Abstract of the dissertation entitled A parental education program for the management of atopic dermatitis in children Submitted by Kong Wing Yin For the Degree of Master of Nursing at The University of Hong Kong in August 2015 In the pediatric ward of a major public hospital in Hong Kong, around 5% of patients admitted were due to eczema. Among them, 30% had poor disease control with repeated admissions. Some studies showed that nurse-led parental education in eczema can lead to better disease management, but it has not been considered in the local setting. Despite a systematic review was conducted, there has been subsequently new evidence that urges for an updated evaluation. Therefore, this dissertation aims to systematically review the up-to-date evidence on the effectiveness of parental education program in reducing the severity of eczema, develop an evidence-based guideline for the program, assess the implementation potential, and plan for a pilot and an evaluation of the program. A systematic search of British Nursing Index, PubMed, CINHAL and PsyInfo

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Abstract of the dissertation entitled
A parental education program for the management
of atopic dermatitis in children
Submitted by
Kong Wing Yin
For the Degree of Master of Nursing
at The University of Hong Kong
in August 2015
In the pediatric ward of a major public hospital in Hong Kong, around 5% of
patients admitted were due to eczema. Among them, 30% had poor disease control
with repeated admissions. Some studies showed that nurse-led parental education in
eczema can lead to better disease management, but it has not been considered in the
local setting. Despite a systematic review was conducted, there has been subsequently
new evidence that urges for an updated evaluation. Therefore, this dissertation aims to
systematically review the up-to-date evidence on the effectiveness of parental
education program in reducing the severity of eczema, develop an evidence-based
guideline for the program, assess the implementation potential, and plan for a pilot
and an evaluation of the program.
A systematic search of British Nursing Index, PubMed, CINHAL and PsyInfo

identified 5 randomized controlled trials (RCTs) that assessed the effectiveness of
parental program in reducing severity of eczema in children. Using the Scottish
Intercollegiate Guidelines Network (SIGN) checklist, three of them had high
methodological quality, and two had acceptable quality. Four studies reported
parental education reduced severity of eczema. Thus, it was considered as sufficient
evidence that supported the implementation of parental education program in
reducing severity of eczema. An evidence-based guideline for parental education was
then developed. The local setting shared similar characteristics with the selected
studies in terms of the eligible participants and settings. It also had the staff
supportive to the change with available resources. Moreover, there would be an
annual cost saving of around HK$650,000. Hence, the proposed education program is
feasible and transferable to the local setting.
Training of staff will be made in one month before embarking on a 3-month pilot
study on ten eczematous patients. Then, a 5-month evaluation study on eczematous
patients would be commenced. The primary outcome is the severity of eczema, while
the secondary outcomes are patient’s satisfaction, frontline staff workload and morale,
admission rate and attendance rate at specialty outpatient clinic, and the cost of
innovation. Finally, the primary and secondary outcomes would be evaluated in order
to identify the effectiveness of the program.

A parental education program for the management
of atopic dermatitis in children
by
Kong Wing Yin
B.Nurs. H.K.U.
A dissertation submitted in partial fulfillment of the requirements for
the Degree of Master of Nursing
at The University of Hong Kong
August 2015

i
Declaration
I declare that this dissertation thereof represents my own work, except where due
acknowledge is made, and that it had not been previously included in a thesis,
dissertation or report submitted to this University or to any other institution for a
degree, diploma or other qualifications.
Signed ______________________________________
Kong Wing Yin

ii
Acknowledgements
I would like to express my sincere gratitude to my supervisor, Dr. Daniel Yee-Tak
Fong, Associate Professor, for his generous guidance, enlightenment and patience in
directing me to the right track throughout the dissertation process.
I would also like to thank the staff of the School of Nursing for their assistance and
teaching in my master study.
Finally, I must express my immense gratitude and appreciation to my dear family,
classmates, friends and colleagues for their love, support and encouragement
throughout my study.

iii
Table of Contents
Declaration ................................................................................................................................ i
Acknowledgements .................................................................................................................. ii
Table of Contents .................................................................................................................... iii
List of Appendices....................................................................................................................iv
Chapter 1. Introduction .......................................................................................................... 1
1.1 Background 1
1.2 Affirming needs 2
1.3 Dissertation Objectives 7
Chapter 2. Critical Appraisal ................................................................................................. 9
2.1 Search and appraisal strategies 9
2.1.1 Identification of Study ........................................................................................................................... 9
2.1.2 Criteria for selecting studies for review ..................................................................................... 10
2.1.3 Data Extraction ..................................................................................................................................... 11
2.1.4 Appraisal strategy ................................................................................................................................ 11
2.2 Results 13
2.2.1 Search Results ........................................................................................................................................ 13
2.2.2 Characteristics of the Studies .......................................................................................................... 13
2.2.2.1 Study Types .......................................................................................................................................... 13
2.2.2.2 Sample Characteristics ................................................................................................................... 14
2.2.2.3 Interventions ....................................................................................................................................... 14
2.2.2.4 Length of follow-‐up .......................................................................................................................... 15
2.2.2.5 Outcome measures ........................................................................................................................... 16
2.2.3 Quality assessment of Studies ......................................................................................................... 16
2.3 Summary and Synthesis of Data 19
2.3.1 Summary .................................................................................................................................................. 19
2.3.2 Synthesis of data ................................................................................................................................... 21
Chapter 3. Translation and Application .............................................................................. 25
3.1 Implementation Potential 25
3.1.1Target Setting ......................................................................................................................................... 25
3.1.2 Target audience .................................................................................................................................... 25

iii
3.2 Transferability of the Findings 25
3.2.1 Comparison of Setting and Audience ........................................................................................... 25
3.2.2 Philosophy of Care ............................................................................................................................... 27
3.2.3Number of clients benefit from the Innovation ........................................................................ 27
3.2.4 Time for Implementation and Evaluation ................................................................................. 27
3.3 Feasibility 28
3.3.1 Freedom on implementation ........................................................................................................... 28
3.3.2 Interference of Staff Functions ....................................................................................................... 29
3.3.3 Administrative Support ..................................................................................................................... 30
3.3.4 Consensus among the Staff and Administrators ..................................................................... 31
3.3.5 Risk of Friction ....................................................................................................................................... 32
3.3.6 Skills of Adopting the Innovation .................................................................................................. 32
3.3.7 Equipment and Facilities .................................................................................................................. 33
3.3.8 Staff Training ......................................................................................................................................... 33
3.3.9 Measuring tool for evaluation ........................................................................................................ 33
3.4 Cost-‐benefit Ratio of the Innovation 34
3.4.1 Potential Risks ....................................................................................................................................... 34
3.4.2 Potential Benefits ................................................................................................................................. 34
3.4.3 Risks of Maintaining Current Practice ........................................................................................ 35
3.4.4Material Cost of Implementing the Innovation ........................................................................ 35
3.4.5 Material Cost for not implementing the Innovation ............................................................. 36
3.4.6 Potential Non-‐material Cost of implementing the Innovation ......................................... 36
3.4.7 Potential Non-‐material Benefits of Implementing the Innovation ................................. 37
3.5 Evidence-‐based Guideline 37
Chapter 4. Implementation Plan .......................................................................................... 39
4.1 Communication Plan 39
4.1.1 Identification of Stakeholders ......................................................................................................... 39
4.1.2 Initiation stage ...................................................................................................................................... 39
4.1.3 Facilitation Stage ................................................................................................................................. 41
4.1.4 Communication Strategies to Sustain Change Process ....................................................... 41
4.2 Pilot Study Plan 42
4.2.1 Objectives of Pilot Study Plan .......................................................................................................... 42

iii
4.2.2 Preparation of the Pilot Study ........................................................................................................ 43
4.2.3 Subject Recruitment Strategies ...................................................................................................... 44
4.2.4 Data Collection ...................................................................................................................................... 45
4.2.5 Data Evaluation .................................................................................................................................... 45
4.3 Evaluation Plan 46
4.3.1 Objectives of Evaluation Plan ......................................................................................................... 46
4.3.2 Outcomes .................................................................................................................................................. 46
4.3.2.1 Patient Outcomes .............................................................................................................................. 46
4.3.2.2 Healthcare Provider Outcomes ................................................................................................... 48
4.3.2.3 System Outcomes .............................................................................................................................. 48
4.3.3 Nature and Number of Clients to be involved .......................................................................... 49
4.3.4 Timing and Frequency of Data Collection ................................................................................. 50
4.3.5 Data Analysis .......................................................................................................................................... 51
4.3.6 Basis for Recommendation of Nurse-‐led Education Program to Eczematous
Pediatric Patients ............................................................................................................................................ 52
References……………………………………………………………………………………………………………… 55
Appendices.....……………………………………………………………………………………………….………… 57

iv
List of appendices
Appendix 1a: Systemic Search Strategies & Results 57
Appendix1b: PRISMA Flowhchart 58
Appendix 2: Table of Evidence 59
Appendix 3: Quality Assessment of Selected Studies 65
Appendix 4: Estimated Set-‐Up Cost of the Parental Education Program of
Management of Eczema (1st – 2nd Year) 75
Appendix 5 : Estimated Operation Cost of the Parental Education Program of
Management of Eczema (3rd year onward) 76
Appendix 6: Evidence-‐based Guideline of Parental Education Program for
Eczematous Children 77
Appendix 7: Level of Evidence Developed by the SIGN 86
Appendix 8: Grading of Recommendations Developed by the SIGN 87
Appendix 9: Recommendation Synthesis Process 88
Appendix 10: Gantt Chart of The Education Program for The Eczematous Pediatric
Patients 90
Appendix 11: Scoring of Atopic Dermatitis Assessment Form 91
Appendix 12: Evaluation Questionnaire of the Education Program for Pediatric
Eczematous Patients 92
Appendix 13: Evaluation Questionnaire for the Nursing and Medical Staff of Pediatric
and Adolescent Medicine Department 93
1
Chapter 1
Introduction
1.1 Background
Atopic Dermatitis is also known as atopic eczema. It is an itchy inflammatory
chronically relapsing skin disease (Williams 2005). Such skin disorder can be acute
with symptoms such as redness, oozing and vesicles. It can also be chronic with skin
thickening or skin pigmentation.
Atopic eczema is one of the most common inflammatory skin diseases in
childhood, affecting a huge number of children worldwide (Asher 2006). Indeed, the
prevalence of atopic eczema has increased by two to three-fold over 30 years (Schram,
2010). Based on the International Study of Asthma and Allergies in Childhood
questionnaire, the three most frequently reported allergic conditions or symptoms in
children aged 14 and below were allergic rhinitis (24.5%), sneezing, a runny or
blocked nose without a cold or flu (14.5%) and eczema (12.4%). The Child Health
Survey conducted by the Surveillance and Epidemiology Branch Centre for Health
Protection of the Department of Health in Hong Kong reported that eczema (25%)
was among the five most frequently reported conditions in children aged 14 or below.

2
In Hong Kong, eczema is one of the most common chronic diseases in children.
Deficient knowledge of disease management and the lack of confidence may
lead to suboptimal management of atopic eczema. In atopic eczema management,
nurses play a vital role in disease management because they can provide
comprehensive education to the parents of the children with atopic eczema. By
providing education with knowledge of disease management, nurses can play a
prophylactic role in preventing the exacerbation of atopic eczema, resulting in a
decrease in both the admission rate at pediatric ward and the follow up frequency in
hospital due to eczema.
1.2 Affirming needs
I considered a pediatric ward setting in the public hospital of the Hong Kong
Hospital Authority, where pediatric patients suffering from eczema with acute skin
inflammation were admitted. About 5% of pediatric patients were admitted with
eczema as current diagnosis at my pediatric ward. 30% of children admitted with
asthma also had past medical history of eczema. Eczema was one of the common
chief complaints of children admitted in my pediatric ward. During the hospital stay

3
in pediatric ward unit, nurses were only allowed to spend very little time on eczema
patients. In local setting, one single nurse had to take care of a team of around 8
patients in one shift. Usually there were 5 or more patients admitted for acute
diagnosis in one team and eczema was considered as less acute diagnosis. Therefore,
nurses spent more time on the urgent treatments for the other patients with acute
diseases in one shift. Thus, less time can be spent on eczematous children and nurses
can only contact the eczematous children’s parents during medication prescription. It
was just around a few minutes and nurses instructed them how to apply the topical
medication on the skin surface. Therefore, when the patient’s skin condition
recovered, they would be discharged without receiving any education on disease
management. Thus, these eczematous children would be frequently re-admitted after a
few months. Almost 30% of the children repeated admissions for the second time or
more for eczema.
For the children with eczema who have regular follow up after discharge from
public setting, their waiting time takes more than a few months. The regular medical
follow up time would be around 10 minutes. Physicians mainly focus on assessment

4
and prescription of medication. Therefore parents and their children with atopic
dermatitis have to manage the disease by themselves with little knowledge of eczema.
Consequently, some of the patients were found to have poor control and compliance
from time to time. Many of them needed to be re-admitted at the pediatric ward for
managing the inflamed poor skin condition. Therefore, a nurse-led parental education
program is needed which can allow more time for nurses to educate patients with
better disease management and control.
Education interventions aim at targeting the children and their caregivers. They
are designed to teach the techniques which are related to prevention and management.
Strategies include instructional lectures, role-playing, printed pamphlets and personal
experience sharing, etc. Education interventions focus on the process how the
caregiver acquires new knowledge and gets better preparation in understanding the
children’s medical’s condition, therefore effective disease management can be
provided. The objective of education programs is to motivate patients and primary
care-givers in solving the problems associated with chronic disease. Meta-analysis of
results has highlighted the need for standardized method so the improvement in

5
self-management of chronic disease can be more precisely assessed (Warsi , 2004 ).
Management of atopic dermatitis should involve symptoms relief treatment,
maintenance of skin integrity, prevention of secondary infection and enhancement of
the quality of life (Ayliffe, 2009). Identifying the predisposing factors, appropriate
skin care and adoption of correct treatments are crucial for desirable outcomes
(Ayliffe, 2009).
The cause of atopic eczema is not clear. It is likely to be environmental factors
and genetic factors. Nevertheless, parents with good compliance can lead to a better
control of the disease management (McHenry, Williams, & Bingham, 1995).
Inadequate knowledge and poor compliance are the main reasons for poor disease
management. Patient education, adequate time for explanation and discussion, and
demonstration of treatments are important for successful management of atopic
eczema (Mc Henry et al., 1995). However, in local context it cannot be met by only
the medical follow-up due to time restraint. Some studies have shown that the benefit
of nurse-intervention is that clinical outcomes can be improved by giving patient
specific education about the etiology and management of eczema (Cork et al., 2005).
6
The nurse-led parental education program in atopic eczema management by
giving specific education on etiology and management is in great demand because of
its potential capability to reduce the admission rate and follow up frequency due to
eczema, and hence a better clinical outcome is expected. Since new evidence emerged
after the systematic review had been done. Hence, there is a need for gathering new
evidence for an updated evaluation.

7
1.3 Dissertation Objectives
This dissertation aims
1.To systematically evaluate the evidence of the effectiveness of parental education
program in atopic dermatitis management for children.
2. To develop clinical guidelines of the parental education program for the
management of atopic dermatitis in local hospitals.
3. To assess the feasibility and implementation potential of the parental education
program for children with atopic dermatitis.
4. To develop evaluation plans to evaluate the parental education program.
The primary care of atopic eczema focuses on the provision of an education
program for the caregivers in disease management. With better control of disease
management, the severity of eczema can be reduced and the affected parents and
children can have a better quality of life. It can also serve as a prophylactic,
cost-effective measure to reduce the admission rate and follow-up frequency due to

8
eczema, so that the workload of healthcare providers in pediatric department can be
relieved.

9
Chapter 2
Critical Appraisal
2.1 Search and appraisal strategies
2.1.1 Identification of Study
Three groups of keywords were used in the search. The first group consisted of
“educational” or “educating” or “education”. The second group consisted of “ atopic
dermatitis” or “eczema”. The third group consisted of “child” or “childhood” or
“children” or “paediatric” or “pediatric”. The above keywords were used in the
search through the electronic resources at The University of Hong Kong Library. A
comprehensive literature search was performed from 17 August 2014 to 13 September
2014 in four databases via The University of Hong Kong Library electronic search
engine to identify studies; which were relevant.
The four databases were:
1. British Nursing Index
2. PubMed
3. CINHAL
4. PsyInfo

10
Details of the search terms and results are shown in Appendix1a. Titles and
abstracts of the resulting citations were first screened according to the selection
criteria. Potential studies were retrieved and the full papers were screened to confirm
their eligibility. In addition, a manual search of reference lists from those five selected
eligible studies was performed to avoid missing any relevant studies. The process is
shown in the PRIMSA flowchart in Appendix 1b.
2.1.2 Criteria for selecting studies for review
Inclusion criteria
1. Randomized controlled trials;
2. Studies involving 0 to 18 years old children with eczema and their parents
3. Studies that evaluated a parental education program for the management of
eczema
4. Studies that included the following outcome measure:
-‐ Severity of eczema in Scoring of Atopic Dermatitis (SCORAD) Index

11
Exclusion criteria
1. Single nurse consultation session
2. Assessment of a web-based program
3. Only medical decision
4. Ongoing studies
2.1.3 Data Extraction
All eligible studies were carefully read and the data were extracted. The details
extracted were presented in terms of study type, level of evidence, subject
characteristics, sample size, interventions, control, outcome measures, length of
follow up and effect size. They are formulated in the table of evidence as shown in
Appendix 2.
2.1.4 Appraisal strategy
Quality assessment was done with reference to the methodology checklist for RCTs
from the Scottish Intercollegiate Guidelines Network (SIGN) (2012 version2.0). The

12
checklists for critical appraisal of the five reviewed studies were performed as shown
in Appendix 3. The internal validity of the studies was evaluated according to the ten
aspects of the design as shown in the following:
-‐ Appropriate and clearly focused question
-‐ Randomization
-‐ Concealment method
-‐ Blinding
-‐ Similarities of participants
-‐ Treatment under investigation
-‐ Standard validity and reliability of all outcomes
-‐ Dropout rate
-‐ Intention to treat analysis
-‐ Comparability of the results at different sites
Each component was rated as Yes, No, or Can’t Say. The details of rating the overall
methodological quality of the study is also shown in the checklist. They were graded
as High Quality (++),Acceptable (+) and Low quality (0).

13
2.2 Results
2.2.1 Search Results
A systematic search was done from 15th August 2014 to 13th September 2014 in
four databases via the electronic resources search engine at Hong Kong University
Library to find all relevant studies regardless of language. A total of 907 citations
were retrieved. After screening the titles, 30 citations were found potentially relevant.
By screening the abstracts, 6 results were relevant and 1 was written in German. The
English version of the study written in German was not found. So, the citation written
in German cannot be included in the systematic review. Finally, five eligible studies
were identified in which the population, interventions and outcomes corresponded to
my study. After reading the reference lists of all five selected studies, no additional
relevant citation can be extracted for systematic review.
2.2.2 Characteristics of the Studies
2.2.2.1 Study Types

14
All of the selected studies were RCTs. All the participants were randomly assigned
to different groups.
2.2.2.2 Sample Characteristics
In the five selected studies, all participants involved were under the age of 18. The
number of participants recruited varied from one another. Two of the studies
(Futamura et al., 2013, Grillo et al., 2006) recruited around 60, while Moore et al.,
2009 and Staab et al., 2002 recruited around 200 participants. One of the studies
(Staab et al., 2006) recruited 1010 participants.
Four of the selected studies (Futamura et al., 2013, Grillo et al., 2006, Moore et al.,
2009, and Staab et al., 2002) designed an education program for eczematous children
of all ages, while another study (Staab, et al., 2006) divided 1010 participants into
three groups according to their age i.e. 3 months to 7 years old, 8 to 12 years old, 13
to18 years old. The baseline mean total SCORAD index of each selected study was
around 40 to 50.
2.2.2.3 Interventions

15
The interventions in Futamura et al., 2013, Grillo et al., 2006, Staab et al., 2002 and
Staab et al., 2006 involved lectures of eczema etiology and disease management,
practical sessions and group experience sharing. In Moore et al., 2009, it involved a
90 minutes nurse-led workshop including education session and an individualized
management plan written according to the eczema clinical practice guidelines but no
group experience sharing.
The duration of each study design varied from 2 to 120 hours. In Staab et al., 2006,
the intervention was three separate education sessions according to the age group, and
the content was specially tailored to their needs. In four of the studies (Futamura et al.,
2013, Grillo et al., 2006, Staab et al., 2002 and Staab et al., 2006), the control groups
received no education while the control group of Moore, et al., 2009 took part in a
dermatologist- led workshop spending an average of 40 minutes with the doctor.
2.2.2.4 Length of follow-up
The length of follow-up among the five selected studies ranged from 3 months to
12 months.

16
2.2.2.5 Outcome measures
All of the selected studies used SCORAD index as one of the measurement tools
for the severity of eczema. For the effect size, four out of five selected studies showed
there was a significant difference in the SCORAD indices between the intervention
and control groups. The mean difference ranged from -4 to -19.93.
2.2.3 Quality assessment of Studies
In general, all selected studies addressed an appropriate and clearly focused
question. Randomization reduces confounding by equalizing independent variables
that have not been accounted for in the experimental design. Blinding is necessary for
minimizing bias from a subjective assessment of outcome measures. Effective
strategies of randomization and blinding are vital for assessing the quality of an RCT
(Pilot & Beck, 2008). Allocation concealment ensures researchers and subjects do not
know the target grouping before the subjects enter the study in order to minimize the
risk of allocation bias.

17
Four of the studies (Futamura et al., 2013, Grillo et al., 2006, Moore et al., 2009
and Staab et al., 2006) mentioned the details of randomization method. While one of
them (Staab et al., 2002) did not report the method of randomization.
Two of the studies (Grillo et al., 2006, Staab et al., 2002) did not state the
concealment method. For blinding, all participants in the five selected studies cannot
be blinded as they noticed that they were receiving education and it was also
impossible for the trainers to be blinded in all studies. The assessors responsible for
scoring the atopic dermatitis scale in three of the studies (Futumura et al., 2013, Grillo
et al., 2006, Staab, et al., 2006) were blinded, as they were not actively involved as
trainers.
The similarities and differences between the intervention and control groups
were well covered in all selected studies, four of them (Futamura et al., 2013, Moore
et al., 2009, Staab et al., 2002 and Staab et al., 2006) showed that there was no
significant difference between the treatment and control groups as they were similar
at the start of the trial. One of the studies (Grillo et al., 2006) did not mention the
differences of demographic data between the intervention and control groups. In

18
addition, the only difference between the two groups was the treatment under
investigation in all studies.
All relevant outcomes were measured in a standard, valid and reliable way among
all selected studies.
RCTs studies were conducted over a period of time prospectively. A dropout rate
of 20% or less is considered as acceptable but it also depends on the study duration
(Polit et al., 2008). Among all five selected studies, one of them (Staab et al., 2002)
showed 72 out of 93 participants (77%) in intervention group were followed up while
73 out of 111 participants (66%) in control group were followed up. The dropout rate
in the study (Staab et al., 2002) was more than 20%. The reason for the dropout
participants was not mentioned in the study. All of the other four selected studies
showed a dropout rate of less than 20%. They are therefore considered acceptable.
In Grillo et al., 2006, the method of intention-to-treat analysis was implemented.
All other four selected studies did not mention the use of intention-to-treat analysis.
Two of the studies (Moore et al., 2009 and Staab et al., 2006) were carried out at more
than one site. In Moore et al., 2009, results were not comparable as participants

19
received different interventions with nurse-led workshop and dermatologist-led
workshop. In Staab et al., 2006, the results were comparable, as all trainers from
multi-disciplinary team had undergone the same 40-hour training program to qualify
as trainers.
In general, among five selected studies, four of them including Futamura et al.,
2013, Moore et al., 2009 and Grillo et al., 2006 and Staab et al., 2006 reported
randomization, method of blinding and concealment process in details. With low risk
of bias in reporting outcome measures, the internal validity can be ensured and
evidence of high quality can be provided.
Four (Futamura et al., 2013, Grillo et al., 2006, Moore et al., 2009, Staab et al.,
2006) out of five selected studies, which measured severity of eczema in terms of
SCORAD index, showed a significant difference between intervention and control
groups. For overall quality assessment, the methodological evidence of Futamura et
al., 2013, Moore et al., 2009, Staab et al., 2006 was rated as high quality.
2.3 Summary and Synthesis of Data
2.3.1 Summary

20
All of the five selected studies applied parental education program in children with
eczema. The Severity Scoring of Atopic Dermatitis (SCORAD) ranged from 0 to 103
was used to measure the severity of eczema including both the subjective and
objective scores. Total score of SCORAD includes several components: the subjective
score is comprised of the extent of affected sites by calculating the rule of 9 with a
maximum score of 20 and the intensity with a maximum score of 63 while the
maximum objective score is 20. The Overall effect of the parental education to reduce
severity of atopic dermatitis among four (Futamura et al., 2013, Grillo et al., 2006,
Moore et al., 2009, Staab et al., 2006) out of five studies were statistically significant.
It provides adequate evidence that parental education program is effective.
Among all studies, four of them (Futamura et al., 2013, Grillo et al., 2006,
Moore et al., 2009, Staab et al., 2002) provided participants of all ages with one
education program, while one (Staab et al., 2006) of the studies divided the
participants in three different age groups. The study (Staab et al., 2006) provided
three education programs that were tailored to their needs.
21
Regarding the intervention components in all five studies, four of them (Futamura
et al., 2013, Grillo et al., 2006, Staab et al., 2002, Staabl et al., 2006) comprised of
lectures on basic information about eczema and practical sessions. All studies except
Moore et al., 2009 involved sharing sessions. Moore et al., 2009 offered a single
nurse-led consultation session.
For the length of follow-up, it should be adjusted to 3 months and six months.
Among all selected studies, only one study (Staab et al., 2002) showed a dropout rate
of more than 20% as the participants in the study were followed a year after while the
control group received no intervention before the one-year follow-up.
The quality of methodological evidence is high enough to support the
effectiveness of nurse-led parental education program in reducing the severity of
eczema.
2.3.2 Synthesis of data
The target group can be children aged from 0 to 18 years old and it is not
necessary to divide them into three different groups. The SCORAD index did not
show a big difference between age specific and non-age specific education program.

22
Therefore, in order to increase the cost-effectiveness, the education program will not
be designed for different age groups. Since it is a parental program, the main target
audience of the education program is the parents instead of the eczematous children.
It is expensive to run a single nurse consultation workshop currently in a pediatric
ward setting in the public sector. The parental education program should allow
parents to share their own experience and practice the treatment prescribed by
physicians in eczema management. Its cost effectiveness is higher than that of the
nurse consultation session due to the limited resource in my unit. Due to limited
manpower and heavy workload in my unit, it does not allow nurses to provide
sufficient time for face-to-face interview with each patient. Due to limited authority of
nurses in Hong Kong, nurses are not allowed to prescribe medication for patients or to
make any referral. So, providing a nurse-led education on knowledge about eczema
management together with a practical session and a group sharing session with all
parents of eczematous children on personal disease management experience is a trial
in moving forward on education in eczema.
23
Motivation and intention to change are essential factors in educational interventions,
and it is well known that intention to change does not certainly lead to behavioral
change (Webb 2006). Therefore, a plan including follow-ups is important and the
length of follow-up needs to be fixed wisely. Both the intervention and control group
should have the follow-up within a suitable period. In between the follow-ups,
participants should receive neither education nor conventional treatment.
Scoring of Atopic Dermatitis (SCORAD) index should be chosen as the
measurement tool for the outcome measure.
In local context, the credibility of a nurse-led workshop is less sufficient than a
dermatologist-led one. Nurses are not allowed to prescribe medicine or make referral
to patients. Regarding the social acceptance in Hong Kong, patients usually prefer
treatments prescribed by physicians rather than nurses. According to the workshops
provided by nurses in the study of Moore et al., 2009, nurses were competent to do so.
The result in the study showed that the participants who attended the nurse-led
workshop ended up with lower severity of eczema than the control group who
attended dermatologist-led workshop. Therefore, it has been proven that the program
24
can be solely run by nurses.
A nurse-led parental education program for atopic dermatitis is suggested to be
held in the activity room in the Specialty Out-patient Department monthly. It will take
a further forward step in disease management education program of atopic eczema.
An evidence-based guideline is needed in order to ensure the quality of evidence
based parental education program for the children with eczema.

25
Chapter 3
Translation and Application
3.1 Implementation Potential
3.1.1Target Setting
The proposed education will be implemented in an outpatient setting instead of
an in-patient one because of inadequate space and time. The proposed parental
education program will include a lecture session and a practical session. The proposed
program can be held in an activity room at the specialty outpatient clinic. The
proposer as the program leader and four Registered Nurses who are qualified for the
pediatric specialty training will be responsible for the proposed program.
3.1.2 Target audience
From my observation, around 5% of patients admitted for eczema as chief
complaint at Pediatric and Adolescent Medicine (PAM) wards. The target audience
will be aged from 0 to 18 years old, with history of eczema referred by doctors or
nurses in the PAM wards and outpatient department.
3.2 Transferability of the Findings
3.2.1 Comparison of Setting and Audience

26
All education programs in the reviewed studies were conducted on outpatient
basis. The target setting of the proposed program is at a specialty outpatient clinic.
Since the education programs in the reviewed studies were conducted in an outpatient
clinic, thus it can be adjusted to fit into the proposed site.
The characteristics of the target audience match greatly with most of the
reviewed studies. They were aged between 0 to 18 years old and were diagnosed with
eczema in the last admission or with a history of eczema.
The participants in the reviewed studies were predominantly Europeans and one
of the reviewed studies targeted at the Japanese patients. As the results obtained from
this study also achieved significantly positive outcomes, therefore cultural difference
may not be one of the main concerns.
In the reviewed studies, some of the eczema workshops were carried out by
pediatricians, psychologists, dietitians and nurses. The eczema workshops in two of
the selected studies were carried out solely by nurses. And these two studies also
obtained significantly positive outcomes. It proves that nurses are capable of
providing eczema education to parents with eczematous children. Therefore, the
27
proposed program can be solely run by nurses.
3.2.2 Philosophy of Care
The philosophy of care in the reviewed studies and the proposed program share
the same objective as they were all devoted to help parents with eczematous children
to reduce the severity and improve their quality of life. Skin condition will be
promoted by educating knowledge of eczema, and a lower symptom score will be
achieved by learning the dermatological management through practical session so as
to promote a better quality of life.
3.2.3Number of clients benefit from the Innovation
At the Pediatric and Adolescent Medicine wards, a total of 300 patients were
admitted and around 5% i.e. 15 of these patients were diagnosed with chief complaint
of eczema monthly. These patients would be referred to outpatient clinic for attending
the nurse-led proposed program. The number of clients who could benefit from this
proposed program should be sufficiently large.
3.2.4 Time for Implementation and Evaluation

28
We will conduct a pilot program to estimate and draft the schedule for
implementation and evaluation. In the preparation phase, it will take 4 months for
designing and planning the program structure, briefing and training the nurses,
printing the reading materials, venue arrangement and the promotion of the eligibility
criteria of referring the patients to the proposed program through internal e-mail and
circulars to doctors and nurses within the department. It will take two months for
seeking approval, four moths for preparation and three months for pilot study. In total,
it will take 9 months for the entire pilot study. Evaluation will be made after that. The
actual implementation will also be carried out for another six months, and it will take
around nine months for the evaluation of the program. In total, it is estimated that the
implementation of the proposed program will take 2 years.
3.3 Feasibility
3.3.1 Freedom on implementation
In the Pediatric department, nurses can have the freedom to introduce an
innovation only if it shows significantly positive outcome on an evidence-based basis.
The proposed program can be implemented after the approval from the administrative
29
level. Nurses in the pediatric specialty outpatient department are encouraged to take
part in the proposed program. Clients have the right to terminate the program when
they think it is undesirable and can give precious feedback for the proposed program
to make particular improvement.
Patient education on eczema is one of the major issues in the pediatric outpatient
clinic. Based on my observation in the local clinical setting, an increasing number of
children are diagnosed as eczema with mild to high severity and about 70% of the
parents with eczematous children do not understand the eczema management plan to
reduce its severity. For this particular group of parents, they have to understand the
importance of the proposed program that can offer them with an evidence-based
management plan.
3.3.2 Interference of Staff Functions
The proposed program will not interfere with the staff functions. Nurses who are
assigned to hold the program will be arranged to receive a training program of 3
two-hour sessions. It is planned to set up in 2016. The training session will be held in
the afternoon when nurses are originally assigned to hold appointments with clients.

30
They will be free from the clients’ appointments. The time-slot available for the
clients to meet nurses will be reduced on those three training days and the preparation
meetings during the preparation phase. No extra working hours are needed. There will
be 4 months of time for staff to prepare all the materials and receive training before
the pilot program. Sufficient manpower will be available for providing the service.
The estimated number of participants served annually will be around 150. It will
take a maximum of 15 hours a week for a nurse to spend on the proposed program
during implementation phase. Over half of the eczematous patients will be
re-admitted due to eczema as chief diagnosis. It will take more working time on the
hospitalized patient care than that on the eczema education. It takes around 2 days of
hospital stay and at least an hour of education to one single patient with limited
knowledge on applying the treatment only during one shift. It takes around 64 hours
for around 4 patients admitted weekly, which is far more than the 15 hours spent on
the proposed program per week.
3.3.3 Administrative Support
Support from the department head and the hospital is needed to put the proposed
31
program into practice. The Chief of Service (COS) and Department Operation
Manager (DOM) encourage the implementation of the evidence-based innovations.
The hospital is conducive to research utilization in obtaining better care outcomes.
The evidence-based protocol of distraction therapy during venipuncture has been
successfully established in the pediatric department.
3.3.4 Consensus among the Staff and Administrators
Both nursing staff and administrators understand the importance of providing
education to parents on different issues so as to provide better patient outcomes. And
both of them have consensus that eczema is a growing and common problem that
many children are suffering from this disease. The affected group will benefit from
the proposed program and the program can reduce the workload of staff ultimately.
The major pockets of resistance are the motivation of the parents of the eczematous
children to attend the nurse-led workshop and the dropout rate due to the control
group that receive no education. The results of evaluation will be unreliable if the
dropout rate is high. In order to reduce the dropout rate in the proposed program, the
length of follow-up cannot be too long. Therefore, the importance of the program
32
information should be emphasized before referring patients to the program. We
should also keep contact with those who are absent from the program. A primary
nurse should be assigned for each individual for follow-up.
3.3.5 Risk of Friction
The implementation of the proposed program may include some potential risks
for the clients. Medical officers and psychiatrist can also be invited to be the
supporters who are available for medical assessments and psychological
consultations.
3.3.6 Skills of Adopting the Innovation
Experienced nurses who are involved in the proposed program are capable of
performing the physical assessment and education, as they are all qualified from
specialty training in the pediatric department. All nurses involved in the proposed
program are qualified to provide comprehensive education on the management of
eczema. No extra special skills are needed to be trained. By receiving the training
workshop, they will be capable of holding the program smoothly and effectively with
enhanced knowledge and communication skills.

33
3.3.7 Equipment and Facilities
The venue will be the activity room in the outpatient clinic. The education
pamphlets, notes and PowerPoint slides will be printed for distribution. Some
souvenirs, food and drinks are needed to be prepared as the incentives to attend the
workshop.
3.3.8 Staff Training
Nurses who are going to hold the program have already understood and learnt
about the epidemiology and management of eczema in their specialty training in the
pediatric department. Three two-hour briefing sessions during their duties will be held
for learning more about the proposed program structure and enhancing
communication skills. Some regular evaluation sessions will be held at a 3-month
interval for evaluating the proposed program.
3.3.9 Measuring tool for evaluation
Scoring System of Atopic Dermatitis (SCORAD) is used to measure the severity
of eczema. There are some existing printed forms in the ward. The score can be

34
calculated by the in-charge nurse.
3.4 Cost-benefit Ratio of the Innovation
3.4.1 Potential Risks
There is no potential risk in this proposed program. All selected studies did not
show negative outcome in the severity of eczema or skills of management.
3.4.2 Potential Benefits
At the client’s level, the proposed program will provide an opportunity to
increase the affected parents’ ability and confidence to improve and maintain their
children’s health, increase physical and psychological well-being, improve quality of
life, increase the compliance and reduce the severity of eczema.
At the staff’s level, the nurses can make decisions from the best education regime
by an evidence-based guideline so as to reduce the inconsistency of eczema
management, gain appreciation from clients so as to increase job satisfaction. The
re-admission rate and follow-up frequency due to eczema can be reduced, thus the
workload of staff will also decrease.
At the organization’s level, it will reduce the healthcare cost on eczematous
35
clients, have better utilization of resources, raise the reputation for client’s
relationship, and create an image of showing respect and encouragement to
implement evidence-based practice to provide the most updated care. It also shows
that the hospital is always striving for the best quality of patient outcomes.
3.4.3 Risks of Maintaining Current Practice
If the current practice is maintained, the parents of eczematous children cannot
obtain much knowledge on eczema and the misconception of prescriptions from
pediatricians cannot be clarified. If the proposed program is not implemented, the
re-admission rate of eczema and the follow-up frequency will remain high, and clients
will keep relapsing in a scratching cycle and the severity can never be improved.
3.4.4Material Cost of Implementing the Innovation
Set-up cost
The budget will be spent mainly on the wages of nurses who are conducting the
proposed program, which is HKD 234 per hour. The annual personnel expenses will
cover the meeting, staff training, program design, operation and evaluation. The direct
cost of the proposed program includes the printed materials e.g. the PowerPoint notes,

36
assessment forms and questionnaires. The total set up cost of the proposed program
would be HKD 273,140 as shown in Appendix 4.
Operational Cost
The majority of operational cost is still the personnel expenses. The personnel
expenses are based on the number of hours of staff spent on running the proposed
program, follow-up sessions with clients and regular evaluation meetings. It is
estimated that from the third year onwards, the cost of the proposed program would
be HKD 143,400 per year as shown in Appendix 5.
3.4.5 Material Cost for not implementing the Innovation
The estimated acute health care cost for patients with eczema admitted to
hospital will be HKD4580 per day and the estimated follow-up cost for one patient
would be HKD 1000 per visit. It is estimated that the medical cost spent on pediatric
eczema will be HKD 927,000 annually. Thus, the material cost for not implementing
the innovation will be the cost spent on repeated admissions and follow-ups, and the
workload of the frontline staff will also increase.
3.4.6 Potential Non-material Cost of implementing the Innovation

37
Staff may have increased stress of adapting the changes when conducting the
proposed program. Staff morale may alter. Nurses may have to put extra effort in
preparing the assessment and evaluation forms, education materials, monitoring the
clients’ progress and evaluation meetings.
3.4.7 Potential Non-material Benefits of Implementing the Innovation
The non-material benefits of implementing the innovation include improved staff
morale due to reduced workload, appreciations from clients by building up a rapport
between nurses and clients, higher quality of life for both the children and parents.
Ultimately it may also increase job satisfaction of nurses and reduce the turnover rate.
3.5 Evidence-based Guideline
An evidence-based guideline was developed for the proposed program to reduce
the severity of eczema in children and is presented in Appendix 6. The evidence
levels of the selected studies were based on Scottish Intercollegiate Guideline
Network (SIGN) as shown in Appendix 7. The recommendations were extracted from
the five selected studies, two (Moore et al., 2009; Stabb et al., 2006) were graded as
1++, and the other three (Futumura et al.,2013; Grillo et al., 2006; Stabb et al., 2002)

38
were graded as 1+. For the grading of the proposed recommendations, they were
determined by the evidence level of each identified studies. These recommendations
were then graded according to Grades of Recommendation (SIGN, 2012a) as shown
in Appendix 8. Tables illustrating the recommendation synthesis process are shown in
Appendix 9.
39
Chapter 4
Implementation Plan
4.1 Communication Plan
4.1.1 Identification of Stakeholders
The stakeholders are the people who may be affected by the proposed program.
In the education program for the eczematous children, stakeholders at the
administrative level are COS, GMN, DOM and the ward managers of wards and
Specialty Out-patient Department (SOPD) who are responsible for allocating
resources and managing manpower for the proposed program. At the frontline level in
Pediatric and Adolescent Medicine wards and outpatient clinic, 30 Medical Officers,
18 Advanced Practice Nurses and 80 Registered Nurses are responsible for providing
health assessments and referring clients. Nurses at Specialty Outpatient Department
are responsible for conducting the education program. The parents of the eczematous
patients aged from 0 to 18 who are admitted to the wards are also part of the key
stakeholders.
4.1.2 Initiation stage
In order to gain support from the administrative level, the proposer of the
40
program will arrange a 1-hour meeting with the ward managers of in-ward and SOPD.
In the meeting, the proposer will report the prevalence of eczema in children, the
effectiveness of the parental education program supported by research evidence and
the protocol of the proposed program that can be held at the Specialty Out-patient
Department. By holding the meeting with a comprehensive written proposal, it helps
to raise the concern of high re-admission rate and frequent follow-ups so that the
managers will understand the needs for change. After getting the agreement from the
ward managers, a formal presentation will be arranged in a monthly departmental
meeting with the DOM. The affirming needs of a nurse-led parental education
program to pediatric eczematous patients will be disseminated in the meeting. The
new proposed program guideline with its transferability and feasibility will also be
presented and written in the proposal. To ease their concern on the impacts that
brought by the proposed program, the cost-benefit ratio will be shown clearly that
benefits from the program can outweigh the costs of implementation. The proposed
program can also alleviate the burden of the workload of the frontline staff. The
initiation stage will take one month.

41
4.1.3 Facilitation Stage
In order to gain a better understanding of the proposed program, a meeting will
be arranged for the frontline staff to understand the needs for change and what are
needed to be accomplished. Five nurses will be selected into the program team. To
avoid interference with routine clinic operations, program team members will be free
from the routine work for the meeting time. The facilitation stage will last for one
month. Full-text articles about the education program will be sent to all frontline staff
in the Pediatric Department via e-mail. Posters including the outline of the program
will be posted in the clinic and the pediatric wards. They can help to raise the staff’s
awareness of the program and can help to encourage them to refer eligible clients.
Posters will also be posted in the eye-catching areas in the Pediatric and Adolescent
Medicine wards so as to draw the attention and raise the parents’ interest to the
program. The communication period will last for one month according to the Gantt
chart in Appendix 10. It will also be used to illustrate the time frame of the program
schedule.
4.1.4 Communication Strategies to Sustain Change Process

42
In order to sustain the change process, nurses’ compliance with the guideline of
the proposed program will be assessed. Monthly on-site audits will be done by the
proposer and the SOPD ward manager. The review reports and the reminders will be
sent to the involved program team members monthly. The records of progress will be
kept and reviewed annually. The SOPD ward manager and the proposer should
maintain a two-way communication with the frontline staff. They have to discuss the
difficulties encountered by the frontline staff in implementing the program and collect
the feedbacks during the monthly review. Amendments should be made to the new
guidelines if necessary according to the opinions collected. Nurses should also keep
monitoring the progress of patient outcomes and share the successful cases of
eczematous children with reduced SCORAD index to encourage their colleagues and
keep the staff morale.
4.2 Pilot Study Plan
4.2.1 Objectives of Pilot Study Plan
A pilot study plan will be conducted prior to the full-scale program evaluation. It
can help to determine the feasibility of the proposed program and can avoid the
43
unexpected difficulties. It can also help to evaluate the proposed program and can
solve the possible problems before its implementation. Training workshops for the
staff and the preparation of materials for presentation will take 4 months. The actual
pilot study will take three months. Another five months will be spent on evaluation of
the pilot study and amendments will be made accordingly before its implementation.
In total, the pilot study plan takes one year before the actual implementation
commenced.
4.2.2 Preparation of the Pilot Study
It will take six months for the preparation of the pilot study. The work meetings
will be held monthly for the program team to plan and follow the progress. The
proposer will be selected as the program leader and communicate with team members
through email regarding the agenda of the meeting. The program team members will
have to attend three two-hour training workshops. The topic of the first session will
mainly focus on epidemiology of eczema. It will also teach the method of topical
application and stress management. The second session will introduce the
evidence-based guideline to standardize the teaching in the proposed program and the
44
use of Scoring Atopic Dermatitis (SCORAD) Index. The use of SCORAD system will
be demonstrated and discussed so that it can help to standardize the scoring of each
program team member. The third session will focus on presentation skills and
consultation skills. The atmosphere of holding an education program is very
important and directly affects the outcome measures. After the training, all the
program team members will be capable of providing evidence-based education and
effective communication. During the promotion period, a 1-hour session to nurses and
medical staff will be held for introducing the proposed program. It will also highlight
the inclusion criteria of eligible participants and their roles in referring cases. A
hotline will be provided for them to contact the program leader for any enquiries.
4.2.3 Subject Recruitment Strategies
The recruitment of eligible subjects will mainly rely on the referrals from the
Pediatric and Adolescent Medicine wards and outpatient clinic. Under the pilot study,
it will recruit 10 eczematous pediatric patients who meet the inclusion criteria of the
proposed program. The nurses and medical officers in Pediatric and Adolescent
Department will also be responsible for accessing the readiness of the parents of the

45
eligible subjects in joining the pilot study. Nurses and pediatricians will be allowed to
refer the eligible subjects to the pilot study with signed consents. The recruitment
period will last for one month before the pilot study.
4.2.4 Data Collection
The severity of eczema will be assessed by the SCORAD index as baseline data.
The demographic data and the treatments that doctors prescribed will also be
recorded.
4.2.5 Data Evaluation
After collecting the data, evaluation has to be done and the period will last for
five months. The program team will hold a debriefing session with the frontline staff.
All possible problems that may happen will be discussed in the debriefing meeting.
After reviewing all the problems, amendments may have to be made according to the
logistics, the program guidelines and the outcome measurements. The confidence
level of using the guideline to carry out the program is also needed to be discussed
during the evaluation period. A 15-minutes group meeting right after the program
with ten participants who have taken part in the pilot study will be held to get the

46
feedbacks on the content, duration and practicability of the program. After collecting
comments from the frontline staff and participants, the guidelines will be discussed
and revised according to their comments.
4.3 Evaluation Plan
4.3.1 Objectives of Evaluation Plan
The aim of evaluation plan is to assess the effectiveness and the clinical benefits
of the proposed program.
4.3.2 Outcomes
4.3.2.1 Patient Outcomes
One of the clinical benefits of the education program is directly reflected by the
severity of eczema. It is determined by the SCORAD Index (Appendix 11) and
assessed by the program team members. The SCORAD index is determined on the
basis of several criteria concerning the extent, intensity as well as subjective signs.
For the extent criteria, the rule of nine is used. It is advised to draw lesion spread
directly on the evaluation sheet and then perform calculation. The marks of total area
47
extent will be regarded as component A (0 to 100) in the formula of calculation. For
the intensity criteria, it will be graded according to the following aspect: erythema,
oedema or papulation, oozing or crust, excoriation, lichenification and dryness. Each
intensity item will be graded from 0 to 3 and the total marks will be regarded as
component B (0 to18) in the formula of calculation. For the subjective symptoms, it
will be measured in the following two aspects: pruritis and sleeplessness for the
average of last 3 days or nights. It will be graded by a 10 cm visual analog scale and
regarded as component C (0 to 20) in the formula of calculation. The total score will
be calculated by the following formula: A/5 + 7B/2 + C. The range of total SCORAD
Index is 0 to103. The severity of the total score that is less than 25 is regarded as mild,
25 to 50 is regarded as moderate, and higher than 50 is regarded as severe.
Another outcome would be patients’ satisfaction. Parents will have to fill a
questionnaire (Appendix 12). It is used to evaluate the patients’ satisfaction to the
program content and to gather the overall comment. There are five questions that
focus on knowledge and management skills of eczema and the program structure. The
last question will be an open-ended question for collecting any other comment.
48
4.3.2.2 Healthcare Provider Outcomes
The comments collected by the involved staff are very important to the proposed
program. The involved staff members are the ones who can directly reflect the
effectiveness and staff morale after running the program. The comments about the
workload of nurses and pediatricians after running the program have to be collected.
There are five questions in the structured questionnaire (Appendix 13). Three of them
will be Yes / No questions. The fourth question is to assess the staff’s satisfaction to
the program. The last question will be an open-ended question for collecting any other
comment.
4.3.2.3 System Outcomes
System outcomes can help to measure the system effectiveness. The admission rate
of the pediatric ward, the attendance rate of pediatric outpatient clinic and the cost of
innovation are the system outcomes.
By receiving a comprehensive education on eczema, the severity can then be
reduced. The admission rate due to eczema and the follow-up frequency of the
eczematous patients should be lowered after attending the proposed program. The

49
number of admissions and follow-ups will be collected and reviewed at baseline, 3
months, 6 months and 1 year.
For the cost of innovation, it should be compensated by the medical cost of the
admissions due to eczema at wards and the follow-up visits at specialty outpatient
clinic. The workload of the staff should be reduced by the program. The medical cost
for the admissions and follow-up visits will be calculated and should be reduced at 3
months, 6 months and 1 year. The cost of innovation will also be calculated at 3
months, 6 months and 1 year.
4.3.3 Nature and Number of Clients to be involved
The nature of the eligible participants should be based on the identified studies. The
inclusion criteria are as follow:
1. Aged between 0 – 18 years old
2. Diagnosed as eczema or with a history of eczema who are under the care of PAM
department
3. One of the parents is available to join the program
The exclusion criteria are:

50
1. The eczematous patient is currently attending a study related to eczema
2. The parents and the patients cannot communicate well in Cantonese.
A convenient sampling method will be used to recruit participants. The sample size
will be determined by the Java Applets For Power and Sample Size. As the SCORAD
index will be analyzed by a paired t-test, with significant effect size of 5 and power as
80%, alpha as 0.05 and the standard deviation as 20, the total sample size of
participants needs to be more than 128. Based on the selected studies, the drop-out
rate in four of them were not more than 20%. If the dropout rate is taken into account,
it has to recruit at least 154 participants for the study.
4.3.4 Timing and Frequency of Data Collection
Before the recruitment period, an approval has to be obtained from the ethics
committee of the Hospital Authority. After getting the approval, nurses and
pediatricians in PAM Department will refer the eligible participants to the study. The
program team members will introduce the proposed program to the potential
participants. If they agree to join, written consents will be obtained before data
collection. Baseline information will then be collected before the program

51
implementation. The 3-hour workshop will also be introduced. Participants will have
to fill a questionnaire about their satisfaction to the program before they leave the
workshop. Follow-ups will be arranged at 3 months, 6 months and 1 year by
interviews. The actual implementation period will last for 9 months. The patient
outcomes will also be assessed by the SCORAD index and patient’s satisfaction will
also be assessed at baseline, 3 months and 6 months and 1 year.
For the staff outcomes, the workload of nurses and pediatricians and all other
comments will be collected and reviewed at baseline, 6 months and one year.
For the system outcomes, the admission rate and the follow-up frequency of the
participants will be documented at baseline, 3months, 6 months and 1 year. The cost
of innovation will be calculated and recorded at baseline, 3 months, 6 months and 1
year for comparison.
4.3.5 Data Analysis
For the demographic data and the types of treatments received by the participants,
descriptive statistics will be used.
For the patient outcome, the severity of eczema will be assessed by the

52
SCORAD index. The score ranges from 0 to 103 and will be assessed at baseline, 3
months, 6 months and 1 year. At each follow-up time, paired t-test will be used to
assess the severity of eczema. For the patient’s satisfaction to the program, it will be
evaluated by the questionnaire and the score of each question will be calculated. It
will use 95% confidence interval to determine the patient’s satisfaction level. For the
open-ended question, all comments will be collected, discussed and analyzed.
For the system outcomes, the admission rate of pediatric ward, the attendance
rate of pediatric outpatient clinic and the cost of innovation will be examined and
evaluated. The admission rate of pediatric ward and the attendance rate due to eczema
of each participant will be recorded within a year after the program implementation.
The differences at 3 months, 6 months and 1 year will also be calculated, compared
and paired t-test will be used for analysis. The cost of innovation will be calculated
and compared to the medical cost at baseline, 3 month, 6 month and 1 year.
4.3.6 Basis for Recommendation of Nurse-led Education Program to Eczematous
Pediatric Patients
The primary objective of the proposed program is to reduce the severity of eczema
53
of pediatric patients. According to the reviewed studies, the changes in the score of
SCORAD index which showed significant difference ranged from -5.2 (Stabb et al.,
2006) to -19.93 (Grillo et al., 2006). The education program will be considered as
clinically effective with a change in SCORAD Index more than -5 at 6 months after
attending the proposed program. This estimation is based on the revised studies as
well as the experience of the proposer. By equipping themselves with better
knowledge and management skills after attending the program, parents of patients
will have better control in managing the disease and thus the severity can be reduced.
For the staff outcome, if over 60% of staff agree that the workload is reduced,
the program will then be considered as effective.
For the system outcomes, the main objective is to reduce the expenditure of the
hospital. There are about 70 admissions to ward and 1200 outpatient clinic visits due
to eczema every year. Each admission lasts for about 5 days. According to the study
shown by the Hospital Authority in 2014, the average inpatient cost per patient per
day was $4580. $687,000 will be saved if the admission rate decreases by 40%. The
average cost of each outpatient attendance is $1000. (Hospital Authority, 2014) It will

54
save $240,000 if the number of visits decreases by 20%. It may save $ 927,000
annually. The estimated budget for the set-up cost would be $273,140. Thus, around
$653,860 will be saved annually. If the expenditure can be reduced, the program is
considered as effective.

55
References
Asher, M. Innes, et al. "Worldwide time trends in the prevalence of symptoms of
asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One
and Three repeat multicountry cross-sectional surveys." The Lancet368.9537 (2006):
733-743.
Ayliffe, Vicki. "Clinical features and management of atopic eczema in
children."Paediatric Care 21.9 (2009): 35-40.
Cork, M., et al. "Predisposition to sensitive skin and atopic eczema."Community
practitioner 78.12 (2005): 440
European Task Force on Atopic Dermatitis. (1993). Severity scoring of atopic
dermatitis: the SCORAD index. Consensus Report of the European Task Force on
Atopic Dermatitis. Dermatology, 186(1), 23-31
Futamura, Masaki, et al. "Effects of a Short-Term Parental Education Program on Childhood Atopic Dermatitis: A Randomized Controlled Trial." Pediatric
dermatology 30.4 (2013): 438-443.
Grillo, Marianne, et al. "Pediatric atopic eczema: the impact of an educational
intervention." Pediatric dermatology 23.5 (2006): 428-436.
Hospital Authority, Careers (2014). Retrieved December 15, 2014 from
http://www.ha.org.hk/visitor/ha_visitor_index.asp?Content_ID=2010&Lang=ENG&
Dimension=100&Ver=HTML
Lenth, R. V. (2006-9). Java Applets for Power and Sample Size. Retrieved May 18,
2014, from http://www.stat.uiowa.edu/~rlenth/Power.
McHenry, P. M., H. C. Williams, and E. A. Bingham. "Management of atopic eczema.
Joint Workshop of the British Association of Dermatologists and the Research Unit of
56
the Royal College of Physicians of London." BMJ: British Medical Journal 310.6983
(1995): 843.
Moore, Elizabeth J., et al. "Eczema workshops reduce severity of childhood atopic
eczema." Australasian journal of dermatology 50.2 (2009): 100-106.
Schram, M. E., et al. "Is there a rural/urban gradient in the prevalence of eczema? A
systematic review." British journal of dermatology 162.5 (2010): 964-973.
Scottish Intercollegiate Guidelines Network. (2012a). SIGN 50: A guideline
developer’s handbook ANNEX B: key to evidence statements and grades of
recommendations. Retrieved Dec 25, 2015, from
http://www.sign.ac.uk/guidelines/fulltext/50/annexb.html.
Staab, Doris, et al. "Evaluation of a parental training program for the management of
childhood atopic dermatitis." Pediatric allergy and immunology13.2 (2002): 84-90.
Staab, Doris, et al. "Age related, structured educational programmes for the
management of atopic dermatitis in children and adolescents: multicentre, randomised
controlled trial." Bmj 332.7547 (2006): 933-938.
Warsi, Asra, et al. "Self-management education programs in chronic disease: a
systematic review and methodological critique of the literature." Archives of Internal
Medicine 164.15 (2004): 1641-1649.
Webb, Thomas L., and Paschal Sheeran. "Does changing behavioral intentions
engender behavior change? A meta-analysis of the experimental
evidence."Psychological bulletin 132.2 (2006): 249.
Williams, Hywel C. "Atopic dermatitis." New England Journal of Medicine352.22
(2005): 2314-2324.

57
Appendices
Appendix 1a: Systemic Search Strategies & Results
British Nursing
Index
CIHNAL PubMed PsyInfo
Search Data 15/8/2014 15/8/2014 15/8/2014 15/8/2014
“educational or educating or education”
and “atopic dermatitis or eczema” and
“Child or childhood or children or
pediatric or pediatric”.
37 26 651 32
Search by titles 3 0 71 4
Search by abstract 1 0 17 0
Manually Remove duplicated & final
number selected
5

58
Appendix 1b: PRIMSA Flowchart
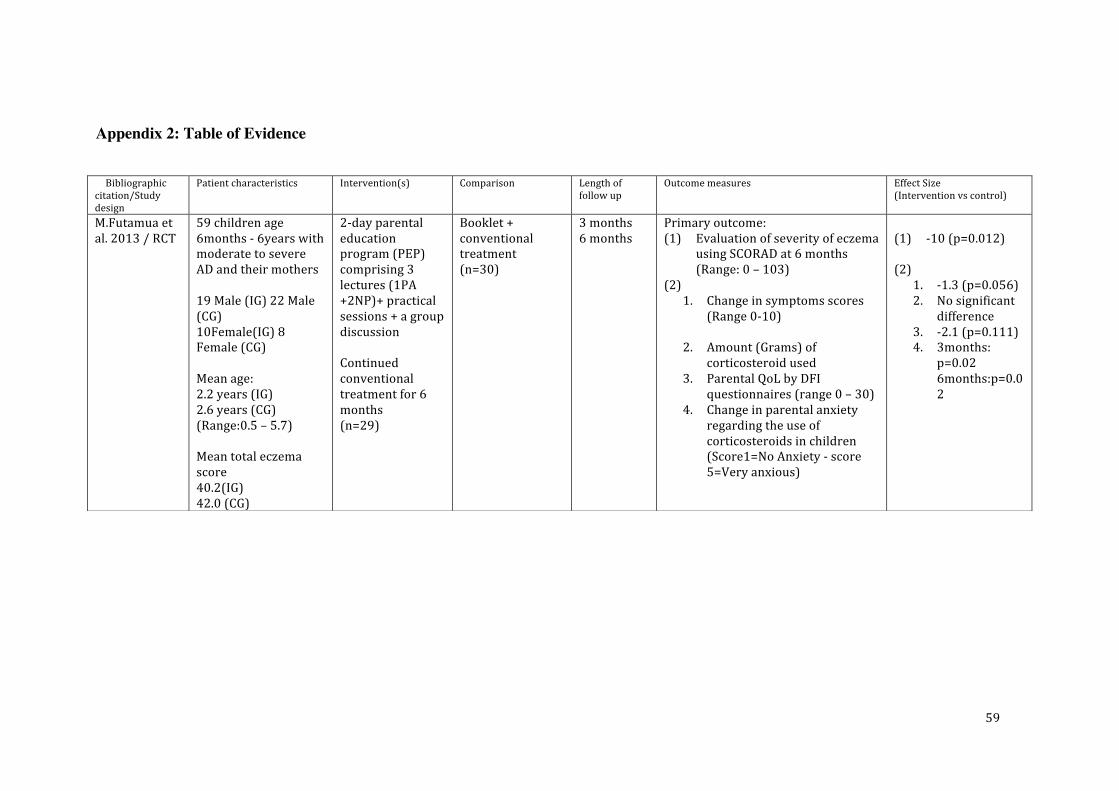
59
Appendix 2: Table of Evidence
Bibliographic citation/Study design
Patient characteristics Intervention(s) Comparison Length of follow up
Outcome measures Effect Size (Intervention vs control)
M.Futamua et al. 2013 / RCT
59 children age 6months -‐ 6years with moderate to severe AD and their mothers 19 Male (IG) 22 Male (CG) 10Female(IG) 8 Female (CG) Mean age: 2.2 years (IG) 2.6 years (CG) (Range:0.5 – 5.7) Mean total eczema score 40.2(IG) 42.0 (CG)
2-‐day parental education program (PEP) comprising 3 lectures (1PA +2NP)+ practical sessions + a group discussion Continued conventional treatment for 6 months (n=29)
Booklet + conventional treatment (n=30)
3 months 6 months
Primary outcome: (1) Evaluation of severity of eczema
using SCORAD at 6 months (Range: 0 – 103)
(2) 1. Change in symptoms scores
(Range 0-‐10)
2. Amount (Grams) of corticosteroid used
3. Parental QoL by DFI questionnaires (range 0 – 30)
4. Change in parental anxiety regarding the use of corticosteroids in children (Score1=No Anxiety -‐ score 5=Very anxious)
(1) -‐10 (p=0.012)
(2)
1. -‐1.3 (p=0.056) 2. No significant
difference 3. -‐2.1 (p=0.111) 4. 3months:
p=0.02 6months:p=0.02

60
M. Griollo, et al, 2006/ Longitudinal RCT
61 pediatric patients (0 -‐16 years) diagnosed with Atopic eczema from the metropolitan area of Adelaide (1) 35 boys & 26 girls (2) Mean age= 4.3 years (Range: 4months to 13 years) (3) Mean SCORAD= 50.97 (IG) 47.7 (CG) (4) Baseline mean DFI= 11.09 (IG) 10.86 (CG) (5) Mean CDLQI= 8.1 (IG) 9.69 (CG) (6) Mean IDQOL= 11 (IG) 8.63 (CG)
2-‐hour education workshop -‐Basic Information of eczema -‐Practical session -‐Sharing session Normal management regimen (n=32)
Routine education medical consultation and management (n=29)
Week 4 Week 12
(1) SCORAD (Range: 0 – 103) (2) DFI (Range: 0 -‐30) (3) CDLQI for 5-‐16years
(Range: 0-‐30) (4) IDQOL for <5 years
(Range: 0-‐30)
(1) Wk4: -‐18.93 (p<0.005) Wk12: -‐19.93 (p<0.05)
(2) No significant difference
(3) Wk 4: No sig difference Wk 12: -‐3.74 (p=0.004)
(4) No significant difference

61
E. Moore et al.,2009/ RCT ++
182 patients new referral for the management of eczema at Royal children’s Hospital in Melbourne (1) 30 boys (IG) 24 boys (CG) 19 girls (IG) 26 girls (CG) (2) Mean age= 3.3 years 2.8 years (IG) 3.75 years (CG) (Range: 0-‐16) (3) Baseline mean SCORAD= 38 (IG) 42 (CG)
Nurse-‐led eczema workshop (n=80) -‐Referral to dermatologist -‐Eczema booklets + cards -‐ Practical session on application -‐Written management plan
Dermatologist-‐led clinic (n=85) -‐Prescription -‐Eczema booklets +cards -‐Educational video Management plan
4 week Follow-‐up
Primary outcome: (1) Severity of eczema as
determined by scores of SCORAD (Range: 0 – 103)
(1) -‐9.93 (P<0.001)
Kupfer et al., 2010 /RCT
185 aged 8 -‐12 years and their parents
6 weekly 2 hours group session (n=102)
Control group Same education program received at 1 year follow up (n=83)
1 year follow-‐up
(1) Differences between training group and control group in coping behavior of children (COPEKI) and parental disease management (FEN)
(2) Changes in training group and control group concerning the psychological variables not due to changes in somatic severity
(1) COPEKI1: -‐3.6(p=0.007) COPEKI2: -‐2.3 (p=0.016)
(2) FEN1: -‐2.4 (p=0.002) FEN2: -‐0.8 (p=0.3) FEN3: -‐1.5 (p=0.002) FEN4: 1.2 (p=0.003)

62
(3) JUCKKI1: castrophizing (p<0.01) JUCKKI2: Coping (P<0.05)
D Stabb et al, , 2002/ Prospective RCT
204( 5 months -‐12 years) suffered from moderate to severe AD (SCORAD > 20 points)at least 4 months
(1) Mean age: 2.7(IG) 3.4 years(CG)
(2) SCORAD index=44(IG) 42(CG)
(3) Duration of disease 2.1(IG) 2.4(CG)
Intervention group parental training 6 group session of 2hour each -‐Presentation of information -‐Experience sharing -‐Practical session (n=93)
Control Group no training (n=111)
1 year follow-‐up
(1) Severity of eczema (SCORAD) (Range 0 – 103)
(2) Treatments costs
(3) QoL (4) Coping strategies
(1) -‐4 (p=0.43)
(2) 92 vs 54 -‐38 (p=0.043)
(3) p=0.016 alpha level set as 0.01 after correction for the number of scales
(4) p=0.013 alpha level set as 0.01 after correction for the number of scales

63
D. Stabb et al., 2006 / Multi-‐centered, RCT
Parents of children with AD 3months-‐18years (1) 3months – 7 years
143Male (IG) 127 Male (CG) 131Female (IG) 117 Female (CG) 8-‐12 years 41 Male (IG) 40 Male (CG) 61 Female(IG)43Female (CG) 13-‐18 years 29 Male (IG)18 Male (CG) 41Female (IG) 32Female (CG) (2 ) Mean age: 3months – 7 years 2.4 (IG) 2.4(CG) 8-‐12 years 9.5(IG) 9.5(CG) 13-‐18 years 14.9(IG) 14.8(CG) (3)Total severity score
Group session of standardized intervention program for AD once weekly for 6 weeks 2hrs each 3months – 7 years receive education+ sessions based ib previously reported work 8-‐12 years separate educational session 13-‐18 years educational sessions tailored to their needs Personal experience sharing Practical session (n=496)
no education (n= 496)
12 months (1) Severity of eczema: By scoring of atopic dermatitis scale (SCORAD) (0-‐103)
(2) Subjective severity: QoL for parents of affected children< 13 years old (Range :0-‐20)
(3) QoL 5 subscales: 1. Psychosomatic wellbeing 2. Effects on social life 3. Confidence in medical
treatment 4. Emotional coping 5. Acceptance of disease
(1) 3Months – 7 Years: -‐5.2 (p=0.0002) 8 – 12 Years: -‐8.2 (p=0.003) 13-‐18 years: -‐14.5 (p<0.0001)
(2) 3Months – 7 Years: -‐1.1 (p<0.001) 8 – 12 Years: -‐2.1 (p<0.001) 13-‐18 years: -‐2.1 (p<0.0022)
(3) 3months -‐ 7 years: All 5 QoL subscales Significant better 8-‐12 years: 3/5 subscales shown significant better improvement

64
(SCORAD) 3months – 7 years: 41.1(IG) 40.6(CG) 8 -‐12 years: 41.8 (IG) 40.4(CG) 13 – 18 years: 43.1 (IG) 40.4 (CG)

65
Appendix 3: Quality Assessment of Selected Studies
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
M Futamura et al. (2013) Effects of a Short-Term Parental Education Program on Childhood Atopic
Dermatitis: A Randomized Controlled Trial, Pediatric Dermatology Vol. 30 no.438-443
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question
Yes R
Can’t say £
No £
1.2 The assignment of subjects to treatment groups is randomised. -Use of computer-generated randomisation list with a block size of eight.
Yes R
Can’t say £
No £
1.3 An adequate concealment method is used.
-Adequate concealment method is used by each patient is picking up a
paper from a total of eight pieces of paper, half of which were labeled
parental education program and half control in a sealed box
Yes R
Can’t say £
No £
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation. Analyses performed before un-blinding of treatment
allocation
-uses digital photographs as they could conceal group allocation and time
of assessment from the objective scorer.
Yes R
Can’t say £
No £
1.5 The treatment and control groups are similar at the start of the trial.
-Well match and shown in table 2 but no p-value was shown.
Yes R
Can’t say □
No £
1.6 The only difference between groups is the treatment under
investigation.
Yes R
Can’t say £
No £
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
Yes R
Can’t say £
No £

66
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
1 in IG lost follow up 2 in CG lost to follow up
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes £
Can’t say £
No £
Does not apply
R
1.10 Where the study is carried out at more than one site, results are
comparable for all sites
Yes £
Can’t say £
No £
Does not apply
R
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise
bias?
Code as follows.
High quality (++)R
Acceptable (+)£
Unacceptable – reject 0 £
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain
that the overall effect is due to the study
intervention?
Yes
2.3 Are the results of this study directly applicable to
the patient group targeted by this guideline?
Yes

67
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Grillo,2006, Pediatric atopic eczema : The impact of an Educational Intervention Pediatric Dermatology,
2006, Vol.23(5), pp.428-436
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes R
Can’t say £
No £
1.2 The assignment of subjects to treatment groups is randomised. -A random number generator was used to place the participants into either the intervention group or control group.
Yes R
Can’t say £
No £
1.3 An adequate concealment method is used.
-Insufficient detail in concealment allocation was provided.
Yes £
Can’t say R
No £
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
- They are receiving the education program, they cannot be blinded.
- Blinding is unclear for the assessor.
Yes R
Can’t say £
No £
1.5 The treatment and control groups are similar at the start of the trial. Yes £
Can’t say P
No £
1.6 The only difference between groups is the treatment under
investigation.
Yes R
Can’t say £
No £
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
Yes R
Can’t say £
No £
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
>80% follow-up 3 lost contact
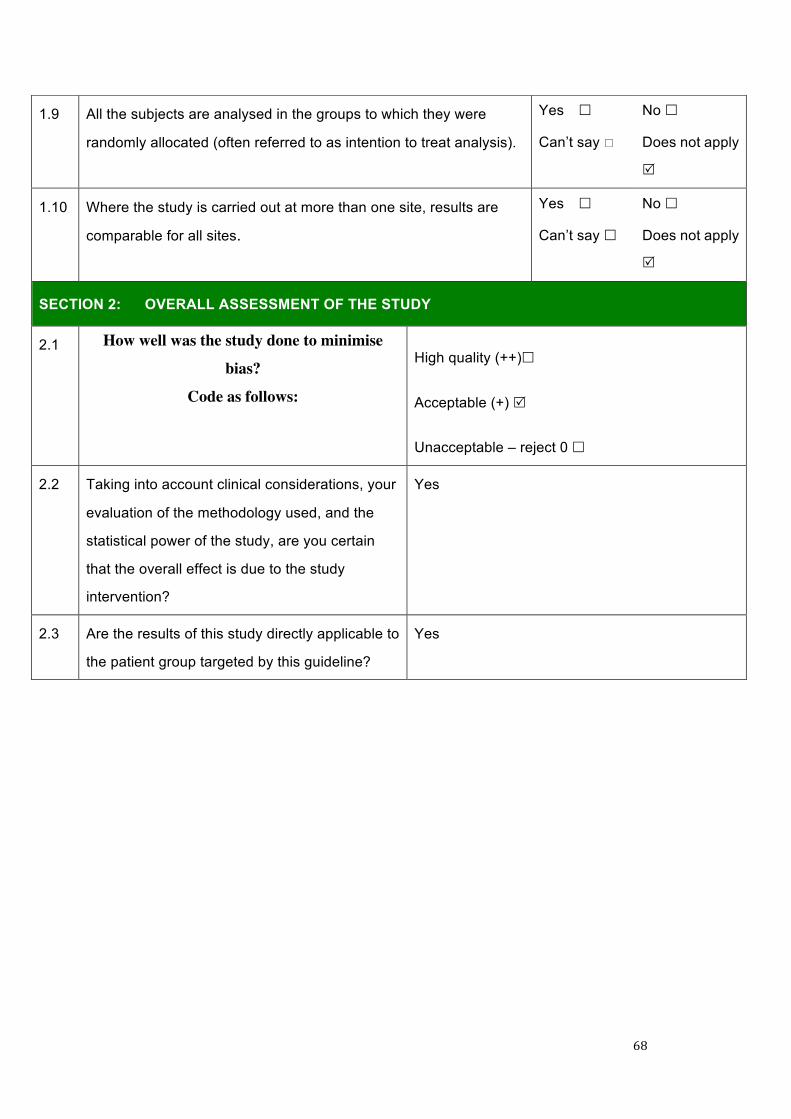
68
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes £
Can’t say *
No £
Does not apply
R
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes £
Can’t say £
No £
Does not apply
R
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise
bias?
Code as follows:
High quality (++)£
Acceptable (+) R
Unacceptable – reject 0 £
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain
that the overall effect is due to the study
intervention?
Yes
2.3 Are the results of this study directly applicable to
the patient group targeted by this guideline?
Yes

69
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Moore et al.(2009) Eczema workshops reduce severity of childhood atopic eczema, Australasian Journal of
Dermatology, 2009, Vol.50(2), pp.100-106
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes R
Can’t say £
No £
1.2 The assignment of subjects to treatment groups is randomised. -They are randomised in block of 10 using (Stata Crop)statistical software.
Yes R
Can’t say £
No £
1.3 An adequate concealment method is used.
-Sequentially numbered sealed opaque envelopes used.
Yes R
Can’t say £
No £
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
-Complete blinding cant be made, minimized by 10 blinded assessment
and assessors. Inter-rater reliability established using Lin concor-dance.
Yes R
Can’t say £
No £
1.5 The treatment and control groups are similar at the start of the trial.
Yes R
Can’t say □
No £
1.6 The only difference between groups is the treatment under
investigation.
Yes R
Can’t say £
No £
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
-All outcome listed
Yes R
Can’t say £
No £
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
13 patiemts lost to follow up >80% follow up

70
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes £
Can’t say R
No £
Does not apply
£
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes R
Can’t say R
No £
Does not apply
£
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise
bias?
Code as follows:
High quality (++)R
Acceptable (+)£
Unacceptable – reject 0 £
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain
that the overall effect is due to the study
intervention?
Yes
2.3 Are the results of this study directly applicable to
the patient group targeted by this guideline?
yes

71
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
D. Staab et al., (2002) Evaluation of a parental training program for the management of childhood atopic
dermatitis. Pediatric Allergy and Immunology, 2002, Vol.13(2), pp.84-90
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes R
Can’t say £
No £
1.2 The assignment of subjects to treatment groups is randomised. Not stated
Yes £
Can’t say R
No £
1.3 An adequate concealment method is used.
Not stated
Yes £
Can’t say R
No £
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
-Cant be blinded as the questionnaires answered by the parents which they
know which group they were in
Yes £
Can’t say £
No R
1.5 The treatment and control groups are similar at the start of the trial.
-No significant difference in any of socio-economic parameters
Yes R
Can’t say □
No £
1.6 The only difference between groups is the treatment under
investigation.
Yes R
Can’t say £
No £
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
Yes R
Can’t say £
No £
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
77% follow-up IG 66% follow-up CG

72
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes £
Can’t say
No R
Does not apply
£
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes £
Can’t say £
No £
Does not apply
R
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)£
Acceptable (+)R
Unacceptable – reject 0 £
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the statistical
power of the study are you certain that the overall
effect is due to the study intervention?
Yes
2.3 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes

73
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
D.Staab, (2006),Age related, structured educational programmes for the management of atopic dermatitis in
children and adolescents: multicentre, randomised controlled trial. Apr 22;332(7547):933-8
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
YesR No £
1.2 The assignment of subjects to treatment groups is randomised. - Randomization was carried out by an independent study centre by computer-generated numbers.
Yes R
Can’t say £
No £
1.3 An adequate concealment method is used.
-The randomization code was concealed in closed envelopes.
Yes R
Can’t say £
No £
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
-Blinding is impossible for the participants who provide most of the
outcome measure by answering questionnaires. Trainers cannot be
blinded.
-The scoring of the AD severity assessors are not involved in the
intervention.
Yes £
Can’t say £
No R
1.5 The treatment and control groups are similar at the start of the trial.
well covered
Yes R
Can’t say □
No £
1.6 The only difference between groups is the treatment under
investigation.
Yes R
Can’t say £
No £
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
Yes R
Can’t say £
No £
1.8 What percentage of the individuals or clusters recruited into each Overall follow up rate is 83%

74
treatment arm of the study dropped out before the study was
completed?
The dropout rate was 17% (10% in intervention group, 24% in control group)
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes £
Can’t say R
No £
Does not apply
£
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes R
Can’t say £
No £
Does not apply
£
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise
bias?
Code as follows:
High quality (++) R
Acceptable (+)£
Unacceptable – reject 0 £
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain
that the overall effect is due to the study
intervention?
Yes
2.3 Are the results of this study directly applicable to
the patient group targeted by this guideline?
Yes

75
Appendix 4: Estimated Set-Up Cost of the Parental Education Program of Management of Eczema (1st – 2nd Year) Items Cost
Personal Cost
Program Team Members Preparation of presenting materials and booklet Work meeting Introductory session Program Session Follow Up Data analysis Nursing Staff training $234 (max RN pay) x 500 hours
$117,000
Medical Introductory Training 30 Medical Officer x 1 hour $464 x 30 hours
$13,920
Nursing Introductory Training
80 Registered Nurse x 1 hour $234 x 80 hours
$18,720
Compensatory Nursing Staff for Program Team Members
$ 234 x 500 hours $117,000
Direct Program Cost
Printing & Photocopying
$5000
Stationery $500
Promotion $1000
Total Set Up Cost $273,140

76
Appendix 5 : Estimated Operation Cost of the Parental Education Program of
Management of Eczema (3rd year onward)
Items Cost
Personal Cost
Program Team Leader Meetings
Introductory session
Data Analysis
Writing Reports
$234 x 50 hours
$11,700
Program Team Members Meetings
Introductory sessions
Running program
Follow-‐up session
$234 x 250 hours
$58,500
Compensatory Nursing
Staff
$234 x 300 hours $70,200
Direct Program Cost
Printing & photocopying $2500
Stationery $500
Total Running Cost $143,400

77
Appendix 6: Evidence-based Guideline of Parental Education Program for
Eczematous Children
An Evidence-‐Based Guideline of Parental Education Program
for Eczematous Children
June 2015

78
Introduction:
It is an evidence-‐based eczema education program for reducing the severity of
eczema in children. The purpose of this guideline is to develop an organized
education program in helping parents of eczematous children to obtained the
knowledge and acquire the skills in managing eczema. It is developed based on
the evidence on the reviewed studies which was graded by the Level of
evidence( SIGN, 2012a) and the recommendations provided in this guideline are
developed from the selected studies and graded according to the Grades of
Recommendation (SIGN , 2012). The in-‐charge nurses should stop this program
if any adverse events occur and should document clearly with the reason.
Rationale of the Guideline
1. To maintain the consistency of nurses in holding the education program on
management of eczema in children
2. To increase nurses’ confidence in holding the parental education program
Objectives of the Parental Education Program
1. To improve confidence and to enhance the skills of parents of eczematous
children in management of eczema

79
2. To improve the severity of skin condition of eczematous children
3. To decrease the admission rate and follow-‐up frequency
Target Group
The targeted participants are parent of children diagnosed as eczema or with a
history of eczema aged between 0 – 18 years old children.
Content of the Program
The education program is organized by five registered nurses who have more
than 5 years experience in pediatric.
Pediatricians and nurses in Pediatric and Adolescent Medicine will refer the
eligible participants and their parents to the parental education program.
The education program lasts for three hours. Follow up will be one month,
three month, six month and one year. The basic information about eczema will
be given in presentation in the first 45 minutes. The remaining time will be run
in form of a group discussion.

80
The schedule of the program
Time Content Aims
30 minutes Presentation
Ø Introduction of the education
program
Ø Basic epidemiology of atopic eczema
Ø Signs and symptoms of atopic eczema
Ø Triggering factors
Ø Basic skin care
- To understand the basic
knowledge of atopic
eczema
90 minutes Group Discussion
Ø Self introduction
Ø Sharing of own experience (e.g.
when and how was it found?
Treatment undertaking? Allergens?
Technique of dealing with itching
behavior? )
- To develop a supportive
and friendly atmosphere
- To learn the different
approaches in tackling
eczema from each others

81
60 minutes Demonstration on treatment application
Return Demonstration
- To develop and strengthen
the skills of wet wrapping
- To learn the common
mistakes in wet wrapping
skills from each others

82
Recommendations
Recommendation 1.0 Recruitment
1.1 The target population would be pediatric diagnosed with atopic eczema
and their parents. The patient should aged from 0-‐18 years old that
includes in-‐patients and outpatients. (Grade A)
All the participants in the selected studies were under 18 years old and their
parents. Both parents and some children who are capable in self-‐management
are also encouraged to join the program. (Futamura et al., 2013; Grillo et al.,
2006; Moore et al., 2009; Stabb et al., 2002; Stabb et al., 2006).(1+, 1+, 1++, 1+,
1++)
Recommendation 2.0 Implementation of the management of eczema
education program
2.1 The education should be conducted in the outpatient clinic. (Grade A)
The program should conduct in the outpatient clinic so as to facilitate the
interdisciplinary communication and can provide a spacious activity room and
staffs at outpatient clinic are experienced in giving primary health education

83
program.(Futamura et al., 2013; Grillo et al.,2006; Moore et al.,2009). (1+,
1+,1++)
2.2 The eczema workshop is suggested to be carried out in a group basis.
(Grade A)
All education program in all selected studies include group session. (Futamura
et al., 2013; Grillo et al., 2006; Moore et al., 2009; Stabb et al., 2002; Stabb et al.,
2006). (1+, 1+, 1++, 1+, 1++). It allows them to share their personal experience
and understand more about the obstacles when managing eczema. Therefore, it
is desirable to carry out the sharing session in a group basis.
2.3 Practical session on wet wrapping and cream application skills should
be included in the program. (Grade A)
Application of treatment such as cream or wet wrapping is demonstrated and
re-‐turn demonstration on trying out the newly learned skills is also encouraged
under a nurse supervision so as to improve the treatment outcome (Futamura et
al., 2013; Grillo et al., 2006; Moore et al., 2009; Stabb et al., 2002; Stabb et al.,
2006).(1+, 1+, 1++, 1+, 1++).
84
Recommendation 3.0 Evaluation and Follow-‐up
3.1 It is suggested to evaluate the program by measuring SCORAD of the
clients at baseline before the program and after the program in order to
evaluate the change in SCORAD. (Grade A)
All the studies measure the baseline SCORAD at follow-‐up session and
calculate the change in severity after the program so as to evaluate the efficacy of
the proporsed program. (Futamura et al., 2013; Grillo et al., 2006; Moore et al.,
2009; Stabb et al., 2002; Stabb et al., 2006).(1+, 1+, 1++, 1+, 1++).
3.2 The length of follow-‐up is set to be one month and 3 month and one
year. (Grade A)
The length of follow up cannot be too long because the dropout rate is high
especially if the participants are in the control group which are having no
intervention. Among all selected studies, only one (Stabb et al., 2002) shown
more than 20% of dropout rate as the first follow-‐up is conducted at one year
after the education program.
85
References
Futamura, Masaki, et al. "Effects of a Short-Term Parental Education Program on Childhood Atopic Dermatitis: A Randomized Controlled Trial." Pediatric
dermatology 30.4 (2013): 438-443.
Moore, Elizabeth J., et al. "Eczema workshops reduce severity of childhood atopic
eczema." Australasian journal of dermatology 50.2 (2009): 100-106.
Grillo, Marianne, et al. "Pediatric atopic eczema: the impact of an educational
intervention." Pediatric dermatology 23.5 (2006): 428-436.
Staab, Doris, et al. "Evaluation of a parental training program for the management of
childhood atopic dermatitis." Pediatric allergy and immunology13.2 (2002): 84-90.
Staab, Doris, et al. "Age related, structured educational programmes for the
management of atopic dermatitis in children and adolescents: multicentre, randomised
controlled trial." Bmj 332.7547 (2006): 933-938.

86
Appendix 7: Level of Evidence Developed by the SIGN
1++ High-‐quality meta-‐analyses, systematic reviews of RCTs*, or RCTs with very low risk of bias
1+ Well-‐conducted meta-‐analyses, systemic reviews of RCTs, or RCTs with low risk of bias.
1-‐ Meta analyses, systematic reviews of RCTs, or RCTs with a high risk of bias.
2++ High quality systematic reviews of case-‐control or cohort studies.
High quality case-‐control or cohort studies with a very low risk of confounding, bias, or
chance and a high probability that the relationship is causal
2+ Well-‐conducted case control or cohort studies with a low risk of confounding, bias, or chance
and a moderate probability that the relationship is causal.
2-‐ Case control or cohort studies with a high risk of confounding, bias, or chance and a
significant risk that the relationship is not causal.
3 Non-‐analytic studies, e.g. case reports, case series
4 Expert opinion
RCT: randomized, controlled trial
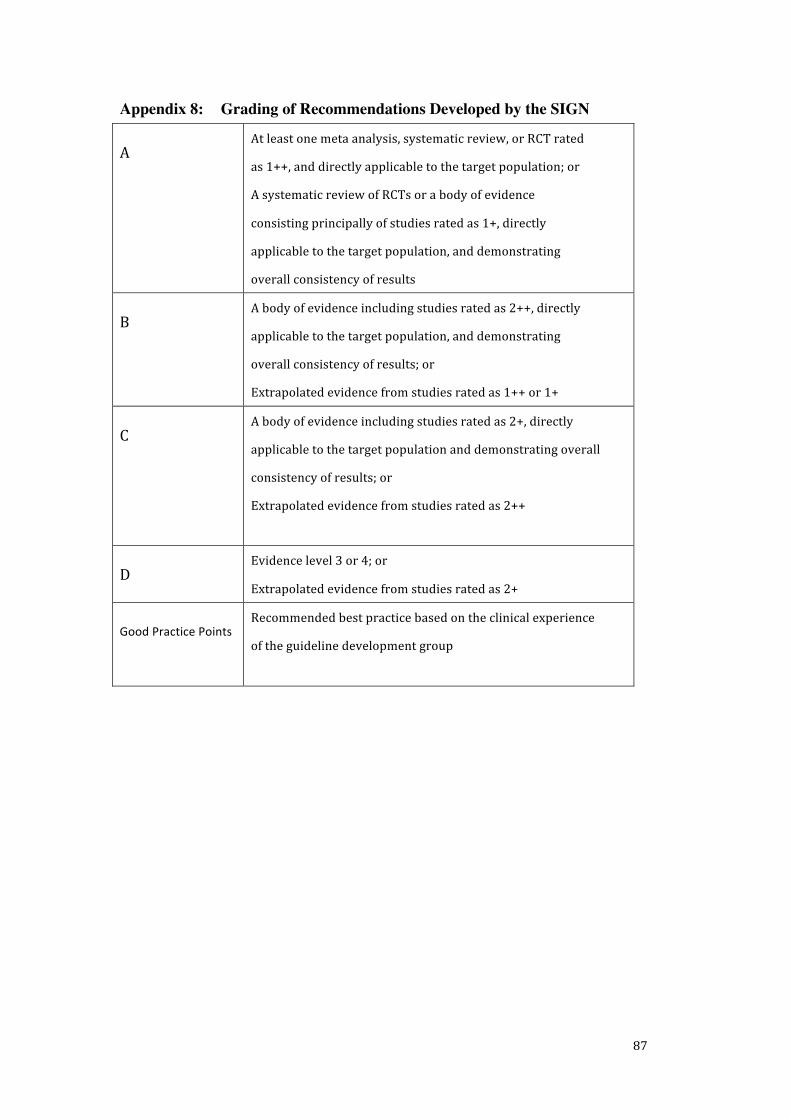
87
Appendix 8: Grading of Recommendations Developed by the SIGN
A At least one meta analysis, systematic review, or RCT rated
as 1++, and directly applicable to the target population; or
A systematic review of RCTs or a body of evidence
consisting principally of studies rated as 1+, directly
applicable to the target population, and demonstrating
overall consistency of results
B A body of evidence including studies rated as 2++, directly
applicable to the target population, and demonstrating
overall consistency of results; or
Extrapolated evidence from studies rated as 1++ or 1+
C A body of evidence including studies rated as 2+, directly
applicable to the target population and demonstrating overall
consistency of results; or
Extrapolated evidence from studies rated as 2++
D Evidence level 3 or 4; or
Extrapolated evidence from studies rated as 2+
Good Practice Points Recommended best practice based on the clinical experience
of the guideline development group

88
Appendix 9: Recommendation Synthesis Process
Recommendation 1.0 Who are the target population?
0-‐7 years old 8 – 12 years old 13-‐18 years old
Futamura et al.,2013 (1+) ✓
Grillo et al., 2006 (1+) ✓ ✓ ✓
Moore et al., 2009 (1++) ✓ ✓ ✓
Staab et al., 2002 (1+) ✓ ✓
Staab et al.,2006 (1++) ✓ ✓ ✓
Recommendation 2.1 Should the education conducted in the outpatient
clinic?
Out-‐patient clinic
Futamura et al.,2013 (1+) ✓
Grillo et al., 2006 (1+) ✓
Moore et al., 2009 (1++) ✓
Staab et al., 2002 (1+)
Staab et al.,2006 (1++)
Recommendation 2.2 Should the eczema workshop be carried out in a group
basis or individual session?
Group Individual
Futamura et al.,2013 (1+) ✓
Grillo et al., 2006 (1+) ✓
Moore et al., 2009 (1++) ✓
Staab et al., 2002 (1+) ✓
Staab et al.,2006 (1++) ✓
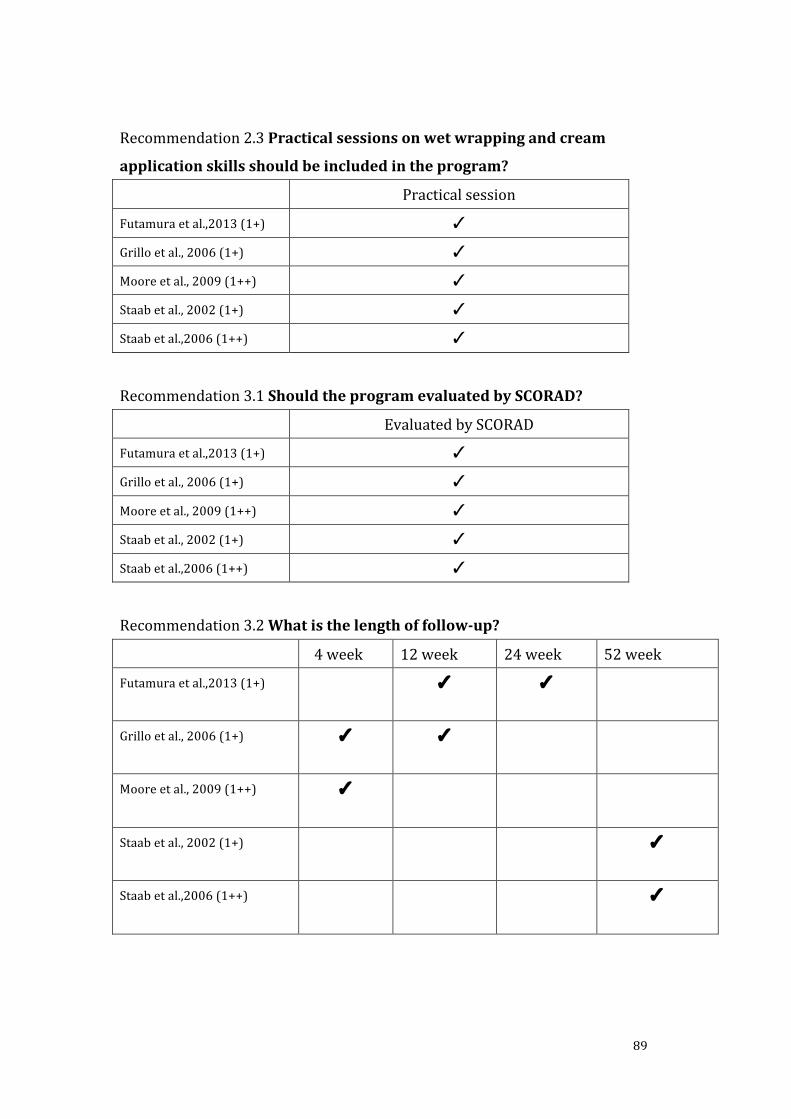
89
Recommendation 2.3 Practical sessions on wet wrapping and cream
application skills should be included in the program?
Practical session
Futamura et al.,2013 (1+) ✓
Grillo et al., 2006 (1+) ✓
Moore et al., 2009 (1++) ✓
Staab et al., 2002 (1+) ✓
Staab et al.,2006 (1++) ✓
Recommendation 3.1 Should the program evaluated by SCORAD?
Evaluated by SCORAD
Futamura et al.,2013 (1+) ✓
Grillo et al., 2006 (1+) ✓
Moore et al., 2009 (1++) ✓
Staab et al., 2002 (1+) ✓
Staab et al.,2006 (1++) ✓
Recommendation 3.2 What is the length of follow-‐up?
4 week 12 week 24 week 52 week
Futamura et al.,2013 (1+) ✓ ✓
Grillo et al., 2006 (1+) ✓ ✓
Moore et al., 2009 (1++) ✓
Staab et al., 2002 (1+) ✓
Staab et al.,2006 (1++) ✓

90
Appendix 10: Gantt Chart of The Education Program for The Eczematous Pediatric Patients
Month
Description
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Preparation of the
proposal and guideline
Approval seeking
Training session to
program team
Promotion +
Introductory Session to
pediatrician and nurses +
Participants Recruitment
Pilot Study
Evaluation of Pilot Study
Actual Implementation
Evaluation

91
Appendix 11: Scoring of Atopic Dermatitis Assessment Form

92
Appendix 12: Evaluation Questionnaire of the Education Program for
Pediatric Eczematous Patients
兒童濕疹護理課程問卷調查
非常不同意
不同意
無意見
同意 非
常同意
此課程可增加你對兒童濕疹的認識 此課程可增加你對兒童濕疹的護理 此課程可減少因兒童濕疹住院或覆診 課程長度適中 你滿意此課程 其他意見
*請在適當位置✔
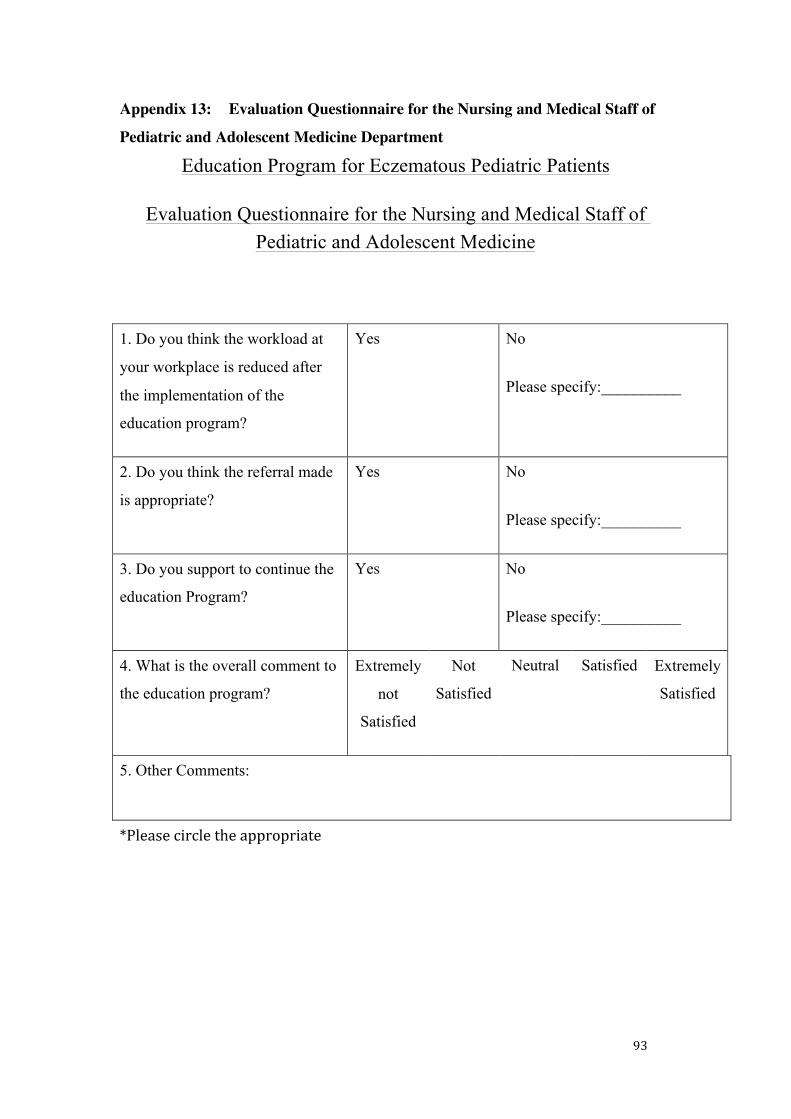
93
Appendix 13: Evaluation Questionnaire for the Nursing and Medical Staff of
Pediatric and Adolescent Medicine Department
Education Program for Eczematous Pediatric Patients
Evaluation Questionnaire for the Nursing and Medical Staff of Pediatric and Adolescent Medicine
1. Do you think the workload at
your workplace is reduced after
the implementation of the
education program?
Yes No
Please specify:__________
2. Do you think the referral made
is appropriate?
Yes No
Please specify:__________
3. Do you support to continue the
education Program?
Yes No
Please specify:__________
4. What is the overall comment to
the education program?
Extremely
not
Satisfied
Not
Satisfied
Neutral Satisfied Extremely
Satisfied
5. Other Comments:
*Please circle the appropriate
Related Documents











