evidence for a GVL effect in
humans has accumulated, initially based on increased relapse rates in certain
circumstances (Weiden et al., 1979; Weiden et al., 1981). Relapse rates are lowest in
patients who develop both acute and chronic GVHD, higher in those who do not
experience GVHD and even higher in recipients o f T-cell depleted or twin HCT (Horowitz
et al., 1990). Further evidence for a GVL effect was provided by numerous studies using
DLI to treat relapse (Drobyski et al., 1993; Kolb et al., 1990; Porter et al., 1994). That
GVL effects exist is now undisputed. However, the main problem in using GVL as an
immunotherapeutic approach is that it is frequently accompanied by unwanted GVHD.
Therefore, a considerable amount of research effort has been focused on separating the
individual components responsible for each reaction and attempting to stimulate GVL
responses without causing life-threatening GVHD. T-cells are foremost in initiating both
GVHD and GVL responses, therefore earlier approaches were designed to selectively
modulate the T-cell compartment. Early attempts to separate GVHD and GVL in mouse
models included ex vivo depletion of GVH reactive cells (Truitt and Atasoylu, 1991; Weiss
et al., 1990), in vivo elimination of GVH-reactive T-cells (Blazar et al., 1994), in vivo
elimination of NK-cells (Johnson and Truitt, 1992), in vivo inhibition o f CD3"" T-cells
(Blazar a/., 1993) use of high dose IL-2 (Sykes et al., 1993) and the use o f IL-4 and
IL-2 to shift the Th cell profile (Fowler et al., 1994). To date however, these approaches
have not made a significant impact on GVHD/GVL therapy in human clinical trials.
A more appealing approach for generating anti-leukaemic responses is to define antigens
that could be used to separate anti-leukaemic from anti-host responses. Antigens that may
represent feasible targets fall into two broad categories, minor histocompatability antigens
(MiHA) and leukaemia-specific antigens. Goulmy et al. (Goulmy, 1997) and Warren et
al. (Warren et al., 1998) have each identified MiHA antigens which may be potential
targets. A prerequisite for MiHA antigens to be GVL and not GVHD targets is that their
expression be restricted to cells of the haematopoietic lineage. Two MiHA antigens
identified by Goulmy et al. (HA-1 and HA-2) and 12 MiHA antigens identified by
Warren et al. appear to fit these criteria and may therefore serve as appropriate targets for
immunotherapy. Mutis et al. (Mutis et al., 1999) and Fontaine et al. (Fontaine et al.,
2001) have since been able to generate CTL specific for MiHA antigens and are
presumably running clinical trials based on this approach. The main drawback governing
34

___________________________________________________________________________________________________________________________________________ C h a p t e r 1
the use o f MiHA antigens as GVL targets is that they will always be utilised in the context
of HCT. Alternative immunotherapeutic approaches that would not require HCT would be
based on the identification of leukaemia specific antigens. The Bcr/abl antigen in CML
(Chen et a i , 1998) and the PML/RARa antigen in acute promyelocytic leukaemia
(Dermime et al., 1996) both represent leukaemia-specific antigens. While specific CTL
against Bcr/abl have now been identified (Clark et al., 2001), CTL have not been
successfully raised against these targets in vitro (Chen et al., 1998; Dermime et al., 1996).
Normal proteins expressed at higher levels on leukaemic cells compared with normal cells
could also be used as targets with proteinase 3 (PR3) and W ilms’ tumour suppressor
having been identified and used to generate CTL responses (Gao et al., 2000; M olldrem
et al., 2000).
Immune reconstitution post-HCT
The successful reconstitution of the immune system after HCT is also an important goal in
HCT biology. The increasing diversity of diseases eligible for treatment by HCT coupled
with HCT related complications and the increasing diversity o f HCT methodology has
highlighted many factors important for the successful reconstitution of immunity post-
HCT. Many different sources of haematopoietic cells are now used in HCT strategies. In
addition, improvements in post-transplant immunosuppression (including T-cell depletion
and other non-specific immunosuppressants) has meant a reduction in GVHD, thereby
allowing expansion of the donor pool to include HLA-matched and mismatched donors
and also full haplotype mismatched donors. Furthermore, the advent o f non-
myeloablative conditioning regimens has allowed HCT to be carried out in patients
previously considered unable to tolerate conventional high dose conditioning (Amrolia et
al., 2000; Kottaridis et al., 2000; McSweeney et al., 2001). However, each o f these
artificially induced situations poses unique problems to HCT recipients in terms o f
susceptibility to infections in the short-term and of regeneration o f the immune system in
the long-term. For example, fatal opportunistic infections occurred in 12-28% o f
unrelated HCT recipients (Davies et al., 1995; Hansen et al., 1998; Hongeng et al., 1997;
Keman et al., 1993; Marks et al., 1993; Oakhill et al., 1996; Ochs et al., 1995) compared
with 4% to 15% o f HLA-matched sibling BMT (Clift et al., 1994; Hongeng et al., 1997;
Marks et al., 1993; Small et al., 1997; Snyder et al., 1993). Recipients o f HLA-matched
sibling allogeneic PBSCT were less susceptible to infection compared with BMT recipients
(Storek et al., 2001). Therefore, the higher lymphocyte doses received by PB SC compare
with BM recipients (Ottinger et al., 1996; Storek et al., 2001; Storek et al., 1997) has a
direct impact on their susceptibility to infection. Recipients of T-cell depleted grafts also
have a higher incidence of infection compared with T-cell replete HCT recipients (Heslop
35

___________________________________________________________________________________________________________________________________________ C h a p t e r 1
and Rooney, 1997; Hongeng et a i , 1997; Marks et al., 1993; O'Reilly et al., 1997;
Oakhill et al., 1996).
The previous observations have all been made in patients who received conventional high-
dose chemo- and/or radio-therapy followed by HCT rescue. An alternative strategy
(although one which still has many associated problems) that has the potential to cure
many haematological disorders is non-myeloablative conditioning followed by HCT. In
contrast to the previous high-dose conditioning regimens that have been used in an
attempt to destroy tumour cells (also enabling engraftment since the host immune system
has also been destroyed), non-myeloablative conditioning does not destroy the host
immune system completely. Therefore, to prevent rejection and facilitate engraftment o f
the “mini-transplant”, more specifically immunosuppressive agents such as fludarabine
have been used in combination with melphalan, busulphan or low-dose TBI (Giralt et al.,
2001; Khouri et al., 1998; McSweeney et al., 2001).
The rationale for such an approach are two-fold; first to enable treatment of elderly
patients using HCT (a patient group that represents a significant proportion o f patients
diagnosed with haematological malignancies; (McSweeney et al., 2001)) and second to
harness the immunotherapeutic potential of HCT to eliminate leukaemic cells that remain
after conditioning. Another advantage of non-myeloablative conditioning is that while
patients do experience mild pancytopenia, the immunodeficiency is unlikely to be as
severe as the immunodeficiency after conventional conditioning strategies. However, no
studies have been published to date detailing the risk o f infections after non-
myeloablative transplants although the maintenance of high granulocyte and lym phocyte
counts will significantly reduce this risk. On the other hand, GVHD remains a significant
problem with up to 47% of non-myeloablative HCT recipients experiencing Grade II-III
acute GVHD (M cSweeney et al., 2001). A recent publication by Kottaridis utilised
Campath-IH as a method of GVHD prophylaxis after non-myeloablative conditioning
(Kottaridis et al., 2000). This was not associated with a higher risk of relapse or infection
in this patient cohort although this approach raises concerns regarding T-cell
reconstitution in these patients. This is of particular importance when considering that
non-myeloablative transplants might be administered to older patients since increasing
patient age has been associated with an inability to regenerate a diverse T-cell
compartment (discussed in the following chapters).
With regard to HCT using conventional conditioning, the increased rate o f infections that
occurs in the first month after HCT very probably results from a deficiency in both
granulocyte and mononuclear cell subsets while late post-HCT infections are probably
due to deficiencies in T- and B-cell subsets (Small et al., 1997; Storek et al., 2000; Storek
et al., 1997). The deficiencies in T-cell numbers and function have been reported by
numerous investigators. While CD8^ T-cell numbers were restored rapidly, CD4^ T-cell
36

C H A I T I ' R
numbers remained low for extended periods post-transplant (Behringer et al., 1999; Small
et al., 1997; Small et al., 1999; Storek et a i , 2000; Storek et a i , 1997) and correlated
with an increased risk of developing infections.
Thymic-dependent and thymic-independent T-cell recovery after HCT
Recent work by Roux et al. demonstrated that the recovery of the T-cell repertoire and T-
cell function after HCT was absolutely dependent on the regeneration of CD4"CD45RA"
T-cells (Roux et al., 2000). Some years earlier, Mackall et al. suggested that T-cells could
be regenerated after chemotherapy or HCT by two different pathways (Mackall et al.,
1995; Mackall et al., 1993; Mackall and Cress, 1997). The first of these is dependent on
maturation of T-cell precursors in the thymus and is hence termed the thymic-dependent
pathway. The second is dependent on proliferation of mature T-cells transferred with the
stem cell graft and is hence termed the thymic-independent pathway (Figure 1.7;
(Mackall et a i , 1996)).
T hym us Peripheral T -cell pool
+chemotherapy
HCT
th y m ic
emigrants
progenitor
CD45RA
/ o extrathym 1C maturation_____indeperuh
homeostatic
Thym ic-dependent < thymic i n d e p e ^ t ^ ( # ) ( $ ) ( g )
proliferation
CD45ROmature T-cells (naïve and memory)
L ym phoidtissues
Thym ic-dependent > thymic- independent
t® ®Thym ic-dependent = thymic
Figure 1.7; Pathways of T-cell regeneration post-HCTA bla t ion o f the T-cell pool by irradiation and /or chem otherapy with H C T rescue is fo l low ed by a period du r in g
w h ich the T-cell c o m p a r tm e n t is regenera ted . During this period T-cells can be genera ted by at leas t tw o
p a thw ays . P roge n i to r ce l ls m igra te into the thym us where they undergo m a tu ra t ion and en te r the T-cell p o o l
as naïve C D 45R A ^ T-cells . Mature T-cells t ransferred with the graft m igra te into se condary ly m p h o id t i s s u e s
w here they expand and pro lifera te , gen e ra t in g a pool o f cells with a C D 45R O ^ (m em o ry ) p h e n o ty p e and a
restr ic ted T C R reperto ire. T he relative co n t r ib u t io n o f these two pa th w ay s to T -cell r e g e n e ra t io n d e te rm in e s
the overa l l p h e n o ty p e o f the T-cel l co m p ar tm en t post-H CT. It is a lso p o ss ib le that p ro g e n i to r cel ls can
d e v e lo p into a p - T C R " T-cel ls at si tes o ther than the thym us but ev idence for this pa thw ay is lacking.
37

C h a i t e r 1
Thymic-independent T-cell regeneration of the T-cell pool results in a population of T-
cells o f memory phenotype (CD45RO0 with a highly restricted T-cell receptor repertoire
(Mackall et al., 1996). These pathways may be particularly important in regenerating a T-
cell compartment in aged (Mackall et at., 1998) or thymic-deficient (Bell et a i , 1987;
Bell et al., 1989; Mackall é t a l , 1993; Miller and Stutman, 1984) transplant recipients. In
humans, the contribution of thymic-dependent pathways to T-cell reconstitution after
chemotherapy and HCT has been inferred from T-cell phenotyping and TCR repertoire
analysis (Roux et al., 2000; Godthelp et al., 1999; Dumont-Girard et a i , 1998; Wu et a i ,
2000). The contribution of thymic-dependent pathways has also been implied by data
from radiographic imaging of the thymus after chemotherapy (Mackall et al., 1995;
Mackall and Gress, 1997), and a broadening of the TCR repertoire with increasing time
post-transplant (Dumont-Girard et al., 1998; Godthelp et al., 1999; Roux et al., 2000; Wu
et al., 2000). In mouse models, thymic-dependent pathways have also been assessed in the
absence of thymic-independent pathways (Mackall et al., 1998).
However, in 1998 Douek et al. published a technique (described earlier) for detecting
recent thymic emigrants in peripheral blood (Douek et al., 1998). The development o f
the TREC assay subsequently enabled the study of thymic-dependent T-cell production
using a simple PCR-based technique. Since the publication o f the TREC assay, we and
others have utilised this technique to evaluate the contribution of the thymus to T-cell
reconstitution after HCT in a variety of settings. The following chapters present the results
of my study and discuss these results in the context of previous knowledge and other
reconstitution results published during the course of my work.
38

___________________________________________________________________________________________________________________________________________C h a p t e r 1
Aims of this thesis
The primary aim of this thesis is to analyse the reconstitution o f the T-cell compartment
in HCT recipients. Due to the diversity of applications o f HCT, I collected samples from
patients with a variety of diseases including patients with haematological malignancies,
bone marrow failure syndromes and immunodeficiency diseases. In addition, patients are
transplanted with several different stem cell sources; therefore samples were collected
from recipients o f bone marrow, peripheral blood and cord blood transplants.
The recovery o f a diverse T-cell compartment after HCT is of crucial importance to the
transplant recipient for re-establishing immunity after transplant. Although a number o f
studies have previously analysed the kinetics o f T-cell recovery post-HCT, few have
carried out a thorough analysis of the recovery of the three main T-cell subsets i.e. naïve,
memory and effector T-cells. Therefore, the first aim of this thesis was to develop a
reliable flow cytometric method to identify naïve, memory and effector T-cells in
peripheral blood mononuclear cell samples and to analyse the kinetics of naïve, memory
and effector T-cell recovery in HCT recipients at various time points post-HCT.
The recovery of naive T-cells has been previously described to be crucial for the
restoration o f diversity in the T-cell compartment. Furthermore, previous studies
suggested that naïve T-cell recovery only took place after “thymic rebound” or
reactivation of the thymus post-HCT. However, these previous suggestions were made
after indirect measurements of thymic output such as naive T-cell recovery itself or
changes in thymus size (increases in thymus size taken as an indicator of increased thymic
output). Therefore, the second aim of this thesis was to utilise TREC measurements
(described earlier) to directly measure thymic output and to relate these measurements to
naïve T-cell recovery.
By combining aim one and aim two, it is possible to gain an overall picture o f T-cell
reconstitution post-HCT. Thymic-dependent pathways can be analysed using TREC
measurements and naïve T-cell recovery, while thymic-independent pathways can be
analysed by the identification and quantification of memory and effector T-cells.
Therefore, the third aim of this thesis was to analyse the contribution o f thymic-dependent
and thymic-independent pathways to the reconstitution of the T-cell compartment.
As mentioned previously, there are an enormous number of variables that can affect
transplant outcome such as stem cell source, T-cell depletion, graft-ver^w^-host disease,
recipient and donor age etc. It is probable that some of these variables will also influence
the recovery of the T-cell compartment. Therefore, the fourth aim of this thesis was to
39

__________________________________________________________________________________________________________________________________________ C h a p t e r 1
analyse (within the limitations of patient numbers) the factors that are important in
determining the kinetics and quality o f T-cell reconstitution post-HCT.
Throughout the course of this study, it became apparent that several factors were o f
crucial importance in terms of their effect on the kinetics and quality o f T-cell
reconstitution. The final aim of this thesis was therefore to consider alternatives to current
HCT protocols and ways in which effective T-cell reconstitution could be achieved as
rapidly as possible post-HCT.
40

C h a p t e r 2
C h a p t e r 2
Materials and Methods
P a t ie n t s
Patients were recruited for this study from a number of transplant centres in the UK and
abroad. These were: The Royal Free Hospital, London, UK; Great Ormond Street Hospital,
London, UK; Ealing Hospital, London, UK; Newcastle General Hospital, Newcastle, UK;
Institute Português de Oncologia, Lisbon, Portugal; University o f Pavia, Pavia, Italy.
Ethical approval for this study was granted by the Royal Free Hospital Ethical Practices
Subcommittee (see Appendix for the study proposal, consent form and patient
information sheet submitted to the Royal Free Hospital Ethical Practices Subcommittee).
For the longitudinal analysis of T-cell reconstitution, blood samples were collected from
recipients o f bone marrow, peripheral blood and cord blood stem cell transplants at 3, 6, 9
and 12 months post-transplant with additional follow up samples collected at 18 and 24
months post-transplant when available. A cross-sectional analysis of long-term immune
reconstitution in SCID patients who received a stem-cell transplant was also carried out.
For this study, one blood sample was collected from each patient at random time points
up to 17 years post-transplant. In addition, blood samples were received from patients o f
various ages with DiGeorge Syndrome. Again, only one blood sample was obtained from
these patients.
Clinical data for each patient relating to their pre-transplant status and post-transplant
outcome was collected. For the patients from the Royal Free Hospital, clinical data was
obtained directly from the Haematology Department patient database and patient notes.
For all other transplant centres, clinical data was kindly provided by the clinicians in
charge o f the patients. Clinical data from all patients was subsequently recorded in a
database created using Filemaker Pro software (Claris, UK).
41

C h a p t c r 2
Processing o f peripheral blood samples
Control blood and serum samples
Umbilical cord blood was collected from normal and caesarean full-term deliveries by
puncturing the umbilical vein. Peripheral blood was collected from healthy individuals o f
both sexes (ages 5-50 years) or in the form of buffy coat preparations from the North
London Blood Transfusion Centre (Edgware, U.K.). To prepare serum samples, cord or
peripheral blood was placed at 37°C for Ih. The blood clot obtained was then spun down
at 1800 rpm for 20 minutes and the serum removed from the upper layer. Human AB^
sera was obtained from the North London Blood Transfusion Centre.
Isolation o f peripheral blood mononuclear cells
Peripheral blood samples with a volume greater than 5ml were transferred to 20m l
Universal tubes containing 500 lU Heparin (CP Pharmaceuticals, Wrexham, UK).
Peripheral blood mononuclear cells (PBMCs) were separated from whole blood by
density gradient centrifugation as follows: 10ml of Lymphoprep (Nycomed Pharma AS,
Oslo, Norway) was added to a 20ml Universal tube. 10ml of whole blood was layered
carefully on top of the Lymphoprep allowing formation o f a defined interface between
the blood and Lymphoprep. The samples were spun at 2200 rpm for 15 min in a Heraeus
2.0 centrifuge (Heraeus, Brentwood, UK) with no braking to allow formation of the buffy
coat layer. Using a plastic pasteur pipette, the buffy coat layer containing PBMCs was
removed from the Lymphoprep-plasma interface and transferred to a 15ml Falcon tube.
To 6ml of buffy coat, 9ml of RPMI 1640 (Biowhittaker, Wokingham, UK) was added and
samples were centrifuged at 1,800 rpm for 10 min. The supernatant was then decanted,
the cell pellet resuspended in a further 15ml RPMI 1640 and the sample spun at 1,600
rpm for 5 min. The cell pellet was then resuspended in 10ml o f RPMI 1640 and cells
counted using a haemocytometer with Trypan Blue exclusion of dead cells. Following the
isolation and counting of PBMCs, cells were either separated into CD4 and CD8 subsets
immediately or cryopreserved in liquid nitrogen until further use.
Cryopreservation o f PBMCs
PBMCs were isolated as described previously. The cells were spun at 1600 rpm for 5 min
and the cell pellet resuspended at a concentration of 5-10x10^ cells/ml in freeze mix. The
cell suspension was then transferred to freezing vials (Marathon Laboratory Supplies,
London, UK) in 1ml aliquots. The freezing vials were placed inside polystyrene boxes
42

_______________ C h a p t e r 2
that were stored at -70°C for a minimum of 24 hours then transferred to liquid nitrogen
until further use.
Prior to use, the cells were thawed rapidly, but not completely, in a 37°C water bath. The
cell suspension was immediately diluted in 10ml of RPMI 1640 for the final stage o f
thawing, centrifuged at 1600 rpm for 5 min and the cell pellet resuspended for use in
further experiments.
Positive selection o f CD4 and CDS subsets from PBMCs
Isolation of CD4 and CDS T-cells was carried out using MACS CD4 or CDS MicroBeads
and positive selection MSVRS" columns with a maximum capacity o f 1x10^ labelled cells,
(Miltenyi Biotec, Bisley, UK). From previous reports on the kinetics of CD4" and CDS" T-
cell recovery after stem cell transplantation, it is well documented that CDS" T-cells
recover more rapidly than CD4" T-cells (Atkinson et al., 19S2; Forman et at., 19S2;
Janossy et at., 19S6). Therefore, the isolation of CD4 cells was always carried out first with
CDS cell isolation being carried out subsequently from the same PBMC sample. After
isolation and counting of the PBMC preparation, a maximum of Ix lO ’ cells were spun in
a 15ml Falcon at 1,600 rpm for 5 min. The supernatant was removed and cells spun
briefly (less than 10 sec) to bring any residual RPMI 1640 to the bottom of the 15 ml
Falcon. The remaining media was carefully removed using a 200pl Gilson pipette
(Anachem Ltd, Luton, UK) and the cell pellet resuspended in SO|ll o f MACS buffer. 20 |il
of MACS CD4 MicroBeads were added, the suspension mixed well by pipetting and
samples incubated for 15 min at 6-12°C. Following this, cells were washed in 1ml o f
MACS buffer and spun at 1,600 rpm for 5 min. During centrifugation o f the cell
suspension the MS"/RS" column was placed in a magnetic separator and washed with 500|il
o f MACS buffer. After centrifugation, the supernatant was completely removed, cells were
resuspended in 500pl of MACS buffer and the cell suspension applied to the MS"/RS"
column. The cell suspension was allowed to run through the column (allowing negative
cells to pass through) and the column was washed 3 times with 500p,l of MACS buffer,
allowing the full volume of each wash to pass through before adding another 500p.l o f
MACS buffer. The column was then removed from the magnetic separator and placed in
a 5ml FACS tube (Becton Dickinson, Oxford, UK). 1ml o f MACS buffer was applied to
the column and the CD4" cells flushed out o f the column using the plunger supplied. The
flow through fraction (CD4 ) from the column (which was collected in a 15ml Falcon) was
subsequently spun at 1,600 rpm for 5 min. The supernatant was carefully and com pletely
removed and the same procedure carried out for the isolation of CDS" cells. The purity o f
the CD4" and CDS" populations (assessed by flow cytometry) obtained using this
technique are shown in Figure 2.1, with the purity of the cell populations being routinely
greater than 90% for CD4" T-cells and greater than 80% for CDS" T-cells.________________
43

C H A F f l î R 2
B> CD4
> CD4
> CD14
> CD14
■> CD 56
> C D 56
Figure 2.1: Purity o f CD4^ and CD8^ populations after positive selection
P osi t ive se lec t ion o f C D 4 (A) and CD 8 (B) p o pu la t ions was carried out and sam ples were s ta ined u s in g
f luo rescen t labelled an t ibod ies against the C D 3 , C D 4 , C D 8, C D 14, C D 5 6 , and C D 19 an t ig e n s then a n a ly s e d
us ing flow cy to m etry . Each plot represen ts an ungated cell p opu la t ion with the p e rcen tage o f each s u b s e t
show n in each quadrant .
Preparation o f cell lysates
Polymerase chain reaction (PCR) amplification of TREC molecules was carried out
directly from a cell lysate rather than carrying out a small scale DNA extraction, enabling
detection of TREC molecules from as few as 2,500 cells per PCR reaction (data not
shown). Cell lysates were prepared from sorted CD4 and CDS cells or PBMCs (when cell
yield from the patient blood sample was insufficient to carry out CD4 and CDS positive
selection). The cells were counted and transferred (minimum of 1x1 O'*, maximum of
2x10^ cells) to a screw-top conical 1.5ml microfuge tube (Sarstedt, Leicester, UK).
Samples were spun at 13,000 rpm for 1 min in a Heraeus Sepatech Biofuge 15 (Heraeus).
Following this, the supernatant was aspirated by vacuum suction and the cell pellet was
either lysed immediately or frozen at -70°C until further use. For every 1x10“ cells in the
cell pellet, lOpl of 1 OOpg/ml proteinase K solution (Boehringer Ingelheim, Ingelheim,
Germany) was layered carefully on top of the cell pellet taking care not to touch the cell
pellet with the pipette tip. For a cell number of less than or equal to 1x10^ cells, a
minimum of 20pl of proteinase K solution was added per tube. The sample was then
vortexed to detach the cell pellet from the bottom of the tube and the sample flicked so
44

__________________________________________________________________________________________________________________________________________ C h a p t e r 2
that the pellet and the proteinase K solution were together at the bottom of the tube. The
samples were then incubated for 1 hour at 56°C in a waterbath, vortexed, spun down
briefly (less than 10 sec) in a Heraeus Sepatech Biofuge 15 and incubated for 15 min at
95°C to inactivate proteinase K. Following this, samples were vortexed then spun at 13,000
rpm for 1 min in a Heraeus Sepatech Biofuge 15. Finally, 5|li1 of cell lysate (equivalent to
a quarter o f the starting cell number in the cell pellet) was added to each PCR reaction.
DNA extraction from whole blood
Peripheral blood samples o f less than 5 ml volume were collected into EOT A vacuum
tubes then frozen at -20°C until further use. Numerous blood samples were received from
paediatric patients less than 5 years of age. Invariably, the volume of blood obtained from
these patients was less than 5ml and very often only l-2m l. Therefore, I did not attempt to
isolate PBMCs or CD4 and CDS cells, but instead carried out TREC analysis on DNA
extracted from whole blood. DNA was extracted using the “salting out” procedure
(Miller et al., 1988). Whole blood samples of less than 5ml were frozen in l-2m l aliquots
at -20°C. At the time of DNA extraction, one aliquot o f blood was thawed rapidly and
transferred to a 15ml Falcon tube. Red cell lysis was carried out as follows: 14ml o f red
cell lysis buffer was added, the tube shaken vigorously then incubated at room
temperature for 10 min. Samples were subsequently spun at 3,500 rpm for 10 min and
the supernatant decanted. 15ml o f red cell lysis buffer was added and the incubation and
centrifugation repeated as previously. The red cell lysis step was repeated 3 times. The
supernatant was decanted after the third wash and 240|il of dHjO and 80pl of proteinase
K stock buffer were added and the white blood cell pellet broken up by mixing with a
1000|il Gilson pipette. 30pl of lOmg/ml proteinase K and 20pl o f 10% SDS were added
and the sample incubated at 55°C overnight. The sample was then transferred to a 1.5ml
eppendorf tube (Elkay, Basingstoke, UK), lOOpl of 5M NaCl was added and the tube
shaken vigorously for 15 sec. The sample was spun at 13,000 rpm for 5 min in a Heraeus
Sepatech Biofuge 15. The supernatant was carefully removed and transferred to a fresh
eppendorf tube containing 1ml of absolute ethanol at -20°C. The tube was capped and
inverted 10-15 times, or until strands of DNA became visible. The sample was incubated
at -20°C for 1 hour then spun at 13,000 rpm for 20 min in a Heraeus Sepatech B iofuge
15, following which the supernatant was decanted and the DNA pellet allowed to air dry.
When the pellet was dry 100|li1 of TE buffer was added and the sample placed on a rotary
mixer for a minimum of 24 hours to resuspend the DNA pellet. The isolated DNA was
subsequently quantified using spectrophotometry.
45

C h a p t e r 2
DNA quantification by spectrophotometry
Since the purified DNA was to be used subsequently to determine TREC frequency in a
quantitative PCR reaction, accurate measurement of DNA concentration was essential and
was carried out using spectrophotometry (Shimadzu UV-1201 Spectrophotometer, Milton
Keynes, UK). 4pl of DNA was diluted in 196|il o f dH20 and the solution mixed well and
transferred to a 200 |il quartz cuvette. The cuvette was placed in the spectrophotometer
(which was previously blanked using 200pl o f dHjO) and DNA concentration measured.
The spectrophotometer measured optical density at a wavelength o f 260nm (A l) to
determine the quantity of DNA and at 280nm (A2) to assess protein contamination. The
ratio o f A1:A2 indicates the purity of the DNA sample with a ratio o f 1.6-1.8 indicating a
DNA sample o f sufficient purity to be used in PCR amplification. To ensure accuracy in
the quantification of DNA concentration, each measurement was carried out in triplicate, a
mean value obtained, and final DNA concentration calculated as nanograms per microlitre
(ng/pl).
Flow cytometric analysis o f lymphocyte subsets
M easurem ent o f absolute lymphocyte and T~cell numbers in w h o le
b lo o d
Absolute lymphocyte and T-cell counts were measured using TriTEST™ reagents and
TRUCOUNT™ tubes (Becton Dickinson, Oxford, UK). We used TRUCOUNT technology
to evaluate absolute numbers o f lymphocytes (CD45^), T-cells (CD3"), helper T-cells
(CD3^CD40 and suppressor/cytotoxic T-cells (CD3"^CD8" ). The TriTEST reagents
consisted o f three antibodies, which were each tagged with a different fluorescent label.
To enable identification of CD4^ T-cells, the TriTEST reagent contained CD3-FITC, CD4-
PE and CD45-PerCP labelled antibodies. To enable identification of CD8" T-cells, the
TriTEST reagent contained CD3-FITC, CD8-PE and CD45-PerCP labelled antibodies. For
each patient sample two TRUCOUNT tubes were used, one for evaluation o f CD4 T-cell
numbers and the other for evaluation of CD8 T-cell numbers. Each TRUCOUNT tube
contained a pellet of latex beads of known quantity. The integrity o f the pellet was
checked and 20\x\ of TriTEST reagent (either CD4 TriTEST or CD8 TriTEST) added to
the bottom o f each tube taking care not to touch the bead pellet with the pipette tip. 50pl
o f anticoagulated whole blood was added to the bottom of the tube by reverse pipetting
using a 2 0 0 |il Gilson pipette. The addition o f a precise volume of 50 |il o f whole blood
was essential, therefore pipettes were calibrated on a regular basis and reverse pipetting
46

________________________________________________________________________________________________________________________________________C h a p t e r 2
used as an alternative to conventional pipetting. Samples were vortexed and incubated for
15 min in the dark at room temperature (20-25°C). 45O|0.1 of IX FACS lysing solution
was added to each tube and samples vortexed gently and incubated for 15 min in the dark
at room temperature (20-25°C). Samples were acquired immediately using a FACScan™
with MultiSET™ software (Becton Dickinson) or stored at 4°C for a maximum of 48
hours until acquisition. CaliBRITE™ beads and FACSComp™ software (Becton
Dickinson) were used prior to acquisition of samples for setting PMT voltages,
fluorescence compensation and checking instrument sensitivity prior to use. Absolute
lymphocyte and T-cell counts were calculated automatically by the MultiSET software by
comparing the number of cellular events to the number o f bead events acquired.
Flow cytometric analysis of T~cell subsets in PBM C popu la t ion s
Previous studies have reported distortions, often for extended periods o f time, in the
lymphocyte and T-cell compartments in recipients o f haematopoietic cell transplants.
Therefore, the recovery of naïve, memory and effector T-cells in patient blood samples
after haematopoietic cell transplantation was assessed. Staining o f PBMC populations for
flow cytometric analysis was always carried out in 96 well round-bottomed plates (Becton
Dickinson). PBMCs were isolated from whole blood as described previously. The cells
were resuspended at a concentration o f IxlOVml in RPMI 1640 and 200|il o f the cell
suspension used for each staining. Plates were spun at 1600 rpm for 5 min at 4°C in a
Heraeus Megafuge 2.0R centrifuge and the supernatant was removed by inverting and
flicking the plate. Cells were washed twice by adding 200 |il of chilled staining buffer and
the plates were spun at 1600 rpm for 5 min at 4°C. Antibody stainings were carried out in
a final volume of 50pl o f staining buffer containing pre-determined optimal dilutions o f
antibodies shown in Table 2.1.
To enable the maximum amount o f data to be extracted from the minimum number o f
PBMCs, samples were triple stained with the antibody combinations shown in Table 2.2.
Using these antibody combinations, lymphocyte subsets were defined as T-cells (CD 30,
naïve CD4" T-cells (C D 45R 0 CD27"), memory CD4" T-cells (CD45R0+CD27+), effector
CD4" T-cells (C D 45R 0T D 27 ), naïve CDS" T-cells (CD45RO CD27"), memory CDS" T-
cells (CD45RO"CD27") and effector CDS" T-cells (CD45RA"CD27 or CD57"CD2S ). The
plates were incubated for 30 min at 4°C then spun at 1600 rpm for 5 min and the
supernatant removed. The cells were then washed twice as described previously. Following
the second wash the supernatant was discarded, the cells resuspended in 100|il of fixing
buffer then incubated for 20 min at 4°C. After fixation the cells were analysed using a
FACScan and CellQuest™ software or stored at 4°C (for a maximum of one week) until
data acquisition. Data obtained from the CellQuest software was expressed as percentages.
47

___________ C h a p t e r 2
Absolute numbers o f naïve, memory and effector T-cells were calculated by com bining
the data from the CellQuest analysis with the TRUCOUNT analysis. Frozen cell samples
from the cord blood transplant recipients were also received. The results from these
patients are expressed in percentages.
Table 2.1: Optimal antibody dilutions fo r staining PBMC populations
A n t i b o d y M a n u f a c t u r e r Label" F in a l d i lu t io n * *
C D 3 BD* P erC P 1 : 1 0
C D 4 BD PerC P 1 : 1 0
CD S BD P erC P 1 : 1 0
C D 4 BD FITC 1 :2 5
C D 4 5 R O S ero tec FTTC 1 : 1 0
C D 5 7 BD FITC 1 : 1 0 0
CD S BD PE 1 : 1 0 0
C D 2 7 BD PE 1 :2 5
C D 2 S BD PE 1 :2 5
C D 4 5 R A S ero tec PE 1 : 1 0
* B D = B e c to n D ick inson (O xfo rd , UK)
# F IT C = f lu o re sc e in i so th io cy an a te , P E = ph y co e ry th r in , P e rC P = per id in in ch lo ro p h y l l p ro te in
** P B M C sa m p le s w e re s ta ined in a f inal vo lu m e o f 50p l
Table 2.2: Antibody combinations enabling identification o f naïve, memory and effector
T-cell subsets by flow cytometry
A n t ib o d y c o m b in a t io n H T C PE P e rC P
1 N il N il N i l
2 C D 4 C D S C D 3
3 C D 4 5 R O C D 4 5 R A C D 4
4 C D 4 5 R O C D 4 5 R A C D S
5 C D 5 7 C D 2 S C D S
6 C D 4 5 R O C D 2 7 C D 4
7 C D 4 5 R O C D 2 7 C D S
48

C h a p t e r 2
A ddition a l antibodies
The anti-CD3 antibody used to stimulate T-cells (0K T 3) was purified by Ms Isabel Perez
Cruz (at the Anthony Nolan Research Institute) from tissue culture supernatant from the
0K T3 hybridoma (ATCC, Maryland, USA).
Anti-CD3-FITC was obtained from Serotec (Oxford, UK) and anti-CD25-PE was obtained
from Harlan Sera-Lab Ltd (Loughborough, UK).
Anti-MCSF antibody (for MCSF neutralisation) and the isotype matched control antibody
(both Mouse IgG2a) were obtained from R&D Systems (Abingdon, UK).
Detection and quantification o f T-cell r e c e p to r
rearrangement excision circles by radiolabelled q u a n t i ta t iv e ,
competitive PCR
Detection o f signal jo in t TREC in healthy control blood samples
For the detection of signal joint TRECs from control blood samples, it was necessary to
use incorporation of radiolabelled nucleotide. I had previously attempted to detect TREC
using conventional PCR, agarose gel electrophoresis and ethidium bromide staining.
However, it became clear that the level of sensitivity of this method was insufficient. I was
subsequently advised by Dr Daniel Douek to use radiolabelled PCR with the incorporation
o f ^^P-labelled dCTP and polyacrylamide gel electrophoresis as an alternative method o f
detection. The detection o f TREC molecules was optimised using cell lysates or DNA
extracted from cells from cord blood and healthy controls varying in age from 18-48
years old. TREC specific fragments were amplified by PCR (see Figure 2.2 for primer
positioning and sequences). To each PCR reaction was added 5|il o f cell lysate (2 ,500-
50,000 cells) or 5 |ll DNA (0.2-l|Xg), lU Platinum Taq (GibcoBRL, Paisley, UK), 2mM
MgClz, 0.25mM dNTPs, lOpM each primer (MWG-Biotech, Milton Keynes, UK) and
l.Tnmol (5|iCi) ^^P-labelled dCTP (NEN Life Science Products, Brussels, Belgium) which
was made up to a final volume of 50pl in Platinum Taq buffer. The samples were m ixed
well, mineral oil was layered on top of the reactions to prevent evaporation and the
reactions placed in a thermal cycler (Hybaid, Ashford, UK). PCR conditions were: 95°C
for 5 min, followed by 90°C, 60°C, and 72°C, each for 30 sec, for 32 cycles. A negative
control in which dHjO was added instead o f DNA, and DNA extracted from an EBV-
49

______________ C h a p t e r 2
transformed B-cell line were run at the same time to control for contamination and
specificity of the primers respectively.
Polyacrylam ide gel electrophoresis
Following amplification, PCR products were resolved using 6% polyacrylamide gels and a
Hoefer SE-600 gel apparatus (Amersham Pharmacia Biotech, Chalfont, UK). Two glass
plates (Amersham Pharmacia Biotech) were cleaned with detergent, rinsed thoroughly
using dHjO then washed a second time using 70% ethanol. After drying, one of the plates
was placed on a flat surface and 1.0mm spacers aligned along the side of the plate. The
second plate was placed on top of the spacers and the bottom edges aligned. Clamps were
slid onto the gel plate assembly one side at a time, making sure they fitted tightly to avoid
leakage o f the gel. Petroleum jelly was smeared along the bottom edge o f the plates to
prevent leakage o f the gel solution and the plates were placed upright in a Hoefer pouring
tray. The plates were secured in place and the 6% gel solution poured between the plates
using a 50ml syringe, taking care to avoid formation of bubbles. After pouring, a 15 well
1.0mm comb was inserted between the plates and the gel was allowed to polymerise for a
minimum of 30 min. After the gel was polymerised the comb was removed and the gel
plates were attached to the upper buffer chamber of the gel apparatus. There were two gel
slots in the upper buffer chamber, therefore two 15 well gels were run simultaneously or
the second gel slot was closed using a perspex block. The lower buffer chamber was filled
with 1.5L of IX TBE and the upper buffer chamber placed in the Hoefer gel apparatus.
Following this, the upper buffer chamber was filled with 500ml o f IX TBE, the wells
flushed out using a 50ml syringe and 15pl of each PCR reaction added per well. Lanes 1
and 15 were not used as these wells ran slower than the rest o f the gel resulting in
distortion of the bands. All gels were run at a constant voltage o f 220V for 150min.
Following electrophoresis, the gel apparatus was dismantled. The TBE was emptied out o f
the upper buffer chamber and the clamps removed from the sides of the glass plates. A
plastic wedge was inserted into one comer o f the glass sandwich and the plates gently
separated. A sheet of Whatman 3MM filter paper (Whatman, Maidstone, UK) was lowered
onto the gel and gently pressed down to ensure proper detachment of the gel from the
glass plate. The gel was then covered in a layer of Saran wrap (Fisher Scientific,
Loughborough, UK) and the gel was dried onto the Whatman filter paper under vacuum
using a slab gel drier (Bio-Rad) at 80°C for 2 hours. The dried gel was exposed to x-ray
film (Genetic Research Instmmentation, Braintree, UK) for 15-60min and the x-ray film
developed using an X-Omat automatic film developer.
50

C h a p t e r 2
Preparation o f internal TREC standard fo r radiolabelled QC-PCR
The quantification of signal joint TREC molecules by quantitative-competitive PCR was
enabled by the addition o f a known quantity of modified TREC molecules to each PCR
reaction, termed the TREC standard. The TREC standard construct was prepared and
provided by Dr Daniel Douek using TREC fragments that had been amplified from cord
blood PBMCs. The TREC fragments were genetically modified by Douek et al. so that the
TREC standard was 60bp shorter than the normal TREC amplicon. This enabled the
TREC and TREC standard fragments to be resolved on a 6% polyacrylamide gel and thus
enabled a comparison of density of the TREC band to the density of the TREC standard
band. The modified TREC fragment was subsequently cloned into the pGEM®-T Easy
vector (Promega) via the 3 ’-thymidine overhangs (for plasmid map see Appendix, Figure
A l) .
Transformation o f the TREC standard plasm id
Upon receipt of the TREC standard, it was essential to grow up a sufficient quantity o f the
plasmid to be able to prepare a set of standards. A 100)il aliquot of competent XL-1 blue
cells (prepared by Dr Louise McGreavey at the Anthony Nolan Research Institute) was
used for transformation of the TREC standard plasmid. l |ig o f plasmid was added to
lOOpl of competent XL-1 blue cells and incubated for 30 min on ice. The cells were then
heat-shocked by incubation in a 42°C water bath for 2 min and the cells incubated for a
further 1-5 min on ice. 1ml of LB was added to the transformation mix. The cells were
then incubated at 37°C for 20-30 minutes and 20pl o f the cell suspension was plated out
on nutrient agar plates containing 50mg/ml Ampicillin (Sigma-Aldrich, Poole, UK). The
plates were then incubated overnight at 37°C.
M iniprep DNA extraction
Individual colonies were selected from the agar plates the following day and transferred to
a 3ml culture of LB-Ampicillin and incubated overnight with shaking at 37°C. The TREC
standard plasmid was subsequently extracted from the bacteria using a GFX™ Micro
Plasmid Prep Kit (Amersham Pharmacia Biotech). 1ml of the overnight culture was added
to a 1.5ml microcentifuge tube (Elkay) and the samples centrifuged at 13,000 rpm for 30
sec to pellet the cells. The supernatant was removed by aspiration and the cell pellet
resuspended in 150p.l o f Solution I with vigorous vortexing. I50p.l o f Solution II was
added and the samples mixed by inverting the tube 10-15 times. 300|il of Solution III was
51

___________________________________________________________________________________________________________________________________________ C h a p t e r 2
added and the sample mixed by inverting the tube until there was formation of a
precipitate. The sample was then centrifuged at 13,000 rpm for 5 min to pellet the cell
debris. During centrifugation, one GFX column per sample was placed in a collection
tube. The supernatant was removed and transferred to a GFX column, the sample
incubated for 1 min at room temperature then centrifuged at 13,000 rpm for 30 sec. The
flow through fraction from the column was discarded and 400 |il of Wash Buffer added.
The sample was then centrifuged at 13,000 rpm for 1 min to remove all Wash Buffer and
dry the column matrix prior to elution. The GFX column was then transferred to a fresh
microcentrifuge tube and 100|il of TE buffer added directly to the top o f the glass fibre
matrix in the GFX column. The sample was incubated at room temperature for 1 min then
centrifuged at 13,000 rpm for 1 min to recover the purified DNA.
Restriction digestion o f miniprep DNA
5|ll o f miniprep DNA and Ipg o f the original TREC standard plasmid (as a positive
control) were digested with 10 units of EcoRI in high salt buffer (Boehringer Ingelheim),
in a final volume of 20|il. The digestion was carried out for 1 hour at 37°C and the
digested products were subsequently run on an agarose gel.
Agarose ge l electrophoresis
PCR products and restriction digests were routinely separated by electrophoresis using
agarose gels. All agarose gels were 1.5% (w/v) and were prepared by dissolving 1.5g o f
electrophoresis grade agarose (GibcoBRL) in 100 ml of IX TBE, which was achieved by
boiling the agarose and TBE in a conical flask in a microwave oven. The agarose solution
was allowed to cool sufficiently and 7|li1 of lOmg/ml ethidium bromide was added taking
care to prevent excessive release o f ethidium bromide vapours. The cooled agarose was
poured into a casting tray containing one or more 14 well combs and the gel allowed to
set. The gel was then placed in a gel tank containing 900ml IX TBE. The digested DNA
samples and molecular size markers (1 Kb and lOObp ladders; Roche Diagnostics, Lewes,
UK) were loaded onto the gel in a solution o f loading buffer (12|li1 DNA + 3 pi 5X
loading buffer) and the gel was run for 50 min at 120V using a Bio-Rad PowerPac 300
(Bio-Rad, Hemel Hempstead, UK). The DNA was then visualised on a U.V.
transilluminator (GelDoc 1000, Bio-Rad) and a photograph taken.
52

C h a p t e r 2
Maxiprep o f TREC standard plasmid
To grow up larger quantities o f the TREC standard plasmid, a medium scale plasmid
preparation was carried out. 1ml of the original miniprep culture (if the plasmid was
confirmed by restriction digestion to be correct) was inoculated into 500ml LB containing
50mg/ml Ampicillin and cultures incubated overnight at 37°C with shaking. The
following day, the plasmid DNA was extracted using a Qiagen Maxiprep Kit (Qiagen,
Crawley, UK). The bacterial cells were harvested by centrifugation at 6,000 rpm in a
Jouan KR22 centrifuge (Jouan, Derby, UK) for 15 min at 4°C. The supernatant was
carefully removed and the pellet resuspended in 10ml o f buffer PI. The cells were lysed
by addition o f 10 ml of buffer P2 and allowed to stand at room temperature for 5 min.
10ml of chilled neutralisation buffer P3 was added to the lysate, mixed gently by
inversion then incubated on ice for 20 min. The sample was then centrifuged at 14,000
rpm in a Jouan KR22 centrifuge. A Qiagen-tip 500 was equilibrated with 10ml o f buffer
QBT before the addition o f the cell lysate. The supernatant was removed and allowed to
enter the Qiagen-tip 500 by gravity flow. The tip was then washed twice with 30ml o f
buffer QC. The DNA was eluted by the addition o f 15ml buffer QF and collected in a
50ml Oakridge centrifuge tube (Nalgene, Hereford, UK). The DNA was precipitated by
the addition of 10.5ml of Isopropanol and the solution centrifuged at 11,000 rpm at 4°C
for 30 minutes in a Jouan KR22 centrifuge. The supernatant was removed and the pellet
washed with 70% ethanol then centrifuged at 11,000 rpm at 4°C for 15 min. The
supernatant was removed and the pellet air-dried. The pellet was then redissolved in 500 |il
of sterile dHjO. The plasmid was checked by restriction digestion as described previously
and additional confirmation was provided by PCR amplification of the modified TREC
molecules using the QC-PCR oligonucleotides shown in Figure 2.2.
Dilution o f TREC standards
The original publication (Douek et al., 1998) that demonstrated that TREC could be used
measure thymic output in normal and HIV-infected individuals used the same TREC
standard construct described previously. The quantification o f TREC was enabled by
addition o f 10% 10 or 10 molecules of TREC standard plasmid to each PCR reaction.
Correspondence with the authors confirmed that these dilutions were within the linear
range of the assay, therefore the same series of dilutions were used in subsequent
experiments. The main consideration in setting up the TREC assay was to minimise
pipetting errors and to keep the assay as consistent as possible. Therefore, 5pi o f TREC
standard (with a concentration o f 10% 10 and 10 molecules per 5pi) was added to each
PCR reaction to avoid inaccuracy. The TREC standard plasmid was first quantified by
53

___________________________________________________________________________________________________________________________________________ C h a p t e r 2
spectrophotometry and the result expressed as ng/jil. One molecule o f TREC standard
plasmid has a molecular weight o f 3 .59x10 ‘*g. Therefore, the number of molecules o f
TREC standard plasmid was calculated per |il of plasmid solution. The TREC standards
were diluted in dH^O to gain a solution with a calculated concentration o f 1x10* TREC
standard molecules per 5|li1. Following this, a series of 10 fold dilutions was set up to gain
a set of TREC standards with a calculated concentration of 1 0 \ 10* and 10 molecules per
5p-l. Each series was checked against aliquots o f standards sent by Dr Daniel Douek and if
the series was correct, the standards were frozen in 50|Ltl aliquots at -20°C. In addition,
when a correct series o f standards was obtained, an aliquot was sent to Dr Daniel D ou ek ’s
laboratory for confirmation.
R a d io labe lled quan tita tive-com petitive PCR
Each PCR reaction contained a DNA or cell sample with an unknown TREC quantity. For
each DNA or cell sample, three PCR reactions were set up containing either 1 0 \ 10* or 10
TREC standard molecules. Therefore, each PCR reaction contained 5|xl o f DNA or cell
lysate, 5p.l TREC standard (at a concentration o f 10 \ 10* or 10 molecules per 5|ll), lU
Platinum Taq (GibcoBRL), 2mM MgCl2, 0.25mM dNTPs, lOpM each primer (MWG-
Biotech) and l.Vnmol (5pCi) **P-labelled dCTP (NEN) which was made up to a final
volume of 50|il in Platinum Taq buffer. The samples were mixed well, mineral oil was
layered on top of the reactions to prevent evaporation and the reactions placed in a
thermal cycler (Hybaid). PCR conditions were: 95°C for 5 min, followed by 90°C, 60°C,
and 72°C, each for 30 sec, for 32 cycles. Following PCR amplification, samples were run
out on 6% polyacrylamide gels to separate the TREC and the TREC standard bands
(which differ by 60bp in size) as described previously.
54

C h a p t e r 2
Calculation of TREC frequency by densitometry
Following exposure of the x-ray film, autorads were scanned and visualised using Bio-Rad
GS-7Ü0 densitometry software (Bio-Rad). The intensities o f the TREC and the TREC
standard bands were measured by the densitometry software and the ratio of TREC:TREC
standard was compared. All densitometry measurements were carried out in triplicate and
the mean value for each band was calculated. TREC frequencies in each cell or DNA
sample were subsequently calculated using the following equation:
Sample TREC density ^ rTREC standard density x 1.1 Standard concentration ( I 0 \ iU' or 1(E) = T R E C Frequency
Because ^^P-labelled dCTP is incorporated in the reaction and there are fewer GC
nucleotides in the TREC standard amplicon, the intensity of the standard band is
multiplied by a correction factor of 1.156.
A A G G C T C T G T C T A G T G T G A T A A C A T T T T G T T A T C T T A T T C A T T G T C T T C A T C C C T G A A A T A C A C T C T G C T C T C T C
# >■C T A T C T C T G C T C T G A A A G G C A G A A A G A G G G C A G C C C T C T C C A A G G C A A A A T G G G G C T C C T G T G G G G A A C A G A G
r.r.r.Tr.rC T C TG T C A AC A A AGGTG ATGd 8 S H R S S B 8 B B I^ W B II ff lB E lC|ACACCTCTGGTTTrTGTAAAGGTOd'
<-rcA cW r CTCTf:/rACCCTGATGCATAGGCACCTGCACCCCGT(I# * R .™ # [« [M [#I«™#IIMI«aACGGGCCCTGT
C T G C T C T T C A T T C A C C G T T C T C A C G A G T T G C A A T A A G T T C A G C C C T C C A T G T C A C A C T G T G T T T T C C A T C C T G G G
G A G T G T T T C A C A G C T A T C C C A A G C C C C A C G C T G A C G A A T C A C G G C C G A A A A C A C A C T C T G A T G C C A G C A C A G A
-< #C C A C G G A G C A A A T G T C A G A C A A G A T C A G C C T C G G A A A A G T G A G T C C T G A T G C G A T G G A A G T G G G C T T C C T C T C
A C A A G G A C T T T G T G T G G A G A T G C G C A G G T G G G C T G T T G G A A
Figure 2.2: Sequence o f the signal joint region in each TREC
T h e s igna l jo in t reg ion was sequenced by Dr D aniel D o u e k ’s labo ra to ry and was later co n f i rm ed in our
lab o ra to ry by M r S teve C ox . T he re c o m b in a t io n site is s h o w n in b o ld t e x t . A lso s h o w n are the p r im e r
se q u en ces and b ind ing si tes for the Q C -P C R assay ( forward and reverse p r im ers s h o w n in y e l lo w ) and for t h e
Taqman® assay ( forward and reverse p r im e rs s h o w n in blue) . T h e sequence and b in d in g site ot the Taqman®
probe is s h o w n in pink. T h e p r im er p o s i t io n s p roduce a 3 6 8 b p am p l ico n in the Q C -P C R assay and a 1 0 7 b p
am p l ico n in the Taqman® assay. T h e d irec t ion o f the b lack a r ro w s represen ts the d irec t ion o f e x te n s io n o f th e
P C R product .
TREC frequencies were subsequently expressed in three ways: (1) TREC per 100,000
cells; (2) Absolute TREC numbers per microlitre of blood {i.e. TREC per 100,000 cells as
a function of absolute T-cell numbers); or (3) TREC per pg DNA.
55

C h a p t e r 2
Detection and quantification o f TREC by Real-Time PCR
The detection and quantification of TREC molecules using radiolabelled QC-PCR was
time consuming, labour intensive and dependent on the use o f a radioisotope. I therefore
decided to optimise the detection and quantification of TREC molecules using real-time
quantitative PCR. Real-Time PCR was carried out using an ABI7700 sequence detection
system (Taqman®) and SDS software (Applied Biosystems, Foster City, CA). The
advantages o f real-time PCR over radiolabelled QC-PCR are that it is faster, less labour
intensive, more accurate and uses fluorescent dyes instead of radioisotopes.
To enable quantification of TREC molecules by real-time PCR it was essential to prepare a
different set o f standards from those used in the radiolabelled assay. 2 |ig o f the standard
construct (see Appendix, Figure A2) was provided by Dr Daniel Douek and the first step
was to grow up larger quantities of the plasmid.
Transformation o f the Taqman® TREC standard plasmid
The TREC standard used in the Taqman® assay was not genetically modified and was the
same size and sequence (confirmed by automated DNA sequencing, data not shown) as
the TREC fragments amplified from any peripheral blood T-cell. The TREC m olecule
was cloned into the pCR-Blunt plasmid (Invitrogen, NV Leek, The Netherlands) which
contained a Zeocin resistance gene (see Appendix, Figure A2). The activity of the
antibiotic Zeocin can be inhibited by high ionic strength, acidity or basicity. Therefore,
the transformation was carried out using low salt bacterial media and agar plates. Zeocin
was used at a final concentration of 25|ig/m l and the transformation was carried out as
described previously.
Miniprep, maxiprep and restriction digestion analysis o f th e
Taqman® TREC standard plasmid
The miniprep, maxiprep and restriction analysis of the Taqman® standard plasmid was
carried out as described previously. The only difference was that low salt SOC media
containing 25|lg/m l Zeocin was used in place of LB media containing Ampicillin.
56

_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ C H A F n : R 2
Optimisation o f the Taqman® standard curve
Unlike radiolabelled QC-PCR, the Taqman® assay does not rely on an internal competitor
molecule in each PCR reaction. Instead, quantification of TREC in any given blood
sample was enabled by the creation of a standard curve of TREC standard molecules with
known concentrations. The sensitivity of the Taqman® detection system is such that it is
possible to accurately quantify any target molecule over seven log orders of magnitude
(10’-1 0 ‘ molecules per reaction). A standard curve was therefore prepared using the
Taqman® TREC standards with a calculated concentration of 10', 10\ 10\ 10\ 10 and 10'
molecules per reaction. The dilution series was calculated in the same way as described
previously with the only difference being that one molecule of the Taqman® TREC
standard weighs 4.19x10 ‘Vg- The dilution series was prepared, amplified and compared
against a dilution series of 10% 10% 10% 10% 10’ and 1 O' molecules per reaction kindly
provided by Dr Daniel Douek (for a representative standard curve see Figure 2.3).
SiamdarW Curve - 1 9 .0 7 .0 1
Unknowns
50.00
45.00
40.00
35.00Standards30.00
25.00
20.00 S lope:15.00 ■ —
V -Intercept10.00 - -
C orrelation C oeff:5.00 ■
iWi T i' t h iiii I-5 .000* 7 0"8
-3 .499
40.522
0.985
10*2 10*3 10*4 10*5
Starting Quantity
10*6
Figure 2.3: Representative standard curve for detection o f TREC using Real-Time PCR A liquo ts o f s tandards with a co n c e n t ra t io n o f 10’-10* m olecu les were frozen at -20°C and used to d e te rm in e
T R E C quan t i ty in the cl in ica l sam ples described p rev iously . T he standard curve was g enera ted a u to m a t i c a l l y
by the A B I7 7 0 0 sof tw are and the quan t i ty o f s ta r t ing tem pla te in the u n k n o w n sa m p le s co m p ared w ith th e
s ta n d a rd values .
Real-Time Quantitative PCR
The PCR reactions were set up in 96-well optical reaction plates (Applied Biosystems); the
plates were sealed using MicroAmp® optical caps (Applied Biosystems) and transferred to
the ABI7700 Sequence Detector. The Taqman® PCR Reagent Kit was not used because
the PCR reactions consistently failed when using the AmpliTaq Gold enzyme. Therefore,
it was necessary to use Platinum Taq (GibcoBrl) and include a background reference dye
57

___________________________________________________________________________________________________________________________________________ C h a p t e r 2
(BD636, (Megabases, Chicago, USA)) in each reaction. This meant that the 7 7 0 0
Sequence Detector had to be recalibrated as detailed in the ABI Users Bulletin number 4
(http:www.appliedbiosystems.com).
Each PCR reaction contained 5pl of DNA, cell lysate or TREC standard, lU Platinum Taq
(GibcoBRL), 3.5mM MgClj, 0.25mM dNTPs, 12.5|iM each primer (Amersham Pharmacia
Biotech), 3.75pM fluorescent labelled probe (5 ’-FAM, 3 ’-TAMRA modifications;
Amersham Pharmacia Biotech), 2 .5 |il Platinum buffer (GibcoBRL) and 0 .25 |il BD 636
reference dye in a final volume of 25pl. Thermal cycler conditions were 95°C for 5 min,
followed by 95°C for 30sec, 60°C for Imin for 40 cycles. Each PCR to determine the
quantity of starting material in a standard or unknown sample was carried out in triplicate.
Quantification o f TREC using Real-Time Quantitative PCR
At the end of each run the AB17700 system’s set-up screen depicts a 96-well plate which
allows the user to enter the quantity of each standard into the corresponding on-screen
wells. The software then plots a standard curve o f Cj (the cycle number at which PCR
signal becomes detectable) versus the standard concentration. To calculate the quantity o f
TREC in an unknown sample, the 7700 software compares the Cj o f the unknown sample
to the standard curve and produces a value for TREC frequency. TREC frequencies were
again expressed in three ways: (1) TREC per 100,000 cells; (2) Absolute TREC numbers
per microlitre blood {i.e. TREC per 100,000 cells as a function o f absolute T-cell
numbers); or (3) TREC per pg DNA.
T-cell functional assays
Preparation o f T-cell lines
PBMCs were plated at a concentration of 1x10^ per ml in RPMI 1640 supplemented with
10 lU/ml Penicillin, lOpg/ml Streptomycin (ICN Biomedicals Inc, California, USA), 10%
normal AB^ human serum, 20ng/ml IL-2 (Hoffman-La Roche, Nutley, New Jersey, USA)
and 35ng/ml anti-CD3 monoclonal antibody for 7 days. Cells were then supplemented
with fresh medium and 20ng/ml IL-2 for another 7 days. At the end of this 14-day cycle
the cell population was restimulated with irradiated autologous PBMCs (500Gy/min, 7
min), anti-CD3 and IL-2 for 7 days then supplemented with fresh medium and 20ng/ml
IL-2 for another 7 days. The resulting T-cell lines were maintained on this 14-day cycle.
58

C h a p t e r 2
The lines were always used in assays on day 14 o f the cycle, when the purity of the T-cell
population was >90%.
M ixed lymphocyte reactions
1x10^ viable PBMCs/well were plated in RPMI plus 10 lU/ml Penicillin and lOpg/ml
Streptomycin in 96 well plates with 5 x 10" irradiated PBMC’s in the presence or absence
of varying concentrations of CB or adult sera. In some cases recombinant M-CSF (kindly
provided by Dr M. Wadhwa at the National Institute of Biological Standards and Control;
NIBSC, Herts, UK), anti-MSCF antibody (lOpg/ml) or an isotype matched control
antibody (lOpg/ml) was added to the cultures. The final volume was always 2 0 0 |il per
well. Cultures were maintained for 6 days with alloantigen at 37"C in 5% CO2 and pulsed
with 0.5 pCi/well o f methyl ^H-thymidine 18 hours before harvesting onto glass fibre
filters. Scintillation counting was performed using an LKB Betaplate counter (Becton
Dickinson, Palo Alto, CA, USA). All cultures were performed in triplicate.
Stimulation o f T-cell lines with anti-CD3 antibody or IL-2
2x10^ viable T-cells/well were plated in RPMI medium plus 10 lU/ml Penicillin and
lOfig/ml Streptomycin in 96 well plates. A predetermined optimal concentration o f anti-
CD3 antibody (determined by the antibody preparation used) was immobilised on some
plates prior to the addition of T-cells. Alternatively T-cell lines were stimulated with IL-2
at a final concentration o f lOng/ml. All T-cell stimulations were carried out in the
presence or absence o f varying concentrations o f cord blood or adult sera and the final
volume was always 200|il/well. Cultures were maintained for 3 days at 37°C in 5% CO2,
pulsed with 0.5 p.Ci/well o f methyl ^H-thymidine then harvested onto glass fibre filters 18
hours after pulsing. All cultures were performed in triplicate.
Analysis o f CD25 expression
1x10^ viable PBMCs/well were plated in RPMI 1640 plus 10 lU/ml Penicillin and lOpg/ml
Streptomycin in 96 well plates with either 5 x 10 irradiated PBMCs (500Gy/min, 7 min)
or an optimal concentration of phytohaemagglutinin (PHA; Abbott Laboratories,
Maidenhead, UK) with cord blood or adult sera. Again the final volume was always 200p.l.
Cultures were maintained at 37* C in 5% CO2. At the end of the incubation (various time
points from 1-168 hours) cells were stained with fluorescent labelled antibodies against
CD3 and CD25 and analysed by flow cytometry.
59

C h a p t e r 2
Analysis o f the frequency o f IL-2 producing T cells
1x10^ PBMCs per well were plated in RPMI in 1:10 plus 10 lU/ml Penicillin and lOpg/ml
Streptomycin in 96 well plates with an optimal concentration of (PHA) and either cord
blood or adult sera. Cultures were maintained at 37°C in 5% CO2 for 3 days. On day 3
post-stimulation with PHA, cells were spun down and restimulated in the presence o f
5ng/ml phorbol-12-myristate-13-acetate (PMA; Sigma-Aldrich, UK), IpM lonom ycin
(Calbiochem, Nottingham; UK) and 3 fxM Monensin (Calbiochem). After a 6 hour
incubation at 37°C in 5% CO2, the cells were taken out of the wells and stained
extracellularly for CD3 and intracellularly for IL-2.
Intracellu lar cytokine staining
Extracellular staining with fluorescent labelled anti-CD3 was carried out as described
previously. After extracellular staining, samples were incubated for 20 min at 4°C in
fixing buffer. Following this, cells were washed twice in chilled permeabilisation buffer.
After washing, cells were stained using either FITC-labelled anti-IL-2 or an isotype
control antibody (both IgG2a subtypes; BD Pharmingen, Oxford, UK). The cells were
incubated for 30 minutes at 4°C in the presence o f these antibodies then washed twice in
permeabilisation buffer and resuspended in fixing buffer after the second wash. Cells
were subsequently analysed using flow cytometry as described previously. The
frequency of T-cells expressing IL-2 was calculated as a percentage o f CD3^ cells.
Buffers and solutions
All individual components were purchased from Sigma-Aldrich or BDH Laboratory
Supplies (Poole, UK) unless otherwise stated. In addition, concentrations are shown as the
working IX solution unless otherwise stated.
Phosphate-buffered saline (PBS): purchased from Biowhittaker as a lOX solution
(17mM KH2PO4, 50mM Na2HP0 4 , 1.5M NaCl), diluted to a IX solution in sterile dH2 0 .
Trypan Blue: 1% Trypan in IX PBS.
Foetal Calf Serum (PCS): Biowhittaker
Freeze mix: 90% FCS and 10% Dimethyl Sulphoxide (DMSO).
60

C h a p t e r 2
MACS buffer: 0.5% bovine serum albumin (BSA) and 2mM EDTA in IX PBS.
Proteinase K solution: 14mg/ml diluted to 100|ig/ml proteinase K solution (Boehringer
Mannheim) in lOmM Tris-HCl buffer pH 8.0.
Red cell lysis buffer (RCLB): lOmM Tris pH 7.5, 5mM MgClj, lOmM NaCl.
Proteinase K stock buffer: lOmM Tris pH 7.5, lOmM EDTA pH 8.0, 50mM NaCl.
TE buffer: lOmM Tris-HCl pH 7.4, ImM EDTA pH 8.0.
FACS lysing solution: provided as a 1 OX concentrate containing 100ml o f a proprietary
buffered solution containing <15% Formaldehyde, <50% Diethylene Glycol; exact
composition not given in manufacturer’s protocol (Becton Dickinson). FACS lysing
solution was diluted to a IX working stock using sterile dHjO.
FACS staining buffer: 0.2% Sodium Azide, 2% FCS in IX PBS.
FACS fixing buffer: 3% Formaldehyde, 0.2% Sodium Azide, 2% FCS in IX PBS.
FACS permeabilisation buffer: 0.1% Saponin, 0.2% Sodium Azide, 2% FCS in IX PBS.
6% Polyacrylamide gels: 7.5ml 40% Acrylamide/Bis solution, 19:1 (Bio-Rad); 300 |il
10% Ammonium Persulphate (Amersham Pharmacia Biotech); 150|ll TEMED
(Amersham Pharmacia Biotech) and 37ml dHzO (sufficient for two gel solutions).
LB media: lOg bacto-tryptone (GibcoBrl), 5g bacto-yeast extract (GibcoBrl) and lOg
NaCl in IL dHjO, pH adjusted to 7.0 using 5M NaOH.
Nutrient agar: 200ml LB media, 3g agar (GibcoBrl).
Solution I: lOOmM Tris-HCl (pH 7.5), lOmM EDTA, 400|Lig/ml RNase I (Amersham
Pharmacia Biotech).
Solution II: 189mM NaOH, 1% (w/v) SDS (Amersham Pharmacia Biotech).
Solution III: buffered solution containing acetate and chaotrope, exact composition not
provided in manufacturer’s description (Amersham Pharmacia Biotech).
Wash Buffer: Tris-EDTA in 80% ethanol (Amersham Pharmacia Biotech).
61

C h a p t e r 2
TBE: lOX stock: 0.89M Tris, 0.89M boric acid, 20mM EDTA solution (Biowhittaker),
diluted 10 fold in dHjO to make a IX solution.
5X loading buffer: 0.25% w/v bromophenol blue, 0.25% w/v xylene cyanol, 15% vwV
Ficoll.
Buffer PI: 50mM Tris-HCl, pH 8.0; lOmM EDTA; lOOpg/ml RNase A (Qiagen).
Buffer P2: 200mM NaOH, 1% SDS (Qiagen).
Buffer P3: 3.0M potassium acetate, pH 5.5 (Qiagen).
Buffer QBT: 750mM NaCl; 50mM MOPS, pH 7.0; 15% Isopropanol; 0.15% Triton®X-
100 (Qiagen).
Buffer QC: l.OM NaCl; 50mM MOPS, pH 7.0; 15% Isopropanol (Qiagen).
Buffer QF: 1.25M NaCl; 50mM Tris-HCl, pH 8.5, 15% Isopropanol (Qiagen).
Low salt (SOC) media: lOg tryptone, 5g NaCl, 5g yeast extract made up to 1 litre and
adjusted to pH 7.5 using IM NaOH.
Low salt agar plates: 200ml of SOC media, 3g agar (GibcoBrl).
62

C h a p t e r 3
C h a p t e r 3
Thymic-dependent versus thymic- independent T-cell reconstitution post-HCT
Introduction
The recovery of peripheral T-cell numbers after an allogeneic HCT is essential to provide
the transplant recipient with an immune system capable of responding to any one o f the
environmental antigens that they might encounter. This is highlighted by studies
demonstrating that increased infectious morbidity in long term HCT recipients was
associated with low CD4" T-cell counts (Storek et a i , 1997). However, patients whose T-
cell counts recover rapidly also experience numerous opportunistic infections (Lum,
1987; Reusser et a i , 1990). These observations suggest that some long-term deficiency in
T-cell function remains. Early reports of T-cell reconstitution after HCT demonstrated
severe imbalances in T-cell subpopulations (Atkinson et al., 1982; de Cast et al., 1985;
Janossy et al., 1986), with a high number of T-cells expressing activation or memory
markers (Hansen et al., 1983; Leino et al., 1991; Storek et al., 1995). The reasons for
these imbalances and increased incidence of infections was elucidated more recently when
a number of studies demonstrated that two pathways are responsible for the regeneration
of T-cell numbers after ablation of the T-cell pool (Mackall et a i , 1995; Mackall et al.,
1993; Mackall and Gress, 1997; Rocha et al., 1989). The first of these is dependent on
maturation of T-cell precursors in the thymus followed by export to the peripheral T-cell
compartment and is termed the thymic-dependent pathway. Due to the random nature o f
T-cell receptor rearrangement events during thymic education this pathway generates a T-
cell compartment with a diverse receptor repertoire (Douek et al., 2000; Dumont-Girard
et al., 1998). The second pathway is reliant on the expansion of mature T-cells that have
been transferred with the stem cell graft and is termed the thymic-independent pathway.
T-cell reconstitution by thymic-independent pathways alone would be predicted to
regenerate a T-cell compartment with a limited receptor repertoire because the
repopulating cells are the progeny of a limited number of precursors (Mackall et al.,
1996).
63

C h a it t jr 3
However, a comprehensive study of thymic-dependent T-cell recovery, particularly in
non-T-cell depleted transplants, has been complicated by two main factors. First, by the
transfer of significant numbers of phenotypically naïve T-cells with the stem cell graft and
second, by the recognition that a more complex phenotypic definition of naïve T cells,
particularly o f naïve CD8* T-cells, was required (De Rosa et a l , 2001).
Nevertheless, a number of studies have analysed both pathways of T-cell regeneration
after HCT and suggested that in the absence of thymic activity, peripheral expansion
mechanisms may be able to restore normal T-cell numbers and that these repopulating T-
cells are graft-derived and of memory phenotype (Behringer et al., 1999; Lowdell et al.,
1998; Small et al., 1999; Storek et al., 2001). In other studies a role for thymic-
dependent reconstitution was implicated, as in the recovery of CD4^CD45RA^ T-cells
following highly T-cell depleted stem-cell transplants. Moreover, the appearance o f
CD4^CD45RA^ T-cells in these studies correlated with diversification o f the T-cell
repertoire (Dumont-Girard et al., 1998; Roux et al., 2000). Also consistent with a role for
thymic-dependent reconstitution, thymus size (as measured by radiographic imaging o f
the thymus) increased after HCT, a phenomenon that was age-dependent and correlated
with recovery of CD4'^CD45RA"’ T-cells (Mackall et al., 1995; Muller et al., 2000). These
studies concluded that thymic output alone in aged individuals may have been insufficient
to fully restore a normal, diverse T-cell compartment.
The aim of this chapter is to address the problems of previous analyses o f thymic-
dependent and thymic-independent pathways in T-cell reconstitution after HCT. The
objectives were to develop a phenotyping method which would reliably identify naïve
CD4^ and CD8" T-cells and also, to measure thymic output directly rather than indirect
measurements such as changes in thymus size or recovery o f CD4"’CD45RA^ T-cells
64

C h m t e r 3
R e su l t s
Recovery o f CD3^, CD4^ and CDS* T-cells post-HCT
A longitudinal analysis of T-cell reconstitution in 26 allogeneic HCT recipients was
carried out. For a detailed description of each patient’s clinical history see Tables 4.1 and
4.2 (Chapter 4). For the purposes of this chapter, patients will be analysed as a single
group, independently of the numerous factors that may influence T-cell reconstitution.
Analysis o f the individual factors affecting T-cell reconstitution is given in Chapter 4.
The first stage in the analysis of the contribution o f thymic-dependent and thymic-
independent pathways was to gain an overall picture of T-cell reconstitution in these
patients by measuring the absolute numbers of circulating T-cells. Total CDS'", CD4"" and
CD8" T-cell numbers were measured at 3, 6 ,9 , 12 and 18-24 months post-HCT (Figure
3.1).
The median number of CD3^ T-cells remained below the normal range for the first 6
months after HCT. The median CDS'" T-cell count was 431 cells per pi (range; 2 1 -3855)
at 3 months post-HCT with only 10 of 26 patients achieving CDS" T-cell counts within the
normal range. Of the remaining patients, 7 of 16 patients were profoundly
immunodeficient with CD3^ T-cell counts of less than 200 CDS'" T-cells per pi.
Nevertheless, CDS^ T-cell recovery was rapid, with 16 of 20 patients tested achieving a
CDS^ T-cell count within the normal range by 12 months post-transplant. Of the
remaining 4 patients on whom I obtained a blood sample at 12 months, only 1 patient had
CDS'" T-cell counts of less than 200 cells per pi.
As for CD4'" T-cell recovery (Figure 3 .IB), median CD4'" T-cell counts at 3 months post-
HCT were 180 cells per pi (range: 4 to 1340) with only 8 o f 26 patients achieving CD4^
T-cell counts within the normal range. Of the remaining patients, 6 o f 18 achieved CD4'"
T-cell counts greater than 200 cells per pi and 12 of 18 patients had CD4^ T-cell counts
of less than 200 cells per pi. By 12 months post-transplant, 16 of 20 patients tested had
restored CD4" T-cell counts within the normal range (median 004^^ T-cell count: 515 cells
per pi; range: 10-1994). Of the remaining patients who had CD4^ T-cell counts below the
normal limits, only one patient had CD4^ T-cell counts below 200 cells per pi.
CD&" T-cell reconstitution (Figure 3.1C) followed a similar pattern to that o f CD4^ T-cells
with a median CD8'" count of 180 cells per pi (range 0 to 3699) at 3 months post-HCT. Of
the 26 patients, 13 of 26 achieved CD8" T-cell counts within the normal range at the 3
months post-transplant. By 12 months post-transplant, median CD8^ T-cell counts were
65

C h a i>t i ;u 3
515 cells per pi (range: 10-2497) and 17 of 20 patients achieved CD8^ T-cell counts
within the normal range.
B10000
6 12 18 24
4 0 0 0
1000 -
1 0 4
246 12 18
M onths post-transplant M onths post-transp lant
5 0 0 0
- - -D,
10-16 1 2 8 24
M onths post-transplant
Figure 3.1: Recovery o f C D 3\ CD4^ and CDS* T-cell subsets after HCT
A bso lu te n u m b ers o f C D T (A), C D T (B) and CD8* (C) T-cel l subsets were measured at va r ious t im e po in ts in
26 patients af ter H CT. T he red bars in each plot represen t the median T-cell coun ts for each time point . T he
g rey d ashed lines represen t the upper and lower l im it o f T-cell coun ts in norm al ind iv iduals . The blue dashed
l ine in (B) rep resen ts a C D 4 count o f 200 cells per pi. Patients with a C D 4 count o f less than 200 cells per pi
were cons idered p ro fo u n d ly im m u n o su p p ressed and were m a in ta ined on an t i -v ira l , a n t i -bac te r ia l and a n t i -
fungal p r o p h y la c t i c m edicat ion .
There is clearly a wide range of C D 3\ CD4* and CD8" T-cell numbers in these patients
after HCT with the majority of patients having T-cell counts out-with the normal range at
3 months post-HCT. Nevertheless, the majority of patients restore T-cell counts to within
the normal range by 12 months post-HCT. These results imply that the recovery of T-cell
numbers can be influenced by factors that vary depending on the individual and the
treatment regimen {e.g. infections, dose of immunosuppression, GVHD etc.). These
factors are analysed and discussed in Chapter 4 but I also tested whether overall T-cell
numbers in this patient group represented a Gaussian distributed or skewed population.
This was carried out using the Kolmogorov-Smirnov (KS) test with KS and P-values
6 6

_________________________________________________________________________________________________________________________________________C h a p t e r 3
using Prism software. Total CD3" and CD4^ T-cell numbers fall within a Gaussian
distribution while the distribution of CDS" T-cells at 3 months falls out-with a Gaussian
distribution (P = 0.007). CD8" T-cell numbers then fall within a Gaussian distribution
after 3 months post-HCT.
The previous results demonstrate that total CD3^, CD4'’ and CDS'" T-cell numbers
recovered to within normal limits in the majority of patients by 12 months post-HCT. In
addition, even though the T-cell populations (for the most part) represent Gaussian
distributed populations, the wide range of values out-with normal healthy control values
suggest that transplant- and patient-specific factors may play a role in influencing T-cell
numbers post-HCT. However, absolute C D 3\ CD4^ and CD8^ T-cell counts give little
information on the origin or diversity of these cells and whether they represent de novo
generated T-cells or mature T-cells that have been transferred with the stem cell graft.
Developm ent o f T-cell phenotyping to detect circulating n a ïv e ,
memory and effector T-cell subsets
To enable the question of the origin of reconstituting T-cells to be addressed in this
cohort of patients, I used flow cytometry and a combination of antibodies which would
enable identification of naïve, memory and effector T-cell subsets. There are a number o f
different circulating T-cell species including various subsets o f helper (CD4" ) T-cells and
cytotoxic (CD8^) T-cells defined by the expression of numerous cell surface markers and
which can be broadly described as naïve, memory or effector T-cells (Table 3.1). A
number of studies have used the appearance of naïve CD4" T-cells (CD45RA"^CD45RO )
after HCT to draw conclusions on the contribution o f thymic-dependent pathways, and
also, the appearance of memory CD4" T-cells (CD45RA CD45R0^) to draw conclusions
on thymic-independent pathways (Dumont-Girard et al., 1998; Foot et at., 1993; Mackall
et at., 1995; Small et a i , 1997; Storek et at., 1995; Weinberg et al., 1995)
67

C H A i > T i ; k 3
Table 3.1: Phenotypic definitions o f nciive, menioty and effector T-cells
■ ■ H ■ ■ ■N a ïv e M em ory E ffe c to r | N a ïv e M em ory E ffe c to r
1 1 1CD45RA +
------ _----------1 4- - 4-
CD45RO - + ! - 4-/int int7-CD27 + 4- 4- -H/int io7^CCR7 -H 4- I + -CD62L 4- 4-/int ! lo /- r 4- 4-/int io /-CD28 4- + r ” + / - i 4- r + / - -CDl la in t/lo 4- 1 4- 1 in t/lo 4- 4-
1B 11 (m ouse) ND ND I n d ' “ T - lo /in t 4-CD44 (m ouse) - 4- r + T - 4- 4-
CD57 - + i - -/+ 4-
[ _ _ Z 3 __________ L T _________ :Data was colla ted from the literature and the current d o g m a regard ing the express ion o f cell su rface m arkers o n naive, m em ory or e ffec to r cells (on hum an cells unless o therw ise stated) is show n. N D = not d e te rm in ed
Antibodies against CD3, CD4, CD8, CD45RA and CD45RO were initially used to identify
naïve and memory T-cells. In the first instance. The profile of CD45RA and CD45RO
staining for a normal healthy control (Age 27) was compared to five patients at 3 months
post-HCT (Figure 3.2). The profile obtained from the normal healthy control
demonstrates an approximately equal proportion of CD45RA^ and CD45RO" T-cells in
the CD4" subset while the majority of cells within the CD8" subset express the CD45RA
antigen. The CD45RA antigen has previously been reported to be a phenotypic marker
enabling identification of naïve CD4* T-cells (Merkenschlager and Beverley, 1989;
Richards et al., 1990; Rothstein et al., 1990; Wallace and Beverley, 1990). However, while
naïve CD8^ T-cells certainly express CD45RA, additional subsets of non-naïve CD8^ T-
cells which express CD45RA have been described (Hamann et al., 1997; Hamann et al.,
1999; Pittet et al., 2000). In each of the patient samples at 3 months post-HCT there were
detectable populations of both CD4" and CD8" T-cells that expressed the CD45RA
antigen, although the cell populations were markedly skewed towards the CD45RO"
phenotype. The fact that there were populations of CD4" and CD8^ T-cells that expressed
the CD45RA antigen in the patients peripheral blood so soon after HCT raised several
possibilities. First, that thymic-dependent pathways were active from very early post
transplant and that these CD45RA"^ T-cells represented de novo generated thymic
emigrants. Second, that these CD45RA^ T-cells represented naïve T-cells that had been
transferred with the stem cell graft, with the third possibility being that the CD45RA
antigen does not represent a truly reliable marker for naïve CD8" or CD4^ T-cells.
68

C h a i t i :k 3
Su
Control
44
CD45RO
B
<eg
iu
Contro
CD45RO
Figure 3.2: Subsets o f CD4* and CD8^ T-cells defined by CD45RA and CD45RO
expression in patients 3 months post-HCT
P B M C p o p u la t io n s from pat ien ts at 3 m on ths p o s t -H C T were sta ined using t lu o re sc e n t - ia b e l le d a n t ib o d ie s
agains t C D 4 , C D 4 5 R A and C D 4 5 R O (A); or C D 8, C D 4 5 R A and C D 4 5 R O (B). Individual patients are iden t i f ied
by their un ique patient n u m b er (UPN) in each plot. The contro l was a normal hea l thy ind iv idual 27 years o f
ag e .
69

C h a p t e r 3
A recent study by De Rosa et a i , using 11-colour, 13-parameter flow cytometry,
demonstrated that by using the CD45RA antigen alone, over 90% of CD4^ T-cells could
be classified as truly naïve. In contrast, the probability o f identifying naïve CD8^ T-cells
using CD45RA alone was 40-90% with this probability increasing with the addition o f
other cell surface markers (De Rosa et al., 2001). I therefore identified a number of cell
surface markers in combination with CD45RA or CD45RO that could identify and
separate naïve, memory and effector T-cells. The available flow cytometer (FACScan,
Becton Dickinson) had three-colour detection capability. Therefore, it was necessary to
identify one other cell surface marker that could be used in combination with either CD4
or CDS and CD45RA or CD45RO. The cell-surface markers CD62L, CD 103 and CD27
were possible candidates. As described previously, CD 103 only represents a phenotypic
marker for CD8^ thymic emigrants and must also be used in combination with CD62L,
CD45RA and CD27. This was out-with the capabilities of the available technology;
therefore CD 103 was discounted. CD62L is expressed on naïve T-cells in combination
with CD45RA and also on memory cells in combination with CD45RO. However, there
does not seem to be a reliable distinction between memory and effector T-cells based on
CD62L expression; therefore, CD62L was also discounted. Previous work by Van Lier et
al. demonstrated that the CD4'" and CD8^ subset could be subdivided into naïve, memory
and effector type T-cells on the basis of CD27, CD45RA and CD45RO expression (Baars
et al., 1995; Hintzen et al., 1993). I tested CD27 in combination with both CD45RA and
CD45RO and it became apparent that the separation of the naïve, memory and effector
cell populations was more consistent using CD45RO in combination with CD27 (data not
shown). It is also known that CCR7 separates memory and effector CD45RO^ T-cell
populations (Sallusto et al., 1999). However, the anti-CCR7 antibody was not available
until relatively late in my study making it impractical to repeat these experiments using
CCR7 instead of CD27.
Therefore, the phenotypic analysis of the post-HCT patients illustrated in Figure 3.2 was
repeated using CD27 and CD45RO. Within the CD4^ (Figure 3.3A) and CD8^ (Figure
3.3B) T-cell subsets in the normal healthy control, a large population o f naïve (C D 45R 0
CD27^) T-cells and a smaller population of memory (CD45RO^CD27^ T-cells were
present. There was also a detectable population of effector (CD45RO^CD27 ) cells within
the CD4^ T-cell subset but not within the CD8^ (CD45RO CD27 ) subset. Analysis of the
patients illustrated in Figure 3.2 {i.e. those patients who had substantial populations o f
CD45RA"’ T-cells at 3 months after HCT) revealed that the expression pattern o f CD45RO
and CD27 was very different from normal individuals. The surprising results from these
analyses were that each patient had a detectable population of CD4"^CD45RO (and
therefore CD45RA"^) cells which were also CD27 and therefore could not be classified as
truly naïve (Figure 3.3A). A number of patients also had populations o f CD4^CD45RO
CD27^ T-cells which represent truly naïve CD4" T-cells, but the percentage of naïve T-
70

C h a it h r 3
cells compared to normal individuals was greatly reduced with the majority of peripheral
T-cells expressing a memory or effector phenotype.
Control
QU
I I II
44
CD45RO
Control
7 # #
CD45RO
Figure 3.3: Subsets o f CD4* and CD8^ T-cells defined by CD27 and CD45RO expression
in patients 3 months post-HCT
P B M C p o p u la t io n s f rom pat ien ts 3 m on ths po s t -H C T were sta ined using t lu o re sc e n t - ia b e l le d a n t ib o d ie s
agains t C D 4 , C D 4 5 R O and C D 27 (A); or C D 8, C D 4 5 R O and C D 2 7 (B). Pop u la t io n s o f naïve (b lue) , m e m o ry
(v io le t) and e ffec to r (red) CD4* T-cells ; naïve (blue) and n o n -n a ïv e (purple) CD8" T -ce l ls are sh o w n for th e
norm al healthy control (27 years old). Individual patients are identified by their U PN in each F A C S plot.
71

_ _ _ _ _ _ _ _ C H A I N E R 3
The CD8^ T-cell subset in these patients at 3 months post-HCT was also markedly
different in terms of the expression of CD45RO and CD27 compared to a normal
individual (Figure 3.3B). The majority of these patients had a reduced population o f
naïve CD8^CD45R0 CD27^ T-cells compared to normal individuals. In addition, while the
majority of CD8"’ T-cells in the normal individual were of a naïve phenotype, the CD8'" T-
cells in these patients were distributed largely among subsets o f memory and effector T-
cells. Also, there were large populations of CD8"^CD45RO' (CD45RA"^) cells which
expressed moderate or low levels of CD27 and therefore cannot be classified as truly
naïve. Van Lier’s group defined numerous subsets, even within normal individuals, o f
CD8^ T-cells based on the expression of CD45RO and CD27 (Baars et al., 1995; Hamann
et at., 1996; Hamann et al., 1997). Furthermore, the highly heterogeneous expression o f
CD45RO and CD27 on CD8^ T-cells in these patients (and the remaining patients in the
study) made the classification o f CD8" T-cells into discrete subsets virtually impossible.
Nevertheless, naïve T-cells were easily identifiable and always formed a tight cluster o f
C D 45R 0 CD27'" cells similar to the profile demonstrated in the normal control.
Therefore, for the purposes of enumeration in the final analysis, CD8‘" T-cells have been
classified simply as naïve (CD45RO'CD27'’‘) or non-naïve (the remaining subsets) on the
basis o f expression of CD45RO and CD27.
Since it was difficult to differentiate between effector and memory cells within the CD8"
T-cell subset using CD45RO and CD27, I decided to look for alternative cell surface
markers that could be used. A subset of CD8^ T-cells which is low in normal individuals
but which has been reported to be greatly increased in patients after HCT (Leroy et al.,
1986; Wursch et al., 1985; Yabe et al., 1990), solid organ transplantation (Legendre et al.,
1985) and viral infections (Joly et al., 1989; Sadat-Sowti et al., 1991; Wursch et al., 1985)
is defined on the basis of expression of CD57 and CD28. Mechanisms inducing the
expansion o f CD8^CD57"^CD28 cells remain poorly defined, but the appearance of this
subset is coincident with high antigenic stimulation of CD8^ T-cells and an immune
deficiency such as that observed in recurrent CMV or HIV infections, or after
transplantation. In addition, the frequency of CD8"^CD57^CD28 cells increased with
increasing age (Merino et al., 1998) and these cells had shorter telomeres (Monteiro et al.,
1996) and a restricted repertoire (Batliwalla et al., 1996) when compared with their CD57
CD28^ counterparts. Together, these observations suggest that the CD8^CD57^CD28
subset has undergone many rounds of replication and has arisen by peripheral expansion
mechanisms.
The previous results are in agreement with studies which demonstrated that CD45RA does
not provide a reliable marker for the identification o f truly naïve CD8"’ T-cells (Baars et
al., 1995; Hintzen et al., 1993). However, contrary to previous findings, these results also
demonstrate that at least in recipients of HCT, CD45RA (when used on its own) is not a
reliable marker for the identification of naïve CD4" T-cells.
72

C h a i>t i ;r 3
T-cell phenotyping strategy
It became apparent from the previous results that it was necessary to use a number o f
antibody combinations to enable identification of naïve, memory and effector T-cell
subsets both in normal individuals and in HCT recipients. The antibody combinations
used throughout this study and the profile obtained in a normal individual is illustrated in
Figure 3.4. Normal healthy control values for some of these subsets have been reported
previously and are illustrated and discussed in the appropriate figures.
CD4 CD45RO
I I I 11 I— I 1 l | I— I I 11 I T T T
CD45RO --------- ►
iCD57 CD45RO CD45RO
Figure 3.4: T-cell phenotyping to monitor the reconstitution o f naïve, memory and effector
T-cells in patients after HCT
P B M C s were iso la ted f rom periphera l b lood sam ples taken from pa t ien ts af ter HCT and sta ined with th e
an t ib o d y c o m b in a t io n s show n. T-cell subsets were analysed by ga t ing on p o p u la t io n s o f C D 3 , C D 4 or C D 8
T -ce l ls (show n in purple in the top right hand corner o f each dot-p lo t) . Th is d a ta il lustrates the d is t r ib u t io n o f
T -ce l ls w ithin dif ferent subsets in a normal healthy individual 27 years o f age.
73

___________________________________________________________________________________________________________________________________________ C h a p t e r 3
Recovery o f naïve CD4^ T-cell numbers
At 3 months post-HCT the number of CD4^CD45RA^ T-cells was greatly reduced below
the normal range with a median number of 10 cells per pi (Range 0 to 172; Figure 3.5A ).
Normal control numbers for C D 45R 0 CD27^ T-cells (in either the CD4" or CDS"” T-cell
subset) were not established, but the number of CD4^CD45RO'CD27'^ T-cells was also very
low with a median of 7 cells per pi (Range 0 to 123; Figure 3.5B). These subsets increased
with time post-transplant but at 12 months post-transplant the number o f CD4^CD45RA^
T-cells still remained below normal control levels with a median value of 130 cells per pi
(Range 0 to 746). Similarly, the number of CD4"^CD45ROCD27'^ T-cells remained low at
12 months post-transplant with a median value o f 130 cells per pi (Range 0 to 847).
Although the results presented previously demonstrate that CD45RA (when used alone)
should be used with caution, the reconstitution of the CD4"^CD45RA" and CD4"^CD45RO'
CD27^ subsets occurred at similar rates. The relationship o f these two subsets was
confirmed using Spearman’s rank correlation coefficient which demonstrated that the
increase in the number of CD4^CD45RA^ T-cells correlated strongly with the increase in
the number of CD4"CD45RO CD27" T-cells (r = 0.84, P < 0.0001).
Therefore, on the basis o f T-cell phenotyping, it would appear that thym ic-dependent
pathways were active in the restoration of peripheral CD4^ T-cell numbers, and that de
novo generated thymic emigrants contributed to the repopulation of the naïve CD4^ T-cell
compartment in patients after HCT. However, this data does not provide any information
on whether the naïve CD4"’CD45RO CD27‘" cells detected in 9 of the patients at 3 months
post-HCT were genuine thymic emigrants or naïve T-cells transferred with the stem cell
graft. Furthermore, the repopulation of the T-cell compartment by naïve T-cells was
insufficient (in the majority of cases) to account for the recovery of total C D 3\ CD4^ or
CD8^ T-cell numbers suggesting that thymic-independent pathways must also be
operative.
Recovery o f memory and effector CD4^ T-cells
Previous studies have reported the rapid recovery of T-cell subsets displaying a memory
or effector phenotype after HCT (Leroy et al., 1986; Lum, 1987; Mackall et at., 1993;
Storek et at., 1995). The suggestions from these reports were that thym ic-independent
pathways were capable of restoring T-cell numbers in the short term, although additional
reports suggested that these expanded cells were limited in repertoire diversity (Gaschet et
at., 1995; Masuko et at., 1996). The contribution of thymic-independent pathways to T-
cell reconstitution post-HCT was assessed by enumeration of T-cells with a memory or
effector phenotype.
74

C h a i t i ;r 3
oDcnn mp£ a12 18 24
M onths post-transplant
3000
1 000 -
Oo°
-W- ooH
1 0 -11 2 18 246
B2000
1 000 -
1 0 0 -
10-U
M onths p ost-tran sp lant
D2000
1000 -
1 0 0 -
10
M onths post-transplant
12 18 24
M onths post-tran sp lant
Figure 3.5: Recovery^ o f naïve, memory and effector CD4* T-cell subsets
A bso lu te n um bers o f C D 4 T D 4 5 R A 'R 0 (A ), n a ïve CD4TD45ROCD27 (B ). m em ory CD4TD45R(rCD27"
(C). and e ffe c to r € 0 4 X 0 4 .3 R O T D27 (O) T -ce lls were calcu la ted from ab so lu te num bers o f C 0 4 " T -ce lls as
d esc rib ed in C hap te r 2. T he grey dashed lines in (A ) represen t the u pper and low er lim its o f C 0 4 T 0 4 5 R A * T-
cell n u m bers in norm al ind iv id u a ls (acco rd ing to (E rkeller-Y uksel et a l . , 1992)). R eference v a lues fo r F ig u re s
(B ). (C ) and ( 0 ) w ere not es tab lished .
In contrast to the recovery of naïve CD4^ T-cell numbers, there were significant numbers
of CD4^ T-cells with a memory (Figure 3.5C) or effector (Figure 3.5D) cell phenotype at
3 months post-HCT. Although reference values for absolute numbers of memory and
effector CD4^ T-cells were not established, the median number of memory CD4^ T-cells at
3 months post-HCT was 79 cells per pi (range: 10-568) increasing to 194 cells per pi
(range 0-1994) at 12 months post-HCT. The absolute number of effector CD4^ T-cells
remained fairly constant over the course of the study with a median number of 45 cells
per pi (range 0-754) at 3 months and 30 cells per pi at 12 months post-HCT.
By analysing the CD4" T-cell compartment as a whole in these 26 patients, it is possible to
draw general conclusions on the contribution of thymic-dependent and thymic-
independent pathways to the reconstitution of CD4^ T-cell numbers (Table 3.2).
75

C h a p t e r 3
Table 3.2: Summary o f reconstitution o f naïve, memory and effector CD4^ T-cell subsets
M onthspost-transp lan t
Total CD4* Naïve CD4* M em ory CD4* E ffector CD4*
3 180 (4-1340) 7(0-123) 79(10-568) 45 (0-754)
6 350 (5-720) 24 (0-189) 111 (0-343) 77 (4-267)
9 330(10-680) 40 (0-196) 155 (0-376) 34 (0-471)
12 520(10-1994) 130 (0-827) 194 (0-1994) 30 (0-823)
A ll v a lu es are g iv en as ce lls p e r m ic ro litre o f b lo o d . T h e m ed ian n u m b ers o f each CD 4^ T -ce ll su b se t w ere
c a lc u la te d fo r the 26 p a tien ts as d esc rib ed p rev io u sly . M ed ian v a lu es a re sh o w n w ith th e ran g e o f each s u b s e t
in b ra c k e ts .
The results presented previously (and summarised in Table 3.2) demonstrate that memory
and effector CD4^ T-cells remained the dominant cell types over the first 9 months post-
HCT. However, although naïve CD4" T-cell numbers are low during this period, the
median naive CD4^ T-cell count increased with time post-transplant and significant
populations of naïve CD4" T-cells were detected at 12 months post-HCT in the majority o f
patients. From this data it appears that thymic-independent pathways restore total
peripheral CD4^ T-cell numbers within 6 months post-HCT by expansion of T-cells with a
memory or effector cell phenotype. The recovery o f naïve CD4‘" T-cells then occurs later
than 6 months post-transplant in the majority of patients.
Similar to the analysis of total CD3" , CD4^ and CDS" T-cell numbers, I carried out
normality testing using the KS-test for the CD4^ T-cell subpopulations. Again, a wide
range of naïve, memory and effector CD4"’ T-cells are present in different individuals. For
the most part, the CD4^ T-cell subpopulations represent Gaussian distributed populations,
although CD4"^CD45RA^ and CD4^CD45R0CD27^ cells do not represent Gaussian
distributed populations at 3 months post-HCT (P = 0.033 and P = 0.006 respectively).
Recovery o f naïve CD8^ T-cells
The previous results demonstrate that the regeneration of peripheral CD4" T-cell numbers
post-HCT is reliant on thymic-independent pathways in the short term with thymic-
dependent pathways contributing to CD4^ recovery in the longer term. The reconstitution
of naïve CD8^ T-cells has been studied to a lesser extent than CD4^ T-cells due to the
difficulties associated with identification o f naïve CD8" T-cells. This is highlighted again
in this patient cohort through the analysis of CD8" T-cells with a CD45RA^ phenotype
(Figure 3.6A). At three months post-HCT, the median number of CD8^CD45RA^ T-cells
was 46 cells per pi (Range 0 to 1950). At 9 months post-HCT 11 o f 16 patients had
restored CD8^CD45RA^ T-cell numbers within the normal range with median
76

__________________ C h a i t i :r 3
CD8XD45RA'" T-cell numbers of 154 (range 0-861). However, it is clear from the data
presented previously that there is more than one species of T-cell contained within the
CD8 CD45RA^ subset and that CD45RA does not provide a reliable marker on its own to
define naïve CD8^ T-cells.
3000
1000 -
IOO --
lO-l
M onths post-transp lant
B2000
loooy
100-
10
D
850 _o
r- '----- 1----- '-----r-6 12 18 24
M onths post-transp lant
4000
_ 1000 -
lOOi
1 0 -1
246 12 18
4000
_ 10001
1 0 0 -
4 -
M onths post-transp lant
12 18 24
M onths post-transp lant
Figure 3.6: Recoveiy o f naïve, memory and effector CDS'" T-cell subsets
A b so lu te n u m bers o f C D 4 5 R A T O (A ), naïve C D 4 5 R 0 C D 2 7 " (B ), non-n a ïv e (C ), and C D 5 7 T D 2 8 (D) CDS"
T -ce lls w ere ca lcu la ted from abso lu te num bers o f CDS'" T -ce lls as described p re v io u sly . The grey dashed l in e s
in (A ) rep resen t the up p er and low er lim its o f C D 8 X D 4 3 R A " T -cell num bers in norm al in d iv id u a ls (G o d th e lp
et a i , 1999). R eference values for F igu res (B), (C ) and (D ) w ere not de te rm in ed .
The recovery of the truly naïve CD8^CD45RO CD27^ subset (Figure 3.6B) was slower than
that of the CD8^CD45RA'' subset. At 3 months post-HCT, the median number o f
C D 8TD 45R O C D 2T ‘ T-cells was 2 cells per pi (Range 0 to 45). Although this subset
increased with time post-transplant the median number of CD8"CD45ROCD27^ T-cells at
12 months post-transplant remained low with a median of 76 cells per pi (Range 0 to
541). A number of previous studies have used only CD45RA to define naïve CD8^ T-cells,
but it is clear from these results that this would result in a substantial overestimate of naïve
circulating CD8" T-cell numbers in post-HCT patients.
77

C h a p t e r 3
The recovery of non-naïve CD8" T-cells was rapid (Figure 3.6C) with the median number
of non-naïve CDS'" T-cells being 179 cells per pi (range 0-3699) at 3 months, rising to a
median of 307 cells per pi (0-2497) by 12 months post-transplant. A number of patients
restored very high non-naive CDS^ T-cell numbers that were significantly higher than the
reference values for the total CDS compartment. This has been observed in a number o f
previous studies although the exact reason for this CDS ‘overshoot’ is unclear (Dumont-
Girard et al., 199S; Singer et at., 19S3; Witherspoon et at., 19S2).
As mentioned previously, due to the heterogeneous expression of CD45RO and CD27 on
different CDS^ T-cells, it was difficult to distinguish discrete populations o f memory and
effector CDS^ T-cells in the majority of patients. I therefore looked at the absolute
number of CDS^ T-cells which were CD57’ CD28 . These cells represent CDS^ T-cells that
have undergone extensive cell division and can therefore be used as a marker for thymic-
independent T-cell reconstitution. Similar to the total CDS’" T-cell population and the
non-naïve CDS" T-cell population, there were significant numbers o f CD8^CD57’ CD2S
cells at 3 months post transplant (Figure 3.6D) with a median number of 77 cells per pi
(range: 0-2683). The median number of CD8’ CD57"^CD28‘ cells increased to 190 cells
per pi (range: 0-2244) at 12 months post-transplant. The normal range o f CD8 T-cell
counts is between 200-900 CD8^ T-cells per pi, with naïve T-cells making up the bulk o f
the CD8 population in healthy controls. The CD8’ CD57’ CD28‘ subset forms only a minor
subset in normal individuals but can make up the majority of T-cells in patients after
HCT. This observation, along with previous reports on the evolution of CD8’’CD57’ CD28
T-cells suggests that the short term reconstitution of CD8" T-cell numbers occurs
primarily through thymic-independent pathways.
Table 3.3: Summary o f reconstitution o f naïve, memory and effector CD8^ T-cell subsets
M onths Total CD8* Naïve CD8* N on-naive CD8* 008*57*28p o st-tran sp lan t
3 180 (4-3699) 2 (0-45) 179 (0-3699) 77 (0-2683)
6 350 (5-3057) 17 (0-74 246 (0-3057) 161 (0-1410)
9 330(10-2093) 15(0-136) 209 (0-2093) 104 (0-1562)
12 520(10-2497) 76 (0-541) 307 (0-2497) 190 (0-2244)
A ll v a lu es are g iv e n as ce lls p e r m ic ro litre o f b lo o d . T he m ed ian n u m b ers o f each CDS^^ T -ce ll su b se t w ere
c a lc u la te d fo r the 26 p a tien ts as d esc rib ed p rev io u sly . M e d ian v a lu es a re sh o w n w ith th e ran g e o f each su b s e t
in b ra c k e ts .
Similar to the results from the analysis of the reconstitution o f CD4^ T-cell subsets, the
recovery of CD8’' T-cells occured in the short term by expansion of CD8'' T-cells with a
memory or effector cell phenotype (Table 3.3). Therefore, thymic-independent pathways
were able to rapidly restore CD8’ T-cell numbers to within the normal range between 3-6
78

___________________________________________________________________________________________________________________________________________C h a în e r 3
months post-HCT. The recovery of naïve CD8^ T-cells was slower and remained low even
at 12 months post-HCT in some patients. Also similar to the CD4" T-cell subset, there were
a number of patients with low but detectable numbers of naïve CDS'” T-cells at 3 months
post-transplant.
Normality testing of the CD8^ subpopulations revealed abnormally distributed
populations within the CD45RA^ subset at 3, 6 and 9 months post-HCT (P = 0.0004, P =
0.04 and P = 0.0003 respectively). The CD8"^CD45R0CD27^, non-naive CD8‘" and
CD8^CD57"^CD28' subsets were all abnormally distributed at 3 months post-HCT (P =
0.0014, P = 0.028 and P = 0.032 respectively), but were restored to a Gaussian
distribution after 3 months post-HCT. The suggestions from this data are two-fold; first,
similar to the CD3^ and CD4^ populations, factors associated with HCT may affect the
repopulation of the T-cell pool; second, since all CD8 subpopulations are affected at 3
months post-HCT, CD8" T-cells may be more susceptible to factors that stimulate or
prevent proliferation of cell death compared with the CD4"’ T-cell population.
The previous results demonstrate that both CD4" and CD8" T-cell numbers are restored in
the short term (less than 6 months post-HCT) through the expansion of T-cells with a
memory or effector phenotype, while in the longer term, naïve T-cells increase in number.
Direct quantification o f thymic-dependent pathways
From the previous results it would appear that measurement of naïve T-cell recovery,
while providing a valuable insight into the role of the thymus in T-cell reconstitution post-
HCT, can lead to inaccurate estimates of the contribution of the thymus to T-cell
reconstitution, particularly in the early stages post-HCT. Clearly, in a TCD transplant
setting where a minimal number of T-cells are transferred with the stem cell graft, the
production of naïve CD4^ and CD8" T-cells can be taken as a marker o f thymic output.
However, in a T-cell replete transplant setting, it is likely that a significant number of naïve
T-cells will be transferred with the stem cell graft, particularly in recipients o f cord blood
transplants. Therefore, while production of naïve T-cells can be used as a marker o f
thymic output, the presence of phenotypically naïve T-cells cannot.
The problems in studying thymic-dependent pathways in a T-cell replete transplant
setting could be reduced by the direct quantification of thymic output.
79

_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ C h a î n e r 3
D etection o f TREC molecules in peripheral blood samples
In the first instance, TREC were measured in sorted CD4^ and CD8^ peripheral blood T-
cells cells using radiolabelled quantitative-competitive PGR (Douek et a i , 1998). However,
there were several disadvantages of this method in that it was time-consuming, labour
intensive and dependent on the use of radioisotopes. I therefore decided to optimise
TREC detection using “Real-Tim e” PCR. This method is rapid (96 well plate format),
accurate and utilises a fluorescent labelled probe instead of relying on a radioisotope for
TREC detection (see Chapter 2: Materials and Methods).
Q uantification o f TREC m olecules in CD4^ and CD8^ T-cells in 2 6
allogeneic H CT recipients
Similar to the measurements of T-cell numbers, absolute TREC measurements were
carried out at 3, 6, 9, 12 and 18-24 months post-HCT. The absolute number o f CD4 and
CD8 TREC in the peripheral blood of 26 allogeneic HCT recipients was calculated as
described in the materials and methods.
Within the CD4" T-cell subset, CD4 TREC (Figure 3.7A) were undetectable in the majority
of patients (21 o f 26) at 3 months post-transplant. The median number of CD4 TREC was
zero per pi (range: 0-1.7) at 3 months post-HCT, zero per pi (range: 0-6.8) at 6 months
post-transplant increasing to a median of 2.3 CD4 TREC per pi (range: 0-276) by 12
months post-transplant. CD8TREC were also very low or undetectable in the majority o f
patients (20 of 26) at 3 months post-transplant (Figure 3.7B). The median number o f
C D 8 TREC was zero per pi (range 0-39) at 3 months post-transplant increasing to 2.61
CD8 TREC per pi (range 0-160) by 12 months post-transplant.
By directly quantifying thymic output, it would appear that there is little or no
contribution from thymic-dependent pathways in the recovery o f either CD4^ or CD8‘" T-
cells in the early stages (less than 6 months) after HCT. Although a number o f patients
have detectable TREC at 3 months post-HCT, most o f the patients who experience
increases in the absolute number o f CD4 TREC and CD8 TREC experience those increases
later than 6 months post-transplant. These observations suggest that thymic-dependent
pathways do play a role in the recovery of CD4^ and CD8^ T-cell numbers post-HCT
although there appears to be a lag-time o f 6-9 months after HCT before thymic output
can be detected. This observation is consistent with the results obtained using T-cell
phenotyping (Figures 3.5 and 3.6).
80

C H A l T I i R 3
B1000
Liia
100-
10 -
JÜB---1 2
o fiii». _jcp_
18
Months post-HCT
Figure 3.7: Increases in numbers o f TREC* T-cells in patients after HCT
A bso lu te num bers o f C D 4 T R E C (A) and CD 8 TREC (B) w ere ca lcu la ted as describ ed p re v io u sly . T he red b a rs
rep resen t m edian num bers o f T R E C at each tim e po in t. T he age range o f the p a tien ts was 6-53 y ears o ld and
th y m ic ou tpu t has been show n to decline w ith in creasing age. T h e grey d ash ed line re p re se n ts the low er l im it
o f the norm al range o f T R E C levels for the o ldest patien t in the study.
These results also confirm previous concerns regarding the analysis of T-cell recovery in
T-cell replete transplants and the possible discrepancy between naïve T-cell numbers and
genuine thymic output. TREC levels were compared with naïve T-cell numbers in the 1 1
patients in whom CD4 CD45RA" T-cells were detectable at 3 months post-HCT and found
that TREC were detectable in only 5 of these patients. Similarly, when TREC levels were
analysed in patients with detectable numbers of CD4 CD45RO CD27^ T-cells at 3 months
post-transplant, TREC were detectable in only 5 of 9 patients. Therefore, by using
additional cell surface markers to define naïve T-cells and by measuring thymic output
directly, it was possible to accurately assess the contribution of thymic-dependent and
thymic-independent pathways to T-cell recovery post-HCT.
Eurther analysis of the contribution of thymic-dependent pathways to T-cell recovery in
each of the 26 recipients of an allogeneic-HCT was carried out by analysing the absolute
CD4 and CDS TREC number in each of the individual patients (Eigure 3.8). Out of 26
HCT recipients, 18 patients experienced increases in TREC levels, with only 9 of 26
restoring TREC levels within the normal range throughout the course of the study.
Maximal TREC numbers varied among these 18 patients with 8 restoring high numbers o f
CD4 and CDS TRECs (>20 TRECs per pi blood) while the remaining 10 patients restored
low to moderate numbers of CD4 and CDS TREC. 8 of the 26 patients did not experience
any detectable rise in TREC levels over the course of the study. Therefore, of the 26
patients, thymic-dependent pathways made a contribution to the recovery of CD4^ and/or
CDS* T-cell numbers in 18 patients. Clearly, there are differences between patients
regarding the extent of contribution of thymic-dependent pathways post-HCT.

C h a i t ï r 3
6 (K )
3(X) -
12 240
Ï
!ï
j
150
100 -
5 0 -
12 240
1 0 -
1260
6
3
012 240
12 240
0 6 12
0 6 12
240 12
120 6
120 6
0 12 24
24120
0 6 12
Months post-HCT
Figure 3.8: Analysis o f absolute TREC numbers in individual patients post-HCT
A b so lu te n u m b ers o f C D 4 ( □ ) o r C D S (■ ) TR EC w ere ca lcu la ted . T h e lo w er lim its o f T R E C n u m b ers in ag e -
m a tch ed c o n tro ls is re p re se n te d by th e d ash ed b lu e line in each p lo t. R e fe ren ce v a lu es w e re k in d ly p ro v id e d b y
D r D an ie l D o u ek (U n iv e rs ity o f T e x a s S o u th -W este rn M edical C e n te r; see A p p en d ix , F ig u re A 3).
82

___________________________________________________________________________________________________________________________________________C h a p t e r 3
Normality testing of CD4 and CD8 TREC levels revealed a significantly skewed, abnormal
distribution at 3, 6 and 9 months post-HCT (P < 0.01 in all cases). The population was
then restored to a Gaussian distribution at 12 months post-HCT. This analysis implies that
TREC levels, while remaining below normal healthy control levels until 12 months post-
HCT are also abnormally distributed within this patient cohort. Furthermore, it is essential
to consider the factors that might be responsible for this skewing of TREC levels post-
HCT.
Relationship between TREC and naïve T-cell numbers
The relationship between naïve T-cells and TREC levels was analysed using Spearman’s
rank correlation coefficients for the 26 patients mentioned previously. For both CD4^ and
CDS’’ T-cells, there was a significant positive correlation between the absolute number o f
naïve T-cells and Absolute numbers of TREC. This correlation was significant at 3, 6, 9
and 12 months post-transplant (Table 3.4). There were insufficient numbers of patient
samples available at later time points to be able to carry out such analyses.
Table 3.4: Relationship between TREC and naïve T-cell numbers
CD4 TREC CD8 TREC
3 months 6 m onths 9 m onths 1 year 3 m onths 6 m onths 9 m onths 1 year
N a ïv e CD4" T -ce ll c o u n t 0.54” 0.66” * 0.77” * 0.96***
N a ïv e CDS* T-cell coun t . . 0.62*** 0.63” 0.69** 0.88***
A b so lu te n u m b ers o f n a ïv e T -ce lls w ere com p ared w ith T R E C n u m b ers u s in g S p e a rm a n ’s rank c o r re la t io n
c o e f f ic ie n t. C o rre la tio n c o e ff ic ie n ts are sh ow n (r v a lues) w ith lev e ls o f s ig n if ic a n c e (b ased on sa m p le s iz e )
re p re se n te d as * P < 0 .0 5 , * * P < 0 .0 0 5 , * * * P < 0 .0 0 0 5 .
The relationship between naïve T-cells and TREC numbers is further demonstrated in
Figure 3.9 which illustrates the change in number of naïve T-cells in one patient who had
high TREC levels and in one patient who did not experience an increase in TREC levels.
This figure is representative of the pattern observed in all 26 patients. From these results, it
is apparent that the regeneration of naïve T-cells in patients after HCT is absolutely
dependent on thymic output and that patients who do not experience a rise in TREC levels
will not reconstitute a significant pool of naïve T-cells. Furthermore, these results suggest
that thymic-independent pathways do not play a role in the restoration o f naïve T-cell
numbers after HCT.
83

C h a i t i ;k 3
1500 300
a.
- 2001000 -
- 1005 0 0 -
126
300 300
- 200 200 -
- 100 100-
Months Post-HCT
Figure 3.9: Reconstitution o f naïve T-cells after HCT is dependent on thymic output
A bso lu te num bers o f naïve C D 4 M O ). naïve CD8^ ( • ) , CIM ^TREC* ( □ ) and C D 8 T R E C * (■ ) T -ce lls are sh o w n
fo r tw o p a tien ts , one o f w hom (Pa tien t 37) ex p erien ced in creases in TREC levels and the o th e r w ho did n o t
(Pa tien t 24). T he low er lim its o f ab so lu te TREC num bers in ag e-m atch ed c o n tro ls is rep re sen ted by the b lue
d ash ed line in each plot.
CD 4^C D 45RO 'C D 27 T-cells and thymic output
It was demonstrated earlier in this chapter that subsets of non-naïve CD4"^CD45RA^ T-cells
exist in a number of HCT recipients. On further analysis, it became apparent that these
cells were only detected in recipients of T-cell replete grafts and not in recipients of T-cell
depleted stem cell grafts. I therefore decided to analyse the recovery of naïve
CD4 CD45RA'^ and non-naïve CD4 CD45RA* T-cell subsets in all recipients of T-cell
replete stem cell grafts. The clinical characteristics of the patients who received T-cell
replete stem cell grafts are given in Table 3.5.
The percentage of naïve (CD4'^CD45RO CD27^) and non-naïve (C D 4T D 45R O CD27 )
CD4 CD45RA^ T-cells and the ratio of naïve:non-naïve T-cells was calculated for each
patient at 3, 6, 9 and 12 months post-HCT (Table 3.6). Patients between ages 6-21 all had
increasing percentages of naïve CD4 CD45RA^ T-cells with increasing time post
transplant and low percentages of non-naïve CD4"^CD45RA^ T-cells at all time points post
transplant. As a result, patients between ages 6-21 had consistently high ratios of
naïve:non-naïve CD4 CD45RA^ T-cells and increases in this ratio with time post
transplant.
84

C h a p t e r 3
T able 3 .5; P a tien t character is ticsUPN Age Diagnosis* Conditioning** T-celI§ GVHEkt
Acute Chronic
Infections# Current status
37 6 ALL C y/T B l 0 .4 3 1 N A live and well25 6 F A C am /C y /T A I 1.48 N N - A live and well36 7 F A C am /C y /T A I 1.48 N N - A live and well12 1 I ALL C y/T B l 0 .1 9 1 N V ZV A live and well2 0 1 5 S A A C a m /C y /F lu 0 .0 9 N N - A live and well9 17 F A C am /C y /T A I 0 .3 9 N N CMV A live and well
39 21 MDS C y /F lu /T B l 2 .8 7 1 E HHV6, T oxoplasm osis, CM V
A live, cG V HD
28 32 cA LL C y/T B I 1.40 N N CNS D ied , re lapse23 38 AM L C a m /F lu /B u 1.72 N N - A live and well3 39 ALL M el/T B l 1.75 N L Beta haem olytic strep A live, cG V HD
104 5 0 NHL C y/T B l 3 .45 I E 5. A u reu s (eye) A live, cG V H D22 53 AM L C y/T B l 2 .6 2 N N CM V A live and well
* FA = Fanconi anaem ia, ALL = acute lym phocytic leukaem ia. AML = acute m yeloid leukaem ia, SAA = severe aplastic anaem ia .
cA LL = com m on acute lym phocytic leukaem ia, M DS = m yelodysplastic syndrom e, N HL = non-H odgkins lym phom a
** Conditioning: Cy = cyclophospham ide, TBI = total body irradiation, TA I = thoraco-abdom inal irradiation. Flu = fludarab ine , Bu
busulphan, M el = m elphalan; Cam = C am path-IH
§ T-cell dose is shown as CD3* cells infusedxlO V kg.
# Infections ie bacteraem ia and pneum onia, virus reactiva tions/in fections occuring within the first year after stem cell HCT. VZV
varicella zoster virus; CM V = cytom egalovirus; CNS = coagulase negative staphylococci; HHV6 = H um an H erpes V irus-6.
# G VHD: A cute G VH D w as graded I-IV in terms o f severity (grade I being the least severe); Chronic G VH D was defined as L =
Lim ited or E = Extensive; N = no clinical GVHD.
By contrast, patients aged between 32-53 did not have greatly increased percentages o f
naïve CD4"^CD45RA" T-cells with increasing time post-transplant and as a result, had
uniformly low ratios of naïve:non-naive T-cells at all time points post-transplant. These
patients had consistently high percentages of non-naive T-cells in comparison to patients
aged between 6-21.
From the previous results, there appears to be two groups o f patients, one group that
restores a high percentage of naive T-cells with time post-transplant (patients aged
between 6-21) and one group who does not (patients aged 32-53). TREC levels in patients
aged 6-21 and patients 32-53 are shown in Figure 3.10A and Figure 3.10B respectively,
TREC could be detected as early as 90 days post-transplant in some of the younger
patients. In addition, thymic output in the younger patient cohort was high such that all
but one patient restored TREC levels within the normal range by 12 months post
transplant. By contrast, thymic output in the older patient group did not reach age-
matched control levels and was either low or undetectable at all time points after HCT.
85

C H A IT I'K 3
Table 3.6: Ratio o f naïve:non-naive CD4*CD45RA* T-cells post-HCTIVrccniagc naïve
CD4-CD4.SRA- T-cellsPercentage non-naïve
C D 4'C 1)45R A ' T-cellsR atio naïve: non-naïve C D 4-C D 45R A ' T-cells
5 6 9 12 5 6 9 12 5 6 9 12
M 9.99 4.48 54.44 55.88 0.14 0.48 0.26 0.64 71 9 210 85
25 12.48 57.72 N/A 8.5.74 0.60 0.58 N/A 0.29 21 65 N/A 289
56 21.54 65.90 N/A 86.15 0.45 1.15 N/A 0,54 48 58 N/A 255
12 25.79 72.90 57.79 51.54 0.51 0.61 1.06 0.45 85 119 56 115
20 0.00 1 1.57 64.48 59.95 0.00 2..57 0.51 0.24 0 5 56 250
y 19.14 58.99 N/A 71.65 1.16 5.64 N/A 0.69 17 11 N/A 104
.59 5.81 65.97 1 1.26 52.95 2.45 0.55 0.27 0.49 2 116 42 67
2X 15.05 22.91 N/A N/A 6.91 4.40 N/A N/A 2 5 N/A N/A
2.5 5.61 0.92 6.55 15.91 2.69 0.92 1.95 1.51 2 1 .5 1 1
.5 19.01 26.11 19.65 16.54 9..54 5.71 2.55 2.80 2 7 8 6
104 0.74 5.15 4.18 2.2.5 15.16 12.61 1.5.77 10.45 0.05 0.25 0..50 0.21
22 12.18 15.77 15,20 8.15 7.15 15.25 8.51 14.77 - 1 0.55
P ercen tag e v a lues rep resen t the num ber o f naïve or n o n -n a ïv e C D T C D 4 5 R A " T -c e lls ex p ressed as th e
p ercen tag e o f CD4* T -cells . T hese values w ere ca lcu la ted for each p a tien t at 3, 6, 9 and 12 m o n th s p o s t
tran sp lan t. N /A : S am p les w ere not av a ilab le from p a tien ts at these tim e po in ts.
u loono-
0 6 9 123
B1
.5000-,
u&
2000-
kCL1000-
ai
Months post-HCT
Figure 3.10; Direct quantification o f thymic output in T-cell replete HCT recipients.
TR EC lev e ls w ere m easured in p o s itiv e ly se lected p o p u la tio n s o f C D 4 ce lls from p a tie n ts 1 to 12 and are
show n as T R E C per I x lO ' so rted ce lls . (A) TR EC levels in so rted C D 4 p o p u la tio n s from p a tien t num b er 3 7
(■ ) , 25 ( A ) , 36 ( T ) , 12 ( ♦ ) , 20 ( • ) , 9 ( □ ) and 39 (A). (B) TREC lev e ls in so rted C D 4 p o p u la tio n s from
pa tien t n u m b er 28 (V ), 23 (0), 3 (O ) , 104 (X ) and 22 (4-). N ote the 10-fold d iffe ren ce b e tw een the Y -axes in
(A) and (B ). T he dashed lines in each p lo t rep resen t the low er lim it o f the no rm al ran g e in a g e -m a tch ed
h e a lth y c o n tro ls .
86

C H A P T E R 3
The recovery o f naïve CD4^CD45RO'CD27^ T-cells is dependent on thymic output,
whereas non-naïve CD4^CD45RO'CD2T T-cells evolve in the absence o f thymic
output
ITie correlation o f thymic output with the recovery o f naïve and non-naïve CD4 CU45RA^ T-
cells was assessed (Table 3.7). The recovery o f naïve CD4 CD45RO CD27 T-cells had a
significant positive correlation with TREC levels at all time points after transplant.
Interestingly, the percentage o f non-naïve CD4 CD4 5 RO CD2 7 T-cells had an inverse
relationship with TREC levels that was significant at 3, 6 and 12 months post-transplant.
Table 3.7: Correlation o f thymic output with CD4^CD45RA^ subsets________________________CD4 TREC
3 month 6 month 9 month 12 month
Naïve CD4^CD45RA^ 0.64* 0.76** 0.73* 0.76**
Non naïve C W C m S R A "^ -0.57* -0.60* -0.51 -0.71*
The percentage of naïve CD4 CD45RA^ and non-naïve CD4 CD45RA^ T-cells was compared against TREC levels
using Spearman’s rank correlation coefficients. Correlation coefficients (r values) are shown with levels of
significance represented as; *P<0.05 and **P<0.005
These results suggest that while thymic output was essential for the recovery o f naïve
CD4 CD45RO CD27^ T-cells, increases in the percentage o f non-naïve CD4^ CD45RO CD27
T-cells only occured in patients who did not experience increases in TREC levels. Therefore,
non-naive CD4 C D 45R 0 CD27 T-cells only developed and were maintained in patients in
whom thymic output was low or absent.
Discussion
The main findings o f this study are: (1) Total C D 3 \ CD4^ and CD8^ T-cell subsets recover to
within normal limits by 6 months post-HCT; (2) In looking for cell-surface markers which
could define naïve, memory and effector T-cell subsets, it became apparent that CD45RA
(when used in isolation) was not a reliable marker that would enable definition o f naïve CD8^
or CD4^ T-cells; (3) The majority o f peripheral blood T-cells displayed a memory or effector
T-cell phenotype during the first 6 months post-transplant, with naïve T-cells appearing later
than 6 months post-transplant; (4) Direct measurement o f thymic-dependent pathways
revealed that the thymus does not contribute to T-cell reconstitution in the majority o f patients
until after 6 months post-transplant; (5) The extent to which thymic-dependent T-cell recovery
occurs varies between different individuals; (6) Reconstitution o f naïve T-cells is absolutely
87

___________________________________________________________________________________________________________________________________________C h a p t e r 3
dependent on thymic output and does not occur without a concomitant increase in TREC
levels.
The majority of the haematological lineages recover relatively rapidly after HCT with the
notable exception of the T-cell lineage, particularly CD4" T-cells, which have been
reported to remain below normal healthy control numbers up to two years post-transplant
(Behringer et a i , 1999; Isaacs, 2000; Lowdell et al., 1998; Small et al., 1999; Storek et
al., 2001). In addition to the reduced numbers, distortions of the T-cell compartment have
also been reported in the early post-transplant period. A number o f reports have
suggested that CDS"' T-cell recovery is relatively rapid, with slower recovery of CD4" T-
cells which results in a prolonged imbalance between helper (CD4^) and cytotoxic (CDS"")
T-cell subsets (Atkinson et at., 1982; de Cast et al., 1985; Forman et a i , 1982; Janossy et
a i , 1986; Mackall et al., 1997). Although distortions among individual T-cell subsets
were evident in terms of the recovery of naïve, memory and effector T-cells, there was no
imbalance in the recovery of total CD4^ and CDS" T-cell subsets in this patient group as a
whole. In the 26 HCT recipients studied, both CD4" and CD8^ T-cell subsets reached
normal limits within 6 months after HCT.
However, several studies have shown that patients who restore normal T-cell numbers
often remain susceptible to opportunistic infections and suggested that a defect in T-cell
function may be one of the reasons for such an increased susceptibility to infection.
Further studies have revealed that restoration of T-cell function in patients after HCT is
reliant on activation of thymic-dependent pathways (Dumont-Girard et a i , 1998; Roux et
a i , 2000).
The second pathway of T-cell regeneration after HCT depends on the expansion o f
mature, graft-derived T-cells and is termed the thymic-independent pathway. Since this
pathway is limited to the expansion of a small number of T-cell clones transferred with
the stem-cell graft, this pathway restores T-cell numbers but does not generate a broad T-
cell repertoire (Mackall et al., 1995; Mackall et al., 1993; Mackall and Gress, 1997;
Rocha et al., 1989). The relative contribution of thymic-dependent and thymic-
independent pathways to T-cell reconstitution post-HCT has been studied using a variety
of methods as outlined previously.
In this study, the majority of peripheral blood T-cells in the CD4 and CD8 compartment
displayed a memory or effector cell phenotype between 3 and 6 months after HCT,
suggesting that thymic-independent pathways rapidly reconstituted the T-cell
compartment after HCT. Such peripheral expansion of memory and effector cells could
be driven by a number of processes including major or minor histocompatability
differences between donor and recipient and/or viral antigens. Alternatively, this
88

_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ C H A I T U R 3
expansion could reflect normal homeostatic mechanisms that control the size of the T-cell
compartment.
A great deal of work has been focused on understanding the regulation of the peripheral
T-cell pool, both under normal circumstances and under conditions o f severe
lymphopenia. Several studies using mouse models have shown that naïve and memory T-
cells, when transferred to a T-cell depleted host, have the ability to expand and proliferate
to fill available space (Bell et al., 1987; Rocha et al., 1989; Tanchot et al., 1997). This so
called homeostatic proliferation is likely to be very limited under normal conditions when
lymphoid tissues contain large numbers of naïve and memory T-cells (Sprent et al.,
1991). However, in patients given chemotherapy and/or pre-transplant conditioning, such
as the 26 HCT recipients studied here, homeostatic proliferation of naïve and memory
cells via thymic-independent pathways could make up a large proportion of repopulating
cells in post-transplant patients. Historically, there has been some debate on whether naïve
T-cells convert to memory T-cells during the process o f homeostatic proliferation (Bell et
al., 1987; Cho et a i , 2000; Goldrath et al., 2000; Rocha et al., 1989; Tanchot et al., 1997;
Tough and Sprent, 1994). Recent studies suggest that naïve T-cells do convert to cells with
a memory phenotype and do not revert back to a naïve phenotype on cessation o f
proliferation (Cho et al., 2000; Tanchot et al., 2001); this point raises one of the
limitations of this study. Previous studies have demonstrated that TREC are diluted out o f
a cell population with each cell division (Douek et a i , 1998). The fact that TREC were not
detected in the majority o f patients at 3 to 6 months post-HCT raises two possibilities. First
and most obvious is that there was no thymic output in these patients. However, the second
possibility reflects the ongoing processes of homeostatic proliferation, meaning that we
cannot discount the possibility that naïve T-cells were exported from the thymus and
stimulated to proliferate and differentiate into memory T-cells in response to homeostatic
signals. Thus it is feasible that thymic-dependent pathways were active at very early stages
after transplant but that these pathways were being masked by the ongoing proliferative
processes. In vivo experiments such as labelling of thymocytes with CFSE would be
necessary to answer these questions.
In addition to these previous results, the identification o f non-naïve CD4^CD45RA^ T-cells
in T-cell replete HCT recipients who do not experience rises in TREC levels raises
questions on the role o f the thymus in regulating peripheral expansion. The inverse
relationship observed between thymic output and non-naïve CD4^CD45RA^ T-cell
numbers suggests that the thymus (or cells produced by the thymus) may inhibit the
development and maintenance of this previously unidentified CD4" T-cell subset in
patients after HCT. Equally, it is important to remember that although a statistical
relationship exists in this instance, this does not necessarily represent a causal relationship
since there are likely to be very complex processes regulating thymic output and
peripheral expansion in post-HCT patients. Nevertheless, previous studies analysing T-cell
89

_________________________________________________________________________________________________________________________________________ C h m ’t e r 3
recovery in lymphopénie hosts have noted that thymic-dependent pathways are used
preferentially to peripheral expansion pathways in thymus-bearing mice and that
peripheral expansion is inhibited by the presence of recent thymic emigrants (Mackall et
al., 1996). The mechanism of this inhibition remains unclear but may be related to the
availability o f soluble factors such as IL-7 (Mackall et at., 2001). A second possibility is
that the thymus produces cells that function as regulatory cells (such as the CD4'^CD25'’
subset) that inhibit homeostatic proliferation. “Bystander cells” that inhibit the extent o f
homeostatic proliferation have been recently suggested to exist (Dummer et al., 2001).
Together, these observations suggest that mechanisms exist to ensure that thymic-
dependent pathways are utilised to regenerate a diverse T-cell compartment whenever
possible, but that peripheral expansion mechanisms restore T-cell numbers in the absence
of thymic output. Whether negative feedback signals are generated by an active thymus to
inhibit peripheral expansion remains unknown.
The way in which these non-naïve CD4"^CD45RO'CD27' cells have evolved in vivo also
remains unknown, but there are at least two potential mechanisms that could generate this
phenotype. Previous studies have demonstrated that CD8^CD45RO CD27‘ cells represent
differentiated effector cells (Baars et a i , 2000; Hamann et al., 1997). Therefore, these
cells may have evolved in a similar manner to differentiated CD8'^CD45RO CD27' effector
T-cells and may represent so-called CD45RO ‘revertants’ . Secondly, it is possible that
these cells represent naïve CD4"^CD45RO CD27" T-cells that have undergone homeostatic
proliferation and that the downregulation of CD27 expression may represent a marker for
homeostatic proliferation of naïve CD4" T-cells in humans, similar to the upregulation o f
CD44 in the mouse (Tanchot and Rocha, 1995; von Boehmer and Hafen, 1993).
The homeostatic control of T-cell numbers was discussed in Chapter 1. After HCT it is
essential that normal homeostasis is restored for a functional immune system to be
established. Several reports have made suggestions as to how this is achieved. Crucially,
the restoration o f naïve T-cell numbers is dependent on thymic output, but recent thymic
emigrants may also have to compete with resident naïve T-cells transferred with the stem
cell graft. A previous study by Hebib et al. suggested that naïve (C D 45RA0 and memory
(CD45RO^) T-cells in patients during the first year after HCT were susceptible to
spontaneous apoptosis when placed in short-term culture (Hebib et al., 1999). This study
also demonstrated that the expanded memory cells were more susceptible to apoptosis
than naïve cells. Hebib et al. further suggested that the increased susceptibility o f memory
cells could be a mechanism to restore normal homeostasis. Thus, by their proposal, T-cells
which exit the thymus would displace those cells which were most susceptible to apoptosis
ie the memory cells. This is in contrast to the work of Tanchot et al. who demonstrated
that the naïve and memory T-cell compartments are independently regulated and that
thymic output will only replace cells within the naïve compartment and not cells within the
memory compartment (Tanchot and Rocha, 1995). Furthermore, the increases in naïve T-
90

___________________________________________________________________________________________________________________________________________ C h a p t e r 3
cell numbers in the 26 HCT recipients in our study were not accompanied by decreases in
memory and effector T-cell numbers. However, it is unclear whether patients with low or
absent thymic output will ever restore a phenotypically normal T-cell compartment,
necessitating long-term analysis o f T-cell reconstitution to address this question. A recent
study by Storek et al. (Storek et a i , 2001) analysed the T-cell compartment in long-term
post-HCT survivors (20-30 years). They demonstrated that although CD4 TREC levels
were significantly lower in HCT-recipients compared with normal individuals, this had no
adverse consequences in terms o f their susceptibility to infection. The question remains
therefore as to how important it is to restore a phenotypically “normal” T-cell
compartment after HCT to be able to have adequate protective immunity.
While the measurement o f thymic-independent pathways can be followed by
reconstitution o f memory and effector T-cells, the measurement of thymic-dependent
pathways after chemotherapy and HCT has been more problematic. The direct
quantification of thymic-dependent pathways has recently been enabled by the
development o f the TREC assay by a number of different groups (Douek et al., 1998;
Okazaki and Sakano, 1988; Poulin et al., 1999). Using the assay published by Douek et
al. (Douek et al., 2000), it was possible to directly measure the contribution of thymic-
dependent pathways to T-cell reconstitution in HCT recipients. The results presented here
demonstrate that thymic-dependent pathways do contribute to T-cell reconstitution after
HCT but that a number o f individuals have no detectable contribution of the thymus to T-
cell reconstitution. In addition, there was a lag-time of between 6-9 months before thymic
out put could be detected in the majority of patients. This delay in thymic output is
significantly longer than in patients who received chemotherapy (Mackall et al., 1995),
but has been observed in previous studies o f allogeneic HCT recipients (Roux et al.,
2000). These observations suggest that some time is necessary to reorganise thymic-
architecture and education of thymocytes from T-cell precursors.
In conclusion, this work has shown that both thymic-dependent and thymic-independent
pathways are active in allogeneic HCT recipients. Furthermore, these results demonstrate
that it is essential that both pathways contribute to T-cell reconstitution after HCT. In the
context o f T-cell reconstitution after HCT, thymic-independent pathways restore T-cell
numbers, but not necessarily fully competent T-cell mediated immunity in the first six
months after HCT. After six months post-HCT, thymic-dependent pathways can be
detected and begin to restore naïve T-cell numbers and the diversity o f the TCR
repertoire.
91

C h a p t e r 4
C h a p t e r 4
Factors affecting T-cell reconstitution
Introduction
The success of haematopoietic cell transplantation is determined by many parameters.
These include the type o f haematological disorder (Burnett and Eden, 1997; Clift et al.,
1993), stage of disease at the time of transplant (Horowitz, 1992), HLA-matching o f
donor and patient and whether the donor and patient are related or unrelated (Davies et
a i , 1997; Gustafsson et al., 2000; Hows et al., 1986; Marks et al., 1993), pre-transplant
conditioning (Feinstein et al., 2001; Michallet et a i , 2001; Morecki et al., 2001; Nagler et
al., 2001), T-cell depletion (Ash et a i , 1991; Gilmore et al., 1986; Prentice et al., 1984),
GVHD prophylaxis (McGlave et a i , 1993), incidence and severity of GVHD (Hansen et
al., 1998; Marks et al., 1993; McGlave et al., 1993), post-transplant infections (Davies et
a i , 1995; Hansen et al., 1998; Hongeng et al., 1997; Keman et al., 1993; Marks et al.,
1993; Oakhill et al., 1996; Ochs et al., 1995; Small et al., 1997; Snyder et al., 1993),
patient age (Madrigal et al., 1997) and stem cell source (reviewed in (Korbling et al.,
2001)). While each of these parameters may have mutually exclusive effects on the
outcome of the transplant, it is the combination of all of these parameters that will
determine the ultimate success of the transplant.
The immediate post-transplant period is followed by a severe and often prolonged
immune deficiency that results in prolonged susceptibility to infection (Hansen et a i ,
1998; Hongeng et al., 1997; Keman et al., 1993; Marks et al., 1993; Oakhill et al., 1996;
Ochs et al., 1995). Although infections that occur in the first month after engraftment
probably result from deficiencies in both granulocytes and other mononuclear cell
subsets, the more prolonged immune deficiency arises from deficiencies in effective CD4^
T-cell and B-cell reconstitution (Small et al., 1997; Small et al., 1999; Storek et al., 2000;
Storek et al., 1997). Later studies showed that restoration of T-cell immunity was
dependent on recovery of the CD4"^CD45RA'’ T-cell (Dumont-Girard et al., 1998; Roux et
al., 2000).
92

_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ C H A P T Ü R 4
The previous observations led to the suggestion that the reconstitution and maintenance o f
effective T-cell immunity after HCT was dependent on education of T-cell precursors in
the thymus (Dumont-Girard et al., 1998; Mackall et at., 1995; Roux et a l , 2000).
Furthermore, these observations generated considerable interest in the factors affecting the
reconstitution o f T-cell immunity through thymic-dependent pathways (Niehues et at.,
2001; Weinberg et al., 2001). Using phenotypic markers of T-cell naivety (primarily the
CD45RA antigen), initial studies demonstrated that increasing patient age had an adverse
effect on the regeneration of naïve CD4" T-cells, presumably due to age-related thymic
involution (Mackall et al., 1995). Some of the problems in using phenotypic markers
such as CD45RA in monitoring T-cell reconstitution were highlighted in Chapter 3.
Recent studies confirmed that increasing patient age had an adverse effect on thymic
output (Douek et al., 1998; Douek et al., 2000). In addition, the thymus has been
demonstrated to be a target of GVHD and the presence o f GVHD after HCT is associated
with decreased TREC levels (Weinberg et al., 2001). There is also some evidence that
thymic output can be influenced by donor lymphocyte infusions (Hochberg et al., 2001)
and pre-BMT radiotherapy (Chung et al., 2001).
The results from Chapter 3 demonstrated that the contribution of thymic-dependent and
thymic-independent pathways to T-cell reconstitution was highly variable between
different individuals and that the recovery of T-cell populations often fell out-with
Gaussian distributions. Therefore, the aim of this chapter is to carry out an analysis of the
factors affecting total T-cell reconstitution, thymic output and memory and effector T-cell
reconstitution. The final analysis was based on 32 patients from the Royal Free Hospital
and the Institute Português de Oncologia, Portugal.
93

C h a p t e r 4
Table 4.1: Clinical characteristics o f patients enrolled in the study
UPN Age Diagnosis* Stem Cell Source
Donorot Conditioning** Infections# Current sta tus
37 6 ALL BM Sibling Cy/TBI Alive and well25 6 FA PB sibling Cam/Cy/TAI - Alive and well26 7 FA PB sibling Cam/Cy/TAI - Alive and well12 11 ALL BM sibling Cy/TBI VZV Alive and well35 14 ALL BM Mis-UD Cam/Cy/Flu/TBI Candida^, Streptococcus
spp.Alive and well
20 15 SAA BM sibling Cam/Cy/Flu - Alive and well9 17 FA BM sibling Cam/Cy/TAI CMV Alive and well
39 21 MDS PB sibling Cy/Flu/TBI HHV6, Toxoplasm osis CMV
Alive, cGvHD
46 22 AA/PNH PB sibling Cam/Cy/Flu VZV, sep ticaem ia Alive and well63 24 CML BM MUD Cam/Cy/Flu/TBI P. aeruginosa, CMV Alive, re lap sed7 27 CML BM MUD Cam/Cy/Flu/TBI MRSA, CNS, HHV6 Alivet])
183 29 CML BM MUD Cam/Cy/Flu/TBI Septicaem ia, CMV Died (septicaem ia)44 30 SAA PB sibling Cam/Cy/Flu T ubercu losis Alive and well28 32 CALL PB sibling Cy/TBI CNS Died (relapse)21 32 AML Ml BM Mis-UD Cam/Cy/Flu/TBI CMV, CNS, Candida^, P.
aeruginosa, Citrobacter, PCPDied (relapse)
152 37 CML PB MUD Cam/Cy/Flu/TBI S. aureus, H. infiuenzae, CMV, MRSA
Alive, resolved cGVHD
29 37 AML PB sibling Bu/Cy - Alive and well59 37 AML PB MUD Cam /Cy/Flu/Bu CNS, HHV6 Alive, cGVHD151 38 AML-M2 BM sibling Cy/Flu/TBI CMV Alive, resolved
cGHVD Alive and well23 38 AML M2 PB sibling Cam/Flu/Bu -
24 38 AML M4 PB sibling Cy/TBI CMV, adenovirus Died, (haem orrhage)3 39 ALL PB sibling Mel/TBI B eta-haem olytic
StreptococcusAlive, cGVHD
31 40 CML PB cousin Bu/Cy - Alive and well34 40 CML PB co u sin Bu/Cy - Alive and well178 45 AML-M5 PB sibling Cam/Cy/Flu/TBI CMV, VZV Alive and well47 45 MM PB sibling Cy/TBI - Alive and well112 47 MDS PB sibling Bu/Cy CMV Alive and well171 50 AML BM sibling Bu/Cy CMV Alive and well33 50 ALL PB co u sin Cy/TBI VZV, encephalitis Alive and well104 50 NHL PB sibling Cy/TBI S. aureus (eye) Alive, cGVHD122 50 MM PB sibling Cy/TBI CMV, sep ticaem ia Died, cGVHD22 53 AML PB sibling Cy/TBI CMV Alive and well
* FA = Fanconi anaemia, ALL = acute lym phocytic leukaemia, AML = acute m yeloid leukaem ia, SA A = severe aplastic
anaem ia, CML = chronic myeloid leukaemia, cALL = common acute lym phocytic leukaem ia, MDS = m yelodysplastic
syndrome, NHL = non-Hodgkins lymphoma, PNH = paroxysmal nocturnal haemoglobinuria, MM = multiple m yeloma.
oc Donors were either HLA-m atched related (siblings or cousins), HLA-m atched unrelated (M U D ) or H LA-m ism atched
unrelated (M is-U D ).
** Conditioning: Cy = cyclophospham ide, TBI = total body irradiation, TAI = thoraco-abdominal irradiation. Flu =
fludarabine, Bu = busulphan, Mel = melphalan. Cam = Campath.
# Infections, i.e. bacteraem ia and pneumonia, virus reactivations/infections occuring within the first year after stem cell
transplant. VZV = varicella zoster virus; CMV = cytom egalovirus; MRSA = methicillin/multi resistant S taph y lo co ccu s
a u reu s\ C N S = cosigu\ase n e g a t\\e S taphylococcus spp .\ HH V6 = Human Herpes Virus-6, P seudom onas aeruginosa', PCF =
P neum ocystis pneum on ia , § Oral Candidiasis.
(|) PCR 4-ve for BCR-abl translocation, but no evidence o f haematological relapse.
94

C h a p t e r 4
Table 4.2: T-cell related clinical dataUPN T-Cell
Depletion*Donor leukocyte
Infusion**T-cell dose#
Acute
GVHD?t
Chronic
GVHD prophylaxiscj) Additional Post-Tx Immune suppression
37 N N 0.43 1 N CsAj/M tx N25 N N 1.48 N N C sA „ N26 N N 1.48 N N CsA , 2 N12 N N 0.19 1 N CsA^/Mtx N35 Y N TCD N N TCD/CsAj N20 N N 0.09 N N CsA,2/Mtx N9 N N 0.39 N N CsA , 2 N
39 N N 2.87 1 E CsA/M tx FK506=c,s te ro id s^
46 Y N TCD N N Myco°c/Mtx N63 Y 8M, 12M TCD N N TCD N7 Y 19M, 22M TCD N N TCD N
183 Y N TCD N N TCD stero id s44 Y N TCD N N CsA,2/Mtx N21 Y N TCD 1 L TCD/CsA,2 stero ids28 N 7 M 1.40 N N C sA /M tx N152 Y N TCD 1 E TCD stero id s29 N N 1.37 N N C sA N59 Y N TCD II L TCD stero id s24 Y N TCD 1 E TCD stero id s,
PUVAvy151 N N 1.45 II E CsA^/Mtx stero id s23 N 8M 1.72 N N CsA^/Mtx N3 N N 1.75 N L C sA /M tx stero id s
31 N N 1.80 N N CsA N34 N N 2.60 N N CsA N47 Y N TCD N N TCD N178 Y N TCD N N CsA, N112 N N N/A II N CsA/M yco N171 N N 1.07 N N CsA /M yco N33 N N 3.56 N N CsA/M yco N122 Y N TCD N E TCD stero id s104 N N 3.45 1 E C sA /M tx stero ids22 N 6M 2.62 N N C sA /M tx N
* T-cell depletion (TCD ) was carried out according to C am path U sers Protocol N o.4 (C am path -IH "In the bag", with in-vivo p r e
transp lan t C am path -IH ).
** 5 patients received DLI w ithin the time fram e o f this study.
# T-cell dose is shown as CD3* cells infusedxlOV kg. T-cell dose in recipients of a T-cell depleted (TCD ) donor product was d e f in e d
as “ u n know n” .
GVHD; A cute G VHD was defined as grade I-IV; Chronic G VH D was defined as L = Lim ited or E = Extensive; N = no clinical GVHD.
$ G V H D prophylaxis: C yclosporin A (CsA) was adm inistered on Day -1 and patients rem ained on CsA for a period of 3 (C s A ,) o r
12 (C sA ,,) m onths; M ethotrexate (M tx) was adm inistered on days +1, +3, and +6.
oc Patien t suffered allergic reaction to CsA and w ere placed on either FK 506 or M ycopheno late (M yco) as a lte rn a tiv e
im m u n o su p p ressiv e therapy .
= Patients undergoing ep isodes of e ither acute or chronic GVHD w ere treated with one or m ore of the following: P re d n is o lo n e ,
M ethy lp redn iso lone , M ycophenolate, w ith additional im m unosuppression using CsA as deem ed appropriate by the clin ic ian
\|/ A dditional GVHD therapy inc luded P sora len A ctivated U ltraviolet A p ho to therapy (P U V A ).
95

___________________________________________________________________________________________________________________________________________C h a p t e r 4
RESULTS
Factors affecting thymic output in recipients o f a l logene ic HCT
The results from Chapter 3 demonstrate that thymic-dependent and thymic-independent
pathways contribute to immune reconstitution by varying degrees in different patients.
The clincial characteristics of the patients analysed in this chapter are detailed in Tables
4.1 and 4.2. Clearly, this is an extremely heterogeneous patient group encompassing a
wide variety of ages and diseases. In addition, the conditioning regimens, haematopoietic
cell sources, graft manipulations and post-transplant immunosuppressants vary between
individuals. Due to the relatively small number of patients in this study and the
heterogeneity of the group, possible factors affecting immune reconstitution were
analysed independently of other variables. Therefore, the effect of patient age was
analysed regardless of whether patients received peripheral blood or bone marrow,
whether the grafts were T-cell depleted or not, whether patients had acute or chronic
GVHD and so on.
Age o f transplant recipient
It is well documented that the thymus involutes as part of the normal ageing process, and
that this involution is paralleled by a gradual decrease in production of thymic emigrants
with increasing age (Aspinall and Andrew, 2000; Douek et a i , 1998; Hollander, 1997;
Mackall and Gress, 1997; Mackall et al., 1997; Mackall et al., 1998). Furthermore, it has
been suggested that older patients may be unable to regenerate normal numbers o f naïve
T-cells after HCT or chemotherapy due to thymic insufficiency. Therefore, the effect o f
patient age on thymic ouput and recovery o f T-cell subsets after HCT was assessed (For
age-matched control TREC values see the Appendix, Figure A3).
The patients detailed in Tables 4.1 and 4.2 were divided into two groups with the first
group ranging from 6-30 years old (n = 13) and the second group ranging from 30-53
years old (n = 19). The groups were divided in this way simply to have significant
numbers within each group since previous reports described a linear decline in TREC
levels throughout life (Douek et al., 1998). There was no significant difference in CD4 or
CD8 TREC levels between the two age groups at 3 months post-transplant with TREC
being uniformly low or undetectable in both groups (Figure 4.1). With increasing time
post-transplant, all of the 6-30 age group experienced increases in TREC levels rising to a
median of 45 CD4TREC (range 0.5-276) and 16 CD8 TREC (range 0.22-160) per |il
blood by 12 months post-transplant. By contrast, the majority o f patients aged 30-53
96

______________________________________________________________________________________________________________________________________________________ C h a i t i -r 4
experienced only slight increases in TREC levels over the first 12 months post-transplant.
The median number of CD4TREC was 1 (range 0-10) while the median number of CDS
TREC was 0.5 (range 0-18) at 12 months post-transplant. The differences in TREC levels
between the two age groups was statistically significant at 6, 9 and 12 months for CD4
TREC, and was statistically significant at 12 months post-transplant for CDS TREC (see
the Appendix, Tables A2 and A3 for P-values).
B1000 1
go 100 i
< ^
0.1 ^
"oo
\c è o ^3
Ôo
o
Q
o * •
0 . 1-
12
Oo°
3
oo
o
8o ° .
O° •
0 °o
^ •o° • •o
0 ••
° ea—#
6 9 12
Months post-HCT
Figure 4.1: Ejfect o f patient age on thymic output
T R E C levels w ere m easured in sorted C D 4 (A ) and C D 8 cells (B) taken from p a tie n ts aged 6 -3 0 y ears old (O ),
and 30-53 years o ld ( • ) . A bso lu te num bers o f C D 4 and CDS T R E C w ere ca lcu la ted as d esc rib ed in the m a te r ia ls
and m ethods. M edian values are rep re sen ted as large open c irc le s for p a tie n ts aged 6 -3 0 and as large c lo se d
c irc le s for pa tien ts aged 30-53 years old.
Therefore, when age alone was taken into consideration, there was a significant adverse
effect of increasing age on thymic output in these patients.
Since age had a significant effect on thymic output, it might be expected that this would
be reflected in the recovery of T-cell subsets after HCT. It was demonstrated in Chapter 3
that thymic output was essential for the recovery o f naïve T-cell numbers, therefore the
rate of reconstitution of naïve T-cells was compared between the two patient groups.
There was no statistically significant difference between numbers of naïve T-cells in the
two patient groups over the first nine months post-transplant (Figure 4.2). However, by 1 2
months post-transplant, there were significantly more naïve CD4* and CDS^ T-cells in the
younger patient group compared to the older patient group. Although differences in
absolute numbers of naïve T-cells did not reach statistical significance until 12 months
post-transplant, the fact that TREC levels were significantly higher in the younger patient
group suggests that the thymus is repopulating the naïve T-cell pool in this group.
97

C h a p t e r 4
B2000
1000'
1 0 -
2000
Oo0(%
o o° °o •
1000
o • : ♦* 100••
G :o *• 0 - r •
o ••• •• 106 9 12
o
X " :
o
ooOqoo • .°0 • •OqO • oo ,
0Q • o • ♦•
oax>« oo#^ ..6 9 12
Months post-HCT
Figure 4.2; Ejfect o f patient age on naïve T-cell recovery
A bso lu te num bers o f n a ive CD4* (A ) and CDS* T -ce lls (B ) w ere m easured in p a tie n ts aged 6 -3 0 y ears o ld (O ),
and 3 0 -53 y ears o ld ( • ) at 3, 6, 9 and 12 m o n th s po st-H C T . M edian v a lu es are rep re sen ted as large o p e n
c irc le s fo r p a tien ts aged 6 -3 0 and as la rg e c lo sed c irc le s fo r p a tien ts ag ed 30 -53 y ears old.
Graft versus host disease
A previous study using TREC to measure thymic output demonstrated that GVHD had an
adverse effect on thymic output (Weinberg et al., 2001). Thymic output and naïve T-cell
recovery was therefore analysed in patients with or without GVHD.
TREC levels in sorted CD4 (Figure 4.3A) and CD8 (Figure 4.3B) cells were measured in
patients who had no episodes of GVHD or patients who had experienced or were
experiencing ongoing chronic GVHD, TREC levels in patients with no GVHD were low or
undetectable for the first six months post-transplant with the majority of patients
experiencing rises in TREC levels between 6 and 12 months post-transplant. Median CD4
TREC levels in patients with no GVHD rose from 0.12 CD4 TREC per pi blood (range 0
to 6.8) to 12 CD4 TREC per pi blood (range 0 to 276) between 6 and 12 months post
transplant.
By contrast, patients experiencing ongoing episodes of chronic GVHD did not experience
a rise in TREC levels at any time point with median CD4 and CD8 TREC levels of less
than 0.1 TREC per pi blood at all time points.
98

C h a i t i ;r 4
BlOOOn
1 0 0 -
II 10
10001
1 0 0 -
10i
oo
oOo
0 . 1-
Oq O
3
0o
ncm,i
n
o o o 00 0,1
12
Months post-HCT
Figure 4.3: Ejfect o f GVHD on thymie output
T R E C levels w ere m easured in sorted C D 4 (A) and CD 8 ce lls (B) taken from p a tien ts w ith no sig n s o f GVHD
(O ), and p a tien ts w ith o n g o in g ch ro n ic GVHD w ith or w ithou t p rio r acute GVHD ( • ) . A b so lu te num bers o f
C D 4 and C D 8 T R E C are show n. M edian values are rep resen ted as large open c irc les for pa tien ts w ithou t GVHD
and as large c lo sed c irc les for patien ts w ith G V H D .
The difference in CD4 TREC levels between patients with or without chronic GVHD was
statistically significant at 9 and 12 months post-transplant with P-values of 0.0016 and
0.006 respectively. The difference in CD8 TREC levels between patients with or without
chronic GVHD was statistically significant at 12 months post-transplant with a P-value of
0.015.
The effects of GVHD on naïve T-cell recovery also do not become apparent until 1 2
months post-transplant in the majority of patients. The numbers of naïve CD4^ and CD8^
T-cells at 12 months post-transplant are significantly reduced in patients experiencing
chronic GVHD compared to patients without GVHD (Figure 4.4; P = 0.0023). It is highly
probable that this reduction in naïve T-cell numbers is a result of reduced thymopoiesis in
patients experiencing episodes of chronic GVHD.
99

C h a it u r 4
1000
£l"3.I« 5 0 0 -
B
-GVHD +GVHD
1000
5 0 0 -
• •
-GVHD +GVHD
Figure 4.4: Naïve T-cell numbers at 12 months post-HCT in patients with or without
cGVHD
A b so lu te n u m bers o f na ïv e CD4* (A) and CD8^ (B) T -ce lls (C D 45R O C D 27") w ere ca lcu la ted for p a tie n ts 1 2
m on ths after H C T w ithou t cG V H D (purp le circles) or w ith o n g o in g cGVHD (b lue squares). T he dashed line in
each p lo t rep resen ts adu lt re fe rence values for CD4* and CD8* T -ce lls defined as naïve on the basis o f C D 45R A
(T ak en from (E rk e lle r-Y u k se l et a l., 1992) and (G odthelp et a!., 1999))
T-cell depletion
The previous results demonstrate that both increasing patient age and chronic GVHD have
an adverse effect on thymic output and reconstitution of naïve T-cells after HCT. It is well
documented from previous studies that T-cells, when transferred to a lymphopénie
environment, have the ability to proliferate spontaneously to fill the T-cell compartment
(Bender et al., 1999; Cho et al., 2000; Ernst et al., 1999; Goldrath and Bevan, 1999;
Mackall et al., 1997; Pereira and Rocha, 1991 ; Rocha et al., 1989; Tanchot et al., 1997).
In addition, previous studies have noted a higher number of naïve CD4^ and CDS'" T-cells
in recipients of T-cell replete stem cell grafts compared to recipients of T-cell depleted
grafts (Lowdell et al., 1998). We also know that TREC frequencies, but not necessarily
absolute TREC numbers, can be affected by contraction and expansion of the T-cell pool
(Douek et al., 1998; Hazenberg et al., 2000; Kong et al., 1998; Poulin et al., 1999).
Therefore, analyses were carried out to assess the effect of T-cell dose (in recipients of T-
cell replete transplants) and T-cell depletion on thymic output and naïve T-cell
reconstitution and all TREC measurements were calculated as absolute TREC numbers to
prevent artefacts of cellular proliferation affecting TREC levels.
100

C h a i t i ; r 4
A common method of GVHD prophylaxis is to deplete the stem cell graft o f
contaminating T-cells (Brenner et ciL, 1986; Gilmore et al., 1986; Prentice et at., 1984).
However, this approach can delay T-cell reconstitution and increase the risk of disease
relapse and infection (Apperley et al., 1988; Daley et al., 1987; Goldman et al., 1988;
Maraninchi et al., 1987; Small et al., 1997). The effect of T-cell depletion on the
recovery of naïve T-cells and thymic function is largely unknown.
I therefore compared naïve T-cell numbers in patients who received either T-cell replete
or T-cell depleted grafts (Figure 4.5). There were significantly lower numbers of naïve
CD4^ (Figure 4.5A) and CD8^ (Figure 4.5B) T-cells in recipients of T-cell depleted
compared with T-cell replete stem cell grafts at 3, 6, and 9 months post-transplant. There
was no significant difference between the two groups at 12 months post-transplant.
B2000
1000 d1000 -
o • •°oO 0
°cfO
104CC0D«
° oO q O , w •
°oo o •
o , o
o o o « # # - o
O o o
& o o
o° •
Months post-HCT
Figure 4.5: Ejfect o f T-cell depletion on naïve T-cell numbers after HCT
A bso lu te num bers o f naïve C D 4" (A) and CD8^ (B) T -cells (C D 4 5 R O C D 27") w ere ca lcu la ted for p a tien ts w ho
rece iv ed T -ce ll rep le te (O ) or T -cell dep le ted g rafts ( • ) . M edian v a lues are rep resen ted as la rge open c irc les fo r
rec ip ien ts o f T -cell rep le te g rafts and as large c losed c irc les for rec ip ien ts o f T -cell d ep le ted grafts .
CD4 and CD8 TREC levels were also significantly lower in recipients of T-cell depleted
grafts compared with recipients of T-cell replete grafts at 3 and 6 months post-transplant
(Figure 4.6). Since the majority of patients do not experience increases in TREC levels
until after 6 months post-HCT, this observation raises one of the limitations of this
analysis. As mentioned earlier, it is probable that TREC^ T-cells are transferred with the
haematopoietic cell graft (albeit that TREC would probably be diluted out from the cell
population in most cases). However, it is not possible to separate de novo generated
TREC^ T-cells from TREC^ T-cells that are transferred with the graft. Therefore, it is
possible that the differences in TREC levels between recipients of T-cell depleted and T-
cell replete grafts reflects depletion of TREC^ T-cells from the graft. No significant
101

C h a i’T i :u 4
difference in TREC levels between recipients of T-cell depleted and T-cell replete grafts
was apparent at 9 or 12 months post-transplant.
BlOOOn
I100
0 . 1-
ooO
0o
bOfSr-
o
••o
O f
O
o •
1 0 -
k2|_ 0,1
o
o
ooo'
O q O
0o o
o
oocnrqi
12 9
OQQO
12
Months post-HCT
Figure 4.6: Effect o f T-cell depletion on the detection o f thymic output
T R E C lev e ls w ere m easured in so rted C D 4 (A) and CD 8 cells (B) taken from p a tie n ts w ho received T -ce ll
d e p le te d ( • ) o r T -cell rep lete g rafts (O ). A bso lu te num bers o f C D 4 and CD 8 TREC are sho w n . M edian v a lu e s
are re p re se n te d as large open c irc les for rec ip ien ts o f T -cell rep le te g ra fts and as large c lo sed c irc le s fo r
re c ip ie n ts o f T -ce ll d ep le ted grafts.
It is possible that these effects are an artefact and actually represent differences between
the two groups of patients who received T-cell depleted and T-cell replete grafts. In
support of this, only one patient under the age of 18 (i.e. the patient group with the
highest level of thymic activity) received a T-cell depleted graft. In addition, 7 out of 14
patients in the T-cell depleted group received a graft from an unrelated donor, raising
questions as to whether thymic education is affected by minor or major histocompatibility
differences.
A number of patients in the T-cell replete group had detectable numbers of TREC and
naïve T-cells at 3 months post-transplant. While our results do not conclusively rule out
the possibility that some of these TREC" T-cells were transferred with the stem cell graft,
results from Douek et al. (Douek et al., 2000) and the majority of the patients presented
in this study suggest that TREC are undetectable until de novo thymopoiesis occurs. This
being the case, we know that de novo thymopoiesis can occur as early as 100 days after
HCT. The fact that TREC were not detected in any of the recipients of T-cell depleted
grafts at 3 months and only one patient at 6 months post-transplant suggests that this may
represent a sampling problem.
The processes that drive proliferation of T-cells in a lymphopénie host may be
responsible for proliferation of the small number of T-cells transferred with a T-cell
1 0 2

__________________________________________________________________________________________________________________________________ C h a p t e r 4
(Brenner et a i , 1986; Gilmore et al., 1986; Hale et a i , 1998; Prentice et al., 1984;
Urbano-Ispizua et al., 2001; Urbano-Ispizua et al., 2001)). Therefore, when a TREC
thymie emigrant is produced during the early stages post-transplant in T-cell depleted
graft recipients, it may be subjected to the same homeostatic pressure as the other
peripheral T-cells and be stimulated to proliferate. If this were to occur on a larger scale,
the detection of TREC molecules and naïve T-cells would not be enabled until a threshold
number of T-cells is reached and homeostatic proliferation slows down. In contrast to the
extremely lymphopénie environment in a TCD transplant recipient, recipients o f T-cell
replete grafts often receive stem cells grafts containing large numbers o f T-cells and are
therefore less reliant on homeostatic proliferation to restore T-cell numbers. This would
subsequently enable naïve T-cell and TREC detection earlier after transplant than
recipients of T-cell depleted grafts.
However, it should be noted that while these processes may be operative, the proof o f such
a hypothesis would require in vivo data. There is no direct evidence that this is the case
other than the fact that TREC detection is possible at 3 months post-transplant in T-cell
replete HCT recipients but is delayed until 6-9 months post-transplant in recipients of T-
cell depleted grafts.
T-cell dose
The previous results demonstrate that T-cell depletion has some short term effect on naïve
T-cell numbers in the periphery, and possibly an effect on thymic output. This analysis
was extended to look at whether T-cell dose in recipients of T-cell replete grafts was
related to naïve T-cell numbers and/or thymic output.
The T-cell dose received by recipients of T-cell replete grafts was shown previously in
Table 4.2. These T-cell doses were compared to naive CD4'’ and CD8^ T-cell numbers at
3, 6, 9 and 12 months post-transplant using Spearman’s rank correlation coefficient. It
might be expected that the strongest relationship would be T-cell dose with T-cell
numbers at 3 months post-transplant. However, there was no correlation between naïve
CDA* or CD8^ T-cell numbers with T-cell dose at 3 months post-transplant (r = 0.24, P =
0.37 for CD4^ T-cells, r = 0.30, P = 0.25 for CD8^ T-cells). Neither was there any
relationship of T-cell dose to naive 004^ T-cell recovery at 6 months post-transplant, or
between T-cell dose and naive CD8^ T-cell numbers at 6 or 9 months post-transplant.
There was a significant inverse relationship between T-cell dose and naive CD4^ T-cell
numbers at 9 and 12 months post-transplant, and naive CD8" T-cell numbers had an
inverse relationship with T-cell dose at 12 months post-transplant.
103

_________________ C h a p t e r 4
The relationship o f thymic output to T-cell dose was exactly the same as naïve T-cell
numbers with no relationship apparent at 3 or 6 months for CD4 TREC and 3, 6 or 9
months for CDS TREC. CD4 TREC did have a negative correlation with T-cell dose at 9
and 12 months post-transplant and CDS TREC numbers were inversely related to T-cell
dose at 12 months post-transplant. However, the significance of these observations is
unknown at present and may represent a chance association rather than a genuine
phenom enon.
Stem cell source: Peripheral blood versus bone marrow
The majority o f patients (22 of 32) received peripheral blood stem cell transplants, with
only 10 of 32 receiving bone marrow transplants. The number of patients within each
group who received T-cell depleted grafts was comparable with 6 o f 10 BM recipients and
S of 22 PB SC recipients. However, I was unable to assess whether there was a significant
difference in T-cell dose between recipients of T-cell replete PB or BM grafts due to the
small numbers of patients within each group. Nevertheless, the separate effects o f T-cell
depletion and T-cell dose on the recovery o f naïve T-cells and thymic output have already
been demonstrated. I therefore analysed the recovery of naïve T-cells and TREC levels in
PBSC or BM recipients regardless of whether the grafts were T-cell depleted or not.
This analysis demonstrated that there was no statistically significant difference in naïve T-
cell recovery or TREC levels between patients who received a PBSC or BM transplant at
any time post-transplant. Therefore, in this patient cohort, stem cell source was not a
significant influence (independent of other factors) on T-cell recovery after HCT.
Donor leukocyte infusions
A recent study by Hochberg et al. (Hochberg et al., 2001) suggested that TREC levels
could be manipulated in vivo by the transfer o f donor lymphocytes as a treatment for
relapsed CML. This data demonstrated an increase in TREC levels post-DLI that was
coincident with restoration of normal donor haematopoiesis and elimination of leukaemic
cells. In the cohort of patients described in Tables 4.1 and 4.2, 5 patients received donor
leukocyte infusions throughout the course o f this study. DLLs were administered because
the patient had either relapsed, or was considered to be at a high risk of relapse. Figure
4.7 shows the change in CD4 and CDS TREC levels before and after DLI in 3 o f these
patients (patient 28 died between 6 and 9 months post-transplant and patient 11 received a
DLI at 18 months post-HCT and I did not receive a sample after this time point).
104

C h a i t h r 4
6
3
0120 612 0
Months post-HCT
Figure 4.7: Ejfect o f donor leukocyte infusions on thymic output
T R E C levels were m easured in sorted C D 4 and CD 8 cells taken from p a t ien ts who received one or more DLI.
Patients are identified by their UPN which is show n in each plot. Abso lu te num bers o f C D 4 T R E C (□ ) and C D S
T R E C (■) are show n. T h e red arrows and red, vertical dashed lines represent the times at which DLI were g i v e n .
T h e horizontal dash ed lines represent the low er limit o f T R E C levels in norm al individuals .
All three patients experienced increases in TREC levels after DLI. Due to the timings o f
the DLI in the patients who showed increases in TRLC it is again difficult to comment on
the role of DLI in these increases. The difficulty in interpretation arises because the
patients received a DLI between 6 and 12 months post-transplant, the time at which the
majority of patients, regardless of whether they received a DLI or not, experienced
increases in TRLC levels. It should be stated however that the data presented by Hochberg
et al. demonstrated TRLC increases in patients who had proven cytogenetic relapse, and
they speculated that the TRLC increase was not a genuine increase, but reflected
elimination of leukaemic cells with an apparent increase in TRLC frequency. The three
patients who experienced TRLC increases in this study had no evidence of relapse and
received a DLI only because they were considered at risk of relapse. Furthermore, while
the data presented by Hochberg et al. was based on TRLC frequencies, the data presented
in this study is based on absolute TRLC counts and would not be affected by elimination
of leukaemic cells. These observations lead me to conclude that the increase in TRLC
numbers was a result of normal de novo thymopoiesis and was probably not related to the
transfer of donor lymphocytes.
Pre-transplant conditioning regimens
Due to the diversity of conditioning regimens and the small number of patients within
each conditioning group (Table 4.1) it was not possible to assess the effect of each
particular conditioning regimen on thymic output and naïve T-cell recovery. However,
there were two aspects of the conditioning regimens that I was able to assess across the
105

_______________________________________________________________________________________________________________________________C h a i t e r 4
patient groups. First, whether these patients received infusions of Campath-IH as part o f
their pre-transplant conditioning regimen. Second, whether total body irradiation had an
adverse effect on thymic output. These two parameters were assessed independently o f
other pre-transplant conditioning agents.
C a m p a th - IH
Campath-IH is an antibody which binds to the CD52 antigen expressed on the surface o f
thymocytes, T and B-cells, monocytes and granulocytes (Eisner et al., 1996; Hale et at.,
1983). The Campath antibodies were originally developed as a method of GVHD
prevention in allogeneic HCT recipients. Campath-IH is a humanised version o f the
original Campath-1G antibody that induces killing of CD52" cells in vivo through
complement activation and antibody dependent cellular cytotoxicity (ADCC) (Hale et at.,
1987; Riechmann et at., 1988). There are numerous problems associated with in vivo
administration of Campath-IH which, due to its short in vivo half-life of approximately
17 days, might be expected to manifest in the short term. However, patients experience
both short term and long-term effects. In the short term, Campath-IH infusions are often
followed by fevers, rigors and nausea which are thought to result from cell activation and
cytokine release upon binding of Campath-IH to CD52"' cells. Other short-term effects
include depression o f granulocyte and platelet counts and elevation of liver enzymes. In
the longer term, Campath-IH produces a profound and often prolonged lymphopenia
characterised by low numbers o f peripheral blood CD4" and CD8^ T-cells, with CD4^ T-
cell numbers remaining below the normal range for greater than 5 years post-transplant in
some patients (Brett et at., 1996; Coles et at., 1999; Jendro et al., 1995). However,
Campath-IH has proven to be an extremely effective therapy for the prevention of GVHD
(Hale et al., 1998; Kottaridis et al., 2000).
I analysed the effects of pre-transplant infusions of Campath-1H on the recovery o f naïve
CD4^ (Figure 4.8A), and CD8^ (Figure 4.8B) T-cells at 3 months post-HCT. Median naïve
CD4^ T-cell counts at 3 months post-transplant were 28 cells per \x\ (range: 0.1 to 109) in
patients who did not receive Campath-IH compared to a median naïve CD4" T-cell count
of less than 10 cells per pi (range: 0 to 45) in patients who received Campath-IH. A
reduction in the number of naïve CD8^ T-cells was also apparent with a median naïve
CD8" T-cell count o f 18 cells per pi (range 0 to 118) in patients who did not receive
Campath-IH compared to less than 10 cells per pi in patients who received Campath-IH
(range 0 to 42). Although naïve T-cell numbers were uniformly low in these patients at 3
months post-transplant, naïve CD4^ and CD8^ T-cell numbers were significantly lower in
patients who received infusions of Campath-IH compared to those who did not (P = 0 .04
for naïve CD4" T-cells, P = 0.04 for CD8^ T-cells).
106

C h a i t i :r 4
B200
■o
100 -
?HïNz
1 0 - 1 — .
-Campath +Campath
200
100 -
1 0 -
-Campath -t-Campath
Figure 4.8: Ejfect o f Campath-1H administration on T-cell recovery at 3 months post-HCT
A bso lu te num bers o f naïve CD4" and CD8" (C D 4 5 R O CD27'") T-cells were ca lcu la ted for p a t ien ts who e i th e r
rece ived (blue t r iang les) or did not receive (purple squares) in fus ions o f C a m p a th - I H as part o f their p r e
transp lan t cond it ion ing . Data is show n for naïve CD4* (A) and naïve CD8* (B) T-cell n u m b ers 3 m o n th s p o s t -
HCT.
There was no significant difference in naïve T-cell counts from patients who received or
did not receive Campath-IH during their pre-transplant conditioning after 3 months post
transplant. This suggests that the effects of Campath-IH in this patient group were short
lived and that naïve T-cell recovery was not affected in the long-term by C am path-1H
treatment.
Campath-IH had no effect on TREC levels at any time points post-transplant suggesting
that Campath-1H infusions had no direct effect on thymic function. Therefore, Campath-
1H effects are on mature donor T-cells or residual patient T-cells.
Total body irradiation (TBI)
A recent study by Chung et al. demonstrated that the dose of radiation received by pre-
HCT patients had a significant adverse effect on thymic cellularity and thymocyte
maturation (Chung et al., 2001). Furthermore, it was suggested in this and other studies
that the defects in thymocyte maturation noted during ageing, chemotherapy, BMT and
GVHD may be related to reduced levels of IL-7 in the thymic microenvironment (Chung
et al., 2001; Mackall et al., 2001; Weinberg et al., 2001).
I therefore made a comparison between patients who received total body irradiation
against those patients who did not (as detailed in Table 4.1). Within the “No TBI” group,
there were 3 patients who received thoraco-abdominal irradiation as an alternative to TBI.
107

___________________________________________________________________________________________________________________________________________C h a p t e r 4
All three o f these patients experienced increases in numbers o f TREC and naïve T-cells
over the course of the study. Contrary to some previous concerns regarding the possibility
of thymic damage by TBI, there was no significant difference in naïve CD4^ or CD8^ T-
cell numbers or TREC levels between patients who received or did not receive TBI as part
of their pre-transplant conditioning (see Appendix, Tables A2 and A3 for P-values).
My conclusions from these results were that TBI did not damage the thymus to such a
degree that there was a significant adverse effect on T-cell development and production.
However, it should be noted that the effects of TBI were analysed in a highly
heterogeneous patient group. For this conclusion to be valid, it is necessary to assess the
effects of TBI in an age- and GVHD-matched patient group.
Im m u n o su p p ress io n
The prevention o f GVHD and graft rejection can be achieved in part by the
administration o f immunosuppressive drugs such as Cyclosporin A (CsA), FK506 and
Rapamycin. However, due to the non-specific action o f these drugs, normal immune
responses, as well as allogeneic responses, are inhibited leaving the transplant recipient
susceptible to opportunistic infections. In addition, because immunosuppressive drugs
interfere with the T-cell signalling apparatus, there may be adverse effects on thymocyte
positive and negative selection signals and T-cell production in the thymus.
Cyclosporin A
A commonly used immunosuppressive agent is CsA, a drug that inhibits the actions o f the
serine/threonine-specific phosphatase Calcineurin. CsA binds to an intracellular protein
known as Cyclophilin (CyP) and the complex of CsA-CyP binds to Calcineurin
preventing Nuclear Factor of Activated T-cells (NF-AT) activation and IL-2 synthesis
(reviewed in (Vander Woude, 1997)). CsA has also been shown to have adverse effects on
thymocyte maturation in mouse models (reviewed in (Damoiseaux et a i , 1997)).
The effects of CsA on naïve T-cell recovery and thymic output were assessed in two
groups of patients who received CsA for either 3 or 12 months post-transplant. The policy
on administration of immunosuppressive drugs within the BMT unit at the RFH is as
follows. Generally, patients who received T-cell depleted stem cell grafts did not receive
additional immunosuppressive drugs. Patients with leukaemias or malignant diseases
generally remained on CsA for a period of 3 months post-transplant. Those patients who
were at risk o f late graft rejection e.g. Aplastic and Fanconi anaemia patients, remained on
108

___________ C h m >t i ;k 4
CsA for a period of 12 months. Patients who experienced episodes of GVHD received
additional immunosuppression in the form of corticosteroids (Prednisolone,
Methylprednisolone, Mycophenolate) with or without CsA as deemed appropriate by the
clinician.
The effects of T-cell depletion were mentioned previously. Therefore, the analysis was
carried out on patients who received T-cell replete transplants and remained on CsA for a
period of 3 or 12 months post-HCT. These patients did not receive any additional
immunosuppression other than a short course of Methotrexate from day -f-1 to -t-6 post-
HCT as GVHD prophylaxis. TREC and naïve CD4" and CD8^ T-cell production was
analysed in patients who received CsA for 3 months (4.9A) or 12 months (4.9B) post-
HCT. In both patient groups, TREC levels and naïve T-cell numbers increased with time
post-transplant. However, due to the small number of patients in each group statistical
analysis was not carried out for these results. Nevertheless, this data demonstrates that
TREC levels do increase even when CsA is being administered. The differences in levels
of naïve T-cells and TREC within each group represent age-related differences in thymic
output and are common to both groups. Again, it may be necessary to analyse the effects
of immunosuppressive therapies in age-matched control groups.
B1000
5 0 0 -
£ 200
100 -
z 200 22
100 -
6 12
30 0
-200
- 100
0 I6
a
1000
5 0 0 -
1 »f 1000
20
5 0 0 -
z 200
100 -
126
3 0 0
- 200
100
3 0 0 _
- 200
- 100
6
Months post-HCT
Figure 4.9: Ejfect o f Cyclosporin A on thymic output and naïve T-cell recovery post-H C T
A bsolu te num bers o f C D 4 T R E C ( □ ) , C D 8 T R E C (■) , naïve CD4* ( O ) and naïve CD8* ( • ) T -ce l ls are s h o w n
for pa t ien ts who received T-cell rep lete grafts and rem ained on CsA for a dura t ion o f 3 m o n th s (A) or 1 2
m o n th s (B) p o s t - t r a n sp la n t . Note the dif ferences in the left and right y -axes b e tw een dif ferent p lo ts . Each
plot represen ts a d if feren t patient identified by their UPN in each plot.
109

C h a i 't i ;r 4
C or t i cos te ro ids
Corticosteroid drugs are powerful anti-inflammatory agents that are used widely to
suppress the harmful effects of GVHD and other autoimmune responses. The effects of
corticosteroid therapy are complex, commonly resulting in inhibition of the expression of
cytokines and adhesion molecules with subsequent effects on lymphocyte activation and
trafficking. In addition, corticosteroids increase endonuclease activity with effects on the
induction of apoptosis in lymphocytes and other cell subsets (Barnes and Adcock, 1993;
Cupps and Fauci, 1982). There are also numerous in vivo and in vitro reports on
corticosteroids and their analogues affecting thymocyte apoptosis and peripheral T-cell
activation events (Leposavic et al., 2001; Leussink et a i , 2001 ; Nambiar et al., 2001 ;
Olsen et al., 1998; Szondy, 1997; Van Laethem et al., 2001 ; Wiegers et al., 2001).
However, the effects of corticosteroids on thymic output and naïve T-cell recovery was
difficult to assess because, of the seven patients who received corticosteroids, six patients
had ongoing chronic GVHD and the remaining patient had autoimmune cytopenias.
Although GVHD is known to have detrimental effects on thymic architecture, the effects
of GVHD on thymic output could equally be attributed to increased thymocyte apoptosis
induced by steroid treatment. Indeed patient 183 (Figure 4.10) did not experience
increases in naïve T-cells or TREC levels (Figure 4.10A) and received corticosteroids as
treatment for autoimmune cytopenias rather than GVHD.
B200 500
IIê z 1000-
500-
1 26
Months post-HCT
Figure 4.10: Reconstitution o f naïve, memory and effector T-cell subsets in Patient 183
Absolu te num bers o f C D 4 T R E C ( □ ) , CDS T R E C (■) , naïve C D A ( O ) and naïve CDS* ( • ) T -ce l ls are s h o w n
in (A); abso lu te num bers o f m em ory C D A (A), effector C D T (0), n o n -n a ïv e CDS" (A) and C D 8 T D 5 T C D 2 8
( ♦ ) T -ce l ls are show n in (B).
no

C h a p t e r 4
However, memory and effector T-cell subsets were present at all time points after
transplant (Figure 4.1 OB). Whether the lack of increase in TREC levels was a direct result
of corticosteroid treatment or o f ongoing autoimmune disease was again difficult to
conclude. Further studies of patients who received steroid treatment in the absence o f
GVHD e.g. patients with rheumatism or chron’s disease, are necessary to evaluate the
separate contribution o f GVHD and steroids to the inhibition o f thymopoiesis.
Factors affecting the recovery of memory and effector T -ce l l subsets post-allogeneic HCT
The previous results demonstrate that there are many factors that can influence the
recovery o f naïve T-cells and thymic output after HCT even when analysed in such a
heterogeneous patient group. Previous studies from other groups, and the results
presented in Chapter 3 demonstrate that T-cell recovery in the short term is almost
exclusively of cells with a memory or effector T-cell phenotype. This observation
suggests that the initial phase of T-cell engraftment is primarily due to the proliferation o f
mature T-cells in the stem cell graft rather than the differentiation o f new T-cells from
haematopoietic progenitors. Furthermore, even though substantial numbers o f
phenotypically mature T-cells are present in the peripheral blood o f patients within 3
months after transplant, functional characterisation of these cells almost always reveals
functional impairment (Lum, 1987; Martin et al., 1987; Reusser et al., 1990; Storek et al.,
1997; Witherspoon et al., 1984). The recovery o f T-cell function (as opposed to T-cell
numbers) is thought to be reliant on the recovery, via thymic-dependent pathways, o f a
diverse pool o f naïve T-cells (Dumont-Girard et al., 1998; Roux et a i , 2000).
Nevertheless, populations of memory and effector cells are almost certainly required to
provide some protection against opportunistic infections in the short-term after transplant.
In the next section, analysis o f some of the factors that drive reconstitution of memory
and effector T-cells has been carried out.
Age o f transplant recipient
The previous results from this study demonstrated an inverse relationship o f patient age
with recovery o f naïve T-cells. It is also generally accepted that naïve T-cell numbers
decrease and memory T-cell numbers increase as part o f the normal ageing process.
Therefore analysis o f the effect o f patient age on the recovery of memory and effector T-
cells after HCT was carried out.
I l l

C H A IT I K 4
There were a higher number of memory CD4^ T-cells in the 30-53 year old patient g roup
at 3 months post-HCT with a median number of memory CD4^ T-cells of 44 cells per pi
(range; 10 to 539) in the 6-30 age group and 126 cells per pi (range: 14 to 568) in the
30-53 age group. This was statistically significant with a P-value of 0.006. However, there
were no significant differences in memory CD4" T-cell numbers between the two groups
at any other time point after transplant.
Similarly, the number of non-naïve CDS'" T-cells was also higher in the 30-53 year old
age group at 3 months post-HCT with a median number of non-naïve CDS'’ T-cells of 94
cells per pi (range: 10 to 973) in the 6-30 age group compared to 573 cells per pi (range
48 to 3699) in the 30-53 age group. The difference in number of non-naïve CD8^ T-cells
between the two age groups was significant at 3 months post-transplant (P = 0.002) and
12 months post-HCT (P = 0.013). Although median non-naïve CDS'^ T-cell counts were
higher at all time points in the older patient group, there was no statistically significant
difference at 6 or 9 months post-transplant.
B
V 1(H)
i
• •e
HKK)- • • ••
•O
••
o t l «° o o * »
, V
1(H) 1e .
• • •o
•o
•o ° 0 . . .
Oo
Oo oo •
••
• ••
anD n o n o o # Q<rD.
M onths post-H C T
Figure 4.11: Ejfect o f patient age on recovery' o f differentiated effector T-cells post-HCT
A bsolu te num bers o f effec tor CD4" T-cells (A) and CD 8"C D 57 ' 'C D 28 ' T-cells (B) were ca lcula ted . Pa t ien ts were
d iv ided into tw o groups: patients be tw een 6-30 years o f age (O ) and patients be tw een 30-53 years o f age ( • ) .
T h e larger circles represent the m edian nu m b er o f effector cel ls for each group.
Analysis of the more differentiated effector-type T-cell subsets (CD4^CD45RO"CD27 and
CD8'^CD57^CD28 ) revealed that the median number of these cells was higher in the older
(30-53 year old) patient group at all time points. The increased number of effector CD4^
T-cells in the older patients (Figure 4.11 A) was statistically significant at 3, 6 and 12
months post-transplant (P = 0.01 at 3 months, P = 0.02 at 6 months and P = 0.03 at 12
months post-HCT). The increased number of differentiated CD8^CD57'^CD28 cells in the
older patient group (Figure 4.1 IB) was also statistically significant at 3, 6 and 12 months
112

___________________________________________________________________________________________________________________________________________ C h a p t e r 4
post-transplant (P = 0.003 at 3 months, P = 0.042 at 6 months and P = 0.025 at 12
months post-HCT).
From this data, it appears that there are higher numbers of CD4^ and CD8^ T-cells that
display a memory or effector phenotype in older individuals after HCT. This data is also
consistent with the notion that thymic-independent pathways are able to restore T-cell
numbers when thymic output is absent or reduced since the older patients have reduced
levels of thymic output and naïve T-cells. Whether a feedback mechanism exists whereby
signals from an active, non-involuted thymus inhibits proliferation and expansion o f
memory and effector T-cells is intriguing, but not proven as yet. Studies by Mackall et al.
demonstrated that peripheral expansion is increased in athymic T-cell depleted mice
compared to thymus-bearing T-cell depleted mice (Mackall et at., 1996; Mackall et al.,
2001). Furthermore, subsequent analysis showed that this increased peripheral expansion
in athymic hosts was a direct result of the absence of thymic emigrants (Mackall et al.,
2001). In addition, some circumstantial evidence for this comes from patients 20, 35, 25
and 26 (detailed earlier in Tables 4.1 and 4.2) who are all less than 18 years old. These
patients have low numbers o f peripheral T-cells over the first six months post-transplant.
However, in contrast to the adults, patients 20, 35, 25 and 26 reconstitute their T-cell
compartment almost exclusively through thymic-dependent pathways with no rapid
expansions o f memory or effector T-cells. This observation suggests that the same as yet
poorly defined mechanism of T-cell regulation that has been observed in mouse models
may be active in these patients.
Graft versus host disease
The inflammatory processes that are ongoing in patients experiencing episodes o f GVHD
might be expected to have an effect on the number o f circulating memory and effector T-
cells in these patients. The results described previously demonstrated that GVHD had an
adverse effect on thymopoiesis. The reconstitution of memory and effector T-cells in
patients experiencing ongoing chronic GVHD was assessed. In contrast to the effects o f
GVHD on thymopoiesis, there was no significant difference in numbers o f memory or
effector CD4"’ or CD8^ T-cells in patients experiencing GVHD compared to patients with
no GVHD at any time post-HCT.
T-cell depletion
The results presented previously demonstrated that naïve T-cell numbers and thymic
output were significantly lower over the first 6-9 months post-HCT in recipients o f T-cell
113

_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ C H A I T E R 4
depleted stem cell grafts compared to patients who received T-cell replete grafts. The
possibility that this might be related to the ongoing processes o f homeostatic proliferation
was discussed.
In contrast to naïve T-cell recovery and thymic output, there were no significant
differences in the reconstitution of memory and effector CD4^ or CD8^ T-cells in
recipients o f T-cell depleted versus T-cell replete grafts at any time post-transplant. The
number o f T-cells transplanted with a T-cell depleted graft is significantly lower than the
number of T-cells transplanted with a T-cell replete stem cell graft. Therefore, the lack o f
difference between the two patient groups must be explained by rapid expansion o f
memory and effector T-cells in recipients of T-cell depleted transplants.
T-cell dose
Similarly, although T-cell dose appeared to have an influence on thymic output and naïve
T-cell recovery in recipients of T-cell replete stem cell grafts, there was no correlation o f
T-cell dose with memory and effector T-cell reconstitution at any time post-transplant.
Stem cell source: Peripheral blood versus bone marrow
No difference was observed in the rate of reconstitution of memory and effector T-cells in
recipients of peripheral blood or bone marrow at any time point post-transplant. As
described previously, there was no difference in the rate o f reconstitution o f naïve T-cells
or levels o f thymic output in patients who received peripheral blood or bone marrow
derived stem cells. Therefore, the reconstitution of all T-cell subsets was similar regardless
of whether patients received peripheral blood or bone marrow derived stem cells. There
are numerous other issues surrounding the use o f either peripheral blood or bone marrow
as the preferred source of haematopoietic stem cells. However, the previous observations
suggest that at least in terms of T-cell recovery, peripheral blood and bone marrow are
equally viable sources of haematopoietic stem cells.
114

C h a p t e r 4
Campath-IH
A significant effect of administration of pre-transplant Campath-IH on naïve T-cell
recovery at 3 months post-transplant was described previously. Therefore this analysis was
extended to look at the effects of Campath-IH administration on the recovery of memory
and effector T-cells.
I analysed the effects o f pre-transplant infusions of Campath-IH on the recovery o f
memory CD4^ (4 .12A) and CD8^ (4.12B) T-cells at 3 months post-HCT. Median memory
CD4* T-cell counts at 3 months post-transplant were 137 cells per pi (range: 45 to 568) in
patients who did not receive Campath-IH compared to a median memory CD4^ T-cell
count of 49 cells per pi (range: 10 to 539) in patients who received Campath-IH as part
of their pre-transplant conditioning. This reduction in memory CD4^ T-cell numbers was
statistically significant at 3 months post-transplant (P = 0.001) but there was no difference
in memory CD4^ T-cell numbers at 6, 9 or 12 months post-transplant. A reduction in the
number of non-naïve CD8^ T-cells was also apparent with a median non-naïve CD8* T-cell
count of 324 cells per pi (range 92 to 1800) in patients who did not receive Campath-IH
compared to 73 cells per pi in patients who received Campath-IH (range 10 to 3699).
Again, there was no difference in non-naïve CD8^ T-cell numbers at 6, 9 or 12 months
post-transplant regardless of whether patients received pre-transplant Campath-IH or not.
ii*
-C am path + C am p ath
B
-C am p ath -(-Campath
Figure 4.12: Ejfect o f Campath-IH administration on memory CD4* and non-naïve CD8^
T-cell recovery at 3 months post-HCT
A b s o lu te n u m b ers o f m em o ry C D T T -ce l ls (A) and n o n -n a ïv e CD8^ T -ce l ls (B) were ca lcu la ted for p a t i e n t s
w h o received (b lue t r iang les) o r did not rece ive (purp le squares) infus ions o f C a m p a th - I H as part o f the ir p r e
t ransp lan t c o n d i t ion ing . T h e b lack bars in each plot represent m ed ian va lues for each pat ien t g roup .
115

C h a i t i ; i< 4
In contrast, there was no difference in the recovery of the more differentiated effector-
type T-cell subsets (CD4TD45RO"^CD27 and CD8^CD57"^CD28 ) at any time points post
transplant whether the patients received pre-transplant Campath-IH or not.
-Campath -t-Campath
B
-Campath +Campath
-TXAà.
-Campath +Campath
Figure 4.13: Ejfect o f Campath-1H administration on reconstitution o f total CD3*, CD4"
and CDS* T-cells at 3 months post-HCT
A bso lu te num bers o f CD3* T-cells (A), CD4* T-cells (B) and CD8" T-cells (C) were ca lcu la ted for p a t ien ts w h o
e i the r received (blue tr iangles) or did not receive (purple squares) infusions o f C a m p a th - I H as part o f their p r e
t ransp lan t cond i t ion ing . T h e black bars in each plot represent m edian values for each patient group.
The recovery of total C D 3 \ CD4" and CD8^ T-cell numbers was also analysed in patients
who received or did not receive Campath-IH as part of their pre-transplant conditioning
regimen. There were significantly lower numbers of C D 3\ CD4^ and CD8'' T-cells at 3
months post-transplant in patients who received pre-transplant Campath-IH compared to
those who did not (Figure 4.13). However, similar to the naïve, memory and effector T-
cell subsets, there was no difference in total C D 3\ CD4^ or CD8" T-cell numbers in
patients who received pre-transplant Campath-IH compared to those who did not at 6, 9
or 12 months post-transplant.
These results demonstrate that of all the parameters that have been analysed separately,
administration of Campath-IH as part of the pre-transplant conditioning regimen is the
only parameter that consistently predicts low T-cell numbers at 3 months post-transplant.
116

C h a p t e r 4
Total body irradiation
The possibility was tested that total body irradiation affected the rate o f reconstitution o f
memory and effector T-cells. Similar to the recovery of naïve T-cells and thymic output,
there was no difference (at any time point) in the rate of recovery o f memory or effector
T-cells in recipients o f TBI compared with patients who received either TAI or no
irradiation in their pre-transplant conditioning protocol. Therefore, at least in this study,
TBI had no discernible effect on either naïve or non-naïve T-cell recovery in allogeneic
HCT recipients.
Im m u n o su p p ress io n
Administration of immunosuppressive agents has been generally accepted to play a role
in the functional impairment o f T-cell responses in post-HCT patients. Although
functional characterisations of T-cell responses were not carried out for the patients in this
study, the possibility that there were differences in reconstitution of memory and effector
T-cell subsets between patients who received CsA for 3 months or 12 months post
transplant was tested.
Cyclosporin A
These patients all received T-cell replete transplants and did not receive any other
immunosuppressive therapy. However, due to the small numbers of patients within each o f
these groups, it was impractical to carry out statistical analyses. Patients on CsA for 3
months and patients on CsA for 12 months post-transplant all reconstituted memory and
effector T-cells after transplant (Figure 4.14). Patients 25, 26 and 20, who remained on
CsA for 12 months, restore only low levels of memory and effector T-cells. However,
these patients are less than 18 years old and the majority of T-cells were produced via
thymic-dependent pathways. Therefore, the low numbers o f memory and effector T-cells
in these patients is probably not related to their remaining on CsA for 12 months. Also,
the remaining patients in both groups do not show a discernible difference in memory
and effector T-cell numbers that could be attributed to CsA.
117

C h a i t i . r 4
B1000-
■a 500-ZZ.9> o4a 1000-?HUo 500-?k"g 0cs 4000-oI1 2000-
37 12
' ' ' '
28
-
M
1000
2.3
12
= 1000
M onths post-H CT
Figure 4.14: Ejfect o f Cyclosporin A on memory and effector T-cell recovery post-H CT
A bso lu te num bers o f m em ory CD4" (A), effec to r CD 4" (0), non-na ïve CD8" (▲) and C D 8 X D 5 7 T D 2 8 ( ♦ ) T-
ceils are show n for pa t ien ts who rem ained on C sA for a dura t ion o f 3 m o n th s (A) o r 12 m o n th s (B) p o s t
t ransplant . Each plot represen ts a d if feren t patient identified by their UPN.
Therefore, it would appear that, similar to naïve T-cell reconstitution and thymic output,
CsA had no obvious effect on memory and effector T-cell reconstitution in this patient
group.
C o r t i co s te ro id s
As for the assessment of corticosteroid effects on thymic output and naïve T-cell recovery,
analysis of the effects of corticosteroids on memory and effector T-cell recovery in these
patients is complicated by the fact that all patients who received corticosteroids (with one
exception) were experiencing ongoing chronic GVHD. However, since there was no
difference between memory and effector T-cell recovery between patients with or without
GVHD, it is reasonable to conclude that corticosteroids did not have a significant adverse
effect on the recovery of memory and effector T-cells post-HCT.
While this conclusion may be valid, it should be noted that the lack of difference between
memory and effector T-cell reconstitution in patients with or without GVHD may be a
result of control of T-cell proliferation by corticosteroid treatment. Therefore, it is
possible that a balance has been set between cellular proliferation in response to
118

_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ C H A I N E R 4
alloantigens and steroid treatment controlling T-cell numbers through induction o f
apoptosis. Alternatively, steroid treatment may prevent activation and proliferation o f
memory and effector T-cell populations and the memory and effector T-cell populations
appear to be maintained at constant levels. Again these results highlight that immune
reconstitution is a complex process influenced by many factors. Furthermore, these results
highlight the need to assess the effects o f steroid treatment on T-cell numbers
independently of inflammatory processes such as GVHD or autoimmune diseases.
Post- t ransplant infection
Up to 30% of patients develop a life-threatening opportunistic infection after an unrelated
HCT (Davies et at., 1995; Hansen et at., 1998; Hongeng et al., 1997; Keman et al., 1993;
Marks et al., 1993; Oakhill et al., 1996; Ochs et a i , 1995), with the incidence being
somewhat lower in the related setting (Clift et al., 1994; Hongeng et a i , 1997; Marks et
al., 1993; Small et al., 1997; Snyder et al., 1993). Furthermore, in either the related or
unrelated setting, the incidence of life-threatening opportunistic infection was
significantly lower in children compared to adults (Small et al., 1999). The overall
incidence of opportunistic infections (ie taking into account life-threatening and non-life-
threatening infections) is likely to be considerably higher. In this study, 23 of 32 patients
(72%) had at least one recorded infectious episode.
Previous studies have reported elevated numbers of CD8"^CD57‘'CD28' cells in patients
post-HCT, in untreated hemato-oncological patients, ageing normal individuals and CMV
infected normal individuals or patients post-HCT (Leroy et al., 1986; Merino et a i , 1998;
Wursch et al., 1985; Yabe et al., 1990). Furthermore, CMV-specific T-cells have been
shown to reside in CD8^ T-cell subsets that display a CD8^CD57"^CD28 or CD45RA^CD27
phenotype (Kern et a i , 1999; Sandberg et a i , 2001). Therefore the effects o f post
transplant infections on the reconstitution of CD8^CD57^CD28 cells and non-naïve CD8"
T-cells were analysed along with the effects o f post-transplant infection on the
reconstitution of memory and effector CD4^ T-cells.
CMV infected individuals versus non-infected individuals:
This analysis compared memory and effector T-cell reconstitution in patients who had no
recorded incidences of opportunistic infections (n = 9) with patients who experienced one
or more CMV reactivations (n = 12). The analysis was only carried out at 3 and 12
months post-transplant because I was unable to obtain patient samples for a number of the
patients at 6 and 9 months post-transplant.
119

C h a p t e r 4
This analysis revealed no significant differences in memory and effector T-cell
reconstitution between patients who experienced one or more CMV reactivations
compared to those who had no history of opportunistic infections. The interpretation o f
this data was difficult because o f the 12 patients who experienced one or more CMV
reactivations, 6 of these patients succumbed to at least one other opportunistic infection.
In addition, previous reports demonstrated that the effects of CMV infections on T-cell
populations occur over a matter of days or weeks with expansions o f memory cells
occurring during periods of CMV reactivation followed by attrition of the responding
cells upon viral clearance (Aubert et a i , 2001). Furthermore, my analysis was based on
the reconsitution of the total memory and effector T-cell pool and not antigen-specific
responses (as measured using MHC-peptide tetramers and ELIspots). However, the fact
that there was no difference in memory and effector T-cell reconstitution between the two
patient groups suggests that post-transplant infections do not have a significant influence
on T-cell reconstitution in the longer term. It may be the case that other factors such as
age and T-cell depletion have an overwhelming influence on T-cell recovery and that
post-transplant infections do not have such a significant effect on T-cell recovery.
Therefore, the correct approach in analysing the influence of post-transplant infections on
T-cell recovery would be to reduce the number of variables and look at age-matched
control groups and recipients o f T-cell depleted and non-T-cell depleted grafts within
these groups. The small number of patients in the present study confounded this type o f
analysis.
D iscuss ion
These results demonstrate that: (1) Increasing age is a significant confounding factor on
thymic output; (2) Although the thymus is still active in older patients, thymic output is
reduced compared to young adults and children; (3) Extended periods o f GVHD, or
immunosuppressive therapy for the treatment of GVHD, has an adverse effect on thymic
output, with few or no TRECs detected in these patients; (4) T-cell depletion and/or pre
transplant Campath-IH administration predicts low naïve T-cell numbers during the early
(less than 9 months) post-transplant period but probably does not affect thymic output
per se\ (5) Campath-IH administration but not T-cell depletion consistently predicts low
memory and effector T-cell numbers at 3 months post-transplant; (6) In this patient
cohort neither immunosuppressive therapy or infections have significant effects on
thymic output or memory and effector T-cell reconstitution possibly due to the
heterogeneity of the patient group.
120

________________________________________________________________________________________________________________________________ C h a p t e r 4
These results confirm previous suggestions (Weinberg et al., 2001) that age alone is a
crucial factor determining the contribution of thymic output to T-cell recovery post-HCT.
An age-related decline in T-cell function has been described in a variety o f clinical
settings (Atkinson et at., 1982; Connors et at., 1997; Forman et a i , 1982; Jendro et al.,
1995; Mackall et al., 1994) and as part of the normal ageing process (Globerson, 1995;
Globerson and Effros, 2000; Timm and Thoman, 1999). This decline in T-cell function
has been linked to the involution of the thymus that begins as early as one year of age
and continues throughout life (George and Ritter, 1996; Kendall et a l , 1980; Steinmann
et al., 1985). This involution is characterised by a reduction in thymus size and weight (as
a consequence of progressive loss of both lymphoid and stromal cells) and the gradual
replacement of thymic tissue with adipose tissue (Hollander, 1997). Although several
hypotheses have been put forward to explain age-related thymic involution (reviewed in
(George and Ritter, 1996)) the exact mechanism remains unclear. Nevertheless, the effect
of increasing age on reduced TREC levels in this study is almost certainly related to age-
associated thymic involution.
Patients who experienced ongoing episodes of chronic GVHD with or without prior acute
GVHD did not experience a rise in TREC levels, and as a result did not reconstitute the
naïve T-cell compartment for the duration of the study. This suggests that either chronic
GVHD, or the immunosuppressive drugs used in its treatment, have an adverse effect on
thymic output.
It is essential to the development of a diverse T-cell compartment, with the capability o f
responding to thousands o f environmental antigens that both thymic-dependent and
thymic-independent pathways work together. Therefore, in situations where one of the
pathways is compromised e.g. loss of thymic output in patients with chronic GVHD, the
recovery o f a normal diverse T-cell compartment could be delayed, possibly for many
years after transplant.
It is well documented that the thymus is a target organ in GVHD. It has also becom e
apparent that thymic damage by alloreactive T-cells may play an important part in the
pathology and development of GVHD (Fukushi et a i , 1990; Hollander et al., 1994; van
den Brink et a i , 2000). The pathology of thymic damage during GVHD includes
elimination o f CD4^CD8' (DP) thymocytes and mature CD4^ (SP) thymocytes, thymic
dysplasia, depletion o f cortical and medullary thymocytes, epithelial cell destruction and
loss o f Hassals bodies (Muller-Hermelink et al., 1987; Ferrara et al., 1991; Ghayur et al.,
1988). With this destruction o f thymic tissue, the impact on the immune system in post
transplant patients includes T-cell lymphopenia with prolonged immunodeficiency and
lack o f appropriate thymic education which results in the appearance o f autoreactive T-
cell clones (Brochu et a i , 1999; Dulude et a i , 1999; Fukushi et al., 1990; Hollander et
al., 1994; Krenger et al., 2000; van den Brink et al., 2000).
121

C h a p t e r 4
The results from this study together with the evidence of GVHD-mediated thymus
damage indicate that the thymus is unable to contribute to T-cell reconstitution in post
transplant patients with chronic GVHD. There is some evidence that upon resolution o f
GVHD, thymic architecture can be restored and thymic education of T-cell progenitors is
able to take place (Ghayur et al., 1988; Hakim et al., 1994). This observation suggests
that therapeutic intervention aimed at reactivating thymic-dependent pathways after
resolution o f GVHD might be successful.
It is also possible that steroid treatment and immunosuppressive drugs used in the
treatment of GVHD had an adverse effect on thymic output. There are numerous in vivo
and in vitro reports on corticosteroids and their analogues that effect thymocyte apoptosis
and which also have adverse effects on peripheral T-cell activation events (Leposavic et
al., 2001; Leussink et a i , 2001; Nambiar et al., 2001; Olsen et al., 1998; Szondy, 1997;
Van Laethem et al., 2001; Wiegers et al., 2001). However, it was not possible to assess the
separate contribution of steroids and GVHD to reduced thymic output due to the small
number of patients in the study. A previous study by Wienberg et al. demonstrated that
TREC levels increased in cord blood transplant recipients even while receiving low-dose
steroids as GVHD prophylaxis (Weinberg et al., 2001). However, their data does not
exclude the possibility that high dose corticosteroids used in GVHD treatment would have
an adverse effect on thymic output.
The effect of the immunosuppressive drug CsA on thymic output appears to be minimal
as demonstrated by a number o f patients who remained on CsA for the duration o f the
study but still experienced rises in TREC levels. However, it is difficult to comment further
due to heterogeneity in the patient groups. It was not possible to compare patients who
received CsA with those who did not because the only patients who did not receive CsA
received T-cell depleted grafts.
Since the early post-transplant period is characterised by a profound immunodeficiency,
it should be beneficial to the transplant recipient to rapidly reconstitute a fully functional
immune system. The recovery o f a self-restricted, diverse T-cell repertoire is dependent
on thymic production o f T-cells from haematopoietic progenitors. Therefore, it is
necessary to consider therapeutic approaches that would facilitate faster immune
reconstitution in recipients of HCT. It is known that GVHD is detrimental to both thymic-
dependent and thymic-independent pathways, therefore GVHD prevention (with the
maintenance o f the GVL effect) remains an important goal. Since the adult thymus is still
capable of producing new T-cells, there is the potential to increase thymic output by
intervention with therapeutic agents. A number of studies have demonstrated increased
thymopoiesis by administration of IL-7 (Andrew and Aspinall, 2001; Bolotin et a i , 1996;
Mackall et al., 2001). IL-7 has been shown in these studies to reduce thym ocyte
122

___________________ C h a p t e r 4
apoptosis, normalise thymic cellularity and as a consequence, increase thymic output.
Other agents that may have a protective effect against or reverse thymic involution include
Leptin (Howard et al., 1999), Tamoxifen (Sfikakis et al., 1998), Tachykinins (Gehme et
al., 1987) and a combination of Keratinocyte Growth Factor (KGF) and IL-7 (Min et al.,
2000)
123

C h a î n e r 5
C h a p t e r 5
Cord blood immunobiology and transplantation
Introduction
The results from Chapter 4 demonstrated that GVHD (or immunosuppressive GVHD
therapy) has an adverse effect on thymic output and delays effective reconstitution of the
T-cell compartment. Since the first cord blood (CB) transplant in 1988, human umbilical
CB has been successfully utilised as an alternative stem cell source to allogeneic bone
marrow or peripheral blood for the treatment o f haematological disorders in children
(Gluckman et al., 1989; Gluckman et al., 1997; Pahwa et a i , 1994; Wagner et al., 1996).
The results of CB transplants performed to date suggest a reduction in GVHD compared
with BM and PBSC transplants (Balduzzi et al., 1995; Cairo and Wagner, 1997; Wagner et
al., 1995). This suggestion, together with other potential advantages of CB transplantation,
has led to considerable interest in CB research.
There have been numerous hypotheses to explain the apparent reduction in GVHD after
CB transplant compared with BM or PBSC transplants. The most popular theory holds
that the CB immune system is naïve and has not been primed to the majority o f
environmental antigens. This naivety is apparent in most of the haematological lineages
including T-cells (summarised in Tables 5.1 and 5.2), B-cells (Garban et al., 1996; Tucci
et al., 1991), NK cells (Dominguez et al., 1998), monocytes (Taylor and Bryson, 1985),
neutrophils (Reddy et al., 1998) and dendritic cells (Hunt et al., 1994).
The majority o f studies have highlighted the phenotypic and functional immaturity of CB
T-cells. Almost all cord blood T-cells express the CD45RA isoform (Table 5.1) whereas
adult T-cells express either CD45RA or CD45RO with the ratio of CD45RA:CD45RO
decreasing with increasing age. In addition, the majority o f CD45RA"^ CB T-cells express
CD38 (Berry et a i , 1992; Rabian-Herzog et al., 1993) while the expression of CD38 on
adult T-cells is restricted to cells with a CD45RO'’ or activated phenotype. Also, adult T-
124

___________________________________________________________________________________________________________________________________________C h a p t e r 5
cells (particularly CD45RO) express the CD29 antigen whereas CD29 expression is either
low or undetectable on cord blood T-cells (Berry et a i , 1992; Rabian-Herzog et al.,
1993). These observations have led to the suggestion that CB CD45RA^ T-cells may be
more immature than their adult CD45RA^ counterparts and are phenotypically similar to
medullary single positive thymocytes.
In terms of functional responses, CB T-cell function has been measured in numerous
studies using readouts such as proliferation, cytokine production and transcription factor
induction to a variety of stimuli. The production of cytokines in response to these stimuli
is summarised in Table 5.2. Studies on the expression of IL-2 by CB and adult T-cells
have yielded conflicting results. It might be expected that, since CB has a higher
proportion of T-helper cell precursors, IL-2 expression would be increased in CB
compared with adult T-cells, but this does not appear to be the case. Generally, cytokine
production and functional responses of CB T-cells are reduced compared to their adult
counterparts, particularly in the expression o f cytokines that are characteristically
expressed by differentiated ThI or Th2 cells (IFN-y and IL-4 respectively). There have
been no reports to date of CB T-cells having an increased production of cytokines
compared with their adult counterparts again highlighting the immaturity o f the CB
immune system.
In addition to these previous observations, preliminary data from our laboratory
suggested that the environment from which CB T-cells are derived {i.e. CB serum) may
influence aspects of the cells phenotypic and functional characteristics (Cohen et al.,
2000). Indeed a number o f immunosuppressive soluble factors have been identified in CB
serum (See Table 5.3). These are too numerous to be described in detail but IFN-a, TGF-
P and M-CSF have all been described to have immunosuppressive effects.
The rationale for these experiments arose from the concept o f viviparity and maternal
tolerance to the allogeneic foetus, but the concepts can equally be applied to other
allogeneic tissue grafts. The mechanisms regulating the immunological acceptance of the
allogeneic embryo leading to successful establishment of pregnancy, and indeed the
general mechanisms of tolerance induction, are not well understood. Clearly, the
development of tolerance in the allogeneic HCT setting is critical for post-transplant
recovery and the establishment of a functional immune system. Therefore, the first aim o f
the work presented in this chapter was to assess whether the function of adult cells was
modified by stimulation in the presence of CB serum and whether CB serum contained
soluble factors that could inhibit cellular responses.
There are a number o f other issues surrounding the use of CB as an alternative to bone
marrow and peripheral blood stem cells. One concerning issue is that the processing o f
cord blood units results in significant cell losses compared to BM and PBSC harvests
125

______________________________________________________________________________________________________________________________________ C h a it e r 5
(Abboud et a i , 1992; Broxmeyer et al., 1989) and that this may have an adverse effect on
engraftment in the short term (Cairo and Wagner, 1997) and immune reconstitution in the
longer term. Although CB is often used as a last resort when HLA-matched related or
unrelated donors are not available, it is essential that CB rapidly reconstitute a functional
immune system. To date, only a few studies have analysed immune reconstitution after
cord blood transplantation (Niehues et al., 2001; Talvensaari et al., 2002; Weinberg et al.,
2001). Therefore, the second aim of this work was to assess reconstitution of the T-cell
compartment in recipients of cord blood transplants and relate this to the results from the
patients described in Chapter 4.
126

C h a i t i : i< 5
Table 5.1: Phenotypic differences between cord blood and adult T-cells
A n t i g e nMean of the
cells expressing Cord blood
percentage of ant igen ± SD
Adult blood
Cord bloodco m pa redwi t hadul t blood
Re f
CD45RA 22.1 ± 2 .5 14.6 ±7.1 CB > AD (Rabian-Herzog er o/., 1993)77 ± 4 42 ± 5 CB > AD (Han er «/., 1995)82 48 CB > AD (Beck et al.. 1994)87.6 ± 5.2 44.8 ± 9 .6 CB > AD (D'Arena et a!.. 1998)31 ± 10 21 ± 7 CB > AD (Berry et a!., 1992)32 ± 1 33 ± 1 No difference (Mills et al.. 1996)84 ± 6 53 ± 20 CB > AD (Harris et c;/., 1992)
CD45RO 32 ± 5 68 ± 2 A D > C B (Han et al.. 1995)16 49 A D > C B (Beck et al.. 1994)12.3 ± 5 .2 55.2 ± 9 .6 A D > C B (D'Arena et al.. 1998)2 25 ± 2 A D > C B (Mills et al.. 1996)
CD38 59 ± 8 21 ± 12 CB > AD (Berry et al., 1992)79.0 ± 10.2 54.0 ± 8.7 C B > AD (Rabian-Herzog et al.. 1993)90 50 CB > AD {Beck et al.. 1994)90 50 CB > AD (D'Arena et al.. 1998)
CD2 72.8 ±7.1 76.6 ±9.1 No difference (Han et al.. 1995)57.4 ± 10.0 78.7 ± 5.4 A D > C B (Rabian-Herzog et al.. 1993)
CD3 59.9 ± 12 74.9 ± 4 .6 A D > C B (D'Arena et o/.. 1998)44.8 ± 13.3 7 1 .9 ± 6 .7 A D > CB (Rabian-Herzog et al.. 1993)62 ± 10 69 ± 7 No difference (Berry et al.. 1992)61.3 ±8.5 70.6 ± 6 .2 A D > C B (Han et al.. 1995)28 ± 1 43 ± 2 A D > C B (Mills et al.. 1996)4 0 ± 1 62 ± 11 A D > C B (Harris et al.. 1992)
CD4 26 ± 1 30 ± 1 No difference (Mills et al.. 1996)48 ± 8 53 ± 7 No difference (Berry et al.. 1992)43.8 ± 5.6 46.1 ± 9 .3 No difference (Han et al.. 1995)31.0 ± 10.8 42.4 ± 7 .2 A D > C B (Rabian-Herzog el al.. 1993)29 ± 13 38 ± 9 AD > CB (Harris et al.. 1992)
CD5 73.1 ± 7 .7 69.2 ± 6 .4 No difference (Han et al.. 1995)58.2 ± 1 1.9 77.2 ± 5 .8 A D > C B (Rabian-Herzog et t//., 1993)
CD7 68.0 ± 12.3 74.1 ± 6 .6 No difference (Rabian-Herzog et al.. 1993)
CDS 11 ± 1 24 ± 2 A D > CB (Mills et tt/., 1996)25 ± 6 24 ± 7 No difference (Berry et o/., 1992)33.9 ± 7.9 31.9 ± 6 .8 No difference (Han et al.. 1995)26.4 ± 6.6 32.1 ± 6.3 A D > CB (Rabian-Herzog et al., 1993)1 7 ± 7 22 ± 6 A D > C B (Harris et al.. 1992)
CD25 2 ± 0 .2 2.5 ± 0.5 No difference (Mills et o/.. 1996)4.1 ± 1.4 9.1 ± 5 . 0 A D > C B (Rabian-Herzog et o/., 1993)
CD29 3 ± 1 24 ± 9 A D > CB (Berry et a i . 1992)4.6 ± 1.8 22.7 ± 5.7 A D > C B (Rabian-Herzog et a i . 1993)
1L-2R Y chain 6.34 ±2 .01 17.97 ± 2 .7 4 A D > C B (Saito et a i . 1996)
T C R a p 28 ± 1 39 ± 2 A D > C B (Mills et o/., 1996)6 1 . 4 ± 9 .4 66.5 ± 7.3 No difference (Han et a i . 1995)43.6 ± 12.2 68.8 ± 6 .4 A D > CB (Rabian-Herzog et a i . 1993)
TCRy6 <1 <1 No difference (Mills et o/., 1996)1.2 ± 0 . 6 3.7 ± 2.9 No difference (Han et a i . 1995)
This table compares the results from different studies that have highlighted phenotypic differences between cord blood and
adult T-cells. The results are summarised indicating whether the surface expression o f different antigens (represented as
mean ± standard deviation, SD) is greater in cord blood than in adult blood (CB > AD) or vice versa (AD > CB).
127

C h a i 'TI-r 5
Table 5.2: A comparison of cytokine production by CB and adult T-cells
Cvtokine Stimulus” Assay'' Adult versus CB R e fe r e n c e
lL-2 Anti-CD3 ELISA, mRNA CB < AD (Benotto cr «/., 1990)Anti-CD3 -t- PMA ELISA, mRNA CB = AD (Beitotto er al., 1990)PMA +A 2 3 1 8 7 ELISA, mRNA CB = AD (Beilotto cf (//., 1990)PHA ELISA, mRNA CB = AD (Bertotto e t a!., 1990)PMA + lonomycin mRNA CB = AD (Lewis et a!.. 1991)Anti-CD3-r PMA mRNA CB = AD (Lewis et a!., 1991)ConA -r PMA mRNA CB = AD (Lewis et al.. 1991 )PHA, KLH ELISA, mRNA CB < AD (Hassan and Reen, 1997)LPS + PHA ELISA CB = AD (Sautois et al.. 1997)PHA ELISA, mRNA CB = AD (Pirenne-Ansart cf a/., 1995)Anti-CD3, anti-CD2 ELISA, mRNA CB < AD (Pirenne-Ansart cf r//., 1995)TPA -t- A23187 CB < AD (Matsuzaki et al.. 1989)Anti-CD2 -r Anti-CD28 ELISA, mRNA CB < AD (Hassan et al.. 1995)PMA -t- lonomycin Intracellular staining CB < AD (Chalmers et al.. 1998)Anti-CD2 ELISA CB < AD (Gerli et al.. 1993)Alloantigen HTLp CB = AD (Cohen et al.. 1999)Freezing/alloantigen ELISA CB < AD (Cohen et al.. 1999)Alloantigen ELISA CB < AD (Risdon et al., 1994)
lL-4 PMA + lonomycin ELISA, mRNA CB < AD (Lewis et al.. 1991 )Anti-CD3 -r PMA ELISA, mRNA CB < AD (Lewis et al.. 1991)ConA + PMA ELISA, mRNA CB < AD (Lewis e t al.. 1991)LPS + PHA ELISA CB < AD (Sautois et al., 1997)PMA + lonomycin Intracellular staining CB < AD (Chalmers et al.. 1998)Alloantigen ELISA CB < AD (Risdon et al.. 1994)
IFN-y PMA + lonomycin ELISA, mRNA CB < AD (Lewis et al.. 1991 )Anti-CD3 + PMA ELISA, mRNA CB < AD (Lewis et al.. 1991)ConA -H PMA ELISA, mRNA CB < AD (Lewis et al.. 1991)LPS + PHA ELISA CB < AD (Sautois et al.. 1997)Anti-CD3 ELISA, mRNA CB < AD ( Pirenne-Ansart er «/., 1995)Anti-CD2 ELISA, mRNA CB < AD (Pirenne-Ansart et al.. 1995)PHA ELISA, mRNA CB < AD (Pirenne-Ansart et al.. 1995)PMA + lonomycin Intracellular staining CB < AD (Chalmers et al.. 1998)Alloantigen ELISA CB < AD (Risdon et al.. 1994)
lL-3 LPS + PHA ELISA CB = AD (Sautois et al.. 1997)Anti-CD3 ELISA, mRNA C B < AD (Pirenne-Ansart et al.. 1995)Anti-CD2 ELISA, mRNA CB < AD (Pirenne-Ansart é ta l ., 1995)PHA ELISA, mRNA CB < AD (Pirenne-Ansart et al.. 1995)
IL-6 LPS -H PHA. ELISA CB = AD (Sautois et al.. 1997)
TGF-P PMA + PHA. ELISA, mRNA CB < AD (Chang et al.. 1994)
TN F-a PMA + ionomycin Intracellular staining CB < AD (Chalmers et al.. 1998)
The level o f cytokine production by adult and CB T-cells has been indicated as a direct comparison between the two. To date
there have been no reports that cytokine production by CB T-cells was greater than adult T-cells.
PMA = phorbol-12-myristate 13-acetate; PHA = phytohaemagglutinin; Con A = concanavilin A; KLH = keyhole limpet
haemocyanin; LPS = lipopolysaccharide; TPA = tissue plasminogen activator.
ELISA = enzyme-linked immunoadsorbant assay; mRNA was detected by Northern blot analysis or by PCR; HTLp = T-
helper lymphocyte precursor assay.
128

C h a i ' t i ;r 5
Table 5.3: Soluble factors detected in adult and CB sera
Factor Adult serum CB serum Reference
IF N -a Detected Detected (E b b esen et al., 1995)
IFN-p Detected Detected (E b b esen et a!., 1995)
I L - i p Detected Detected (Sa la fia et al., 1997)
IL-3 Detected Detected (W estg ren et al., 1995)
IL-4 Not done Detected {Hata et al., 1997)
lL -6 Detected Detected (W estg ren et a i , 1995)
1L-IÜ Detected Undetected (C o h en et al., 2000)
T N F - a Not done Detected ( H a i a e t a l . , 1997)
S C F Detected Detected (W estg ren et al., 1995)
M -C S F Undetected Detected (C ohen et al., 2000)
G M -C S F Undetected Detected ( W es tg ren et al., 1995)
Solub le H L A c lass 1 Detected Detected (R u ss w u rm et al., 1997)
Solub le H L A class 11 Detected Detected (R u ss w u rm et al., 1997)
1.2 5 -D ih y d ro x y v i i a m in D Detected Detected (Se ino et a l., 1982)
T h y r o g l o b u l i n Detected Detected (Sulov ic et a l. , 1984)
R everse T 3 Detected Detected (Su lov ic et a l., 1984)
T h y ro id - s t im u la t in g h o rm o n e Detected Detected (Sulov ic et a l., 1984)
T h y r o x i n e Detected Detected (Sulov ic et a l., 1984)
Solub le ICAM -1 (C D 45) Detected Detected ( Krauss et al ., 1998)
Solub le V C A M -1 (C D 106) Detected Detected (K rauss et al., 1998)
S olub le E -se lec t in (C D 62E ) Detected Detected (K rauss et al., 1998)
H y p o x a n t h i n e Detected Detected (L ip p -Z w a h le n et al., 1983)
L F S -b in d in g p ro te in Detected Detected (R o o s et al., 1997)
S olub le C D 14 recep tor Detected Detected (R o o s et al., 1997)
A n t i -G M -C S F Detected Detected (R ev o l te l la et al., 1997)
A n t i -G -C S F Detected Detected (R ev o l te l la et al., 1997)
C C I 6 Detected Detected (De Jo n g h et al., 1998)
IFN = interferon; IL = interleukin; TNF = tumour necrosis factor; SCF - stem cell factor; M-CSF = macrophage colony
stimulating factor; GM-CSF = granulocyte/macrophage colony stimulating factor; ICAM = Intercellular adhesion molecule;
VCAM - vascular cell adhesion molecule; LPS = lipopolysaccharide; G-CSF = granulocyte colony stimulating factor; CCI6 =
Clara cell protein.
129

C h a p t e r 5
RESULTS
Cord Blood (CB) Immunobiology: The CB microenvironment
As mentioned previously, an increasing number of studies have highlighted the
phenotypic and functional immaturity of the CB immune system. The majority o f these
studies have focused on the differences in the cellular components o f CB compared to
adult peripheral blood. In the following experiments, adult PBMCs or T-cells were
stimulated in the presence of CB or adult serum and their functional responses were
measured. Due to time restrictions, these experiments were not extended to analyse the
functional responses o f CB T-cells. The aim of these experiments was to assess whether
the CB microenvironment (CB serum) induced different functional responses (of adult
cells) compared with adult serum.
The effect o f adult and CB serum on the mixed lymphocyte reaction
The induction o f GVHD in patients after an allogeneic HCT is essentially an
immunological response of the transfused cells against the patient’s tissues. The most
physiologically relevant in vitro model of the post-HCT milieu is the mixed lym phocyte
reaction (MLR). Using this system it is possible to analyse functional responses of PBMC
populations using either fully HLA-disparate cell populations or using cell populations
mismatched at one or more HLA-loci. The concerns in these experiments were not with
the effects of individual HLA-antigen mismatches. Therefore, all MLR experiments
described in this report were carried out using non-tissue-typed PBMC populations.
To test whether differences were apparent between CB and adult serum in their abilities to
sustain the MLR, adult PBMCs were stimulated using irradiated allogeneic stimulator cells
in the presence o f CB or adult serum (Figure 5.1). Neither adult nor CB serum was able to
sustain proliferation o f the PBMC population at serum dilutions o f 1:100 or more.
However, at dilutions less than 1:100, all adult serum samples enhanced the alloresponse
by varying levels. CB sera also enhanced proliferation at dilutions less than 1:100 but the
response was always lower than with adult serum. The difference between proliferation in
the presence of CB and adult serum was significant at both 1:10 and 1:4 serum dilutions.
Therefore, although proliferation o f adult PBMCs in response to allostimulation occurred
in the presence o f CB serum, this proliferation was significantly lower than with adult
serum.
130

C h a i >t i ; i< 5
8 0 0 0 1
3 6 0 0 0 -
c a 4 0 0 0 -
^ 2000-
O g 8 O
Serum dilutions
Figure 5.1: Allogeneic stimulation of PBMCs in the presence o f adult and CB serum.
Adult P B M C s (responder cells) were incubated with irradiated al logeneic P B M C s ( s t im u la to r cells) at a r a t io
o f 2:1 (1 X 10' : 5 x 10'* cells /well) with varying concen tra t ions o f adult and CB sera. T h is f igure d e m o n s t r a t e s
pro lifera t ion o f P B M C popula tions s t im ula ted in the presence o f adult (A) or cord b lood (B) sera measured b y
incorpora t ion o f 'H - thym id ine . (C) M ean 'H - thym id ine incorpora t ion o f P B M C s in cuba ted in all adult ( □ ) and
C B ( ■ ) sera. T h is f igure is represen ta t ive o f 5 exper im en ts each con ta in ing be tw een 8 and 10 se rum sa m p le s .
Levels o f s ig n i f ican ce are represented as **P< 0 .005 , ***P< 0 .0 0 0 5 c o m p a r in g adult and hum an sera b y
S tu d e n t ’s t-test.
The effect of adult and CB serum on the proliferation of human T-cel l
l in es
Although the MLR could be considered the most physiologically relevant in vitro model
of the allogeneic transplant setting, the incorporation of ' H-thymidine is a marker o f
overall proliferation and reflects proliferation of all cell types within the PBMC
population. Therefore, I proceeded to analyse the activation and proliferation of a pure
population of T-cells {i-e. T-cell lines, which were greater than 90% CD3^ see Chapter 2:
Materials and Methods) in the presence of CB or adult serum. A variety of different
stimuli were tested.
The proliferation of a human T-cell line in response to immobilised anti-CD3 in the
presence of either CB or adult serum is shown in Figure 5.2. Since the T-cell lines used in
these experiments represent a population of activated cells, there was always a baseline
proliferative response in the absence of either cord or adult serum. Nevertheless, the
proliferative response of the T-cell line was increased with increasing concentrations o f
adult serum, while CB serum had no effect. This difference in proliferation between CB
131

_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ C h a i t i :r 5
and adult serum was significant at serum dilutions 1:200, 1:20, and 1:2. Therefore, when
activated T-cells were stimulated through their T-cell receptor (by CD3 cross-linking),
adult serum was able to enhance activation and act as a growth factor whereas CB serum
was not.
B•5
Hi lg*X
90000-1
8 0 0 0 0 - T7 0 0 0 0 - /6 0 0 0 0 -
*i/I5 0 0 0 0 -
4 0 0 0 0 -
3 0 0 0 0 -
20000 -1 ...............1 1 1 1
Serum dilutions
Figure 5.2: Ejfect of different sera on the mitogen specific proliferation o f a T-cell line
A pred e te rm in ed opt im al concen tra t ion o f an t i -CD 3 an t ibody was im m o b i l i s e d in the a p p ro p r ia te n u m b er o f
wells in a 96 well plate. T o each well, 2x10 “ viable T cells were p lated in RPM l 1640 with an t ib io t i c s in th e
p resence or absence o f adult (O ) or CB ( ■ ) sera. Results are expressed as the m ean o f 8 adult o r 8 CB sera + SD.
T h is f igure is represen ta t ive o f 3 exper im ents . Levels o f s ignif icance are represen ted as * P < 0 .0 5 , * * P < 0 . 0 0 5
c o m p a r in g adult and hum an sera by S tu d en t ’s t-test.
Since the T-cell lines used in the previous experiment represented an activated T-cell
population, I also analysed the effect of CB and adult serum on the IL-2 specific response
(Figure 5.3). In the absence of IL-2 and serum there was no proliferation of the T-cell
line on day 3 post-stimulation (data not shown). However, there was significant
proliferation on day 3 post-stimulation of the T-cell line in the presence of IL-2 but in the
absence of serum. This was not unexpected since the requirements for proliferation of an
activated T-cell population are less stringent than for a resting T-cell population. With the
addition of increasing concentrations of adult serum (Figure 5.3A) there was no
augmentation of IL-2 specific proliferation. Unexpectedly, the addition of increasing
concentrations of CB serum significantly enhanced the proliferation of the T-cell lines
reaching a maximal proliferation at a serum dilution of 1:100. The differences in the
132

_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ C h a i t ~i : r 5
proliferative responses in the presence of CB and adult serum were significant at dilutions
below 1:1000. This result was unexpected since stimulation in the presence of CB serum
in the MLR and using anti-CD3 antibody stimulation had resulted in a significantly
reduced response in the presence of CB serum compared to adult serum.
25000-1
20000 -
s 15000-
g -S 10000-
5 0 0 0 -
ooo
!l2 5 0 0 0 1
20000 -
1 5 0 0 0 -
10000 -
5 0 0 0 4
Serum dilutions
Figure 5.3: Ejfect o f different sera on the IL-2 specific proliferation o f a human T cell line
H u m an T cells w ere p lated at 5 x 10^ cells /well in 96 well plates with vary ing c o n c e n t r a t io n s o f adult and CB
sera plus lO ng/m l r lL-2. The g rap h s d e m o n s t r a te H th ym id ine in c o rp o ra t io n o f IL-2 st im ula ted T c e l l s
incubated with individual adult (A) and CB (B) sera. (C) M ean th ym id ine in c o rp o ra t io n o f all adult ( □ ) and
CB ( ■ ) sera + SD. T h is figure is representa t ive o f 1 o f 5 exper im ents . L evels o f s ign if icance are represen ted as
* P < 0 .05 . **P< 0 .005 co m p ar in g adult and h u m an sera by S tu d en t ’s t-test.
133

C h a i t u k 5
To further investigate this increased response of activated T-cells to IL-2 when incubated
in the presence of CB serum compared with adult serum, I decided to analyse the
expression of components of the IL-2 receptor complex. Specifically, I wanted to test
whether stimulation in the presence of CB serum affected CD25 expression on T-cells.
The expression o f CD25 on adult PBMC following stimulation in th e
presence o f adult and CB serum
Adult PBMCs were activated in the MLR in the presence or absence of different dilutions
of adult or cord blood serum samples for 6 days. On day 6 post-stimulation, PBMCs were
stained using fluorescent-labelled antibodies against CD3 and CD25 then analysed using
flow cytometry (Figure 5.4).
20
QU BC 15
I£I 104H‘o
Î .
P<0.01 P<0.02
1 :1 0 0 1 :1 0 0 0
• ••
. ^•
O
Serum
Figure 5.4: Expression of the lL-2 receptor a chain (CD25) on adult PBMC's following
allostimulation in the presence of adult and CB sera
Adult P B M C s ( responder cells) were incubated with or w ithou t irradiated a l lo g e n e ic P B M C s ( s t im u la to r
cells) at a rat io o f 2:1 in the presence o f different c o n c e n t ra t io n s of adult (O) or CB ( • ) sera. T he ce lls were
incuba ted in a hum id if ied ch am b er at 37°C in 5% CO, for 6 days. C e lls were then doub le -s ta in ed for C D 3 and
C D 2 5 and su bsequen t ly analysed by flow cy tom etry . Results are expressed as the p e rcen tag e o f CD3* c e l l s
that exp ress C D 23 . T h is figure is rep re sen ta t iv e o f 3 e x p e r im en ts . S ta t is t ica l a n a ly s e s were carried out
c o m p a r in g cells incuba ted in adult and hum an sera by S tu d en t ’s t-test.
134

C h a it l r 5
For both serum dilutions analysed (1:100 and 1:1000) there was a statistically significant
difference in CD25 expression between T-cells stimulated in the presence of CB or adult
serum. Therefore, incubation of adult PBMCs in the presence of CB serum significantly
enhanced CD25 expression on T-cells compared to cells stimulated in the presence o f
adult serum.
Allostimulation in the MLR is a weaker stimulation than that achieved using mitogens
such as anti-CD3 and PHA. Therefore, the following experiment was carried out to assess
whether CD25 expression also differed between T-cells stimulated using PHA in the
presence of CB or adult serum. In addition, CD25 expression was measured over a time
course from 0-168 hours post-stimulation.
100
i0£ 80 - e
as
6 0 -
?H
C 4 0 -
Ë&
01 10 100 1000
P-vahies
2 h r = 0.0039 6 h r = 0.0052 168 h r = 0.0007
0 1
Tim e (hours)
T r10 100 1000
Figure 5.5: The ejfect of different sera on CD25 expression on T-cells stimulated with PHA
1x10 ' adult periphera l b lood m o n o n u c lea r ce lls were p lated per well in a 96-w el l plate. C e lls were s t im u la te d
w ith a p re -de te rm ined optimal d i lution o f P H A (1 :1000) and incuba ted in a 1:100 d ilu t ion o f adult (A) or C B
(B) sera at 37°C in 5% C O ,. At d ifferent t ime po in ts , a plate was rem oved and the cells s ta ined u s in g
f luo rescen t labelled a n t ibod ie s aga ins t CD3 and C D 25. The cells were su bsequen t ly ana lysed by f low
c y to m e t ry . Results are p resented as the percen tage o f CD3* cells that exp ressed C D 2 5 . S ta t is t ica l a n a l y s e s
w ere carr ied out co m p ar in g ce lls incubated in adult and CB by S tu d en t ’s t-test.
135

C h a p t e r 5
Adult PBMCs were simulated using PHA (in the presence o f a 1:100 dilution o f CB or
adult serum) and the expression of CD25 on CD3" gated cells monitored over a time
course of 0-168 hours (Figure 5.5). Similar to allostimulation, there was an increased
expression of CD25 on the T-cells incubated in CB serum compared to cells incubated in
adult serum. Statistically significant differences were apparent at 2, 6 and 168 hours post
stimulation. Therefore, regardless of the method of stimulation, CD25 expression was
significantly upregulated after stimulation of PBMCs in CB serum compared with adult
serum.
I then decided to analyse whether the increased proliferation in response to IL-2
stimulation and increased expression of CD25 also resulted in increased IL-2 production
by stimulated T-cell populations.
The effect o f adult and CB serum on IL-2 production from T-cells in a
stim ulated PBM C population
IL-2 production from T-cells within adult PBMC populations was measured after a 24-
hour stimulation using PHA in the presence of either CB or adult serum (carried out by
Dr Katarzyna Bogunia-Kubik at the Anthony Nolan Research Institute using an IL-2
ELISA). IL-2 was also measured in all adult and CB serum samples to make sure that any
IL-2 detected after stimulation was a result of IL-2 production by the stimulated cells and
did not reflect serum-derived IL-2. However, IL-2 was not detected in any of the CB or
adult serum samples. In PBMC populations stimulated using PHA, there was no significant
difference in the amount o f IL-2 detected in culture supernatants from cultures stimulated
in the presence o f adult or CB serum. The mean IL-2 production by PBMCs stimulated in
the presence o f adult serum (n=10) was 1612.7 ± 576.6 pg/ml compared to 1519.0 ±
888.0 pg/ml from PBMCs stimulated in the presence o f CB serum (n=10).
In addition to Dr Bogunia-Kubik measuring IL-2 levels by ELISA, I carried out
intracellular staining o f PBMC populations which enabled analysis o f IL-2 production at
the single cell level and assessment of the frequency of T-cells producing IL-2. These
results demonstrated that the frequency of IL-2 producing cells was actually higher in
PBMC populations stimulated in the presence of CB serum compared to adult serum
(Figure 5.6). This difference was statistically significant (P = 0.001).
136

Chaitkr 5
8H do ^
IIF
7-1
6 -
5-
4-
2 -
8o
oooT
Adult
I
I
P = 0.001—I----------CB
Figure 5.6: Analysis of the percentage of lL-2 producing T-cells after stimulation in the
presence o f CB or adult serum
PBMCs w ere p lated in RPMI164Ü plus an t ib io t ic s in the presence or ab sence o f adult (O) or CB ( • ) se ra
(1 :10 d i lu t ion) and a p rede te rm ined optim al concen tra t ion o f PHA. T he cultures were s t im ula ted for 7 days
and then rest im ula ted with p h o r b o l -1 2 - m y r i s t a t e - 13-acetate (PMA), i o n o m y c in and m o n e n s in . The c e l l s
were then sta ined extracellu lar ly for C D 3 and intracellularly for lL-2. C e lls were subseq u en t ly ana lysed b y
How cy tom etry and the percentage o f CD3* cells ex p ress in g lL-2 was calculated . S ta t is t ica l an a ly ses were
carr ied out com p ar in g the sam ples incubated in adult serum with those incubated in CB sera by S tu d en t ’s t-
t e s t .
Measurement o f cytokines in adult and cord blood serum
There have been numerous reports on soluble factors present within CB serum (See Table
5.3). However, none of these reports detail soluble factors that can sufficiently explain the
findings of this study. For example high levels of I F N - a , a cytokine known to suppress
T- and B-cell function (Krishnaswamy et al., 1996; Niwano et a i , 1989; Oka et a i , 1992;
Peters et al., 1986; Peters et al., 1986), have been reported in CB serum (Ebbesen et al.,
1995; Paulesu et al., 1991 ; Zdravkovic et al., 1997). However, it is unlikely that IFN -a is
responsible for enhancing the IL-2 specific proliferation of T-cell lines or increasing
CD25 expression on adult PBMCs after stimulation in the presence of CB serum.
Therefore, to determine whether another soluble factor (possibly an anti-inflammatory
cytokine) was present within cord blood serum that could explain some of these results,
CB and adult serum samples were sent to Dr Meenu Wadhwa (National Institute for
Biological Standards and Controls). CB and adult serum samples were analysed for the
presence of IE -10, IL-13 and M-CSF; the functions of which are diverse but have all been
shown to either directly or indirectly inhibit T-cell function (Cash et al., 1994; de Waal
Malefyt et al., 1991 ; de Waal Malefyt et al., 1991; Munn et a i , 1999; Sakurai et a i , 1996;
Sher et al., 1991 ).
137

CHAITI K 5
1000
100- o1Î 0c12 10-
u
B e lowassayde tec tionlimit
IL -10
A dult CB
IL -13
Adult CB
M C S F
A dult CB
IL -2
A dult CB
Figure 5.7: Concentration o f cytokines in adult and CB serum
T h e presence o f lL-2, I L - 10. IL-13 and M -C S F in different adult (O) or CB (■ ) serum sa m p le s was d e te rm in ed
by Dr M eenu W adhw a using ELlSAs. Levels o f s ig n if icance are represen ted as *P<0.01 and * * P < 0 .0 0 2 and
w ere de te rm ined by com p ar in g adult and CB sera by S tu d en t ’s t-test.
The levels of IL-2, IL-10, IL-13 and M-CSF detected in CB and adult serum samples is
illustrated in Figure 5.7. IL-2 and IL-13 were not detected in any of the serum samples
tested. However, IL-10 was detected in all of the adult serum samples (mean ± SD = 104 ±
55.5 ng/ml) but only one of the CB samples. Conversely, M-CSF was not detected in any
of the adult serum samples but was detectable in 6 of 7 CB serum samples (mean ± SD =
3.8 ± 2.3ng/ml).
The role o f M-CSF in CB serum
A previous study described that recombinant human M-CSF inhibited the mouse MLR
(Sakurai et al., 1996). In addition, the fact that M-CSF was detected in 6 of 7 CB serum
samples and was also found in maternal plasma during normal pregnancy (Tsakonas et
al., 1995) raised the possibility that the M-CSF detected in CB serum was playing a role in
the inhibition of the allo-response described in Figure 5.1.
To determine whether this same inhibition was occurring in the human MLR, increasing
concentrations of recombinant M-CSF were added to the MLR in the presence of adult
serum (Figure 5.8). Similar to the mouse MLR, M-CSF inhibited the human MLR in a
dose-dependent manner.______________________________________________________________
138

C h a i t ü r 5
IIIIX
15000-
12500-J
10000-
7 5 0 0 -
5 0 0 0 -
2500
T
[MCSF] (ng/ml)
Figure 5.8: M -CSF inhibits the human MLR
5x1 O'"responder cells were incubated with M -C S F for 2 hours at 37'*C in 5% CO.- I x l O ' irradiated s t im u la to r
ce lls were then added to the plates and cultures were subsequently incubated at 37"C in 5% C O . for 6 days. T he
results represent the m ean o f the tripl icates at each M -C S F concen tra t ion 4- SD.
The next experiment was therefore to neutralise the M-CSF within CB serum using an
anti-M-CSF antibody then monitor PBMC proliferation in the MLR. As expected, upon
blocking M-CSF action using neutralising antibodies, there was an increase in allo-specific
proliferation in the presence of CB serum after addition of the anti-M-CSF antibody
compared with the isotype control antibody. These results indicate that M-CSF within CB
serum is in part responsible for the reduced allo-specific proliferation described in Figure
5.1. However, in attempting to illustrate that the anti-M-CSF antibody did not affect the
proliferation of cells stimulated in the presence of adult serum, the results were
inconsistent (Figure 5.9). In some experiments there was an increase in the alloresponse
with the anti-M-CSF antibody but not with the control antibody and in other experiments
this increase was not apparent. Nevertheless, an increase in proliferation of cells stimulated
in the presence of CB serum was always witnessed.
139

CHAITI K 5
40000Adult sera
P = 0.32
CB sera
30000
20000
10000
20000 -
P = 0.33
5 0 0 0 -
10000-
5 0 0 0 -
20000P = 0.03
10000-
5000
Experiment A
1-------------rControl Anti-M CSF
20000 -
P = 0.09
15000-
10000-
5000-
Control Anti-M CSF
Experiment B
M ean C P M fo r each con d itio n
A du lt S e raControl antibody Anti-MCSF Aniibody
Experiment A 20639 .7 14602.2Experiment B 4862.9 6782.9
C o rd B lood S e raAnti-MCSF A n tiW y
11782.3 17350.41759.6 7269.4
Figure 5.9: The role of M-CSF in cord blood (CB) sera
T o d e te rm ine w h e th e r M -C S F in CB sera played a role in h ib i t in g the a l logene ic r e sp o n se , a n t i -M -C S F
n eu t ra l i s in g an t ibody (or an iso type m atched con tro l ; Mouse IgG2a) was added to m ixed l y m p h o c y t e
reac t ions incuba ted in a 1:10 dilution o f adult or CB sera. T he results represen t the m ean o f tr ip l ica te cu ltu res
o f cel ls incubated in different sera (in the p resence o f the contro l a n t ibody or the M -C S F n e u t r a l i s i n g
an t ibody) . Stat ist ical ana lyses were perfo rm ed using S tu d e n t ’s t-test.
140

___________________________________________________________________________________________________________________________________________ C h a itter 5
Summary and discussion o f CB immunobiology
These results demonstrate that there are differences in the soluble factors present in CB
and adult serum and that these differences have an effect on T-cell functional responses
when tested in vitro. The main findings from these results are: (1) The proliferative
response o f adult PBMCs to allostimulation is reduced in the presence of CB serum
compared with adult serum; (2) The proliferative response o f T-cell lines to anti-CD3
stimulation is also reduced in the presence o f CB serum compared to adult serum; (3)
Conversely, the proliferative response of T-cell lines to IL-2 stimulation is increased in the
presence of CB serum compared to adult serum; (4) The IL-2 receptor a chain CD25 is
expressed at higher levels on adult PBMCs stimulated (either by allostimulation or PHA)
in the presence of CB serum compared with adult serum; (5) M-CSF was detected in CB
but not in adult serum; (6) M-CSF inhibited the human MLR in a dose-dependent
manner; (7) Proliferation o f PBMCs stimulated in the presence of CB serum increased
upon blocking M-CSF action.
Human recombinant M-CSF has been shown to inhibit the mouse MLR (Sakurai et a i ,
1996). The results presented here support a role for M-CSF in the inhibition o f the MLR
using human cells. Furthermore, it appears that the M-CSF detected in CB serum may be
responsible for the reduced proliferation of adult PBMCs when stimulated in the presence
of CB serum compared with adult serum. However, these results appear confusing since T-
cells do not express the receptor for M-CSF (Stanley et al., 1997) and therefore M-CSF in
CB serum could not have been acting directly on the T-cell population. A recent
publication by Munn et al. (Munn et a i , 1998) demonstrated that the expression o f
indoleamine 2,3-dioxygenase (IDO) during murine pregnancy was required to prevent
rejection of the allogeneic foetus by maternal T-cells. Furthermore, this group
demonstrated that monocytes that differentiated under the influence o f M-CSF acquired
the ability to suppress T-cell proliferation in vitro via rapid and selective degradation o f
tryptophan by IDO (Munn et al., 1999). It is possible that this same mechanism is
responsible for the inhibition of the MLR demonstrated in our laboratory. However, this
mechanism does not explain the observation that the anti-CD3 induced proliferation o f
pure T-cells was not enhanced with CB serum but was enhanced with adult serum. Neither
does this mechanism explain the results obtained with the IL-2 specific proliferation o f T-
cell lines or higher levels o f CD25 expression on cells stimulated in the presence o f CB
serum compared with adult serum. Therefore, it is possible that other soluble factors
within CB serum (of which there are many) may be responsible for the results presented
here.
Regardless o f the mechanisms responsible, these results suggest that the microenvironment
from which CB cells are derived can influence functional responses o f adult cells. Whether
141

C h a itter 5
these results are sufficient to explain the maintenance of pregnancy or the reduced
severity of GVHD after CB transplantation remains to be determined.
CB Transplantation: Reconstitution of the T-cel l
com partm ent
The reconstitution of the T-cell compartment in recipients of CB transplants has not been
extensively studied as yet and many questions remain unanswered as to the ability of CB
grafts to sustain long term haematopoiesis. Weinberg et a i analysed 12 CBT recipients
and demonstrated that thymopoiesis was rapid (detected by 100 days post-transplant) and
sustained for a long period (patients analysed up to 2 years post-transplant). In addition, it
was demonstrated that a number of CBT recipients developed supranormal TREC levels
compared with normal age-matched controls (Weinberg et al., 2001). Another recent
study by Niehues et at. analysed 63 CBT recipients from either related or unrelated
donors and demonstrated that CDS'” and CD4^ T-cell numbers normalised to within age-
matched control levels within 12 months post-CBT while CD8^ T-cells normalised earlier
at 7.9 months post-SCT (Niehues et a i , 2001). These and other results (Klein et ai., 2001;
Moretta et al., 2001) suggest that CB stem cell grafts are capable o f rapidly reconstituting
the T-cell compartment via thymic-dependent pathways.
Peripheral blood samples from 11 CBT recipients were obtained through collaboration
with Dr Franco Locatelli (University of Pavia, Pavia, Italy) and these were taken at various
time points between 1-15 months post-CBT. T-cell reconstitution in these patients was
analysed and compared with age-matched recipients of BM and PBSC transplants (also
described in Chapter 4) from the Royal Free Hospital. A summary of the patient’s
transplant-related clinical data is shown in Table 5.4. All patients were less than 18 years
of age at the time of transplant and all received a T-cell replete stem-cell graft. Data on
absolute numbers o f CD3" cells infused with the stem cell grafts and absolute numbers o f
C D 3\ CD4'’ and CD8^ T-cells at each time point after transplant were requested for the
CBT recipients but were not received. Therefore, the following T-cell reconstitution data is
presented as naïve (CD45RO C D 270 CD4" and CD8^ T-cells as a percentage o f the total
CD4^ or CD8"’ T-cell population. In addition, TREC data is presented as TREC per 1x10^
cells as an alternative to absolute TREC counts.
Thymic output and naïve T-cell recovery in these patients is illustrated in Figure 5.10. To
summarise the BM and PBSC recipients (Figure 5.10A), 5 of 6 patients restored TREC
levels to within the normal range by 12 months post-transplant. In addition, the
percentage o f naïve CD4"’ and CD8’' T-cells exceeded 50% o f the CD4"’ and CD8"
population in 5 of 6 patients post-transplant. These results suggest that thymic-dependent
142

_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ C h a p t e r 5
pathways are restored to normal levels in these patients and that this facilitates the
restoration o f the naïve T-cell pool. The results presented in Chapters 3 and 4 also
demonstrate that absolute numbers o f naïve T-cells in these patients were within the
normal range by 12 months post-transplant.
Table 5.4 Transplant related clinical data on recipients o f CB, BM and PBSC transplantsUPN Age Diagnosis' Conditioning** Stem Cell GVHD* Source
Acute ChronicInfections# Current status
37 6 ALL Cy/TBI BM 1 N Alive and well25 6 FA Cam/Cy/TAI PB N N - Alive and well26 7 FA Cam/Cy/TAI PB N N - Alive and well12 11 ALL Cy/TBI BM 1 N VZV Alive and well20 15 SAA Cam /Cy/Flu BM N N Alive and well9 17 FA Cam/Cy/TAI BM N N CMV Alive and well66 4 Dys Con Cy/Flu CB N N - Alive and well67 1 SCID Bu/Thio/Flu CB 1 N - Alive and well68 6 ALL Cy/TBI/Thio CB 1 N PC P R elap sed70 5 ALL Bu/Thio/Flu CB II N Fever of unknown
originAlive and well
71 5 ALL TBI/Thio/Flu/ALG CB N N Alive and well72 4 Thai Bu/Thio/Flu CB N N PCP, CMV Alive and well147 2 Thai Bu/Thio/Flu CB 1 N - Alive and well148 13 FA Cy/TBI CB N N - Alive and well188 6 Thai Bu/Thio/Flu CB N N - Alive and well189 3 JMML Bu/Cy/Mel CB II N CMV Alive and well187 2 Thai Bu/Thio/Flu CB N N - Alive and well
# FA = Fanconi A naem ia, ALL = A cute Lym phocytic Leukaem ia. SAA = Severe A plastic A naem ia, Dys Con = D y sk e ra to s is
C ongenita, SCID = Severe Com bined Im m unodeficiency; Thai = Thalassaem ia; JM M L = Juvenile M yelom onocytic Leukaem ia.
** Conditioning: Cy = cyclophospham ide, TBI = total body irradiation, TA I = thoraco-abdom inal irradiation. Flu = fludarabine, Bu =
busulphan, Thio = thiotepa, ALG = anti-lym phocyte globulin, Mel = melphalan; Cam = C am path-IH
# G VHD: A cute G V H D was graded I-IV in term s o f severity, the least severe form being grade I. No periods of chronic GVHD w ere
n o te d .
# Infections i.e. bacteraem ia and pneum onia, virus reactivations/infections occuring w ithin the first year after stem cell HCT. VZV =
varicella zoster virus; CM V = cytom egalovirus; PCP = Pneum ocystis pneum onia .
143

Chaitur 5
100
I ™ I 0S 100 30
20
20
B0 6 1 2 12 12
100188
100187
O)VH
CJD2s
100
s&
100
189
148
68
71
147
00 126
30
20
10
030
20
10
20
10
H50Mn
X1
X?
H»Wn
!X
X%
Months post-HCT
Figure 5.10: Thymic output and naïve T-cell recovery in recipients o f CB transplants
compared with age-matched recipients of BM or PBSC transplants
T R E C levels w ere m easu red in P B M C (A ), sorted CD4^ ( □ ) or sorted CD8* ( ■ ) cell popula t ions in pa tients le s s
than 18 years o f age w h o received BM or PBSC (A), or CB (B) t ran sp lan ts . Naïve CD4* (O) and CD8"^ ( • ) T-
cells are represen ted as a percen tage o f the total C D T or CD8* T-cell population. T he dashed b lue line in each
plot represen ts the low er limit o f T R E C levels in normal age-m atched contro ls . Patients are iden t i f ied by th e i r
U P N in the top-left hand co rner o f each plot.
144

___________________________________________________________________________________________________________________________________________ C h a p t e r 5
By contrast, only 1 of the CB transplant recipients restored normal TREC levels
throughout the course o f the study. The remaining patients had low or undetectable
TREC levels. This is also reflected in the recovery of naïve CD4^ and CDS'" T-cells in that
only 4 patients had greater than 50% naïve CD4^ or CDS^ T-cells at the last time point o f
analysis. However, there are two important points that should be raised regarding TREC
measurements in these patients. First, that only 3 of the 11 CBT recipients were followed
up for 12 months or more after transplant. Although none of these three patients achieved
TREC levels within the normal range, it is possible that some of the remaining 8 patients
would have achieved TREC levels within the normal range by 12 months post-transplant.
Secondly, that these samples were sent from Italy on dry ice. Upon thawing, cell recovery
in a number o f samples was poor, sometimes less than 10% of the starting number. In
these cases, there was not enough material to carry out sorting o f CD4'' and CDS^
populations and TREC were measured in unseparated PBMC populations.
Nevertheless, the implications from these results are that reconstitution o f the naïve T-cell
compartment is delayed in CB transplant recipients. Therefore, it is possible that
peripheral expansion mechanisms restore memory and effector T-cell numbers in the
short term as a compensation mechanism. However, as mentioned previously, we did not
receive data on absolute T-cell numbers and it is therefore difficult and highly speculative
to comment on the overall reconstitution of the T-cell compartment based only on
percentage values from flow cytometry.
The results from Chapter 4 suggested that a number of factors were important in
determining the contribution of the thymus to reconstitution o f the T-cell compartment
post-HCT. The most important of these were age and GVHD, with little or no influence o f
stem cell source {i.e. BM or PBSC) on thymic output. Since the patients described in this
chapter are age-matched, the difference between CB and BM/PBSC recipients could not be
a result of differences in age. Although this patient group is small, the incidence o f acute
GVHD was similar between the two groups with 2 of 6 BM/PBSC transplant recipients and
5 of 11 CB transplant recipients experiencing some acute GVHD (albeit mild GVHD o f
grade I or II). No incidences o f chronic GVHD were recorded, therefore, the differences
in thymic output between the two patient groups were probably not related to GVHD. It
should be noted that the two cohorts of patients were from different transplant centres and
that the conditioning regimens differed between the centres. However, the major
difference between these two patient groups is the stem cell source and it is important to
consider the possibility that reconstitution o f the T-cell compartment by thymic-
dependent pathways may be delayed in recipients of CB compared with BM or PBSC
transplant recipients.
145

_________________________ C h a p t e r 5
Discuss ion
The results presented in this chapter demonstrate two main points; firstly that the cord
blood microenvironment is different from the adult blood environment and that this can
influence T-cell functional responses. Secondly, that reconstitution o f the T-cell
compartment via thymic-dependent pathways after CB transplants appears less efficient
than BM or PBSC transplants. These two observations may have important consequences
for the outcome of CB transplants and their utilisation as an alternative to BM or PBSC
transplants.
Before discussing these results, it is worth mentioning some of the practical advantages
and disadvantages of CB transplantation and why CB may provide a valuable alternative
for patients who may not otherwise have HLA-matched related or unrelated BM or PBSC
donors. The first advantage is that CB collection is straightforward with no risk to the
donor from general anaesthesia, mobilisation drugs or hospitalisation, all of which are
problematical for BM or PBSC donors. CB can be collected either in utero or ex utero
after clamping o f the umbilical cord. After collection, the cord blood product is separated
and cryopreserved until needed. The establishment o f CB banks (Gluckman et a i , 1993;
Hakenberg et al., 1998; Navarrete et al., 1998; Querol et al., 1998; Rubinstein et al.,
1993) has meant that the period from request of the CB unit until transplantation is
significantly shorter than for BM and PBSC transplants. This point is particularly
important for young children with inherited metabolic and some haematologic disorders
{e.g. severe aplasia), in whom disease progression or infection is problematic unless the
HCT is carried out as soon as possible. A further advantage o f using CB is that the
product is less likely to be contaminated by viral antigens such as CMV and EBV
compared with either BM or PBSC harvests (reviewed in (Warwick, 2000)). In addition,
the use o f CB may overcome the scarcity of donors for patients o f non-Caucasian origin.
The potential immunological advantages of CB will be discussed later but there is some
evidence suggesting that the reduced incidence and severity o f GVHD post-CBT may
allow more HLA-mismatches to be tolerated. This will again increase the pool o f potential
donors.
Of course there are several important disadvantages and problems associated with the use
of CB compared with BM or PBSC grafts. The relatively low number o f cells collected in
each CB unit has raised concerns regarding engraftment and long term immune
reconstitution (Cairo and Wagner, 1997). In addition, it seems likely from the results
presented so far (Gluckman et a i , 1997; Gluckman, 2000; Locatelli et a i , 1999;
Rubinstein et al., 1998; Sanz et al., 2001) that due to the small number of cells, CB only
represents a feasible alternative stem cell source for children. Attempts have been made to
circumvent these problems by expanding CB progenitors ex vivo (Butler, 2000), but so far
146

___________________________________________________________________________________________________________________________________ C h a în e r 5
these attempts have been unsuccessful. There are also numerous moral, ethical and legal
issues regarding the use of CB for transplantation, but these are discussed in detail
elsewhere (Ende, 1992; Fernandez, 2000).
Perhaps the most interesting of the previous advantages, at least from the immunologists
point of view, is that there is an apparent reduction in the incidence and severity o f GVHD
after CB transplants compared with BM or PBSC transplants. The current hypothesis
proposes that this is due largely to the immunological naivety of the CB immune system.
With regards to this apparent reduction in GVHD after CB transplants, there were concerns
that this would also have an impact on the graft-ver^w^'-leukaemia (GvL) effect. Thus,
there were fears that CB transplant recipients would be more susceptible to leukaemic
relapse. However, a number of studies demonstrated a role for CB NK and lym phokine-
activated killer (LAK) cells in GvL reactivity (Harris, 1995; Harris et al., 1994; Keever et
al., 1995). While the GvL reactivity of CB does not seem to be compromised when tested
in vitro, long term follow up and assessment of the risk of leukaemic relapse provide the
most important data. Recent analyses of CB transplant outcome from the Eurocord
registry demonstrated a reduced GVHD but similar rates of leukaemic relapse in unrelated
CB transplant recipients compared with unrelated BM transplant recipients (Rocha et al.,
2001). Furthermore, there have been no reports of increased rates o f leukaemic relapse
after CB transplants suggesting that the GvL effect is maintained.
The study of the CB and neonatal immune system (studies prompted by this apparent
GVHD phenomenon and the increased susceptibility o f neonates to infection) have
revealed numerous differences between the CB and the adult immune system. Focusing
on the differences between CB and adult T-cells, numerous studies have noted reduced
proliferation (to a variety o f stimuli; (Bertotto et a i , 1990; English et al., 1992; Gerli et
al., 1989; Lucivero et al., 1996; Matsuzaki et a i , 1989), reduced cytokine production
(Chalmers et al., 1998; Lewis et al., 1991; Risdon et al., 1994) and reduced cytotoxic
activity (Harris et al., 1992; Keever et al., 1995; Risdon et al., 1995; Risdon et al., 1994)
of CB T-cells compared with adult T-cells. In addition, the majority o f CB T-cells express
phenotypic markers characteristic of naïve T-cells (illustrated in Table 5.1). While several
studies concluded that CB T-cells were functionally deficient compared with their adult
counterparts (Chalmers et a i , 1998; Chipeta et a i , 1998), results from our laboratory
suggest that CB T-cells simply require a stronger stimulus to achieve full activation
(Bogunia-Kubik et al., 2000; Perez-Cruz et a i , 2000).
That there are functional differences and/or differences in activation thresholds between
adult and CB T-cells is now generally accepted. However, there were no suggestions that
the CB microenvironment (CB serum) played a role in influencing CB T-cell functional
responses. By stimulating adult PBMCs or T-cells in the presence o f CB serum and
comparing this to the response of adult PBMCs stimulated in the presence o f adult serum,
147

___________________________________________________________________________________________________________________________________________C h a p t e r 5
it became apparent that the adult cells responded to an allogeneic stimulus in a similar
manner to CB cells (Cohen et al., 2000).
The identification o f M-CSF within CB sera prompted investigation of the effects of M-
CSF in the MLR and also, whether neutralisation of M-CSF increased the proliferation o f
adult cells stimulated in the presence of CB sera. This was confirmed and it seems likely
that the M-CSF within CB sera was, at least in part, responsible for the reduced
proliferation of adult cells when stimulated in the presence of CB sera.
The fact that the CB microenvironment suppresses T-cell responses is perhaps not
surprising. For a successful pregnancy to be maintained, mechanisms must exist to
prevent rejection of the allogeneic foetus. The role of M-CSF in CB sera in suppressing T-
cell responses may be related to the catabolism of tryptophan both at the maternal-foetal
interface and possibly in the placenta itself (Munn et a i , 1999; Munn et a i , 1998). There
are numerous mechanisms in addition to tryptophan catabolism which have been
described in an attempt to explain the lack of an allo-response against the foetus. These
include a shift of the maternal immune system towards a “suppressive” Th2 like profile
(Bennett et al., 1997; Chaouat et al., 1997; Lin et al., 1993; Raghupathy, 1997; Wegmann
et al., 1993); expression of HLA-G (Carosella et a i , 1999; Hammer et a i , 1997; Hammer
et al., 1997) and Fas ligand (Uckan et al., 1997; Zorzi et a i , 1998) at the maternal-foetal
interface; and regulatory yÔ T-cells which suppress the maternal anti-foetal response
through TGF-(3 production. Additionally, there are likely to be other immunosuppressive
factors present in CB serum that could be involved.
While the results presented here demonstrate that CB serum can influence T-cell
functional responses, it is unknown whether these results will translate into a clinically
relevant phenomenon. One important point to consider is that due to the cryopreservation
and storage procedure after CB collection, CB serum is not transfused into the recipient
with the cellular material. Therefore, immediately after infusion, CB cells are exposed to
the complex milieu of the transplant recipient’s body. Although not proven, it seems
unlikely that the immunosuppressive effects o f CB serum in vitro would be maintained in
vivo.
The outcome of all haematopoietic stem cell transplants is determined by many genetic
and environmental factors, some of which were outlined in Chapter 4. The fact that CB
stem cell grafts are phenotypically and functionally different from BM and PBSC grafts,
coupled with the fact that significantly lower cell numbers are infused in CB transplant
recipients has raised concerns regarding engraftment and immune reconstitution.
Engraftment does not seem to be problematic, although delays in platelet recovery
(Wagner et al., 1996) have been reported.
148

___________________________________________________________________________________________________________________________________________C h a p t e r 5
The potential of cord blood to sustain long term immune reconstitution is less well
characterised with only a few studies published to date (Klein et a i , 2001; Moretta et al.,
2001; Niehues et al., 2001; Weinberg et al., 2001). As well as the other advantages of CB
as a source of stem cells for transplantation, CB also has theoretical advantages over BM
and PBSCs in terms of immune reconstitution potential. Compared to adult cells,
haematopoietic progenitor cells from CB are enriched in the most primitive stem cells,
producing long term repopulating stem cells in vivo (Broxmeyer et al., 1989; Broxmeyer
et al., 1992). In vitro culture in the presence of growth factors also yields significantly
higher numbers o f haematopoietic progenitors from CB than adult blood. In addition, CB
cells have been shown to have significantly longer telomeres than adult cells (Lansdorp et
al., 1994; Vaziri et a i , 1994). All these properties o f CB cells theoretically gives them a
proliferative advantage over adult cells and may compensate for the relatively low
numbers of stem cells contained in a single CB unit. Therefore, it should be feasible to
reconstitute adults and children using cord blood.
The data published so far does not reveal any delays in lymphocyte reconstitution after
CB compared with BM transplants at least in children (Klein et al., 2001; Moretta et al.,
2001; Niehues et al., 2001; Weinberg et al., 2001). In addition, the analysis o f thymic
output after CB transplants using the TREC assay (Klein et a i , 2001; Weinberg et al.,
2001) demonstrated high levels o f thymic output in children comparable with the results
from patients after BM transplants. However, in contrast to these studies, the results
presented in this chapter show significantly lower levels o f thymic output and naïve T-cell
recovery in CBT recipients compared with age-matched BM or PBSC recipients. This may
represent a genuine difference in the reconstitution potential of CB grafts compared with
BM and PBSC grafts. However, as mentioned previously, cell recovery in a number o f
samples was poor and it is possible that selective loss of naïve T-cell populations occurred
during the freezing process. For our purposes, it will be important to measure thymic
output and naïve T-cell recovery on fresh {i.e. non-cryopreserved) blood samples from
CB transplant recipients. Furthermore, it is clear that further studies on the reconstitution
of the immune system using CB compared with adult blood stem cells are necessary.
149

C h a p t e r 6
C h a p t e r 6
Thymic function in paediatric primary immunodeficiency patients
Introduction
Primary immunodeficiency diseases are characterised by a susceptibility to recurrent and
often fatal opportunistic infections as well as other immunological problems such as
autoimmune diseases. Many types of primary immunodeficiency diseases have now been
identified with a wide spectrum of clincial manifestations and underlying genetic causes.
Severe combine immunodeficiency (SCID) is a rare fatal syndrome characterised by
profound deficiencies of T- and B-cell function (Bortin and Rimm, 1977; Fischer, 1992).
Since the initial report of a patient with SCID over 50 years ago the genetic origins of the
disease have been demonstrated to be highly variable (Fischer, 1992; Giblett et a i , 1972;
Griscelli et a i , 1978; Noguchi et al., 1993; Fuel et a i , 1998; Russell et a i , 1995; Schwarz
et al., 1996; White et al., 2000). Nevertheless, the clinical course of the disease is
consistent, with susceptibility to infection leading to death in infancy being the inevitable
outcome of the disease. However, significant advances have been made in treatment
options for SCID patients over the past 30 years with HCT proving an extremely
successful therapy (Buckley et a i , 1999; Fischer et al., 1990). In addition, gene therapy
offers a more recent alternative to HCT for the correction of the genetic defect leading to
SCID (Fischer et a i , 2000).
However, with regard to HCT, this treatment option has numerous associated problems.
GVHD and infections (as a result of delayed immune reconstitution) remain significant
barriers to the success of this therapy. In addition, a number o f SCID patients remain
deficient in T-cell function in the long term and (with only a few exceptions) none of the
transplanted SCID patients restore normal B-cell function, remaining dependent on
infusions o f immunoglobulins throughout life.
150

___________________________________________________________________________________________________________________________________________ C h a p t e r 6
Clearly, the absence of T-cells in SCID patients before HCT gives us a unique opportunity
to study the development o f T-cells in the absence o f a competing immune system. The
previous results from chapter 4 demonstrated that some aspects of pre-transplant
conditioning could affect thymic output. However the SCID patients reported previously
(Buckley et al., 1999) did not receive any pre-transplant conditioning and therefore
allowed the study o f thymic-dependent reconstitution in the absence o f pre-transplant
conditioning or a competing immune system. However, SCID patients have very small
thymuses that weigh less than 1 gm and lack thymocytes and correct thymic architecture.
This has prompted speculation that the SCID thymus would be unable to support T-cell
maturation after HCT (Buckley et al., 1997; Neuhaus and Briner, 1986; Nezelof, 1992). A
recent study by Patel et al. alleviated these concerns somewhat by demonstrating that the
SCID thymus was able to support T-cell maturation in patients after HCT (Patel et al.,
2000). However, thymic output was not sustained over the course of the study and
declined to undetectable levels by 17 years post-HCT. This observation, along with the
lack o f B-cell function noted in patients after HCT has raised further concerns over
engraftment o f the most primitive self renewing stem cells.
Therefore, the first aim of this chapter was to assess thymic-dependent reconstitution
(using TREC analysis) in two groups of SCID patients who were between 1 and 17 years
post-HCT. These groups were divided into patients that received pre-transplant
conditioning and those who did not. Where possible, T-cell phenotyping was also carried
out.
Another primary immunodeficiency disease that offers a unique opportunity to study
thymic function and T-cell development is the DiGeorge syndrome. The DiGeorge
syndrome is a rare congenital disorder in which the thymus, parathyroids and heart all fail
to develop properly. In complete DiGeorge syndrome, patients have severely reduced or
absent T-cell function (Markert et a i , 1999). However, the severity of the syndrome varies
a great deal. Similar to SCID, the genetic causes o f DiGeorge syndrome are not fully
understood although a deletion within chromosome 22q l 1.2 is most frequently observed
(de la Chapelle et al., 1981; Driscoll et al., 1993).
Several therapies have been used to treat the immunodeficiency associated with DiGeorge
syndrome. HCT has been attempted but has been limited in its (Borzy et al., 1989; Bowers
et al., 1998; Goldsobel et al., 1987; Markert et al., 1998). Thymus transplantation has
also been considered as a treatment option (August et al., 1968; Daga et a i , 1984;
Markert et al., 1997; Pahwa et a i , 1979) but these attempts have also been largely
unsuccessful (Borzy et al., 1979; Dictor et al., 1984; Reece et al., 1981). A recent study
by Markert et al. analysed DiGeorge syndrome patients who received thymic tissue
transplants. This study was able to demonstrate that grafted thymic tissue was able to
151

___________________________________________________________________________________________________________________________________________ C h a p t e r 6
reconstitute the T-cell compartment and that survival of the patients was extended for a
considerable period of time (Markert et al., 1999).
Therefore, the second aim of this chapter was to evaluate thymic function in a number o f
DiGeorge syndrome patients (defined on the basis o f having the 2 2 q ll.2 deletion) as part
of their clinical evaluation.
152

C h a p t e r 6
R e su l t s
H CT fo r the treatment o f SCID
A study of thymic output in transplanted SCID patients was carried out using peripheral
blood samples from SCID patients provided by Dr Andrew Gennery (Newcastle General
Hospital) and Dr Adrian Thrasher (Great Ormond Street Hospital).
A relatively small number of patients are transplanted for SCID each year in the UK.
Therefore, to enable collection of a significant number of patient samples in a short
period of time, it was decided that the post-HCT follow up should be a cross-sectional
analysis rather than a longitudinal study. As a result, only one blood sample was taken
from each patient. Depending on the volume of blood obtained (often less than 2ml), a
variable amount o f data was obtained for each patient sample. Where possible T-cell
phenotyping and TREC analysis was carried out for each blood sample.
The SCID thymus: detection o f thymic activity post-H CT
The SCID patients were split into two groups, one o f which received pre-transplant
conditioning and the other that did not. Thymic output in these two groups was quantified
and compared with age-matched healthy controls (Figure 6.1). Encouragingly, some level
of thymic output was detected in the majority of patients in agreement with previous data
(Patel et al., 2000) that the SCID thymus is able to support thymopoiesis. Median TREC
levels in DNA extracted from whole blood from normal individuals were 2980 TREC per
pg DNA (range 1311-9420). Interestingly, TREC levels were higher in those patients who
received pre-transplant conditioning with a median TREC level of 3726 TREC per pg
DNA (range 0-15000) compared with SCID patients who did not receive pre-transplant
conditioning (median TREC per pg DNA = 120; range 0-1400). Although this was not
statistically significant (P = 0.13 using the Mann Whitney U-test), there was a clear
difference between the two groups and these results suggest that this study should be
extended to a larger group of patients.
153

c HAITI-R 6
<za
iuGCH
15000-
10000-
5 0 0 0 -
o
oo
ooo
— I— Normal +Conditioning -Conditioning
Figure 6.1 : TREC levels in SCID patients after HCT
T R EC levels were measured using DNA extracted from w hole b lood (using EDTA as the a n t i c o a g u la n t ) .
P a tien ts were d ivided into two groups i.e. SCID pat ien ts w ho received p re - t r an sp la n t c o n d i t io n in g ( • ) and
patients w h o did not receive p re-t ransp lan t c o n d i t ion ing (A). All pa t ien ts were t ran sp lan ted before r e a c h in g
age 1. A ge-m a tch ed control T R E C values are also show n ( O ) . The black bars represen t the m edian values fo r
each group.
Patel et al. demonstrated that TREC levels in non-conditioned SCID patients reached peak
levels by 2 years post-HCT then declined to virtually undetectable levels by 12 years post-
HCT (Patel et a i , 2000). It was difficult to carry out this type of analysis due to the small
number of patients. Nevertheless Figure 6.2 illustrates TREC levels in the same patients as
Figure 6.1 between 2 and 17 years post-HCT. The first observation from this graph is that
several of the conditioned SCIDs have very high TREC levels even up to 7 years post-
HCT. Of the non-conditioned SCIDs, none of these patients had high TREC levels
regardless of the time point at which they were measured. Also, similar to previous
observations, TREC levels were either low or undetectable at 12-17 years post-transplant
in both conditioned and non-conditioned patients. The questions arising from these
observations are whether the increased thymopoiesis in conditioned SCID patients
compared to non-conditioned patients is related to engraftment of donor stem cells.
154

C h a i t i ;r 6
lOOOOOn
<zQ
U
uQgH
10000J
1000-
100-
10
oo o
##
_Q_
10
Time post-HCT (years)
I15
Figure 6.2; TREC levels in SCID patients at different time points after HCT
T R EC levels were measured using DNA extracted from w hole b lood (using EDTA as the a n t i c o a g u la n t ) .
Pa t ien ts were d iv ided in to two g roups i.e. SCID patients w ho received p re - t ransp la n t c o n d i t io n in g ( O ) and
pat ien ts w ho d id not rece ive pre-t ransp lan t cond i t ion ing ( • ) .
Case study o f a non-conditioned SCID
Throughout the course of this study, one of the non-conditioned SCID patients (UPN 42)
received a “top-up” of peripheral blood from his original donor. The phenotype of this
patient was T B*NK, later discovered to have a mutation in the JAK-3 enzyme. The initial
transplant was performed at Great Ormond Street Hospital when the patient was less than 1
year old. This consisted of a single infusion of peripheral blood from an HLA-matched
sibling in the absence of pre-transplant conditioning. After the first infusion of peripheral
blood the patient remained clinically well but was deficient in B-cell function and reliant
on infusions of IVIG. Chimaerism analysis revealed that T-cells were of donor origin and
B-cells were of recipient origin. I received a blood sample from this patient 17 years post
transplant when the patient was experiencing persistent development of warts and other
immunological problems. It was suggested that this might be due to failure of appropriate
T-cell responses and possibly a lack of new T-cell maturation in the thymus. The patient
received a top-up of donor lymphocytes shortly after the first blood sample was taken and
a second blood sample was taken 3 weeks after the patient received their top-up. T-cell
phenotyping and TREC analysis was performed using these two samples. The change in
TREC levels and T-cell subsets before and after this patient received a top-up of donor
cells is shown in Figure 6.3.
155

CH A ITkR 6
Before the patient received the top-up it was evident that TREC levels and T-cell subsets
were abnormal. While TREC were detectable in both CD4 and CDS subsets pre-top-up,
they were significantly below the lower limits of TREC levels in normal controls. In
addition, there was an inversion of the normal CD4:CD8 ratio suggesting a distortion in
the regulation of T-cell subsets.
10000
5000
CD4 TREC CDS TREC
Pre Post
10000
b 5000
Pre Post
CD4:CD8
Pre Post
100
50
Naïve CD4
Pre Post
Memory CD4-------------------------------- 100 n-------------------------------- 100-,
s Su u1 n 1®& 50 % 50-to cr 21
at.
-------------------------------- 0-at
-------------------------------- 0-Pre Post
Effector CD4
Pre Post
100
50 -
Naïve CDS
Pre Post
100
50 -
Non-naïve CDS
Pre Post
100
50
CDS+S7+2S-
Pre Post
Figure 6.3; TREC and T-cell subsets in Patient 42 before and after peripheral b lood
infusions
T R E C levels and naïve, m em ory and e ffec to r T-cell subsets were m easured in patient 42 before and after a to p -
up o f d o n o r ly m p h o c y te s . TREC were measured in sorted C D 4 and CDS subsets . T he T-cell subsets are
rep re sen ted as the pe rcen tage o f the total C D 4 or CDS subset. The blue dashed line in p lo ts (A) and (B)
rep resen ts the low er limit o f TREC levels in age-m atched hea l thy con tro ls . T he blue dashed line in plot (C)
rep re sen ts the C D 4 :C D S ratio in norm al indiv iduals .
156

C h a p t e r 6
As mentioned previously, a second blood sample was taken at 3 weeks after top-up. There
was a slight increase in TREC levels although they remained below TREC levels in age-
matched healthy controls. In addition the CD4:CD8 ratio remained unchanged. There was
a slight decrease in the percentage of naïve CD4^ and CD8^ T-cells and a slight increase in
the percentage o f memory CD4^ and CD8" T-cells, but no change in the percentage o f
effector CD4'’ or CD8^CD57"^CD28‘ subsets. Although this sample was taken shortly after
the “top-up” it appears that the top-up had little influence on restoring a phenotypically
normal T-cell compartment.
Two other SCID patients from Great Ormond Street Hospital are awaiting top-up
infusions o f peripheral blood from their original donors. Clearly, a more detailed analysis
is necessary to determine the effectiveness of this approach in restoring full T-cell
mediated immunity. However, it is unlikely that this approach will facilitate stem cell
engraftment or restoration o f B-cell function.
Thymic output and the DiGeorge syndrome
The previous results demonstrate that measuring TREC levels proves a useful addition to
conventional techniques for measuring T-cell engraftment and maturation after HCT. The
following section evaluates thymic output in a number o f patients diagnosed as having
DiGeorge syndrome on the basis of having the 2 2 q ll .2 deletion. Peripheral blood
samples from these patients were kindly provided by Dr Andrew Gennery (Newcastle
General Hospital), Dr Colin Michie (Ealing Hospital) and Dr Adrian Thrasher (Great
Ormond Street Hospital).
Similar to the SCID patients described previously, the blood samples obtained from these
patients were small (l-2m l), therefore TREC were measured on all samples and T-cell
phenotyping was carried out when possible.
TREC measurements in blood samples from the DiGeorge syndrome patients made and
the results are shown in Figure 6.4. There are a number of patients with no detectable
TRECs, but on the other hand, several patients had detectable TRECs with 5 o f 12 patients
having TREC levels within normal limits. Two of the five patients in whom we could not
detect TREC died throughout the course of the study and all 5 patients in whom we could
not detect TREC were defined as having complete DiGeorge syndrome.
157

20000 -
C h a p t e r ô
<I
U
g
10000-
oo
o oo
Age matched controls
-----DiGeorge syndrome
patients
Figure 6.4: Thymie output in patients with DiGeorge syndrome
T REC levels were m easured us ing DNA ex trac ted f rom w ho le b lood (us ing EDTA as the a n t ico ag u lan t ) . T he
T R E C values for the D iG eo rg e s y n d ro m e patients (A) are sh o w n a longs ide a g e -m a tc h e d healthy con tro ls ( O ) .
Table 6.1 : T-cell phenotyping and TREC levels in 5 DiGeorge syndrome patients
U P N 192 U P N 205 U P N 1 9 0 U P N 197 U P N 206
N aïve C D 4 * 4 3 51 4 6 5 2 6 2
M e m o ry C D 4 5 2 4 2 5 2 4 3 3 6
E ffecto r C D 4 3 6 2 5 2
Naïve CDS 3 6 3 4 4 0 6 2 6 0
N o n -n a ïv e C D S 6 4 6 6 4 6 3S 4 0
CDS*57*2S 5 2 4 S 2 7
T R E C /p g DNA** 1 7 6 6 S 420 551 2 1 7 7 1 6 7 2 S
* Values for all T-cell subsets are shown as the percentage of the total CD4 or CD8 subset** DNA was extracted from whole blood samples (using EDTA as anticoagulant). TREC values are shown as TREC per pg DNA.
The results from T-cell phenotyping of patients on whom we gained a sufficiently large
volume of blood (greater than 5ml) are given in Table 6.1. There was a significant
proportion of cells in both CD4 and CD8 compartments that were phenotypically naïve
and TREC were detected in all five of these patients. Therefore, even though all of these
patients had the 22ql 1.2 deletion, this did not always result in a lack of thymopoiesis and
naïve T-cells. The measurement of TREC levels in DiGeorge syndrome patients could
therefore be useful in their clinical evaluation and should be considered as a routine test
in defining the exact phenotype o f each patient.
158

C h a p t e r 6
Discuss ion
The previous results demonstrate that: (1) The thymus in both SCID and less severe
DiGeorge syndrome patients is capable of supporting thymopoiesis; (2) The long-term
maintenance o f thymic function in SCID patients after HCT may depend on the
administration of some pre-transplant conditioning; (3) TREC measurements are a
valuable addition to clinical evaluation of both SCID patients after HCT and in the
evaluation o f patients with DiGeorge syndrome.
The treatment o f SCID using non-conditioned HCT has proven extremely successful in
terms o f overall patient survival. However, this form of therapy is far from ideal and
several problems remain. GVHD and infection are two problems that are common to all
forms of HCT. In addition, the administration of non-conditioned HCT to SCID patients
does not correct the deficiency in B-cell function (Buckley et a l , 1997; Buckley et al.,
1999). Also, the results presented here and those of Patel et al. (Patel et al., 2000) suggest
that in non-conditioned SCID patients there is a wave of thymopoiesis over the first 12
months post-transplant and then a steady decline in TREC levels over the following 12
years post-transplant. It is not known whether pluripotent haematopoietic stem cells from
the donor persist and preferentially differentiate into T-cells, or whether com m on
lymphoid progenitors in the donor product migrate into the thymus and differentiate into
T-cells. From the results presented here and the results of Patel et a i , it seems likely that
the latter has occurred and that long term loss o f thymic emigrants is the result, since
common lymphoid progenitors do not have the capacity for self renewal (Kondo et al.,
1997).
The majority o f patient samples from Newcastle General Hospital were from SCID
patients who received pre-transplant conditioning. It will be interesting in the future to
analyse thymic function in these long-term patients and consider whether pre-transplant
conditioning really is beneficial for long-term maintenance of thymic function. If this
turns out to be the case, the potential benefits will have to weighed against the increased
risk o f neutropenia, the need for red-cell and platelet transfusions, mucositis, veno-
occlusive disease, lung disease, growth suppression, sterility, and a 15 percent risk o f
subsequent cancer associated with conditioned transplants (Clement-De Boers et a i ,
1996). A more preferable option would be the administration o f HCT after non-
myeloablative transplants, an option which is currently being pursued by investigators at
Great Ormond Street Hospital (Amrolia et a i , 2000).
Given that there are many problems associated with the treatment of SCID using HCT, a
considerable amount o f work has been focused on developing gene therapy for
159

___________________________________________________________________________________________________________________________________________C h a p t e r 6
correction o f the genetic defect leading to SCID (Fischer et a i , 2000; Heim and Dunbar,
2000). This provides a feasible option since SCID usually develops due to a mutation in a
single gene (Amaiz-Villena et al., 1992; Chan et a i , 1994; Fischer, 1992; Giblett et at.,
1972; group, 1995; Noguchi et at., 1993; Fuel et at., 1998; Soudais et a i , 1993).
However, for patients with DiGeorge syndrome, the genetic complexity of the disease
(reviewed in (Botta et al., 2001)) does not make it a realistic target for intervention using
gene therapy strategies. HCT and transplantation o f thymic tissue have also been relatively
unsuccessful in treating DiGeorge syndrome (Borzy et al., 1979; Dictor et al., 1984;
Markert et al., 1998; Reece et al., 1981) although both therapies raise interesting research
questions as to the reconstitution of T-cells in the absence of a thymus or mechanisms o f
tolerance induction by grafted allogeneic thymus tissue. It will be interesting to see how
the treatment o f SCID, DiGeorge syndrome and other primary im m unodeficiency
diseases progresses over the coming years.
160

C h a p t e r 7
C h a p t e r 7
Conclusion
The aim o f this thesis was to assess the reconstitution o f the T-cell compartment post-
allogeneic HCT, The results demonstrated that memory and effector T-cells were the
predominant cell type that appeared during the early post-HCT recovery period (less than
6 months post-HCT) and that naïve T-cell recovery occurred later and was dependent on
thymic output. The inherent characteristics o f each cell type, the composition o f each
haematopoietic cell graft and the treatment regimen that HCT recipients are subjected to
are equally important in providing an explanation for these results. The immune system
o f the HCT recipient has been (for the most part) destroyed by intensive pre-transplant
chemo- and radiotherapy which leaves a vacant space to be repopulated by the incom ing
haematopoietic cell graft. I described earlier that T-cells, when transferred to a
lymphopénie environment, proliferate to fill the available space and some of the
mechanisms that control this process. The cells with the least stringent requirement to
undergo such homeostatic proliferation are o f an effector and memory phenotype.
Therefore, memory and effector T-cells proliferate in the post-HCT milieu and rapidly fill
the memory and effector T-cell “n iches”. The pre-transplant conditioning regimens
cause significant damage to normal healthy cells as well as malignant cells, resulting in the
elaboration o f many inflammatory cytokines that may also contribute to the rapid
expansion o f memory and effector cells.
It is possible that the intensive pre-transplant conditioning regimens may also damage
elements o f the thymus and result in a slow reconstitution o f naïve T-cells via thymic-
dependent pathways. However, my results were unable to conclusively demonstrate that
this was the case. In addition, naïve T-cells have more stringent requirements than
memory or effector T-cells to undergo homeostatic proliferation. Furthermore, recent
studies suggest that naïve T-cells convert to a memory phenotype during homeostatic
proliferation (Cho et a l , 2000; Tanchot et al., 2001). Therefore, the only way in which T-
cells with a naïve phenotype can be reconstituted is through thymic-dependent pathways.
Although I demonstrated that naïve T-cells can be produced from the thymus as early as
100 days post-transplant, the majority o f patients did not experience increases in TREC
levels or naïve T-cell numbers until 6-9 months post-transplant. Whether this reflects a
genuine delay caused by reorganisation (or repair) o f the thymic architecture, expansion
161

___________________________________________________________________________________________________________________________________________ C h a p t e r 7
o f thymic emigrants in the lymphopénie environment or a slower build up o f thymic
emigrants to within the detection limits o f the assay is unknown.
Overall, the results presented in this thesis demonstrate that the thymus plays a significant
role in the recovery o f the T-cell compartment after HCT. These results and data from
previous studies demonstrate that the thymus is essential for the reconstitution o f naïve T -
cells and therefore the reconstitution o f a diverse T-cell compartment. However, the extent
to which recent thymic emigrants contribute to formation o f the T-cell compartment after
HCT can be influenced by many factors. Increasing age has a significant adverse effect
on thymic output even though thymic T-cell production was demonstrated in many older
HCT recipients. The presence o f clinical acute or chronic GVHD also had an adverse
effect on thymic output.
The effects o f increasing age and chronic GVHD on thymic output were significant even
though they were analysed independently o f all other factors. In my study, no other
factors had a significant effect on thymic output when analysed across groups which
included a variety o f different age and GVHD groups. Therefore, future studies to
evaluate the factors that may affect thymic output in humans should be carried out in age-
matched control groups (preferably in young HCT recipients <18 years o f age) and in the
absence o f clinical GVHD. Administration o f CsA and irradiation to patients pre-and
post-HCT has been proposed to cause thymic damage and a reduction in thymic output.
However, the small groups o f patients in this study made evaluation o f these effects
virtually impossible.
The observation that GVHD has an adverse effect on thymic output raises a “chicken and
eg g ” question. Does acute GVHD prevent appropriate thymic education and tolerance
induction thereby leading to chronic GVHD or does the lack o f thymic education
(particularly in older patients) exacerbate the development o f acute and chronic GVHD
by not establishing central tolerance in the first place? The establishment o f central
tolerance is dependent on deletion o f the self-reactive TCR repertoire in the thymus.
However, the role o f the thymus in establishing tolerance o f the haematopoietic cell graft
to the recipient post-HCT is unclear. While a significant number o f mature T-cells are
transplanted with each haematopoietic cell graft (even in T-cell depleted HCT recipients)
it is possible that the education o f T-cell precursors is essential for establishing tolerance
of the haematopoietic cell graft to the recipient’s tissues. This may be a direct result o f
restoring the T-cell population exclusively via thymic-dependent pathways. Alternatively,
establishing tolerance after HCT may be dependent on production o f regulatory T-cell
subsets such as the CD4"^CD25 subset that has been described in recent studies (and
possibly other as yet unidentified regulatory T-cell subsets). It would be useful in future
studies to analyse the reconstitution o f CD4^CD25^ T-cells in relation to thymic output
162

____________________________________________________________________________________________________________________________________________C h a p t e r 7
and to further relate CD4 CD25^ T-cell reconstitution to the development (or absence) o f
acute or chronic GVHD post-HCT.
A significant question that arises from this work is whether strategies to reverse age-related
thymic involution would be beneficial to the transplant recipient. The rationale for such a
strategy would be to restore a diverse T-cell repertoire as rapidly as possible after HCT
with a view to reducing morbidity and mortality due to infections exacerbated by
deficiencies in T-cell immunity. However, we do not know the level o f TCR diversity that
protects against infections compared with the diversity at which patients are susceptible. It
would seem logical that increasing the number o f TCR specificities would enable an
increased diversity o f pathogen responses. However, the cross-reactivity inherent in TCR
binding means that immunity to a wide range o f pathogens could be conferred by
relatively few TCR clones. A recent study by Storek et al. analysed immune reconstitution
in a cohort o f long-term post-HCT survivors (20-30 years post-HCT). They demonstrated
that long-term survivors, while unable to regenerate normal number o f thymic emigrants,
did not have a significantly increased risk o f infection compared with their original
donors or normal individuals (Storek et a i , 2001). However, this analysis does not
provide a conclusive answer to the short-term problem o f susceptibility to infectious
pathogens.
As mentioned previously, thymic output in younger patients can be detected by 3 months
post-HCT, but is delayed until 6-9 months post-HCT in adult HCT recipients. Whether this
translates into a clinically significant increased risk o f older patients developing infections
in the short-term after HCT compared to younger patients is unknown. Evaluation o f TCR
diversity, TREC levels and the incidence o f infections between a large hom ogeneous
group of adult and paediatric HCT recipients during the first year post-HCT will be
essential to answer this question. Furthermore, it would be useful to analyse the
development o f antigen-specific responses in patients who experience “thymic rebou n d ”
compared with those who do not. Previous studies have compared global T-cell responses
to tetanus toxin (TT) in patients who experienced or did not experience “thym ic
rebound” and demonstrated that TT responses did not develop until after “thym ic
rebound” had taken place (Roux et a i , 2000). However, due to the small number o f
patients in this study, the clinical significance o f this observation was not addressed (other
than the fact that vaccinations should possibly be delayed until after thymic rebound is
demonstrated). An interesting approach which has been enabled recently by the
development o f MHC Class I tetramers (Altman et al., 1996), would be to monitor a
variety o f anti viral, antigen-specific responses (e.g. CMV or EBV) post-HCT. The
reconstitution o f anti-CMV and -EBV T-cell responses post-HCT has already been
analysed by several investigators (Aubert et al., 2001; Cwynarski et al., 2001; Liu et al.,
2002; Yoshimi et al., 2002). It will be interesting in future studies to analyse the
reconstitution o f other anti viral (and also Class II restricted CD4^ T-cell responses when
163

____________________________________________________________________________________________________________________________________________C h a p t e r 7
Class II tetramers become available) immune responses post-HCT and to relate the
development o f these responses (or lack of) to thymic output.
The data from Chapter 6 on thymic output in children with primary im m unodeficiency
diseases illustrate several key points. First, it seems likely that transplantation o f SCID
patients in the absence o f pre-transplant conditioning (and hence stem cell engraftment)
will lead to exhaustion o f T-cells (and possibly other lineages) and increased susceptibility
to infections. In addition, the lack o f durable stem cell engraftment in these non
conditioned patients may prove to be a significant problem for gene therapy approaches
currently being developed for the treatment o f SCID. Indeed, these concerns are
significant enough that investigators at Great Ormond Street Hospital are now
administering pre-transplant conditioning to SCID patients as part o f a gene therapy
protocol. However, it is unknown whether the lack o f stem cell engraftment in non
conditioned SCID HCT-recipients is a simple “space” issue or whether the transplanted
stem cells are actively rejected by an as yet undefined immunological mechanism. The
development o f non-myeloablative conditioning regimens may go some way towards
making the compromise between long-term maintenance o f immune function and the
risks inherent in administering conventional myeloablative conditioning regimens. In
addition, the results from the SCID and DiGeorge patients suggest that the TREC assay
can be a valuable tool for assessing the overall immune competence o f these patients in
co-operation with standard immunologic evaluation techniques. Consideration should
therefore be given to using the TREC assay as a routine tool for monitoring o f HCT and
immunodeficiency patients.
Finally, these results further demonstrate the importance o f co-operation between the
fields o f Immunology and Haematology. Immunological monitoring using measurements
o f T-cell phenotype and function will continue to have an important role in post-HCT
evaluations. As techniques improve further it may also be possible to monitor antigen-
specific responses to a wide variety o f pathogens and possibly to use adoptive
immunotherapy to “fill gaps” in the TCR repertoire. While this approach does not seem
likely to be in common practice for some time (due to the difficulties in expanding CTL
clones in vitro), it may be possible to improve immune reconstitution by reactivating the
thymus. The fact that thymic output was detected in a significant number o f adult
recipients in my study, coupled with preliminary observations from other groups (Min et
a i , 2000), suggests that this approach may be feasible. In addition, stimulating thymic-
dependent pathways post-HCT may have a positive influence on re-establishing central
and peripheral tolerance. Clearly, the results presented here are only the beginning in
understanding the exact role that the thymus plays in restoring the T-cell repertoire after
HCT in both young and aged individuals. Furthermore, the type o f immune reconstitution
monitoring described in this thesis could (and possibly should) be adopted for routine
haematology laboratories to assess the reconstitution o f the immune system post-HCT.
164

C h a p t e r 7
This approach will also prove useful when analysing the effectiveness o f strategies aimed
at reactivating the thymus and improving the quality o f immune reconstitution post-HCT.
165

Appendix
A I ’I’I-.NIMX
Xmn I 2009
S ea l 1890
pGEPT-T Easy /aeZ V tdor j
(3015bo)
A pa 1 14Aatll 20S ph\ 26B s iZ I 31Nco 1 37BalZ 1 43N o l\ 43Sac II 49fc o P 1 52
Spe 1 64EcoR 1 70Not 1 77ÔS/ZI 77Psi 1 88Sa/I 90A/del 97SacI 109B s iX \ 118Nsi\ 127
141t SPG
1 Sian
TREC PCR Product
AAAGAGGGCAGCCCTCTCCAAGGCAAAATGGGGCTCCTGTGGGGAACAGAGGGGTCjCCTCTGTCAACAAAGGTGATGCCACATC CCTTTCAACCA TG CTG A CACCTCTG GTnTTG TA A AG G TG CCCACTCCTG TG {signal joint )CACGGTGATGCATAGGCACCTGCACC CCGTGCCTAAACCCTGCAGCTGGCACGGGCCCTGTCTGCTCTTCATTCACCGTTCTCACGAGTTGCAATAAGTTCAGCCCTCCATG TCACACTGTGTTTrCCATCCTGGGGAGTGTTrCACAGCTATCCCAAGCCCCACGCTGACGAATCACGGCCGAAAACACACTCTGAT GCCAGCACAGACCACGGAGCAAATGTCAGACAAGATCAGCCT
TREC standard PCR product
AAAGAGGGCAGCCCTCTCCAAGGCAAAATGGGGCTCCTGTGGGGAACAGAGGGGTGCCTCTGTCAACAAAGGTGATGCCACATC CCTTrCAACCATGCTGACACCTCTGGTTTTTGTAAAGGTGCCCACTCCTGTGGTGGTGCACGGTGATGCATAGGCACCTGCACCCC GTGCCTAAACCCTGCAGCTGGCACGGGCCCTGTCTGCTCnCATTCACCCACAGCTATCCCAAGCCCCACGCTGACGAATCACGGC CGAAAACACACTCTGATGCCAGCACAGACCACGGAGCAAATGTCAGACAAGATCAGCCT
Figure AI : TREC standard construct fo r radiolabelled QC-PCR
T h e m od ified T R E C am plicon was c lo n ed into the T -overh an g in the vec to r and the p lasm id w as g ro w n up as
d escrib ed in the m a te ria ls and m ethods. T he am p lico n g enera ted from the standard c o n s tru c t w as 3 0 0 b p
co m p ared w ith a 360bp am plicon g en era ted from norm al con tro l and p a tien t b lo o d sa m p le s. T he sequence o f
the T R E C PC R p roduct and the T R E C standard PCR product are show n.
166

AIM’H NDIX
Y 11 cri-n -tij r . ■ ‘•'y-A c;,c .'ïc 'xA ' A rrv r :c -A -fE r '5t ^ T : - a .C OCCAac, c ~-a t 1‘TA'ï O'.. •iACO c-l- r : i /s
CTCTOTTCTT Tv^TCCC.TAC'i CC /AL I.'AVIC UUÛT i JCAL A AJ.ICC A JTUC C ;"u\TC r-l','.'r
'.V. I M.-.,l 21I l I I I
c T i : ;V '.3 :T ,v i ' üV A T L V J'.ucT u l c u î ATc;::A ;:rA i:--A A i::r;c: :% - i: ( 'A c ;T J Lc A C ’-T c i^ A T A z c : '; .c y : 'i '( :c :A A c c A T ic i c r n lA n c c T A n 'i T o a t c a t -t-c c c c o c c o t c a c a
c::n\rç;j\'i Tc; ag" O ÎA C C T fA i-O T C C Blunt PCR Product
.• tîjsil I à! î I-.xrtI Iccrojjvn'ci' scA.a.A.A
ÜCj\C 1TA/A:A CdT.-TAT•■'Yl TX p cn cM"|Yi
TCC«TC CAC TÜÀCcUVC'JV AïCïAGA Û :CC/LYl;LüL v:GjAIA{:T::A'TAAncp pG^ATCAÇTACC:ACi.üic ACLCCcuLcc AUCicjTAcc TA::A'r::TC::n nc'TTAAn
i\1 : ) forwa-d (-2l):< U-Iir; iiç iGTlAiTAiTAc; /v u .UACTGU ::i:ürc::Tr:'r AcjAACïjTffvT CACTGWAAA ACCCTC3C3T 4>CCACCATAATC TT.V.n-CiACC CnÇAnnAAAA TCPTOCAGCA CTOA'l'CCT'.T ICCCALAUU .\
B lunt
Figure A2: Standard construct fo r the detection of TREC using Real-Time PCR
T h e stan d ard co n stru c t w as p repared as desc rib ed in the m aterials and m ethods. T he am plicon g en e ra ted du ring
R ea l-T im e PC R w as 107bp.
167

A i' i ' t :N i ) ix
100000- 0.93- 0.88
X
ïU W OSH 100 4
1000 -
50 7525
Age (years)
Figure A3: Age-matched healthy control TREC values
C D 4 (O ) and C D 8 ( • ) TREC lev e ls were m easured by Dr D aniel D ouek u sin g the sam e R eal-T im e PC R
d e tec tio n m ethod d escribed in C h a p te r 2 (M ate ria ls and m ethods). S ince the c o n c e n tra tio n o f the s ta n d a rd s
w as co n firm ed to be the sam e as those used by Dr D o u e k 's la b o ra to ry . 1 used these values as m y a g e -m a tch ed
co n tro l g ro u p .
168

_____________________________________________________________________________________________________________________________________________ A p p e n d ix
The following tables list the results of statistical analyses of the factors affecting thymic
output and reconstitution of T-cell subsets post-HCT (discussed in Chapter 4). For each
table, the factors listed were analysed independently of all other factors. Patient groups
were defined as described in Chapter 4 and were compared using the Mann Whitney U-
test. A P-value of <0.05 was considered significant. Significant P-values are highlighted in
red.
Table A l: Factors affecting overall reconstitution o f the T-cell compartment post-HCT
Parameter Total CD3 Total CD4 Total CDS
3 6 9 12 3 6 9 12 3 6 9 12
Patient a g e 0.013 0.016 0.123 0.729 0 .008 0.221 0.400 0.064 0.003 0.061 0.211 0.602
cGVHD 1.000 0.236 0.563 0.899 0.258 0 .190 0.710 0.764 0.346 0.449 0.536 0.799
S tem cell 0 .080 0.179 0.939 0.675 0.037 0 .865 0.483 0.878 0.092 0.671 0.943 0 .783so u rc e
Donor type 0.045 0.043 0.267 0.012 0.274 0.567 0 .125 0.036 0.027 0.266 0.293 0.103
Cam path-1 H 0.042 0.108 0.362 0.341 0.003 0.119 0 .113 0 .583 0.024 0.324 0.356 0.544
T-cell depletion 0.022 0.091 0.095 0.084 0.378 0.061 0.182 0 .107 0.116 0.150 0.113 0.404
Table A2: Factors affecting reconstitution o f naïve CD4* T-cells and CD4 TREC
Parameter3
Naïve6
CD49 12 3
CD46
TREC9 12
Patient age 0.2314 0.2659 0.1011 0.0005 0.3725 0.0190 0.0136 0.0044
cGVHD 0.0714 0.3255 0.0676 0.0130 0.1137 0.3270 0.0016 0.0064
Stem cell source 0.1751 0.7958 0.5864 0.1066 0.7365 0.6721 0.2459 0.1474
Donor type 0.0255 0.0954 0.0679 0.8815 0.1863 0.4153 0.6089 0.8821
Campath-1 H 0.0402 0.3539 0.5457 0.1604 0.4834 0.8758 0.4234 0.3936
TBI 0.2063 0.7464 0.6571 0.0722 0.1391 0.0833 0.3694 0.1195
T-cell depletion 0.0004 0.0005 0.0400 0.2325 0.0330 0.0128 0.8148 0.4361
169

A p p e n d ix
Table A3: Factors affecting reconstitution o f naïve CD8^ T-cells and CD8 TREC
Parameter Naïve CD8 CDS TREC
3 6 9 12 3 6 9 12
Patient a g e 0.2418 0.1822 0.1457 0.0010 0.6349 0.0515 0.1011 0 .0028
cGVHD 0.7085 0 .7833 0.3154 0.0023 0 .3632 0 .1267 0 .0545 0.0147
S tem cell source 0.2411 0.3295 1.0000 0.1066 1.0000 0.7437 0 .5200 0 .1375
Donor type 0.0471 0 .1033 0.8345 0.6547 0.1367 0.1745 0 .2712 0.6221
Cam path-1 H 0.0416 0 .6867 0.1903 0 .0743 0.2995 0.7775 0.9314 0 .3782
TBI 0 .1358 0.6318 0 .6922 0 .0215 0.2259 0.1279 0.5518 0.0956
T-cell depletion 0 .0016 0.0161 0.0400 0 .1465 0.0167 0.0267 0.3865 0.2470
Table A4: Factors affecting reconstitution o f memory and effector CD4^ T-cell subsets
Parameter Memory CD4 Effector CD43 6 9 12 3 6 9 12
Patient a g e 0.0058 0.0710 0.0831 0.6009 0 .0096 0 .0216 0.1728 0 .0338
cGVHD 0.1532 0.7124 0 .4969 0.0864 0 .1603 0 .3593 0.1728 0 .1235
S tem cell source 0 .0217 0.8377 0.2214 0 .6573 0 .0227 0 .4325 0 .2573 0 .7714
Donor type 0.2018 0.3070 0 .1529 0 .4339 0.8196 0 .8984 0 .6218 0 .0624
C am path-1 H 0.0012 0 .1077 0.1359 0.1397 0 .1260 0.9476 0 .3865 0.0116
TBI 0 .1388 0.9539 0 .3006 0 .1228 0.3103 0 .4523 0.2564 0 .9247
T-cell depletion 0.3472 0.1564 0 .0939 0.7226 0 .6025 0 .8690 0.6065 0 .4384
Infection 0.6713 N/A N/A 0.2284 0 .3750 N/A N/A 0.4136
Table A5: Factors affecting reconstitution o f non-naïve and CD8^CD57^CD28' subsets
Parameter3
Non-naïve6
CDS9 12 3
CDS+57+2S6 9 12
Patien t a g e 0 .0018 0 .0569 0 .1457 0.0127 0.0029 0.0418 0.2370 0 .0247
cGVHD 0.3431 0 .3568 0.4082 0.0743 0.2888 0.3977 0 .3977 0 .0743
Stem cell so u rce 0 .0726 0.7074 0 .9278 0.1465 0.1335 0.4735 0.9278 0.2709
D onor type 0.0176 0.1602 0 .5543 0.2480 0 .0512 0.1477 0.1477 0 .4106
Cam path-1 H 0.0147 0 .2935 0.4363 0.0795 0.0568 0.2004 0.2004 0.1166
TBI 0.6721 0.4381 0.2783 0.7768 0.4334 0 .4174 0.4174 0.6141
T-cell depletion 0 .1233 0 .1564 0 .2224 0.8213 0.5294 0.0927 0 .0927 1.0000
Infection 0.3860 N/A N/A 0.4908 0.0906 N/A N/A 0.4136
170

____________________________________________________________________________________________________________________________________________ A p p e n d ix
Study proposal sent to the Royal Free Hospital E th ica l
Practices Subcommittee
Aims and objectives o f project
We aim to analyse the reconstitution of the T cell compartment post bone marrow
transplantation. We aim to study the diversity of the T cell repertoire through analysis o f
the TCR VB chain usage. In addition we aim to demonstrate that any increase in the
diversity of the TCR VB chain repertoire correlates with the emergence of naive T cells
which have recently exited the thymus. This is enabled by development o f a new
technology which detects recent thymic emigrants in peripheral blood.
Scientific background o f study
Both extrathymic and intrathymic pathways of T-cell reconstitution can be exam ined
using two strategies, firstly through evaluation of the T-cell receptor repertoire and
secondly by analysis of T-cell receptor gene rearrangement events. Both techniques
require RNA and DNA which can be obtained from peripheral blood.
The role o f the thymus in seeding the peripheral T-cell compartment in later life and
particularly post-BMT is unclear. This is in part due to the fact that in humans, there was
previously no known method to distinguish phenotypically between cells that have
recently emigrated the thymus and long-lived naive cells in the periphery and therefore to
quantify thymic output. A new technique termed the "TREC assay" facilitates
identification of recent thymic emigrants. TCR-rearrangement excision circles (TRECs)
are generated during thymic education and are the products of excisional rearrangement
o f TCR genes. The TCR alpha chain locus in its germ line configuration contains a large
portion o f TCR delta genes. During thymic education the T-cell differentiates to becom e
either an alpha-beta, or a gamma-delta T-cell, a process which requires rearrangement o f
either the alpha or delta TCR loci. Commitment to the alpha-beta T-cell lineage results in
the excision o f TCR delta genes (which are no longer needed by the committed cell) from
the genome which generates TCR-rearrangement excision circles (TRECs). TRECs are
stable, are not duplicated during mitosis, and are therefore diluted out with each cycle o f
cell division. This means that only cells which have recently exited the thymus will have a
detectable level of TRECs. We are in the process o f setting up the "TREC assay" at the
Anthony Nolan. This work will provide insight into thymus activity post-bone marrow
transplantation and may lead to strategies aimed at reactivating the thymus.
171

A i'1>i ;n i )IX
Participant consent form
PARTIC IPANT CONSENT FORM
TITLE OF PROJECT
A n a l y s i s o f T C e l! R e c o n s titu tio n b y R ocunt T hym ic E m ig r a n t s P o st B o n e M arrow T r a n sp la n ta tio n .
T h e p a tie n t s h o u ld c o m p le t e tn e w h o le o f th is s h e e t t t ie m s e lv e s
H a v e y o u r e a d th e P a tie n t Inform ation S h e e t s ' ) Y E S / N O
H a v e y o u h a d a n o p p o r tu n ity to a s k q u e s t io n s a n d d i s c u s s Y E S I N Oth is s tu d y ?
H a v e y o u r e c e iv e d s a t is fa c to r y a n s w e r s to alt y o u r q u e s t io n s ? Y E S / N O
H a v e y o u r e c e iv e d e n o u g h in form ation a b o u t th e s tu d y ? Y E S / N O
T o w h o m h a v e y o u s p o k e n ? Or / Mr / Mrs,________________________________________
D o y o u u n d e r s ta n d th a t y o u a r e f r e e to w tin d r a w from th e s tu d y a t a n y t im e , w ith o u t h a v in g to g iv e a r e a s o n forw ith d r a w in g a n d w itfto u t a f fe c t fr g y o u r fu tu re m e d ic a l c a r e ? Y E S I N O
D o y o u a g r e e to e n t e r y o u r th is s tu d y a n d in d o in g s o g iv e p e r m is s io n for th e r e s e a r c h e r s to h a v e a c c e s s to y ou rmedical notes? YES ! NO
D o y o u g iv e p e r m is s io n for u s to n otify you r G P th a t y o u h a v ee n t e r e d thi s s tu d y ? Y E S I N O
D o y o u a g r e e to e n te r in th is s tu d y ? Y E S I N O
P a t ie n t 's n a m e _____________________________________________________________________(in b lo c k le t te r s )
S ig n a t u r e D a te I___ I_____ I___I
D r's s i g n a t u r e D a te I___ I_____ I___I
D r's n a m e _____________ _____________________________________________________________(in b lo c k le t te r s )
P a r e n t /g u a r d ia n (if u n d a r i 8 ) D a te I____ I I I
N a m e (in b lo ck le t t e r s ) _________________________________________ ______________ _______________
Fite on e copy in poljcnls notes. o«e ospy in CRF and on e copy lo palisni.
172

____________________________________________________________________________________________________________ Ai’Pi:nuix
Participant information sheet
PARTICIPANT INFORMATION SHEET
Title of Project
Analysts oi T Cell Reconstituîlon by Rcconl Thymic Emigrants Post-Bone M arrow Transplantation.
We at the Anthony Nolan Research Institute are currently embarking on a project to investigate tne reconstitution of the immune system aller Dene marrow transplantation. As you will be awnre, the immune system ts severely depleted alter pre-transplant conditioning. Research has shown that the thymus plays a major role in immune system reconstitution, but the full ex ten t ot this role still romains unclear. This project uses newly developed techniques which will provide valuable mformation about the aciivily cl trie ihymus In patients after bone-marrow transplantation.
To help us carr^f out this work we require 2ûmis of blood. These sam ples would be taken at the same time as the regular checks you will have al the hospital and will not require you to have any extra venepunctures,
TRANSPt_ANT RECIPIENTS- blood is roquircd pnor to transplant and al 0, 3, 6, 9 and 12 months afterwards.
DONORS- bicod is required at once at your pre-donation health check.
The çq'ls e x t ru d e d from Utsae samples will only be used for the resea rch project you have agreed to lake part in.
I am willing to take part in this study and agreo to provide the oamplos requested. Your medical records will be examined by researchers from The Anthony Nolan R esearch Institute, who are outside the employment of the NH5.
173

____________________________________________________________________________________________________________________________________________A p p e n d ix
Publica t ions
The following publications were generated during the course o f this thesis. In addition, I
have included a list of abstracts accepted for oral or poster presentations at national and
international conferences.
Paul R Fallen, Louise McGreavey, J Alejandro Madrigal, Mike Potter, Mark Ethel, H Grant
Prentice, Paul J Travers (2001). Reconstitution o f the T-cell compartment post allogeneic
haematopoietic stem cell transplant (submitted).
Paul R Fallen, Louise McGreavey, J Alejandro Madrigal, Mike Potter, Mark Ethel, H Grant
Prentice, Paul J Travers (2001). Identification o f non-naïve CD4+CD45RA+ T-cell subsets
in recipients of allogeneic haematopoietic stem cell transplants (submitted).
Shara B.A. Cohen, Joanna Wooley, Katarzyna Bogunia Kubik, Prasad Natarajan, Reena
Kotecha, Lavina Belaramani, Paul R. Fallen, Isabel Perez-Cruz and J Alejandro Madrigal
(2000). Macrophage Colony Stimulating Factor (M-CSF) within cord blood sera may be
partially responsible for the reduced proliferation of cord blood T-cells. Eur.Cytokine
Netw. 11 (4): 608-17.
Isabel Perez-Cruz, Paul Fallen, J. Alejandro Madrigal, Shara B.A. Cohen (2000). Naive T
cells from cord blood have the capacity to make Type 1 and Type 2 cytokines.
Immunology Letters 75 (1), 85-88.
K. Bogunia-Kubik, I. Perez-Cruz, P. R. Fallen, J.A Madrigal, S B.A. Cohen (2000). Cord
blood (CB) lymphocytes have a low frequency of cytokine producing T cells due to a high
threshold For Activation. Immunology Letters 72 (3), 145-146.
P. Fallen, S.B.A.Cohen (2000). Cord Blood T Cells. In: CB Characteristics: Role In Stem
Cell Transplantation. Ed: S.B.A. Cohen, E. Gluckman, P. Rubinstein, J.A. Madrigal. M.
Dunitz, Lond. UK, 39-59.
S.B.A. Cohen, I. Perez-Cruz, P. Fallen, E. Gluckman, J.A. Madrigal (1999). Analysis o f
the cytokine production by cord and adult blood. Human Immunol. 60 (4): 331-336 .
Review.
174

________________________________________________________________________________________________________________________________ A p p e n d ix
A b s tra c t s
PR Fallen, LE McGreavey, M Potter, M Ethel, HO Prentice, JA Madrigal, PJ Travers
(2000).
Reconstitution o f the T-cell Compartment Post-Allogeneic Stem Cell Transplant.
http:24/2/02/www.ukcbig.org.uk/meeting2000/abstracts.html Abstract A l
Louise McGreavey, Paul R. Fallen, Mark Ethel, Mike Potter, H. Grant Prentice, Paul J.
Travers, J. Alejandro Madrigal (2000). Analysis of Reconstitution of the T-cell
Compartment in Patients Undergoing Stem Cell Transplantation. ASHI 2000, Oral
Presentation, International Scholar Award
PR Fallen, LE McGreavey, M Potter, M Ethel, HG Prentice, JA Madrigal, PJ Travers
(2000). Reconstitution of the T-cell Compartment Post-Allogeneic Stem Cell Transplant.
Eur. J. Immunogenetics. 27 (4), p275 A7.2, Oral Presentation for Promega Young
Scientist Award
Louise McGreavey, Paul Fallen, Paul Travers, Mike Potter, Alejandro Madrigal (2000).
Analysis of T-cell Receptor Reconstitution by Recent Thymic Emigrants and V|3 Chain
Repertoire in Patients Undergoing Bone Marrow Transplantation. Keystone 2000 B4 T-
Lymphocyte Activation (Abstract 335), Poster Presentation.
P R . Fallen, K. Bogunia-Kubik, I. Perez-Cruz, M. Tesfamicael, J.A. Madrigal, S.B.A.
Cohen (1999). The phenotypic and functional characteristics of cord blood (CB) and adult
natural killer cells are not comparable. Eur. J. Immunogenetics. 26, p53 A4.2, Oral
Presentation
I. Perez-Cruz, P R. Fallen, J.A. Madrigal, S.B.A. Cohen (1999). CD45RA-I-CD34- naive
lymphocytes from cord blood can achieve high IL-2 and IL-4 production compared to
their adult counterparts Eur. J. Immunogenetics. 26, p53 A4.3
K. Bogunia-Kubik, I. Perez-Cruz, P. Fallen, M. Tesfamicael, J.A. Madrigal, S.B.A. Cohen
(1999). Does the cellular microenvironment explain the reduced cytokine production o f
cord blood lymphocytes? Eur. J. Immunogenetics. 26, p54 A4.4
175

B ib l io g r a p h y
Bibliography
Abbas, A. K., Murphy, K. M., and Sher, A. (1996). Functional diversity of helper T
lymphocytes. Nature 383, 787-93.
Abboud, M., Xu, F., La Via, M., and Laver, J. (1992). Study o f early hematopoietic
precursors in human cord blood. Exp Hematol 20, 1043-7.
Aderem, A., and Ulevitch, R. J. (2000). Toll-like receptors in the induction o f the innate
immune response. Nature 406, 782-7.
Adibzadeh, M., Pohla, H., Rehbein, A., and Pawelec, G. (1995). Long-term culture o f
monoclonal human T lymphocytes: models for immunosenescence? Mech Ageing Dev
83, 171-83.
Ahmed, R., and Gray, D. (1996). Immunological memory and protective immunity:
understanding their relation. Science 272, 54-60.
Akira, S., Takeda, K., and Kaisho, T. (2001). Toll-like receptors: critical proteins linking
innate and acquired immunity. Nat Immunol 2, 675-80.
Alam, S. M., Travers, P. J., Wung, J. L., Nasholds, W., Redpath, S., Jameson, S. C., and
Gascoigne, N. R. (1996). T-cell-receptor affinity and thymocyte positive selection. Nature
381, 616-20.
Allen, R. D. (1993). Differential cytokine expression in acute and chronic murine graft-
versus-host-disease. European Journal of Immunology 23, 333-337.
Allen, R. D., Staley, T. A., and Sidman, C. L. (1993). Differential cytokine expression in
acute and chronic murine graft- versus-host-disease. Eur J Immunol 23, 333-7.
Alt, F. W., Oltz, E. M., Young, F., Gorman, J., Taccioli, G., and Chen, J. (1992). VDJ
recombination. Immunol Today 13, 306-14.
Altman, J. D., Moss, P. A., Goulder, P. J., Barouch, D. H., McHeyzer-Williams, M. G., Bell,
J. I., McMichael, A. J., and Davis, M. M. (1996). Phenotypic analysis of antigen-specific T
lymphocytes. Science 274, 94-6.
176

B ib l io g r a p h y
Amrolia, P., Caspar, H. B., Hassan, A., Webb, D., Jones, A., Sturt, N., Mieli-Vergani, G.,
Pagliuca, A., Mufti, G., Hadzic, N., Davies, G., and Veys, P. (2000). Nonmyeloablative
stem cell transplantation for congenital immunodeficiencies. Blood 96, 1239-46.
Anderson, G., Hare, K. J., Platt, N., and Jenkinson, E. J. (1997). Discrimination between
maintenance- and differentiation-inducing signals during initial and intermediate stages
of positive selection. Eur J Immunol 27, 1838-42.
Anderson, G., Jenkinson, E. J., Moore, N. C., and Owen, J. J. (1993). MHC class Il-positive
epithelium and mesenchyme cells are both required for T-cell development in the
thymus. Nature 362, 70-3.
Andrew, D., and Aspinall, R. (2001). 11-7 and not stem cell factor reverses both the
increase in apoptosis and the decline in thymopoiesis seen in aged mice. J Immunol 166,
1524-30 .
Antica, M., and Scollay, R. (1999). Development of T lymphocytes at extrathymic sites. J
Immunol 163, 206-11.
Antin, J. H., Bierer, B. E., Smith, B. R., Ferrara, J., Guinan, E. C., Sieff, C., Golan, D. E.,
Macklis, R. M., Tarbell, N. J., Lynch, E., and et al. (1991). Selective depletion o f bone
marrow T lymphocytes with anti-CD5 monoclonal antibodies: effective prophylaxis for
graft-versus-host disease in patients with hematologic malignancies. Blood 78, 2139-49.
Apperley, J. F., Mauro, F. R., Goldman, J. M., Gregory, W., Arthur, C. K., Hows, J., Arcese,
W., Papa, G., Mandelli, F., Wardle, D., and et al. (1988). Bone marrow transplantation for
chronic myeloid leukaemia in first chronic phase: importance o f a graft-versus-leukaemia
effect. Br J Haematol 69, 239-45.
Arguello, J. R., Little, A. M., Pay, A. L., Gallardo, D., Rojas, I., Marsh, S. G., Goldman, J.
M., and Madrigal, J. A. (1998). Mutation detection and typing o f polymorphic loci
through double-strand conformation analysis. Nat Genet 18, 192-4.
Amaiz-Villena, A., Timon, M., Corell, A., Perez-Aciego, P., Martin-Villa, J. M., and
Regueiro, J. R. (1992). Brief report: primary immunodeficiency caused by mutations in
the gene encoding the CD3-gamma subunit of the T-lymphocyte receptor. N Engl J Med
327, 529-33.
Arnold, B., Dill, O., Kublbeck, G., Jatsch, L., Simon, M. M., Tucker, J., and Hammerling,
G. J. (1988). Alloreactive immune responses o f transgenic mice expressing a foreign
transplantation antigen in a soluble form. Proc Natl Acad Sci U S A 85, 2269-73.
177

B iBLIOC'iRAPHY
Arstila, T. P., Casrouge, A., Baron, V., Even, J., Kanellopoulos, J., and Kourilsky, P.
(2000). Diversity o f human alpha beta T cell receptors. Science 288, 1135.
Ash, R. C., Casper, J. T., Chitambar, C. R., Hansen, R., Bunin, N., Truitt, R. L., Lawton, C.,
Murray, K., Hunter, J., Baxter-Lowe, L. A., and et al. (1990). Successful allogeneic
transplantation of T-cell-depleted bone marrow from closely HLA-matched unrelated
donors. N Engl J Med 322, 485-94.
Ash, R. C., Horowitz, M. M., Gale, R. P., van Bekkum, D. W., Casper, J. T., Gordon-Smith,
E. C., Henslee, P. J., Kolb, H. J., Lowenberg, B., Masaoka, T., and et at. (1991). Bone
marrow transplantation from related donors other than HLA- identical siblings: effect o f
T cell depletion. Bone Marrow Transplant 7, 443-52.
Aspinall, R., and Andrew, D. (2000). Thymic atrophy in the mouse is a soluble problem
of the thymic environment. Vaccine 18, 1629-37.
Aspinall, R., and Andrew, D. (2000). Thymic involution in aging. J Clin Immunol 20,
250-6 .
Atkinson, K., Hansen, J. A., Storb, R., Goehle, S., Goldstein, G., and Thomas, E. D. (1982).
T-cell subpopulations identified by monoclonal antibodies after human marrow
transplantation. I. Helper-inducer and cytotoxic-suppressor subsets. Blood 59, 1292-8.
Aubert, G., Hassan-Walker, A. P., Madrigal, J. A., Emery, V. C., Morte, C., Grace, S., Koh,
M. B., Potter, M., Prentice, H. G., Dodi, I. A., and Travers, P. J. (2001). Cytomegalovirus-
specific cellular immune responses and viremia in recipients of allogeneic stem cell
transplants. J Infect Dis 184, 955-63.
August, C. S., Rosen, F. S., Filler, R. M., Jane way, C. A., Markowski, B., and Kay, H. E.
(1968). Implantation o f a foetal thymus, restoring immunological competence in a patient
with thymic aplasia (Digeorge's syndrome). Lancet 2, 1210-1.
Baars, P. A., Maurice, M. M., Rep, M., Hooibrink, B., and van Lier, R. A. (1995).
Heterogeneity of the circulating human CD4+ T cell population. Further evidence that the
CD4+CD45RA-CD27- T cell subset contains specialized primed T cells. J Immunol 154,
17-25.
Baars, P. A., Ribeiro Do Couto, L. M., Leu sen, J. H., Hooibrink, B., Kuijpers, T. W., Lens,
S. M., and van Lier, R. A. (2000). Cytolytic mechanisms and expression o f activation-
178

B ib l io g r a p h y
regulating receptors on effector-type CD8+CD45RA+CD27- human T cells. J Immunol
765, 1910-7.
Babbitt, B. P., Allen, P. M., Matsueda, G., Haber, E., and Unanue, E. R. (1985). Binding o f
immunogenic peptides to la histocompatibility molecules. Nature 317, 359-61.
Babcock, S. K., Gill, R. G., Bellgrau, D., and Lafferty, K. J. (1987). Studies on the two-
signal model for T cell activation in vivo. Transplant Proc 79, 303-6.
Balduzzi, A., Gooley, T., Anasetti, C., Sanders, J. E., Martin, P. J., Petersdorf, E. W.,
Appelbaum, F. R., Buckner, C. D., Matthews, D., Storb, R., and et al. (1995). Unrelated
donor marrow transplantation in children. Blood 86, 3247-56.
Banchereau, J., Briere, F., Caux, C., Davoust, J., Lebecque, S., Liu, Y. J., Pulendran, B., and
Palucka, K. (2000). Immunobiology of dendritic cells. Annu Rev Immunol IS, 767-811.
Barnes, D., MJ., C., and Loutit, J. (1956). Treatment of murine leukaemia with x-rays and
homologous bone marrow. Br Med J 2, 626.
Barnes, P. J., and Adcock, 1. (1993). Anti-inflammatory actions o f steroids; molecular
mechanisms. Trends Pharmacol Sci 14, 436-41.
Basson, M. A., and Zamoyska, R. (2000). The CD4/CD8 lineage decision: integration o f
signalling pathways. Immunol Today 27, 509-14.
Batliwalla. P., Monteiro, J., Serrano, D., and Gregersen, P. K. (1996). Oligoclonality o f
CD8+ T cells in health and disease: aging, infection, or immune regulation? Hum
Immunol 48, 68-76.
Beatty, P. G., Hansen, J. A., Longton, G. M., Thomas, E. D., Sanders, J. E., Martin, P. J.,
Bearman, S. 1., Anasetti, C., Petersdorf, E. W., Mickelson, E. M., and et al. (1991). Marrow
transplantation from HLA-matched unrelated donors for treatment o f hem atologic
malignancies. Transplantation 57, 443-7.
Beck, R., and Lam-Po-Tang, P. (1994). Comparison of cord blood and adult b lood
lymphocyte normal ranges: a possible explanation for decreased severity o f graft versus
host disease after cord blood transplantation. J Immunol Cell Biol 72, 440-444.
Behringer, D., Bertz, H., Schmoor, C., Berger, C., Dwenger, A., and Finke, J. (1999).
Quantitative lymphocyte subset reconstitution after allogeneic hematopoietic
179

BroLICX3RAPHY
transplantation from matched related donors with CD34+ selected PBPC grafts un selected
PB PC grafts or BM grafts. Bone Marrow Transplant 24, 295-302.
Bell, E. B., Sparshott, S. M., Dray son, M. T., and Ford, W. L. (1987). The stable and
permanent expansion of functional T lymphocytes in athymic nude rats after a single
injection of mature T cells. J Immunol 139, 1379-84.
Bell, E. B., Sparshott, S. M., Drayson, M. T., and Hunt, S. V. (1989). The origin o f T cells
in permanently reconstituted old athymic nude rats. Analysis using chromosome or
allotype markers. Immunology 68, 547-56.
Bender, J., Mitchell, T., Kappler, J., and Marrack, P. (1999). CD4-H T cell division in
irradiated mice requires peptides distinct from those responsible for thymic selection. J
Exp Med 190, 367-74.
Bennett, W. A., Lagoo-Deenadayalan, S., Whitworth, N. S., Brackin, M. N., Hale, E., and
Cowan, B. D. (1997). Expression and production of interleukin-10 by human
trophoblast: relationship to pregnancy immunotolérance. Early Pregnancy 3, 190-8.
Berenson, R. J., Andrews, R. G., Bensinger, W. I., Kalamasz, D., Knitter, G., Buckner, C. D.,
and Bernstein, I. D. (1988). Antigen CD34-I- marrow cells engraft lethally irradiated
baboons. J Clin Invest 81, 951-5.
Berry, S. M., Fine, N., Bichalski, J. A., Cotton, D. B., Dombrowski, M. P., and Kaplan, J.
(1992). Circulating lymphocyte subsets in second- and third-trimester fetuses:
comparison with newborns and adults. Am J Obstet Gynecol 167, 895-900.
Bertotto, A., Gerli, R., Lanfrancone, L., Cmpi, S., Arcangeli, C., Cemetti, C., Spinozzi, F.,
and Rambotti, P. (1990). Activation of cord T lymphocytes. II. Cellular and molecular
analysis o f the defective response induced by anti-CD3 monoclonal antibody. Cell
Immunol 127, 247-59.
Bird, J. J., Brown, D. R., Mullen, A. C., Moskowitz, N. H., Mahowald, M. A., Sider, J. R.,
Gajewski, T. F., Wang, C. R., and Reiner, S. L. (1998). Helper T cell differentiation is
controlled by the cell cycle. Immunity 9, 229-37.
Blackburn, E. H. (2001). Switching and signaling at the telomere. Cell 106, 661-73.
Blazar, B. R., Taylor, P. A., Panoskaltsis-Mortari, A., Buhlman, J., Xu, J., Flavell, R. A.,
Komgold, R., Noelle, R., and Vallera, D. A. (1997). Blockade of CD40 ligand-CD40
180

BmUOGRAPHY
interaction impairs CD4+ T cell-mediated alloreactivity by inhibiting mature donor T cell
expansion and function after bone marrow transplantation. J Immunol 158, 29-39.
Blazar, B. R., Taylor, P. A., Snover, D. C., Bluestone, J. A., and Vallera, D. A. (1993).
Nonmitogenic anti-CD3F(ab')2 fragments inhibit lethal murine graft- versus-host disease
induced across the major histocompatibility barrier. J Immunol 150, 265-77.
Blazar, B. R., Taylor, P. A., and Vallera, D. A. (1994). In vivo or in vitro anti-CD3 epsilon
chain monoclonal antibody therapy for the prevention o f lethal murine graft-versus-host
disease across the major histocompatibility barrier in mice. J Immunol 152, 3665-74.
Bluestone, J. A. (1995). New perspectives of CD28-B7-mediated T cell costimulation.
Immunity 2, 555-9.
Bogunia-Kubik, K., Perez-Cruz, I., Fallen, P. R., Madrigal, J. A., and Cohen, S. B. (2000).
Cord blood lymphocytes have a low frequency of cytokine producing T cells due to a
high threshold for activation. Immunol Lett 72, 145-6.
Boise, L. H., Minn, A. J., June, C. H., Lindsten, T., and Thompson, C. B. (1995). Growth
factors can enhance lymphocyte survival without committing the cell to undergo cell
division. Proc Natl Acad Sci U S A 92, 5491-5.
Boise, L. H., Minn, A. J., Noel, P. J., June, C. H., Accavitti, M. A., Lindsten, T., and
Thompson, C. B. (1995). CD28 costimulation can promote T cell survival by enhancing
the expression o f Bcl-XL. Immunity 3, 87-98.
Bolotin, E., Smogorzewska, M., Smith, S., Widmer, M., and Weinberg, K. (1996).
Enhancement o f thymopoiesis after bone marrow transplant by in vivo interleukin-7.
Blood 88, 1887-94.
Bonini, C., Ferrari, G., Verzeletti, S., Servida, P., Zappone, E., Ruggieri, L., Ponzoni, M.,
Rossini, S., Mavilio, F., Traversari, C., and Bordignon, C. (1997). HSV-TK gene transfer
into donor lymphocytes for control of allogeneic graft-versus-leukemia. Science 276,
1719-24.
Bordignon, C., Bonini, C., Verzeletti, S., Nobili, N., Maggioni, D., Traversari, C., Giavazzi,
R., Servida, P., Zappone, E., Benazzi, E., and et al. (1995). Transfer o f the HSV-tk gene
into donor peripheral blood lymphocytes for in vivo modulation o f donor anti-tumor
immunity after allogeneic bone marrow transplantation. Flum Gene Ther 6, 813-9.
181

B ib l io g r a p h y
Bortin, M. M., and Rimm, A. A. (1977). Severe combined immunodeficiency disease.
Characterization of the disease and results of transplantation. JAMA 238, 591-600.
Borzy, M. S., Hong, R., Horowitz, S. D., Gilbert, E., Kaufman, D., DeMendonca, W.,
Oxelius, V. A., Dictor, M., and Pachman, L. (1979). Fatal lymphoma after transplantation
of cultured thymus in children with combined immunodeficiency disease. N Engl J Med
301, 565-8.
Borzy, M. S., Ridgway, D., Noya, F. J., and Shearer, W. T. (1989). Successful bone
marrow transplantation with split lymphoid chimerism in DiGeorge syndrome. J Clin
Immunol 9, 386-92.
Botta, A., Amati, F., and Novelli, G. (2001). Causes of the phenotype-genotype
dissociation in DiGeorge syndrome: clues from mouse models. Trends Genet 17, 551-4.
Bowers, D. C., Lederman, H. M., Sicherer, S. H., Winkelstein, J. A., and Chen, A. R.
(1998). Immune constitution of complete DiGeorge anomaly by transplantation o f
unmobilised blood mononuclear cells. Lancet 352, 1983-4.
Braun, M. C., He, J., Wu, C. Y., and Kelsall, B. L. (1999). Cholera toxin suppresses
interleukin (IL)-12 production and IL-12 receptor betal and beta2 chain expression. J
Exp Med 189, 541-52.
Brenner, M. K., Grob, J. P., and Prentice, H. G. (1986). The use o f monoclonal antibodies
in graft versus host disease prevention. Haematologia 19, 167-76.
Brett, S., Baxter, G., Cooper, H., Johnston, J. M., Tite, J., and Rapson, N. (1996).
Repopulation o f blood lymphocyte sub-populations in rheumatoid arthritis patients
treated with the depleting humanized monoclonal antibody, CAMPATH-1 H.
Immunology 88, 13-9.
Brochu, S., Rioux-Masse, B., Roy, J., Roy, D. C., and Perreault, C. (1999). Massive
activation-induced cell death of alloreactive T cells with apoptosis o f bystander
postthymic T cells prevents immune reconstitution in mice with graft-versus-host disease.
Blood 94, 390-400.
Bromley, S. K., laboni. A., Davis, S. J., Whitty, A., Green, J. M., Shaw, A. S., Weiss, A., and
Dustin, M. L. (2001). The immunological synapse and CD28-CD80 interactions. Nat
Immunol 2, 1159-66.
182

BmUOüRAPHY
Bross, D. s., Tutschka, P. J., Farmer, E. R., Beschomer, W. E., B raine, H. G., Mellits, E. D.,
Bias, W. B., and Santos, G. W. (1984). Predictive factors for acute graft-versus-host disease
in patients transplanted with HLA-identical bone marrow. Blood 63, 1265-70.
Broxmeyer, H., Douglas, G., Gangoc, G., and Cooper, S. (1989). Human umbilical cord
blood as a potential source of transplantable haematopoietic stem-progenitor cell.
Proc.Natl Acad Sci USA 86, 3828-3832.
Broxmeyer, H. E., Hangoc, G., Cooper, S., Ribeiro, R. C., Graves, V., Yoder, M., Wagner, J.,
Vadhan, R. S., Benninger, L., Rubinstein, P., and et, a. 1. (1992). Growth characteristics
and expansion o f human umbilical cord blood and estimation o f its potential for
transplantation in adults. Proc Natl Acad Sci 89, 4109-13.
Bruno, L., von Boehmer, H., and Kirberg, J. (1996). Cell division in the compartment o f
naive and memory T lymphocytes. Eur J Immunol 26, 3179-84.
Buckley, R. H., Schiff, R. I., Schiff, S. E., Markert, M. L., Williams, L. W., Harville, T. O.,
Roberts, J. L., and Puck, J. M. (1997). Human severe combined immunodeficiency;
genetic, phenotypic, and functional diversity in one hundred eight infants. J Pediatr 130,
378-87 .
Buckley, R. H., Schiff, S. E., Schiff, R. I., Markert, L., Williams, L. W., Roberts, J. L.,
Myers, L. A., and Ward, F. E. (1999). Hematopoietic stem-cell transplantation for the
treatment o f severe combined immunodeficiency. N Engl J Med 340, 508-16.
Buelow, R., Burlingham, W. J., and Clayberger, C. (1995). Immunomodulation by soluble
HLA class I. Transplantation 59, 649-54.
Bunjes, D., Heit, W., Arnold, R., Schmeiser, T., Wiesneth, M., Carbonell, F., Porzsolt, F.,
Raghavachar, A., and Heimpel, H. (1987). Evidence for the involvement o f host-derived
OKT8-positive T cells in the rejection of T-depleted, HLA-identical bone marrow grafts.
Transplantation 43, 501-5.
Burnett, A. K., and Eden, O. B. (1997). The treatment of acute leukaemia. Lancet 349,
270-5 .
Busch, D. H., Pilip, I. M., Vijh, S., and Pamer, E. G. (1998). Coordinate regulation o f
com plex T cell populations responding to bacterial infection. Immunity 8, 353-62.
Butcher, E. C., and Picker, L. J. (1996). Lymphocyte homing and homeostasis. Science
272 , 60-6.
183

B ib l io g r a p h y
Butler, A. F,, EJ; Graham, GJ. (2000). Ex vivo expansion of cord blood cells: The clinical
potential. In Cord Blood Characteristics: Role in Stem Cell Transplantation, S. Cohen, ed.
(London: Martin Dunitz), pp. 169-204.
Cairo, M. S., and Wagner, J. E. (1997). Placental and/or umbilical cord blood: an
alternative source of hematopoietic stem cells for transplantation. Blood 90, 4665-78.
Callan, M. P., Tan, L., Annels, N., Ogg, G. S., Wilson, J. D., O'Callaghan, C. A., Steven, N.,
McMichael, A. J., and Rickinson, A. B. (1998). Direct visualization of antigen-specific
CD8-I- T cells during the primary immune response to Epstein-Barr virus In vivo. J Exp
Med 187, 1395-402.
Calvo, C. R., Amsen, D., and Kruisbeek, A. M. (1997). Cytotoxic T lymphocyte antigen 4
(CTLA-4) interferes with extracellular signal-regulated kinase (ERK) and Jun NH2-
terminal kinase (INK) activation, but does not affect phosphorylation of T cell receptor
zeta and ZAP70. J Exp Med 186, 1645-53.
Cao, X., Shores, E. W., Hu-Li, J., Anver, M. R., Kelsall, B. L., Russell, S. M., Drago, J.,
Noguchi, M., Grinberg, A., Bloom, E. T., and et al. (1995). Defective lymphoid
development in mice lacking expression of the common cytokine receptor gamma chain.
Immunity 2, 223-38.
Capone, M., Hockett, R. D., Jr., and Zlotnik, A. (1998). Kinetics of T cell receptor beta,
gamma, and delta rearrangements during adult thymic development: T cell receptor
rearrangements are present in CD44(+)CD25(+) Pro-T thymocytes. Proc Natl Acad Sci U
S A 95, 12522-7.
Carlos, T. M., and Harlan, J. M. (1994). Leukocyte-endothelial adhesion molecules.
Blood 84, 2068-101.
Carosella, E. D., Rouas-Freiss, N., Paul, P., and Dausset, J. (1999). HLA-G: a tolerance
molecule from the major histocompatibility complex. Immunol Today 20, 60-2.
Carteron, N. L., Schimenti, C. L., and Wofsy, D. (1989). Treatment o f murine lupus with
F(ab')2 fragments o f monoclonal antibody to L3T4. Suppression of autoimmunity does
not depend on T helper cell depletion. J Immunol 142, 1470-5.
Cash, E., Minty, A., Ferrara, P., Caput, D., Fradelizi, D., and Rott, O. (1994). Macrophage-
inactivating IL-13 suppresses experimental autoimmune encephalomyelitis in rats. J
Immunol 153, 4258-67.
184

B ib l k x '.r a p h y
Chalmers, I. M., Janossy, G., Contreras, M., and Navarrete, C. (1998). Intracellular
cytokine profile o f cord and adult blood lymphocytes. Blood 92, 11-8.
Chalmers, I. M. H., Janossy, G., Contreras, M., and Navarrete, C. (1998). Intracellular
cytokine profile o f cord and adult blood lymphocytes. Blood 92, 11-18.
Chambers, C. A., Kuhns, M. S., Egen, J. G., and Allison, J. P. (2001). CTLA-4-mediated
inhibition in regulation of T cell responses: mechanisms and manipulation in tumor
immunotherapy. Annu Rev Immunol 19, 565-94.
Chambers, C. A., Sullivan, T. J., and Allison, J. P. (1997). Lymphoproliferation in CTLA-
4-deficient mice is mediated by costimulation-dependent activation o f CD4+ T cells.
Immunity 7, 885-95.
Chan, A. C., Kadlecek, T. A., Elder, M. E., Filipovich, A. H., Kuo, W. L., Iwashima, M.,
Parslow, T. G., and Weiss, A. (1994). ZAP-70 deficiency in an autosomal recessive form
of severe combined immunodeficiency. Science 264, 1599-601.
Chang, M., Suen, Y., Lee, S. M., Baly, D., Buzby, J. S., Knoppel, E., Wolpe, S., and Cairo,
M. S. (1994). Transforming growth factor-beta 1, macrophage inflammatory protein-1
alpha, and interleukin-8 gene expression is lower in stimulated human neonatal compared
with adult mononuclear cells. Blood 84, 118-24.
Chaouat, G., Tranchot Diallo, J., Volumenie, J. L., Menu, E., Gras, G., Delage, G., and
Mognetti, B. (1997). Immune suppression and Thl/Th2 balance in pregnancy revisited: a
(very) personal tribute to Tom Wegmann. Am J Reprod Immunol 37, 427-34.
Chavin, K. D., Qin, L., Woodward, J. E., Lin, J., and Bromberg, J. S. (1994). Anti-CD2
monoclonal antibodies synergize with FK506 but not with cyclosporine or rapamycin to
induce tolerance. Transplantation 57, 736-40.
Chen, C. H., Chanh, T. C., and Cooper, M. D. (1984). Chicken thymocyte-specific antigen
identified by monoclonal antibodies: ontogeny, tissue distribution and biochemical
characterization. Eur J Immunol 14, 385-91.
Chen, W., Qin, H., Reese, V. A., and Cheever, M. A. (1998). CTLs specific for bcr-abl
joining region segment peptides fail to lyse leukemia cells expressing p210 bcr-abl
protein. J Immunother 21, 257-68.
185

B ib l io g r a p h y
Chipeta, J., Komada, Y,, Zhang, X. L., Deguchi, T., Sugiyama, K., Azuma, E., and Sakurai,
M. (1998). CD4+ and CD8+ cell cytokine profiles in neonates, older children, and adults:
increasing T helper type 1 and T cytotoxic type 1 cell populations with age. Cell
Immunol 183, 149-56.
Cho, B. K., Rao, V. P., Ge, Q., Eisen, H. N., and Chen, J. (2000). Homeostasis-stimulated
proliferation drives naive T cells to differentiate directly into memory T cells. J Exp Med
192, 549-56.
Chung, B., Barbara-Bumham, L., Bar sky, L., and Weinberg, K. (2001). Radiosensitivity o f
thymic interleukin-7 production and thymopoiesis after bone marrow transplantation.
Blood 98, 1601-6.
Clark, R. E., Dodi, I. A., Hill, S. C., Lill, J. R., Aubert, G., Macintyre, A. R., Rojas, J.,
Bourdon, A., Bonner, P. L., Wang, L., Christmas, S. E., Travers, P. J., Creaser, C. S., Rees,
R. C., and Madrigal, J. A. (2001). Direct evidence that leukemic cells present HLA-
associated immunogenic peptides derived from the BCR-ABL b3a2 fusion protein. Blood
98, 2887-93.
Cleaver, S. A. (1993). The Anthony Nolan Research Centre. Bone Marrow Transplant 11,
38-40 .
Clement-De Boers, A., Oostdijk, W., Van Weel-Sipman, M. H., Van den Broeck, J., Wit, J.
M., and Vossen, J. M. (1996). Final height and hormonal function after bone marrow
transplantation in children. J Pediatr 129, 544-50.
Clift, R. A., Appelbaum, F. R., and Thomas, E. D. (1993). Treatment o f chronic m yeloid
leukemia by marrow transplantation. Blood 82, 1954-6.
Clift, R. A., Buckner, C. D., Thomas, E. D., Bryant, E., Anasetti, C., Bensinger, W. I.,
Bowden, R., Deeg, H. J., Doney, K. C., Fisher, L. D., and et al. (1994). Marrow
transplantation for patients in accelerated phase of chronic myeloid leukemia. Blood 84,
4 3 6 8 -7 3 .
Cohen, S. B., Morgan, C. L., Perez-Cruz, I., Perandin, F., Martinez, B., and Madrigal, J. A.
(2000). Cord blood serum does not increase lymphocyte responses in comparison to
adult serum. Hum Immunol 61, 111-4.
Cohen, S. B., Perez-Cruz, I., Fallen, P., Gluckman, E., and Madrigal, J. A. (1999). Analysis
of the cytokine production by cord and adult blood. Hum Immunol 60, 331-6.
186

B ib l io g r a p h y
Cohen, S. B., W oolley, J., Bogunia-Kubik, K., Natarajan, P., Kotecha, R., Belaramani, L.,
Fallen, P. R., Perez-Cruz, I., and Madrigal, J. A. (2000). Macrophage colony stimulating
factor (M-CSF) within cord blood sera may be partially responsible for the reduced
proliferation of cord blood T cells. Fur Cytokine Netw 11, 608-17.
Coles, A. J., Wing, M. G., Molyneux, P., Paolillo, A., Davie, C. M., Hale, G., Miller, D.,
Waldmann, H., and Compston, A. (1999). Monoclonal antibody treatment exposes three
mechanisms underlying the clinical course of multiple sclerosis. Ann Neurol 46, 296-304.
Collins, R. H., Jr., Shpilberg, O., Drobyski, W. R., Porter, D. L., Giralt, S., Champlin, R.,
Goodman, S. A., Wolff, S. N., Hu, W., Verfaillie, C., List, A., Dalton, W., Ognoskie, N.,
Chetrit, A., Antin, J. H., and Nemunaitis, J. (1997). Donor leukocyte infusions in 140
patients with relapsed malignancy after allogeneic bone marrow transplantation. J Clin
Oncol 15, 433-44.
Connors, M., Kovacs, J. A., Krevat, S., Gea-Banacloche, J. C., Sneller, M. C., Flanigan, M.,
Metcalf, J. A., Walker, R. E., Falloon, J., Baseler, M., Feuerstein, I., Masur, H., and Lane, H.
C. (1997). HIV infection induces changes in CD4+ T-cell phenotype and depletions
within the CD4+ T-cell repertoire that are not immediately restored by antiviral or
immune-based therapies. Nat Med 3, 533-40.
Corr, M., Slanetz, A. E., Boyd, L. F., Jelonek, M. T., Khilko, S., al-Ramadi, B. K., Kim, Y.
S., Maher, S. E., Bothwell, A. L., and Margulies, D. H. (1994). T cell receptor-MHC class I
peptide interactions: affinity, kinetics, and specificity. Science 265, 946-9.
Cupps, T. R., and Fauci, A. S. (1982). Corticosteroid-mediated immunoregulation in man.
Immunol Rev 65, 133-55.
Cwynarski, K., Ainsworth, J., Cobbold, M., Wagner, S., Mahendra, P., Apperley, J.,
Goldman, J., Craddock, C., and Moss, P. A. (2001). Direct visualization o f
cytomegalovirus-specific T-cell reconstitution after allogeneic stem cell transplantation.
Blood 97, 1232-40.
Cyster, J. G. (1999). Chemokines and cell migration in secondary lymphoid organs.
Science 286, 2098-102.
D'Arena, G., Musto, P., Cascavilla, N., Di Giorgio, G., Fusilli, S., Zendoli, F., and
Carotenuto, M. (1998). Flow cytometric characterization o f human umbilical cord blood
lymphocytes: immunophenotypic features. Haematologica 83, 197-203.
187

B iBLIÜCiRAI^HY
Daga, S. R., Siddiqui, H. M., Lokhande, M. P., Chandrashekhar, L., Prabhu, P. G., and
Kansaria, B. N. (1984). Immuno-reconstitution by thymie transplant in DiGeorge's
syndrome. Postgrad Med J 60, 537-9.
Daley, J. P., Rozans, M. K., Smith, B. R., Burakoff, S. J., Rappeport, J. M., and Miller, R. A.
(1987). Retarded recovery of functional T cell frequencies in T cell-depleted bone
marrow transplant recipients. Blood 70, 960-4.
Damoiseaux, J. G., Beijleveld, L. J., and van Breda Vriesman, P. J. (1997). Multiple effects
o f cyclosporin A on the thymus in relation to T-cell development and autoimmunity. Clin
Immunol Immunopathol 82, 197-202.
Davies, S. M., Shu, X. O., Blazar, B. R., Filipovich, A. H., Kersey, J. H., Krivit, W.,
McCullough, J., Miller, W. J., C., R. N. K., Segali, M., Wagner, J. E., Weisdorf, D. J., and
McGlave, P. B. (1995). Unrelated donor bone marrow transplantation: influence o f HLA
A and HLA B incompatability on outcome. Blood 86, 1636-1642.
Davies, S. M., Wagner, J. E., Shu, X. O., Blazar, B. R., Katsanis, E., Orchard, P. J., Kersey, J.
H., Dusenbery, K. E., Weisdorf, D. J., McGlave, P. B., and Ramsay, N. K. (1997).
Unrelated donor bone marrow transplantation for children with acute leukemia. J Clin
Oncol 15, 557-65.
de Gast, G. C., Verdonck, L. P., Middeldorp, J. M., The, T. H., Hekker, A., vd Linden, J.
A., Kreeft, H. A., and Bast, B. J. (1985). Recovery of T cell subsets after autologous bone
marrow transplantation is mainly due to proliferation o f mature T cells in the graft. Blood
66, 428-31.
De Jongh, R., Vranken, J., Kenis, G., Bosmans, E., Maes, M., Stans, G., De Ley, M., and
Heylen, R. (1998). Clara cell protein: concentrations in cerebrospinal fluid, serum and
amniotic fluid. Cytokine 10, 441-4.
de la Chapelle, A., Herva, R., Koivisto, M., and Aula, P. (1981). A deletion in chrom osom e
22 can cause DiGeorge syndrome. Hum Genet 57, 253-6.
De Rosa, S. C., Herzenberg, L. A., and Roederer, M. (2001). 11-color, 13-parameter flow
cytometry: identification of human naive T cells by phenotype, function, and T-cell
receptor diversity. Nat Med 7, 245-8.
de Villartay, J. P., Hockett, R. D., Coran, D., Korsmeyer, S. J., and Cohen, D. I. (1988).
Deletion o f the human T-cell receptor delta-gene by a site-specific recombination. Nature
335, 170-4.
188

B iBLIOGRAI’HY
de Villartay, J. P., Lewis, D., Hockett, R., Waldmann, T. A., Korsmeyer, S. J., and Cohen, D.
I. (1987). Deletional rearrangement in the human T-cell receptor alpha-chain locus. Proc
Natl Acad Sci U S A 84, 8608-12.
de Waal Malefyt, R., Abrams, J., Bennett, B., Figdor, C. G., and de Vries, J. E. (1991).
Interleukin lO(IL-lO) inhibits cytokine synthesis by human monocytes: an
autoregulatory role of IL-10 produced by monocytes. J Exp Med 174, 1209-20.
de Waal Malefyt, R., Haanen, J., Spits, H., Roncarolo, M. G., te Velde, A., Figdor, C.,
Johnson, K., Kastelein, R., Yssel, H., and de Vries, J. E. (1991). Interleukin 10 (IL-10) and
viral IL-10 strongly reduce antigen-specific human T cell proliferation by diminishing
the antigen-presenting capacity of monocytes via downregulation o f class II major
histocompatibility complex expression. J Exp Med 174, 915-24.
De Wit, D., Van Mechelen, M., Zanin, C., Doutrelepont, J. M., Velu, T., Gerard, C.,
Abramowicz, D., Scheerlinck, J. P., De Baetselier, P., Urbain, J., and et al. (1993).
Preferential activation of Th2 cells in chronic graft-versus-host reaction. J Immunol 150,
361-6 .
Delon, J., Kaibuchi, K., and Germain, R. N. (2001). Exclusion o f CD43 from the
immunological synapse is mediated by phosphorylation-regulated relocation o f the
cytoskeletal adaptor moesin. Immunity 15, 691-701.
Demotz, S., Grey, H. M., and Sette, A. (1990). The minimal number o f class II MHC-
antigen complexes needed for T cell activation. Science 249, 1028-30.
Dermime, S., Bertazzoli, C., Marchesi, E., Ravagnani, F., Blaser, K., Comeo, G. M.,
Pogliani, E., Parmiani, G., and Gambacorti-Passerini, C. (1996). Lack of T-cell-mediated
recognition of the fusion region o f the pml/RAR- alpha hybrid protein by lymphocytes o f
acute promyelocytic leukemia patients. Clin Cancer Res 2, 593-600.
Dhodapkar, M. V., Steinman, R. M., Krasovsky, J., Munz, C., and Bhardwaj, N. (2001).
Antigen-specific inhibition of effector T cell function in humans after injection o f
immature dendritic cells. J Exp Med 193, 233-8.
Dictor, M., Fasth, A., and Oiling, S. (1984). Abnormal B-cell proliferation associated with
combined immunodeficiency, cytomegalovirus, and cultured thymus grafts. Am J Clin
Pathol 82, 487-90.
189

BmUOC'iRAPKY
DiSanto, J. P., Muller, W., Guy-Grand, D., Fischer, A., and Rajewsky, K. (1995).
Lymphoid development in mice with a targeted deletion of the interleukin 2 receptor
gamma chain. Proc Natl Acad Sci U S A 92, 377-81.
Dominguez, E., Madrigal, J. A., Layrisse, Z., and Cohen, S. B. (1998). Fetal natural killer
cell function is suppressed. Immunology 94, 109-14.
Doney, K., Leisenring, W., Storb, R., and Appelbaum, F. R. (1997). Primary treatment o f
acquired aplastic anemia: outcomes with bone marrow transplantation and
immunosuppressive therapy. Seattle Bone Marrow Transplant Team. Ann Intern Med
126, 107-15.
Dong, C., Juedes, A. E., Temann, U. A., Shresta, S., Allison, J. P., Ruddle, N. H., and
Flavell, R. A. (2001). ICOS co-stimulatory receptor is essential for T-cell activation and
function. Nature 409, 97-101.
Donskoy, E., and Goldschneider, I. (1992). Thymocytopoiesis is maintained by blood-
borne precursors throughout postnatal life. A study in parabiotic mice. J Immunol 148,
1604-12.
Douek, D. C., McFarland, R. D., Reiser, P. H., Gage, E. A., Massey, J. M., Haynes, B. F.,
Polis, M. A., Haase, A. T., Feinberg, M. B., Sullivan, J. L., Jamieson, B. D., Zack, J. A.,
Picker, L. J., and Koup, R. A. (1998). Changes in thymic function with age and during the
treatment of HIV infection. Nature 396, 690-5.
Douek, D. C., Vescio, R. A., Betts, M. R., Brenchley, J. M., Hill, B. J., Zhang, L., Berenson,
J. R., Collins, R. H., and Koup, R. A. (2000). Assessment of thymic output in adults after
haematopoietic stem-cell transplantation and prediction of T-cell reconstitution. Lancet
355, 1875-81.
Driscoll, D. A., Salvin, J., Sellinger, B., Budarf, M. L., McDonald-McGinn, D. M., Zackai,
E. H., and Emanuel, B. S. (1993). Prevalence of 2 2 q ll microdeletions in DiGeorge and
velocardiofacial syndromes: implications for genetic counselling and prenatal diagnosis. J
Med Genet 30, 813-7.
Drobyski, W. R., Hessner, M. J., Klein, J. P., Kabler-Babbitt, C., Vesole, D. H., Margolis, D.
A., and Keever-Taylor, C. A. (1999). T-cell depletion plus salvage immunotherapy with
donor leukocyte infusions as a strategy to treat chronic-phase chronic m yelogenous
leukemia patients undergoing HLA-identical sibling marrow transplantation. Blood 94,
43 4 -4 1 .
190

BIBLIOCiRAPHY
Drobyski, W. R., Keever, C. A., Roth, M. S., Koethe, S., Hanson, G., McFadden, P.,
Gottschall, J. L., Ash, R. C., van Tuinen, P., Horowitz, M, M., and et al. (1993). Salvage
immunotherapy using donor leukocyte infusions as treatment for relapsed chronic
myelogenous leukemia after allogeneic bone marrow transplantation: efficacy and
toxicity o f a defined T-cell dose. Blood 82, 2310-8.
Drobyski, W. R., Morse, H. C., 3rd, Bums, W. H., Casper, J. T., and Sandford, G. (2001).
Protection from lethal murine graft-versus-host disease without compromise o f
alloengraftment using transgenic donor T cells expressing a thymidine kinase suicide
gene. Blood 97, 2506-13.
Dudley, E. C., Girardi, M., Owen, M. J., and Hayday, A. C. (1995). Alpha beta and gamma
delta T cells can share a late common precursor. Curr Biol 5, 659-69.
Dulude, G., Roy, D. C., and Perreault, C. (1999). The effect of graft-versus-host disease on
T cell production and homeostasis. J Exp Med 189, 1329-42.
Dummer, W., Ernst, B., LeRoy, E., Lee, D., and Surh, C. (2001). Autologous regulation o f
naive T cell homeostasis within the T cell compartment. J Immunol 166, 2460-8.
Dumont-Girard, P., Roux, E., van Lier, R. A., Hale, G., Helg, C., Chapuis, B., Starobinski,
M., and Roosnek, E. (1998). Reconstitution of the T-cell compartment after bone marrow
transplantation: restoration of the repertoire by thymic emigrants. Blood 92, 4464-71.
Durham, M. M., Bingaman, A. W., Adams, A. B., Ha, J., Waitze, S. Y., Pearson, T. C., and
Larsen, C. P. (2000). Cutting edge: administration of anti-CD40 ligand and donor bone
marrow leads to hemopoietic chimerism and donor-specific tolerance without
cytoreductive conditioning. J Immunol 165, 1-4.
Durie, F. H., Aruffo, A., Ledbetter, J., Crassi, K. M., Green, W. R., Fast, L. D., and Noelle,
R. J. (1994). Antibody to the ligand of CD40, gp39, blocks the occurrence o f the acute
and chronic forms o f graft-vs-host disease. J Clin Invest 94, 1333-8.
Dustin, M. L., Ferguson, L. M., Chan, P. Y., Springer, T. A., Golan, D. E. (1996).
Visualization of CD2 interaction with LEA-3 and determination o f the two-dimensional
dissociation constant for adhesion receptors in a contact area. J Cell Biol 132, 465-74.
Dustin, M. L., and Cooper, J. A. (2000). The immunological synapse and the actin
cytoskeleton: molecular hardware for T cell signaling. Nat Immunol 1, 23-9.
191

B iBLIOGRAI’HY
Ebbesen, P., Hager, H., Norskov-Lauritsen, N., Aboagye-Mathiesen, G., Zdravkovic, M.,
Villadsen, J., Liu, X., Petersen, P. M., Bambra, C., Nyongo, A., and et al. (1995).
Concurrence of high levels of interferons alpha and beta in cord and maternal blood and
simultaneous presence o f interferon in trophoblast in an African population. J Interferon
Cytokine Res 15, 123-8.
Effros, R. B., Allsopp, R., Chiu, C. P., Hausner, M. A., Hiiji, K., Wang, L., Harley, C. B.,
Villeponteau, B., West, M. D., and Giorgi, J. V. (1996). Shortened telomeres in the
expanded CD28-CD8-I- cell subset in HIV disease implicate replicative senescence in HIV
pathogenesis. Aids 10, F I7-22.
Effros, R. B., Boucher, N., Porter, V., Zhu, X., Spaulding, C., Walford, R. L., Kronenberg,
M., Cohen, D., and Schachter, F. (1994). Decline in CD28-t- T cells in centenarians and in
long-term T cell cultures: a possible cause for both in vivo and in vitro
immunosenescence. Exp Gerontol 29, 601-9.
Effros, R. B., and Pawelec, G. (1997). Replicative senescence of T cells: does the Hay flick
Limit lead to immune exhaustion? Immunol Today 18, 450-4.
Egen, J. G., and Allison, J. P. (2002). Cytotoxic T lymphocyte antigen-4 accumulation in
the immunological synapse is regulated by TCR signal strength. Immunity 16, 23-35.
Egerton, M., Scollay, R., and Shortman, K. (1990). Kinetics o f mature T-cell development
in the thymus. Proc Natl Acad Sci U S A 87, 2579-82.
Eisner, J., Hochstetter, R., Spiekermann, K., and Kapp, A. (1996). Surface and mRNA
expression of the CD52 antigen by human eosinophils but not by neutrophils. Blood 88,
4684-93 .
Ende, N. (1992). Collection of umbilical cord blood for transplantation. Blood 80, 1623;
discussion 1624.
English, B. K., Hammond, W. P., Lewis, D. B., Brown, C. B., and Wilson, C. B. (1992).
Decreased granulocyte-macrophage colony-stimulating factor production by human
neonatal blood mononuclear cells and T cells. Pediatr Res 31, 211-6.
Erkeller-Yuksel, F. M., Deneys, V., Yuksel, B., Hannet, I., Hulstaert, F., Hamilton, C.,
Mackinnon, H., Stokes, L. T., Munhyeshuli, V., Vanlangendonck, F., and et al. (1992).
Age-related changes in human blood lymphocyte subpopulations. J Pediatr 120, 216-22.
192

BIBLKX'iRAPHY
Erlich, H. A., Opelz, G., and Hansen, J. (2001). HLA DNA typing and transplantation.
Immunity 14, 347-56.
Ernst, B., Lee, D. S., Chang, J. M., Sprent, J., and Surh, C. D. (1999). The peptide ligands
mediating positive selection in the thymus control T cell survival and homeostatic
proliferation in the periphery. Immunity 11, 173-81.
Ernst, B. B., Surh, C. D., and Sprent, J. (1996). Bone marrow-derived cells fail to induce
positive selection in thymus reaggregation cultures. J Exp Med 183, 1235-40.
Fahey, J. L., Sama, G., Gale, R. P., and Seeger, R. (1987). Immune interventions in
disease. Ann Intern Med 106, 257-74.
Fehling, H. J., and von Boehmer, H. (1997). Early alpha beta T cell development in the
thymus of normal and genetically altered mice. Curr Opin Immunol 9, 263-75.
Feinstein, L., Sandmaier, B., Maloney, D., McSweeney, P. A., Maris, M., Flowers, C.,
Radich, J., Little, M. T., Nash, R. A., Chauncey, T., Woolfrey, A., Georges, G., Kiem, H. P.,
Zaucha, J. M., Blume, K. G., Shizuru, J., Niederwieser, D., and Storb, R. (2001).
Nonmyeloablative hematopoietic cell transplantation. Replacing high- dose cytotoxic
therapy by the graft-versus-tumor effect. Ann N Y Acad Sci 938, 328-37; discussion 337-
9.
Fernandez, M. (2000). Ethical, legal and socio-economic issues related to blood cell
therapy and transplantation. In Cord Blood Characteristics: Role in Stem Cell
Transplantation, S. Cohen, ed. (London: Martin Dunitz), pp. 249-260.
Fischer, A. (1992). Severe combined immunodeficiencies. Immunodefic Rev 3, 83-100.
Fischer, A., Hacein-Bey, S., Le Deist, F., Soudais, C., Di Santo, J. P., de Saint Basile, G., and
Cavazzana-Calvo, M. (2000). Gene therapy of severe combined im m unodeficiencies.
Immunol Rev 178, 13-20.
Fischer, A., Landais, P., Friedrich, W., Morgan, G., Gerritsen, B., Fasth, A., Porta, F.,
Griscelli, C., Goldman, S. F., Levinsky, R., and et al. (1990). European experience o f
bone-marrow transplantation for severe combined immunodeficiency. Lancet 336, 850-4.
Fontaine, P., Roy-Proulx, G., Knafo, L., Baron, C., Roy, D. C., and Perreault, C. (2001).
Adoptive transfer o f minor histocompatibility antigen-specific T lymphocytes eradicates
leukemia cells without causing graft-versus-host disease. Nat Med 7, 789-94.
193

B ib l io g r a p h y
Foot, A. B., Potter, M. N., Donaldson, C., Cornish, J. M., Wallington, T. B., Oakhill, A., and
Pamphilon, D. H. (1993). Immune reconstitution after BMT in children. Bone Marrow
Transplant 11, 7-13.
Forman, S. J., Nocker, P., Gallagher, M., Zaia, J., Wright, C., Bolen, J., Mills, B., and Hecht,
T. (1982). Pattern of T cell reconstitution following allogeneic bone marrow
transplantation for acute hematological malignancy. Transplantation 34, 96-8.
Foulds, K. E., Zenewicz, L. A., Shedlock, D. J., Jiang, J., Troy, A. E., and Shen, H. (2002).
Cutting edge: CD4 and CD8 T cells are intrinsically different in their proliferative
responses. J Immunol 168, 1528-32.
Fowler, D. H., Kurasawa, K., Husebekk, A., Cohen, P. A., and Gress, R. E. (1994). Cells o f
Th2 cytokine phenotype prevent EPS-induced lethality during murine graft-versus-host
reaction. Regulation of cytokines and CD8+ lymphoid engraftment. J Immunol 152,
1004-13.
Fowler, D. H., Kurasawa, K., Smith, R., Eckhaus, M. A., and Gress, R. E. (1994). Donor
CD4-enriched cells of Th2 cytokine phenotype regulate graft- versus-host disease without
impairing allogeneic engraftment in sublethally irradiated mice. Blood 84, 3540-9.
Foy, T. M., Aruffo, A., Bajorath, J., Buhlmann, J. E., and Noelle, R. J. (1996). Immune
regulation by CD40 and its ligand GP39. Annu Rev Immunol 14, 591-617.
Freeman, G. J., Borriello, F., Hodes, R. J., Reiser, H., Hathcock, K. S., Laszlo, G.,
McKnight, A. J., Kim, J., Du, L., Lombard, D. B., and et al. (1993). Uncovering o f
functional alternative CTLA-4 counter-receptor in B7- deficient mice. Science 262, 907-
9.
Freitas, A. A., and Rocha, B. (2000). Population biology of lymphocytes: the flight for
survival. Annu Rev Immunol 18, 83-111.
Freitas, A. A., Rosado, M. M., Viale, A. C., and Grandien, A. (1995). The role o f cellular
competition in B cell survival and selection of B cell repertoires. Eur J Immunol 25, 1729-
38.
Fridkis-Hareli, M., Abel, L., and Globerson, A. (1992). Patterns o f dual lym phocyte
development in co-cultures of foetal thymus and lymphohaemopoietic cells from young
and old mice. Immunology 77, 185-8.
194

B ib l io g r a p h y
Fukushi, N., Arase, H., Wang, B., Ogasawara, K., Gotohda, T., Good, R. A., and Onoe, K.
(1990). Thymus: a direct target tissue in graft-versus-host reaction after allogeneic bone
marrow transplantation that results in abrogation of induction of self-tolerance. Proc Natl
Acad Sci U S A &7, 6301-5.
Gagliardi, M. C., Sallusto, P., Marinaro, M., Langenkamp, A., Lanzavecchia, A., and De
Magistris, M. T. (2000). Cholera toxin induces maturation o f human dendritic cells and
licences them for Th2 priming. Eur J Immunol 30, 2394-403.
Gallimore, A., Glithero, A., Godkin, A., Tissot, A. C., Pluckthun, A., Elliott, T., Hengartner,
H., and Zinkemagel, R. (1998). Induction and exhaustion o f lym phocytic
choriomeningitis virus-specific cytotoxic T lymphocytes visualized using soluble
tetrameric major histocompatibility complex class I-peptide complexes. J Exp Med 187,
1383-93 .
Galy, A., Travis, M., Cen, D., and Chen, B. (1995). Human T, B, natural killer, and
dendritic cells arise from a common bone marrow progenitor cell subset. Immunity 3,
4 5 9 -7 3 .
Galy, A., Verma, S., Barcena, A., and Spits, H. (1993). Precursors o f CD3-i-CD44-CD8-t-
cells in the human thymus are defined by expression o f CD34. Delineation of early events
in human thymic development. J Exp Med 178, 391-401.
Gao, L., Bellantuono, I., Elsasser, A., Marley, S. B., Gordon, M. Y., Goldman, J. M., and
Stauss, H. J. (2000). Selective elimination of leukemic CD34(-f-) progenitor cells by
cytotoxic T lymphocytes specific for W T l. Blood 95, 2198-203.
Garban, P., Ericson, M., Roucard, C., Rabian-Herzog, C., Teisserenc, H., Sauvanet, E.,
Charron, D., and Mooney, N. (1996). Detection of empty HLA class II molecules on cord
blood B cells. Blood 87, 3970-6.
Garcia, K. C., Degano, M., Speir, J. A., and Wilson, I. A. (1999). Emerging principles for
T cell receptor recognition of antigen in cellular immunity. Rev Immunogenet 1, 75-90.
Garlisi, C. G., Pennline, K. J., Smith, S. R., Siegel, M. I., and Umland, S. P. (1993).
Cytokine gene expression in mice undergoing chronic graft-versus-host disease. M ol
Immunol 30, 669-77.
Garside, P., Hutton, A. K., Severn, A., Liew, P. Y., and Mowat, A. M. (1992). Nitric oxide
mediates intestinal pathology in graft-vs.-host disease. Eur J Immunol 22, 2141-5.
195

B ib l io g r a p h y
Gaschet, J., Denis, C., Milpied, N., Hallet, M. M., Romagne, F., Necker, A., Vivien, R.,
David-Ameline, J., Davodeau, F., Bonneville, M., and et al. (1995). Alterations o f T cell
repertoire after bone marrow transplantation: characterization o f over-represented subsets.
Bone Marrow Transplant 16, 427-35.
George, A. J., and Ritter, M. A. (1996). Thymic involution with ageing: obsolescence or
good housekeeping? Immunol Today 17, 267-72.
Gerli, R., Agea, E., Muscat, C., Tognellini, R., Fiorucci, G., Spinozzi, F., Cemetti, C., and
Bertotto, A. (1993). Activation of cord T lymphocytes. III. Role of LFA-l/ICAM -1 and
CD2/LFA-3 adhesion molecules in CD3-induced proliferative response. Cell Immunol
148, 32-47.
Gerli, R., Bertotto, A., Crupi, S., Arcangeli, C., Marinelli, I., Spinozzi, F., Cemetti, C.,
Angelella, P., and Rambotti, P. (1989). Activation of cord T lymphocytes. I. Evidence for
a defective T cell mitogenesis induced through the CD2 molecule. J Immunol 142, 2583-
9.
Ghayur, T., Seemayer, T. A., Kongshavn, P. A., Gartner, J. G., and Lapp, W. S. (1987).
Graft-versus-host reactions in the beige mouse. An investigation of the role o f host and
donor natural killer cells in the pathogenesis of graft-versus-host disease. Transplantation
44, 261-7.
Ghayur, T., Seemayer, T. A., and Lapp, W. S. (1988). Association between the degree o f
thymic dysplasia and the kinetics of thymic NK cell activity during the graft-versus-host
reaction. Clin Immunol Immunopathol 48, 19-30.
Ghayur, T., Seemayer, T. A., and Lapp, W. S. (1987). Kinetics of natural killer cell
cytotoxicity during the graft-versus- host reaction. Relationship between natural killer cell
activity, T and B cell activity, and development of histopathological alterations.
Transplantation 44, 254-60.
Ghayur, T., Seemayer, T. A., Xenocostas, A., and Lapp, W. S. (1988). Complete sequential
regeneration o f graft-vs.-host-induced severely dysplastic thymuses. Implications for the
pathogenesis o f chronic graft- vs.-host disease. Am J Pathol 133, 39-46.
Giblett, E. R., Anderson, J. E., Cohen, F., Pollara, B., and Meuwissen, H. J. (1972).
Adenosine-deaminase deficiency in two patients with severely impaired cellular immunity.
Lancet 2, 1067-9.
196

BffiL iaiR A PH Y
Gilmore, M. J., Patterson, J., Ivory, K., Brenner, M. K., Graphakos, S., Janossy, G.,
Hoffbrand, A. V., and Prentice, H. G. (1986). Standardization o f T-cell depletion in HLA
matched bone marrow transplantation. Br J Haematol 64, 69-75.
Giralt, S., Thall, P. F., Khouri, I., Wang, X., Braunschweig, L, Ippolitti, C., Claxton, D.,
Donato, M., Bruton, J., Cohen, A., Davis, M., Andersson, B. S., Anderlini, P., Gajewski, J.,
Komblau, S., Andreeff, M., Przepiorka, D., Ueno, N. T., Molldrem, J., and Champlin, R.
(2001). Melphalan and purine analog-containing preparative regimens; reduced- intensity
conditioning for patients with hematologic malignancies undergoing allogeneic
progenitor cell transplantation. Blood 97, 631-7.
Globerson, A. (1995). T lymphocytes and aging. Int Arch Allergy Immunol 107, 491-7.
Globerson, A., and Effros, R. B. (2000). Ageing o f lymphocytes and lymphocytes in the
aged. Immunol Today 21, 515-21.
Globerson, A., Sharp, A., Fridkis-Hareli, M., Kukulansky, T., Abel, L., Knyszynski, A., and
Eren, R. (1992). Aging in the T lymphocyte compartment. A developmental view. Ann N
Y Acad Sci 673, 240-51.
Gluckman, E., Broxmeyer, H. A., Aurebach, A. D., Friedman, H. S., Douglas, G. W.,
Devergie, G. W., Devergie, A., Esperou, H., Thierry, D., Socie, G., and Lehn, P. e. a.
(1989). Hematopoietic reconstitution in a patient with Fanconi's anemia by means o f
umilical-cord blood from HLA-identical siblings. N. Engl. J. Med, 1174-1178.
Gluckman, E., Rocha, V., Boyer-Chammard, A., Locatelli, F., Arcese, W., Pasquini, R.,
Ortega, J., Souillet, G., Ferreira, E., Laporte, J. P., Fernandez, M., and Chastang, C. (1997).
Outcome of cord-blood transplantation from related and unrelated donors. Eurocord
Transplant Group and the European Blood and Marrow Transplantation Group. N Engl J
Med 337, 373-81.
Gluckman, E., Wagner, J., Hows, J., Keman, N., Bradley, B., and Broxmeyer, H. E. (1993).
Cord blood banking for hematopoietic stem cell transplantation: an international cord
blood transplant registry. Bone Marrow Transplantation 11, 199-200.
Gluckman, E. R., V; Chevret, S. (2000). Related and unrelated cord blood transplantation.
In Cord Blood Characteristics: Role in Stem Cell Transplantation, S. Cohen, ed. (London:
Martin Dunitz), pp. 210.
Glucksberg, H., Storb, R., Fefer, A., Buckner, C. D., Neiman, P. E., Clift, R. A., Lemer, K.
G., and Thomas, E. D. (1974). Clinical manifestations o f graft-versus-host disease in
197

B ib l io g r a p h y
human recipients of marrow from HL-A-matched sibling donors. Transplantation 18,
295-304 .
Godthelp, B. C., van Toi, M. J., Vossen, J. M., and van Den Elsen, P. J. (1999). T-Cell
immune reconstitution in pediatric leukemia patients after allogeneic bone marrow
transplantation with T-cell-depleted or unmanipulated grafts: evaluation of overall and
antigen-specific T-cell repertoires. Blood 94, 4358-69.
Goldman, J. M., Gale, R. P., Horowitz, M. M., Biggs, J. C., Champlin, R. E., Gluckman, E.,
Hoffmann, R. G., Jacobsen, S. J., Marmont, A. M., McGlave, P. B., and et al. (1988). Bone
marrow transplantation for chronic myelogenous leukemia in chronic phase. Increased
risk for relapse associated with T-cell depletion. Ann Intern Med 108, 806-14.
Goldrath, A. W., and Bevan, M. J. (1999). Low-affinity ligands for the TCR drive
proliferation of mature CD8+ T cells in lymphopénie hosts. Immunity 11, 183-90.
Goldrath, A. W., and Bevan, M. J. (1999). Selecting and maintaining a diverse T-cell
repertoire. Nature 402, 255-62.
Goldrath, A. W., Bogatzki, L. Y., and Bevan, M. J. (2000). Naive T cells transiently acquire
a memory-like phenotype during homeostasis-driven proliferation. J Exp Med 192, 557-
64 .
Goldsobel, A. B., Haas, A., and Stiehm, E. R. (1987). Bone marrow transplantation in
DiGeorge syndrome. J Pediatr 111, 40-4.
Goulmy, E. (1997). Human minor histocompatibility antigens: new concepts for marrow
transplantation and adoptive immunotherapy. Immunol Rev 157, 125-40.
Grakoui, A., Bromley, S. K., Sumen, C., Davis, M. M., Shaw, A. S., Allen, P. M., and
Dustin, M. L. (1999). The immunological synapse: a molecular machine controlling T
cell activation. Science 285, 221-7.
Grayson, J. M., Zajac, A. J., Altman, J. D., and Ahmed, R. (2000). Cutting edge: increased
expression of Bcl-2 in antigen-specific memory CD8+ T cells. J Immunol 164, 3950-4.
Griscelli, C., Durandy, A., Virelizier, J. L., Ballet, J. J., and Daguillard, F. (1978). Selective
defect o f precursor T cells associated with apparently normal B lymphocytes in severe
combined immunodeficiency disease. J Pediatr 93, 404-11.
198

B ib l io c '.r a p h y
Groettrup, M., and von Boehmer, H. (1993). T cell receptor beta chain dimers on
immature thymocytes from normal mice. Eur J Immunol 23, 1393-6.
group, W. s. (1995). Primary immunodeficiency diseases. Report o f a WHO Scientific
Group. Clin Exp Immunol 99 Suppl 1, 1-24.
Grubeck-Loebenstein, B., Lechner, H., and Trieb, K. (1994). Long-term in vitro growth o f
human T cell clones: can postmitotic 'senescent' cell populations be defined? Int Arch
Allergy Immunol 104, 232-9.
Guckel, B., Berek, C., Lutz, M., Altevogt, P., Schirrmacher, V., and Kyewski, B. A. (1991).
Anti-CD2 antibodies induce T cell unresponsiveness in vivo. J Exp Med 174, 957-67.
Gudmundsdottir, H., Wells, A. D., and Turka, L. A. (1999). Dynamics and requirements
of T cell clonal expansion in vivo at the single-cell level: effector function is linked to
proliferative capacity. J Immunol 162, 5212-23.
Guillen, F. J., Ferrara, J., Hancock, W. W., Messadi, D., Fonferko, E., Burakoff, S. J., and
Murphy, G. F. (1986). Acute cutaneous graft-versus-host disease to minor
histocompatibility antigens in a murine model. Evidence that large granular lym phocytes
are effector cells in the immune response. Lab Invest 55, 35-42.
Gustafsson, A., Remberger, M., Winiarski, J., and Ringden, O. (2000). Unrelated bone
marrow transplantation in children: outcome and a comparison with sibling donor
grafting. Bone Marrow Transplant 25, 1059-65.
Gutstein, N. L., Seaman, W. E., Scott, J. H., and Wofsy, D. (1986). Induction of immune
tolerance by administration of monoclonal antibody to L3T4. J Immunol 137, 1127-32.
Hakeniberg, P., Kogler, G., and Wemet, P. (1998). NETCORD: a cord blood allocation
network. Bone Marrow Transplant 22 Suppl 1, S I7-8.
Hakimi, F. M., CL. (1997). The Immune System: Effector and target o f Graft-versus host
disease. In Graft-vs.-Host Disease, J. D. Ferrara, HJ; Burakoff, SJ, ed. (New York: Marcel
Dekkeir, Inc.), pp. 257-290.
Hakim., F. T., Payne, S., and Shearer, G. M. (1994). Recovery of T cell populations after
acute graft-vs-host reaction. J Immunol 152, 58-64.
199

BmUCXlRAPHY
Hale, G., Bright, S., Chumbley, G., Hoang, T., Metcalf, D., Munro, A. J., and Waldmann, H.
(1983). Removal o f T cells from bone marrow for transplantation: a m onoclonal
antilymphocyte antibody that fixes human complement. Blood 62, 873-82.
Hale, G., Cobbold, S. P., Waldmann, H., Easter, G., Matejtschuk, P., and Coombs, R. R.
(1987). Isolation of low-frequency class-switch variants from rat hybrid myelomas. J
Immunol Methods 103, 59-67.
Hale, G., Zhang, M. J., Bunjes, D., Prentice, H. G., Spence, D., Horowitz, M. M., Barrett, A.
J., and Waldmann, H. (1998). Improving the outcome of bone marrow transplantation by
using CD52 monoclonal antibodies to prevent graft-versus-host disease and graft
rejection. Blood 92, 4581-90.
Hamann, D., Baars, P. A., Hooibrink, B., and van Lier, R. W. (1996). Heterogeneity of the
human CD44- T-cell population: two distinct CD4+ T- cell subsets characterized by
coexpression o f CD45RA and CD45RO isoforms. Blood 88, 3513-21.
Hamann, D., Baars, P. A., Rep, M. H., Hooibrink, B., Kerkhof-Garde, S. R., Klein, M. R.,
and van Lier, R. A. (1997). Phenotypic and functional separation of memory and effector
human CD8+ T cells. J Exp Med 186, 1407-18.
Hamann, D., Kostense, S., Wolthers, K. C., Otto, S. A., Baars, P. A., Miedema, F., and van
Lier, R. A. (1999). Evidence that human CD8+CD45RA-I-CD27- cells are induced by
antigen and evolve through extensive rounds of division. Int Immunol 11, 1027-33.
Hammer, A., Hutter, H., Blaschitz, A., Mahnert, W., Hartmann, M., Uchanska-Ziegler, B.,
Ziegler, A., and Dohr, G. (1997). Amnion epithelial cells, in contrast to trophoblast cells,
express all classical HLA class I molecules together with HLA-G. Am J Reprod Immunol
37, 161-71.
Hammer, A., Hutter, H., and Dohr, G. (1997). HLA class I expression on the materno-fetal
interface. Am J Reprod Immunol 38, 150-7.
Han, P., Hodge, G., Story, C., and Xu, X. (1995). Phenotypic analysis o f functional T-
lymphocyte subtypes and natural killer cells in human cord blood: relevance to umbilical
cord blood transplantation. Br J Haematol 89, 733-40.
Hansen, J. A., Atkinson, K., Martin, P. J., Storb, R., Longton, G., and Thomas, E. D.
(1983). Human T lymphocyte phenotypes after bone marrow transplantation. T cells
expressing la-like antigen. Transplantation 36, 277-81.
200

B ib l io g r a p h y
Hansen, J. A., Clift, R. A., Mickelson, E. M., Nisperos, B., and Thomas, E. D. (1981).
Marrow transplantation from donors other than HLA identical siblings. Hum Immunol 2,
31-40 .
Hansen, J. A., Clift, R. A., Thomas, E. D., Buckner, C. D., Storb, R., and Giblett, E. R.
(1980). Transplantation of marrow from an unrelated donor to a patient with acute
leukemia. N Engl J Med 303, 565-7.
Hansen, J. A., Gooley, T. A., Martin, P. J., Appelbaum, P., Chauncey, T. R., Clift, R. A.,
Petersdorf, E. W., Radich, J., Sanders, J. E., Storb, R. P., Sullivan, K. M., and Anasetti, C.
(1998). Bone marrow transplants from unrelated donors for patients with chronic m yeloid
leukemia. N Engl J Med 338, 962-8.
Harding, C. V., and Unanue, E. R. (1990). Quantitation of antigen-presenting cell MHC
class Il/peptide complexes necessary for T-cell stimulation. Nature 346, 574-6.
Harris, D. T. (1995). In vitro and in vivo assessment o f the graft-versus-leukaemia activity
o f cord blood. Bone Marrow Transplantation 15, 17-23.
Harris, D. T., LoCascio, J., and Besencon, P. J. (1994). Analysis o f the alloreactive
capacity o f human umbilical cord blood: implications for graft-versus-host disease. Bone
Marrow Transplantation 14, 545-553.
Harris, D. T., Schumacher, M. J., Locascio, J., Besencon, P. J., Olson, G. B., DeLuca, D.,
Shenker, L., Bard, J., and Boyse, E. A. (1992). Phenotypic and functional immaturity o f
human umbilical cord blood T lymphocytes. Proc Natl Acad Sci U S A 89, 10006-10.
Hassan, J., ONeill, S., ONeill, L. A., Pattison, U., and Reen, D. J. (1995). Signalling via
CD28 of human naive neonatal T lymphocytes. Clin Exp Immunol 102, 192-8.
Hassan, J., and Reen, D. (1997). Cord blood CD4+ CD45RA+ T cells achieve a lower
magnitude o f activation when compared with their adult counterparts. Immunology 90,
397-401 .
Hata, T., Kawamura, T., Pujiwaki, R., Aoki, S., Hata, K., and Inada, K. (1997). Interleukin-
4, interleukin-10, and soluble tumor necrosis factor receptors in cord blood. Gynecol
Obstet Invest 43, 155-7.
Hatzakis, A., Touloumi, G., Karanicolas, R., Karafoulidou, A., Mandalaki, T.,
Anastassopoulou, C., Zhang, L., Goedert, J. J., Ho, D. D., and Kostrikis, L. G. (2000).
Effect o f recent thymic emigrants on progression of HIV-1 disease. Lancet 355, 599-604.
201

B ib l k x ir a p h y
Hayflick, L., and Moorhead, P. S. (1961). The serial cultivation o f human diploid strains.
Exp Cell Res 25, 585-621.
Hazenberg, M. D., Otto, S. A., Cohen Stuart, J. W., Verschuren, M. C., Borleffs, J. C.,
Boucher, C. A., Coutinho, R. A., Lange, J. M., Rinke de Wit, T. F., Tsegaye, A., van
Dongen, J. J., Hamann, D., de Boer, R. J., and Miedema, F. (2000). Increased cell division
but not thymic dysfunction rapidly affects the T-cell receptor excision circle content o f
the naive T cell population in HIV-1 infection. Nat Med 6, 1036-42.
Hebib, N. C., Deas, O., Rouleau, M., Durrbach, A., Charpentier, B., Beaujean, P., Yemant, J.
P., and Senik, A. (1999). Peripheral blood T cells generated after allogeneic bone marrow
transplantation: lower levels of bcl-2 protein and enhanced sensitivity to spontaneous and
CD95-mediated apoptosis in vitro. Abrogation o f the apoptotic phenotype coincides with
the recovery of normal naive/primed T-cell profiles. Blood 94, 1803-13.
Heim, D. A., and Dunbar, C. E. (2000). Hematopoietic stem cell gene therapy: towards
clinically significant gene transfer efficiency. Immunol Rev 178, 29-38.
Hertz, C. J., Kiertscher, S. M., Godowski, P. J., Bouis, D. A., Norgard, M. V., Roth, M. D.,
and Modlin, R. L. (2001). Microbial lipopeptides stimulate dendritic cell maturation via
Toll- like receptor 2. J Immunol 166, 2444-50.
Heslop, H. E., and Rooney, C. M. (1997). Adoptive cellular immunotherapy for EBV
lymphoproliferative disease. Immunol Rev 157, 217-22.
Hintzen, R. Q., de Jong, R., Lens, S. M., Brouwer, M., Baars, P., and van Lier, R. A. (1993).
Regulation o f CD27 expression on subsets of mature T-lymphocytes. J Immunol 151,
2426-35 .
Hochberg, E. P., Chillemi, A. C., Wu, C. J., Neuberg, D., Canning, C., Hartman, K., Alyea,
E. P., Soiffer, R. J., Kalams, S. A., and Ritz, J. (2001). Quantitation of T-cell neogenesis in
vivo after allogeneic bone marrow transplantation in adults. Blood 98, 1116-21.
Hoffmann, J. A., Kafatos, F. C., Jane way, C. A., and Ezekowitz, R. A. (1999). Phylogenetic
perspectives in innate immunity. Science 284, 1313-8.
Hollander, G . A., Widmer, B., and Burakoff, S. J. (1994). Loss o f normal thymic
repertoire selection and persistence of autoreactive T cells in graft vs host disease. J
Immunol 152, 1609-17.
202

BIBLICXTiRAPHY
Hollander, G. B. S. (1997). Thymie T-cell development. In Graft-vs.-Host Disease, J. D.
Ferrara, HJ; Burakoff, SJ, ed. (New York: Marcel Decker, Inc.), pp. 1-50.
Hongeng, S., Krance, R. A., Bowman, L. C., Srivastava, D. K., Cunningham, J. M., Horwitz,
E. M., Brenner, M. K., and Heslop, H. E. (1997). Outcomes of transplantation with
matched-sibling and unrelated-donor bone marrow in children with leukaemia. Lancet
350, 767-771.
Horowitz, M. B., MM. (1992). The role of registries in evaluating the results o f bone
marrow transplantation. In Bone marrow transplantation in practice, B. J. Treleaven J, ed.
(Edinburgh: Churchill Livingstone), pp. 367-377.
Horowitz, M. M., Gale, R. P., and M., S. P. (1990). Graft-versus-leukemia reaction after
bone marrow transplantation. Blood 75, 555-562.
Howard, J. K., Lord, G. M., Matarese, G., Vendetti, S., Ghatei, M. A., Ritter, M. A., Lechler,
R. 1., and Bloom, S. R. (1999). Leptin protects mice from starvation-induced lym phoid
atrophy and increases thymic cellularity in ob/ob mice. J Clin Invest 104, 1051-9.
Howie, D., Spencer, J., DeLord, D., Pitzalis, C., Wathen, N. C., Dogan, A., Akbar, A., and
MacDonald, T. T. (1998). Extrathymic T cell differentiation in the human intestine early
in life. J Immunol 161, 5862-72.
Hows, J. M., Yin, J. L., Marsh, J., Swirsky, D., Jones, L., Apperley, J. P., James, D. C.,
Smithers, S., Batchelor, J. R., Goldman, J. M., and et al. (1986). Histocompatible unrelated
volunteer donors compared with HLA nonidentical family donors in marrow
transplantation for aplastic anemia and leukemia. Blood 68, 1322-8.
Hu, H., Huston, G., Duso, D., Lepak, N., Roman, E., and Swain, S. L. (2001). CD4(-t-) T
cell effectors can become memory cells with high efficiency and without further division.
Nat Immunol 2, 705-10.
Hunt, D. W., Huppertz, H. 1., Jiang, H. J., and Petty, R. E. (1994). Studies o f human cord
blood dendritic cells: evidence for functional immaturity. Blood 84, 4333-43.
Hunziker, L., Klenerman, P., Zinkemagel, R., and Ehl, S. (2002). Exhaustion of cytotoxic
T cells during adoptive immunotherapy o f virus carrier mice can be prevented by B cells
or CD4(4-) T cells. Eur J Immunol 32, 374-382.
203

BffiLIOGRAPHY
Hutloff, A., Dittrich, A. M., Beier, K. C., Eljaschewitsch, B., Kraft, R., Anagnostopoulos, L,
and Kroczek, R. A. (1999). ICOS is an inducible T-cell co-stimulator structurally and
functionally related to CD28. Nature 397, 263-6.
lezzi, G., Scheidegger, D., and Lanzavecchia, A. (2001). Migration and function o f
antigen-primed nonpolarized T lymphocytes in vivo. J Exp Med 193, 987-93.
Ito, H., Kurtz, J., Shaffer, J., and Sykes, M. (2001). CD4 T cell-mediated alloresistance to
fully MHC-mismatched allogeneic bone marrow engraftment is dependent on CD40-
CD40 ligand interactions, and lasting T cell tolerance is induced by bone marrow
transplantation with initial blockade o f this pathway. J Immunol 166, 2970-81.
Jackson, S. P., and Jeggo, P. A. (1995). DNA double-strand break repair and V(D)J
recombination: involvement of DNA-PK. Trends Biochem Sci 20, 412-5.
Jacob, J., and Baltimore, D. (1999). Modelling T-cell memory by genetic marking o f
memory T cells in vivo. Nature 399, 593-7.
Jameson, S. C., and Bevan, M. J. (1998). T-cell selection. Curr Opin Immunol 10, 214-9.
Jamieson, B. D., Douek, D. C., Killian, S., Hultin, L. E., Scripture-Adams, D. D., Giorgi, J.
V., Marelli, D., Koup, R. A., and Zack, J. A. (1999). Generation of functional thymocytes
in the human adult. Immunity 10, 569-75.
Janossy, G., Prentice, H. G., Grob, J. P., Ivory, K., Tidman, N., Grundy, J., Favrot, M.,
Brenner, M. K., Campana, D., Blacklock, H. A., and et al. (1986). T lymphocyte
regeneration after transplantation of T cell depleted allogeneic bone marrow. Clin Exp
Immunol 63, 577-86.
Jendro, M. C., Ganten, T., Matteson, E. L., Weyand, C. M., and Goronzy, J. J. (1995).
Emergence of oligoclonal T cell populations following therapeutic T cell depletion in
rheumatoid arthritis. Arthritis Rheum 38, 1242-51.
Jenkins, M. K., and Schwartz, R. H. (1987). Antigen presentation by chemically m odified
splenocytes induces antigen- specific T cell unresponsiveness in vitro and in vivo. J Exp
Med 165, 302-19.
Johnson, B. D., and Truitt, R. L. (1992). A decrease in graft-vs.-host disease without loss
of graft-vs.-leukemia reactivity after MHC-matched bone marrow transplantation by
selective depletion of donor NK cells in vivo. Transplantation 54, 104-12.
204

B iBLIOGRAI’HY
Joly, p., Guillon, J. M., Mayaud, C., Plata, P., Theodorou, I., Denis, M., Debre, P., and
Autran, B. (1989). Cell-mediated suppression o f HIV-specific cytotoxic T lymphocytes. J
Immunol 143, 2193-201.
Kadowaki, N., Ho, S., Antonenko, S., Malefyt, R. W., Kastelein, R. A., Bazan, P., and Liu,
Y. J. (2001). Subsets o f human dendritic cell precursors express different toll-like
receptors and respond to different microbial antigens. J Exp Med 194, 863-9.
Kaech, S. M., and Ahmed, R. (2001). Memory CD8+ T cell differentiation: initial antigen
encounter triggers a developmental program in naive cells. Nat Immunol 2, 415-22.
Kaisho, T., and Akira, S. (2001). Dendritic-cell function in Toll-like receptor- and
MyD88-knockout mice. Trends Immunol 22, 78-83.
Kane, L. P., Lin, J., and Weiss, A. (2000). Signal transduction by the TCR for antigen.
Curr Opin Immunol 12, 242-9.
Kansas, G. S. (1996). Selectins and their ligands: current concepts and controversies.
Blood 88, 3259-87.
Kearney, E. R., Pape, K. A., Loh, D. Y., and Jenkins, M. K. (1994). Visualization o f
peptide-specific T cell immunity and peripheral tolerance induction in vivo. Immunity 1,
327-39 .
Kearney, E. R., Walunas, T. L., Karr, R. W., Morton, P. A., Loh, D. Y., Bluestone, J. A., and
Jenkins, M. K. (1995). Antigen-dependent clonal expansion o f a trace population o f
antigen- specific CD4+ T cells in vivo is dependent on CD28 costimulation and inhibited
by CTLA-4. J Immunol 155, 1032-6.
Kedl, R. M., Rees, W. A., Hildeman, D. A., Schaefer, B., Mitchell, T., Kappler, J., and
Marrack, P. (2000). T cells compete for access to antigen-bearing antigen-presenting
cells. J Exp Med 192, 1105-13.
Keever, C., Abu-Hajir, M., Graf, W., McFadden, P., Prichard, P., OqBrien, J., and
Flomenberg, N. (1995). Characterization of the alloreactivity and anti-leukemia reactivity
o f cord blood mononuclear cells. J Bone Marrow Transplant 15, 407-19.
Keever, C. A., Abu-Hajir, M., Graf, W., McFadden, P., Prichard, P., O'Brien, J., and
Flomenberg, N. (1995). Characterization of the alloreactivity and anti-leukemia reactivity
of cord blood mononuclear cells. Bone Marrow Transplant 15, 407-19.
205

B ib l io g r a p h y
Kendall, M. D., Johnson, H. R., and Singh, J. (1980). The weight o f the human thymus
gland at necropsy. J Anat 131, 483-97.
Kennedy, M. K., Glaccum, M., Brown, S. N., Butz, E. A., Viney, J. L., Embers, M.,
Matsuki, N., Charrier, K., Sedger, L., Willis, C. R., Brasel, K., Morrissey, P. J., Stocking, K.,
Schuh, J. C., Joyce, S., and Peschon, J. J. (2000). Reversible defects in natural killer and
memory CD8 T cell lineages in interleukin 15-deficient mice. J Exp Med 191, 771-80.
Kern, P., Khatamzas, E., Surel, I., Frommel, C., Reinke, P., Waldrop, S. L., Picker, L. J., and
Volk, H. D. (1999). Distribution of human CMV-specific memory T cells among the
CD8pos. subsets defined by CD57, CD27, and CD45 isoforms. Eur J Immunol 29, 2908-
15.
Keman, N. A., Bartsch, G., Ash, R. C., Beatty, P. G., Champlin, R., Filipovich, A., Gajewski,
J., Hansen, J. A., Henslee-Downey, J., McCullough, J., and et al. (1993). Analysis o f 462
transplantations from unrelated donors facilitated by the National Marrow Donor
Program. N Engl J Med 328, 593-602.
Keman, N. A., Flomenberg, N., Dupont, B., and O'Reilly, R. J. (1987). Graft rejection in
recipients o f T-cell-depleted HLA-nonidentical marrow transplants for leukemia.
Identification o f host-derived antidonor allocytotoxic T lymphocytes. Transplantation 43,
842-7 .
Khomts, A., Mondino, A., Pape, K. A., Reiner, S. L., and Jenkins, M. K. (1998). A natural
immunological adjuvant enhances T cell clonal expansion through a CD28-dependent,
interleukin (IL)-2-independent mechanism. J Exp Med 187, 225-36.
Khouri, I. P., Keating, M., Korbling, M., Przepiorka, D., Anderlini, P., O'Brien, S., Giralt,
S., Ippoliti, C., von Wolff, B., Gajewski, J., Donato, M., Claxton, D., Ueno, N., Andersson,
B., Gee, A., and Champlin, R. (1998). Transplant-lite; induction of graft-versus-
malignancy using fludarabine- based nonablative chemotherapy and allogeneic blood
progenitor-cell transplantation as treatment for lymphoid malignancies. J Clin Oncol 16,
2817-24 .
Kieper, W. C., and Jameson, S. C. (1999). Homeostatic expansion and phenotypic
conversion of naive T cells in response to self peptide/MHC ligands. Proc Natl Acad Sci U
S A 9 6 , 13306-11.
Kieper, W. C., Prlic, M., Schmidt, C. S., Mescher, M. P., and Jameson, S. C. (2001). 11-12
enhances CD8 T cell homeostatic expansion. J Immunol 166, 5515-21.
206

BffiLia'iRAPHY
King, D. W., Reed, E., and Suciu-Foca, N. (1989). Complexes of soluble HLA antigens
and anti-HLA autoantibodies in human sera: possible role in maintenance o f self
tolerance. Immunol Res 8, 249-62.
Kishi, H., Borgulya, P., Scott, B., Karjalainen, K., Traunecker, A., Kaufman, J., and von
Boehmer, H. (1991). Surface expression of the beta T cell receptor (TCR) chain in the
absence o f other TCR or CD3 proteins on immature T cells. Embo J 10, 93-100.
Kishimoto, H., and Sprent, J. (1999). Strong TCR ligation without costimulation causes
rapid onset of Fas- dependent apoptosis of naive murine CD4-I- T cells. J Immunol 163,
1817-26.
Kitamura, D., Roes, J., Kuhn, R., and Rajewsky, K. (1991). A B cell-deficient mouse by
targeted disruption of the membrane exon of the immunoglobulin mu chain gene. Nature
350, 423-6.
Klein, A. K., Patel, D. D., Gooding, M. E., Sempowski, G. D., Chen, B. J., Liu, C.,
Kurtzberg, J., Haynes, B. F., and Chao, N. J. (2001). T-Cell recovery in adults and
children following umbilical cord blood transplantation. Biol Blood Marrow Transplant 7,
4 5 4-66 .
Klein, J., and Sato, A. (2000). The HLA system. First of two parts. N Engl J Med 343,
702-9 .
Klein, J., and Sato, A. (2000). The HLA system. Second of two parts. N Engl J Med 343,
782-6 .
Koh, M. B., Prentice, H. G., and Lowdell, M. W. (1999). Selective removal o f alloreactive
cells from haematopoietic stem cell grafts: graft engineering for GVHD prophylaxis.
Bone Marrow Transplant 23, 1071-9.
Kolb, H. J., Mittermuller, J., Clemm, C., Holler, E., Ledderose, G., Brehm, G., Heim, M.,
and Wilmanns, W. (1990). Donor leukocyte transfusions for treatment o f recurrent
chronic myelogenous leukemia in marrow transplant patients. Blood 76, 2462-5.
Kolb, H. J., Schattenberg, A., Goldman, J. M., Hertenstein, B., Jacobsen, N., Arcese, W.,
LJungman, P., Ferrant, A., Verdonck, L., Niederwieser, D., and et al. (1995). Graft-versus-
leukemia effect of donor lymphocyte transfusions in marrow grafted patients. European
Group for Blood and Marrow Transplantation Working Party Chronic Leukemia. Blood
86, 2041-50.
207

BiBLiaiR A PH Y
Kondo, M., Weissman, I, L., and Akashi, K. (1997). Identification of clonogenic com m on
lymphoid progenitors in mouse bone marrow. Cell 97, 661-72.
Kong, F., Chen, C. H., and Cooper, M. D. (1998). Thymic function can be accurately
monitored by the level of recent T cell emigrants in the circulation. Immunity 8, 97-104.
Kong, P. K., Chen, C. L., Six, A., Hockett, R. D., and Cooper, M. D. (1999). T cell
receptor gene deletion circles identify recent thymic emigrants in the peripheral T cell
pool. Proc Natl Acad Sci U S A 96, 1536-40.
Korbling, M., Anderlini, P., and Hematology, T. A. (2001). Peripheral blood stem cell
versus bone marrow allotransplantation: does the source of hematopoietic stem cells
matter? Blood 98, 2900-8.
Kottaridis, P. D., Milligan, D. W., Chopra, R., Chakraverty, R. K., Chakrabarti, S.,
Robinson, S., Peggs, K., Verfuerth, S., Pettengell, R., Marsh, J. C., Schey, S., Mahendra, P.,
Morgan, G. J., Hale, 0 ., Waldmann, H., de Elvira, M. C., Williams, C. D., Devereux, S.,
Linch, D. C., Goldstone, A. H., and Mackinnon, S. (2000). In vivo CAM PATH-IH
prevents graft-versus-host disease following nonmyeloablative stem cell transplantation.
Blood 96, 2419-25.
Krangel, M. S., Hemandez-Munain, C., Lauzurica, P., McMurry, M., Roberts, J. L., and
Zhong, X. P. (1998). Developmental regulation of V(D)J recombination at the TCR
alpha/delta locus. Immunol Rev 165, 131-47.
Krauss, T., Azab, H., Dietrich, M., and Augustin, H. G. (1998). Fetal plasma levels o f
circulating endothelial cell adhesion molecules in normal and preeclamptic pregnancies.
Eur J Obstet Gynecol Reprod Biol 78, 41-5.
Krenger, W., and Ferrara, J. L. M. (1996). Dysregulation o f cytokines during graft-versus-
host disease. J. Hematol. 3, 3-14.
Krenger, W., Rossi, S., Piali, L., and Hollander, G. A. (2000). Thymic atrophy in murine
acute graft-versus-host disease is effected by impaired cell cycle progression o f host pro-
T and pre-T cells. Blood 96, 347-54.
Krishnaswamy, G., Smith, J. K., Srikanth, S., Chi, D. S., Kalbfleisch, J. H., and Huang, S. K.
(1996). Lymphoblastoid interferon-alpha inhibits T cell proliferation and expression o f
eosinophil-activating cytokines. J Interferon Cytokine Res 16, 819-27.
208

B iBLIOCjRAPHY
Krummel, M. F., and Allison, J. P. (1996). CTLA-4 engagement inhibits IL-2
accumulation and cell cycle progression upon activation of resting T cells. J Exp Med
183, 2533-40.
Ku, C. C., Murakami, M., Sakamoto, A., Kappler, J., and Marrack, P. (2000). Control o f
homeostasis of CD8+ memory T cells by opposing cytokines. Science 288, 675-8.
Kundig, T. M., Schorle, H., Bachmann, M. P., Hengartner, H., Zinkemagel, R. M., and
Horak, I. (1993). Immune responses in interleukin-2-deficient mice. Science 262, 1059-
61.
Kundig, T. M., Shahinian, A., Kawai, K., Mittrucker, H. W., Sebzda, E., Bachmann, M. F.,
Mak, T. W., and Ohashi, P. S. (1996). Duration o f TCR stimulation determines
costimulatory requirement o f T cells. Immunity 5, 41-52.
Lafferty, K. J., Prowse, S. J., Simeonovic, C. J., and Warren, H. S. (1983). Im m unobiology
of tissue transplantation: a return to the passenger leukocyte concept. Annu Rev Immunol
1, 143-73.
Lafferty, K. J., and Woolnough, J. (1977). The origin and mechanism of the allograft
reaction. Immunol Rev 35, 231-62.
Lansdorp, P. M., Dragowska, W., Thomas, T. E., Little, M. T., and Mayani, H. (1994).
Age-related decline in proliferative potential of purified stem cell candidates. Blood Cells
20, 376-80.
Lanzavecchia, A., and Sallusto, F. (2000). Dynamics o f T lymphocyte responses:
intermediates, effectors, and memory cells. Science 290, 92-7.
Laouar, Y., and Crispe, I. N. (2000). Functional flexibility in T cells: independent
regulation of CD4+ T cell proliferation and effector function in vivo. Immunity 13, 291-
301.
Lawrence, M. B., and Springer, T. A. (1991). Leukocytes roll on a selectin at physiologic
flow rates: distinction from and prerequisite for adhesion through integrins. Cell 65, 859-
73.
Lee, C. K., Kim, K., Welniak, L. A., Murphy, W. J., Muegge, K., and Durum, S. K. (2001).
Thymic emigrants isolated by a new method possess unique phenotypic and functional
properties. Blood 97, 1360-9.
209

B ib l io c î r a iw
Lefrancois, L., and Puddington, L. (1995). Extrathymic intestinal T-cell development:
virtual reality? Immunol Today 16, 16-21.
Legendre, C. M., Guttmann, R. D., Hou, S. K., and Jean, R. (1985). Two-color
immunofluorescence and flow cytometry analysis of lymphocytes in long-term renal
allotransplant recipients: identification of a major Leu-7+/Leu-3-i- subpopulation. J
Immunol 135, 1061-6.
Leino, L., Lilius, E. M., Nikoskelainen, J., Pelliniemi, T. T., and Rajamaki, A. (1991). The
reappearance o f 10 differentiation antigens on peripheral blood lymphocytes after
allogeneic bone marrow transplantation. Bone Marrow Transplant 8, 339-44.
LeMaoult, J., Messaoudi, I., Manavalan, J. S., Potvin, H., Nikolich-Zugich, D., Dyall, R.,
Szabo, P., Weksler, M. E., and Nikolich-Zugich, J. (2000). Age-related dysregulation in
CDS T cell homeostasis: kinetics of a diversity loss. J Immunol 165, 2367-73.
Lenschow, D. J., Walunas, T. L., and Bluestone, J. A. (1996). CD28/B7 system of T cell
costimulation. Annu Rev Immunol 14, 233-58.
Leo, A., and Schraven, B. (2001). Adapters in lymphocyte signalling. Curr Opin Immunol
13, 307-16.
Leposavic, G., Obradovic, S., Kosec, D., Pejcic-Karapetrovic, B., and Vidic-Dankovic, B.
(2001). In vivo modulation of the distribution of thymocyte subsets by female sex steroid
hormones. Int Immunopharmacol 1, 1-12.
Leroy, E., Calvo, C. P., Divine, M., Gourdin, M. P., Baujean, P., Ben Aribia, M. H., Mishal,
Z., Vemant, J. P., Parcet, J. P., and Senik, A. (1986). Persistence o f T8+/HNK-1 +
suppressor lymphocytes in the blood of long- term surviving patients after allogeneic
bone marrow transplantation. J Immunol 137, 2180-9.
Leussink, V. I., Jung, S., Merschdorf, U., Toyka, K. V., and Gold, R. (2001). H igh-dose
methylprednisolone therapy in multiple sclerosis induces apoptosis in peripheral b lood
leukocytes. Arch Neurol 58, 91-7.
Lewis, D. B., Yu, C. C., Meyer, J., English, B. K., Kahn, S. J., and Wilson, C. B. (1991).
Cellular and molecular mechanisms for reduced interleukin 4 and interferon-gamma
production by neonatal T cells. J Clin Invest 87, 194-202.
Lewis, S. M. (1994). The mechanism of V(D)J joining: lessons from molecular,
immunological, and comparative analyses. Adv Immunol 56, 27-150.
210

BiBLKXiRAPHY
Lin, H., Mosmann, T. R., Guilbert, L., Tuntipopipat, S., and Wegmann, T. G. (1993).
Synthesis o f T helper 2-type cytokines at the maternal-fetal interface. J Immunol 757,
4 5 62-73 .
Lind, E. P., Prockop, S. E., Porritt, H. E., and Petrie, H. T. (2001). Mapping precursor
movement through the postnatal thymus reveals specific microenvironments supporting
defined stages of early lymphoid development. J Exp Med 194, 127-34.
Lipp-Zwahlen, A. E., Tuchschmid, P., Silberschmidt, M., and Due, G. (1983). Arterial
cord blood hypoxanthine: a measure of intrauterine hypoxia? Biol Neonate 44, 193-202.
Liu, J., Anderson, B. E., Robert, M. E., McNiff, J. M., Emerson, S. G., Shlomchik, W. D.,
and Shlomchik, M. J. (2001). Selective T-cell subset ablation demonstrates a role for T1
and T2 cells in ongoing acute graft-versus-host disease: a model system for the reversal o f
disease. Blood 98, 3367-75.
Liu, Z., Savoldo, B., Huls, H., Lopez, T., Gee, A., Wilson, J., Brenner, M. K., Heslop, H. E.,
and Rooney, C. M. (2002). Epstein-Barr virus (EBV)-specific cytotoxic T lymphocytes
for the prevention and treatment o f EBV-associated post-transplant lymphomas. Recent
Results Cancer Res 159, 123-33.
Livak, F., Petrie, H. T., Crispe, I. N., and Schatz, D. G. (1995). In-frame TCR delta gene
rearrangements play a critical role in the alpha beta/gamma delta T cell lineage decision.
Immunity 2, 617-27.
Livak, F., and Schatz, D. G. (1996). T-cell receptor alpha locus V(D)J recombination b y
products are abundant in thymocytes and mature T cells. Mol Cell Biol 16, 609-18.
Locatelli, P., Rocha, V., Chastang, C., Arcese, W., Michel, G., Abecasis, M., Messina, C.,
Ortega, J., Badell-Serra, I., Plouvier, E., Souillet, G., Jouet, J. P., Pasquini, R., Ferreira, E.,
Gamier, P., and Gluckman, E. (1999). Factors associated with outcome after cord blood
transplantation in children with acute leukemia. Eurocord-Cord Blood Transplant Group.
Blood 93, 3662-71.
Lodolce, J. P., Boone, D. L., Chai, S., Swain, R. E., Dassopoulos, T., Trettin, S., and Ma, A.
(1998). IL-15 receptor maintains lymphoid homeostasis by supporting lym phocyte
homing and proliferation. Immunity 9, 669-76.
211

B iBLICX'iRAPHY
Lollo, B. A., Chan, K. W., Hanson, E. M., Moy, V. T., and Brian, A. A. (1993). Direct
evidence for two affinity states for lymphocyte function- associated antigen 1 on activated
T cells. J Biol Chem 268, 21693-700.
Lowdell, M. W., Craston, R., Ray, N., Koh, M., Galatowicz, G., and Prentice, H. G. (1998).
The effect of T cell depletion with Campath-IM on immune reconstitution after
chemotherapy and allogeneic bone marrow transplant as treatment for leukaemia. Bone
Marrow Transplant 21, 679-86.
Lowenberg, B., Wagemaker, G., van Bekkum, D, W., Sizoo, W., Sintnicolaas, K., Hendriks,
W. D., and Hagenbeek, A. (1986). Graft-versus-host disease following transplantation o f
'one log' versus 'two log' T-lymphocyte-depleted bone marrow from HLA-identical
donors. Bone Marrow Transplant 1, 133-40.
Lucas, B., Vasseur, P., and Penit, C. (1994). Production, selection, and maturation o f
thymocytes with high surface density of TCR. J Immunol 153, 53-62,
Lucivero, G., Dalla Mora, L., Bresciano, E., Loria, M. P., Pezone, L., and Mancino, D.
(1996). Functional characteristics of cord blood T lymphocytes after lectin and anti-CD3
stimulation. Differences in the way T cells express activation molecules and proliferate.
Int J Clin Lab Res 26, 255-61.
Lum, L. G. (1987). The kinetics of immune reconstitution after human marrow
transplantation. Blood 69, 369-80.
Lyons, D. S., Lieberman, S. A., Hampl, J., Boniface, J. J., Chien, Y., Berg, L. J., and Davis,
M. M. (1996). A TCR binds to antagonist ligands with lower affinities and faster
dissociation rates than to agonists. Immunity 5, 53-61.
Mackall, C. L., Bare, C. V., Granger, L. A., Sharrow, S. O., Titus, J. A., and Gress, R. E.
(1996). Thymic-independent T cell regeneration occurs via antigen-driven expansion o f
peripheral T cells resulting in a repertoire that is limited in diversity and prone to skewing.
J Immunol 156, 4609-16.
Mackall, C. L., Fleisher, T. A., Brown, M. R., Andrich, M. P., Chen, C. C., Feuerstein, I. M.,
Horowitz, M. E., Magrath, I. T., Shad, A. T., Steinberg, S. M., and et al. (1995). Age,
thymopoiesis, and CD4+ T-lymphocyte regeneration after intensive chemotherapy [see
comments]. N Engl J Med 332, 143-9.
Mackall, C. L., Fleisher, T. A., Brown, M. R., Andrich, M. P., Chen, C. C., Feuerstein, I. M.,
Magrath, I. T., Wexler, L. H., Dimitrov, D. S., and Gress, R. E. (1997). Distinctions
212

B ib l io g r a p h y
between CD8+ and CD4+ T-cell regenerative pathways result in prolonged T-cell subset
imbalance after intensive chemotherapy. Blood 89, 3700-7.
Mackall, C. L., Fleisher, T. A., Brown, M. R., Magrath, I. T., Shad, A. T., Horowitz, M. E.,
Wexler, L. H., Adde, M. A., McClure, L. L., and Gress, R. E. (1994). Lym phocyte
depletion during treatment with intensive chemotherapy for cancer. Blood 84, 2221-8.
Mackall, C. L., Fry, T. J., Bare, C., Morgan, P., Galbraith, A., and Gress, R. E. (2001). IL-7
increases both thymic-dependent and thymic-independent T-cell regeneration after bone
marrow transplantation. Blood 97, 1491-7.
Mackall, C. L., Granger, L., Sheard, M. A., Cepeda, R., and Gress, R. E. (1993). T-cell
regeneration after bone marrow transplantation; differential CD45 isoform expression on
thymic-derived versus thymic-independent progeny. Blood 82, 2585-94.
Mackall, C. L., and Gress, R. E. (1997). Pathways of T-cell regeneration in mice and
humans: implications for bone marrow transplantation and immunotherapy. Immunol
Rev 157, 61-72.
Mackall, C. L., and Gress, R. E. (1997). Thymic aging and T-cell regeneration. Immunol
Rev 160, 91-102.
Mackall, C. L., Hakim, F. T., and Gress, R. E. (1997). Restoration o f T-cell homeostasis
after T-cell depletion. Semin Immunol 9, 339-46.
Mackall, C. L., Punt, J. A., Morgan, P., Farr, A. G., and Gress, R. E. (1998). Thym ic
function in young/old chimeras: substantial thymic T cell regenerative capacity despite
irreversible age-associated thymic involution. Eur J Immunol 28, 1886-93.
Mackinnon, S., Papadopoulos, E. B., Carabasi, M. H., Reich, L., Collins, N. H., Boulad, F.,
Castro-Malaspina, H., Childs, B. H., Gillio, A. P., Keman, N. A., and et al. (1 9 9 5 ).
Adoptive immunotherapy evaluating escalating doses of donor leukocytes for relapse o f
chronic myeloid leukemia after bone marrow transplantation: separation o f graft-versus-
leukemia responses from graft-versus-host disease. Blood 86, 1261-8.
Madden, K. S., Raj an. S., Bellinger, D. L., Felten, S. Y., and Felten, D. L. (1997). A ge-
associated alterations in sympathetic neural interactions with the immune system. Dev
Comp Immunol 21, 479-86.
213

BiBLiaiR A PH Y
Madrigal, J. A., Scott, I., Arguello, R., Szydlo, R., Little, A. M., and M., G. J. (1997).
Factors influencing the outcome of bone marrow transplants using unrelated donors.
Immunology Reviews 157, 153.
Maki, K., Sunaga, S., Komagata, Y., Kodaira, Y., Mabuchi, A., Karasuyama, H., Yokomuro,
K., Miyazaki, J. I., and Ikuta, K. (1996). Interleukin 7 receptor-deficient mice lack
gammadelta T cells. Proc Natl Acad Sci U S A 93, 7172-7.
Mallick, C. A., Dudley, E. C., Viney, J. L., Owen, M. J., and Hay day, A. C. (1993).
Rearrangement and diversity o f T cell receptor beta chain genes in thymocytes: a critical
role for the beta chain in development. Cell 73, 513-9.
Mandigers, C. M., Meijerink, J. P., Raemaekers, J. M., Schattenberg, A. V., and Mensink,
E. J. (1998). Graft-versus-lymphoma effect of donor leucocyte infusion shown by real
time quantitative PGR analysis of t(14;18). Lancet 352, 1522-3.
Maraninchi, D., Gluckman, E., Blaise, D., Guyotat, D., Rio, B., Pico, J. L., Leblond, V.,
Michallet, M., Dreyfus, P., Ifrah, N., and et al. (1987). Impact of T-cell depletion on
outcome o f allogeneic bone-marrow transplantation for standard-risk leukaemias. Lancet
2, 175-8.
Markert, M. L., Boeck, A., Hale, L. P., Kloster, A. L., McLaughlin, T. M., Batchvarova, M.
N., Douek, D. C., Koup, R. A., Kostyu, D. D., Ward, F. E., Rice, H. E., Mahaffey, S. M.,
Schiff, S. E., Buckley, R. H., and Haynes, B. F. (1999). Transplantation of thymus tissue
in complete DiGeorge syndrome. N Engl J Med 341, 1180-9.
Markert, M. L., Hummell, D. S., Rosenblatt, H. M., Schiff, S. E., Harville, T. O., Williams,
L. W., Schiff, R. I., and Buckley, R. H. (1998). Complete DiGeorge syndrome: persistence
of profound immunodeficiency. J Pediatr 132, 15-21.
Markert, M. L., Kostyu, D. D., Ward, F. E., McLaughlin, T. M., Watson, T. J., Buckley, R.
H., Schiff, S. E., Ungerleider, R. M., Gaynor, J. W., Oldham, K. T., Mahaffey, S. M.,
Ballow, M., Driscoll, D. A., Hale, L. P., and Haynes, B. F. (1997). Successful formation o f
a chimeric human thymus allograft following transplantation of cultured postnatal human
thymus. J Immunol 158, 998-1005.
Marks, D. I., Cullis, J. O., Ward, K. N., Lacey, S., Syzdlo, R., Hughes, T. P., Schwarer, A. P.,
Lutz, E., Barrett, A. J., and Hows, J. M. (1993). Allogeneic bone marrow transplantation
for chronic myeloid leukemia using sibling and volunteer unrelated donors. A
comparison o f complications in the first 2 years. Ann Intern Med 119, 207-14.
214

B id l io g r a p h y
Marmont, A. M., Horowitz, M. M., Gale, R. P., and al!!, e. (1991). T cell depletion o f
HLA-identical transplants in leukaemia. Blood 8, 2120-?
Marquez, C., Trigueros, C., Fernandez, E., and Toribio, M. L. (1995). The development o f
T and non-T cell lineages from CD34-I- human thymic precursors can be traced by the
differential expression of CD44. J Exp Med 181, 475-83.
Marrack. P., Bender, J., Hildeman, D., Jordan, M., Mitchell, T., Murakami, M., Sakamoto,
A., Schaefer, B. C., Swanson, B., and Kappler, J. (2000). Homeostasis o f alpha beta TCR-h
T cells. Nat Immunol 1, 107-11.
Martin, P. J. (1991). Increased disparity for minor histocompatibility antigens as a
potential cause of increased GVHD risk in marrow transplantation from unrelated donors
compared with related donors. Bone Marrow Transplant 8, 217-23.
Martin, P. J., Hansen, J. A., Storb, R., and Thomas, E. D. (1987). Human marrow
transplantation: an immunological perspective. Adv Immunol 40, 379-438.
Mason, D. W., and Williams, A. F. (1980). The kinetics o f antibody binding to membrane
antigens in solution and at the cell surface. Biochem J 187, 1-20.
Masuko, K., Kato, S., Hagihara, M., Tsuchida, F., Takemoto, Y., Izawa, K., Kato, T.,
Yamamori, S., Mizushima, Y., Nishioka, K., Tsuji, K., and Yamamoto, K. (1996). Stable
clonal expansion of T cells induced by bone marrow transplantation. Blood 87, 789-99.
Matsui, K., Boniface, J. J., Steffner, P., Reay, P. A., and Davis, M. M. (1994). Kinetics o f
T-cell receptor binding to peptide/I-Ek complexes: correlation of the dissociation rate
with T-cell responsiveness. Proc Natl Acad Sci U S A 97, 12862-6.
Matsuzaki, N., Saji, F., Okada, T., Sawai, K., Kameda, T., Tanaka, T., Negoro, S., and
Tanizawa, O. (1989). Demonstration o f functional immaturity o f signal transduction
pathways in human cord T cells. Cell Immunol 124, 252-63.
McAdam, A. J., Chang, T. T., Lumelsky, A. E., Greenfield, E. A., Boussiotis, V. A., Duke-
Cohan, J. S., Chernova, T., Malenkovich, N., Jabs, C., Kuchroo, V. K., Ling, V., Collins, M.,
Sharpe, A. H., and Freeman, G. J. (2000). Mouse inducible costimulatory m olecule
(ICOS) expression is enhanced by CD28 costimulation and regulates differentiation o f
CD4-I- T cells. J Immunol 165, 5035-40.
McFarland, R. D., Douek, D. C., Koup, R. A., and Picker, L. J. (2000). Identification of a
human recent thymic emigrant phenotype. Proc Natl Acad Sci U S A 97, 4215-20.
215

B ib u c x îr a p h y
McGlave, P., Bartsch, G., Anasetti, C., Ash, R., Beatty, P., Gajewski, J., and Keman, N. A.
(1993). Unrelated donor marrow transplantation therapy for chronic m yelogenous
leukemia: initial experience of the National Marrow Donor Program. Blood 81, 543-50.
McHeyzer-Williams, M. G., and Davis, M. M. (1995). Antigen-specific development o f
primary and memory T cells in vivo. Science 268, 106-11.
McSweeney, P. A., Niederwieser, D., Shizuru, J. A., Sandmaier, B. M., Molina, A. J.,
Maloney, D. G., Chauncey, T. R., Gooley, T. A., Hegenbart, U., Nash, R. A., Radich, J.,
Wagner, J. L., Minor, S., Appelbaum, F. R., Bensinger, W. I., Bryant, E., Flowers, M. E.,
Georges, G. E., Gmmet, F. C., Kiem, H. P., Torok-Storb, B., Yu, C., Blume, K. G., and
Storb, R. F. (2001). Hematopoietic cell transplantation in older patients with hem atologic
malignancies: replacing high-dose cytotoxic therapy with graft-versus- tumor effects.
Blood 97, 3390-400.
Medzhitov, R., and Jane way, C. A., Jr. (1997). Innate immunity: the virtues o f a nonclonal
system of recognition. Cell 91, 295-8.
Merino, J., Martinez-Gonzalez, M. A., Rubio, M., Inoges, S., Sanchez-Ibarrola, A., and
Subira, M. L. (1998). Progressive decrease o f CD8high-t- CD28-I- CD57- cells with ageing.
Clin Exp Immunol 112, 48-51.
Merkenschlager, M., and Beverley, P. C. (1989). Evidence for differential expression o f
CD45 isoforms by precursors for memory-dependent and independent cytotoxic
responses: human CD8 memory CTLp selectively express CD45RO (U C H Ll). Int
Immunol 1, 450-9.
Michallet, M., Bilger, K., Garban, F., Attal, M., Huyn, A., Blaise, D., Milpied, N., Moreau,
P., Bordigoni, P., Kuentz, M., Sadoun, A., Cahn, J. Y., Socie, G., Thomas, X., Arnaud, P.,
Raus, N., Lheritier, V., Pigneux, A., and Boiron, J. M. (2001). Allogeneic hematopoietic
stem-cell transplantation after nonmyeloablative preparative regimens: impact o f
pretransplantation and posttransplantation factors on outcome. J Clin Oncol 19, 3340-9.
Miller, J. F. (2001). Ruby anniversary: forty years o f thymus immunology research. Nat
Immunol 2, 663-4.
Miller, R. A., and Stutman, O. (1984). T cell repopulation from functionally restricted
splenic progenitors: 10,000-fold expansion documented by using limiting dilution
analyses. J Immunol 133, 2925-32.
216

BIBLIOC iRAI’HY
Miller, S. A., Dykes, D. D., and Polesky, H. F, (1988). A simple salting out procedure for
extracting DNA from human nucleated cells. Nucleic Acids Res 16, 1215.
Mills, K., Gross, T., Varney, M., Heimann, D., Reed, E., Kessinger, A., and Talmadge, J.
(1996). Immunologic phenotype and function in human bone marrow, blood stem cells
and umbilical cord blood. Bone Marrow Transplant 18, 53-61.
Min, D., Taylor, P., Chung, B., Panoskaltsis-Mortari, A., Farrell, C., Lacey, D., Blazar, B.,
and Weinberg, K. (2000). Protection from thymic epithelial cell injury by pre-BMT
keratinocyte growth factor; a new approach to speed thymic reconstitution after lethal
irradiation. In ASH (San Francisco: Blood), pp. 474a.
Min, D., Taylor, P., Chung, B., Panoskaltsis-Mortari., Farrell, C., Lacey, D., Blazar, B., and
Weinberg, K. (2000). Protection from thymic epithelial cell injury by pre-BMT
keratinocyte growth factor: a new approach to speed thymic reconstitution after lethal
irradiation. In ASH (San Francisco: Blood), pp. 474a.
Mitchell, T. C., Hildeman, D., Kedl, R. M., Teague, T. K., Schaefer, B. C., White, J., Zhu, Y.,
Kappler, J., and Marrack, P. (2001). Immunological adjuvants promote activated T cell
survival via induction of Bcl-3. Nat Immunol 2, 397-402.
Molldrem, J. J., Lee, P. P., Wang, C., Felio, K., Kantarjian, H. M., Champlin, R. E., and
Davis, M. M. (2000). Evidence that specific T lymphocytes may participate in the
elimination of chronic myelogenous leukemia. Nat Med 6, 1018-23.
Mombaerts, P., Clarke, A. R., Rudnicki, M. A., lacomini, J., Itohara, S., Lafaille, J. J., Wang,
L., Ichikawa, Y., Jaenisch, R., Hooper, M. L., and et al. (1992). Mutations in T-cell antigen
receptor genes alpha and beta block thymocyte development at different stages. Nature
360, 225-31.
Mondino, A., Khoruts, A., and Jenkins, M. K. (1996). The anatomy of T-cell activation
and tolerance. Proc Natl Acad Sci U S A 93, 2245-52.
Monks, C. R., Freiberg, B. A., Kupfer, H., Sciaky, N., and Kupfer, A. (1998). Three-
dimensional segregation of supramolecular activation clusters in T cells. Nature 395, 82-
6 .
Montecino-Rodriguez, E., Clark, R., and Dorshkind, K. (1998). Effects o f insulin-like
growth factor administration and bone marrow transplantation on thymopoiesis in aged
mice. Endocrinology 139, 4120-6.
217

B ib l io g r a p h y
Monteiro, J., Batliwalla, F,, Ostrer, H., and Gregersen, P. K. (1996). Shortened telomeres in
clonally expanded CD28-CD8+ T cells imply a replicative history that is distinct from
their CD28+CD8+ counterparts. J Immunol 156, 3587-90.
Morecki, S., Gelfand, Y., Nagler, A., Or, R., Naparstek, E., Varadi, G., Engelhard, D.,
Akerstein, A., and Slavin, S. (2001). Immune reconstitution following allogeneic stem cell
transplantation in recipients conditioned by low intensity vs myeloablative regimen. Bone
Marrow Transplant 28, 243-9.
Moretta, A., Maccario, R., Fagioli, F., Giraldi, E., Busca, A., Montagna, D., Miniero, R.,
Comoli, P., Giorgiani, G., Zecca, M., Pagani, S., and Locatelli, F. (2001). Analysis o f
immune reconstitution in children undergoing cord blood transplantation. Exp Hematol
29, 371-9.
Moser, B., and Loetscher, P. (2001). Lymphocyte traffic control by chemokines. Nat
Immunol 2, 123-8.
Moskophidis, D., Laine, E., and Zinkemagel, R. M. (1993). Peripheral clonal deletion o f
antiviral memory CD8+ T cells. Eur J Immunol 23, 3306-11.
Mosmann, T. R., and Sad, S. (1996). The expanding universe o f T-cell subsets: T hl, Th2
and more. Immunol Today 17, 138-46.
Mu, X. Y., and Thoman, M. L. (1999). The age-dependent cytokine production by
murine CD8-I- T cells as determined by four-color flow cytometry analysis. J Gerontol A
Biol Sci Med Sci 54, B 116-23.
Muller, S. M., Kohn, T., Schulz, A. S., Debatin, K. M., and Friedrich, W. (2000). Similar
pattern of thymic-dependent T-cell reconstitution in infants with severe com bined
immunodeficiency after human leukocyte antigen (HLA)-identical and HLA-nonidentical
stem cell transplantation. Blood 96, 4344-9.
Muller-Hermelink, H. K., Sale, G. E., Borisch, B., and Storb, R. (1987). Pathology of the
thymus after allogeneic bone marrow transplantation in man. A histologic
immunohistochemical study of 36 patients. Am J Pathol 129, 242-56.
Munn, D. H., Shafizadeh, E., Attwood, J. T., Bondarev, L, Pashine, A., and Mellor, A. L.
(1999). Inhibition o f T cell proliferation by macrophage tryptophan catabolism. J Exp
Med 189, 1363-72.
218

B ib u o g r a p h y
Munn, D. H., Zhou, M„ Attwood, J. T., Bondarev, L, Conway, S. J., Marshall, B., Brown, C.,
and Mellor, A. L. (1998). Prevention of allogeneic fetal rejection by tryptophan
catabolism. Science 281, 1191-3.
Murali-Krishna, K., Altman, J. D., Suresh, M., Sourdive, D. J., Zajac, A. J., Miller, J. D.,
Slansky, J., and Ahmed, R. (1998). Counting antigen-specific CD8 T cells: a réévaluation
of bystander activation during viral infection. Immunity 8, 177-87.
Murali-Krishna, K., Lau, L. L., Sambhara, S., Lemonnier, F., Altman, J., and Ahmed, R.
(1999). Persistence of memory CD8 T cells in MHC class I-deficient mice. Science 286,
1377-81.
Murphy, W. J., Reynolds, C. W., Tiberghien, P., and Longo, D. L. (1993). Natural killer
cells and bone marrow transplantation. J Natl Cancer Inst 85, 1475-82.
Mutis, T., Verdijk, R., Schrama, E., Esendam, B., Brand, A., and Goulmy, E. (1999).
Feasibility o f immunotherapy of relapsed leukemia with ex vivo- generated cytotoxic T
lymphocytes specific for hematopoietic system- restricted minor histocompatibility
antigens. Blood 93, 2336-41.
Myung, P. S., Boerthe, N. J., and Koretzky, G. A. (2000). Adapter proteins in lym phocyte
antigen-receptor signaling. Curr Opin Immunol 12, 256-66.
Nagata, S., and Suda, T. (1995). Fas and Fas ligand: Ipr and g Id mutations. Immunol
Today 16, 39-43.
Nagler, A., Aker, M., Or, R., Naparstek, E., Varadi, G., Brautbar, C., and Slavin, S. (2001).
Low-intensity conditioning is sufficient to ensure engraftment in matched unrelated bone
marrow transplantation. Exp Hematol 29, 362-70.
Nambiar, M. P., Enyedy, E. J., Fisher, C. U., Warke, V. G., Juang, Y. T., and Tsokos, G. C.
(2001). Dexamethasone modulates TCR zeta chain expression and antigen receptor-
mediated early signaling events in human T lymphocytes. Cell Immunol 208, 62-71.
Navarrete, C., Warwick, R., Armitage, S., Fehily, D., and Contreras, M. (1998). The
London Cord Blood Bank. Bone Marrow Transplant 22 Suppl 1, S6-7.
Nestel, F. P., Price, K. S., Seemayer, T. A., and Lapp, W. S. (1992). Macrophage priming
and lipopolysaccharide-triggered release of tumor necrosis factor alpha during graft-
versus-host disease. J Exp Med 175, 405-13.
219

BIBLIOGRAI’HY
Neuhaus, T. J., and Briner, J. (1986). Morphology of original and transplanted thymuses
in severe combined immunodeficiency. Pediatr Pathol 5, 251-70.
Nezelof, C. (1992). Thymic pathology in primary and secondary im m unodeficiencies.
Histopathology 21, 499-511.
Niehues, T., Rocha, V., Filipovich, A. H., Chan, K. W., Porcher, R., Michel, G., Ortega, J. J.,
Wemet, P., Gobel, U., Gluckman, E., and Locatelli, F. (2001). Factors affecting
lymphocyte subset reconstitution after either related or unrelated cord blood
transplantation in children — a Eurocord analysis. Br J Haematol 114, 42-8.
Niwano, Y., Hansen, T. R., Kazemi, M., Malathy, P. V., Johnson, H. D., Roberts, R. M., and
Imakawa, K. (1989). Suppression of T-lymphocyte blastogenesis by ovine trophoblast
protein- 1 and human interferon-alpha may be independent o f interleukin-2 production.
Am J Reprod Immunol 20, 21-6.
Noguchi, M., Yi, H., Rosenblatt, H. M., Filipovich, A. H., Adelstein, S., Modi, W. S.,
McBride, O. W., and Leonard, W. J. (1993). Interleukin-2 receptor gamma chain mutation
results in X-linked severe combined immunodeficiency in humans. Cell 73, 147-57.
Nosaka, T., van Deursen, J. M., Tripp, R. A., Thierfelder, W. E., Witthuhn, B. A.,
McMickle, A. P., Doherty, P. C., Grosveld, G. C., and Ihle, J. N. (1995). Defective
lymphoid development in mice lacking Jak3. Science 270, 800-2.
O'Garra, A. (1998). Cytokines induce the development of functionally heterogeneous T
helper cell subsets. Immunity 8, 275-83.
O'Herrin, S. M., Slansky, J. E., Tang, Q., Markiewicz, M. A., Gajewski, T. F., Pardoll, D.
M., Schneck, J. P., and Bluestone, J. A. (2001). Antigen-specific blockade o f T cells in
vivo using dimeric MHC peptide. J Immunol 167, 2555-60.
O'Reilly, R. J., Small, T. N., Papadopoulos, E., Lucas, K., Lacerda, J., and Koulova, L.
(1997). Biology and adoptive cell therapy of Epstein-Barr virus-associated
lymphoproliferative disorders in recipients o f marrow allografts. Immunol Rev 157, 195-
216.
Oakhill, A., Pamphilon, D. H., Potter, M. N., Steward, C. G., Goodman, S., Green, A.,
Goulden, P., Goulden, N. J., Waldmann, H., and Cornish, J. M. (1996). Unrelated donor
marrow transplanation for children with relapsed acute lymphoblastic leukaemia in
second complate remmision. Br. J. Haematology 94, 574-578.
220

B m u a iR A P H Y
Ochs, L., Shu, X. O., Miller, J., Enright, H., Wagner, J., Filipovich, A., Miller, W., and
Weisdorf, D. (1995). Late infections after allogeneic bone marrow transplantations:
comparison of incidence in related and unrelated donor transplant recipients. Blood 86,
3 9 79-86 .
Oehen, S., and Brduscha-Riem, K. (1999). Naive cytotoxic T lymphocytes spontaneously
acquire effector function in lymphocytopénie recipients: A pitfall for T cell memory
studies? Eur J Immunol 29, 608-14.
Oehme, P., Hecht, K., Jumatov, J., Repke, H., Hilse, H., and Cordova, A. (1987). Prevention
of stress-induced involution of the thymus in rats by substance P (S P l-11) and its N-
terminal fragment SP l-4 . Pharmazie 42, 34-6.
Ohbo, K., Suda, T., Hashiyama, M., Mantani, A., Ikebe, M., Miyakawa, K., Moriyama, M.,
Nakamura, M., Katsuki, M., Takahashi, K., Yamamura, K., and Sugamura, K. (1996).
Modulation o f hematopoiesis in mice with a truncated mutant o f the interleukin-2
receptor gamma chain. Blood 87, 956-67.
Oka, H., Hirohata, S., Inoue, T., and Ito, K. (1992). Effects o f interferon-alpha on human
B cell responsiveness: biphasic effects in cultures stimulated with Staphylococcus aureus.
Cell Immunol 139, 478-92.
Okazaki, K., and Sakano, H. (1988). Thymocyte circular DNA excised from T cell
receptor alpha-delta gene complex. Embo J 7, 1669-74.
Olsen, N. J., Olson, G., Viselli, S. M., Gu, X., and Kovacs, W. J. (2001). Androgen
receptors in thymic epithelium modulate thymus size and thymocyte development.
Endocrinology 142, 1278-83.
Olsen, N. J., Viselli, S. M., Fan, J., and Kovacs, W. J. (1998). Androgens accelerate
thymocyte apoptosis. Endocrinology 139, 748-52.
Opferman, J. T., Ober, B. T., and Ashton-Rickardt, P. G. (1999). Linear differentiation o f
cytotoxic effectors into memory T lymphocytes. Science 283, 1745-8.
Ottinger, H. D., Beelen, D. W., Scheulen, B., Schaefer, U. W., and Grosse-Wilde, H. (1996).
Improved immune reconstitution after allotransplantation o f peripheral blood stem cells
instead o f bone marrow. Blood 88, 2775-9.
Pahwa, R. N., Fleischer, A., Than, S., and Good, R. A. (1994). Successful hematopoietic
reconstitution with transplantation of erythrocyte-depleted allogeneic human umbilical
221

B ib l io g r a p h y
cord blood cells in a child with leukemia. Proceedings of the National Academy o f
Sciences of the United States of America 97, 4485-8.
Pahwa, S., Pahwa, R., Incefy, G., Reece, E., Smith wick, E., O'Reilly, R., and Good, R. A.
(1979). Failure o f immunologic reconstitution in a patient with the DiGeorge syndrome
after fetal thymus transplantation. Clin Immunol Immunopathol 14, 96-106.
Park, S. Y., Saijo, K., Takahashi, T., Osawa, M., Arase, H., Hirayama, N., Miyake, K.,
Nakauchi, H., Shirasawa, T., and Saito, T. (1995). Developmental defects o f lym phoid
cells in Jak3 kinase-deficient mice. Immunity 3, 771-82.
Patel, D. D., Gooding, M. E., Parrott, R. E., Curtis, K. M., Haynes, B. P., and Buckley, R. H.
(2000). Thymic function after hematopoietic stem-cell transplantation for the treatment
o f severe combined immunodeficiency. N Engl J Med 342, 1325-32.
Paulesu, L., Bocci, V., King, A., and Loke, Y. M. (1991). Im m unocytochem ical
localization o f interferons in human trophoblast populations. J Biol Regul Homeost
Agents 5, 81-5.
Pawelec, G., Sansom, D., Rehbein, A., Adibzadeh, M., and Beckman, 1. (1996). Decreased
proliferative capacity and increased susceptibility to activation-induced cell death in late-
passage human CD4-k TCR2+ cultured T cell clones. Exp Gerontol 31, 655-68.
Penninger, J. M., and Crabtree, G. R. (1999). The actin cytoskeleton and lym phocyte
activation. Cell 96, 9-12.
Pereira, P., and Rocha, B. (1991). Post- thymic in vivo expansion of mature alpha beta T
cells. Int Immunol 3, 1077-80.
Perez-Cruz, 1., Fallen, P., Madrigal, J. A., and Cohen, S. B. (2000). Naive T cells from cord
blood have the capacity to make Types 1 and 2 cytokines. Immunol Lett 75, 85-8.
Perillo, N. L., Walford, R. L., Newman, M. A., and Effros, R. B. (1989). Human T
lymphocytes possess a limited in vitro life span. Exp Gerontol 24, 177-87.
Peschon, J. J., Morrissey, P. J., Grabstein, K. H., Ramsdell, F. J., Maraskovsky, E., Gliniak,
B. C., Park, L. S., Ziegler, S. F., Williams, D. E., Ware, C. B., and et al. (1994). Early
lymphocyte expansion is severely impaired in interleukin 7 receptor-deficient mice. J Exp
Med 180, 1955-60.
2 2 2

BffiLIOC'.RAPHY
Peters, M., Ambrus, J. L., Zheleznyak, A., Walling, D., and Hoofnagle, J. H. (1986). Effect
of interferon-alpha on immunoglobulin synthesis by human B cells. J Immunol 137,
3153-7 .
Peters, M., Walling, D, M., Kelly, K., Davis, G. L., Waggoner, J. G., and Hoofnagle, J. H.
(1986). Immunologic effects o f interferon-alpha in man: treatment with human
recombinant interferon-alpha suppresses in vitro immunoglobulin production in patients
with chronic type B hepatitis. J Immunol 137, 3147-52.
Petersdorf, E. W., Gooley, T. A., Anasetti, C., Martin, P. J., Smith, A. G., Mickelson, E. M.,
Woolfrey, A. E., and Hansen, J. A. (1998). Optimizing outcome after unrelated marrow
transplantation by comprehensive matching of HLA class 1 and 11 alleles in the donor and
recipient. Blood 92, 3515-20.
Pirenne-Ansart, H., Paillard, P., De Groote, D., Eljaafari, A., Le Gac, S., Blot, P.,
Franchimont, P., Vaquero, C., and Sterkers, G. (1995). Defective cytokine expression but
adult-type T-cell receptor, CD8, and p561ck modulation in CD3- or CD2-activated T cells
from neonates. Pediatr Res 37, 64-9.
Pittet, M. J., Speiser, D. E., Valmori, D., Cerottini, J. C., and Romero, P. (2000). Cutting
edge: cytolytic effector function in human circulating CD8+ T cells closely correlates with
CD56 surface expression. J Immunol 164, 1148-52.
Ploegh, H. L. (1998). Viral strategies of immune evasion. Science 280, 248-53.
Porter, D. L., Roth, M. S., McGarigle, C., Ferrara, J. L., and Antin, J. H. (1994). Induction
of graft-versus-host disease as immunotherapy for relapsed chronic myeloid leukemia. N
Engl J Med 330, 100-6.
Posnett, D. N., Sinha, R., Kabak, S., and Russo, C. (1994). Clonal populations o f T cells in
normal elderly humans: the T cell equivalent to "benign monoclonal gammapathy". J Exp
Med 179, 609-18.
Poulin, J. F., Viswanathan, M. N., Harris, J. M., Komanduri, K. V., Wieder, E., Ringuette,
N., Jenkins, M., McCune, J. M., and Sekaly, R. P. (1999). Direct evidence for thymic
function in adult humans. J Exp Med 190, 479-86.
Prentice, H. G., Blacklock, H. A., Janossy, G., Gilmore, M. J., Price-Jones, L., Tidman, N.,
Trejdosiewicz, L. K., Skeggs, D. B., Panjwani, D., Ball, S., and et al. (1984). Depletion o f T
lymphocytes in donor marrow prevents significant graft- versus-host disease in matched
allogeneic leukaemic marrow transplant recipients. Lancet 1, 472-6.
223

B ib l io g r a p h y
Puel, A., Ziegler, S. F., Buckley, R. H., and Leonard, W. J. (1998). Defective IL7R
expression in T(-)B(+)NK(+) severe combined immunodeficiency. Nat Genet 20, 394-7.
Querol, S., Gabarro, M., Amat, L., Gonzalez, S., Gomez, M. D., de la Calle, O., Madoz, P.,
Badell, I., and Garcia, J. (1998). The placental blood program of the Barcelona Cord
Blood Bank. Bone Marrow Transplant 22 Suppl 1, S3-5.
Rabian-Herzog, C., Lesage, S., Gluckman, E., and Charron, D. (1993). Characterization o f
lymphocyte subpopulations in cord blood. J Hematother 2, 255-7.
Raff, M. C. (1973). T and B lymphocytes and immune responses. Nature 242, 19-23.
Raghupathy, R. (1997). Thl-type immunity is incompatible with successful pregnancy.
Immunol Today 18, 478-82.
Reddy, R. K., Xia, Y., Hanikyrova, M., and Ross, G. D. (1998). A mixed population o f
immature and mature leucocytes in umbilical cord blood results in a reduced expression
and function o f CR3 (GDI lb/CD 18). Clin Exp Immunol 114, 462-7.
Reece, E. R., Gartner, J. G., Seemayer, T. A., Joncas, J. H., and Pagano, J. S. (1981).
Epstein-Barr virus in a malignant lymphoproliferative disorder o f B- cells occurring after
thymic epithelial transplantation for combined immunodeficiency. Cancer Res 41, 4 243-
7.
Reinhardt, R. L., Khoruts, A., Merica, R., Zell, T., and Jenkins, M. K. (2001). Visualizing
the generation o f memory CD4 T cells in the whole body. Nature 410, 101-5.
Rengarajan, J., Szabo, S. J., and Glimcher, L. H. (2000). Transcriptional regulation o f
T hl/Th2 polarization. Immunol Today 21, 479-83.
Res, P., Martinez-Caceres, E., Cristina Jaleco, A., Staal, F., Noteboom, E., Weijer, K., and
Spits, H. (1996). CD34+CD38dim cells in the human thymus can differentiate into T,
natural killer, and dendritic cells but are distinct from pluripotent stem cells. Blood 87,
5 1 9 6 -2 0 6 .
Reusser, P., Fisher, L. D., Buckner, C. D., Thomas, E. D., and Meyers, J. D. (1990).
Cytomegalovirus infection after autologous bone marrow transplantation: occurrence o f
cytomegalovirus disease and effect on engraftment. Blood 75, 1888-94.
224

B œ u o c '.R A JW
Revoltella, R. P., Laricchia-Robbio, L., Moscato, S., Genua, A., and Liberati, A. M. (1997).
Natural and therapy-induced anti-GM-CSF and anti-G-CSF antibodies in human serum.
Leuk Lymphoma 26 Suppl 1, 29-34.
Richards, S. J., Jones, R. A., Roberts, B. E., Patel, D., and Scott, C. S. (1990). Relationships
between 2H4 (CD45RA) and UCHLl (CD45RO) expression by normal blood CD4-I-CD8-,
CD4-CD8+, CD4-CD8dim-i-, CD3+CD4-CD8- and CD3-CD4- CD8- lymphocytes. Clin
Exp Immunol 81, 149-55.
Richter, A., Lohning, M., and Radbruch, A. (1999). Instruction for cytokine expression in
T helper lymphocytes in relation to proliferation and cell cycle progression. J Exp Med
190, 1439-50.
Riechmann, L., Clark, M., Waldmann, H., and Winter, G. (1988). Reshaping human
antibodies for therapy. Nature 332, 323-7.
Ringden, O., Groth, C. G., Erikson, A., Granqvist, S., Mansson, J. E., and Sparrelid, E.
(1995). Ten years' experience of bone marrow transplantation for Gaucher disease.
Transplantation 59, 864-70.
Risdon, G., Gaddy, J., Horie, M., and Broxmeyer, H. E. (1995). Alloantigen priming
induces a state o f unresponsiveness in human umbilical cord blood T cells. Proc Natl
Acad Sci U S A 92, 2413-7.
Risdon, G., Gaddy, J., Stehman, F. B., and Broxmeyer, H. E. (1994). Proliferative and
cytotoxic responses of human cord blood T lymphocytes following allogeneic
stimulation. Cell Immunol 154, 14-24.
Ritter, M., and Crispe, I. (1992). The Thymus (Oxford, UK: IRL Press).
Rocha, B., Dautigny, N., and Pereira, P. (1989). Peripheral T lymphocytes: expansion
potential and homeostatic regulation of pool sizes and CD4/CD8 ratios in vivo. Eur J
Immunol 19, 905-11.
Rocha, V., Cornish, J., Sievers, E. L., Filipovich, A., Locatelli, F., Peters, C., Remberger, M.,
Michel, G., Arcese, W., Dallorso, S., Tiedemann, K., Busca, A., Chan, K. W., Kato, S.,
Ortega, J., Vowels, M., Zander, A., Souillet, G., Oakill, A., Woolfrey, A., Pay, A. L., Green,
A., Gamier, F., lonescu. I., Wemet, P., Sirchia, G., Rubinstein, P., Chevret, S., and
Gluckman, E. (2001). Comparison of outcomes o f unrelated bone marrow and umbilical
cord blood transplants in children with acute leukemia. Blood 97, 2962-71.
225

B ib l io g r a p h y
Rodig, S. J., Meraz, M. A., White, J. M., Lampe, P. A., Riley, J. K., Arthur, C. D., King, K.
L., Sheehan, K, C., Yin, L,, Pennica, D., Johnson, E. M., Jr., and Schreiber, R. D. (1998).
Disruption of the Jakl gene demonstrates obligatory and nonredundant roles o f the Jaks
in cytokine-induced biologic responses. Cell 93, 373-83.
Romagnani, S. (1994). Lymphokine production by human T cells in disease states. Annu
Rev Immunol 12, 227-57.
Roos, T., Martin, T. R., Ruzinski, J. T., Leturcq, D. J., Hillier, S. L., Patton, D. L., and
Eschenbach, D. A. (1997). Lipopoly saccharide binding protein and soluble CD 14
receptor protein in amniotic fluid and cord blood in patients at term. Am J Obstet
Gynecol 177, 1230-7.
Roth, D. B., Menetski, J. P., Nakajima, P. B., Bosma, M. J., and Gellert, M. (1992). V(D)J
recombination: broken DNA molecules with covalently sealed (hairpin) coding ends in
scid mouse thymocytes. Cell 70, 983-91.
Roth, D. B., Nakajima, P. B., Menetski, J. P., Bosma, M. J., and Gellert, M. (1992). V(D)J
recombination in mouse thymocytes: double-strand breaks near T cell receptor delta
rearrangement signals. Cell 69, 41-53.
Roth stein, D. M., Sohen, S., Daley, J. P., Schlossman, S. P., and Morimoto, C. (1990).
CD4+CD45RA+ and CD4+CD45RA- T cell subsets in man maintain distinct function and
CD45RA expression persists on a subpopulation o f CD45RA+ cells after activation with
Con A. Cell Immunol 129, 449-67.
Roux, E., Dumont-Girard, P., Starobinski, M., Siegrist, C. A., Helg, C., Chapuis, B., and
Roosnek, E. (2000). Recovery of immune reactivity after T-cell-depleted bone marrow
transplantation depends on thymic activity. Blood 96, 2299-303.
Rubinstein, P., Carrier, C., Scaradavou, A., Kurtzberg, J., Adamson, J., Migliaccio, A. R.,
Berkowitz, R. L., Cabbad, M., Dobrila, N. L., Taylor, P. E., Rosenfield, R. E., and Stevens,
C. E. (1998). Outcomes among 562 recipients of placental-blood transplants from
unrelated donors. N Engl J Med 339, 1565-77.
Rubinstein, P., Rosenfield, R. E., Adamson, J. W., and Stevens, C. E. (1993). Stored
placental blood for unrelated bone marrow reconstitution. Blood 81, 1679-90.
Russell, S. M., Tayebi, N., Nakajima, H., Riedy, M. C., Roberts, J. L., Aman, M. J., M igone,
T. S., Noguchi, M., Markert, M. L., Buckley, R. H., and et al. (1995). Mutation o f Jak3 in
226

BmUOÜRAPHY
a patient with SCID; essential role of Jak3 in lymphoid development. Science 270, 797-
800.
Russwurm, G. P., Mackler, A. M., Fagoaga, O. R., Brown, W. S., 3rd, Sakala, E. P., Yellon,
S. M., and Nehlsen-Cannarella, S. L. (1997). Soluble human leukocyte antigens,
interleukin-6, and interferon-gamma during pregnancy. Am J Reprod Immunol 38, 256-
62.
Sadat-Sowti, B., Debre, P., Idziorek, T., Guillon, J. M., Hadida, P., Okzenhendler, E.,
Katlama, C., Mayaud, C., and Autran, B. (1991). A lectin-binding soluble factor released
by CD8-I-CD57-I- lymphocytes from AIDS patients inhibits T cell cytotoxicity. Eur J
Immunol 21, 737-41.
Saito, S., Morii, T., Umekage, H., Makita, K., Nishikawa, K., Narita, N., Ichijo, M.,
Morikawa, H., Ishii, N., Nakamura, M., and Sugamura, K. (1996). Expression o f the
interleukin-2 receptor gamma chain on cord blood mononuclear cells. Blood 87, 3344-
50.
Sakurai, T., Yamada, M., Simamura, S., and Motoyoshi, K. (1996). Recombinant human
macrophage-colony stimulating factor suppresses the mouse mixed lymphocyte reaction.
Cell Immunol 171, 87-94.
Salafia, C. M., Sherer, D. M., Spong, C. Y., Lencki, S., Eglinton, G. S., Parkash, V., Marley,
E., and Lage, J. M. (1997). Fetal but not maternal serum cytokine levels correlate with
histologic acute placental inflammation. Am J Perinatol 14, 419-22.
Sallusto, P., Lenig, D., Forster, R., Lipp, M., and Lanzavecchia, A. (1999). Two subsets o f
memory T lymphocytes with distinct homing potentials and effector functions. Nature
401, 708-12.
Salomon, B., and Bluestone, J. A. (2001). Complexities of CD28/B7: CTLA-4
costimulatory pathways in autoimmunity and transplantation. Annu Rev Immunol 19,
225-52 .
Sandberg, J. K., Fast, N. M., and Nixon, D. F. (2001). Functional heterogeneity o f
cytokines and cytolytic effector molecules in human CD8+ T lymphocytes. J Immunol
167, 181-7.
Sano, S., Takahama, Y., Sugawara, T., Kosaka, H., Itami, S., Yoshikawa, K., Miyazaki, J.,
van Ewijk, W., and Takeda, J. (2001). Stat3 in thymic epithelial cells is essential for
227

BIBLIÜC'iRAPHY
postnatal maintenance o f thymie architecture and thymocyte survival. Immunity 15, 261-
73.
Sanz, G. F., Saavedra, S., Flanelles, D., Senent, L., Cervera, J., Barragan, E., Jimenez, C.,
Larrea, L., Martin, G., Martinez, J., Jarque, L, Moscardo, P., Plume, G., Andreu, R.,
Regadera, A. L, Garcia, L, Molla, S., Solves, P., de La Rubia, J., Bolufer, P., Benlloch, L.,
Soler, M. A., Marty, M. L., and Sanz, M. A. (2001). Standardized, unrelated donor cord
blood transplantation in adults with hematologic malignancies. Blood 98, 2332-8.
Sautois, B., Fillet, G., and Beguin, Y. (1997). Comparative cytokine production by in vitro
stimulated mononucleated cells from cord blood and adult blood. Exp Hematol 25, 103-
Schlissel, M., Constantinescu, A., Morrow, T., Baxter, M., and Peng, A. (1993). D ouble
strand signal sequence breaks in V(D)J recombination are blunt, 5'-phosphorylated, RAG-
dependent, and cell cycle regulated. Genes Dev 7, 2520-32.
Schmitt, C., Ktorza, S., Sarun, S., Blanc, C., De Jong, R., and Debre, P. (1993). CD34-
expressing human thymocyte precursors proliferate in response to interleukin-7 but have
lost myeloid differentiation potential. Blood 82, 3675-85.
Schwartz, R. H. (1990). A cell culture model for T lymphocyte clonal anergy. Science
248, 1349-56.
Schwarz, K., Gauss, G. H., Ludwig, L., Pannicke, U., Li, Z., Lindner, D., Friedrich, W.,
Seger, R. A., Hansen-Hagge, T. E., Desiderio, S., Lieber, M. R., and Bartram, C. R. (1996).
RAG mutations in human B cell-negative SCID. Science 274, 97-9.
Scollay, R. G., Butcher, E. C., and Weissman, I. L. (1980). Thymus cell migration.
Quantitative aspects of cellular traffic from the thymus to the periphery in mice. Eur J
Immunol 10, 210-8.
Scott, I., O'Shea, J., Bunce, M., Tiercy, J. M., Arguello, J. R., Firman, H., Goldman, J.,
Prentice, H. G., Little, A. M., and Madrigal, J. A. (1998). Molecular typing shows a high
level o f HLA class I incompatibility in serologically well matched donor/patient pairs:
implications for unrelated bone marrow donor selection. Blood 92, 4864-71.
Seddon, B., Legname, G., Tomlinson, P., and Zamoyska, R. (2000). Long-term survival
but impaired homeostatic proliferation of Naive T cells in the absence of p561ck. Science
290, 127-31.
228

BmUCK'iRAPHY
Seino, Y., Ishida, M., Yamaoka, K., Ishii, T., Hiejima, T., Ikehara, C., Tanaka, Y., Matsuda,
S., Shimotsuji, T., Yabuuchi, H., Morimoto, S., and Onishi, T. (1982). Serum calcium
regulating hormones in the perinatal period. Calcif Tissue Int 34, 131-5.
Sfikakis, P. P., Kostomitsopoulos, N., Kittas, C., Stathopoulos, J., Karayannacos, P., Dellia-
Sfikakis, A., and Mitropoulos, D. (1998). Tamoxifen exerts testosterone-dependent and
independent effects on thymic involution. Int J Immunopharmacol 20, 305-12.
Shahinian, A., Pfeffer, K., Lee, K. P., Kundig, T. M., Kishihara, K., Wakeham, A., Kawai,
K., Ohashi, P. S., Thompson, C. B., and Mak, T. W. (1993). Differential T cell
costimulatory requirements in CD28-deficient mice. Science 261, 609-12.
Shaw, A. S., and Dustin, M. L. (1997). Making the T cell receptor go the distance: a
topological view of T cell activation. Immunity 6, 361-9.
Sher, A., and Coffman, R. L. (1992). Regulation of immunity to parasites by T cells and T
cell-derived cytokines. Annu Rev Immunol 10, 385-409.
Sher, A., Fiorentino, D., Caspar, P., Pearce, E., and Mosmann, T. (1991). Production of IL-
10 by CD4+ T lymphocytes correlates with down- regulation of Thl cytokine synthesis in
helminth infection. J Immunol 147, 2713-6.
Sher, A., Oswald, I. P., Hieny, S., and Gazzinelli, R. T. (1993). Toxoplasma gondii induces
a T-independent IFN-gamma response in natural killer cells that requires both adherent
accessory cells and tumor necrosis factor-alpha. J Immunol 150, 3982-9.
Shinkai, Y., Koyasu, S., Nakayama, K., Murphy, K. M., Loh, D. Y., Reinherz, E. L., and
Alt, F. W. (1993). Restoration o f T cell development in RAG-2-deficient mice by
functional TCR transgenes. Science 259, 822-5.
Shores, E. W., Nakayama, T., Wiest, D. L., Takahama, Y., Sharrow, S., and Singer, A.
(1993). Structurally distinct T cell receptor complexes on developmentally distinct T cell
populations in severe combined immunodeficiency mice expressing a TCR beta
transgene. J Immunol 150, 1263-75.
Singer, C. R., Tansey, P. J., and Burnett, A. K. (1983). T lymphocyte reconstitution
following autologous bone marrow transplantation. Clin Exp Immunol 51, 455-60.
Small, T. N., Avigan, D., Dupont, B., Smith, K., Black, P., Heller, G., Polyak, T., and
O'Reilly, R. J. (1997). Immune reconstitution following T-cell depleted bone marrow
229

BEBLKXj RAPHY
transplantation: effect of age and posttransplant graft rejection prophylaxis. Biol Blood
Marrow Transplant 3, 65-75.
Small, T. N., Papadopoulos, E. B., Boulad, F., Black, P., Castro-Malaspina, H., Childs, B.
H., Collins, N., Gillio, A., George, D., Jakubowski, A., Heller, G., Fazzari, M., Keman, N.,
MacKinnon, S., Szabolcs, P., Young, J. W., and O'Reilly, R. J. (1999). Comparison o f
immune reconstitution after unrelated and related T-cell- depleted bone marrow
transplantation: effect of patient age and donor leukocyte infusions. Blood 93, 467-80.
Smith, S. R., Terminelli, C., Kenworthy-Bott, L., and Phillips, D. L. (1991). A study o f
cytokine production in acute graft-vs-host disease. Cell Immunol 134, 336-48.
Snyder, D. S., Chao, N. J., Amy Ion, M. D., Taguchi, J., Long, G. D., Negrin, R. S.,
Nademanee, A. P., O'Donnell, M. R., Schmidt, G. M., Stein, A. S., and et al. (1993).
Fractionated total body irradiation and high-dose etoposide as a preparatory regimen for
bone marrow transplantation for 99 patients with acute leukemia in first complete
remission. Blood 82, 2920-8.
Soares, M. V., Borthwick, N. J., Maini, M. K., Janossy, G., Salmon, M., and Akbar, A. N.
(1998). IL-7-dependent extrathymic expansion o f CD45RA4- T cells enables preservation
of a naive repertoire. J Immunol 161, 5909-17.
Soudais, C., de Villartay, J. P., Le Deist, F., Fischer, A., and Lisowska-Grospierre, B.
(1993). Independent mutations of the human CD3-epsilon gene resulting in a T cell
receptor/CD3 complex immunodeficiency. Nat Genet 3, 77-81.
Sperling, A. I., Auger, J. A., Fhst, B. D., Rulifson, I. C., Thompson, C. B., and Bluestone, J.
A. (1996). CD28/B7 interactions deliver a unique signal to naive T cells that regulates cell
survival but not early proliferation. J Immunol 157, 3909-17.
Spits, H. (1994). Early stages in human and mouse T-cell development. Curr Opin
Immunol 6, 212-21.
Sprent, J., Schaefer, M., Hurd, M., Surh, C. D., and Ron, Y. (1991). Mature murine B and
T cells transferred to SCID mice can survive indefinitely and many maintain a virgin
phenotype. J Exp Med 174, 717-28.
Sprent, J., and Tough, D. F. (1994). Lymphocyte life-span and memory. Science 265,
1395-400 .
230

B ib l io g r a p h y
Springer, T. A. (1994). Traffic signals for lymphocyte recirculation and leukocyte
emigration: the multistep paradigm. Cell 76, 301-14.
Stanley, E. R., Berg, K. L., Einstein, D. B., Lee, P. S., Pixley, F. J., Wang, Y., and Yeung, Y.
G. (1997). Biology and action of colony—stimulating factor-1. Mol Reprod D ev 46, 4-10.
Steinman, R. M. (1991). The dendritic cell system and its role in immunogenicity. Annu
Rev Immunol 9, 271-96.
Steinmann, G. G., Klaus, B., and Muller-Hermelink, H. K. (1985). The involution of the
ageing human thymic epithelium is independent of puberty. A morphometric study.
Scand J Immunol 22, 563-75.
Storek, J., Dawson, M. A., Storer, B., Stevens-Ayers, T., Maloney, D. G., Marr, K. A.,
Witherspoon, R. P., Bensinger, W., Flowers, M. E., Martin, P., Storb, R., Appelbaum, F. R.,
and Boeckh, M. (2001). Immune reconstitution after allogeneic marrow transplantation
compared with blood stem cell transplantation. Blood 97, 3380-9.
Storek, J., Espino, G., Dawson, M. A., Storer, B., Flowers, M. E., and Maloney, D. G.
(2000). Low B-cell and monocyte counts on day 80 are associated with high infection
rates between days 100 and 365 after allogeneic marrow transplantation. Blood 96, 3290-
3.
Storek, J., Gooley, T., Witherspoon, R. P., Sullivan, K. M., and Storb, R. (1997). Infectious
morbidity in long-term survivors o f allogeneic marrow transplantation is associated with
low CD4 T cell counts. Am J Hematol 54, 131-8.
Storek, J., Joseph, A., Espino, G., Dawson, M. A., Douek, D. C., Sullivan, K. M., Flowers,
M. E., Martin, P., Mathioudakis, G., Nash, R. A., Storb, R., Appelbaum, F. R., and
Maloney, D. G. (2001). Immunity of patients surviving 20 to 30 years after allogeneic or
syngeneic bone marrow transplantation. Blood 98, 3505-12.
Storek, J., Witherspoon, R. P., and Storb, R. (1995). T cell reconstitution after bone
marrow transplantation into adult patients does not resemble T cell development in early
life. Bone Marrow Transplant 16, 413-25.
Sullivan, K. M., Deeg, H. J., Sanders, J., Klosterman, A., Amos, D., Shulman, H., Sale, G.,
Martin, P., Witherspoon, R., Appelbaum, P., and et al. (1986). Hyperacute graft-v-host
disease in patients not given immunosuppression after allogeneic marrow transplantation.
Blood 67, 1172-5.
231

B h îl io g r a p h y
Sulovic, V., Siljak, B., and Sinadinovic, J. (1984). Senim T4, T3, r-T3, TSH and Tg levels
in cord blood and maternal circulation at the time of delivery. Exp Clin Endocrinol 83,
256-62 .
Swain, S. L., Hu, H., and Huston, G. (1999). Class Il-independent generation of CD4
memory T cells from effectors. Science 286, 1381-3.
Sykes, M., Abraham, V. S., Harty, M. W., and Pearson, D. A. (1993). IL-2 reduces graft-
versus-host disease and preserves a graft-versus- leukemia effect by selectively inhibiting
CD4+ T cell activity. J Immunol 150, 197-205.
Sykes, M., Szot, G. L., Nguyen, P. L., and Pearson, D. A. (1995). Interleukin-12 inhibits
murine graft-versus-host disease. Blood 86, 2429-38.
Szebeni, J., Wang, M. G., Pearson, D. A., Szot, G. L., and Sykes, M. (1994). IL-2 inhibits
early increases in serum gamma interferon levels associated with graft-versus-host-disease.
Transplantation 58, 1385-93.
Szondy, Z. (1997). Methylprednisolone and 2-chloroadenosine induce DNA
fragmentation at different stages o f human T-lymphocyte development. Immunol Lett 58,
59-65 .
Takeshita, S., Toda, M., and Yamagishi, H. (1989). Excision products o f the T cell
receptor gene support a progressive rearrangement model o f the alpha/delta locus. Embo
J 8, 3261-70.
Talvensaari, K., Clave, E., Douay, C., Rabian, C., Garderet, L., Busson, M., Gamier, P.,
Douek, D., Gluckman, E., Charron, D., and Toubert, A. (2002). A broad T-cell repertoire
diversity and an efficient thymic function indicate a favorable long-term immune
reconstitution after cord blood stem cell transplantation. Blood 99, 1458-1464.
Tamura, H., Dong, H., Zhu, G., Sica, G. L., Flies, D. B., Tamada, K., and Chen, L. (2001).
B7-H1 costimulation preferentially enhances CD28-independent T-helper cell function.
Blood 97, 1809-16.
Tan, J. T., Dudl, E., LeRoy, E., Murray, R., Sprent, J., Weinberg, K. I., and Surh, C. D.
(2001). IL-7 is critical for homeostatic proliferation and survival of naive T cells. Proc
Natl Acad Sci U S A 98, 8732-7.
232

BIBLIOGRAI’HY
Tanchot, C., Le Campion, A., Leaument, S., Dautigny, N., and Lucas, B. (2001). Naive
CD4(+) lymphocytes convert to anergic or memory-like cells in T cell-deprived
recipients. Eur J Immunol 31, 2256-65.
Tanchot, C., Lemonnier, F. A., Peramau, B., Freitas, A. A., and Rocha, B. (1997).
Differential requirements for survival and proliferation o f CDS naive or memory T cells
[see comments]. Science 276, 2057-62.
Tanchot, C., and Rocha, B. (1995). The peripheral T cell repertoire: independent
homeostatic regulation o f virgin and activated CD84- T cell pools. Eur J Immunol 25,
2 127-36 .
Tanchot, C., Rosado, M. M., Agenes, P., Freitas, A. A., and Rocha, B. (1997). Lym phocyte
homeostasis. Semin Immunol 9, 331-7.
Taylor, P. A., Lees, C. J., Waldmann, H., Noelle, R. J., and Blazar, B. R. (2001).
Requirements for the promotion of allogeneic engraftment by anti-CD 154 (anti-CD40L)
monoclonal antibody under nonmyeloablative conditions. Blood 98, 467-74.
Taylor, S., and Bryson, Y. J. (1985). Impaired production o f gamma-interferon by
newborn cells in vitro is due to a functionally immature macrophage. J Immunol 134,
1493-7.
Terstappen, L. W., Huang, S., Safford, M., Lansdorp, P. M., and Loken, M. R. (1991).
Sequential generations o f hematopoietic colonies derived from single nonlineage-
committed CD34+CD38- progenitor cells. Blood 77, 1218-27.
Thomas, E., Lochte, H., Cannon, J., Sahler, O., and Ferrebee, J. (1959). Supra-lethal whole
body irradiation and isologous marrow transplantation in man. J Clin Invest 38, 1709.
Thomas, E., Storb, R., Clift, R. A., Fefer, A., Johnson, F. L., Neiman, P. E., Lemer, K. G.,
Glucksberg, H., and Buckner, C. D. (1975). Bone-marrow transplantation (first o f two
parts). N Engl J Med 292, 832-43.
Thomas, E. D., Storb, R., Clift, R. A., Fefer, A., Johnson, L., Neiman, P. E., Lemer, K. G.,
Glucksberg, H., and Buckner, C. D. (1975). Bone-marrow transplantation (second o f two
parts). N Engl J Med 292, 895-902.
Thomis, D. C., Gumiak, C. B., Tivol, E., Sharpe, A. H., and Berg, L. J. (1995). Defects in B
lymphocyte maturation and T lymphocyte activation in mice lacking Jak3. Science 270,
794-7 .
233

B m u œ R A P H Y
Thomis, D. C., Marktel, S., Bonini, C., Traversari, C., Gilman, M., Bordignon, C., and
Clackson, T. (2001). A Fas-based suicide switch in human T cells for the treatment o f
graft- versus-host disease. Blood 97, 1249-57.
Thompson, C. B., Lindsten, T., Ledbetter, J. A., Kunkel, S. L., Young, H. A., Emerson, S.
G., Leiden, J. M., and June, C. H. (1989). CD28 activation pathway regulates the
production of multiple T-cell- derived lymphokines/cytokines. Proc Natl Acad Sci U S A
86, 1333-7.
Tiberghien, P., Cahn, J. Y., Brion, A., Deconinck, E., Racadot, E., Herve, P., Milpied, N.,
Lioure, B., Gluckman, E., Bordigoni, P., Jacob, W., Chiang, Y., Marcus, S., Reynolds, C.,
and Longo, D. (1997). Use of donor T-lymphocytes expressing herpes-simplex
thymidine kinase in allogeneic bone marrow transplantation: a phase I-II study. Hum
Gene Ther 8, 615-24.
Timm, J. A., and Thoman, M. L. (1999). Maturation of CD4+ lymphocytes in the aged
microenvironment results in a memory-enriched population. J Immunol 162, 711-7.
Tomlinson, M. G., Lin, J., and Weiss, A. (2000). Lymphocytes with a complex: adapter
proteins in antigen receptor signaling. Immunol Today 21, 584-91.
Tough, D. P., and Sprent, J. (1994). Turnover o f naive- and memory-phenotype T cells, J
Exp Med 179, 1127-35.
Troutt, A. B., and Kelso, A. (1993). Lymphokine synthesis in vivo in an acute murine
graft-versus-host reaction: mRNA and protein measurements in vivo and in vitro reveal
marked differences between actual and potential lymphokine production levels. Int
Immunol 5, 399-407.
Truitt, R. L., and Atasoylu, A. A. (1991). Contribution o f CD4+ and CD8+ T cells to
graft-versus-host disease and graft-versus-leukemia reactivity after transplantation o f
MHC- compatible bone marrow. Bone Marrow Transplant 8, 51-8.
Tsakonas, D. P., Nicolaides, K. H., Tsakona, C. P., Worman, C. P., and Goldstone, A. H.
(1995). Changes in maternal plasma macrophage-colony stimulating factor levels during
normal pregnancy. Clin Lab Haematol 17, 57-9.
Tucci, A., Mouzaki, A., James, H., Bonnefoy, J. Y., and Zubler, R. H. (1991). Are cord
blood B cells functionally mature? Clin Exp Immunol 84, 389-94.
234

BffiUOGRAPHY
Turke, P. W. (1997). Thymic involution, Immunol Today 18, 407.
Uckan, D., Steele, A., Cherry, Wang, B. Y., Chamizo, W., Koutsonikolis, A., Gilbert-
Bamess, E., and Good, R. A. (1997). Trophoblasts express Fas ligand: a proposed
mechanism for immune privilege in placenta and maternal invasion. Mol Hum Reprod 3,
655-62 .
Unanue, E. R. (1984). Antigen-presenting function o f the macrophage. Annu Rev
Immunol 2, 395-428.
Urbano-Ispizua, A., Carreras, E., Marin, P., Rovira, M., Martinez, C., Fernandez-Aviles, F.,
Xicoy, B., Hemandez-Boluda, J. C., and Montserrat, E. (2001). Allogeneic transplantation
o f CD34(+) selected cells from peripheral blood from human leukocyte antigen-identical
siblings: detrimental effect of a high number o f donor CD34(-h) cells? Blood 98, 2352-7.
Urbano-Ispizua, A., Rozman, C., Pimentel, P., Solano, C., de la Rubia, J., Brunet, S., Perez-
Oteiza, J., Ferra, C., Zuazu, J., Caballero, D., Carvalhais, A., Diez, J. L., Espigado, I.,
Martinez, C., Campilho, F., Sanz, M. A., Sierra, J., Garcia-Conde, J., and Montserrat, E.
(2001). The number of donor CD3(+) cells is the most important factor for graft failure
after allogeneic transplantation of CD34(+) selected cells from peripheral blood from
HLA-identical siblings. Blood 97, 383-7.
Vacchio, M. S., and Ashwell, J. D. (1997). Thymus-derived glucocorticoids regulate
antigen-specific positive selection. J Exp Med 185, 2033-8.
Valitutti, S., Muller, S., Celia, M., Padovan, E., and Lanzavecchia, A. (1995). Serial
triggering of many T-cell receptors by a few peptide-MHC complexes. Nature 375, 148-
51.
van den Brink, M. R., Moore, E., Ferrara, J. L., and Burakoff, S. J. (2000). Graft-versus-
host-disease-associated thymic damage results in the appearance o f T cell clones with anti
host reactivity. Transplantation 69, 446-9.
van Ewijk, W., Hollander, G., Terhorst, C., and Wang, B. (2000). Stepwise development o f
thymic microenvironments in vivo is regulated by thymocyte subsets. Development 127,
1583-91 .
Van Laethem, F., Bans, E., Smyth, L. A., Andris, P., Bex, F., Urbain, J., Kioussis, D., and
Leo, O. (2001). Glucocorticoids attenuate T cell receptor signaling. J Exp Med 193, 803-
14.
235

B ib l io g r a p h y
Van Parijs, L., and Abbas, A. K. (1998). Homeostasis and self-tolerance in the immune
system; turning lymphocytes off. Science 280, 243-8.
Van Parijs, L., Ibraghimov, A., and Abbas, A. K. (1996). The roles of costimulation and
Fas in T cell apoptosis and peripheral tolerance. Immunity 4, 321-8.
Van Parijs, L., Peterson, D. A., and Abbas, A. K. (1998). The Fas/Fas ligand pathway and
Bcl-2 regulate T cell responses to model self and foreign antigens. Immunity 8, 265-74.
van Stipdonk, M. J., Lemmens, E. E., and Schoenberger, S. P. (2001). Naive CTLs require
a single brief period of antigenic stimulation for clonal expansion and differentiation. Nat
Immunol 2, 423-9.
Vander Woude, A. B. B. (1997). Immunosuppression and Immunophillin Ligands:
Cyclosporin , FK506 and Rapamycin. In Graft-vs.-Host Disease, J. D. Ferrara, HJ;
Burakoff, SJ, ed. (New York: Marcel Dekker, Inc.), pp. 111-150.
Vaziri, H., Dragowska, W., Allsopp, R. C., Thomas, T. E., Harley, C. B., and Lansdorp, P.
M. (1994). Evidence for a mitotic clock in human hematopoietic stem cells: loss o f
telomeric DNA with age. Proc Natl Acad Sci U S A 97, 9857-60.
Vella, A., Teague, T. K., Ihle, J., Kappler, J., and Marrack, P. (1997). Interleukin 4 (IL -4)
or IL-7 prevents the death of resting T cells: stat6 is probably not required for the effect
o f IL-4. J Exp Med 186, 325-30.
Vella, A. T., McCormack, J. E., Linsley, P. S., Kappler, J. W., and Marrack, P. (1995).
Lipopoly saccharide interferes with the induction of peripheral T cell death. Immunity 2,
261-70 .
Verschuren, M. C., Wolvers-Tettero, I. L., Breit, T. M., Noordzij, J., van Wering, E. R., and
van Dongen, J. J. (1997). Preferential rearrangements of the T cell receptor-delta-deleting
elements in human T cells. J Immunol 158, 1208-16.
Via, C. S. (1991). Kinetics of T cell activation in acute and chronic forms o f murine graft-
versus-host disease. J Immunol 146, 2603-9.
Via, C. S., Rus, V., Gately, M. K., and Finkelman, F. D. (1994). IL-12 stimulates the
development of acute graft-versus-host disease in mice that normally would develop
chronic, autoimmune graft-versus-host disease. J Immunol 153, 4040-7.
236

B iblkxt.r a p h y
Viola, A., and Lanzavecchia, A. (1996). T cell activation determined by T cell receptor
number and tunable thresholds. Science 273, 104-6.
Viola, A., Schroeder, S., Sakakibara, Y., and Lanzavecchia, A. (1999). T lymphocyte
costimulation mediated by reorganization o f membrane microdomains. Science 283, 680-
2 .
Viret, C., Wong, F. S., and Jane way, C. A., Jr. (1999). Designing and maintaining the
mature TCR repertoire: the continuum of self-peptide:self-MHC complex recognition.
Immunity 10, 559-68.
Volkmann, A., Zal, T., and Stockinger, B. (1997). Antigen-presenting cells in the thymus
that can negatively select MHC class Il-restricted T cells recognizing a circulating self
antigen. J Immunol 158, 693-706.
von Andrian, U. H., Chambers, J. D., McEvoy, L. M., Bargatze, R. P., Arfors, K. E., and
Butcher, E. C. (1991). Two-step model of leukocyte-endothelial cell interaction in
inflammation: distinct roles for EEC A M -1 and the leukocyte beta 2 integrins in vivo. Proc
Natl Acad Sci U S A 88, 7538-42.
von Andrian, U. H., and Mackay, C. R. (2000). T-cell function and migration. Two sides
of the same coin. N Engl J Med 343, 1020-34.
von Boehmer, H., and Fehling, H. J. (1997). Structure and function of the pre-T cell
receptor. Annu Rev Immunol 15, 433-52.
von Boehmer, H., and Hafen, K. (1993). The life span of naive alpha/beta T cells in
secondary lymphoid organs. J Exp Med 177, 891-6.
von Freeden-Jeffry, U., Vieira, P., Lucian, L. A., McNeil, T., Burdach, S. E., and Murray,
R. (1995). Lymphopenia in interleukin (IL)-7 gene-deleted mice identifies IL-7 as a
nonredundant cytokine. J Exp Med 181, 1519-26.
Wagner, J., Rosenthal, J., Sweetman, R., Shu, X., Davies, S., Ramsay, N., McGlave, P.,
Sender, L., and Cairo, M. (1996). Successful transplantation of HLA-matched and HLA-
mismatched umbilical cord blood from unrelated donors: analysis o f engraftment and
acute graft-versus-host disease. Blood 88, 795-802.
Wagner, J. E., Keman, N. A., Steinbuch, M., Broxmeyer, H. E., and Gluckman, E. (1995).
Allogenic sibling umbilical-cord-blood transplantation in children with malignant and
non-malignant disease. Lancet 343, 214-219.
237

BlBLICXiRAPHY
Wallace, D, L., and Beverley, P. C. (1990). Phenotypic changes associated with activation
of CD45RA+ and CD45RO+ T cells. Immunology 69, 460-7.
Wang, J., and Klein, J. R. (1994). Thymus-neuroendocrine interactions in extrathymic T
cell development. Science 265, 1860-2.
Wang, M., Stepkowski, S. M., Wang, M. E., Tian, L., Qu, X., Tu, Y., He, G., and Kahan, B.
D. (1996). Induction of specific allograft immunity by soluble class I MHC heavy chain
protein produced in a baculovirus expression system. Transplantation 61, 448-57.
Ward, S. G., and Cantrell, D. A. (2001). Phosphoinositide 3-kinases in T lym phocyte
activation. Curr Opin Immunol 13, 332-8.
Warren, E. H., Gavin, M., Greenberg, P. D., and Riddell, S. R. (1998). Minor
histocompatibility antigens as targets for T-cell therapy after bone marrow
transplantation. Curr Opin Hematol 5, 429-33.
Warwick, R. B., JA. (2000). Reducing the risks of disease transmission in cord blood
transplantation. In Cord Blood Characteristics: Role in Stem Cell Transplantation, S.
Cohen, ed. (London: Martin Dunitz), pp. 149-168.
Webb, L. M., Foxwell, B. M., and Feldmann, M. (1999). Putative role for interleukin-7 in
the maintenance o f the recirculating naive CD4+ T-cell pool. Immunology 98, 400-5.
Wegmann, T. G., Lin, H., Guilbert, L., and Mosmann, T. R. (1993). Bidirectional cytokine
interactions in the maternal-fetal relationship: is successful pregnancy a TH2
phenomenon? Immunol Today 14, 353-6.
Weiden, P. L., Flournoy, N., Thomas, F. D., Prentice, R., Fefer, A., Buckner, C. D., and
Storb, R. (1979). Antileukemic effect of graft-versus-host disease in human recipients o f
allogeneic-marrow grafts. N Engl J Med 300, 1068-73.
Weiden, P. L., Sullivan, K. M., Flournoy, N., Storb, R., and Thomas, F. D. (1981).
Antileukemic effect o f chronic graft-versus-host disease: contribution to improved
survival after allogeneic marrow transplantation. N Engl J Med 304, 1529-33.
Weinberg, K., Annett, G., Kashyap, A., Lenarsky, C., Forman, S. J., and Parkman, R.
(1995). The effect of thymic function on immunocompetence following bone marrow
transplantation. Biol Blood Marrow Transplant 1, 18-23.
238

B ib l io g r a p h y
Weinberg, K., Blazar, B. R,, Wagner, J. E., Agura, E., Hill, B. J., Smogorzewska, M., Koup,
R. A., Betts, M. R., Collins, R. H., and Douek, D. C. (2001). Factors affecting thymic
function after allogeneic hematopoietic stem cell transplantation. Blood 97, 1458-66.
Weiss, L., Weigensberg, M., Morecki, S., Bar, S., Cobbold, S., Waldmann, H., and Slavin, S.
(1990). Characterization of effector cells o f graft vs leukemia following allogeneic bone
marrow transplantation in mice inoculated with murine B- cell leukemia. Cancer Immunol
Immunother 31, 236-42.
Weissman, I. L. (2000). Translating stem and progenitor cell biology to the clinic: barriers
and opportunities. Science 287, 1442-6.
Wekerle, T., Kurtz, J., Ito, H., Ronquillo, J. V., Dong, V., Zhao, G., Shaffer, J., Sayegh, M.
H., and Sykes, M. (2000). Allogeneic bone marrow transplantation with co-stimulatory
blockade induces macrochimerism and tolerance without cytoreductive host treatment.
Nat Med 6, 464-9. taf/DynaPage.taf?file=/nm/joumal/v6/n4/full/nm0400_464.html
taf/DynaPage.taf?file=/nm/joumal/v6/n4/abs/nm0400_464.html.
Wekerle, T., Sayegh, M. H., Hill, J., Zhao, Y., Chandraker, A., Swenson, K. G., Zhao, G.,
and Sykes, M. (1998). Extrathymic T cell deletion and allogeneic stem cell engraftment
induced with costimulatory blockade is followed by central T cell tolerance. J Exp Med
187, 2037-44.
Wells, A. D., Walsh, M. C., Sankaran, D., and Turka, L. A. (2000). T cell effector function
and anergy avoidance are quantitatively linked to cell division. J Immunol 165, 2432-43.
Welsh, R. M., Selin, L. K., and Razvi, E. S. (1995). Role o f apoptosis in the regulation o f
virus-induced T cell responses, immune suppression, and memory. J Cell Biochem 59,
135-42.
Weng, N. P., Levine, B. L., June, C. H., and Hodes, R. J. (1995). Human naive and
memory T lymphocytes differ in telomeric length and replicative potential. Proc Natl
Acad Sci U S A 92, 11091-4.
Westgren, M., Ek, S., Remberger, M., Ringden, O., and Stangenberg, M. (1995). Cytokines
in fetal blood and amniotic fluid in Rh-immunized pregnancies. Obstet Gynecol 86, 209-
13.
White, H., Thrasher, A., Veys, P., Kinnon, C., and Gaspar, H. B. (2000). Intrinsic defects o f
B cell function in X-linked severe combined immunodeficiency. Eur J Immunol 30, 732-
7.
239

BIBLIOGRAI’HY
Wiegers, G. J., Stec, I, E., Klinkert, W. E., Linthorst, A. C., and Reul, J. M. (2001).
Bidirectional effects o f corticosterone on splenic T-cell activation: critical role o f cell
density and culture time. Neuroendocrinology 75, 139-48.
Williamson, E., Garside, P., Bradley, J. A., and Mowat, A. M. (1996). IL-12 is a central
mediator of acute graft-versus-host disease in mice. J Immunol 157, 689-99.
Windmill, K. F., and Lee, V. W. (1999). Influences o f surgical castration on the thymus o f
male rats. J Reprod Immunol 44, 29-39.
Witherspoon, R. P., Lum, L. G., and Storb, R. (1984). Immunologic reconstitution after
human marrow grafting. Semin Hematol 21, 2-10.
Witherspoon, R. P., Lum, L. G., Storb, R., and Thomas, E. D. (1982). In vitro regulation o f
immunoglobulin synthesis after human marrow transplantation. II. Deficient T and non-T
lymphocyte function within 3- 4 months of allogeneic, syngeneic, or autologous marrow
grafting for hematologic malignancy. Blood 59, 844-50.
Wong, P., and Pamer, E. G. (2001). Cutting edge: antigen-independent CD8 T cell
proliferation. J Immunol 166, 5864-8.
Wu, C. J., Chillemi, A., Alyea, E. P., Orsini, E., Neuberg, D., Soiffer, R. J., and Ritz, J.
(2000). Reconstitution of T-cell receptor repertoire diversity following T-cell depleted
allogeneic bone marrow transplantation is related to hematopoietic chimerism. Blood 95,
352-9 .
Wursch, A. M., Gratama, J. W., Middeldorp, J. M., Nissen, C., Gratwohl, A., Speck, B.,
Jansen, J., D'Amaro, J., The, T. H., and De Gast, G. C. (1985). The effect o f
cytomegalovirus infection on T lymphocytes after allogeneic bone marrow
transplantation. Clin Exp Immunol 62, 278-87.
Yabe, H., Yabe, M., Kato, S., Kimura, M., and Iwaki, K. (1990). Increased numbers o f
CD8+CD11-I-, CD8+CD11- and CD8+Leu7+ cells in patients with chronic graft-versus-
host disease after allogeneic bone marrow transplantation. Bone Marrow Transplant 5,
295-300 .
Yoshimi, A., Tsuge, I., Namizaki, H., Hoshino, Y., Kimura, H., Takahashi, Y., Watanabe, N.,
Kuzushima, K., and Kojima, S. (2002). Epstein—Barr virus-specific T-cell cytotoxicity is
mediated through the perforin pathway in patients with lymphoproliferative disorders
after allogeneic bone marrow transplantation. Br J Haematol 116, 710-715.
240

B ib l io g r a p h y
Yoshinaga, S. K., Whoriskey, J. S., Khare, S. D., Sarmiento, U., Guo, J., Horan, T., Shih, G.,
Zhang, M., Coccia, M. A., Kohno, T., Tafuri-Bladt, A., Brankow, D., Campbell, P., Chang,
D., Chiu, L., Dai, T., Duncan, G., Elliott, G. S., Hui, A., McCabe, S. M., Scully, S.,
Shahinian, A., Shaklee, C. L., Van, G., Mak, T. W., and et al. (1999). T-cell co-stimulation
through B7RP-1 and ICOS. Nature 402, 827-32.
Young, J. W., Papadopoulos, E. B., Cunningham, I., Castro-Malaspina, H., Flomenberg, N.,
Carabasi, M. H., Gulati, S. C., Brochstein, J. A., Heller, G., Black, P., and et al. (1992). T-
cell-depleted allogeneic bone marrow transplantation in adults with acute nonlym phocytic
leukemia in first remission. Blood 79, 3380-7.
Yu, S., Abel, L., and Globerson, A. (1997). Thymocyte progenitors and T cell
development in aging. Mech Ageing Dev 94, 103-11.
Yu, X., Carpenter, P., and Anasetti, C. (2001). Advances in transplantation tolerance.
Lancet 357, 1959-63.
Yu, X. Z., Bidwell, S. J., Martin, P. J., and Anasetti, C. (2001). Anti-CD3 epsilon F(ab')2
prevents graft-versus-host disease by selectively depleting donor T cells activated by
recipient alloantigens. J Immunol 166, 5835-9.
Yu, X. Z., Bidwell, S. J., Martin, P. J., and Anasetti, C. (2000). CD28-specific antibody
prevents graft-versus-host disease in mice. J Immunol 164, 4564-8.
Zdravkovic, M., Knudsen, H. J., Liu, X., Hager, H., Zachar, V., Aboagye-Mathiesen, G.,
and Ebbesen, P. (1997). High interferon alpha levels in placenta, maternal, and cord
blood suggest a protective effect against intrauterine herpes simplex virus infection. J Med
Virol 51, 210-3.
Zhang, L., Lewin, S. R., Markowitz, M., Lin, H. H., Skulsky, E., Karanicolas, R., He, Y., Jin,
X., Tuttleton, S., Vesanen, M., Spiegel, H., Kost, R., van Lunzen, J., Stellbrink, H. J.,
Wolinsky, S., Borkowsky, W., Palumbo, P., Kostrikis, L. G., and Ho, D. D. (1999).
Measuring recent thymic emigrants in blood o f normal and H IV -1-infected individuals
before and after effective therapy. J Exp Med 190, 725-32.
Zinkemagel, R. M. (1996). Immunology taught by viruses. Science 271, 173-8.
Zinkemagel, R. M., and Doherty, P. C. (1974). Restriction o f in vitro T cell-mediated
cytotoxicity in lymphocytic choriomeningitis within a syngeneic or sem iallogeneic
system. Nature 248, 701-2.
241

B ib u o g r a p h y
Zlotnik, A., and Moore, T, A. (1995). Cytokine production and requirements during T-
cell development. Curr Opin Immunol 7, 206-13.
Zorzi, W., Thellin, O., Coumans, B., Melot, F., Hennen, G., Lakaye, B., Igout, A., and
Heinen, E. (1998). Demonstration of the expression of CD95 ligand transcript and
protein in human placenta. Placenta 19, 269-77.
Zuniga-Pflucker, J. C., and Lenardo, M. J. (1996). Regulation o f thymocyte developm ent
from immature progenitors. Curr Opin Immunol 8, 215-24.
242
Related Documents